#Sterilization
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr was acquired by Yahoo for $1.1B in 2013.
Text
Just a heads-up that if you're in the US and you never want to be pregnant, sterilization surgeries are currently 100% covered by insurance policies that are compliant to the Affordable Care Act. They are considered preventative care. Bilateral salpingectomy (removal of the fallopian tubes) is essentially 100% effective at preventing pregnancy, and it otherwise doesn't mess with your hormones. It also reduces rates of ovarian cancer by around 80%. This surgery is usually done laparoscopically and the recovery isn't too difficult. I had my surgery on a Thursday and went back to my desk job on Monday.
Bilateral salpingectomy doesn't affect periods, but I also had an endometrial ablation around a decade ago and it got rid of my periods. It can be done at at the same time as bilateral salpingectomy. People have mixed experiences with this, so do your research and talk to a doctor about it, but it may get rid of your period or at least make them much lighter/more tolerable.
If you're interested in sterilization, I would recommend having it done sooner rather than later, as I imagine conservatives are going to go after the Affordable Care Act as soon as they can (I have read that it's funded through the end of this year, but take that with a grain of salt), and sterilization may become a target in and of itself as well.
There's tons more detailed information at r/Sterilization, including a list of doctors who will sterilize people without children/younger people. I highly recommend reading up more there! Just wanted to give a PSA that sterilization is something you can do, it's currently free*, it's not too intense of a recovery process, and it's extremely effective. I'm elated I got it done and I want to empower other people to get it done if it'll give you peace of mind.
*Be careful and do your research first of course, insurance companies love trying to screw people out of their money, but it should be completely free if you're using providers that are in-network. Be sure to read about insurance coding, as it can affect what is/isn't covered. Also endometrial ablation might not be covered, so read up on that if you want to go that route as well.
#reproductive rights#reproductive health#us politics#sterilization#birth control#childfree#pro choice#antinatalism#tokophobia#health insurance#IDK what else to tag this as#I'm soooo glad to be sterile!!#I hope this will be helpful info to someone#go forth and get those tubes yeeted!!
210 notes
·
View notes
Text
LIST OF DOCTORS IN THE US WHO WILL PERFORM STERILIZATION IF YOU HAVE A UTERUS
Hello everyone- the following is a link to a Google doc containing hundreds of doctors in the US, Canada and Europe who are willing to perform sterilization on individuals who are 21+ regardless of marriage or parental status.
This list has existed for years and is a collaborative effort from patients all over the world to assist people in controlling their own fertility.
The document refers to tubal ligation, however they may offer other methods- for example, bilateral salpingectomy (aka “bisalp”) which is more effective and is becoming more popular with doctors than ligation.
If you know a doctor who performs this type of sterilization, and they are not on this list, please submit their name and location to the email provided at the top of the document.
PLEASE SHARE THIS WHEREVER YOU CAN.
The only thing we can control right now are the actions we take and the community we choose to build with each other.
220 notes
·
View notes
Photo
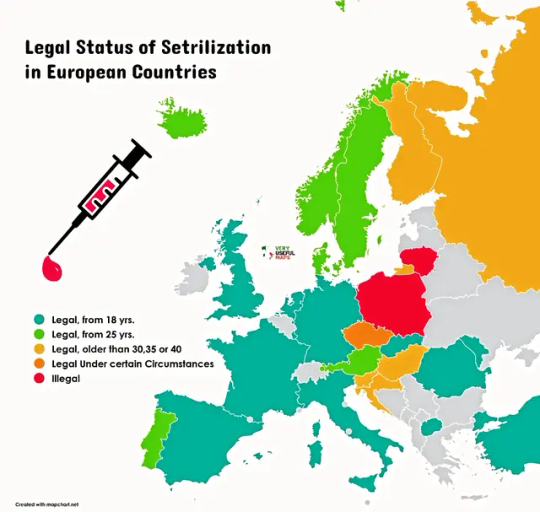
Legality of Contracęptive Stęrilizatįon in Europe
by very_useful_maps/instagram
85 notes
·
View notes
Text
Controversial opinion: I think if you want to sterilize yourself, you should be able to without any requirements. No one should have to have kids, be married, or be above a certain age. True autonomy is impossible to acheive without realizing this.
1K notes
·
View notes
Text
youtube
NEW VIDEO: STERILIZATION : Choice, Guilt and Necessity
Reproductive rights, generational trauma, and a history of violence against Indigenous women in Canada and the United States.
#ali nahdee#sterilization#native women#indigenous women#cultural genocide#reproductive rights#ICWA#roe v wade#Youtube
148 notes
·
View notes
Text
Women who may be considering sterilization after the election results, may I direct you to the r/childfree subreddit’s list of doctors who are supportive of this choice and will help you? It’s an amazing resource, organized by location/state.
I got sterilized earlier this year with a bilateral salpingectomy and I’m happy to share any info about the process (although I live in Canada so can’t tell you about American costs or insurance). It was a very quick, easy, safe surgery, and I’m deeply grateful every single day that I was able to make that choice for myself. Feel free to DM, send me an ask, or reblog if you want more info. Happy to help however I can.
#birth control#sterilization#project 2025#2024 election#feminism#bodily autonomy#women’s rights#reproductive rights#reproductive health#reproductive freedom#reproductive justice#childfree#planned parenthood#family planning
123 notes
·
View notes
Text
I've been spayed! My bilateral salpingectomy went fantastic and my surgical team was wonderful and affirming and even put on The National in the OR while I was getting settled because I said it was my favorite band. ❤️
I was so prepared for this to be a difficult fight but it was such a wonderfully powerful and affirming experience having a doctor who never doubted my choice and empowered me as an adult to make adult decisions about my body.
If anyone wants a rec for an incredible NYC-based gynecological surgeon, shoot me an ask. Or if you just have questions about the procedure, I'm happy to answer!
#sterilization#female sterilization#bilateral salpingectomy#childfree#the pain is pretty mild so far kinda like period cramps#not the BAD period cramps i get more like a normal day idk
124 notes
·
View notes
Text
How my now-sterilized ass sleeps at night knowing that I’m one of the millions of ‘selfish’ women “contributing to low birth rates”

38 notes
·
View notes
Text

By: Christina Buttons
Published: Apr 4, 2024
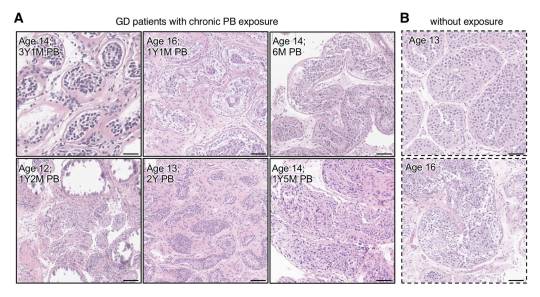
[ Figure 2: Representative images of Hematoxylin and Eosin-stained sections of testicular tissue biopsied from the testis from GD patients (A) with and (B) without PB exposure. ]
In a groundbreaking study from the Mayo Clinic, a globally recognized leader in medical research and patient care, researchers examined the effects of puberty blockers on testicular development in gender dysphoric male children. Their investigation revealed evidence of mild to severe atrophy in the sex glands of these children, leading the authors to express doubt in the claims of “reversibility” often made about puberty blockers.
The authors assert, “We provide unprecedented histological evidence revealing detrimental pediatric testicular sex gland responses to [puberty blockers].”
This preprint study, not yet peer-reviewed, presents evidence that puberty blockers induce significant cellular changes, impacting testicular development and sperm production in ways that are not fully reversible, with potentially permanent effects on testicular function and fertility. It challenges the longstanding view of puberty blockers as a reversible "pause button" on puberty.
As noted by the researchers of this study, no long-term studies exist for the use of puberty blockers in the context of stopping puberty for gender dysphoric children, and many potential health consequences remain unknown. In particular, the long-term impact on reproductive health is uncertain, making this study critical for filling this knowledge gap.
To address these unknowns, the Mayo Clinic has established the largest collection of testicular samples for patients aged 0-17 years, including those with gender dysphoria who have and have not yet received puberty blocker treatment, creating a database of over 130,000 individual cells for analysis.
Using a novel approach, the research team meticulously analyzed testicular tissue samples from youths undergoing puberty blocker treatment, with those not on puberty blocker treatment serving as controls. This comparison provides important insights into the potential cellular and molecular changes induced by these drugs.
Key Findings
The study utilized the Mayo Clinic's Pediatric Testicular Biobank for Fertility Preservation, which has been recruiting patients primarily from pediatric urology departments since 2015. Researchers analyzed testicular specimens from 87 young individuals (ages 0-17) undergoing fertility preservation surgery for various health reasons. Among these, 16 were gender dysphoric boys between the ages of 10 and 16, all of whom began identifying as transgender girls between the ages of 2 and 15. At the time of surgery, 9 patients (56%) were already on puberty blockers, with exposure ranging from 3 to 52 months. The authors noted that 100% of the 16 children would eventually go on to take them, highlighting “the widespread nature of PB intervention in this demographic.”
Among nine patients treated with puberty blockers, two exhibited unusual features in their testicles upon physical examination. One patient had abnormalities in both testicles, including incomplete development of the tunica albuginea, which is a protective covering around the testicles. The other patient had a right testicle that was difficult to detect.
In one part of the tissue-level analysis, over 400 testicular biopsy samples were analyzed and stained to examine the differences between those treated with puberty blockers and those who were not. Comparisons showed that testicular development in those treated with puberty blockers was abnormal compared to non-treated individuals. There was variability in how individuals responded to puberty blockers, leading to different outcomes in testicular development, including the degeneration of testicular tissues.
The study authors presented a case of a 12-year-old patient who underwent treatment with puberty blockers for 14 months. In this individual, 59% of the sex glands showed complete atrophy, along with the presence of microlithiasis—a condition where small clusters of calcium form in the testicles. This insight suggests that puberty blockers could lead to lasting structural changes. Additionally, research has shown a link between testicular microlithiasis and testicular cancer.

[ D) Representative images of normal (top) and fully atrophied sex gland (bottom). ]
This study also utilized single-cell analysis to investigate the effects of puberty blockers and aging on testicular cell composition. It took a very detailed look at individual cells from the testicles of a 14-year-old who had been on puberty blockers for over 4 years. The study analyzed a total of 130,100 cells, including 11,199 cells from the juvenile puberty blocker-treated patient.
The study observed that over 90% of the cells responsible for sperm production in this patient were stunted at an early developmental stage, unable to progress further. Additionally, it found "pathologically" higher and lower levels of two types of support cells (Sertoli cells) necessary for healthy sperm development. These findings suggest that puberty blockers can disrupt the normal maturation process of cells critical for sperm production.
In another part of the analysis, the authors found distinct cell-specific changes, including altered expression patterns of puberty-associated genes in endothelial cells, due to puberty blocker treatment. The authors believe that these drugs might induce juvenile testicular atrophy in part by disrupting the normal function of testicular endothelial cells.
Another aspect of the study focused on examining the effects of puberty blockers on the genetic activity of early-stage sperm cells, revealing significant changes that could potentially influence their development and fertility. By analyzing the activity of specific genes within these cells, the researchers found that puberty blockers may have caused alterations in gene expression, affecting processes crucial for the normal growth and function of these cells. This analysis suggests that the use of puberty blockers in gender dysphoric youth could have lasting implications for their reproductive health, particularly by impacting the ability of these early-stage sperm cells to mature properly.
Study Impact
Puberty blockers are increasingly used as a treatment for gender dysphoric youth to halt the development of secondary sex characteristics, such as breast development and widening of hips in females, or the growth of facial hair and deepening of the voice in males. Thousands of children in the United States are placed on this medical pathway as part of the gender-affirming model of care, under the presumption that these drugs are safe and fully reversible.
However, many aspects of the long-term consequences of puberty blockers, which have been administered to children off-label in an experimental manner, remain unknown. This study contributes valuable insights into the potential irreversible harm these treatments can cause to bodily and reproductive functions.
Arguably, the most critical finding is the evidence of mild to severe sex gland atrophy in children treated with puberty blockers. This atrophy signifies potential damage or impairment to the structures essential for sperm production, raising serious concerns about the long-term fertility impacts of these drugs for these individuals.
Given the Mayo Clinic's esteemed reputation in the medical and research communities, should the study pass peer review without any issues, its findings will carry significant weight.
Broader Implications
Puberty blockers belong to a group of synthetic gonadotropin-releasing hormone (GnRH) analogues. These drugs act on the pituitary gland to hinder the release of chemical signals that typically trigger the production of estrogen and testosterone. Historically GnRH analogues were used to treat conditions such as prostate cancer, fibroids, and endometriosis and, in some cases, as a measure to chemically castrate sex offenders.
In children, puberty blockers prevent the natural changes of puberty driven by sex hormones and have been used to treat central precocious puberty, a condition where a child begins to sexually mature much earlier than usual. In gender dysphoria, puberty blockers are administered experimentally, lacking long-term testing.
Notably, the U.S. Food and Drug Administration (FDA) has not approved puberty blockers and sex hormones for use in pediatric gender care. No clinical trials have substantiated the safety of these drugs for such non-approved applications and manufacturers of puberty blockers have repeatedly declined to conduct safety trials for their use on this cohort.
While puberty-blocking drugs are often promoted as “safe,” "reversible" and a "pause button" on puberty, these characterizations seem to stem from their approved use for treating central precocious puberty in younger children, not their burgeoning off-label use for managing gender dysphoria in adolescents.
Past studies have indicated possible negative effects on bone density and brain health. There is also a concern that these drugs might solidify gender dysphoria in adolescents, potentially leading them down a lifelong road of biomedical interventions. Following reports in 2016 of suicidal ideation in children administered puberty blockers, the FDA instructed drug manufacturers to include a warning about potential psychiatric issues on the drugs' labels.
Puberty blockers are increasingly administered to adolescents at Tanner Stage 2, the first signs of puberty. Research shows administering puberty blockers at this stage, followed by cross-sex hormones, may result in infertility, sterility, and sexual dysfunction. Furthermore, they inhibit the development of mature male genitalia, making it difficult to create a pseudovagina in the event of a later vaginoplasty due to a lack of sufficient tissue.
The National Health Service England recently announced it would no longer prescribe puberty blockers to youth outside of research settings and closed down its only national clinical service for pediatric gender medicine, following a review that deemed the service "not safe.”
Several European countries, including Sweden, Finland, the UK, Denmark, and Norway have updated their guidelines for youth transition to align with systematic evidence reviews, the gold standard in evidence-based medicine. These reviews concluded that the risks associated with youth transition outweigh any purported benefits. Consequently, these countries have implemented restrictions on medical interventions, prioritizing psychotherapy as a first-line response for minors experiencing gender-related distress.
==
They're sterilizing boys and giving them cancer. When "god" does it, we call him evil. When humans do it, we call it "gender affirming care."
#Christina Buttons#puberty blockers#atrophy#medical scandal#medical malpractice#medical corruption#sterilization#fertility#irreversible#gender affirming care#gender affirming healthcare#gender affirmation#queer theory#gender ideology#gender identity ideology#intersectional feminism#religion is a mental illness
238 notes
·
View notes
Note
Can fertility have something to do with gender identity, and can sterilization be a sort of medical transition? I'm nonbinary, and have always believed "I just am not the type of person who has kids." I don't feel strongly that being a woman is "wrong" for me, but being biologically able to bear children has caused dysphoria I've never even heard about before. It's not about fear, responsibility or physical changes. It's a personal boundary? I'm wondering if someone's thought of this, or if it's my place to make the call on whether this is a gender thing for me.
Sure. Fertility has often been tied to gender, so it makes sense that sometimes they overlap. I've seen and talked to people, including cis people, about how their fertility was intertwined with their gender and its almost always a very interesting discussion.
I honestly think it's more common than you'd think. Think of the amount of people who struggle with fertility and then mourn about feeling like they're not man/woman enough, etc. (Though obviously also that's got some complicated internalized/bigotry going on...)
I think it's definitely your call whether it's a gender thing. Its your gender, your fertility, you get to define how they intersect and all that.
I'm just saying if it is a gender thing for you, you're definitely not alone in that. I've met many a person who's wanted to be sterilized and it was connected to their gender [cis, trans, etc].
Hope this helps! Let me know if you have any other questions. <3
85 notes
·
View notes
Text






#black history#blacklivesmatter#black lives matter#black women#maternalhealth#fannie lou hamer#black people#racial injustice#sterilization#black health
43 notes
·
View notes
Note
and bitches how do I get sterilized (afab) i thought i might want kids in my 30s but i cant really risk it can i i just dont know what to do
Hi sweetness. I suspect a lot of people are in your boat right now. Personally, I got my first IUD implanted in January of 2017. NOTE THE TIMING. I also had a friend get her tubes tied around that time.
The most important thing to remember is that getting sterilized as an AFAB person is over 99% effective and pretty damn permanent. So if you think you just can't risk getting pregnant SOON, but you might want to SOME DAY... then don't get sterilized. Explore another option. Again, I have an IUD and thoroughly recommend it.
It's a fairly simple out-patient procedure, but as with any surgery, it comes with health risks. Sterilization for AMAB people is slightly less risky. Make sure to take all that into account.
So if you truly want to get sterilized, here's what I (a non-doctor) recommend:
The very first step is to make sure you have a primary care physician and health insurance. Your PCP is the one who will refer you for the surgery. Make an appointment and tell them this:
"I would like to be sterilized via a tubal ligation. I've carefully considered this for a long time, and after doing significant research and discussing it with my loved ones, I've determined it's the best decision for my future."
A lot of people get pushback from their doctors when they request sterilization. That's why you want to make it abundantly clear that this is not a sudden whim, but something you've put serious thought into. And married folks will sometimes be asked to clear it with their spouse first (that happened when my husband requested a vasectomy).
They might try to talk you out of it. They may flat out refuse to refer you. If this happens, just calmly say: "Thank you for your time. Since you won't help me with my healthcare needs, I will be seeking a new primary care physician at this time." Then get yourself a new doctor.
Under the ACA (the Affordable Care Act, aka Obamacare) the procedure will be completely free with your insurance. That's why it's important to make sure you have health insurance before you request the procedure. The Trump administration is sure to try repealing the ACA again (in his first term, John McCain was literally the deciding vote on overturning the ACA, and he's fucking dead now and congress is full of MAGA sycophants). So you need to work quickly in case your sterilization will no longer be covered.
I strongly recommend you seek more advice from healthcare professionals. @plannedparenthood is also a great resource for everything to do with reproductive healthcare. But this should help you get the ball rolling.
Good luck, my dear. Here's more of our advice:
How to Prepare for a Post-Roe World (Bonus Episode)
How To Get an Abortion
How (and Why) to Take Back Reproductive Rights: On Pulling Weeds and Fighting Back
Did we just help you out? Say thanks with a Patreon donation!
#sterilization#tubal ligations#get your tubes tied#prochoice#reproductive healthcare#reproductive rights
65 notes
·
View notes
Text
For anyone considering tying their tubes in light of today's news, here's a link to a nationwide, crowd-sourced list of doctors who are willing to perform sterilization.
65 notes
·
View notes
Note
Heyy
If you are comforable, can you talk about what the surgery meant? Like, was ut anything painful, were there complications, something unexpected?
I’m so so happy to answer questions about this and I hope if anyone is on the fence about it that I can give you some perspective if it helps to make a decision! I do want to wait a little longer and make a bigger post about it with some resources once I can confidently discuss the entire recovery and make sure all the billing gets sorted, but I can share some info now, too!
The surgery I had is called a Bilateral Salpingectomy, which is the removal of Fallopian tubes. A lot of providers are switching to this as the standard of care over doing a tubal ligation—my doctor doesn’t do tubal ligations at all anymore! I originally called and tried to make a consult to ask if one was better than the other to have her help me decide which one to do, but she doesn’t even do ligations anyway. Removing the tubes completely is also a HUGE reduction in the risk of ovarian cancer because most ovarian cancer starts in the Fallopian tubes.
You do keep your uterus and ovaries, so you’ll still get periods, and you won’t go into menopause or anything and if you’re a person who likes your ovary hormones you won’t have to take hormones. Everything still works down there, you just won’t have tubes letting eggs loose in your uterus! This also means that if you changed your mind you can still do IVF later in life if you want to carry a child.
If you’re in the United States and you have insurance, CHECK YOUR INSURANCE because this might be completely covered! If your plan is ACA compliant it’s required to cover sterilization as a form of birth control. There are some weird loopholes and we know that insurance will try to dick around and wiggle out of paying, but if everything is in place and it’s coded correctly you might even be able to have this surgery for free. There are TONS of resources and posts on Reddit that can help, and some info here from the National Women's Law Center (pardon the gendered language, my uterus bros!)
r/childfree on Reddit also has a huge directory of providers who will not give you a hard time about getting sterilized, since so many people have had to navigate doctors refusing to do it or making them jump through hoops if they’re too young or unmarried or whatever. One of the doctors on this list is in my insurance network so I gave her a call. I WAS A LITTLE WEIRDED OUT BECAUSE THE OFFICE WHERE SHE WORKS IS “FAITH BASED” AND THEY HAVE LIKE BIBLES AND PRAYERS ALL OVER THE PLACE???? But tbf that’s pretty common in my area and despite the creepy presence of Jesus in the gynecologist’s office, it was SO easy and she was so friendly and there was no hassle at all and she didn’t push back on me ONCE. I went in and she told me the whole process, answered some questions, and we got to scheduling right away.
From the time I called until the day of surgery it was about two months! I didn't need to do pre-op bloodwork because I had done it recently and my labs all looked fine last year, but I did have an appointment last month for an ultrasound because I had told my doctor about some issues I was having and she had offered to take a look in case there was anything that needed surgical intervention so that she could maybe do it while she was in there doing the bisalp lol, but I didn't need any extra surgery! 🥳
So far I didn’t have any complications and nothing unexpected! The surgery itself took about 45 minutes, and I was at the hospital for about 4 hours. I arrived two hours early to do paperwork and get prepped for surgery (cleaning the incision site, changing into the hospital gown, urine test, pre-op medication, IV, etc) and then I was in recovery for about an hour afterwards before I went home. I remember being awake and talking to the nurse and my sister-in-law and I remember looking at the clock and thought I was in recovery for like 30 minutes but then later on in the day she told me I had been awake for about an hour on and off but I kept falling back asleep. I was in a complete blackout LOL she told me all the stuff I was saying and the jokes I was making and I’m like, yeah that sounds like me LOL but I have ZERO recollection.
Basically they wheel you into the operating room, help you onto the table, and then they gave me some oxygen and asked me to take some deep breaths and next thing I know I’m waking up in recovery! Very easy on my end haha. I read that some people get really nauseous from anesthesia (and apparently the guy next to me was puking his guts out and I was commenting on it but I don’t remember LOL I feel so bad, I hope he didn’t hear me) but I was okay! When I woke up my stomach kinda hurt from the incisions but not in a nausea kinda way.
Mostly it’s just felt like a combination of bad period cramps and like, how your abs feel the day after a hard ab workout. My core is very tender and it’s hard to sit up and I’m trying to move slowly but I’ve been okay walking around and I was fine on the stairs and stuff!
My throat also felt scratchy from being intubated but I was just drinking fluid all day and that helps, and it burned the first time I peed because you get a catheter during surgery but otherwise that’s not an issue. Vaginal bleeding/spotting it also normal for the first couple days but it’s pretty light for me.
I work from home so I’m only taking 2 days off—I worked late on Monday and Tuesday this week so I only have a half day tomorrow to like check my emails and cover some stuff that I’m skipping while I’m out haha but time off work is going to vary depending on what you do. My doctor even told me I’d probably be okay going back to work today but I wanted to take an extra day just to be indulgent with myself. This probably wouldn’t be possible if I didn’t work from home, though, so your situation might not look like mine. I was told I shouldn’t drive my car for a week so I wouldn’t have been able to drive into the office.
Anyway this is something I wanted to do for a long time and honestly it was politics that pushed me to finally take action--I caved and made the consult appointment a couple weeks after the inaguration. The state I live in has made abortion almost impossible and there have been talks about the death penalty for people having abortions, and prosecuting people for leaving the state to have them done elsewhere. A lot of this is Overton window bullshit but it’s just too scary for me to risk. And honestly I’m at a point in my life where I’m not even sure how much interest I have in sex anymore but I am so worried about the potential of being assaulted and having to deal with a pregnancy on top of it, it’s just not worth it. I just really do not want to have to worry about it.
My insurance said they’ll pay for it 100% — there are still some loopholes I’m trying to figure out about my deductible and whatnot and no one is giving me a straight answer LOL but I’m willing to deal with the medical debt for the foreseeable future if I feel safe and just got it over with. The hospital sent me an estimate for like $10,000 LMAO but I think they just plugged the codes into a generator because my insurance said that wasn't correct and that as long as it's coded as being preventative birth control that it will be fine. I am really really feeling very concerned about the future of the ACA and the birth control mandate and reproductive rights so I wanted to get it done while I’m still legally able to, because I wouldn't be surprised if this gets rolled back.
So if you’ve been considering this like please look into getting it done! Check the Reddit list to see if there’s anyone in your area you can talk to for a consult and check if your insurance will take care of it! Not all insurance plans are ACA compliant but if you have an ACA compliant plan you shouldn't have a problem! And if you’re like me and you’ve known you never wanted kids but you just haven’t gotten around to taking measures, it might be wise to just get it done now while we’re still allowed to!!!
28 notes
·
View notes
Text
I can’t believe I actually am sterilized now. It feels so surreal but then I look at my incisions and I get all giddy that I have this lasting control over my own body.
42 notes
·
View notes
Text
A Senate committee studying a bill to establish a criminal offence with respect to sterilization procedures heard emotional testimony from a survivor of coerced sterilization on Thursday.
"It's like you wiped out a generation," Nicole Rabbit, a member of Survivors Circle for Reproductive Justice, an organization for Indigenous women who are survivors of coerced and forced sterilization, told the committee in Ottawa.
Bill S-250 an Act to Amend the Criminal Code (sterilization procedures) would make forced and coerced sterilization punishable under the Criminal Code by up to 14 years in prison.
Full article
Tagging: @politicsofcanada
#cdnpoli#canada#canadian politics#canadian news#canadian#bill s-250#forced sterilization#coerced sterilization#sterilization#Indigenous#genocide#reproductive rights#reproductive health#reproductive justice#bodily autonomy#senate
210 notes
·
View notes