#shes so round
Text


















Lilly with twins (part 2)
3K notes
·
View notes
Text
Please look at this cat

thank you for your time
#Shes so round#Like a cinnamon roll#Cat#round cat#sleepy cat#Cute cat#Sleepy cat#black cat#cute animals
87 notes
·
View notes
Note
I cant stop rotating I May Be Stupid in my brain I've been staring at that picture for so long bee holy shit I'm losing my mind

embrace that thang
#i was rotating her in my mind the entire time i drew this i Understand#shes so Round#beloved kip 💏#answered#bee talks
8 notes
·
View notes
Text
We got a dog!!!! Wheeeee!!!
3 notes
·
View notes
Note
Boy oh boy, you've caught the Spy x Family hype too, huh?
I can see the appeal, but I'm currently occupied with Elder Scrolls lore and character friendships right now. Cheerio to you. 🥂
*head in hands* i have a policy of not following the hype train but on account of me knowing spyxfamily existed for the last two years and actively choosing not to read it, i'm still following my principles >:(((
4 notes
·
View notes


Text
why aren't there more mysteries that take place in nursing homes & retirement communities. i want to watch a group of deranged retirees-cum-amateur-detectives combine their powers of:
decades of life experience
boredom-fueled busybody shamelessness
access to the most gossipy next-door-neighbors in existence
"I am too old to be arrested and/or give a shit" attitude
and solve crimes. this should be an enormous subgenre.
#their sidekick/Watson/pet hacker is a 15 year old grandkid who hangs out with gram gram on the weekends#her only power is that she has above average search engine skills and flexible knees#which is completely sufficient to round out the group's skill set#they involve her in heist style operations#on the rare occasion she gets caught housebreaking she explains her grandma locked herself out of the condo and asked for help getting in#then this sweet slightly addled old lady shows up and explains she got the address mixed up#it's so confusing when you're old & all the houses look alike and oh she's so sorry to have caused so much trouble#and meanwhile the teenager is rolling her eyes bc she's aware gram gram was a career criminal & con artist for 50 years#anyway gimme a 80-year-old con artist turned amateur sleuth who loves getting older because people are less suspicious of little old ladies#this all takes place in florida naturally
37K notes
·
View notes
Text
People call Heaven Official’s Blessing / TGCF a slow burn but Hua Cheng is literally courting Xie Lian like they are DATING. Slow burn who??? They’re sleeping next to each other on straw mats and Xie Lian’s offering to cook him dinner and they’re bantering across THE HOME THEY SHARE like a bunch of desperate hussys
San Lang LEAVES XL WITH A KEEPSAKE OF THEIR TIME TOGETHER SLOW BURN WHOMST
They have A DATE in HC’s armoury where they HOLD HANDS and XL pets San Lang’s quivering sword I-
Hua Cheng basically throws himself at this man he’s like you want a sword?? All of them ?? You want ALL THE SWORDS?? Fuck it take the whole room THE WHOLE ROOM JUST COME VISIT I WILL CLEAN THEM FOR YOU
Like he isn’t the king of a whole realm with shit to do
And this is just the first half of the first book—again I ask the world SLOW BURN WHOMST
#this is half in jest#but#I know some people don’t count it as “real until they kiss but THIS is honestly so gay of them#it’s in the subtext it’s in everything THAT ISNT a kiss#it’s so queer#Hua Cheng is ALL IN XL is just too innocent to Grasp It#XL is saying “come round to my tiny shack whenever sleep on my mat with me BEST FRIEND I will be your home” and HC is SUFFERING#the armoury scene is favourite of the entire thing#I was like my brother in Christ HAVE YOU NO SHAME#and knew immediately I would love him forever#tgcf#heaven official's blessing#mxtx tgcf#hua cheng#xie lian#hualian#she’s being unhinged again
4K notes
·
View notes
Text

Traffic Gals- Introducing Gem!
#secret life#secret life smp#zombiecleo#geminitay#pearlescentmoon#ldshadowlady#trafficblr#traffic smp spoilers#traffic spoilers#life series spoilers#SEASON 5 AND IT MEANS IM BACK ON MY BULLSHIT LETS GOOOOOOOOOO#My Gem design is basically just a dorito. She is a rounded triangle to me in the same way that Pearl is a stick#I watched some episodes half way through drawing this and im going feral RHHRHRHHR#idk what the offical spoiler tag is so im just- using as many as i found ig#my art
8K notes
·
View notes
Text
anyone out there who enjoys both Bive and The Smiler i’m boutta summon all of you cuz I MADE A SMILER INSPIRED BIVE AVATAR MUAHAHAHAHAA



#she’s so me bro it’s insane#hey guys this is my gender#regretevator#regretevator bive#bive#bive regretevator#smiler#the smiler#alton towers#roblox#is this an oc??? nah…….#okay no oc tag#i saw someone’s art of a smiler inspired bive the other day and had an aneurism /pos#roblox avatar#my user is berserrkerrr follow me on roblox i wanna get to 1k grrrrr#i used to have 1k but over 100 accounts got banned so i’m stuck at like 930 sumn sobs#ignore the double glasses on her i wanted to use the smaller ones to add the bridge area cuz the big glasses didn’t have it#pretend it’s only that one pair of glasses#the round ones#yea
1K notes
·
View notes
Text





she didn’t have to put the mirror there, but she did, for us, and i just think that’s neat
742 notes
·
View notes
Text
What is the difference between a tubal pregnancy and an ectopic pregnancy?
In ectopic pregnancy, implantation occurs in a site other than the endometrial lining of the uterine cavity, i.e., in the fallopian tube, horn of the uterus, cervix, ovary, or abdominal or pelvic cavity. Ectopic pregnancies cannot be carried to term and eventually rupture or involute.
Early symptomatology includes pelvic pain, metrorrhagia, and tenderness to the vaginal touch, especially when the cervix is displaced.
Syncope or hemorrhagic shock may occur upon rupture. Diagnosis is based on beta-hCG measurement and pelvic ultrasound. Treatment consists of laparoscopic or open surgical resection or IM methotrexate injection.
The incidence of ectopic pregnancy is approximately 2/100 diagnosed pregnancies.
Etiology of ectopic pregnancy
Factors that particularly increase the risk of ectopic pregnancy include
Tubal lesions
A history of ectopic pregnancy (risk of recurrence 10-25%)
History of pelvic inflammatory disease (especially Chlamydia trachomatis)
Previous abdominal surgery especially on the fallopian tubes, including tubal ligation
Other specific risk factors for ectopic pregnancy include
Intrauterine device (IUD) contraception
Infertility due to tubal damage
Smoking
History of induced abortion
Pregnancy is less likely to occur when an intrauterine device (IUD) is in place; however, about 5% of these pregnancies are ectopic.
Pathophysiology of ectopic pregnancy
The most common location of ectopic pregnancies is the fallopian tube, followed by the uterine horn. Cervical pregnancies, in a caesarean scar, the ovary, the abdomen or the interstitium of the fallopian tube are rare.
( You can follow your Pregnancy & Baby Tracker Pro week by week )
Heterotopic pregnancies (both ectopic and intrauterine) occur in only 1/10,000 to 30,000 pregnancies, but may be more common among women who have used ovulation induction or assisted reproductive technologies such as in vitro fertilization and gamete intrafallopian tube transfer (GIFT); in such cases, the reported rate of ectopic pregnancies is ≤ 1%.
The structure containing the fetus usually ruptures after 6 to 16 weeks. Rupture results in hemorrhage that may be progressive or rapid enough to cause hemorrhagic shock. Intraperitoneal blood irritates the peritoneum. The later the rupture, the more rapid the bleeding and the higher the mortality.
Symptomatology of ectopic pregnancy
Symptoms of ectopic pregnancy vary and are often absent until rupture occurs. Most patients present with pelvic pain (sometimes in the form of cramping) and/or vaginal bleeding. There may or may not be a delay or absence of menstrual bleeding, and the patient may not know that she is pregnant.
Rupture may be heralded by sudden severe pain, followed by syncope or symptoms of hemorrhagic shock or peritonitis. Rapid hemorrhage is more likely in ruptured ectopic pregnancies.
Pain on mobilization of the cervix, unilateral or bilateral adnexal tenderness on vaginal touch, or an adnexal mass may be present. The uterus may be slightly enlarged (but less than expected from delayed menstruation).
Diagnosis of ectopic pregnancy
Quantitative serum human chorionic gonadotropin beta subunit (beta-hCG)
Pelvic ultrasound
Sometimes laparoscopy
An ectopic pregnancy is suspected in any woman of childbearing age with pelvic pain, metrorrhagia, or unexplained syncope or hemorrhagic shock, regardless of contraceptive use, sexual intercourse, or delayed menses. The results of physical examinations (including pelvic touch) are neither sensitive nor specific.
A ruptured ectopic pregnancy is a surgical emergency because it causes maternal hemorrhage with a risk of death; prompt diagnosis is essential.
The first step is a urine pregnancy test, which is nearly 99% sensitive in diagnosing pregnancies (ectopic and others). When the urine beta-hCG test is negative and the clinical signs are not strongly suggestive of ectopic pregnancy, further testing is unnecessary unless the symptoms recur or worsen.
If the urine beta-hCG is positive or the clinical signs are strongly suggestive of ectopic pregnancy, a quantitative serum beta-hCG measurement and pelvic ultrasound are not indicated.
When the quantitative serum beta-hCG is < 5 mIU/mL, ectopic pregnancy is excluded. When ultrasound detects an intrauterine gestational sac, an ectopic pregnancy is highly unlikely except in the woman who has used assisted reproductive techniques (which increases the risk of heterotopic pregnancy); however, a cornual or intra-abdominal pregnancy may initially present as an intrauterine pregnancy.
Ultrasound images suggestive of an ectopic pregnancy (seen in 16 to 32%) of cases include complex masses (mixed solid and cystic masses), particularly in the adnexa, and fluid effusion from the cul-de-sac of Douglas.
If the serum beta-hCG is above a certain level (called the discriminatory zone), the ultrasound should detect a gestational sac in case of intrauterine pregnancy. This level is usually about 2000 mIU/mL. If the beta-hCG level is above the discriminatory zone and no intrauterine gestational sac is detected, an ectopic pregnancy is likely. The use of the transvaginal route or color Doppler can improve detection rates.
If the beta-hCG level is below the discriminatory zone and the ultrasound is negative, it may be an early intrauterine pregnancy or an ectopic pregnancy. If the initial clinical workup suggests an ectopic pregnancy (e.g., significant peritoneal irritation or hemorrhage), diagnostic laparoscopy may be necessary for confirmation.
When an ectopic pregnancy appears unlikely and the patient is stable, plasma beta-hCG levels can be monitored on an outpatient basis (typically every 2 days). Normally, the level doubles every 1.4 to 2.1 days until day 41; in an ectopic pregnancy (as in non-progressive pregnancies), levels may be lower than expected and do not double as rapidly.
If the beta-hCG level does not rise as expected or falls, the diagnosis of spontaneous miscarriage or ectopic pregnancy should be considered.
#pregnant kink#pregnancy#make me huge#huge pregnant belly#belly movement#squirming#preggolife#pregnant#pregnant women#pregnantbeauty#pregnantbelly#big belies#mother#sexy belly#long post#multiples#vintage preg#progress#shes so round#twins
0 notes
Photo



Once again, in another river, on another island, the power of the beast lord awakens to save someone else.
#orv#omniscent reader's viewpoint#orv spoilers#shin yoosung#kim dokja#kdj#so we can agree best daughter?#across all the rounds?#if you think otherwise you are just wrong#anyway i love how kdj and sys come full circle during jttw arc#except this time she saves him!#(i took some creative liberties with this scene)
3K notes
·
View notes
Text
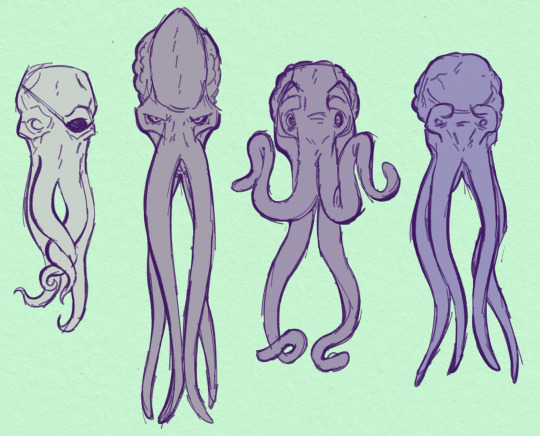
SQUIDZ
(left to right gideos from the infernal tides comics, emperor, my tav pennybun, and omeluum)
#art#bg3#pennybun#omeluum#the emperor#gideos#illithid#mind flayer#look at emp's fucking torpedo head. why are you so long#omeluum and gideos are round...#penny's head is bigger thanit looks here she's more horizontal since she was a dragonborn before
494 notes
·
View notes
Text



So what's wrong with Clara, then? There's nothing wrong with her. Why haven't you made her immortal? Well, look how you turned out.
#dwedit#doctor who#userveronika#usertennant#userteri#scifiedit#ashildr#twelfth doctor#clara oswald#twelveclara#*#honestly idk if this will make sense to anyone but me but#the doctor saved ashildr and the doctor saved clara but ashildr is clara and ashildr is the doctor too.......... and so is clara#or more intelligibly: ashildr's arc at its base is the same arc that twelve and clara have together. except she plays both roles#ashildr starts as clara and ends as the doctor. like you can SEE the moment it switches from ashildr-as-clara to ashildr-as-doctor#but clara ALSO starts as clara and ends as the doctor. (''we could you know... stop off on the way'' ''gallifrey. the long way round'').#and the doctor gets to watch the exact same storyline play out in front of him without ever realizing it and incapable of ever stopping it#.....does any of that make sense. i'm writing these tags at 3am so idk fjdkslsls#but really this gifset is just 'ashildr: the twelveclara redux'
750 notes
·
View notes
Text





did some screenshot edits for fun :]
ogs r under the cut ^^





#i always love it when they put extra care into the lineart with those close up shots so i wanted to try to emulate that#precure#star twinkle precure#hikaru hoshina#elena amamiya#lala hagoromo#madoka kaguya#yuni#i kinda wish i had better screenshot but </3 these were to test the waters#but madoka ahh she was so much fun <3#lala was easily the hardest tho lol. id draw her more but i hate coloring green </3 especially that blue green color#also giving lala rounded eyebrows is my favorite thing now i think it looks so much better on her lol#eyestrain#PC
741 notes
·
View notes
Last Seen Blogs

worldsentwined
Worlds Entwined

ghada3b
Gh

ragnarsghost
Ragnar Redbeard's Ghost

dadascrazylife69
Untitled

perfectpanties
Perfection