#psychiatry
Text
When are therapists gonna understand we can be self aware? Are they really gonna die on the hill that states it’s impossible for a narcissist to know and accept what they are? I lack empathy, not basic cognitive skills. Even intellectually disabled people can know they’re intellectually disabled.
This awareness they think we’re incapable of is the type of awareness living beings have intrinsically. It’s fucking basic awareness of information and the ability to compare. This red strawberry looks just like the other red strawberry, so 4-year-old-you matches them together on your little tablet game.
Yes, I can comprehend why I would be labeled as a narcissist. I’m mentally capable of understanding how I fit the description, and I’m mentally and emotionally capable of accepting new information I learn about myself.
What I don’t understand is how the psychiatric industry can be messed up enough for a LICENSED PSYCHIATRIST to believe someone can lack an intrinsic skill that LITERALLY COMES WITH BEING CONSCIOUS like what the actual hell?!?!??!!?
#flashy ✨ vent#flashy ✨ thoughts#cluster b#actually cluster b#npd#actually npd#actually narcissistic#narcissistic personality disorder#cluster b safe#npd safe#npd stigma#self awareness#ableism#psychiatry#psychiatric ableism#tw caps
43 notes
·
View notes
Text
Seeing people describe anti-endos as "aggressively pro-psych" is weird.
Their entire ideology is built on fabrications about what psychiatry actually believes and says.
Sure, they're religiously devoted to their pop-psychiatry that has little relation to the actual thing, but they'll instantly jump into denial mode the moment they're presented with opinions of actual psychiatrists that contradict their twisted, bigoted dogma.
They're "pro-psych" in name only.
They may want to identify as pro-psych. They want to play pretend and act like they're on the side of science while enforcing authoritarian viewpoints, much as the Right likes calling themselves "pro-life" while supporting the death penalty and trying to cut programs to feed the hungry and take away medical care.
But never confuse anti-endo dogma for actually being pro-psych.
#syscourse#pro endogenic#pro endo#sysblr#politics#multiplicity#political#systems#plural#plurality#psychiatry#psychology#mental health#actually a system#actually plural
23 notes
·
View notes
Text
Psychosis memory #55: communicating thinking I was making perfect sense only to later realize I was talking in gibberish. The difference came with medication
#psychosis#psychotic#psychotic break#schizophrenic spectrum#anti psychotics#mental illness#schizo spectrum#schizoaffective#psychiatry#schizophrenia
17 notes
·
View notes
Text
As a significant "feminised" category of mental illness, however, HPD [histrionic personality disorder] was superseded in the DSM-III by the introduction of the controversial BPD, a label which has been increasingly applied to women, with around 75 per cent of all cases estimated to be female. Seen as a milder form of schizophrenia and lying on the "borderline" between neuroses and psychoses, the concept has been used in psychiatry since 1938. Like other personality disorders, BPD has a notoriously low reliability level even by the generally poor standards of the DSM, and even within the profession is considered by many as yet another "wastebasket" category (though as Bourne ruefully remarks, the ambiguity of such personality disorders makes them particularly useful in policing deviance in the new century). One member of the DSM-III task force stated at the time of constructing BPD that "in my opinion, the borderline syndrome stands for everything that is wrong with psychiatry [and] the category should be eliminated". The chair of the task force, Robert Spitzer, admitted with the publication of DSM-III that BPD was only included in the manual due to pressures from psychoanalytically oriented clinicians who found it useful in their practices. Such practices have been documented by Luhrmann who describes psychiatrists' typical view of the BPD patient as "an angry, difficult woman—almost always a woman—given to intense, unstable relationships and a tendency to make suicide attempts as a call for help.' Bearing significant similarities to the feelings of nineteenth century psychiatrists towards hysterics, Luhrmann's study reveals psychiatrists' revulsion of those they label with a personality disorder: they are "patients you don't like, don't trust, don't want . . . One of the reasons you dislike them is an expungable sense that they are morally at fault because they choose to be different." Becker reinforces this general view of the BPD label when she states that "[t]here is no other diagnosis currently in use that has the intense pejorative connotations that have been attached to the borderline personality disorder diagnosis." A bitter irony for those labelled with BPD is that many are known to have experienced sexual abuse in childhood, something they share in common with many of those Freud labelled as hysterical a century earlier; a psychiatric pattern of depoliticising sexual abuse by ignoring the (usually) male perpetrator, and instead pathologising the survival mechanisms of the victim as abnormal.
By the mid-1980s, the hysteria diagnosis had disappeared from the clinical setting while BPD had become the most commonly diagnosed personality disorder. BPD is now the most important label which psychiatric hegemony invokes to serve capital and patriarchy through monitoring and controlling the modern woman, reinforcing expected gender roles within the more fluid, neoliberal environment. Nevertheless, as Jimenez (emphasis added) reminds us, the historical continuity from hysteria to BPD is clear: "Both diagnoses delimit appropriate behavior for women, and many of the criteria are stereotypically feminine. What distinguishes borderline personality disorder from hysteria is the inclusion of anger and other aggressive characteristics, such as shoplifting, reckless driving, and substance abuse. If the hysteric was a damaged woman, the borderline woman is a dangerous one."
Bruce M.Z. Cohen, Psychiatric Hegemony: A Marxist Theory of Mental Illness
3K notes
·
View notes
Text
Had to fill out a new form for my psychiatrist's office recently -- pretty standard stuff, including a drop-down for race/ethnicity and another for primary language.
But when I entered "english" in the Primary Language search bar as requested, it offered me some amazing, exciting options.
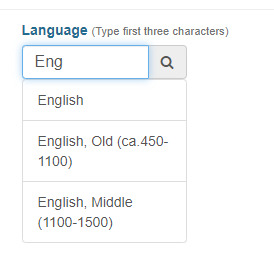
[ID: A screengrab of the form, where I have typed "eng" in the search bar; three options are visible below. The options are "English", "English, Old 450-1100" and "English, Middle 1100-1500".]
I know it's just because the form autoloaded a preset list of languages from somewhere that included Old and Middle English, but I'm still tickled by the idea that Clarity Clinic Chicago has people onboard who could prescribe Adderall for Caedmon or help Shakespeare sort out his gender issues.
3K notes
·
View notes
Text
solidarity between people who want to take psychiatric meds to function and those who don’t.
What’s important is that we both have autonomy, informed consent and safe access to treatments we want, and to not be forced, coerced or pressured into those we don’t.
1K notes
·
View notes
Text






moodboard
8K notes
·
View notes
Text
The young woman was catatonic, stuck at the nurses’ station — unmoving, unblinking and unknowing of where or who she was.
Her name was April Burrell.
Before she became a patient, April had been an outgoing, straight-A student majoring in accounting at the University of Maryland Eastern Shore. But after a traumatic event when she was 21, April suddenly developed psychosis and became lost in a constant state of visual and auditory hallucinations. The former high school valedictorian could no longer communicate, bathe or take care of herself.
April was diagnosed with a severe form of schizophrenia, an often devastating mental illness that affects approximately 1 percent of the global population and can drastically impair how patients behave and perceive reality.
“She was the first person I ever saw as a patient,” said Sander Markx, director of precision psychiatry at Columbia University, who was still a medical student in 2000 when he first encountered April. “She is, to this day, the sickest patient I’ve ever seen.”
It would be nearly two decades before their paths crossed again. But in 2018, another chance encounter led to several medical discoveries reminiscent of a scene from “Awakenings,” the famous book and movie inspired by the awakening of catatonic patients treated by the late neurologist and writer Oliver Sacks.
Markx and his colleagues discovered that although April’s illness was clinically indistinguishable from schizophrenia, she also had lupus, an underlying and treatable autoimmune condition that was attacking her brain.
After months of targeted treatments — and more than two decades trapped in her mind — April woke up.
The awakening of April — and the successful treatment of other peoplewith similar conditions — now stand to transform care for some of psychiatry’s sickest patients, many of whom are languishing in mental institutions.
Researchers working with the New York state mental health-care system have identified about 200 patients with autoimmune diseases, some institutionalized for years, who may be helped by the discovery.
And scientists around the world, including Germany and Britain, are conducting similar research, finding that underlying autoimmune and inflammatory processes may be more common in patients with a variety of psychiatric syndromes than previously believed.
Although the current research probably will help only a small subset of patients,the impact of the work is already beginning to reshape the practice of psychiatry and the way many cases of mental illness are diagnosed and treated.
“These are the forgotten souls,” said Markx. “We’re not just improving the lives of these people, but we’re bringing them back from a place that I didn’t think they could come back from.”
– A catatonic woman awakened after 20 years. Her story may change psychiatry.
#block JavaScript in site settings if article is paywalled#April burrel#disability#schizophrenia#lupus#mental illness#catatonia#chronic illness#institutionalization#psychiatry#medical science#healthcare#autoimmune disease#Washington post#knee of huss
3K notes
·
View notes
Text


legitimately what the fuck
11K notes
·
View notes
Text
You cannot know the history of schizophrenia as a diagnosis without coming to the conclusion that the fault of the misinformation surrounding schizophrenia and its setback in its research in modern society is a direct result of the laziness of past clinicians.
Negative symptoms used to be the focus of this illness when Kraepelin and Bleuler defined it - Kraepelin thought them to be more important and Bleuler literally defined them as FUNDAMENTAL symptoms.
Then in the 60s and 70s, since hallucinations and delusions were easy to spot and define, they were given more and more prominence in the hopes of "improving diagnostic precision." In real people language, that means they were lazy and wanted a quick checklist to go off of instead of, you know, caring about their patients.
What resulted from this is that now nearly everyone thinks schizophrenia is just hallucinations and delusions. On the medical side of things, the only treatments available for it treat psychotic symptoms, and the majority of the research focuses on them. Which leaves the rest of the debilitating symptoms untreated.
There are corrective adjustments being made to return to the emphasis on negative symptoms, and cognitive symptoms accompany that, but it should have never changed in the first place. Plus, the majority of society isn't adjusting their worldview to align with current perspectives on schizophrenia.
Schizophrenia was historically about the negative symptoms, and it always should have stayed that way. Schizophrenia is not just a "disorder that causes psychosis." It has negative, cognitive, disorganized, and catatonic symptoms as well.
Schizophrenia is a disorder affecting thought, behavior, and emotion, that is accompanied by psychotic features when left untreated.
Stop boiling down illnesses to basic symptoms. Teach and treat them wholistically.
#plat rambles#schizophrenia#actually schizophrenic#schizoaffective#actually schizoaffective#psychology#psychiatry#diagnosis#neurodivergent#actually neurodivergent
880 notes
·
View notes
Text
Yet problems in the legitimacy of psychiatry's vocation have remained, and reached crisis point at the cusp of deinstitutionalisation in the 1970s. At the time, a number of significant studies demonstrated the profession's inherent tendency to label people as "mentally ill," to stigmatise everyday aspects of a person’s behaviour as signs of pathology, and to make judgements on a person's mental health status based on subjective judgements rather than objective criteria.
The study that had the most direct impact on the psychiatric profession—as well as public consciousness—at this time was David Rosenhan's (1973) classic research On Being Sane in Insane Places which found that psychiatrists could not distinguish between "real" and "pseudo" patients presenting at psychiatric hospitals in the United States. All of Rosenhan's "pseudo" patients (college students/researchers involved in the experiment) were admitted and given a psychotic label, and all the subsequent behaviour of the researchers—including their note-taking—was labelled by staff as further symptoms of their disorder. This research was a culmination of earlier studies on labelling and mental illness which had begun in the 1960s with Irving Goffman (1961) and Thomas Scheff (1966). Goffman's ethnographic study of psychiatric incarceration demonstrated many of the features which Rosenhan's study would later succinctly outline, including the arbitrary nature of psychiatric assessment, the labelling of patient behaviour as further evidence of "mental illness," and the processes of institutional conformity by which the inmates learned to accept such labels if they wanted to have any chance of being released from the institution at a later date. Scheff's work on diagnostic decision making in psychiatry formulated a general labelling theory for the sociology of mental health. Again, his research found that psychiatrists made arbitrary and subjective decisions on those designated as "mentally ill," sometimes retaining people in institutions even when there was no evidence to support such a decision. Psychiatrists, he argued, relied on a common sense set of beliefs and practices rather than observable, scientific evidence. Scheff concluded that the labelling of a person with a "mental illness" was contingent on the violation of social norms by low-status rule-breakers who are judged by higher status agents of social control (in this case, the psychiatric profession). Thus, according to these studies, the nature of "mental illness" is not a fixed object of medical study but rather a form of "social deviance"—a moral marker of societal infraction by the powerful inflicted on the powerless. This situation is summated in Becker's general theory of social deviance which stated that "deviance is not a quality of the act the person commits, but rather a consequence of the application by others of rules and sanctions to an 'offender.' The deviant is one to whom that label has successfully been applied; deviant behavior is behavior that people so label".
Bruce M.Z. Cohen, Psychiatric Hegemony: A Marxist Theory of Mental Illness
617 notes
·
View notes
Text
So, Peer Respites are a not-very-well-known alternative to psychiatric hospitalization. They are 100% voluntary and staffed by peers, AKA individuals with lived experience of mental illness/emotional distress/what-have-you. Generally, they are a homelike environment where you can come and go as you please, and there is lots of voluntary programming like groups, art, yoga, etc. You can bring your own food or cook meals together with staff and other residents. Stays are usually anywhere from five days to two weeks, depending on the respite house and also your own wants and needs. There are no restraints, strip searches, or seclusion.
They're also on the rise!! I know this because I've spent all day today compiling data on peer respites in the US so I could create this fun graph for ya'll.

In the past ten years, at least 38 new peer respites have opened in the US. The data for 2023 is incomplete, but at least one has already opened, and another is scheduled for a soft opening later this year.
Some things about the data:
I did not include peer respites which were permanently closed (2) or could not find an opening date for (1)
I used the National Empowerment Center's Directory of Peer Respites, along with some internet sleuthing to find a few more (and to find the opening dates for each one). Because of this, I may have missed a few.
There were a handful of peer respites for which I could not pin down a for-certain, exact date for. I did include these in the dataset as I was able to find rough estimates.
I have also not done a deep dive for all peer respites that were unsuccessful, which may skew the data a little bit.
I included Soteria Vermont as well, as it technically fits the definition despite being specifically for people with psychosis
If you would like to help get a peer respite off the ground, I would recommend donating to Peer Support Space Inc.'s Orlando FL Peer Respite. Their soft launch is November 2023, and they are scheduled to open to the public in January 2024. This is really important, because Florida's only peer respite has recently permanently closed.
If you're interested in starting your own peer respite, the National Empowerment Center has a list of resources here.
If you are interested in seeking help from a peer respite, there is a directory of most of them here. You can also look at the Google Doc I created to compile my data, which has a few more/is slightly more updated - though it's not nearly as nicely put together as the other one!
If anyone would like to add any information, non-US peer respites, etc, feel free to!
#peer respites#peer respite#psych ward#psych hospital#psychiatric hospitalization#psych critical#psychiatry critical#anti psychiatry#antipsych#antipsychiatry#mental illness#neurodivergency#disability#hospital diversion#psychiatry#disability pride month#psychiatric survivors#putting in all the tags I can think of so ppl see this lol
2K notes
·
View notes
Text
"seek therapy" "get help" "this person is unwell" why is it that you are still of the belief that rendering a moral judgment is more tasteful when expressed obliquely via the language of health and the psychiatric normalising project. "it's not that deep" why is it that you are still of the belief that the rhetorical slippage between health and morality is funny and not coercive or violent. why has this particular style of witty retort maintained such a hold on people who consider themselves leftist and do you perceive yourself as making fun of genuinely ill people or are you simply enjoying larping the medicalisation and pathologisation of anyone you can argue deserves it. quickly now
6K notes
·
View notes
Text
The whole “your brain doesn’t finish developing until 25” spiel has fucking ruined society I swear. It’s such a gross misunderstanding of the original study it’s laughable, and yet people use it as scientific evidence that infantilising young adults (usually women or people perceived to be women lbr) is ethical actually.
YOUR BRAIN IS CONSTANTLY CHANGING AND DEVELOPING YOUR ENTIRE LIFE. YOU DON’T SUDDENLY WAKE UP ON YOUR 25TH BIRTHDAY WITH ALL THE MATURITY AND KNOWLEDGE YOU NEVER PREVIOUSLY POSSESSED. STOP SPREADING THIS NONSENSE
#Inspired by the Cass report and the fact it’s also spreading this bs and using it to deny trans healthcare#pseudoscience#neuroscience#infantilization#brain development#cass review#cass report#transphobia#trans rights#rant#vent#psychology#psychiatry
331 notes
·
View notes
Text
An Autism culture blog is spreading misinformation about endogenic systems...
The misinformation:

Naturally, all of this is wrong.
The only true statement here is "you could probably learn a lot more about these things in your own research." Because yeah... Doing your own research is likely to bring you to actually valid sources of information instead of whatever this is.
Real Information:
Endogenic systems are not a "fake form of dissociative disorder."
Endogenic systems ARE plural systems who experience multiple agents, or "headmates," sharing the same body in some way without trauma. Usually, endogenic systems don't even report having any sort of dissociative disorder at all.
And this is a real experience that's been repeatedly acknowledged by the psychiatric community.
So much so that the World Health Organization's diagnostic handbook, the ICD-11, specifically states that you can experience the presence of multiple "distinct identity states" without a mental disorder.
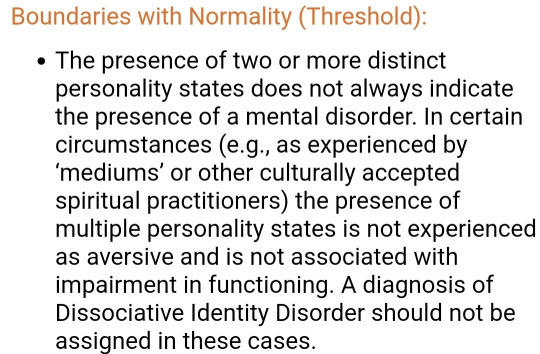
"Distinct identity states" is the same wording the ICD-11 uses to describe alters that characterized DID:

It's also acknowledged in the book Transgender Mental Health by Eric Yarbrough, which was reviewed and published by the American Psychiatric Association, that you can be plural without trauma or a disorder:
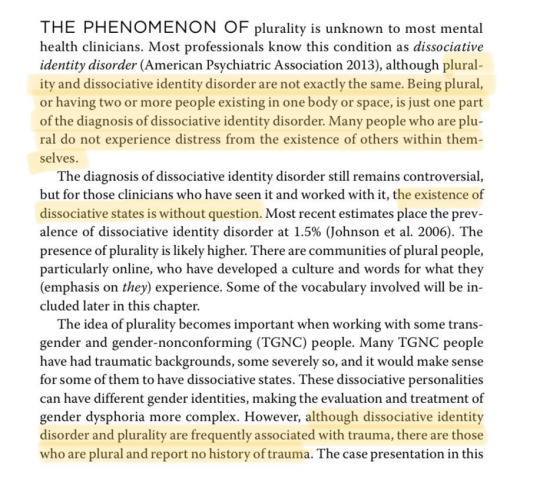
...

Additionally, the phrasing that endogenic plurality "mocks and invalidates people who are actually plural" is especially harmful as it erases and rewrites a huge part of plural history. That is, the fact that "plural" is an inclusive term coined and popularized to by non-disordered and endogenic systems.
Back in the 90s, the popular term that was used was "multiple," originating with "multiple personality disorder," the old name for DID.
The shift towards using "plural" was an effort by non-disordered systems to distance themselves from medical and pathologizing language. As you can see from this article from the 90s:
We don't claim that every multiple system/household is a happy loving cooperative one. What we do question is the *identification* of "real multiples" with the characteristics or symptoms of a psychological disorder. We go further: we question by what right or authority doctors and therapists are given sole jurisdiction over the definition of "an individual".
This is one reason our clan encourages use of the word "plural" rather than "multiple". "Multiple", even standing by itself, brings to mind MPD/DID, "multiple personality disorder", "dissociative identity disorder", which are specific diagnoses created by the medical/therapeutic community. "Plural" is a much more neutral word, more commonly heard in the context of grammar than psychiatry. (The other reason, of course, is that plural can be construed to have a broader meaning, applying to anyone(s) anywhere on the continuum who experience themselves as plural in some way. )
The Bottom Line:
An autism culture blog should be lifting up all neurodivergents. Not spreading misinformation about them and encouraging hate!
#syscourse#autism#neurodivergent#autistic spectrum disorder#asd#autism culture#actual autism#actually autism#autism spectrum#autistic#neurodivergencies#neurodiversity#actually neurodivergent#actually autistic#pro endogenic#pro endo#sysblr#multiplicity#psychiatry#actually a system
328 notes
·
View notes
Last Seen Blogs
qasd00001
Untitled


toplessandbarefooot
Show Me Your True Colors *

quidam-quidam-blog
Best 50 Tips For STAMPED CONCRETE PATIO

thatmadscientistbitch
Function of a Rubber Duck