#Bilateral Pleural Effusion
Text
“Madame A, 38” (France ~1975)
A woman identified only as “Mme. A” in a medical journal was killed by a legal abortion in France, reported at the end of the year that abortion was legalized essentially on demand. She was six weeks pregnant when she went to an abortionist only identified in the medical journal as “Dr. X.”
Mme. A’s pre-op examination showed no health problems. As a precaution, she was prescribed antibiotics in advance. She was led to believe she was in the hands of an expert, who claimed to have carried out over 1,400 abortions without complications. However, this claim would soon prove to be suspicious given what he failed to recognize.
The aspiration abortion was done in only three minutes with no anesthesia. Nobody noticed even the slightest anomaly and Mme. A was discharged from the abortion facility two hours later. Dr. X. reported that she wasn’t in pain even though she herself said that she was, albeit that the pain wasn’t severe at that point and she wasn’t worried.
Over the next two days, Mme. A’s pain increased. On the third day, she got a referral for a different doctor. This doctor observed her for a few hours and then performed emergency surgery, realizing the condition she was in.
Dr. X. had failed to notice even the slightest anomaly during the abortion or any pain after it, but he had inflicted serious injuries. He had torn a hole through Mme. A’s uterus, then perforated her small intestine through the hole. She was now suffering generalized peritonitis and needed a resection of the small intestine along with drainage for abscesses.
The day after her emergency surgery, Mme. A worsened. She was developing dypsnea and large bilateral hemorrhagic pleural effusions. On the fifth day, she was admitted to the ICU at Antoine-Béclère Hospital. She was under constant intensive care for 15 days, but this was further complicated by pulmonary embolism and digestive bleeding from stress ulcers. Just as her condition seemed to be somewhat under control, she suffered a recurrence of the pulmonary embolism. She died on her 16th day in Intensive Care, leaving a 10-year-old and a 9-year-old without their mother.
The medical journal that documented Mme. A’s death labeled her course of complications as “unfortunately classic” when operating on a patient with peritonitis, partial evisceration, pulmonary embolism, abscesses and internal bleeding. It was noted in the review of her case that suction abortion is a surgical operation and should not be treated as trivial. It was recommended that abortion clients be monitored in a real hospital setting for 2 to 3 days afterwards. The surgery department of the hospital submitting Mme. A’s case stated that, “the official and even legislative publicity of the safety of the method also has a certain responsibility in our eyes.” Even though it was now legal and done by a self-proclaimed “expert,” abortion was still not a safe operation or one to be taken lightly.
#tw abortion#pro life#unsafe yet legal#tw ab*rtion#unidentified victim#tw murder#abortion#abortion debate#death from legal abortion#tw malpractice#tw negligence#tw death
7 notes
·
View notes
Text

A nursing-home patient was intubated in the field for respiratory distress and hypoxia. On arrival, breath sounds were decreased on the left during ETT (endotracheal tube) verification. His sat on 100% oxygen with the ETT is 98%. A CXR is done. What do we do next?
--
The CXR shows white-out of the left lung. There are four possible causes - (1) the ETT is malpositioned (right main-stem bronchus, typically) and the left lung isn’t aerated, (2) large pleural effusion, (3) complete infiltration of the left lung (pneumonia or bleeding), and (4) obstruction of the left airways by mucus, cancer / mass, or food. All four problems can happen at once.
The first thing to check is to see where the ETT is on the CXR. You can see that it is correctly positioned above the carina. If the ETT is in the right main-stem, pull the ETT back and repeat a CXR. You can also see an air bronchogram in the left lung field, suggestive of pneumonia. A CT scan shows bilateral effusions and alveolar infiltrates with partial collapse of the left lung. The patient needs a bronchoscopy, which showed severe mucus plugging. After removing the obstructions, a repeat CXR looks better.
--


5 notes
·
View notes
Text
So like I used to struggle really badly with alcoholism and it could've killed me. I had alcoholic ketoacidosis multiple times, alcoholic hepatitis, malnutrition (which almost turned to refeeding syndrome in the hospital), and withdrawals. Then when I got sober I had gallstones which blocked bile ducts and caused further liver problems, acute pancreatitis, and bilateral pleural effusion. I also have a congenital heart disorder which increases my chance of sudden cardiac arrest. And I've been suicidally depressed since the age of 12.
In one week, I turn 27. You know what that means!
0 notes
Note
I'm a mother with metastatic (stage ll) breast cancer with a 10-month-old daughter who was born with cerebral palsy.that my life has been in recent years, thank you for coming this far and giving me all your support, for those who do not know the hard battle I face and for which I try to reach their hearts. . . . . In search of support I briefly tell you my situation.
My name is maua, 5 years ago I was driving to meet my best friend, suddenly my vision was double, my vision was going in and out, I remember pulling into a parking lot, I just thought to call someone, but I couldn't dial from my phone , I lost consciousness, when I woke up I couldn't coordinate or make rational decisions, I woke up repeating over and over again that I had to go home, by then I thought I had the flu with a very bad headache, the doctors came and one of They told me that I had bronchitis and sinusitis, a month later the symptoms had not disappeared, by then I had already gone to the specialist for the third time. After much concern, finally a doctor ordered a chest x-ray because the x-rays showed that I had a pleural effusion in my right lung, other doctors objected saying that it was not necessary, days later while I was taking a shower I found a lump in my breast, after rigorous examinations they ended up diagnosing me with metastatic breast cancer. I then had chemotherapy and a bilateral mastectomy (removal of both breasts), reconstructive surgery, and implant placement.
Harvesting or freezing my eggs before the chemo was not an option, they said that there was a high probability that the chemo would affect my fertility, this shattered my illusions because I really dreamed of being a mother. After the surgery I was considered cancer free, 4 years later I got pregnant, in February 2022 I gave birth to my little Elly, the delivery was complicated, my pregnancy was traumatic due to my history of cancer, my little love of 3 pounds and 6 ounces was born 10 weeks early. Elly was born with cerebral palsy, during the pregnancy I had several threats of abortion, by the mercy of God my baby grabbed my uterus tightly, she cannot breastfeed her, but I am content with having her on my chest and giving her warmth and protection as much as I can, Its care is special, it requires rigorous treatments and it is not cheap. I always refused to ask for help with my cancer, but seeing my baby so delicate and defenseless I understood that I need everyone, these are difficult times, we have a very hard road ahead of us at home, my daughter needs all the help possible.
I lived a life in remission for almost 5 years before developing a bad cough during flu season, a few months after giving birth I felt like everything was wrong, made several doctor visits, had a chest X-ray due to my history , they found fluid in my lungs, after draining and analyzing it, it was evidenced that there were breast cancer cells, after more cancer tests it was found not only in my lungs, but in my liver and bones, at the age of 33 I was diagnosed with metastatic breast cancer (stage Il) a few years later I found out that the cancer had invaded my brain as well.
However, today I am stable and most of the cancer is gone, but I am still on continuous treatment that I am not allowed to stop. Since my cancer was found I have had 57 chemo infusions, 10 IM injections, countless Il/port sticks, too many pills to count, 1 pleurx drain to my lung, 4 JP drains, x2 thoracentesis, 9 surgeries, 2 interventional radiology procedures , 1 biopsy, 1 mammogram, 2 x-rays, 2 ultrasounds, 6 hospitalizations, plus ED visits, 17 CT scans, 3 CT scans, 20 MRIs, 2 bone scans, palliative radiation, 1 seizure, 7 gamma knife treatments, 1 craniotomy , 8 doctors/surgeons, countless amazing nurses, NPs PAs, lots of scars, and thousands of dollars in medical bills and counting. However, I am here with a beautiful gift from God in my arms, this can only be called a miracle, God wants me here and I must fight for it and my little girl needs me.
please help me with anything you want to help me
im not able to donate but i will share, i hope your get the money you need, you went through alot :(
1 note
·
View note
Note
I'm a mother with metastatic (stage ll) breast cancer with a 10-month-old daughter who was born with cerebral palsy.that my life has been in recent years, thank you for coming this far and giving me all your support, for those who do not know the hard battle I face and for which I try to reach their hearts. . . . . In search of support I briefly tell you my situation.
My name is maua, 5 years ago I was driving to meet my best friend, suddenly my vision was double, my vision was going in and out, I remember pulling into a parking lot, I just thought to call someone, but I couldn't dial from my phone , I lost consciousness, when I woke up I couldn't coordinate or make rational decisions, I woke up repeating over and over again that I had to go home, by then I thought I had the flu with a very bad headache, the doctors came and one of They told me that I had bronchitis and sinusitis, a month later the symptoms had not disappeared, by then I had already gone to the specialist for the third time. After much concern, finally a doctor ordered a chest x-ray because the x-rays showed that I had a pleural effusion in my right lung, other doctors objected saying that it was not necessary, days later while I was taking a shower I found a lump in my breast, after rigorous examinations they ended up diagnosing me with metastatic breast cancer. I then had chemotherapy and a bilateral mastectomy (removal of both breasts), reconstructive surgery, and implant placement.
Harvesting or freezing my eggs before the chemo was not an option, they said that there was a high probability that the chemo would affect my fertility, this shattered my illusions because I really dreamed of being a mother. After the surgery I was considered cancer free, 4 years later I got pregnant, in February 2022 I gave birth to my little Elly, the delivery was complicated, my pregnancy was traumatic due to my history of cancer, my little love of 3 pounds and 6 ounces was born 10 weeks early. Elly was born with cerebral palsy, during the pregnancy I had several threats of abortion, by the mercy of God my baby grabbed my uterus tightly, she cannot breastfeed her, but I am content with having her on my chest and giving her warmth and protection as much as I can, Its care is special, it requires rigorous treatments and it is not cheap. I always refused to ask for help with my cancer, but seeing my baby so delicate and defenseless I understood that I need everyone, these are difficult times, we have a very hard road ahead of us at home, my daughter needs all the help possible.
I lived a life in remission for almost 5 years before developing a bad cough during flu season, a few months after giving birth I felt like everything was wrong, made several doctor visits, had a chest X-ray due to my history , they found fluid in my lungs, after draining and analyzing it, it was evidenced that there were breast cancer cells, after more cancer tests it was found not only in my lungs, but in my liver and bones, at the age of 33 I was diagnosed with metastatic breast cancer (stage Il) a few years later I found out that the cancer had invaded my brain as well.
However, today I am stable and most of the cancer is gone, but I am still on continuous treatment that I am not allowed to stop. Since my cancer was found I have had 57 chemo infusions, 10 IM injections, countless Il/port sticks, too many pills to count, 1 pleurx drain to my lung, 4 JP drains, x2 thoracentesis, 9 surgeries, 2 interventional radiology procedures , 1 biopsy, 1 mammogram, 2 x-rays, 2 ultrasounds, 6 hospitalizations, plus ED visits, 17 CT scans, 3 CT scans, 20 MRIs, 2 bone scans, palliative radiation, 1 seizure, 7 gamma knife treatments, 1 craniotomy , 8 doctors/surgeons, countless amazing nurses, NPs PAs, lots of scars, and thousands of dollars in medical bills and counting. However, I am here with a beautiful gift from God in my arms, this can only be called a miracle, God wants me here and I must fight for it and my little girl needs me.
please help me with anything you want to help me
💙
0 notes
Note
I'm a mother with metastatic (stage ll) breast cancer with a 10-month-old daughter who was born with cerebral palsy.that my life has been in recent years, thank you for coming this far and giving me all your support, for those who do not know the hard battle I face and for which I try to reach their hearts. . . . . In search of support I briefly tell you my situation.
My name is rebecca, 5 years ago I was driving to meet my best friend, suddenly my vision was double, my vision was going in and out, I remember pulling into a parking lot, I just thought to call someone, but I couldn't dial from my phone , I lost consciousness, when I woke up I couldn't coordinate or make rational decisions, I woke up repeating over and over again that I had to go home, by then I thought I had the flu with a very bad headache, the doctors came and one of They told me that I had bronchitis and sinusitis, a month later the symptoms had not disappeared, by then I had already gone to the specialist for the third time. After much concern, finally a doctor ordered a chest x-ray because the x-rays showed that I had a pleural effusion in my right lung, other doctors objected saying that it was not necessary, days later while I was taking a shower I found a lump in my breast, after rigorous examinations they ended up diagnosing me with metastatic breast cancer. I then had chemotherapy and a bilateral mastectomy (removal of both breasts), reconstructive surgery, and implant placement.
Harvesting or freezing my eggs before the chemo was not an option, they said that there was a high probability that the chemo would affect my fertility, this shattered my illusions because I really dreamed of being a mother. After the surgery I was considered cancer free, 4 years later I got pregnant, in February 2022 I gave birth to my little Elly, the delivery was complicated, my pregnancy was traumatic due to my history of cancer, my little love of 3 pounds and 6 ounces was born 10 weeks early. Elly was born with cerebral palsy, during the pregnancy I had several threats of abortion, by the mercy of God my baby grabbed my uterus tightly, she cannot breastfeed her, but I am content with having her on my chest and giving her warmth and protection as much as I can, Its care is special, it requires rigorous treatments and it is not cheap. I always refused to ask for help with my cancer, but seeing my baby so delicate and defenseless I understood that I need everyone, these are difficult times, we have a very hard road ahead of us at home, my daughter needs all the help possible.
I lived a life in remission for almost 5 years before developing a bad cough during flu season, a few months after giving birth I felt like everything was wrong, made several doctor visits, had a chest X-ray due to my history , they found fluid in my lungs, after draining and analyzing it, it was evidenced that there were breast cancer cells, after more cancer tests it was found not only in my lungs, but in my liver and bones, at the age of 33 I was diagnosed with metastatic breast cancer (stage Il) a few years later I found out that the cancer had invaded my brain as well.
However, today I am stable and most of the cancer is gone, but I am still on continuous treatment that I am not allowed to stop. Since my cancer was found I have had 57 chemo infusions, 10 IM injections, countless Il/port sticks, too many pills to count, 1 pleurx drain to my lung, 4 JP drains, x2 thoracentesis, 9 surgeries, 2 interventional radiology procedures , 1 biopsy, 1 mammogram, 2 x-rays, 2 ultrasounds, 6 hospitalizations, plus ED visits, 17 CT scans, 3 CT scans, 20 MRIs, 2 bone scans, palliative radiation, 1 seizure, 7 gamma knife treatments, 1 craniotomy , 8 doctors/surgeons, countless amazing nurses, NPs PAs, lots of scars, and thousands of dollars in medical bills and counting. However, I am here with a beautiful gift from God in my arms, this can only be called a miracle, God wants me here and I must fight for it and my little girl needs me.
please help me with anything you want to help me
donate via PayPal is all I have
funniest scam I ever read
0 notes
Text
Tuberculosis and Infertility
Tuberculosis and Infertility
Chronic infections like tuberculosis (TB) may cause damage to the reproductive systems of both men and women, affecting both reproduction and hormone production. While the course of multiplication is restricted to the exhibition of the genital plot, a dysfunction in the production of hormones might have expansive results all over the body. This can occur as a result of the dynamic sickness, however, may likewise go on in its idle or lethargic state.
Female reproductive changes
Genital tuberculosis may be found in high-risk groups, such as infertile individuals; repetitive unnatural birth cycles; ectopic conceptions; irregular menstruation, such as amenorrhea, oligomenorrhea, and menorrhagia; adnexal mass persistent pelvic torment; TB history in the family; and previous TB history.
Around 20% of patients with genital TB have a family background of TB in a close relative. Approximately 30%–40% of those questioned provide evidence of prior pleural effusion, peritonitis, osseous, lymph node, or pulmonary TB. TB may be the cause of infertility associated with an adnexal mass in 39% of cases. In the majority of cases, the fallopian tubes are the likely site of the initial infection, and bilateral involvement is common. Hydrosalpinx and tubercular salpingitis are well-known and proven causes of infertility.
Between 50 and 70 percent of cases involve the uterus, mostly the endometrium and occasionally the myometrium. Asherman’s syndrome-related amenorrhea and oligomenorrhoea are also known entities. In between 20% and 30% of cases, the ovaries may be involved. This large number of states can prompt extremely durable deformation of the genital lot and loss of fertility.
Male Reproductive changes
Infertility occurs because genital TB in men is damaging in nature, with scarring and fibrosis that might persevere even after successful clinical administration. Granulomatous masses in the acute phase, fibrosis, and scarring as the disease progresses, or after treatment typically obstruct the epididymis and vas.
On local examination, a bilaterally enlarged nodular epididymis and vas deferens, which may or may not have formed sinuses, are indicative of TB. Semen parameters may reveal obstructive azoospermia, azoospermia, or severe oligospermia with normal volume fructose-positive ejaculate in cases of isolated epididymal or vas involvement. The hormonal profile and spermatogenesis are normal in such instances.
Contrarily, tubercular scarring of the prostate, seminal vesicle, and ejaculatory ducts will clinically present as low-volume, fructose-negative ejaculate, emulating obstruction in these structures. An unexplained decrease in the volume of ejaculation associated with azoospermia and progressing to aspermia may also be a sign of male genital TB.
The majority of these patients have multifocal obstruction, for which assisted reproduction is preferable to surgical intervention. Ejaculatory duct obstruction with non-distended atrophic seminal vesicles is the diagnostic sign of tuberculosis.
Assisted Reproduction
Female patients with Asherman’s syndrome blocked fallopian tubes, or diminished ovarian reserve may benefit from assisted reproduction. In male patients, helped proliferation is demonstrated by oligoasthenoteratozoospermia, ongoing prostatitis, epididymitis, or obstructive azoospermia.
Ejaculatory channel block with atrophic original vesicles is analytic of TB; Assisted reproduction may be their only option for conception because the majority of these patients have a multifocal obstruction that prevents surgical reconstruction.
Pregnancy rates in IVF appear to rely on the seriousness of the illness and are better if the sickness is analyzed early. Poor ovarian response, poor oocyte quality, and a hostile uterine environment are all blamed for poor outcomes, according to reports. As a result, it may be necessary for many patients to use surrogacy or oocyte donation as a form of third-party reproduction.
0 notes
Text
Diagnostic value of pleural Fluid Adenosine deaminase in patients with Pleural Tuberculosis by Sina Parsay M.D in Journal of Clinical Case Reports Medical Images and Health Sciences

ABSTRACT
Background and Objectives: Extra-pulmonary tuberculosis occurs in about 10-20% of patients with tuberculosis. It most commonly manifests as tuberculous lymphadenitis or pleural effusion. Pleural fluid Adenosine deaminase (ADA) activity considered as a useful biomarker for detecting pleural tuberculosis. The purpose of this study was to evaluate the diagnostic accuracy of pleural fluid adenosine deaminase level in patients with pleural tuberculosis.
Methods: In this study, 113 patients with exudative pleural effusion with unknown underlying diagnosis, were enrolled. Physical examination, chest CT, ADA level of pleural fluid, direct thoracoscopic examination, and biopsy of pleura were obtained for all individuals. ADA level and thoracoscipoc appearance of the lesions was then compaierd among the patients with regard to the pleural biopsy report as the diagnostic goldstandard.
Results: The diagnosis of tuberculous pleurisy was established in 40 individuals based on the pathology reports. The mean ADA level of the TB and the non-TB group was 39.90±22.93 IU/L and 30.74±38.27 IU/L, respectively (P-value=0.167). Sensitivity, specificity, positive predictive value, and negative predictive value of ADA test were 35%, 86.30%, 58.33%, and 70.79%, respectively.
Conclusion: Based insuffiecient sensitivity and specificity of ADA, in patients with unexplained exudative pleural effusion especially in those with a high suspicion of tuberculous pleurisy, despite the low level of ADA, direct thoracoscopic pleural evaluation with obtaining multiple biopsies of pleura is highly recommended.
Keyword: Pleural Effusion, Thoracoscopy, Tuberculosis, Diagnostic Accuracy, Extra-pulmonary tuberculosis, Adenosine deaminase
INTRODUCTION
Tuberculosis is a chronic bacterial infection caused by Mycobacterium tuberculosis. It remains a disease with a high rate of mortality in the world especially in developing and low-income countries 1. Extrapulmonary tuberculosis occurs in about 10% -20% of patients and the most common forms of involvement are tuberculous Lymphadenitis and tuberculous pleural effusion 2.
Pleural tuberculosis (TB) which is the topic of this study, is characterized by symptoms such as chest pain, cough, and fever. Chest Radiography of these patients shows a small to moderate unilateral pleural effusion which is lymphocyte dominant in serologic evaluations. The condition also could be bilateral within the minority of cases 1, 3. The prevalence of tuberculosis among all patients with pleural effusion is between 4-22%, and pleura is involved in 3-23% of patients with tuberculosis 4, 5.
Different diagnostic methods have been used to diagnose pleural tuberculosis, including thoracentesis, measurement of serum and pleural fluid adenosine deaminase (ADA) level, pleural biopsy, and thoracoscopy assisted pleural examination and biopsy 3.
Measuring ADA activity in pleural fluid is an easy, inexpensive, fast, and useful way for diagnosing TB in endemic areas, such as South Africa, Asia, Brazil, Spain, and Eastern Europe 6-8. Based on literature a cut-off point of 40 U/L of ADA activity in a lymphocyte dominant pleural fluid is diagnostic for pleural TB. But the validity of the test is not generally accepted by consensus 9-11
With the advancement in endoscopic techniques and video equipment, thoracoscopy has been suggested as a diagnostic and therapeutic modality in patients with pleural tuberculosis, and become more popular among the physicians. Thoracoscopic findings of these patients include caseous necrosis, miliary nodules, exudative pleural effusion, and pleural adhesion or fibrotic septa 12-14.
Considering the important role of ADA in the diagnosis of pleural tuberculosis, evaluating the correlation between pleural ADA level and thoracoscopic findings of pleural tuberculosis seems necessary
15, 16.
This study aims to determine the correlation of the pleural fluid ADA activity and its diagnostic accuracy in histologically confirmed cases of pleural tuberculosis.
MATERIALS AND METHODS
In this cross-sectional study, 113 patients from those who referred to the cardiothoracic surgery department of Tabriz University of Medical Science with unexplained exudative pleural effusion were enrolled. The study population was measured by GPOWER software with a confidence interval of 95% and a test power of 80%. All patients had a pleural effusion with unknown etiology and candidated for thoracoscopy and biopsy. Patients were excluded from the study in case of transudative pleural effusion, post-traumatic effusion, known pulmonary disorders, history of pulmonary or pleural malignancies, and history of radiotherapy on the thoracic cavity.
All patients underwent thoracoscopic study with direct evaluation of the pleural cavity. Multiple pleural biopsies and pleural fluid specimen for ADA analysis were obtained. All tissue samples were evaluated by a certain pathologist and ADA was measured using ADA Reagent Kit in an acredited laboratory of the affiliated university. The ADA level of greater than or equal to 40 U/L considered as diagnostic for TB. According to the pathologic reports, patients were divided into two TB and non-TB groups. The demographic data, examination and thoracoscopic findings, as well as ADA levels were compared between two groups.
Data were collected and analyzed by IBM SPSS statistic for windows version 23.0. (IBM Corp., Armonk, N.Y., USA). Descriptive data were reported using mean, standard deviation, relative, and absolute frequencies. Chi2, paired sample t-test, independent t-test. and repeated measure ANOVA were used for analytical comparison of the variables between the groups as needed. The p-value of less than 0.05 was considered statistically significant. Sensitivity and specificity were calculated based on patient-level analysis of gathered data using confusion matrix and relying on pathologic results as the gold standard diagnostic test.
ETHICAL CONSIDERATION
The study was approved by the ethics committee of Tabriz University of Medical Science under the approval number of 5/d/8716-94/5-6/3. All diagnostic and therapeutic interventions were performed regarding the routine management of patients; no additional intervention or cost was imposed on participants in this study. Patients’ data were recorded as encoded variables without mentioning the name of any participant. None of the patients' personal information was included in this research.
Informed consent was obtained from each participant; nevertheless, patients were excluded from the study in cases they were reluctant to participate in the study.
RESULTS
Of the total 113 patients, 73 (58.4%) were male, and 40 (32.0%) were female, and 42 (33.6%) were smokers. The mean age of the patients was 49.77 ± 18.71 years.
The diagnosis of TB was confirmed in 40 patients according to the histopathologic reports. These patients were stratiffied as the case group (known as group A), and the other 73 with a diagnosis of nontuberculous pleural effusion were considered as the control group (known as group B).
As depicted in Table-1 dyspnea, cough, and pleuritic chest pain were the dominant symptoms of patients at the time of admission with a frequency of 66.37%, 48.67%, and 40.7% respectively. The frequency of fever and weight loss were30.97%, and 28.31%, respectively among the patients. Table-1 also demonstrates demographic data of individuals separately for each study groups.
Regarding the thoracoscopic examination, pleural effusion, pleural adhesion band, miliary nodules, and caseous necrosis were found in 100%, 67.5%, 70%, and 60%, of the group A respectively (Table-2). Among the control group (group B), pleural effusions, thickening of pleura and miliary nodules were the dominant manifestations with a frequency of 100%, 46.57%, and 30.13% respectively (Table-2). The underlying cause of pleural effusion among the patients in control group was: metastasis (23.28%), mesothelioma (5.47%), inflammation (32.87%), fibrosis (36.98%), and fungal infection (1. 36%) as depicted in Table-2.
The mean ADA level was 39.90 ± 22.13 IU/L in group A and 30.74 ± 38.27 IU/L within group B individuals which did not differ statistically significantly between the two study groups (p=0.167).
As delineated in Table-3, 35% of patients in group A has ADA level of greater than 40 (as a diagnostic cut-off for TB) compared to 13.7% in group B (p>0.05). Bar chart for these amounts is also illustrated in figure-1. Sensitivity, specificity, positive predictive value, and negative predictive value of ADA test were measured 35%, 86.30%, 58.33%, and 70.79% respectively (Table-4). Figure-2 demonstrates the ROC curve of ADA test measures.
Figure 1: Chest X-ray reveals pulmonary edema after ICU admission
Figure 1: Chest X-ray reveals pulmonary edema after ICU admission
Figure 1: Chest X-ray reveals pulmonary edema after ICU admission
After 24h of fully controlled mechanical ventilation and 6800ml of diuresis the sedation medication was terminated and the patient extubated uneventfully. No further ventilation support or vasoactive medication was required. The patient recovered in the matter of 72 hours and was discharged from the hospital on the day 7 with a mild arterial hypertension, that was treated by Hydrochlorthiazide 25mg a day.
After 24h of fully controlled mechanical ventilation and 6800ml of diuresis the sedation medication was terminated and the patient extubated uneventfully. No further ventilation support or vasoactive medication was required. The patient recovered in the matter of 72 hours and was discharged from the hospital on the day 7 with a mild arterial hypertension, that was treated by Hydrochlorthiazide 25mg a day.
DISCUSSION
In this study, 113 patients (73 males and 40 females) with unexplained pleural effusion were evaluated for probable pleural tuberculosis by using thoracoscopic examination and biopsy. Meanwhile, the ADA level was measured for all individuals regardless of pathologic findings. The diagnosis of pleural TB established only in 40 individuals according to the histopathologic reports. The ADA level among these tuberculous pleurisy patients was 39.90 ± 22.13 IU/L compared to a level of 30.74 ± 38.27 IU/L in nontuberculous individuals, which was not statistically significant. Based on our results, the ADA test yield a sensitivity, specificity, positive predictive value, and negative predictive value of 35%, 86.30%, 58.33%, and 70.79% respectively.
In a study performed by Van et al., the causes of pleural effusion were evaluated among 95 patients in Netherland. According to their results, they have found tuberculous pleurisy just in five patients, among them the high ADA activity was only detected in four individuals. On the other hand, the underlying pathologies other than TB could raise the ADA activity based on their study. The authors conclude that the high ADA activity level in a country with low tuberculosis incidence is not accurate enough to establish the diagnosis of tuberculous pleurisy 17.
Tian et al. found a sensitivity and specificity of 84.4% and 91.8% for ADA in diagnosing tuberculous pleurisy by evaluating 190 patients with pleural effusion. The cause of pleural effusion was TB in 141 patients of their study population 18. The difference between the results of our study compared to the recently mentioned research is explainable by the high overall incidence of TB in the country in which Tian et al., performed their study.
Valdes et al., in their study, revealed that measuring pleural ADA level is a useful parameter for the diagnosis of tuberculous pleurisy by evaluating 405 patients with pleural effusion. All 91 cases of pleural TB in their study showed an ADA level of greater than 47 IU/L, compared to the elevation just in 5% of non-tuberculous patients 15.
Zemlin et al. demonstrated that measuring the ADA2 isoenzyme is more accurate, and it is superior to ADA in diagnosing tuberculous pleurisy by performing a study on 951 pleural fluid samples, including 387 patients with TB. They suggested that measuring ADA2 level is better to use as a routine test among patients with pleural effusion in endemic areas for TB 11.
Technically, the predictive value of an indicator such as ADA does not only depend on its sensitivity and specificity, but also the incidence of the disease in the study region is also effective 8, 9, 11, 16, 19, 20. The inconsistency between the results might have happened due to the variable prevalence of TB and different sample sizes in which the mentioned studies were performed.
The strength of this study was the use of pathlogical confirmation for the diagnosis of the underlying cause of the pleural effusion in the studied patients. The patients with the diagnosis other than pleural tuberculosis was also considered as a reliable corntol group for calculating the diagnostic accuracy of the applied method. Somehow, the shortness of the study sample size was a weakness of our study. Howere, it should be considered that the overall prevalence of the TB within the population in which the study takes place may alter the results of the study; then, it should also be considered as a limitation of the study.
By comparing our results with previous studies, it can be concluded that the sensitivity, specificity, and accuracy of this test are not suffiecient enough; so, ADA is not utterly useful in diagnosis of pleural TB. Therefore, in patients with pleural effusion with undetermined origin and in patients with a high level of suspicion of TB infection, despite the low ADA level, thoracoscopic evaluation of pleural cavity with obtaining multiple biopsies of pleura would be more appropriate.
Also, in cases with high ADA level and lack of proper response to TB treatments, for further investigation and rule out the other diagnosis, thoracoscopy and pleural biopsy could be beneficial.
However, further studies with larger sample size are suggested.
Acknowledgments: Not applicable
Source of Funding : None
For more information: https://jmedcasereportsimages.org/about-us/
For more submission : https://jmedcasereportsimages.org/
#Pleural Effusion#Thoracoscopy#Tuberculosis#Diagnostic Accuracy#Extra-pulmonary tuberculosis#Adenosine deaminase#ADA#pathology#Mycobacterium#Radiography#TB#IBM SPSS#Sina Parsay M.D#jcrmhs
0 notes
Text
What Are The 5 Important Steps To Be Followed For A Trauma Care Patient?

Having 1 million lives lost to traumatic accidents in India alone, it is crucial to understand the 5 most important steps followed for a trauma care patient. Trauma care for the patient begins before arrival at the hospital by local emergency aid providers which include Basic Life Support (BLS), Advanced Cardiac Life Support (ACLS), and Pediatrics Advanced Life Support (PALS). The moment a patient is brought into the emergency department, a team of best doctors in Horamavu enquires about the ambulance staff, witnesses and any individuals involved in the accident to understand the severity and nature of the accident. Meanwhile, the patient is connected to a pulse oximeter, cardiac monitor, and a blood pressure machine to record the vital signs. Once the situation is gauged, the trauma care patient goes through the primary survey beginning with sequential steps of A.B.C.D.E with the most vital areas taking precedence.
● Airway
● Breathing
● Circulation
● Disability
● Exposure/environmental control
Understanding ABCDE:
Now that we have understood the primary trauma care provided to the patient, let's move on to understanding the first step of investigation - the Airway.
Airway
When the patient is attended to, one person stands at the head of the bed and assesses the situation of the airway of the patient to locate any of the following obstacles:
● Foreign bodies
● Swelling in the tongue
● Blood
● Vomitus, or
● Saliva
However, the classic technique adopted by trauma care doctors is to question and engage in conversation with the patient by asking for any difficulty in breathing, talking or any coarseness in the throat, etc. Once the airway is treated,the best doctors in Horamavu move on to investigate the breathing.
Breathing
Once the airway is dealt with, best doctors in Horamavu move on to assessing the next step in the primary survey (ABCDE) , i.e, Breathing. One may consider airway and breathing to be the same concepts. However, do note, airway is the path for oxygen to enter and carbon dioxide to leave the body, whereas, breathing is a mechanism which involves the following parts:
● Lungs
● Diaphragm
● Chest wall / ribs
● Intercostal muscles, and
● Intercostal neuro-vasculature
Once the physical examination is complete, the patient is sent for imaging to eliminate the following:
● Fractures
● Diaphragmatic injury
● Pleural effusion,
● Pneumothorax,
● Parenchymal injury,
● Foreign bodies, etc.
Assessing the above is essential to eliminate any obstruction while breathing as well as identify internal bleeding so as to avoid cardiovascular complications. A trauma care patient needs to be assessed thoroughly by a team of doctors who are specialised in emergency care.
Circulation
Once breathing is assessed and all complications have been successfully dealt with, the patient’s circulation is looked into. The essential components of a circulatory system are the heart, blood and the vasculature. Looking into any deformities that obstruct blood flow in the body can be detrimental to any vital organs. Areas of concern for a trauma patient are usually mechanical, pressure and electrical related injuries which can affect blood flow within the body.
After recording vital signs of the patient, it is crucial for the doctor to check for strength and presence of central v/s peripheral pulses and how they compare bilaterally. Next, the doctor needs to examine the patient’s skin colour/decolouration, warmth and any obvious deformities that can affect the blood flow. To eliminate possibilities of internal bleeding and blood vessel ruptures is through the following imaging modalities:
● CT exam
● X-Ray
● Ultrasound
Internal bleeding is harmful as it can lead to major blockages within arteries and further cause more complications.
Disability
This section of the survey involves the neurological status of the trauma patient which is determined using the following tools:
● Glasgow Coma Scale (GCS)
● Pupillary size and response
● Blood glucose levels, and
● Drug and alcohol levels.
If the patient shows deficit in any of the above categories, they are rushed for CT imaging of the brain as well as the cervical spine to investigate further.
Exposure/Environmental Control
Having understood the 4 stages of primary survey which relate to the patient’s airway, breathing, cardiovascular activity, and neurological deficits, let's move on to the final stage- exposure. In this stage, the team of doctors at hospital in Horamavu remove clothing, articles or any protective layering from the patient to uncover lacerations, bruises and any other injuries having been hidden earlier. Keeping in mind the body temperature of the patient, trauma bays are built with higher temperatures than the rest of the emergency ward.
This level of concern is shown at the Trust-in Hospital, a multispeciality hospital situated in Horamavu, Bangalore with over 15+ departments, 24/7 emergency care along with ICU, Imaging, Pharma, and much more.
Conclusion:
Once the primary care is taken care of, the team of doctors at the hospital in Horamavu draft an ideal course of treatment depending on the results from the above tests and imaging. Keeping the patient’s comfort in mind, they are provided with extra care whenever required. Call Trust-in Hospital at +91-80-45174949 / +91-8050706071 / 72 for their quick response and hassle free emergency team.
Author Profile:
Trust-in Hospital is a major multi-speciality medical hospital in Bangalore. Its mission is to provide high-quality, personalised healthcare to patients. The best and most skilled specialists work at this cutting-edge hospital. It integrates advanced medical technologies and modern infrastructure to provide comprehensive and cost-effective care to both outpatients and inpatients using a multidisciplinary approach.
#trauma care#hospital in horamavu#doctors in horamavu#health blogs#health articles#multispeciality hospital in bangalore
0 notes
Text
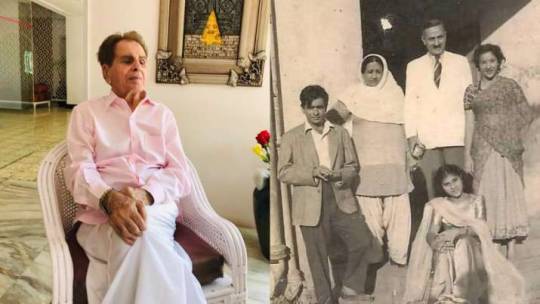
Dilip Kumar shares rare throwback pic with Nargis
Dilip Kumar shares rare throwback pic with Nargis
Image Source : TWITTER/DILIP KUMAR
Dilip Kumar shares rare throwback pic with Nargis
Veteran actor Dilip Kumar got discharged from the hospital on Friday after he was diagnosed with bilateral pleural effusion, the legendary actor shared a priceless throwback picture on his social media. He took to his Twitter handle and shared a photograph in which the veteran actor could be seen standing just…
View On WordPress
#1950 film Babul#Babul#Bilateral Pleural Effusion#Dilip Kumar#Dilip Kumar Health#Jwar Bhata#Mughal-e-Azam#Nargis#Naya Daur#Qila#Ram Aur Shyam#Saira Banu
0 notes
Text
Dilip Kumar shares his picture after being diagnosed with bilateral pleural effusion; Saira Banu issues a statement : Bollywood News
Dilip Kumar shares his picture after being diagnosed with bilateral pleural effusion; Saira Banu issues a statement : Bollywood News
Veteran actor Dilip Kumar was hospitalised on Sunday morning after he complained of breathlessness. The actor is currently in Hinduja Hospital in Mumbai. After running a couple of tests, he was diagnosed with bilateral pleural effusion.
Amid a health scare of the 98-year-old, fans of the star started praying for his good health. On Monday evening, Dilip Kumar shared the latest picture of himself…

View On WordPress
#Banu#bilateral#bilateral pleural effusion#Bollywood#Breathing issue#diagnosed#Dilip#Dilip Kumar#Dilip Kumar Health#Dilip Kumar hospitalised#effusion#health#hospital#issues#Kumar#News#Oxygen support#picture#pleural#Saira#Saira Banu#shares#statement
0 notes
Text
In an outpatient setting it’s easy to get too focused on a patient’s chief complaint. But doing so narrows your differential too quickly and can make you miss big stuff. Examples of actual CC vs Dx I’ve seen in my office in the past month:
CC: heart palpitations
Dx: DKA
CC: allergies
Dx: acute cor pulmonale with large pleural effusion —> stage 4 lung cancer
CC: painful hemorrhoids
Dx: metastatic cancer to rectum
CC: constipation, bloating
Dx: splenomegaly, liver failure, varices, ascites
CC: fatigue
Dx: A-fib with RVR
CC: cough
Dx: bilateral PEs, COVID pneumonia
Some of the patients above obviously looked sicker than their CC implied, but some (DKA, A-fib, rectal cancer) looked perfectly normal and well. Just because they look well doesn’t mean they are well. Do your due diligence.
223 notes
·
View notes
Text
Words - Spoken and Written
My muscles feel it, the normal heaviness that accompanies any movement from point A to point B. My spirit usually tries to finds a way to feel light, to strive for a certain levity that is associated with happiness and laughter floating on breezes. Lately, there is no finding that space. It’s lost with all the tears I’ve shed, the time that’s gone and the memories I don’t have the energy to make.
I have been really sick for the last six weeks. Sicker than I have been during the pandemic which was pretty bad to begin with. The constant stress had all of my conditions in constant flare meaning everything I have is working overtime to make me feel like complete shit. During these six weeks it has been nothing but paranoia, fear and to be honest unexplained illness. Aggressive symptoms and inflammation, extremely precarious mental health and emotional feelings, everything being more than it needs to be. Ever.
Eventually, weeks after an ER visit I was diagnosed with bilateral pleural effusions as well as pericarditis - two conditions typical for Lupus patients when the disease is active.
I am still under treatment. Why? Because I’m still experiencing symptoms of pericarditis (tachycardia meaning an elevated heart rate for no real reason), my lungs still don’t feel right on the left side where the pleural effusion was worse. Still trying to figure out exactly why this disease is doing its best to make me feel my worst. It’s obvious the pandemic hasn’t helped, stress does nothing but aggravate autoimmune conditions and since I have a slew of them I have been sick everyday since last year. Even with the walks, even with the meditation, even with the naps and baths and different therapies. Even with all of the positive things I’ve done to try to alleviate my symptoms or help myself, I have failed.
I still don’t feel well and my body is showing me that I am right. My kidneys continue to struggle, so much so that even a high dosage of oral steroids wasn’t enough to stop my feet from swelling to two times their size. An emergency IV infusion of steroids was necessary to stop whatever the Lupus was attempting to do to my organs. It’s scary as it always is and shows me once again how close my mortality is. Closer than yours is even with Covid out there in the world.
Covid just makes my experience all the more scary: because I can do all the things but needing other people to do the things has been a huge disappointment. All the other things that aren’t easy for me either. But I do them. It’s weird how I feel the responsibility to my family, and even further than that, to everyone else, to do what just feels like the right thing.
I am worried. It makes sense for me to be worried as my heart and lungs are pretty important and Lupus changing their functionality is just beyond my realm of comprehension. My kidney issues, even the anxiety and depression are things that felt almost like a morbid rite of passage, most Lupus patients have kidney issues, most suffer with issues surrounding their mortality, most have issues with acceptance of loss. We struggle, and it’s not just physically.
I wanted to write because I have felt stuck in a way that felt suffocating. My words have felt like they’ve been trapped in my heart, my mouth, and on my fingertips. I’ve spoken more on Instagram because it has felt comfortable there and authentic. At least my frustration, sadness, anger and of course my happiness too - is on display in a way that just feels right.
Writing on the other hand felt preachy as I described it to a close friend. Writing about my illness has never felt forced or like a chore. Yet, I felt like no one wanted to hear this story over and over again. No one wanted to read my words that express pain and things they don’t understand. Things they too are afraid of for me and because of me. Writing about my disappointment feels old but also feels like something that I need to do for me, regardless of what people really want to read.
It’s strange. It became a love hate relationship with writing the words but not speaking them.
I’ve found that I needed to understand how I really felt about what was happening to me before I could put the words in on paper, for the world to read. Even though it’s real to me, it feels real when I write it, as real as it did when I spoke it. Maybe I was the one that lost the interest in my written word, I'll never know. Right now, communication is what feels right and whatever way it takes for me to get there is the path I am willing to walk.
#Words#SpokenWords#WrittenWords#Lupus#LupusNephritis#ChronicIllness#NYC#Brooklyn#Writer#Disabled#ChronicPain#Pericarditis
2 notes
·
View notes
Text
Juniper Publishers- Open Access Journal of Case Studies
Treatment if Pericarditis in an HIV-Infected Patient in a Regional Hospital in Thies (Senegal)
Authored by Bammo M
Summary
Pericarditis is a common and serious cardiovascular disease during HIV infection. In sub-Saharan Africa, tuberculosis is the most common etiology; however, other infectious causes of pericarditis pose a problem of diagnosis and treatment. We report the case of a patient living with HIV 1 for 3 years without ARV treatment who developed a purulent pericarditis treated at regional hospital of Thiès.
We highlight the diagnostic difficulties of this condition in the decentralized zone and the means of treatment of this pathology, fatal if it is not treated early.
Keywords: Purulent pericarditis; HIV infection; Diagnostic difficulties
Introduction
HIV seroprevalence in the Thiès region is 0.3% in 2017. The treatment of PLWAs has been decentralized to the regions and health districts since 2013 with free antiretroviral treatment [1].
a) The immunodepression induced by this virus is at the origin of several affections and/or opportunistic infections responsible for morbidity and mortality, among which cardiac involvement with histological lesions in 60% of cases and clinical expression in 30% of cases.
b) The involvement of the pericardium occupies an important part among these cardiac attacks.
c) The etiological factors of pericarditis vary with the course and magnitude of HIV-induced immune deficiency.
Various causes of pericarditis have been reported in the literature but pericarditis of unidentified (idiopathic) cause can reach 45% of cases [2]. We report the case of an HIV-infected patient who developed a purulent greenish pericarditis of unknown etiology. The objective of this case presentation is to highlight the diagnostic difficulties of this condition in a decentralized environment.
Observation
Mr. Y N is a 26-year-old man, who has sex with a well-known man (MSM), single without children, from the city of Thiès. He presented himself in consultation at the hospital of Thiès October 10, 2016 for a quintessential cough with a notion of hemoptysis of low abundance not objectified. A retrosternal thoracic pain rhythmized by the breathing and a dyspnea with orthopnea type evolving since 15days and exacerbated for a few hours. He also complains of a progressive weight loss of 24kilos in 3years.
For only antecedent, this patient was diagnosed infected with HIV 1, asymptomatic, after a voluntary screening 3 years ago without treatment because He cannot be found. At admission, the patient had a fever at 38.3°C, an impairment of general condition, he was sleepy and cachectic weight 42 kg with BMI: 12.8Kg/m2.
Clinical examination revealed NYA grade 4 dyspnea, tachycardia at 108beats/min and arterial hypotension (BP 100/50mmHg). The heart sounds were muffled. Pericardial friction was not perceptible. There was no paradoxical pulse. Crackling rattles were heard on auscultation at the two pulmonary bases
The rest of the examination found diffuse prurigo and oropharyngeal candidiasis.
The electrocardiogram revealed, in addition to sinus tachycardia, a peripheral low voltage with probable right ventricular hypertrophy, while the chest X-ray showed cardiomegaly and bilateral low-grade pleural effusions.
Complementing the exploration, transthoracic echocardiography confirmed the presence of a pericardial effusion of great abundance without fibrin network. The exploratory puncture aims to produce a purulent yellow-greenish liquid. A percutaneous drainage under xiphoidal under local anesthesia was performed, allowing the evacuation of two liters of greenish-yellow pus free with good tolerance without complications.
The biology revealed an inflammatory syndrome with a CRP of 61.76mg/l and an accelerated sedimentation rate at the first and second hours. There was; microcytic hypochromic anemia at 5.5g/dl, 78.7% neutrophil polynucleosis. Cytobacteriological examination of the pericardial fluid identified 65% of lymphocytes, gram-negative bacilli, but the culture on solid medium was negative. GeneXpert MTB/RIF performed on sputum and pericardial fluid was negative.
As treatment, the patient received an intravenous administration of Ceftriaxone at a rate of 100mg/kg/day; Metronidazole 30mg/kg/day. It was temporarily (3 days) associated with gentamicin (3mg/kg/day) and Prednisone 20mg/day for 5 days. He had also received Furosemide Injection: 40mg/day, Captopril 25mg daily; Enoxaparin 0.4 per day; DLlysine acetylsalicylate 100mg/day. The evolution was marked on day 6 of treatment by a disappearance of cough and dyspnea as well as apyrexia (37°4).
Cardiac echocardiography on day 14 showed a poor pericardial effusion plate insufficient for surgical drainage. The patient was put on antiretroviral therapy and on cotrimoxazole prophylaxis.
The patient was seen six months after discharge in cardiology for signs of late complication; it was stable, with a weight gain of 12kg. Moreover, the M6 ultrasonography showed a quasi-total regression of the pericardial effusion with a slight thickening of the pericardium.
Discussion
This case of purulent pericarditis is singular by its clinical presentation in a PvVIH lost sight of 3 years
Many HIV-infected patients have cardiac involvement [3]. The prevalence of pericardial lesions is regularly reported in all African clinical series: nearly 28% in the Democratic Republic of Congo (DRC) and 35.3% in Congo Brazzaville [2]. In Senegal, already in 1984, D. SOW et al reported a prevalence of purulent pericarditis of 11% in pediatric hospitalized children [4]. I. Thiam found 2.5% of cases of tuberculosis pericarditis with microscopic discovery [5]. Ngouala G. in a study conducted in a decentralized area (Louga) found 3.7% of pediatric cases of tuberculous pericarditis [6].
Pericarditis remains however a serious and rare entity which is almost always fatal because of a late management. The presence of clinical signs and paraclinical examinations allow rapid diagnosis in order to start early treatment [7]. This patient had advanced dyspnea, febrile chest pain on a febrile deterioration of the general condition that had been evolving for 15 days, and effusions indicating delayed diagnosis [3].
The dominant functional symptomatology in the literature is dyspnea of effort and deterioration of the general state. This finding has been made in Africa by several authors [3,8]. Fever is also a reason for frequent consultation. For Cohen, the presence of fever and dyspnea is suggestive of purulent pericarditis or myocarditis [8].
The deafening of heart sounds and tachycardia were the stethoacoustic signs present in our patient and most found in the Niakara and Pio studies, which reported respectively 43.7% and 47.5% of cases [4,8].
The low rate of pericardial friction reported in the literature may be related to the abundance of pericardial effusion [8,9]. He was not present with our patient. Acute pericarditis can be caused by a wide variety of etiologies, which can be infectious or non-infectious [10].
Possible causes include connective tissue disorders, malignancies, radiation, heart lesions, uremia, and infections (including viral, bacterial, and fungal etiologies) [10,11]. In the majority of cases (45 to 80%), infectious pericarditis is of viral origin [11,12].
Bacterial pericarditis is a rare cause of acute pericarditis in the era of modern antibiotics with an incidence of less than 1% [13,14]. The most common living microorganisms involved are Streptococcus sp, Staphylococcus sp, Haemophilus sp and Mycobacterium tuberculosis [15,16].
Pericarditis in a seropositive person, living in Africa in addition, should first look for a tuberculous etiology [3,5,6]. It occurs most often in the early stage of infection, but can also occur in the AIDS stage [3].
No primary infectious focus was found in our patient; the etiological investigation was difficult in our working conditions in the decentralized zone because of the absence of a performing microbiological laboratory, however the favorable evolution under probabilistic antibiotherapy with broad spectrum allowed us to retain the hypothesis of a cause non-specific bacterial.
Predisposing conditions for bacterial pericarditis are immunosuppression, malignant tumors, pre-existing pericardial effusion, alcoholism, uremia, thoracic trauma, cardiac and thoracic surgery, and the insertion or use of catheters for drain the pericardial fluid [15]. This case of pericarditis occurred on HIV-related immunosuppression. The Niakara study in Ouagadougou had a seroprevalence of HIV of 47% out of 79 cases followed for 75 months from 1993 to 1999, reinforcing the work that established a correlation between HIV infection and pericarditis especially in Black Africa [3]. During HIV infection, the occurrence of pericarditis with pericardial effusion is common.
The mechanisms are multiple; pericarditis may be related to viral infection by HIV or other viruses, bacterial or fungal superinfection in an immunocompromised patient or the presence of Kaposi’s lymphoma or sarcoma [3,10,15]. Laboratory assessment may reveal systemic inflammation with leukocytosis and elevated CRP and SV [15]. The chest X-ray usually shows cardiomegaly with an abnormal heart shape. Pulmonary infiltrates, pleural effusion and mediastinal enlargement may also be present [15,16].
The ECG often makes it possible to evoke the diagnosis, especially in its acute form by the Holtzman stages. The signs that we observed at the ECG have no specificity as demonstrated by a piece of literature [9].
In our case, none of the paraclinical examinations were directed to the diagnosis of pericarditis. Echocardiography remains the first-line imaging examination for the diagnosis of pericardial effusion by specifying abundance and location. The abundance of the effusions facilitates the ultrasonography diagnosis of these pericarditis [3,9], as was the case in our patient; he had significant pericardial effusion without cardiac tamponade.
The treatment is based on probabilistic antibiotherapy in the absence of bacteriological data of pericardial fluid and / or blood culture. Surgical drainage is often necessary [8,9]; it allowed our patient to evacuate two liters of greenish yellow pus without complications. Even under treatment, the rate of complications and deaths remains high, with a lethality rate close to 40% secondary to tamponade, pericardial constriction or sepsis [15- 17].
Conclusion
Although rare, purulent pericarditis usually responds to probabilistic treatment provided that a tuberculosis etiology is eliminated even in a health facility with limited means. Early recognition and rapid intervention are essential to the success of the treatment whose etiological research is confronted with daily technical difficulties in a decentralized environment.
For more articles in Open Access Journal of Case Studies please click on: https://juniperpublishers.com/jojcs/index.php
#JuniperPublishers#Juniper Publishers Contact#Gastrointestinal Surgery#Infectious Diseases#Obstetrics and Gynaecology#Ophthalmology
1 note
·
View note
Text
GGOs are opaque areas where you can still see underlying lung markings whereas consolidations are opaque areas that obscure the underlying lung markings. In COVID-19 pneumonia, you can see GGOs early on and then as it worsens, you can see consolidations. So the CXR looks like atypical pneumonia.
Summary of potential chest radiograph findings in covid-19 pneumonia
Most patients with covid-19 infection have a mild illness and do not develop pneumonia3
The chest radiograph may be normal in up to 63% of people with covid-19 pneumonia, particularly in the early stages7111625 (but there is uncertainty around this estimate, ranging from 0% to 63%)
Changes include ground glass (68.5%),10 coarse horizontal linear opacities, and consolidation.12 These are more likely to be peripheral and in the lower zones, but the whole lung can be involved711
Ground glass appearance is common in earlier presentations and may precede the appearance of consolidation1112
Bilateral lung involvement is most common (72.9%) (but can be unilateral in 25%).10
Signs suggestive of potential comorbidities on chest radiography might be obscured by signs of covid-19 pneumonia
The appearance of nodules, pneumothorax, or pleural effusion (1-3%) might be incidental, caused by covid-19 or by comorbidities
Source: https://www.bmj.com/content/370/bmj.m2426
1 note
·
View note
Text
Emerging infectious agents: an unusual case of Metapneumovirus pneumonia in an adult patient by Greco GF in Journal of Clinical Case Reports Medical Images and Health Sciences

ABSTRACT
Human Metapneumovirus (hMPV), a relatively new virus, is a common cause of acute respiratory infection, especially common in the pediatric population. Despite hMPV infection in adults is possible, this rarely results in serious clinical manifestation. Here, we describe a hypoxemic respiratory failure related to pneumonia in an adult patient in whom hMPV was detected in respiratory samples.
KEYWORDS
Human Metapneumovirus; SARS-CoV-2; Covid-19.
CASE HISTORY
A 61-yr-old caucasian man presented to the Emergency Department (ASST Mantua Hospital, Mantua, Italy) with fever up to 39°C, poorly responsive to antipyretics, nocturnal dyspnea and productive cough with mucus-purulent sputum for three days. On physical examination he appeared in good general condition, collaborating and oriented. The following parameters were recorded: blood pressure 140/90mmHg, heart rate of 100 beats min-1; respiratory rate of 23 breaths min-1; and body temperature of 38.4°C. His arterial oxygen saturation on room air was 87%. Chest examination revealed abnormal breath sounds with rhonchi and fine crackles in the middle lobe and inferior lobes bilaterally, no wheezes were heard. Laboratory findings revealed lymphocytosis (81000 x 103/µl), low platelet count (113000 x 106/µl) and an increase in alanine transaminase value (59 U/L), total bilirubin value (1.13 mg/dL) and CPR value (112 mg/L). Room air arterial blood gas analysis showed a normocapnic hypoxemia: pH 7.43, carbon dioxide tension 40.5 mmHg, oxygen tension 60.4 mmHg, and HCO3 24 mmol L-1. The SARS-CoV-2 antigen detection test on nasopharyngeal swab was negative. A chest radiograph showed multiple, small, patchy opacities in the right upper and middle lobe and no pleural effusion was observed. Based on these findings he was admitted to the Respiratory Department.
His medical history included chronic lymphocytic leukemia in follow-up which did not require any specific treatment. He denied taking any medications or to be a smoker, he drinks a glass of wine once a day and has no known allergies. The patient was a farmer who cultivates wheat and maize but he had no animal exposure and no travel history in the last few years. There is no family history or childhood history of respiratory complaints. He was vaccinated with three dosesagainst the SARS-CoV-2 infection (Pfizer) but not against the influenza virus.
Based on the patient’s presentation and testing results, on suspicion of bacterial pneumonia he was empirically treated with IV Piperacillin/Tazobactam, the patient required oxygen support at 3L min-1 and an inhalation therapy with Beclomethasone/Formoterol was set up ex adiuvantibus. In the following days, several microbiological investigations were carried out to determine the etiology of pneumonia: blood culture, urinoculture, sputum culture, Legionella, Haemofilus and Pneumococcus serologic tests, Legionella pneumophila and Pneumococcal urinary antigen test, all of which were negative.
A nasopharyngeal swab FilmArray Respiratory Panel Assay (NP FARP) was then requested: it was positive for human Metapneumovirus and the result was confirmed by repeating the test. For non responder fever and further increase of CPR (230 mg/l) and PCT (0.27 ng/ml), Levofloxacin and later Meropenem were added in the perspective of a resistant bacterial etiology. On the 6th hospitalization day a chest computed tomography (CT) scan was obtained (Figures 1 and 2) which demonstrated large opacities with gradient borders, distributed in the peribronchial area at the right upper lobe, middle lobe and both the lower lobes; they tended to the confluence configuring parenchymal consolidations with aerial bronchogram at the level of the cost-phrenic angle. Imaging also showed bilateral hilar and mediastinal lymphadenopathy (max diameter 3.4 x 2 cm), splenomegaly and absence of pleural effusion. Blood chemistry tests for HIV, Aspergillus antigen and galactomannan were also investigated but turned out negative. To rule out other infectious agents the patient underwent bronchoscopy with bronchoalveolar lavage (BAL) into the middle lobe. BAL provides material for various microbiological and cytological tests: Gram stain, culture, Koch’s bacillus DNA, Galactomannan, Cytomegalovirus and P. Jirovecii and immunological analysis were negative. From respiratory virus panel on BAL only human Metapneumovirus was isolated, this unique microbiological data was according to the NP FARP’s result, thus supporting and confirming the new hypothesis of a viral pneumonia in an adult patient with probable secondary mild immunosuppression due to his hematological disease. About ten days after entering the ward, there was a gradual decrease of CPR and a progressive improvement in clinical conditions and respiratory function to allow the suspension of oxygen therapy. At the end of hospitalization, pulmonary function tests were performed and showed a restrictive syndrome (FEV1/FVC 76.2, TLC 68% and VC 79% of predicted) and mild reduction of diffusion capacity (DLCO 62% and KCO 99%), probably representing the residual functional impairment due to viral pneumonia. The patient finally suspended all therapies and at discharge was referred for a one-month follow-up visit.
DISCUSSION
Human Metapneumovirus (hMPV), a relatively new virus first discovered in 2001, has been detected in 4-16% of patients with acute respiratory infections [1] [2] [3]. In particular, a recent review of 48 previous articles, including 100,151 patients under the age of five hospitalized for CAP, identified this virus as a cause of pneumonia in 3.9% of patients [4]. A recent study of 1386 hospitalized adult patients identified hMPV pneumonia in only 1.64%, indicating that it was much less common than in the infant population [5]. Metapneumovirus causes disease primarily in infants, but rarely can infect immunosuppressed individuals and elderly as well. Seroprevalence studies have shown that 90-100% of 5-10 years old children have previous infection [6]. Reinfection can occur during adulthood because of defected immunity acquired during the first contact with hMPV and/or because of different viral genotypes. The incubation period varies widely but is typically 3-5 days. The disease severity depends on the patient's condition and it ranges from mild upper airway infection to life-threatening pneumonia or bronchiolitis [7]. Clinically, Metapneumovirus infection is often indistinguishable from RSV infection, particularly in the pediatric population, and common symptoms include hypoxemia, cough, fever, upper and lower airway infections and wheezing [8]. hMPV infant patients are often hospitalized for bronchiolitis and pneumonia [9]. In young adults, a flu-like syndrome with fever may occur in a small number of instances, but infection in geriatric subjects may cause severe clinical manifestations such as pneumonia and, in rare cases, death [10].
As described in this case, it was not surprising that antibiotics and corticosteroids were administered in most patients infected with Metapneumovirus mainly for two reasons: in most cases the specific diagnostic tests for hMPV are not carried out at admission and/or physicians prefer to continue steroid and antibiotic treatment to control potential unidentified bacterial infections in patients in which no etiological agent had been identified associated with hMPV infection. The overuse of these drugs could therefore be reduced through the adoption at admission of specific diagnostic tests for such etiological agent, especially if specific risk factors are present (age, immunodepression, etc.). In addition, the adoption of such tests could reduce the nosocomial spread of this virus, allowing an early isolation of the infected patient [11].
Conflicts of interest: The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript. Funding: The authors report no involvement in the research by the sponsor that could have influenced the outcome of this work.
Authors’ contributions : All authors contributed equally to the manuscript and read and approved the final version of the manuscript.
For more information: https://jmedcasereportsimages.org/about-us/
For more submission of articles: https://jmedcasereportsimages.org/
#Human Metapneumovirus#SARS-CoV-2#Covid-19#Metapneumovirus pneumonia#Emerging infectious agents#Greco GF#jcrmhs#casereports
0 notes
Last Seen Blogs

minsukie
Minsukie❄

fictional-men-have-my-heart
A college student (at the moment)

harlequinartist
Harlequin Artist

wordjames
GENT

vianawesley
Sem título