
A collection of humor, study resources, news, and stories in the medical field.
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by cranial-rectosis and here's what we found interesting.
Average Info
Notes Per Post
23K
Likes Per Post
14K
Reblog Per Post
10K
Reply Per Post
9
Time Between Posts
2 months
Number of Posts By Type
Photo
8
Text
5
Link
3
Conversation
1
Last Seen Tumblr Blogs





Fun Fact
In Q3 of 2020, 31% of US users access the Tumblr app daily.
Photo


1. Scalp:
5 layers S - the Skin on head from which head hair grows
C - Connective tissue. A dense subcutaneous layer of fat and fibrous tissue that lies beneath the skin, containing the nerves and vessels of the scalp. A - The Aponeurosis called epicranial aponeurosis (Galea Aponeurotica). It is a tough layer of dense fibrous tissue which runs from the frontalis muscle anteriorly to the occipitals posteriorly. L - The loose areolar connective tissue. In scalping the scalp is torn off through this layer. It also provides a plane of access in craniofacial surgery and neurosurgery. This layer is sometimes referred to as the “danger zone” because of the ease by which infectious agents can spread through it to emissary veins which then drain into the cranium. P - The pericranium is the periosteum of the skull bones and provides nutrition to the bone and the capacity for repair. It may be lifted from the bone to allow removal of bone windows
2. Skull: It supports the structures of the face and provides a protective cavity for the brain. The skull is composed of 2 parts:
- the cranium - the mandible
The human skull is generally considered to consist of 22 bones—8 cranial bones and 14 facial skeleton bones. In the neurocranium these are the occipital bone, 2 temporal bones, 2 parietal bones, the sphenoid, ethmoid and frontal bones.
The bones of the facial skeleton are the vomer, 2 nasal conchae, 2 nasal bones, 2 maxilla, the mandible, 2 palatine bones, 2 zygomatic bones, and 2 lacrimal bones. Some sources count a paired bone as one, or the maxilla as having two bones (as its parts); some sources include the hyoid bone or the three ossicles of the middle ear but the overall general consensus of the number of bones in the human skull is the stated twenty-two. 3. Dura mater:
Thick membrane that is the outermost of the three layers of the meninges. The dura surrounds the brain and the spinal cord and is responsible for keeping in the cerebrospinal fluid. 4. Arachnoid 2nd layer of the meninges 5. Pia mater
3rd layer of meninges
6. Subarachnoid space
Space between arachnoid mater and pia mater It is occupied by spongy tissue consisting of trabecular (delicate connective tissue filaments that extend from the arachnoid mater and blend into the pia mater) and intercommunicating channels in which the cerebrospinal fluid (CSF) is contained. 7. Cerebral cortex
The Cerebral Cortex is made up of tightly packed neurons and is the wrinkly, outermost layer that surrounds the brain. It is also responsible for higher thought processes including speech and decision making . The cortex is divided into four different lobes, the frontal, parietal, temporal, and occipital, which are each responsible for processing different types of sensory information.
3K notes
·
View notes

Text
Unfeeling
It wasn’t all that long ago when an ambulance pulled into the bay with a code in progress. The patient was apneic and in asystole on the scene but EMS personnel were providing full life support measures. This scenario is really rather common, however this time the patient was unusual; it was a baby, only a few weeks old. He had been fine one minute and then had just …stopped. The usual things we consider in the death of child, physical violence, drugs, etc were not this case. This case was every parents’ nightmare scenario – their beautiful healthy baby, without any warning, just stopped breathing.
The child was whisked into a trauma bay and after running several cycles of the life support protocol a cardiac rhythm was obtained. The mother, who had come with the ambulance was hysterical. The father drove the car and arrived minutes later looking utterly hopeless. Return of circulation was of little comfort to them based on how they looked as their child was transported to the PICU. However the code itself was all very textbook. We didn’t know it at the time, but the boy would not survive.
Despite this incredible tragedy the department kept moving because it must. Ironically enough I diagnosed a teenager with a 17 week pregnancy minutes later. The ED doc and the pediatric attending discussed the evidence of using bicarb with epinephrine in infants. More patients checked in with various non-emergent ailments, unaware of why they were kept waiting so long. And I felt nothing. My mind knew this was tragic but I did not feel sad. But I also knew I should feel sad which then made me question my lack of emotional response.
As I related this story and these thoughts to some fellow residents days later a rather extraordinary thing happened. I began hearing similar stories from them. One broke down rather inexplicably but then related how she’d been involved in a similar pediatric code in the ED. It had been months earlier and she’d felt nothing at the time too. My story had made it all come back to her, however this time with emotions. Another resident, one of the most stoic in our program, teared up as he recalled participating in a pediatric withdrawal of care. A third shared how she had recently delivered a late pre-term baby after in intra-uterine fetal demise. She felt nothing at the time and still had no particular emotional response to that delivery.
Physicians receive very little training in how to deal with the difficult feelings around death and I imagine it’s the same for other providers, nurses, and first responders. One thing that nobody ever said to me, and it took a long time to realize, is that it’s okay to feel nothing. Based on my colleagues’ responses most of us will have experiences that should arouse emotion but don’t. Unfortunately medical training does not typically push us to share these experiences and we are left feeling isolated and guilty. Many of us will bear witness to terrible tragedy and not feeling doesn’t mean not caring. It may simply be that we are not in the right headspace to process those feelings but will at a later time. It may be that burying an emotional response is a deep defense mechanism to protect ourselves. It may be that a particular tragic event, for whatever reason, will just never provoke an emotional response. Regardless of the reason, if you are in the healthcare profession you will at times have experiences that should provoke emotion, but only leave you feeling nothing. And that’s okay.
462 notes
·
View notes

Text
When I'm still awake studying at 3AM and reflect on my decision to go to Med School

264 notes
·
View notes
Text
Admission #192: Best Friends Forever, MD
Dr. T: Sorry I couldn’t give this presentation yesterday. I was in court. Dr. R (from the back of the auditorium, yelling): Because of those drug charges? Dr. T: Haha, very funny. But seriously, I was testifying in court as an expert witness. Dr. R (yelling): As an expert badass and hottie, woo! Dr. T: Stop before the residents see mommy and daddy fighting. Dr. R (still yelling): I get to be daddy, right?
-Dr. T, guess that makes him mommy; Dr. R, has implied that the residents are the kids

23 notes
·
View notes

Link
Its that time of year where those of us who are in the upper-level courses have the massive 1 week review in every class of all the biology that has come before. I have a few tricks that help me remember the most simple concepts in Bio, that will hopefully help you guys save time too. Some of...
174 notes
·
View notes

Link
It’s obvious that prior to your medical school interview, you should be comfortable talking about yourself. Often overlooked, however, is the importance of being articulate on other topics. Increasingly, medical schools are assessing applicants’ true interest in medicine by asking about topics...
279 notes
·
View notes
Photo

Me, as we approach the second round of midterms.
294 notes
·
View notes
Text
Trying to repair the GPA I got myself freshman year

1K notes
·
View notes
Link
I’m on cardiology right now, and yesterday the fellow taught us some basics for interpreting EKGs. The trick is the have a thorough algorithm and do it every time so you don’t miss anything.
Disclaimer: Obviously this is just a cursory intro so folks won’t look like...
5K notes
·
View notes
Photo
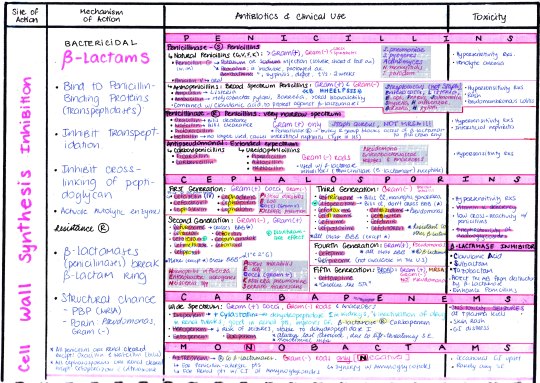
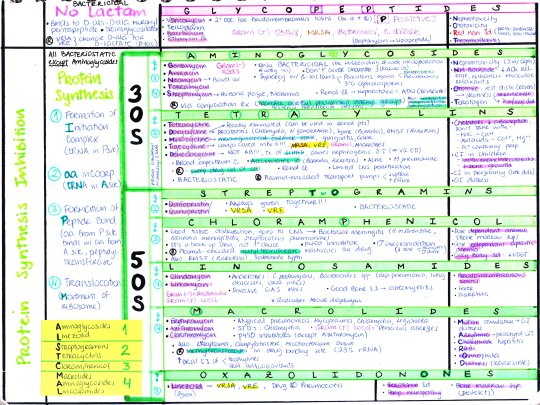
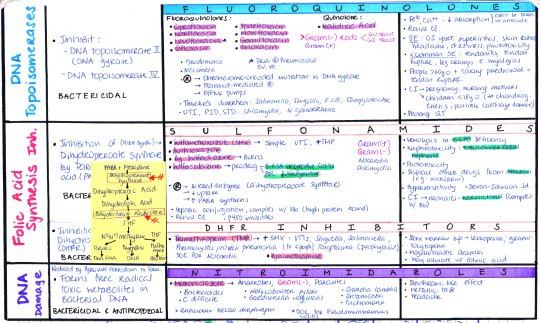
ANTIBIOTICS: COMPLETE CHART
[Download: AB1, AB2, AB3]
[Antibiotic Cheat Sheet]
2K notes
·
View notes
Conversation
This drugs Inhibit...
Leflunomide: Dihydroorotate Dehydrogenase (DH) [Carbamoyl phosphate --> Orotic Acid]
Mycophelonate: Inositol Monophosphate (IMP) DH
Ribavirin: IMP DH [IMP --> GMP]
Hydroxyurea: Ribonucleotide Reductase [UDP --> dUDP]
6-MP (& Azathioprine): PRPP Amidotrasnferase (de novo purine synthesis) [PRPP --> 5-phopsphoribosylamine --> IMP]
Allopurinol: non-competitive inhibitor of Xanthine Oxidase [Xanthine --> Uric Acid]. Allosteric Inhibitor of PRPP Amidotrasnferase
5-FU: Thymidylate synthase [dUMP --> dTMP]
Pyrimethamine: Dihydrofolate (DHF) Reductase
Trimethoprim: DHF Reductase
Methotrexate: DHF Reductase [DHF --> THF = no dUMP --> dTMP]
Rifampin: DNA dependant RNA polymerase [inhibits sigma (promoter) and rho (terminator)] in RNA transcription
Actinomycin: RNA polymerase 2, RNA polymerase α2ββ
α-amanitin (amanita phalloid mushroom): RNA polymerase 2
Quinolones: DNA topoisomerase II (DNA gyrase
Fomepizole: alcohol dehydrogenase
Disulfiram: acetaldehyde dehydrogenase
Beta-lactams: peptidoglycan cross-linking in cell wall
Glycopeptides: peptidoglycan formation by binding D-ala-D-ala portion on cell wall
Aminoglycosides: initiation complex in protein synthesis & translocation
Linezolid: initiation complex in protein synthesis
Streptogramins: aminoacyl-tRNA (aa incorporation) in protein synthesis
Tetracylins: aminoacyl-tRNA (aa incorporation) in protein synthesis
Cloramphenicol: peptide bond formation in protein synthesis
Macrolides: translocation in protein synthesis
Lincosamides: translocation in protein synthesis
Fluoroquinolones: DNA topoisomerase II (DNA gyrase) & DNA topoisomerase IV
Sulfonamides: dihydropteroate synthase
Trimethoprim: dihydrofolate reductase
Rifampin, Rifabutin (rifamycins): DNA-dependant RNA-polymerase
Ethambutol: arabinosyltransferase, inhibits synthesis of arabingalactan, no cell wall.
INH: synthesis of mycolic acids, need bacterial catalase-peroxidase, encoded by KatG gene. Resistant if deletion of KatG gene
Azoles: 14alpha-demethylase, thus inhibits ergosterol synthesis from lanosterol
Flucytosin: DNA/RNA synhesis, active metabolite inhibits thymidilate synthase (5-FC --> cytosine deaminase --> 5-FU --> 5- Fd-UMP)
Echinocandins (-fungin): beta glucan, thus inhibit cell wall synthesis
Terbinafine: squalene epoxidase, thus inhibit the formation of squalene epoxide from squalene
Griseofulvin: mitosis, interferes microubule fx.
Chloroquine: detoxification of heme into hemozoin; heme accumulates, heme toxic for plasmodia.
465 notes
·
View notes







