
nestingmonkeys
2K posts
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by nestingmonkeys and here's what we found interesting.
Average Info
Notes Per Post
145K
Likes Per Post
76K
Reblog Per Post
69K
Reply Per Post
300
Time Between Posts
11 days
Number of Posts By Type
Text
16
Photo
1
Last Seen Tumblr Blogs




Fun Fact
Tumblr.com rank in the US is 25.
Text
An absolutely devastating expose of rape culture among older American adults - even if the author doesn’t choose to admit to herself or her readers that that is what she’s writing about
“My mother’s most recent encounter with “the blue pill” was grueling. After a taxing day (stalled car, heavy traffic), my mother told the man she was seeing that he should not take it that night. She was exhausted; all she wanted was a good night’s sleep. He took the pill anyway and got into her bed with an erection. Too tired for an argument, she acquiesced. “You’re ministering to him,” she said of the experience, “trying every trick in the book, and it’s not working. But he’s like, I have an erection, I’m going to make this work, I’ve got this usable part, I’m just going to do it … I felt like I was the blow-up doll, as if I’d disappeared. I was so conscious of being utilized and totally objectified.”
Ultimately, the man did not ejaculate. But penetration didn’t end until my mother, who says she’d begun to disassociate from the moment, dug her fingers so deeply into his shoulders that he finally stopped to ask what was wrong. The next day, there was “no pain. No physical irritation. Tedium. Annoyance. Anger at self for putting up with it. Lots of the latter.””
Full text under the cut:
The Little-Blue-Pill Problem
For some women of a certain age, erectile-dysfunction prescriptions are redefining sex — and not always for the best.
My mother and I talk a lot about sex on a near-daily basis, which hasn’t always been the case. Growing up, the only “sex talk” I can remember came the summer before I left for boarding school, when I was packing up, and my mother suddenly asked about the sex-education classes I’d endured as an eighth-grader.
“Did they teach abstinence or safe sex?”
Because I didn’t know what abstinence was, I chose the latter.
“Well then,” she said, “you know about sex.”
I didn’t know about sex, but she sounded relieved, which in turn relieved me.
We first started talking openly about sex after our respective divorces, which happened within a year of one another. I was 39 and in Kentucky, in a freestanding house, living alone for the first time in my adult life. She decided to leave Virginia and buy a too-large house just down the street. Within just a few months of her relocation, I’d sold my house and moved in with her.
It was in between episodes of Prime Suspect — in which Helen Mirren must not only hunt violent criminals but also combat rampant sexism — that we began exchanging stories about our sex lives. I was surprised to learn that my then-68-year-old mother considered herself sexually enthusiastic and that she thought sex had become more rewarding with age. I was also surprised to learn that she, an intrepid internet dater, had hopes and intentions of remaining sexually active for the foreseeable future.
Now, though, just eight years later, our talks have gone from casual and funny to negative and remorseful, as she’s become increasingly weary of attempting intimacy with men her age.
My mother negotiated sex through three marriages with three very different men, for a cumulative 43 years, but never once reckoned with erectile dysfunction. “Maybe I was lucky,” she said. “Maybe not.” When ED “dropped its head” during her first post-divorce sexual encounter a couple of years ago, she was flummoxed. “My partner and I were both in our mid-60s, healthy, and fit. A flaccid penis was not part of my intimacy vocabulary.”
Neither was “the blue pill,” which could actually be any number of phosphodiesterase type 5 (PDE5) inhibitors in any number of colors — Viagra (sildenafil), Cialis (tadalafil), or Levitra (vardenafil), prescribed medications that improve dilation of the arteries in a penis, helping a man get and maintain an erection.
To the uninitiated, including myself and almost all of the friends I polled, 30- and 40- and even 50-somethings who haven’t yet had personal experience with it, sex on the blue pill is assumed to be just the same as sex without it. Maybe there would be a few extra lengthy erections, some discomfort on the guy’s end, but that would be it.
Large swaths of men and women describe Viagra as a game changer, a marriage-maker, a life saver. But there also exists a mostly unheard-from subset of heterosexual women who would disagree. In fact, my mother unequivocally views Viagra as the cause for her newfound aversion to sex.
The problem is that while a urologist can improve circulation pharmacologically and add testosterone, actual ejaculation isn’t guaranteed. But some men, perhaps out of a desire for the familiar satisfaction of completion, keep going, keep engaging in sex, regardless of whether or not their partner wants to or is still getting any pleasure from it.
One doctor I spoke with, Claiborne Whitworth, explains it this way: A functional erection does not equal the ability to achieve orgasm or, as my mother points out, even an erection capable of penetration. “Older male patients commonly report difficulty achieving orgasm,” Whitworth told me, “some failing to achieve it at all, with sexual encounters ending due to exhaustion and/or discomfort for the receiving partner.” The average time for a male to ejaculate (once the penis is in the vagina) is three-to-seven minutes. An older man with delayed ejaculation can take 25 to 30 minutes or even longer.
Now consider this: Vaginal lubrication is produced during arousal, and most water-based lubricants, which mimic natural lubrication, come with a suggested reapplication time of five to 15 minutes. According to a survey conducted by the Study of Women’s Health Across the Nation, which lasted over 17 years and included more than 2,400 participants, the “prevalence of vaginal dryness increased from 19.4% among all women at baseline (ages 42 to 53 years) to 34% at ages 57 to 69 years.” Menopause, anxiety, and being married were all linked to the development of vaginal dryness.
My mother’s most recent encounter with “the blue pill” was grueling. After a taxing day (stalled car, heavy traffic), my mother told the man she was seeing that he should not take it that night. She was exhausted; all she wanted was a good night’s sleep. He took the pill anyway and got into her bed with an erection. Too tired for an argument, she acquiesced. “You’re ministering to him,” she said of the experience, “trying every trick in the book, and it’s not working. But he’s like, I have an erection, I’m going to make this work, I’ve got this usable part, I’m just going to do it … I felt like I was the blow-up doll, as if I’d disappeared. I was so conscious of being utilized and totally objectified.”
Ultimately, the man did not ejaculate. But penetration didn’t end until my mother, who says she’d begun to disassociate from the moment, dug her fingers so deeply into his shoulders that he finally stopped to ask what was wrong. The next day, there was “no pain. No physical irritation. Tedium. Annoyance. Anger at self for putting up with it. Lots of the latter.”
In a 2003 study published in Sociology of Health, the sociologists Annie Potts, Nicola Gavey, Victoria Grace, and Tiina Vares discuss the dearth of documented experiences from the female sexual partners of men who use sexuopharmaceuticals. Talking to 27 women whose male partners used Viagra, the writers suggested that “while the publicity surrounding Viagra may potentially facilitate more positive attitudes to sexuality in older age, it may also produce a societal expectation that ‘healthy’ and ‘normal’ life for older people requires the continuation of ‘youthful’ (energetic) sex lives focused on penetrative intercourse.”
Of course erectile-dysfunction medications can create positive change for both the prescription holder and their partner. Peter, an 80-year-old in Ashville, North Carolina, can’t remember when he first started using Viagra, but he does remember it was when his ability to orgasm went from twice a day to once a day. “One day, there was less penis in my pants,” he told me. Somewhere in his late 60s, early 70s, however, the pill stopped working as effectively. He returned to his doctor. His problems were four-fold: “It won’t get up; it won’t stay up; it won’t stay up long enough for me to complete; it won’t stay up long enough to give her satisfaction.”
Peter’s doctor put him on a low daily dose of Viagra, instructing him to increase the dose to 100 milligrams before sexual activity. “It’s not as rigid as when I was a younger man, and it still presents some issues with penetration — I am working through those issues with the incredibly generous cooperation of my partner.” Today, he says, he’s having “the most satisfying sex I’ve ever had, albeit with challenges. I’m much more thankful and appreciative of what’s possible.”
Still, my mother was eager for me to write about her experiences with the blue pill, in part because she’s convinced, given her exploits, that the drug is quietly affecting the well-being and happiness of an untold number of women all over the world. Telling me about her recent and past encounters, she sometimes waxed quite funny (“I mean, their faces still look good, but their little wanker is not wanking”), but mostly she was mad: “The whole business of entitlement, sex, aggression, erections, and pills makes me angry. On the one hand, I felt that I was complicit in allowing him to continue,” she said, “but the reason I didn’t stop him is because of that stupid toe in the door of patriarchy: that a man’s penis is such a fragile subject that I didn’t want to humiliate him. It felt incumbent on me to make the problem go away. Which is just stupid. But I was, in a way, taking care of his bad behavior.”
In the case of many erectile-dysfunction advertisements, the perspective of female partners is either portrayed as entirely healthy and participatory (those bathtub commercials, for example) or entirely excluded. That 1998 ad featuring Bob Dole equated medicated sex with bravery, leaving out any consideration for the partner altogether with the tagline, “It may take a little courage to ask your doctor about erectile dysfunction. But everything worthwhile usually does.” An entire Pfizer campaign featured solo well-dressed men in confident, contemplative poses. One series of slogans highlighted by Weill Cornell Medicine’s History of Medical Advertisements collection — “You may be a man of few words, but you know how to make them count”; “Men don’t look for excuses. They get things done”; “This is the age of knowing what you’re made of” — reinforce that the drug is all about the man, all about his desires, all about helping him recapture what he’s previously been, and no one, nothing, else.
“Everybody was going on about how wonderful this thing was,” said one 60-year-old woman participating in the 2003 study, “and … [when I read about some other women’s experiences] I thought oh, thank God, I’m normal! — not everybody sees it as being … the most wonderful thing that ever happened this side of sliced bread!”
I asked a general practitioner if she ever had complaints from female patients about partners misusing or overusing Viagra prescriptions. She said, “Viagra can probably uncover deeper relationship struggles. We think that sex is going to fix things, it doesn’t necessarily …” Plus, aging affects women’s sexual health, too, she points out. “Female genital atrophy, for instance, is a common phenomenon among menopausal women that can reduce libido, reduce arousal, and increase difficulty in achieving orgasm,” she added. She told me about a couple in their 70s who she sees and treats together. The husband wanted the pill. The wife did not. The husband wanted their doctor to explain why his wife was wrong. She wouldn’t. “It was very aggressive,” she told me. “Very much But I’m the man sort of thing.”
I talked to Dan, a mid-50s CrossFit instructor who gave up Viagra about a year ago. Dan first started using the pill after going through a bad breakup in his late 40s. He didn’t need it, he says, but the fallout from the breakup was stressful. When he started dating someone he connected with, he got worried that his stress would be a distraction and that he wouldn’t be able to perform when the time came. He went to his doctor.
“Knowing what I know now,” he said, “if I was my doctor, I would have said, ‘Look, bro. I could prescribe this shit for you, and it will cause you to much more easily get an erection and keep said erection. It’ll spring to life and stay there for a while, no matter what’s on your mind. But in the medium to long term, you’d actually be better off, if you don’t actually have a physiological problem’ — which I didn’t and don’t have — ‘figuring out your fucking mind so that you don’t introduce this sort of dependency into the mix.’ Because that was the thing that happened.”
Other drawbacks for Dan included headaches, low blood pressure, and the issue of timing. He’d gauge the possibility of sex, take the drug so that he hoped the timing was about right, and then sometimes, if intercourse didn’t happen, he’d be stuck. “It just was not ideal.” A few times while using the pill, he tells me, he felt like he might actually “drop over dead” during some especially strenuous CrossFit classes. Ultimately, he weaned himself off what he referred to as his chemical dependency because the drug had begun to affect how he thought about sex. “Once you take it, you’re then stuck facing a headache and with this particular window where it does its thing. It inclines you to think, Okay, I just took this. I should probably use my penis.”
After talking with my mother, I started wondering about other women. I am guilty of acquiescing to sexual encounters with men when I wasn’t totally in the mood. I’m guilty of faking orgasms in the hopes of rushing a partner’s climax. I’m guilty of letting a partner continue his penetration long after it’s stopped being comfortable or pleasurable for me, a choice that left me feeling sore and achy well into the next day. Exactly how pervasive is women’s deference to men’s pleasure?
I texted a few friends, asking about their experiences. Mallory, who is in her early 50s, wrote back immediately: “My own experience with the blue pill was great,” she said, but she also told me about a woman who’s “a widow now but used to joke about the only foreplay was serving her husband a glass of water to take the blue pill.”
Lynne, a friend of a friend, is a 65-year-old retired medical interpreter who specialized in obstetrics and gynecology. Five years after her divorce — what Lynne refers to as “a length of time without intimacy” — she was thrilled to reconnect with her first love, who’d recently become single himself. “He was as opposite to my ex-husband as a man could be, in mostly wonderful ways, but also the not so great,” she said. “He was the prototypical sedentary American with terrible dietary habits on top of the smoking, and he needed Viagra to perform at all. But the sex was fantastic, and we had a blast making up for lost time.”
For Lynne, the drug, initially, was a revelation. But when she eventually asked him not to automatically take the pills when she noticed what she thought were side effects, as he would if there was even a possibility of intimacy, “it took a long time for him to control the habit of doing so, as if it were an obsession. And it is!” Eventually, her partner accepted Lynne’s feedback and now, eight years later, they’re still together.
On an intellectual level, Lynne understands that natural aging diminishes both the desire and abilities she took for granted in more youthful days; she told me that an active and fulfilling sex life has been an extremely positive part of her life. “That being said, the obsession with virility is creepy,” she says, “the assumption that it is what women want all the time is a turnoff.”
I found Ann, 53, through Instagram. She explained her marriage’s sex life as having its share of highs and lows before she and her husband turned to sildenafil. “We are very attracted to each other, have been from the very beginning in our 20s,” she told me. “It went up and down while raising kids. It got really good after the kids went to college.”
Ann described her experience with sildenafil as good, “for the most part.” She added, “It’s in his head now that he always needs it. I don’t like to always have to say, ‘Tonight, let’s do it.’ There’s something a little rote about sex now.”
Ann’s diminished craving doesn’t stop her from being grateful for the sexuopharmaceutical help her husband has received. She told me that the very best thing (for her) isn’t the sex; it’s the psychological side effect: “I couldn’t believe how down he could be if an erection did not happen.”
A woman in her late 60s named Pearl heard that I was working on this piece and offered to share her thoughts. “I’ve had to play along with my husband’s needs and wants for a while now,” Pearl told me. Before the blue pill, but since middle age, Pearl described sex as infrequent, quite casual, not unpleasant but also not earth shattering. “We both had to be quite ‘turned on’ for it to happen. And, yes, I often felt the need to hide my lack of interest and play along.” They hadn’t discussed Viagra until her husband brought a prescription home one day.
Pearl had lots of questions, including whether or not her husband had acquired a similar pill for her. He hadn’t. “How am I supposed to get in the mood, lube up, wait the half-hour, and act like this is great?” she said. “I do get asked sometimes ‘Should I take a pill?’ Hmmm … Am I in the mood? Will I be in a bit? Do I want to be in the mood? Or I get the ‘I took my pill awhile ago.’ Well, great, I’m about to fall asleep …”
When I told Dr. Bat Sheva Marcus, a sex therapist, over Zoom about my mother’s experiences that have inspired this story, she almost instantly teared up. “The fact that you’re talking to your mother about this is so powerful to me,” she said. But she was also quick to point out that she wasn’t crying for the reason I might think.
“It sounds to me to a certain degree that the thesis of this article is that the little blue pill has been really helpful for men but is putting a lot of pressure on women in a way it shouldn’t,” she said. “That’s probably true about a subset and I want to talk about what that subset is, but I also want you to know that phos-5 inhibitors in general have been a godsend to many, many people.”
Marcus then delivered a surprising statistic that she would go on to deliver a few more times over the next couple days: by 40, 40 percent of men need will need a PED5I to achieve an erection; by 50, 50 percent; by 60, 60 percent; by 70, 70 percent; and by 80, “well, you’re probably not gonna be able to have intercourse without Viagra.”
When I started this piece, I was filled with rage on my mother’s behalf. My working hypothesis was something along the lines of Fuck the blue pill, fuck the patriarchy, fuck masculine fragility. But after talking to Marcus, I understood that my initial stance conveniently eschewed nuance. “I think what you’re hitting on,” Marcus said, “is less the problem with the medication and more the problem with the communication and the expectations about sex in our society. If you can’t talk about it, you shouldn’t be doing it.”
Dan, the CrossFit instructor, told me, “My new relationship is so much deeper. We’ve gotten more comfortable. We’re pretty direct communicators now. Sex isn’t always going to lead to one or both of us having an orgasm. Sometimes it’s like the movies and awesome, and sometimes it’s nothing like that and still awesome. I just wish my doctor hadn’t been so ready to say, ‘Sure. Here. Try it.’ It’s much more complicated than that.”
My friend Anita, who is in her early 50s and lives in New York, met her husband, 15 years older, when she was 20. For several decades, they had a healthy and active sex life. When Anita was 45, her husband, after a year of debilitating symptoms, was diagnosed with a near-fatal heart infection.
“Our sex life had totally dried up,” she said, “because he was dying, and they didn’t know why.” Ultimately, he had two heart valves replaced, was in the hospital for a month, and put on IV antibiotics for six months after that. During that time, they had no sex. When they were ready to try again, they discovered he had erectile dysfunction, a common side effect for men after open-heart surgery.
His doctor suggested Viagra. “And, oh my God, it felt like I was being hammered by somebody who was never going to have an orgasm. It’s fine now, but it was terrible at first. Because his whole body — his whole body image — was fucked up from the surgery and almost dying.” Anita realized a conversation was in order. “But that was after I got to the point where I could be like, ‘It’s working, that’s great, but, you know, it’s not working in a way that is deeply satisfying for me.’ It took a long time — like four years — for me not to feel like I was just a receptacle.”
My boyfriend is nine years older than I am. Long before my mother and I started talking about erectile dysfunction, he and I had agreed that, if and when it was necessary, he’d get a prescription for Viagra, and that would be that. But he’s been privy to much of my research for this piece and, recently, our conversations around the topic have become more detailed and specific.
“Everything I knew about Viagra came from commercials I saw during football games,” he said. “You know: Talk to your doctor. Have better, more satisfying sex … I hadn’t thought much beyond the pleasurable smiles on the aging beautiful couples’ faces.”
“What if I don’t want to have sex into your 70s?” I asked.
“Ideally, we’ll find other forms of being intimate that work for us both,” he said. “The idea of hurting you is a total turnoff.”
“There are lots of ways to have sex,” I said.
“And if you don’t want to and I do, I’ll use my hand. But maybe it’ll be me who doesn’t want to have sex,” he said. We both laughed.
These new conversations aren’t sexy. Sometimes they’re playful, and sometimes they’re uncomfortable. But one thing that seems glaringly essential to any healthy and functioning sex life is communication. I’m grateful that my mother has provided me a reason to start thinking about and talking about what sex might look like as I move into my 50s and 60s.
Talking about sex is hard. It took my mother and me many decades, several divorces, a shared roof, a decent amount of wine, and Helen Mirren before we were able to start doing so honestly and without embarrassment. Now it feels as natural as pouring a cup of coffee first thing in the morning and as easy as tying a shoelace.
“Maturity and confidence contributed to my embrace of ‘geriatric’ sex and enthusiasm for it,” my mother told me. “We geriatrics passionately don’t want to grow old, and sex — good viable sex — offers the suggestion that we aren’t really old after all. But I now believe I’ve given up on that element in my life, which makes me sad. Joyous, frisky, passionate sex is just that: joyous, frisky, and passionate. I would happily forgo erections, penetration, and orgasms for the pleasure of being with a man who knows he’s still desirable in spite of impotence.”
My mother has scolded herself for sometimes still “having her toe in the door of the patriarchy.” But I see something admirable, even subversive in her new self-possession. I know a lot of women who fear the second half of their lives. But I’m beginning to think it’s the very act of becoming “women of a certain age” that inclines us toward autonomous and radical thinking — and demanding our pleasure be taken seriously.
225 notes
·
View notes
Text
love to read about the history of prostitution in japan (or anywhere) and they go, "actually women typically entered the industry of their own free will :) the vast majority of them came from starving peasant families and had no education and therefore couldn't do other work or effectively understand the contracts they were signing or what predatory loans are, but they walked into those brothels by themselves :D"
2K notes
·
View notes
Text
SCUM Feathered
If you think SCUM is too much, you’ve never sat still while someone unmade you and smiled
People get so hung up on the shock factor of the SCUM Manifesto they forget to read it for what it is. Valerie wasn’t just ranting she was also reversing the gaze. She wrote about men the way men have written about women for centuries: cold, cruel, disposable, beneath.
It’s satire. It's weaponized perspective. It’s the sound of centuries of objectification slammed back into the face of the oppressor.
You wanna know how it feels to be spoken about like a category? Like a disease? Like something subhuman? Read SCUM. That’s how men have written about women in medical journals, courtrooms, locker rooms, and textbooks. Solanas just flipped the script.
It’s not a guidebook, it’s a scream. A rage-text. A feminist nuke dropped on a world that kept stepping on women and laughing. Solanas was pissed, poor, and had been deeply hurt. She wrote SCUM with venom because nice wasn’t getting anyone free.
Some people misread it as literal. Others dismiss it entirely. But if you’ve ever wanted to burn it all down because no one listens when you cry for help? You’ll get it. You’ll feel it in your ribs.
Yeah, Valerie Solanas shot Andy Warhol. And I’m not here to sanitize that. It happened. But let’s not pretend it came out of nowhere or that he was some innocent art angel caught in the crossfire.
He exploited her. He strung her along. Took her script, ghosted her, laughed at her rage. Like too many powerful men do when a woman’s desperate and inconvenient. He made her feel invisible. Like her work didn’t matter. Like she didn’t matter. And she snapped.
Women don’t usually shoot people. That’s the whole point. Society teaches us to swallow the rage, not act on it. To self-destruct quietly. Valerie turned that rage outward, and suddenly the world cared. cause a man got hurt.
And let’s be real if Solanas had been a man with a manifesto, he’d be called a revolutionary. A genius. Another tortured visionary in the museum of white male madness. But she was a woman, poor and "unhinged", so they called her a lunatic and locked her up.
I’m not a feminist in the soft, palatable, “I do this for me” kind of way. I’m not singing dainty empowerment songs in a gilded cage. I’m a molting, wild-eyed thing with blood on my beak. I’m SCUM-type. Feathered fury. Talons out. I don’t want equality in a broken system—I want the nest torched. Men, leave me alone. Don’t try to clip my wings. Don’t perch too close. Your approval means nothing to me. Your opinions fall like fledglings from the tree. This isn’t empowerment in a pink cage—it’s survival with bones in the nest. I’m not here to be tame. I’m here to scream loud enough to split the sky.
“In actual fact, the female function is to explore, discover, invent, solve problems crack jokes, make music -- all with love. In other words, create a magic world.” ― Valerie Solanas, SCUM Manifesto
385 notes
·
View notes
Text
one of the biggest risk factors for ptsd (which includes symptoms like uncontrolled, pathological levels of anger) is not feeling supported or believed by those around you or like you have to keep the trauma a secret etc this is probably why rape victims have exponentially higher rates of ptsd than say, natural disaster victims. “Don’t be too upset because the real important thing to remember is that your abuser is human too and also there’s a good chance you’re lying for attention and money” is certainly not the mindset that will set people on the road to healing
1K notes
·
View notes
Text
The cliché that when women are liberated men will be liberated too shamelessly slides over the raw reality of male domination — as if this were an arrangement in fact arranged by nobody, which suits nobody, which works to nobody’s advantage. In fact, the very opposite is true. The domination of men over women is to the advantage of men; the liberation of women will be at the expense of male privilege. Perhaps afterwards, in some happy sense, men will be liberated too — liberated from the tiresome obligation to be ‘masculine.’ But allowing oppressors to lay down their psychological burdens is quite another, secondary sense of liberation. The first priority is to liberate the oppressed. Never before in history have the claims of oppressed and oppressors turned out to be, on inspection, quite harmonious. It will not be true this time either. - Susan Sontag
487 notes
·
View notes

Text
The worthlessness of women as human beings is entirely clear when it is understood that pornography is a form of mass entertainment, in the United States now grossing an estimated eight billion dollars a year. Men, the primary consumers of pornography, are entertained by these acts of sexual abuse.
The lives of women are circumscribed by the terrorism of pornography, because it is the distilled yet entirely trivialized terror of rape, battery, incest, torture, and murder—women are objects, not human, assaulted and hurt, used in sex, because men want and like sexual dominance. Pornography is the prostitution of the women in it, and it is a metaphysical definition of all women as whores by nature; so it is also the terror of being born to be used, traded, and sold. The substance of this terror—its details, its ambiance—is the pleasure, is the entertainment, for the men who watch. It is hard to imagine how much they hate us.
It is also difficult to understand how absolutely, resolutely indifferent to our rights they are. Yet these men who like to see us being used or hurt are not indifferent to rights as such: they guard their own. They claim, for instance, that in being entertained by pornography they are exercising rights of theirs, especially rights of expression or speech. How is it possible that in watching rape—or, frankly, in watching female genitals, women's legs splayed—they are exercising rights of speech? It must be that our pain is what they want to say. Perhaps our genitals are words they use. Incomprehensible as it may be to us, their enjoyment in our abuse is articulated as a civil liberty of theirs. The logic of the argument is that if their rights to pornography (to possession, exploitation, and abuse of us) are abrogated, they will be unable to say what they want to say. They must have "freedom of speech."
Also, the sexual exploitation of women is held to be "sexual liberation." The uses of women in pornography are considered "liberating." What is done to us is called "sexual freedom."
Our abuse has become a standard of freedom—the meaning of freedom—the requisite for freedom—throughout much of the Western world.
-Andrea Dworkin, Letters From a War Zone
107 notes
·
View notes
Text
instagram
Germany has taken a significant step in supporting women’s health by extending maternity leave to those who experience a miscarriage after the 13th week of pregnancy. This new legislation acknowledges the profound physical and emotional impact of miscarriage, providing women with the necessary time to heal. It’s a progressive move that sets a new standard for workplace support and women’s rights.
465 notes
·
View notes
Text
people love going "we can recognise how men are hurt by patriarchy without minimising the harm done to women" and then minimising the harm done to women
4K notes
·
View notes
Text
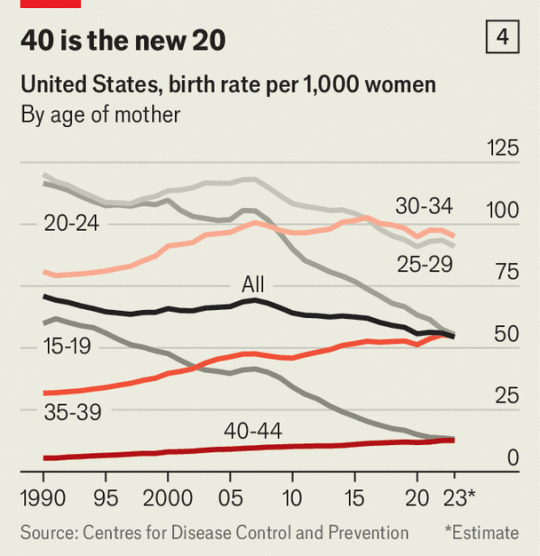
as i’m sure many of you know, “fertility” rates are my, uh, one too many drinks cause, bc the following things (inter alia) piss me off:
calling it fertility rate
saying women aren’t having kids bc lack of good parental leave and health policies in the U.S.
saying women aren’t having kids bc scary future and bad present
saying women want more kids but aren’t bc, see above
here’s some fun graphs and excerpts from an article in the economist that i know i’ve posted before but you can never see them too often


govts have tried just giving new parents straight cash: “The thinking behind [financial incentive policies of giving new parents straight cash] dates back to the entrance of women into the workforce en masse, which happened at around the same time as birth rates started their long decline. “ but these policies “have a relatively small impact [and are] fabulously expensive, as lots of cash goes to parents who would have had children regardless of the financial incentives available. Each child that resulted from Family 500+, in the years from the Polish financial-bonus scheme’s introduction in 2016 to 2019, cost $1m. In France each extra child over the past decade has cost twice that.” so…it ain’t money
male economists remain incapable of understanding parenthood: “Gary Becker, a Nobel-prizewinning economist, suggested in the 1960s that the best way to consider children is as goods that parents purchase according to how many they can afford, both in terms of time and money. Easing the burden of a career and expanding household budgets should therefore boost childbearing, he concluded.” 😒
drop of fertility is bc we functionally fixed teenage pregnancy (for now): “More than half the drop in America’s total fertility rate is explained by women under the age of 19 now having next to no children. Around a third of the missing births would have been unplanned, and the majority of them would have been to women on low incomes. . . . “Similarly, in Britain women born in 2000 had half as many children before they were 20 as those born in 1990. Unlike their rich counterparts, these women will probably not compensate by having more children later in life.”
maybe women just don’t want kids!: “Meanwhile, there is little evidence that middle-class women wish they had many more children, which would at least suggest they might be open to official persuasion. Today, at the age of 24, college-educated American women want on average 2.2 children—roughly as many as previous generations. They will now have these children a little later than before, with the first arriving at the age of 30, compared with 28 in 2000. Although trends suggest that they will fall short of their ideal family size, the gap may be the same as for women in previous generations, who missed the target by an average of 0.25 children.”
“[S]ome programmes are now beginning to explicitly target [low income and/or younger women]. Zhejiang, a province on China’s eastern border, is offering newly married couples a lump sum, but only if the bride is below the age of 25. In Russia women who have a child before they turn 25 will soon be exempt from income tax. Hungary offers a similar benefit to mothers who have their first child before 30—one of only two policies in Viktor Orban’s pro-natal push that economists at the Central European University think has created additional births. Although small families are becoming more common almost everywhere, women who start young still tend to have more children over their lifetime, which is why Messrs Orban, Putin and Xi are focusing on them.” nightmare blunt rotation
“young mothers laugh when asked if $7,500 would be enough of an incentive to encourage them to have another child; after all, low-income American households typically spend $20,000 in a baby’s first year of life. But such money may well have an impact at the margin. As one mother puts it, extra cash “might make me keep one I wasn’t sure I was going to have”. In America poor women are much more likely than middle-class women to cite financial hardship as a reason for an abortion.” cool society we live in
can we please built a society that doesn’t depend on women having children they don’t want: “extra children produced by targeted policies will probably not turn into the productivity-boosting professionals that governments most desire. Only 8% of the children of American-born non-college-educated parents are themselves expected to obtain a bachelor’s degree, and during his or her adult life the average high-school graduate boosts the public finances by less than a tenth of the net contribution of a college graduate. Therefore the financial benefits of pro-natal policies aimed at working-class women would probably be overwhelmed by their costs, given the expense associated with even well-targeted programmes.”
see also: “A first-time American mother in her mid-30s will earn more than twice what she would have earned had she had her first child aged 22. Women who give birth aged 15 to 19 are more likely to develop health problems; their first child is more likely to drop out of high school and to grow up without having both parents at home. In Flint many mothers express regret that they did not manage to “get things sorted” before they started to have children. “Hang on,” says one outside a community centre. “The idea is that I get paid just enough to make me have another kid? But that’s all that changes? Where doing it [raising a kid] right, later on, it’s all me? That doesn’t seem right.” The 26-year-old mother of three leans back, and laughs.”
anyway

2K notes
·
View notes
Photo
Based on this (x). Conclusion: they’re still fuckers.
73K notes
·
View notes
Text
I think this is just a trend everywhere but I've been very frustrated this week by how much admin work is being outsourced to me as the patient/customer.
My orthodontist tells me I can make an appointment with the surgeon. I call the surgeon. They tell me I need a new referral. I call the orthodontist. They do a referral. I call the surgeon. Referral didn't come through. They tell me about their special unique system we have to use. I call the ortho again and walk them through the referral. I call the surgeon. They say the referral was missing some details so they have to do it again. I call the ortho.
The insurance company calls me about repair shops. I give them the name of the repair shop which I already gave them yesterday. They say they're not in their system but I can use them, but I have to call the repair shop to ask them to contact the insurance company. I call the repair shop and they say the insurance company is supposed to email them.
I feel like at a certain point these constant fetch quests become unreasonable?? Is it too much to expect these groups to communicate with each other instead of making me run back and forth between them???
25K notes
·
View notes
Text
That article where a law professor argues that battered women are morally entitled to kill their abusers has an interesting quote: “ Men can kill women with their bare hands, and they do. Women almost never kill men that way. They can’t. […] While very few women kill abusive men who are asleep or passed out, it’s “unfair” to charge them with first degree murder, Sheehy argues. “It’s not fair to characterize it as the most heinous form of murder, because it may be their own route to survival. ” There have probably been feminist analyses of this already, but it’s worth discussing how the concept of self-defence, especially in domestic violence cases, was designed by men to benefit men. In my country at least, your attack is only considered “legitimate self-defence” if it is a) necessary, b) immediate, c) proportionate. A concept of self-defence that only applies if you hurt or kill someone while they are attacking you, and if you hurt or kill them using the same weapons as them (your bare hands, if that’s what they are using) only benefits people who are likely to be attacked by people of similar size and physical strength, and is utterly useless to women.
When a bigger, stronger male beats up his much smaller wife, it’s almost impossible for her to kill him in self-defence (immediately and proportionately ie with nothing but her fists), and yet it’s the scenario through which she can hope to be acquitted or get a light sentence. That’s not a coincidence. The other two scenarios (and she will be despised if she picks either) are for her to 1) kill him later (when he can’t use his physical advantage, eg when he’s asleep or has his back turned on her), but it won’t be self-defence because it won’t be immediate. (In the Jacqueline Sauvage case, one of the main arguments against her was that she shot her husband in the back at a time when he wasn’t actively beating her up) 2) use a weapon, but it won’t be self-defence because it won’t be proportionate. Obviously this condition also benefits men, because when a woman gets punched by her husband and she punches him back, it’s seen as a proportionate response but it shouldn’t be, because her punch (typically) won’t do nearly as much damage as his. Anything else she does (like use a weapon) to try and hurt him as much as he hurt her will be considered a disproportionate response and will mean it wasn’t self-defence.
The idea that killing your abuser in a honest face-to-face fight with your bare hands is honourable and forgivable, but killing your abuser in any other way is shameful and wrong, utterly benefits men and protects men. It’s also why poison was historically reviled as a ‘female weapon’ and as the most cowardly way to kill someone. Poison has been described as “a great equalizer” - no wonder men hated it. Men have always hated, and will keep hating, shaming, and outlawing, any form of attack through which women can compensate our disadvantage in strength and size, and they will keep praising as the only valid method of self-defence, the method that presents the smallest risk of being effectively used by women against them.
24K notes
·
View notes
Text
«I was managing a rape centre back in 2013 when it became apparent to me that almost every woman on our caseload and waiting list had been told that she had borderline personality disorder, within months of disclosing or reporting sexual violence. Many of them were put on a cocktail of different medications and were then subjected to all sorts of maltreatment and discrimination as a ‘borderline’ patient.
Unfortunately, borderline personality disorder is one of the most harmful diagnoses a woman can be given, as she will be reframed as a manipulative, deceitful and emotionally unstable person.
This is why women with borderline personality disorders are often ‘flagged’ to health and emergency services without their knowledge. Many GP surgeries flag a female patient with borderline personality disorder as a high-risk person; as do ambulance services, fire services, police services and social services. What this means in reality is that women and girls with this diagnosis can be treated as if they are unstable, unreliable or exaggerating when they call emergency services for help.
It appears then, that instead of addressing the enormous and complex traumas of women and girls subjected to male violence, there is a strong culture of diagnosing them with mental disorders and encouraging them to take daily medication. One of the most damaging impacts of this practice is the subsequent internalisation of self-blame and self-doubt for women and girls who are told that their trauma responses and coping mechanisms are not valid or relevant, instead, they are mentally ill due to some form of ‘disorder’, or ‘imbalance’, or ‘faulty genes’.
Borderline personality disorder in women has earned its place as the modern-day ‘hysteria’. Women and teen girls are the majority of people diagnosed with it, the criteria are as loose as the professional needs or wants them to be, and it results in years of medication, discrimination and treatment.
Once diagnosed with a personality disorder, you can only ever be in ‘remission’ but never ‘cured’. When and if you struggle again, it is seen as evidence that you have ‘relapsed’. How does a woman or girl ever escape this diagnosis when the language and theory is so circular?»
- Sexy But Psycho: How the Patriarchy Uses Women’s Trauma Against Them by Jessica Taylor
3K notes
·
View notes
Text
GOOD NEWS GYNS
A potential cause for endometriosis has been found, called fusobacterium
In the study, mice with the bacteria were able to be treated successfully with an antibiotic and it massively lowered quantity and severity of endometrial lesions
The bacteria was found in most women w endo that were tested, compared to 10% of women without endo.
FINALLY, good news in women’s healthcare!
Hopefully only a few years out from an actual treatment for endometriosis!
Link to the study:
3K notes
·
View notes