#whump reference
Text
Announcing MEDLEY: A Medical Primer for Writers (Summer Edition)

Are you a writer?
Do you need to know things about medicine for your fiction works?
Have you considered taking a 100% online class about it?
Starting Tuesday, June 4th and running for 9 weeks is MEDLEY.
Topics include:
WEEK 1: (US) Hospitals and the People Who Work in Them
WEEK 2: The Physical Exam
WEEK 3: Codes and ACLS
WEEK 4: Remote and Improvised Medicine 1
WEEK 5: Remote and Improvised Medicine 2
WEEK 6: Recovery and Aftermath
WEEK 7: Historical Medicine
WEEK 8: Mental Healthcare
WEEK 9: Bonus Episode
This is the second time I'm running this course so hopefully the kinks are nice and ironed out this time.
Price is $36 per person ($4/week).
Two scholarships are available no questions asked.
Contact me at [email protected] for more information/to sign up.
75 notes
·
View notes
Text
Some headcanons regarding TMNT physiology
Over the years, I have come up with some headcanons regarding how I believe the Ninja Turtles' bodies work. I thought that perhaps it might be nice to finally share them with all of you.
These don't apply to all the iterations, of course, but they are pretty well universal in my mind, and I tend to incorporate most of them into my fanfics.
The Turtles (like leatherback sea turtles, echidnas, and some dinosaurs) are mesotherms, meaning they are neither warm nor cold blooded. They are, instead, in a middle-ground: they internally generate heat, but not to a constant temperature. In the Turtles' case, they will shiver when cold, and their bodies will not shut down right away when the temperature dips too low, though they may lose some energy and find it hard to concentrate.
Unlike many other modern reptiles and amphibians, who have a three-chambered heart, the Turtles have four-chambered hearts (like mammals and dinosaurs) that are larger and stronger than average human hearts and located at the center of their chests.
While the average human blood capacity is around five liters, the Turtles have about seven. Much of the blood flows under the shell -- a remnant of their lives as ordinary turtles, whose own blood does so in order to warm them when they bask. This means that the Turtles could lose close to three liters of blood before dying, while a human would only be able to lose two.
Their blood is also highly efficient at clotting, but that also means that storing blood for transfusions is difficult, and so must be directly transfused from one turtle to another in emergency situations.
Owing to their extensive circulatory system, they also have a larger lung capacity than humans and more oxygen-rich blood, and so are able to hold their breath for extended periods of time without adverse effects. Other than this, the Turtles' respiratory system is very much like humans', utilizing a diaphragm to inflate and deflate their lungs.
Like regular turtles, they do not have ribs, but rather their carapaces and plastrons serve that purpose, and they have muscles under their shells that keep their internal organs right where they belong.
Also like regular turtles, their spines curve along the insides of their shells. A direct hit on the center of their shells, then, could cause damage to their spinal column and nervous system, but fortunately their vertebral shields offer a fair amount of protection, so it would take quite an impact.
The Turtles are highly resistant to most infections and diseases, which increases their immunological responses. They do not get sick easily, and they recover quickly.
While their scales are not apparent, they are integrated into their skin, making it tougher than human skin. It takes a very hard hit to raise a bruise, and it is difficult to cut through without a very sharp or pointed blade.
Their bones are similar to humans, but are more resistant to breaking. They also heal quicker and stronger if they are broken.
Their muscles are also very close to human-like, but they are stronger than an average human due to compensating for the extra weight they carry in their shells. Because of this, their ligaments and tendons are also tougher, and it is difficult for them to have a joint dislocated.
Their sense of smell is more acute than humans, but not to an extreme degree. They are also not as bothered by foul smells (though this has more to do with living in a sewer than their physiology).
Their eyes are a bit tougher and more resistant to damage than human eyes due to a protective membrane that covers them. They see a bit better than humans in dark places and underwater.
Their hearing is somewhat more attuned to lower frequencies than human hearing, and is not dependent on external ears but rater an internal auditory system (making direct damage to their hearing unlikely).
They are capable of being knocked unconscious, but it takes a significant impact. Permanent or lingering damage to their brains is unlikely due to their structure, and so they also do not tend to suffer the same side-effects that humans would in the same circumstances (nausea, memory loss, etc.).
Although their nutritional needs are similar to humans, they do not need to eat every day, and in fact can get by quite well without food for a week if necessary (though they won't enjoy it). When food is readily available, however, they will eat as much as possible to store up energy. Their metabolism does not slow down when they do not eat, so overexerting themselves when they haven't had any food for a while can burn them out suddenly.
Their sleep schedules are much like most diurnal animals, though they are able to stay awake for extended periods of time and can get by on little sleep, if necessary. There have been times when they have been awake for days on end, getting by on short one hour naps here and there. In general, though, they like to have a regular sleep/wake cycle.
Like other reptiles, the Turtles never stop growing throughout their lifetimes; however their growth is slow, topping off at about 1-2 inches every five years.
Does anyone have anything they would like to add to the list? I actually had fun compiling it!
#tmnt#teenage mutant ninja turtles#ninja turtles#fanfic#fanfic reference#rise of the teenage mutant ninja turtles trailer#rottmnt#tmnt 2003#tmnt 2012#tmnt 2007#tmnt bayverse#tmnt vs batman#tmnt comics#tmnt mutant mayhem#tmnt mm#whump#whump reference#tmnt 1987#tottmnt#tales of the tmnt
981 notes
·
View notes
Text
Random whumpy fainting stuff
From a person who passes out almost daily from dehydration and POTS
Fainting can be dramatic (eyes rolling back, falling to the floor, etc), but it can also be subtle sometimes. Even standing up, your whumpee could just sway in place a bit, eyes going unfocused and dilated. Maybe those around them grow concerned as they realize whumpee is unresponsive, before moving to touch them, shake their shoulder, and watching with horror as whumpee tips over and slumps to the floor.
When your whumpee is coming to, there’s often a few seconds where they are aware of and can understand everything around them, but are unable to move or talk. Just laying there, maybe mumbling something quietly or waving a hand at most, body still coming back online.
Whumpee catching themself passing out, deliberately breathing slow and deep in an attempt to not faint, even as they slowly feel their thoughts leaving them. The darkness fuzzing in on the corners of their vision and masking their surroundings, and the last, frustrated thought of “well, shit” as they sink to the ground, breathing exercises having failed them.
Alternatively, there can also be a few seconds after (before??) coming to when your whumpee isn’t cognizant of what is happening, but it appears like they are. They may sit up, even respond to a basic question, and then blink awake, completely disoriented at already being upright and moving.
Everyone around them freaking out, disorienting whumpee even further as they wake up to the concerned voices and roaming hands and prodding and questions. Whumpee attempting to brush everyone off, appease everyone, to just get away as they maybe stagger to their feet or curl into a ball.
#my ramblings#my prompts#Whump#whump prompt#whump prompts#whump scenario#whump scenarios#collapse whump#fainting whump#whump inspo#whump community#whump reference#ALSO NOBODY SHOULD PASS OUT FOR MORE THAN LIKE 20 SECONDS#If your whumpee doesn’t pop up like a daisy out of the snow you’ve killed it
834 notes
·
View notes
Note
Can you tell me about bruises? I've been trying to research but I think I'm pretty terrible at it. One thing I can't seem to find an answer to is how quickly they form? Like, if I have my blorbo take a hit, how long until the area is black and blue? Does it depend on some factors? What are those factors? TIA!
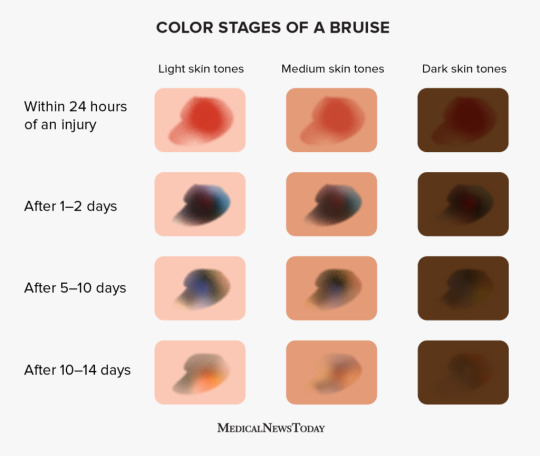
This is the best reference I have found for what bruise stages look like. Generally the "within 24 hours" section starts within 1-2 hours.
132 notes
·
View notes
Text

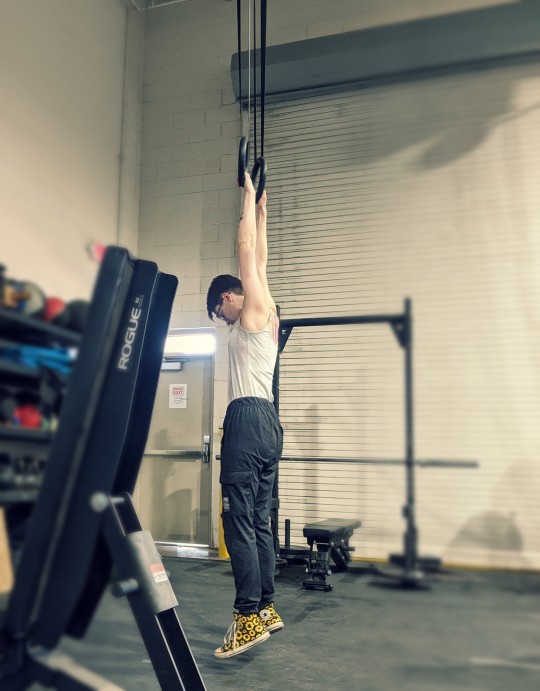
no setting the scene this time, just some refs for the next time you wanna dangle a whumpee (feat. me being a drama queen at the crossfit gym)
more under the cut!



more whump art refs:
pet crate | basement | white shirt | gut spill
#id have loved to set the stage better but there's only so much you can do in a piblic space lol#im lucky no one popped in ahahaha#anyone can use these! i just like providing helpful poses ahaha#whump reference#whump art ref#whump photography#whumblr#calico face reveal ish#the plus side is the building goves you a decent warehouse vibe
81 notes
·
View notes
Text
whump generators i have found
these were saved in my bookmarks so idk which account they were made by, feel free to add on to this post if they are yours or you know of any more
fantasy generator
random generator
random generator 2
torture generator
for when your brain is smashed banana 🍌
#whump#whump community#whump generator#whump generators#whump prompts#whump prompt#whump reference#whump ref
322 notes
·
View notes
Text
a comprehensive overview of burns and burn treatment: whump writer reference edition
extremely long post ahead! here's the lowdown:
Degrees of a burn (first through sixth)
First aid
Medical treatment
Complications and infection
A Whump Writer's Reference/Recap
End notes
(also huge shout out to @i-eat-worlds for helping me out! this is all inspired by a one-shot, and they hopped in to give me some ideas and things to research. thank you worlds!)
(disclaimer: I am not a doctor, nor have I been to medical school. this is done through research and from the eyes of a writer. if I have incorrectly listed something, correct me via an ask and I will change it. thanks for understanding!)
1. Burn degrees
There are six degrees of burns. The first three, lower level degrees, are the most common. Here's a quick overlook on all of your options:
First degree: A superficial burn affecting only the outer layer of skin. Symptoms include redness, itchiness, dryness, and a low-to-medium level of pain. Scarring is possible, but minimal.
Partial second degree: Extends past the outer layer of skin and partially into the second layer. Symptoms include darker red tones, blistering, swelling, white splotches, and higher levels of pain. Complications include infections.
Deep second degree: Extends deeper into the second layer of skin. Symptoms include severe pain, dark red, blistering and swelling. Scarring is much more common here.
Third degree: Burns surpassing the skin layers and entering the layer of fat below it. Symptoms include black, brown, yellow or white leathery skin, either intense pain or numbness if nerve endings were burned, loss of feeling and movement.
Fourth degree: Extending into muscle. Symptoms include complete lack of pain, burn site is charred and blackened or white and lifeless, possible exposure of bone. Complications include infection, loss of feeling, and can require amputation.
Fifth and sixth degrees: Past muscle and into or through bone. Symptoms include exposed or charred bone, similar to fourth degree in coloration. Complications result in permanent body damage, total loss of skin and nerve endings, and fatalities from just the burn.
2. First aid
Upon immediately receiving a mild burn covering a small portion of your body, such as your forearm or hand, run it under lukewarm or cool water* for twenty minutes. This will encourage the skin to cool and release trapped heat, reducing damage later.
Ice cold or freezing water will cause blood vessels to constrict. This lowers the blood supply to the burn, further damaging the tissues, and increasing swelling, pain, and chances of scarring.
*If there is no running water, immersing or using a wet towel are your next best options. Keep in mind that cloth contact on a burn is painful and despite the cooling effect will still be uncomfortable.
Upon receiving a severe burn (third degree and beyond), you'll want to cover the wound with a clean cloth and get to emergency help immediately.
If the skin is broken, do not use water. Any possible pathogens or bacteria can get inside the body and cause sepsis, which we'll go over in the next section.
Upon a victim receiving burns on over 20% of their body, you'll want to remove any jewelry, belts or tight items to release heat and promote breathing. Cover the burn in a clean dry cotton cloth if possible. Check for symptoms of shock, and administer CPR if necessary. Call services to bring care to you, or aid the victim in getting to emergency care immediately.
Although you want to remove metal and jewelry, you do not want to attempt the removal of cloth stuck to the skin. Doing so can cause open wounds and increase the chances of infection, detailed in the next section.
3. Medical treatments
Upon entering medical assistance, the victim will first be stabilized with oxygen/machine breathing and fluids. After the patient is stabilized, focus returns to the burn.
There are three main goals to medical treatment of a burn: reducing/minimizing oedema, or fluid buildup in tissue, reducing tissue damage, and preventing infection. Treatments include:
1. Fluid replacement: Replacing fluids to the body through an intravenous (IV) or intraosseus (IO) infusion. Fluid loss can be caused by dehydration, vomiting, diarrhea, bleeding, or fluid shifts*.
2. Hyperbaric treatment: exposing the body to 100% oxygen content. This can increase circulation, reduce oedema, and assist in the preservation of damaged tissue.
3. Uses of antibiotics or topical ointments: Aloe vera is a topical lotion used to cool minor burns like sunburns. Mafenide is the most commonly used antibiotic to protect against infection in severe burns, and bacitracine for minor burns.
To clean a burn wound, rinse it in water and wash it gently. Pat it dry, and cover it in an antibiotic ointment. Then, cover it with a clean, dry gauze, and wrap it with a bandage. Avoid sticking bandages that will pull against damaged skin, and avoid rubbing alcohol, iodine and hydrogen peroxide, which will slow the healing of the wound. Do not pop blisters, as it increases the chances of infection. Change the bandages daily.
4. Complications and infection
And my favorite part: everything that goes wrong even after the initial burn.
1. Shock: A condition occurring after injury when the body isn't getting enough blood flow. This is an extremely lethal complication.
There are four kinds of shock, but the most common is hypovolemic. Symptoms can include pale, clammy skin, rapid and shallow breaths, rapid pulse, anxiety, confusion, disorientation, weakness, nausea and vomiting.
To treat shock: if the victim's legs are unaffected, raise them above their heart, immobilize any fractures and administer first aid, loosen any tight clothing, and maintain the victim's body temperature. The warmer they are, the faster the blood flow.
2. Capillary leak syndrome: A condition common in burns, when anti-inflammatory chemicals are released, causing the capillary walls to shrink and allow fluids like plasma and water to leak out.
The body's blood pressure rapidly drops. White blood cells can escape, which assists in initial burn treatment, but now that it's outside the capillaries, any fluids lost can no longer circulate, leading to dehydration. This is the main cause of oedema, as stated above. Symptoms of CLS include malaise, lightheadedness, headache, and feeling faint or dizzy.
To treat CLS: Fluid replacement to ensure dehydration does not become too severe, and hyperbaric oxygen treatment can assist in increasing blood flow. Capillary permeability will lessen close to a day after the initial burn is recieved.
3. Hypothermia: A significant drop in body temperature, most commonly associated with prolonged exposure to the cold.
Yes, you read that right--you can get hypothermia from a burn. Victims of burns covering a large amount of body surface area (BSA) will have trouble retaining warmth, due to the heat of the burn attempting to escape. Symptoms include shivering, exhaustion, confusion, numbness in extremities, difficulty speaking or thinking and slow pulse.
To treat hypothermia: Treat the patient in a warm area, ensure any fluids in their IV or IO are warm, let them drink something warm, give them blankets, etc. etc.
4. Infection: when a wound is infected, bacteria or pathogens have entered and compromised the healing process. If left untreated, the infection can spread to the bloodstream and cause sepsis, an extremely dangerous condition resulting in organ failure or even death.
Infections are incredibly serious complications, especially when the burn covers more than 20% of the victim's BSA. Symptoms include fever, discoloration of the wound, pus or other leakage, increased heat around the wound, and possible foul smells emanating from it.
To treat infection: Additional antibiotics should be taken, possible added painkillers, daily cleaning may be increased to more than once a day. Occasionally products made from ionic silver may be used, which provide quicker clearing of infection.
5. Sepsis: Inflammation throughout the entire body, caused by infections leaking into the bloodstream. Critical and incredibly fatal if not treated properly.
Symptoms of sepsis may include but are not limited to: chills, dizziness, low blood pressure, fever, shivering, low temperature, confusion and altered consciousness, rapid and short breathing, delirium, rapid heart rate, organ dysfunction, skin discoloration and exhaustion.
To treat sepsis: Continue fluid replacements, possible mechanical ventilation, added use of antibiotics and steroids, added use of a catheter. Essentially, full hospitalization with constant medical attention until the body fights off remaining infections.
5. A Whump Writer's Reference/Recap
A short ending section of things to think about when writing a scene with a burn victim whumpee.
Before delving into the scene, decide which degree of burn your whumpee receives. First aid, treatment and symptoms will all depend on that.
When writing from the whumpee's point of view, use comparisons. Not everyone knows what it feels like to fall torso first into the bonfire at the house party, but everyone can imagine the flood of panic when you touch a hot stove--so use that metaphor and elevate it. The more description of the pain, the more involved you'll feel.
When writing from an outsider's point of view, don't be afraid to be gruesome. Be visceral. There are levels of discovery to a burn--initial receiving, panic and chaos, and seeing the entire wound--so really get those details in, make the reader see that burn in their mind's eye.
The pattern goes burn administered, first aid, medical treatment, and recovery/complications, so if you're like me and have trouble laying out scenes, use that as a backbone.
Touching a severe burn and removing your hand can take the skin with it! It's gross, but great for shock factor!
All those times I said "do not do this, do not do that"? Ignore 'em when you're writing. You can make the worst of the situation. Not everyone knows first aid, so if you want the pain, let your caretakers screw up, and badly. The consequences are listed too, so play around!
Some words to use when describing the pain of a burn:
Burn, fire, flame, inferno, blinding, flash, disintegrate, digging, agony, pull, tear, rip, burrow, cave, searing, roaring, boiling, sizzling, melting, ache, pins and needles, blurring, catch, white hot, coil, threading, frenzy, howling, writhing, thrashing, pulsing, torture, numbing, chafing, loss of feeling
And some words to describe someone who's been badly burned:
Pale, pallid, heaving, shaky, shivering, dizzy, swaying, hissing, panic, sweating, fluttering, weak, nauseous, thready pulse, limp, hoarse, shuddering, slumped, in and out of consciousness, exhausted, mumbling, murmuring, incoherent
6. End notes
things to look up for further study: burn pathophysiology, capillary permeability, and first aid treatment of burns. this is all just for first glance and ideas, if you get stuck in a scene like I did, so do further research if you want to!
thanks for reading, folks! i hope you enjoyed this very very long post. do you want to see more of these, or do you prefer the shorter prompts? if I make another reference list like this, what would you like to see?
have a cookie for making it to the end 🍪 and go drink some water. i hope you have a wonderful day!
(sources: Mayo Clinic, Cleveland Clinic, National Institutes of Health, and many others. this isn't an official research paper, it's a tumblr post, and I don't claim to have written the articles myself. these words are compiled for wide range of reference for writers specifically, and not for deliberate study. thank you for reading!)
#whump#whumpblr#whump prompt#whump reference#reference post#whump community#burn whump#burns#burning#medical post#medical whump#hurt/comfort
135 notes
·
View notes
Text
Volume warning!!
In this short, this voice actress demonstrates different types of screams, and I thought.... That's something the Whump Community has to see. Or hear, rather.
#I wish i could insert the video without making viewers link through youtube but i didn't want to remove credit or views#lady whump#female whump#female whumpee#whump#whumpblr#whump reference#screaming#irl whump#(i mean she's clearly acting but i get that it might warrent that tag)#inspo#torture#drowing#whump prompt
30 notes
·
View notes
Text
Electrocution Reference
Don't ask why, but I stuck my tongue on a charger (I thought it wasn't plugged in but it was). I didn't realize what it's like to be electrocuted (aside from a little shock)
My vision went blue and white, my ears rang, and my tongue went numb. I felt like I was underwater and that my life was flashing before my eyes. All of this happened in the span of a millisecond.
Once I snapped out of it, it's like I was pulled out of water. There was a bang as my ears popped, followed by my vision returning and the feeling coming back in my tongue.
I realized my heart was beating fast and I had a headache that wasn't present before. My hair was all over the place and I couldn't think for a second.
I am better now! :D
--
Do what this info what you will.
Don't try this at home XD
#whump#whump scenario#whump prompt#whump community#whump writing#electrocution#electric whump#electric shock#writing reference#whump reference#writing tools#writing inspiration#my prompts
34 notes
·
View notes
Note
worlds I need your medical knowledge. possible long-term symptoms of repeated non-lethal electrical shock to the body? would nerve damage and numbness be reasonable? what are your thoughts?
- @whump-kia
thanks for the ask, Kia!
quick disclaimer: I am not medical professional. Take all this with a grain of salt. Or like, 110% of your daily sodium intake.
So, electrical injury severity and pattern is influenced by a couple of different factors. The voltage of the current, weather it’s AC or DC, the surface area the current made contact with, and pathway the current took through the body all play a role in how your character would be injured.
One of the most dangerous things that electrical shocks cause are Arrhythmias (irregular heart rhythms). Some arrhythmias can cause cardiac arrest, but you’ll need a voltage higher than 50 volts if you want to go down that route. Cardiac arrest can have all sorts of complications, but that’s out of the scope of this post lol.
Electrical injuries also cause electrical burns. The burns will be visible at both contact points: where the current entered the body, and where it exited into the ground. There will be a trail of damage following the path the current took to the ground. Electricity doesn’t necessarily have to travel far to hurt, and cause a lot of damage. The burns can get infected, leading to sepsis, and significant electrical damage to muscles can cause rhabdomyolysis and compartment syndrome. Both rhabdo and compartment syndrome can cause an acute kidney injury (AKI), which could definitely affect someone long term.
DC current is normally a single shock (through I assume yours is a little more intentional than usually) that throws someone and can cause blunt trauma.
AC current causes tetany, or involuntary muscle contractions. These are very painful and can lead to muscle damage. AC injuries have a higher complication rate than compared to DC injuries.
On the neuro side, we’ve got peripheral neuropathy. This occurs in about 17% of electrical burn cases, so it’s fairly common. Symptoms include muscle weakness, paralysis, atrophy, and tingling, pain and numbness in the affected limb(s).
As long as your current passed through the limb you want to injure, nerve damage is absolutely in the cards for your poor fictional characters. Repeated current applied to a limb would also likely lead to muscle damage as well, particularly at the joints, on top the nervous system damage.
Sources:
Overview of peripheral neuropathy
More in depth about neurological injuries associated with electrical burns (plus fun case study)
Overview of electrical burns and the factors that effect them
In depth article about electrical injuries
In depth article about electrical burns
If anyone has more to add, please do!
#worlds babbles#whump reference#medical tw#electrical burns#burns tw#hope this was helpful#i would highly recommend looking at the sources#specifically the last two#Stat pearls my beloved#it’s very#very nice#long post
9 notes
·
View notes
Text
Building Your Home Pharmacy
So you're in the OTC med section of the pharmacy. You've got 100 bucks burning a hole in your pocket (or maybe like $15 cause you're just starting). You're a new adult who wants to build yourself a tidy home pharmacy.
Well first you've got to know some stuff about over the counter (OTC) meds. This is the post to help you do it.
What are OTC meds? They are medications you can buy from a pharmacy or grocery store without needing a prescription. They have been deemed relatively safe and relatively easy to dose without a doctor's intervention. This does not mean they can't be dangerous, just that the general public can generally be trusted not to accidentally kill themselves with them on the regular. Keep that in your mind for later.
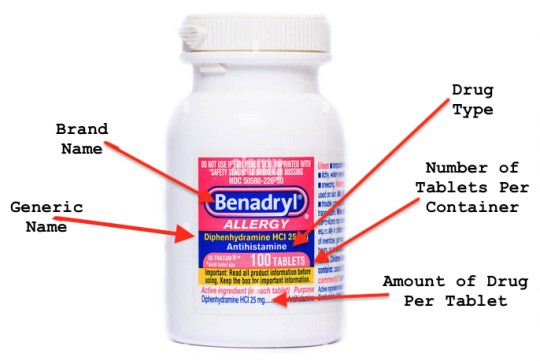
Note that all the medications discussed below are given in their generic names. In order to find these names, look below the brand name on a medication bottle:
Pain Medications:
Acetaminophen/Paracetamol: This is a non-NSAID pain reliever and fever reducer, so it's great for people who can't take NSAIDs due to stomach or kidney issues. Works best for headaches and fevers, but works on other types of pain as well. Technically works best as a suppository, but still works some orally. No increased risk of bleeding. Don't take more than directed. Seriously. This one can kill you or seriously damage your liver.
Ibuprofen: NSAID. Works against pain, inflammation, and fever. Take on a full stomach or you could get ulcers. Don't take if you have kidney problems. You can take this with acetaminophen.
Naproxen: NSAID. Probably the most effective for pain, but works against inflammation and fever as well. Lasts 12 hours. Don't take high doses continuously or you will get kidney problems. You can take this with acetaminophen.
Aspirin: NSAID. This was the first NSAID and it's definitely here to give you stomach ulcers if you don't take it on a full stomach. Technically it works for pain, inflammation, and fever. Most people today take it as a blood thinner. You can take this with acetaminophen.
Allergy/Cold/Congestion Medications:
Diphenhydramine/Doxalamine: First Generation Antihistamines. These are great for nighttime allergies, coughs, insomnia, nausea, and itching. Most people get drowsy from these, but some people get really hyper, especially kids.
Cetirazine/Loratadine/Fexofenadine: Second Generation Antihistamines. These work for allergies and itching and don't cause as much drowsiness.
Phenylephrine/Pseudoephedrine: Decongestants. These work by mimicking epinephrine, making the blood vessels in the nose and sinuses smaller. This makes the nose and sinuses less stuffy, but it raises blood pressure (so don't take if that's a problem for you). Pseudoephedrine is also restricted- you must be an adult to purchase and you can only buy so much. You have to talk to a pharmacist to get it because it can be used to make methamphetamine.
Triamcinolone/budesonide/fluticasone Nasal Spray: These are steroid sprays. They work similarly to the decongestants but only in the nose, and generally don't travel to the rest of the body.
Guifenesin: This is an expectorant, not a decongestant. It works by thinning the mucous in the lungs and airway. This makes it easier for you to cough it up. You have to drink a lot of water with this for it to work, though.
Dextromethorphan: This is a cough suppressant. It works by blocking signals in the brain that tell you to cough. Pretty much everything interacts with this one so if you take any medications talk to your doctor first. Depending on where you live you may have to talk to a pharmacist to get this one due to the potential for abuse.
Digestive Medications
Loperamide: This is an antidiarrheal. It works by decreasing the amount of squishing around your intestines are doing, which helps you hold your diarrhea and lets you continue to function. It is an opioid, but is not absorbed from your digestive tract so it doesn't make you high.
Bismuth Subsalicylate: This works for diarrhea as well, but also nausea, heartburn, and the prevention of traveler's diarrhea. Don't take if you're allergic to salicylates or aspirin. Taking this for an extended period of time can also cause bismuth toxicity.
Calcium Carbonate: This is an antacid. It is very basic pH wise, so can help change the pH of stomach contents pretty quickly. This is usually used for heartburn. If you take any other medications, this can prevent you from absorbing them if you take them within two hours. Using for long periods can cause rebound heartburn when you stop taking it.
Cemetidine/Famotidine/Ranitadine: These are gastric acid reducers, and they work by blocking the type of histamine that is necessary for the production of stomach acid. They are usually used for heartburn and ulcers.
Omeprezole/Esomeprezole: These are also gastric acid reducers, but they work by blocking a different part of the very complicated way our stomachs make acid. After years and years of taking these you might get some bone density problems.
Bisocodyl/Senna: These are laxatives. They work by increasing the movement of the intestines. It's important not to take these consistently unless you can't poop at all without them, or you seriously will not be able to poop without them.
Docusate/Propylene Glycol: These are stool softeners. They work by increasing the amount of water in the intestines. These are pretty safe to take all the time if you need to.
Simethicone: This is a surfactant. It works by accumulating all the gas bubbles in the intestines so they can be expelled. It's usually used for painful gas.
Topical Medications:
Clotrimezole/Miconazole: These are antifungal preparations. They treat yeast infections, athletes foot, jock itch, and ringworm.
Triple Antibiotic Ointment: This is a cream that contains antibiotics. Ostensibly you're supposed to put this on small cuts to decrease risk of infection. IRL just clean it with soap and water and then put some vasaline on it. Studies have shown it works just as well.
Hydrocortisone: This is a steroid cream. You put it on itchy things (bug bites, poison ivy, etc...) and it makes them not itch as much. This one actually works and is generally better than diphenhydramine creams that can't be used on poison ivy.
Permethrin: This is an insecticide. It will help get rid of head and body lice.
Zinc Oxide: This is a skin protectant. It helps prevent diaper rash and chafing. It also makes things feel better once you've already chafed. Technically it is also a sunblock, but it will make you look like a ghost while you're wearing it.
Family Planning:
Levonorgestrel: This is known as the morning after pill. It works by blocking ovulation, so that a sperm and egg cannot meet, preventing pregnancy. It can be taken up to 5 days after unprotected sex, though it works better the sooner it is taken.
Devices:
Blood Sugar Meter/Strips/Lancets: These help measure the amount of sugar in your blood. They are usually used by people with diabetes.
Blood Pressure Cuff: This measures blood pressure automatically with a cuff around the upper arm or wrist. It is usually used by people with high blood pressure.
Ketogenic Test Strips: This measures the amount of ketones in the urine. Ketones are a byproduct of fat breakdown, usually found when the body cannot breakdown carbohydrates for energy and begins to break down fat instead. Usually people who are on a ketogenic diet or people with diabetes use these.
Peak Flow Meter: This measures the amount of air that can be used by the lungs. They are usually used by people with asthma or COPD.
Great, Which Ones Do I Need?
I'd recommend look over the list and see which ones would be most useful for you, and start with those. Over time, collect ones that would be most embarrassing to not have, and then the ones that you're pretty sure you'll never use.
Note that in a dry, unopened package (including inside blister packs), drugs last well beyond their expiration dates. So if you don't use a certain med all that often, get a smaller package of it.
Great, Which Ones Can I Take at the Same Time?
Good question. I'm going to say that if you take any prescription medications, you always want to check with your doctor before taking anything OTC. However, I recommend you use an interaction checker like this one if you want to take more than one OTC med at the same time. One can be found here.
Note:
Loperamide CANNOT be taken with cimetidine/ranitidine/famotidine. This causes bad heart rhythms.
Don't take two meds from the same category together (like cimetadine with ranitidine, or ibuprofen with naproxen, or diphenhydramine and fexofenadine unless a doctor tells you to).
Most antacids (calcium carbonate, sodium bicarbonate) will prevent the absorption of other medications, so take them two hours apart from anything else you take.
Don't drink alcohol with loperamide, detromethophan, acetaminophen, or any antihistamines.
#Adulting#Adulting reference#young adults#new adults#whump reference#writing reference#medications#over the counter medication#OTC#reference
1K notes
·
View notes
Text
Treasure trove of writing reference for the medical aspect of whump
youtube
I love Dr. Chris Raynor’s way of presenting, using 3D diagrams and memes. I learned a lot from this and thought all you whump writers would like it too. It’s all about the science of torture methods; but honestly the information in it could apply to non-torture-based whump as well.
#whump community#whump reference#torture tw#death tw#this guy’s way of teaching is so much better than my senior year anatomy course (which was ALL textbook)#He makes anatomy interesting like my English teachers made literature interesting#Anyway I’ve subscribed and I’m probably not going to shut up about him lol#Obsessed#whump resources#Youtube
20 notes
·
View notes
Text
Almost Paradise s2
Just rambling thoughts. I love so much that as soon as Alex, Kai and Ernesto are tied up back to back, Kai and Ernesto start untying Alex while he distracts the bad guys and gets himself beaten up.
Teamwork and familiarity with each other so they can make that decision without having to discuss it. It ain’t the Leverage ot3 level of synergy, but nothing will ever match that, and it’s still excellent.
My whump-loving mind adores that he is automatically the one out in danger, which fits with the episode with Bob (that they’ve done the sort of thing with Alex before where they exchange him for a hostage, and that he went through hell with them trying to catch the waterboarder). He’s there to relax and not get stressed, but he’s still doing dangerous undercover stuff, which is a break from the stress of real life so that’s okay 😌 Don’t have to worry about boats breaking down when you’re actively trying to annoy a dangerous criminal.
Snarky grin with blood in his mouth? Yes please.
21 notes
·
View notes
Text
Uncommon Whump Tropes
I compiled the answers to my recent uncommon whump trope question into a list for everyone's reference. Enjoy!
CW: very brief mentions of teeth whump, minor whump, female whumpees, noncon body modification
Feral hissy kitten whumpees, the bitey scratchy ones who scream incoherently at their rescuer/caretaker rather than use their talking words. The ones who can’t be made to understand they’re not going to be hurt anymore
Medieval fantasy dungeon/torture chambers
Female whumpee and platonic male caretaker
When person 1 passes something to person 2, via kiss or other pda, to help P2 escape somewhere, especially if there had been some kind of prior misunderstanding between them
Good old-fashioned chloroforming
Mind control and mind control-adjacent tropes like hypnosis
Whumpers who are subtlety scary
Childhood trauma/minor whump
Whipping
Teeth whump
Older whumpees
Whumpees who aren't conventionally attractive
Non-“innocent sweetie” whumpees: bastards, confused himbos, feral ladies, baffled aristocrats, tormented monsters, traumatized immortals, frightened Everyday Gals who react by throwing things and yelling, questionable antiheroes
Whumpees who turn bitter. Whumpees who are angry and complicated. Recoveries that are tough. Caretakers that don’t know what to do because a little nice touch and sweet words aren’t enough
Captive whumpees that slowly manipulate the situation they're in, gaining enough favor and trust with the whumper till it's the right moment for the tables to be turned and whumpee can get their revenge
Snakes used on the whumpee
Female whumpees
Small whumpers
Whumpers that aren't the physically stronger ones
Whumpees who aren't honorable, who lie and scheme and cheat their way out of their bad situation
Whumpees who aren't defiant, because they're smart enough to know all that defiance will get them is more pain. They aren't stoic because they know the whumper wants to hear them begging and crying
Manipulative whumpees. They bend, pretending to break, until their whumper gives them an opening
Villain whumpers who aren’t interested in captivity. They just love to antagonize the hero, do they care about stealing or blowing up the city, no not that much. But they love getting on hero’s nerves and beating them and mentally dragging them down until they can hardly do it anymore, and then just moving onto a new hero when it gets to boring for them
Androids, or human whumpees inside mech suits that get ripped to shreds during a fight so that the circuitry is exposed
Average whumpees, whumpees who aren’t super muscular and have more realistic proportions, whether they are large, medium, or small
Caretaker with some sort of trauma already in their past, and they’re desperate to protect whumpee, who’s probably someone older. The caretaker— having been scarred and trying to grasp at any bonds they have made as comfort— takes care of the person who should probably be taking care of them, and then, when the whumper comes in and does what they know best, the caretaker goes ballistic. They do unexpected, dangerous things to themselves behind whumpee’s back. They get themselves so deep in their deals with whumper just to be able to get whumpee out, because caretaker would inflict pain on an entire continent before letting whumpee go. And when the whumpee’s out, caretaker is too far in to turn back now… maybe they’ll force the whumpee back, they’ll be safer with them anyways…
Monster whump. More claws, wings, fur, long ears, tails
More queerplatonic Whumpee/Caretaker relationships
Female whump (that isn't non-con). Ladies can break their arms and get kicked in the gut too
Being conditioned into submission and having trouble shaking it, i.e. even days after the shock collar has been removed they still almost never speak unless spoken to
Human experimentation
Unique stress positions, especially ones where the pain builds up over time
Noncon body modification, but more extreme than piercings & tattoos, e.g. wings/ears/tails/etc, or cybernetic things
Sci-fi themed whump that's not about androids
Whump involving timelines, time loops, alternate universes and other stuff like that
Physical signs of whump for supernatural whump that aren’t scars or lost body parts, like changed eye colors or new appendages or like marks on your soul
Forced mind control self-whump while the caretaker watches but doesn't know they're under mind control, or even a non-consensual situation because it's just barely mild-looking enough until the caretaker leaves because they really thought they were doing the right thing by trying to step in but they were told they were just interrupting and now they feel bad. And the whumpee has no idea what’s going on but when they come to and are being weakly willful to the whumper but they are informed that the caretaker saw and didn’t care, breaking the last part of the whumpee’s will that was barely holding out
More accidental trauma reveal
Lab whump
Lady whump (and lab lady whump)
Feral whumpees
Spitting blood
That trope where the group has to explore their loved one’s mindscape to save them and secret trauma is revealed in their memories
Being presented with a fear that is wholly mind numbing and the annoying character not poking fun at the one that's scare
“Phantom pain” but not in the traditional amputee sense, e.g. whumpee’s arm gets cut off in a corrupted video game and he still feels the pain of it IRL despite his real-life arm being intact…or alternative forms perhaps being: sharing a soul with someone and feeling the pain that they feel, characters with past lives feeling old injuries from their predecessors, or a mecha story where damage done to the mech is felt by its pilot
The plot allowing enough time for a newly disfigured character to process and grieve over their new appearance, e.g. Spiderman 3; the worst/best part is Peter did this to him, which adds that best-friends-do-permanent-damage-to-each-other-but-they-remain-good-friends layer. They could overcome that sense of betrayal, even if Harry ended up dying
Character getting kidnapped while sick
Teams saving someone from hypothermia
Colleagues as caretakers
Seizure aftercare
Dehydration after a long spell somewhere hot, like working hard outside, and whumpee doesn’t feel the heat exhaustion and dehydration creep up on them, which can lead to a fever
General extremes of heat, when someone pushes their own body to the limit and doesn’t realize until it’s too late, and their coworkers and friends have to pick up the pieces, leading to some pretty difficult conversations about looking after yourself and listening to your own needs
Whumpee leaves or disappears and after some time is found again with a big injury by caretaker with no context
Brainwashed Whumpee randomly switching between their brainwashed personality and their original one. Top tier: the original is stoic and grouchy but the brainwashed is either really goofy or lovey-dovey - and their loved ones go from finding this funny, to finding it unsettling because the original personality is reacting to it with terror
Shapeshifting whumpers. Whumpers that can effortlessly infiltrate and adapt to whumpees' friend circle even before (or after) whump. Whumpers that shapeshift into whumpee's loved ones during whump. Whumpers that basically catfish whumpee by turning into multiple different people and all "befriending" Whumpee, just to see the look on whumpee's face after the "I have friends who will find me" moment
Older pet whumpees, e.g. pets on the verge of being put down or past their prime time of use being berated for being so slow and weak and useless. Pets knowing they’re on borrowed time and knowing that their master is so merciful as to keep their worthless ass alive
Impalement through the neck/strung up by the neck
Being forced to apologize to everyone for making them worry while you were being tortured/otherwise suffering
Whumpees who aren't male and white
Redeemed villains that are too scared to ask for help and they end up hiding all their injuries from the hero(es)
TW: noncon/abuse/nsfw
Tickling, either consensually dubcon or against whumpee's will
More nsfw/dubcon (basically noncon but the whumpee doesn't really have a choice to resist)
Noncon touching (SEXUAL)
#whump#whump tropes#whump list#whump reference#whump ideas#whump scenarios#whump inspiration#tropes#writing tropes#whumpee#whumper#caretaker#pet whump#torture#injury#blood#gore#fear#heroes and villains#general cw#whump prompts#whump prompt list#triggers#content warning
191 notes
·
View notes
Note
Is the whole "sucking poison out of a wound"-thing entirely fictional or is there some truth behind it?
This was a real recommendation in the mid-1900s, but it has been found to not work very well and probably do more harm than good.
It does not seem like sucking the venom out of a wound is particularly helpful. Or at least, not helpful enough to negate the risks associated with making a wound (most references that talk about sucking venom out of the wound also want you to cut across the wound) and then exposing the caregiver to blood against mucous membranes, which could transmit blood borne infections.
This cutting and then sucking venom extraction method seems to have been popular in the 1970s, but by the late 1980s it had gone out of favor. Today we use compression wraps to slow the spread of the venom instead.
64 notes
·
View notes
Text
uhhh here, have some whump references

(more below the cut)

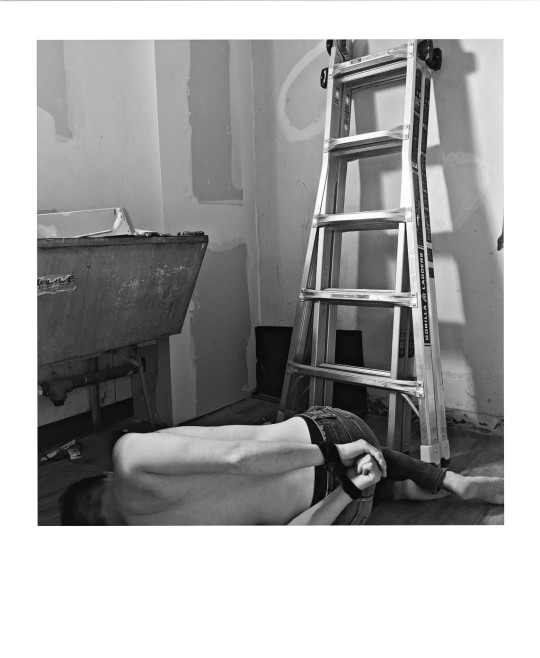

big thanks to the guy I keep in my basement 🥰 /j it's me
#courtesy of your local whump-loving gnc chick#realized my new haircut + the sorry state of the laundry room can be good for something#tw partial nudity#whump#whump reference#i used to pose as my own art ref all the time#i should do it more often tbh#deleted like 10 more because they looked off#but the corner ones are 👌👌 poses#calico almost face reveal#whump photography
304 notes
·
View notes
Last Seen Blogs

philomena-famulok
philomena famulok

nauseca
Hm

dizzyhslightlyvoided
Dizzy the Void

scarycroww
sydney

toadst0ne
now tobacconist dot tumblr dot com