
doctorfiction
Doctor Fiction
a real life MD diagnosing imaginary people
20 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs

ouyama-chan
head empty only oikawa

coralduckpatrolexpert
Sans titre

kimwexlersponytail
The big guns... with a ponytail!

jelly-jebu-blog-blog
Dark Princess

lazysoulflower
tThings I like and do
Text

I'll be here from 12:45-2:15 on Saturday the 9th. Stop by and get your books signed, buy a copy if you don't have one (And I can sign that, too), chat about novel writing, jellyfish, and the art of the thriller. Maybe pick up some cool shades while you're here, too!
3 notes
·
View notes
Text
A Quick Word of Thanks
Henry and I would like to express our appreciation for all of the kind words regarding the blog post and the novel.

Thanks, you all made him do the Airedale grin.

And Max, the latest addition. No smile. He's still mad that Henry appears in the book and he doesn't.

In all seriousness . . .Thanks for the great reception and don't forget to send me your medical questions.
Yours,
Doctor Fiction
10 notes
·
View notes
Text
Go Ahead . . .Suspend My Disbelief!
Question: Do you have any general suggestions for an author who wants to write a thriller with a medical theme as its hook?
This question is very timely for me as I am just starting a new book. I would like to say that this is my second novel, but like many authors, I have a number of books in progress and struggle to find the one that inspires me to push through to the end.
That said, I took a look at my “works in progress,” and found that they all have something in common.
I like searching the web for a new scientific breakthrough or discovery that fills me with hope and scares the shit out of me simultaneously.
There . . . you see . . . we have the makings of a good thriller already. Kind of like Schrodinger’s Cat, it’s both alive and dead at the same time.

I am delighted and somewhat surprised to announce that my debut novel, Immortal Red, has just become an Amazon Best-Seller in the Medical Thriller, and Crime & Mystery / Science Fiction genres.
As such, I will use it as one of my examples for how to select an idea / premise for a novel. Shameless Plug: The eBook edition of Immortal Red is on sale for a limited time for $0.99 on Amazon. CLICK HERE for a deeper explanation and the opportunity to buy at $0.99 if you wish. While searching the web for second-hand parts for an ancient Lotus Elan and a used tweed jacket on Poshmark, I came across this article about a unique creature.
Fact: Turritopsis dohrnii, the dime-sized jellyfish with the bright red stomach, is the only creature on earth with the gift of immortality (notice that the title of the novel, Immortal Red, is chosen from the headline). When confronted with death due to advanced age, starvation, or trauma sufficient to kill but not obliterate, turritopsis dohrnii has the ability, through a process called transdifferentiation, to repair itself by converting adjacent healthy cells of one type into precise replacements for damaged cells of another type. This is not unlike a fetal stem cell, except for the fact that turritopsis can do this a seemingly endless number of times. Through this mechanism, turritopsis is able to effect a complete repair of all damaged tissue and emerge young and healthy.

Now I was intrigued and looked for a way to make this a universal concept, something that would appeal to everyone.
Questions: Would you want to live forever? Would you kill to be able to live forever? If everyone you know and love—dies of old age—would you want to go on? Would you be motivated to do anything if you had all the time in the world?
Suspension of Disbelief: A marine biologist snorkeling off the coast of Cape Fear discovers the jellyfish and takes it to her lab for further study. She kills the little invertebrates over a hundred times only to have them come back to life, new and perfect. She wonders if there may be mammalian applications. The Institute finds her research interesting but unimportant and cancels funding. Her husband works for the eighty year-old director of a CIA black ops division charged with doing jobs too dirty for the rest of the agency to touch. Surprise, the aged director offers to fund her research—and we’re off on a tale filled with a diverse cast: Nick, an archaeologist turned CIA “fixer,” who is dying, Tommie, a Native American who has died more times than he cares to remember, and Lucy, a young graduate student on the run with the “Cliff’s Notes” for immortality.
Procedure: At this point, I had to invent science sufficiently credible to allow human application of transdifferentiation. I took liberties with the existing science, but remained true to basic scientific and medical principles to allow the reader to suspend disbelief.
Here is another example of a simultaneously hopeful and horrifying scientific “breakthrough.”
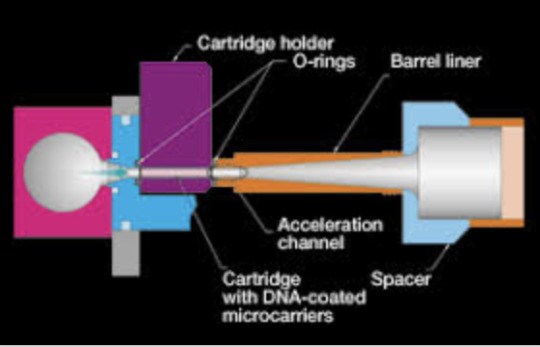
CRISPR: (Clustered Regularly Interspaced Short Palindromic Repeats) By use of a hand-held “gene gun” scientists are able to coat a heavy-metal projectile with specific gene material and literally fire it into a cell, inserting this genetic material into a strand of DNA to repair the strand or eliminate the sequence of certain diseases such as Cystic Fibrosis. . .
or to create a genetically modified “super” tomato.

All well and good until a Chinese scientist used the process in utero to create genetically modified super-twins. He’s now in prison, and there is a selective moratorium on the use of CRISPR in humans.
But once the cat is out of the bag . . .

The internet is chock full of tidbits like this if you just dig a bit. Below are the workings of machinations of one such headline:
“Combining a Virus and Genetic Material for Insertion into a Human Genome.”
Consider the following premise: the military, searching for a way to offset its ever shrinking ranks decides that it needs to create soldiers who can operate on the battle field without the constraints of conscience or the PTSD that often results from such activities.
The researchers note that the limbic system plays a vital role in the inhibition of violence and manifestation of the inevitable mental trauma of these actions. A plan is developed to insert DNA from the limbic system of a reptile into the limbic system of a test subject. Researchers note that reptiles are able to attack their prey without anger or regret. They simply do what is necessary to survive.
Ideally, the effects would be limited in both time and scope, manifesting on the battlefield and dissipating soon afterward. To that end, a decision is made to combine the type-specific DNA with a virus and literally give the subject’s limbic system a short-term “cold.”
What could possibly go wrong?
Well—it turns out—not only are the changes not limited to the target organ—the subjects are also contagious.
This premise happens to be the idea behind Elegant Beasts, a novel I am currently working on.
Below you will find the teaser prologue illustrating the evolution of an idea from Science Fact to Created Science to Suspension of Disbelief.
Elegant Beasts
Prologue
What if? The two most dangerous words in the English language. What if he hadn't ignored that nagging pain in his gut? Or better yet, what if he had never worked for that chip manufacturer growing those damn silicon crystals for micro-circuits and then cleaning them with trichloroethylene?
But that had been 1973. Who knew, another provocative word pairing, that “Tricky” would turn out to be one of the most potent hepatic carcinogens the world had ever seen? A time bomb that could sleep soundly for decades before waking to spawn a tumor that would quietly, double every 6-8 months, seeding the lung and regional lymph nodes. before bursting free, to take out its host in six months.
“Damn.” Albert Fontaine, MD rolled on his left side, brought his knees to his chest and palpated the growing mass under his right ribs. If he lay perfectly still, in a tight fetal position there was no pain. But moving—well— that was something else.
But, this morning, something was different. He didn't know what. But it didn't matter, given his present circumstance, different was good. The mass felt, not so much smaller, but softer, somehow less of a challenge to his survival.
Elizabeth Gilmore, PhD in Genetics and Virology or as he nicknamed her, Elizardbeth, now shortened to simply Lizard had told him this was just a “taste” of what was possible. A cure for the incurable. But at what cost he thought, picking at the scaly rash that had appeared on his forearms.
Life for his humanity. But not the life he had now. Was it a good trade? He supposed it was a matter of perspective and belief. He was no longer the Catholic schoolboy who accepted everything the nuns told him. But he was not quite ready to accept the Kansas rock band's thesis that “all we are is dust in the wind.”
The skin of the creature was the worst part.
Albert Fontaine had always been fascinated with skin. It was an overlooked wonder of evolution and accident, a twenty-one-square foot organ with an exceptional ability to regenerate itself. He had once read that dead skin cells accounted for a billion tons of dust in the atmosphere and he wanted to believe it, but as a scientist, he had no faith in how they’d arrived at that figure. Measured how many cells the average individual lost in a year, he supposed. 30,000 cells a minute? Was that right? Skin was always changing. Microbes roved its surface, fighting disease, the miniature populations unique to the species they protected. Fontaine liked this idea of humans hosting one kind of vibrant community and dogs another and baboons and sharks yet another. He was not religious, but this felt close: every moving creature a solar system for another world, every beating heart a sun, each world contained by living, seething skin.
Albert brushed the now vaguely greenish flakes from the rash on his forearm.
Lizard had hinted at the existence of another subject, someone months further along in their “treatment.”
And so, Fontaine had broken into Elizabeth Gilmore’s lab to see for himself.
Broken in wasn’t quite the correct term, since he had used a key card to gain access, but he’d acquired the duplicate key card under a false premise. So whatever that was, it was enough that he felt jumpy. He was not given to criminal activity; he did not get speeding tickets, he did not cross against the light, and he did not eat donuts from bags labeled with other people’s names in the break room. So long as the rules made sense, he was a rule follower.
But Elizabeth Gilmore’s research did not make sense. She had been one of DARPA’s (Defense Advanced Research Project Agency) “golden girls,” a rising star in charge of a government-funded “super soldier” program. Fast forward six months: The Lizard had been unceremoniously booted from her high-tech digs in the Virginia Tech research center and banished to a hastily outfitted lab in one of the many dozens of remote abandoned buildings that dot the nearby Radford Army Ammunition Plant Army Base
As Fontaine prowled through her lab, he tried to look as if he belonged, although he didn’t truly believe he would be interrupted. It was after hours for most of the staff and he’d watched Gilmore leave as he arrived. She worked the twelve-hour day shift that was typical here, seven am to seven pm. Fontaine was on the exact opposite, pulling nights since beginning his circadian skin research.
Gilmore’s lab was impeccable, not just spotlessly clean but fastidiously organized. A radio had been left on and it played the glimmering ‘80s music she listened to relentlessly. He’d somehow expected her research to be secret, hidden away, but the isolation chamber was clearly labeled.
Fontaine hadn’t been able to see anything through the glass square in the door, so he dutifully scrubbed down and searched for a hazard suit. Finding none, he considered his options. Given his dismal prognosis he decided to go for it.
The door opened with a snake-like hiss as the chamber decompressed. His vision adjusted slowly to the faint red lighting.
There it was.
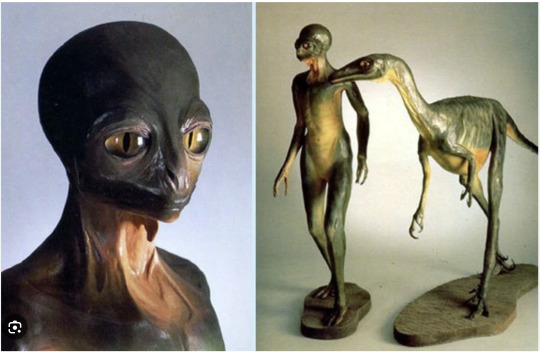
One fell straight into uncanny valley just to look at it. Two legs, two arms, those frightful hands, the eyes. Was it a thing that looked human or a human that looked like a thing? It was impossible for Fontaine to tell which direction the slider was being pushed.
And the skin was the worst part. On some areas of the body, it was smooth and hairless, the surface marked only by striations that reflected the arid environment of the isolation chamber. But on other others, particularly the arms and the face —
He was reminded suddenly of his younger brother, a miracle baby. He’d been born with Harlequin Ichthyosis, a rare skin disorder that left him plated with a thick armor of his own skin, a tiny stegosaurus-human chimera. The red, scaly plaques had to be operated on to keep his limbs from auto-amputating, and to this day he had to constantly manage his scaly, red skin.
Looking at Gilmore’s research, he was reminded not of the adult his brother had become, but the tiny, scaled hybrid in the ICU he had begun as.
“Dr. Fontaine, you seem lost.”
Fontaine startled.
She was there. Of course, she was there.
Elizabeth Gilmore stood just outside the isolation chamber, her narrow, shapely face framed in the thick glass window. He saw the thick blue lanyard at her neck; she had not left at all.
“What is the use of such research?” Fontaine demanded, his voice raised in order to be heard. “What practical application can there possibly be?”
Gilmore smiled. It was neither amused nor friendly. “It cured her anxiety disorder entirely.”
Her. Somehow it was far worse to think about the creature as possessing a gender.
“This is unethical,” he told her.
Gilmore merely blinked at him.
“How did you even get someone to volunteer for this?” he asked.
Gilmore looked away for a moment; she was tapping something into the keypad. When she looked back at him, her smile was gone. She said, “They wander in after hours.”
He heard the lock slide into place.
15 notes
·
View notes
Note
Hi! I have a character that is shot in the head by assassins and ends up permanently blind, but without any other brain damage. As currently is, the bullet goes through the optic nerves - but is this realistic? Is there enough room between the optic nerves and the frontal lobe for a bullet to pass through? Or would it make more sense for the bullet to go somewhere else, like the occipital lobe? Thanks!
Hi! I have a character that is shot in the head by assassins and ends up permanently blind, but without any other brain damage. As currently is, the bullet goes through the optic nerves-but is this realistic? Is there enough room between the optic nerves and the frontal lobes for a bullet to pass through? Or would it make more sense for the bullet to go somewhere else, like the occipital lobe? Thanks!
This is a fantastic question and shows a good basic grasp of neuroanatomy. While a gunshot to one of the optic nerves would result in partial blindness, it would also most probably result in death, or at the very least, a devastating loss of cognitive function. Rendering the victim totally blind would require a second assault on the other optic nerve. The sum total of these combined injuries would be death or at the least a persistent vegetative stage with no conscious brain function. Occipital lobe injury is a more plausible scenario. Even so, it’s still a very densely populated building with some very sensitive neighbors.
We will approach this dilemma in our usual manner: a minimal number of needed terms, simplified anatomy, physiology and pathophysiology with a drawing to answer your question and a twist that you might find useful in your story.
PROBLEM:
An assassin’s bullet renders a character blind but otherwise sensate with minimal to nil collateral sequelae.
SOLUTION:
What you are looking for is cortical blindness. I am going to give you a plausible scheme for this and present a related condition called blindsight that you may find applicable to your protagonist.
TERMS:
Sight: The special sense by which the color, shape, position and form of objects is perceived when the light from those objects strike the retina.
Blind: Unable to see, lacking the sense of sight.
Cortical Blindness: Loss of vision with an undamaged eye due to injury to the Occipital Cortex.
Blindsight: The ability of individuals with blindness to detect and respond to visual stimuli despite lacking awareness of having seen anything.
Occipital Cortex: Paired region of the brain divided by a sulcus (a narrow tract separating organs). It is located in the posterior and inferior aspect of the brain and takes its name from the nearby occipital bone. It is the site of Visual 1.
ANATOMY, PHYSIOLOGY, and PATHOPHYSIOLOGY
A brief (as humanly possible) explanation of vision as it applies to your scenario; Use this in conjunction with the Illustrations for a walkthrough of the pathways for sight and blindsight.
Retina: Located at the “back” of the eye, this structure creates 2D image and converts it into electrical impulses to be transmitted to Visual 1 in the Occipital Cortex for processing. The receptors include Rods for light-sensing and gray-scale imaging and Cones for the perception of color. This organ then compresses the data to allow transfer along the limited capacity of the Optic Nerve.
Optic Nerves: Known as Cranial Nerve II (CNII), they carry monocular (one -sided) input from the Retina of each eye to the Optic Chiasm where they are converted to binocular signals.
Superior Colliculus: Paired structures in the midbrain that receive input from the optic nerve. Loosely, they allow the cortically blind to perceive and react to movement even though they cannot “see” it in the conventional sense.
Optic Chiasm: The X-shaped area where the Optic Nerves cross and combine the images from both eyes allowing for binocular and stereoscopic vision.
Optic Tracts: These continuations of the Optic Nerves carry information from both left and right eyes from the Optic Chiasm to the LGN.
Lateral Geniculate Nucleus (LGN): One of the nine nuclei the visual inputs pass through on their way to Visual 1; this nucleus is the major relay center for impulses to Visual 1.
Optical Radiations: The sorted fibers from the LGN represent the final transmission pathway to Visual 1.
Visual 1 (V1): Located along the Calcarine Fissure, this structure is the primary processing center for visual data associated with basic sight perception.
Calcarine Fissure: Narrow openings along the medial aspects of the paired Occipital Cortices where the Optical Radiations from the Lateral Geniculate Nucleus link to Visual 1.

SIGNIFICANCE:
So, the take home is this: To result in complete cortical blindness, an injury occurring prior to Visual 1 would need to be penetrating and duplicated on the contra lateral (opposite side.) Due to the other critical structures in this area, the result of the direct contact and “shock wave” of the penetrating missile (bullet) would be gross deformity, loss of cognitive and midbrain function and at best, survival on a respirator.
The only plausible scenario for a single insult resulting in bilateral cortical blindness without gross deformity and loss of cognitive and motor function would be a midline non-penetrating or minimally penetrating injury to the posterior occiput bone.
PATHOPHYSIOLOGY:
A gunshot anywhere along the described pathway will result in a visual defect, but only one spot will cause total Cortical Blindness while preserving the appearance of the eye and giving a chance to avoid catastrophic collateral damage or death.
Both Eyes: This would indeed result in total blindness but would grossly disfigure both eyes and almost certainly be fatal.
Optic Nerve through the Optic Radiation: To cause total Cortical Blindness would require a shot on both sides and would pass through the Frontal and or Parietal Lobes. Damage would again be catastrophic with a near one-hundred percent certainty of death.
SOLUTION:
The only real possibility would be a single shot through the center of the Posterior Occiput. If the bullet were small bore (22/25 ACP) and round nose, (take a look at my previous post on the effects of different size bullets) there is the possibility that the bullet would not penetrate the occipital bone, but rather the shock wave would shatter the occiput and drive fragments through the narrow sulcus to the Calcarine Fissures bilaterally and result in total Cortical Blindness with little collateral damage.
This is a “long-shot” (excuse the pun,) but it is the most viable scenario and there are anecdotal accounts of precisely this mechanism and outcome.
Fictional Applications:
The fact that this injury leaves all of the “upstream” transmission, integration, and coding intact allows for some interesting story applications:
Blindsight:
The protagonist is able to “see” things that others cannot:
The protagonist cannot see what’s in front of them …

. . . but now has the ability to “see” events that are occurring elsewhere. These could be events happening now, events that are about to happen, or “cold case” events that have gone unsolved.
This provides a ready-made opportunity for introspection and character arc:
Egocentric — Altruistic (Dr Strange)
Bully — Protector (Pretty Woman))
If you need a Superhero:
Powerless — Powerful (Spiderman)
Or if you need a Supervillain:
Meek — Aggressor (Megamind)
Consider the possibilities with a smashing title such as 2020 Blindsight, or Visual 1.
doctorfiction
The Doctor is In
“When to call me: you’ve been stabbed, shot, poisoned, separated from an appendage, knocked or beaten unconscious, run over by a tractor mower, or generally about to bleed to death. Otherwise, leave me alone.”
— Aurelius Hogue MD, Doc Hollywood, 1991
Welcome. This blog belongs to a long time MD, a short time MFA. Doctor by profession, novelist by habit.
What I do on this blog: Every week, I’ll design infections, injuries, psychoses and neuroses for your fictional characters. You tell me the effect you want and I’ll tell you how they get there. Think of it as medical care in reverse.
What I don’t do on this blog: I do not diagnose or treat your real life infections, injuries, or psychiatric conditions. I do not help you undertake real-life nefarious pursuits. This advice is meant to be taken only in the spirit it is intended: helping bad things happen to good characters, fact meeting fiction.
Ground Rules: My ask box is always open, but the Doctor is only in once a week. Please keep your novel’s specifics out of your message. No character names, keep the scenarios general — we want it to be useful for more than one writer, if we can. Please do provide age and sex and any pertinent pre-existing conditions. I don’t need to see your character’s insurance card.
What is your chief complaint?
The Doctor is in.
— The Doctor
364 notes
·
View notes
Note
Is it actually useful to dig bullets out of your own arm in a public restroom in an emergency situation, or is that something that just happens in movies?
About self-surgery in the bathroom of the local Exxon Station… Psychologically we all feel that getting the bullet out will help the problem but generally speaking it is best to let sleeping dogs lie and to bastardize Hamlet, “Get thee to a surgery.” The greatest concerns immediately post gunshot are circulation and airway. You are probably not going to have a breathing problem other than hyperventilation from fear, if you are shot in the arm. Your big concerns are bleeding and nerve damage. Have your character dorsiflex (hyper extend) his wrist, make an “O” with his thumb and index finger, spread his fingers apart, and then smile when he realizes everything is still hooked up. He flexes his arm a few times to see if blood is spurting or just oozing. If its just oozing, cover with a wad of moist paper towels, tear of a shirt sleeve and wrap tight enough to apply pressure to the wad of paper towel, but not tight enough to constrict. Have the character check the pulse at his wrist and note the color and temperature of his arm. If the arm is cold, pale white, numb or the nerve check is bad, your character has problems and needs to find his/her buddy who is an EMT.
The only indication for digging out the bullet would be if the bleeding is uncontrollable, otherwise, the bullet may actually be tamponading the tissue and slowing the bleeding at this point. Infection is later concern. The wound will ultimately need attention and the character will need antibiotics, but he has a few hours to worry about that.
If the bullet does need to come out, no probing with a pocket knife. Consider having him pour rubbing alcohol over a pair of “needle nose” pliers (from the nearest convenience store,) and then gently probe the wound path until he feels the metallic click of the plier’s tip on the bullet. He can then try to open the pliers, grasp the bullet and retrieve it. Apply firm pressure for 5 minutes and observe. If no bleeding he can do the towel and shirtsleeve thing. If significant bleeding, have him apply as much direct pressure as necessary to stanch the bleeding.
If your character is in the habit of being shot, he may carry a “Bloodstopper” product. They are small, useful, and I have them nearby all the time. The powder can be sprinkled on and will help with clotting. There is a product that you can insert directly into the wound track, “ouch,” that has the same chemical. They can buy your character some time.

The Doctor is In. Want to ask a question? Read the guidelines first.
11K notes
·
View notes
Note
Hey Doc, how realistic is a “mild” punctured lung? Like, an ice pick in the top of the lung. Will that kill you after an hour or so?
First, my apologies; Doctor Fiction has spent the last few weeks wrapping up some developmental copyediting coursework and revising the prologue and epilogue of my latest novel. I have a backlog of excellent questions that I will work through as quickly as possible.
An injury of this type is called a Traumatic Pneumothorax.
Pneumothorax has many fiction applications and is a great device to incapacitate, or if the plot warrants, terminate a character. The medical sequelae (outcome) can be mild and develop over hours to days or catastrophic and occur in less than a minute or anything in-between.
As usual, we begin with a little anatomy and physiology, progress to pathology, and finish with a few fiction applications.
The Good, the Bad, and the Ugly:

Anatomy and Physiology: (The Good)
Lungs: Paired organs used to exchange carbon dioxide, the bodies waste gas, carbon dioxide, for oxygen (oxygen makes up approximately 21% of what passes for “fresh air” in our current environment.)
Thoracic Cavity: The lungs are contained within the Thoracic or Chest cavity. This cavity is lined with a slippery membrane called the pleura.
Pleura: This membrane lines the thoracic cavity. It secretes a serous fluid that keeps the lung in direct contact with the inner wall of the chest cavity but allows it to slide freely while breathing.
Pleural Space: This is a potential space between the lung surface and the cavity wall. Any injury or disease process that converts this potential space into an actual space is called a Pneumothorax.
Pericardial Sac: This is a double-walled sac containing the heart. It is located in roughly the center of the chest cavity and contains a pericardial membrane that functions like the pleural membrane for the heart.
Trachea and Bronchi: This is the “breathing tube.” Think of it as an inverted “Y” with one bronchus branching off the trachea to each lung and the trachea or root of the Y accessing the outside air via the mouth and nose.
Alveoli: There are over six hundred million of these tiny air sacs in the lung. Each one communicates with the circulatory system via its own venule and arteriole which are connected by a capillary bed wrapped around the alveoli.
The venules carry oxygen-depleted blood and carbon dioxide to the Capillary Bed where the inspired oxygen is extracted and the carbon dioxide discarded. The arterioles then carry the oxygen-rich blood back to the heart where it is distributed to the body and the whole process repeats itself.

Pneumothorax: (The Bad)
A pneumothorax is the creation of air space between the chest wall and the lungs for ANY reason. Pneumothoraxes (sounds like a character from Dr. Seuss) can be categorized two ways:

By their etiology, that is their cause, which can be spontaneous or traumatic.
Spontaneous Pneumothorax
· Medical condition: asthma, lung cancer, or chronic pulmonary disease
· Genetics: Cystic Fibrosis, Marfan’s Syndrome, or Ehlers-Danlos Syndrome
· Physical Attributes: Thin males between the ages of 15-34 have a five-fold risk
· Lifestyle: Smokers have a twenty-two-fold risk increase over non-smokers
Traumatic Pneumothorax
· Penetrating Chest Wound: gunshot, stabbing, foreign bodies (open to outside)
· Blunt Trauma: fractured rib (closed to outside)
· Barotrauma: sudden pressure change: SCUBA and blast injuries (closed)
The second and more germane classification is by their presentation as Simple or Tension. In the most basic terms, a Simple pneumothorax is the creation of a space between lung and chest wall which is uncomfortable, may require intervention, but does not expand and is not life-threatening.
This qualifies as, The Bad, but it does not qualify as …
Tension Pneumothorax: (The Ugly)
youtube
Each time you take a breath, a small amount of air moves into the space between the lungs and the chest wall and cannot escape. This results in several forms of badness:
· The air trapped between the lung and the chest wall does not pass through the alveoli, and as such, cannot replace the carbon dioxide waste with needed oxygen.
· With each breath, the space grows larger and pushes against the lung (tension pneumothorax), compressing the alveoli and further decreasing function.
· This ever-expanding bag of air pushes against the pericardial sac and compresses the heart, decreasing cardiac output. This is rapidly fatal without immediate intervention. The “Adam’s Apple” or trachea shifts or “points” to the side where the pneumothorax is. (this information will be helpful later)

If the stab wound has pierced a blood vessel, potential space may be filling with blood as well, creating a hemopneumothorax an all too common occurrence here in the emergency department knife and gun club.
The Cure
In an Emergency Room:
In a Closed Pneumothorax insert a chest tube with a one-way valve so that each inhalation will force air out, decrease the size of the air pocket, and alleviate the symptoms.
Treating Open Pneumothorax is a rapid-succession two-step procedure:
· Close the sucking chest wound to stop the influx of air through the chest wall
· Insert a chest tube as above to decrease the size of the pneumothorax.

In the case of hemopneumothorax; if the bleed has stopped, the chest tube will clear the blood. If not, surgery is required to “tie-off” the bleeder.
And now … Fiction:
So, your character is in the field, far removed from a hospital. This is well and good if you want him to die. If not …
Suppose your character has suffered a closed tension pneumothorax:
· Blast Injury: the character has punctured a lung due to over-pressure. They may have other injuries as well.
· Blunt Trauma: fall from a height, hit by a car, smacked by a bear, etc.
· SCUBA: saw a monster on the bottom, came up to quickly and dropped a lung due to pressure change
Improvised Chest Tube:
Supplies: a pocket knife, ink pen, plastic glove, duct tape, and left-over alcohol from last night’s festivities.
Technique: have your rescuer pick a spot halfway between the armpit and the nipple on the affected side (remember the tracheal shift) and count down four or five ribs.

Clean the area with the alcohol. Clean the pocket knife with the alcohol. Remove the cartridge from the ink pen and use the barrel without the clicker. Cut a finger off the glove with your knife and cut a hole in the tip of the glove finger. Slip the glove finger over the non-pointy end of the ink pen barrel and secure with a small strip of duct tape.

Your rescuer will need to make a small puncture over the rib and push the pointy end of the ink pen barrel over the top of the rib so that it enters the chest cavity. There will be a slight “whoosh” of air as the pneumothorax decompresses; the vein, artery, and nerve of the rib run along the bottom and MUCH badness will occur if they are injured. The area around the pin is sealed and secured with wide strips of duct tape.
If the injury is an open tension pneumothorax:
· Knife Wound
· Puncture wound of any type: tree branch, punji stick, fence picket, etc.
· Gunshot Wound
If the hole is small, your rescuer could insert the makeshift chest tube as above through the opening. Alternatively, the hole could be covered with duct tape to create a closed pneumothorax and the chest tube inserted in the as above.
If there are no supplies for a chest tube, a flap valve can be created by taking a piece of plastic wrap or thin ground cloth sufficient to cover the wound and securing it on three sides with duct tape. The open side functions as a flap valve, letting the air escape but not reenter the pneumothorax.

This may get your character to a hospital.
This is a long post, but now that you know the anatomy, physiology, and pathophysiology you can use it in your writing.
Click the link below for the rules for questions
https://doctorfiction.tumblr.com/post/181400956523/the-doctor-is-in
439 notes
·
View notes
Note
The protagonist in my speculative fiction novel needs to have a problem that will eventually incapacitate him but starts with very subtle changes that become more apparent over time. I was thinking seizures, but that doesn't seem very subtle. Any ideas?
Actually, seizures are an excellent choice for what you are trying to accomplish. Seizures run the gamut from nearly imperceptible to impossible to ignore.
Let’s start with a definition of the term seizure, progress quickly through the different types, their etiologies (causes) and how they manifest, and finish up with a seizure disorder appropriate to your genre and protagonist.
Simply put, a seizure is an abrupt, abnormal electrical disturbance of the brain resulting in an aberrant motor (muscle) or sensory (thought or sensation) response.

Seizures can be caused by fever, head trauma, brain bleeding, chemical imbalance, drug/alcohol use, or a space-occupying lesion (a brain tumor or growing mass of any kind). For fiction purposes, we will be concentrating on the space-occupying lesions and how they affect Neurons ( the cells that allow the brain to send and receive information).
Motor neurons: The brain uses these to make muscles move.
Sensory neurons: This is how the brain receives information from the body and the outside world.
Seizures are classified into two general types: Generalized and Focal (Partial).
**When identifying seizure types, the terms Focal and Partial are interchangeable.**
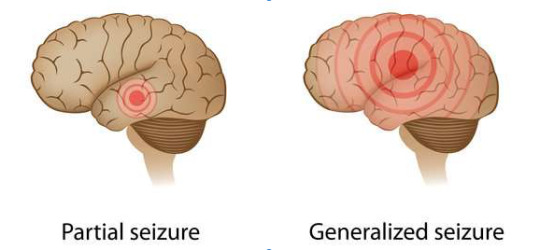
Generalized seizures tend to involve all areas of the brain. This category includes a number of subtypes:
Tonic-Clonic: Formerly referred to as a gran mal (French for great evil); this is what most people visualize when they hear the word seizure. The subject is on the ground, unresponsive, arms and legs jerking. The patient may drool or suffer incontinence (loss of bowel/bladder control). The episode lasts from a few seconds to several minutes. The event is dramatic and frightening to bystanders and the subject.
Absence: The subject stares into space as if ignoring you. These seizures last only a few seconds and are more common in the young.
Atonic: Sometimes called “drop-out” seizures, these are characterized by muscle weakness. The subject generally remains alert, but the muscles go weak and they drop what they are holding and may fall to the ground. These also are of short duration.
There are other subtypes of Generalized seizures, but the focus of our attention in this post is limited in scope and will deal primarily with the subtler and more fiction-worthy Focal variety.
Focal seizures are so named because they occur in a specific region of the brain and produce symptoms (at least initially) limited (focal) to that area.

The subject may have an altered mental status, but unlike a Generalized seizure, they are usually conscious and often aware and terrified by the manifestations of the seizure. We will explore two types of Focal seizures:
Complex Focal Seizures: These can cause blank stares, lip-smacking, pill rolling movements and laughing, crying, or screaming for no reason. This type of seizure is interesting and does have some obvious uses as a fiction vehicle.
Simple Focal Seizure: These seizures affect how we perceive our surroundings and can cause motor (movement) disorders or changes in mood or emotion. This type is especially well-suited to fiction. The following are a few of the possible symptoms:
Isolated involuntary twitching of fingers
Blank stares
Hallucinations: seeing, smelling and hearing things that are not there or morphing things that are there into something else.
Déjà vu sensations
Sudden mood or emotional changes
Dilated pupils
Seconday Generalized Seizure: This is a type of Focal seizure that spreads to the entire brain and can cause gran mal whole-body seizures. It can be because of multiple affected areas.
The inside of the skull is a closed space. When something foreign occupies that space, it exerts pressure on whatever structure is nearby. If the pressure becomes great enough, it will alter the signal passing through the Neurons causing a Focal abnormality. The nature of the abnormality depends on what part of the brain is sending or receiving the signal.

Now that you have a very basic idea of the nature of Focal (partial) seizures, let’s apply the principles to fiction.
For Example:
A young environmental scientist is taking water samples near an abandoned chemical plant. He is surprised to find tiny tadpole-like organisms swimming in the toxic runoff. The small creatures are whipping their tails and actually break the surface of the water. As he moves closer, there is a marked increase in activity. As he bends down to take a sample, one of the small red- brown creatures lands on his upper lip. Startled, he inhales deeply and feels a burning sensation in his nose. He sneezes, the sensation passes, and he returns to collecting samples. On the ride home, he develops an intense headache and ringing in his ears. He blows his nose many times, but cannot clear the noxious smell of the polluted water. Over the next several weeks, the headaches increase and he notices that he has developed an intermittent facial tic and an occasional uncontrollable twitching of his right index finger. He finds that he has difficulty forming words and misinterprets road signs and speech.
When he is found mumbling and walking in circles in the laboratory parking lot, his research partner takes him to the emergency room where a CT Scan reveals multiple small growths in various areas of his brain.
He is admitted to the hospital for further testing. That night, he complains to the nurse that he feels like “things” are crawling under his skin. She summons the on-call doctor who finds him naked on the floor having a gran mal seizure, his body covered with a red-brown rash.
Doctor Fiction expects someone to write this book and will look for it on the NYT Bestseller list next fall.
127 notes
·
View notes
Note
I have a female protag in her early 50’s with a bad case of the could’ve/would’ve/should’ves. Are there any physical, mental, or emotional symptoms she would manifest? Coping mechanisms? Thanks, doc!
This intriguing medical question with virtually limitless literary permutations is made even more poignant by the recent Valentine’s Day. The problem is boiling it down to a reasonable essence for this post. As always, we will start with a description of the entity at hand, touch on the physical, mental, and emotional manifestations and end with some ideas on using this concept in fiction.
In the broadest terms, you are talking about Nostalgia, a term contrived from the Greek words nostos (homecoming) and algia (ache).
Nostalgia is all about memories, the things that make us who we are. But memories are imprecise things. They tend to mutate with time, with each remembrance erasing and replacing the original with a “close, but no cigar” copy. Freud would say that you don’t actually remember the long-ago event, you remember a memory of a memory of a memory.
Memories are formed as the result of an event. Not all memories stick around forever. We have short-term and long-term memory. A short-term memory (looking at a menu and telling the waiter what you want a bowl of chili) may last only as long as it takes to place your order. If, however, the bowl of chili causes an allergic reaction and you are taken to the emergency department where you meet and marry the most beautiful nurse you have ever seen, your brain may see fit to move this event to long-term storage.
youtube
Memories are Made of This
And now—a shameless oversimplification of neuroanatomy that would have earned me a guaranteed FAIL in medical school.

Limbic System: a phylogenetically ancient portion of the brain encompassing several structures dealing with emotions and memories.
Amygdala: an area of the limbic system dealing with emotion (especially fear) and the selection of which memories are stored. The more intense the emotion, the more likely the selection for long term storage.
Hippocampus: not a college for water-dwelling herbivores, but an area of the limbic system dealing with the forming, storing, processing, and retrieval of memories. It is very receptive to sight, sound, smell, and taste. Hence, the ability of these stimuli to evoke memories based on stimuli present at the time the stored event occurred.
Hypothalamus: this area is, in effect, a repository for the hormones responsible for happiness, sadness, anger, and in a very broad and loose sense, motivation.
Nostalgia can take on many forms. It is important to remember that nostalgia is not a medical diagnosis. As such, the following labels are only a contrivance but may prove useful to the purveyor of fiction.
Nostalgia is almost always a comparison of past to present. How your character views the past depends in large part on their level of satisfaction with the present. Using the character’s sub-textual comparison, we will divide nostalgia into three broad categories and tag each with a representative song, allowing Doctor Fiction to take his own walk down Memory Lane:
Contemplative: The character is relatively satisfied with their life and the way they have lived it to this point. This is more or less the “could’ve” individual. They have a very positive recollection of an event and fantasize for a moment how “could’ve” turned out if they had taken a different path. They enjoy the bittersweet memory for a bit and “push on” with the life they have. The effect is similar to watching a very evocative movie. Some linger longer than others, but they put the memory “back in the box,” and function as before.
youtube
Constructive: This character may have had some hard knocks but uses these remembrances to look toward a positive future. Life may have given them lemons, but that’s how you make lemonade. Maybe they “would’ve” if they’d thought about it, but they didn’t. These characters view the present as better than the past and envision a future better than the present.
youtube
**Unfortunately, I am limited to five youtube postings. Please copy and paste the addresses for the songs listed but not embedded. They do help illustrate the point.
The Highwayman(by Jimmy Webb, as performed by Johnny Cash, Chris Christopherson, Waylon Jennings, and Willie Nelson,)
https://www.youtube.com/watch?v=aFkcAH-m9W0
Constrained: These poor souls don’t just remember the past, they are trapped in it. We can divide this group into a couple of subcategories:
Melancholy: They have some great memories, but then it all went bad and it’s going to get worse. They cling to their recollections and cannot move forward.
Regardless of their age, they suffer from “old soul” syndrome. They are miserable human beings, but they make great characters.
Bookends (Simon and Garfinkle) https://www.youtube.com/watch?v=sovVYInjHjw
Morose: These characters are also trapped in the past but, unlike the melancholy, they have no good memories, but spend their time mourning what never was.
youtube
Nostalgia was made for writers. In fiction, the author “cherry-picks” life, presenting only that which is interesting and serves to advance the story. The story is a series of ever-escalating events, and of greater importance, how the protagonist reacts to them. This is what defines character and eventually brings us to a resolution and conclusion.
The brain also “cherry-picks,” based on intensity and relevance, which memories it will retain: the bar for retention, as in writing, is quite high and most events do not make the cut.
The character’s perception of satisfaction or dissatisfaction with their state of being is greatly influenced by the comparison of past and present when they recall those memories. That perception is an amalgam of what has happened since the memory events occurred and any underlying personality disorders or diagnosis will influence whether their nostalgia is contemplative, constructive, or constrained.
I hope the post and the musical selection will be useful in your writing.
As we are in the Valentine season, I will leave you with one of my favorite dishes, a near perfect stew of hope, fear, introspection, and melancholy.
youtube
51 notes
·
View notes
Note
I'm just going to assume you're the ghost of Michael Crichton. No, no. You can't convince me otherwise. :)
“The man’s gaze lingered, then soft-focused and seemed to look both at and through him at the same time. He sensed fatigue and regret, but something else—resolve. It was as if he had one foot in this world and one in the next, like a ghost tired of the haunting, but with business to finish before he moved on. This was a man with a mission. It sure wasn’t real estate and he hoped it wasn’t murder. One last squeeze and he let the man’s hand go.”
25 notes
·
View notes
Text
Leeches
elliebrie said:
Love your blog. I have a question for you! Are leeches still used in modern medicine? If so, what kind of uses do they have? Thanks!!
Yes, Hirudo Medicinalis (the medical leech) is definitely on the comeback trail after a six-decade hiatus.
The History
Hirudotherapy (bloodletting with leeches), has been with us for over 3500 years. Hirudo is Latin for leech. They are depicted on the wall of ancient Egypt. The Greeks and Romans believed that the blood contained four essential Humors, (blood, yellow bile, black bile, and phlegm). These humors were responsible for a person’s personality and health. All mental and physical disorders save trauma, were thought to result from an imbalance of these humors. The physician priests of the day believed that bloodletting would restore humoral balance and aid in healing. Although the scientific rationale lay centuries in the future, experience taught that bloodletting with leeches had significantly fewer consequences than mechanical Venipuncture (opening veins with a sharp object to remove blood).
In 1215, the Catholic Church decreed that clergy could no longer engage in the practice of surgery, as this brought them into contact with blood which was thought to contaminate men of the church. As most physicians were clergy, this degraded the practice of surgery and hence bloodletting to a non-medical craft status. The gap was quickly filled by a new class of practitioner, the surgeon/barber, who became the dentist, orthopedist, wound care specialist and yes, bloodletter of the day. This somewhat artificial separation exists today with most state boards licensing “physicians and surgeons,” and the curious English habit of addressing surgeons as “mister’ rather than doctor.

After removing the leeches from their patrons, the barbers would soak up the excess blood with cloths which were then wrapped around poles to advertise their trade.

The concept of humor as a controlling factor in disease and personality was widely accepted through the mid 16th century. The scientific and medical research and reasoning of the next two centuries gradually eroded the concept and by the mid 18th century it was fully debunked. The practice of bloodletting and Hirudotherapy, however, persisted due to the empiric (experience-based observation) improvement in some patients with infection or conditions such as Polycythemia Vera (a condition where the patient has too much blood).
By the early 20th century Hirudo Medicinalis had been consigned to the bogs and ponds of medical history by all but a few “alternative” practitioners.
“Electrolux . . . the biggest sucker of them all” (Blue, Jefferson. Undercover Blues DVD. Directed by Herbert Ross. Culver City, 1993)

Hirudo Medicinalis: this classy European import hails primarily from Hungary and Sweden and has been the gold standard for centuries. Its domestic counterpart, Macrobdella Decora is a perfectly acceptable substitute, but who wants carp eggs when they can have caviar.
Hirudo (I think we are familiar enough now to be on a first name basis), are 8-20 cm in length and brown with rusty red stripes. They are hermaphroditic, have 5 pairs of eyes, consume 10 times their weight in blood in 20-30 minutes, and can survive 3-6 months on a single feeding. They have suckers on both ends and fully functional digestive tract.

The anterior or head sucker covers the mouthparts which consist of 3 jaws with over one-hundred tiny teeth. This is followed by a pharynx (throat), salivary glands, crop (a storage stomach) intestines, rectum, anus, and a posterior sucker (used to aid in movement and attachment. The sucker forms a tight seal and brings the jaws into contact with the skin. The teeth puncture the skin (see the characteristic “tripod” bite above), the leech feeds for 20-30 minutes and then detaches. The salivary glands secrete compounds which anesthetize (numb) the ski, making the bite painless, anticoagulate (prevent clotting), thrombolyse (dissolve existing clots), are anti-inflammatory (prevent or reduce swelling), vasodilate (increase blood flow), and antibacterial (reduce or inhibit the growth of bacteria). Although these secretions have evolved to facilitate the leeches’ phlebotomy (the removal of blood), they have significant medical benefits in certain circumstances.
Reattachment of Severed Digits
When fingers or toes are severed and reattached arteries (supply blood to tissue) and even nerves can be reattached. The tiny veins (drain blood from tissue) can-not be reattached and must, over time, regenerate. This creates a situation where the reattached digit becomes engorged with blood, painful, subject to infection, and can not receive new blood because it is filled with blood from which the nutrients and oxygen have been used up. Tissue swells, non-flowing blood clots, infection sets in and the digit is lost.
· keeps blood from clotting and dissolves existing clots (anticoagulate, thrombolyse)
· relieves pressure by draining excess blood until veins regenerate (phlebotomy)
· dilates vessels to increase the flow of incoming blood (vasodilate)· decreases pain (anesthetize)
· decreases tissue swelling due to irritation/manipulation (anti-inflammatory)
· inhibits the growth of bacteria (antibacterial)
Cosmetic/Reconstructive Surgery of Face or Breast A similar situation exists where circulation is poor. Blood pooling and swelling starve the tissue, leading to infection, ischemia (lack of oxygen) and tissue death. The chemicals found in the Hirudo saliva protect the delicate soft tissues.
· same actions as above (anticoagulate, thrombolyse, vasodilate, anesthetize, anti-inflammatory, antibacterial, and, phlebotomy)
Osteoarthritis
This painful joint condition is characterized by pain, swelling, and decreased function. Chronic treatment of pain and inflammation with compounds like ibuprofen can lead to kidney problems and severe stomach inflammation and ulcer disease.
· Decrease pain without irritating the gastrointestinal system (anti-inflammatory, anesthetize)
· Increase blood flow (vasodilate)
The anticoagulant, thrombolytic chemical found in the saliva is called Hirudin. This chemical has the added benefit of encouraging slow steady bleeding for hours after removal.
Cautions
· Patients with clotting disorders or those on blood thinners· Serious, even anaphylactic (life-threatening allergic reactions), allergic reactions to any component
· Infection from the bacteria found in a non-certified leech
Writerly Stuff
Imagine the protagonist lost in a wilderness with bogs and ponds. The character breaks a hand in a fall resulting in severe bleeding into the hand tissue. The swelling compromises the blood supply to the hand. Being days from the nearest town, there will be permanent dysfunction and possible loss of the hand before reaching medical care. The character finds leeches in one of the bogs and puts several on the affected hand.
· the hand is saved, OR
· a life-threatening infection results from the wild leech, OR
· the patient has a severe allergic reaction
For those into speculative fiction, the leech could be alien or an unknown species whose saliva Peptide (short chain amino acid), induces a premise-rich mutation in your protagonist. If you like fish stories, consider
Ichthyotherapy (the medical use of fish) which has endless speculative fiction possibilities. Can you say Aquaman?
Or, Helminthic Therapy (the medical use of parasites). You could write the next Contagion.
Click the link below for the rules for questions
https://doctorfiction.tumblr.com/post/181400956523/the-doctor-is-in
534 notes
·
View notes
Note
Love your blog. I have a question for you! Are leeches still used in modern medicine? If so, what kind of uses do they have? Thanks!!
11 notes
·
View notes
Note
Is it possible for a character with a pacemaker to still suffer from a heart attack (or experience any potentially lethal heart disease which causes similar symptoms?) Thank you so much!
There are some very neat things you can do with and to characters with a pacemaker. Let’s start with a VERY brief description of cardiac electrophysiology followed by what a pacemaker is, how it works, and the different types. We will finish with what they can and can’t do (the essence of your question,) and some suggestions for using them in a story. We will deal only with implanted pacemakers and skip the fancy ones used in the emergency department and cardiac labs.

Doctor Fiction’s Pacemaker Primer (simplified but conceptually accurate)
Knowing and using the terms in BOLD as appropriate will add credibility to your story.
Take a breath. The oxygen goes to your lungs where thousands of teeny air sacs lie next to even teenier vessels that take the oxygen (O2) and give up carbon dioxide (CO2). Relax and exhale, you just got rid of the CO2 and you’re ready to suck in another load of O2.
The O2 rich blood makes its way through the circulatory system to the to the Left Ventricle (the major pumping chamber of the heart) where it is pumped through the arteries to all parts of the body (brain, digestive organs, kidneys, muscles, skin, etc.)—everywhere that O2 is used. The equally teeny veins of those organs accept the O2 and give up their waste CO2. This system of veins returns the CO2-laden blood to the heart’s Right Ventricle where it is pumped over to the lungs to repeat the cycle. The average resting heart beats about 70 times a minute and the average respiratory rate is about 16 times per minute. A well-conditioned person may have a resting heart rate in the 50s.
The heart is a unique blend of muscle and nerve. The heart has an intrinsic pacemaker (node) which fires a minute electrical charge about 70 times per minute. Each charge results in a heartbeat (contraction.) If the firing rate is too slow (Bradycardia), it may not meet the body’s demands.
Potential symptoms of Bradycardia: (less than 50/min)
Near Syncope (dizziness, vision closing in from sides, ringing in ears, weak legs, confusion, nausea)
Syncope (a brief period of loss of consciousness, fainting and fall)
Angina (heart pain due to inadequate O2 caused by PARTIAL blockage or overwork)
If the underlying heart disease is serious enough, the heart may quiver in an unorganized fashion (Fibrillation) that does not result in pumping blood. When blood-flow stops, breathing stops, and brain damage begins. If the complete lack of blood flow lasts more than several minutes, the damage will be irreversible. Damage is also happening to the heart and the rest of the body but those systems have a much greater potential for recovery.
An implanted pacemaker is a small device with a lithium battery which is implanted under the skin and wired into the heart. They augment or in some cases replace the heart’s natural pacemaker. The batteries will generally last 5 years or longer. The device is implanted near the left shoulder in a pouch created just below the left clavicle (collarbone)
For our purposes we’ll limit our discussion to two types of devices: those that pace only and those that pace and defibrillate (ACIDs)
Asynchronous pacemakers fire at a preset rate regardless of what the heart’s intrinsic pacemaker is doing, generally 60-70 times per minute. These were the original pacemakers and are rarely used now.
Synchronous or Demand pacemakers are able to sense the heart rate and fire only when the rate falls below a predetermined number, say 50.
Automated implanted cardioverter defibrillators (ACIDs) are able to sense and attempt to correct bothTachycardia (rapid heart rate) and Fibrillation. ACIDs generally are also pacemakers.
Ventricular Tachycardia occurs when an ailing heart beats 120-300 times a minute. This can cause many of the same symptoms listed above (as well as chest pain and a fluttering feeling in the chest,) places a great strain on the heart, and frequently leads to the rapidly fatal Ventricular Fibrillation mentioned above.
The ACIDs correct Tachycardia by giving a short series of minute electric shocks timed to interrupt the abnormal rhythm encouraging the heart to return to regular rhythm. In Ventricular Fibrillation, the ACID delivers a larger shock which momentarily stops the heart and allows the natural or implanted pacemaker to resume normal rhythm.
A heart attack (Myocardial Infarction, MI) is generally caused by a blockage in one or more of the Coronaries (the small arteries which supply the heart). Neither an Implanted Pacemaker nor an ACID can open a blocked artery.
What they can do:
· Electrically treat Bradycardia, Ventricular Tachycardia, and Ventricular Fibrillation and avoid their symptoms and bad outcomes.
· Lessen the pain of Angina (which chest pain but not a heart attack)
· Improve cardiac efficiency by maintaining regular rhythm (heartbeat)
What they can’t do:
· Clear a blockage in the Coronary Arteries (chief cause of heart attack)
· Repair muscle damaged in previous heart attacks
Pacemaker /defibrillators are great at reducing Morbidity (disease symptoms) and Mortality (death from Ventricular Fibrillation).
Some devices also treat atrial fibrillation (quivering of the smaller pre-loading heart chamber). AF does NOT directly lead to heart attacks and is not covered here.
But YES, your character can still have a heart attack and suffer from other serious disease in spite of having a pacemaker.
Now for a few ways to use pacemakers and irregular rhythms in your writing.
Most of your characters with pacemakers will probably be over 50 or have some kind of obvious genetic or acquired Cardiomyopathy (heart muscle disease). To expand your age bracket, consider giving your character Brugada’s Syndrome.
Brugada’s is a genetically linked condition predisposing late teen to early 30s subjects (male and Asian predominance) to Ventricular Tachycardia and Ventricular Fibrillation with a high incidence of sudden death. Characters with this syndrome could pass out at any time and expire without warning if warranted in your story. An ACID improves Morbidity and Mortality (those words again.)
Possible plot devices using Pacemaker/ACID:
Do not store cellphone in a shirt pocket over the pacemaker.
Keep the following at least 6 inches from pacemaker: hairdryers, shavers, sewing machines, electric ultrasonic toothbrushes, and large magnets of any kind (stereo speakers.)
Stay at least 2 feet away from induction cooking ranges.
Don’t do any arc welding.
Avoid MRI (Magnetic Resonance Imaging).
Pacemakers can set off airport security scanners.
The Doctor is In. Want to ask a question? Read the guidelines first.
82 notes
·
View notes
Note
Are there certain injuries that are more commonly seen in young women abused by their boyfriends?
You will notice that this posting consists of a single entry. I had already chosen 3 questions for this week’s posting when this appeared in my inbox. As you know, my answers are generally infused with a fair dose of whimsy.
I felt this question deserved a forum of its own undiluted by humor. Fear not, the 3 previously chosen questions will appear next week.
It is my fervent hope that the inspiration for this question is purely literary.
One of the most common misconceptions is to limit the concept of abuse to physical violence. Abuse springs from a desire to control. The perpetrator accomplishes this task through a combination of physical, emotional, social and financial gambits.
I will answer the question with a most disheartening fictional Emergency Room encounter.
As I am a writer, talking to other writers, I have exercised poetic license. The patient presented here is a fictitious amalgam of partner abuse injuries I have treated in the Emergency Department. My hope is that this will both answer the question and further raise awareness of this epidemic.
The post is quite long but please bear with me and read it all. I hope it will both educate and aid in the literary treatment of this epidemic issue.
Abbreviations: CC/chief complaint, HPI/ History of Present Illness, ROS/Review of Systems, PMHx/Past Medical History, CM/ current medications, PSHx/Past Surgical History, Imaging/ (X-ray, CT, MRI, Ultrasound), Dx: Diagnosis, and TX. If you are “getting all medical” in your story, the format shown below adds great credibility, allowing you to present information for discussion without appearing as an “info-dump.”
Physical examination was as follows: Pertinent POSITIVES are in bold
23 NOV 20XX
CC: L leg pain, headache and chest wall pain.
HPI: A 22-year-old female sits on the exam table. She is accompanied by her 25-year-old boyfriend. The boyfriend is bent over and whispering in her ear. She is nodding. They separate and he half smiles when I enter the room with a nurse.
The patient has swelling and yellow-brown bruising about the left eye. Although it is a hot summer evening, she is wearing a long-sleeve blouse, jeans, and socks. Her partner is wearing cut-offs, short-sleeve T-shirt and steel-toe work boots with gray socks.
She c/o Left lower leg pain, left upper arm pain, right rib pain made worse with deep breathing, abdominal pain without nausea and headache with blurred vision on left. She states that she sustained the injuries when she tripped over a rug and fell onto a “coffee table.” She denies LOC. (loss of consciousness) She also complains of left lower leg pain, worsened by weight-bearing. She c/o low abdominal pain associated with fall. Her partner interjects, stating that she can be clumsy and fell off the front porch 2 months prior sustaining arm, chest head injury. She denies ETOH (alcohol.) The nurse tells her she looks familiar. The patient responds that she was in the E.D. a couple of months ago after “falling off the front porch.” Her partner laughs and volunteers that she’s a bit clumsy. The patient is crying, appears deferential and stares at the floor during history.
ROS: Positive for Head trauma with pain and swelling about R eye. Blurred vision R eye. A headache. Right side chest pain worse with deep breathing, and pain mid-portion L upper arm. Abdominal pain. Increased frequency of urination. Fatigue. Irregular infrequent menses. (LMP 4 months prior)
PMHx: Depression with Anxious Mood
Second Trimester Abortion secondary to fall
Abdominal Pain/chronic of unknown etiology
Fracture Right Wrist after fall
OB-GYN: G2/P0/Spontaneous AB2 (2 pregnancies, no births, 2 non-medically induced abortions)
CM: Prozac 20mg daily
PSHx:
D&C after traumatic abortion
Open Reduction and Internal Fixation Right Wrist Fracture
Social: Patient states she feels safe at home when queried.
Negative ETOH or illicit drug usage. 3 cigarettes per day
The nurse gives the patient a gown for the examination and asks the boyfriend and me to step out. He is reluctant but complies.
In the hall, the E.R. clerk hands me an EDie. report on the patient.
An EDie report is a computer-generated list of every emergency department visit to any E.R. for a given patient in a given time period.
The patient’s Edie reveals she has had nine visits in the past 12 months. Five visits have been for musculoskeletal “fall” trauma, two for abdominal pain, and one for anxiety. The clerk pulls me aside and states that the patient’s partner has had two E.D. visits in the past year, one for injuries sustained in a fight at work and another for evaluation after an arrest for driving while intoxicated.
When I question the partner regarding the patient’s repeated fall injuries, he states again that she falls a lot, becomes visibly agitated and says he has to go outside for a smoke.
Exam:
General: Patient alert and oriented x 3. No acute physical distress.
Head: Scaring of eardrums, L>R consistent with childhood ear infections vs healed traumatic rupture from blunt trauma. Questionable Left hemotympanum (blood behind the eardrum.) Obvious dental caries (tooth decay) in upper and lower molars. Chipped teeth: Right upper central incisor upper and Left lower canine.
Neck: Trachea midline, neck veins flat, Tenderness with Range of Motion. Generalized tenderness with palpation, no spinous tenderness. Blue-green fingertip bruising noted, one left, three right at the level of the trachea. (strangulation injury either “throttling or near strangulation to establish control)
Heart: Rate 102 and regular, without murmur.
Chest/Back: Lungs clear to auscultation without quiet areas. Black-blue fingertip bruising left breast. Multiple areas of bruising. Bright erythema (redness) with underlying edema noted of anterolateral aspect R ribs 5-7. Significant tenderness and crepitus (grating or crackling) over the affected area with inspiration. No tenderness or crepitus or step-off noted on spinal exam. Numerous bruises L/R chest and back. These cover the spectrum, ranging from Black-Blue-Green-Yellow and Brown.
Abdomen: Non-distended, non-tympanic with positive bowel sounds. The uterus is non -palpable. There is a large area of erythema noted in the suprapubic area with associated tenderness. A single circular 4mm burn with eschar is noted 7.5cmm inferior to the umbilicus.
Genital/Pelvic: Deferred at patient request (follow-up ob-gyn exam to be scheduled) Upper Extremities: No gross deformity. Warm and well perfused with good bilateral peripheral pulses. Fingertip erythema noted over mid-portion Left Humerus. Numerous areas of fingertip bruising. As with back and chest, these range from black to brown. Right extremity and balance of left extremity have a similar appearance. In addition, there are a total of 9 (4 right arm and 5 left arm) 5mm circular scars (cigarette burns) consistent with old healed 2nd-degree burn.
Lower Extremities: Warm and well perfused with good bilateral peripheral pulses. No gross deformity, no shortening or external rotation of leg when supine. SLR (Straight-Leg-Raise) negative left and right. Again, numerous bruises of various colors left and right over the Anterior Tibia. Abrasion and erythema with underlying edema (swelling) and tenderness left mid anterior tibia. No crepitus.
Neurological: Cranial and Spinal Nerves intact by exam. Gait not tested until post-X-ray due to painful weight-bearing.
Psyche: Cooperative, minimally conversational with direct query. Flat affect with overt signs of Depression with Anxious Mood
Labs:
1)Urine HCG (pregnancy test) negative
2) Urinalysis 2+blood and numerous WBC (white blood cells), with numerous motile trichomonads (trichomoniasis)
3) CBC, CMP WNL (Within Normal Limits)
Imaging:
1) Head CT w/o contrast: small 2 mm LEFT tempo-parietal subdural hematoma. No other acute pathology but there is scattered parenchymal (brain tissue) scarring consistent with old microbleeds. No facial/nasal/orbital fractures seen.
2)Left Tibia/Fibula X-ray: No acute bony or soft tissue abnormality seen. Evidence of old, healed nondisplaced fracture anterior tibia.
3)Left Humerus X-ray: spiral fracture mid humeral shaft with no angulation and good apposition.
4)Chest X-ray with Right Rib detail: Acute nondisplaced fractures right ribs 3-5. Old rib fractures noted in various states of healing R ribs 3,5,6 and L ribs 4-7. No pneumothorax, no acute cardiopulmonary process.
DX: 1) Traumatic Subdural Hematoma
2)Abdominal Contusion
3)Contusion Left Tibia
4) Spiral Fracture
5) Nondisplaced fractures R ribs 3-5
6) Trichomoniasis
7) Amenorrhea
8) Acute on Chronic Depression
*****Symptom Cluster suggestive of Domestic Abuse*****
Consult: Social Services
Hospital Administration on Call
Hospital Security
Additional History: Patient is presented with diagnosis and informed of concerns regarding potential abuse scenario. Patient denies abuse and asks to see her partner. Security is sent to the parking area to retrieve partner. When security approaches partner’s vehicle, he speeds from the parking lot.
When the patient is informed of partner’s departure, she becomes tearful and agrees to update history.
Patient and partner were introduced at a local bar and began dating three years prior. Both shared a common bond of having dropped out of high school. Her partner was a laborer at a local scrapyard. Patient clerked at a local department store while taking night courses to finish high school. She admits to social drinking while her partner was a moderate to heavy drinker given to occasional binging. They moved in together and shared rent until he told her he would leave unless she quit her job and high school completion courses. When the patient’s family complained, he forbid her to have personal or telephone contact with her family. Her partner was involved in a physical altercation at work and was taken to the E.R. for treatment of injuries. Employer mandated testing was positive for alcohol and cannabis, at which point he was discharged from his job. At this point, he increased his alcohol intake and began an escalating pattern of abuse. He forced her to sell her car to pay rent, utilities, and grocery expense but placed the proceeds in his checking account. At this point, the patient informed her partner that she was pregnant and he beat her violently for the first time. Punching her repeatedly in the abdomen until she passed out from pain. The patient subsequently miscarried. Patient packed clothes and was leaving with a friend. Partner blocked driveway and tearfully apologized. Over the protests of her friend, she agreed to remain with him. Partner encouraged her to take a cleaning job at a local business but confiscated her checks forcing her to bring peanut butter sandwiches to work for her lunch. He refuses to allow dental visits due to cost and forbids the use of oral contraceptives because it will encourage her to be promiscuous at work. When she returns home from work and finds him in bed with a female neighbor, he states that he did it to show her what would happen if she were unfaithful. Shortly thereafter, the patient developed a frothy malodorous vaginal discharge, itching and pain with intercourse.
Emergency Department TX:
I.V. of normal saline @ 100ml/hr
Flagyl 500mg PO (by mouth) for Trichomonal Vaginitis
Splinting, sling left arm for Humeral Fracture
Consults: Presented patient history and physical to Hospitalist at a tertiary medical center. Documented acceptance of patient and arranged transport.
Disposition: Patient is transferred by ALS Ground (Advanced Life Support Ambulance) to tertiary care medical center where she was admitted to Neuro-Surgery for observation of her brain bleed with consults to Orthopedics, Ob-Gyn, and Social Services.
Notification of local law enforcement regarding high index suspicion of domestic assault
The fictitious chart above is NOT an exaggeration:
Physical Injuries:
U.S. Department of Health and Human Services reports that domestic violence is the cause of more injuries in women ages 15 to 44 than all other injuries combined with more than 1 million women per year seeking care in the E.D. One fourth of these women will require admission, and greater than one in ten will require major medical treatment. Nearly 4 million women are beaten in their homes every year. ONE IN FOUR women will experience domestic violence in her lifetime.
The above patient has evidence of significant physical abuse.
Bruises: direct trauma to the skin appears first as a bright red area and over the course of a 10- day period the color of the injury progresses from black to brown as noted above. This allows the injury to be aged. Numerous bruises of different colors indicate a pattern of continuing abuse.
Fingertip bruises are a result of the very common grasp injuries used to control the abused woman.
Burns: numerous 4mm circular injuries/scars in various states of healing indicate cigarette burns. These are commonly inflicted as punishment. Arm burns are common. Burns near the genitalia establish complete dominance and maximum humiliation.
Head Trauma: You will recognize the epidural hematoma from a previous posting. The patient’s Head CT also showed evidence of scaring indicating a pattern of repeated blows to the head over time. The eardrum scars revealed blows forceful enough to cause rupture of the eardrum. The patient has several chipped teeth indicating repeated blows to the mouth over time.
Fractures: The X-rays Physical exam revealed an old nasal bone and septal fracture. Multiple rib fractures both new and in various states of healing support ongoing abuse. The spiral fracture of the Humerus (upper arm bone) is a result of grasping and rotational stress and is a classic abuse fracture. The fingertip erythema (fresh injury) combined with this fracture is considered abuse until proven otherwise. The healing/healed fractures on the patient’s tibia (shin) suggest she has been struck repeatedly with a hard object (steel toe boots or a club of some kind.)
Abdominal Injury: The blows to the abdomen represent the abuser’s attempt to terminate a perceived pregnancy due to the patient’s lack of menstrual cycle.
Emotional Abuse:
The effects of emotional abuse, while invisible, are no less devastating. Abused women have a markedly increased incidence of substance abuse including smoking. Low self-esteem and a feeling of hopelessness lead to loss of educational, relationship, and educational opportunities. Abused women have a fivefold increased risk of anxiety and depression.
Financial Abuse:
The abuser generally denies the woman access to finances which restricts access to dental/health care, work-appropriate clothing and personal care items necessary to secure quality employment.
Social Abuse:
The abuser generally restricts access to family, friends, social outings and even media information to limit the possibility of abuse exposure.
General Health Abuse:
Abusers generally engage in behavior which can have profound negative effects on the abused woman. A preponderance of abusers lack even a high school diploma and consider an educated or trained female a threat. Even the educated abuser fears the empowerment of a woman with a marketable skill. Generally speaking, domestic abusers are substance abusers exposing the woman to the hazards of their impaired driving, the violence of their drug suppliers, and the ramifications of their frequent brushes with law enforcement. The “risk-taking” behavior of the abuser will also frequently put the woman at risk for both minor and serious sexually transmitted disease.
Women at greatest risk for injury from domestic violence include those with male partners who abuse alcohol or use drugs, are unemployed or intermittently employed, have less than a high-school education, and are former husbands, estranged husbands, or former boyfriends of the women.
Having said this, there are lawyers who beat their Ph.D. wives, physicians who manipulate their girlfriends, college professors who take advantage of their students, and politicians, actors and director/producers who use their power to exploit women.
I hope this response will further heighten awareness of this epidemic and as a positive side effect provide some insight in depicting these characters in your writing.
Thank you for your indulgence. I promise next week’s trio of postings will be a return to Doctor Fiction’s usual mixture of banter, brilliance, and bullshit.
The Doctor is In. Want to ask a question? Read the guidelines first.
199 notes
·
View notes
Note
I have characters hiding in the wilderness with limited supplies. Would it be possible to use human hair for stitches on a bad cut?
A gut e string has a diameter of .58 mm2-0 chromic collagen gut suture has a diameter of .35 mmTensile strength of gut e string straight .20kgTensile strength of 3-0 collagen gut
Tensile strength of horsehair straight line 0.585kg (meets U.S. Pharmacopia Standards)
Tensile strength of horsehair knot 0.399kg (meets U.S. Pharmacopia Standards)
Your question brings to mind the time that I carved a five-inch gash in my thigh with a chainsaw. Being too embarrassed to confront my comrades in the emergency department, I forced my significant other to first assist while I did a 3-layer closure in the barn. You can improvise, but I now longer wear shorts.
In an ideal world, Jerimiah Jones and Grizzly Adams would have thought to bring a first aid kit with suture material and needle. Apparently. your guys bugged out in a hurry and are laying low. So, we will help them improvise.
Since you used the word “bad,” I assume we are repairing a serious laceration, which will require a two-layer closure. This happens when the wound is so severe that it hangs open requiring “inside” and “outside” stitching.
The” inside” stiches have to be strong enough to hold the wound together, while the “outside” stitches just approximate the skin edges until they can grow back together. The interior sutures needs to be absorbed by the body, while the skin sutures are snipped apart and pulled out when the skin has resealed.
For many years, the ideal inside suture was made of ultrathin strips of collagen from cattle or sheep intestine twisted to a single filament. This strand was very strong yet would dissolve in a matter of 3—45 days. This suture did all the work, while the outside suture merely “sealed the deal” These were called catgut sutures. They were not really catgut but cattle/sheep gut. They were first called kit gut, because gut was also used for a small fiddle called a kit. This eventually became catgut.
Which brings me back to your intrepid mountain men, one of which should certainly have a violin. That violin should have a gut E string.
A gut E string has a diameter of .58mmThe tensile strength of a gut E string is 0.20 kgA standard 2-0 gut medical suture has a diameter of .35mmThe tensile strength of a standard 2-0 gut is 0.12kg
This is the amount of straight-line weight the suture can tolerate before breaking.
The fiddle string will be your internal suture.
Now for the human hair suture issue. We will assume that your characters do not have a fishing kit with nylon line which would be excellent closing suture.
A recent study compared horse hair and 4-0 Prolene (monofilament nylon) sutures. I commonly use 4-0 Prolene for light skin closure in the Emergency Department.
Horse hair diameter 0.19mmTensile strength 0.585kg4-0 Prolene monofilament suture 0.19mmTensile strength 0.592kgHuman hair average diameter is 0.07mmTensile strength 0.113kg
The human hair is too thin and lacks the tensile strength to be used as anything but an ocular suture.
The horsehair and the 4-0 Prolene had near identical tensile strength and equal performance as suture material.
If you don’t have a sewing needle, you can fashion a workable needle from the thorn of a Hawthorn tree. Select the smallest diameter thorn you can find and use a second thorn to create an eye for your needle. Sterilize your needle, and both suture materials in iodine or rubbing alcohol if available. If not, the highest proof booze will work and as fallback, soap and water with a rinse. The infection risk increases as you move down the chain, but as “The Duke” would say, “A man’s gotta do what a man’s gotta do”
Remember: Removal times vary.
Face 3-5 daysScalp 7-10 daysArms/Legs 10-14 daysJoints 14 daysTrunk 10 days
The tensile strength of a possum hair is…

(x)
The Doctor is In. Want to ask a question? Read the guidelines first.
1K notes
·
View notes
Note
At what point is an untreated concussion from, say, a fall in a fight debilitating if the character is really active while leaving it alone?
As a writer, you have many TBI (Traumatic Brain Injuries) to choose from. The effect can be anything from, “It’s nuttin,” to “He’s dead Jim.”
Concussion are graded 1 – 3 in increasing severity.
Grade 1 No LOS (loss of consciousness) with symptoms gone in 15 minutesGrade 2 No LOS and symptoms longer than 15 minutesGrade 3 LOS for even a few seconds
The character you describe will be grade 1 or grade 2, as grade 3 is usually incapacitated immediately. A grade I or 2 could have symptoms of headache, blurred vision, nausea, dizziness, or confusion lasting as long as you need it. Symptom onset will probably be within moments for a concussion. Think of concussion as something that effects a widespread area of the brain and gives the victim the generalized symptoms above.
You may want to consider contusion or “brain bruise.” This causes a more localized symptom due to mild to severe brain bleeding and swelling. Like a bruise on your arm or leg, but in an enclosed space. These symptoms are sometimes somewhat slower in onset, longer lasting andoften more specific and dramatic. They include difficulty moving a specific body part, difficulty understanding speech or speaking, and memory loss.
Moving up the scale, you might want to choose an epidural or subdural hematoma (bleed.) The brain is covered by a thick membrane that lies between the brain and the skull. It is called the dura. The major arteries that supply the brain are between the dura and the skull. When one of these is torn, they bleed quite rapidly with the onset of symptoms in seconds to a few hours.
These are catastrophic and have a very high mortality rate if not treated surgically. Your fighter could go out in seconds to minutes but he’s going to stay that way without treatment.
The last thing to consider is the subdural. These are the smaller vessels that the epidurals feed. They lie between the dura and the brain. The onset of symptoms is generally much slower, days to even weeks. While occasionally fatal, they can resolve spontaneously leaving zero to varying permanent symptoms. These are very common in people who fall or are struck a lot. If your character is an alcoholic, he is the perfect set-up for a subdural.
You can use the spectrum of injury above to design the time of onset, specificity, severity and permanency you need for your character.
See the Mechanism of Concussion here.

The Doctor is In. Want to ask a question? Read the guidelines first.
112 notes
·
View notes
Note
Hello! my character wanders the Canadian wilderness, in December, in an area of around 0 to -5 Celsius, with no pants or shoes. She has a big thick ski jacket that hits mid-thigh, and a fleece underneath. what's her timeline for losing toes/ect?
This is a great question and the premise you have established is compelling.
Why is this character wandering in the “Great White North,” clad in only knee length ski parka and fleece?
The short answer to your question is: At an effective temp of 0 Celsius, frostbite could occur on bare feet in less than 30 minutes. Wind and or moisture could cut that to as little as 15 minutes. If your pre-story includes alcohol, barbiturates, opiates, or benzodiazepines (Prince Valium), the time could be cut to 10 minutes.
Frostbite does not necessarily mean gangrene and tissue loss. Give this beautiful barefoot girl 2-3 hours at 0 Celsius, wet or snow-covered ground, and a 20 KM/HR wind and she can progress to frozen toes in half that time. If the character has diabetes, Raynaud’s Phenomenon/Disease, or a previous frostbite, the tendency to severe and permanent damage is greatly increased.If your character is compos mentis there are measures, she could take to decrease risk.
Assuming she does not have to keep moving to avoid capture, she can seek a wind protected, dry area, and if possible, build a fire.
Your hypothalamus has a thermostat that wants to keep your core temperature at 37C (That’s 98.6F if you live in Detroit instead of Windsor.) As a matter of survival, your hypothalamus will decrease blood flow to your fingers/ nose, penis/toes, to maintain that temp. So, if Barefoot can find dry, calm and start a fire to warm her core, she can stave off the frostbite.
Exercising a frostbitten part to warm it up is an ABSOLUTE no-no. The ice crystals in the frostbitten area literally grind the tissue. So, if she keeps walking on numb feet…
I hope this helps. You have put your character in a horrible position—What more could we ask for?

The Doctor is In. Want to ask a question? Read the guidelines first.
61 notes
·
View notes
Note
I need a character to be both shot in a meaningful way but useful for the rest of my book's climax. Where can I shoot them and how many times without them dying from blood loss. Is that even a thing?
When I was a surgical resident at the Knife and Gun Club in Brooklyn, I had the honor of treating a young male who welched on a bet with his “made” bookie. The bookie did not want to kill his clients as that tends to render the debt uncollectable. Fiduciary concerns dictated that he educate rather than eradicate his past due clients. He carried a .25 ACP semi-automatic pistol and a much larger 45 ACP. As he was in collection mode, the bookie shot this particular client 4 times with the 25 ACP. Being a scholar of gunshot, his ammunition of choice was a round with 50 grains of powder, a weight of 2 grams, and a velocity of 230 meters/second. The bullet has a round nose and generally does not fragment.
Kinetic Energy (KE) = 0.5 x mv2
Where:
m equals mass (kg)v equals velocity (meters / second)
Soooo…
(KE) = 0.5 x (.003kg) x (227 meters / second)2(KE) = 0.5 x (.003) x (51,529) = 77.3 JWhere:1 joule equals 1kg*m2s2
To put this in perspective, the 45 ACP pistol round contains 185 grains of powder, weighs 15 grams and has a velocity of 260 meters/sec.
(KE) = 0.5 x (0.015kg) x (260 m/s) 2(KE) = 0.5 x (0.015) x (67,600) = 507 J
Orrrr… nearly 7 times the kinetic energy of the .25 ACP
This is important because the damage done to the human body is directly proportional to the amount of kinetic energy delivered. When a bullet has low KE, the damage is done mostly (may I use an ly adverb?) by penetration. When a bullet has high KE, the damage is exponentially increased by the hydraulic shock of all that KE. being dissipated in a fluid medium. A huge shock wave displaces fluid, shatters organs, ruptures vessels, creates a large entry wound and an even larger exit wound.
So, if you want the debtor is just a “slow pay,”, a few well chosen shots from a .25 will send the message, whereas, if the debt is deemed uncollectable, a single shot from the .45 ACP will close the account and deter others from total non-payment.
Back to to our young scuffaw. He was shot 4 times with the .25 ACP. Fortunately, it was February and he was wearing heavy clothing. Shot one went through a heavy padded canvas coat, wool sweater, flannel shirt cotton undershirt, and thermal long johns. The bullet entered his left side, glanced off a rib and lodged in the intercostal muscle between ribs 5 and 6. Painful, but not life threatening. Shot two struck the patient in his left buttock as he turned to run. It traversed the more than ample fat of his behind, barely penetrating the fascia of the Gluteus Maximus. Tender with every step, but treatable. Shot three was the most serious and could have been fatal if left untreated. As the patient ran, he was struck in the back. The bullet entered between right ribs 5 and 6, penetrated the intercostal muscle and nicked the right lung, causing a pneumothorax and necessitating a chest tube to inflate the collapsed lung. Shot 4 was the most interesting. The shootee was now 15 - 20 feet from the bookie. The “lucky” shot struck him in the back of the head, high on the right parietal bone. Its KE spent, the bullet penetrated the skin and tracked along the outside of along the skull, coming to rest in the middle of the patient’s forehead under the skin. Embarrassing but easily removed through a half inch incision with mosquito forceps. Any of these shots may well have been fatal if fired from a 45 ACP. As it was, the patient’s chest tube was removed in two days, he was discharged on antibiotics and able to return to gambling and his job at the Fulton Street Fish Market in less than a week.
Determine the amount of damage you wish to inflict on your character and choose caliber of weapon and placement of shot to achieve your goal.
The Doctor is In. Want to ask a question? Read the guidelines first.
125 notes
·
View notes