#iv cannula types
Text
IV Cannula Types and Their Role in Modern Healthcare
Intravenous (IV) cannulas, often referred to as IV catheters, play a vital role in modern healthcare. They are indispensable tools used by medical professionals to provide essential fluids, medications, and blood products directly into a patient's bloodstream. Understanding the various IV cannula types is crucial for healthcare practitioners as it allows them to select the most appropriate device for the specific medical situation. In this article, we will explore the different IV cannula types and their essential role in contemporary healthcare.
Types of IV Cannulas
There are several types of IV cannulas available, each designed to meet distinct clinical needs. The choice of IV cannula type depends on factors such as the patient's condition, the purpose of the infusion, and the patient's vein characteristics. Here are some common types of IV cannulas:
1. Peripheral IV Cannulas: These are the most common type and are used for short-term infusions. Peripheral IV cannulas are typically inserted into veins in the arms, hands, or legs. They are available in various sizes and are suitable for a wide range of applications.
2. Midline IV Cannulas: These catheters are longer than peripheral IV cannulas and are designed for patients who require intravenous therapy for a more extended period, typically up to four weeks. They are inserted into larger veins in the upper arm.
3. Central Venous Catheters (CVCs): CVCs are long, flexible tubes that are inserted into large central veins, often near the heart. They are used for delivering medications, total parenteral nutrition (TPN), and chemotherapy. Common types of CVCs include subclavian, jugular, and femoral lines.
4. Peripherally Inserted Central Catheters (PICCs): PICCs are long, thin catheters inserted through a peripheral vein, usually in the arm, and advanced into the central circulation. They are used for extended courses of treatment and reduce the need for multiple needle sticks.
5. Winged or Butterfly Cannulas: These are small, short cannulas with wings that help stabilize the device once it's inserted. They are often used for pediatric patients or those with small or fragile veins.
The Role of IV Cannulas in Modern Healthcare
IV cannulas are indispensable in modern healthcare for a multitude of reasons:
1. Rapid Medication and Fluid Administration: IV cannulas allow healthcare providers to administer medications and fluids quickly and directly into the bloodstream, ensuring that the treatment takes effect promptly.
2. Continuous Monitoring: Many patients in critical care settings require continuous monitoring of their vital signs. IV cannulas provide a convenient way to obtain blood samples for laboratory tests and monitor parameters like oxygen levels and electrolyte balance.
3. Pain Management: In cases of severe pain, IV cannulas are used to deliver pain-relieving medications, providing rapid relief to patients.
4. Emergency Situations: IV cannulas are crucial in emergency situations such as trauma, shock, or cardiac arrest, where rapid access to the circulatory system can be a matter of life or death.
5. Long-Term Therapies: Patients with chronic conditions often require long-term intravenous therapy. This is where devices like PICCs and CVCs come into play, allowing for extended treatment without frequent insertions.
Denex International: Your IV Cannula Exporter
When it comes to types of IV cannula and their role in modern healthcare, it's essential to have access to reliable and high-quality medical supplies. Denex International is a trusted IV cannula exporter, providing a wide range of IV cannula types to healthcare professionals worldwide. With a commitment to quality and patient safety, Denex International offers a variety of IV cannulas, including peripheral IV cannulas, midline IV cannulas, CVCs, PICCs, and more.
Denex International's products meet international standards, ensuring that healthcare providers have access to the best tools for patient care. Whether you require IV cannulas for short-term or long-term therapies, Denex International can supply the right solution. As an established exporter, they understand the critical role IV cannulas play in modern healthcare and are dedicated to supporting the needs of healthcare institutions, clinics, and hospitals worldwide.
Contact Us
Name- Denex International
Phone- 0124 4115465
0 notes
Text
Intravenous Cannulation (IV)
An IV cannula, or intravenous cannula, is a thin, hollow tube typically made of materials like polyurethane or Teflon. Its design prioritizes ease of insertion into a patient's vein, ensuring a secure and painless connection for intravenous cannula administering fluids and medications. Denex International takes pride in providing IV Cannula with advanced features for optimal patient care.
Key Features of IV Cannula :-
Wings for Stability: Our IV Cannula is designed with wings for enhanced stability during insertion, ensuring precise placement and minimizing the risk of displacement.
Integrated Port: The inclusion of a port adds versatility, allowing simultaneous administration of multiple medications or fluids without the need for additional punctures.
Diverse Sizing Options: Recognizing that healthcare is not one-size-fits-all, we offer a range of sizes to meet the unique needs of your patients, ensuring optimal performance in various medical scenarios.
Color Coding for Ease: Our color-coded IV Cannula simplifies the identification process, making it easy for healthcare professionals to select the appropriate size and gauge, thereby enhancing workflow efficiency.
IV Cannula Sizes and Types

IV Cannula come in various sizes and types, each designed to accommodate different medical needs and patient conditions. The size of an IV cannula is typically determined by its gauge (G), with the type referring to the specific design or purpose.
Sizes (Gauges) and Colors:
14G (Orange) - Rapid fluid administration, high flow rates.
16G (Medium Grey) - Versatile, used for various intravenous therapies.
18G (Deep Green) - General fluid administration and medication delivery.
20G (Pink) - Commonly used for a wide range of intravenous therapies.
22G (Deep Blue) - Ideal for medications, blood transfusions, and delicate approaches.
24G (Yellow) - Suitable for gentle and less invasive approaches, such as in pediatrics.
26G (Violet) - Ultra-fine needle for neonatal care or highly delicate veins.
Types of IV Cannulas:
Peripheral IV Cannula: The cornerstone of intravenous therapy for short-term treatments, offering accessibility and versatility.
Central Line IV Cannula: Tailored for prolonged treatments, inserted into prominent veins near the heart.
Midline Catheter: Balancing immediacy and extended use, suitable for treatments lasting more than five days but less than a month.
Denex IV Cannula Specifications:
Catheter made from Medical Grade Virgin PTFE (Teflon) for higher quality.
Color-coded caps for easy gauge identification.
Sharp 3-facet bevel with a back-cut imported needle for ease of cannulation.
Non-return silicon valve for venflon intermittent medication in the port.
Adheres to ISO: 10555 part V specifications.
Uses of IV Cannula:
Fluid Administration: Rapid and controlled infusion of fluids, electrolytes, and blood products.
Medication Delivery: Swift and precise administration of medications directly into the bloodstream.
Blood Transfusions: Facilitation of seamless transfer of donor blood or blood components.
Monitoring and Diagnostics: Access point for diagnostic procedures and continuous monitoring.
Emergency Situations: Quick and efficient means of intervention in emergencies.
Why Choose GST Corporation Limited:
Quality Assurance: Rigorous testing ensures our IV Cannulas meet and exceed global healthcare standards.
Innovation: Constant investment in research and development for cutting-edge healthcare solutions.
Global Reach: As a trusted exporter, our products contribute to global healthcare excellence.
An Intravenous Cannula (IV), also known as an IV catheter, is a medical device used for delivering fluids, medications, or blood products directly into a patient's bloodstream. It is a thin, hollow tube made of materials like polyurethane or Teflon, designed for insertion into a vein. The IV cannula typically features a sharp, beveled tip to facilitate smooth penetration of the skin and vein.
#iv cannula#iv cannula price#intravenous cannula#cannula for iv#intravenous cannulation#types cannula
0 notes
Text
#iv dressing types#peripheral iv dressing#medical iv dressings#iv cannula dressing#changing peripheral iv dressing#iv types#choosing an iv site#iv type#types of iv#Covalon Technologies
1 note
·
View note
Text
Thank you so much @yandere-paramour for commissioning me.
Commission description: I got in a freak accident where in hs where I was in theatre rehearsal and basically a 4x4 fell directly onto my head and I was severely concussed for the Next month. Can you write this happening to Reader and Yves cannot prevent it in time? and he's very upset and angry at himself and Reader is just absolutely fucked up and nearly helpless.
tw: injury, yandere themes
(2632 words)
He oversaw your entire hospital residency. Yves didn't trust the doctors and nurses that were there, he would be the one to administer any treatment. Yves would also be the one to give you bed baths and clean any messes you may have made due to losing some control over your bladder or bowels. Yves had seen all of you.
All he needed to do was talk to a few people, pull some strings, forge a few signatures, and erase a handful of records.
You were in deep throbbing pain, only made manageable by the painkillers you were made to eat. But you couldn't think straight either, everything is just too hazy and foggy. The slightest bit of light bothers you to no end, luckily you were vaguely aware Yves was around to be with you. He knew what to do, he always knew what to do.
You could make out your boyfriend's hushed voice as he spoke through the phone. Squinting your eyes, you could discern a blurry image of Yves holding his smartphone in one hand, and the other typing away on his laptop. You had always found his voice soothing, but it sounded like he was upset, it didn't help that you were barely registering the words he was saying.
Noticing that your drugs are slowly wearing off, Yves quickly ended the call and walked over to you in large strides. You closed your eyes and he didn't say anything, only the shuffling and rustling of what you think came from the medical equipment reached your ears. Occasionally, you open your eyes only to close them again, catching glimpses of Yves toggling with your cannula and a filled syringe.
You were too concussed to question why Yves is doing the nurses' or doctors' job, or if he was even qualified to do so. You were just glad that he was by your side.
Soon, you felt the relief and newfound wooziness from the freshly administered IV painkillers and something else. You were sent to your own world when Yves pulled himself away to clean up and put everything back in place.
You felt him caress your cheek and kiss you on the forehead. After that, you felt the mattress of your hospital bed dip as Yves got on, he tucked himself under your blanket and spooned you from behind.
It was baffling how that wooden plank dislodged itself from somewhere and hit you. Just you, out of all the people present there. He does routine checks on the places where you frequent, the theatre didn't appear to be dilapidated, nor did his numerous tests yield any conclusions that could help him predict this outcome. That damned building passed all his safety checks, likewise, your coworkers weren't a threat to your life.
He buried his head in the crook of your neck, closing his eyes as he breathed in your scent. Yves was deep in thought while he tenderly rubbed the palm of your hands, it's not foul play. If it was, he already knew from the footage from a few dozen cameras he hid around the theatre. Moreover, he did his research on every single one you knew or knew you. The idea of someone trying to end your life is possible, but not plausible.
Yves had replayed that one video over and over again to try and discern the cause of the wooden plank falling from the top. It seemingly... isn't caused by anything. No matter how he digitally enhanced it, no matter how many times he watched it until it was positively seared into his brain, Yves found nothing of note. It just detached from the ceiling and fell. He frowned each time he had to remember the instant it slammed right into your head.
He even paid the theatre a visit just to investigate the site of impact itself. Bewilderingly, he could discern advanced signs of weakness in the surrounding areas that weren't there a day before but would have taken a few months to form through natural means. He swabbed everything and all his tests came out nothing. Yves was undetected by the owners of that building or the authorities because he broke in during the dead of night and scaled the beams quietly and skillfully. He balanced himself on a taut rope while he snapped pictures of the sites.
He called up people who he thought could give him advice and more information about the matter, but to no avail. It's almost like this was caused by something paranormal, there were no conceivable reasons as to how or why this happened. Even if there was, it defied the laws of physics in this reality.
Regardless of how strange and unexpected this event was, Yves was upset that he didn't think of a failsafe for this. He thought of everything but not this, because it was just so implausible.
You groan in discomfort, nothing feels right and you want your mind back now. However, there really isn't anything Yves could do and all the other relatively instantaneous healing methods he knew of would cause more significant harm than good. So, for now, you're stuck like this.
He sighed, murmuring that he was here to assure you. Well, at least this has given him a new set of data that he otherwise wouldn't go out of his way to induce and collect; there is at least that silver lining.
Yves frowned as he parted away from you, despising the cold nipping at him without you as his soft heater. But he has a lot to do, he has to maintain the life that you built for yourself while you're out of commission for at least a month.
He pressed a kiss on your forehead once more, ensuring that you were completely passed out from the drugs before taking out his phone again to make a few more important calls.
-
He transferred you to his humble abode a few days later, after determining that you were stable enough for him to resume your care outside of the hospital. You could barely walk, talk, or open your eyes, you were entirely helpless. Mumbling semi-incoherent words to try and communicate your needs and wants. Luckily for you, Yves clearly knew what you wanted just by your body language alone, so you were never too angry or frustrated that he couldn't understand you.
Unfortunately for your friends and family who would visit you from time to time, you were babbling in a language from another planet. They're either too loud, too panicky, or too pungent-smelling to be around with. It's as if the air was ruined by their presence. Your poor, concussed mind thought everyone else was just idiots and Yves is the only intelligent lifeform there.
Such an attentive man, he is. Yves would politely shoo them out of your shared bedroom when they got too much, he would then spend a few more minutes entertaining them with small talk downstairs before ultimately making them leave the property. The ones who truly care about you are glad you are under Yves's supervision.
However, if you were just lucid enough, you would question how Yves knew that you wanted a blanket from your heavy slurring, how he knew that you wanted to be hugged at that very moment by just watching you blink, how he knew what hurts by an incomprehensible grumble.
A few times, you did catch yourself realizing that you may have been completely unintelligible in verbalizing your wants. Still, he gave you exactly what you needed before you could correct yourself.
You always look forward to meal times, as he would never fail to whip up something delicious yet nutritious enough; packed chock full of vitamins, and minerals to your healing process. The best part was that he would spoon-feed you while sitting on his lap, it's ridiculously comfortable and you felt like absolute royalty. Strangely and fortunately for you, it never once felt degrading or patronizing. At most, you felt heavily nostalgic and had a strong sense of sadness that you couldn't conjure up an idea as to why. But it would all ebb away with every spoonful Yves fed you or every kiss he gave to show his appreciation for your cooperation.
Yves wouldn't allow you to use your phone or watch the television, he wouldn't allow anything in his house to emit too bright of a light. Which you were grateful for since it reduces the pain dramatically, and he would keep you fully engaged by reading stories from his library. They're always so exhilarating to hear as the protagonists always possess a wonderful personality that closely matches yours, allowing you to immerse yourself in whatever whimsical and fantastical world of his storybook. His smooth, baritone voice lulled you to sleep more times than you can count, letting you continue the story in your dreams.
Sometimes, you want to experience that particular story again, so you would pick up the book Yves read from. Only to find that its' pages are seemingly filled with illegible graphite chicken scratch. Asking him about it will lead him to tell you he wrote each and every single one of those pieces, they're all based on your proudest achievements and your life journey.
When Yves promised that he would take care of you to the fullest, he meant it. He wouldn't allow you to shower on your own, nor did he let you stand too long. He prepared a stool for you to sit on as streams of warm water washed over your nude body, Yves would roll his sleeves up and clean you up while you merely remained there in a daze; you didn't have to do anything, Yves would work up a lather on your hair and massage your scalp, he would gently scrub your skin with his smooth hands and apply an impossibly long list of skincare products that leaves your skin happy and glowing.
Yves is rarely apart away from you when you're this needy. And he enjoys it, savoring every second he spends with you. Yves would take his time styling your hair, stroking it, and collecting any strands you may have shed for data. Applying hair oil and caring for your body, he wouldn't have had the chance to do this when you're perfectly healthy, as you would either get too uncomfortable, bored, or too busy for him to do this for you.
In many ways, this accident was a blessing in disguise. For you to make up for all the missed bonding times with him; it's not that Yves is elated with you being severely concussed, but he isn't too upset over it either.
"Is this the color you want for your base?" He asked, ensuring his voice wasn't above the volume threshold. Yves brought up a bottle of nail polish in your favorite color.
You gave him a thumbs up, as nodding can cause you pain.
"What design would you like?" Yves continued asking, putting the polish away so he could begin to prep your fingernails. He had your hand limply resting on a towel draped over his thigh.
You opened your mouth to speak, but it was gibberish and garbled. But you were so used to talking like this and your brain is still healing from the damage, that you couldn't tell something was wrong.
Yves merely hummed in response while he skillfully pushed your cuticles in, they were softened by some cuticle oil he applied earlier. He needed no extra enlightenment even though you spoke in a tongue that no human could ever comprehend easily, Yves already knew what you wanted. He only asked that to give you an illusion of control.
You relaxed to the soothing music playing in the background while Yves continued with his manicure on you, skillfully using his tools to create intricate works of art on your nails. It's amazing how he could do that with laser precision in dim light.
Perhaps you tried holding a conversation with him, and you did. Albeit one-sided, Yves seemingly responds to your words normally as if he truly understood. But he was actually doing some very complex "guesswork" that was apparently accurate all the time. However, if there is one thing for certain, he memorizes all the sounds that left your mouth and movements you made no matter how random or unnecessary.
If thinks that you're getting too under-stimulated, he will recite one of the many stories he wrote for you to listen to and immerse yourself in. Yet, he wouldn't get distracted, continuing his work with elegance and expertise.
You were mesmerized by how he would hold his brush, how he would administer a graceful stroke, and how he would do the details of such an impossibly beautiful masterpiece.
You smiled and cheered when you saw your nails, all that there was left for you to do was wait for the polish to dry. The corners of his lips were also pulled up into a pleased grin, feeling absolutely delighted to see you beaming like that. He couldn't resist pecking you on the apples of your cheeks, as he might accidentally squeeze you out of his cuteness aggression if he didn't at least expel some of it.
He cleaned up after himself and put the items away. You were still giddy over your nails and he was in joy too. Yves then sat right next to you, resting his head on your shoulder and letting his silky, jet-black hair tickle you in the nose.
Yves closed his eyes and relaxed at the sound of your heavenly giggles, nuzzling his head further into the side of your neck to keep the playfulness alive. He would occasionally litter your shoulder with kisses too.
Eventually, the atmosphere calms back down to a gentle lull, where you would be lying on his lap as Yves runs his fingers through your hair. A soft smile graced his face as he watched you stare at his artwork, feeling flattered and honored that you liked it.
Yves always knew the potential of himself enjoying the aftermath of such a tragedy happening to you was there. But he didn't anticipate that he loved it this much. As bad as it sounds, Yves is unwilling to think about the time when you will inevitably heal and leave him alone all over again to live your life.
His smile faltered a bit thinking how you're most likely going to go back to that theatre to work again, cutting the time that he's used to have with you short by a drastic amount. He is going to miss tender moments like these so awfully...
Yves paused when he noticed that you drifted into slumberland, softly breathing as your lips were slightly parted and drool running down the sides of your mouth. Yves chuckled a bit as he wiped them away with his thumb.
He blinked as he thought about the situation at hand even more.
You are such a strong, resilient person, who endured far worse than a measly headache. And it seems like your recovery process isn't too agonizing for you to bear, you're fine.
And, you would definitely be fine if Yves extended that duration for a few more weeks; he needs to make sure that you're fully healed before allowing you to go back into the real world. You would also be fine to consume a bit more sugar than usual, he knows you better than yourself.
Yves brought your hands and grazed his fingertips against your nails to see if it was fully dried. They were, and he gave them each a kiss.
The next few hours were spent with Yves watching you sleep, his green eyes were unblinkingly trained on you.
#oc yves#yandere concept#tw yandere#yandere oc x reader#yandere x you#yandere male#yandere x reader#male yandere oc x reader#yandere oc#yandere#thank you so much for your commission#male yandere#yandere x y/n#male yandere x reader#tw yandere content#cw yandere
81 notes
·
View notes
Text
Touch - Ch. 11
tw: medical language, scenes of torture (slicing of skin, beaten reader)


Waking up had never hurt so much. There was a cannula in your nose and an IV in your hand. Every intake of breath burned in your lungs. Your eyes blinked away the light, looking around the room as you took in your surroundings.
To your left, you could see the door to your room and a couple chairs sat next to your bed. A computer and other medical equipment took up the corner next to your bed. At the foot of your bed stood your bed table, covered in different floral arrangements and cards. To your right, a wall of windows covered by heavy curtains sat above a small couch where a man sat, head in his hands.
“Kyle?” you questioned, voice cracking from the lack of use and the cotton type dryness of your mouth. Kyle shot off the couch and to your side, grabbing a cup of water with a straw and holding it to your lips. You wrapped your lips around the end and sucked, groaning at the relief of the water wetting your palate.
“Thanks,” you croaked out as he smiled down at you, the perfect white of his teeth almost shining in the low light of the room. “How long have I been out?” you asked, looking around the room again with a furrowed brow.
“Two days. Those hits you took really did you in. Otherwise, you’re alright. You were dehydrated and over tired,” Kyle explained calmly, moving to sit in the armchair tucked into the right corner next to your bed.
“Is every-” You coughed, groaning at the pain of using your throat and Kyle shushed you before speaking. “Price and I are alright, normal scrapes and scratches. Johnny got treated for a piece of rebar that tore a chunk out of his side. He’s actually in the next room,” he informed you, sitting back in the chair. “Si?” you inquired, not missing that Kyle had left the big brute out of his roll call.
“He was really hurt, dove,” he drug a hand down his face, closing his eyes to take a deep breath before his chocolate eyes met yours. “He’s in the ICU. Fractured his tibia and broke his fibula. But the docs are concerned about the sternal fracture,” he continued, watching you for your reaction.
“Can I see them?” you croaked out your question, using the remote to lift the head of your bed so you were sitting. “We’d have to ask the doc, but we were mainly just waiting for you to wake up,” he answered, standing and coming to the side of the bed to take your hand.
“I’m so glad you’re okay, dove. We thought we were going to lose you.” He brought your hand to his face and you cupped his jaw gently while he leaned forward to press a gentle kiss to your temple before resting his forehead against yours for the soft, quiet moment of relief to wash over both of you.
The silence was filled with slow breaths as the two of you reveled in the presence of the other. Unfortunately, the silence was broken as your doctor came in and smiled. “Well, look at that. Our sleeping beauty has awoken,” she chirped, much too happy for this early in the morning. “Everything looks good. We do encourage you to get up and walk around a little throughout the day. Don’t stress yourself though,” she continued, chipper as ever.
“Can I see Johnny and Simon?” you asked, eyes eager and glassy as you gazed at the doctor. “Hm, I don’t see why not. Mr. Mactavish is next door. He’s been awake all night asking for you. Mr. Riley is in a medically induced coma to allow for his wounds to heal more. He put up quite the fight when he first woke up, but you’re welcome to see him,” she concluded, watching you and Kyle with a keen eye.
With a brief goodbye and directions to Kyle to make sure you didn’t stress too hard or take out your IV, the doctor disappeared again. You were already working on getting out of the bed, grateful someone had thought to put some grippy socks on your feet.
Kyle rushed around the end of the bed, grabbing the sterile, papery robe that hung next to the door. He slid it over your shoulders and tied it around your waist so your back end wasn’t exposed.
Together, the pair of you trekked next door and you let out a sigh of relief when you found Johnny awake. “Johnny…” you sighed out his name, shuffling over to the bed and dragging Kyle along behind you. “Petal, you’re okay. I didn’t get to see you before they took me in for surgery and then everything with Si-” His words were cut off as you draped yourself over him in a careful hug and he placed his hand over the back of your head, sighing at the relief of your presence.
Kyle’s hand rubbed over your back until you stood from your spot, bringing a hand to gently cup Johnny’s jaw. “Thank you,” you whispered, looking over your shoulder to Kyle. “To all of you. You saved me and I don’t know how I’ll ever repay you.”
“I can think of a few things, little bird.” John stood at the door, a soft smile on his face as he looked at the scene before him. You shuffled over to him, pushing past Kyle and wrapping your arms around the waist of the Captain. “I’ll do it. Whatever it is,” you murmured against his chest, so happy that they were okay. His bulky arms wrapped around you and you felt him breathe you in as his chest expanded.
Before he could break his long running streak of not crying (he cried when they brought Simon in but he won’t tell you that), he sniffled and pulled back, hands on your shoulders as he looked you over. His eyes hardened slightly at the bandage still around your throat, but overall he was glad you were okay.
“Kyle, why don’t you stay here with Johnny? I’ll take her to see Simon,” John offered, pulling you into his side. Kyle nodded and the two men said their goodbyes as John ushered you from the room.
As you walked alongside him, you noticed his steps were measured and slow in order to not outpace you. He kept you tucked into his side, the IV pole in the other hand as he led you to Simon’s room.
“I want you to be prepared to see him. He doesn’t look like the Simon you remember right now. He was crushed under some rubble,” you gasped and interrupted his speech before he squeezed your shoulders. “He’ll be okay, birdie. He just needs time.”
John pushed open the door to Simon’s room and you gasped as the form of him came into view. He was bruised everywhere. The blood pooling under his skin as his chest lay wrapped tightly from being opened to reset bones. His leg was wrapped up in a cast, propped up on some pillows and you could feel the tears welling up in your eyes.
Stumbling to his side, you pulled a chair up next to the bed and curled up on the seat, resolute in not leaving. You took his battered hand in yours and gently drug your fingertips over the ragged skin. “Si, oh god, I miss you. I know they say you’ll be okay, but this is all my fault,” you muttered through tears as they ran freely down your face.
A hand came to rest on your shoulder which brought your attention to the other man in the room. John squatted down so he was at eye level with you. “In no way is this your fault. This is the consequences of our actions, not yours. Karma, if you will,” he reassured you, an edge to his voice as he grumbled the last sentence. You didn’t respond, just turned back to face Simon.
With a sigh, John stood and pressed a long kiss to the top of your head before stepping back. He was relieved that you, Johnny and Kyle were okay. But until Simon woke, he knew the entire group would be thrown off.

Simon couldn’t see much, a burlap sack covering his eyes. Light peaked through the holes in the fabric, illuminating shapes in the room. There was someone across from him, mimicking his position. Tied to a chair, slumped in the seat while the sounds of whimpers floating to his ears.
Your whimpers. He growled low in his throat, yanking on his bindings. “Get your hands off her!” he bellowed, keeping his panic and worry in a tidy little box and letting his anger rage on the surface. He yanked at his bindings again when the hood was removed and he blinked away the sudden light.
“O-ho! Look who finally woke up, precious. Just in time to watch me slice you into shreds,” his captor jovially exclaimed, clapping Simon on the shoulder. Simon, no, Ghost’s teeth snapped at the hand as he finally got his bearings and the face of Darin Moses filtered into his view.
Beady eyes smiled down at him as Moses moved over to where you sat, crying through the swelling of your eye. The glint of a knife blinded Simon for a moment before your scream met his ears. The knife sliced into the top of your thigh, blood immediately beginning to soak the fabric of your pants. Over and over and over. Slice and scream.
“Si, oh god, I miss you. I know they say you’ll be okay, but this is all my fault.”
Where was your voice coming from? Your fault? No, luv, it’s not your fault. His. His fault. Didn’t protect you well enough. Shouldn’t have left you alone.
Slice and scream. Over and over and over until everything went black.
It was the same. Burlap sack. Blinking away the light. Your beaten face. This time General Shepherd stood over you.
Slice and Scream. Over and over and over.
Again. Burlap sack. Blinking away the light. Your beaten face. Phillip Graves slicing away at your skin.
Slice and scream. Over and over and over.
“Simon, please, get better. The doctors are going to wake you up soon. I’ll be right here, my love.”
Slice and scream. Slice and scream. Slice and scream.
I'm not sure how many more parts there will be of this fic, but we're getting close to the end.
Thank you for all of the support on this fic!

#captain john price#call of duty x reader#johnny soap mactavish#kyle gaz garrick#poly!141#simon ghost riley#cod fanfic smut#johnny soap mctavish x reader#kyle gaz x reader#simon riley x reader#simon riley x you#simon ghost x reader#john price#johnny soap mctavish x you#john price x plus size reader#john price x reader#john price x you#kyle garrick#kyle gaz x you#touchau
45 notes
·
View notes
Text
Awake
Alice was 27 years old, standing at 5’4 with a slimmer build. She had shorter, dark brown hair with bangs that came just above her shoulders, and brown eyes that were normally behind a pair of glasses. Alice was the cute, shy, artsy, eccentric type, who was beautiful in a unique sort of way. She enjoyed and partook in pretty much any creative medium, and lived a more unconventional, bohemian type of lifestyle. Since Alice wasn’t quite like most girls, it isn’t a stretch of the imagination to believe that her time in our emergency department was quite unusual and memorable.
It all started last night. Alice was sitting on the trauma room table in the upright position, stripped down to just her bra and underwear. She had EKG electrodes stuck all over her chest, IV lines in both arms, and a nasal cannula in. She was breathing rapidly, taking deep, dramatic breaths, almost gasping at times. She had one hand on her chest, and a visibly pained, uncomfortable look was on her face. Alice squirmed around somewhat on the table, clearly distressed from the onslaught of symptoms that developed seemingly out of nowhere for her. She experienced shortness of breath, chest pains, heart palpitations, indigestion, and pain in her back between the shoulder blades. The heart monitors chirped and beeped loudly, displaying abnormal vital signs. Alice’s heart rate was in the 150s, her blood pressure was 80/45, and her oxygen saturation was surprisingly normal considering her most glaring, obvious symptom was shortness of breath.
“hi, I’m Dr Lindsay. What brings you to our emergency department tonight?” Dr Lindsay asks in a calm tone, entering the trauma room and approaching the table where Alice sat. Alice was wide eyed, trying everything she could to fight whatever was going on inside her body. She looked over at Dr Lindsay, and attempted to reply. “my… my…chest…” Alice told Dr Lindsay in a breathy, winded tone. “your chest hurts?” Lindsay asked, trying to confirm. Alice nodded. “it… it really hurts…” Alice said weakly. “I feel… I feel like….” Alice continued, but paused, feeling a bit lightheaded and dizzy. “you feel like what sweetie?” Dr Lindsay asked, wondering where she was trying to go with that statement. “like I’m going to die…” Alice replied, looking Lindsay right in the eye. “well, myself and our ER team are here to try our best and make sure that doesn’t happen, ok?” Lindsay said to Alice, to which she nodded in acknowledgement. “so can I ask a couple questions?” Dr Lindsay asks, to which Alice nods. “good! Let’s start off with an easy one. Can you tell me your name?” the doctor asks. “Alice…” she replies in a labored, weakened voice. “anna? That’s my girlfriend’s name.” Lindsay said. Alice was shaking her head no. “AHN. YUH.” Alice cleared up for Lindsay, still having a tough time breathing, let alone talking. “oh, I’m sorry for the misunderstanding! Alice. It’s nice to meet you! Just wish it wasn’t here in the ER of course. Anyways, how about I ask some other questions?” Lindsay continued, Alice nodding in response. “ok, great. So do you have a history of asthma, breathing problems, or lung problems?” Dr Lindsay asked. Alice shook her head, indicating she did not. “alright, good. What about any heart problems?” Lindsay asked. Again, Alice shook her head to tell the Dr no. “ok ok. What about blood clots?” asked Lindsay. Alice couldn’t muster up enough power to get the words out, but she mouthed “no” to Lindsay. The questions didn’t seem to get any tangible info the ER team could use. Lindsay asked more questions such as: “any medications?” “any allergies?” “any use of illegal drugs?” “any chance you’re pregnant?”. Even though Dr Lindsay didn’t get any helpful answers, she ordered the nurses to draw labs to be sent off to the lab for analysis. The tests she ordered were a CBC, BMP, toxicology screening, HCG, d-dimer, and a cardiac enzyme test. In the meantime, there was only so much that could be done. Nurses Heather, Lin, and Nancy stuck around to push meds to treat symptoms and keep an eye on the monitors to make sure there weren’t any changes to Alice’s vital signs.
A little while went by without any major changes or updates one way or the other. But then out of nowhere, things went completely sideways. Alice started gasping, her breaths becoming more shallow. Her eyes started to roll back, and she struggled to remain conscious. “Alice? Stay with us sweetie!” nurse Nancy shouted, doing a firm sternal run on Alice. The patient groaned in response, drifting in and out of consciousness. “I’m getting Dr Lindsay back in here.” Lin said, exiting the room with a pep in her step. The heart monitors showed more worrisome vital signs, showing that Alice’s heart rate was in the 180s, and her blood pressure was taking a nosedive. “P…please…” Alice uttered weakly to nurse Nancy and nurse heather. “d-don’t let me die…” Alice continued, having to put in maximum effort to get her words out. “it’s gonna be ok sweetie, we’re gonna take care of you.” Nurse Nancy told Alice in a calm, soothing, reassuring tone.
It didn’t take long for Dr Lindsay and nurse Lin to come back into the room. Everyone gave Dr Lindsay the update on what was taking place, and also explained that the labs hadn’t come back yet. While discussing what the next move would be, Alice’s eyes rolled back, and let out a calm exhale. Her tense, squirming body fell limp. Her rapidly rising and falling chest was completely motionless. “Alice? Alice?!” nurse heather asked anxiously, doing a sternal run that received no reaction from Alice. Nancy took a carotid pulse, placing 2 fingers on Alice’s neck. “no pulse Linds.” Nancy called out, shaking her head. Lindsay paused and looked up at the monitors. “pulseless v-tach. Lower the bed and start CPR! Get her intubated, then we’ll shock!” Lindsay barked, taking charge of the hectic situation that was developing.
The bed was lowered, and Alice’s bra was snipped off, allowing her perky b-cup tits with pierced nipples to spill out. Nurses Heather placed the heel of her hand on the middle of Alice’s chest, beginning to push down hard and fast repeatedly. At the head of the bed, nurse Nancy had a laryngoscope and 7.0 ET tube, which she carefully navigated into the young lady’s airway, securing it in place with a blue tube holder once she confirmed the correct placement. Lin got the defibs and meds from the crash cart set up for the doctor. But post intubation, a weird development occurred. Alice’s eyes opened slowly, then blinked a few times. Her eyes scanned the room, looking at the chaos unfold around her. She felt something on her chest and looked down, seeing Heather performing chest compressions. Alice moaned, horrified at this sight. “Huh?” Heather uttered, thinking she saw Alice blink and look around the room. “hey, let’s pulse check. I think I saw her blink.” Heather announced. “ok ok. Hold CPR.” Lindsay nodded in approval. CPR was halted, and Alice’s body went completely limp, her eyes wide open, completely glazed over and devoid of life. “no pulse, still v-tach on the monitors.” Nancy replied, taking a carotid pulse, also ambu bagging. “alright, let’s shock her. Charging paddles to 200. Everyone…CLEAR!” Lindsay ordered, readying the defibs paddles, pressing them up against Alice’s bare chest, sending the first shock of the night into her body. Alice grunted, her body tensing up and flopping on the table in response. The first shock didn’t eliminate v-tach, so the paddles were gelled, charged to 250 joules, and the next shock was delivered. KA-THUNK! Alice’s chest shot up, and her back arched, her eyes remaining wide open, staring helplessly above. “still nothing, resume CPR.” Ordered Dr Lindsay.
“…5…6…7…8…” heather counted out under her breath, getting the ball rolling on the next cycle of compressions. “MMMPH!!!” Alice tried to yell, one of her hands reaching towards her mouth to pull the tube out. Everyone was taken aback. “what the?!” nurse Lin said, not sure what to think of what she was looking at. “Calm down sweetie!” nurse Nancy told Alice, gently nudging her hand away from the breathing tube. “hold compressions!” Lindsay shouted. Heather promptly stopped CPR. And just like that, Alice’s muffled moans and shrieks stopped, her body falling limp again, the same deadly rhythm present on the monitor, along with no pulse. “let’s shock again. Charging to 300!” Lindsay shouted out. The paddles were gelled, charged, and pressed back up, another shock being delivered. Alice’s body was effortlessly thrown around on the table, the electricity running through her body in an instant. “damn it, she’s in v-fib now. Going again at 360. Everyone…CLEAR!” Lindsay commanded, shocking the patient again. Alice’s toes scrunched at the far end of the bed, showing off the matte black nail polish on her toes and the soft, delicate, velvety wrinkles throughout the soles of her size 7 feet. This shock failed to restore a heartbeat, so Lindsay delivered another shock immediately afterwards. “MMMMMPH!!!” Alice yelled, feeling every last bit of that shock. “still no pulse, resume compressions.” Lindsay ordered, placing the defbs back on the crash cart. Heather restarted CPR, and it didn’t take long for Alice to realize. Alice blinked a few times, her eyes scanning the room, watching the team work on her. She moaned and groaned, her eyes becoming teary. Alice’s eyes locked with Lindsay’s. The doctor was taken aback. “can you understand me?...” Lindsay asked a bit nervously. Alice held eye contact and nodded “yes”. Alice then reached out with one hand, holding onto Lindsay’s hand for dear life. “hmmmph….” Alice tried to say something to Lindsay. “we’re gonna do everything we can for you, ok?” Lindsay replied, holding the young lady’s hand. Alice nodded, still holding Lindsay’s hand and maintaining eye contact. Nancy gently stroked Alice’s hair. “it’s gonna be ok sweetie…you’re doing great.” Nancy said in a calm, reassuring voice.
After a few cycles of chest compressions and a dose of epinephrine and atropine, Dr Lindsay felt it was time to shock again. Compressions were held, and the right grip Alice had on Lindsay’s hand loosened, and Alice became unconscious once again. The paddles were charged to 360 joules, and she was defibbed again. THUNK! Alice’s torso bounced around on the table, her pretty brown eyes wide open. No change was noted, so Alice was defibbed again at 360 joules. Her shoulders shrugged and her body tensed up, before relaxing a split second later. Alice received another shock, but unfortunately she deteriorated into PEA, so CPR was resumed.
Heather had restarted chest compressions, and medications were injected into the IV line. Alice regained consciousness almost immediately after CPR resumed. Alice moaned, her arms flailed, freaking out at the sight of her own cardiac arrest. “stay still for us!” Lin stepped in, gently restraining Alice’s arms. Alice’s screams were muffled from the breathing tube, but the absolute terror she was experiencing was all over her face. Alice looked down, seeing Heather do CPR. Alice saw her chest cave in, her tits bounce around, and her belly ripple out. “mmmm!!!” Alice moaned, tears beginning to stream down her face. “it’s on sweetie…” Nancy told Alice, gently stroking her hair again. Alice cried hysterically, watching her chest get pumped violently.
Several minutes went by with no changes, and another dose of meds were pushed into the IV line. The tension was absolutely palpable in the room. The team had seen everything, but never this. “linds… I have a question…” heather asked, still pumping away vigorously. “go for it Heather.” Replied Lindsay. “with all due respect, what the hell is going on? She’s ya know… technically dead, but she’s looking right at me blinking…” heather asked, continuing CPR, Alice making eye contact, clearly listening to the conversation. “well, it’s something I only read about…” Lindsay said to heather. There was an awkward pause in the room, Alice’s eyes looking back and forth between Lindsay and heather, wanting to know the answer herself. “go on?...” heather asked in response, not satisfied with Lindsay’s incomplete answer. “I read a case report in Denmark or somewhere like that where a guy went into cardiac arrest and regained consciousness mid code. They said it was because the chest compressions created good enough perfusion and blood flow to the brain to restore consciousness.” Explained Dr Lindsay. “so how’d the guy in Denmark do? Did he make it?” heather asked, still going to town on Alice’s chest. There was pause. Lindsay sighed. “no. I think the guy died…” Lindsay reluctantly said. Alice’s eyes widened after hearing that, a look of fear all over her face. “it’s ok Alice! We’re gonna do everything we can for you!” Lindsay replied in a nervous, but somewhat reassuring tone.
The code continued with no progress whatsoever. Alice’s rhythm had deteriorated from PEA to agonal over the next little bit. She was still receiving chest compressions and wide awake during them. She had calmed down a bit, her crying stopped. She was holding Lindsay’s hand tightly, her eyes scanning around the room. Heather was absolutely gassed from all the CPR she performed, so she swapped with nurse Lin, hoping she had the magic touch. There wasn’t really a pause during the swap, and Alice never lost consciousness. “hmmp…” Alice tried to say something, looking up at Lin starting CPR. “it’s ok, Heather is just tired. Normally we switch who does CPR every now and then in situations like this. This is completely normal.” Lindsay explained, holding Alice’s hand, trying to keep her calm. Heather stood off to the side taking a breather. “man… they don’t teach you this shit in nursing school…” Heather said under her breath, referencing the events of Alice’s code up to that point.
A lot more time had went by, and Alice’s rhythm had deteriorated from agonal to asystole. Nonetheless, Alice stayed conscious the entire time. “meds in.” Heather called out, injecting another dose of epinephrine and atropine. “that’s the last dose of meds we can use. She’s maxed out on meds…” Lindsay explained. “what do we do?!” Lin asked, still doing CPR, Alice listening and watching. “let’s see if the meds kick in over the next little bit and go from there.” Lindsay replied, hoping and praying that these meds got a shockable rhythm back. But each minute ticked by, one more tense and anxious than the previous, asystole still on the monitors. The room was eerily quiet, Lin continuing chest compressions. Time continued to tick by with no change, and the team knew deep down they’ve done all they could, but there was a dilemma on what to do since Alice was still clearly conscious. Lindsay decided to break the silence. “Alice?” Lindsay asked. Alice looked over at Lindsay, making eye contact, her head bobbing gently from the force of the chest compressions she was receiving. “Alice… we’ve done everything we could for you. We’ve shocked your heart, given you the maximum amount of medications possible, and did CPR for almost 40 minutes, and your heart still isn’t beating. Unfortunately, there’s nothing more we can do…” Lindsay explained. Alice was terrified, beginning to cry and moan, shaking her head “NO!!!” at Dr Lindsay. “I know… I know…” Lindsay replied, trying to sympathize. “we’ll stop whenever you’re ready, ok?” Lindsay said, trying to offer some sort of compromise in the horrible situation. Alice cried hysterically, shaking her head passionately indicating “No!”.
Alice tried to buy herself as much time as possible, avoiding all eye contact with the members of the ER team. Alice cried, looking around the room trying to process the fact that she was experiencing her last moments. A teary eyed Alice regained some semblance of composure after several minutes, reestablishing eye contact with Dr Lindsay. Alice gently placed her hands on top of nurse Lin’s, nodding at Lindsay, indicating it was ok to stop CPR. Nurse Lin held CPR, and the monitors immediately went flat. Alice’s eyes glazed over completely, but still looked right into Lindsay’s. Nurse Nancy detached the ambu bag and turned off the heart monitors. Lindsay sighed. “time of death, 8:21pm.” Lindsay announced, stunned from the events she just witnessed. The EKG electrodes were then disconnected, and the defib gel was wiped off of Alice’s bruised, battered chest. The IV lines were taken out, and her body was covered up, hiding the haunting gaze on her face. A toe tag was filled out and placed on the big toe of her left foot. The tag dangled against Alice’s cute, wrinkly soles. Alice was a one in a million, unique girl, and unfortunately, she died an equally unique death in our emergency department.
108 notes
·
View notes
Text
In the shadows
Pairing: Stiles Stilinski x reader
Warnings: Violence
Chapter: 1.12
The feeling of being dragged underwater is what wakes you, and when your eyes flutter open, you’re surprised to be in a hospital bed and not a pool of water. Your body, which is covered in bandages and bruises, aches. Two nurses are in the room as well, both looking concerned, but neither of them say anything.
You look around the sterile room and notice Sheriff Stilinski yelling at Jackson. At least that jackass was alright. Suddenly, all the fear comes flooding back. Peter's face flashed before your eyes, his eyes glowing red as his jaw opened, sharp fangs replacing his human teeth.
“No!” You lunge forward. “Stiles run!”
Hearing your sudden outburst and yelling his son's name, the sheriff tries to enter the room but is denied access. Your parents had gone out of town to visit friends the previous morning, so I guessed they hadn’t returned to Beacon Hills yet.
One of the nurses begins fidgeting with the IV bag, which is attached to the cannula in the back of your hand. You notice her injection has something to it. “Hey, what the hell?”
Everything quickly becomes blurry; you struggle to keep your eyes open, and when you do manage to, you instantly feel sick, noticing the walls around you keep changing. You look up and see a man in scrubs pushing your bed, with the same nurse who knocked you out beside him.
“Peter?”
Smirking, Peter pulls down the mask covering his face. “I always said you weren’t dense, Mori.”
—
“I don’t understand; explain it again.”
Peter rolls his eyes and lets out a dramatic sigh. “I’ve already told you the plan twice.”
“You probably shouldn’t have drugged me then.”
He puts one of his sharp claws underneath your chin and says, “Careful.”
“Stiles won’t help me hack into Scott’s laptop until he knows you’re safe and sound." His voice oozes with sarcasm. “I need both Scott and Derek to kill the Argents.”
“Scott will never help you.”
“Oh, he will.” Peter pulls out a mobile from his pocket and dials; the phone only rings for a few seconds before someone answers. “As promised, I’ve not harmed her yet.”
“𝙼𝚘𝚛𝚒, 𝙼𝚘𝚛𝚒!”
“Stiles!”
“𝙰𝚛𝚎 𝚢𝚘𝚞 𝚘𝚔𝚊𝚢?”
You didn’t know how to answer him. Your cuts and bruises were beginning to heal on their own, but you were stuck alone in a room with the alpha. “I’m with Peter.”
“Time to hold up your end of the deal, Stiles.”
“𝙾𝚔𝚊𝚢, 𝚞𝚖, 𝚐𝚒𝚟𝚎 𝚖𝚎 𝚊 𝚏𝚎𝚠 𝚜𝚎𝚌𝚘𝚗𝚍𝚜.”
Peter smiles with a strange look in his eyes, twirling your hair around his finger while you listen to Stiles typing on a laptop through the phone.
“𝙸’𝚟𝚎 𝚐𝚘𝚝 𝚒𝚝. 𝙸𝚝 𝚜𝚊𝚢𝚜 𝙳𝚎𝚛𝚎𝚔 𝚒𝚜 𝚋𝚎𝚒𝚗𝚐 𝚔𝚎𝚙𝚝 𝚊𝚝 𝚑𝚒𝚜 𝚘𝚠𝚗 𝚑𝚘𝚞𝚜𝚎.”
Peter slams the phone down, causing it to break. He seems lost in the light for a while before turning to you and running his claw along your jawline before pricking your skin just below your ear enough for it to bleed. "Fascinating." His eyes glow slightly as he watches them heal. Peter shifts his gaze to meet yours. “Did you know your brother is back in town?”
“K—Kyle?”
“Yes, and we wouldn’t want anything to happen to him, now would we?”
You shake your head and say, “No, what is it you want from me?”
“The Argents want to leave, but you're going to get Kate and Allison to Derek’s location within the next hour.”
“And in exchange, you won’t hurt my brother, Stiles, Scott, Derek, or Lydia?”
He nods.
“And what if I can’t?” Tears roll down your cheeks. “I don’t know Allison that well; she wouldn’t just skip plans on leaving town to hang out with me.”
“Don’t worry, I’ll tell you exactly what to say. And if you tell anyone what we are planning, even Stiles, you can kiss your parents and brother goodbye.”
—
As you step further into the forest, you realize that you don't know what to do or how completely out of your depth you are. You did exactly as Peter said and called Allison and tearfully told her Scott had lied to you as well about being a werewolf, but you knew where he was and wanted to confront him.
It hadn’t sunk in how big of a mistake you made until you saw both Kate and Allison welding weapons when they got out of Kate’s car. You felt even more unease when Kate handed you a pellet gun. “Do you know how to handle this?”
“No,” you say, shaking your head, and try to push the gun back to her. “I’ve never even held one.”
“Take it,” she says firmly. “Trust me, we are dealing with rabid dogs whose only purpose is to kill.”
“She’s right, Mori; you need to be able to protect yourself.”
It was sad to see how brainwashed Allison had become. Reluctantly, you took the gun from Kate.
You were trying so hard to keep your brother and friends safe from Peter that you hadn’t thought about the Argents trying to kill them. You clear your throat. “What are you planning on doing to Scott once you find him?”
Kate slows her pace, so Allison can’t hear anything her aunt says. Kate cocks her brow and says, “Whatever's necessary to stop him from harming Lydia. Is that going to be a problem?”
You remain silent. Stiles had texted you, saying Kate was the one who set the fire in The Hale’s house, killing everyone.
Kate was a cold-blooded killer; at least that’s what you kept telling yourself to justify handing her over to the alpha to protect your friends.
“Shh,” Kate says, putting her fingers to her lips. “You hear that?”
Allison nods, but you look around clueless until you spot Derek and Scott walking towards what remains of the Hale house. Out the corner of your eye, you notice Kate raising her gun, and without thinking it through, you kick Kate in the shin and say, “Scott, Derek, run!”
Kate throws you to the ground easily and holds you there while pointing her arrow at Derek.
“You don’t need to do this,” you plead. “Allison, you’re not a murderer; just let them go.”
She ignores you and shoots Derek in the shoulder and then in the leg before firing a flash bolt. The flash causes your vision to become fuzzy, and the feeling of being dragged underwater returns.
—
You feel weak as someone helps you stand. “Derek?”
“You good?”
You nod. “Are you; you’ve just been shot twice?”
Shooting a glare in Allison’s direction, he scoffs, “I’m fine.”
Hearing a clattering sound coming from his home, he shoots his head in that direction. “What’s wrong?”
“Scott’s in trouble.”
“Go, go.” When Derek lets go, you stumble slightly but hold onto a tree for support.
You feel like you’re burning up, but there’s nothing physically wrong with you. You roll up your sleeves to look at the bite mark on your arm and are horrified to see it was completely healed. The sudden urge to scream overtakes you, so you do. As you scream, you feel a wave of panic and frustration as the sound of rushing water overflows all your other senses. You only come back to reality when you feel a familiar warmth of arms wrapping around you.
You don’t even need to open your eyes to know who it is, “Stiles.”
“It’s okay.”
When the smell of smoke fills your nostrils, you open your eyes to see Peter's burning body falling to the ground. Squeeze Stiles tightly. “What am I?”
He whispers, “I don’t know, but we’ll figure it out, I promise.”
You cling to Stiles as Scott chases after Derek, begging him not to kill Peter. “Wait! You said the cure comes from the one who bit you. Derek, if you do this, I'm dead. Her father, her family—what am I supposed to do?”
Claws extend from Derek’s nails as he raises his arm up.
“Wait! No, no! Don't!”
Derek slashes Peter's throat, then slowly stands, and I’m a distorted voice saying, “I'm the Alpha now.”
—
𝙵𝚛𝚘𝚖 𝚂𝚝𝚒𝚕𝚎𝚜 —
𝙻𝚢𝚍𝚒𝚊’𝚜 𝚋𝚒𝚝𝚎 𝚑𝚊𝚜 𝚑𝚎𝚊𝚕𝚎𝚍.
𝙵𝚛𝚘𝚖 𝚂𝚌𝚘𝚝𝚝 —
𝙷𝚊𝚟𝚎 𝚢𝚘𝚞𝚛 𝚙𝚊𝚛𝚎𝚗𝚝𝚜 𝚐𝚘𝚝𝚝𝚎𝚗 𝚑𝚘𝚖𝚎 𝚢𝚎𝚝? 𝙸𝚏 𝚗𝚘𝚝, 𝚢𝚘𝚞 𝚌𝚊𝚗 𝚜𝚝𝚊𝚢 𝚊𝚝 𝚖𝚒𝚗𝚎 𝚝𝚘𝚗𝚒𝚐𝚑𝚝.
𝙵𝚛𝚘𝚖 𝚂𝚝𝚒𝚕𝚎𝚜 —
𝙷𝚘𝚠 𝚊𝚛𝚎 𝚢𝚘𝚞 𝚏𝚎𝚎𝚕𝚒𝚗𝚐?
𝙵𝚛𝚘𝚖 𝙰𝚕𝚕𝚒𝚜𝚘𝚗 —
𝙸’𝚖 𝚜𝚘𝚛𝚛𝚢.
𝙵𝚛𝚘𝚖 𝚂𝚝𝚒𝚕𝚎𝚜 —
𝙰𝚗𝚜𝚠𝚎𝚛 𝚖𝚎, 𝙱𝚎𝚕𝚕𝚒𝚜𝚊𝚛𝚒𝚘
Gulping down, you shove the phone into your pocket; you couldn’t think straight with different messages coming through at once.
“Where do they think you are?
“At home, I guess.”
“Why did you come here alone?”
Derek lets out a dark chuckle as he walks across the creaking floorboards. His house was dark, and the only part of him you could see was his glowing red eyes. But unlike with Peter, you didn’t feel scared; you knew Derek wouldn’t hurt you.
“I want to know what I am.”
#Teen wolf#stiles stilinski/you#stiles stilinski/reader#stiles stilinski x reader#stiles stilinski x you#teen wolf rewrite#teen wolf fanfic#stiles stilinski#stiles stilinski fanfiction#Stiles Stilinski x fem reader#Stiles Stilinski fanfic#teen wolf x reader#teen wolf x you#teen wolf fanfiction#In the shadows
89 notes
·
View notes
Text
patron saint of the lost causes (2/2)
“You can stop looking at him like that.” Taki’s voice is frank, but not unkind.
Katsumi could not be less in the mood for whatever the hell kind of conversation this is about to be. “Like what,” he replies anyhow.
“Like you broke his best friend."
ao3 link | part 1
Given every piece of information Katsumi knows or can infer about Tanuma Kaname, it is the most on-brand thing in the world right now for him to be looking both embarrassed and apologetic while also lying in a goddamned hospital bed. Still very much connected, he might add, to all the equipment necessary to prevent his own body from cooking up his brain and all his organs. Doesn’t mean it isn’t weird. And bad. Very weird and very bad.
They’re allowed in to see him in groups of no more than three at a time, and for no more than ten minutes each. He’d been awake and asking about them, but his fever’s still high if no longer imminently lethal, and he’s apparently still groggy from coming off the tail end of some sedative they’d pumped into him hours ago to keep him from shivering while they’d worked to combat said fever. He’s with Natsume, and they’re the first ones in, and that really, truly and honestly blows. Because Natsume’s silent and tense beside him, because Tanuma’s somehow managing to both look like a ghost and also like he really wouldn’t mind ghosthood all that much, eyes that he can’t even keep open all the way fixed on his lap. At least if Nishimura had come in before him, he’d have had a handful of stupid jokes up his sleeve.
Doesn’t help, obviously, that they’ve seemingly got him hooked up to the complete goddamn works here: the IV drip, the cords of the vitals monitors snaking out from the rumpled neck of the yukata-type gown they’ve got him in. The low beeping from the absolute behemoth of the monitor itself beside the bed that’s got to be 15 years old at least, blocky numbers and jagged lines, hills and valleys in neon colors scrolling the tiny black screen. The chunky wired clip on his finger that Katsumi vaguely recognizes from TV but cannot for the life of him remember its purpose. And to cap it all off, the oxygen tube thing—cannula?—under his nose (which, what the hell, can he not even breathe properly right now). Like it’s all been pulled from some film set for dramatic flair. Maybe less sleek, with more underfunded-isekai-emergency-room vibes, but if anything that just piles on the nightmare fuel.
And he looks embarrassed about it. The fuck.
For few vastly uncomfortable seconds, nobody says anything at all. He’d thought Natsume would take the reins on this, but he doesn’t even look to see what the holdup is, because Katsumi himself is still mucking through what there even is to say. No matter that he’s had hours to prepare, even practiced it once or twice in the bathroom mirror like an absolute lunatic, but he’s also been roundly warned by the others that any variation of why the fuck didn’t you say anything was off limits.
It’s Tanuma who eventually speaks first. “I—“
“Save it,” is the first thing out of Katsumi’s mouth, because of course it is. Tanuma winces, and Natsume promptly elbows Katsumi in the ribs. Off to a great start. “We already know,” he amends. “Your dad told us you probably didn’t realize.”
Tanuma looks up, then. And yes, his gaze is maybe still little drug-hazed, but Katsumi’s still not sure how to feel about the look on his face, like Katsumi’s a math problem he can’t quite work out. He nods, slowly. “I’m sorry.”
The room isn’t even a room, really, just one cramped, curtained-off corner of a space containing three other beds. There’s a single, worn chair wedged in beside the bed, and Natsume drops into it now, now at Tanuma’s eye level. He reaches out, and Katsumi doesn’t miss the split half-second where his hand falters midair before coming to rest carefully on Tanuma’s forearm, fingertips just skimming the IV tube taped there.
“Sensei checked around,” Natsume tells him, tone gentle but serious. Huh. Little abrupt, not the first thing Katsumi would’ve expected out of his mouth here. “He said there wasn’t anything he could find, but. You weren’t attacked, were you?”
Tanuma frowns, like he wasn’t immediately expecting the question either, but then something seems to click behind his eyes. “I don’t think so?” he starts, and purses his lips like he’s thinking. His words are lower and slower than normal, but otherwise he doesn’t actually seem all that out of it, just exhausted. “I don’t remember that much. But I think it’d feel…different, than this.”
Something in the set of Natsume’s shoulders loosens, just barely. “How are you feeling?”
“Better,” he says, after a moment of consideration. And Katsumi doesn’t mean to snort, it just sort of comes out, but he immediately feels like a dick when Tanuma’s mouth twists and he drops his gaze again. But before he can backpedal on that, Natsume shoots him a look that could strip paint right off a wall, and he figures that shutting the fuck up is the best course of action.
But to be perfectly fair to himself, the guy can’t even sit up on his own without the raised end of the bed, and his face is the same eggshell color as the cheap sheets tucked around him, wherever it isn’t blotched up from his fever of fucking 39.
“…I mean,” Tanuma starts again, “not great or anything, but. Headache’s mostly gone, and,” he turns his head a little to indicate the blue pillow-like object under his head that Katsumi is only just realizing is an extra large jelly ice pack thing. “These are really cold but they’re helping a lot. There’s some more under my arms and legs.” He raises his shoulder a bit, and Katsumi notices the slight lumpiness of the yukata on the sides of his chest that must be more ice packs tucked under his armpits.
Natsume lets out a breath. “That’s good,” he says, and his smile seems much less forced now, softer. “Before you’re discharged, we’ll make sure nothing was out there, so. Don’t worry.”
“I won’t,” Tanuma says, and he’s clearly picked up on the undercurrent of fear in Natsume’s questions. “Thank you.”
It’s not like it’s a bad thing to see Natsume willing to actually feel his goddamn feelings in front of other people, it’s a definite improvement over the vapid not-quite-smiles and the empty eyes he and his classmates called creepy when they were kids. But this, he can definitively say, also sucks. Nishimura had briefly mentioned something about Natsume having been pretty shaken up when Kitamoto had been hospitalized for some minor accident a few months back, but it seems to go deeper than that, here. As if he’d implicitly blame himself for any and all nasty youkai shit in this apparently nasty-youkai-shit-infested-town. When he wasn’t even there. And, granted, Natsume might not respond well to it coming from Katsumi, but it is dumb, and Natsume should know that he is in fact being dumb.
The thought of said nasty youkai shit makes Katsumi remember to fish the little wood talisman out of his pocket. Maybe it’s not the time to bring it up, when Natsume’s freaked out enough as it is, but they’re going to be kicked out of here in about seven minutes. Some ENT had pried it out of Tanuma’s fingers in the back of the ambulance when they were trying to get an IV into his arm, and had passed it over to Katsumi. He found out soon enough that Taki had made the thing, using some obscure old exorcism texts from her grandfather’s library, which he’d honestly found pretty impressive until Sensei had had to ruin it by noting that the flimsy thing would have about the same repellent power against an average youkai that a squirt gun might have on a bear. Which, at least, made it seem it less likely that he’d been clinging to it because he really thought something was going to attack them. But when Katsumi had tried to return it to Taki, she’d given him a maddeningly incomprehensible look and just said, “Give it to him yourself.”
So he is. Hope she’s happy, because he for one feels some heavy sort of way about it that he does not have the energy to parse out right now.
“You dropped something,” he says, because that’s simpler than the truth. There’s not really room to squeeze himself in near Natsume at the bedside, and the other side’s got that mammoth monitor machine taking up most of the narrow space, so he just sort of hovers behind Natsume somewhere beside Tanuma’s legs. He reaches over, drops the talisman lightly on his knee.
Tanuma blinks down at it, slowly raises his hand to place overtop of it. The movement is awkward and slow, between the clip on the finger of this hand and the gel pack wedged under his arm, but his remaining fingers close around it. He looks up at Katsumi, eyes wide. “You—“
“It’s whatever,” he says with a shrug, before Tanuma can even get the words out. He’s not in the mood to be thanked right now. “It, uh. Looked pretty important, though. You were squeezing it damn tight enough.”
That earns him a sharp over-the-shoulder look from Natsume, a don’t-you-fucking-tease-him-or-so-help-me-god face if ever Katsumi saw it.
Katsumi ignores him. That wasn’t the point. Because despite the fact that Sensei had patrolled the area, and that it made the most sense that he’d been clinging to the talisman out of some delirious attempt at self-soothing, if there was any chance he’d been desperate to grab for it because it was better than nothing at all if something was hanging around, that’d be pretty damn good information to have before any of them have to walk that road again. Maybe seeing it would jog his memory.
Apparently not, though. He manages, awkwardly, to flip the thing over so it rests in his palm, even though it jostles the clip just enough to elicit a few abrupt pi-pi-pis from the machine beside him. “All I really remember,” he says, at length, “is leaving home, then Lawson, kind of, and then, ah.” His eyes flick upwards, for the barest second, not even making it up to Katsumi’s eyes before his gaze drops right back down like a stone.
“What?”
Tanuma’s fingers close tight as they’re able around the talisman, and he looks so thoroughly miserable that Katsumi’s starting to be sorry he asked.
“I remember throwing up on you,” he mutters.
And that startles a chuckle out of Katsumi. It’s a sharp, awkward sound in the hush of the room. But it feels good, like a crack forming some gigantic dam that barely fits in his chest anymore. Another follows.
Natsume glares.
And okay, yes, it’s got to be a dick move to be laughing right now. The splotchy bits of Tanuma’s face have grown even splotchier as he stares down at his talisman, and the heart monitor’s tempo has kicked up a bit.
“Seriously?” Katsumi manages, catching his breath, before Natsume gets the chance to declare war here. “That’s the part you remember.” The guy’s subconscious must really have it out for him, because Tanuma legitimately looks like he’s about to faint.
And that’s no good, either.
“Look,” he starts, and drops down to perch awkwardly on the bedside edge somewhere near Tanuma’s shin, opposite Natsume. At least like this he’s not looming like a creep over the foot of the bed anymore. “For life-threatening situations? Free pass. And I got some new threads out of it anyways,” he says, plucking at the sleeve of his borrowed shirt. “Timeless classics.”
They actually look fine, some nondescript green button down and dark chinos belonging to Shigeru-san, though when he’d thrown them on this morning he’d barely even registered what he was wearing anyhow. Nishimura, Kitamoto and Taki are all wearing the same clothes they’d worn yesterday, still a little damp from being hastily laundered and hung to dry indoors overnight, but Katsumi’s things are currently still soaking in a bucket of oxygen cleaner on the Fujiwaras’ veranda, and Natsume’s clothes are all a size too small for him.
“It’s not your fault for getting sick,” Natsume tells him, gentle but direct, when Tanuma doesn’t immediately respond. Which is exactly what Katsumi just said. But whatever. Tanuma huffs out through his nose, a soft halting sound that makes an odd little whistle over the top of the cannula, and finally looks up at Katsumi. There’s something taut behind his eyes, but least he looks marginally less like wants to evaporate into the goddamn ether anymore.
“I, just.” He shifts in his seat a little, swallows, but keeps talking. “This all must’ve been…a lot, for you, so. I’m sorry. Thanks for getting help.”
“‘Course.” Katsumi shrugs, still not really sold on the idea of being thanked right now. “I’m not a total monster.”
That, at least, elicits some sorry little suggestion of a smile from him. He’ll take it.
“But, with your dad saying you didn’t realize, though,” he starts, before he can think better of the question. “Has this happened before?”
Natsume looks a little wary, as though he’s ready to shut this conversation right down if need be—which, fair enough—but is also watching Tanuma like he isn’t exactly not curious, either.
But Tanuma says, “Sort of?” and cocks his head like he’s trying to remember. “In third or fourth grade, maybe. There was this school clean-up event just before the summer break, and…I don’t exactly remember what happened, but I guess the teachers realized when they did a head count at lunch.” He shakes his head a little. “Anyways. That town was…we didn’t live there long.”
Katsumi’s not at all sure what to make of that last bit, though Natsume looks perturbed by it. But something’s not quite adding up regardless. “Wait,” he says, frowning, “if this was a school clean-up, wouldn’t you all have been working in pairs or groups or something?”
Tanuma shrugs. “I guess?”
“You got ditched,” Katsumi concludes, flatly. “That’s fucked up.”
“…I mean…” He’s starting to look uncomfortable again, his fingers picking at the edges of the talisman. “I couldn’t actually attend school there all that often, so. I didn’t really know many people’s names, or anything. It’s okay, really.”
No, it’s fucked up, he wants to say, only to remember the other person in the room right now. Natsume doesn’t look particularly happy to hear this story, but he doesn’t look surprised, either. Like he very much gets it. And Katsumi’s acutely aware that he himself the last person who should have anything to say about any of this at all.
And the kicker is, yeah, he knows how cruel and ugly kids can be to each other, because god knows Katsumi was, but this doesn’t even sound like that. Tanuma had recounted it as though he were as good as a stranger to his classmates, and vice versa.
Katsumi glances at the talisman again, at the marker ink that’s gone splotchy in the corners visible under pale fingertips. And, unwillingly, he thinks of some sickly nine-year-old, lying lost behind some tree or tool shed, nobody looking for him at all.
A long buzz from his pocket punctuates the silence. Then another. Katsumi doesn’t need to fish his phone out to know it’s Mom. Again.
“It’s fine,” he mutters, when two pairs of eyes flick towards him. “I’ll get it later.”
He’s been putting off actually speaking to her; he knows Touko-san called her sometime yesterday and since then he’s mostly just been sending her messages to check in and vaguely reassure her. He’ll have to talk to her soon, but he likes to think he’s got enough dignity left in him to not want that to happen anywhere remotely near any of these guys. The thought makes something itch in his throat.
“You know,” Tanuma starts, after a moment, voice quiet but clear. “It really is okay for you to go.”
“Nah.” Katsumi shrugs. “Like I said. Nothing better to do back home either. Except get nagged about holiday homework.”
Tanuma nods, once. He doesn’t necessarily look unhappy, but there’s a thread of unease in his voice. “You’re welcome to stay,” he says, “but…you’re here for, what, five more days? Six? And, ah.” He casts a glance at that giant beeping machine beside him, then around the cramped room that doesn’t even have a window or real walls. And he looks so tired. “I’ll be here. And then on bedrest when I’m out, they said, so…”
Katsumi frowns. “…so?” he echoes. “Is this about the cleaning? ‘Cause fuck the cleaning.”
Tanuma just blinks, nonplussed, and Natsume sighs and rubs vaguely at his temple like he’s got a headache coming on. “Shibata,” he mutters, but there’s no bite to it.
Katsumi rolls his eyes. “I meant, it’s not your problem right now.”
“But it shouldn’t just be yours, either,” Tanuma says, gaze drifting back to that damned machine again. “You’re here because I asked, and now there’ll be even more, with less time.”
This is starting to feel like a stupid conversation to Katsumi, because he has the suspicion that even Tanuma’s dad wouldn’t be all that bothered right now about offending someone’s dead great-great-aunt on Obon with a dusty altar or two. So it’s probably for the best that Natsume speaks up before Katsumi has the chance to.
“He is right that you don’t need to worry about it right now,” Natsume tells him. “But, there’s still plenty of time, too. And Sensei and I can try and find some extra hands, too.”
“Extra…” Tanuma frowns. “Would that work, though?”
Katsumi’s not a hundred percent on the specifics here, but he’d heard in passing from Sensei that most of the local youkai population weren’t too keen on hanging out around Yatsuhara Temple. Natsume’s finger drums lightly on the bedrail, like he’s considering, and then there’s a flash of…something…in his eyes, something steely enough to maybe just unnerve your run-of-the-mill forest-dwelling flesh-eating folkloric monster.
It’ll be fine.
“Either way, it’s just an extra day or so, right? We’ll get it done,” Natsume says, decisively.
“Yeah, we spent a lot of the first couple days just kind of fucking around, anyhow,” Katsumi adds. It’s not all that true—there had been a little downtime in the evenings, some idle rounds of shogi on the veranda, placing bets against each other on pocket change and cheap snacks, but they’d all more or less collapsed into the lumpy borrowed futons by 10PM each night. It still sounds like a helpful thing to say. Maybe. “We’ll just hustle a bit. It’s all good.”
Tanuma looks torn. “I…thank you. Really. But, I’m the one that actually lives there.” His expression settles on a rueful smile. “And I couldn’t even walk to the store, so. I’m sorry.”
Okay, yeah, no, this is stupid, actually.
Katsumi huffs. “Yeah, all according to your big evil master plan, huh. Luring us all here just to do all the heavy lifting.”
Natsume’s head snaps up sharply at that, and Tanuma just stares, but Katsumi plows on.
“Because that’s how chronic illness works, right? If you can’t just guess and pinpoint all its exact fucking whims day to day, which, by the way, are caused by invisible invisible monsters half the time anyways, then you’re just a super inconsiderate guy, huh. Oh, and dramatic. ‘Cause that’s totally what we’ve all been sitting out there thinking.”
He’s met with silence, from both of them. Which is, basically, the worst possible reaction to receive when you’ve just been on the verge of shouting at someone stuck in a hospital bed. Natsume had looked, at first, reflexively ready to bite right back, but instead he’s watching Tanuma, like he’s holding his breath. They both are.
It’s not a term he’s given much thought to before. Ever, really. Until earlier, hearing Tanuma’s father’s half of a hushed, somber call with some relative or another from the lobby (“…symptoms of heatstroke, but the chronic illness had exacerbated the situation, so at the moment, he’s…”).
Katsumi wonders, vaguely, how they’ve must’ve had him classified in his charts over the years. Generalized Youkai Shenanigan Disorder must be a real head-scratcher to the medical community at large.
But he looks normal, is the thing. A bit underslept, sure. And lugging heavy boxes around all day gets him winded a little faster than the others. And he takes more care than the rest of them to stop for water, but that’s just being responsible. It wasn’t like he hadn’t kept up, hadn’t been fine.
Katsumi had only got the most cursory of explanations, back when they’d first met. That he’d been sick as a kid a lot, moved around often because of it, that it had gotten a lot better when he’d moved here, met Natsume. And he looks so shockingly ordinary that Katsumi would’ve never known.
And Katsumi doesn’t know if anything really was out there in that dusty field with them. Doesn’t think it matters, ultimately.
Maybe it is better these days. And maybe it’s pointless to even speculate, if he hasn’t lived it. But it sure as hell sounds to Katsumi like living with a landmine buried in your skin. Doesn’t matter how deep down it’s sunk, how quiet it seems. Not like it’s not there.
Nobody’s said anything, still. Natsume’s watching Tanuma. Tanuma’s watching his own lap.
“Am I kicked out?” Katsumi asks, arms folding.
“No.”
Katsumi barely hears him; his voice sounds half-stuck and dried-up. But then Tanuma looks up, fully, and his eyes are wet.
Shit.
“I mean.” He clears his throat. It doesn’t do much. “Soon? But. Not by me.” He seems to realize about the tears, then, and absently reaches up to scrub at his eyes.
Which, naturally, knocks the mysterious beeping finger clip right off, sending it flying right over the side of the bed.
The behemoth next to the bed immediately starts pi-pi-pi-ing, urgent and shrill, and Katsumi swears, swooping down to snag the little clip by the wire now dangling over the bedrail, and slides it back onto Tanuma’s finger. He doesn’t have a clue if it’s on backwards or not, and is only pretty sure that it had been on his index finger before, but at the very least the noise dies down. And he can’t hear anybody rushing in to check if they’ve killed someone, for the moment.
“Sorry,” Tanuma murmurs, while Natsume readjusts the cannula thing he’d knocked a little crooked. The tube’s kind of misty now, just under his nose, and Katsumi briefly wonders what happens if that thing gets too clogged up with snot to work properly.
Because Katsumi had to go and run his mouth.
Natsume fishes out the talisman from where it’s fallen into the sheets, and presses it back into Tanuma’s palm. “We came to help,” he tells him, snatching a corner of the bedsheet to help mop up his cheeks before he can forget again about the clip, or jostle the IV port or gel packs. “So let us. And rest, okay?”
“Yeah,” Katsumi mutters. “That.” He feels like he’s hovering, blunt and mean and too big for his own skin for this tiny-ass non-room. Glances at his watch, scuffs his heel on the floor. “It’s almost time. You know Nishimura’s probably gonna deck me for making you cry.”
Katsumi can’t immediately clock the sharp little hiccup as laughter. Sounds a little more like an injured corgi to him, but when he looks at Tanuma, there’s a little waver in the set of his mouth, and his shoulders have relaxed, just a bit.
Natsume’s expression is dry—you’d have brought it on yourself if he does—but he seems mollified, his hand having found its careful way back onto Tanuma’s arm like it was coming back home.
Tanuma looks up. His eyes are still red-rimmed, but that desolate look has receded somewhat. “You didn’t—“ he starts.
“I mean, I did,” Katsumi counters.
Tanuma smushes his lips together, tries again. “I’m okay.”
Katsumi raises an eyebrow, makes a vague sweep of the arm around the terrible little space, all the equipment crammed around and connected to him. “Yup. Clearly.”
Tanuma sighs, just looks at him for a moment. And maybe it’s not an improvement, Katsumi thinks, if Tanuma’s circling back to just finding him exhausting to talk to, but then that’s no worse than yesterday before all this shit began.
“Thank you,” Tanuma tells him, finally. His voice is soft but sure.
Katsumi shrugs. Always down to bully a hospital patient. I’m your guy.
But the words dig in, stick in place like nettles. And it hurts, kind of, a nagging sort of prickle embedded in Katsumi’s chest.
It’s not so bad, though.
“Sure,” he offers. “Now rest up, or else. This place is the worst.”
***
#natsume yuujinchou#natsume's book of friends#natsume yuujinchou fanfic#natsume yuujinchou fanfiction#tanuma kaname#shibata katsumi#natsume takashi#nishimura satoru#kitamoto atsushi#taki tooru#goodlucktai#owlet's fanfic#finished just in time for obon#thanks for the kind tags on the last chapter guys#it's been a hot minute and I struggled to get this done so it made me really happy to see#posted at 4:30AM because time is a mere human construct
26 notes
·
View notes
Note
Just found your blog based on your new fic, which I loved! I was most excited by the medical accuracy knowledge. Do you have any old posts or thoughts about the medical accuracy for Danger Magnet Strand’s NDEs? I know the show is A Bit Not Good with that. I can’t find anything useful on recovery from severe hypothermia and it is driving me nuts.
I could literally write a dissertation on how terrible the medicine in this show is, but I will do my utmost to keep from doing that. Everyone at work makes fun of me, but I fell in love with these damn characters.
The shooting drives me absolutely crazy. “Well, it missed the subclavian artery, so he’s fine!” No. Absolutely not. He would at the very LEAST need physical therapy. It’s his shoulder! Do you know how much is happening up there??? Here have a picture... (under the cut because I am long winded)

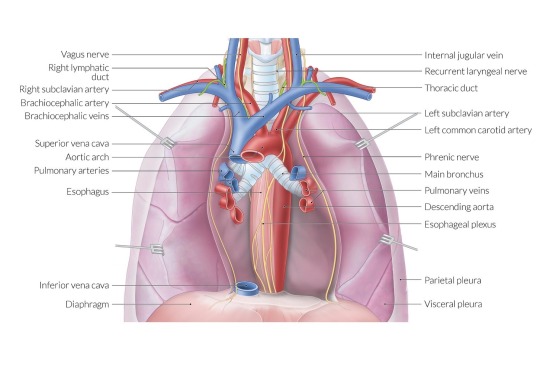
TK would’ve come in as a trauma alert GSW to the chest. His chest!!! And he’s back at work in 10 days??? No!
I’m assuming they had him in a coma as a result of hypovolemic shock? I don’t know. It remains unclear. But that boy literally only had a nasal cannula the whole time? At the MINIMUM he would’ve come out of surgery with the following:
Art line
Central line
Temp sensing foley
NG/OG tube
AT THE MINIMUM 1 chest tube. Probs more tbh.
But I digress. You’re here for severe hypothermia. And boy do I have some THOUGHTS on this.
First of all, ECMO started in the back of a rig??? No, fucking way.
But this is supposed to be about TK, so…
You’re telling me this kid ran naked out into negative degree temperatures and rolled around on the frozen ground and there wasn’t any frostbite? Ha!
Let’s start from the beginning. So the call to the ER for TK would be traumatic arrest with ROSC achieved in the field. He should be intubated before he arrived, but this show doesn’t care about intubation. So let’s say they bag him all the way to the hospital.
When he arrives in the ER he’d be taken to the trauma room and 8 million things would happen at once. The first thing would be intubation. If a patient is intubated they need (at the very minimum) the following:
Sedation and paralytic medications
Central line
Art line
Temp sensing foley
OG tube
Because of the severe hypothermia his temperature would be monitored with a nifty esophageal thermometer. While the temp sensing foley gives bladder temp it’s behind until he’s warmed up enough.
He would also get warm IV fluids and peritoneal lavage, which is where we poke a hole in your tummy and introduce warm fluid that way. He’d also get the bair hugger which is a fun little plastic blanket type thing that inflates with warm air. (We break out the machine on night shift and put it at the nurses station. Best thing ever invented.)
Labs would be drawn and be all over the place because ice blood!! We’d probably be able to get him up to an ICU bed in an hour or two. I’d say he’d be a 1:1 for whatever ICU nurse gets him just because with all the monitoring for the first few hours it’s be impossible to get out of that room. If the nurse was 1:2 with a patient like TK the other patient would (re: should) be an easier patient. But in this post COVID world that ain’t happening. 😂
Recovery would be a verrrrrrry long road. With concern for arrhythmias and hypoxic brain injury and muscle atrophy. And then just soooo many other things. And the reason you can’t find anything useful is probably because TK would’ve died in the real world. Not a lot of people come back from that.
So this got away from me. I’m sorry. Here have some links.
This is a great article about hypothermia
And here’s a video of an actual hypothermic patient being treated in the ER so you can see all of the equipment that would be needed.
Obviously, I love to talk medicine. My inbox is always open for this. Just be prepared for me to go overboard. Sorry.
No idea if this helps or not. 🤷♀️
14 notes
·
View notes
Text
@lediableblanc-amoureuxdechats
Continued from here !
She knew she was being a bit of a bitch. In hindsight, she wouldn't feel great about it- the poor nurse was only trying to do her job. But Rogue was angry.
And scared.
If Remy had been under Hank's care, not only would she know he was okay, but he'd be with other mutants like himself and she'd be at his side right now.
Instead, he was stuck in a hospital. A normal, every day, hospital. And she didn't trust a damn soul in this place with his care if they knew what he was. Add to that that they weren't letting her in to see him…
Oh, her anxiety was through the damned roof. And that meant her temper was getting there, too.
"Miss, it's against policy-"
Rogue pointed a gloved finger directly at the nurse, this simple action (coupled with her tone and the expression she wore) enough to get the other woman to stop talking. "I know. It ain't visitin' hours. I ain't his wife. I'm not family. So you won't lemme see 'im. But I'm tellin' ya- that's my man in there. An' I ain't movin' from this spot 'til ya let me in t'see 'im. Ya understand me? So you can take yer policies an'-"
Her eyes snapped towards the door at that sound. Remy had hit the call button and alerted the nurse to his need for something.
Rogue's heart raced.
The nurse quickly excused herself then... had to shut the door in Rogue's face because she had followed the nurse closely, as if thinking she could sneak right in behind her. Which, of course, didn't work and left the southerner practically fuming. She was right there on the verge of stomping her foot like an angry child or, worse, kicking in the door.
Why the hell couldn't they just let her in? Just for a couple minutes. Just long enough to check on him. To see him. (To... probably then refuse to leave his room, all things considered.)
But she needed to know: Was Remy okay? Were they treating him well? Was the nurse being kind? Or was she the type to be short and bitter with him all because of his eyes?
Oh, if that was the case…
Her foot tapped rapidly against the floor, and the sounds of the rest of the hospital still busy at work were starting to grate on her. Too loud. Too much. Too crowded. She felt it in her stomach, in her chest, a pressure at the back of her head that made her feel like she might explode…
She just wanted to see Remy. Even if she had to make a scene. There wasn't a soul who'd be able to keep her from him.
Yet she still took a small step back to let the nurse out of the room when the door opened.
Except, the woman didn't shut the door behind herself this time…
Rogue's eyes narrowed at her.
"He said to let you in," The nurse explained, though she didn't seem too happy about it. Maybe she was just frustrated that she'd argued with Rogue all that time for nothing. Or maybe she was just tired of the whole situation. Rogue… hadn't been making it easy on her.
"That wasn't so hard, was it?" Rogue asked. Then, realizing she was being snarky despite getting what she wanted, she felt a bit of shame. Her next words were said more genuinely. "Thank you. I'm just worried 'bout 'im..."
"I know," Was the only answer back before the nurse walked away and Rogue was stepping into Remy's room, shutting the door behind herself.
She breathed a sigh of relief as the door clicked closed, then she raised her gaze to look at Remy. Her Remy. Lying in a hospital bed. Patched up. IV in his arm. Oxygen being fed to him through a cannula. They hadn't told her what was wrong with him, just that he was stable. He was alive.
Her chest tightened as she stared at him, and she wasn't sure if she wanted to start scolding him for his recklessness or if she just wanted to kiss him.
She couldn't kiss him, unfortunately, so a bit of scolding was in order. (Besides, it was always easier to express herself through anger...)
"Remy Etienne LeBeau, you reckless idiot," There was some fire behind her words, arms crossed, that stern look finally spreading across her face as she approached his bed. Brows furrowed. Lips pursed. Jaw clenched. There were about a thousand things she wanted to say to him, but they were all bouncing around in her head a thousand miles per hour and she was having trouble sorting them out. So the silence that followed that first sentence wasn't because she wanted to be silent, it was because she was struggling with what to say next.
Her eyes moved from him to take in the room, as if searching for anything to be wary of. Any signs of tampering or cruelty. She saw nothing of the sort, but that didn't mean she wasn't still slightly on guard.
What she did find was a chair near his bed. One that she dragged even closer, seating herself so near to him that her knees were bumping that hospital bed frame that cradled his mattress.
Now that she'd had a second to sort her thoughts, she was back to speaking. Whether that was a good thing for Remy or not, she wasn't quite sure yet.
"What were you thinkin'? Goin' out there by yerself. Ya coulda been killed!" She quickly raised a finger to stop him from chiming in despite her question- speaking was probably hard for him right now. She would do the speaking, instead. "Ya can't go doin' stupid stuff like that, ya hear me?" And there, finally, was that wavering in her tone that gave away the fear she'd felt. The bit of relief that she was holding onto for the fact that he was alive. "If you'd've died, I woulda brought ya back just t'chew ya out for it." And, she wasn't a religious woman, but god help whoever the hell managed to kill Remy LeBeau, because they'd have to face her.
She reached out towards him, trying to keep her hand steady. Carefully, she placed one hand against his. The other found itself moving up, fingers gingerly brushing through his hair. She just needed to touch him. Even with the fabric of her glove between. She needed to feel him beneath her fingertips.
She was quiet again, just for a few seconds, just long enough to watch him, to calm her racing heart.
When she spoke again, her voice was softer.
"Ya ain't leavin' me. Not like that. Got it? Ya want outta this relationship, yer gonna have t'do better'n tryin' t'get yerself killed," A joke. A small one, maybe ill timed, but it was an attempt, nonetheless.
#v; ''i cannot hide myself from you. i cannot hide my heart from my heart.'' // lediableblanc amoureuxdechats#lediableblanc amoureuxdechats#((I'm a sucker for the angst/fluff combo of injured Remy and anrgy/scared but attentive Rogue <3#So sorry for the fairly quick reply xD))#((Well- quick for me anyway ^^;))
9 notes
·
View notes
Text
India’s Top Triangular Bandage | Tubular Bandage | IV Cannula Fixator | Gauze Swab | Manufacturers
Triangular Bandage Manufacturers

We are the forefront manufacturer, exporter, and supplier of high-quality Triangular Bandage. It has earned us wide appreciation due to its quality, durability, and hygienic nature. Available in different forms either plain or pictorial, this bandage is generally used for first aid purposes.
Fabricated as per the medical standards using high-grade fabric and is free from external contaminants, this bandage is highly durable as it is manufactured(Triangular Bandages Manufacturers) with high precision. Further, clients can avail of this product at the most affordable price.
Features:
Material: Strong unbleached cotton fabric.
Bandage in the shape of a triangle.
Application / Usage: Hospital / Clinics
Made of 100% cotton
Complete with two heavy-duty safety pins
Most essential emergency First Aid equipment
Sizes:
96 cm x 96 cm x 135/136 cm
90cm x 90cm x 127cm
90cm x 90cm x 125cm
60cm x 60cm x 90cm
Also available in non-woven fabric.
Triangular Bandage is being manufactured and supplied by a company reputed because of excellent product quality.
Medilivescare Manufacturing is known as India’s Top Triangular Bandage Manufacturers. We provide high-quality Cotton Triangular Bandages at a very affordable price. We provide OEM Service and are known as a leading Triangular Bandage Supplier and Triangular Bandage Exporters in India. Our Triangular Bandages are exported to various African and Middle East countries.
Gauze Swab Manufacturers

Due to its extensive software Gauze swabs(Gauze Swab Manufacturers) are available both in sterile and unsterile shapes, with different ply and types relying on the absorbency required. We manufacture extensive specification and packing, and packaging SKUs for Gauze Swabs.
Sterile Gauze Swabs – Non-Sterile is a high-quality product and is trusted all across the globe. Non Sterile is being synthetic and supplied by the business enterprise reputed because of its fantastic product fine, pleasant service, and professional approach. Scroll all the way down to see specifications and evaluations.
We have also manufactured(Gauze Swab Manufacturers) a Non-Sterilized Gauze Swab. We offer the best quality highly absorbent non-sterilized Gauze Swabs in accordance with the Pharmacopeia Standards. Our product serves the desires of several commercial fitness care provider companies such as hospitals, nursing houses, etc. Our Swabs skip via rigorous assessments for quality manipulation, cloth structures, and softness due to uniform discovery free especially absorbent gauze cloth.
We are Top Gauze Swab Manufacturers in India. We offer Sterile Gauze Swab, No sterile gauze swabs, Gauze Swabs with or without X-Ray Detectable Thread, Surgical Gauze Dressing, and/or Gauze Pads at the lowest prices. Superior quality and affordable prices are guaranteed. We provide OEM also for numerous customers for Gauze Swab. We deliver Gauze swabs in specific qualities and percent sizes in step with customer requirements. We are Top Gauze Swab Manufacturers and the Best Gauze Swab Exporters in India.
Features:
Made of 100% cotton. Bleaching is done by Hydrogen peroxide & de-mineralized water.
All swabs are with folded edges - therefore No loose threads.
Available with or without an X-Ray detectable line.
Available in Quality B.P. Type 13 & B.P. Type 17.
Sizes available :
5 x 5cm (4 / 8 / 12 ply)
7.5 x 7.5cm (4 / 8 / 12 ply)
10 x 10 cm (4 / 8 / 12 ply)
10 x 20cm ((4 / 8 / 12 ply)
Available in 1, 2, 4, 5 & 10 pcs packing and Sterile / Non-sterile as per customer/project requirements.
Available in 100 pcs. packing as non-sterile.
Other customized sizes are also available such as:
35x40cm
10 x 60cm.
Product Features List :
High Absorption Capacity.
Swabs have Folding Edges, so there is no chance of loose thread.
Made from Cotton Gauze Fabric
Usage :
For cleaning and swabbing wounds.
For dressing low exudates wounds

Tubular Bandage is a high-quality product and is trusted all across the world. Tubular Bandage is being manufactured and supplied by a reputed company because of its excellent product quality, friendly service, and professional approach. We are known as India’s Top Tubular Bandage Manufacturers in India.
Tubular Elastic Bandage presents uniform compression and guide of the appendages with minimal threat of constriction. It is easy to apply and comfy to wear, without the need for any clips or tape to hold it in location. Compressive power stays regular over a long length of use.
This versatile, bandage is low in cost and a better replacement for elastic wraps and other trendy supports. Holds bloodless/hot packs or bandages in place.
Washable
Breathable and Hypoallergenic
Uniform compression
Soft to the touch, good to feel
Dermophilic, hypo-allergic, causes no rash, is soft to touch, good to feel, washable and breathable.
Tubular(Tubular Bandage Manufacturers) design allows pull-on, quick and easy wearing and fitting without any pins or tapes.
The fawn color matches skin color for better aesthetics and can be worn inconspicuously under clothing.
Product Information
Cotton Stockinet Roll / Cotton Ribbed Stockinet.
Stockinet roll crafted from pleasant lengthy-staple cotton yarn and woven on a circular loom.
A free loop knitted fabric has inherent four-way stretch assets.
Hypoallergenic Seamless Product Made from high high-quality, excellent, long stapled cotton that stays cool all through summers and warm at some point in winter.
The cloth is hypoallergenic, cleanable, breathable, soft to the touch, and feels good. Knitted on modern-day machines for a four-way stretch.
Lightweight, seamless, long-lasting, snug healthy and remains in the role for a long time.
Easy pull-on put-on is made possible with the aid of the tubular design. The packaging is convenient and in particular designed with aspect slits for smooth unrolling.
Smooth texture, shrink-resistant, and skin-friendly.
Available sizes:
4.2cm x 10m.
5cm x 10 meters.
6.25cm x 10 meters.
7.5cm x 10 meters.
10cm x 10mtrs.
12.5cm x 10 meters.
15cm x 10 meters.
Customized sizes are also available.

IV Cannula Fixator is very helpful for fixing IV Cannula and for general use. Made as per B. P. standards. Skin-collared elastic foam grip cannula fixator and porous adhesive used for air circulation. Cannula Fixators(IV Cannula Fixator Manufacturers) are highly elastic bandages that are for supporting the syringe entered into the human body to resist any strain and pain. It is made up of top-quality fabric which allows the passing of air and humidity very easily. The adhesive used is free from any toxins which makes the product skin friendly.
Product Information:
IV Cannula Fixator is shaped well to give a perfect grip over the I.V. Cannula(IV Cannula Fixator Manufacturers) during hospitalization.
Moisture-responsive High Moisture Vapour Transmission rate Film.
Low allergy grid pattern adhesive.
Porous adhesive to allow skin breathing.
Easy and Painless to do away with, because of skinny-non adhesive edges and leaves no residue after removal.
The IV Cannula fixator fastens the tube firmly to the pores and skin, whilst the pad covers the point of injection. The dressing allows air and humidity to skip freely.
The Material used does now not irritate the pores and skin and no strains of the adhesive continue to be at the pores and skin after removal.
Advanced Features:
Fixes the cannula prevents plain
Prevents infusion-related phlebitis
Breathable pores on a bandage for better skin health.
Better flexibility gives better support, the patient can move easily
Instruction for use:
Tear the pouch
Remove the release paper
Note: If you have any quarry about the quality and Price then please click the given below:
Gauze Swab Manufacturers in India
IV Cannula Fixator Manufacturers in India
Tubular Bandage Manufacturers in India
#Hospital#Medical Bandages#Hospital Uniforms#Triangular Bandages#Tubular Bandages#IV Cannula Fixator#Gauze Swab Manufacturers#Gauze Swab Manufacturers in India#Surgical Gloves#Surgical Gown#Nitrile Gloves#Manufacturer#Exporter#Supplier#India
2 notes
·
View notes
Text
Tag Game About You
Thanks for tagging me @a-reader-and-a-writer and @topguncortez
Nickname: Jessie, Merlin (my work nickname because I’m the IV cannula wizard and always managed to place catheters), ‘Bob’ from my Natasha @callsign-phoenix
Star sign: Virgo
Height: 5 foot 5 inches
Last thing I googled: Christmas biscuit recipes
Song stuck in my head: ‘Just the girl’ by the Click Five
# of followers: #footprintsinthesxnd500
Amount of sleep: 6 hours
Dream job: Veterinary Nursing which I’m training to be so I consider myself very lucky to be fulfilling my childhood dream.
Wearing: jeans and a sweatshirt
Movie/book that summarises me: Les Misérables (yes it’s a musical but it was a book first and it’s embedded in my soul)
Fav song currently: ‘Anti-Hero’ by Taylor Swift
Aesthetic: outdoor type, hiking and running with my spaniel, paddle boring, books, combat boots, messy buns
Fav authors: Jojo Moyes, Bernard Cornwell just to name a few 😂
Random fun fact: I watched the first mission impossible film today at the age of 20. No clue why it’s taken me so long 😂
Tagging: @callsign-phoenix @blue-aconite @imjess-themess @callsign-dragonbaron @mayhem24-7forever @sunlightmurdock
3 notes
·
View notes
Text
What is the ACLS Bradycardia Algorithm?
The ACLS (advanced cardiovascular life support) bradycardia algorithm is a protocol that healthcare providers use to manage patients with bradycardia. Bradycardia is a condition that slows down the heart rate to less than 50-60 beats per minute. Signs and symptoms of bradycardia include altered mental state, fatigue, hypotension, sweating, ischemic chest discomfort, acute heart failure, or signs of shock. In most cases, an individual with bradycardia does not get sufficient oxygenated blood to various parts of their body. Failure to treat bradycardia can lead to severe conditions such as syncope. However, it is worth noting that an individual may also experience a slow resting heart rate due to age or physical fitness activities. This blog will help you understand the ACLS bradycardia algorithm, its key steps and how to identify the underlying cause.
Causes of bradycardia
Identifying the main causes of bradycardia is important for effective treatment and management of the condition. Some of the factors that may cause bradycardia include:
Hypothyroidism
Inflammatory diseases
Imbalance of electrolytes
Myocarditis
Obstructive sleep apnea
Hypertension
Tissue damage due to heart attack, heart disease, or aging
Congenital heart defect
Essential steps in the ACLS bradycardia protocol
Understanding and effectively applying the ACLS bradycardia algorithm can be life-saving in critical situations. Every step is designed systemically to address and manage the symptoms of bradycardia and stabilize the patient’s condition promptly. Here are the steps of ACLS bradycardia:
Airway opening:
Ensure the patient’s airway is open. If not, you must assist the patient with breathing. You can do so while using the following steps:
Airway management: Begin by conducting an assessment of the patient’s airway. This will inform you if it is clear or not. Obstruction of the airway leads to inadequate oxygenation and may further exacerbate bradycardia. To assist the patient in maintaining the airway, you can apply techniques like jaw-thrust or head-tilt. If need be, you can also consider advanced airway management.
Assisting breathing: Once you establish that the patient is not breathing well, assist their breathing with ventilation using a bag-mask device or provide supplemental oxygen. Proper ventilation is crucial to improve the patient’s oxygen supply and lower the risk of further complications.
Administer oxygen if hypoxemic:
To measure the patient’s level of oxygen saturation in the body, use a pulse oximeter. Low oxygen levels, usually below 94%, mean that you must administer supplemental oxygen. You can deliver this either through a non-rebreather mask or a cannula. The method you will use depends on how severe the hypoxemia is. Moreover, it is not enough to administer oxygen. You need to conduct a continuous assessment of the patient’s oxygen saturation. This will guide you on how to adjust the flow rate of oxygen accordingly to ensure sufficient oxygenation.
Attach cardiac monitor for rhythm identification, monitor blood pressure and oximetry:
Use a cardiac monitor to evaluate the patient’s heart rhythm. This will guide you to know if the bradycardia is caused by a conduction problem or if it’s due to a particular type of arrhythmia. Secondly, you must measure the patient’s blood pressure to assess for hypotension. This is a critical indicator as it shows the patient’s hemodynamic stability. With bradycardia, a patient can experience lowered blood pressure and reduced cardiac output. Lastly, you must keep a record of the oxygen saturation levels. This information is necessary to ensure that the patient has adequate oxygen being delivered to body tissues.
Establish IV access:
To facilitate the administration of fluids, medicine, and other forms of treatment, you must obtain intravenous (IV) access. Consider using a large-bore catheter if it's available. This allows you to infuse medication or fluids more rapidly if necessary. Get ready to administer medications like atropine or other drugs as indicated in the bradycardia algorithm. If the patient is in shock or hypovolemic, provide them some fluids.
Obtain a 12-lead ECG:
To obtain a 12-lead electrocardiogram (ECG), place electrodes on the patient. This will provide a comprehensive view of the patient’s heart’s electrical activity, allowing you to diagnose the type of bradycardia. You will also be able to identify other underlying ischemic or structural changes in the patient’s heart. Additionally, conduct an analysis of the ECG to determine which type of bradycardia the patient has. It might either be an atrioventricular block or sinus bradycardia. This information will guide you on the treatment decisions to take.
Evaluate for symptoms:
Evaluate the patient’s symptoms to determine if bradycardia is causing major symptoms. Look out for symptoms such as signs of shock, altered mental status, ischemic chest discomfort, or acute heart failure. If any of these symptoms is present, proceed with the algorithm. Follow the protocol to administer the necessary interventions and appropriate treatments. Interventions taken should be guided by how severe the underlying causes and symptoms are. You can choose to provide pacing, pharmacological treatment, or any other measure as indicated in the algorithm.
Pharmacological treatment:
After evaluating the symptoms, you can go on and administer the pharmacological treatment. Consider the following options as guided by the protocol:
Atropine: This is the first-line drug administered for symptomatic bradycardia. Administer 1 mg IV push, and you can repeat this every 3-5 minutes up to a total dosage of 3 mg. If the patient is not responding to atropine, consider giving transcutaneous pacing. The other option is epinephrine infusion (2-10 mcg/kg per minute. This should be titrated to the patient’s response). You can also administer dopamine infusions (5-29 mcg/kg per minute, titrated to the patient’s response).
Consider expert consultation:
After attending to the patient and if they fail to respond to treatment, seek expert consultation. If transcutaneous pacing is unavailable or ineffective, consider using transvenous pacing.
Conclusion
Bradycardia affects individuals of different age groups based on factors such as age, diet, and certain medical conditions. As per the ACLS bradycardia algorithm, you must evaluate a patient's symptoms to determine how severe the condition is. This will guide you on the appropriate treatment measures to take to help save a life and prevent further complications for a patient.
1 note
·
View note
Text
What is the ACLS Bradycardia Algorithm?
The ACLS (advanced cardiovascular life support) bradycardia algorithm is a protocol that healthcare providers use to manage patients with bradycardia. Bradycardia is a condition that slows down the heart rate to less than 50-60 beats per minute. Signs and symptoms of bradycardia include altered mental state, fatigue, hypotension, sweating, ischemic chest discomfort, acute heart failure, or signs of shock. In most cases, an individual with bradycardia does not get sufficient oxygenated blood to various parts of their body. Failure to treat bradycardia can lead to severe conditions such as syncope. However, it is worth noting that an individual may also experience a slow resting heart rate due to age or physical fitness activities. This blog will help you understand the ACLS bradycardia algorithm, its key steps and how to identify the underlying cause.
Causes of bradycardia
Identifying the main causes of bradycardia is important for effective treatment and management of the condition. Some of the factors that may cause bradycardia include:
Hypothyroidism
Inflammatory diseases
Imbalance of electrolytes
Myocarditis
Obstructive sleep apnea
Hypertension
Tissue damage due to heart attack, heart disease, or aging
Congenital heart defect
Essential steps in the ACLS bradycardia protocol
Understanding and effectively applying the ACLS bradycardia algorithm can be life-saving in critical situations. Every step is designed systemically to address and manage the symptoms of bradycardia and stabilize the patient’s condition promptly. Here are the steps of ACLS bradycardia:
Airway opening:
Ensure the patient’s airway is open. If not, you must assist the patient with breathing. You can do so while using the following steps:
Airway management: Begin by conducting an assessment of the patient’s airway. This will inform you if it is clear or not. Obstruction of the airway leads to inadequate oxygenation and may further exacerbate bradycardia. To assist the patient in maintaining the airway, you can apply techniques like jaw-thrust or head-tilt. If need be, you can also consider advanced airway management.
Assisting breathing: Once you establish that the patient is not breathing well, assist their breathing with ventilation using a bag-mask device or provide supplemental oxygen. Proper ventilation is crucial to improve the patient’s oxygen supply and lower the risk of further complications.
Administer oxygen if hypoxemic:
To measure the patient’s level of oxygen saturation in the body, use a pulse oximeter. Low oxygen levels, usually below 94%, mean that you must administer supplemental oxygen. You can deliver this either through a non-rebreather mask or a cannula. The method you will use depends on how severe the hypoxemia is. Moreover, it is not enough to administer oxygen. You need to conduct a continuous assessment of the patient’s oxygen saturation. This will guide you on how to adjust the flow rate of oxygen accordingly to ensure sufficient oxygenation.
Attach cardiac monitor for rhythm identification, monitor blood pressure and oximetry:
Use a cardiac monitor to evaluate the patient’s heart rhythm. This will guide you to know if the bradycardia is caused by a conduction problem or if it’s due to a particular type of arrhythmia. Secondly, you must measure the patient’s blood pressure to assess for hypotension. This is a critical indicator as it shows the patient’s hemodynamic stability. With bradycardia, a patient can experience lowered blood pressure and reduced cardiac output. Lastly, you must keep a record of the oxygen saturation levels. This information is necessary to ensure that the patient has adequate oxygen being delivered to body tissues.
Establish IV access:
To facilitate the administration of fluids, medicine, and other forms of treatment, you must obtain intravenous (IV) access. Consider using a large-bore catheter if it's available. This allows you to infuse medication or fluids more rapidly if necessary. Get ready to administer medications like atropine or other drugs as indicated in the bradycardia algorithm. If the patient is in shock or hypovolemic, provide them some fluids.
Obtain a 12-lead ECG:
To obtain a 12-lead electrocardiogram (ECG), place electrodes on the patient. This will provide a comprehensive view of the patient’s heart’s electrical activity, allowing you to diagnose the type of bradycardia. You will also be able to identify other underlying ischemic or structural changes in the patient’s heart. Additionally, conduct an analysis of the ECG to determine which type of bradycardia the patient has. It might either be an atrioventricular block or sinus bradycardia. This information will guide you on the treatment decisions to take.
Evaluate for symptoms:
Evaluate the patient’s symptoms to determine if bradycardia is causing major symptoms. Look out for symptoms such as signs of shock, altered mental status, ischemic chest discomfort, or acute heart failure. If any of these symptoms is present, proceed with the algorithm. Follow the protocol to administer the necessary interventions and appropriate treatments. Interventions taken should be guided by how severe the underlying causes and symptoms are. You can choose to provide pacing, pharmacological treatment, or any other measure as indicated in the algorithm.
Pharmacological treatment:
After evaluating the symptoms, you can go on and administer the pharmacological treatment. Consider the following options as guided by the protocol:
Atropine: This is the first-line drug administered for symptomatic bradycardia. Administer 1 mg IV push, and you can repeat this every 3-5 minutes up to a total dosage of 3 mg. If the patient is not responding to atropine, consider giving transcutaneous pacing. The other option is epinephrine infusion (2-10 mcg/kg per minute. This should be titrated to the patient’s response). You can also administer dopamine infusions (5-29 mcg/kg per minute, titrated to the patient’s response).
Consider expert consultation:
After attending to the patient and if they fail to respond to treatment, seek expert consultation. If transcutaneous pacing is unavailable or ineffective, consider using transvenous pacing.
Conclusion
Bradycardia affects individuals of different age groups based on factors such as age, diet, and certain medical conditions. As per the ACLS bradycardia algorithm, you must evaluate a patient's symptoms to determine how severe the condition is. This will guide you on the appropriate treatment measures to take to help save a life and prevent further complications for a patient.
0 notes
Text
IV Cannula vs IV Catheter: Understanding the Differences

In the medical field, intravenous (IV) access is a fundamental procedure used for administering fluids, medications, and blood products directly into the bloodstream. Two common devices used for this purpose are the IV cannula and the IV catheter. While these terms are often used interchangeably, they refer to different types of medical devices, each with its unique characteristics and applications. Understanding these differences is crucial for medical professionals to ensure appropriate use in patient care.
IV Cannula
An IV cannula, often simply referred to as a cannula, is a small, flexible tube that is inserted into a vein to provide access for intravenous therapy. Typically made of plastic, an IV cannula consists of a hollow needle with a thin, flexible tube that remains in the vein once the needle is withdrawn. The primary function of an IV cannula is to serve as a conduit for the infusion of fluids and medications.
IV cannulas are categorized by size, which is determined by the gauge of the needle. Sizes range from 14 gauge (large) to 24 gauge (small), with smaller gauges being used for patients with smaller veins or for less viscous fluids. The choice of size depends on the specific needs of the patient and the type of therapy being administered.
IV Catheter
On the other hand, an IV catheter is a broader term that encompasses various types of devices used for intravenous access. It refers to any tube or catheter inserted into a vein to administer fluids or medications. Unlike an IV cannula, which specifically denotes a device with a needle that is withdrawn, an IV catheter may include devices such as central lines, peripheral lines, and other specialized access tools.
IV catheters can be categorized based on their insertion site and purpose. For instance, peripheral IV catheters are inserted into veins in the arms or hands and are typically used for short-term therapy. Central venous catheters, inserted into larger veins like the jugular or subclavian veins, are used for long-term treatments or for administering medications that require central circulation.
Key Differences
1. Design and Insertion: An I.V. cannula is designed with a needle that is removed once the device is in place, leaving a thin, flexible tube for infusion. An IV catheter, in contrast, may include a broader range of devices, including those that remain in place with various anchoring systems.
2. Application: IV cannulas are generally used for short-term access and are commonly found in emergency or routine medical procedures. IV catheters, due to their variety, can be used for both short-term and long-term access, depending on the specific needs of the treatment.
3. Types and Sizes: While IV cannulas are categorized mainly by gauge size, IV catheters include a wider range of designs and insertion sites. This makes IV catheters more versatile for different medical needs, from simple infusions to complex central venous access.
4. Duration of Use: IV cannulas are usually used for short durations, such as during a hospital stay or for specific procedures. IV catheters, especially central lines, can be used for extended periods, such as for ongoing treatments in chronic conditions.
Denex International: Leading the Way in IV Access Solutions
When it comes to high-quality IV access devices, Denex International stands out as a premier IV Cannula Manufacturer and IV Catheter Manufacturer in India. With a commitment to excellence and innovation, Denex International produces a range of IV cannulas and IV catheters designed to meet the highest standards of safety and efficacy.
Their products are engineered to ensure ease of use, reliability, and patient comfort, adhering to stringent quality controls and regulatory standards. Whether you are seeking an Ivcannula for routine infusions or a specialized IV catheter for complex treatments, Denex International provides solutions that healthcare professionals can trust.
In summary, while both IV cannulas and IV catheters serve the essential function of intravenous access, they differ in design, application, and usage duration. Understanding these differences helps in selecting the appropriate device for each patient’s needs. For top-quality IV access devices, Denex International remains a leading choice, delivering products that support effective and safe medical care.
Contact Details
Name- Denex International
Phone- 0124 4115465
Email- [email protected]
#iv cannula#iv catheter#iv cannula vs iv catheter#iv cannula manufacturer#iv catheter manufacturer#iv catheter exporter
0 notes
Text
IV cannulas with wings and ports are indispensable in modern medical practice, offering enhanced stability, additional access points, and improved safety for both patients and healthcare professionals.
0 notes
Last Seen Blogs

boysdontcrytoday
What Is Crying?

diorkiller
***

the-silent-angel
The Lonely Assassin You Can Never Recall

zoshlihe09
Detrás de las palabras.

aniket-sah
Untitled