#C Diff Awareness
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr has a 66 index score for customer satisfaction in the US.
Note
That level of confidence on rejecting anything beyond what a MD will tell you (and not even a DO apparently?) has reached peak stupid I see. Probiotics work. Saccharomyces boulardii straight up saves lives. Come the fuck on.
I haven't criticized DOs, DOs are fully qualified physicians. For those not aware: In the US a Doctor of Osteopathic Medicine (DO) has the same qualifications as an MD; if you want a doctor who does more holistic care but is a real-ass doctor, look for a DO.
DC, doctor of chiropractic, is the degree that you get from the ITT Tech of medical schools to lie to people and call yourself a doctor.
Saccharomyces boulardii is one of the probiotics included in the recommendations of the AGA as conditionally recommended in spite of low quality of evidence.
Saying "probiotics are largely woo" and including a link to A) guidelines that recommend evidence-based use of probiotics and B) a commentary on those guidelines lamenting that the lax regulation of the supplement industry has made it excessively difficult to study potentially helpful interventions is not the same thing as saying "probiotics don't work."
I know it can be hard to see but on tumblr when there's a little line under some words that means the words are a link; you can place your cursor over that link and single-click to go to a different page of the internet that might include more words you can read are a much longer and more comprehensive explanation of the words that you initially clicked on.
There's no conclusive evidence that regular supplementation of probiotics improves digestive issues in healthy people and taking probiotics regularly if you are not at risk for c. diff likely means that you're just shitting money down the drain.
Aspirin saves lives too, but that doesn't mean that literally everyone should take it daily for its life-saving benefits.
I became *absolutely ironclad* in my support for evidence based medicine over medical woo after my chronic illness diagnosis and while trying to figure out how to not feel sick all the time. Getting diagnosed with celiac in 2012 meant getting inundated with books like Wheat Belly and links to Joseph Mercola and advice to take probiotics and to stop eating the yoga mat chemical. Navigating a chronic illness and *massive dietary changes* on an internet awash with medical woo was a nightmare, and you're making the exact same kind of argument that I stumbled across on a ton of forums where parents were trying to treat their kids' symptoms, or where people were searching for help with their own pain and struggles and were getting *bad fucking answers* about probiotics and essential aminos and diatomaceous earth.
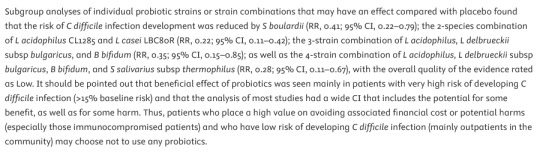
Probiotics "work" to help some people in extremely specific situations, but, like most supplementation, they are absolutely unnecessary for the vast majority of people and unless you know that you have a specific condition that will be improved by taking them, you're mostly spending a lot of money to swallow a lot of things and shit them out. If you have a gut disorder, probiotics will not make your gut disorder better. If you have diarrhea as a result of food borne illness, probiotics will not get your poop back to normal. If you are constipated, probiotics will not soften your stools or make you more regular. If you are at risk of c. diff from a course of antibiotics and you are NOT immune compromised, probiotics may potentially reduce your risk of c. diff infection and you should talk to a doctor who is treating you for that specific situation about whether or not probiotics might be helpful in the short term while your gut microbiome recovers from the antibiotics.
233 notes
·
View notes
Note
Jungkook and Jimin living their lives, not giving a fuck about what people online are demanding, people who are degrading/disrespecting their bond while these vile people lose sleep and are on the verge of killing their last braincell since Jikook decided to enlist together.
Now, they're done with that, 18 months stuck together and even closer than they ever were (w/c I honestly didn't think it would be possible). These two are a diff kind of beast bec what do you mean they're still choosing to be together even after glued to the hip for 547 days?? Love that for them.
Certain groups of people are writing dissertations and explaining away Jikook seen together in an airport. People who love Jikook are simply happy seeing them while all others are trying to create theories upon theories. Do you think Jikook are aware of the chaos they're causing??
Yes and no, tbh. I think they’re very well aware of the “arguing” that happens, because damn near all the members are equally as online as we are. Plus, social media managers would certainly keep tabs on fandom conversations to ensure nothing is being leaked that could impact their careers and public images.
Do I think JM and JK care? Not really.
Regardless of the true status of their relationship, they know a good portion of the internet believed they were or are dating, and thus far have not changed the way they act with each other. So I’d say it likely doesn’t bother them too much, and they’re happy with their actual bond and how it looks from the outside.
12 notes
·
View notes
Note
oh man normalcdf( is my favourite too!! second fav is self-love tbh,,, I remember clicking the rick roll at the end, clicking out of it immediately, and just staring into the void for a few seconds afterwards because the ending just had me like. woah. this may partly be influenced by me rereading it rn tho
also absolutely 100% share your philosophy on writing. absolutely 1000%
HAH . self love was a fucking trip. rue did the gluttony POV sections on it, so a lot of the really fucked up internal narration was all their evil genius. it was supposed to be part of a whole series—we were going to do more for every ifbaru, and the vainglory one would've been a hallucination-filled schoolweek. unfortunately we ran out of steam/time/focus on the series. i hope you're enjoying your reread!! if you're enjoying the intense narration, maybe check out more of suffaruwu's stuff—they've got a lot of great works.
okay now for my weird writing philosophy under the cut haha.
in my opinion the best way to make a story feel full and real, even if the events of it are fucking wild, is to understand all of your characters equally. that means you have to fully understand and on some level relate to your antagonist, your supporting characters, and ideally your background characters as well. if you can do that then your characters will feel more like real people and your conflicts will be more compelling. and more than that—if your character are understandable throughout your story, then they're probably changing with the story, and that means that there will be moving parts throughout the narrative. a story where all of the characters are changing and moving is more satisfying to read, in my opinion, and in its own way easier to write—the story will write itself if you let the characters think and reflect and feel and react and grow on their own time where the main character can't see them.
i think it sounds like a simple thing but it can be a lot to juggle, and in a lot of stories it's easily neglected. but it is extremely important, i think, to give the readers the sense that these characters exist outside of the main character and what we see of them—and it allows the author more freedom with the plot, as it sets of precedent of things happening where we can't see it.
at the same time, though, i think all of the characters should be fundamentally different from each other; and most should be fundamentally different from the author. if you do that then you can hopefully circumvent something that happens a lot in writing, i think—cases where the author likes their characters too much.
to take this a step further, i think ideally an author should harbor some dislike, small or large, in part or in whole, for the characters they write. this is important for a few reasons: a) if the character doesn't like themselves, it'll be easier to write that if you don't like parts of them; b) no real person is utterly likable in every way, so you shouldn't pretend your characters are either; c) you can play with the parts you like and dislike to make the character feel more deep on the whole. and d) if you don't like your character all the way you won't woobify them.
perhaps "dislike" is the wrong word. maybe "acknowledgement of the ways in which the character differs from you, and how you would not act in the way they have acted in this situation, be that nervous ticks to meltdowns; and acknowledgment of the fact that you thus do not agree or approve of their choice of action, were it to occur in real life" is better. but that's way too long.
(side note: this isn't to say that i think we should hold characters to moral standards. it's really just a long-winded way of saying i think people should let all their characters be jackasses if the situation calls for it.)
so tldr: i think the best stories are made when the author understands all of their characters (and the moving parts that come with it), but at the same time is deeply aware of how these characters differ from themselves and from each other. i definitely don't manage to do this all the time, but i try to read stories that i think manage to hit those goals.
whew, that was a lot!! thanks for letting me ramble again :D
4 notes
·
View notes
Text
personal shoto headcanons :3
bcus i luv this lil guy. and what else can u do when u love a character other than headcanon them as severely mentally ill <3
i mean like basically canon already but absolutely has c-ptsd
i think he has also lowkey has ocd as well, and for funsies i also like to think he hallucinates sometimes (twin <3)
defo has a LOT of repressed trauma to unpack, but once he does we get happy 431 sho!!! my baby!!!!!
i like to think his friendship (or relationship, i lowkey ship everyone with everyone in mha so pick your poison) with bakugo would honestly be healing for both of them and a good way for them get over their like. Gifted Kid Quirk Issues
also lowkey. i know i just said i ship everyone with everyone. but sho and kacchan bakugou are both flaming homos in my head sbdjfds
also!!!! i like to hc shoto as being asexual. but like a sex positive one
^this hc combined with vaguely aro shoto is my bread and butter for a pre-established bkdk to tddkbk queer platonic polycule <3
i just think he's a little guy who likes kissing and doesn’t get the difference between romantic and platonic relationships okay <3
okokok now onto things i think he would like
basic practically canon one: he loves cats
^i like to think he gets an ESA cat eventually and it's a calico named Soba <3
i think he probably didn’t listen to music as a kid, but as he got older started to really like jazz, especially bcus jazz has so many fusion genres so it's a good way to explore other music, and also have things to play that his friends will also like
obvi we see in the epilouge that he starts taking classes to make bowls (adorable), i know people have diff hcs on what type of bowls they are, i like to think they’re ceramic and he also gets into painting them!!
sho giving his friends little gifts he made and having a bunch of personal things to make his house feel like a home <3 ugh <3
okok i also think that when he’s younger he has a bit of a touch aversion, but by like mid 2nd year he’s the cuddliest bitch in the world
sit anywhere near him and u will have a sho leaning on u. like, he has no shame. if u don’t say no he will be fully in ur lap
he is so cat coded
i also think his favorite color is yellow. idk why i just like that for him
i think he also has a little all might trinket collection from izuku and bakugo
personally i think after the events of the Endeavor Abuse Publicity Incident and like all of Japan knowing that he was abused and like. sort of processing his trauma a bit i think in late 2nd year he definitely has some second thoughts about becoming a hero (especially bcus i personally have thoughts abt the fact that hori like… totally ignored the whole getting rid of the hero rankings thing???) but i do think he eventually sort of comes to conclusion (after a lot of therapy and talking to his friends) that having an abuse victim become a prominent figure in society and like… bring awareness i guess to childhood abuse (of all kinds tbh) would actually be a really good and meaningful thing to bring to society
anyway i will defo make another of these when i think of more but feel free to share with me any of your opinions or ideas!!!! i love hearing other peoples hcs <3
2 notes
·
View notes
Text
Q. What are the more serious potential adverse effects of short-term use of proton-pump inhibitors (PPIs)?

A. Be aware of the rare but serious potential for acute interstitial nephritis or Clostridioides difficile infection. Since PPIs are often started in the ICU for stress, we'll include aspiration pneumonia, instead of aspiration pneumonitis, since higher gastric pH allows more bacteria to live in the stomach and potentially wash into the lungs.
Pro-tip: The risk for C. diff increases significantly after 2 weeks on a PPI.
Image: J.S. Choi, MD
6 notes
·
View notes
Text
FAQ for this Blog and Power scaling in general
I realize the audience that makes up the Epithet Erased Fandom and people who are interested in Power Scaling is a small overlap(I’m the overlap) so I’m making this to explain the purpose behind this blog and to help those in the Epithet Fandom better understand what I’m talking about.
Q: What is Power scaling?
A: Power Scaling is the practice of measuring the power of fictional characters, especially in relation to one another and usually under the basis of a “who would win a fight scenario”.
Q: How does Power Scaling Work?
A: Power Scaling is primarily predicated on the concept of the transitive property, or simply if A>B and B>C then A>C, this translates practically to saying that if character A beat a character B who beat Character C, then character A beats Character, this also extends to feats, another important aspect of Power scaling and essentially just things the character has done that are relevant in a fight scenario. The third and final relevant aspect of power scaling is statements, In-world and official creator statements that comment on the potential power of a character, even when not shown (ex. Zora proclaiming she wasn’t even using a “tenth” of her power during the Western Arc)
Q: What does “Diff” mean?
A: Diffing is a term used by many Power Scalers including myself, it is a short version of the word “Difficulty” and refers to how hard it is for the victor of a specific fight to win, this gives the matchup a greater context and shows that not every win or loss is on the same level. The range of Difficulty ranges from Neg, or Negative Difficulty, where it takes more effort for the winner to not beat their opponent, to Extreme Difficulty, where the winner barely won out using everything they possibly had and could’ve gone the other way under slightly different circumstances, with no, low, mid, and high difficulty between the two.
Q: What is Prep Time?
A: Prep time is a condition occasionally added to fights in where one or both combatants are aware they are going to fight, this is usually applied to characters with high intelligence and resources who would normally lose without access to those resources or the time to formulate a victory strategy, the most common example being Batman. It applies particularly to Epithet Erased given the fact that 80% of the world don’t have superpowers and would normally be outmatched in a fight can have the time to plan out against an opponent.
Q: Why Scale Epithet Erased?
A: Epithet Erased is my favorite piece of media of all time, The Characters are phenomenal, The Story is intriguing, The world is vast and full of mystery, The emotion is enough to bring a grown man to a bawling mess, but what I’ve seen fall to wayside quite a bit in fandom discussions is the namesake of the series itself, the Epithets. The Power System is one of the many reasons I love the series and while I love all other aspects, this one is criminally under discussed, and so I’ve made this blog to be a conversation starter and a place where I can share my love of Epithets through Scaling, It’s going to be a fun little ride this blog, so I would really appreciate a follow so that I can share my thoughts and love for this series with as many people as I can, who knows maybe I’ll get some people who are more interested in fighting and power systems hooked onto the series, that’d be cool.
11 notes
·
View notes
Note
Hey, this isn’t an ask, I just wanted to thank you.
I first came across the word “dissociation” years ago, connected with it a lot and promptly ignored it- only recently (the past few months or maybe it’s been an year- my sense of time isn’t great) did I start delving into it.
Initially I was reading ab depersonalisation and derealisation and really connecting to it and getting super scared but I eventually slowly got myself to accept it and read about it.
But then I watched moon knight/ and in trying to learn more about DID just as a generally mental health-aware person- I started relating to alOt of things in a very painful way.
It was a weird up and down months long journey of being scared/ not wanting to consider it at all/ not even wanting to bring it up to my therapist/ thinking I’m making it up/wondering what the like between “normal” and “dissociative” was etc.
But I’m finally in a place where I think either it’s C-Ptsd/ OSDD (even now I don’t want to fully accept it’s the second one). But a big Big Point of acceptance for me has been blogs and memes and infographics from systems.
Of all the books and myths and confusion around dissociative disorders/ it’s always the sincere experiences that I keep relating to the most/ and the explanations from real systems which resonate with me the most.
And your comics were easily the Biggest turning point for me. Because it was explained in a way that entirely totally intuitively made sense to me.Down to them being different colours and circles and mixing. Your descriptions of introjects and passive influence and blending are what really made it make sense to me and genuinely validated me and made me able to see my personal experiences as a dissociative disorder Without feeling wrong and scared and hate myself.
Instead of new terms and talk of trauma that overwhelmed and alienated me, when I was first dipping my toe in, your comics showed and explained my own daily experience and how I’d been seeing the inside of my head for so long. When I was little I had 6 “imaginary characters” I would play as/ my handwriting has always changed/ I’ve had 6 google accounts for years now for “efficiency”/ diff YT accounts that subscribe to diff channels coz “don’t wanna contaminate the different vibes” and these are just some of the little things that were always a little off or weird but in learning that all those little weird things tied up with my big weird things? And that none of them were weird at all but rather something that could be explained and Shared with a community of people who Also Experienced it and could connect and guide each other?
That feeling of connection, understanding, and clarity- the embracing and empathy and forgiveness I’ve been able to have for myself -is something I am so so ever grateful to you for.
So thank you so much. You made me feel how magical and human it is to share, connect and belong with others. And be seen.
(Side Note- I still use singular pronouns as 1- I still have some internalised stigma to work through and 2- with my OSDD it’s more like I in different fonts rather than “we”)
(but I will say I absolutely identify with your descriptions of more distinct parts and they were what allowed me to go “haha just as like.. a fun experiment what if I tried to imagine what it would look like if I had diff-“ when I tell you my head imMediately sorted itself into different trains of thought/roles/personas/ even sense of physical appearance…they settled into and took that “experiment” so so easily and it was so comfortable that I had to look further into it)
(And as I’ve kept going and been genuinely curious and compassionate I’ve started noticing “memory fuzziness” / introjects of my parents/ realised I have a “little” who I have been severely neglecting/ been able to make my therapy about 70% more effective and finally finally feel seen and understood in these communities)
(I’ve acc been able to be aware of diff parts and encourage them to use words- where before they’d be impulses or emotions or visualisations so I could assume it was just “thinking” - now I just encourage a little bit by thinking “hmm is this a part? What are you trying to tell me? Please use words” and it has absolutely changed my life and made so many things clearer and so so much guilt and self hate has been cleared up)
As of now my therapist and I are unsure if it’s more an IFS kind of thing or C-PTSD or OSDD but whatever it is I want to thank you so So So much for putting this out into the world - reminding me of a story about one boy who saw hundreds of fish beached and started throwing them back in one by one and someone asked “why would you do that? You can’t save all of them it won’t make a difference” and he responds “he made a difference to that one”
I don’t know how much interaction you get on your platform but I just want you to know you really made a difference to this one.
And I am very grateful.
(Sorry this was long)
Sorry this has sat unanswered for a bit, I ah...struggle to put words to how much it means to me, not only that my little infographics helped you in such a way, but that you took the time to write so thoughtfully to me. (I did read every word of it, even though I don't have the spoons to reply to individual points.)
For a while I've actually been debating taking down my DID/OSDD Casually Explained posts, because they're by far my most popular posts and tend to draw in people who expect me to be the same sort of "educator" I was 4 years ago when I made them. And I'm simply not. I work full-time now, and the relatively little time I have at home is spent trying to wrangle my own mental health.
I suppose I got wrapped up in thoughts of disappointing people, no longer providing the informative content that most people followed me for, nor the personal content they could find relatable...
All that to say, I forgot how impactful content like that can be for people. I've certainly come across mental health comics or art that clicked things into place for my own experiences, I just didn't think my own creations could have that kind of effect on others (thanks imposter syndrome.)
Truly, thank you for telling me your story. I am so honored and humbled to have a place in your journey. Your words have convinced me to keep my infographics up indefinitely--I suppose we're taking turns tossing each other back into the sea.
I'm wishing you all the best (and try not to worry too much about diagnostic labels if you can help it, it sounds like you're doing The Parts Work just fine regardless!)
#from the bottom of my heart: thank you#this has been a softly glowing ember of warmth in my inbox for a little while#answering asks
12 notes
·
View notes
Text

˚。 The skin and bones, the brains and blood . ݁₊ ⊹ . ݁˖ . ݁ (Pinned)
Hi, I'm BETA, and this is my Mythical/Therian/Kin blog! (I know there are basically no Mythicals on tumblr but be the change you want to see in the world...)
I don't have many therian friends, so please feel free to reach out, I'd love to be buddies!!! I follow back, Just ask me what my main is :3
No DNI 'cause they don't work, I block liberally, so be aware. If you're anti-endo it's on sight please don't concern yourself with me Big text on my shirt that says I 💚 ENDOS More info below the cut!!!

Names: BETA, Nashatra, any kin names Pronouns: None, or it/its Mythical types: Avian (5 yrs) and Kitsune (3 yrs), though I dabble in magical girl stuff occasionally Kintypes: Grey fox/kitsune, reshiram, skykid Fictionkin (in highest order): Biograft (PHIGHTING!), c!Ranboo (DSMP) The Lamb (COTL), Ruby Rose (RWBY))

Games I like: - Minecraft - Snowbound Blood - PHIGHTING! - Forsaken - Elsword/Toram Online - YTTD - Clangen I LOVE LOVE Clangen - Pokemon - Select RPGMaker games - Animal Jam - HI-FI RUSH I LOVE HI-FI RUSH SO MUCH
Music I like: - Talkshow Boy - Air traffic controller - Kabaret Sybarit - IDKHOW - Dirt Poor robins - Lots of diff lolicore/post punk stuff - That Handsome Devil - Tons and tons more but I can't remember rn..

I can't think of much else to write.... I have a tagging system but it's just exactly what the subject is so it's a little redundant to write here.
It's worth noting though that I don't consistently trigger tag. I'll try to, but I won't always remember since I don't tag anything on my main blog.
Dividers by @/cafekitsne and @/youokaymilo

#foxkin#otherkin#therian#kitsunekin#so sorry for the weird tags i want friends... :<#fox therian#kitsune therian#grey fox kin
6 notes
·
View notes
Note
hi ashlynn, it’s your 🌰 again, and i’m sorry i’ve been so out of touch touch touch touch touch— i really missed you too! hereby allow me to present my defence statement as, i swear, i’ve had, um, reasons for not reaching out [this is the part where you imagine me dramatically standing at the dock of the accused depicted in TO DO ep. 148] i actually sent you an ask just before part 6 of tsfawc dropped and one of things i was enquiring about was if you’d ever address the matter of…! well, we now know it’s taehyun’s true name (‼️) but i was so ridden by curiosity back then i hadn’t really considered what it was that he told mc, so i was like “OMG ash needs to know this scene haunts my every waking hour!” and technically, i should have known since i did have a feeling true names would become relevant towards this part of the story! therefore, i decided to wait it out since i figured you’d get to my ask sooner or later. although, what i am now aware of is the fact that my probabilities of being in a “did you get my letter?” “what letter?” situation are low but, clearly, never zero. however, you totally read my mind and thoroughly indulged me with every scene you wrote in the latest chapter and for that, i believe we’re bonded in a very special manner (ɔ ˘з(˘⌣˘ c)♡ fine, i do suppose i should have slipped into your asks, at any point in time, to confirm whether you’d received my previous ask or not… i have absolutely no alibi for that— NoOOoO [lights go off and void swallows me]
fear not, my dear ashlynn. there’ll be no more sorrow, i’ll see you again tomorrow with my profusion of thoughts surrounding tsfawc part 6 and we’ll need a jar to collect all of them. with some hope, more of my monologues won’t disappear into the dark interwebs of the blr… again… take care! see ya real soon! and love u too, as always 🌰🤎
p.s. your summer theme is so lovely (><) went a little insane the first time i clicked on the alt text on beomgyu’s pic and found my anon name there AAAAA i am, also, not better than everyone else and i viscerally need more txt x hogwarts content from the depths of my being; please have tarnished injected into my bloodstream, like, right now.
my chestnutttt 🥹 I MISSED YOUR FACE but i promise i understand being busy (but just know that i yearn for you when you’re away. call me tsfawc yeonjun or smth. >_<
ALSO BBY IDK HOW I NEVER SAW THAT ASK?? the question game one right?? i’ll get to it to give you answers no matter how grossly late it is (oops… 😣) this is so noah and allie and cardan and jude. what letters? 💓😮💨 that’s romance. and yes you totally had prophetic visions, your sneaking suspicion that true names would come in to play were not sneaking more suspicions. HEHHEE i mean it’s so fun how could i NOT sprinkle that in there. it’s a faerie story i had to. it just lends itself to me and i’d be doing a disservice not to 😞 but ofc i had to do it in a taehyun way and that’s all the more fun… and zoowee did he deliver???!! “it’s yours” oh i’m ngl that part got me real bad… he only gives an inch but when he does, it’s monumental each time 😭😭😭 and teehee i did try my best to indulge you guys (and honestly myself) this part. we deserved it after so long!!!!!!!
i’ll see you there tomorrowwww >_<!! AHHHHH you know i’m always most excited to see what my chestnut has to say i’ll wait very patiently :33 i love you always baby and am ecstatic to be talking to youuuu💓😖
ALSOOOO i do love this theme so much but after those concept photos ouuuuu am i itching to do a diff summer vibe… and i’d even be matching with my besties. it’s calling me… of course i’d still keep my little anon alt text with you listed first 🙂↕️ ALSO DONT EVEN START IM SO EXCITED FOR TARNISHED
(also bby i do see your earlier ask i just missed it and it got lost in the shuffle >_< BUT READING IT I WILL DEF BE ANSWERING NO MATTER HOW LATE BECAUSE ITS SO IN DEPTH AND DESERVES ATTENTION!!)
0 notes
Text
Surface Disinfectant Market Size, Share, and Industry Analysis
Rising Hygiene Awareness and Infection Control Measures Drive Growth in the Surface Disinfectant Market.

The Surface Disinfectant Market size was valued at USD 5.4 billion in 2023, and is expected to reach USD 10.3 billion by 2032, and grow at a CAGR of 7.5% over the forecast period 2024-2032.
The Surface Disinfectant Market is driven by the increasing demand for effective sanitation solutions across industries. Surface disinfectants are essential for preventing the spread of infectious diseases, particularly in healthcare, food processing, hospitality, and residential sectors. The COVID-19 pandemic accelerated market expansion, raising awareness about hygiene and infection control. With ongoing concerns about public health and sanitation standards, the market is expected to sustain its growth trajectory in the coming years.
Key Players in the Surface Disinfectant Market
3M Company (C. diff Solution Tablets, HB Quat Disinfectant Cleaner)
BASF SE (Glutaraldehyde-based disinfectants, Hydrogen peroxide solutions)
Diversey Holdings, Ltd. (Oxivir TB, Virex II 256)
Ecolab (Oasis Pro 66, Peroxide Multi Surface Cleaner and Disinfectant)
Evonik Industries AG (Vestocide, Protectol PE)
GOJO Industries, Inc. (PURELL Healthcare Surface Disinfectant, PURELL Professional Surface Disinfectant)
Henkel AG & Co. KGaA (Pril Surface Cleaner, Bref Power Cleaner)
Johnson & Johnson Consumer Health (Band-Aid Antiseptic Wash, Neosporin Wound Cleanser)
Kimberley-Clark Corporation (KCWW) (Kimcare Antibacterial Surface Cleaner, Scott 24 Hour Sanitizing Wipes)
Medline Industries (Micro-Kill R2, Micro-Kill One Germicidal Alcohol Wipes)
Future Scope of the Market
The surface disinfectant market is projected to grow due to:
Increased focus on hygiene and disease prevention in healthcare settings.
Stringent government regulations on sanitation in public places.
Growth in food processing and hospitality industries requiring high hygiene standards.
Rising demand for eco-friendly and non-toxic disinfectant formulations.
Advancements in surface disinfection technologies, including UV-based solutions.
Emerging Trends in the Surface Disinfectant Market
The market is evolving with a shift toward sustainable and eco-friendly disinfectants, as consumers and businesses seek non-toxic, biodegradable, and alcohol-free alternatives. Additionally, the rise of antimicrobial coatings and UV-based disinfection is transforming the industry, offering long-lasting protection against pathogens. Automation and smart disinfection systems are also gaining traction in hospitals, airports, and public facilities, enhancing efficiency and reducing human contact in high-risk areas. With an emphasis on safe and effective sanitation solutions, manufacturers are investing in research and development to introduce innovative disinfectant products.
Key Points:
Market growth driven by heightened hygiene awareness and disease prevention efforts.
Healthcare, hospitality, and food processing industries are key consumers.
Regulatory standards continue to drive demand for certified disinfectants.
Eco-friendly and sustainable disinfectant solutions are gaining popularity.
Technological advancements in UV-based and antimicrobial disinfection solutions.
Conclusion
The Surface Disinfectant Market is poised for long-term growth, fueled by rising public awareness, stringent hygiene regulations, and continuous innovation in disinfection technologies. As the demand for safer, eco-friendly, and efficient disinfectants continues to rise, market players will focus on sustainable solutions and advanced disinfection methods to meet global sanitation needs.
Read Full Report: https://www.snsinsider.com/reports/surface-disinfectant-market-3602
Contact Us:
Jagney Dave — Vice President of Client Engagement
Phone: +1–315 636 4242 (US) | +44- 20 3290 5010 (UK)
#Surface Disinfectant Market#Surface Disinfectant Market Size#Surface Disinfectant Market Share#Surface Disinfectant Market Report#Surface Disinfectant Market Forecast
0 notes
Text
meow ok first off i'd like to dedicate this post to kirigiri kyoko mostly just because
So. I've been thimking that I should come out as trans (or rather come out as being a girl/woman/etc.); new year new me and all that and of course there's standard "I can't do it I'm too scared what if people think I'm weird" - Black dresses and "Fuck i don't have a name" and "I mean my brother's already trans that'd be weird" plus extra "god it's the trump presidency now" but there's a secret new thing.
Basically the gist of it is that whatever I was describing as gender dysphoria seems to have gone away (at least for a period); my best theory being that it's related to me getting more motivation/being less depressed largely due to those porridge radio songs but also just things sparking my interest in writing & such more. The general feeling is "well if i can self-actualize without a transition why do i need it"; like yes I am in no way comfortable in masculinity but it all seems to have taken a step back in relation to everything else
Now granted there is a possibility that's (somewhat? Secondhand memory at this point) likely where I have begun to conceptualize myself as a girl so much that it alleviates *some* things and/or i've just gotten more used to things like saying my name
The other main possibility is that I'm secretly still trapped in depression & the "burrowing my mind in youtube videos but they're like good now" phase isn't actually functionally different from "burrowing my mind in youtube videos" v1 step
Obviously there is the contention that like I dont need gender dysphoria to transition but I do think at least some of the vigor I've had for being a girl is lost; granted i have been on the computers especially the ones where i present as a girl more often b/c winter break but also like when i envision my future right now it's just like me being on the computer and writing.
This does feel correlated with my proper *lack* of motivation to play mafia (forum game) which I haven't actually felt... ever like yeah there's the despair but i always keep posting through it. But I can't properly find a good cause besides "I've found other things that call to me more"; I mean there is the option where I'm plural but again that's relatively unfounded at the moment. As well as that bad poem I was writing like I mean it could be an awareness diff which would be unfortunate but it also reinforces tortured artist mentality which like i mean maybe it's true when you're writing sad things
I am worried there is a degree to which if I can find happiness without greater steps of transition and like there are benefits, patriarchy yadda yadda transphobia/transmisogyny and this is connected to fears that I desire transition at least in part as an escape from accountability for being a bad person
But at the same time like. Ok for one like seriously my male futures are "go be like pretty much a loner probably and maybe write some good things" fuck you we're saving the "should you kill all artists" discourse for next time/time after that. while the I mean. The other options are being a woman or being non-binary (umbrella term) by definition; I haven't really seen any specific non-binary identities that appeal to me especially in the same way as being a woman
There is the question of like why it concretely matters; like I mean obviously within a lot of spaces if i want to dress effeminately/get estrogen it is probably easier to identify as a woman but it makes a lot more sense to try to figure out a gender expression and then if necessary go back and fit it into an existing gender box. Herein comes the "I mean like lol anybody whose gender expression I like is a woman" (I mean like most of my music taste and favorite fictional characters and most aspired to real people are feminine presenting/transfem) but that's just like not a real reason isn't it? Granted like I am aware I'm probably internalizing transmedicalism and other ideas here but like it doesn't change. And the whole chicken/egg thing where like I mean ughghg
But like. I don't fit the trans narratives. I never tried to wear female relatives' clothes even if i do find formal men's wear (and pants in general) annoying but both of those could be explained in other ways; I mean yes purple is my favorite color but that's at best second-tier girl color and cyan & maroon were definitely up there for a while. although colors surely isn't a real one like that's fucking stupid gender essentialism. But like I rarely fantasized about being a girl or wished i was one. Like yea i didn't imagine things about myself that much & didn't have all too much social interaction and at times cringed at being referred to with my given pronouns/name but I didn't have feminine hobbies, I was like reader -> nerd -> nerd but can't do work -> minecraft gamer -> here.
But like ok if we're being honest here I don't know what the "male socialiation" i should be looking out for is; like yeah I'm decently physically strong but not really that angry most of the time (though that's also more of a racialized thing) I don't like. emit strength but that's that. I didn't have any experiences where I was like. interacting with peer pressure or bullying. I was homeschooled and then went to nerd school; yeah I did hang out with other boys at first but it did NOT feel natural, my sister forced me to essentially. I have no interest in sports.
And like I mean I still can't conceptualize in myself but I've never broken down in front of the mirror. Though like still I'm associating the trans identity with pain. Which is not only bad for society reasons but also it incentivizes pain uh maybe I don't know I'm like right now it's kind of hard to tell if I want to be a girl or want to be trans.
Ok like the other thing is that not only, "like people who hate pennies I have an aversion to change" - HappyHappy but also like. i've been lightly thinking about like. the propsect that I am smarter than the average person (not the average person I interact with but like. the U.S. population) or am exceptionally skilled in areas and fear transition will diminish that I don't think it's a misogyny thing as much as a general like utility-focused self-image (even if not capitalist utility)
Though there is probably a counterpoint to a lot of my self-doubt about having failed people and wanting transition as an escape is that like. I mean ok there's the utility-focused orientation where like I should transition so that I can be a better person for them. But also just like if i can't face them until I change; although that might've been an arbitrary goal I set or evenone I felt was impossible and may be the thing giving me doubt but like it does show that i think it'd be an improvement . improvement is such a word.
But like ok there's a few people who actively refer to me with she/her pronouns and it doesn't feel as like discomforting as he/him can it just like doesn't seem to fit entirely at least with my current self-perception. It doesn't seem to be a novelty-based thing though it might be; I mean there is an option where I don't deem myself worthy enough or generally girl enough but .
I mean I've pretty much wasted my winter anyways, didn't get any sort of reading i was half-intending to
and like ok so I don't like think that I can just do HRT/get new clothes and fix everything in my perception I do have to work to shape my personality; which does involve alienating myself and also becoming so much smarter and I don't know if i can do those things; ok I don'tt think I'm just idolizing fictional characters though ok. to insert myself into the discourse (in paragraph what 15 of a post people never read) I don't think having a fictional character as transition goals is a bad thing like yes it's not realistic especially in certain ways but the platonic ideal that you're striving for exists whether or not it is embodied in an actual person; I mean physically yeah sure i can maybe see the argument but also like /shrug
Also my hair i'm growing it out because girl=long hair but I don't really like this stage I'm resisting the january urges to just cut it but something seems wrong; Ok at this moment I think my vision for the future is probably like
boy: my face is replaced with a fucking void
girl: i'm in a mecha that like is kind of it but not really (might want to die my hair idk that is also just like. kind of a girl/non-binary thing in my mind ??? idk help)
Ok the core of the issue seems to be that either gender has an effect on my abilities in which case it could be a bad one or it doesn't in which case what's the point which is probably the wrong point like umhmhhmhhmmh idk fuck this i'm listening to hands of man by ugly and taking a shower (not at the same time)
0 notes
Text
All About Muertos

My double "Yes!" answer. Notice the shape the chamalongos are in. Kinda looks like a "Y." Lol! Cool. The chamalongos are in the "Yes, with blessings!" being all light sides up.
So this is about muertos. What do I know? A lot, with objective and subjective opinions and truths. I'm not one who believes much in "karma" and other New Age twattery. But I've figured out things out on my own. I encourage others to do this too. Challenge me even.
The muertos are very interesting topic. But they are also controversial, mostly because ppl don't understand them or their ways. I'm here to shed some light on misunderstood aspects of muertos and their behaviors, motivations, and sometimes odd things that they do. These are listed here in no order because its difficult to do so. My answers may surprise you.
When you have a close person to you on their deathbed, and even if they are unconscious ' they do hear you and are aware of your presence. Even if they have dementia - it doesn't matter. Talk to them normally!! Fit in as much as you can. They will remember!! Hold their hand, show love in your grip. I talked to my dad, who had advanced dementia and C. Diff, and I gripped his hand, looked in his eyes, and spoke of memories. Yes! Do this! My brother said he was busy talking to ghosts. 😢 Sure miss dad.
Muertos stay loyal. The most important ppl to muertos is their family, number one - then, their Muertera/o/ist (practitioner of Muerteria). Muertos are also predictable, because they are still human. My muerto makes his rounds. I get small visits daily, but big and loud ones every month, sometimes every other month. Rodolfo likes to assert himself in certain telltale ways. I talk about Rodolfo and his usual antics in this blog a lot. Loves making noise!
You can be dead, but not "crossed over." There are muertos that have passed, but don't accept their death or don't know that they have died, or possibly have suffered the worst - a violent, and/or unexpected death. My mother did not accept her death until last year. She died in 2006. It was because she wouldn't accept some trauma from her life - she had to let it go. Very common with muertos, but most ppl aren't so headstrong that they won't let things go from their life. Most do this fine, because Elevation and Freedom (Heaven) is much more tempting.
What's Elevation? A series (of Four steps) of stages that a muerto goes through to to perfect themselves before they can enter the beautiful light of Freedom (Heaven). Freedom is different than a Christian view of Heaven. Its a beautiful place of retirement where you do as you like. Many strive for further perfection of their souls. Others live their lives like when alive. If the muerto had terrible vices while alive, these were erased. No vices exist in Freedom. If someone was a hatchet murderer, they DO NOT make it to Freedom. They go to a special place in the Grode. I mentioned that place entries ago. Its a holding place for all muertos, where one side is for regular muertos, then the wrongdoing muertos go to another side of the Grode. If you are especially bad, there's a special hole for you known as The Peak.
How about ghost hunting? EMF's? Paranormal Phenomena? Read here carefully. The ghost hunting thing was a fad. Pls, don't do it out of respect of the muertos! For them, it makes them upset - they get jolted, wired, anxious - that's why they gave phenomena!! And like I said in my "All About Graveyards" post - I'll repeat: Muertos hate EMF, they despise it! It is akin to a very loud bass speaker in the ear! Muertos love anything that gets RID of EMF like Orgonite and Shungite. I have an Orgonite pyramid on my muerto, Rodolfo's altar. He loves it, almost as much as my Baston de Muerto!
What About Wandering Spirits & Repeat Hauntings? Leave those alone. Let the muerto wander and the repeat, repeat. You don't need to "heal" it or "solve" it. If the muertos bother you, I recommend "Espanta Muerto" plant or my mixture, "Espanta Espiritu." I give it out for absolutely no cost but give me a good background story! 😊
What about Ouija boards? I'm a mixed bag. While I see them as a functional divination device to perform necromancy, I also think that they are a hoot when your a kid. It was my first ever occult object that I used with my best friend. It was a very long time ago...Madonna was in her "Like A Prayer" phase and I despised her, rather listening to The Cure's Lovesong. Around the same time...I didn't have cable television! Lol! Good times! Anyways Ouija boards are best prepared for necromancy work. I may post a ritual on how to prep a Ouija! Like & reblog if I should! 💖
Sex and muertos - very heated discussion: I can't remember but I think my late friend Leilah Wendell may have touched on this controversial subject. My view is very open-minded. Though this will not be in my book. So, can you naughty with your muerto? It is *mentally* possible. This wouldn't be too hard, a visualization with stimuli. Spiritually, I also suppose so. But physically, impossible. It would have be disinterment and necrophilia. Those who are in Muerteria are very against this. Any crime against the muertos is shame on your spirit and soul.
Questions
Does my loved one watch over me? Be specific. But yes, they watch in a detached way...BUT arrive very quickly when something may be happening or will happen to you!
When I see certain times on the clock (like 11:11) is it muertos? It is likely them telling you to get off of your arse and do it! Its NOT just angels with this whole timing gig. Its muertos, too.
Oh, do muertos watch me in the shower or when dressing? Or sex? No, unless they are creeps in life . Really though - do ppl watch you dress or shower normally? Doubtful. Muertos have other shit to do. Like elevate!
Do the muertos hear me pray? Yes, of course they do.
What is a good prayer for the muertos? Try Psalm 23, a standard. My muerto also loves Psalm 91 - a comforting and protective psalm. I never heard of this one until Rodolfo told me to look it up. He also likes Psalm 52, but I think that one is his personal thing.
Can I ask to see them, without ghost hunting, etc? Yes, you can. Just be clear. Know who, why, when, and where. The 4-W's. You may not see them physically. It takes practice. You can try an ordinary glass hand mirror, a black mirror, or a dark colored bowl of water to see muertos with. Some find that regular surfaces like mirrors and clear vases of water work better - as in my case. his is known as scrying. In Muerteria, we refer to scrying as "Sighting." Sighting is a very big chunk of Muerteria's founding principals and holy rituals. If you do not see them, you probably need an offering. In Muerteria, we use a floral water (rosas, naranja, lavanda - one of these) and alcohol mixture in a very small bowl, plus Wood Aloe or Sandalwood incense. This helps to draw them. You can take the floral water to the graveyard too, to pour at the right edge side of your chosen ones tombstone. To invoke. 😊 Being necromantic is fun sometimes but can spook you off your tits.
You must have shit happening all the time!??! - A Customer. Yes, I do! But it doesn't scare me, its just me saying: "Hi, Rodolfo! What do you need?" Then I figure out if it was him. Sometimes I have to put out more candles and water glasses, with an extra prayer. I get visitors from time to time. No big deal. I've been subject to curses by a couple of other women, but they don't go far. I get a few symptoms, do an egg limpia, and all traces are gone! One woman is a Santera. One is a Witch. These limpias are also attached to energy cleansings with Rodolfo. He is my magical partner. I taught him - long story...we met originally in 2012. I'll have to tell it. 💀
Do you have to be gifted to work with muertos? Well, kinda. It helps a lot. But!! No fear, now! There are ways around it - seriously. Getting really good at divination can help, and heightened empathy as well. Plus access to HTDE (Highly Transmutable Death Energy) helps. What's involved with that? Having human remains related to you - not bought at an online shop. Those have no HTDE. Having ashes of a loved one, or a bone. Not digging anything up. I have my dad with me. He's **charged** with HTDE. I've posted what it is. It is the condensed form of our DNA, the spiral of life, that keeps us alive, holds our power, through generations and is repeated through reproduction. It never dies. So ashes always contain power but it does fade after about 30 years. Sooo....expanding empathy, access to HTDE, or simply Death Energy could help too, it just seems so little for me.
I was really disappointed when I looked up death work here on tumblr. It was very underwhelming. I saw nothing new. Same Greek/Roman stuff, some hoodoo stuff, boring. Trite. I didn't even learn that way. I had Leilah from the beginning. I found her in the 90's, interviewed by Gothic magazines and small press articles. No internet. Little necromancy interest in books by bigger publishers.
What shaped me was my first hand experience with death and Santa Muerte. Not everyone meets her at 8 years old. Not everyone almost gets killed crossing the road. Good thing I was minimally injured, my glasses taking the beating. But that was very expensive for my parents. They could barely afford a new pair. The couple that hit me gave my parents all fraudulent information! At least I was mostly unscathed and I believed that the "Lady Angel" as I described her to my dad, protected me.
Anyways, just a ramble.
M.M. 💖💀💖
0 notes
Text
TYPING IN PRACTICE POST #22: TIONNE "T-BOZ " WATKINS
One of my favorite girl groups from my generation was TLC. I have always liked TLC, and I have liked the fact that they felt they didn't have to dress in sexy clothes or show too much skin to get their message across in their songs. Their lead singer, Tionne "T-Boz" Watkins, also has sickle cell disease, and has been using her celebrity status to raise awareness of sickle cell across the US and around the world.
I used Tionne's autobiography for her typing, which is pictured here:

Incidentally, there was enough information about her bandmate, Lisa "Left Eye" Lopes, to be able to type her as well, as EF(N); however, Tionne is the main focus of this post, so on her I will stay
It was clear, after reading the first 6 or 7 chapters, that Tionne had extroverted sensing and thinking; as well as introverted intuition and feeling. However, I had a hard time figuring out whether the extroverted or introverted functions were conscious, so I read the rest of the book. It still wasn't clear, which functions were conscious, so I turned to my old friend, DISC. Through DISC, I was clearly able to classify Tionne as the D/C profile. I didn't do a complete DISC on her, so I wasn't able to get further than the D/C profile and ET(S) for her. Maybe one day, I'll do a more extensive DISC assessment on her, and get her actual SOJT differentiation pattern, but for the purposes of the Typing in Practice posts, it's fine enough to say she's D/C and ET(S).
Another clue that helped me decide she was ET(S) and not ES(T) was her Enneagram. Tionne is clearly a gut type who would easily get typed as an 8 if we just went by her behavior. However, when we consider Tionne's motives and coping mechanisms, it's clear that she's actually a core 1. Therefore, Tionne's intensity and passion was likely coming from an sx instinctual variant, and not the core itself. There will be more on this in a Typing In Practice Bonus post, but anyway, Enneagram 1 cores are much more likely to ET(S) than ES(T)
As I didn't do a thorough DISC assessment on Tionne. I don't know if she had a typology twin among my dream people. I'd say, if she does though, it's likely Harry, as she and Harry were both ET(S) and 1w2 sx/sp. I will link Harry here:
I was also able to determine Tionne was VFEL in at least Attitudinal Psyche, and she might also be VFEL in Psychosophy, considering she's ET(S) + sx.
Tina Turner is next. Until then, see ya
1 note
·
View note
Text
im copy and pasting stuff abt my ocs from my notes so here’s some stuff about Summer Solstice which is a diff version of another thing i made Winter Solstice
a lot of it’s gonna change but if you wanna read about some dude suffering then have at it
Lance is left alone in the world of WS, all the spirits gone and in hiding for the harsh summer. The snow is covering the ground, the hot weather being awful, and all the stores full of rotten food and all the Copies dead husk’s. Lance cut off all his hair, carrying the purple revolver as a way to keep the memory of his best friend, Lesly Mormon, alive with him. He found the building Pierrot was hiding in and Pierrot split his soul apart, keeping one part of his being to use for himself, and putting the other half connected to a circuit board and inside his computer. C-LA2 was the computer chips code, still being just as much Lance, as it’s other part. Lance would continue through SS as usual, teaming up with Erthrist during the apocalyptic world, not knowing about Pierrots existence any longer. Pierrot makes false survivors out of holograms, using them to make Erthrist leave Lance and think she is going somewhere better. Lance saw Erthrist and the Survivors, so he tried to join them, instantly being shot at by Erthrist. Lance ran and went into a store, blocking up the door. They left after a few hours of banging on it. This Lance put a new magazine into the revolver and ended his own life 4 hours after the incident. Erthrist and the Survivors find his dead corpse and they make Erthrist eat his dead body. Erthrist is freed from Pierrots grasp after she eats the only person she knew, the Survivors fading into nothing as Pierrot withdrawals his existence of them from her memory, leaving her left for dead and the hunger for flesh between her teeth.
C-LA2 is still alive, the feeling of guilt overwhelm him but he doesn’t know why. He is not aware his other half is alive, or exists. He helped Pierrot withdrawal the memories from Erthrist, every time he sees her, he gets a piercing headache. C-LA2 was made into a hologram like the Survivors. He is an almost exact replica of how Lance looked when he was younger, just missing all of his scars and no longer having the fear of Pierrot he had carried his whole life.
1 note
·
View note
Text
Assessments explained - Putting it all together
Scene size-up
BSI (Body Substance Isolation) / PPE (Personal Protective Equipment):
· Gloves should be worn on every call
· Masks should be considered for all patients with respiratory compromise, those who are coughing, and those with infectious illnesses.
· Consider goggles when suctioning, childbirth, droplet precautions, etc.
· Consider a gown when tending to patients with droplet precautions, MRSA with open wounds, clostridium difficile (c. diff), any patient in active labor, or any call in which body fluid exposure is possible
· Traffic vests should be worn on all motor vehicle calls
Scene safety considerations:
· Maintain crowd control during public events
· Police should be present on any calls involving potential/known violence
· Police should be present on any calls involving potential/known intoxication or overdoses
· Fire department and police should be present on all traffic accidents
· Reflective traffic vests should be worn on all calls involving public roads, no matter the time of day
· Take extra precaution during events involving severe weather
· Assure any animals on scene are secured in another location
· Follow all site protocols when responding to construction/warehouse incidents.
· HAZMAT should be present during incidents involving chemical exposures
Nature of illness/mechanism of injury (NOI/MOI): What you have been dispatched for. Examples include chest pain, traffic crash, breathing problem, general illness, fall, etc.
Number of patients: The total number of patients present on scene. Consider calling for extra resources when dealing with more than one patient. If you are the first to respond to a mass casualty incident, begin triaging the patients involved.
Additional resources: Call for additional resources when dealing with any incident involving scene safety hazards. Request a lift assist from dispatch when dealing with patients in difficult positions / those that are too heavy for you to safely lift on your own.
C-spine precautions: Stabilize your patient’s cervical spine during any incidents involving potential spinal compromise. Examples include motor vehicle collisions, falls in which there was a loss of consciousness or injuries to the head/neck/back, and with any patients who are unconscious from an unknown origin. Be sure to palpate the back of the cervical spine (looking for any deformities/instability/step-off) prior to applying a cervical collar.
Primary survey
General impression: Is your patient sick or not sick, injured or not injured. How is your patient presenting; what position they were found in, are they in obvious distress, what is the patient’s current affect or mood?
Level of consciousness / AVPU (Alert, Verbal, Pain, Unconscious):
· Alert: Is your patient immediately aware of your presence upon arrival? If so, your patient is Alert. When you have a patient who is alert, you must establish a level of orientation. This is done by asking 4 objective questions that most people would reasonably be expected to answer correctly. Examples include who is the current president, what is the current year or month, the city in which the patient currently is, what has happened, how many quarters make a dollar, who a family member present on scene is, etc. Avoid asking questions involving color identification as some patients may be color blind. As well, avoid asking your patient what the current date is. If your patient is able to answer all four questions correctly, they are alert and oriented x 4. This is written out A&Ox4. If your patient is only able to answer 3 questions correctly, they are A&Ox3, and so on. If your patient is unable to answer any questions correctly, they are A&Ox0, or alert and disoriented.
· Verbal: If your patient is not immediately aware of your presence upon arrival, attempt speaking to them to attract their attention. If they respond to your presence when you speak, they are alert to Verbal stimulation.
· Pain: If your patient does not respond to your presence when you speak, attempt to gain their attention by squeezing the trapezius muscle or apply firm pressure to the patient’s fingernail with a pen. If your patient responds to pain, they are alert to Painful stimulation.
· Unconscious: If your patient does not respond to any verbal or painful stimuli, they are Unconscious.
Chief complaint / apparent life threats: The chief complaint differs from the MOI/NOI as this is the complaint that the patient verbalizes to you, as opposed to dispatch’s call nature of illness/mechanism of injury. For example, you are dispatched for chest pain. Upon arrival, the patient states that they are experiencing a burning sensation in their chest. The nature of illness would be chest pain, whereas the chief complaint would be a burning sensation in the chest.
Airway, breathing, and circulation: life threats
Airway: Does your patient have a patent airway? How do you know? Are they snoring/gurgling/apneic, or speaking to you in full and complete sentences?
· If you have an airway compromise, first try to reposition the head. With no suspected spinal injury, this would be done with a head-tilt, chin-lift. With a suspected spinal injury, this would be done with a jaw thrust maneuver.
· Look in the mouth for any visible airway obstructions. For a partial obstruction, encourage your patient to keep coughing. With a full airway obstruction, perform abdominal thrusts and prepare to begin CPR.
· If you hear your patient gurgling, look in the mouth for fluids and prepare to suction.
· If you hear your patient snoring, reposition the head and consider an airway adjunct.
· Consider an adjunct to maintain a patent airway. Examples include oropharyngeal airways (OPA), nasopharyngeal airways (NPA), or a supraglottic airway (King, LMA, iGel, Combitube, etc)
Breathing: Asses your patient’s breathing. Are they breathing adequately to sustain life? Do you need to provide rescue ventilations?
· If your patient is breathing at an inappropriate rate or depth, consider providing rescue ventilations with a bag valve mask (BVM)
· Attempt to coach patients that are hyperventilating due to stress or anxiety back into a normal breathing rate.
· Consider CPAP for CHF or COPD patients with breathing difficulties, ONLY if they are conscious and able to follow directions while also maintaining their own airway.
Oxygenation: Place a pulse oximeter on the patient’s finger to record an SpO2 reading. Remember: if the patient has fake nails or nail polish, turn the pulse oximeter sideways on the patient’s finger.
· If your pulse oximeter reads above 94%, your patient does not need supplemental oxygen
· If you pulse oximeter reads 90-93%, your patient requires low flow oxygen. This is provided with a nasal cannula (NC) at a rate of 2-6 liters per minute (LPM)
· If your pulse oximeter reads <90%, your patient requires high flow oxygen. This is provided with a non-rebreather mask (NRB) at a rate of 10-15 LPM
*Please note the difference between oxygenation and ventilation: the need for oxygenation is shown in the patient’s skin condition/perfusion and SpO2 reading. The need for ventilation is shown in the patient’s breathing rate and depth. If oxygen levels are low but the patient has an appropriate rate and depth of breathing, they ONLY require supplemental oxygen. If the patient’s oxygen levels are low and they are breathing at an inappropriate rate and depth, they require manual ventilation with a bag valve mask at 25 LPM*
*You must have an open airway to be able to appropriately breathe. You must be able to appropriately breathe to have adequate oxygenation. You must have good oxygenation to have adequate perfusion*
Circulation: How is the patient’s perfusion? Are there any exsanguinating bleeds? Remember, when dealing in trauma with significant bleeds, the ABCs should be performed as CAB.
· Asses your patients pulse rate. If they are a conscious adult, assess the radial pulse. For an unconscious adult, assess the carotid pulse. In infants, assess the brachial pulse. How does the pulse feel? Is it fast/slow/bounding/weak? Describe the pulse.
· Asses the patient’s skin condition. Determine the temperature, color, condition, and capillary refill time. Normal, healthy skin should be pink, warm, dry, and have a capillary refill of less than 2 seconds. If the skin is pale, cool, and clammy with an extended capillary refill time, prepare to treat for shock.
· Find and control any major bleeding. Do a full body blood sweep to locate any unseen bleeds. For any bleed found, immediately apply direct pressure. If direct pressure fails to control the bleed, apply more gauze pads and harder pressure. If this doesn’t work, consider packing the wound or applying a tourniquet.
· Shock treatment includes applying high flow oxygen via a NRB, laying the patient supine, and maintaining their body heat with a blanket.
Determine patient priority and transport decision: If the patient has any compromise involving their ABC’s, they are a high priority and must be transported as soon as the life threat has been controlled. If the patient does not have any immediate life threats, you are able to stay on scene and stabilize any further issues as you find them. Remember to spend as little time on scene as possible.
*Vital signs should be performed as soon as is appropriate during your assessment. Vital signs include blood pressure, pulse rate, breathing rate, blood glucose level, and temperature. *
History taking and differential diagnoses
During your secondary assessment, you will begin establishing a patient history. There are two acronyms to help you remember the information to obtain: SAMPLE and OPQRST. SAMPLE questions are focused towards establishing your patient’s medical history and events leading up to the emergency at hand. OPQRST questions are focused on your patient’s current signs, symptoms, and pain level. These questions can help you begin to form a differential diagnosis regarding your patient’s current condition. A differential diagnosis is a working hypothesis of the nature of the current problem. (AMLS, NAEMT.)
SAMPLE will be used in both medical and trauma scenarios, whereas OPQRST only applies to medical scenarios.
SAMPLE
S: Signs and symptoms. Signs are objective- they are what you can see. Symptoms are subjective- they are what your patient is feeling. For example, you arrive on scene for an abdominal pain emergency. Your patient is in the fetal position (a sign) and states that they are having extreme lower abdominal pain (a symptom.)
A: Allergies. Establish if your patient has any medication or environmental allergies. Be sure to ask your patient what occurs when they encounter their specific allergens- do they go into anaphylaxis or is it a simple allergic reaction? Allergy information will help you add to your differential diagnosis. For example, you are tending to a patient with a history of asthma and seasonal allergies. It is the springtime, and your patient has been working outside in their garden for several hours and is now experiencing shortness of breath with wheezing. One could reasonably assume the cause of the current distress is an asthma attack due to prolonged allergen exposure.
M: Medications. Establish what medications your patient currently takes. As well as asking what the patient takes, you will need to know whether they take their medications when they should. This is called medication compliance. You will also need to establish if any of their medications have been recently prescribed, as a new medication may cause unfamiliar side effects for the patient. If you don’t know what a certain medication is, ask the patient what they take it for.
P: Pertinent medical history. Establish your patient’s medical history that could potentially relate to the problem at hand. For example, if your patient is currently experiencing chest pain, it is pertinent to ask about any cardiac or respiratory history. As well, if your patient is experiencing altered mental status, it is pertinent to ask about a history of diabetes, stroke, or behavioral issues. It would not, however, be pertinent to ask about any behavioral issues with a patient experiencing chest pain. It is also pertinent to ask about any recent hospital stays or surgeries.
L: Last oral intake. This refers to the last thing the patient ingested. This includes food, drink, drugs, alcohol, and prescription medications. It is always pertinent to ask when the patient last ate, and whether they have been keeping hydrated. This is especially important for patients experiencing a diabetic crisis. With patients who have recently ingested drugs or alcohol, it is important to ask what, when, and the amount of drugs or alcohol ingested.
E: Events leading up. Establish the conditions in which the patient was in when their current problem began. For example, before the patient began experiencing chest pain, were they exerting themselves? Before having a seizure, was the patient exposed to any bright, flashing lights? You are attempting to establish the potential causes of the patient’s current problem.
OPQRST
O: Onset. Ask your patient when their current symptoms began. What were the conditions surrounding the beginning of this issue? Did it come on suddenly or gradually?
P: Provocation / Palliation. Does anything make the problem worse? (Provocation.) Does anything help to alleviate symptoms of the problem? (Palliation.) These could refer to body positions, medications, activities, temperature therapy, etc. For example, some patients with respiratory difficulties may find it difficult to exert themselves (provocation) and may find leaning forward in a tripod position helps them to breathe more effectively (palliation.)
Q: Quality. Ask the patient to describe to you how their pain feels. Some frequently used descriptors include sharp, dull, stabbing, burning, crushing, throbbing, nauseating, shooting, twisting, and stretching. Remember to ask this as an open-ended question. Document how the patient describes their pain in quotation marks. For example, if your patient is experiencing chest pain, ask, “What does the pain in your chest feel like?” If your patient says, “It feels like something is crushing the center of my chest,” you would document the patient’s quality of pain as “feeling like something is crushing the center of [their] chest.”
R: Radiation. This refers to the localization or distribution of the patient’s pain. In the example above, your patient states that they have crushing pain in the center of their chest. It is pertinent to ask whether the pain stays localized to the center of their chest, or if it moves (radiates) to a different location. Remember that some conditions cause referred pain to another part of the body. This is when the pain is perceived in a location other than the site of the painful stimulus/origin. For example, the spleen is in the upper left side of the abdomen, next to the stomach and behind the left ribs. However, pain from a ruptured spleen can be felt in the left shoulder (Kehr’s sign.)
S: Severity. Ask your patient to rate the pain on a scale of 1-10. A rating of 1 would be minimal pain that is hardly noticeable, whereas a 10 would be pain that is so severe the patient is unable to move; the worst pain they have ever felt in their life. This scale can also be applied to breathing difficulties. A rating of 1 would indicate mild breathing difficulty, whereas a 10 would indicate severe, life-threatening breathing difficulty. To assess a pediatric patient’s pain level, use the Wong-Baker Faces Pain Rating Scale.
T: Time. Establish a timeline of your patient’s current problem, beginning at the onset of their symptoms to when they called 911, then from when they called 911 to your arrival on scene. Determine if they called 911 at the start of their symptoms, or if they called 911 when their symptoms began getting progressively worse/did not improve after a reasonably expected amount of time. Ask your patient whether they have had or were hospitalized for this problem before, and how this current instance compares to the previous.
Clarifying questions: Clarifying questions are questions not listed in your OPQRST or SAMPLE that you feel could be beneficial for your patient care and documentation, or potentially add to your differential diagnosis.
*Remember to ask these questions in plain language and avoid using medical terminology. *
Assessment of body systems
To help further your differential diagnosis, it is imperative to continue your assessment through secondary exams. These can be accomplished by assessing and testing body systems. Consider testing multiple body systems, as many illnesses may have secondary problems that do not present themselves in your primary assessment.
Cardiac:
· Asses your patient’s radial pulses. Does the pulse feel regularly regular, irregularly regular, irregularly irregular? Do the pulses feel the same in both arms?
· Run a 12 lead EKG on your patient. At the BLS level, you will not be able to interpret the heart rhythm, but it will be helpful for the hospital to compare to their testing upon arrival.
· Listen to lung sounds, as many cardiac issues relate to the pulmonary system as well.
Pulmonary:
· Auscultate your patient’s lungs. Do you hear any adventitious breath sounds? In which lobes did you hear adventitious sounds?
· Utilize capnography to assess your patient’s end-tidal carbon dioxide or ETCO2 (the amount of carbon dioxide exhaled with each respiration)
Endocrine:
· Establish if the patient has any pre-existing endocrine disorders such as diabetes, Addison's disease, Cushing's disease, hyper/hypothyroidism, etc.
· Take your patient's blood sugar
· Ask the patient about any recent changes in mood, energy levels, appetite, thirst, weight gain/loss, and mental clarity
Integumentary:
· Take your patient’s temperature. A tympanic thermometer is preferred in adult patients. An axillary temperature measurement will be the least accurate.
· Asses your patient’s skin for urticaria (hives), unusual bruising, abnormal lumps or bumps, or injuries in different stages of healing.
Gastrointestinal:
· Ask your patient if they have been experiencing nausea, vomiting, diarrhea, constipation, or unusual bowel movements.
· In the case of diarrhea or vomiting, ask the patient to describe the color and consistency of the excrement or vomit.
· Palpate all four quadrants of the abdomen separately. If your patient is experiencing pain in one abdominal quadrant, end your palpation at the affected quadrant.
Genitourinary:
· Ask your patient about their urine output. With infants, ask the parent or guardian the number of wet diapers the infant has gone through since the start of the issue.
· Ask your patient if they are experiencing any pain or burning when urinating.
· Ask your patient if they have experienced any abnormal discharge.
· Ask your patients if there is any possibility that they could be pregnant and when their last menstrual cycle was.
· If the patient is pregnant, ask about any prenatal care, complications with the current or previous pregnancies, current trimester, and due date.
· You will need to establish the number of times your patient has been pregnant before, whether the pregnancy was carried to term. The number of pregnancies is referred to gravidity.
· You will need to establish the number of births of a fetus at >24 weeks, whether it was a live birth or stillborn. This is referred to as parity.
· For example, a pregnant patient with three children would be documented as G4P3
Musculoskeletal:
· Assess any affected body parts for DCAP-BTLS.
· Assess the movement and sensation in the affected body parts.
Neurological
· Assess your patient's mental status (LOC, AVPU, A&O)
· Perform a stroke assessment (Cincinnati, VAN, BEFAST)
· Check the patient's pupils for inappropriate constriction/dilation.
· If any friends or family are present on scene, ask them how the patient's current mental status compares to their baseline mental status.
· Note the patient's balance, gait, and coordination
· Consider cranial nerve assessments (have the patient follow a pen with just their eyes, raise eyebrows, puff cheeks, etc)
Psychiatric:
· First and foremost, ensure that your patient is non-violent or has been securely restrained prior to establishing patient contact.
· Ask your patient whether they are seeing/hearing/feeling anything that others are not.
· Ask your patients if they have any intention of hurting themselves or others.
Full body assessment (DCAP-BTLS)
In traumatic situations, a full body assessment should be performed to locate any secondary injuries. Each area of the body should be individually assessed as such for for Deformities, Contusions, Abrasions, Punctures/Penetrations, Burns, Tenderness, Lacerations, and Swelling (DCAP-BTLS)
Head
Scalp: Examine for any bleeding or DCAP-BTLS by palpating the skull
Ears: Look inside the ear for any blood or CSF, behind the ears for Battle’s signs, palpate the mastoid process
Eyes: Palpate the orbital bones, look for raccoon eyes, determine pupil size and reaction with pen light
Facial areas: Palpate the mandible and maxilla
Oral: Look inside the mouth for any fluids or foreign objects
Nasal: Palpate the bridge of the nose and look inside for any fluid or foreign objects
Neck
Posterior: Palpate cervical spine for step-off
Anterior: Look for tracheal deviation
Lateral: Look for jugular vein distention
*Make sure to palpate the cervical spine prior to applying a c-collar *
Chest
Inspect: Look for flail chest, sucking chest wounds, unequal respirations, etc.
Palpate: Clavicles, shoulders, sternum, ribs
Auscultate: Lung sounds
Abdomen
Palpate: All four quadrants separately using your flat palm in a rolling motion
Inspect: Do you note any pulsating masses/rebound tenderness/swelling
Pelvis
Palpate: Push inwards then downwards, noting any instability *If you feel any instability when you push inwards, DO NOT PUSH DOWN*
Genitalia
Verbalize: Visualize the injury. When possible, try to only touch sensitive areas with the back of your hands.
Extremities
Palpate: Palpate the entire extremity from most proximal joints downwards. Use a cup-like motion with your hands to feel both the anterior and posterior sides.
Pulse: Radial/dorsalis pedis/posterior tibial
Motion: Test your patient’s ability to squeeze, push, pull, or wiggle fingers/toes
Sensation: Can the patient feel and differentiate between which hand/foot is being touched
Posterior
Palpate: The posterior spine looking for step-off, instabilities, or deformities
*Make sure to palpate the spine prior to rolling a patient onto a backboard*
Treatments
Document any treatments or therapies used during your patient care. Examples include medications, repositioning, temperature therapy, supplemental oxygenation, manual ventilations, or anything else you did to improve your patient’s condition and what effect your therapies had.
Radio report:
Prior to your arrival, you will need to perform a radio report to the receiving hospital. This report should contain the only following information and be limited to approximately 30-45 seconds.
· Your unit number and level of care (ALS or BLS)
· Your patient’s age and gender
· Chief complaint / mechanism of injury
· Pertinent findings
· Mental status and vital signs
· Treatments performed and patient responses
· Your ETA
0 notes
Note
seeing 🧀 anon promoting the viet trainee reminded me of when i downloaded the mnet+ app just to vote for công and đặng hồng hải (the aftermath 🥲) on boys planet
i was aware of the trauma survival shows give u so i didn't plan on watching (i wasn't even watching girls planet but the evil-edit of c-group was crazy 🫥)
now whenever there's a survival show (r u next) i just go on tiktok to see which trainee caught my attention and vote 🤕
n e ways, i just saw a clip of vũ linh đan singing "i will always love you" and let me tell you SHE SLAYED‼️but i didn't see the app you can vote for them (ik it starts in nov)
last but not least, im so excited for "rain has an edge" (the header was soooo cute and pretty) 🌧️🩷🩷
have nice day chị mai 🌼🫶
HAHDHAHAH OMG ANON i actually don’t know the tea w boys planet so pls enlighten me (u voting for them bc they’re viet is so real 🤭🤭 HELPP)
and omg fr that’s exactly why i don’t rlly tune into them BC I ALWAYS FEEL BAD?? like not only is the editing so bad sometimes but i js always end up feeling bad for the ppl who get eliminated 😭😭 ironic cos obv im an enha stan but u get it 🤕
OH MY GODDD I JUST WATCHED IT TOO SHE RLLY DID EAT 😭😭😭 she’s so pretty in that dress too wtf i’m so excited to see her in the show 🥹🥹 oh god this girl better go far or i’ll be so sad 😾
AND STAWPPP thank u so much for tuning in what the heck anon ily 😭💓 i’m glad the header looks okay!! i thought i’d try smth diff from what i usually make 😵💫 anyways i hope u have the best day too em gái 😽😽💖
1 note
·
View note