#otpf
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
BuzzFeed published a report claiming that Tumblr was utilized as a distribution channel for Russian agents to influence American voting habits during the 2016 presidential election in Feb 2018.
Note

(@ kioku) HI I hope you like these flowers!! Bye! (He'd run away in the fastest possible way n faceplant).
(@ jiu) HI PREZ I heard you liked rice!! You look kinda pale and I hope you are ok!!
(HI PARA IK THESE ARE PRETTY LOW QUALITY BUT I WAS THINKING OTPF THE WOE ORANGES BE UPON YE MEME N I THINK CAN WOULD TRY TO APPROACH THEM)


WAAAAH? Flowers?! I love flowers! Thank you so mu-- ah, he's running?!
THANK YOOOU!! THEY'RE BEAUTIFUL AND I PROMISE I'LL HOLD ONTO THEM REALLY TIGHTLY! Dang... I didn't get to ask for his name... Ooh! Yikes. That looked like it hurt. Hold on, I'm on my way!
There is no need to fret over me, though I appreciate both your concern and your gift. Thank you.
(( First Innamorati and now you? How do people keep finding out what I favor...? I must behave more carefully... ))
THANK YOU FOR THIS BY THE WAY ITS SO CUTE AND FUN I ADORE IT. WOE, CAN BE UPON YE!
#jiu: eats plain rice everyday + is seen eating nothing but plain rice + is visibly at ease when eating plain rice#also jiu: HOW did they know i liked rice this is ABSURD#alnst oc: jiu#alnst oc: kioku#speaking: jiu#speaking: kioku#asks
21 notes
·
View notes
Text
COMMUNITY SERVICE , AT THE EDGE OF CLOSING THE CHAPTER
Cato Manor is a settlement about 7 kilometres from Durban's city centre. The area has primary schools, a clinic, a market, and a multi-purpose centre. Cato Manor has faced significant challenges, including struggles over housing and service delivery, which have led to tensions and a high number of assassinations of activists and political figures, high rates of substance use and unemployment. It comprises many black South Africans, with the majority speaking Isizulu and some people from foreign nationals.

Community fieldwork is going to these communities as occupational therapy student to learn and get exposure to their context, issues, and the broader community to get training for practice in community settings. They may learn how to enter the communities, be part of them, assess their context and needs and intervene under the scope of healthcare and occupational therapy. Community practice in occupational therapy book states that practising in a community setting provides occupational therapists/students with a realistic view of the client ‘s life and promotes better treatment outcomes as therapy occurs in a context; it shifts the student from intervening as per the textbook but as per client needs and that of their environment. As part of that training, I am placed in the Cato Manor community, as required by the community module in Ukzn. I want to take a train of thought with this blog, go back and relook at how the community block has been and how my view of occupational therapy practice in the community has influenced my approach to interventions. It will highlight the influence and impact of personal factors and how theoretical information has influenced intervention in this community.
As an occupational therapy student entering the community, my initial understanding of the therapist’s role was limited. I believe it involved learning about clients’ contexts, identifying barriers to occupation, and implementing interventions. However, this perspective was akin to putting cabbage in a water bottle, constrained and incomplete.
According to Brownson (1998), community occupational therapy transcends individual client treatment. It extends to working with systems that impact individual and group abilities to engage in occupations and set goals. This aligns precisely with the Occupational Therapy Practice Framework (OTPF), which emphasises the interconnectedness of individuals within their communities (AOTA, 2008). I only gained a similar understanding while in the community from reading the papers written by grade 9 learners as they shared their challenges; in our attempt to solve these challenges, it was clear that they were rooted in the system of the community, and for intervention, one must start from the system of the community. being almost at the edge of the community block, I have gained a holistic understanding of the role of occupational therapy in fieldwork that effective intervention is when it goes outside of the walls of the clinic or hospital but intervenes with even the social, environmental aspects of the person, treating the community. one may ask how is the community treated? This question is as broad as the role of OT in the community. However, to name just a few that were relevant to Cato Manor Clinic or specify, it through health promotion, promoting health and well-being of the community, teaching and raising awareness to issues that impact or hinder healthcare accessibility and occupations, such as mental health, stigma, and inequality. This was done by programmes run in the community such as Phila Mntwana, maternal mental health, and reproduction health. The viewpoint discussed above is held by occupational therapists today, who understand that participation in occupations and activities at home, school, work, and community supports and maintains health. Developing and putting into practice occupational-based strategies that aim to include and participate a population in occupations that promote community health, occupational therapy actively engages in programs and services to support the health of communities and people (Estrany-Munar et al., 2021).
Reflecting on my time in Cato Manor, I’ve realised how important it is to embrace the full scope of occupational therapy, especially in community settings. Focusing on the whole person and their environment, taking a holistic approach and practising cultural humility is essential. I’ve learned that effective therapy goes beyond just helping individuals; it also involves tackling broader community issues and being mindful of how culture and religion influence interventions. In this community, we relied heavily on the Person-Environment-Occupation (PEO) model, which first examines how people interact with their surroundings and how social factors impact their lives. This model guided my approach and helped me plan specific, relevant, practical interventions. It became clear that effective interventions must address both personal and community challenges.
On a personal level, this experience has strengthened my commitment to fairness and supporting those in need, regardless of their socioeconomic status or cultural background. when working with children in a daycare centre that lacked toys, I had to be sensitive to their circumstances. Instead of bringing in store-bought toys, I focused on interventions that encouraged using materials they could easily access and create themselves. This experience emphasised the importance of cultural sensitivity and resourcefulness in community practice, ensuring that interventions are effective, sustainable, and respectful of the community’s way of life.
Cato Manor is an alive community with a rich cultural diversity, but it also faces significant challenges, such as the stated and a strained healthcare system.
As part of handing over and closing this chapter, the following community students need to immerse themselves in the community’s context and acknowledge the profound influence of culture, religion, socioeconomic factors, and nationality on the lives of the people in this community. The work was rooted in understanding this diversity, and I recommend that the next group take the time to build their awareness and relationships within the community,we relied on the Person-Environment-Occupation (PEO) model to guide our interventions. This model helped us see how the environment and social factors intersect with individual challenges, leading to more effective implementation of interventions. The next group must continue using this model, as it solidifies the understanding of the community’s needs holistically. it' was a lens through which to view the interconnectedness of the people and their surroundings in Cato Manor community.


References
Estrany-Munar, M. F., Talavera-Valverde, M. N., Souto-Gómez, A. I., Márquez-Álvarez, L. J., & Moruno-Miralles, P. (2021). The Effectiveness of Community Occupational Therapy Interventions: A Scoping Review. International Journal of Environmental Research and Public Health, 18(6), 3142. https://doi.org/10.3390/ijerph18063142
Jones, A. B. P. (n.d.). Community Practice in Occupational Therapy: What Is It? In Jones and Bartlett Publishers. http://samples.jbpub.com/9780763760656/60656_ch01_doll.pdf
Brownson, R. C., Fielding, J. E., & Maylahn, C. M. (2009). Evidence-Based Public Health: A Fundamental Concept for Public Health Practice. Annual Review of Public Health, 30(1), 175–201. https://doi.org/10.1146/annurev.publhealth.031308.100134
0 notes
Text
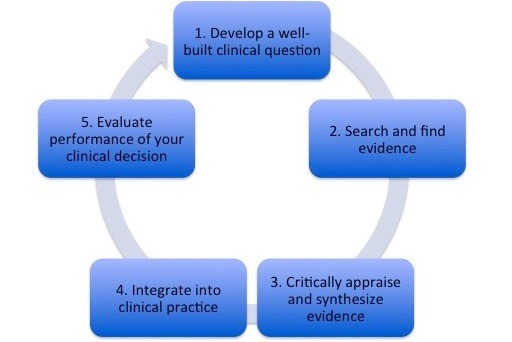
Reflect on evidence-based practice to guide your intervention.
Have you ever questioned yourself about how occupational therapists decide on the appropriate intervention for a patient? This is done by using evidence-based practice, which refers to the integration of research findings into our daily patient care practices and clinical decision-making. This allows us as occupational therapists to apply the results of scientific studies, clinical trials, and other forms of research to guide our intervention decisions and improve patients' ability to engage in areas of occupation independently (Physiopedia, 2024). In this blog, I will be description of the OT process, discussing the importance of evidence-based practice in OT when planning intervention and how I apply it in fieldwork, and what I learned.
According to OTPF, when working with the patient, I use the OT process, which includes evaluating, intervening, and determining the outcome. The first step that I take when I get the patient is to use standardized assessments, clinical observations, and interviews with the patient to gather information about the patient. A thorough assessments and understanding of the patient are only the beginning. I then ask myself the question, which says, How does occupational therapy plan for intervention? This is where evidence-based practice comes into play in my session. I used to find the best and most adequate research to guide my intervention decisions. Then, lastly, look at the outcomes. I measure them using the same method of evaluation, which I determine through a comparison of the patient’s initial evaluation with the patient’s function through the rehabilitation stages.
Evidence-based practice is important in occupational therapy intervention planning as it helps to select interventions that have been demonstrated through research to be effective in achieving desired outcomes for clients. This increases the likelihood of successful treatment and emphasizes interventions that are safe for clients. This promotes client-centeredness and increases the likelihood that interventions will be acceptable and meaningful to clients. (American Psychological Association, 2020). During the fieldwork, I planned the session without researching the TB spine. This was a negative factor, as I was concerned about the client's unstable spine and assumed he needed to sit while wearing a corset for support of the spine. This resulted in planning a dressing activity that was not client-centered, as I didn’t consider the client’s level of creative ability, or functional prognosis. The level of creative ability include looking at the ability to handle the object as he has poor hand function and functional prognosis, including consideration of the time when interventions were provided to the client. So, the consideration of the above was going to help me plan a client-centered session. However, my supervisor provided help with the activity that was provided to the client.
At the university, we are not exposed to most conditions, and it was my first time with a client who had spasms. I struggled with how I would address them during the session. This was a positive factor, as I had been exposed to an unknown condition and had the opportunity to do research to better understand it. This helps me, regarding the planning of the intervention, to include them in the handling principles. During the fieldwork, feedback from a supervisor is crucial, as it helps with how to address them during the session, which was much easier than the handling principles that I provided to the client.
I'm grateful for the learning experience I gained during my fieldwork, and I believe it will enhance my ability to apply evidence-based practice. Throughout the fieldwork, I received valuable feedback from my supervisor, which has been instrumental in refining my clinical skills. My supervisor encouraged the use of activity analysis, which helps in incorporating evidence-based interventions into intervention planning sessions. This has been vital in improving my understanding and experience with evidence-based practice in occupational therapy. Additionally, I've learned the importance of asking questions to deepen my knowledge and address aspects I may have overlooked as a student.
In conclusion, evidence-based practice is super important in occupational therapy. It helps us make the best choices for our patients by using research and our expertise to tailor interventions to their needs. My fieldwork showed me how crucial it is, especially when dealing with new conditions like spasms. Thanks to feedback from my supervisor and my constant learning, I've gotten better at using evidence-based approaches. I'll keep focusing on this in my work because it helps me help my patients reach their goals and be more independent in their everyday lives.
References
Physiopedia. (2024). Evidence Based Practice (EBP). Physiopedia. https://www.physio-pedia.com/Evidence_Based_Practice_(EBP)
American Psychological Association. (2020). Publication manual of the American Psychological Association (7th ed.).
Gillen, G., & Schell, B. A. B. (2019). Introduction to evaluation, intervention, and outcomes for occupations. In B. A. B. Schell & G. Gillen (Eds.), Willard and Spackman’s occupational therapy (13th ed., pp. 710–713). Philadelphia: Wolters Kluwer.
0 notes
Text
Community Chronicles: Embracing Diversity-> Healing Holistically
Walking into the community, a physically, culturally and intellectually different being 5 weeks ago, was daunting. It was daunting because that is the expectation set of the community block. Having previous students always describe community as the hardest block, there is so much fear walking into the community, solely because we are different. When I think about it, we have always been taught our differences separate us, but this block has shown me it doesn’t have to be that way. Our differences teach us that everyone has something to contribute, and that it gives way to use other people’s experiences and lessons to shape life and therapy itself.

As we treat, individually and collectively in our communities, we recognize there is so much more to what falls into the notion of “holistic intervention”. We walk and take the journey with each individual in the community and this way, we are always being exposed to challenges or barriers. This paves the way for us to start thinking further about where to intervene, how to change generational systems while still approaching this with cultural humility, who to speak to and when to advocate. These are notions that we have learnt for the first time away from the prescribed way of treatment in hospitals and clinics we learn through the medical model. As our aim moves to a community-level practice approach, we see the gaps and work our way into not only clinics but schools, community halls, feeding initiatives, the library, businesses and homes. If we use theory to justify this practice, we are implementing intervention through promotive and preventative measures, addressing as many of the challenges before it reaches a point of long-term harm to the community. (Lauckner et al., 2018)

Culturally and contextually appropriate interventions is one of the most important components I’ve learnt to attempt to use in my intervention. Although the fundamentals of occupational therapy are constant as set out in the OTPF and other frameworks, the implementation strategies should always be customized to the community's unique cultural and environmental characteristics. (Taylor, 2004) I have learnt the value of taking into account the socioeconomic, cultural and environmental factors that make way for barriers and strengths. The cultural dynamics of the community also had a significant impact on how people perceived their health or their circumstances. In order to provide client-centered care, with the help of ongoing research, communication with members in the community and help from the community I accepted the challenge of learning, comprehending and adjusting to various cultural ideas and practices as an OT student.
We had also discovered that the success of our time spent on projects is largely dependent on collaboration. Engaging with transdisciplinary teams and other healthcare providers helped develop integrated strategy to address the community needs. Just by communicating, creating relationships and keeping our promises, we were able to access more resources and perspectives to offer increased holistic care and assistance to people and communities. My collaboration with nurses, teachers, stakeholders and community workers added to my mental OT Toolbox as we brainstormed and discussed ideas and challenges. It was through this interprofessional teamwork, I learned the value of group problem-solving and the power of different viewpoints. (Vaughan, 2023)
This aided in an area with huge gaps seen, sustainability. As a student in the last block, I have seen a variety of short-term projects that sought to solve urgent problems but had little lasting effect. We have had to come up with more sustainable solutions and adaptations to ensure carryover and continuity after the block. Training local community members on OT relevant knowledge enhances the success and long-term effect as these principles will be ongoing, as we ran training amongst staff at schools on red flags in children and a programme to match this as well as the NPO Denis Hurley Centre on psychodynamics and education on our profession. (Rivera, 2023) In addition, equipping individuals who experience occupational marginalization through skill-building workshops and advocacy initiatives can help cultivate a sense of initiative and inclusion within the community, as we attempt to focus on strengths in the youth development programme and advocate for easier access to contraception for teenage girls. (Sayers, 2023)
A part of what contributes to this sustainability however, is involving the relevant parties who agree and are willing to take the initiative and be a part of the drive and call for action in the community.
In addition to some of the professional insights gained, my experience in the community has had a profound impact on my personal growth. It taught me resilience and adaptability as I confronted challenging and unfamiliar circumstances while overcoming the lack of resources, cultural differences, and language barriers which required me to step out of my comfort zone, brushing up on my isiZulu and communication skills.

Working in the community also highlighted the urgency of social justice and equitable healthcare. Witnessing the levels of poverty boosted my awareness of my role as an advocate for marginalized populations. This experience instilled within me a sense of social responsibility, fueling my passion for taking action in community development.
Looking ahead to my community service year, these lessons have direct implications for the way forward. Continuing to prioritize cultural competence and adapt my practice to the unique needs and perspectives of the community as I seek opportunities to engage with local traditions, beliefs, and customs to ensure a culturally sensitive approach to therapy. I will aim to continue to build strong working relationships with members of the MDT and TDT to provide comprehensive, client-centered and community-centered care. By actively engaging in lifelong learning and fostering a culture of shared learning, I can contribute to a more integrated healthcare system that maximizes the potential impact of therapy.

I aim to continue to explore proactive initiatives, innovative techniques and equipment that can be adapted in rural settings to address the challenges of limited resources. This could include community-based interventions and collaboration with local organizations and stakeholders to leverage resources and maximize impact and carryover. Advocacy for improved healthcare infrastructure for accessibility and increased funding for rural healthcare must also remain a priority for OTs. Through these interventions, communications and initiatives, the aim is to drive the change to start addressing as many areas of the social determinants of health in a sustainable way.

In retrospect, my initial apprehension about the community block seems like a distant memory now. I discovered that our differences were not barriers but bridges to understanding. As we immersed ourselves in the community, we realized that the concept of "holistic intervention" goes far beyond what we initially understood. We were forced to expand our critical thinking and approach, learning to advocate, adapt, and apply theory to practice in innovative ways. Our aim shifted towards addressing challenges at their root, preventing long-term harm to the community.
In the end, the community block has not only broadened our horizons but also deepened our commitment to holistic care. We now understand that it's not enough to treat individuals in isolation; we must consider the entire community as a client, nurturing its well-being from every angle. Through cultural humility and a collective effort, we're not just changing lives but also transforming generational systems. This block has not only challenged us but has also equipped us to make a real impact on the communities we serve. Our journey continues, and as we move forward, we carry with us the valuable lessons learned in these five weeks, lessons and conversations that will shape our practice for years to come.

References:
Barker, L. N., & Ziino, C. (2010). Community rehabilitation: “home versus centre” guidelines for choosing the optimal treatment location. International Journal of Rehabilitation Research, 33(2), 115–123. https://doi.org/10.1097/mrr.0b013e32832e6c73
Lauckner, H., Leclair, L., & Yamamoto, C. (2018). Moving beyond the individual: Occupational therapists’ multi-layered work with communities - Heidi Lauckner, Leanne Leclair, Cynthia Yamamoto, 2019. British Journal of Occupational Therapy. https://journals.sagepub.com/doi/abs/10.1177/0308022618797249
McGrath, J. R., Marks, J., & Davis, A. (2023). Towards interdisciplinary rehabilitation: further developments at Rivermead Rehabilitation Centre - Joanna R McGrath, Julie A Marks, Alison M Davis, 1995. Clinical Rehabilitation. https://journals.sagepub.com/doi/10.1177/026921559500900407
Rivera, J. (2023). A Scoping Review of Interventions Delivered by Occupational Therapists in School Settings. Journal of Occupational Therapy, Schools, & Early Intervention. https://doi.org/10.1080//19411243.2023.2232806
Sayers, B. (2023). Collaboration in School Settings: A Critical Appraisal of the Topic. Journal of Occupational Therapy, Schools, & Early Intervention. https://www.tandfonline.com/doi/full/10.1080/19411240802384318
Taylor, R. R. (2004). Chronic fatigue syndrome: traditional and community-based approaches to rehabilitation. Health & Social Care in the Community, 12(3), 171–185. https://doi.org/10.1111/j.1365-2524.2004.00485.x
Vaughan, E. M. (2023). The Rationale and Logistics for Incorporating Community Health Workers Into the Multidisciplinary Team - Elizabeth M. Vaughan, Aliye B. Cepni, Uyen Phuong N. Le, Craig A. Johnston, 2023. American Journal of Lifestyle Medicine. https://journals.sagepub.com/doi/10.1177/15598276231151866
0 notes
Text
Theory Vs Practice
Theory vs Practice
To understand this, interlink between theory and practice, we must first understand the theoretical part of it.
The OT process.
According to the OTPF 4 The OT process is a process taken by occupational therapists when offering services to a patient, it is the evaluation, intervention, and outcome. This is a client-centred mode of delivering OT services that ensures that the intervention practitioners give is guided by the assessment findings from the evaluation, and of course, we later must measure the outcome of our intervention, so we can reflect on the treatment if it is helping us towards our goals and the patient’s own goals. The OTPF puts its beautifully when it goes on to say that this process occurs in the purview of the OT domain, which is our client factors, context, performance skills, performance patterns and occupations. These domains go on and simplify this process by outlining to us, what do we need to do, what needs to be our focus, and what is our goals. To take for an example a mother after sustaining an Upper limb fracture a mother (which is her role, performance patterns) may not be able to take care of child, in terms of washing for him (occupation). So, then it becomes a point of interest for OT practitioners as to how do they intervene and what do we do to enable this patient to be able to carry out her roles and occupation.
Function and performance in occupations is our end goal but we do not only work on these but look at all the barriers that are opposing participation in activities, we also look at the context, how the environment poses as a barrier to participation, and with our priority being mostly function and independence our reasoning guides us to look at the client holistically, because it is not beneficial if we are going to improve the patient's wheelchair use skill, without focussing at the 3 steps at the entrance blocking access to the house, are we going to discharge the patient just to have them lie in bed the entire day, so it then becomes important that we look at all the factors that are into play, as outlined by the OPTF as our domains.
But now that theory (although not all) but how is it implemented into practice.
My lecturers had this saying, ‘Sometimes no matter how hard you plan, life will always happen’ and no matter how prepared one is with the theory it does not mean everything will be a success in practice. Especially in an acute hospital setting with very high patient turnover. In the days of fieldwork, I had faced predominantly people with CVA, it is a very common disorder in the South African context but with varying symptoms, the most challenging have been those with communication disorder because with those patients assessment will be lacking, due to them not being able to provide more information about the context and environment.
But also the challenge of trying to jumble assessing and treating, to formulate a suitable treatment plan, you first need thorough assessment and I never seemed to be able to do both, because whenever I choose to do comprehensive evaluations I’d take the entire time I have with that patient, and before you know it the patient will be discharged, because they are now medically stable. Obviously, in those situations I have had to prioritize treatment, I am thinking of the patient I received in a half day and had to start my assessments, the patient according to my findings does not have any bed mobility, but I later was informed that the patient was going to be discharged. So, then my OT process which was going to follow a pattern was disturbed at this point I had not done thorough assessments but had to move on to treatment. In consideration of the little time and as I had the patients family at the ward, I rushed to do caregiver training because as much as I wanted to fight a system that is unintentionally promoting secondary complications in discharging a Gogo who still needs thorough OT intervention, I still had to respect they bonding time as a family as this was during visiting hours, so I rushed to show the caregiver without informing my supervisor of the sudden changes, and when I went back to my supervisor and told them they comment was I should do caregiver training and contact the OTs for assistance with writing a referral.
My first week has been navigating this crisis of having a patient and then the next day not having one, I have reflected on this with the OTs as they are more used to this, and they say their strategy has always been to assess and treat at the same time, which means treat as the problems arise. Quite efficient right, but how with a third-year level and countable treatment experience.
Do things get better from here?
What else can I do to be more efficient?
Is there something I am not considering, what do you guys think?
And of course, I need to rely more on my supervisor, because had I called them and made them part of this caregiver training session I could have given the patient a better package to take home and allowed the supervisor to correct and add my thoughts because at that moment the patient was priority.
0 notes
Text
“To not have your suffering recognized, is an almost unbearable form of violence", Androl Lanitov

Psychologically, we all have something going on. It is either all of us are undergoing, pain or hardship if not it is either you have been here, or you are going to be here. According to the DSMV TR, this starts to be a problem when it affects one's occupations and roles. The 4th OTPF defines occupations as everyday personalized activities that people do as individuals, families, and communities to occupy time as it brings meaning or purpose to life, or they are supposed to do it.
There are a lot of things that affect our occupational engagement such as life-changing events that lead to physical impairment or psychological impairment. In our blog today we are going to discuss mental health that have been neglected so much in our societies or the last thing we address or notice just like Cinderella in the ”Prince Charming” stories. According to WHO (2021), they are largely unrecognized and untreated because mental health conditions are particularly vulnerable to social exclusion, discrimination, stigma, educational difficulties, risk-taking behaviors, physical ill-health, and human rights violations. These are mostly induced by our cultural norms and lack of knowledge of what mental illness is.
Having not heard of mental health presentations in my life until I was exposed to the course that deals with mental health had a negative impact on how I viewed mental illness. You can visit my previous blog on my journey battling with mental illness at https://www.tumblr.com/mzeken/726054270181457920/i-may-not-be-there-yet-but-im-closer-than-i-was?source=share. But now I can proudly say I am equipped when it comes to mental illnesses and interventions. With fewer people understanding what mental illness can be, does impacts how people seek mental illness intervention and when. When I look back and reflect on what some of my family members have been going through, I see the need for health intervention. But because there was none too little exposure to mental illness, awareness, or campaigns from the health department they didn’t understand what they were going through and that even if you are suffering from depression and substance abuse, your life can still be meaningful again.
With more articles being published on mental health, especially in South Africa, we see that in the ancient days, it was totally neglected but now, according to the Policy Framework and Strategic Plan 2013-2023, they plan to further transform mental health services and ensuring that quality mental health services are accessible for everyone, equitable, comprehensive and are integrated at all levels of the health system. This is done by paying a huge amount of money to Mental Health which used to be the last thing on the health budget, given that it has been producing high death rates not only in SA but the whole world. Developing monthly awareness of mental health conditions, giving out posters, and being active on social media about these campaigns is how they are trying to reach out to everyone. Living in South Africa where public health is prioritized, we can count ourselves as privileged.
If you know a friend or see anyone suffering from mental health conditions you can suggest some of these sites to them SADAG online, Adcock Ingram Depression & Anxiety Helpine, and https://www.youtube.com/watch?v=qLS8wVJP9i8 on YouTube. Sharing information anytime is important, they might not need it now but in the future, they might recall your name. I know what it feels like to be drowning underwater and having to suffer in silence. With 14.3% of deaths worldwide, or approximately 8 million deaths each year, we cannot do everything alone, but together we can help save lives.
(592 Words)
Link to the DSMV: the American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th edition. Arlington, VA., American Psychiatric Association, 2013

0 notes
Text
Ontario Teachers getting rich off lockdowns, China's genocidal slave state, and the Great Reset.
Ontario Teachers getting rich off lockdowns, China’s genocidal slave state, and the Great Reset.
. The Ontario Teachers Pension Fund (OTPF) is one of the largest investment funds in the world with 221.2 Billion in assets, all of originating from the Ontario taxpayer paying their 60-100k a year salaries for teaching your kids how 2+2=4 is racist. This is up from the 191.1 Billion Dollars reported in 2018. The financial success isn’t surprising given the focus of investment for Ontario’s self…

View On WordPress
#Ontario School closure#Ontario Teachers#Ontario Teachers Covid19#Ontario Teachers Great Reset#Ontario Teachers Pension Plan#Ontario teachers Union#OTPF
0 notes
Text
you may think that i’m over my Lotor hype but you’d be sadly mistaken.
70 notes
·
View notes
Video
instagram
activities that are “fundamental to living in a social world, they enable basic survival and well-being.” #OTPF • as an OT— i would argue every day is for self-care! BUT typically we just have more time to dedicate to ourselves on Sundays. • So I challenge you this Sunday to choose just 2 things to participate in that enable your well-being in this social world of ours! • happy Sunday from @lifesoccupations ! • check @jaymieraefta and her amazing illustrations. (i’m a fan 🙋🏼♀️) (at Sunday Funday Colorado)
0 notes
Text
How I’m Preparing for the NBCOT as a 1st Year OT Student
The National Board for Certification (NBCOT) Exam, is the exam that OT students take in the U.S. after completing an accredited OT program. Passing this exam allows you to apply for your state license.
From my understanding, OT students generally study for 4-6 weeks for the exam after graduating because this exam covers everything you should have learned in OT school. In order to save myself the frustration of thumbing through old notes, I’m taking the time to organize my notes as I move through each quarter of OT school.
So, without further ado, here’s a bulleted summary of the steps I’m taking to prepare for the NBCOT as a 1st year OT student:
I made a chart in a word doc that has the most recent exam outline (https://www.nbcot.org/en/Students/Study-Tools/Exam-Outline). I have a column for the content covered within each domain/task. And another column where I write in which courses I’ve taken thus far that are applicable to the content covered in the domain/task. For certain courses I put in parentheses containing information that would give me more specifics on the notes/topic/week we covered relevant material.
I also regularly make summary sheets of the information I’m learning. For example, for the Theory course I’m currently taking, for each new model we learn, I make a 1-page infographic that contains all the information I need to know. Another example is for my Conditions course, for each condition we cover, I make a summary table that includes: condition description, signs/symptoms, etiology, effected performance skills (as per the OTPF 3rd edition), and affected body structures and functions (as per the OTPF 3rd edition). The conditions summary sheets I make are guided by the learning objects of the course which requires us to link concepts from the OTPF to facts we learn about each condition. I keep a copy of each study sheet I make in a separate computer file (labeled NBCOT) so that I have everything organized when it comes time to study for the NBCOT. I also feel that these sheets will be helpful when reviewing key information before fieldwork placements.
A general principle that I have as of right now is to try to absorb everything and make connections to my experiences and observation hours to make the information stick.
Another general principle of mine is to take good notes that I will be able to refer back to. The key point here is that if I consistently do the work now, do it well, and keep my work organized, it will pay off in the future by saving me time that could be used actively studying.
#ot#otd#ots#occupational therapy#occupational therapy school#occupational therapy student#ot school#ot student#NBCOT#study#prep#preparation#summary sheet#summary page#studyblr#gradblr#grad student#grad school#graduate student#graduate school#exam#NBCOT exam#studying#preparing
1 note
·
View note
Text
Occupational Therapy eBooks for sale
40 pesos for each EBOOK ( SOFT COPY ), unless otherwise stated
Link of the file will be sent to your email (kindly message me) when payment has been received & verified
▪️▫️▪️▫️▪️▫️▪️▫️▪️▫️▪️▫️▪️▫️▪️▫️▪️▫️
OT eBOOK TITLES:
Addy's Occupational Therapy Evidence in Practice for Physical Rehabilitation
Atehison's Conditions in Occupational Therapy 2011
Blunden's Occupational Therapy for Child and Adolescent Mental Health
Bobath's Adult Hemiplegia - Evaluation and Treatment, 3e, 1990
Bundy's A guide to sports and injury management
Carr and Shepherd's Stroke Rehabilitation - Guideline for exercise and training to optimize motor skill, 2003
Case-Smith and O'Brien's Occupational Therapy for Children & Adolescents, (SELECTED CHAPTERS ONLY), 7E, 2015
(5 php per chapter)
Case-Smith's CH 7 - Motor Control or Motor Learning Case-Smith's CH 8 - Hand Function Eval and Intervention
Case-Smith's CH 14 - Feeding Intervention
Case-Smith's CH 15 - ADL and Sleep
Case-Smith's CH 16 - IADL, Driving, Community Participation
Case-Smith's CH 25 - Transition to Adulthood
Case-Smith's CH 28 - Neuromotor - Cerebral Palsy
Case-Smith's CH 29 - Pediatric Hand Therapy
Case-Smith and O'Brien's Occupational Therapy for Children, 6E, 2010
Chandler's Movement Assessment of Infants, 1980
Christiansen & Baum's Performance, Participation and Well-Being, 2005
Clutton's Occupational Therapy in Housing building on firm foundations, 2006
Cooper's Occupational Therapy in Oncology and Palliative Care, 2e, 2006
Coppard and Lohman's Introduction to Splinting A Clinical Reasoning and Problem-Solving Approach, 2008
Cox' Occupational Therapy and Chronic Fatigue Syndrome, 2000
Creek's Core Concepts of Occupational Therapy, The
Crouch's Occupational Therapy in Psychiatry and Mental Health, 5E, 2014
Davidson's Cognitive Behavioural Interventions in Physiotherapy and Occupational Therapy
Dawson's Smart but Scattered, 2009
Dehn's Essential Clinical Procedures, 3E
Delaney's 101 Games and Activities for Children with Autism, Asperger's, Sensory Processing Disor…
Deusen's Assessment in Occupational Therapy and Physical Therapy
Donaghy's Cognitive Behavioural Interventions in Physiotherapy and Occupational Therapy
Donatell's Sports Specific Rehabilitation
Dunn's Bringing Evidence into Daily Practice
Dziedzics's Rheumatology - Evidence-Based Practice for Physiotherapists and Occupational Therapists, 2010
Edman and Preston's Occupational Therapy and Neurological Conditions, 2016
Edman's Occupational Therapy and Stroke, 2010
Enderby's Therapy outcome measures for Rehabilitation Professionals Speech and Language Therapy, Physiotherapy, Occupational Therapy, Rehabilitation Nursing, 2e
Fawcett's Principles of Assessment and Outcome Measurement for Occupational Therapists and Physiotherapists Theory, Skills and Application
Grieve's Neuropsychology for Occupational Therapists - Cognition in Occupational Performance
Henderson's Hand Function in the Child
Hong's Occupational Therapy in Childhood, 2002
Kielhofner's Conceptual Foundations of Occupational Therapy Practice, 4e, 2009
Kielhofner's Research in Occupational Therapy - Methods of Inquiry for Enhancing Practice
Levy's Occupational and Environmental Health Recognizing and Preventing Disease and Injury, 6e, 2011
Lorenzo's Practice and Service Learning in Occupational Therapy, 2006
MacRae’s Psychosocial OT, 3rd Ed
Machover’s Draw A Person Test (DAPT - Interpretation)
McIntyre's Occupational Therapy and Older People, 2005
Miltenberger's Behavioral Management Technique, 5e, 2012
Mooney's Occupational Therapy in Orthopaedics and Trauma
Neenan, Dryden's Cognitive Behaviour Therapy_100 Key Points and Techniques (2014)
Kielhofner's Research in Occupational Therapy - Methods of Inquiry for Enhancing Practice, 2006
OTPF 1 (2002)
OTPF 2 (2008)
OTPF 3 - OT Practice Framework- Domain & Process 3rd Edition
Pellerito & Miller's Preparing for the Occupational Therapy National Board Exam
Pedretti's Occupational Therapy - McHugh Pendleton, Heidi
Raines' Bobath Concept (theory and clinical practice in neurological rehabilitation)
Raphael-Grimm's Art of Communication in Nursing and Health Care, The
Ritsner's Handbook of Schizophrenia Spectrum Disorders, Volume III, 2011
Rodger's Occupation Centred Practice with Children - A Practical Guide for Occupational Therapists, 2010
Rodger's Occupational Therapy With Children, 2006
Roy's The Rehabilitation Specialist's Handbook, 4E
Sames' Documenting Occupational Therapy Practice, 3e, 2015
Stone's Occupational Therapy and Duchenne Muscular Dystrophy, 2007
Taylor's The Intentional Relationship Occupational Therapy and the Use of Self
Trombly's Occupational Therapy
Uniform Terminology for OT, 3e
Willard and Spackman’s Occupational Therapy, 11E
Wilson's Occupational Therapy for Children with Special Needs, 1998
Wright's Occupational Therapy and Life Course Development, 2009
▪️▫️▪️▫️▪️▫️▪️▫️▪️▫️▪️▫️▪️▫️▪️▫️▪️▫️
CLICK HERE to see the masterlist of all eBooks/notes for sale: https://docs.google.com/document/d/1RD_Qd6E6mvimb8bzr_sS5wazPYowpP9O38h55YQfuJI/edit?usp=sharing
**** Price is negotiable is your buying more than 2 e-books****
DESCRIPTION IN GENERAL:
May contain highlights/notes
File is 100% working
can be in the form of .PDF or .EPUB
Don’t hesitate to ask me if you have any questions or should you want any sample pictures of its content :)
PAY ME THRU
GCash (7/11 kiosk)
Load transfer
Paymaya (7/11 qr code will be sent for you to pay the cashier)
Exact amount on meetup
For shipping, thru:
LBC
Lalamove
Grab
++ shipping fee (to be shouldered by the buyer)
If meet up
dala ka USB to copy the file
i’ll send you the location once confirmed buyer ka na (UST Area, along España)
Should there be any problem in downloading the file, kindly message me and I will resolve it as soon as possible. Thank you:)
CONTACT ME here or at [email protected]
#occupationaltherapyebooks#occupationaltherapybooks#OTebooks#OTbooks#occupationaltherapyfiles#occupationaltherapyPDF
1 note
·
View note
Text
Evidence-based practice to guide your intervention:
Have you ever questioned yourself about how occupational therapists decide on the appropriate intervention for a client? This is done by using evidence-based practice, which is defined as the integration of the evidence from clinical research with clinical expertise and the client’s preferences to guide intervention decisions with the goal of improving the client's outcomes (American Occupational Therapy Association, 2020). The blog will outline the reflection on how the student therapist used evidence-based practice when planning interventions for clients.
The occupational therapist gets the client, do their assessments, and plans intervention by following these stages: referral, which is the first step, where the client is referred to the occupational therapist due to some limitations. The following stages are screening, assessment, and intervention planning. In these three stages, the occupational therapist conducts the initial interview, gets all the information that will be needed from the client, do all the assessments holistically using standardized and non-standardized assessment forms, and then plans the intervention sessions by integrating the evidence from the OTPF with the findings of the client. The most important part is assisting patients to regain their independence by engaging them in meaningful activities and also by doing adaptations at home, such as putting rails in the bathroom to promote independence in toileting and bathing and ramps to allow the client to enter the home entrance independently. All of this is done using evidence-based practice. The occupational therapist needs to find the best available evidence to guide intervention decisions.
The occupational therapy interventions are based on research and are adapted to align with each patient's skills, condition, activity demands, needs, and interests. The occupational therapist uses research literature to find all the studies that are relevant to the intervention of the client and evaluate the evidence gotten. Things that need to be considered in these studies are study design, sample size, and the statistical analysis used in the research. The occupational therapist needs to do an assessment to allow holistic intervention, also evidence-based practice is not only about following research only but the things like culture, social context, beliefs, and values. The occupational therapist, after integrating the evidence with clinical expertise, then makes intervention decisions that are client-centered. Meaning there must be cooperation between an occupational therapist and the client to help clients participate in meaningful, satisfying, and health-promoting occupations by involving the patient in making decisions during the therapeutic intervention planning, Hunter (2021). An occupational therapist uses a combination of interventions, such as therapeutic exercises, adaptive equipment, and environmental modifications.
According to Melnyk (2022), the use of evidence-based practice has become increasingly important in the field of occupational therapy, and it is critical that you begin considering the evidence as you provide your interventions to the clients. Evidence-based practice ensures that your treatment techniques are effective. Analyzing the best research ensures that the treatments that you use with your patients actually work. In occupational therapy, it is your duty to continue to evaluate the outcomes of your intervention by doing thorough research and clinical observations to make sure that it is effective for the client. It is also important to make any necessary adaptations to ensure that the client is getting the best intervention and care.
Evidence-based practice is very important to me as a student occupational therapist, as it will enrich my knowledge and experience on how to plan successful interventions for my clients. In the fieldwork for finals, the supervisor gave me two patients to work with. My first client was diagnosed with a right CVA. I started by doing an interview with him. I was asking relevant questions in order to do the research and plan the intervention. I did all my assessments, and I asked him about the occupations that he finds limitations in when performing them, and he mentioned that he wants to learn to dress independently since it took him a long time to do the dressing of the lower limb. I think the activity I chose for the client was relevant and client-centered; he was going to dress the lower limb without back support and was expected to reach for the clothes in a standing position. The aims were to improve trunk control as well as standing balance.
In my fieldwork practicals, I have found that evidence-based practice has been essential to my personal growth as a student therapist, and I need to continue to consider it every time to make sure that my treatment activities are effective for the client. From the feedback I get from my supervisor, I think it will help me plan effective treatments. In terms of evidence-based practice, I learned that it is important to know everything about the client and integrate it with the evidence from clinical research to guide intervention decisions with the goal of improving the client's outcomes.
I am happy with the learning experience I got from fieldwork, and I think it will help me improve in terms of using evidence-based practice. During the fieldwork practicals, I received valuable feedback from my supervisor that has helped me improve my clinical skills and approaches. The supervisor always wants us to think critically about the evidence and integrate it with our own clinical expertise. This will help me improve my experience and understand the use of evidence-based practice in occupational therapy. I also learned to ask questions in order to learn more and grow as an occupational therapist.
In conclusion, evidence-based practice allows you to help your patients make informed choices for their occupational therapy programs. Also, it gives you confidence and allows you, as an occupational therapist, to easily answer the questions that clients have about your interventions. It is important to not focus only on research; you also need to integrate the evidence with clinical expertise, culture, and roles to create an effective intervention. From now on, I will make sure that I use evidence-based practice whenever I meet with the client in order to achieve their goals.
References
American Occupational Therapy Association (AOTA): https://www.aota.org/
Hunter. (2021). Critiquing the Canadian model of client-centered enablement (CMCE) for indigenous contexts. Canadian Journal of Occupational Therapy.
https://guides.lib.uw.edu//hsl/ebprehab
Melnyk, B. (2022). Evidence-based practice in nursing & healthcare: A guide to best practice. Lippincott Williams & Wilkins.
0 notes
Text
Theory vs Practice
To understand this, interlink between theory and practice, we must first understand the theoretical part of it.
The OT process.
According to the OTPF 4 The OT process is a process taken by occupational therapists when offering services to a patient, it is the evaluation, intervention, and outcome. This is a client-centred mode of delivering OT services that ensures that the intervention practitioners give is guided by the assessment findings from the evaluation, and of course, we later must measure the outcome of our intervention, so we can reflect on the treatment if it is helping us towards our goals and the patient’s own goals. The OTPF puts its beauty when it goes on to say that this process occurs in the purview of the OT domain, which is our client factors, context, performance skills, performance patterns and occupations. These domains go on and simplify this process by outlining to us, what we need to do, what needs to be our focus, and what are our goals. To take for example mother after sustaining an Upper limb fracture a mother (which is her role, performance patterns) may not be able to take care of the child, in terms of washing for him (occupation). So, then it becomes a point of interest for OT practitioners as to how they intervene and what we do to enable this patient to be able to carry out her roles and occupation.
Function and performance in occupations is our end goal but we do not only work on these but look at all the barriers that are opposing participation in activities, we also look at the context, how is the environment posing as a barrier to participation, and with our priority being mostly function and independence our reasoning guides us to look at the client holistically because it is not beneficial if we are going to improve the patient's wheelchair use skill, without focussing at the 3 steps at the entrance blocking access to the house, are we going to discharge the patient just to have them lie in bed the entire day, so it then becomes important that we look at all the factors that are into play, as outlined by the OPTF as our domains.
But now that theory (although not all) but how is it implemented into practice.
My lecturers had this saying, ‘Sometimes no matter how hard you plan, life will always happen’ and no matter how prepared one is with the theory it does not mean everything will be a success in practice. Especially in an acute hospital setting with very high patient turnover. In the days of fieldwork, I have had I have faced predominantly people with CVA, it is a very common disorder in the South African context but with varying symptoms, the most challenging has been those with communication disorder because with those patients that assessment will be lacking, due to them not being able to provide more information about the context and environment.
But also the challenge of trying to jumble assessing and treating, to formulate a good treatment plan, you first need thorough assessment and I never seemed to be able to do both, because whenever I choose to do thorough assessments I’d take the entire time I have with that patient, and before you know it the patient will be discharged, because they are now medically stable. So obviously in those situations I have had to prioritize treatment, I am thinking to the patient I received in a half day and had to start my assessments, the patient according to my findings does not have any bed mobility, but I later was informed that the patient was going to be discharged. So, then my OT process which was going to follow a pattern was disturbed at this point I had not done thorough assessments but had to move on to treatment. In consideration of the little time and as I had the patients family at the ward I rushed to do caregiver training because in as much as I wanted to fight a system that is unintentionally promoting secondary complications in discharging a Gogo who still needs thorough OT intervention I still had to respect they bonding time as family as this was during visiting hours, so I rushed to show the caregiver without informing my supervisor of the sudden changes, and when I went back to my supervisor and told them they comment was I should do care giver training and contact the OTs for assistance with writing a referral.
My first week has been navigating this crisis of having a patient and then the next day not having one, I have reflected this with the OTs as they are more used to this, and they say they strategy has always been to assess and treat at the same time, which means treat as the problems arise. Quite efficient right, but how with a third-year level and countable treatment experience.
Do things get better from here?
What else can I do to be more efficient?
Is there something I am not considering, what do you guys think?
And of course, I need to rely more on my supervisor, because had I called them and made them part of this caregiver training session I could have given the patient a better package to take home and allowed the supervisor to correct and add my thoughts because at that moment the patient was priority.
1 note
·
View note
Text
“I may not be there yet, but I’m closer than I was yesterday” Jose N. Harris.

Image from Google (meme generator)
What once seemed impossible, and not for me, feels more tangible and right in front of my eyes these days. Me becoming an Occupational Therapist. This is a journey for me, and I am feeling every step of the way. Steve Maraboli once said the road to success is always under construction. Fasten your seat belt as I take you through my journey up until this far. I have always wanted to be something in the Health and Sciences profession, but I couldn’t figure out what until I overheard the title of OT.
In every classroom either in primary or high school there will always be a high-flyer. I overheard one from my matric class stating that she will be an OT if not a medical doctor. The title of being an OT fascinated me as I have never heard of such before and never knew that it existed in my town hospital, Ingwavuma Mosvold Hospital. I did not only end up applying for OT via CAO but getting to meet an interesting local OT. She explained to me what occupational therapy is and the areas under occupational therapy (geriatrics, pediatrics, psychiatry, general physical conditions, and medico-legal. Occupational therapy is defined in the OTPF as the therapeutic use of everyday life occupations with persons, and groups for the purpose of enhancing or enabling participation. I never knew what OT is until my first year. I knew the definition but didn’t understand the concept nor was I able to describe it to others and it all started making sense in my second year (https://carrieschmittotd.com/wp-content/uploads/2021/04/AOTA-Occupational-Therapy-Practice-Framwork-OTPF-4th-edition.pdf.).
I did my first year in 2020, and there was the outbreak of covid which resulted in no longer having contact classes on campus but moving back home and adjusting to online learning. This was a hard time for me given the area I am from (connectivity issues, electricity problems. Basically, deep rural areas). With being unable to attend and do my work I ended up not passing all my modules as I was also not submitting on time. I got depressed as had my goals that after 4 years this degree must be put in motion and helping others. I did not even know about sites like SADAG (https://www.sadag.org/. ) that could have helped me cope with depression. Having to swallow the pill that my friends passed did not cause more only heartache but also negatively affected my self-esteem. If I knew what Occupational Therapists are capable of, I would have also seen one for myself for anxiety management and time management sessions. Sometimes I do get very anxious and depressed I use the skills that I was taught during lectures and have been sharing with others not only my patients on practicals but also family.
Time went by and did my second year, 2022 as during 2021 I was redoing the module I failed. Started going on practice putting the theory into practice. With the lecturer, helping friends, supervisors, and sites like OT rex on YouTube (at https://www.youtube.com/@OTRex) helped me understand what our focus as Ots is and how we also use activities as assessment tools and interventions. It made me realize that what is normal in me, my family, my culture, or my community may not be normal for others. This emphasized the importance of being open-minded, respectful, sympathetic with others, non-judgemental, and patient.
This journey has been a roller coaster for me. It does happen that you put in effort on your work and marks don’t reflect that, you are reminded of your failures. Then this calls one to go back to their drawing board and strategies. It is when you keep on pushing. We are no longer driven by the clock but the passion. Looking at the differences we can make in other people’s lives, we must keep on keeping on. Khalid once said, “You can do anything if you put your mind to it” Eastside. This time around I feel like I am closer to being a certified Occupational Therapist with no student at the end compared to 2020. I am standing on the edge. For more information on what occupational therapists do please visit this page: (https://www.aota.org/-/media/corporate/files/advocacy/state/resources/practiceact/ot-definition-for-aota-model-practice-act.pdf. )
{Total Number of words: 696}
0 notes
Photo

One.. two… THREE! 🐾 I love jumping on the bed & posed for momma 😻 #tuxncinnybrown #cinnybrown #tuxncinnamon (at Newnan, Georgia) https://www.instagram.com/p/CZKZD3-OTpF/?igshid=NGJjMDIxMWI=
0 notes
Text
god I fucking love Lotor and his lady Galra generals
21 notes
·
View notes