
juniperpublishers-ecoa-blog
Juniper Publishers | ECOA
Juniper Publishers : Ecology and Conservation Science: Open Access is an Interdisciplinary
Journal publishes papers examining the complex and varied systems
43 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs

theobviousparadox
Random musings of a wannabe writer.

krnst4r
mike !!

behavioraleconomics
behavioral economics情報収集

imbalonely-blog
Rants

mateagracia-blog
Untitled
Text
Combination Of Oncolytic Newcastle Disease Virus (Ndv) and Vaccine Vector Adenovirus (Adv) as a Potential Virotherapy for Cancer: A Systematic Review | Juniper Publishers
Juniper Publishers-Open Access Journal of Anatomy Physiology & Biochemistry
Authored by Ferbian Milas Siswanto
Abstract
Cancer is a disease with high morbidity and mortality, one of the leading causes of death in the world. Nowadays, the foremost clinical cancer therapy in a patient are surgery, chemotherapy and/or radiotherapy. Despite of the great amount of research on cancer and advance technology in medicine, the mortality rate of cancer remain high due to limited therapeutic effects and additional side effects of current therapy. Here we provide an overview on the virotherapy using the combination of Newcastle disease virus (NDV) and the adenovirus (AdV). Both NDV and AdV possess an oncolytic activity and a potential as vector vaccine. However, oncolytic activity of NDV is more potent than adenovirus. In contrast, the AdV potential as a vector of cancer vaccines is better than NDV. Therefore, in this paper, we discuss the development of a virotherapy combination by utilizing oncolytic activity of NDV, and vaccine vector AdV simultaneously for cancer therapy to improve the effectiveness of therapy against cancer.Conclusion: Decreased estrogen level following ovariectomy causes osteoporosis.
Keywords: Newcastle disease virus; Adenovirus; Virotherapy; Cancer
Abbrevations: NDV: Newcastle Disease Virus; AdV: Adeno Virus; VVND: Velogenic Viscerotropic Newcastle Disease; PBMC: Peripheral Mononuclear Cells; HN: Hemaglutinin-Neuraminidase; TRAIL: TNF-Related Apoptotic-Inducing Ligand; JNK: c-Jun N-terminal Kinase; NOS: Nitric Oxide Synthase; dsDNA: Double-Stranded DNA; NK: Natural Killer; CAE: Carcioembryonic Antigen; TLRs: Toll like receptors
Introduction
Cancer is a disease with high morbidity and mortality that leads to death. Until now, cancer is still the leading cause of death in humans. In 2012, approximately 14.1 million cases of cancer have been reported worldwide, and have caused the deaths of 8.2 million people (about 15% of all deaths). It is characterized by uncontrolled cell division, invade surrounding tissue, and metastasize to other organs in the body. The four most commonly reported cancers are lung, breast, colon, and prostate cancer. However, all organs in the human body can be cancer regardless of age, gender, ethnicity, diet, and environment [1]. Generally, cancer is caused by decreased cell death or increased cell proliferation. In other words, any dysregulation of cell cycle or apoptosis will result in uncontrolled cell growth or malignancy [2].Cancer occurs due to genetic and environmental factors that cause deviations in the growth regulation of stem cell populations. Improving knowledge of the molecular processes underlying cancer development, as well as advances in diagnostic techniques, radiotherapy technology, and chemotherapy, has increased the survival rate of cancer patients. However, recent therapy has not greatly improved the survival of cancer patients who have undergone metastasis. Although modern technology has been developed, cancer is still afflicted millions of people worldwide [3]. This is because, in addition to the limited therapeutic effects, radio and chemotherapy also cause side effects [1]. The ideal cancer therapy is a therapy that selectively kills malignant cells, and does not damage other normal cells in the body. Currently, radiotherapy, chemotherapy, and surgery are the most common modalities in cancer therapy. However, these therapies often cause harmful side effects [4] and often lead to resistance [5].Therefore, the development of cancer therapy with high effectivity and selectivity for cancer cells with minimum side effects becomes crucial. The idea of using bacteria and viruses to treat malignancy in humans began in the mid-1800s in which tumor regression was associated with bacterial and viral infections [6]. The development of cell culture technique and virus technology in the early 1950s led researchers to learn more about the potential of viral therapy in human and small animal tumors [7]. The virus is then proven to be useful as an oncolytic agent and immunostimulator. Newcastle disease virus (NDV) that naturally infected poultry, and adenovirus (AdV) that causes human flu, is a potential viral combination as a virotherapy and immunotherapy agent. NDV can directly kill cancer cells (oncolytic activity) and adenovirus can help to stimulate the immune system to recognize cancer cells (immunostimulator activity).
Newcastle Disease Virus (NdV) as an Oncolytic Agent
Newcastle Disease Virus (NDV) is a virus of the order Mononegavirales because it has single strand RNA, negative polarization, unbranded and linear genome [8]. Furthermore, this virus occupies the family of paramyxoviridae due to its pleomorphic envelope, round-shaped with a diameter of 100- 500nm, but some are in the form of filaments [9]. This virus causes Newcastle disease that attacks various poultry, especially chickens. Until now, Newcastle disease has been found in various parts of the world including Indonesia, and the cases of velogenic viscerotropic Newcastle disease (VVND) have been reported in Indonesia [10]. In Indonesia, Newcastle disease is endemic as indicated by the finding of this case throughout the year [9].NDV was firstly reported to possess an oncolytic activity in the mid-1950s [11]. The clinical evaluation of this virus as an anticancer agent over the last few decades shows its safety and effectivity. The effectivity of NDV application is based on high oncolytic activity, and safety of its use is based on replication that selectively attacks tumor cells and does not damage normal cells. Scientists are interested in the use of NDV because it replicates more rapidly in tumor cells than normal cells in humans, and cause oncolytic effects [12]. NDV replicates 10,000 times faster in cells undergoing neoplasmic changes than normal human cells in general [13,14]. There are several molecular pathways that cause the oncolytic effects of NDV, such as apoptosis pathway [1,15]. Induction of apoptosis by NDV includes a series of virus entry processes, replication, de novo protein synthesis and activation of caspases [16]. NDV induces apoptosis through both extrinsic and intrinsic pathways.NDV-induced apoptosis is generally mediated by intrinsic pathway during the late stage of infection, while in the early stage of infection is more likely to be mediated by extrinsic pathway [17]. Activation of intrinsic pathway involves the increased activity of p53 and Bax proteins, as well as decreased expression of the Bcl-2 gene [18] which will activate the Caspase 9. The matrix protein (M protein) of NDV binds to Bax protein and increases apoptosis [19]. Whereas, the extrinsic pathway of apoptosis is induced by NDV-mediated activation of pro-apoptotic cytokines such as IFN-α and TNF-α in peripheral mononuclear cells (PBMC) via its Hemaglutinin-Neuraminidase (HN) proteins [20,21]. The HN protein of NDV also induces expression of TNFrelated apoptotic-inducing ligand receptor (TRAIL) [22,23] which further activate caspase 8 [17]. A study has shown that NDV initiates the synthesis of nitric oxide synthase (iNOS), thus increasing apoptosis via the NFκB pathway [24,25].NDV-infected mouse PC12 pheochromocytoma cell was proved to induce the activation of reticulum endoplasma eIF2a kinase (PERK) resulting in phosphorylation of eIF2a and caspase 12 activations. Endoplasmic reticulum stress may be responsible for the activation of apoptotic pathways in cancer cells infected with NDV [26]. In addition, the induction of the external pathway by NDV also the activation of c-Jun N-terminal kinase (JNK) and p38 pathways, and decreased Akt pathway activity [27]. NDV has an excellent potential as a highly selective virotherapy candidate. This selective effect arises because of the restriction of V protein by host and secretion of virus-induced cytokines (IFN-γ and TNF-α) [28]. The first step of infection by NDV occurs in all types of cells in the body, while the second step (associated with viral replication) occurs only in tumor cells because this stage is terminated very quickly in normal cells [5]. In general, the specificity of NDV to cancer cells occurs because of damage to antiviral pathways and apoptosis in cancer cells [29].In addition to direct cytopathic effects, NDV anti-cancer activity is associated with the activation of both innate and adaptive immune responses. NDV infection initiates the macrophage-induced synthesis of enzymes that increase antitumor activity in both in vitro and in vivo studies [30]. NDV stimulates monocytes that play a role in killing tumor cells via TRAIL induction [31]. The activation of natural killer (NK) cells is also involved in the cytotoxicity mediated by NDV [20]. However, to induce host immune system, the use of cancer vaccines is believed to have far more effective effects than the immunostimulator effects of NDV. The immunotherapeutic approach aims to promote the host antitumor immune response that can destroy tumor cells in both primary and metastaticaffected sites [32]. Genetic therapy-based cancer vaccination technology has been widely developed, with the virus being the most popular vector studied. Adenovirus, in addition to having oncolytic activity, is a very potential and widely used vector on cancer gene therapy and as a vaccine to express foreign antigens [33].
Adenovirus (AdV) as a Vaccine Vector
Adenovirus is a group of viruses from the Adenoviridae family responsible for 5-10% of upper respiratory infections, gastroenteritis, conjunctivitis, and cystitis (CDC, 2015). It has no envelope, icosahedral capsid with a diameter of 70-90 nm and the double-stranded DNA (dsDNA) [34]. Adenovirus has long been used as a vector for gene therapy due to its ability to influence cell biological activity, tolerate large genetic modifications, and encode proteins without integrating into the host cell genome. More specifically, the virus is used as a vector for administration of therapeutic targets, either in the form of recombinant DNA or proteins [35].Several studies using various antigens proved that adenovirus (AdV) is potential as a vector of cancer antigens such as glycoprotein 33 (GP33) from lymphocytic viral choriomeningitis [36], carcioembryonic antigen (CAE) [37], beta-galactosidase antigen [38], GM-CSF antigen (such as T-VEC and Pexa-Vec) [39], E7 antigen from human papillomavirus [40], the gp100 antigen and TRP-2 antigen [41]. It may enhances cellular immunity mediated by T-cell CD8+ cells and IFN-γ- mediated humoral immune specific to cancer cells. The use of AdV as a vaccine vector is relatively safe to use with intradermal methods [42]. Adenovirus administration may stimulates ligand expression of Toll-like receptors (TLRs) and may alter cancer immunosuppressive and proinvasive microenvironment becoming proinflammatory, thus facilitating immunocompetent cells to fight against cancer [39,43,44].
General Perspective
Both NDV and AdV have oncolytic activity and potential as vector vaccine for cancer. However, oncolytic activity of NDV is more potent than adenovirus. In contrast, the AdV potential as a vector of cancer vaccines is better than NDV. Therefore, the development of a virotherapy combination by utilizing oncolytic activity of NDV, and vaccine vector AdV for cancer simultaneously are expected to improve the effectiveness of therapy against cancer. The use of an appropriate combination ratio of these two agents will improve their therapeutic potential for cancer [45,46].
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Anatomy Physiology & Biochemistry please click on: https://juniperpublishers.com/apbij/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/apbij/APBIJ.MS.ID.555649.php
35 notes
·
View notes
Text
Observational Study: Cancer Cases Treated with Homeopathy in the Basque Country/Navarre between 2013 and 2015
Juniper Publishers-Open Access Journal of Complementary Medicine & Alternative Healthcare
Authored by Victoria Claramunt Palou
Abstract
The Study included 50 women and 15 men aged between 11 and 85 years. There we 44 patients with advanced tumour disease and 21 with early-stage disease. Conventional cancer treatment was chosen by 64 patients and one of them chose homeopathy only. Four patients made important changes in their lifestyle, and 8 had bio-decoding sessions. All patients had taken homeopathic medicines as palliative care tailored to different stages of their disease. A single drug treatment was used in 18 cases, based on the entire case. Ten cases we treated by applying Banergi protocols and constitutional medicine, and 37 cases were treated with different successive or combined drugs, depending on the state of the patient at the time, with the Minotti protocol for palliative care being applied in 9 cases. The predominant homeopathic dilutions were centesimals. The great variability of medications used on each of the patients shows the individuality of patient symptoms with the same clinical diagnosis, as well as the great variability in the criteria of homeopathy doctors when establishes a therapeutic strategy.Homeopathy has helped to control the tumour disease (patient free of disease) in 10 cases of early stage cancer and 12 cases of advanced tumour disease. Homeopathy was only palliative in 7 cases of early-stage cancer, in 22 cases of advanced tumour disease, and in five other cancers without staging. Homeopathy did not work in one case of early stage cancer, in two cases of advanced tumour disease, and in one case without staging. There were 5 cases in which results could not be assessed at the time of the study. According to the subjective assessment by the homeopathic doctor, homeopathy contributed to the control of tumour disease (patient free of disease with biological and /or imaging tests) in 22 cases, it was palliative in 34 cases, 4 patients died, and 5 cases cannot yet be evaluated. According to the assessment by the patient, it helped to control and improve their quality of life in 55 cases and it does not help them at all in 5 cases. This observational study has enabled us to evaluate the effectiveness of our work in the context of our clinical reality and more accurately describe all parameters involved in the case, including conventional treatments and their impact. Patient opinion is part of the evaluation of the results and requires questionnaires that can be adapted and standardized. Homeopaths carry out their work within an ethical framework bound by civil responsibility and respect for patient autonomy, open to collaboration with the work of the other professionals with a common goal, which is none to cure, relieve the patient, and contribute to the advancement of knowledge.
Keywords: Advanced tumour disease; Early-stage disease; Lifestyle; Bio-decoding; Palliative; minotti protocol; Patient free of disease; Staging; Standardized
Introduction
Homeopathy exercised by doctors is abided to a deontological code common to the medical profession and to a social responsibility setting established by law. Moreover, we homeopath doctors respect the patient’s autonomy and do not compete with other therapeutic possibilities. We homeopath doctors are willing to collaborate with other medicine professionals and to equip ourselves with investigation and evaluation tools that will permit progress of the scientific knowledge.What does homeopathy offer to oncology patients?Active listening, reflection scenarios, full symptomatic patient treatment and use of medicines with few and reversible adverse effects compatible with chemotherapy, radiotherapy and hormonotherapy. Another, not least important aspect is that a homeopathy treatment is short and inexpensive.Reflection scenario: raising awarenessThese four questions open a therapeutic space of active listening for the patient and the doctor (Figure 1). The patient evolves from being a case of adenocarcinoma to being an ill individual to whom we intend to help by searching for the most accurate medicine that suits him, his suffering and the tumor. The patient must understand his vulnerability and those facts, emotions or ways of life that make him sicken. For that he is given a reflection space. We do not speak about statistics or predictions. We commit ourselves to him, to help and attend his needs. Undoubtedly, in our job as homeopath doctors this active listening is part of our therapeutic grounding.Approaching the oncology patientThe oncology patient is a complex one. Besides his natural illness (the tumor), he also presents an artificial sickness derived from the adverse effects of his oncological treatment. Moreover, the impact of the diagnosis as well as the disease prognosis that, just by themselves, many times destabilize the patients, must be also be considered. For the homeopath, restoring the mental and physical equilibrium of the patient is a priority. Help him bear the treatments, make him lead the processes and maintain the hope alive, are also essential. In this case, a respectful atmosphere for cooperation would be the ideal for the patient and the treatment’s result.
Observational Study (Appendix 1)Samplea.
65patient cases with different cancer diagnosis are collected at homeopath consultations in the Basque country/ Navarre during the period 2013-2015.b. Monitoring for 18 of the cases has been done at a health public service (primary attention) as for the rest 47 cases monitoring has been done at private consultationc. Patients from both sexes: 50 women and 15 mend. Ages between 11 and 85 years olde. A total of 44 patients present an advanced tumor diseasef. 21 patients present the disease in an initial localized phase
Diagnoses
Table 1 shows the diagnoses along with the correspondent phase and number of cases. Simultaneous treatments to the homeopathy treatment (Table 2).Common treatmentCommon treatment includes a combination of different procedures in which following different protocols, chemotherapy, radiotherapy, surgery and hormonotherapy can be combined for a healing or palliative purpose.Lifestyle changeLifestyle changes include change processes in habits such as diet or tobacco consumption, as well as changes in work, personal or family relations starting by a conflict awareness raising from the patient.
Biode Coding
Awareness raising and emotional unloading in relation to the conflict that unleashes the disease following a specific technique.Used strategies at the homeopathy consultationa. All sample patients have taken palliative treatment adapted to various disease stages.b. Patients given a single medicine base on the situation and patient’s constitution: 18 cases.c. Banergi protocols and patient constitution based medicine: 10 cases.d. Other combined or successive medicines adapted for the patient: 37 cases.e. Minotti’s protocol (PAC): 9 cases.
Potency usage in prescriptions
Table 3 shows the prescribed potencies. The homeopathic medicine stimulates the healing capacity of every patient. Moreover, it also, at the same time, acts in the mental, emotional and physical areas. It is this aspect to which we refer when we speak about totality. The homeopathic medicine is compatible with other treatments and has few adverse effects. The great variety of the medicines used in each patient expresses the symptom individuality of the patients with the same clinic or anatomopathological diagnose. Also, expresses the great criteria variability of the homeopath doctor when establishing a therapeutic strategy.*Solution to the following medicines: ADN 6 CH, Hepatine 6 CH, Bone marrow 6 CH, Cardine 6 CH, Anilium 6 CH, Hairy Cranium Area 6 CH (Dr. Minotti’s formule).
Homeopathy effectiveness estimation at the case management
Homeopathy has contributed to control the tumor disease (free of disease patient) at the following cases (Table 4):a. Localized tumor disease (N0, M0): 10 casesb. Advanced disease (from phase II onwards): 12 casesHomeopathy has turned out to be palliative only at the following cases (Table 5):i. Localized tumor disease (N0, M0): 7 casesa. Advanced illness (from phase II onwards): 22 casesb. Non-determined phase cases: 5 casesii. Homeopathy has not worked in the following cases (Table 6):a. Localized tumor disease (N0, M0): 1 caseb. Advanced illness (from phase II onwards): 2 casesc. Non-determined phase cases: 1 case (Table 7)iii. Efficacy estimation based on the doctor:a. Contributes to control the tumor disease (at the actual moment, free of illness patient with biopsy, image, scoreboards, endoscopy, etc. records): 22 cases.b. Contributes only to palliate the effects of the disease or treatment (chemotherapy and radiotherapy), quality of life, tolerance to adverse effects: 34 cases.c. Dead patients: 4 cases.d. Cannot yet be established if the treatment works: 5 cases.e. Treatment does not work: 4 casesiv. Effectiveness estimation based on the patient:a. Has helped to control and improve my quality of life during the treatment: 55 cases.b. Has not helped at all: 5 cases.c. Without opinion: 5 cases.
Used homeopathic medicines1) Constitution based medications:A. Natrum Muriaticum: 9 cases.B. Pulsatilla: 8 cases.C. Lachesis: 4 cases.D. Calcarea Carbonica: 4 cases.E. Veratrum: 2 cases.F. Staphisagria: 8 cases.G. Samarium: 1 case.H. Alumina: 1 case.I. Germanium: 1 case.J. Ustilago: 1 case.K. Sepia: 8 cases.L. Aurum Metallicum: 6 cases.M. Ferrum Phosphoricum: 3 casesN. Aconitum: 3 cases.O. Sulphur: 2 casesP. Aranea Diadema: 1 case.Q. Silicea: 1 case.R. Ignatia: 1 case.S. Argentum Nitricum: 1 case.2) Medicines in relation to the tumor disease:A. Conium Maculatum: 14 cases.B. Phytolacca: 10 cases.C. Kalium Carbonicum: 4 cases.D. Chelidonium: 3 cases.E. Hydrastis Canadensis: 3 cases.F. Asteria Rubens: 2 cases.G. Rhododendron: 1 case.H. Carcinosinum: 8 cases.I. Thuya: 9 cases.J. Kalium Bichromicum: 3 cases.K. Calcarea Phosphorica: 3 cases.L. Ruta: 2 cases.M. Carbo Animalis: 2 cases.3) Table 8 shows the medicines used with palliative purpose for:A. Radio dermatitisB. MucositisC. Nauseas and vomitsD. WeaknessE. SadnessF. FearG. SwellingH. Post-operativeI. AnemiaJ. LeukopeniaK. ThrombocytopeniaL. Helps to dieM. Dyspnea.
How can we know, with accuracy, the effectiveness of our intervention?
To us, homeopaths, can be reproached that we do not publish our results, which is true, we barely do it. The purpose of the homeopathy associations and academies, is to offset this reality raising awareness amongst our colleagues of the importance of recording the cases homogenously and of publishing clinical results, at least, in our magazines. Due to the nature of the homeopathic practice, we must also explore new designs to contrast our results. We must change the subjective assessment of our work with validated tools from the general medicine sphere such as the life quality tests proposed by the EORTC (European Organization for Research and Treatment of Cancer) and other tools proposed by the ECH (European Committee for Homeopathy). In one word, use the common language of science to contrast our results. We prepare ourselves to search a respectful collaboration with other medicine professionals that help patients from a conventional perspective. This is the propose of integrative medicine: the patient improves and the science makes progress [1-6].
Conclusion
At the presented sample, we are conscious that at the time of collecting the data, the free of illness patients still have a long journey of regular medical checks and that, at worse, they might present relapses of their tumor disease. Our purpose as doctors is to be available at this stage of the patients’ life. Nowadays, one of the cancer treatments objectives, in those cases in which the illness cannot be cured, is to make the disease a chronic one. In our sample, there are two patients that present this situation and undoubtedly, homeopathy along with other procedures (palliative chemotherapy, hormonotherapy, etc.) helps them to get along with their lives.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Complementary Medicine & Alternative Healthcare please click on: https://juniperpublishers.com/jcmah/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/jcmah/JCMAH.MS.ID.555726.php
26 notes
·
View notes
Text
The Prevalence of Bovine Trypanosomiasis in JabiTehnan District of Amhara Regional State, Ethiopia

Juniper Publishers-Open Access Journal of Cell Science & Molecular Biology
Authored by Melak Wondie
Abstract
Cross sectional study was conducted in Jabi Tehnan District of West Gojjam Administrative Zone of Amhara Regional State, Ethiopia to determine the prevalence of bovine trypanosomiasis. In the parasitological survey, blood samples of 164 cattle were examined using a buffy coat technique. The Packed Cell Volume (PVC) value of each animal was also measured using hematocrit reader. The overall prevalence of trypanosomiasis was found to be 15.24% and it consists of 9.76% and 20.73% in Adankegne and Ergib peasants’ association, respectively (X2=5.783, p=0.056). The most positive cases were due to Trypanosoma congolense (T. congolense ) (80%) followed by Trypanosoma vivax (T. vivax)(20%). The mean(PCV) values of parasitaemic and aparasitaemic animals during the study period were 20.75% and 25.07%, respectively. The variation in mean PCV values were statistically significant (p=0.01). The study also demonstrated statistically significant (X2=13.886, p=0.001) variations in prevalence between sexes of cattle, which were 10.67% and 19.1% in female and male animals, respectively. The present prevalent study generated valuable information on the epidemiology of bovine trypanosomosis in the study area and revealed that trypanosomosis was an important disease affecting the livestock production
Keywords: PCV; Prevalence; Trypanosoma congolense; Trypanosoma vivax; Bovine
Introduction
Livestock is backbone of the socio-economic system of most of the rural communities of Africa [1]. Ethiopia is known for its large and diverse livestock resource endowments. Livestock is primarily kept on small holdings where it provides drought power for crop production, manure for soil fertility and fuels, serves as a sources of family diet and sources of cash income (from sale of livestock and livestock products). Despite large livestock population, Ethiopia fails to optimally utilize this resource due to different constrains facing the livestock subsector. Shortage of nutrition, reproductive insufficiency, management constraints and animal disease are the major constraints [2]. One of the diseases hampering the livestock subsector is trypanosomosis [3]. Trypanosomosis is a complex disease of protozoa that is caused by different species of unicellular parasites (trypanosome) found in the blood and other tissues of vertebrates, including livestock, wild life and people [4]. Trypanosomosis limited to the extension of natural herds particularly in Africa were the presence of the tsetse fly density access to woodland and savanna areas with good grazing potential [3]. It is a serious constraint to agricultural production in extensive areas of the tsetse infested regions which accounts over 10 million squares of the tropical Africa [5].Ethiopia is one of the countries suffering from the impact of trypanosomosis. In Ethiopia, it is estimated that some 10 to 14 million heads of cattle and an equivalent number of small ruminants together with a significant number of equines and camels, are exposed to the risk of trypanosomosis [6]. Six species of trypanosomes are recorded in Ethiopia and the most important trypanosomes in terms of economic loss in domestic livestock are the tsetse transmitted species T. congolense, T. vivax and T. brucei [3].Tsetse flies in Ethiopia are confined to western and south-western parts of the country between 33°C and 38°C E longitude and 5°C and 12°C N latitude. It is estimated to cover an area of 140, 000, 220, 000 km2[7]. Tsetse infested areas follow the major river systems; namely, Abay (Blue Nile), Baro, Akobo, Didessa, Ghibe and Omo river systems [8]. Five species of Glossina (Glossina morsitans submorsitans, G. pallidipes, G. tachinozdes, G.f. fuscipes and G. longipennis) have been recorded in Ethiopia [3]. According to National Tsetse and Trypanosomosis Investigation and Control Center [7], tsetse transmitted animal trypanosomosis still remains as one of the largest causes of livestock production losses in Ethiopia. The effects of trypanosomosis is not only the direct losses resulting from mortality, morbidity, infertility of the infested animals and costs of controlling the disease, but also due to indirect losses, which include exclusion of livestock and animal power-based crop production from the huge fertile tsetse infected areas. Annual estimated losses for Ethiopia as a result of trypanosomosis is roughly $200 million, in terms of mortality and morbidity losses in livestock (excluding utilization of fertile land for crop and livestock production) and the costs included in controlling the disease [9].The most prevalent trypanosome species in tsetse infested areas of Ethiopia are T. congolense and T. vivax. Rowlands et al. [10] reported a prevalence of 37% for T. congolense in Southeastern Ethiopia. Abebe and Jobre [11] reported an infection rate of 58% for T. congolense , 31.2% for T. vivaxand 3.5 % for T. bruceiin Southern Ethiopia. In the same report it is also indicated that 8.71% infection rate was recorded in the highlands (tsetse free areas) of which 99% is due to T. vivax. Different workers [12- 14] indicated a prevalence of 17.2%, 21% and 12 % in Metekel district, in upper Didesa Valley and Southern Rift valley areas of tsetse transmitted regions, respectively, and the dominant species was T. congolense .In the western part of Amhara Regional State bordering the Abay river basin, one of the north western tsetse belt areas of Ethiopia, tsetse transmitted trypanosomes are becoming a serious threat for livestock production and agricultural activity in particular. Reports made by the Regional Veterinary Laboratory in 1999 indicated the presence of tsetse fly transmitted trypanosomosis in three districts of the region (Bure, Jabi Tehnan, and Ankesha) bordering the Abay valley areas. A preliminary survey conducted in Dembecha district by the Ethiopian Science and Technology Commission and West Gojjam Veterinary Office in 2001 indicated a trypanosome infection rate of 23% with a dominant species of T. congolense and tsetse fly identified was G. morsitans. Therefore, this study was undertaken to determine the prevalence of bovine trypanosomosis, to identify the dominant species of trypanosomes involved, and to assess the PCV values of cattle in relation to the risk factors associated with the disease.
Materials and Methods
Study area
The study was conducted in Jabi Tehnan district of west Gojjam Administrative Zone of Amhara Regional State. The district covers an area of 112,772.1 ha and bordered by Quarit and DegaDamot in East, Burie in West, Sekela in North, and Dembecha and Abay River in the South. The annual mean temperature for most part of the district is 14-32°C and the elevation varies from 1500-2300 mm above sea level (m a. s. 1) with mean annual rain fall of 1250mm. The livestock populations that are found in Jabi Tehnan district include cattle, sheep, goats, horses, mule, donkey and poultry. Among these animals, cattle are the dominant species raised in the area. The cattle population in the district is estimated to be about 187,481[15] (Figure 1).Study animalsThe study was conducted on local Zebu cattle. These animals were raised in different villages of Adankegne and Ergib of Jabi Tehnan district. The animals examined in this particular study were representing different Kebeles. Sex and body conditions of cattle were also being recorded accordingly.
Study design
The retrospective data of cross sectional survey was conducted to determine the prevalence of bovine trypanosomosis. The two sites were selected based on their higher prevalence of trypanosomosis than any other Kebeles of Jabi Tehnan district.
Sample size and sampling methods
The sample size was calculated using previous prevalence of 11.7% by [17] and desired absolute precision of 5% as per the standard procedure described by Thrusfield [18] shown below. An estimated minimum sample size of 159 cattle was obtained; however, we were able to examine 164 cattle for our study.
Study Method and Procedure
Buffy coat technique
Blood was collected from an ear vein using heparinized microhematocrit capillary tube and the tube was sealed. A heparinized capillary tube containing blood was centrifuged for 5 minutes at 12,000rpm. After centrifugation, trypanosomes were usually found in or just above the buffy coat layer. The capillary tube was out using a diamond tipped pen 1mm below the buffy coat to include the upper most layers of the red blood cells and 3mm above to include the plasma. The content of the capillary tube was expressed on to slide, homogenized on to a clean glass slide and covered with cover slip. The slide was examined under x40 objectives and x10 eye piece for the movement of parasite [19].
Measuring of packed cell volume (PCP)
Blood samples were obtained by puncturing the marginal ear vein with a lancet and collected directly into a capillary tube. The capillary tubes were placed in micro-hematocrit centrifuge with sealed end outer most. The tube was loaded symmetrically to ensure good balance. After screwing the rotary cover and closing the centrifuge lid, the specimens were allowed to revolve at 12,00rpm for 5 minutes [4,20]. Tubes were then placed in hematocrit and the readings were expressed as a percentage of packed red cells to the total volume of whole blood. Animals with PCV ≤ 24% were considered to be anemic [21].Data analysisRow data on individual animals and parasitological examination results were inserted into MS Excel spread sheets to create a data-base. Students t-test were employed to compare between the two-independent mean PCV values of animals from an individual site (peasant’s association). Chi-square test was also employed to assess the association between the risk factors and the disease. While analyzing data, p-values (p)<0.05 were registered as statistically significant. Otherwise, recorded as insignificant.
Result
Prevalence
Out of the total 164 (75 females and 89 males) cattle examined, 25 (15.24%) were found positive to trypanosomosis. The prevalence varied between different study areas, in which 9.76% (n = 8) and 20.73% (n = 17) were recorded at Adankegne and Ergib peasant’s association, respectively. The variation in the prevalence of bovine trypanosomosis between the study sites were not statistically significant (X2= 5.783; p = 0.056) (Table 1 and Figure 2). The most prevalent trypanosome species in the study area was T. congolense (80%) followed by T. vivax(20%) (Table l and Figure 2). The prevalence of bovine trypanosomosis showed statistically significance difference between sexes of cattle, in which, higher in male animals (19.1%) as compared to females (10.67%) (X2= 13.886; p = 0.001) (Table 2 and Figure 3).
Hematological findings
Discussion
The study revealed that the prevalence of bovine trypanosomosis in the area was 15.24% (25/164) which was higher compared with the previous findings of Bitew et al. [17] in the same area (11.7%). The difference in prevalence might be due the site from which the blood samples were collected. However, there were tsetse control intervention, and continuous treatment of sick animals as well as deforestation for the cultivation of land. These activities could have led to the reduction of tsetse fly population along with the decline of tsetse borne trypanosomosis in the study area. But the continuous and longtime utilization of trypanocidal drugs particularly Diminazin aceturate in the study area contribute for the development of drug resistance, so that the prevalence of trypanosomosis was higher than the previous finding due to the above reasons.In this study, two species of trypanosomes; namely, T. congolense and T. vivax were retrieved from inspected cattle. Majority of infections were also due to T. congolense. The higher proportion of T. congolense infection in the study area was in agreement with trypanosome species prevalence data from other tsetse infested region of Ethiopia where T. congolense is the most prevalent species in cattle [11]. In the same report it was also indicated that in tsetse free area of highlands, 99% of prevalence was due to T. vivax [12-14]. But in this study area, the prevalence of T. vivaxwas less than T. congolense in both peasant associations because the two sites are located adjacent to tsetse infested belts. Leak [22] and Degneh et al. [23] also indicated that T. vivax was highly susceptible to treatment while the problems of drug resistance were higher in T. congolenseM.In the current study, higher infection rate of trypanosomosis was detected in males (19.1%) as compared to in female cattle (10.67%) with statistically significant difference (X2= 13.886; p = 0.001). Different researchers work supported this finding [22- 25]. Although the variation was not statistically significant, Yalew and Fantahun [26], and Teferi and Biniam [27] had also reported higher prevalence of bovine trypanosomes in males than in females (X2 = 0.85, p=0.35 and X2= 0.10, p>0.05, respectively). According to Gemtessa and Dera [28], the higher prevalence of trypanosomes in males rather than in females might be related to the hardworking of male animals. Similarly, the variation in the prevalence between the two sexes might also be associated with that male animals travel longer distances to tsetse abundant areas for draught and ploughing purposes, and the journey creates stress leading to susceptibility to the infection [23,)].In contrast to this study,Kitila et al. [30] at Yayo District Illuababora Zone of Western Oromia and Tamirat et al. [31] at Enemorena Ener Woreda of Gurage Zone were found higher prevalence of bovine trypanosomosis in female cattle than males.Comparing the mean PCV values of cattle, significantly (p=0.01) low PCV was recorded in parasitaemic animals (25.07%) (SD = 0.989; df = 6; t-value = 8.069) than in aparasitaemic animals (20.75%) (SD = 1.601; df = 152; t-value = 40.316). This finding was in line with previous works conducted at different regions of Ethiopia by many authors [22,25]. In the absence of other diseases causing anemia, a low PCV value of individual animals is a good indicator of trypanosome infection [23,32]. Trypanosomosis might adversely lower the PCV values of infected animals [33]. A survey conducted in cattle in Hawagelan District of West Wellega Zone [34] revealed that the mean PCV of trypanosome infected animals was significantly lower (20.8±3.2 %) compared to non-infected animals (24.9±3.8 %). A later study in Northwest Ethiopia [35] in cattle experimentally infected with T. vivaxi solates also showed that the mean PCV, Hb and total RBC count were lower (p < 0.001) in all infected groups than in noninfected control animals. In Nigeria, domestic ruminants that were naturally infected with trypanosomes had significantly lower (p<0.05) PCV and RBC counts compared to uninfected animals [36]. Lower herd average PCVs for trypanosomepositive cattle compared to trypanosome-negative cattle have also been reported from Ghana [37], Zambia [32], Cameroon [38] and Gabon [39].In spite of the fact that trypanosome infection has significant association with risk factors such as age and body condition scoring, as reported by many scholars, this study had not demonstrated and regarded as limitations.
Conclusion
From this study it is possible to conclude that trypanosomosis is an important disease and a potential threat affecting the health and productivity of cattle. The major species of trypanosomes in the study area were T. congolense and T. vivax. To sum up, infection with trypanosomosis negatively affects PCV and body condition of animals. This indicated that trypanosome infection of cattle causes loss of body weight and production. Trypanosomosis control measures should be targeted on tsetse fly destruction and control methods such as pour-on and effective trypanocidal drug applications. Similarly, rearing or raising of trypanosomosis resistance cattle breeds is now a day in practical. Otherwise, the problems will increase through the aide of global warming. In conclusion, further study on the occurrence of tsetse and trypanosomosis at different season of the year at different altitudes and species of animals should be conducted.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Cell Science & Molecular Biology please click on: https://juniperpublishers.com/ijcsmb/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/ijcsmb/IJCSMB.MS.ID.555649.php
35 notes
·
View notes
Text
Soft Clay Treatment Using Geo-Foam Beads and Bypass Cement Dust | Juniper Publishers

Juniper Publishers-Open Access Journal of Civil Engineering
Authored by Mahmoud Samir El-kady
Abstract
Soft clays are usually classified according to their undrained shear strength, Cu. Values of Cu less than 12.5kPa are associated with very soft clays, whereas, soft clays possess undrained shear strength ranging between 12.5kPa and 25kPa. In addition to the low shear strength of soft clays, they experience high compressibility upon loading. This is why soft clays are considered as problematic for foundation purposes. Also, Geo-foam is an industrial material, characterized by a very low unit weight (average of 20kg/m3) compared to that of the soil. Having a density ranging from 1.0% to 2.5% of that of soil EPS possesses a compressive strength ranging between 70kPa and 140kPa and an elastic modulus ranging between 5MPa and 12MPa, According to Horvath (1997). EPS Geo-foam blocks are used in a wide range of geotechnical applications as a light weight fill.So, the main objective of this study is to investigate the geotechnical properties of soft clay with Geo-foam beads and bypass cement dust. Also, investigate the possibility of preparing low strength excavatable fill mixtures. For studying the effect of (Geo-foam beads + CBPD) / soft clay on fluid-state and hardened properties of new fill, experimental work was carried out on two groups of mixture (A&B). Different ratios of (Geo-foam beads + CBPD) were added to the mixture to study its effect on flow consistency, dry unit weight, unconfined compressive strength, and shear strength. The results of test conducted on the materials illustrated that, cement bypass dust and excess foundry sand can be successfully used to procedure self-compaction, self-leveling excavatable flowable fill material. The unconfined compressive strength of the studied mixtures without Geo-foam ranged between 271.8kPa and 1405.14kPa at CBPD between 3.88% and 18.63%. The Cohesion values for group with Geo-foam with ranged between 50kPa and 20kPa at Geo-foam between 0.32% and 1.35%. The friction angle of group with Geo-foam with ranged between 10 and 22kPa at CBPD between 0.32% and 1.35%.
Keywords: Geo-foam Beads; Bypass Cement Dust; Flowable Fill; Shear Strength
Introduction
EPS Geo-foam blocks are used in a wide range of geotechnical applications as a light weight fill. The primary function of Geo-foam is to provide a lightweight void fill below a highway, bridge approach, embankment or parking lot [1]. EPS Geo-foam minimizes settlement on underground utilities. Geo-foam is also used in much broader applications, the major ones being as lightweight fill, green roof fill, compressible inclusions, thermal insulation, and (when appropriately formed) drainage. Expanded polystyrene (EPS) Geo-foam has been used as a geotechnical material since the 1960s. EPS Geo-foam is approximately 1% the weight of soil and less than 10% the weight of other lightweight fill alternatives. As lightweight fill, EPS Geo-foam reduces the loads imposed on adjacent and underlying soils and structures [3].EPS Geo-foam is not a general soil fill replacement material but is intended to solve engineering challenges. The use of EPS typically translates into benefits to construction schedules and lowers the overall cost of construction because it is easy to handle during construction, often without the need for special equipment, and is unaffected by occurring weather conditions [3]. EPS Geo-foam can be used to replace compressible soils or in place of heavy fill materials to prevent unacceptable loading on underlying soils and adjacent structures. The high compressive resistance of EPS Geo-foam makes it able to adequately support traffic loadings associated with secondary and interstate highways [4]. Also, using EPS Geo-foam eliminates the need for compaction and fill testing, reduces the construction time and minimizes impact to the existing roadway and adjacent structures and/or buried utilities [5]. Experimental work was carried out on two groups of mixture (A&B) and different ratios of (Geo-foam beads + CBPD) were added to the mixture to study its effect on the geotechnical properties.
Experimental Program Material characteristics
The soft clay was dried in the oven at 110C. It is passing through sieve size of 0.25mm. Soft clay characteristics are listed in Table 1.Also, the unit weight of the Geo-foam beads is 15.0kg/m3. The size of the Geo-foam beads is 5.0mm Figure 1a.Mixture proportionsThe experimental work was divided into two groups, each with the same size of 600cm3. Group A was divided into five subsamples without the use of Geo-foam and mixed with increasing percentages of CBPD (50g) for each sample and different percentages of water. In addition, the B group was divided into five sub-samples and mixed with increasing percentages of Geo-foam (5g) for each sample as well as different percentages of water with stable weight of CBPD as shown in the following Tables 2-5.
Experimental Work and Results Flow consistency
Samples were mixed for groups A-B for different percentages of water as shown in Figure 1b. The consistency flow of the samples was measured for each sample. It is found that the flow consistency increased slightly for group B than for group A. So, the flow consistency was measured in laboratory as listed in (Tables 6-7 ) for the two groups. Although the percentage of water present in the B samples, the effect of the presence of Geofoam beads than bypass cement dust on soil was clear as shown in Figure 2.Unconfined compressive strengthThe studied mixtures for each group were molded and hardened. Unconfined compressive strength was obtained by the Triaxial test for the studied mixtures as shown in Figures 3. It was found that with the increase of cement bypass dust, the unconfined compressive strength increased significantly and especially for the samples (A4 - A5) compared to a slight increase in the values of the strain% as shown in Figure 4. Also, compressive strength values are also stabilized with increasing mixing rates in cement bypass dust from approximately 14 to18% as shown in Figure 5. This shows the significant effect of cement bypass dust on compressive strength of studied samples.Shear strengthShear box test was carried out on the studied samples. The samples were loaded with increasing stresses (50-100-150kPa)and the shear stresses were calculated versus horizontal displacement (mm). We took samples (A4-B4) for examples as shown in Figures 6-7. Shear strength parameters were obtained from direct shear test and it is concluded that CBPD affected in the cohesion of the group A samples as shown in Figure 8. On the contrary, angle of internal friction was increased significantly when increasing the ratio of Geo-foam beads for group B samples as shown in Figure 9 [6-10].
Conclusion
This paper presented an experimental study of various samples of soft clay mixed with different percentages of Geofoam beads and cement bypass dust. The following conclusions may be drawn:A. The results of test conducted on the materials illustrated that, cement bypass dust and excess foundry sand can be successfully used to procedure self-compaction, selfleveling excavatable flowable fill material.B. The dry unit weight of the studied mixtures for group without Geo-foam ranged between 1.40 and 1.6 gm/cm3 at CBPD between 3.88% and 18.63%.C. The dry unit weight of the studied mixtures for group with Geo-foam ranged between 0.65 and 1.20 gm/cm3 at Geo-foam between 0.32% and 1.35%.D. The unconfined compressive strength of the studied mixtures without Geo-foam ranged between 271.8kPa and 1405.14kPa at CBPD between 3.88% and 18.63%.E. The unconfined compressive strength of the studied mixtures with Geo-foam ranged between 230kPa and 120kPa at Geo-foam between 0.32% and 1.35%.F. The Cohesion values for group without Geo-foam with ranged between 62kPa and 105kPa at CBPD between 3.88% and 18.63%.G. The Cohesion values for group with Geo-foam with ranged between 50kPa and 20kPa at Geo-foam between 0.32% and 1.35%.H. The friction angle of group without Geo-foam with ranged between 3 and 11° at CBPD between 3.88% and 18.63%.I. The friction angle of group with Geo-foam with ranged between 10° and 22° at CBPD between 0.32% and 1.35%.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Civil Engineering please click on: https://juniperpublishers.com/cerj/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/cerj/CERJ.MS.ID.555701.php
49 notes
·
View notes
Text
Bioethical and Biosafety Issues in Biomaterials Used in Oral Rehabilitation | Juniper Publishers
Juniper Publishers-Open Access Journal of Material Science
Authored by D’Souza DSJ
Abstract
With recent advances in biotechnology, there has been a plethora of biomaterials in the form of various dental materials and maxillofacial implants, being routinely used for comprehensive oral rehabilitation. Even though these have considerably enhanced the treatment outcomes, but at times the improper application and lack of safety precaution with these have raised many moral and ethical issues. Due to commercial and marketing pressures, technological developments in biomaterials have led to ethical issues being conveniently buried. Lack of stringent regulations and want of strict institutional control results in products that are not truly safe for patients to be marketed and used by unsuspecting clinicians.Clinicians need to be aware of the various bio-safety aspects of the biomaterials that are commonly in use and also ensure that the patients’ rights of informed consent, beneficence, non-malfeasance and autonomy are protected. There is an urgent need for all healthcare specialists to be aware of the bioethical concerns associated with these advanced materials and technologies so that they are better equipped to utilise them safely and confidently.
Introduction
The field of biotechnology today is moving ahead at a rapid pace with newer products and superior biomaterials for oral rehabilitation being constantly discovered, however the mandatory level of simultaneous clinical applications research always seems to be playing catch-up. There are inherent safety related checks and balances within the system when it comes to clinical trials and bio-safety issues in animals and human trials, yet this time lag is often considered as an unnecessary hurdle or speed bump on the road to progress. It is crucial that the clinical trials follow all the steps and systematic reviews that are necessary to ensure that all manufacturer claims are verified and adverse reactions are minimal if not nil. Clinicians also need to be aware of the potential danger in using biomaterials that are not properly tested and should not be swayed by promotional pressure from marketing agents.Biomaterials and oral rehabilitationThe use of a wide array of biomaterials for oral rehabilitation has been known from the earliest times. Extracted teeth, silver, gold and a mind-boggling range of other materials are recorded as having being utilised with varying degrees of success in the maxillofacial region [1]. While the uses of biomaterials in other applications in the human body have been fairly predictable and successful there are myriad challenges in the rehabilitation of the oral and maxillofacial region. The presence of saliva, interaction with food and other commonly consumed liquid sand the physical assault of Masticatory forces all causes significant stress and wear and tear on the biomaterials used in the oral cavity.In recent years, there has been a plethora of biomaterials and related biomedical technology, in the form of various rehabilitative dental materials and maxillofacial implants, being routinely used for comprehensive oral rehabilitation. Undoubtedly these have all dramatically improved the scope of treatment, but, these advancements have raised many moral and ethical issues. As the goal to be the first in the market is paramount, many a time, commercially-driven technological development in biomaterials have led to ethical issues being conveniently buried. Laxity in regulations and want of strict institutional control results in products that are not truly safe for the patients to be marketed freely and may also further lead to products that are not fully licensed to enter into the system.Responsible clinicians need to be aware of the various biosafety aspects of the biomaterials that are commonly in use and also ensure that the patients’ rights of beneficence, non-maleficence and autonomy are protected. There is an urgent need for all healthcare specialists to be aware of the bioethicalconcerns associated with these advanced materials and technologies so that they are better equipped to utilise them safely and confidently.Biocompatibility and biosafetyBiocompatibility maybe described as the property of a biomaterial to function in a predictable manner when applied to the body, without causing a chronic inflammatory reaction, undesirable biological response, foreign body reaction or toxicity, as a result of interaction between the host tissues and the biomaterial [2]. There is no single material that is completely inert from the physiological point of view since, one or more of the components may be potentially toxic or irritating3. In addition, chemical by-products produced during cure of the material or as a result of interaction with other materials in the region may also produce undesirable effects [3]. It is therefore imperative that all clinicians have an in-depth knowledge about the characteristics and properties of materials and their likely interaction within the biological environment before utilizing them for oral rehabilitation.There is a wide range of adverse biological events following the utilization of restorative materials in the oral region and therefore biocompatibility testing has to be undertaken as a strategic and structured approach. Present consensus on testing of biocompatibility is that the method should be rapid and costeffective and also by avoiding animal testing as far as practicable. Modern test designs try to simulate the in-vivo situation as closely as possible. This may be accomplished by including suitable barriers between the material and the target cells, by constructing appropriate target cells, and or by applying biomarkers for estimating the biological side effects [4].Commonly adverse reactions to materials used for oral rehabilitation occur as a result of their direct contact with soft or mineralized tissues, or due to leaching out of some corrosion or degradation by-products. The use of multiple metallic restorations manufactured from alloys with differing compositions will show a more rapid degradation when immersed in saliva due to galvanic action. If these chemical by-products are ingested, they may manifest as both local or systemic reactions [5]. Materials designed for oral use are manufactured with the aim of being inert and insoluble. The quanta of leachable components are minimal and so routinely toxic reactions are unlikely to occur. Despite this fact, severe allergic reaction may be provoked in a sensitized individual by even miniscule concentrations of the allergen [6]. Thus contact allergic reactions (Type IV reactions) are the most common observed as side effects in the dental clinic. Assessment of possible reactions to the biomaterials is therefore a constant challenge and all clinicians must be aware of and report any adverse outcomes promptly and thoroughly [7-9].When evaluating adverse reactions to materials used in prosthodontic appliances, a variety of situations must therefore be taken into consideration. This is because some materials come only in brief contact with the patients such as when making an impression or registering a bite of the patient. In contrast, dental prostheses are intended to remain in-situ for decades. A number of factors need to be taken into account when estimating adverse biological reactions to prosthodontic materials [5]. Among these include: the type, form, contour, extent of the prosthesis, any medication used by the patient, salivary flow rate, xerostomia, oral hygiene, quality of fit, and function of the prosthesis. All these conditions may affect local reactions in addition to those caused by the materials per se [10]. Biological films, ‘pellicles’, of salivary origin will also accumulate on the materials. They differ in composition depending on the material and on the properties of the patients’ saliva. The irrigating effect of saliva is also difficult to assess. However, a distinct difference exists between material reactions intra-orally and extra-orally, with those on skin being more frequent and more severe [11].
Bio-safety concerns of biomaterials
Casting alloys: The alloys commonly used for manufacturing of dental prostheses contain varying amounts of trace metals such as nickel, chromium, cobalt, cadmium and beryllium. These are known to cause potentially hazardous reactions and are of concern especially for the dental technicians during the casting and finishing procedures. Adverse reactions in the oral cavity to casting alloys are observed due to release of components from the alloys, following corrosion when immersed in saliva [12-15].Polymer-based restorative materials: Many of the restorative materials used in oral rehabilitation are polymerized resin-based materials that are cured by heat, light, or by chemical activators at room or mouth temperature. Their composition includes accelerators (amines), co-polymers, such as butyl-methacrylate (BMA), plasticizing agents such as dibutyl-phthalate, and inhibitors such as hydroquinone. Various shade matching components to simulate natural tooth and gingiva colour are also present. These may not pose a danger for clinical use in patients’ but have a potential hazard to the dental mechanics who routinely grind and polish the prosthesis made from these resin-based materials. If the materials are not fully cured in the dental laboratory, the presence of free monomer radicals of methyl methacrylate may cause toxic reactions or allergic responses in previously sensitized individuals [16-19].Implant materials: The field of oral rehabilitation was dramatically transformed by the demonstration of ‘osseo integration’ of alveolar bone with titanium implants, as described by Brane mark. Since then many materials have been used to manufacture dental implants, such as high impact polymers, cobalt-chromium alloys, vitreous carbon, titanium, and aluminium oxide alloys, ceramic, and synthetic hydroxylapatite [20]. The main research has been focussed on the region or interfaces between alveolar bone and the implant as well as ultramicroscopic studies on the pattern of in-growth of bone into the implant surface. One of the main reasons for the failure of dental implants is due to failure of osseointegration.This may be primary failure due to improper surgical technique; or it may be secondary following loading of the implant, and secondary infection [20]. Another area that needs investigation is the effect of nano-particles of metals, polyethylene, and ceramics which cause a biological response at the implant bone interface. Focussed research is vital for comprehensive biosafety evaluations of implant biomaterials and biological effects of nano-toxicology both from the aspect of biomedical applications and the long term in-vivo effects [21,22].Graft materials: There are many types of bone graft materials being routinely used for oral rehabilitation. These may be auto grafts, xenografts or allografts. The known sources for xenografts are bovine bone, porcine bone, horse bone and natural coral. Despite the claims of absolute safety of these products, the discovery of bovine spongiform encephalopathy (BSE) and porcine endogenous retroviruses (PERVs) needs to be kept in mind [23]. Ethically as well, the need to inform the patients of the source of the graft materials is mandatory where the patient may have some religious reservations against certain types of grafts. The method of sourcing and bio-safety testing must be definitely checked by the clinician before opting to use any of these graft materials
Conclusion
There is an increased demand on the various materials being utilized for oral rehabilitation to be functionally biocompatible, esthetically acceptable and economically viable for all groups of patients. It is therefore imperative that better strategies are designed to evaluate, predict, and assess material safety aspects both at the manufacturing hub as well as the consumer end. The researchers must be ethical in their reporting of in-vitro and in-vivo effects of all novel bio-materials as well as newer technologies to treat oral disease. Clinically driven research networks and practitioner groups should be involved in ethically driven patient trials to ensure that all newer products or technology goes through exhaustive and systematic clinical evaluation. Reliable research protocols will ensure that the various bio-safety aspects are looked after and the frequency of adverse reactions in oral rehabilitation is minimized. There is an ethical and moral requirement for all clinicians to be aware of the limitations, outcomes, reactions of the various materials that they routinely employ in the oral rehabilitation of the patients. Evidence-based evaluation must be the watchword and clinicians must be careful not to be swayed by commercial and marketing pressures.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Material Science please click on: https://juniperpublishers.com/jojms/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/jojms/JOJMS.MS.ID.555553.php
47 notes
·
View notes
Text
Present Development in Horticulture | Juniper Publishers

Juniper Publishers-Open Access Journal of Horticulture & Arboriculture
Authored by Shoukat Sajad
Mini Review
Horticulture is a branch of agriculture that deals with science, art, and business development of growing plants. It includes all type of plants such as, vegetables, fruits, medicinal plants, sprouts, mushroom, and algae etc., and also non-food crops like ornamental plants, trees, and grass. A horticulturist is a person who applies his knowledge, technology, and skills to grow plants intensively that are used by humans for food and non-food needs. Horticulture involves nine areas of study such as, Arboriculture, Turf management, Floriculture, Landscape horticulture, olericulture, pomology, viticulture, oenology, and postharvest physiology. The Journal of Horticulture is an open access journal that publishes high impact research articles.Foster et al. [1] studied the effect of different growing environments in modifying first expression of root–stock-induced dwarfing of the scion. An experiment was conducted in which Royal Gala trees were grafted onto the three different vigor clonal root stocks such as M27’, ‘M9’, and ‘M793’and grown in three different locations. The growth and detailed architectural measurement were done over first year and repeated for the second year. This work demonstrated that primary axis or sylleptic shoot termination is consistently expressed by M9 and M27 dwarfing rootstock in different growing environments and years. Tus, this study provided new phenotypic information for future studies for elucidating the genetic and physiological bases for apple root–stock induced dwarfing.Babatunde et al. [2] tried to obtain information on interaction of tillage passes and NPK fertilizers application rates on some growth factors of Amaranthus viridis. The soil treatment of this experiment includes three levels of tillage passes (0, 3, and 6) that equivalent to the soil density 1.7, 1.3, and 1.5g/cm3 respectively and four levels of NPK fertilizers (0, 100, 150, and 200kg/ha). This experiment was continued for three replications in randomized designed plots. This experimental result summarized that the effects of interactions between tillage and fertilizers rates were observed on stem girth, fresh weight, plant height, root length, and percent of N, P, and K uptake. The increase in plant height and improved uptake of phosphorous were observed at T2F2 (6 passes and 150kg/ha). Thus, they concluded that T2F2 (6 passes and 150kg/ha) NPK fertilizer application could be more suitable for the optimum yield for Amaranthus viridis on sandy clay soil.The passion fruit belongs to Passifloraceae family that is native of southern Brazil through Paraguay to northern Argentina. Matheri et al. [3] tried to study the phenotypic variations existing between Purple and Brazil varieties, as well as their hybrids that are developed by KALRO. The phenotypic variations were observed by applying principle component technique and cluster analysis statistical tools of Minitab 17.0 software to discriminate the accessions based on seven quantitative morpho-agronomic traits targeted with replication per plant and variety. The dendrogram and scatter plot clustered indicates the phenotypic relatedness within the varieties. Thus, this study affords the current body of knowledge on passion fruit breeding.Zhang et al. [4] studied the cold tolerance of Kentucky blue grass at the genomic level. For this they sequenced and analyzed the Kentucky blue grass transcriptomes under cold treatment and control treatment by RNA-seq and de novo assembly. At the same time they also aimed to identify more transcription factors associated to cold tolerance. In this study, nearly 3,896 unigenes were identified between control and cold treated plants and several transcriptional factors were identified as differentially expressed genes. Thus, this study provided valuable resource for the studies on the transcriptional regulation of cold tolerance.Yuan et al. [5] aimed to study the role of PuADF in fruit ripening. Expression of ADF gene, named PuADF, which is down-regulated during fruit ripening. The screening of cDNA library from ‘Nanguo’ pear fruit using PuADF as bait identified two proteins that interacted with PuAS and PuDAD1that are associated with program cell death. This expression PuAS and PuDAD1 was affected by ethylene. Thus, they concluded that PuADF is involved in ethylene-mediated fruit ripening and interact with PuAS and PuDAD1, which in turn are involved in fruit ripening.The Japanese beetle (Popillia japonica) one of the mostwide spread and destructive insect pest which damages various fruits, field, and garden crops. Management of these beetles with bacillus thuringiensis galleriae is possible but its activity is not long lasting. Maier et al. [6], hypothesized the management of Japanese beetle with Kaolin clay. Its mechanism includes repellency, impairment or disruption of ovi position and feeding activity. The abrasive mineral present in Kaolin clay promotes the cuticle disruption and digestive system obstruction. Various field tests with Kaolin clay in different application rates effectively minimized the feeding damage caused by Japanese beetles and no side-effects were recorded on several fruit weight. Thus, Kaolin clay is a good alternative for the management of Japanese beetle.The Japanese beetle (Popillia japonica) one of the mostwide spread and destructive insect pest which damages various fruits, field, and garden crops. Management of these beetles with bacillus thuringiensis galleriae is possible but its activity is not long lasting. Maier et al. [6], hypothesized the management of Japanese beetle with Kaolin clay. Its mechanism includes repellency, impairment or disruption of ovi position and feeding activity. The abrasive mineral present in Kaolin clay promotes the cuticle disruption and digestive system obstruction. Various field tests with Kaolin clay in different application rates effectively minimized the feeding damage caused by Japanese beetles and no side-effects were recorded on several fruit weight. Thus, Kaolin clay is a good alternative for the management of Japanese beetle.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Horticulture & Arboriculture please click on: https://juniperpublishers.com/jojha/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/jojha/JOJHA.MS.ID.555578.php
27 notes
·
View notes
Text
Indication-Specific Approach to Filler Injections
Juniper Publishers-Open Access Journal of Dermatology & Cosmetics
Authored by Sabine Zenker
Summary
Facial aging is a complex process resulting in appearance of wrinkles and folds as well as sagging and volume loss. This article does outline a science-based, indication-specific therapeutic concept for filler injections to the aging ace.
Keywords: Indication specific treatment; Filler; Fill; Ftimulate; Volumize
The Age-Related Three-Dimensional Facial Changes
Even though facial aging starts at the surface by showing signs of skin aging, the changes go far beyond the skin: it finally involves all other facial structures such as the muscles, retaining ligaments, fat pads and the bony structures. Predominantly and for a youthful and appealing look, the architecture and position of the fat pads is pivotal. But over time, the facial fat pads get redistributed, they do atrophy and get separated [1-6]. Further to this, a remarkable bony resorption takes place and doesn`t give the needed structural support [3,6,7]. All this results in deflation, volume loss and sagging in a three-dimensional way [6,8].
Typical Indications for Filler Treatments
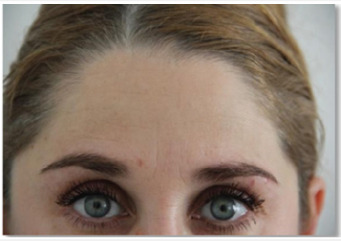
Here, very importantly, filler treatments come into play. Any treatment in aesthetic dermatology does require an indication-specific treatment approach, the individual diagnosis has to be set up in order to decide for the respective treatment plan. Typical indications for filler treatments are:WrinklesCreases, wrinkles and folds are a typical sign of skin aging and can give facial expressions an unwanted negative touch (Figure 1).Volume LossFurther changes such as the appearance of shades, furrows, volume loss and overall sagging are the next typical indication for facial filler injections to restore facial proportions in order to get back the pleasing facial features one had in the past or to improve aspects such as shape, form and volume of a face; basically, it`s about to give back a healthy look with natural fullness and soft and smooth transitions (Figure 2).
Treatment Concept for Wrinkles by Filler Injections
Here, the concept of filling wrinkles [direct filling by hyaluronic acid [HA]] and of dermal stimulation by polycaprolactone [PCL] will be discussed.For direct filling by hyaluronic acid, typical indications on forehead- or perioral lines etc.. , the filler is injected intra-dermally in a retrograde fashion [“blanching”] by serial-puncture- or linear- threading, using a sharp needle [30G ½”] [9]. The author does mix the respective hyaluronic acid with local anesthetics in a ratio up to 30% [off-label-use!] to basically achieve an optimal integration of the filler material in the superficial dermis. The correction should never be done over the clinical endpoint. To control filler placement, author often uses injection systems as this increases the accuracy of filler placement and its dose which reduces side effects such as pain and bruising to improve the overall aesthetic outcome in especially such very superficial injections [10]. The result of this direct filling technique with hyaluronic acid lasts -depending on material used and individual conditions- for some months (Figure 3-6).The stimulation technique by filler using polycaprolactone [PCL] is especially suited if an immediate filling is desired. Additionally, the effect of collagen stimulation starts appr. 3 months after injection. Polycaprolactone is a biodegradable filler material consisting of microparticles of PCL suspended in a gel carrier [carboxy-methyl-cellulose [CMC] with both, volumizing and stimulating capacities [11,12]. This filler has to be placed using a 25G 1½” blunt tipped cannula in a subscision-wise way: PCL is fanned sub-dermally in a fan pattern to cover the whole area to be treated in a retrograde fashion; the point of insertion is chosen in a 90° angle and in the middle of each respective fold. The approximate amount of filler to be injected is 0.1cc (Figure 7,8).
Treatment Concept for Volume Loss by Filler Injections
The treatment of the three-dimensional volume loss will be showcased here by demonstrating techniques for the midface. He tTypical indications here are the sunken-in frontal part of the cheek and the sagged lateral part.To plan the individual injection strategy, to identify to be treated areas with its entry points as well as the danger zones, facial mapping is pretty use- and helpful (Figure 9).Here, typically highly visco-elastic hyaluronic acid fillers with a good volumizing capacity [13,14], Calcium Hydroxylapatite, CaHA [Radiesse©], a calcium particles based filler [15,16] or Polycaprolactone [PCL] are used. The use of blunt tipped cannulas results in a more atraumatic [15], quicker treatment procedure, especially when the filler needs to be placed over “longer distances” [16-22].The following pictures illustrate typical entry points for this treatment concept, the Cheek-Apex- Entry-Point and the Zygomatic Entry-Point.The Cheek Apex Entry-Point, entry-point to treat the sunkenin frontal part of the chees, is the point around which the frontal projection of the cheek will be reconstituted (Figure 10).Sunken-in frontal part cheekStarting point is the Cheek Apex Entry-Point. The filler is injected in a bolus technique [„gunshot- wise“], in a retrograde way and placed supraperiostally; according to the clinical needs, more injections medial and eventually lateral of the first entrypoint are performed in a “banana-wise” way. Amount of filler per point is approximately 0.1cc. Augmentation is conducted up to the clinical endpoint.Sagged lateral part cheekStarting point is the Zygomatic Arch Entry-Point. The filler is injected in a fanning technique in retrograde fashion starting supraperiostally and ending up subdermally on the most lateral part of the to be injected area. Amount of filler per point is approximately 0.1-0.2cc. Augmentation is conducted up to the clinical endpoint.Using these two techniques the frontal projection of the cheeks as well as the lateral lifting can be effected in a customized and individual way.Here, the following illers are used: hyaluronic acid Perfectha© Subskin and Calcium Hydroxylapatite [Radiesse©] [mixed with Lidocain 1% in a 20% ratio]. As equipment, a blunt tip cannula 25G/38mm is used [Steriglide®] (Figure 12-16).
Summary
Age related facial changes such wrinkles, volume loss and sagging can be easily and individually treated by filler. The indication-specific filler treatment approach helps to identify the respective indications. Thanks to the versatility of degradable fillers, they can serve for all, filling, stimulating as well as volumizing.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/journals.php
For more articles in Open Access Journal of Dermatology & Cosmetics please click on: https://juniperpublishers.com/jojdc/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/jojdc/JOJDC.MS.ID.555554.php
19 notes
·
View notes
Text
Review on General Effective & Therapeutic Diabetic Wound Management

Juniper Publishers- Open Access Journal of Diabetes & Obesity
Authored by Blessing Nimasajai XS
Abstract
Diabetes mellitus is a syndrome of disordered metabolism with abnormally high blood glucose levels (hyperglycemia) (Tierney 2002). According to the latest 2016 data from the World Health Organization (WHO) it is estimated that globally 422 million adults are living with diabetes mellitus .The different types of diabetes are type 1 diabetes (diminished production of insulin) “insulin-dependent diabetes mellitus” ( IDDM) or “juvenile diabetes” , type 2 diabetes (impaired response to insulin and β-cell dysfunction) “non-insulin-dependent diabetes mellitus” (NIDDM) or “adult-onset diabetes” and the other is gestational diabetes which occurs during pregnancy. All type shows signs and symptoms like hyperglycemia, excessive urine production, compensatory thirst, increased fluid intake, blurred vision, unexplained weight loss, lethargy, and changes in energy metabolism. Uncontrolled diabetes mellitus may cause many complications, one of the most serious complication is diabetic wound. This article is based on various research reviews and it was written because most of the people were suffering with diabetic wound and finally they are going for amputation, which is really a painful event and according to me all body parts is very much important for all human being and as early as from the creation of human being by God , the human body is created with all necessary parts & it is our duty & responsibility in caring & protecting the humans body parts as much as possible from amputation. Drop of insulin in blood leads to diabetes mellitus and its complication leads to diabetic ulcer and finally some diabetic ulcers lead to the loss of body parts. To prevent from amputation on behalf of diabetic ulcer, all health care professionals should give more concentration in therapeutic diabetic wound management.
Keywords: Diabetes mellitus; Insulin; Hyperglycemia; Diabetic ulcer; Amputation; Complication
Introduction
“Wounds don’t heal the way you want them to, they heal the way they need to. It takes time for wounds to fade into scars. It takes time for the process of healing to take place. Give yourself that time. Give yourself that grace. Be gentle with your wounds. Be gentle with your heart. You deserve to heal.” - Dele OlanubiDiabetes mellitus is a group of metabolic disorder characterized by hyperglycemia resulting from deficiency in insulin secretion and its imbalance. The increased blood sugar level in diabetes mellitus is associated with long-term damage, dysfunction, and failure of various organs such the eyes, kidneys, nerves, heart, and blood vessels. As per 2016 data from the World Health Organization (WHO) shows the estimation of 422 million adults are living with diabetes mellitus worldwide. Diabetes prevalence has been rising more rapidly in middle- and low-income countries [1]. The major cause of blindness, kidney failure, heart attacks, stroke and lower limb amputation is diabetes mellitus. WHO projects that by 2030, diabetes will be the seventh leading cause of death worldwide. The different types of diabetes are type 1 diabetes (diminished production of insulin) “insulin-dependent diabetes mellitus” (IDDM) or “juvenile diabetes”, type 2 diabetes (impaired response to insulin and β-cell dysfunction) “ non-insulin-dependent diabetes mellitus” (NIDDM) or “adult-onset diabetes” and the other is gestational diabetes which occurs during pregnancy. All type shows signs and symptoms like increase blood sugar level, excessive urine production, increased thirst, increased fluid intake, blurred vision, unexplained weight loss, lethargy, and changes in energy metabolism. Diabetic ulcers are growing more rapidly due mainly to increased incidence of both Type I and maturity-onset diabetes in the developed (high-GDP) countries around the world [2]. The prevalence of diabetic ulcers is rising at 9% annually. At present, this pool of patients is growing faster than the new technologies are reducing the incidence of wounds by healing them uncontrolled diabetes mellitus may cause many complications, one of the most serious complication is diabetic wound. This article is based on various research reviews and it was written because most of the people were suffering with diabetic wound and finally they are going for amputation, which is really a painful event and according to me all body parts is very much important for all human being and as early as from the creation of human being by God, the human body is created with all necessary parts & it is our duty & responsibility in caring & protecting the humans body parts as much as possible from amputation [3]. Drop of insulin in blood leads to diabetes mellitus and its complication leads to diabetic ulcer and finally some diabetic ulcers lead to the loss of body parts. To prevent from amputation on behalf of diabetic ulcer, all health care professionals should give more concentration in therapeutic diabetic wound management. Diabetic wound is a major health problem and its management involves a multidisciplinary approach (Figure 1). This review aims to provide an information regarding the current management strategies of diabetic wound, from prevention to the options for treatment. The authors believe that it may be useful to primary healthcare providers who were involved in the prevention or management of diabetic wound.
Definition/Terminology
Diabetes mellitus is defined as a chronic disease caused by imbalance between insulin by the pancreas and its demand. It leads to increased concentrations of glucose in the blood, which in turn damage many of the body’s systems, the blood vessels and nerves [4].Diabetic wound is a wound which occur because of various factors, such as mechanical changes in conformation of the bony architecture of the foot, peripheral neuropathy, and atherosclerotic peripheral arterial disease, all of which occur with higher frequency and intensity in the diabetic population.Diabetic wound risk factorsRisk factors includes poorly fitted or poor-quality shoes, poor hygiene (not washing regularly or thoroughly), improper trimming of toenails, alcohol consumption, eye disease from diabetes, heart disease, kidney disease, obesity, tobacco use (inhibits blood circulation) etc.
Cause of diabetic wound:1. Increase Blood Sugar Levels: Diabetes is a metabolic disease that causes elevated levels of glucose in the blood. Elevated blood glucose levels stiffen the body’s arteries and narrow its blood vessels, restricting the delivery of the blood and oxygen needed to support the body’s natural healing abilities.2. Decrease or Poor Circulation: Individuals with diabetes are at an increased risk for peripheral arterial disease (PAD), a condition that restricts blood flow to the feet and legs. PAD is especially problematic for those with chronic wounds, particularly diabetic foot ulcers, because it can seriously inhibit the body’s ability to heal. If left untreated, PAD can lead to amputation of the affected limb.3. Peripheral Neuropathy /Nerve Damage: A lack of circulation in the extremities can result in a reduced supply of oxygen and nutrients to the body tissue and nerves, which is necessary for healing. Over time, nerves in these areas may become damaged, decreasing the sensation of pain, temperature and touch, making patients vulnerable to injury.4. Immune System Issues: One of the roles the body’s immune system is to clear away dead, damaged tissue and build new skin cells once a wound or injury has occurred. Diabetes can slow a person’s immune system, which affects the body’s ability to send white blood cells to fight bacteria in an infected diabetic foot ulcer.5. Infection: Because diabetics tend to have weaker immune systems, their bodies are more susceptible to infection. Particularly in those with diabetes, it’s common for a wound to develop an infection like non-healing diabetic foot ulcers.Types /classification of diabetic woundThere are two most common diabetic wounds. They are external origin diabetic wounds and internal origin diabetic wounds. Due to peripheral neuropathy, wounds of external origin, such as skin cuts, burns, bumps and bruises, may often go unnoticed by the diabetic patient [5]. If external wounds go unnoticed for some time, delayed treatment can put the patient at risk for further complications. Wounds of internal origin, such as skin ulcers, ingrown toenails or calluses, can lead to the breakdown of skin and surrounding tissue, increasing the risk of bacterial infections.Signs & symptoms of diabetic woundCommon signs and symptoms of diabetic wound are chronic pain or completely painless, signs of inflammation (swelling, redness, heat, pain and loss of function), signs of infection (pus drainage, discharge, bad odor and dead tissue), numbness and dullness (signs of nerve damage), fever and/or chills (signs of progressively worsening infection that can be limb-threatening or even life-threatening).Diagnostic evaluations for diabetic woundDiagnostic evaluations for diabetic wound include history collection, physical examination, examination of the ulcer, testing for loss of sensation, testing for vascular status, laboratory investigations (blood tests), pulse-volume recording, ultrasonography, ankle-brachial index, radiography, computed tomography, magnetic resonance imaging, bone scans, and angiography [6].Factors that delay diabetic wound healingLocal factors are continued pressure over the site, desiccation and dehydration, trauma, edema, infection or heavy colonization, necrosis, maceration caused by incontinence, lack of oxygen delivery to the tissues, etc., [7]. Systemic factors are old age, obesity, chronic diseases, malnutrition, vascular insufficiency, immunodeficiency, smoking, stress, etc., (Table 1 & 2).Management of diabetic woundA. The essential components of diabetic wound management are:B. Treating underlying disease processesC. Ensuring adequate blood supplyD. Local wound care, including infection controlE. Antibiotic for infected diabetic woundsF. Tissue debridementG. Inflammation and infection controlH. Moisture balance (optimal dressing selection)I. Epithelial edge advancement.J. Pressure offloading.a. Avoid bandaging over toes as this may cause a tourniquet effect (instead, layer gauze over the toes and secure with a band- age from the metatarsal heads to a suitable point on foot)b. Use appropriate techniques (e.g. avoiding creases and being too bulky) and take care when dressing weightbearing areasc. Avoid strong adhesive tapes on fragile skind. Avoid tight bandaging at the fifth toe and the fifth metatarsal head (trim the bandage back)e. Ensure wound dead space is eliminated (e.g. use a dressing that conforms to the contours of the wound bed)f. Remember that footwear needs to accommodate any dressing.g. Vacuum-assisted closure: Vacuum-assisted closure (VAC) is a new method in wound care which speeds wound healing by causing vacuum, improving tissue perfusion and suctioning the exudates.h. Hydrotherapy: The process of providing an adequate amount of liquid to bodily tissuesi. Treatment of charcot foot: Charcot neuropathic osteoarthropathy (CN), commonly referred to as the Charcot foot, the diabetic Charcot foot syndrome is a serious and potentially limb-threatening lower-extremity complication of diabetes. The diabetic Charcot foot is an inflammatory syndrome characterized by varying degrees of bone and joint disorganization secondary to underlying neuropathy, trauma, and perturbations of bone metabolism. Management includes Offloading at the acute active stage of the Charcot foot is the most important management strategy and could arrest the progression to deformity, antiresorptive drugs, Surgical treatment of Charcot arthropathy of the foot and ankle is based primarily on expert opinion [8]. Surgery has generally been advised for resecting infected bone (osteomyelitis), removing bony prominences that could not be accommodated with therapeutic footwear or custom orthoses, or correcting deformities that could not be successfully accommodated with therapeutic footwear, custom ankle-foot orthoses, or a Charcot Restraint Orthotic Walker.j. Surgical Care, surgical wound closure & bone resection: Diabetics have higher risks of wound healing complications following surgery. Surgical wounds can easily become chronic wounds, such as pressure ulcers, without the right care. There are several types of wound dressings available, including the following:a) Alginates: Alginate dressings encourage debridement and absorb wound drainage.b) Collagens: These work well for surgical wounds in diabetics by encouraging blood vessel and new tissue growth.c) Foams: Foam dressings have a high absorption rate, provide thermal insulation, and create moist healing environments.d) Silvers: Silver-based dressings draw in bacteria and neutralize them, making them an excellent choice for preventing wound infections.Armstrong et.al proposed a classification model for surgical management of the diabetic foot based on fundamental variables present in the assessment of risk and indication like presence of neuropathy (loss of protective sensation), presence or absence of an open wound & presence or absence of any acute limbthreatening infection [9]. According to the classes of diabetic foot surgery, class III (curative) and class IV (emergency) procedures involve a current diabetic foot ulcer or open wound. Emergency procedures are those performed to limit the spread of acute, limb-threatening infections. This class of surgery may be performed in the presence of limb ischemia to prevent further spread of the infection. The potential for vascular intervention should be considered either concomitant with this procedure, or in the immediate postoperative hospitalization period. he goals of the curative procedure is to speed up the healing of the diabetic foot wound and prevent recurrence of this wound. Surgical decision making is heavily dependent on the type of wound and its location. It is our experience that most chronic ulcerations present in the diabetic foot are a direct result of increased plantar pressure in the presence of peripheral neuropathy. The surgical goal for these types of ulcers is to relieve the source of increase in pressure. Some of the most time-honored procedures involve some sort of bone resection. This type of procedure aids in eliminating pressure underlying the wound. In the forefoot, bone resection has been well documented as able to heal a wound faster, prevent ulcer reoccurrence, and lower the incidence of infection compared with conservative treatment [10-13]. This may include isolated metatarsal head resection [14-16], pan metatarsal head resection, transmetatarsal amputation (TMA), exostectomy, and partial calcanectomy.a. Revisional surgery for is frequently needed to control diabetic foot infections and for bony architecture may be required to remove pressure points. Such intervention includes resection of metatarsal heads or ostectomy.b. Vascular reconstruction: Vascular surgeons, radiologists and plastic surgeons should form an integral part of the diabetic foot team. Here the potential limitation of investigation or reliance on symptoms in the diabetic patient are discussed. The acute presentation of the patient with a diabetic foot may necessitate emergency drainage or abscess formation and debridement of infected necrotic tissue, if necessary, prior to formal investigation and reconstruction. Detailed investigation should include intra-arterial digital subtraction angiography, with or without color flow duplex. These investigations will help to delineate the most beneficial interventional management. This may include a combination of interventional radiological techniques, proximal and distal vascular reconstruction, and indeed the combination of femorocrural, popliteal-crural reconstruction with plastic surgical techniques. Distal reconstruction in combination with split skin grafts and/or free flap closure may also help to preserve the limb in diabetic patients with severe necrosis and infection which requires extensive debridement.c. Skin grafts, Tissue-cultured skin substitutes, Xenograft: Advanced therapies for foot wounds are saving limbs, restoring mobility, and improving the lives of many people with diabetes who suffer from non-healing foot ulcers (Figure 2). Skin substitutes can consist of bioengineered or artificial skin, autografts (taken from the patient), allografts (taken from another person) or xenografts (taken from animals). According to Dieckmann et al. skin substitutes can be divided into two broad categories: biomaterial and cellular. Biomaterial skin substitutes do not contain cells (acellular) and are derived from natural or synthetic sources. Natural sources include human cadaveric skin processed to remove the cellular components and retain the structural proteins of the dermis and collagen matrix obtained from bovine and porcine sources. Synthetic sources include degradable polymers such as polylactide and polyglycolide. Whether natural or synthetic, the biomaterial provides an extracellular matrix that allows for infiltration of surrounding cells. Cellular skin substitutes are distinguished by their origin: xenogeneic (from nonhuman species), autologous (from the patient), and allogenic (from another human). Keratinocytes and fibroblasts obtained from these sources are cultured in vitro to produce the cellular material used to make the substitute. However, the classification of skin substitutes into either biomaterial or cellular is not completely accurate since the two are combined into several wound care products. Human tissue can be obtained from human donors, processed, and used exactly in the same role in the recipient-skin for skin, tendon for tendon, bone for bone. These uses are regulated as human tissue intended for transplantation, if the proposed clinical use and manufacturing methods are consistent with definitions of “Homologous Use” and “Minimal Manipulation”. Human tissue and cells may also be used as a source of cells for culturing to produce cellular-derived material for wound healing.d. Hyperbaric Oxygen Treatment: Hyperbaric Oxygen Therapy is a treatment option for diabetic patients with a foot ulcer, where the patient inhales 100% oxygen in a pressurized chamber. This method helps the body increase the oxygen levels in the blood. It also exposes the affected tissues to more oxygen than would otherwise be present, thus allowing for enhanced healing. Hyperbaric oxygen therapy (HBOT) has been promoted as an effective treatment for diabetic foot wounds, it improves wound tissue hypoxia, enhancing perfusion, reducing edema, down regulating inflammatory cytokines, promoting fibroblast proliferation, collagen production, and angiogenesis make it a useful adjunct in clinical practice for “problem wounds,” such as diabetic foot ulcers. Hyperbaric oxygen therapy increases the saturation of oxygen in the blood, due to the enhancement of atmospheric pressure. Increased oxygen can promote white blood cell activity, encourage tissue development and induce capillary growth. This method can be beneficial for a variety of conditions but is proving exceptionally promising in the treatment of diabetic foot ulcers.e. Dietary Managements: Nutrient deficiencies have influence of wound healing in a different way. Malnutrition and/ or nutrient deficiencies can impair collagen synthesis, prolong inflammation, decrease phagocytosis (causing dysfunction of B and T cells), and decrease the mechanical strength of the skin. High-protein, high-calorie, nutrient-enriched supplements may be recommended between meals if food intake doesn’t meet a patient’s needs for wound healing. Arginine and glutamine are two amino acids that have been studied extensively for their role in wound healing. In addition, beta-hydroxy-methyl buterate, which is a metabolite of the amino acid leucine, has been linked with improved wound healing and tissue regrowth. People with diabetes do not heal as efficiently as people with normal blood sugar levels. Certain foods can also help keep your blood sugar optimal.f. blood sugar levels: Certain foods can also help keep your blood sugar optimal.Protein helps to repair tissuea. Fishb. Shellfishc. Eggs (egg whites have protein and no cholesterol)d. Cheese (low fat is better for your heart)e. Poultryf. Lean meatg. Nut butters (peanut butter, almond butter, cashew butter, etc.)Carbohydrates give you energya. Starch (bread-whole grains are best-cereal, noodles, rice, barley, kasha)b. Starchy vegetables (sweet or white potatoes, corn, peas, beans)c. Non-starchy vegetables (broccoli, green beans, asparagus, salad greens)d. Fruite. Milk (drinking milk, soymilk or yogurt)Fat allows you to absorb your fat-soluble vitamins-A, D, E, Ka. Oil (olive and canola oil are best for your heart)b. Nuts (are good for your heart and health)c. Avocado (is good for your heart)d. Margarine (pick one without trans-fat)e. Butter (use more sparingly)The following vitamins are excellent to heal wounds most efficientlyA. Vitamin C-foods with high levels:a. Peppers (especially red)b. Kiwi fruit, Tomatoesc. Citrus fruits (oranges, grapefruits)d. BroccoliB. Vitamin A-foods with high levels:a. Orange colored fruits/vegetablesb. Dark green leafy vegetablesC. Vitamin E-foods with high levels:a. Whole grainsa. Whole grainsb. Wheat germc. Dark leafy green vegetablesd. Eggs**e. Nuts and seedsD. Vitamin B-foods with high levels:a. Whole grains (wheat and oats)b. Fish and seafoodc. Poultry and meatd. Eggs**E. Zinc-foods with high levels:a. Oysters (very high)b. Beans** Egg yolks contain vitamins and cholesterol while egg whites contain proteinA. Restriction of Activity: Many evidence-based cases studies show that increase activity delays in wound healing process, so therefore it is important to minimize the activities to the affected extremitiesB. Amputation may be indicated in circumstances during Ischemic rest pain that cannot be managed by analgesia or revascularization, a life-threatening foot infection that cannot be managed by other measures, a non-healing ulcer that is accompanied by a higher burden of disease than would result from amputation. In some cases, for example, complications in a diabetic foot render it functionally useless and a well performed amputation is a better alternative for the patient.C. Ultra-MIST Therapy, non-contact, low frequency, nonthermal ultrasound has a pain-free delivery through a fluid/ saline mist that acts as the medium to deliver energy to the diabetic wound and induce fast healing.
Steps to Avoid Amputation: Implementing A Global Wound Care PlanDiagnosis of diabetes (+/_ peripheral sensory neuropathy)
AIM: Prevent the development of a diabetic wounda. Implement diabetic wound prevention care plan that includes treatment of co-morbidities, good glycemic control and pressure offloadingb. Annually perform general foot examination:c. Use 10g monofilament to assess sensory statusd. Inspection of the feet for deformitiese. Inspection of footwear for wear and tear and foreign objects that may traumatize footf. Maintain skin hydration (consider emollient therapy) for skin healthg. Offer patient education on checking feet for traumah. Ensure regular review and provide patient education
Development of diabetic wound
AIM: Treat the ulcer and prevent infectiona. Determine cause of ulcerb. Agree treatment aims with patient and implement wound care plan:c. Debride and regularly cleanse the woundd. Take appropriate tissue samples for culture if infection is suspectede. Select dressings to maintain moist wound environment and manage exudate effectivelyf. Initiate antibiotic treatment if infection suspected and consider topical antimicrobial therapy if increased bio burden is suspectedg. Review offloading device and ensure footwear accommodates dressingh. Optimize glycemic control for diabetes managementi. Refer for vascular assessment if clinically significant limb ischemia is suspectedj. Offer patient education on how to self-manage and when to raise concerns
Development of vascular disease
AIM: Prevent complications associated with ischemiaa. Ensure early referral to vascular specialist for arterial reconstruction to improve blood flow in patients with an ischemic or neuro ischemic ulcerb. Optimize diabetes control
Ulcer becomes infected
AIM: Prevent life- or limb-threatening complicationsa. For superficial (mild) infections-treat with systemic antibiotics and consider topical antimicrobials in selected casesb. For deep (moderate or severe) infections-treat with appropriately selected empiric systemic antibiotics, modified by the results of culture and sensitivity reportsc. Offload pressure correctly and optimize glycemic control for diabetes managementd. Consider therapy directed at biofilm in wounds that are slow to heal
Active management of the ulcer and co-morbidities should aim to prevent amputationa. Where amputation is not avoidable:b. Implement skin and wound care plan to manage surgical wound and optimize healingc. Review regularly and implement prevention care plan to reduce risk of recurrence or further diabetic wound on contralateral limb
Prevention of diabetic wounda. Inspect feet daily: The CDC recommends people with diabetes inspect their feet every day for cuts, blisters, calluses, red spots, swelling and other abnormalities. Regularly trim toenails straight across to avoid ingrown toenails. If cannot see or reach the feet, use a mirror or ask for the assistance of a doctor, family member or caregiver. In addition to daily examination, have the doctor or podiatrist check your feet at least once per year.b. Protect the feet from infection: Washing the feet each day is an important part of the diabetic foot care routine. Wash feet in lukewarm water (not hot water, which can scald and blister feet), and dry feet thoroughly afterward. Once dry, rub moisturizing lotion or cream on the tops and bottoms of feet. Do not apply lotion between toes, as this could foster bacterial growth. Don’t forget to put on socks and shoes, even if you are just staying in your home, to avoid stepping on something sharp and becoming injured.c. Manage/ control diabetes mellitus: Keeping the blood sugar, blood pressure and cholesterol levels in check can prevent most of the complications related to diabetes, including nonhealing diabetic foot ulcers. Work with primary care physician to develop a diabetes self-management plan that may include healthy diet, regular exercise, blood sugar monitoring, smoking cessation and adherence to medication as directed.
Summary
A diabetic wound is an open sore or wound that occurs in approximately 15 percent of patients with diabetes and is commonly located on the bottom of the foot. This article review gives a brief knowledge regarding diabetes it’s signs and symptoms, how to manage diabetic wound and other complication. Physical examination of the extremity having a diabetic ulcer can be useful in the management of diabetic wound. The staging of diabetic foot wounds is based on the depth of soft tissue and osseous involvement. A complete blood cell count should be done, along with assessment of serum glucose and creatinine levels. The management of diabetic wound requires offloading the wound by using appropriate therapeutic footwear, daily saline or similar dressings to provide a moist wound environment, debridement when necessary, antibiotic therapy if osteomyelitis or cellulitis is present, optimal control of blood glucose, and evaluation and correction of peripheral arterial insufficiency. As a human being we all have the responsibility to protect our body parts from such chronic diseases.
Conclusion
As per various evidence-based reviews clearly states that 84% of lower limb amputations have a history of diabetic wound. Diabetic wound and amputations significantly reduce the quality of life. Also, while checking on hospital admission, most of patients got admitted with diabetes. Therefore, it’s a very much important in caring diabetic patients with effective diabetic wound care for improving their quality of life.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Diabetes & Obesity please click on: https://juniperpublishers.com/crdoj/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/crdoj/CRDOJ.MS.ID.555743.php
49 notes
·
View notes
Text
Comparison of Enhanced Solubility Profile Analysis of Thermodynamic Parameters and Pharmacokinetic Profile Related to Tamoxifen Citrate Solubilisation
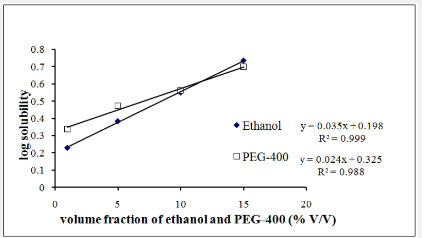
Juniper Publishers-Open Access Journal of Drug Designing & Development
Authored by Biswajit Mukherjee
Abstract
The aim of this study was to investigate the improvement of solubility of a poorly water soluble drug tamoxifen citrate (TC) by various methods such as cosolvency, micellisation, and complexation. Cosolvents (ethanol, polyethylene glycol-400), surfactants [polyoxyethylene sorbitan monooleate (Tween-80), poloxamer-407 and poloxamer-188], and cyclodextrins [β-cyclodextrin (BCD) and hydroxypropyl-β-cyclodextrin (HPBCD)] were used as solubilizing agents in this study. Solubility improvement approaches showed variable degrees of solubility improvement of TC. Among the solubilizing agents used, the modified β-cyclodextrin was found to be the most effective. The solubility of TC was enhanced to 6.31 mmolL-1 in water (about 7.1 fold solubility improvement) using 0.05% m/v hydroxy propyl-β-cyclodextrin. Different thermodynamic parameters, enthalpy and entropy, were analyzed for solubility enhancement of TC with different cyclodextrins which showed enthalpy not the entropy was the driving force for TC solubilisation. The less positive enthalpy of BCD complexation than HPBCD complexation signifies the higher solubilising efficacy of HPBCD. Pharmacokinetic study was performed using HPBCD as solubility enhancer at its optimized concentration which also resulted in improved bioavailability when compared to the bioavailability obtained with free tamoxifen.
Keywords: Tamoxifen citrate; Solubility; Cosolvent; Surfactant; Cyclodextrin; Pharmacokinetic
Introduction
Tamoxifen citrate (TC) is an antiestrogenic drug and is first choice treatment of breast cancer in both pre- and post-menopausal women. The antiestrogenic effects may be related to its ability to compete with estrogen for binding sites in target tissues such as breast [1]. Chemically, TC is the isomer of a triphenylethylene derivative. The chemical name is (Z) 2-[4-(1,2-diphenyl-1-butenyl) phenoxy]-N,N-dimethylethanamine-2-hydorxy-1,2,3-propane tricarboxylate. Following a single oral dose of 20 mg tamoxifen, an average peak plasma concentration of 40 μg L-1(range 35 to 45 ng ml-1) occurred in 4-7 h after dosing [2,3] and this indicates poor bioavailability of the drug. Poorly water-soluble drugs often provide limited bioavailability if dissolution is the rate-limiting step in overall oral absorption process [4]. Since TC is poorly soluble in water (equilibrium solubility inwater at 37 °C is 0.5 mg ml-1) [5], it is ,therefore, important to improve its solubility to ameliorate its bioavailability [6].Although there has been enormous amount of research works performed using different techniques of solubilisation, yet a comparative profile is very scarce. In this study, the effect of different solubilisation approaches such as micellar solubilisation, complexation by cyclodextrins and cosolvency on the aqueous solubility of TC has been presented in a comparative approach. An attempt has been made to provide an insight into the mechanism of solubilisation of TC particularly by complexation based on analysing thermodynamic parameters, since complexation was found to be the most successful approach among the methods tried.
Experimental Materials
Poly (ethylene glycol) 400 (SRL Pvt. Ltd., Mumbai, India), β-cyclodextrin (Hi Media Laboratories Pvt. Ltd., Mumbai, India), tween-80 (S.d. Fine Chemical Limited, Mumbai, India), absolute ethanol (Merck Ltd., Mumbai, India) were obtained commercially. Hydroxypropyl-β-cyclodextrin, poloxamer-407, poloxamer-188 were purchased from Sigma-Aldrich, Bengaluru, India. TC (Khandelwal Laboratories Pvt. Ltd., Mumbai, India) was a gift sample.Phase Solubility StudyIn each of the different approaches (cosolvency, micellisation, and complexation) of solubilisation, solubility of TC was determined by placing an excess amount of TC (10 mg) in water (5 ml), in different test tubes containing increasing concentrations (Table1) of various cosolvents, surfactants and the complexation agents so that the total volume in each case remained to 5 ml. Three sets of sample vials were prepared for each particular solubilising agent. The test tubes were shaken mechanically in a shaker water bath at 37°C for 48 h. At equilibrium (after 2 days, as preliminary studies showed that this period of time was sufficient to ensure saturation at 37°C), aliquots were removed, centrifuged for 10 min at 10000 rpm. After proper dilution with water the samples were analyzed spectrophotometrically at 275 nm using Shimadzu UV/Vis spectrophotometer (Japan) [7] taking appropriate blank solution. The cosolvents used were ethanol, poly (ethylene glycol) 400 and glycerine. The surfactants were polyoxyethylene sorbitan monooleate (Tween 80), poloxamer-407 and poloxamer-188. The complexation ligands were β-cyclodextrin (BCD) and hydroxypropyl-β-cyclodextrin (HPBCD).Thermodynamic Parameters for Different Cyclodextrin ConcentrationsThermodynamic analysis was performed by measuring the solubility measurement with BCD and HPBCD concentration (0.05% m/v to 0.5% m/v) at different temperatures (300, 310 and 320 K) (Tables 2&3). Rest of the procedure was same as the phase solubility study. Gibbs and van’t Hoff equations were used to estimate the thermodynamic parameters, enthalpy (ΔHo), entropy (ΔSo) and Gibbs free energy (ΔGo).The general form of van’t Hoff equation for calculation of thermodynamic parameters:ln K = ΔSo/R -ΔHo/RTorlog K= -(ΔHo/ 2.303R) 1/T + ΔSo/ 2.303RThe Gibbs equation gives the values of (ΔHo) and (ΔSo) and therefore, the values of (ΔGo) were calculated in each case from the equation.ΔGo= ΔHo – T ΔSoFor a plot of ln K versus 1/T, slope = –ΔHo/R and intercept = ΔSo/R were calculated.Where, K (equilibrium constant) represents either S (drug inherent solubility) or K1:1 (equilibrium constant considering 1:1 complex formation). The values of S were initially estimated from the phase solubility diagrams) [8].Pharmacokinetic Study by LC-MS/MSSwiss albino mice (either sex, 25-30 g) were purchased from registered breeders, and were given normal standard diet with tap water ad libitum. Animals were kept under a 12 hrs light dark cycle. The animals were maintained in this condition for at least one week prior to the experiment. All experiments were conducted as per the guidelines of the animal ethics committee (AEC), Jadavpur University, Kolkata.Animals were divided into two groups (10 animals in each group) and fasting condition for at least 24 h prior to the experiment. Animals from the free drug group (FD) were given tamoxifen citrate at 10 mg/kg oral dose and animals of the test group (CD) were given HPBCD (as a solubility enhancer at the concentration of 0.5% w/v) along with TC in an equivalent oral dose of 10 mg/kg. mixing in water. After oral dosing mice were anaesthetized with diethyl ether. Blood samples were collected by heart puncture technique at various time points from 0.25 h, 0.5 h, 1h, 2 h, 4 h, 8h and 24 h. Blood samples were centrifuged at 6000 rpm for 5 min and plasma were collected and stored at -80°C until further study by LC-MS/ MS.LC-MS/MS AssayWorking stocks of TC were prepared by serial dilution in HPLC grade methanol. Working stocks and blank plasma were spiked to prepare calibration control (CC) and quality control (QC) samples. Liquid liquid extraction (LLE) technique was used for the extraction of CC, QC and test samples.The plasma concentrations of TC in both the groups were determined by LC-MS/MS assay using a method described by Choi and Kang [9]. At first, 0.05 ml butyl paraben (IS) of concentration 8μg/ml in methanol was added to 0.2 ml acetonitrile and 0.2 ml of plasma sample. This mixture was vortexed and centrifuged at 13,000 rpm for 10 min and 0.05 ml of the supernatant was loaded to LC-MS/MS (LC: Shimadzu Model 20AC, MS: AB-SCIEX, Model: API 4000, Software: Analyst 1.6) for analysis. Plasma data were plotted against time and PK parameters were determined by WinNonlin software (Certara,UK).
Results and Discussion Cosolvency
Figure 1 shows straight lines in semi-logarithmic plot of TC solubility vs. volume fractions of the experimental cosolvents. Solubility study of TC with different concentrations of the cosolvents, ethanol and PEG-400 at 37°C showed that efficiency of ethanol (15% V/V) as cosolvent was higher (6.10-fold) than that of 15% PEG-400 (5.62-fold) compared to the inherent solubility of TC in water.Cosolvents are widely used in pharmaceutical industry for solubilisation purpose. They work by reducing hydrogen bond density of aqueous system and create a less polar environment in bulk [10]. This results in more solubilisation of sparingly soluble or less soluble drug molecules. Cosolvents generally possess non-polar regions which do not interact strongly with water and they decrease the capability of water molecules to squeeze out non-polar solutes from the aqueous system [11]. A relationship between the total drug solubility (Dtot) and cosolvent concentration © in a drug-cosolvent-solvent mixture has been described by using the equation, log Dtot = log Du+ σC [12,13] where, Du and σ are drugs solubility in water and cosolvent solubilisation power, respectively. The value of σ is inversely correlated with the polarities of both the solute and the cosolvent. The more non-polar the solvent and the solute, the larger is the σ value [14].Figure1 shows straight lines in semi-logarithmic plot of TC solubility vs volume fractions of the experimental cosolvents. The findings suggest exponential increase in TC solubility with the increasing concentration of the cosolvent, ethanol and PEG- 400. Both ethanol and PEG-400 obey 1st order solubilisation kinetic. For a single non-polar solute, cosolvent solubilisation power ‘σ’ depends only on cosolvent polarity [14]. Table 1 indicates that solubility enhancement of TC follows the cosolvent order as: EtOH (σ: 0.036) > PEG-400 (σ: 0.025). The less polar is the cosolvent, the more effective it is at disrupting hydrogen bonding interactions in water molecules [15]. In the present study, more efficient improvement of solubility of TC by ethanol may be because ethanol is the less polar solvent than PEG-400 [14].Dtot- total drug solubility in a mixed solvent and cosolvent concentration ©. Du- drug solubility in water. BCD: β-cyclodextrin; HPBCD: hydroxyl propyl-β-cyclodextrin.MicellizationFigure 2 shows the effects of poloxamer-407, poloxamer-188 and Tween 80 on solubility profiles of TC, respectively which indicates that TC solubility was enhanced in the surfactant order as: poloxamer-407 (5.36-fold) > Tween80 (5.30-fold) > poloxamer-188 (3.20-fold).Micelle formation is one of the important mechanisms to solubilise solutes. Incorporation of solute molecules to the micelles depends on the degree of non-polarity of solutes and their micellar partitioning performances [11].The more nonpolar the solute, the more likely it is to be incorporated near the nonpolar core or center of micelles [11]. Researchers have described a relationship of micellar surfactant concentration and solubility of solute (drug) [15,16]. Total drug solubility (Dtot) depends on inherent solubility (Du) and concentration of micellar surfactant (S) (i.e., the total surfactant concentration minus the critical micellar concentration) and is presented by Dtot= Du + κ D uS[10], where κ is micellar partition coefficient. Product of κ and Du reflects number of surfactant molecules required to solubilise one solute molecule [14].Table 1 indicates that TC solubility was enhanced in the following sequences: poloxamer-407 (κ: 2.28) > Tween-80 (κ: 0.97) > poloxamer-188 (κ: 0.25). Poloxamer-407 was found to improve the solubility of TC maximally among the surfactants tested. Due to higher micellar partitioning, more non-polar TC molecules were incorporated in the poloxamer-407 micelles.ComplexationFigure 3 shows a linear relationship between TC solubility with different concentration of BCD and HPBCD used to solubilize TC. HPBCD showed higher solubilisation of TC than natural BCD. The solubility improvement of TC was about 5.8-fold with 0.5% m/v BCD and 7.1-fold with 0.5% m/v HPBCD compared to the original solubility of TC in water.The solubility of TC with different cyclodextrins has been described using the following equation, Dtot = Du + KDuL[14], where L is the total ligand concentration, and K is the complexation constant/ solubilisation capacity of the drug-ligand complex. Dtot and Duhave been described earlier. Table 1 shows that the solubilisation capacity K1:1 of HPBCD (0.68) is slightly greater than that of natural BCD (0.48). The modified β-cyclodextrins have been widely used and reportedly have higher solubilisation capacity than natural BCD for most drugs [17,18]. Complexation constant or solubilising capacity, K, depends on the geometry and polarity of the solute molecules and compatibility between the solute and the cyclodextrin cavity [15].Except for differences in size, the overall geometries of the cyclodextrins are similar. Each having a torus equals to the length of the appropriate number of glycosides. The derivatized cyclodextrins are characterized by the nature, position and degree of the substituents and there they differ in the available sites. Size and structure of the molecules are important for formation of inclusion compounds. Structurally smaller drug insertion (as compared to CD cavity) is not energetically favored and for appropriately larger solutes, they can fill most of the CD cavity and form the more stable complexes. Thus, TC solubilisation capacity of HPBCD is higher by forming HPBCDTC inclusion complex than that of BCD. Again, equilibrium analysis of drug cyclodextrin complex within the experimental concentration range (data not shown) was found to be of 1:1 stoichiometry which has been reported to happen with a low ligand concentration, as at higher ligand concentration higher order complexes are formed [14]. In conclusion, HPBCD is a better complexation ligand for TC than natural BCD.Thermodynamic ParametersThermodynamic parameters calculated are shown in Table 1. It shows the effect of increasing experimental temperatures and concentrations of both the cyclodextrins on TC solubilisation. The solubility of TC was increased with both the conditions. TC solubility was characterized by a negative ΔG°, indicative of spontaneous dissolution and positive ΔH° indicative of endothermic dissolution [19]. Van der Waal interactions, hydrogen bonding, hydrophobic interactions, release of highenergy water molecules from the cavity of cyclodextrin and release of strain energy in the ring of cyclodextrin structure etc. are the known driving forces for the formation of cyclodextrin inclusion complexes with foreign molecules [20]. These interactions cause conformational changes in cyclodextrin structure, dissolvation to complex stability and drug solubility. Breakdown of water structure around a solute creates a higher positive ΔS° and a positive ΔH° known to be governed by hydrophobic interaction [21]. In the present study dissolution thermodynamics of TC in aqueous BCD and HPBCD were characterized by a positive ΔH°(Figures 4&5), indicative of endothermic dissolution [19].Reports suggests that complex formation with BCD and HPBCD yields negative or positive ΔH°and negative or positive ΔS° [22]. In our study both BCD and HPBCD complex formations resulted in positive ΔH° as well as positive ΔS°. Breakdown of water structure around TC creates a large positive ΔS° and a positive ΔH° (Tables 2&3), apparently governed by hydrophobic interactions [23]. Positive ΔS° for TC may be attributed to transfer of TC from polar aqueous medium to nonpolar cavities of CDs [18]. Positive ΔH° indicates endothermic dissolution thermodynamics of TC in aqueous BCD and HPBCD. In this experiment, the enthalpy difference (ΔH°) decreased with the increasing concentrations of BCD and HPBCD.This is favourable for a thermodynamic process to happen and in this case, enthalpy was the driving force for complexation of TC with BCD and HPBCD. The entropy difference (ΔSo) decreased with (Tables 2&3) increasing BCD and HPBCD concentrations. The entropy was not the driving force for complexation of TC with CDs. With respect to the HPBCD, the complexation of natural BCD with TC is characterized by less positive enthalpy, the contribution from which the solubility improvement profile of TC with BCD is lesser than HPBCD.Pharmacokinetic AssayThe study result of pharmacokinetic assay by LC-MS/MS was represented by the plasma concentration-time profile (Figure 6).The pharmacokinetic parameters of tamoxifen as a free drug (FD) and along with a solubility enhancer HPBCD (HCD) (Table 4) revealed that Area under the curve (AUC) and maximum concentration reached (Cmax) for tamoxifen was much higher in case of CD than FD which indicated that cyclodextrin had a clear effect on improving the bioavailability of tamoxifenMean±SD (n=6), AUC; area under the plasma concentration time curve from 0 h to infinity, Cmax; peak concentration, Tmax; time to reach the peak concentration, MRT; mean residence time; CL; total body clearance. HCD; hydroxy propyl β cyclodextrin added to tamoxifen, FD; tamoxifen as a free drug.On other hand, clearance rate was higher for FD in comparison with HCD which may be due to the faster elimination of tamoxifen when administered alone (FD) than with a solubility enhancer (HCD). After in vivo administration, free tamoxifen due to its poor solubility was absorbed less but eliminated quickly after absorption. On the other hand, tamoxifen-HPBCD complex was absorbed faster and distributed in the system with a slower elimination.
Conclusion
The water solubility of TC was increased 7.1-fold in the presence of 0.5% m/v HPBCD, compared to 0.5% m/v natural BCD (increase 5.8-fold). Thermodynamic parameters derived from TC solubility in the presence of various concentrations of BCD and HPBCD at several temperatures reveal that the solubility of TC increased with an increase in temperature. Besides, TCBCD complex formation was a characteristic of a very strong hydrophobic interaction. Furthermore, pharmacokinetic study was also representing the similar observation with higher Area under the plasma concentration-time curve and peak plasma concentrations of TC, when administered along with HPBCD. However, clinical trial will be needed to conclude the simultaneous oral administration of cyclodextrin along with tamoxifen to enhance the bioavailability in human.
For more Open Access Journals in Juniper Publishers please click on:
For more articles in Open Access Journal of Drug Designing & Development please click on: https://juniperpublishers.com/napdd/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/napdd/NAPDD.MS.ID.555624.php
25 notes
·
View notes
Text
Respect for Parliament? Do VIP Criminals Want Complete Immunity for Committing Crimes, Corruption and Human Rights Violations?
Juniper Publishers-Open Access Journal of Social Sciences & Management studies
Authored by Yunis Khushi
Opinion
Sanctity of vote, respect and dignity of parliament, dignity and respect of elected members and other related issues have become central and extremely hot topics of debates in media since the disqualification of Mian Nawaz Sharif as Prime Minister as well as politician and chairman of Muslim League N for rest of his life. The questions that need to be answered are: Have the current or the previous Parliaments been true representatives of the people of Pakistan? If not, then why respect such a parliament, which has not worked as representative of the people? Should white collar VIP criminals continue to enjoy complete freedom to loot the national wealth? Should so called elected representatives be given total and complete immunity from being answerable to courts of law for crimes they commit? Why should people of Pakistan give respect to the so-called elected representatives who do not work for the interests of the masses and long-term interests of the country? Why should people respect such representatives who enjoy best state facilities and loot national wealth and invest it abroad i.e. Dubai, USA, Australia and UK? Why should masses respect such parliamentarians who treat masses as mere insects? Why should people of Pakistan respect such parliamentarians who do not bother to even think of doing any legislation for the betterment of the masses? Why should people respect such parliamentarians who have destroyed all the state institutions just for the sake of their vested interests? Do parliamentarians understand the sanctity of vote? Have they given any respect to the votes of the masses?The crimes and wrong-doings of the parliamentarians against the masses and the country have been as below: They have treated masses as their property and slaves. They have been subservient to their party leadership. They acted as kings in the areas they controlled. They only legislated for protecting their vested interests or the interests of their leadership. They never made any legislation for the betterment of the masses or keeping in view the long-term interests of Pakistan. They promoted crime, extremism, terrorism and poverty in the country. They corrupted all the state institutions just to protect their vested interests. They have been committing worst kind of human rights violations including rape, gang rapes and murders against the people of Pakistan. Many of them are involved in running private jails, bonded labor etc. Majority of them are feudal lords, industrialists and businessmen and they do not bother to pay income taxes to the state. By selling their votes in Parliament for millions of rupees to the candidates for Prime Minister ship, President or Chairman Senate, time and again they proved that they are saleable commodities, and anyone can buy them for heavy amounts of money. They use terror, goons and guns to get votes from the poor in their constituencies. They do not have consciousness or courage to challenge the anti-masses and anti-Pakistan policies of their party leadership. They are more after money through commissions and perks rather than solving the problems of their voters.They promoted moral degradation, law and order and criminality in the country. Majority of them is without any ability to read and analyses the legal documents and legislation draft and offer any positive and constructive criticism. They are just dummying to act as yes-men and women to obey the orders of their party leaders. Since 60 per cent of the population lives below the poverty line so they buy votes of poor for RS.1000/- or a bag of flour and then forget the very poor that they are representing. They have strong control and hold on the bureaucracy and police of their areas and use them to crush their opponents and people of their constituencies. They take huge amounts as loans and never pay them back. They invest the looted wealth in Dubai, Switzerland, England, Australia and USA. They are responsible for promoting political instability, economic dependence, poverty, hunger, suicides, unemployment, crime, human rights violations, insecurity, corruption and many other evils in Pakistani society. They have been working against the long-term interests of the country and its people. They worst traitors and enemies of Pakistan and its people. They have never given any respect to the people of Pakistan and their votes.The billion-dollar questions are: How can the parliamentarians who do not have any sanctity for the votes of people of Pakistan demand that they should be respected only because they have come through votes of the people? Why should they be called peoples’ representatives only because they get only 30 per cent votes and that too by rigging elections and using money and violence during the electoral process? Why should people of Pakistan respect the bunch of elite robbers who are the worst enemies of Pakistan and its people? Why should people of Pakistan or judiciary care for the sanctity of the persons who never cared for the sanctity of the votes of the people, sanctity of judiciary and other state institutions? Why do they constantly demand that institutions must remain in their limits? Why do they continue to demand that Courts must do their job and the politicians must be allowed to do their job? What have politicians done for the people of Pakistan during the past 70 years? Should politicians be allowed to do the very job that they have been doing for the past 70 years i.e. of promoting crime, poverty, corruption, human rights violations, political instability, dependency of Pakistan on other powers, and extremism and terrorism? Are they demanding total immunity from being questioned by any court of law for committing crime, promoting poverty, corruption, human rights violations and other wrongs to Pakistan and its people?The problem is not that they are bothered about the sanctity of the vote, rather, they are worried about the tightening of noose around them by judiciary for corruption they have been committing for the past more than 40 years. Also, because they want total immunity from being questioned by any institutions and they want a free hand for committing corruption and for playing with the lives and dignity of the people of Pakistan.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Social Sciences & Management studies please click on: https://juniperpublishers.com/asm/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/asm/ASM.MS.ID.555575.php
37 notes
·
View notes
Text
Experience Outside of Clinical Trial with Everolimus
Juniper Publishers-Open Access Journal of Research and Reviews
Authored by Beatriz Losada Vila
Keywords
Keywords: Metastatic; Visceral; Chemotherapy; Letrozole; Hematological; Capecitabine.Go toIntroductionLuminal metastatic breast cancer has undergone a major breakthrough thanks to the emergence of mTOR inhibitors to the progression of aromatase inhibitors as shown by studies such as BELLE-2 and BOLERO-2 (1,2). The aim of our study is to reflect the clinical characteristics of patients treated with ever olimus in our Hospital as well as the toxicity derived from them.
Material and Methods
Retrospective study of 5 patients diagnosed in the University Hospital of Fuenlabrada in treatment with ever olimus outside clinical trials during last 2 years.Go toResults100% of the patients are <65 years old (1 premenopausal, on treatment with gnRH analogue), with an ECOG 0-1 in 100%. 40% started as a metastatic disease. Disease-free interval was greater than 2 years in 100% of the patients.20% present 3 or more metastatic locations, while the remaining 80% present between 1-2 locations. 100% have visceral involvement. The indication of everolimus in the 5 patients was as much in 1st line as in 2nd, 3rd, 4th and 5th line. The patient who received everolimus in the first line was due to progression to aromatase inhibitor during the adjuvant setting. Regarding the treatments previously received, 60% were treated with fulvestrant, while also 60% had previously received chemotherapy for metastatic disease. 80% were on exemestane in combination with everolimus, while 20% combined it with letrozole. The starting dose of everolimus was 10 mg in all patients. The median time on everolimus was 7.5 months (2-14), presenting in 60% (3/5) toxicity, being 2/3 in the first 15 days and 1/3 in the following 15-30 days. A patient continues with everolimus at present. The most frequently reported toxicity is as mucositis in 60% (2/3 grade 3, 1/3 degree 2) that requires dose delay in all of them and dose reduction to 5 mg in 2/3. The second most frequent toxicity was pneumonitis (2/5 = 40% grade 1 and 2 respectively). All patients received mouthwash with dexamethasone prior to the onset of everolimus. As a hematological toxicity, only grade 1 plaquetopenia stands out in 20%. The maximum response was in the form of stability in 3/5 (60%), no partial or complete reduction, while progression was in 2/5 (40%) at the first re-evaluation test [1,2].Treatment regimens that received the progression were hormonal therapy (fulvestrant) in 20% while the remaining 60% were on chemotherapy with nab paclitaxel, capecitabine or the combination of gemcitabine + vinorelbine. One patient (20%) continues with everolimus as we presented previously.
Conclusion
a. The median time on everolimus was 7.5 months, requiring dose reduction to 5 mg in 60% of patients.
b. The most frequently reported toxicity is as mucositis and pneumonitis.
c. The profile of patients who are being treated outside the clinical trial are patients <65 years with ECOG 0-1 and several metastatic localizations (visceral involvement).
d. Chemotherapy is the treatment most used when progression.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/journals.php
For more articles in Open Access Journal of Reviews & Research please click on: https://juniperpublishers.com/arr/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/arr/ARR.MS.ID.555625.php
32 notes
·
View notes
Text
Managing Felons in the Emergency Department

Juniper Publishers-Open Access Journal of Anesthesia & Intensive Care Medicine
Authored by Larry B Mellick
Short Communication
The management of felons is another myth that needs to be busted or at least seriously adjusted.Felons are pyogenic infections of the pulp space of the distal finger or thumb.These infections are essentially a compartment syndrome of the finger pad.However, this is not your typical compartment syndrome because the pulp of the fingertip is divided into multiple small compartments by 15 to 20 septa that extend from the periosteum to the skin(Figure 1). The inflammatory edema that results because of the infection causes significant pain and tissue necrosis may result.Because these septa attach directly to the periosteum, osteomyelitis may develop.On the other hand, a bonafide abscess may or may not develop and a sizeable fluid collection will usually not be present.As demonstrated in the screenshot below, (Figure 2) treatment recommendations for felons are heavily weighted towards incision and drainage.In the past through and through, hockey stick or fish mouth incisions have been recommended.However, current recommendations seem to emphasize a less aggressive approach.For example, a unilateral longitudinal approach is recommended because it spares the sensate volar pad and is felt to achieve adequate drainage.If the felon points toward the volar fat pad, a longitudinal volar approach is recommended.After the incision is made the septa are dissected using a blunt technique and a small wick is often recommended.Here is where the common management recommendations and I part ways.First, these recommendations are based purely on consensus and have almost no supporting evidence-based literature.The research is essentially non-existent, and these treatment recommendations come from consensus opinions based on clinical experience[1]. Nevertheless, on the surface these recommendations would seem to make sense.If we are dealing with a compartment syndrome of the finger, why wouldn’t a finger fasciotomy be the desired intervention?And, in addition to releasing pressure within the septa, one might simultaneously drain an associated abscess.But, I would argue that the fasciotomy typically done in compartment syndromes involves the release of a continuous fascia sheath surrounding a large, well defined and tightly enclosed extremity compartment with clearly identified neurovascular bundles. In the fingertip, we are dealing with 15 to 20 small compartments created by fibrous septa and a neurovascular bundle made up of very small branching nerves and blood vessels that are not easily avoided by the scalpel blade.The truth is that the highly sensory and vascular fingertip is dependent on the health of these small, branching nerves and blood vessels.Additionally, finger pad stability is reportedly dependent on these septa not being seriously violated. In fact, it is for this reason that the more extensive fish mouth or hockey stick (“J”) incisions are no longer recommended. The truth is that I, personally, think that most felons can be treated with antibiotics alone.And, with the easier accessibility of ultrasound machines in the emergency department we can easily determine which felons contain sufficient abscess collections needing to be drained.Using techniques to avoid near field acoustic distortion such as a water bath or large amounts of ultrasound gel we can easily determine the presence or absence of a fluid collection(Figure 3).Once purulent fluid collections are noted a decision can be made as to whether they are large enough to deserve incision and drainage.Very small fluid collections should be left alone or aspiration with an 18-gauge needle can be attempted.Even if purulent material is not successfully aspirated, that large needle can be redirected several times to decompress tissue spaces within the finger pad (Figure 4). Following the needle decompression maneuvers the fingertip is massaged vigorously to further decompress the finger pad.Often serosanguinous fluids will be expressed with this technique and afterwards a less indurated fingertip may be noted.If a sizable abscess is noted, a simple stab incision with the sharp tip of a number 11 blade into the abscess localized by ultrasound is recommended. Blunt dissection afterwards may be necessary but should not be extensive or prolonged.Finally, radiographs to search for evidence of an osteomyelitis or a foreign body, digital blocks with a long acting anesthetic to control pain and appropriate antibiotics to cover MRSA infections are other important management recommendations. In summary, a kinder, gentler and less aggressive incision and drainage approach is being recommended.Well known potential complications of a felon and felon drainage include an anesthetic fingertip, a neuroma, and an unstable finger pad. These complications can be best avoided by a more surgically restrained approach that is based on appropriately performed ultrasound examinations.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/journals.php
For more articles in Open Access Journal of Anesthesia & Intensive Care Medicine please click on: https://juniperpublishers.com/jaicm/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/jaicm/JAICM.MS.ID.555725.php
8 notes
·
View notes
Text
Bioactive Potential of Turbinaria Conoides (J Agardh) Kuetz: In vitro and In vivo
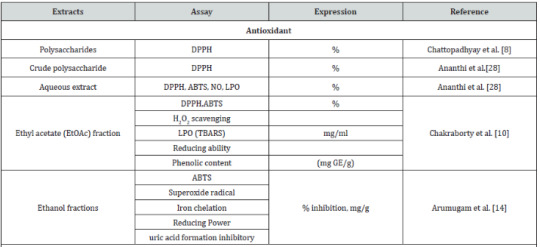
Juniper Publishers-Open Access Journal of Bioequivalence & Bioavailability
Authored by Ponnan Arumugam
Abstract
Brown seaweeds including Turbinaria conoides have been used as food since ancient times which are widely consumed in Asian region than that of in Europe and America. Though, the chemical composition varies with species, habitat, maturity and environmental conditions however they are excellent sources for the bioactive phytochemicals with rich dietary fiber, minerals, non-digestible polysaccharides and capacity to absorb inorganic substances from their surroundings. The main bioactive phytochemicals are steroids, phenolics, flavonoids, reducing sugars, fucosterol, sulfated polysaccharides including fucoidan, neutral glucan, guluronic and alginic acid. These phytochemicals are responsible for the following biological properties such as antioxidant, anti-inflammatory, antimicrobial, and anti-cancer. Therefore, in the present work was clearly documented about the bioactive potential of T. conoides with respect to their phytochemicals in both model of in-vitro and in-vivo.
Keywords: Brown algae; Turbinaria conoides; Phytochemicals; Biological activities
Introduction
It is well known that marine algae have budding source because of their numerous health-promoting effects including antioxidant, anti-inflammatory, antimicrobial, and anti-cancer [1,2]. Particularly, brown seaweeds gripped with rich novel antioxidants which are more acceptable than synthetic /chemical components [3]. Henceforth, marine macroalgae are believed to exhibit potent biological impact especially due to phenolic compounds as well as carotenoids, ascorbic acid, glutathione, sulphated polysaccharides, fucoxanthin, astaxanthin, polyphenols, phlorotannins, phospholipids, flavonoids, bromophenols and so on [4,5]. This rich bioactive phytochemicals are also there pretty in Turbinaria. It is brown algae belong to the family of Sargassaceae (brown algae) under the order of Fucales. It is consist of only 22 species so far described in which highest diversity was found in south west Asia akin to India, Srilanka where documented around 14 species. T. turbinate was only present in the Atlantic Ocean where as three species such as T. conoides, T. decurrens and T. ornate found in the South Pacific Ocean [6]. It traditionally been used as a fertilizer, insect repellent, pesticide, anti-bacterialcidal and also antioxidant, anti-inflammatory, and anti-cancer due to bioactive phytochemicals [7,8]. Apart, essential components digestible proteins along with mineral salts (K, Ca, and Fe) and polyunsaturated fatty acids along with wealthy source of dietary fiber and iodine content which play an immense role in enhancing the food quality and biochemical homeostasis [9]. Therefore, in the present review work was aimed to illustrate the potential biological properties of T. conoides with respect to their phytochemicals in both model of in-vitro and in-vivo.Antioxidant and its phytochemicalsVarious methods are essential to give an overall idea about the broad spectrum of antioxidant activity of phyto/chemical components [10]. Radical scavenging is one of the most powerful mechanisms by which antioxidants inhibit oxidation process. Many in-vitro methods has been used to examine scavenging of free radicals in which most often used are ABTS Radical cation, DPPH radical, and reactive oxygen species (ROS), such as superoxide anion, hydrogen peroxide, peroxyl radicals, hydroxyl radical, singlet oxygen and peroxynitrite. ROS are responsible for oxidative damage in the human body as well as in the food samples [11]. ABTS oxidized to give the radical cation (ABTS.+) as blue in colour and decolorized by water-soluble and lipid-soluble food samples/extracts and is expressed as TEAC (Trolox equivalent antioxidant capacity) [12,13]. Using the method, total antioxidant activity (TAA) of T. conoides was documented in the range 46-85% in hexane, dichloromethane, ethyl acetate and aqueous fraction (Table 1). Relative antioxidant activity (RAA) was also found ≥1 in the ethyl acetate fraction than that of other fractions. Apart, the highest superoxide radical scavenging activity was reported in ethyl acetate fraction (77% at the 80μg/ml) and better than ascorbic acid (74% at 30μg/ml) [14].In general, metal ions (Fe2+) can also kindle and speed up oxidative damage later on leads to lipid peroxidation which is inhibited by chelators either decreasing metal reactivity or by physically partitioning the metal away from the lipids [15]. It is well know that bioactive compounds like phenolic acids, flavonoid, quercetin, and phenolic glycosides are potentially participate to chelate metal ions which is determine by Spectrophotometry [10]. Iron chelation and uric acid inhibition activities of ethyl acetate fraction of T. conoides were reported in the range of 15-70% [14]. The reducing capacity assay is one of the methods to reduce the oxidative damage by inhibiting the peroxidation process. This process can be done by low molecular weight antioxidants which is able to donate electrons to reactive oxygen species. It can be determined by simple methods:a) The FRAP assay, based on the reduction of the Fe3+/ tripyridyltriazine complex [16],b) The direct reduction of Fe3+ ferricyanide complexes andc) Electrochemical methods [17,18]. Reducing power exhibited by solvent extracts of Turbinaria spp. was comparatively higher than α-tocopherol [19].Antimicrobial and its phytochemicalsAntimicrobial properties of T. conoides were determined by disc diffusion method which was well documented by many research articles (Table 1). Arumugam P et al. [14] reported that among the four solvent fractions of T. conoides, ethyl acetate fraction exhibited highest antibacterial activity which was comparable to the standard, streptomycin against Bacillus subtilis, Enterococcus faecalis and Pseudomonas aeruginosa. Similarly, out of four solvent fractions, petroleum ether extract reported to be showed effective antibacterial activity [20]. The antimicrobial activity of T. conoides was also reported in dose dependent activity of all four extracts and highest activity exhibited at 500μg/mL [21]. It is mainly due to secondary metabolites like phenolic compounds which may explore inhibiting effect on microbial growth based on their chemical constitutions and concentrations [22]. Consecutive extraction of T. conoides with n-hexane, cyclohexane, methanol and ethanol: water (1:1) was also documented with their antibacterial and antifungal activities by disc diffusion method. In which, cyclohexane extract was possessed a broad array of antibacterial activity and exhibited remarkable antifungal property over the other extracts [23]Anti-inflammatory, anti-genotoxicity and its phytochemicalsDuring the oxidative damage of cell or tissue, several inflammatory mediators such as histamine, bradykinin, serotonine, and prostaglandins are released and stimulate the inflammation and nociceptors by the induction of pain [24]. These mediators are occupied in tissues with high content of water and plasma during arachidonic acid metabolism via cyclo-oxygenase and lipo-oxygenase enzyme pathways [25]. The first phase of inflammation begins immediately up to an hour after injection of carrageenan by the release of histamine and serotonin whereas the second phase started after one hour and up to three hours by the release of bradykinin, protease and prostaglandins [26]. Antiinflammatory effect of ethyl acetate fraction of T. conoides were reported to be significantly (P < 0.05) better than that of control and indomethacin (Table 1). The reduction of paw volume was found to be dose dependent. The acetic acid induced abdominal writhes in mice were recovered significantly from all the tested doses of T. conoides. Ethyl acetate fraction of T. conoides might have capable of reduce inflammation through stabilizing the lysosomal membrane. In addition, the analgesic effect of T. conoides on the tail immersion-test in mice was found to be dose dependent and significantly reduce the pain response by the increase of reaction [27]. Recent report on T. ornate extract revealed their better anti-inflammatory and free radical scavenging property due to fucoidan like sulfated polysaccharides [28]. T. conoides reported to have better antipyretic activity by restoring many hematological and biochemical parameters under toxic environment [29]. In general, exposure of any environmental toxin/genotoxin leads to genetic damage which is determined by mouse bone marrow micronucleus assay described by [30]. For each bone marrow/peripheral blood cells (experimental/control), 2,500 polychromatic erythrocytes (with or without micronuclei) and a corresponding number of normal chromatic erythrocytes (NCEs) were scored under a light microscope. Ethyl acetate fraction of T. conoides reported to be 72% anti-genotoxic activity against 4-NQO induced genotoxicity [27]. These biological activities of T. conoides are mainly due to rich source of bioactive compounds such as fucosterol, sulfated polysaccharides fucoidan, neutral glucan, guluronic and alginic acid [28,31].Anticancer and its phytochemicalsCytotoxicity assay has been considered as the cell killing property of a chemical compound which is independent mechanism from the programmed cell death pathway [32]. Cytotoxicity of ethyl acetate fraction of T. conoides was reported to be significant and comparable to the standard of quercetin (Table1). Hence, cytotoxicity and antioxidant of T. conoides were well correlated and concentration dependent. The anticancer analysis exhibited that the number of accumulated cancer cells was significantly (p < 0.05) higher in the proliferative G0/ G1 phase and a significant decrease in the S phase, after 48h of treatment with ethyl acetate fraction of T. conoides. Similarly, T. conoides showed (43%) statistically (p < 0.05) significant increase of apoptotic cells than that of quercetin standard (32%, 80 μg/ml) [15]. Other reports revealed that cell cycle arrest leads to increase in sub-G0/G1 cell population after treatment with increasing doses of linalool terpenoid [33]. Cyclohexane extracts of T. conoides exhibited effective cytotoxicity in human embryonic lung cells [24]. Anticancer activity of fucosterols obtained from T. conoides was explored in various cancer cell lines [8]. Steroid from ethyl acetate extract of T. conoides reported to be effective cytotoxic in HeLa cells [34]. Various extract obtained from a variety algae collectively demonstrated that the brown algae have a potential source of phytochemicals exhibiting biological activities on tumor cells [35].
Conclusion
It is well know that T. conoides possess large content of dietary fiber, minerals, steroids, phenolics, flavonoids, reducing sugars, fucosterol, sulfated polysaccharides including fucoidan, neutral glucan, guluronic and alginic acid. As results, it exhibited different biological properties such as antioxidant, antimicrobial, anti-inflammatory and anti-cancer. Many articles revealed that cyclohexane and ethyl acetate extracts/fraction of T. conoides have potential bioactive phytochemicals with different biological properties.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com
For more articles in Open Access Journal of Bioequivalence & Bioavailability please click on: https://juniperpublishers.com/mabb/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/mabb/MABB.MS.ID.555625.php
42 notes
·
View notes
Text
Characterization of Infections Associated with Health Care in Pediatrics Bogotá 2017-Juniper Publishers
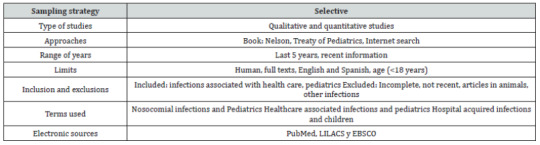
Juniper Publishers-Open Access Journal of Pediatrics & Neonatology
Authored by Maria C Mejía
Abstract
Background: Infections associated with health care (iahc) are all infections contracted by a patient during treatment in a hospital or other health center, and that said patient was not and was not incubating at the time of admission. In the world, 1 in 20 inpatients are affected, and in colombia the incidence is 5.9% of all hospitalized patients.
Objective:To describe the characteristics of HAI in pediatrics and to characterize the terms used during the care of pediatric patients with HAI.
Methods: Descriptive study divided into three phases; phase 1: a systematic search was performed on HAI in pediatrics in ebsco, pubmed and lilacs; phase 2: clinical cases of infections were designed, which were delivered to health professionals who had contact with the pediatric population, requesting that they make a brief analysis of the cases to make a theoretical model of predictive or present factors at the time of diagnosis, phase 3: the records of patients diagnosed with HAI during the period between 2014-2016 were reviewed and the demographic, social and clinical characteristics of these patients were identified. Frequencies were calculated, and the qualitative data were analyzed atlas ti 8.0.
Results: In the systematic search, predictive terms of common HAI were identified in the three databases as neonates, male sex, surgery among others, terms used by health professionals were obtained that coincided with those found in the scientific literature and finally were identified and analyzed the HAI cases of a third level clinic, finding an HAI rate of 0.46 per 100 hospital discharges.
Conclusion: There are terms that can be interpreted as predictive factors contributing to the early diagnosis of a HAI.
Keywords: Cross infection; Pediatrics; Forecasting
Background
The world health organization (who) defines as an infection associated with health care (HAI) “any infection contracted by a patient during his treatment in a hospital or other health center, and that said patient did not have nor was incubating at the time of your entry. “ the HAI can affect patients in any type of environment in which they receive health care, they are the most frequent adverse event during the provision of health services, and no institution or country can claim to have solved the problem [1]. A study conducted by the who showed that more than 1.4 million people around the world suffer complications from infections acquired in the hospital; the most frequent infections being: those related to surgical wounds, urinary tract and lower respiratory tract, with higher prevalence in the surgical, orthopedic and intensive care unit (icu) services [2]. This phenomenon increases the morbidity and mortality of the users of the health system, increases the costs of the system, constitutes a biological risk for professionals, involves legal medical situations and also influences the quality aspects of the health service provider [3]. According to the who, an average of 8.7% of hospitalized patients have hais, of which 4384 are children [4]; the pan american health organization (paho) estimates that hais affect one in every 20 hospitalized patients, which corresponds to a total of 4.1 million patients per year, of which around 37,000 die [5]. In canada, some 220,000 hospital infections per year contract, resulting in 8,000 deaths related to this cause; in latin america, the prevalence of HAI is between 5% and 12% of hospitalized patients [6]. In chile, there are about 70000 cases of HAI and this has a cost of approximately usd 700,000. In colombia, the incidence of HAI is 5.9% of the total number of hospitalized patients and in bogotá it is 2.4 per 1,000 hospital discharges. In the pediatric population, the incidence of mortality from hais is 1.7 deaths per 1000 live children [7,8].In colombia, the national institute of health (ins) together with the national system of surveillance in public health (sivigila), responsible for providing information on events that affect the health of the colombian population in a systematic and timely manner [9], has two tools for the notification of cases the first corresponds to epidemiological prevention guidelines and control of HAI [10] and diagnostic criteria for infections associated with health care to be used for notification to the subsystem of epidemiological surveillance of iacs [11]; the second tool is a web application of the national subsystem for surveillance of infections associated with health care - HAI designed for the mandatory notification of infections associated with medical devices, antimicrobial resistance and antibiotic consumption by primary generating units of data (upgd); these tools facilitate the analysis of epidemiological indicators and the generation of reports [12,13]. Despite the implementation of the aforementioned tools, in the first quarter of 2017 there was a decrease in the reporting of HAI cases associated with the use of devices in 52.77% compared to the same period of 2016, a situation that can be be related to weaknesses in the surveillance processes of the upgd and the difficulties in the handling of the notification tool, this may correspond to the absence of an opportune diagnosis, since the mandatory notification to sivigila is made immediately after having a confirmed diagnosis of HAI, that is, after identifying an infectious process, in order to initiate antibiotic management; therefore, it is a late notification that does not lead to the prevention of the event and yes, to the increase of the bacterial resistance [14].There are multiple options for an early diagnosis of HAI, which are divided into two groups; a clinical one, corresponding to signs and symptoms, which must be evaluated by medical personnel and a paraclinical one that includes laboratory tests [15]. In the last group, the blood culture stands out as the “gold standard” for the diagnosis of HAI and biomarkers such as simple pcr and pcr with modified dna, the latter generates an almost immediate report of the presence of an infection; procalcitonin, which has become a useful tool, both for diagnosis and for monitoring medical treatment; interleukin 6, definitive to define the treatment of HAI; endotracheal aspirate and catheter culture, among others [16-21]. Additionally, different diagnostic or predictive scales are available to evaluate infections in pediatrics, which relate clinical variables with laboratory parameters and apply to hais, among which are nosep i / ii and newborn scale of sepsis (sos), among the most used [22]; there are even systematized tools that emit alerts when detecting a possible HAI, achieving an opportunity in the diagnosis and treatment of the infection, however this type of tools are barely in the early phase of implementation and there are still no clear results in the hospital community [23]; taking into account that colombia is a developing country, there are limitations to the use of certain paraclinical exams, mainly due to the cost that they generate for the health system; what conditions a diagnosis of HAI based on the clinical examination and laboratory tests, such as simple pcr, the blood count; and the blood culture that can take about 48 hours to identify definitive results that allow clinical behaviors to be taken. For this reason, the initial treatment is empirical and this contributes to the increase of the bacterial resistance (24). The objective of this research is to describe the demographic and social characteristics, as well as the clinical characteristics of the patients and the HAI in pediatrics and to characterize the terms used during the care of pediatric patients with HAI.
Methods
A descriptive study composed of three phases was carried out.First phaseA systematic search was carried out in the databases ebsco, pubmed and lilacs, on articles that address the topic of medical terms related to HAI using the starlite strategy (Table 1) [25]. 626 articles were obtained in the period between June 2014 and June 2017 articles of which, after applying the selection criteria explained in table 1, 116 were selected to be analyzed and it was found that there are common terms in the three databases, that is, they are frequent in more than 75% of the selected articles, such as: neonates, male sex, prematurity, low weight, icu, prolonged hospital stay, cyanotic heart disease, venous catheter, nasogastric tube, corticosteroids, cannula orotracheal, mechanical ventilation, parenteral nutrition, pleural tube, bladder catheter, toys, immunosuppression, surgery, enteral nutrition, neutropenia, neoplasia, gastrointestinal disease, respiratory disease, tracheostomy, hiv (Table 2).Second phaseSubsequently, in order to identify the terms used by health personnel (paediatricians, neonatologists, general practitioners, residents, nurses) within the clinical histories during the phase of suspicion or diagnosis of a patient with HAI, they were designed four clinical cases, one contained signs and symptoms suggestive of the start of an infection, another contained paraclinicos confirmatory of infection, another was an HAI and a last was the negative control which did not suggest infection (see supplementary material 1). The clinical cases were included in a questionnaire that requested to write to the health professional an evolution of the clinical case. The questionnaire was applied in three health institutions of the city of bogotá and additionally, it inquired about the health area in which the professional practiced, the time of experience and the place where he worked. The data were analyzed with the atlas ti program, .8.1 taking into account that they were qualitative data (Table 3 & 4).CJNC: Clínica Juan N. CorpasCase 1: signs and symptoms suggestive of the onset of an infection, Case 2: negative control, Case 3: Confirmatory paraclinics of infection, Case 4: HAI confirmed.Third phase: once the terms used in the scientific literature and in the clinical cases analyzed by health professionals in contact with the pediatric population were identified, the records of patients diagnosed with HAI in a third-level clinic during the study period were reviewed. Time between august 2014 and august 2016, the records were obtained through two sources, the first was the database obtained from the department of epidemiology of the institution and the second, from the search for cie diagnoses 10 related to HAI in the general database of the institution, the two databases were compared and a total of 96 cases of HAI were obtained, of which 12 corresponded to pediatric patients; 6 neonates and six older than 30 days of age; we found an average age of 12.3 days in neonates and 12 years in the other patients, an incidence of 75 infections per 1000 days of hospital stay was calculated. Of the total number of patients, 75% were male, all lived in urban areas; 91.6% of the population belonged to a middle stratum, however all were of the subsidized health regime. Regarding the family environment, we found that 83% of patients were cared for by their mothers who had an average age of 37 years, in terms of the academic training of caregivers 83% were high school graduates and 17% had technical studies.In the evaluation of clinical variables of the patients, it was identified that the most frequent type of feeding during the days of hospital stay was enteral, followed by breastfeeding; the most frequent HAI was the bloodstream infection associated with the use of catheter, the most used diagnostic method was the culture of catheter tip followed by physical examination, the most frequently isolated microorganism was staphylococcus epidermidis as a producer of HAI, half of the cases of HAI was presented in the nicu and the remaining half in other hospitalization services; the most used medical devices were the venoclysis equipment that was used in all patients, followed by the central catheter in four patients, and nasal cannulas in 33.3% of the population studied; 75% of the cases had some type of isolation, with contact being the most frequent (Table 5). Finally, based on the information found in the three sources: scientific literature, surveys of health professionals and review of medical records, a triangulation of the information was carried out and, in addition to identifying the most frequently used terms, it proposes a list of terms and characteristics that could alert the triggering or the presence of an HAI in real time which includes characteristics of the patient such as male sex or age less than 30 days of life; clinical characteristics such as the use of any invasive medical device, especially the use of venous catheter, surgical intervention, hospitalization in the icu, enteral nutrition and prolonged hospital stay, that is, more than 7 days in any hospitalization service (Table 6).OSI: Operative Site Infection, NICU: Neonatal Intensive Care Unit.
Discussion
This investigation allowed to identify the characteristics and terms related to HAI, aspects that could be considered as warning signs during the first approach in pediatric patient care; determined the HAI events in pediatrics in a third level clinic and identified the social, demographic and clinical characteristics of the population studied. The innovative aspect of this study is that it provides information from three sources of data: the scientific literature, the clinical practice of health professionals and the records in medical records; in which the terms used were found to coincide; the foregoing assumes that the theory is not far from the practice and that the identified terms can be considered to make an early and accurate diagnosis of an HAI or to alert about the probability of suffering it during medical attention [24, 26-31, 67- 89]. It has been described that the first to identify this type of infection are the nurses or the epidemiological surveillance departments of the health entities, but with the terms found in this research, this role of early identification of HAI can be attributed to any professional of the health in contact with the patient [12,23- 24].The place of selection of participants, allowed to identify individuals of different socioeconomic level, the majority belonging to medium and low stratum, aspect that has evidenced relation with the presentation of HAI in other studies carried out [24]. Contrary to some studies that identify the rural area as a risk factor for contracting an infection, in this study none of the cases lived in a non-urban area [142-143]. It was found that the majority of patients who acquired an hai were male, a finding consistent with multiple studies, which estimated that for every two male patients, one was female [144-148]. As well as studies conducted in north america and europe, the most frequent HAI was related to bloodstream infection associated with catheter use, and the most isolated microorganism was the staphylococcus epidermis present in the catheter tip culture; this finding is consistent with what was found in this research [149-153]. The literature describes multiple risk factors for contracting an HAI and some authors indicate that the combination of several of these factors may increase the risk of acquiring an HAI; it is also known that hais prolong the hospital stay of hospitalized pediatric patients, increase their morbidity and mortality and cause greater economic and human expenses that affect the health system [154-160]. The authors considered as a limitation the low number of cases found during the study period.Finally, based on the results obtained, a list of characteristics that can alert the health professional about the presence of an HAI in the first contact with the patient is proposed, for this purpose, in a future investigation it is intended to generate a probability score of risk that will allow classifying patients in those with low, medium and high risk of HAI, at different times of hospitalization, including: admission, 24-48 hours, 49-72 hours and 73-96 hours. It would be of great value, due to the importance of reducing the HAI in the institutions, giving greater weight to the prevention of them with this information.
Conclusion
Most of the patients are male, they are cared for by one of the parents only, they belong to the middle stratum and they are subsidized. The most frequent HAI was the infection associated with the use of venous catheter. There are common characteristics and terms related to HAI that can alert on the appearance or course of an infection of this type. It is important to focus on the prevention of hais from the first contact with the patient through the use of basic tools such as epidemiological characteristics and clinical history.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/journals.php
For more articles in Open Access Journal of Pediatrics & Neonatology please click on: https://juniperpublishers.com/ajpn/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/ajpn/AJPN.MS.ID.555766.php
18 notes
·
View notes
Text
Juniper Publishers Address

Juniper Publishers Address
427 W Duarte Rd, Suite E, Arcadia,
California, CA 91007United States
https://juniperpublishers.com/contact-us.php
0 notes
Text
Juniper Publishers Contact Info
Juniper Publishers Contact InfoPhone: +1-805-200-4030Fax: 1-855-420-6872Email: [email protected]
Web : www.juniperpublishers.com
0 notes
Text
Juniper Publishers Contact Number
Juniper Publishers Contact NumberPhone: +1-805-200-4030
https://g.page/Juniper_Publishers?share
0 notes