
lupine-publishers-gjapm
Journal of Anesthesia and pain Medicine
The journal scope encompasses the knowledge in medical research of the topics related to anesthesia practice, airway management, anesthetic administration, preoperative and postoperative considerations, pain management, inhalational anaesthetics
120 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs

murrzula
Murr's Monsters

clovw
Clow

fallasleepinthemeadow
Lost In The Dreamland

coffeetimeblr-blog
Coffee Time!

ishyg786
Untitled
Text
Happy Thanksgiving 2022!!

Thanksgiving is a joyous invitation to shower the world with love and gratitude. Forever on Thanksgiving the heart will find the pathway home. The more you practice the art of thankfulness.
Wish you a very happy and blessed Thanksgiving!
0 notes
Text
Wishing you a Magical and Blissful Holiday!
Have a Merry Christmas and a Happy New year!
I hope Santa is good to you this year because you only deserve the best.
Merry Christmas from our family to yours. Take nothing for granted and be thankful that you have such great family and friends to spend this joyous season with.

Wishing you a delightful Christmas and a very Happy New year in Advance.
0 notes
Text
Lupine Publishers | The Importance of Pragmatic over Explanatory Randomised Controlled Trial in Musculoskeletal Physiotherapy Practice

Lupine Publishers | Orthopedics and Sports Medicine
Abstract
Depending on the choice of research methodology, there are several research designs such as a single observational case study, a cohort or case-controlled design, nonrandomised and randomised controlled trials (RCTs). While RCTs are widely considered as the gold standard for assessing the effectiveness of different physiotherapy interventions, there are two types of RCT mainly explanatory and pragmatic RCT. It is the opinion of the author a pragmatic RCT approach that not only have realistic treatment sessions but also involve less costs and personnel are best suited for musculoskeletal studies undertaken in a normal clinical environment to enhance their generalisation.
Introduction
Research evidence suggests the number of physiotherapy treatment sessions varies over treatment episodes [1], however, according to the Chartered Society of Physiotherapy [2] (CSP, 2011) the average physiotherapy (face-to-face) treatment sessions per episode of care for a patient was on average four-with a first to follow-up ratio of 1:3.4. The minimum number of physiotherapy treatments per episode was one with maximum of six treatment sessions. These figures were from the research findings of a large comprehensive review of physiotherapy outpatient services across the United Kingdom by JJ Consulting on behalf of the [2] CSP (2011). These figures are important benchmarks for Physiotherapy managers and physiotherapy service providers to them guide on staffing levels and management of caseloads to support a range of areas such as business planning, capacity and demand management, and service re-design. Thus, it is important for researchers and those funding physiotherapy researches to take into consideration the average number of treatment sessions that occurs in normal clinical practice when developing research designs that investigates the effectiveness of treatment interventions in musculoskeletal practice. This is so that the findings of such research could easily be transferable to real physiotherapy clinical situations. Pragmatic randomized controlled trials (RCTs) are designed and conducted to establish the clinical effectiveness of interventions i.e. does this intervention work under usual clinical conditions? (Tunis et al 2003 and Tunis 2005). According to [3] for a trial to fulfil the requirements of the design and conduct of a pragmatic RCT, it should have the nine dimensions for assessing the level of pragmatism in a trial. These include eligibility, recruitment, setting, and organisation, flexibility in delivery, flexibility in adherence, follow-up, primary outcome and primary analysis. Although most pragmatic RCTs follow this protocol in their design and conduct, some of them that have investigated the clinical effectiveness of interventions in musculoskeletal conditions such as low back pain (LBP) but have done so with follow-up contact of the study participants in excess of the usual practice (Table 1). Follow-up visits (timing and frequency) are pre-specified in the protocol of RCTs. However, “follow-up visits are more frequent than typically would occur outside the trial (i.e., under usual care)” [3] Loudon et al (2015) (Table 1).
Table 1: A PRECIS follow-up assessment of some trials.
Table 1 shows that in some randomised controlled trials (RCTs) on musculoskeletal physiotherapy interventions that there are difficulties with transferring the results of those trials into daily clinical practice due to their unrealistic treatment occasions. For example, an RCT [4] that was conducted to evaluate the relative efficacy of strengthening exercises versus spinal manipulation on low back pain (LBP) patients were provided a one-hour session twice per week for 6 weeks – bringing the total treatment episodes to 12 one-hour treatment sessions. Similarly, [5] Alp et al, (2014) in a RCT of management low back pain that investigated selfmanagement (unsupervised exercise) versus group biomechanical exercise used 45-60 minute, 3 times per week for 6 weeks as their treatment regime. The findings of these trials are in sharp contrast to the [2] CSP (2011) findings on the maximum number of treatments per episode care, which was six. Furthermore, anecdotal evidence suggests that initial musculoskeletal physiotherapy treatment is maximum of one hour and follow-up treatment ranges from 20- 45 minutes. The implications of the treatment regimens of both RCTs [4,5] suggests that they have unrealistic treatment occasions which cannot be transferred to practice. It is therefore imperative for clinical trials investigating the effects of physiotherapy interventions to take into consideration that study designs should mirror what occur in normal clinical practice. There are many different research designs ranging from a single observational case study, a cohort or case-controlled design, to experimental studies such as nonrandomised and randomised controlled trials (RCTs). Each design has its own strengths and weaknesses. The choice of methodology may be influenced by factors such as the research question, ethical issues, sample size and funding [6]. Although case studies are likely to demonstrate clinically significant improvement in outcomes of pain and function, it must not be forgotten that they cannot rule out the effects of natural resolution, bias and other confounders such as the real cause of the improvement (Ainsworth & Lewis 2007). However, single case studies should provide some motivation for conducting the appropriate and necessary trials such as nonRCTs and RCTs [7]. NonRCTs can detect associations between an intervention and an outcome, however they cannot rule out the possibility that the association was caused by a third factor linked to both intervention and outcome [8]. RCTs are widely considered as the gold standard for assessing the effectiveness of different interventions such as shoulder injections, because they allow us to be confident that a difference in outcome can be directly attributed to a difference in the treatments, rather than some other confounding variables (age and gender) [9,10]. However, other factors, such as patient’s clinical experience of the intervention, as well as the quality and quantity of treatment received been suggested to play a role in determining treatment outcomes [11]. Therefore, an RCT that combines these aspects by investigating the effectiveness of the interventions in real life clinical situation is important. To achieve this, RCTs investigating the effectiveness of two interventions (usual or routine versus intervention) to treatment should as part of their research methodology take into consideration the practicality of number treatment sessions, follow-up regimes and outcomes that are comparable to those observed in every day clinical practice – both in community and acute settings. This so that any treatment effect from those studies can be easily transferable to normal clinical practice situations. RCTs help to reduce the risks of bias (threats to interval validity), mostly selection bias, and are thus best suited for research designs about the effectiveness of different interventions [12]. However, it is the opinion of Cochrane, that randomisation does not, of itself, enhance the applicability of the results of a trial (external validity) to situations other than the exact one in which it was conducted [13]. It is possible for a trial to be free of bias but lacking in its application beyond the immediate clinical environment in which it was conducted [12]. This view was strongly re-echoed by [14] which it stated: “Lack of consideration of external validity is the most frequent criticism by clinicians of RCTs, systematic reviews, and clinical guidelines” [14]. To resolve this problem [12] has suggested the use of well-designed trials that adopt a pragmatic approach. Therefore, it is my opinion that for a pragmatic RCT approach to be adopted as a research design, it should have realistic treatment occasions and transferable to normal clinical environment where most people with musculoskeletal conditions are easily, are diagnosed and treated [15] to enhance its generalisation.
Pragmatic Versus Explanatory Randomised Controlled Trial
[16] describe two different types of RCT, explanatory and pragmatic. They proposed a distinction between explanatory and pragmatic trials. It is their view that many trials (such as explanatory trials) were limited in their applicability beyond the artificial, laboratory environment. Explanatory trials are aimed at validating a physiological hypothesis by specifically proving a causal relationship between administration of a treatment (a drug) and a physiological outcome (such as inflammation) [16]. Although pragmatic trials do not necessarily decrease occasions of service or necessarily curtail follow-up, they provide an explanation between interventions and treatment outcomes, and they are intended to inform healthcare decision-making. This decision involves the choice between two or more treatments occurring in real life clinical environment. On the other hand, explanatory trials provide knowledge about the effects of precisely defined interventions applied to selected groups under highly controlled conditions; however, they are not applicable in normal physiotherapy practice that lack such highly controlled environments. Pragmatic trials have been offered as a solution in that they retain the rigour of randomisation but are still applicable to normal clinical practice [17] (Relton et al 2010). It is for these reasons that musculoskeletal studies should adopt a pragmatic approach which takes into account realistic treatment occasions which occurs in a normal clinical so that findings from such trials can be easily transferable to practice. For example [18], in a pragmatic RCT that investigated exercise versus group biomechanical exercise in chronic low back patients using a one-hour session per week, which what obtains in every day, practice. The implication of this study findings is that it has realistic treatment occasion that is easily transferable to practice. The differences between the two approaches are also highlighted in the use of efficacy and effectiveness [19]. Explanatory trials deal with efficacy as these studies assess differences in effect between two or more conditions under ideal, highly controlled conditions. Although the tight controls of explanatory trials result in maximal internal validity, external validity could be lost (Alford 2007) because replicating them under normal clinical practice is difficult. Explanatory trials are thought to be well suited to medical drug trials, which are usually double or triple blinded, and involve the use of a placebo control group (Alford 2007). Pragmatic RCTs utilise effectiveness, which assesses differences in effect between two or more conditions in normal clinical circumstances, thus retaining internal validity and enhancing external validity (Alford 2007). It is the opinion of Alford (2007) that pragmatic RCTs are generally more suited to assessing musculoskeletal interventions such as exercise prescription for managing low back or shoulder pain. Explanatory trials are usually more expensive, take more time and involve more personnel, unlike pragmatic trials. These difficulties are the reasons why a pragmatic approach is best suited for musculoskeletal research within the community. The benefits are that less extra costs or personnel would involve in such studies because they are more likely to take place within normal clinical hours with the usual staff involved.
Pragmatic Randomised Controlled Trial-Why it is Important
In a normal community practice where most people with musculoskeletal pain are diagnosed and managed [15], a pragmatic RCT design is important if they have realistic treatment, occasions, which can be transferred to practice. A pragmatic RCT is aimed at determining the effectiveness of two or more interventions under the usual conditions or real-life settings in which they are applied [20]. Pragmatic trials including RCT are aimed at ensuring that the care delivered in the setting in which trials are conducted matches the care delivered in the setting to which its results are applied [3]. Pragmatic RCTs are generally linked with clinical practice and they incorporate clinical outcomes that are relevant to inform decision makers such as patients, clinicians, health commissioners and policy makers about interventions that are applicable to a wide range of clinical settings [20]. These trials adopt minimal exclusion criteria in order for the patients to reflect those receiving care within the normal population [20]. This is so that treatment interventions and decision making by both the patients and healthcare providers regarding the management of musculoskeletal conditions could be enhanced. Musculoskeletal studies should include participants drawn from a population of patients attending a community (MSK) service as they would representative of the general population. The benefits of pragmatic trials less costs and personnel because they are more likely to take place within normal clinical hours with the usual staff involved. The nine dimensions for assessing the level of pragmatism in a trial (Figure 1), as proposed in the pragmaticexplanatory continuum indicator summary 2 (PRECIS-2) tool should be adoped by musculoskeletal studies so that they can be easily transferred to practice [3]. With the current economic climate and given the pressure to improve healthcare delivery within the community, pragmatic RCTs have received widespread support and acceptance from clinicians, researchers and policy makers [21]. Healthcare commissioners and policy makers are very interested in pragmatic trials because they are designed to answer important and relevant questions, which are centred on comparative effectiveness of interventions in the normal clinical practice [22]. However, those trails should not only have realistic treatment sessions but also involve less costs and personnel. Since the local Clinical Commissioning who commissions musculoskeletal practice are interested in knowing the clinical outcomes, involving them and GPs during the planning stages of musculoskeletal research is very important. This is consistent with the suggestion by [22] that decision makers such healthcare providers and policy makers should be included in the design of pragmatic trials.
Conclusion
While RCTs are widely considered as the gold standard for assessing the effectiveness of different interventions such as shoulder injections, there are basically two types of RCT mainly explanatory and pragmatic RCT. Although each design has its own strengths and weaknesses, the choice of methodology may be influenced by factors such as the research question, ethical issues and clinical practice environment [6-31]. It is the opinion of the author a pragmatic RCT approach that not only have realistic treatment sessions but also involve less costs and personnel are best suited for musculoskeletal studies undertaken in a normal clinical environment to enhance their generalisation.
For more Orthopedics and Sports Medicine Open Access Journal (OSMOAJ)
Please Click Here: https://lupinepublishers.com/orthopedics-sportsmedicine-journal/index.php
10 notes
·
View notes
Text
Lupine Publishers | Laparoscopic Right Hemicolectomy and Primary Anastomosis for Tubulovillous Polyp with Preoperative Endoscopic Tattooing as A Preventive Treatment in High Risk Colorectal Cancer Patient Case Report and Review
Lupine Publishers | Open Access Journal of Oncology and Medicine (OAJOM)
Abstract
Background
VA/TVAs are thought to be the advanced precursors in the “adenoma-carcinoma” pathway. Right-sided colon cancer accounts for approximately 30% of bowel cancer in women and 22% in men, Curative treatment for right-sided colonic cancer includes right hemicolectomy with or without adjuvant chemotherapy. We present a 43-year-old female, with history of a father who died from colon cancer, she has a history of high blood pressure, obesity, and epilepsy, presenting hematochezia. A colonoscopy was performed with evidence of a granular scattered lateral growth lesion in the ascending colon, which cannot be resected by mucosectomy, which is why an endoscopic biopsy and tattoo was performed. The result of histopathology with tubulovillous polyp without evidence of dysplasia.
Keywords: Tubulovillous Polyp; Colorectal Cancer; Endoscopic Tattooing; Hemicolectomy; Laparoscopic Surgery; Preventive Treatment
Abbreviations: CRC: Colorectal Cancer; VA/TVA: Tubular Adenomas and Villous/Tubulovillous Adenomas; SSA: Sessile Serrated Adenomas: TSA: Traditional Serrated Adenomas; HP: Hyperplastic Polyps
Introduction
It is well established that colorectal cancer (CRC) develops from a series of precursor epithelial polyps [1], which include conventional adenomas, incorporating tubular adenomas and villous/tubulovillous adenomas (VA/TVA) and serrated polyps, incorporating hyperplastic polyps (HP), sessile serrated adenomas (SSA) and traditional serrated adenomas (TSA). VA/TVAs are thought to be the advanced precursors in the “adenoma-carcinoma” pathway [2]. Risk factors include advancing age, male gender, highfat, low-fiber diet, tobacco use, and excess alcohol intake (more than eight drinks a week). Individuals with a family history of polyps, colorectal cancer, and intestinal polyposis carry a higher risk of developing colon polyps [3]. Right-sided colon cancer accounts for approximately 30% of bowel cancer in women and 22% in men [4] Curative treatment for right-sided colonic cancer includes right hemicolectomy with or without adjuvant chemotherapy [5]. Depending on the pattern of growth, these tumors can be villous, tubular, or tubulovillous. A polyp with more than 75% villous features, i.e., long finger-like or leaf-like projections on the surface, is called a villous adenoma, while tubular adenomas are mainly comprised of tubular glands and have less than 25% villous features. A tubulovillous adenoma is referred to as an adenoma with both features. Tubular adenomas are the most common type of colonic adenomas, comprising a prevalence of more than 80% [6]. Although villous adenomas are more likely to become cancerous, this reflects the fact that they generally have the largest surface area due to their villous projections. If adjusted for surface area, all types of adenomas have the same potential to become cancerous [7]. The clinical significance of polyps arises from the fact that more than 95% of colon adenocarcinoma originate from polyps. Errors in localization account for a 6.3% rate of alteration in preoperatively colonic resection [8], endoscopic localization is highly inaccurate, with a 21% rate of error endoscopic tattooing is an alternative, although different techniques are used for tattooing, it is important to be consistent in the pattern of marking and to clearly document the method in the colonoscopy report. The authors recommend that tattoo be placed in 3 separate areas around the circumference of the lumen distal to the lesion [9]. Right colectomy is the procedure recommended for tumors proximal to the proximal transverse colon. Principles of right-sided resection include abdominal exploration for distant disease, mobilization and medialization of the right colon and hepatic flexure to allow for resection and anastomosis, and high ligation of the ileocolic pedicle and right branch of the middle colic artery [10] obtaining better post-surgical results with a minimally invasive and preventive approach.
Materials and Methods
We present a 43-year-old female, with history of a father who died from colon cancer, she has a history of high blood pressure, obesity, and epilepsy, presenting hematochezia. A colonoscopy was performed with evidence of a granular scattered lateral growth lesion in the ascending colon, which cannot be resected by mucosectomy, which is why an endoscopic biopsy and tattoo was performed (Figure 1). The result of histopathology with tubulovillous polyp without evidence of dysplasia. A preoperative protocol is started based on abdominal tomography and preoperative laboratories, with no evidence of alterations.
Results
Performing pneumoperitoneum at 15mmHg, a diagnostic laparoscopy is started, the ileocecal valve is identified , an opening of the meso in the terminal ileum is performed at 10 cm from the valve, sectioning with a 60 mm endoGIA stapler, opening the right TOLD fascia, and subsequent opening of the right mesocolon with a 5 mm ligasure, with adequate identification of the right colic artery, the hepatic angle of the colon is released until the endoscopic tattoo is identified and the transverse colon is sectioned using an endoGIA stapler 60 mm 7 cm distal to the tattoo. The serous plane of the terminal ileum and transverse colon is faced laterally with 2-0 silk, a 1 cm opening is made in the distal portion of the ileum and colon, through which a 60 mm endoGIA stapler is inserted and stapling is performed, to perform side-to-side anastomosis, closure of the anastomosis with 2-0 prolene with continuous surjete, surgical piece is extracted by port in the left hypochondrium, 2 drains are left and closed by planes (Figure 2). At 24 hours after surgery, the patient had no abdominal pain, no bloating, nausea, or vomiting. The drains with little serohaematic expenditure, the patient is left fasting for 4 days and on the 5th day an intestinal transit is carried out with a water-soluble medium without evidence of leaks (Image 4), starting a progressive liquid diet and discharging from the hospital on the 6th day without incidents or accidents (Figure 3).
Discussion & Conclusion
A standardized approach to endoscopic tattooing will avoid confusion for the surgeon at the time of laparoscopy. This is crucial to help provide the best oncologic resection for the patient. Endoscopic tattooing is a well-known technique and helps to obtain better pre and post-surgical results with minimal invasion, however it is important to know the guidelines for the correct performance of this technique as well as take it into account to offer to patients in whom injuries are identified risk as well as concomitant hereditary factors an alternative of minimally invasive resection adequately delimiting the margins of the lesion with a faster recovery while preserving the safety of the procedure as it was presented in the case of our patient. Considering these strategies and the individualization of each patient, potential risk factors as well as clinical presentation as a therapeutic and preventive opportunity for colorectal cancer.
For More Open Access Journal of Oncology and Medicine Articles Please Click Here: https://lupinepublishers.com/cancer-journal/index.php
14 notes
·
View notes
Text
The Optimal Pain Management Methods Post Thoracic Surgery: A Literature Review| Lupine Publishers
Journal of Surgery|Lupine Publishers
Abstract
Post-operative pain control is one of the key factors that can aid in fast and safe recovery after any surgical interventions. Thoracic surgery can cause significant postoperative pain which can lead to delayed recovery, delayed hospital discharge and possibly increased risk of chest complications in the form of atelectasis and even lower respiratory infections. Therefore, appropriate pain management following thoracic surgery is mandatory to prevent development of such morbidities including chronic pain.
Keywords:
Thoracic Surgery, Analgesia, VATS, Robotics, Thoracotomy
Introduction
Thoracic surgical procedures can result in severe pain which can present as a challenge to be appropriately managed postoperatively. In particular, thoracotomies are well known for their severity of pain due to the incision, manipulation of muscles and ligaments, retraction of the ribs with compression, stretching of the intercostal nerves, possible rib fractures, pleural irritation, and postoperative tube thoracotomy [1]. Recognition of this has contributed to the development of minimally invasive techniques such as video assisted thoracoscopic surgeries (VATS) and lately robotic surgery [1]. These techniques not only aim to produce better aesthetic results, but also reduce post-operative pain and enhance recovery without compromising the quality of treatment offered. Poor pain management can lead to several and serious complications such as lung atelectasis, hypostatic pneumonia due to avoidance of deep breathing in these patients as a result of pain and superimposed infection [1]. Pain management as a result, does not only lead to greater patient satisfaction, but it also reduces morbidity and mortality in patients undergoing thoracic surgery [2]. Historically, post-operative pain management for thoracic surgery involved the use of narcotics alongside parenteral or oral anti-inflammatory agents [2]. Post chest tube removal patients typically are transitioned to oral analgesia. Multiple additional pain control adjuncts were also implemented with differing levels of success [1]. Over time, intra-operative techniques have been developed which aims to target pain reduction postoperatively [2]. As our understanding of both pain management and the factors that play a role in the development of pain has increased, we have been able to target these and improve postoperative pulmonary morbidity and pain scores [1,2]. We aim to review different means of pain control in this paper in order to assess their effectiveness in achieving optimum results.
Thoracotomy
The mechanism of pain in thoracotomy involves the innervation of the intercostal, sympathetic, vagus and phrenic nerves [3]. Additionally, shoulder pain may result from stretching of the joints during the operation.
After a thoracotomy, pain can persist for two months or more, and in certain incidences it recurs after a period of cessation. The incidence of chronic pain post thoracotomy is reported to be 22-67% in the population [4]. Good surgical technique and effective acute post-operative pain treatment are evident means of preventing post-thoracotomy pain and consequent pulmonary complications [4]. Due to the multifactorial character of the pain, a multimodal approach to target pain is advised. Typically, both regional and systemic anaesthesia are administered. A combination of opioids such as fentanyl or morphine are typically used [5]. A variety of techniques for the administration of local anaesthetics are available at present, and the effectiveness of each is assessed in this paper.
a) Thoracic Epidural Analgesia (TEA)
TEA was the most widely used method of means of analgesia. It was the gold standard means of pain relief [6,7]. It is typically inserted prior to general anaesthesia, at the level of T5-T6, midway along the dermatomal distribution of the thoracotomy incision. A study by Tiippana et al. [8] measured the visual analogue scale (VAS) in order to assess the presence of pain during rest and at the time at which they coughed in 114 patients of whom 89 had TEA and 22 who had other methods of pain control. TEA was effective in alleviating pain at rest and during coughing. In TEA patients, the incidence of chronic pain of at least moderate severity was 11% and 12% at 3 and 6 months, respectively. The study found that at one week after discharge, 92% of all patients needed daily pain medication. The study advised for extended postoperative analgesia for up to the week post-discharge to be administered in order to manage this. The study however concluded overall, that TEA was effective in controlling evoked post-operative pain. However, the study did encounter problems of technical form in 24% of the epidural catheters. The incidence of chronic pain, however, was lower compared with previous studies where TEA was not used. Several other studies support that TEA is superior to less invasive methods. According to Shelley B. et al. [9] TEA was preferred by 62% of the respondents over paravertebral block (PVB) with 30% and other analgesic techniques with 8%. Limitations of this technique included hypotension and urinary retention. Certain patients with active infection and on anticoagulation are excluded from epidural placement.
b) Paravertebral Block (PVB)
PVB is considered an effective method for pain management and its use has been increased in the recent years. This technique involves injecting local anaesthetic into the paravertebral space and it is able to block unilateral multi-segmental spinal and sympathetic nerves. Previous studies have shown that it is effective in achieving analgesia and is associated with a lower incidence of side effects such as nausea, vomiting, hypotension and urinary retention [10,11]. As the lungs are collapsed, it is associated with a lower risk of pneumothorax.
In a study by Davies R.G. et al. [10] there was no significant difference in pain scores, morphine consumption and supplementary use of analgesia between TEA and PVB. The rate of failed technique was lower in PVB (OR =0.28, p=0.007). Respiratory function was improved at both 24 and 48 hours with PVB but only significantly improved at 24 hours.
c) Intercostal Nerve Block (ICNB)
ICNBs are generally administered as single injections at least two dermatomes above and below the thoracotomy incision [12]. It is performed percutaneously or under direct vision, using single injections or through placement of an intercostal catheter. It can also be formed using cryotherapy. It is associated with reduced post-operative pain scores; however, it is less effective than TEA in controlling chronic pain [12]. This was illustrated by a study by Sanjay et al. [12] which found that patients that underwent ICNB had higher pain scores 4 hours post-operatively, than those who received epidural anaesthesia using 0.25% bupivacaine (p<0.05). The study concluded that in the early post-operative period there was significant impact in pain relief for both techniques, but thereafter, epidural anaesthesia was proven to significantly reduce post thoracotomy pain over ICNB. Due to the multifactorial nature of post-thoracotomy pain, various approaches are required in order to target pain. ICNBs are useful in the blockade of intercostal nerves, whilst PVB and TEA appear to block the intercostal and sympathetic nerves. Due to the inability of regional anaesthesia to block the vagus and phrenic nerves which are implicated in the pathophysiology of pain, NSAIDs and opioids are required as adjuncts. TEA is proven to be the most effective means of treating pain alongside PVB; however, it is associated with more side effects than PVB. At present, there are a limited number of studies directly comparing pain control and post-operative outcomes between PVB and TEA. There is no conclusive evidence that either method is superior to the other regarding pain control.
Video-Assisted Thoracoscopic Surgery (VATS)
Existing evidence supports the noninferiority of thoracic PVB when compared to TEA for postoperative analgesia [13]. PVB is versatile and may be applied both unilaterally or bilaterally. It can be used to avoid contralateral sympathectomy, consequently minimising hypotension. This is an apparent advantage it has over thoracic epidural. Furthermore, it offers a more favourable side effect profile when compared to epidural anaesthesia. At present, the factors taken into consideration when selecting a regional technique include tolerance of side effects associated with TEA, consensus on best practice/technique, and operator experience [13]. A randomised controlled trial by Kosiński et al. [14] compared the analgesic efficacy of continuous thoracic epidural block and percutaneous continuous PVB in 51 patients undergoing VATS lobectomy. The primary outcome measures were postoperative static (at rest) and dynamic (coughing) visual analogue pain scores (VAS), patient-controlled morphine use and side-effect profile. The study found that pain control (VAS) was superior in the PVB group at 24 hours, both at rest (1.7 vs3.3, p=0.01) and on coughing (5.8 vs 6.6, p=0.023), and control of pain at rest was also superior in the PVB group at 36 hours (3.0 vs 3.7 (p=0.025) and at 48 hours (1.2 vs 2.0, p=0.026). There were no significant differences in the postoperative morphine requirements. In regard to side-effect profile, the study showed that the incidence of postoperative urinary retention (defined as no spontaneous micturition for 8 hours or ultrasound-assessed volume of the urinary bladder >500ml) was greater in the epidural group (64.0% vs 34.6%, p=0.0036), as was the incidence of hypotension (32.0% vs 7.7%, p=0.0031). There was no significant difference in the incidence of atelectasis (4.0% vs 7.7%, p=0.0542). However, the incidence of pneumonia was significantly more frequent in the PVB group (3.8% vs 0%, p=0/0331). Kosiński et al. concluded that PVB is as effective as thoracic epidural block in regard to pain management as it offers a superior safety profile with minimal postoperative complications. A further randomised controlled trial by Okajima et al. [15] compared the requirements for postoperative supplemental analgesia in 90 patients who received wither a PVB or thoracic epidural infusion for VATS lobectomy, segmentectomy or wedge resection. The main outcome measures were pain scores at rest (verbal rating scale 0= none and 10=maximum pain), blood pressure, side effects and overall satisfaction scores relating to pain control (1=dissatisfied and 5=satisfied). The study found a similar frequency of supplemental analgesia (50mg diclofenac sodium suppository or 15mg pentazocine intramuscularly) for moderate pain in both groups, with 56% of those in the PVB group requiring ≥2 doses, compared to 48% in the epidural group (p=0.26). Hypotension, defined as a systolic blood pressure <90mmHg, occurred more frequently in the epidural group (21.2% vs 2.8%, p=0.02). There was no difference in the incidence of pruritus (3.0% vs 0%, p=0.29) and post-operative nausea and vomiting (30.3% vs 25.0%, p=0.62) between both groups. The study found no statistical difference between patient-reported satisfaction in pain control between epidural and PVB using the verbal rating scale (5.0 vs 4.5, p=0.36). The study concluded that PVB offered additional to equivalent analgesia to epidural, a lower incidence of haemodynamic instability postoperatively. A further study by Khoshbin et al. [16] performed an analysis on 81 patients undergoing VATS for pleural aspiration +/- pleurodesis, lung biopsies or bullectomy. The main outcome was postoperative pain levels, documented every 6 hours and scored against the Visual analogue Scale (0= no pain, 10= worst possible pain). In both PVB and epidural groups, bupivacaine 0.125% was the local anaesthetic of choice, with clonidine added to the epidural infusion at 300μg in 500ml. The study showed that there was no significant difference in mean pain scores between PVB or EP (2.1 vs 2.9, p=0.899), therefore concluding that PVB is as effective as epidural in controlling pain post-VATS.
Robotic Lung Surgery
Minimally invasive techniques are considered advantageous over open surgical approaches due to their shorter recovery times, reduced perceived levels of pain post-operatively and shorter postoperative length of stay in hospital [17-19]. Robotic surgery has become a popular method in recent years. Debate remains regarding whether robotic surgery is superior to VATS in regard with pain reduction. A case control study by Louie et al. [19] compared 45 robotic assisted lobectomies (RAL) to 34 VATS lobectomies. The study showed that both groups had a similar mean ICU stay (0.9 vs 0.6 days) and a mean total length of stay (4.0 vs 4.5 days). The study showed that patients that underwent robotic lobectomies had a shorter duration of analgesic use post-operatively (p=0.039) and a shorter time resuming to normal everyday activities (p=0.001). A limitation in this study was an inaccurate record of the amount of pain relief used by the patients, ultimately working as a confounding factor when interpreting the results. In a separate study by Jang et al. [18] 40 patients undergoing RAL were compared retrospectively to 80 VATS patients (40 initial patients and 40 most recent patients), all with resectable non-small cell lung cancer. The study showed that the post-operative median length of stay was significantly shorter in RAL patients compared to the initial VATS patients. The rate of post-operative complications was significantly lower in the RAL group (10%) compared to the initial VATS group (32.5%) and similar to the recent VATS group (17.5%). Post-operative recovery was easier for patients in both the RAL and VATS group due to earlier mobilisation, allowing them to return to their everyday activities quicker. In a retrospective review by Kwon et al. [17] 74 patients undergoing robotic surgery, 227 patients undergoing VATS and 201 patients undergoing anatomical pulmonary resection were assessed and compared with regard to acute (visual pain score) and chronic pain (Pain DETECT questionnaire). The study showed that there was no significant difference in acute or chronic pain between patients undergoing robotic assisted surgery and VATS. Despite no significant difference in pain scores, 69.2% of patients who underwent robotic-assisted surgery felt the approach affected their pain versus 44.2% of the patients who underwent VATS (p=0.0330). These results all support the superiority of robotic surgery over VATS and open approaches with regard to pain, length of hospital stay and recovery times. Both robotic surgery and VATS have their benefits i.e. two-versus three-dimensional view, instrument manoeuvrability, and reduced post-operative pain.
Conclusion
Since post-thoracotomy pain is multifactorial, a multimodal approach is required. In particular, ICNB blocks the intercostal nerves, and PVB and TEA appear to block the intercostal and sympathetic nerves. NSAIDs and opioids are required as valgus and phrenic nerve cannot be blocked by regional anaesthesia. TEA is evident to be the most effective in treating pain alongside with PVB. It is however associated with more side effects than PVB.
To know more about our Journal of Surgery click on https://lupinepublishers.com/surgery-case-studies-journal/
To know more about Lupine Publishers click on https://lupinepublishers.us/
To know more about Open access publishers click on Lupine Publishers
18 notes
·
View notes
Text
Is There A Neck-Shoulder Syndrome?| Lupine Publishers

Lupine Publishers| Anesthesia and pain medicine Journal
Abstract
Concomitant presentation of neck and shoulder pain is a common clinical scenario which can present a significant diagnostic and therapeutic dilemma. Neck and shoulder pain presentations can be separated into four different categories: Primary neck pathology with referred pain to the shoulder, primary shoulder pathology with referred pain to the neck, primary neck and primary shoulder pathology, and primary neck pathology resulting in secondary shoulder pathology. Primary neck pathology resulting in secondary shoulder pathology is mechanically plausible but not proven. Authors are proposing this scenario to be described as “neck-shoulder syndrome.” For instance, C5 and/or C6 cervical radiculopathy can result in rotator cuff, deltoid, biceps and scapular muscle weakness as these nerve roots innervate the shoulder girdle musculature which in turn could produce shoulder/scapular muscle imbalance resulting in shoulder impingement signs. A patient may present with features of both cervical radiculopathy and shoulder impingement syndrome in this scenario. At this time there are no agreed clinical criteria for a diagnosis of “neck-shoulder syndrome.” As with any other syndrome, management differences can only be well studied once the entity has been properly defined. In this article, authors set out to summarize how to best approach patients presenting with both neck and shoulder pain while describing features of proposed “neck-shoulder syndrome.” It is paramount to take a comprehensive and holistic approach towards patients presenting with concomitant neck and shoulder pain as the symptoms may not always represent isolated entities.
Keywords: Neck and shoulder pain; Neck-shoulder syndrome; Pain treatment; Differential diagnosis of neck and shoulder pain
Introduction
Co-existent neck and shoulder pain has been described in limited fashion in the literature as a unique diagnosis, but the concomitant presentation of neck and shoulder pain is a common scenario in primary care and orthopedic offices [1,2]. Gorski et al described “shoulder impingement syndrome” where patients presented with neck pain secondary to rotator cuff tendinopathy [1]. Compere et al described a “neck, shoulder, and arm syndrome” which primarily referred to neuropathic pain in the neck, shoulder and arm resulting from a brachial plexus lesion [2]. When patients present with both neck and shoulder pain, it can present a significant diagnostic dilemma[3]. “Hip spine syndrome” has recently been described, and “neck-shoulder syndrome” likely represents an analogous entity involving the cervical spine and upper limb [4]. It is estimated that among primary care office visits, neck pain accounts for approximately 20-30% and shoulder pain for 10-20% of musculoskeletal complaints. From this population, combined neck and shoulder problems account for approximately 6-10% [3,5,6,7].
Discussion
Concomitant neck and shoulder pain presentations can be separated into four different categories: Primary neck pathology with referred pain to the shoulder, primary shoulder pathology with referred pain to the neck, primary neck and primary shoulder pathology, and primary neck pathology resulting in secondary shoulder pathology
Primary neck pathology with referred pain to the shoulder
An isolated C5 and/or C6 radiculopathy without shoulder pathology could certainly present with neck and shoulder pain due to C5 and C6 dermatomal symptoms corresponding to the shoulder region. C5 or C6 myotomal pain can cause pain in the deltoid, scapula and biceps, and can mimic shoulder pathology [8,9]. This scenario is typically straightforward as the physical examination will be absent of shoulder impingement signs. Classically, cervical radiculopathy examination can demonstrate positive cervical root impingement signs (Spurling’s maneuver), myotomal weakness, dermatomal sensory abnormalities and blunted reflexes in a specific root distribution. Several neuropathies involving brachial plexus and its proximal branches will also refer pain to neck and shoulder simultaneously.
Primary shoulder pathology with referred pain to the neck
Primary shoulder pathology should not directly lead to neck pathology, and such cases are not well described in the literature. Nevertheless, patients with shoulder pathology may develop pain and tightness in the trapezius muscle on the ipsilateral side and referred pain in the cervical area. Restricted motion at the glenohumeral joint may also lead to overuse and pain in the scapulothoracic musculature. A general concern in musculoskeletal medicine is that symptomatic pathology in a joint may refer pain to a joint below and/or above.
Primary neck and primary shoulder pathology
Degenerative arthritis can affect multiple joints. Thus, many patients may have both glenohumeral arthritis and cervical spondylosis. The radiographic incidence of glenohumeral arthritis is reported as 32.8% in people over 60 years of age [10]. Radiographic evidence of cervical spondylosis is present in 50% of people over 50 years of age and 75% of individuals over 65 years of age [11]. As both conditions are common, both can present as “pain generators.”
Primary neck pathology resulting in secondary shoulder pathology
Primary neck pathology resulting in secondary shoulder pathology is mechanically plausible although not proven. For instance, C5 and/or C6 cervical radiculopathy can result in rotator cuff, deltoid, biceps and scapular muscle weakness as these nerve roots innervate the shoulder girdle musculature. This could produce muscle imbalance and poor shoulder/scapular mechanics. A patient may present with features of both cervical radiculopathy and shoulder impingement syndrome in this scenario. In clinical practice, it is not uncommon to see a patient with chronic neck pain presenting with insidious onset of shoulder pain later in the course. Authors are proposing this unique presentation be referred to as “neck-shoulder syndrome.” Although most clinicians would treat this as separate neck and shoulder pain, they may be related diagnoses.
Literature Search
We conducted a comprehensive search in the PubMed database in order to identify relevant studies on “neck-shoulder syndrome.” Based on the review of the available literature, there are no agreed upon clinical criteria for a diagnosis of “neck-shoulder syndrome” despite its common clinical presentation nor is there a well described “neck-shoulder syndrome.” As with any other syndrome, management differences cannot actually be studied until the entity has been appropriately defined. This article will concentrate on how to best approach patients presenting with both neck and shoulder pain while describing features of proposed “neckshoulder syndrome.”
Presentation
In patients presenting with neck and shoulder pain, a thorough history is paramount in identifying the etiology of the patient’s pain.
Location: Patients with primary neck pathology can experience pain extending beyond the neck based on the etiology. Disorders that affect the lower cervical nerve roots will often result in pain distal to the shoulder which can be characterized by radiation into the arm in a clear dermatomal or myotomal distribution [12]. In addition, Dwyer et al described reproducible pain patterns that can refer into the shoulder, trapezius and occiput from cervical zygapophyseal joint pathology [13-15]. Pain from a primary shoulder problem can also refer pain to the neck, periscapular region and distally into the arm although not typically extending below the elbow [16]. Associated paresthesias are not classically associated with a primary shoulder problem.
Onset: Onset of symptoms is also a key component of the history. Degenerative cervical pathology can have insidious onset although acute disc herniations can have a sudden onset that may be precipitated by trauma. Whiplash injuries are known to precipitate neck pain which can be of myofascial and/or cervical facet in origin. Shoulder disorders can also be of insidious (overuse injuries) or acute onset (trauma). Sudden onset of shoulder pain with restricted motion can be associated with acute calcific tendinitis or adhesive capsulitis. Neuralgic amyotrophy (Parsonage Turner syndrome/ brachial neuritis) has a unique presentation where patients usually experience severe, acute pain following exercise, recent illness, immunization, surgery or trauma [17]. As the initial severe pain starts to resolve, neurological deficits will become apparent, which is in contrast to most presentations of cervical radiculopathy where pain will continue with associated neurological symptoms. Onset of symptoms plays a key role in proper identification of proposed “neck-shoulder syndrome.” Development of shoulder pain (especially in the absence of injury) after onset of neck/radicular pain can be considered primary neck pathology with secondary shoulder pathology and can be referred to as “neck-shoulder syndrome.” Shoulder pain in this scenario is likely secondary to rotator cuff and periscapular muscle weakness/imbalance caused by C5 and/or C6 cervical radiculopathy. This clinical scenario is not well studied in the literature, hence prevalence and incidence is not known. Among patients with cervical radiculopathy, studies report a frequency of C5 nerve root involvement at 5-10%, C6 at 20-25%, and C7 at 45-60% [12,18].
Exacerbating factors: Pain with overhead arm movements generally suggests primary shoulder pathology. However same pattern can also be present in peripheral neuropathies like thoracic outlet syndrome and spinal accessory, suprascapular, or axillary neuropathy. Shoulder pain with side lying on the affected upper limb tends to be associated with shoulder impingement and acromioclavicular joint arthropathy.
Features of systemic diseases: In patients who present with neck and shoulder pain in the absence of trauma, the history will need to include an assessment for widespread involvement that may suggest systemic disease processes like fibromyalgia, polymyalgia rheumatica, myofascial pain syndrome and myopathy.
Red flags: The history should also include an evaluation for findings to suggest a disease process that requires more urgent evaluation. Red-flag symptoms to assess for include gait imbalance, hand clumsiness, bowel/bladder dysfunction (cervical myelopathy), pain after high impact trauma (fractures), unintentional weight loss (Pancoast tumor), chest pain (cardiac ischemia), blurry vision, nausea/vomiting and vertigo (vertebral artery dissection/ insufficiency).
Physical Examination
In addition to a detailed history, a thorough physical examination is key for proper diagnosis and identification of the pain generator(s). A thorough neurological exam plays an essential role in distinguishing neck from shoulder pathology. Sensory, motor and reflex changes in a specific nerve root distribution are characteristic of cervical radiculopathy. C5 and C6 cervical radiculopathies may result in periscapular and shoulder/rotator cuff muscle weakness while C7 radiculopathy is unlikely to cause shoulder weakness. Rotator cuff pathology may result in shoulder weakness with preserved elbow flexion while a C5 radiculopathy can result in weakness of both. Testing deltoid strength with the arms at the sides instead of in shoulder abduction can aid in differentiating pain inhibition versus true weakness.
Provocative Testing
Provocative testing can assist in the diagnosis of cervical and shoulder disorders [9, 19]. Among them, provocative tests for shoulder impingement may help distinguish primary versus secondary shoulder pathology in proposed “neck-shoulder syndrome”(Table 1) [18-30].
In patients with neck and shoulder pain, one test by itself may not have enough sensitivity and specificity to make a diagnosis and most physical exam maneuvers are not pathognomonic. A combination of multiple exam components and a thorough history are necessary to accurately identify the etiology of symptoms.
Table 1: Provocative tests for common cervical and shoulder problems and reported validity.

Diagnostic Testing
When presented with both neck and shoulder pain, history and physical exam should dictate appropriate use of diagnostic tests. Although imaging studies such as radiography, CT and MRI can reveal many pathologies, further testing should be done to identify the true pain generator. When suspecting pain mediated by a cervical zygapophyseal joint, cervical diagnostic medial branch blocks can be considered. A shoulder injection of lidocaine with or without corticosteroid can be done for diagnostic and perhaps therapeutic reasons. In cases of secondary shoulder pathology, this may give the patient partial benefit, but a primary cervical pathology should still be investigated [9]. Electrodiagnostic testing with electromyography (EMG) and nerve conduction studies (NCS) can be employed when suspecting myopathy, brachial plexopathy, peripheral neuropathy or radiculopathy. When evaluating neck and shoulder pain, scientific evidence suggests using a combination of history, physical examination, imaging modalities, diagnostic injections and electrodiagnostic study to make the appropriate diagnosis.
Treatment
Success of any proposed treatment algorithms will depend on an accurate diagnosis. There is scant evidence on how to approach the concomitant presentation of neck and shoulder pain. Treatment should be geared toward the primary site of pathology whether it be the cervical spine or the shoulder [3]. Lack of current literature evidence underscores the importance of describing a “neckshoulder syndrome,” as it can lead to studies looking at management differences. It can be hypothesized that in patients with cervical radiculopathy with secondary rotator cuff impingement, treatment of the primary lesion will likely yield eventual improvement at the secondary site although no studies have been done on this topic.
Conclusion
The concomitant presentation of shoulder and neck pain is a common scenario in primary care and orthopedic offices and can present a diagnostic and therapeutic dilemma. A careful history and thorough physical examination along with ancillary studies can often yield the correct diagnosis and successful treatment. Primary neck pathology resulting in secondary shoulder pathology is mechanically plausible but not proven. Authors are proposing this scenario to be described as “neck-shoulder syndrome.” Appropriately describing a “neck-shoulder syndrome” can lead to further studies looking at management differences. A prospective study looking at incidence of shoulder impingement signs in chronic C5 and/or C6 radiculopathy patients could be helpful in delineating diagnostic criteria for “neck-shoulder syndrome.” Above all, it is paramount to take a comprehensive and holistic approach towards patients presenting with concomitant neck and shoulder pain as the symptoms may not always represent isolated entities.
Acknowledgements
The authors would like to thank Dr. David Janerich for his help with the development of the article.
For more Lupine Publishers Open Access Journals Please visit our website:
https://lupinepublishers.us/
For more Global Journal of Anesthesia & Pain Medicine articles Please Click Here:
https://lupinepublishers.com/anesthesia-pain-medicine-journal/index.php
To Know More About Open Access Publishers Click on Lupine Publishers: https://lupinepublishers.com/
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
#Lupine Publishers#Lupine Publishers Group#Open Access Journals#Anesthesia Jounal#Pain medicine#pain management#general anesthesia#local anesthesia#surgery#post operative#critical care
3 notes
·
View notes
Text
Lupine Publishers | Historical Silahtaraga Power Plant-Black Sea Decovil Line Research, Double Military Decovil Photogrammetry Study
Lupine Publishers- Anthropological and Archaeological Sciences Journal Impact Factor
Abstract
In this article, which we prepared in addition to the works carried out by tracing a lost cultural heritage, In 1915 Turkish geography, investigation and photogrammetry study on the narrow-gauge railroad line built to transport coal from the Black Sea coast to the Golden Horn will be included. In the study, a CAD model created by measurements made from old photographs related to the subject will be used as data in the prototype to be produced by SLS (Selective Laser Sintering) method. Then, we believe that the miniature model and production adventure of the Decovil locomotive, which we have brought to the present with the noncommercial serial production of the model, will be the means of remembering at least a cultural heritage that has not reached today.
Introduction
In this part of the study, the research of the historical railway and its archaeological importance will be shared. In this review, news published on the internet pages and books and some collection materials prepared by the researchers were used. The narrow-gauge railroad line located in the boundaries of Istanbul, in Kagithane district was founded in 1915. In order to uncover the lost story of this railway which ended in 1950 with the dismantling of the rails, a book published named “100 years later on the trail of a lost railway”. In the study carried out by the Municipality of Kagithane as a multi-disciplinary team, the team of writers created an important task in bringing the cultural heritage to the present day by bringing together the written documents, photographs and pieces of the railway which have the chance to reach today.
In the studies, many details related to the narrow-gauge railroad line, which was built for the purpose of transporting coal from the lignite basin in Agacli (25 km area starting from Kilyos to the Terkos Lake on the Black Sea coast) to the power plants in the Golden Horn, have been delivered to our day[1]. If we need to share some valuable details about the railway: The Kagithane- Black Sea decovil line, which was effectively used to meet energy needs during the First World War, was built between 1914 -1916 and is 57 km long (Figure1). The distance between the rails of the railway is 60cm and this system is called as decovil [2]. The name dekovil comes from the company founded in 1875 of the surnames of the French engineer and businessman Paul Decauville who lived between 1846 -1922 [3].
The period when the line was established, World War I continues in the region. There is an energy problem in Istanbul due to the imports of coal stopped from the UK due to the war and the damage of ships bringing coal from Zonguldak to the region during the war. The fact that the Canakkale Strait was closed due to the war made it impossible to import coal through the Mediterranean. In the Ottoman geography of the period, coal was used as an energy source in ships and power plants rather than domestic fuel. Today it is a museum building; the building, known as Silahtaraga Power Plant of the period, meets the electricity needs of Istanbul (Figure2). With the planned decovil line, it is aimed to evaluate the coal reserve on the Black Sea coast and to transport it to the Silahtaraga Power Plant without the need for sea transportation. In this way, the solution to the energy problem of Istanbul will be produced. Although the existence of the coal reserves of Agacli, Ciftalan region on the Black Sea coast has been known since the Byzantine Period, no studies have been conducted to make the reserve available for use. After the preliminary investigation, it is determined that the desired yield can be obtained by mixing the lignite coal in the region with Zonguldak hard coal, and it is decided to use the coal in the region and construction of the decovil line is started. The entire installation works are photographed by Hasan Mukadder Dolen, the railway regiment officer of the period.
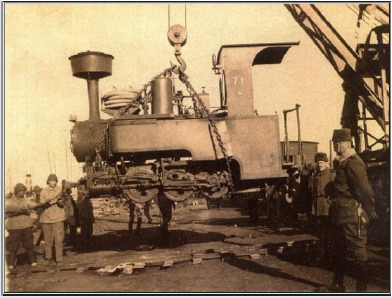
The period when the line was established, World War I continues in the region. There is an energy problem in Istanbul due to the imports of coal stopped from the UK due to the war and the damage of ships bringing coal from Zonguldak to the region during the war. The fact that the Canakkale Strait was closed due to the war made it impossible to import coal through the Mediterranean. In the Ottoman geography of the period, coal was used as an energy source in ships and power plants rather than domestic fuel. Today it is a museum building; the building, known as Silahtaraga Power Plant of the period, meets the electricity needs of Istanbul (Figure2). With the planned decovil line, it is aimed to evaluate the coal reserve on the Black Sea coast and to transport it to the Silahtaraga Power Plant without the need for sea transportation. In this way, the solution to the energy problem of Istanbul will be produced. Although the existence of the coal reserves of Agacli, Ciftalan region on the Black Sea coast has been known since the Byzantine Period, no studies have been conducted to make the reserve available for use. After the preliminary investigation, it is determined that the desired yield can be obtained by mixing the lignite coal in the region with Zonguldak hard coal, and it is decided to use the coal in the region and construction of the decovil line is started. The entire installation works are photographed by Hasan Mukadder Dolen, the railway regiment officer of the period. Hasan Mukadder Dolen’s photo collection was left to his grandson Emre Dolen after his death in 1975. It is known that many photographs and information about the historical railway have survived through this channel. Following the first line completed in 1915, a second line was built in Ciftalan in 1916. Railway rails and locomotives produced by Germany’s decovil line, with many stations, vehicles and employees is important in terms of energy logistics of the period. It is mentioned in the historical documents that the rails and locomotives transported from Germany to the Ayestefanos Railway Regiment warehouses in Yesilkoy by the Danube River were later brought to Eyup, Silahtaraga by ships (Figure3).
The first line starts from Silahtaraga and reaches Agacli village after Kagithane stream; the other line runs through the Belgrade forests to the village of Ciftalan. The light rail line that reached the Black Sea coast from Kagithane, which is the famous promenade of the period, undertook an important duty in coal transportation during the years it was established, but was forgotten by being out of use in time. The line was transferred to the Ministry of Commerce in 1922 and to the Ministry of Economy after the proclamation of the Republic [4]. Although traces of the line disappeared in the region after 1956, the rails remained largely underground and in many regions the rails were removed. It is known that one of the locomotives is currently located in the Celtek coal mine depot of the Special Provincial Administration of Amasya. In the photogrammetry study for the protection of cultural heritage, CAD model will be created by using original photographs of locomotives known as Zwilling Heeres Feldbahn (Double Military Decovil) produced in Munich in 1890 by Krauss Werkshof [1] (Figures 4 & 5). The first prototype of the model produced with SLS (Selective Laser Sintering) one of today’s 3d print technologies, will be used for silicon mould technique in mass production.
Literature on Photogrammetry
In this part of the article, the photogrammetry study carried out with measurements taken from photographs of locomotives used in historical railway will be shared. In this context, sharing of literature knowledge about photogrammetry and its usage areas and then modelling study were included in the study. Visual analysis techniques are used in many scientific research areas. In the fields of anthropology and sociology, from the use of photographs of past periods [7] to airborne imaging technologies[8]; visual analysis techniques in different scientific fields from ecology, geography to medical science [9], are basically based on the use of photography as a source of information. Photographs used as data in the social field allow interpretations, social-cultural determinations and visual analysis of the time of the photograph [10]; in technical fields, it can also be used as a digital data source. The use of photography for numerical data acquisition will be explained within the framework of photogrammetry concept. The word, which consists of a combination of ancient Greek “photos” (light), “grama” (drawing) and “metron” (measurement), means measuring with the help of pictures. Photogrammetry, which is used only in mapping, has been used in different areas in the following years. Basically, the photographic analysis to determine the shape, size and position of an object is called photogrammetry [11]. Photogrammetry is divided into three main sections (topographic photogrammetry, interpretation photogrammetry, special purpose photogrammetry) according to the application areas. Photogrammetry used in the fields of architecture, dentistry and archaeology is included in this third group [12]. In recent years, many studies have been done to document the cultural heritage with photogrammetric methods [13], photogrammetry has been used extensively in histor ical works documentation and model formation processes [12]. In such studies, the measurements taken on the photos allow the creation of the 3-D model of the historical work on the computer with digital photogrammetric techniques [14]. While the measurement process is carried out with the points and lines determined by the software, different methods can be used. In our study, the CAD model, which is designed with the measurements with calliper and ruler from old photographs, will be discussed within the scope of special-purpose photogrammetry.
Modelling Process
In this part of our study, we will discuss the modelling process created by taking measurements from the historical photographs of the railway line locomotive of Kağithane. In the modelling study, the locomotive CAD model was created in CATIA V5. The modelling; cabin, nose, mechanical parts and rails, including a total of 4 body consists of (Figure 7). Part design tools are used in the modelling. The modelling of the locomotive as 4 bodies is taken into consideration for the production criteria for the silicone mould to be needed during mass production. In this sense, the model has been modelled and divided into pieces so as to enable post-production assembly. In the modelling study, first the technical drawings (Figure 6) made by Alan Prior were used for general information about the model; in the detail drawings, black and white photographs taken from different angles were used. After the results of modelling, some forms are very detailed for the casting process and line softening is performed according to the model casting process (Figure 7).
Data Transfer to 3d Printing System After Modelling
(STL File, Quality Problems) STL (Stereolithography) data is needed for additive manufacturing of the model. The CAD data generated for this reason is exported in the STL format in the CATIA software. In this process, STL mesh quality is important for the surface quality of the model to be produced. The quality of the prototype to be produced with SLS will affect the quality of the silicone mould from this prototype. The quality problems in the STL data are related to the number of mesh on the surface and the settings of the CATIA display and the necessary arrangement is made as follows: First, the screen settings are set in the ”tools“ - ”options” – “performance” section in the top menu of the CATIA Part Design module. In this section, the 3D Accuracy and 2D Accuracy “fixed” values are revised to “0.01”. The value 0.01 remains constant until changed again. The next editing is done in the CATIA STL Rapid Prototyping module. In the “tesselation” command, with “sag” value, 0.001mm and “grouped” option preference, the mesh quality of each part is determined (Figure 8: on the effect of mesh quality adjustment on surface quality in STL data).
Model Production Process
The technique used in the prototype production is SLS (Selective Laser Sintering) and the material used is PA 2200 (polyamide). If we need to give basic information about SLS production system: The SLS technique is made by sintering micron-size polymer powder in layers, using laser power. In 1986, Carl Deckard, a student at the University of Texas, developed this method of powdered material, which he called PGLSS (Part Generation by Layer wise Selective Sintering). Later on, this production technique called SLS, (with the description text: computer-aided laser apparatus which sequentially sinters a plurality of powder layers to build the desired part in a layer-by-layer fashion) is patented on October 1986 [15]. The method of SLS production is as follows: Firstly, files saved in STL format are opened in Netfabb software and settled in the production area. (Figure5). All parts are sliced at intervals of 0.1 mm (100 microns) after placement. Then the file sliced into 100 microns is saved in SLI format. Although there are 60 microns slicing options within the system, 100 microns will be sufficient for the desired quality. Then the process will continue in the EOS PSW software. After the material preference and parameter selection in EOS PSW software, the file will be transferred to the production bench. The material preference is selected as PA2200 and the layer thickness is 100 microns. The production parameter is then determined. After the prototype production to be performed in EOS P110 (Figure 9), silicone moulding will be carried out for mass production.
The first prototype produced with PA 2200 material, is used to form the silicone mould. After that, the model which is replicated in the manufacturer company by casting process from polyester material is painted with handwork and the final product is obtained (Figure 10). In classical applications, the silicone mould is taken from the prototype modelled by the sculptor and polyester casting process is performed. In the prototype production subject to our study, the process was completed by using digital technologies and methods. In the study, modelling was performed in parametric cad software, enabling the revisions needed in the process to be made quickly.
For More Lupine Publishers Open Access Journals Please visit our Website:
https://lupinepublishers.us/
For More Anthropological and Archaeological Sciences Articles Please Click Here:
https://lupinepublishers.com/anthropological-and-archaeological-sciences/
To Know More About Open Access Publishers Please Click on Lupine Publishers
Follow on LinkedIn: https://www.linkedin.com/company/lupinepublishers
Follow on Twitter: https://twitter.com/lupine_online
36 notes
·
View notes
Text
Lupine Publishers | Post Endodontic Pain Reduction using three Irrigants with Different Temperature

Lupine Publishers | Journal of Otolaryngology Research Impact Factor
Abstract
Objective: The purpose of this research was to evaluate whether meticulous irrigation with three different temperatures would help in a decrease dental pain.
Materials and Methods: All 120 patients had teeth chosen for conventional RCT for prosthetic reasons in teeth with vital pulps. All canals were cleaned and shaped with Reciprocal files. Final irrigation was done with cold saline solution (6 OC, 4 OC, and room temperature).
Results: A total of 120 of 135 patients (69 females and 51 male) were included whereas 15 were excluded as not achieving the necessities of the study. All patients presented with a vital upper or lower molar, premolar, or front teeth. No statistically major change (P>0.05) between the groups was found regarding the degree or duration of pain.
Conclusion: The approach in both selecting the patients participating in the research and analyzing the data in this research allows us to determine that cryotherapy is an aid of clinical procedures to clean and shape the canals to decrease the occurrence of post-endodontic pain and the need for medication in patients presenting with a diagnosis of vital pulp.
Keywords: Apical healing; Flare-ups; Pain; Post endodontic pain; Post-operative pain
Introduction
Post-endodontic pain is an undesirable sensation occurred in patients regardless of the preoperative periapical status of the tooth treated. Therefore, prevention and management of post endodontic pain are essential in endodontic practice [1]. Organic material, microorganisms, and irrigating solutions extruding beyond the apical constriction during root canal therapy (RCT) will originate inflammation and periodontal ligament complications, such as severe pain or flare-ups. It must be noticed that the amount of extruded material (debris and/or irrigate) varies widely in the reported studies which indicate problems and inconsistencies in treatment methodologies [2-4]. Recent literature has showed that keeping apical patency would not generate more postoperative difficulties [5-7]. A recently issued in vitro study showed that intracanal delivery of cold irrigating solution at 2.5 °C with negative pressure flushing reduced the external surface temperature to close 10 °C [8-10], would be enough to create a local anti-inflammatory beneficial consequence in peri radicular tissues. Cryotherapy proposes that using cold over some procedures may decrease the diffusion of nerve signs, bleeding, edema, and local inflammation and is therefore effective in the reducing of pain. Therefore, the purpose of this research was to evaluate whether meticulous irrigation with three irrigating practices with different temperature would help in a decrease of post-endodontic pain.
Three expert endodontists with a private practice of 17 years and skilled in the procedures and procedures studied were included in the research and performed 40 RCTs each (a total of 120) in upper/lower front or back teeth with irreversible pulpitis recognized by pulp sensitivity testing with hot and cold. Pulpal response tests were achieved by the main author, and a digital X ray diagnosis was documented by three certified clinicians. Additional clinical necessities for patients´ inclusion were as follows: Necessities of the research were agreed and spontaneously accepted, healthy patients were included, teeth with enough coronal structure and diagnosed with vital pulps, no previous RCT, and no analgesics or antibiotic consumption 7 days before the procedures. A total of 120 of 135 patients (69 females and 51 male) aged 18 – 60 years were referred and integrated in this research, whereas 15 were rejected as not accomplishing the necessities wanted. All participants showed with a vital upper or lower molar, premolar or front teeth designated for conventional RCT for dental rehabilitation reasons.
Methods
Dental procedures
Root canal treatment was done in one visit. Topical anesthetic (Anesthesia Topical, Astra, Mexico) was used. Patients received 2 carpules of articaine 2% with epinephrine 1:200,000 (Septodont, Saint-Maur des-Fosses, France). Situations in which supplementary anesthesia was needed, intra-ligamental anesthesia (2mL articaine 2%) was supplied. For the upper front teeth, the solution was administered by tender and slow local infiltration. For the lower teeth, one of the carpules was used for the lingual and alveolar nerve block, the other one for a moderate bucal infiltration nearby the tooth to be treated.
Irrigation protocols
Group 6 °C. The R25 (size 25/ .08) instrument was employed in tinny and curved canals, and R40 files (40/ .06) were used in broad root canals. Three in-and-out pecking series were employed with a fullness of not more than 3mm until getting the calculated WL. Patients allocated to this group receive a final irrigation with 5mL of cold (6 °C) 17% EDTA followed by 10mL of cold (6 °C) sterile saline solution dispensed to the WL using a cold (6 °C) metallic micro-cannula.
Group 4: Canals were instrumented as in group A. Patients allocated to this set received a final irrigation with 5mL of cold (4 °C) 17% EDTA followed by 10mL of cold (4°C) sterile saline solution dispensed to the WL using a cold (4 °C) metallic micro-cannula for 1 minute.
Group RT: The R25 (size 25/ .08) instrument was employed in tinny and curved root canals, and R40 files (40/ .06) were used in wide canals. Three in-and-out series were employed with a space of not more than 3mm until getting the calculated WL. Reciprocal instruments were used in one tooth only (single use). Participants allocated to this control group were treated similarly to the experimental groups, except that they received a final flush with 5mL (room temperature) of 17% EDTA followed by 10 mL (room temperature) of sterile saline solution delivered to the WL.
Statistical analysis
The related issues preoperatively recorded were integrated into the examination as follows: age and sex, occlusal contacts, and maxilla or mandibular teeth. Changes in the strength of pain among groups were studied using the ordinal (linear) X2 test. Variances in VAS-recorded standards after 24, 48, and 72 hours and in the quantity of analgesic intake among the two groups tested.
Results
Table 1: Distribution by group of teeth and location.
Table 2: Kruskal/Wallis test applied to the post-endodontic pain.
Table 1 displays the distribution of variables; a total of 120 participants took part in this study: 69 (57.5%) were women, and 51 (42.5%) were men. The ages fluctuated among 18 and 60 years; 87 (72.5%) were upper teeth, and 33 (27.5%) were lower teeth. The clinical management of the patients is showed in Table 1. No significant modification (P > 0.05) between the groups was encountered concerning the grade or period of pain. Rendering to the VAS examination, marks were seen 24 – 72 hours late in the 3 groups with a significant decline successively (Tables 2 & 3).
Table 3: Kruskal/Wallis test applied to the post-endodontic pain.
Discussion
Pain is tough to comprehend and calculate especially when it occurs unexpectedly in patients. The major trouble in knowledge painful and discomfort is the participant’s individual valuation and its dimension. For this objective, organization of the estimation form has to be entirely understood by participants. In our research, a simple spoken classification was followed in the feedback procedure with four classes: no pain, slight, modest, and intense pain. These classes were clearly comprehended by participants and were described by the occurrence or nonappearance of the necessity for pain-relieving treatment. Preoperative pain is one of the main predictors of post-endodontic pain [11-14]. Thus, only teeth with irreversible pulpitis indicated for RCT because of prosthodontic purposes were treated in this research. In our research, we reduced the variation in the procedures following protocols based on recommendations by authors and manufacturers. While successful endodontic treatment depends on various variables, an important point to consider in the shaping of the root canal system is the amount of the irrigating solution. Proper disinfecting and filling the root canal system is facilitated by the keeping of its original shape from the entrance to the apical third, without any iatrogenic event.
Conclusion
According to the conditions established for this study, there was no statistically significant difference between the instrumentation systems assessed.
For more Lupine Publishers Open Access Journals Please visit our website: h
http://lupinepublishers.us/
For more Journal of Otolaryngology Impact Factor articles Please Click Here:
https://lupinepublishers.com/otolaryngology-journal/
To Know More About Open Access Publishers Please Click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
44 notes
·
View notes
Text
Ganglion Impar Pulsed Radiofrequency for Intractable Coccydynia| Lupine Publishers
Lupine Publishers| Anaesthesia & Pain Medicine Journal
Abstract
Patient with coccydynia are often not easy to manage, the aim of this single case study was to describe the outcome of ganglion impar pulsed radiofrequency (PRF) of patient with intractable coccydynia. A 31 years old presented with severe coccydynia, symptom provocation occurred during long sitting, pain reached high level (NRS: 8/10). MRI showed degenerative changes in the sacrococcygeal junction. A first session of impar ganglion PRF for 8 min was applied and the patient was improved 80% for few months (NRS: 2-3/10), although the results of this case report cannot be generalized, it describes the successful outcome of patient with severe coccydynia.
Keywords: Coccydynia; Impar ganglion; Pulsed radiofrequency
Introduction
Ganglion impar is the lowest paravertebral sympathetic chain, which is placed at the anterior aspect of sacrococcygeal disc used to be blocked in many chronic pain conditions originating from pelvic structures such as the coccyx. Coccydynia is one of chronic pain syndrome which is usually intractable to known therapeutic modalities such as medications, steroid injection and physical therapy manipulation, in addition, there are invasive approaches such as neurolysis with alcohol, phenol or ablative radiofrequency, these approaches are neurodestructive techniques. PRF is a neuromodulative application that has been used for years for chronic pain syndromes. We present a case of coccydynia successfully treated with PRF for neuromodulation of the ganglion impar.
Patient Description
A 31-year-old man healthy, working as software developer, had pain over the coccyx started in 2015 without any history of trauma, increasing with time. The pain triggered with the prolonged sitting which made his work very difficult and start thinking to change his job, seen by many doctors, MRI of spine coccyx requested concluded degenerative changes in the sacrococcygeal junction Figure 1, he had been diagnosed as coccydynia and treated with conservative management including medications, coccyx steroid infiltrations and physical therapy manipulations , after the failure of conservative methods patient was referred to our pain clinic by his orthopedist, at this stage he became depressed because of functional limitation and job problems he described the pain as 8/10 point on verbal numerical rating scale (NRS). The clinical examination found the pain originated from coccyx. The ganglion impar block test was explained to the patient, done with lidocaine 1 % (5ml) which came positive, so patient planned for PRF of ganglion impar. He was admitted to the operating theater in prone position on the table, with a pillow under the anterior superior iliac spine to flatten the normal lumbar lordosis. First, intravenous access was inserted, and monitors were attached. The midline of the sacrococcygeal area was cleaned with antiseptic and sterile drapes were placed. Lidocaine 1% (5mL) was used for skin infiltration over the coccyx. A 22-gauge RF needle 10cm (Cosman electrode CU TM) with an active tip of 5mm was inserted through the sacrococcygeal disc to the anterior surface of the coccygeal disc, with the guidance of anteroposterior and lateral fluoroscopy view of the sacrum and coccyx. After negative aspiration, the fluoroscopic image was observed as 2mL of nonionic radiocontrast was injected to confirm the good placement of the needle Figure 2. Before applying PRF, sensory and motor tests were checked, which showed a sensory response at 0.35V (50Hz), a motor response below 2Hz. The treatment was maintained for 4min twice when the temperature at the needle tip did not exceed 42C. The total treatment time was 8min. He described the pain as zero on the NRS post procedure. After the procedure, the patient kept under close monitoring to check for any complications. Five months later, patient improved almost 80% and he was asked to describe the pain once more, and it was within two to three points NRS [1-4].
Figure 1: MRI of spine coccyx: degenerative changes of sacrococcygeal junction.

Figure 2: Impar ganglion PRF: trans-sacrococcygeal needle placement with contrast injection.
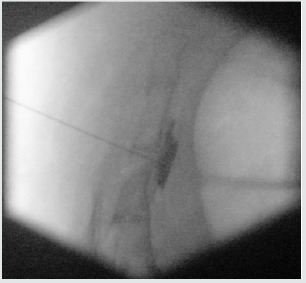
Comment and Discussion
Coccydynia is one of chronic pain syndrome difficult to manage, adversely affects quality of life, and the outcome of conservative methods is very poor. There are trials showed that PRF application is not only effective but also safe for nerve tissue because of its application of 42C. There are also other choices in the relief of coccydynia, such as ablative RF application and coccygectomy. These methods are more invasive and have higher risks of adverse effects compared with PRF application. Pulsed radiofrequency as new alternative practice in chronic pain is not widely used in the management of coccydynia and We believe that the transsacrococcygeal disc approach using PRF for ganglion impar block is not only simple but also effective for the treatment of coccydynia [5-8]
For more Lupine Publishers Open Access Journals Please visit our website:
https://lupinepublishers.us/
For more Global Journal of Anesthesia & Pain Medicine articles Please Click Here:
https://lupinepublishers.com/anesthesia-pain-medicine-journal/index.php
To Know More About Open Access Publishers Click on Lupine Publishers: https://lupinepublishers.com/
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
#Lupine Publisers#Lupine publishers group#open access journals#anaesthesia#anesthesia journals#pain medicine journal#post-operative management#surgery#cardiac anesthesia#cardiothoracic anesthesia#pain management journal
0 notes
Text
Lupine Publishers | Hypertrophic Cardiomiopathy in Children: The Need of Heart Transplantation

Lupine Publishers | Journal of Cardiology & Clinical Research
Abstract
Hypertrophic cardiomyopathy (HCM) is the most common cardiac disease affecting the cardiac muscle. It can manifest in different forms with or without left ventricular outflow obstruction, with or without right ventricle involvement. Forms with biventricular hypertrophy seem to have poor prognosis. In our case, we describe a young patient with sarcomeric biventricular hypertrophic cardiomyopathy (MYH7 mutation), the poor prognosis of this form and strategies options adopted after failure of medical treatment. It is not always easy the management of hypertrophic cardiomiopathy, after medical treatment failure, especially in children. In some cases, heart transplantation is the only one therapeutic option.
Keywords: Hypertrophic Cardiomiopathy; Right Ventricular Hypertrophy; Heart Transplantation
Introduction
Hypertrophic cardiomiopathy (HCM) is the most common cardiac disease affecting the cardiac muscle and is characterized by heterogeneous genetic, morphological, functional, and clinical features. It is also one of the main causes of sudden cardiac death (SDC) in the young. Left ventricular hypertrophy with left ventricular outflow obstruction (LVOTO) is the most characteristic feature of HCM. There are also variant of HCM without LVOTO, with apical hypertrophy, with medio-ventricular obstruction and with right ventricular hypertrophy. The treatment and the prognosis of HCM seem to be variable on the basis of different forms, the age at presentation, sarcomeric gene mutations or rare phenocopies. Heart transplantation (HT) is the only therapeutic option for selected patients with HCM and refractory heart failure. In effect ESC guidelines recommend heart transplantation in eligible patients who have an LVEF < 50% and NYHA functional Class III–IV symptoms despite optimal medical therapy or intractable ventricular arrhythmia (II a); in eligible patients with normal LVEF (50%) and severe drug refractory symptoms (NYHA functional Class III–IV) caused by diastolic dysfunction (II b)[1].
Right ventricular hypertrophy (SRVH) is a relatively rare subtype of HCM. The anatomic, genetic, clinical, and prognostic characteristics of patients with SRVH and the clinical relevance of these characteristics have not been described widely in the literature [2,3]. MYBPC3 gene mutations have previously been described in two patients with RV hypertrophy. In a recent study, 90% of HCM patients with SRVH were found to possess relevant sarcomere protein mutations and variations in the MYH7 (Myosin heavy chain 7) and TTN genes, followed by variations in MYBPC3. Always in this study 73% of HCM patients with SRVH and multiple sarcomere gene mutations had poor prognosis. 7 In addiction MYH7 mutations can cause hypertrophic cardiomyopathy or skeletal myopathies with or without cardiac involvement, on the basis of the side of mutation. In our case, we describe the poor prognosis and treatment strategies of a young patient with biventricular hypertrophic cardiomyopathy and MYH7 mutation.
Case Report
A 12-year-old young woman with familiarity for hypertrophic cardiomyopathy (mother and mother’s twin with biventricular hypertrophic cardiomiopathy and MYH7 mutation) was hospitalized in our hospital for dyspnea after mild-moderate efforts and reduced functional capacity (NYHA Class II). Mother and aunt of the patient were asymptomatic with good functional capacity. Patient had the same genetic mutation of mother and aunt (p.Asn696Ser heterozygosis MYH7) but with increased and poor phenotypic expression [4]. Echocardiography and cardiac magnetic resonance were performed showing a hypertrophic cardiomyopathy with right ventricular involvement. Precisely, cardiovascular imaging showed left ventricle asymmetric hypertrophy especially at the level of anterior and inferior wall (basal and mild anterior wall =14 mm, z score= 3,5; antero-lateral basal wall = 12 mm, z score 2,78; mild inferior wall = 14 mm and apical inferior wall = 12 mm) with normal ejection fraction (FE = 62% at CMR) and moderate diastolic dysfunction (panel B and D). In addiction wall thickness of right ventricle outflow and basal-mild free wall were increased (= 13 mm) with apical obstruction and development of maximum gradient of 10 mmHg (PANEL A and C) [5,6] (Figure 1).
Figure 1.
The function of right ventricle was at inferior limits (FE = 51% at CMR, TAPSE = 16 mm at echocardiography). Thus the patient had an interesting right ventricle involvement and moderate diastolic dysfunction of left ventricle. She had not arrhythmia at ECG-Holter but she had reduced functional capacity. also demonstrated at stress test. Stress test was suspended at 6 min (Bruce Protocol) after pre-syncopal symptoms: lack of adaptation of the blood pressure to the effort was observed. In addition, from several months she had pre-syncopal episodes at the peak of the effort. ECG showed left ventricular hypertrophy and biatrial enlargement. Pro BNP was increased = 5841 pg/ml. Considering clinical situation, we decided to start medical treatment with betablockers (bisoprolol) but the patient didn’t tolerate medical treatment. Thus, we decided to start low dose of captopril without improvement of symptomatology. Also, treatment with diuretic was not tolerate by patient [7,8]. Therefore, considering symptom refractory to medical therapy, the poor prognosis and the impossibility to optimize medical treatment, we decided to plan cardiac transplantation, the only option possible at this moment.
Thus right catheterization was performed and patient was inserted in heart transplantation list. ICD implantation was not considered in the absence of ventricular arrhythmia and other factors. Discussion: hypertrophic cardiomyopathy associated with MYH7 mutation and right ventricle involvement seems to have poor prognosis, especially if right ventricle hypertrophy is severe [9]. In effect the young patient had a greater right ventricular hypertrophy compared than mother and aunt. In these cases, after medical treatment failure, heart transplantation seems to be the only strategy to improve symptomatology and quality of the life of the patient. Especially in pediatric population, it is not always easy the management of hypertrophic cardiomiopathy after medical treatment failure and heart transplantation seems to be the only one therapeutic option. Other study are needed to study some variants of HCM with right ventricle hypertrophy, their treatment and prognosis.
For more Cardiovascular Research go through the below link
https://lupinepublishers.com/cardiology-journal/index.php
To Know More About Open Access Publishers Please Click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
34 notes
·
View notes
Video
youtube
Lupine Publishers - A Unique Challenge: Laparoscopic Management of anAde…
https://www.youtube.com/watch?v=N3m0MtAbmaU&feature=youtu.be
34 notes
·
View notes
Text
Lupine Publishers | Lupine publishers | Modern Tools and Techniques for Diagnosis and Prognosis of Salt Affected Soils and Poor- Quality Waters
Lupine Publishers |Agriculture Open Access Journal
Introduction
Soil salinity and brackish ground water are primary concerns for reduced productivity in the arid and semiarid regions of the World covering 953 million ha of land [1]. In India, it occupied 2% of the TGA and is distributed in fifteen states that covered Genetic plain, central arid and semiarid regions, southern peninsular plain and coastal areas [2]. Transportation and deposition of salts at the lower topographic zones are primary processes controlling genesis and distribution of salty soils in the Genetic plain besides high evaporation in arid zone, salty parent materials and brackish ground use in peninsular plain and inundation of saline sea water in coastal areas are other soil salinization processes [3]. Factors of anthropogenic origin include the use of salty ground water and canal water for irrigation in poorly drained soils of arid and semiarid regions that caused the emergences of water logging, salinization and losses of soil/crop productivity [4,5].
Traditional methods of soil survey using aerial photographs and soil profile studies require enough time and manpower for soil characterization which is limited to small areas. Temporal dynamics of salts is also an important issue which is usually unaddressed in soil survey studies. Indian Remote Sensing Technology (Resources at I&II) with improved spatial and spectral resolutions have facilitated the diagnosis of salt affected soils in less time and cost effective manner with limited resources. For delineation and characterization of salt affected soils on a reconnaissance scale, a methodology was developed integrating remote sensing data with ground truth and soil studies [6]. Legends were developed to address nature, characteristics and extent of saline and sodic soils for land reclamation & management. Prognostic studies on soil salinity were also conducted using high resolution remote sensing data (SPOT, MODIS etc.) in Western Yamuna, Bhakra and Sir hind (Haryana and Punjab states); IGNP (Rajasthan state), Sharda Sahayak (Uttar Pradesh state), Ukiah Kakarpar (Gujarat state), Upper Krishna (Karnataka state) and Gandak (Bihar state) canal command areas of India to quantify soil salinization processes integrating topography, soil texture, hydrology and sub-surface soil and aquifer characteristics Spatial variability of salts was studied at farm scale in the Shivari (at Lucknow, Uttar Pradesh state) and Nain (at Panipat, Haryana state) experimental farms of ICAR-CSSRI, representing sodic soils of the Middle- and saline soil and salty groundwater in the Trans-Gang tic plains of India [7,8].
Interpretation of IRS data facilitated the identification strongly salt affected soils by the white to yellowish white tones and high spectral contrast of salt crusts from barren surfaces. Based on the dark blue/black to grey tones in the infrared range (SWIR), the waterlogged soils were clearly identified in canal irrigated areas showing stagnated water at soil surface with poor natural drainage. High reflectance from dry salts during June and freshly precipitated moist salts during March and October enabled the detection of sodic soils and areas with sodic (with high RSC, Residual Sodium Carbonate, and SAR, Sodium Adsorption Ratio) ground water [9]. Contrarily sodic soils with normal ground water showed mixed red and spotted while signatures and high NDVI values for crops with good vegetative covers. Moderately and slightly sodic soils showed mixed spectral signatures for salt crusts, moderate cropping density and surface wetness and is authenticated by ground truth study. The dark red tones of healthy vegetation and high NDVI values are found for normal cropped areas. Differential absorption from seasonal water logging and surface ponding were established in the infrared regions (SWIR) with higher accuracy [8]. Combination of red and infra red bands helped in segregating saline and sodic soils located in different geographic regions (Singh and Mandal 2007). Integration of thermal band interpretation helped in segregating salty areas and sand dunes [10].
Sodic soil profiles indicated prominent natric horizon with clay illuviation, iron and manganese mottles with higher moisture content and calcareous materials at sub-surface depths. Soils showing high PHS, ESP and SAR values and the dominance of carbonate and bicarbonates of sodium in the saturation extract indicated sodic nature [11]. High moisture content in soil profiles, salt accumulation at the root zone and salt dynamics in wet and dry cycles are common features of waterlogged (surface ponding), high water table depth (potential water logging) and seasonal water logging in the canal irrigated areas respectively [12]. Continuous use of salty ground water for irrigation in arid and semiarid regions caused salt enrichment in soil profiles. Periodic inundations of saline sea water in coastal fringes, and the use of salty water for fisheries development projects have abandoned large areas of good agricultural lands out of cultivation. Water samples with high pH and SAR values and at places high RC are typical qualities of water in arid and semiarid regions [13]. Water logging, high clay contents, smectite clay minerals and poor to very poor (sporadic) cropping density and ground water quality are some of the constraints in the peninsular plain, causing difficulty in the detection and delineation of salt affected soils [5]. Black soils of Peninsular (F) region were classified as sodic, as soil ESP (Exchangeable Sodium Percent>5) is becomes critical at this stage. For management purposes, the complex saline-sodic soils of A (alluvial), B(aeofluvial/arid) and H(others) are classed as sodic. Due to high salt enrichment in soil profiles, typical soils in coastal (D), deltaic© and mud flats mangrove swamps (G) were classified as saline. Benchmark salt affected soils were also identified to support monitoring and management of salt affected soils [14] distributed in fifteen agroclimatic and seven physiographic regions in India (CSSRI 2002- 2005). Interactive databases with climate and geology revealed largest areas (67%) in the 300-1000 mm rainfall, followed by 75% in the strong hypothermic (25-27.5oC) temperature zones and 39% in the Pleistocene and recent geological formations [15]. Recent IRS data [16] revealed distribution of salt affected soils (315617 ha) in 18 districts of Haryana state that showed an increase in areas under saline soils to 145054 ha and decrease of sodic soils to 170563 ha, apparently due to soil salinization in irrigated areas and sodic land reclamations (CSSRI 2017-18). Attempts were also taken to update sodic soil database in Uttar Pradesh and areas of saline soils in Gujarat state [17-21].
For more Lupine Publishers Open Access Journals Please visit our website:
https://lupinepublishersgroup.com/
For more Agriculture Open Access Journal articles Please Click
Here: https://www.lupinepublishers.com/agriculture-journal/
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
44 notes
·
View notes
Text
Lupine Publishers | The Dynamics of Mounds-Clusters in the Mouhoun Bend (Burkina Faso)

Lupine Publishers- Anthropological and Archaeological Sciences Journal Impact Factor
Abstract
Mounds are human made accumulations of settlements debris of varying size and shapes, found in different parts of the world. In West Africa, they tend to be located in relatively flat lands, at low elevations, in wetlands, marshlands or flood plains. Some are large single mound sites. Others are made of groups of scattered or clustered mounds – mound-clusters -, spread over varying surface extent. The dynamics of such settlement systems is still poorly understood partly because of inadequate field methodology. Ethno-historical and ethnographic data from West Africa recent past are relied upon to suggest some of the key processes behind mounds clustering: ethnicity, craft affiliations, or a combination of both. The Mouhoun Bend Archaeological Project (MOBAP 1997- 2000) was designed to address this issue. The field methodology was articulated on testing all mounds parts of the mound-clusters under investigation. Two mound-clustering strategies were identified:
a. Tight-clustering resulting in the formation of a large “single mound site”, and
b. Loose-clustering with scattered individual mounds of different size and shape.
Residential and craft requirements combined differentially in the 2000 years Mouhoun Bend settlement history, have generated the settlement patterns investigated in the study area. The ethnicity component of the identified dynamics – that is plausible – could not be tracked with the current methodology and is accordingly undecidable.
Introduction
The Mouhoun bend was settled by iron-using communities in the first millennium BCE (Figure 1, Table 1). The climate was wetter [1]. The Sudanian savanna and the Mouhoun River offered a diversified resources mix that allowed for the stabilization and growth of these mixed farming fishing populations. Their settlements consisted of multi-mound complexes – moundclusters. The sample of sites excavated within the Mouhoun Bend Archaeological Project (MOBAP 1997 – 2000) offers an entry into the dynamics of this kind of settlement that developed and spread in the study area for a little more than 2000 years, from ca. 700/500 BCE to 1650 CE (Figure 1, Table 1).
Table 1: Radiocarbon dates from the Mouhoun Bend Archaeological Project.
Key: LLNL = Lawrence Livermore National Laboratory:
* Radiocarbon dates from iron objects processed by Dr. Andrea C. Cook at Lawrence Livermore National Laboratory, UC Berkeley.
*1 = from an iron ring
*2 = from a small iron spear
*3 = from a large iron spear
Mounds result from the piling up on the same spot of human occupation by-products. They include habitation features, craft installations, collapsed building material as well as discarded and abandoned material culture. They are therefore exclusively human-made and, depending on circumstances, can be either well preserved or significantly disturbed by erosion agencies. These formation processes that combine cultural (C-transforms) and natural (N-transforms) are well understood in general [2,3].
Habitation mounds dating from the Late Stone Age onwards are recorded in different parts of West Africa, from the Chadian basin to Mali and Guinea [4-18]. They consist either of a single small or large mound or of multiple mounds (mound-cluster). It has been suggested that mound-clusters may have derived from residential segregation, inhabited by different specialized more or less endogamic groups such as blacksmiths, potters, hunters, fishing folks, bards, etc. [19,20]. Distinct mounds are thus axiomatically considered to materialize residential segregation, and as such, are the signature of craft-specialization. The explanation is tautological. No excavation program was implemented to test the accuracy the hypothesis mentioned above. The testing procedure may have required an appropriate methodology, consisting at least of the probing of all the mounds part of the settlement complex under investigation, a precise and fine-grained chronology backing detailed analyses of material culture, architecture, and subsistence remains. It is then and only then that variation – or lack thereof – can be assigned to differences in social status. These principles have guided the field strategy implemented in the Mouhoun Bend Archaeological Project [21,22].
The Mouhoun River flows from the SW to NE, winds its course in a U-shape bend to follow a N-S direction (Figure 1). The study area located in the Sudano-sahelian zone is delimited in the north and northeast by the meandering river course. It measures 40km East-West (3o 11’ North / 3o 32’ East) and 38km North-South (12o 30’/ 12o 45’ latitude North). The land, prone to cyclical droughts, is flat with elevation ranging from 294 to 249m above sea level. The vegetation is characteristically a highly anthropic wooded savanna, with the protected shea-butter tree (Butyrospermum parkii) largely predominant, followed by different kinds of Acacia sp.
Figure 1: Distribution of archaeological sites in the Mouhoun Bend (Burkina Faso).
Three mound-clusters located in in different environments were selected for excavation: Diekono in the Mouhoun River floodplain, Kerebe-Sira-Tomo (KST) on the cliff delimiting the river valley, and Tora-Sira-Tomo (TST) and its satellite Gnambakouon-Sira- Tomo (GST) on the topographic rise in the central part of the study area. Each of the above mentioned sites is comprised of a number of mounds of different size and shape, iron-working workshops, and laterite quarries.
The Dynamics of TST and KST Mound-clusters
The long-term pattern of growth of inhabited space within a mound cannot be assessed with the field methodology implemented in this case, with one test unit per mound. A general time line of the settlement complex formation can nonetheless be reconstructed.
TST settlement complex (12o 35’ 07” N and 3o 22’ 07” E) is located at 280m asl. With 17 distinct mounds, it is the largest settlement complex of the study area, spread over 900m westeast and 500m north-south, some 45ha in total surface extent (Figure 2). TST-3, the largest mound stretched along the north edge measures 260m west-east, and 120m north-south. All 17 mounds were tested after three field seasons (1997, 1999, and 2000). Five, TST-1 (Iron smelting), TST-2 (quarry), TST-4 (cloth weaving and dyeing workshop), TST-9 (cemetery), and TST-17 (oil production workshop), are special purpose sites. The fourteen remaining ones were standard habitation mounds with varying occupation intensity
Figure 2: Tora-Sira-Tomo settlement complex.
KST settlement complex is located on the cliff top along the edge of the Mouhoun River valley (Figure 3). The complex consists of eleven more or less distinct mounds stretched on 350m westeast and 600m north-south. The cluster is made of three distinct sites categories: a quarry (KST-2) located at some 800m east, iron-working stations both smelting and forging, and habitation mounds. Habitations mounds, clustered in the north, resulted in the formation of a large 15ha village site. All iron-working stations, arranged along a roughly ENE-WSW axis, are concentrated at 100 to 200m along the south flank of the main habitation cluster. KST settlement complex was inhabited from the second half of the first millennium BC to the second half of the thirteenth-century AD, with an important 500 years occupation hiatus in the second half of the 1st millennium AD. The development of TST and KST settlement complexes can be arranged in four successive phases, from the middle of the first millennium BC to the middle of the second millennium AD.
Figure 3: The evolution of TST settlement complex.
Phase I (650 BC-800 AD)
At TST, the initial settlement phase (650 BC-800 AD) that started in the mid-1st millennium BC is documented at TST-1, TST-2, and TST-3-East (Figure 4, Table 2). The earliest occupations are found at TST-1, an iron-smelting site dated to 650-395 BC (Figure 5), TST-2, the quarry site that provided raw material for house construction and iron production, and finally, the blacksmith workshop exposed at the bottom of TST-3-East probe.
Figure 4: View of TST-1 iron smelting furnace.
Figure 5: Differential mounds size in m2 during TST phase IV (1400 – 1650 CE).
Table 2: Tora-Sira-Tomo mound cluster at Phase I (650 BC – 800 AD).
KST settlement complex phase I dated to 350 BC-150 AD was shorter. It is documented in the west-central part of the complex, in KST-1A and KST-2 the quarry site (Figure 6). KST complex grew in two directions during its phase II dated to 250 – 550 AD. KST- 1B and KST-3 areas were settled. The mound was of an irregular potato- shape, oriented SW-NE. KST-2, the quarry site, was relied upon for the supply of iron ore and construction material during the whole existence of the settlement complex
Figure 6: Kerebe-Sira-Tomo settlement complex.
Phase II (800 – 1100 AD)
TST Phase II (800-1100 CE) settlement with a total of 8 mounds, witnessed the foundation of 5 new sites. They were arranged in two sub-clusters of four sites each: TST-1, TST-2, TST-3, and TST-6 in the west, and TST-4, TST-12, TST-13, and TST-15 in the east (Figure 4, Table 3). The western sub-cluster consisted of two residential mounds: TST-3 and TST-6, and two special purpose sites: TST- 1(iron-smelting and ritual) and TST-2 (quarry). The eastern subcluster includes TST-13 and TST-15 residential sites, and TST-4 (weaving and cloth dyeing workshop) and TST-12 (a blacksmith workshop) special purpose sites (Holl 2014). KST complex was abandoned during all the second half of the 1st millennium AD, from ca. 550 to 1000 AD.
Table 3: Tora-Sira-Tomo mound cluster in Phase II (800 – 1100 AD).
Phase III (1100 – 1400 AD)
TST settlement complex reached its maximum extent during phase III (1100-1400 AD) with the addition of 7 new sites. All 15 mounds (Figure 4 & 7, Table 4) were located in the space delineated during phase I and II. The new additions are set in two patterns. TST-5, TST-7, TST-8, and TST-10 present a rectilinear arrangement of equidistant mounds at 100m from one to the next. TST-5, TST- 7, and TST-8 residential mounds ‘sits’ on burials dug deep in the laterite crust in what may have been an earlier cemetery. TST-14, TST-16, and TST-17 are along the northeastern flank of the complex, at 100m from one to the next, in a linear east-west arrangement. TST-14 and TST-16, were residential and TST-17 a karité oil production workshop.
Table 4: Tora-Sira-Tomo mound cluster in Phase III (1100 – 1400 AD).
Figure 7: The evolution of KST settlement complex.
KST complex also witnessed an accelerated growth during Phase III (1000-1250). KST-IA and 1B, KST-2 (quarry site), KST-3, KST-4 (occupation I and II), KST-5, and KST-6 (Figure 6) were all inhabited and in use. Fire destroyed habitation units from KST-3 occupation I and KST-4 occupation II (Figure 8 & 9), located along the southeast flank of the complex. There was also a significant intensification of iron-working, with the foundation of workshops devoted to iron-smelting, blow-pipes making, and blacksmithing along the south margins of the main village.
Phase IV (1400 -1650 AD)
TST settlement complex shrunk significantly during Phase IV (1400-1650 AD). The number of inhabited sites dropped from 15 to 9. The eastern part of the cluster was abandoned (Table 5, Figure 4). A new restricted access cemetery was founded at TST-9. TST-3, TST-4, TST-5, TST-6, TST-7, and TST-8, were residential. TST-1, TST- 2, and TST-9, respectively iron-smelting site, quarry, and cemetery, were special purpose sites. In general, with the exception of TST- 8 set between TST-4 and TST-7 (Figure 4), the distance between neighboring mounds oscillates around 100m.
An identical phenomenon occurred at KST. The inhabited space also shrunk considerably during KST phase IV (1250-1450 AD) (Figure 6). Shallow occupation evidence is documented at KST-4 occupation III and IV, then used as a cemetery.
Figure 8: Partial view of KST phase III domestic unit.
Figure 9: Habitation complexes from Phase III KST-4 .
Table 5: Tora-Sira-Tomo mound cluster in Phase IV (1400 – 1650 AD).
Variability of mounds clustering processes
Data collected from the excavation of four settlement complexes point to the existence of two main mound-clustering strategies: a tight and a loose one. KST settlement complex that lasted from ca. 350 BC to 1450 AD, with a half millennium occupation hiatus in the second half of the 1st millennium AD, features tight-clustering (Figure 7 & 8). All the residential sites, with the exception of KST- 4, are tightly packed in a 15ha village. Iron-working sites located along the south periphery of the village display no habitation. Craft people and work crews were KST villagers who commuted to their workshops during the iron-production seasons.
TST-GST settlement complex with a total of 20 mounds features the loose-clustering strategy. The mound-sites, 17 for TST and 3 for GST are well demarcated, with each sub-set presenting a large dominant mound. Residential and special purpose sites are represented in varying combinations all along TST settlement complex occupation history.
Archaeological data indicate that flexible strategies were adopted by the different ‘self-sustaining’ autonomous ancient villages during the 2200 years’ occupation of the Mouhoun bend. In KST, craft people resided in the village and commuted to their workshops located in the southern outskirts of the complex. In the TST alternative, with more or less inter-phase variations, craft people built their residence in distinct places and supplied local communities from their workshops. There is no fixed and permanent pattern of residential and occupational segregation in the analyzed archaeological record [21,22].
Peer-village interaction
The study area is relatively flat. The recorded settlement complexes are more or less evenly distributed in the landscape. In site-catchment analysis terms, each village is surrounded by rings of cultivated fields, fallow zones, and bush [23,24]. At their peak, during the first centuries of the 2nd millennium AD, each of the recorded settlement complex was a large autonomous and selfsustaining village. Some, like KST and Kirikongo, were compact villages with a few outlying mounds and special purpose sites. Others, as was the case for TST – GST and Diekono, were spread out with a multiplicity of distinct mounds.
There are no significant wealth differences. Grave-goods and burial offerings are too marginal to be significant. Some individuals, male, female, children, and infants, were nonetheless buried in “restricted access” cemeteries while others were buried in their compounds. This differential treatment points to subtle variations in social status without detectable and/or durable material correlates. The accelerated growth at the beginning of the 2nd millennium AD initiated a scramble for land, villages rivalry, violence, and wars.
Fire: accidents or wars?
Burnt houses were recorded in some of the excavated mounds. It is the case at TST-3-West in occupation I and II, dated to 1000- 1150 AD. Domestic installations belonging to two successive occupations were totally burnt down. KST complex also present two instances of burnt domestic installations dated to 1050 – 1380 AD: one at KST-3 occupation I and the other at KST-4 occupation II. In the latter case, a whole household complex with its food supply was destroyed by fire (Figure 9). Similar cases of burnt installations dated to 1300-1450 AD were recorded at Kirikongo, Mound III, level 8 and Mound IV, level 7 [8]. These events took place during a period of accelerated growth that triggered violent confrontations.
War, Violence and surgery
There is no direct one to one correlation but the unrest indicated by burnt houses is partly corroborated by traumatic injuries found on some of the deceased. Two male and female adult individuals buried in the same context at TST-7 appears to have been victims of the same violent encounter. One, a 35-50 years old adult female presents 4 well healed cranial fractures on the occipital, frontal, and left parietal. The other, an impressive 1.95m tall 45+ years old male presents two distinct episodes of trauma. He recovered from previous blows indicated by a well healed circular defect on the occipital. He has multiple trephinations with no signs of healing on the right, left parietals and frontal, showing that the second series of blows was fatal. Remarkably, both adults present similar blows patterns: they were hit on the frontal, occipital, left and right parietals, as if the aggressors were well trained fighters [25-27]. The surgery may have taken place after a violent raid. Finally, a 9-11 years old pre-adolescent, individual 18 from phase IV TST- 9 cemetery, presents multiple peri-mortem depressed cranial features made by a sharp object, that was very likely the cause of death [26].
The recorded evidence on traumatic injuries is dated to phase III (1000-1200 AD) and IV (1250-1500 AD) when the area witnessed a significant growth acceleration followed by the onset of devolution. There are convincing evidence of conflict and intervillage warfare during the first half of the second millennium AD. The nature and characteristics of the kind of warfare that may have developed in the area during this phase of accelerated growth are difficult to decipher. The tactics involved may have consisted of surprise raiding and counter-raiding with the aim of seizing supplies and host [27-37].
Conclusion
Each village had its autonomous system of government, with horizontally differentiated groups. These mixed farming communities included a number of craft specialists, potters, ironsmelters and blacksmiths, masons, cloths weavers and dyers, karite-oil producers, as well as part-time warriors, and healers (surgeons). The Mouhoun Bend peer-villages were autonomous and self-sustaining but not autarkic. A general compatibility of “worldviews” is suggested by the strong coherence of mortuary practices. Despite variations, pottery decoration techniques and syntax suggest a shared cultural universe. The mound-dwellers of the Mouhoun Bend developed an original socio-political system that, for approximately two centuries, from 1200 to 1400 AD, existed on the periphery of the powerful expansionist Mali Empire.
For More Lupine Publishers Open Access Journals Please visit our Website:
https://lupinepublishers.us/
For More Anthropological and Archaeological Sciences Articles Please Click Here: https://lupinepublishers.com/anthropological-and-archaeological-sciences/
To Know More About Open Access Publishers Please Click on Lupine Publishers
Follow on LinkedIn: https://www.linkedin.com/company/lupinepublishers
Follow on Twitter: https://twitter.com/lupine_online
49 notes
·
View notes
Text
Mini OPCAB Coronary Artery Bypass Surgery Plus Medical Treatment: An Option for High Risk Coronary Patients| Lupine Publishers
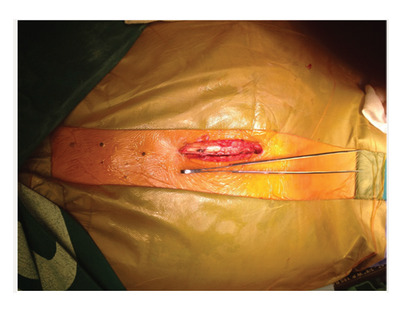
Journal of Surgery| Lupine Publishers
Abstract
MINI OPCAB surgery (Xiphoid Approach) is a surgical technique in which the left internal mammary artery is bypassed to the Anterior Descending Artery (ADA) by a medial inferior sternotomy Fourteen high risk patients with multiple coronary disease with a preoperative logistic Euroscore of 10.86 were operated and follow up with medical treatment and strictly control of risks factors MACE at 80 months was 0% and Survival at 7 years 82% (KM) Although is an alternative the combination of Mini OPCAB operation plus medical treatment in high risk. Patients with multiple vessels coronary disease, more experience is needed to confirm this initials results. Statistical analysis applied the student test (SPSS program), with p<0.05 were considered significant
Keywords: Mini Opcab; Minimally Invasive Coronary Surgery; Coronary High Risk Patients
Introduction
In high-risk patients with multiple vessel disease who are not candidates for conventional surgery with extracorporeal circulation or for percutaneous procedures as a single treatment, the alternative of left mammary artery to left internal descending artery bypass graft surgery without extracorporeal circulation offers advantages over medical treatment [1,2].
Figure 1:
Figure 2:
a) The MIDCAB operation
b) Is effective to treat high risk patients with multiple vessel disease. Greater long-term follow-up is necessary to clarify the indications and validate the procedure for this type of patients.
c) MINI OPCAB surgery (Xiphoid Approach) is a surgical technique in which the left internal mammary artery is bypassed to the Anterior Descending Artery (ADA) by a medial inferior sternotomy approach in the 3rd or 4th intercostal space, leaving intact the sternal manubrium (Figures 1 & 2). Long-term results have already been published, reaching 82% survival at 12 years (Kaplan-Meier).
d) This presentation describes the experience with this surgical technique in our institution [3,4].
Materials and Methods
Fourteen high risk patients with multiple vessel coronary artery disease with mean age of 71.07 years (±9.051, 95% CI), 21% women and mean preoperative Logistic EuroSCORE of 10.68 (±5.407, 95% CI), were operated-on in the last 7 years, followed up in our institution with strict medical treatment and control of risk factors.
Result
Operative mortality in this series was 0%, the incidence of perioperative infarction was 0%, the average duration of surgery was 2 hours and 20 minutes; 10 (71%) patients were extubated in the operating room and average hospital stay was 2 days and 11 hours. Following the intervention, one patient received a stent in the right coronary artery and another in the circumflex artery for presenting large arteries with severe lesions. In this group of patients, major adverse cardiovascular events were 0% at 80 months. Survival rate was 82% at 7 years (Kaplan-Meier); an 85-year-old woman died 5 years after surgery due to stroke.
Conclusion
The combination of a MINI-OPCAB surgery for bypass of the left internal mammary artery to the left anterior descending artery [5,6] together with an adequate medical treatment and a hybrid treatment when the right coronary artery or circumflex artery are of high caliber, is a viable option for elderly and high-risk patients. More experience is needed to confirm these initial results.
For more information about our Journal click on Surgery Journal
https://lupinepublishers.com/surgery-case-studies-journal/
To know more about Lupine Publishers Click on https://lupinepublishers.us/
For more Open access publishers click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
25 notes
·
View notes
Text
Lupine Publishers |Scientific Student Societies: A Way of Scientific Research Vocations Boosting
Lupine Publishers| Journal of Surgery
Abstract
Born in Russia at the end of the XIXth century the Scientific Student Societies have developed a rather original way of initiation and involvement of the young in the scientific research during High School and University cursus. All through the XXth century and up to now, they have given several generations of Russian scientists an adequate pre formation consisting not only of skill acquisition in their future speciality but also in planning, realization and organization of scientific research and sharing of its results. Their popularity was also due to the high degree of initiative and autonomy left to the students.
Introduction
In our days, when most of young people with a diploma of physician are no more inspired by a scientific career possibility, and though Occidental World has general negative opinion about Russia and its institutions, it is not forbidden to exhume some moments which have proved efficacy and may be useful for.com now. Such an interesting institution (from my point of view) was the Scientific Student Societies (SSS) [1], existing in all the High Schools and Universities, but may be especially activated in Medicine Faculties. They were created in the end of XIXth century by famous scientists such as VI Vernadski (Figure1) and his colleagues in Sankt Petersburg (1882) and in the beginning of the XXth century by NE Jukovski (Figure 2) in Moscow (1909) [1-4]. In the 30-ies they were reactivated and widespread through all the country. After the 2nd World War, SSS were also working in the other countries of the “East Bloc”. The links and experience exchanges were current between them (International meetings and conferences, scientific information share, student exchanges and so on). Presently in the XXIth century they have not disappeared: “NIRS” - student scientific research work - remains a preoccupation of the academic staff in Universities and High Schools as well as different Ministries of the Russian Federation. Student scientific associations still exist, may be a little modified, sometimes independently as “Meridian”, “Luch” (that means ray or beam). Books including scientific articles written by students are still published [5-7], regional and national competitions are organized.
Description and Commentaries
The SSS aims were: to popularize scientific research among students, to find out the most talented among them and to help them to develop towards an eventual scientific career. It was also a mean for students to acquire deeper knowledge in one or several disciplines and to choose their future speciality. The Student Scientific Circles eventually provided the departments with qualified helpers, as a just return for the teaching staff mobilisation during the young researcher’s formation. The structure schema of the SSS is presented in Figure 3. At the basis level was the Circle. As soon as they wanted, students were invited to join a student scientific circle by the department of their choice and to begin their initiation according to their trends with one of the assistant or docent. At this level, the students learned step by step how to manage scientific literature, to review it, to deepen their knowledge’s in the chosen subject, to acquire technical skills and, last but not least, to participate to the research of their mentor/supervisor, or even to start their own investigations on their personal research topic.*NB. The work performed within the SSS activity differed from end of cycle obligatory works, but the members of SSS were allowed to include their personal data in the end of cycle work, if it was adequate. The students - members of a circle - elected their president - responsible who organized periodic reunions for reviewing the work performed by the circle members. During these meetings experienced assistants and docents or professors were invited to present lectures or demonstrations helping the students to assess the peculiarities and the research specifics of the discipline (Figure 4). The best student ‘works were selected and recommended for reporting at Faculty and inter Faculties student scientific conferences.
The next level was Faculty and University or High School Scientific Student Society. The department circles joined forming faculty and institute Student Scientific Societies (SSS), which were gathered as University or High School SSS. They were handed by students and only supervised by a responsible chosen among docents and professors of the Faculty. Students elected their president and delegates for contacts with other faculties, institutes of the country and of foreign countries. They organized faculty conferences, Inter-faculty scientific sessions. Their activity was financed either by the Professional Union of their School or by the University budget. The most promising students - members of SSS were further recommended for scientific work either in the department where they started their work, or in Scientific Research Institutes and other High School Faculties (according to the young specialist’s will and the possibilities of the aforementioned institutions). The Ministries took into account the SSS activity of the young specialist when his future was considered after the end of his cursus. Besides career start consideration, other awards were current: scientific books, scientific travels, being the co-author of a “chief’s paper, and so on. So the students made acquaintance not only with the individual searching process itself (Figure 5), but also with elements of organizing scientific research, co-operative investigation, discussion and peer evaluation of its results both by other students and by the Faculty staff scientists. Students also learned to communicate at different levels and, if they wanted, to prepare themselves to a scientific career. If not, nevertheless the aptitudes obtained during their work in the SSS was precious for their further professional activity: acquaintance with special literature research methods, reviewing and critics of scientific publications, acquisition of some technical skills, capacity to plan scientific research and organize scientific meetings.
It is estimated that about 20% of the students attended the SSS. Among them about 30% have presented a valuable work (compilation, fundamental or applied research). Most of the exmembers of SSS have pursued a career in the previously chosen specialty. In Russia, all through the years 1930-1990 and up to now most of those who have followed a successful scientific or pedagogic career, were ancient members of the SSS. (That does not mean that without SSS a scientific career was not possible). Many of the students, even foreigner hosts, who have passed through this “school” have been later eminent scientists of their countries (for instance: Academician VI Shumakov - the first Director of the Transplantation Institute in Moscow, Professor VM Filipov - present Rector of the Russian University od People Friendship; Professor R Roman Ramos - Dean of the Medicine Faculty of the Mexico Autonomous University)
Conclusion
The SSS have given several generations of motivated Russian scientists an adequate pre formation consisting not only of skill acquisition in their future speciality (especially precious in surgical disciplines) but also in planning, realization and organization of scientific research and share of its results. This was capital for a developing country and remains important nowadays. The large autonomy and initiative given to the students in the SSS has certainly contributed to their popularity and success. This experience ought to be adapted to the conditions of our present society development and could enhance individual initiative and motivation, as well as collective research organization. It ought to be included into Faculties staff task and financing.
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
30 notes
·
View notes
Text
Lupine Publishers | Model Development for Life Cycle Assessment of Rice Yellow Stem Borer under Rising Temperature Scenarios
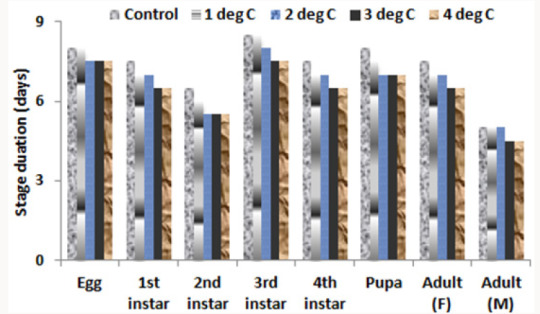
Lupine Publishers | Agriculture Open Access Journal
Abstract
A simple model was developed using Fortran Simulation Translator to study the influence of increased temperature on duration of various life cycle phases of yellow stem borer (YSB) in Bangladesh environment. Model was primarily based on Growing Degree Day concept, by also including cardinal temperatures sensitive for specific growing stages of YSB. After successful calibration and validation of the model, it was taken for climate change (only temperature rise considered in the present study) impact analysis on the growing cycle of YSB. Temperature increase values of 1, 2, 3 and 4 oC were considered and compared with the Control (no temperature rise), by using historic weather of representative locations in eight Divisions of Bangladesh. Differential spatial response in the life cycle of YSB under various temperature rise treatments was noticed, and in general the growing cycle hastened with the rising temperature. The life cycle of YSB is likely to be reduced by about 2 days for every degree celcius rise in temperature, while averaged over locations. This means that there will be 2.0-2.5 additional generations of YSB in pre-monsoon season about 2.9-3.2 in wet season of Bangladesh. There is a need to include the phenology module developed in subsequent design of population dynamics model for YSB.
Keywords: Model; Growing degree days; Yellow stem borer; Life cycle assessment; Temperature rise
Introduction
Yellow stem borer (YSB) is the most destructive and widely distributed insect-pest of rice. It causes dead heart or white head, depending on infestation time and significantly reduces rice yields by 5-10% and even up to 60% under localized outbreak conditions [1]. It can grow in places having temperature >12 oC and annual rainfall around 1000mm. Generally, temperature and high relative humidity (RH) in the evening favors stem borer growth and development [2]. The female moth oviposits from 1900 to 2200hr in summer, 1800 to 2000 hr in spring and autumn, and deposits one egg mass in a night and up to five nights after emergence. Optimum temperature is 29 oC having 90% RH for maximum number of eggs deposition. Optimum temperature for egg hatching is 24-29 oC with 90-100% RH. Larvae die at 35 oC and hatching is severely reduced when RH goes to below 70% [1]. Larvae can�t molt at 12 oC or below and they die. The last instar larvae can survive unfavorable growth condition as diapauses, which is broken by rainfall or flooding. In multiple rice cropping, no diapauses takes place. The pupal period can last for 9-12 days and the threshold temperature for its development is 15-16oC.
The number of generations in a year depends on temperature, rainfall and the availability of host [1]. The occurrence of the pest is generally the highest in wet season [3]. Since there are many stem borer species, the average life cycle of rice stem borers varies from 42-83 days [4], depending on growing conditions. This implies that heterogeneous population can be found in the same rice field. Manikandan [5] also reported that development time by different phases of YSB decreases with higher temperature and thus increased population likely in future at early growth stages of rice crop. However, no such data is available in Bangladesh. Keeping the acute problem of YSB in Bangladesh, the present study was undertaken to develop a simple phenology-based) model to assess the life cycle of YSB in two major growing seasons of rice and subsequent taking it to evaluate the effect of rising temperature on growth cycle of rice yellow stem borer in representative locations of eight Divisions of Bangladesh.
Materials and Methods
Model description
Model for assessing the phenology of yellow stem borer was written in Fortran Simulation Translator and the compiler used is FSTWin 4.12 [6]. This model will subsequently be used to develop population dynamics model for YSB in rice-based cropping systems prevalent in Bangladesh. Growing degree days (GDD) concept was used for this purpose, with base temperature assumed as 15 degree Celsius, below which growth and development activity in the life cycle of YSB does not take place. Each day, average temperature (mean of maximum and minimum temperatures) minus the base temperature is integrated over the growing cycle, and subsequently the development stage is achieved when critical value for attainment of a particular stage is crossed.
In the INITIAL phase, the GDD is taken as zero, which is read one time during running of the model
INCON GDDI, initial value of GDD = 0.
In the DYNAMIC phase, the program is executed daily till the FINISH Condition is achieved.
DAS, days after start of simulation = INTGRL (ZERO, RDAS)
PARAM RDAS, day increment rate = 1.
The development stage can be expressed in development stage (0-1), but in the present study not used for development stage identification, which we will use in further design of population dynamics model in coming times.
DVS, development stage = INTGRL (ZERO, DVR)
DVR, rate of development stage increase, Arbitrary Function Generator- a well defined FST function=AFGEN (DVRT, DAVTMP)
Since the age of male is relatively lower than the age of the female, so the computation is done separately as indicated below:
*FOR FEMALE
FUNCTION DVRT = -10.,0., 0.,0.,15.,0.,35.,0.03325,40.,0.0415
*FOR MALE
FUNCTION DVRT = -10.,0., 0.,0.,15.,0.,35.,0.0342,40.,0.0426
Base temperature below which the activities do not take place, degree celcius, is given as under:
PARAM TBASE=15.
Reading of weather data, on daily time step, is read through external file, as per well defined format for FST compiler, as given below:
WEATHER WTRDIR=‘c:\WEATHER';CNTR=’ GAZI’;ISTN=1;IYEAR= 200
Where, various climatic elements are used as below:
RDD is solar radiation in J/m2/day
DTR = RDD
TMMX is daily maximum temperature; COTEMP is the climate change, temperature rise switch for evaluating the impact of temperature rise on the phenological development of the life cycle of YSB. TMMN is daily minimum temperature.
DTMAX = TMMX+COTEMP
DTMIN = TMMN+COTEMP
DAVTMP, average temperature (derived parameter) = 0.5* (DTMAX + DTMIN)
DDTMP, day time average temperature, derived parameter = DTMAX - 0.25* (DTMAX-DTMIN)
COTEMP is temperature rise/fall switch
PARAM COTEMP = 0.
DTEFF, effective temperature after deducting the base temperature = AMAX1(0., DAVTMP-TBASE)
SVP, is saturated vapor pressure in mbar, calculated from temperature (derived value)
SVP = 6.11*EXP (17.4*DAVTMP/(DAVTMP+239.1))/10.
VP is Actual vapor Pressure, mbar, an input for running of the modelAVP = VP
AVP = VP
RH is relative humidity, expressed in %, derived from the vapor pressure as below:
RH = AVP/SVP*100.
In the present study, only temperature and relative humidity effects are undertaken for computation of the phonological stages of the life cycle of YSB, although we have described the other climatic elements as part of the FST compiler, but the other parameters will also be used in deriving the population dynamics model, which we will take up in later course of time.
Since the development stages of YSB are influenced by relative humidity also, so we have to introduce the correction factor for including the effect of humidity, as below:
DAVTMPCF, RH induced temperature correction = DAVTMP*CFRH
TMPEFF=DAVTMPCF-TBASE
CFRH is the Correction Factor for relative humidity for judging temperature is computed as below: i.e. during hatching (CFRHH) and larva formation (CFRHL) stages, computed as below:
CFRH, correction factor for RH=INSW (GDD-EGHATCH, CFRHH, DUM11)
DUM11=INSW (GDD-979.9,CFRHL,1.)
Where INSW is FST Function, if GDD<979.9, then CFRHHD is taken and otherwise DUM11
CFRHH=AFGEN (CFRHHT, RH)
CFRHL=AFGEN (CFRHLT, RH)
FUNCTION CFRHHT=50.,0.9,60.,0.9,75.,1.,90.,1.1
FUNCTION CFRHLT=50.,0.95,60.,0.95,75.,1.,90.,1.05
WDS, wind speed in m/sec = WN
RRAIN, daily rainfall in mm = RAIN
TRAIN, total rainfall in mm = INTGRL (ZERO, RRAIN)
GDD is growing degree days, expressed in degree Celsius-days, is calculated as below:
GDD=INTGRL (GDDI, TMPEFF)
On the basis of literature search from the published literature, the growing degree days for various stages were computed and used in development of the model, and is described as below:
EGHATCH is the thermal degree days requirement for egg hatch, is as below:
PARAM EGHATCH=119.7
INSTAR1 is thermal degree days for end of first instar 1 stage
PARAM INSTAR1=224.9
INSTAR2 is thermal degree days for end of second instar stage
PARAM INSTAR2=317.0
INSTAR3 is thermal degree days for end of third instar stage
PARAM INSTAR3=438.7
INSTAR4 is thermal degree days for end of fourth instar (larva) stage
PARAM INSTAR4=550.3
PUPA, is thermal degree days for end of pupa stage
PARAM PUPA=662.452
ADULT LONGIVITY is thermal degree days for end of adult longevity, which is different for male/female, For Male=741.484 and Female=773.538, depending upon the defined parameter SEX
ADULT=INSW (SEX-1.05, FEMALE, MALE)
SEX=1. For female and 2. For male
PARAM SEX=2.
PARAM MALE, growing degree days for male = 741.484
PARAM FEMALE, growing degree day for female = 773.538
Critical temperature above which the egg hatching stops is defined as below:
DEATH=REAAND (EGHATCH-GDD, DTMAX-40.)
HATMI, minimum temperature below which the Hatching stops, is defined as below
PARAM HATMIN=15.
DEATH1=REAAND (EGHATCH-GDD, HATMIN-DTMIN)
LATMIN, minimum temperature below which larval growing stages stop, and is given as under:
PARAM LATMIN=12.
DEATH2=INSW (GDD-EGHATCH,0.,REAAND(INSTAR4-GDD,LATMIN- DTMIN))
REAAND is FST Function, which will be 1 when both the variables within parenthesis are greater than zero; otherwise the value will be 0.
Duration of various stages is computed as below:
EGHATCHD is egg hatch duration, in days and computed as below:
EGHATCHD=INTGRL (ZERO, DUM1)
DUM1=INSW (EGHATCH-GDD,0.,1.)
INSTAR1D is INSTAR1 Termination Day
INSTAR1D=INTGRL (ZERO, DUM2)
DUM2=INSW (INSTAR1-GDD, 0.,1.)
INSTAR2D is INSTAR2 Termination Day
INSTAR2D=INTGRL (ZERO, DUM3)
DUM3=INSW (INSTAR2-GDD, 0.,1.)
INSTAR3D is INSTAR3 Termination Day
INSTAR3D=INTGRL (ZERO, DUM4)
DUM4=INSW (INSTAR3-GDD, 0.,1.)
INSTAR4D is INSTAR4 Termination Day
INSTAR4D=INTGRL (ZERO, DUM5)
DUM5=INSW (INSTAR4-GDD, 0.,1.)
PUPAD is PUPA Stage Termination Day
PUPAD=INTGRL (ZERO, DUM6)
DUM6=INSW (PUPA-GDD,0.,1.)
ADULTD is Adult Life End Day
ADULTD=INTGRL (ZERO, DUM7)
DUM7=INSW (ADULT-GDD, 0.,1.)
Stop of Run Condition is as under:
FINISH DEATH > 0.95
FINISH GDD> 775.
Integration conditions for running of the program are as under:
TIMER STTIME = 360., FINTIM = 600., DELT = 1., PRDEL = 1.
TRANSLATION_GENERAL DRIVER='EUDRIV’
PRINT DAY, DOY, DVS, RH, AVP, SVP, WDS, TRAIN, GDD, DAVTMP, DAVTMPCF, ADULTD, PUPAD
In the TERMINAL stage, the final values at the stop of model run can be written in an external file:
CALL SUBWRI (TIME, COTEMP, EGHATCHD, INSTAR1D, INSTAR2D, INSTAR3D, INSTAR4D, PUPAD, ADULTD)
END
Reruns options for evaluating the impact of temperature rise on the development stages of the YSB can be run through this given below procedure:
PARAM COTEMP=1.
END
PARAM COTEMP=2.
END
STOP
Experimental
Growing degree days for attainment of various growing stages in the life cycle of YSB were collated from the published literature in this region. The model was calibrated with 2003 weather data of Bhola district of Bangladesh against the findings of Manikandan [5] at 30 oC. After model calibration, it was subsequently taken to climate change window, temperature rise only considered in the present study. Eight divisions (Dhaka, Mymensingh, Rajshahi, Rangpur, Sylhet, Khulna, Chittagong and Barisal) of Bangladesh were taken and one representative location was chosen from each division and historic weather data of 35 years were taken for running of the model and the duration of each development stage was computed and compared amongst temperature rising conditions. In the present study, daily temperature rise from 1-4 oC were considered for two growing seasons, .com rice season i.e. premonsoon (April to June) and Aman Rice season i.e. Monsoon (late June to November) of Bangladesh.
Figure 1: Days required for completion of growth stages of rice yellow stem borer with increased temperature by 1, 2, 3 and 4 degree celcius in the growing environment of Bhola, Bangladesh.
Results and Discussion
During the test period, minimum temperature averaged 26�0.115 and maximum temperature around 31�0.32, with the average temperature around 30 oC, which was used for calibration and validation of the model, and the model performed satisfactorily well, through nice agreement between observed and simulated results (Table 1). Depending on growth stages, the percent deviations were within the limit of model errors. The application of model for specific years of Bhola district showed that the growth stages of rice yellow stem borer (YSB) were decreasing (Figure 1) by about 1.76 days per degree rise in temperature (Y=1.7X+54.6; R2=0.932). This indicated that YSB is likely to infest more rice plants in future under increased temperature conditions. Ramya [7] also reported that YSB would likely to develop faster, oviposit early and thus enhanced population build up than expected. There are reports that temperature increase by 2oC may cause 1-5 times additional life cycles of insects in a season [8].
Table 1: Validation of various growth phases (days) of rice yellow stem borer.
Results, from represented locations in the eight Divisions of Bangladesh, showed that growth stage of YSB varied depending on season (Table 2). In .com pre-monsoon season, life cycle of YSB would likely to be completed within 47-53 days, depending on locations and temperature rise from 1-4 degree celcius. Similarly in Aman wet season, it would about 45-50 days for temperature rice from 1-4 degree celcius. However, under the Control (no temperature rise) condition, it requires around 52 days for T. Aman and 55 days for .com. Our findings indicate that growth cycle of YSB is likely to decrease by 2.04 days per degree rise in temperature in the .com season and 1.70 days in T. Aman season (Figure 2). Similar results were reported by Manikandan [5]. Generally, insect population build up depends on favorable weather conditions and availability of host. So, there will be ups and downs in the peak build ups in a cropping season [9]. Although model data needs to be cautiously adopted, it clearly showed that with climate change impact the infestation of YSB would be increased, which might be cause of yield reduction, if not proper management is taken at the right time [10].
Figure 2: Total life cycle duration of yellow stem borer as influenced by temperature rise during .com and T. Aman, season (averaged over eight Divisions of Bangladesh).
Table 2: Developmental phases (in days) of rice yellow stem borer as influenced by temperature rise in different growing seasons.
Conclusion
Yellow stem borer of rice crop is a major concern in Bangladesh. Dead hearts and white heads caused by YSB significantly reduce growth and yield of rice crops, especially in .com (Pre-monsoon) and T. Aman (Monsoon) seasons. There is a need to understand the phenology i.e. life cycle assessment and population dynamics of YSB in the growing environments of Bangladesh. In the present study, a simple model, as written in Fortran Simulation Translator (FST), was developed to assess the life cycle of YSB. The model was primarily based on growing degree day�s concept, by also considering cardinal temperatures for specific phenological/ development growth stages of YSB. The model was successfully validated with the growing environment of Bhola district of Bangladesh. Subsequently, the model was taken to assess the impact of rise in temperature on life cycle of YSB in representative locations of eight Divisions of Bangladesh. The response was spatiotemporally and seasonally variable. The life cycle hastened with the rise in temperature by 1-4 degree celcius. We, in near future, plan to develop a population dynamics model for YSB and to subsequently link it with the rice growth model to evaluate the yield reductions associated with YSB infestations.
Acknowledgement
We greatly acknowledge the support of Krishi Gobeshona Foundation, Dhaka, Bangladesh in conducting this research through CRP-II project.
https://lupinepublishers.com/agriculture-journal/pdf/CIACR.MS.ID.000144.pdf
For more Lupine Publishers Open Access Journals Please visit our website: https://lupinepublishersgroup.com/
For more Agriculture Open Access Journal articles Please Click
Here: https://www.lupinepublishers.com/agriculture-journal/
To Know More About Open Access Publishers Please Click on Lupine publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
33 notes
·
View notes
Text
Lupine Publishers | Treatment of Infected Primary Teeth using Modified Antibiotic Paste
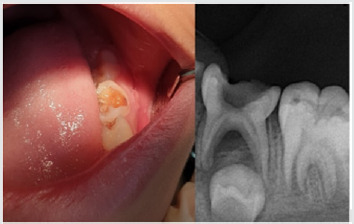
Lupine Publishers | Journal of Pediatric Dentistry Impact Factor
Abstract
Objectives: Treatment of pulpectomized primary molars with chronic infection using a mixture of three antibiotics: Metronidazole, Ciprofloxacin, and Doxycycline mixed with Macrogol or Propylene Glycol (modified 3MIX-MP) as an intracanal medicament before the complete cleaning and shaping and obturation.
Study design: A 7 years old child with infected primary molar came to our clinic for treatment. A detailed medical history and drug allergy were taken. Ciprofloxacin (500mg), Metronidazole (500mg) and Doxycycline (100mg) tablets divided in the proportion of 1:3:3 (one part of Ciprofloxacin, three parts of Metronidazole, and three parts of Doxycycline) and mixed with propylene glycol to form an ointment. Biomechanical preparation was done. The modified 3MIX-MP paste placed in the pulp chamber then temporary filling. The patient was recalled after 2 weeks. The tooth was obturated and restored then a stainless-steel crown placed. Then reevaluated at 3rd, 6th, and 12th months.
Results: Excellent clinical and radiographic success when compared to conventional pulpectomy and non-instrumentational lesion sterilization tissue repair therapy.
Conclusion: Treatment of Primary molar with modified 3MIX-MP, followed by instrumentation and obturation provided excellent clinical and radiographic success when compared to non-instrumentational lesion sterilization tissue repair therapy.
Keywords: Pulp infection; Pulpectomy; Modified antibiotic paste; Primary molars; Chronic, infected pulp; Modified 3 MIX-MP; Pulpectomy; Triple antibiotic paste; Primary teeth
Introduction
The first topical antibiotic introduced to endodontics was Grossman’s polyantibiotic paste in 1951, later many topical antibiotics have been introduced with varying combinations, few of those include Septomixine forte; PBSC (Combination of Penicillin, Bacitracin, Streptomycin and Caprylate sodium), and Clindamycin. However, none of these combinations has proven to be 100% successful in eliminating all the bacterial strains from the root canal system [1-5].
Materials and Methods
A child aged 7 years old with chronic infection related to the lower left primary molar came to our clinic for treatment of the infected molar (Figure 1). Treatment was explained to the parents and written informed consent was taken from parents before start of the study. A detailed medical history and previous illness with a history of drug allergy were taken from the parents, then the mentioned primary molar was diagnosed clinically, the molar was badly decayed with signs of chronic infection such as: gingival swelling and tenderness to percussion. A radiographic examination was done and a per radicular radiolucency was found, with no excessive root resorption. Commercially available chemotherapeutic agents such as Ciprofloxacin (500mg) (Omacip, NPI Pharma, Oman), Metronidazole (500mg) (Anazol, JPI, Saudi Arabia), and Doxycycline (100mg) (Tabocine, TPMC, Tabuk) tablets were obtained [6,7], then these tablets were crushed into fine powder using sterile porcelain mortar and pestle. These powdered drugs were transferred into three separate sterile glass containers, capped tightly and stored in the refrigerator until its use. Just before use, each powdered drug was divided in the proportion of 1:3:3 (one part of Ciprofloxacin, three parts of Metronidazole, and three parts of Doxycycline) and were mixed with propylene glycol and polyethylene glycol to form an ointment. Reddy GA et al. Trairatvorakul and Detsomboonrat, Jaya et al., Cruz et al. also followed the similar protocol of preparation of 3MIX antibiotic paste [8-11].
Figure 1: Preoperative illustration.
Figure 2: Postoperative illustration.
Preoperative clinical and radiographical signs and symptoms were recorded. The tooth was anesthetized using 2% Xylocaine with 1:80,000 adrenalin and isolated with rubber dam. Access opening was performed using round bur, Biomechanical preparation was done using k files from size 10–25. The root canals were chemically cleaned with 1% sodium hypochlorite solution and dried with paper points. The 3MIX-MP paste placed in the pulp chamber and pressed with dampened cotton pellet and temporized with Cavit. The patient was recalled after 2 weeks for evaluation. The tooth was obturated with reinforced zinc oxide eugenol (IRM, Dentsply) using lentulo spirals. Then restored with glass ionomer restorative material (Riva self-cure, SDI) and reinforced by placing stainless steel crowns (Figure 2). Further, the treated tooth was reevaluated both clinically and radiographically at 3rd, 6th, and 12th months intervals postoperatively (Figure 3). At the time of revisits, the tooth was examined clinically for any signs of failure that includes a report of spontaneous pain, presence of swelling, sinus tract and mobility. Radiographic evaluation was done to check the radiolucency and signs of resorption. The tooth was asymptomatic without pain, swelling, sinus tract and mobility also there was no increase in furcation radiolucency or development of root resorption which is abnormal for the age of the child.
Figure 3: 12 months Follow up.
Results
Excellent clinical and radiographic success when compared to conventional pulpectomy and non-instrumentational lesion sterilization tissue repair therapy.
Discussion
This study was approved by “Research Ethics Committee, Taibah University, College of Dentistry, TU CD-REC”. The concept of Non-Instrumentation Endodontic Therapy introduced by Niigata university school of dentistry; Japan has gained reputation as it proved to attain 100% sterility in the root canal system [12- 15]. They recommended a technique similar to pulpotomy where debriding only the pulp chamber of chronically infected primary teeth and placing medicament (ciprofloxacin, metronidazole, and minocycline) near the root orifice without preparing the radicular portion. Cruz et al. suggested vehicles such as macrogol and propylene glycol (3MIX–MP) and demonstrated that these vehicles will carry the medicament deep into the dentinal tubules, thus aid in effective eradication of bacteria [11]. Metronidazole (Nitroimidazole compound) due to its wide spectrum of antibacterial action against anaerobes (Ingham et al. 1975) gained importance as the 1st choice drug for triple antibiotic paste preparation [16,17]. Metronidazole binds to the DNA and disrupts its helical structure and thus leads to rapid cell death. However, metronidazole even at higher concentrations could not eradicate all the bacteria thus indicating the necessity of some additional drugs to sterilize these lesions [15]. The two other antibacterial drugs, i.e. ciprofloxacin, and minocycline, in addition to metronidazole (3MIX) were added in an effort to eliminate all bacteria [8,10,15,18]. The 2nd choice of drug ciprofloxacin is a synthetic fluoroquinolone with rapid bactericidal action. It inhibits the enzyme DNA gyrase of bacteria. It exhibits very potent activity against Gram-negative bacteria but very limited activity against Gram-positive bacteria. Most of the anaerobic bacteria are resistant to ciprofloxacin. Hence, it is often combined with metronidazole in treating mixed infections. The 3rd choice of drug was minocycline. It is a semisynthetic derivative of tetracycline, primarily bacteriostatic, inhibiting protein synthesis by binding to 30S ribosomes in susceptible organisms and exhibits broad spectrum of activity against Gram-positive and Gramnegative microorganisms [3].
In our present study we replaced Minocycline with Doxycycline due to the difficulty in obtaining Minocycline, and before using the Doxycycline as a replacement we have done further searches for previous studies to ensure that both medications have the same effect and this replacement will not affect the efficacy of the mentioned mix. The already done studies concerning the difference between both Doxycycline and Minocycline revealed that still no statistically significant differences had been demonstrated in clinical trials when comparing Minocycline with Doxycycline, and investigators had concluded that both are equally effective. And they differ in their adverse event profile [19]. Considerably fewer adverse effects have been reported for Doxycycline than Minocycline; the adverse effects for Minocycline are 5 times more common than for Doxycycline [19]. We have followed the same protocol of Reddy GA et al. of extirpation of both necrotic coronal as well as all accessible radicular pulp tissue and then complete obturation, which is reported successful clinically over 16th month follow-up [9]. Although the previous studies have demonstrated that the LSTR (Lesion Sterilization Tissue Repair) technique as one of the successful techniques for management of chronically infected primary teeth, the controversies aroused about the duration of therapeutic activity of the medicament and leaving the infected material in the radicular region. So that the present study planned where in treated tooth were revisited after 2 weeks for medicament removal and obturation.
Conclusion
All the primary teeth with chronic infection which were treated using modified 3MIX-MP, followed by the instrumentation and obturation provided excellent clinical and radiographic success when compared to conventional pulpectomy and noninstrumentational lesion sterilization tissue repair therapy.
For more Lupine Publishers Open Access Journals Please visit our website:
http://lupinepublishers.us/
For more Open Access Journal on Pediatric Dentistry articles Please Click Here:
https://lupinepublishers.com/pediatric-dentistry-journal/
To Know More About Open Access Publishers Please Click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
22 notes
·
View notes