
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by nondu21 and here's what we found interesting.
Average Info
Notes Per Post
1
Likes Per Post
1
Reblog Per Post
0
Reply Per Post
0
Time Between Posts
1 month
Number of Posts By Type
Text
11
Last Seen Tumblr Blogs




Fun Fact
The most popular pages on Tumblr are about Minecraft, GIFs, and David J. Peterson.
Text
An Occupational Therapist for The People Not to The People:
Community no longer describes the place that I am found in. Community is the experiences of people around me, from the ladies on the bus that have carried me through this journey, to the women I encounter daily at the clinic then to the man I will encounter once in a lifetime. I within myself am a construct of community. A community of faults with thoughts and positions that require refining, mindsets that require strengthening & magnifying. There is so much unlearning and unpacking that I have been subjected to move from the bare minimum mindset that I subconsciously fallen in to moving to a sense of urgency that much like Kenville itself requires. To become an ACTIVIST of health and a FEMINIST of life. Its similar to being born again and the beauty of it is that you may stumble and fall but we are all born resilient.

[Retreived from google, 28 May 2020]
Resilience is not rare gem that is sacred and hard to find but difficult to maintain. One of my biggest lessons during my practice at Kenville is that being resilient is key. In my second week at Kenville, I had felt immense pain and fatigue from my annual visits of mother nature. I allowed the pain to consume me, my thoughts and my actions that guide my performance. This resulted in a wasted day. I could have seen more patients. Imparted better knowledge for the youth development. Interacted better with my team. And been the best version of myself. The sad reality is that as occupational therapist we are not at leisure of allowing our personal occurrences to affect us. These communities need us on our best days and on our worst days for the betterment of their lives. There is no time for excuses we need to make best of the little time we have with them.

[Retrieved from google, 28 May 2021]
Community has been an eye-opening experience to how uninformed I am about gravity of the challenges people are experiencing. The privilege that I have born into has given me the academic knowledge of how factors such as HIV/AIDS, Poverty, Apartheid and Unemployment affect our societies, or so I thought. Being interwoven into the community has shown me how the minds of the people of the community are still oppressed. While observing my Caucasian colleague of mine give a health promotion speech the people scoffed and refused to listen claiming not knowing the language. Before I began to translate, I found that indeed they understood her but would not speak English simply because they did not want to feel suppressed in the safety of their community. That in itself shows the long-lasting effects of the apartheid regime and how it has wounded the people in ways that cannot be undone but has further disadvantaged them in their thinking and positionality. English is a universal language that will provide them so many more opportunities and not merely the language of the oppressor. Also, they had missed the point of the health promotion speech and further implicated on their poor health seeking behaviour. This indicated to me that the mindset of these people require a shift and for that to occur there needed to be a shift in a way in which I approached the community and its individuals. This has pushed me to improve on my own health promotion speeches to make them more engaging and relatable to the people and to challenge the community members about negative behaviour.
This shift of mindset internally within me is not easy. I am a creature of habit (unproductive habits to say the least) and the one thing about community is that there is no such thing as routine or gold standard. It is everchanging and dynamic construct. One needs to be critically reflective of oneself continuously and flexible to the needs of each individual whether it be the clients we see, the nurse I am advocating to for my client and the security guard rushing to help whenever he can. Occupational therapists wear many masks and need to adapt to their environment much like a chameleon. Which is quite ironic because we spend so much of our time unmasking individuals’ behaviours, to unmasks the injustices faced by those individuals and to unravel systems that are put in place. We are a distinguished profession that achieves the solution to these issues through advocating for our clients, problem solving through creative intervention (Oven,2020) and breaking stereotypes of what health practitioners should be like.
The job that we do is not pretty, it is messy and complicated much like the lives we encounter at Kenville. What makes us more unique is that we understand the live hoods of the people we are servicing for and their context within a third world country making us humanists before being therapists (Hunt,2008). First world country policies do not work for us, we are obliged to go beyond the ‘boarders’ and even to ask ourselves if the boarders placed are even necessary? We are Occupational therapists for the people not to the people. For instance, a young man who works in Joburg due to decreased job opportunities in Durban presented with many psychosocial issues felt inspired by my speech to open up about what had occurred in his life and seek assistance. He was honest about how referring to someone else would result in him not attending therapy, even though he wishes to continue therapy, this requires a flexibility in my thinking. What alternative methods can I use to ensure this young man receives the therapy he deserves? What ‘boarders’ can I cross? Can I possibly move him to a zoom platform for intervention during my practice hours? These are all question that need to be pacing through my mind. With critical thinking and analysis, we are able to fully analyse individuals in a wholistic way from their client factors, to the political implications on their lives and occupational choices. This is what makes us client-centred in a community setting.
There is still so much left for me to experience at Kenville. Barriers of my mindset that require refining. I am here to fully experience the morphing and changes that will result in a therapist that goes beyond the norm for her clients. An activist of health and feminist of life.
Reference List:
Hunt, M. R. (2008). Ethics beyond borders: how health professionals experience ethics in humanitarian assistance and development work. Developing World Bioethics, 8(2), 59-69.
[Image] Retrieved from https://www.google.com/url?sa=i&url=https%3A%2F%2Fbayart.org%2Fexcuses-quotes%2F&psig=AOvVaw0u10o33A4ODKMPO6HVgphq&ust=1622305647277000&source=images&cd=vfe&ved=0CAIQjRxqFwoTCNjO99Dl7PACFQAAAAAdAAAAABAD
[Image]Retrieved from https://www.google.com/url?sa=i&url=https%3A%2F%2Fhome.hellodriven.com%2F50-resilience-quotes.html&psig=AOvVaw2MEOpvyCDq2iRgZUKVKZkY&ust=1622304287422000&source=images&cd=vfe&ved=0CAIQjRxqFwoTCMiwr8jg7PACFQAAAAAdAAAAABAD
Oven, A., & Lobe, B. (2020). Creative occupational therapist: It's about the client using focus groups to explore creativity in occupational therapy. The Journal of Creative Behavior, 54(1), 51-61.
0 notes
Text
The Significant Role of Occupational Therapy in the implementation of Sustainable Development Goals in Low Economical Communities
As I ventured deep into the community, I encountered idle women, gazing at their children who are wandering on the streets instead of the enriching knowledge of their books. Young healthy men meeting at the same shelter daily to sit and discuss sweet nothings and within the shanty town the sickly elderly stowed away to care for the young that have fallen victim to the system. Why are South Africans continuously falling into the cracks? Are the “regulations” of Sustainable Goal Development that government has set in place really serving the people or decorative measures? How do we as Occupational Therapists fit into the grand scheme of things?
Sustainable Development Goals are interconnected goals that are aimed to improve on the economic growth, health wellbeing and protection of the environment (Pradhan et al., 2017). These goals were formulated by the United Nations to have a united front to resist the everchanging and increasing issues that are arising within the world. However, we find that the implementation of these goals especially on a local level is not often as simple and straight forward as written down on paper. And that the implementation of these SDGs into communities is often poorly constructed for the community and contextually unsustainable. Therefor there is a gap for occupational therapy due to our “focus and knowledge” (Wagman et al.,2020) to work within the communities as we have an in-depth understanding of human occupation, contextual factors impacting t aton individuals and how individuals are integrated and form their community. At Kenville Community we have implemented programmes that are sustainable that will empower the community aligned with 5 of the goals of outlined in the SDG. Below we will discuss how we met these goals through projects and interventions we conduct at the clinic.
("PAGE and the Sustainable Development Goals | PAGE", 2021)
Goal 2: Zero Hunger
This SGD is directed in ensuring food security, nutritional food, and sustainable food systems for all people within the world. However, we find that there is difficulty in achieving this goal because of way in which food is produced and consumed in the globe ( Franzo, 2019). We have a gardening project placed at Kenville whereby community members are encouraged to cultivate the crops that are planted. In reward for taking care of the gardening they are also able to take fresh produce home. This project not only provides them with organic foods that are not processed but also providing the community with farming skills. This is a very important skill that can be carried out throughout their lives. This will aid in alleviating the financial difficulties that members of this community face.
Goal 3: Good Health and Well Being
This SDG is aimed to “ensure healthy lives and promote well-being for all at all ages” (Micah,2020) This we achieve through providing health promotion talks at the clinic to provide the clients with an increase understanding of what health is. As defined as Who health promotion “enables people to increase control over their own health. It covers a wide range of social and environmental interventions that are designed to benefit and protect individual people’s health and quality of life by addressing and preventing the root causes of ill health, not just focusing on treatment and cure.”( WHO as cited in "Defining Health Promotion and Disease Prevention - RHIhub Toolkit", 2018) We highlight health issues that are prevalent such of HIV/AIDS, TB, Malaria, Pneumonia, COVID 19 etc to bring awareness and reinstate the importance of prevention of the spread of these illnesses. We have designated weeks to speak about each issue comprehensively. We also focus on issues that communities especially of color do not view as ‘health issues’ pertaining to mental health and mental health (depression, anxiety and stress). This is especially important in our one-on-one interventions to highlight mental health especially in mothers. We speak to mothers about the importance of self-care and invite them to maternal health groups that can provide them with strategies to cope with motherhood and being individuals.
Goal 4: Quality education
In South Africa we have a constitution that stresses that we all have the right to education.We aid in the achievement of this goal through providing intervention at different scholastic levels. At Kenville we attend creches and aid in supplying the owners with materials that stimulate prerequisite scholastic skills kids for the children. Such as engagement in fine motor skills that improve on their ability to write, sensory stimulation and Cognitive stimulation to improve the children’s skills in memory, following instructions and basic concepts like counting and reciting alphabets. We also screen for developmental milestones in children to aid in the children meeting the level that his/her peers are on. We also intervene in primary school to screen for difficulties in scholastic performance to see if the child can competently compete against those in his grades. We look at handwriting skills, visual perceptual skills, and social skills to find areas to assist the child in improving on. We also work hand in hand with teachers by giving comprehensive feedback and what the teachers can apply in the classroom specifically for that child’s needs in order for them to compete with children in their class. We also work with the youth development at the Sea Cow Lake high school. We provide the children with study strategies in conjunction with other topics that are prevalent within their society. Due to occupational therapists deep understanding on human performance and skills we are able to identify intrinsic issues that teachers are not skilled in identifying. This way children receive a well catered for education that is sensitive to their needs. At the school we also provided the students with education on varsity and how to apply at a university level we aim to encourage continued learning for individuals for improved occupational performance in all stages of their life.
Goal 5 Gender inequality
As noted in my previous blogs beforehand that there is still a huge a between females and males in our country due to a system of patriarchy that is persistent within our society. We at Kenville aim to combat gender inequality by speaking out on these issues when we view them both within and outside the clinic. This way we are fixing the views and perspectives on a large spectrum. We also have programmes such as the KITE programme (a women empowerment programme) that aim to bridge the financial difficulty that women are encountering by employing them and providing them with entrepreneur skills that would not be exposed to otherwise.
Goal 8 Decent work and economical growth
The beauty of the KITE project mentioned above is the dynamic function as it aids in alleviating the eighth SDG aimed at providing inclusive work and providing economic growth within communities for all (Rai, 2019). We are able to provide women within the society that are prone to having higher numbers of unemployment in the community to alleviate the burden of unemployment. However, I did find that due to little exposure to work the women often have no understanding of job requirements and ethical practice this project will definitely aid in the base line vocational training of the women. We also are planning to re-implement a Jumbo tyre project to train women to make equipment from the tyres. This will also aid in improving skills that they can utilise in other jobs such as in factories etc.
As noted above we do not merely provide projects that are therapist directed but our scope of practice ensures that there is a learning of skill so that individuals are self-sustaining. So that even if the projects at Kenville fall through or government is unable to provide, they are able to take what they have learnt and apply it in different settings and contexts. That is the crux of our practice is to enable and empower individuals and to remove the crutches that obstruct them from their growth and independence.
Reference Lisit:
Defining Health Promotion and Disease Prevention - RHIhub Toolkit. (2018). Retrieved 21 May 2021, from https://www.ruralhealthinfo.org/toolkits/health-promotion/1/definition
Fanzo, J. (2019). Healthy and sustainable diets and food systems: the key to achieving sustainable development goal 2?. Food ethics, 4(2), 159-174.
Micah, A. E., Su, Y., Bachmeier, S. D., Chapin, A., Cogswell, I. E., Crosby, S. W., ... & Moghadaszadeh, M. (2020). Health sector spending and spending on HIV/AIDS, tuberculosis, and malaria, and development assistance for health: progress towards Sustainable Development Goal 3. The Lancet, 396(10252), 693-724.
PAGE and the Sustainable Development Goals | PAGE. (2021). Retrieved 21 May 2021, from https://www.un-page.org/page-and-sustainable-development-goals
Pradhan, P., Costa, L., Rybski, D., Lucht, W., & Kropp, J. P. (2017). A systematic study of sustainable development goal (SDG) interactions. Earth's Future, 5(11), 1169-1179.
Rai, S. M., Brown, B. D., & Ruwanpura, K. N. (2019). SDG 8: Decent work and economic growth–A gendered analysis. World Development, 113, 368-380.
Wagman, P., Johansson, A., Jansson, I., Lygnegård, F., Edström, E., Björklund Carlstedt, A., ... & Fristedt, S. (2020). Making sustainability in occupational therapy visible by relating to the Agenda 2030 goals–A case description of a Swedish university. World Federation of Occupational Therapists Bulletin, 76(1), 7-14.
0 notes
Text
Understanding positionality and its affects both personally and professionally
As a young black female Christian woman growing up in a country full of great diversity and therefor mass adversity to my perspectives and approaches to life, it was important for me to develop a standpoint. This is better known as positionality which is ones social and political context that creates their identity in terms of race, class, gender, and sexuality (Dictionary,2018). Our “standpoint/positionalities” guides our outlook on life and subsequently unknowingly formulating prejudices. Now what happens when you’re a practicing or training health practitioner with prejudices and preconceptions in a country of great diversity? What domino affects occur? Most importantly when does unlearning of these perspectives begin?
My mother was the typical “imbokodo” (stone used to describe women in South Africa for their strength and perseverance) having educated herself despite her father’s objections, worked, brought up her children, kept her home and left a marriage that was of no benefit to both parties despite ridicule from family and neighbours. She was the epitome of a feminist and as you can assume this attribute was passed onto me from the very milk that I breastfed upon. My mother’s experiences taught me a great first lesson that another individual and their opinions are valid and accepted in life but are not by any means your measure of success, map to life and key to happiness. In my quest to be self-efficient and independent I found that I had developed a lack of empathy towards women who actively chose to remain in none mutually beneficial relationships. Recently while talking to an elderly Mr R, at Kenville I realised that patriarchy is a system so imbedded within our society that it takes years of being subjected to inequalities and unlearning before females stand up against it, and in Mrs R it took seven to be exact. As a maturing health practitioner, it was important for me to understand that often one’s positionality can in fact change, most importantly through guidance and understanding.
While on the topic of patriarchy I was recently engaged in a conversation on a bus ride to clinical practical’s in with my peers, I quickly found that we didn’t all share the sentiments towards feminism. While in my state of dismay, I found enlightenment through their well rationale reason that our new generation of women and male no longer accompany patriarchy with misogyny. Patriarchy although a system that puts men in a state of power and control and a thorn to the development and prosperity of feminism (Acker,1898), is not always parallel with misogyny, rather it was argued that misogyny a system built on sexism that undermines women that was practiced by most men in patriarchy. It is not a prerequisite of patriarchy rather a product of poor constructed patriarchy. The new generation allows patriarchy to function based on the four conditions: considering the male has good leadership qualities, clear communication occurs between both female and male, both parties shared similar political and religious beliefs to prevent imposed ideologies on a certain partner and most importantly when the women willingly submits herself as a under the male’s dominion (a concept often highlighted in the Bible and as I Christian grapple with). Although I may not identify with them and the stubborn voice in my head screams ‘brainwashed’, it is noteworthy that these young women were raised in similar homes as me and had equal academic opportunities as me and had thought well about their opinions and positionality. There are moments to speak out and fight for your stances and moments of recognising and understanding differences especially when one’s rights are not implicated upon.
(Lorde, 1980) An image holding the quote of famous feminist and activist Audre Lorde which highlights the importance of accepting differences.
Much like my father I have always had a strong sense of nationality and pride a blessing and a curse. My father’s family who are actually of Swati decent now identify as Zulu after years of having settled in Ngwavuma an area in KZN close to the eSwatini Boarder as means of survival they adopted There is a strong conform or begone culture in South Africans. For example, I feel strongly that South Africa is economically incapable of taking care of its citizens and burdened by the increased number of foreign nationals that have settled. Such a statement resulted in a heated argument between myself and my Angolan friend. I think our positionality politically should not necessarily affect our behaviour. For instance, I am against xenophobia which South Africa has an increased rate of xenophobia especially post 1994. The dynamic relationship between human rights, xenophobia and migration in South Africa highlights the issue of South Africans insensitivity considering our own racial segregation that we have just recovered from (Crush, 2001).At Kenville cultural sensitivity and confidentiality is important as we have been notified of the xenophobic attacks that have occurred the previous year. My political stance has no implication on my ability to give comprehensive treatment to all, and I will do so with great appreciation. The factors impacting on our positionality affect only our positionality and not each other.
An image that reflects factors that impact on positionality.
My love for my people and improvement of their livehoods is one of the many driving forces of why I chose Occupational Therapy a degree unknown commonly by people of colour who often experience occupational deprivation due to prejudices that certain occupations are “for white people” such sayings are engrained into our thoughts from a young age and creates backward societies. While on practical’s my supervisor said something that really stuck out to me in my first week that we should have an engaging toy outside for the children to play on, a thought quickly popped into my head questioning if we were allowed to do that? This highlighted the issue that as children of colour we are raised to be quiet and to blend in, falling into the background. But why is this still a prerequisite skill post-apartheid South Africa? The problem with these simple disciplinary sayings is that by saying that we should be quiet and fit in we have a young generation that does what is expected of them and not what is required of them, does not fight the system in order to be accepted by a system that is meant to serve them. In our community block we are expected to question the system, create chaos, a chaos that advocates for change. Which I am still gaining confidence in speaking against broken systems that no longer serve their purpose.
At Kenville we look at an individual as a single construct because we understand that in and outside of their immigrant stuts, political views, gender and social construct they are first an individual. Equal with every right to comprehensive health. We understand that these factors may have impacted them in some way and have led to the circumstances that they are experiencing but that their positionality is changeable. We can utilise maternal health groups, health promotion talks, active aging groups and empowering projects like the KITE project to facilitate a shift in their mindset and outlook in life. But this is only achieved through them experiencing this first hand. Which is why we aim to be consistent in our engagement and improvement of the Kenville community.
What I would like to close with is to know when your positionality is valid or invalid to create change. To be an individual that is willing to be educated by life experiences to develop your own thinking and conceptualisation of the world. We are all individuals on a journey called life with different destinations and at any point in time your position may change drastically and once ignorance arises flee that place of comfort and allow for your mind to be renewed. Nothing grows in a shady area except raspberries and plums. In a world full of raspberries and plums be rather be a strawberry.
Reference list
Acker, J. (1989). The problem with patriarchy. Sociology, 23(2), 235-240.
Lorde, A.(1980) Age, Race, Class and Sex: Women Redefining Difference,.Retreived from: https://www.colorado.edu/odece/sites/default/files/attached-files/rba09-sb4converted_8.pdf
Crush, J. (2001). The dark side of democracy: Migration, xenophobia, and human rights in South Africa. International migration, 38(6), 103-133.
What's Positionality & What Does It Have to Do With You? (2021). Retrieved 14 May 2021, from https://www.dictionary.com/e/gender-sexuality/positionality/
Writing Strategies: What’s Your Positionality? (2019). Retrieved 14 May 2021, from https://weingartenlrc.wordpress.com/2017/01/09/research-writing-whats-your-positionality/
0 notes
Text
Unraveling Maternal and Child Health within the Multilateral Challenges of the South African Society and the Intricate Role Occuptional Therapy Has.
Maternal health and child health is a delicate and intricate topic that is often overlooked especially in the context of South Africa whereby there is a general lack of understanding and acknowledgement of health concerning mother and child. As defined by WHO “Maternal health refers to the health of women during pregnancy, childbirth and the postnatal period. Each stage should be a positive experience, ensuring women and their babies reach their full potential for health and well-being”. WHO (2021)
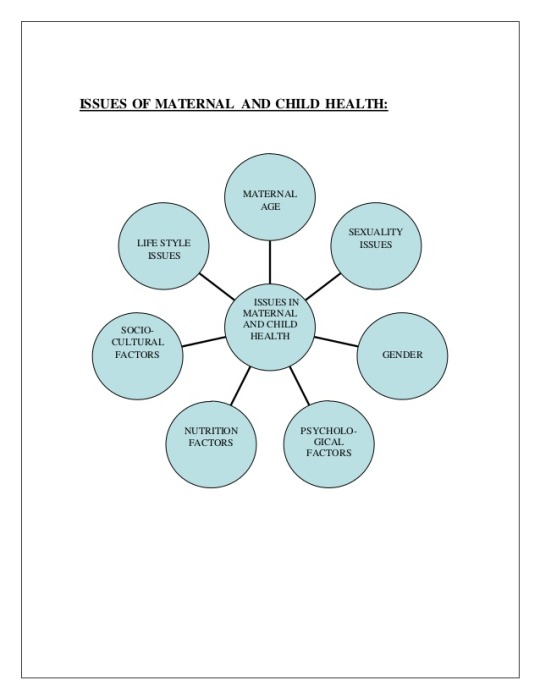
We need to unravel factors that hinder maternal health and child health in a South African context to better understand and navigate this topic. One of the first issues which include gender issues an increased appreciation or discrimination of a child based on them either being a boy or girl child. Jhinjar (2019) We find that fathers will neglect or deny children that are female as they do not add “value” to the family. This links into the socio-cultural issues in South Africa whereby we are still experiencing a society of patriarchy whereby women are dependent on partners for financial resources. Therefore, limiting the mother’s access to health care during pregnancy and after childbirth, if the partner does not value medical health care. Another factor in maternal and child health is the decreased deliverance of proficient primary health specifically in childbirth of lower economical individuals due to poor work attitude of staff, poor emergency responses, and poor services at the facility level that result in traumatic childbirth for both the mother and the baby. Lumbini (2018)
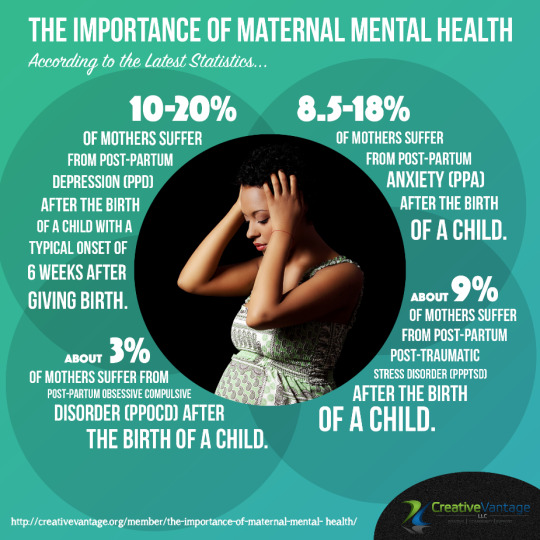
(Image from: http://creativevantage.org/member/the-importance-of-maternal-mental-health/)
An arising issue resulting from overtly dominant males is gender-based violence as noted in a study that women in such controlled relationships who are intimate with males that are HIV positive are at a high risk of HIV infection. Dunkle et al (2004). This also puts the child at risk of infection during pregnancy and complications in pregnancy such as early labour, injury to the foetus upon impact. Resulting in a child with cognitive dysfunction or developmental delays which decreases their future quality of life and independence in their community. Lifestyle conjunction with poor nutrition issues whereby women are partaking in unhealthy habits such as smoking, eating non-nutritional food during and after pregnancy and supplying the child with inadequate nutrition. Also is expected to take care of household chores independently during this time (unequal gender roles Resulting in them neglecting care for themselves and the unborn child. Lastly, it is important to understand that all of the above factors consequently result in a poor mental state of the mother.
One may find themselves perplexed or powerless with the factors mentioned above, possibly saying to oneself “where to from here”, “what is the solution to these issues”. This is why we have multifaceted professions such as Occupational Therapists to help address these issues and advocate for change.
Occupational Therapy has an intricate role to play in the education and promotion of maternal and child health. At Kenville clinic we work at a community-based level whereby we have shifted from traditional medical-based intervention to more family orientated/centred approaches. Washington (2009) This assists in formulating appropriate and realistic intervention for the mother and child that they can carry over into their everyday life. We have gaged a huge opportunity, as there is an increased number of pregnant women, as well as mothers with children of different ages attending the clinic. The main focus was to promote and educate mothers at the clinic about what exactly maternal health is and building a sense of understanding and trust with the therapist. As noted in some literature that “the mother-therapist relationship and effective communication are essential components in fostering perceived confidence and competence of family members". Washington (2009). A reoccurring issue is that mothers were often resistant to come to therapy as they did not want to lose their line as well as having health promotion speeches that weren’t as impactful or informative as they should be. This is an important area of improvement for me as a therapist.
Another important role that occupational therapists play is to screen children for any developmental delays alongside the mom present and to investigate the mother for any psychological determinates/mental state. Maternal mental health is very important in maternal health and child health during and post-pregnancy. At the clinic, we encourage the importance of pregnant women to communicate with nurses during childbirth when they feel they are experiencing extreme pain, complications, or prolonged labor to prevent injury to themselves or the child. We also highlight the importance of the mother to care for her personal needs as an individual during and post-pregnancy. Therapists and mothers discuss issues that are worrisome such as financial struggles, poor family support systems, and mental health issues. Strategies are discussed among themselves s such as self-care days: reflecting on what is going on around them, partaking in activities that enrich them as individuals: communicating with having family members or partners about assisting in childcare when they are feeling overwhelmed or exhausted. An initiative that is implemented at Kenville is a Moms and Tots Group in conjunction with Maternal Health Group, that will aid in uplifting mothers in their confidence in positively stimulating their children in their development and simultaneously being aware of their self-care. Important topics will be discussed about financial stability, lifestyle changes, assertiveness, roles at home to provoke mothers into thinking, and identifying issues that are presented and strategies to implement. Encouraging women that don’t focus on their negatives, but that problem solve and tackle their issues head-on. Such as the KITE project that creates job opportunities for mothers to sell second-hand clothes to the community, to encourage self-sufficiency and some financial enrichment. It warmed my heart to hear Miss X (a member of the KITE project) say, " The money that I make here, although it may be small for some makes me feel empowered, I can buy bread, clothes for my children, and even lend my husband money when he goes to work. Waking up in the morning and standing at these stalls helps me focus on my future and not the problems that I cannot fix". As occupational therapists this music to our ears as our main object is for individuals to participate in meaningful occupations. Lastly but certainly not least is to look at family constructs and helping mothers to have healthy homes whereby all family members feel accepted and acknowledged. In one of my recent cases, I had overlooked the dynamics of a newborn and its effects on a child that is present. My supervisor enlightened the mother on issues that may arise ad coping strategies such as ensuring mothers engages their older children to feel important and cared for, for good self-esteem. Child health matters for both the children that we see and the ones we do not encounter.
So, you may be asking yourself “this is informative but where to from here” or “what am I to do”. It’s simple. Care enough. Enough to spread the word about maternal health and child health in a society that overlooks women and children's needs. To help build a society and systems that care deeply for mothers who carry the future of our society first in their wombs and later in their hearts. Fostering a cluster of women who are empowered, in charge, and changing their narrative for both themselves and their children.
Reference List:
Dunkle, K. L., Jewkes, R. K., Brown, H. C., Gray, G. E., McIntryre, J. A., & Harlow, S. D. (2004). Gender-based violence, relationship power, and risk of HIV infection in women attending antenatal clinics in South Africa. The Lancet, 363(9419), 1415-1421.
Lembani, M., de Pinho, H., Delobelle, P., Zarowsky, C., Mathole, T., & Ager, A. (2018). Understanding key drivers of performance in the provision of maternal health services in eastern cape, South Africa: a systems analysis using group model building. BMC health services research, 18(1), 1-12.
Prosper, I.(2015)Maternal Mental Health Care. Image Retrieved from: http://creativevantage.org/member/the-importance-of-maternal-mental-health/
Washington, K., & Schwartz, I. S. (1996). Maternal perceptions of the effects of physical and occupational therapy services on caregiving competency. Physical & Occupational Therapy in Pediatrics, 16(3), 33-54.
Image from: http://creativevantage.org/member/the-importance-of-maternal-mental-health/
0 notes
Text
Week 3 : Advice For Your Future Self
In my last blog I highlighted the importance of reflection on your performance as a student in health science.For today’s blog I will be using my reflection to give my future self some guide into how to carry themselves in their journey in occupational therapy as a student and as a therapist.
The first would be to plan.

Planning is an important aspect in our treatment in Occupational Therapy and the intricate thinking and shaping developed in making an activity that will define how therapeutic our sessions are. This includes making Plan A, B, C, D and maybe even E. This is because individuals are everchancing and patients often present differently on different days. Not only should this be applied in gradings of a write up but even the types of activities chosen to do with the client. If the client is objecting to an activity than their performance and participation will be futile and therefor make therapy tedious. By planning for multiple scenarios and interests for the client it allows therapy to be flexible and client centered.
The second would be to believe in myself .
“ The worst enemy to creativity is self doubt” (Path.S) Althought occupational therapy is scientifically based there is no doubting the creativity that goes into much of our therapy. Applying that creativity requires much self belief which often I have difficulties in harnessing. One of the main things I know I have to work on is my symptoms of imposter syndrome which is a psychological pattern in which an individual doubts their skills, talents or accomplishments and has a persistent internalized fear of being exposed as a "fraud". (Impostor syndrome, 2020) This stems for a lack of self belief. This can reflect in therapy sessions whereby sessions lose their meaning due to the therapist becoming too self aware, causing the session to become less client centered.
The third advice would be to communicate. It’s okay to ask for help.
Much like in my last blog communication is a lacking aspect in my approach to my learning. Such as reaching out to a members of my MDT, supervisosrs and lecturers regarding any confusion that I may be encountering in my sessions with my client. Being independent may be a blessing but as in any case too much of anything is unhealthy. Especially when it comes to treatment it is important to communicate information to people involved in the clients day to day life. This will be to ensure carry over of skills to the family members, facilitators and members of the MDT. Even through I have grown much more confident in asking for redirection there is always room for improvement.
Fourthly would be to say it’s okay to fail. As long as you keep trying.
Failing is one of the biggest fears of most individuals, but what I have learnt about failure is that it gives way to better thinking and revealing potential that you did not think was possible. Reflection one of my sessions that was a complete fail in my first block whereby the client could not partake in the activity because of the session was not set at his level and to my third block whereby the activity was not beneficial. Honestly these were the two occasions that I felt the most therapeutic for my clients. I planned a new session within five minutes that would meet the aims of my sessions and that the clients enjoyed. Had I not failed at my initial sessions I would not be aware of the potential that lies within and how much I actually knew and understood. Failure allowed me to grow in my self belief in my capabilities in my journey as a student in occupational therapy and my efficiency in planning sessions .( Which normally takes me a good two hours on a good day)

And last but not least. Have fun. Be passionate .
Although this is a cliche saying I feel that it fully summarizes my advice to my future self. When the rush of handing in case studies and write ups hit. The only thing that begins to matter is the marks. The passion is lost and blocks become boring and routine. Occupational Therapy is not just a scientific , exercise or diatic form of treatment. It is creative and uses enjoyable activities to provide treatment. Our main goal is always to ensure that the clients enjoy therapy in the same way this needs to be applied to myself. If as a therapist I don’t enjoy what I am doing clients can pick up on the negative energy which will affect their participation in therapy. Also losing passion in what I do will affect how affective I am in therapy and growing a positive and an excitement for therapy today will benefit me humiungously when I am working and there is no supervisor to check up on me.
To summarize it all in a short message to myself. Always put your best foot forward not to impress others but rather to impress and show respect to yourself.
Refrence List:
Encrypted-tbn0.gstatic.com. 2020. [online] Available at: <https://encrypted-tbn0.gstatic.com/images?q=tbn:ANd9GcQmRYU7FJPD00bxZXMOpYvFpjTGG9ZTogA_bQ&usqp=CAU> [Accessed 30 November 2020].
En.m.wikipedia.org. 2020. Impostor Syndrome. [online] Available at: <https://en.m.wikipedia.org/wiki/Impostor_syndrome> [Accessed 30 November 2020].
Encrypted-tbn0.gstatic.com. 2020. [online] Available at: <https://encrypted-tbn0.gstatic.com/images?q=tbn:ANd9GcROy6B73xCt755s3kVMUWkG6P9djFolSgM-HA&usqp=CAU> [Accessed 30 November 2020].
Goodreads.com. 2020. Self Doubt Quotes (198 Quotes). [online] Available at: <https://www.goodreads.com/quotes/tag/self-doubt> [Accessed 30 November 2020].
0 notes
Text
In A Nutshell. Coming Out Of Your Shell.
As in any approaching ending or conclusion of a process it is important to have a take away. Much like in Occupational Therapy it is important for the client to have grown out of disfunction into somewhat of functionality and independence, we as occupational therapy students need to move from our level knowledgeability and skills. And develop new fluidity and skill sets in our continuously everchanging profession.
A common mistake that I am guilty of is a stagnant approach in programme planning for my clients. in my last block there was much growth in my planning as I was pushed to use different frameworks , models and approaches for my clients as defined below the provide the backbone of treatment.
- Framework guides therapists in skilled observation by clearly identifying the domain of occupational therapy practice and outlining the occupational therapy process of evaluation, intervention, and outcome measurement (AOTA, 2014)
-The use of models provides structure and assists occupational therapists to produce proper, profession-specific, scientifically-based intervention.
Since every individual with an illness presents differently from next even if their diagnosis are the same. it is important for our treatment to be unique and to explore the different frameworks, programme and approaches to tailor suit it to the client. During my Virtua Case Studies both my clients were diagnosed with Depression and had a history of homelessness. However I used more of a rehabilitative programme for one client and more of the educational approach for the other as she presented on a higher cognitive function. This way the therapy planned would be beneficial to each individual. This experience has made me more confident in my skills in treatment planning.

The second aspect that I saw much growth in is my fear of communicating with my supervisors and speaking on areas that I find challenging. Shifting view of my supervisors from my adversary to my mentors. There is still much room for improvement in this area but i have taken a step forward in this area. There are countless benefits to this such as receiving validation on what you are doing right ( which is always great for my ego) as well as getting a push towards the right direction. Speaking to a trained professional also assists in cutting out unnecessary information that I would be digging through and focusing on as a student.
To conclude it all much potential has been explored and growth has been unlocked. In the wise words of Charles Schulz “ is no heavier burden than an unfulfilled potential.”
Reference List:
AOTA. (2019). Using the Occupational Therapy Practice Framework to Guide the Evaluation Process and Make Assessment Choices in School Practice [Ebook]. Retrieved from https://www.aota.org/~/media/Corporate/Files/Publications/CE-Articles/CE-Article-February-2019-Framework-School-Practice.pdf
https://emilysquotes.com/fear-is-a-thief-because-fear-robs-you-before-you-even-begin/(Image)
Sweatt, L. (2020). 15 Quotes to Inspire You to Reach Your Greatest Potential | SUCCESS. Retrieved 12 November 2020, from https://www.success.com/15-quotes-to-inspire-you-to-reach-your-greatest-potential/
Vermaak, M. E., & Nel, M. (2016). From paper to practice-academics and practitioners working together in enhancing the use of occupational therapy conceptual models. South African Journal of Occupational Therapy, 46(3), 35-40.
0 notes
Text
Covid 19 : Trick or Treat
Trick-or-treating is a traditional Halloween custom for children and adults in some countries.. “The "treat " is usually some form of candy, although in some cultures money is given instead. The "trick" refere to a threat, usually idle, to performa mischief on the homeowner(s) or their property if no treat is given. (Trick-or-treating, 2020) Similarly this Tradition and Covid 19 are present in all countries and varied amounts. As well as having brought people together and has lead to some discomfort and pain. This time has also revealed the ugly monsters and systems that have been put in this world dressed up as beautiful systems meant for all to flourish.
As an individual studying in a field that speaks of hope and views life occurrences as part of what makes us unique irregardless of whether it is good or bad , there is no doubt that for some this year has indeed been a half empty half full kind of a year.

(Is the glass half empty or half full?, 2020)
Many students have had to drop out of school due to financial constraints and others have had to continue school despite death of a family member because life keeps moving. The most beautiful thing about Covid 19 is that it brought us all to a stand still and gave us time to reflect on what we have , how far we have come, how far we want to go and how resilient we are.
University was definitely a combination of both trick and treat. Having been introduced to the concept of online learning which has revolutionized education as a whole. Allowing us to study from home. And very little time at practical venues. The repeated exposure to our patients made my clinal reasoning develope faster and probed for critical thinking- in a short span of time for the therapeutic benefit of my client . Skills sets such as observation , analysis interpretation , reflection , interference , explaination and problem solving. (2011-2020, 2020)
To admit online learning has been a blessing and curse in disguise . On one hand it has made education efficient and convenient but it has also resulted in longer days bed and a mind full of “ I will do it later”. The jump back into practicals assisted in reinforcing my schedule into place and refocusing my goals.
“Life is 10 percent what you make it and 90 percent how you take it “- Irving Berlin
Reference List :
Medium. 2020. Is The Glass Half Empty Or Half Full?. [online] Available at: <https://medium.com/cuble/is-the-glass-half-empty-or-half-full-72829ad44035> [Accessed 23 October 2020].
En.m.wikipedia.org. 2020. Trick-Or-Treating. [online] Available at: <https://en.m.wikipedia.org/wiki/Trick-or-treating> [Accessed 23 October 2020].
2011-2020, (., 2020. Critical Thinking | Skillsyouneed. [online] Skillsyouneed.com. Available at: <https://www.skillsyouneed.com/learn/critical-thinking.html> [Accessed 23 October 2020].
0 notes
Text
WEEK 2:
Two heads are better than one, no term could possibly better describe the treatment plan of a person. The treatment plan of a person is very intricate and well planned out. It needs to be a wholistic as possible yet specific to each need of the client. Therefore, the multidisciplinary team was formulated.
“A multidisciplinary team is a group of health care workers who are members of different disciplines (professions e.g. Psychiatrists, Social Workers, etc.), each providing specific services to the patient. The team members independently treat various issues a patient may have, focusing on the issues in which they specialise.” ("Multi-disciplinary team - HSE.ie", 2020). In this way the client is fully able to receive care to each need. The key principle for the multidisciplinary team to work is communication. There are two lines of communication that are commonly used in a hospital setting which is verbal and written communication. In my experience in hospital I have found that the easiest and most efficient way to communicate with other members of the multidisciplinary team is through the patient files. This file contains all the assessments done, plans and interventions done by each practitioner. This file has helped me in saving much time that I would have used going to the doctor to better understand the diagnosis, where I had all the information present for me on what the client’s comorbidities and main diagnosis. Giving more of my time to the client.

(An Image of the line involved in the multidisciplinary team)
However, it is important for the team to be on a verbal communication. Especially when liaising about the patient’s reaction to your sessions. I have found that the nurses are a very vital part of the multidisciplinary team. They spend the most time with the clients and have a clear picture of the client prior and post intervention. I found that my client was not eating all his food which contains the nutrients necessary in the recovery process. As the occupational therapist it was vital for me to communicate to the nurses the implications that came from the client not finishing his food. As well as personally requesting that they ensure that he does his ward exercise program every morning and night. This is also known as advocating which is to “speak or write in favour of; support or urge by argument; recommend publicly” as per Dictionary.com. The last responsibility that I play in the multidisciplinary team is when I hand a handover form of my assessments, interventions done and plans to the OT to take over after I leave. This is a written communication and the last step in caring for your client.
The carry over plan will you formulate will aid the remaining team member on what factors to focus on. It is important to give a prioritised precise step by step plan of what that is required. The weakest team player defines the strength and efficiency of the team.
Reference List:
Definition of advocating | Dictionary.com. (2020). Retrieved 22 July 2020, from https://www.dictionary.com/browse/advocating
Mickan SM. Evaluating the effectiveness of health care teams. Australian Health Review, 2005, 29(2):211–217.
MS Variance: The ‘co-ordinated multidisciplinary team meeting’ and what that term really means. (2020). [Image]. Retrieved from https://www.google.com/url?sa=i&url=https%3A%2F%2Fmultiplesclerosisacademy.org%2F2018%2F12%2F14%2Fthe-coordinated-multidisciplinary-team-meeting%2F&psig=AOvVaw3HrAHUlqaExCPdO1R8aPwM&ust=1595519935580000&source=images&cd=vfe&ved=0CAIQjRxqFwoTCPjynZGd4eoCFQAAAAAdAAAAABAD
Multi-disciplinary team - HSE.ie. (2020). Retrieved 22 July 2020, from https://www.hse.ie/eng/services/list/4/mental-health-services/dsc/communityservices/multidisciplinaryteam.html
0 notes
Text
Week 1 : Clinical Reasoning and Cultural Humility
Clinical reasoning is defined as the process used by the OT practitioners to understand the clients occupational needs , make decisions about intervention services ,and think about what we do.(Gates ,1992)
In my field block clinical reasoning has assisted me in formulating sessions and activities that tackle actual problem areas that the client may face. For example during practicals when dealing with a patient with a hand issue the patient is was wholistically screened for impairments in cognition, physical , emotional and environmental aspects. Then using the findings and the implications I would began to deal with the biggest issue which was remediating the hand skills lost post injury so the client can be independent in activities of daily living which is the most basic domain of OT . If the hand cannot be remediated then rehabilitative steps will be taken where the client will be trained to use assistive devices for the loss of function and maybe transferring hand dominance to the non dominant hand. It helped me in choosing the necessary steps to intervening and preventing me to haphazardly dismiss the clients hand totally. However I found that when dealing with Paeds there is much room for improvement in my clinical reading especially as this is my first experience in the block. My supervisor assisted me formulating meaningful sessions for the baby as she made me think deeper into the child’s developmental stages using Erickson’s stages’ of psychosocial development.

When dealing with the child I learnt that it is important to incooperate the mother into tasks as the child trusts her in order for the child to comply and warm up to me. As well as knowing to be flexible as a child is very unpredictable. Choosing activities that the baby will be willing to do but are overall therapeutic to her.
Another important aspect in occupational is Cultural Humilty/Cultural Sentitivity. Which is “defined bya lifelong-orientated approach to working with people with diverse cultural backgrounds and a recognition of power dynamics in health care” (Brown 1984)We live in a ethnically diverse culture that is ever changing. As a health practitioner one should be aware of cultural norms. Like when dealing with an adult male it is important to address them as sir or their surnames. As my client is Zulu when communicating with him I often refer to him as “baba” which is a Zulu for father but can be used in a professional way to address an older Zulu male. Also when presenting tasks I used Zulu to speak to him as well as translating the MOCA into Zulu as he is confident in it.
My first week of OT Feildwork has assisted in refining my skills as a student. It has given me experience that has grown me in my clinical practice to critically plan intervention. And ask myself why at each step.
Reference List:
Gates ,G.(1992).Clinical reasoning. Topics In Nutrition,7(3)74-80.doi:10
(2020).[Image].Retreived from https://in.pinterest.com/pin/77053843606015945/
Brow,G.(1984).Murray Kempton.Social Text,(9/10),280.doi:10.2307/4666563
0 notes
Text
Week 3 :Communication Skills
Communication is one of the most basic instincts of humans from birth a child’s innate nature is to show joy, discomfort or hunger through physical or verbal communication. As per the Transactional Model of communication ‘communication is the exchange of a message between sender and receiver where each takes turns to turn or receive messages’ .(Transactiomal Moddl of Communication -Businesstopia,2020) This basic concept is especially needed in the rehabilitation of a patient.
Therapists and doctors need to work together to form the multidisciplinary team and one of the main qualities of the efficiency of this team is communication.

These are the different lines involve in treatment of a patient. The most common way these practitioners liase is through patient files where they write client functional aspect to inform the next member of what to expect from the patient. They also comminicate through email, phone calls and meetings in the morning to prep the team .
In my experience at this hospital I have found it quiet hard to communicate verbally with other health practitioners mainly because the hospital is such a huge hospital and everyone has to be at different places with different patients. The patient files have assisted immensely in what doctors and other health care members need to voice about the client. However I’m up coming pracs I would like to have more in depth communication with the health team members as ( such as being present at the patient when the doctor does his rounds or assist the physiotherapist ) to improve my working relationship with them .
Then most importantly my communication with the client. Which is very vital in treatment. Having a good communication with the patient impacts therapy either negatively or positively. One communication key I need to work on when it comes to my client is to be more firm in what the therapy entails so they can receive effective treatment.
0 notes
Text
Week 2: Reflecting on Treatment Planning
Occupational Therapy is very client centred meaning that it focuses on the clients interpretation and understanding of their situation. Other than the therapists view on what is important to be treated, however in most cases the therapists opinion is integrated into the treatment especially if client does not have good insight into their occupational capacities post injury. The client centred approach was developed by Carls Rogers in the 1940′s.
The approach is one built on three qualities:1 unconditional positive regard, genuines and empathetic understanding’("10 Person-Centred Therapy Techniques Inspired by Carl Rogers [+PDF]", 2020).
These principles allow for the sessions to become more interactive as the client will feel more accepted and considered and therefor becoming more responsive as they feel responsible for their recovery as well.
When beginning my treatment planning I firstly needed to understand my clients diagnosis and possible prognosis. My client is diagnosed with TB Meningitis which is an airborne disease that travels in the bloodstream and affects organs and tissues of the body. It also has many complications shown on the link below: (https://positivepsychology.com/client-centered-therapy/) one of which is a stroke which my client presents with symptoms of such as a slightly spastic arm which is going into a flexed contracture pattern. Also I still need to determine my clients stage of illness.
To be more client centred I have chosen the following levels of intervention preventative, remedial and rehabilitative phase to be comprehensive in my treatment but still recognising my clients desires. She has voiced her main concern as wanting to walk independently. Which I found was an important area to treat but requires other problem areas to be first addressed, Such as her spastic arm which would serve as an inhabitant to her walking with a walking aid as she needs to have good dynamic sitting balance before she can stand. This will be explained in the clients in the following session so she can see her desire to walk as an end point to our treatment. Therefor splinting and activities such as dressing of upper limb will take priority over walking. Also doing NDT training will assist in the clients rehabilitation.
Functional Resting Splint

During feedback from our supervisor we were also reminded that we should focus on more than on sub programme to benefit our clients. I will also focus on the clients educational domain as she is a student which would require a focus on her cognition. As she has an impaired memory capacity she will require stimulation of this area such as 24 hour orientation which will be requested by me of the nurses. At the same time understanding that there is limited interaction between the therapist and the client as I am at an acute hospital. Therefore requiring a wholistic treatment plan as well as a quick and simple discharge plan.
As an O.T. student I am quickly realising that there is only so much we can do as therapist more especially in the economy we live in and how that impacts the health of the occupants of South Africa. There are many changes that still need to taken in our health care system to really benefit the people.
Refrences:
1.10 Person-Centered Therapy Techniques Inspired by Carl Rogers [+PDF]. (2020). Retrieved 5 March 2020, from https://positivepsychology.com/client-centered-therapy/.
1 note
·
View note