
Statistics
We looked inside some of the posts by medicslacks and here's what we found interesting.
Average Info
Notes Per Post
65K
Likes Per Post
37K
Reblog Per Post
28K
Reply Per Post
49
Time Between Posts
2 months
Number of Posts By Type
Text
6
Note
8
Photo
3
Last Seen Tumblr Blogs





Fun Fact
Total funding amounts to $125.3M.
Text
Am now the Orthopod on the other side of that initial conversation lol. And if a Resp F1 called me now, the conversation would go pretty much exactly the same 😂😭
The policy in hospitals I’ve worked in is that Osteomyelitis goes to the medics for abx- usually they’ll get IVs in hospital so you can check they’re responding/ are no longer septic, then carry on for however long it takes until you can sort out a PICC line and send them home for ongoing IV abx in the community till they’ve had 6 weeks, then 4-6 weeks further of PO.
Surgeons only get involved if something needs debriding or draining. If the foot is attached to a diabetic, Vascular. If not, Ortho.
I’ve been told by quite a few Medics over the years that since Surgeons are doctors too, we should be able to manage medical problems in our patients. Fair. But the other side of that is that if they only have medical problems, why are they under Surgery in the first place? The most common argument I hear back as an Orthopod is with regards to conservatively managed fractures which need physio and pain control so often end up under Medics.
Well if the management of the pain isn’t surgical fixation, then they need medicine? Surgeons are going to give them Paracetamol, Morphine, Codeine, Gabapentin, Diazepam and Diclofenac. No laxative or PPI.
I promise you Betty with her L4 fragility fracture and no peripheral neurological symptoms is going to do better and get home much faster under Medics.
It seemed really unfair to me as a Medical F1 that surgery wouldn’t take seemingly “obvious” surgical problems, but now I realise every surgical bed that is taken by a patient who just needs medical management is a patient waiting longer at home or in hospital for actual surgery.
I cannot tell you the number of times I have had patients cry to me about how much pain they are in when I’ve had to call and cancel them the night before their scheduled surgery because I’ve been told there are no beds to bring them into, we already have 5 DTAs in ED and that patient is at home “stable”. Or because we have too many major traumas or NoFs, the Trauma List is full… so the trimalleolar ankle fracture is going to have to roll for the 6th day in a row… can I go tell her she can eat?
Referrals Are A Pain In The Foot...
ORTHO: “Has he been seen by a Tissue Viability Nurse?”
“No. We figured since this is likely osteomyelitis, he should be referred to Ortho directly.”
“Well we need them to see it first and then refer to us.”
“Okay.”
TVN: “It’s probably osteomyelitis. Please order an MRI to confirm and then refer back to Ortho.”
ORTHO: “Oh, you didn’t mention he has diabetes. Are his BMs stable?”
“They were fluctuating between 17 and 32 when he was first admitted, but he was reviewed by the Diabetic Specialty Nurse and they’re now under control.”
“Okay that’s good. But since it’s related to his diabetes, he’s not suitable for Orthopaedics anymore. You need to refer him to the Surgical Reg.”
SURGERY: “Sorry I only take referrals for general surgery. You need to refer him specifically to the Vascular surgeons.”
VASCULAR: “Have you sent a written referral?”
“Well I tried but they said I needed to call you first to let you know we need to refer somebody to you or else you won’t know to check the referrals box.”
“Okay, do the referral and we’ll come and see him.”
“Thank you so much.”
WARD CLERK: “Oh good you’re back from lunch. I have a message for you. The Vascular Registrar called about your patient- he won’t see him until you get the MRI and confirm that it’s osteomyelitis.”
“……….”
RADIOLOGY: “Hi would it be possible to get this MRI Foot done some time today to confirm or rule out osteomyelitis?”
“Has he been seen by Orthopaedics or the Vascular team to confirm that it’s likely osteomyelitis?”
“Ortho says it’s not their problem since it’s related to his diabetes and Vascular won’t do anything until we get the MRI.”
“Is he unwell?”
“Well… we’ve had to do an MCA and DoLS on him because he’s delirious from the sepsis which we suspect is from osteomyelitis due to his diabetic foot ulcer.”
“Okay. We’ll try and get it done today.”
MRI FOOT WAS NOT DONE UNTIL TWO DAYS LATER WHEN PATIENT WAS NO LONGER DELIRIOUS AS PATIENT REPEATEDLY REFUSED TO BE TAKEN DOWNSTAIRS FOR MRI SCAN.
ENDO: “He has an infected diabetic foot ulcer. The MRI showed it wasn’t osteomyelitis but we still think the infection might have caused his sepsis. We’ve investigated other possible causes and haven’t found any. He is no longer septic and has full capacity again.”
“Are his respiratory symptoms under control?”
“He never had any.”
“So what’s he doing on the Respiratory ward?”
“I don’t know. I think maybe he coughed once in A&E. Would you be able to come and review his foot and suggest further management?”
“Has he been seen by the Diabetic Specialty Nurse?”
“Yes.”
“Tissue Viability Nurse?”
“Yes.”
“Has he been seen by Orthopaedics or Vascular?”
“No they both said he’s not suitable for them.”
“Okay. Well since he’s better and his BMs are under control, we don’t really need to see him anymore. Just refer him to the Diabetic Foot team and they’ll discuss him at the MDT.”
109 notes
·
View notes
Text
Rota flexibility has been the number one factor in whether or not I enjoy a Rotation. This is made easier by having a well-staffed rota, but I’ve found that in a true chicken and egg scenario, a flexible rota is often a well-staffed one.
Nothing to do by 3pm? We do not all need to be sitting here sweating in this tiny, windowless office with only 2 computers.
Somebody go home.
4 F1s, 2 CSTs and 3 Regs on EGS? It’s so much easier for everybody who wants to to go to Theatre.
This often requires last minute swaps and adjustments which isn’t possible in a department that sticks to the mandatory 6 weeks notice. In news that will surprise nobody, this often leads to the worst case scenario of having 5 people in with nothing to do by 12 on one day, and quite literally nobody in on another…
With a lot of people set to rank Deaneries and Rotation soon, if you can find out what a particular Deanery, Trust or hospital’s policy is on 1) swapping rotations and 2) rota flexibility/ coordination. It tends to vary Department to Department and is usually easier on Surgical rotations where there tends to be a Trainee responsible for ‘in house’ swaps vs. Medical Staffing where it is a mammoth task and usually has an entire Administrative Team following specific rules and guidelines 🌚
Both have been fundamental factors as to why I’m having such a great time in Core Surgical Training.
9 notes
·
View notes
Note
Oh and another question. Is it possible if I graduated from med school(european country) to practise in the uk without extra training? My fiance is from london and I'm currently a final year med student. He wants me to move there but I don't want to have to do a lot of time consuming extra things
I’m so far out of medical school I haven’t got a clue whether Brexit affected it, but when I graduated (2018), EU students applied through the same route as us.
Given the number of UK trainees who initially didn’t get training posts this year, I’d assume it’s still the same.
OK hang on, I looked it up. Here’s what the official guidance is.
I would have linked to the Eligibility Information Page but it’s taking me to a 404- Page Not Found. So here’s the link for the full FAQ page instead.
https://foundationprogramme.nhs.uk/faqs/2-year-foundation-programme-applications-faq/
3 notes
·
View notes
Note
How much does a junior doc get paid? I'm curious because here its an average of 3k / month
Lol, much less. I got taxed incorrectly and ended up making less than 1K in a month at one point in FY1.
Dividing how much I was paid by the number of hours I was actually spending at work means I made less than minimum wage for the majority of my first year as a doctor.
Yeah, definitely wouldn’t recommend coming here as a doctor for the money.
3 notes
·
View notes
Text
Just took a year out of medicine to work as COO for a start up.
On reflection, the way we behave and are treated as doctors working in the NHS is utterly bizarre. Guys, it’s really not normal to be made to feel like a naughty child or to be spoken to like you’re an idiot when you’re very obviously not. Especially not at work.
I’ve recently been thinking back on several incidents that upset me throughout my FY training and they were all incidents that I just would not tolerate now and can’t believe the audacity of the people who made me feel that way. I repeat… at work.
I’m not entirely sure why despite so many difficulties for doctors being directly related to communication and conflict resolution, they just kind of stop teaching these skills to us as soon as we’re thrown into the field of medicine. We’re expected to just pick it up, but I’d argue these skills are just as important for our clinical practice as our clinical knowledge and so should be formally taught.
When your only reference point is being treated like a stupid, misbehaving child by everyone- you start to think that’s normal. And it’s just not. What you say and how you respond is a learnable skill but you have to first be given the opportunity to realise that the way you’re being treated or spoken to is objectively unacceptable. And then learn how to confront it while remembering the person you’re speaking to is also… at work.
I am both optimistic and cautious to be taking this change in attitude, expectation and behaviour back into surgical training from August. Like I said, the NHS is a weird world to work in when you’ve taken a step back for a while and the ground rules are a bit different. The potential benefits to my own well-being and career happiness is so significant though I think I’ll take the risk and let you guys know how it goes.
3 notes
·
View notes
Text
Can anyone else who works with Trauma & Orthopaedics patients please confirm that the one legal thing you would make immediately illegal if you had the power to is trampolines?
6 notes
·
View notes
Note
Oh also, ask your Seniors to explain things to you that you don’t understand. Having never had a Gen Surg rotation throughout my Foundation Years, I’d just ask the Ortho Regs and Consultants or Gen Surg SHOs and Regs at my hospital to explain it to me if they knew about it or had encountered it in clinical practice and could give me a real example.
I found that much less boring and much more focused than reading about it in a book.
Hi, I have to say that I am inspired by your active recall post. Just wondering, what do you do with the questions that you do get wrong? Do you write down notes for them? And also, are these just notes for the question or notes for that entire topic (like the extra notes on passmedicine). Thank you, Michael
Hi Michael,
I would work through a few different things to see what level of note taking and time commitment works best for you to get the results you’re happy with. Back in medical school I tried things like making notes from the explanations and reading around the topic etc.
But I value doing other things with my time than just studying for work-related exams given how much of my time is already spent being AT work lol. So here’s my slacker version of active recall:
I just do question banks.
This helped me pass both MRCS Part A and Part B first time despite Part B being an OSCE exam.
If I keep getting something wrong, I will narrow down the question filters to answer all of the ones on that specific topic/ category. I rarely make notes other than to write down quick aide memoires or to write out a particular fact I think is VERY important. Otherwise I’ll just re-do the questions I got wrong and re-read the explanations.
For Part B I found that an added layer to this was to read the explanation and then explain it back to myself from memory until I could essentially teach it to myself without looking at the question/ answer, working out blocks in my understanding as I sat there talking it through to myself.
I don’t make a lot of notes because I never re-read them so I just repeat questions I got wrong or flagged ones I only guessed by accident in the banks. I don’t have the patience to make my own questions but I can see how they would be very helpful.
Something to note though- I have never been particularly interested in passing an exam WELL, I just want to pass so I don’t have to study for it again. Idk if that’s a great attitude to have but I don’t really mind if people think “Oh she’s the girl who only passed an exam by ONE mark.” Because in my own head I’m thinking “I can now bypass CST and apply directly to T&O as a Registrar because I passed this exam and I DON’T have to spend any more time studying the pathophysiology of obstructive jaundice.”
13 notes
·
View notes
Photo
Literally medicine is so much easier when you really grasp the basic foundation knowledge and these notes have been an unexpected gift ✨
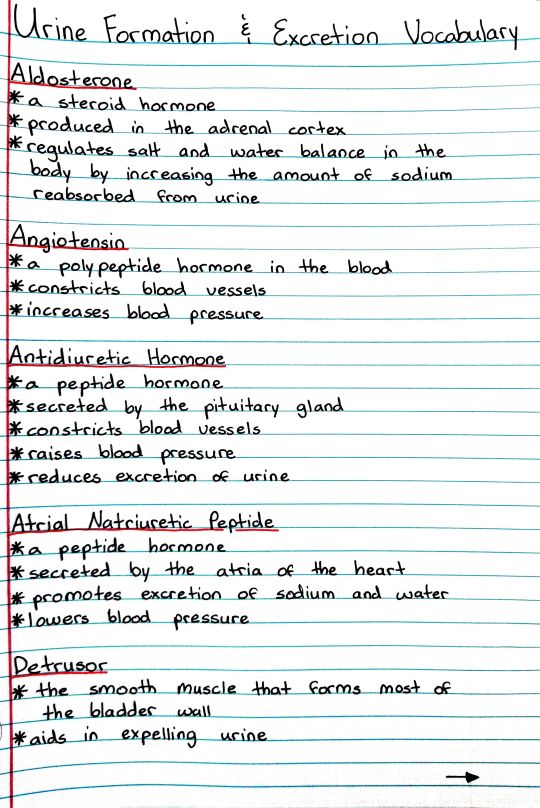
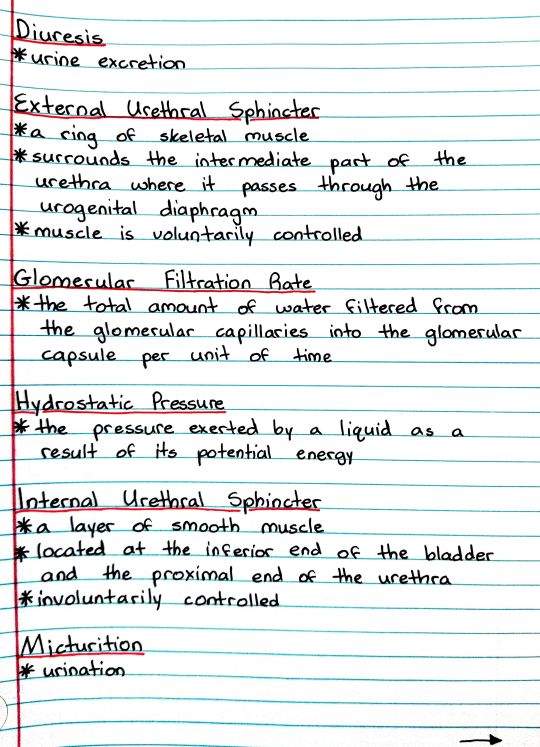
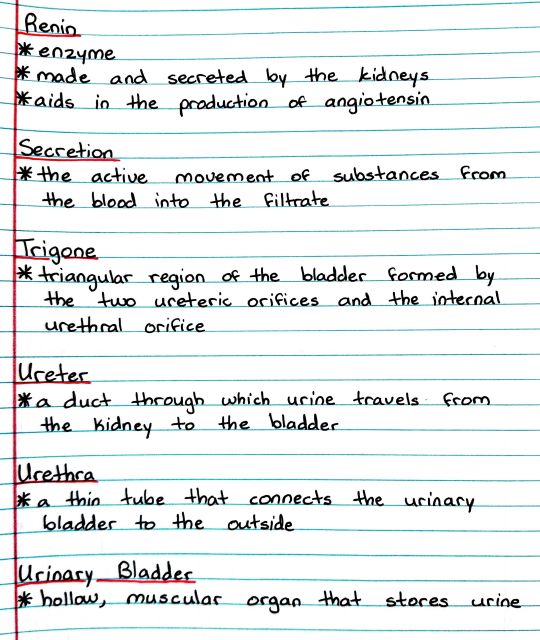
Patreon | Ko-fi
60 notes
·
View notes
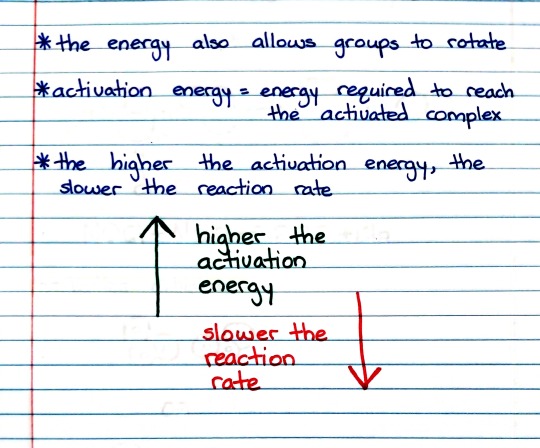
Photo
What a nice throwback refresher literally about 10 years after I last picked up a chemistry textbook lol.

Patreon | Ko-fi
20 notes
·
View notes
Note
What will you be doing this year?
Working in a medical education company that sells to the NHS. My long term plan is to work my way up through the Training and Recruitment side of the NHS so I can have a direct say in how to change the current abomination of Specialty Recruitment and compromised training of doctors due to “Service Provision Requirements”.
It’ll be good to know more about the business and management side of the NHS so I know what I’ll have to contend with to improve things in future for those of us working on the clinical side.
I will also be locuming T&O to keep my clinical skills and patient communication etc up to scratch, gain operating experience and finish up extra projects to boost points for ST3 Applications later this year :)
3 notes
·
View notes
Note
Hi, I have to say that I am inspired by your active recall post. Just wondering, what do you do with the questions that you do get wrong? Do you write down notes for them? And also, are these just notes for the question or notes for that entire topic (like the extra notes on passmedicine). Thank you, Michael
Hi Michael,
I would work through a few different things to see what level of note taking and time commitment works best for you to get the results you’re happy with. Back in medical school I tried things like making notes from the explanations and reading around the topic etc.
But I value doing other things with my time than just studying for work-related exams given how much of my time is already spent being AT work lol. So here’s my slacker version of active recall:
I just do question banks.
This helped me pass both MRCS Part A and Part B first time despite Part B being an OSCE exam.
If I keep getting something wrong, I will narrow down the question filters to answer all of the ones on that specific topic/ category. I rarely make notes other than to write down quick aide memoires or to write out a particular fact I think is VERY important. Otherwise I’ll just re-do the questions I got wrong and re-read the explanations.
For Part B I found that an added layer to this was to read the explanation and then explain it back to myself from memory until I could essentially teach it to myself without looking at the question/ answer, working out blocks in my understanding as I sat there talking it through to myself.
I don’t make a lot of notes because I never re-read them so I just repeat questions I got wrong or flagged ones I only guessed by accident in the banks. I don’t have the patience to make my own questions but I can see how they would be very helpful.
Something to note though- I have never been particularly interested in passing an exam WELL, I just want to pass so I don’t have to study for it again. Idk if that’s a great attitude to have but I don’t really mind if people think “Oh she’s the girl who only passed an exam by ONE mark.” Because in my own head I’m thinking “I can now bypass CST and apply directly to T&O as a Registrar because I passed this exam and I DON’T have to spend any more time studying the pathophysiology of obstructive jaundice.”
13 notes
·
View notes
Note
are you applying for specialty training this year or thinking of an fy3 etc?
I took an FY3 year in Trauma & Orthopaedics. Had an incredible time, learned loads, gained a lot of experience, passed MRCS Part B- dropped the Dr 🙌🏽 and am now looking into skipping CST and applying directly for a T&O ST3 Number after taking this coming year out of clinical practice to do something different that I find really interesting.
That’s the “In Summary” answer but if you have any follow up questions, lmk.
5 notes
·
View notes
Note
do you know anything about getting into cambridge for grad med? or about lucy c college, hughes hall, wolfson college or st edmunds college in general?
I’m really sorry I don’t since I never applied for Graduate Entry. Fortunately I do know that times have changed and there are Youtube videos breaking down the specifics. I know this because my friend made one ages ago let me see if I can find the link.
Here you go hope it helps! The topic breakdown in the Description looks like it may be pretty helpful to you but I haven’t personally watched this video so I don’t know how specifically it gets into if Cambridge is any different to other Grad Medical programmes at other Universities.
youtube
0 notes
Text
Lool I feel you. My inner sense of peace is intensely grateful to the drawers full of empty notebooks I have bought over the years when out solo shopping. “I’m going to journal about my feelings in this nice new notebook that’ll make me feel better.” 🌚 Just the purchase is cathartic now.
If I ever get rich, I will only buy Moleskine notebooks for everything
94 notes
·
View notes
Note
Hi! I'm planning on going to medical school in the future and I'm not sure what I want to specialize in. Do you have any stories about what pushed you to choose your specialization?
(sorry this is so long, I’m actually hoping other people with very different interests and personalities to mine also reply and give you some different perspectives so it may get even longer though lol)
Each specialty provides a different type of reward. One way you could think about it is that this is a career and you will dedicate decades of hard work to it, so what kind of work would you want to do every day that will feel rewarding to you.
I picked Trauma & Orthopaedics because the daily work feeds exactly what I find personally rewarding.
It’s not a diagnostic specialty- I get to provide solutions to problems instead of trying to figure out what the problem even is. It’s logical- there’s an algorithm or a classification for everything and you can work backwards from an injury to figure out how it happened, you can spend hours discussing how best to fix it or if you even should... It’s hands on- about as practical as it gets. I’m actually not naturally all that great with practical skills but it’s not like I’m bad... just not naturally gifted at it and I have to work harder to be good. But I like that. It’s something I can really work on and conquer throughout my career. It requires a lot of communication with a lot of different people. Constantly. I like that. Not a lot of people die and people with the most horrendous injuries sustained through the most horrifying to mundane mechanisms usually walk out... I also get on really well with Orthopods. It helps.
I excluded Medicine because I didn’t enjoy the diagnostic side enough and even the thought of one day having to be the only Med Reg in an entire hospital overnight covering Take and Wards has me feeling exhausted. Phenomenal medics I’ve worked with have all loved the mystery of the human body. They thrive on figuring out what’s happening and why. It always feels like solving a jigsaw. Start with the corners- oh central crushing chest pain radiating up to your jaw and into your left arm? HMMMM. Then the colours that obviously go together from there- oh you have angina and hypertension and you’ve recently been told you’re at risk of developing diabetes and you’ve got a family history of MIs? HMMMMMMMM. And then just raggo trying to put together anything that fits together but doesn’t necessarily attach to the corners- oh but you’re on the pill and had a TKR recently and had a 17 hour flight during which you didn’t stand up to walk around at all and you’re also feeling short of breath? HMMMMMMMMMM.
Brief Summary Of Why I Excluded Other Specialties:
A&E- disgusting shift patterns
Anaesthetics/ ITU- beeping machines give me a headache and I like being able to speak to my patients so would prefer if they weren’t GCS 3 for the majority of my time with them.
Breast- actually considered this, I just enjoy Ortho more
Cardiology- cannot interpret ECGs
Dermatology- clusters of dots have always made me feel ill and Derm conditions unfortunately often present as clusters of dots. The patients are often self-conscious enough without my irrational phobia making them feel as though even their doctor is grossed out
Endocrinology- too much diabetes, I like the algorithmic diagnostic process though
Gastro- too much poo. But I like Gastro medics.
Gen Surg (inc. all intra-abdominal Specialties)- too much poo
GP- too much dealing with chronic conditions. However, allows the best life style by far and their trainees are super protected because GPs themselves have so much power as they didn’t give away all their leadership and management roles like hospital Consultants did way back in the day.
Neurology- the brain is a huge unknown, I can’t deal with the uncertainty
Neurosurgery- the rewards sometimes feel far too small and the losses far too great. Also every time I get a response on referapatient from one of the Neurosurgical Regs I have to steel myself for the barrage of sarcastic comments and rhetorical questions. Lol why are you guys so mean? To be fair I’d probably be mean too if I had to deal with like 100 ?CES referrals a night.
Obs & Gynae- perineal tears!
Oncology/ Palliative- too much death. Despite trying to remain neutral, I get really inexplicably attached to random patients and it would definitely happen and some of them would definitely die and I’d definitely be really miserable when they did.
Pathology- cannot interpret pink blobs on slides
Plastics- burns good heavens the smell
Psychiatry- the rewards come slowly, not enough ongoing practical clinical experience. The outcomes can be phenomenal and far-reaching, especially Inpatient Psychiatry, but there is an understanding that it takes a lot of time for real change to come
Respiratory- the sight of sputum triggers a horrific gag reflex from me and I almost vomited multiple times on my FY1 Resp rotation. I like Respiratory medics a lot.
Urology- "WE ARE NOT A CATHETERISATION SERVICE!”
Vascular- the surgeries are way too long, way too often
#medblr#uk medblr#specialties#medicine#docblr#how to pick a specialty#i tag everyone seriously i want to know how other people decided
20 notes
·
View notes
Text
Here are my notes on Professor Robert Sapolsky’s Introduction to Human Behavioural Biology. I love the way he teaches, all of the examples and anecdotes to really help you grasp what exactly what concept he’s trying to teach. I think it’s important knowledge.
I really enjoyed this and actually want to learn it so I made notes.
The video is freely available and if having these notes makes understanding the lecture itself any easier to follow or understand, I’m happy to have made them.
youtube





pls excuse my typos 🤙🏽
#medblr#uk medblr#lecture notes#robert sapolsky#introduction to human behavioural biology#Youtube#studyblr#studyspo
47 notes
·
View notes
