
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by lillianeshaw and here's what we found interesting.
Average Info
Notes Per Post
0
Likes Per Post
0
Reblog Per Post
0
Reply Per Post
0
Time Between Posts
12 seconds
Number of Posts By Type
Text
17
Last Seen Tumblr Blogs





Fun Fact
Total funding amounts to $125.3M.

Text
Overview
Worldwide, women are suffering from reproductive health inequities which have persisted for decades. In an over medicalized system dominated by physicians, birthing women are frequently exposed to many non-consensual and unnecessary procedures which have no scientific backing. Despite being recognized by the World Health Organization and other institutions, women continue to be excluded from participating in the birthing process and are subjected to coercive and abusive practices throughout their labor. Obstetric violence has become an invisible and naturalized form of violence, and poses a serious violation of human rights. It is necessary to acknowledge the flaws which plague maternity care and to emphasize the lack of autonomy of laboring women.
In recent years, growing trends in the excessive use of medical interventions during childbirth, along with an unsettling presence of abusive and disrespectful practices towards pregnant and birthing individuals, have drawn attention to a global issue concerning human rights and childbirth. Though not yet fully recognized, the term “obstetric violence” describes the systematic problem of institutionalized, gender-based violence that many women are subjected to throughout the processes of gestation, delivery, puerperium, and the reproductive cycle. Due to the high number of cesarean sections performed and an increase in complications from pregnancy or childbirth, women in the United states have one of the highest rates of maternal mortality. This mistreatment of women and birthing people in the childbirth setting has become normalized as routine care, disproportionately impacting women of color, indigenous women, members of the LGBTQ+ community, and other marginalized communities around the world.
My interest in pregnancy and female reproductive care is what drew me to research the issue of obstetric violence. For many years, I had considered pursuing a career in obstetrics and gynecology, and have recently shifted my focus to midwifery. My intention with this career path is to provide comfort, security, and empowerment to women in an area where they are often perceived and treated as inferior. In the future, it is believed that adopting human rights-based constitutions and bodies of law that address obstetric violence would aid in solving the issue. The frequent occurrence of negative obstetric experiences indicates a need to transform perinatal care provision which requires a collective effort from all those involved.
0 notes
Text
Glossary
Obstetric Violence: an infringement of women’s human rights to non-discrimination, liberty and security of the person, reproductive health and autonomy, and freedom from cruel, inhuman, and degrading treatment; cruel, dishonorable, inhuman, humiliating, threatening treatment by health professionals, causing physical, psychological and emotional harm to assisted women
Cesarean Section: a surgical operation for delivering a child by cutting through the wall of the mother's abdomen
Comprehensive Care: care that is aligned with the patient’s expressed goals of care and healthcare needs; considers the impact of the patient’s health issues on their life and wellbeing, and is clinically appropriate
Epidural: an epidural anesthetic, used especially in childbirth to produce loss of sensation below the waist.
Episiotomy: a surgical cut that is made at the opening of the vagina during childbirth, thought to aid a difficult delivery and prevent the rupture of tissues
Gender: the characteristics of women, men, girls and boys that are socially constructed
Kristeller Maneuver/Fundal Pressure: an aggressive and painful procedure in which a woman’s body is heavily pushed upon to move the baby
Postpartum Post-Traumatic Stress Disorder: usually associated with a traumatic birthing experience but may also link to having a previous diagnosis of PTSD, experiencing infertility, or giving birth to a baby with health complications; a condition of persistent mental and emotional stress occurring as a result of injury or severe psychological shock, typically involving disturbance of sleep and constant vivid recall of the experience, with dulled responses to others and to the outside world
Puerperal: during or relating to the six-week period following childbirth
Rape Culture: the normalization and tolerance of sexual violence against women. In maternity care, rape culture is where the appropriation and control of the pregnant body is ubiquitous
0 notes

Text
Invisible wounds: obstetric violence in the United States
Diaz-Tello, Farah J. D. 2016. “Invisible wounds: obstetric violence in the United States.” Reproductive Health Matters 24(47).
"1. We will contact the Department of Children and Family Services about your refusal to undergo a Cesarean section and other care and treatment recommended by your physicians and the high risks your refusals have on your life and health, as well as the life and health of your unborn child.
2. We will begin a process for an Expedited Judicial Intervention Concerning Medical Treatment Procedures. This is a proceeding for expedited judicial intervention concerning medical treatment procedures relating to the delivery of your child.
3. If you present to our hospital in labor, and your physician deems it clinically necessary, a Cesarean section will be performed with or without your consent."
Though forced cesarean sections are violent and illegal, instances are seldom redressed by courts. The performance of forced surgeries indicates a larger, underlying pattern of disrespect and abuse toward pregnant and birthing women by healthcare providers and medical institutions.
Unnecessary surgeries are emotionally difficult and physically harmful for mothers and can lead to greater health and fertility risks. Many women who have undergone cesarean surgery are wrongfully made to believe they will be unable to achieve VBAC (vaginal birth after cesarean).
In the hospital setting, women hold less power than their physicians and experience significant pressure and loss of autonomy in maternity care. Women’s capacity for pregnancy has been used historically to sanction their exclusion, demonstrating that obstetric violence is more than a simple battery.
Women who attempt to refuse cesarean surgery frequently receive threats of child apprehension, even after signing acknowledgement forms that they are acting against medical advice and waiving liability. The women are often exposed to insistent shouting and swearing before they eventually undergo the surgery against their will.
Victims of obstetric violence leave the experience of birth feeling betrayed and frightened in addition to the physical challenge of giving birth (vaginally or surgically). Some women experienced trauma that required therapy or changed the course of their reproductive lives. Their birth was described as “an excruciating and terrifying experience”.
The monetary value ascribed to harm to women during birth is low, almost non-existent, and the perception of liability risk to the fetus is significantly overestimated. This encourages physicians to pressure and coerce women out of fear of malpractice and provides little incentive for attorneys to take on cases on a contingent fee basis. And, for women who do manage to find an attorney, they may discover their case is time barred or subject to unpredictable statutes of limitations.
The World Health Organization (WHO) issued a statement on the prevention and elimination of disrespect and abuse during facility-based childbirth. The organization declared obstetric violence as an “important public health and human rights issue” and urged governments to research, recognize, and redress disrespectful and abusive maternity care.
Latin America was the first to legally address the issue of obstetric violence, recognizing it as a part of the Organic Law on the Right of Women to a Life Free of Violence.
The issue of obstetric violence requires provider education and greater connection between health infrastructure and civil society advocacy to address harmful gender norms.

0 notes
Text
“The World Health Organization (WHO) confirms that caesarean section rates higher than 10% are not associated with lower maternal and newborn mortality on a population level.” (Sadler et al. 2016:49)
0 notes
Text
Several Obstetric Violence Observatories have been founded, which, in 2016, released a common statement declaring obstetric violence as one of the “most invisible and naturalized forms of violence against women, constituting a serious violation of human rights.” (Sadler et al. 2016:50)
0 notes
Text
0 notes
Text
Obstetric violence in the daily routine of care and its characteristics
Jardim, Danúbia M. B. and Celina M. Modena. 2018. “Obstetric violence in the daily routine of care and its characteristics.” Revista Latino-Americana de Enfermagem 26.
“Obstetric violence portrays a violation of human rights and a serious public health problem and is revealed in the form of negligent, reckless, omissive, discriminatory and disrespectful acts practiced by health professionals and legitimized by the symbolic relations of power that naturalize and trivialize their occurrence.”
Gestation (pregnancy) is no longer understood as a physiological event of life, but one that requires excessive control. In the birthing scenario, women are controlled by their environment and surrounded by institutional rules and protocols. These controls make them discredit their capacity to give birth.
Data from the World Health Organization (WHO) reveals obstetric violence is a global issue; women are being assisted in a violent manner everywhere in the world. They experience situations of mistreatment, disrespect, abuse, negligence, violation of human rights by health professionals, especially during delivery and birth.
Half-naked women are left in the presence of strangers or alone in unfriendly settings, in positions of total submission with open and raised legs in stirrups, and their genital organs exposed. Many women are frequently denied the presence of a companion of their choice, receive little to no information about various procedures performed during their care, are subjected to routine and repetitive painful vaginal examinations without justification, are deprived of their right to food or walking, must undergo frequent use oxytocin to accelerate labor, and suffer unconsented procedures such as cesarean surgeries, episiotomies, artificial rupture of membranes, prophylactic intravenous medications, and fundal pressure.
Though experienced by all groups, women of low socioeconomic and educational status, ethnic minorities, adolescents, substance users, homeless women, and women without prenatal care experience significantly more adverse health outcomes and mistreatment during pregnancy and childbirth.
Following the stereotype that women’s knowledge, and that of birthing women in particular, is inferior and unreliable due to their more emotional and irrational nature, technology and medical staff become the most reliable sources of knowledge in the labor room.
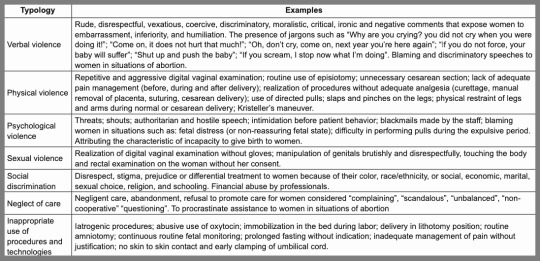
The WHO has typified forms of obstetric violence into five categories: 1) routine and unnecessary interventions and medicalization; 2) verbal abuse, humiliation, or physical aggression; 3) lack of resources and inadequate facilities; 4) practices performed by residents and professionals without the woman’s permission after providing her comprehensive, truthful, and sufficient information; 5) discrimination on cultural, economic, religious, and ethnic grounds
Obstetric violence is a feminist issue. Patriarchal oppression has led to the under-evaluation, oppression and objectification of the female body, limiting the power and way of expression of women. Labeled as reproductive bodies, women’s subjectivity is annulled and they are deprived of any right of choice.
Professionals attempt to justify acts of obstetric violence through explanations of work overload, scarce of human resources, physical and mental exhaustion, and lack of adequate infrastructure in institutions. These excuses demonstrate a lack of commitment of health professionals and allow for ethical relationships between patients and providers to become inhuman, highly technological, and invasive.
Women are suffering in silence without knowing they were violated. Women are lacking in knowledge of their sexual and reproductive rights, making them unable to recognize whether or not they suffered violent acts because they blindly trust their caregivers.
It is fundamental to give visibility to the problem with the creation of channels for denunciation and accountability of the different actors involved which have contributed to the issue of obstetric violence. The creation of laws, ordinances, and public policies to protect women against obstetric violence, and acknowledgement of their right to care free of violence and autonomy over their bodies must be pursued.
0 notes
Text

Though commonly used in delivery rooms, there is no reliable evidence to suggest fundal pressure is effective in progressing labor. In certain situations, fundal pressure can contribute to complications and injury to the baby.
0 notes
Text
Birthing women as a group are systematically disbelieved as a result of the implicit bias that women are less rational than men and lack certain epistemic capacities, which are historically grounded ideas about the uterus and the female reproductive system. (Cohen Shabot 2021:642)
0 notes
Text
“The female body and its natural processes were - and continue to be - portrayed as abnormalities, disease, or deviances. Professionals lay discourses referring to the diagnosis of pregnancy, to pregnancy symptoms, and to the pregnant woman's return to the normal state after birth are some of several discrete markers of the male normalization.” (Sadler et al. 2016:51)
0 notes
Text
Birthing women are mistakenly considered “riskily vulnerable, out of control, and incapable of accountability or good decision-making, to an even greater degree than the ill.” (Cohen Shabot 2021:637)
0 notes
Text
Coercion and non‐consent during birth and newborn care in the United States
Logan, Rachel G., Monica R. McLemore, Zoe Julian, Kathrin Stoll, Nisha Malhotra, and Saraswathi Vedam. 2022. “Coercion and non‐consent during birth and newborn care in the United States.” Birth (Berkeley, Calif.) 49(4).
In the United States, Black, Indigenous, and People of Color (BIPOC) experience more adverse health outcomes and report mistreatment during pregnancy and birth care. Black and Indigenous women are two to three times more likely to die from childbirth than white women.
In the United States, 98% of women give birth in facilities (ie, hospitals), which for women with uncomplicated pregnancies, is associated with higher rates of interventions and adverse outcomes for both mothers and newborns relative to care in birth centers and planned births in homes
People who had a planned hospital birth were four times as likely to report pressure than those who had a planned community birth. People identifying as Black were significantly more likely to report non-consented procedures than participants identifying as white. Continued, those who did not have the same practitioner throughout prenatal care and those who had a physician or nurse rather than a midwife during labor and birth also reported non-consented procedures more. People who had a cesarean or instrumental vaginal birth were 30 times more likely to report pressure to have a cesarean than those who had a spontaneous vaginal birth.
“Respectful maternity care (RMC) is an approach to care that emphasizes the fundamental human rights of childbearing people, newborns, and families to autonomy, dignity, privacy, access to services, informed choice, emotional support and companionship, and freedom from mistreatment, discrimination, coercion, and abuse.” The implementation of midwives and doulas under the RMC model into prenatal care has been proven to demonstrate equitable, evidence-based care, while recognizing the individualized needs of both parents and newborns.
New care paradigms are needed to transform care experiences and to ensure that health equity and human rights are at the center of care provision. Adopting a human-rights based framework such as reproductive justice is suggested to be incorporated into health professionals curriculum to ensure care is equity-oriented and anti-racist.
Practitioners’ failure to meet professional standards threatens service users’ reproductive autonomy and may contribute to ongoing inequities. Reducing mistreatment in perinatal care, such as coercion to accept services and non-consented procedures, can help mitigate ongoing inequities.

0 notes
Text
Some healthcare providers simply do not realize their insensitivity and loss of compassion: “We are trained not only in how to do such things but in how to do them almost without noticing, almost without caring, at least in the ways we might care in different circumstances or settings.” (Lokugamage and Pathberiya 2017:3-4)
0 notes
Text

Epidurals can require laboring women to remain still for 10-15 minutes, even during contractions. Some anesthesiologists use fear of paralyzation to coerce women to comply with their demands.
0 notes
Text
Conclusion
The recognition of the concept of obstetric violence as a form of violence against women is important to the movement towards respectful, women-centered maternity care. The extensive use of medical intervention, physician bias, insufficient education, poor communication, and legal inadequacies greatly contribute to the ongoing inequities in perinatal care in hospital settings. Under the Respectful Maternity Care model, women may become supported in giving birth in a way that fulfills their choices and expectations. Despite growing awareness of the issue of obstetric violence, little is being done to progress. The frequent occurrence of negative obstetric experiences indicates a need to transform perinatal care provision which requires a collective effort from all those involved.
With the intention of pursuing a career in midwifery, I hope to make positive impacts on the lives of expectant mothers. For years I have been fascinated by the processes and experiences of pregnancy, labor, and postnatal care. I have a great interest in women’s rights and feel extremely passionately about providing women with the reproductive knowledge they need and are entitled to as they prepare for the birth of a child. From the sociological education I have received, I have become aware of the injustices within the healthcare system. Since first learning about the concept of obstetric violence, I knew I wanted to understand its existence and prevalence.
This research has contributed significantly to my understanding of obstetric violence and its implications. It was particularly interesting to read about existing case studies and understanding how the current legal system contributes to the maintenance of this issue. In the future, I would love the opportunity to conduct in-depth interviews with new mothers to understand their birthing experiences. I intend to use the knowledge gathered from this research and future research to spread awareness and further the movement towards maternal equity.
0 notes