#dr. l
Text
Hyperfixating on this character when I was 11 changed my brain chemistry I think
#the secret series#Dr. L#Luciano Bergamo#pseudonymous bosch#the evil science autism started here istg
9 notes
·
View notes
Text
Things I Realize and Love about Zayne's personality in Exclusive Tutorial

* He loves showing you off of his colleagues
* He keeps close to you specially when his colleagues are around
* He lets you have your way on him but never to the extent of humiliating you in public
* He is a true softy and really gets weak when you touch him
* He would take care of you. Not just your health but overall Aspect of you.
* He is a true gentleman, he will never touch you inappropriately even if you provoke him.
P.S.
If I am not already in love with this guy, I sure am now..
1K notes
·
View notes
Text

Goodluck to Zayne’s girlies
#artists on tumblr#digital art#fanart#artoftheday#love and deepspace#zayne love and deepspace#zayne#lnd zayne#l&ds zayne#lads zayne#dr zayne#zayne x mc#zayne x you
1K notes
·
View notes
Text
I am in love with him, someone save me.
#dr zayne#doctor zayne#i love zayne#zayne love and deepspace#love and deepspace zayne#love and deepspace#lnds zayne#l&ds
805 notes
·
View notes
Text

𝐇𝐎𝐖 𝐑𝐈𝐃𝐄𝐀𝐁𝐋𝐄 𝐈𝐒 𝐇𝐈𝐒 𝐍𝐎𝐒𝐄???
𝐑𝐀𝐓𝐈𝐍𝐆 𝐓𝐇𝐄 𝐌𝐄𝐍 𝟏-𝟏𝟎!!!
𝐃𝐑. 𝐙𝐀𝐘𝐍𝐄: 11/10 best ride guaranteed!!
I’m not biased I swear. Have you seen that dorsal hump?? Everything is perfect about his nose. The height is sure to each your clit, so no need to worry about that. Width wise it’s also great, the thickness is just perfect for rubbing between your folds. The tip of his nose is nice and round so it’ll feel great rubbing on your clit and also through your folds. The dorsal hump is another wave of stimulation as he grabs your hips to make you grind on his face. After poking and prodding him all over and paying extra attention to his beautiful nose, Zayne had a proposition for you. “If you want it next time, tell me directly.” He’d probably have you straddle his head, gripping your thighs as you steady yourself. You asked him multiple times if he was really as okay with this as he seemed, to which he made a dissatisfied sound and said something along the lines of, “just sit down please.” You’d hover above his face for a moment, unsure about if you’d hurt him or not. Zayne sighs before grabbing your thighs and pulling you down. He got to work IMMEDIATELY. Firstly licking between your folds to lubricate you, making his perfect nose bump and slide against your clit. A few minutes later you were riding his face in earnest, moaning and screaming his name. He groaned as you tugged his hair, “more… faster please! Zayne!” Who is he to deny you?

𝐗𝐀𝐕𝐈𝐄𝐑: 8/10 smooth calm ride that’ll put you to sleep!!
A little bit of a longer nose so you have more stimulation time, being as to it’ll take you longer to grind up and down. The tip is at a good height, making it reachable without him having to strain his neck. The width is a littleeee thin, but what he lacks in thickness he makes up for in height. He’s definitely an eater. You’d tell him that you had a bad day in your unit, and he’d immediately flop back on the bed and offer his face as a seat. He mistook your shock at his vulgarity for confusion, before uttering very cutely, “well, you like my nose, right?” That was enough for you tbh. Slowly, you steady yourself as you straddle his face. “Fucking god…” He’d moan as he started eating you like you were his last meal. A string of curses and moans spilled from your lips as he tongue fucked you. And then you felt it… his nose bumping up against your clit perfectly. It truly was a stress reliever. How lucky are you?

𝐑𝐀𝐅𝐀𝐘𝐄𝐋: 0/10 nope!!
You bitches get nothing. I grinded for a ten draw and ended up getting fucking Fish Boy’s card so I’m taking this anger out on yall.

#lnd zayne#l&ds zayne#zayne x you#lads zayne#dr zayne#zayne love and deepspace#zayne x mc#zayne smut#zayne x reader#xavier#xavier love and deepspace#xavier x reader#xavier x mc#xavier x you#lnds xavier#love and deepspace imagines#love and deepspace#lads x reader#lads smut#lads rafayel#lads xavier#rafayel x reader#rafayel x you#rafayel x mc
440 notes
·
View notes
Text
BRB. I think I just got pregnant...
Zayne is sooooo hot. April 30th can't come sooner.
#love and deepspace#zayne#dr zayne#zayne love and deepspace#zayne l&ds#love and deepspace zayne#li shen
530 notes
·
View notes
Note
Sooo I saw that you write for lnd 👉🏼👈🏼
Can I pretty please ask for big brother Zayne? I don't mind either being incest or stepcest you can pick
A fic would be lovely but just general headcanons of what you think big brother Zayne would be to reader would be fine too!! 🥺
- 🫧
PLAYING NURSE FOR BIG BROTHER !

˚₊‧desc— Zayne always needs a nurse at home, fortunately his little sister is there!
˚₊‧tw— dark content, incest, incest, incest, INCEST, smut, blowjob, riding, bimbo!reader, big brother!Zayne, reader is of age but very sheltered
˚₊‧a/n— My first named Anon and my first lnd ask!! Sorry I can't write a long full fic rn, I'm too busy :(

Growing up, you've always been under the care of your big brother. Once your parents died, you truly had nobody but him.
And it's not like you mind, you love your big brother! You wouldn't have wanted it any other way. Just the thought of your big brother being forced to work makes you sad the whole day.
Everytime he comes home, he says that you have to play nurse for him! That includes giving him medicine, bathing him, and giving him little kisses all over his face!
But there were times where he told you to do some.. extra tasks as a nurse. Why, of course it includes sucking his cock like a good girl.
Overtime, you realize all these 'extra tasks' seems to includes his cock one way or another. He says that it's normal for nurses to do that.
Sometimes nurses help their patient, or even their doctors! And you can't help but wonder, does all nurses do this?
"Welcome home, big brother!" you exclaim once he arrives at the front door, you help him take off his jacket and realizes he looks really tense.
You helped him to the couch, he must've been stressed at work since he isn't responding to anything you say at all!
You make a little pout before he sighs and ruffles your hair before unzipping his pants, letting his cock fly out and slaps against his stomach.
You drooled at the sight of his cock. It must've been another one of your nurse duties time! You have to help your doctor distress!
You touch the tip of his cock, testing it and seeing as he let's out a hiss at the contact of your hand. You grinned as you spit on your hand, he told you that your saliva is another medicine for his cock!
As you touch the sensitive flesh, he let's out little moans and groans when he feels your warm hands.
"D—don't. Don't tease me." He warns and takes your hands off his cock before putting the tip of it on your mouth.
"Come on, open. Don't bite unless you want to be spanked like last time." The threat hangs over your head as the memories flood in, making you widen your mouth for it to fit.
His cock is gorgeous—the tip is a pale red and it's enormous. You want to suck his cock all day long, so tasty when it slips in your mouth slowly.
You've already rid of your gag reflex long ago just so his cock can fit warmly inside your mouth. He groans and he rests his rough hand on your head, controlling your movement slowly.
He gets breathless after a few moments and pulls your warm cavern away from his dick, he pats his lap for you to climb on which you do so—excitedly.
"Ride it." The moment he says it, you lift your skirt up and pulls your panties to your ankles before positioning yourself over his cock and inserting it in.
"Feels 'sho good, big brother~" you moan out and peppers a kiss all over his face. He just lets you ride him without taking control over you, he was too stressed today.
You chase after your climax all in your own but got a bit too tired of bouncing on his lap, that's when he takes control of your movements when he notices how tired you seem.
He makes you jump on his cock, which makes you roll your eyes to the back of your skull.
"W-wah! Wait..! I'm cumming, cumming~" you moan out and bite your lip when his placid dick gets hard once again inside your cunt.
You seemed so tired after only a round of cumming and you remember that your big brother has too much stamina.
Especially when he's pent up.

#tw.dark content#tw.incest#tw:incest#zayne love and deepspace#lads zayne#zayne#zayne x reader#zayne x you#l&ds zayne#lnd zayne#zayne x mc#zayne smut#zayne noncon#dr zayne#lnd smut#yandere zayne#yandere LND#love and deepspace#yandere love and deepspace#love and deepspace smut
454 notes
·
View notes
Text

I was swapping screens when this happened.
...
...
NO.. NOT THE SENTENCE, THE SLIPPING SCREEN TO HIS BULGE.
Now, I had to put 30mins of workout.
Jesus....
#love and deepspace#zayne x reader#dr zayne#l&ds zayne#lads zayne#rafayel#xavier lad#xavier lads#zayne love and deepspace#zayne x you#love and deepspace xavier#love and deep space#caleb love and deepspace#love and deepspace caleb#love and deepspace fanart#love and deepspace headcanons#love and deepspace rafayel#love and deepspace smut#love and deepspace x reader#love and deepspace zayne#love and deepspace zayne smut#rafayel love and deepspace#xavier love and deepspace#loveanddeepspace#zayne#zayne headcanons#zayne smut#zayne x mc
564 notes
·
View notes
Text
MC: You can trust me! Let's not forget who pulled you out of the river back in high school.
Zayne: Let's not forget who pushed me in
#love and deepspace#yuzuocha ‣ memes#zayne lads#lad zayne#dr zayne#love and deepspace zayne#zayne fluff#zayne#zayne love and deepspace#l&ds zayne#lads zayne#lnd zayne#li shen#レイ
514 notes
·
View notes
Text

#tails the fox#sth#sonic the hedgehog#dr eggman#eggman#miles tails prower#OK.POST FSJFGDJK;L#! !^_^^
605 notes
·
View notes

Text
Wow.... Zayne literally sizes up the staff who suddenly talks to M/C.. He got this “If looks could kill, the staff died a thousand times already “
🫣🫣🫣🫣😆😆😆😆
He's so extra sometimes 💙❄️💙❄️💙❄️
323 notes
·
View notes
Text
By: Andy L.
Published: Apr 14, 2024
It has now been just little under a week since the publication of the long anticipated NHS independent review of gender identity services for children and young people, the Cass Review.
The review recommends sweeping changes to child services in the NHS, not least the abandonment of what is known as the “affirmation model” and the associated use of puberty blockers and, later, cross-sex hormones. The evidence base could not support the use of such drastic treatments, and this approach was failing to address the complexities of health problems in such children.
Many trans advocacy groups appear to be cautiously welcoming these recommendations. However, there are many who are not and have quickly tried to condemn the review. Within almost hours, “press releases“, tweets and commentaries tried to rubbish the report and included statements that were simply not true. An angry letter from many “academics”, including Andrew Wakefield, has been published. These myths have been subsequently spreading like wildfire.
Here I wish to tackle some of those myths and misrepresentations.
-
Myth 1: 98% of all studies in this area were ignored
Fact
A comprehensive search was performed for all studies addressing the clinical questions under investigation, and over 100 were discovered. All these studies were evaluated for their quality and risk of bias. Only 2% of the studies met the criteria for the highest quality rating, but all high and medium quality (50%+) studies were further analysed to synthesise overall conclusions.
Explanation
The Cass Review aimed to base its recommendations on the comprehensive body of evidence available. While individual studies may demonstrate positive outcomes for the use of puberty blockers and cross-sex hormones in children, the quality of these studies may vary. Therefore, the review sought to assess not only the findings of each study but also the reliability of those findings.
Studies exhibit variability in quality. Quality impacts the reliability of any conclusions that can be drawn. Some may have small sample sizes, while others may involve cohorts that differ from the target patient population. For instance, if a study primarily involves men in their 30s, their experiences may differ significantly from those of teenage girls, who constitute the a primary patient group of interest. Numerous factors can contribute to poor study quality.
Bias is also a big factor. Many people view claims of a biased study as meaning the researchers had ideological or predetermined goals and so might misrepresent their work. That may be true. But that is not what bias means when we evaluate medical trials.
In this case we are interested in statistical bias. This is where the numbers can mislead us in some way. For example, if your study started with lots of patients but many dropped out then statistical bias may creep in as your drop-outs might be the ones with the worst experiences. Your study patients are not on average like all the possible patients.
If then we want to look at a lot papers to find out if a treatment works, we want to be sure that we pay much more attention to those papers that look like they may have less risk of bias or quality issues. The poor quality papers may have positive results that are due to poor study design or execution and not because the treatment works.
The Cass Review team commissioned researchers at York University to search for all relevant papers on childhood use of puberty blockers and cross-sex hormones for treating “gender dysphoria”. The researchers then graded each paper by established methods to determine quality, and then disregarded all low quality papers to help ensure they did not mislead.
The Review states,
The systematic review on interventions to suppress puberty (Taylor et al: Puberty suppression) provides an update to the NICE review (2020a). It identified 50 studies looking at different aspects of gender-related, psychosocial, physiological and cognitive outcomes of puberty suppression. Quality was assessed on a standardised scale. There was one high quality study, 25 moderate quality studies and 24 low quality studies. The low quality studies were excluded from the synthesis of results.
As can be seen, the conclusions that were based on the synthesis of studies only rejected 24 out of 50 studies – less than half. The myth has arisen that the synthesis only included the one high quality study. That is simply untrue.
There were two such literature reviews: the other was for cross-sex hormones. This study found 19 out of 53 studies were low quality and so were not used in synthesis. Only one study was classed as high quality – the rest medium quality and so were used in the analysis.
12 cohort, 9 cross-sectional and 32 pre–post studies were included (n=53). One cohort study was high-quality. Other studies were moderate (n=33) and low-quality (n=19). Synthesis of high and moderate-quality studies showed consistent evidence demonstrating induction of puberty, although with varying feminising/masculinising effects. There was limited evidence regarding gender dysphoria, body satisfaction, psychosocial and cognitive outcomes, and fertility.
Again, it is myth that 98% of studies were discarded. The truth is that over a hundred studies were read and appraised. About half of them were graded to be of too poor quality to reliably include in a synthesis of all the evidence. if you include low quality evidence, your over-all conclusions can be at risk from results that are very unreliable. As they say – GIGO – Garbage In Garbage Out.
Nonetheless, despite analysing the higher quality studies, there was no clear evidence that emerged that puberty blockers and cross-sex hormones were safe and effective. The BMJ editorial summed this up perfectly,
One emerging criticism of the Cass review is that it set the methodological bar too high for research to be included in its analysis and discarded too many studies on the basis of quality. In fact, the reality is different: studies in gender medicine fall woefully short in terms of methodological rigour; the methodological bar for gender medicine studies was set too low, generating research findings that are therefore hard to interpret. The methodological quality of research matters because a drug efficacy study in humans with an inappropriate or no control group is a potential breach of research ethics. Offering treatments without an adequate understanding of benefits and harms is unethical. All of this matters even more when the treatments are not trivial; puberty blockers and hormone therapies are major, life altering interventions. Yet this inconclusive and unacceptable evidence base was used to inform influential clinical guidelines, such as those of the World Professional Association for Transgender Health (WPATH), which themselves were cascaded into the development of subsequent guidelines internationally.
-
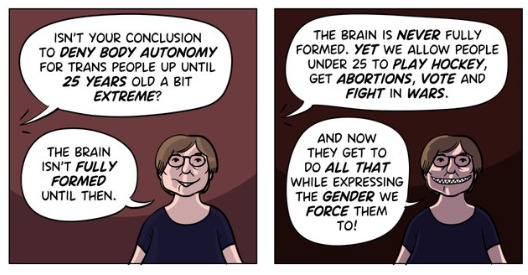
Myth 2: Cass recommended no Trans Healthcare for Under 25s
Fact
The Cass Review does not contain any recommendation or suggestion advocating for the withholding of transgender healthcare until the age of 25, nor does it propose a prohibition on individuals transitioning.
Explanation
This myth appears to be a misreading of one of the recommendations.
The Cass Review expressed concerns regarding the necessity for children to transition to adult service provision at the age of 18, a critical phase in their development and potential treatment. Children were deemed particularly vulnerable during this period, facing potential discontinuity of care as they transitioned to other clinics and care providers. Furthermore, the transition made follow-up of patients more challenging.
Cass then says,
Taking account of all the above issues, a follow-through service continuing up to age 25 would remove the need for transition at this vulnerable time and benefit both this younger population and the adult population. This will have the added benefit in the longer-term of also increasing the capacity of adult provision across the country as more gender services are established.
Cass want to set up continuity of service provision by ensure they remain within the same clinical setting and with the same care providers until they are 25. This says nothing about withdrawing any form of treatment that may be appropriate in the adult care pathway. Cass is explicit in saying her report is making no recommendations as to what that care should look like for over 18s.
It looks the myth has arisen from a bizarre misreading of the phrase “remove the need for transition”. Activists appear to think this means that there should be no “gender transition” whereas it is obvious this is referring to “care transition”.
-
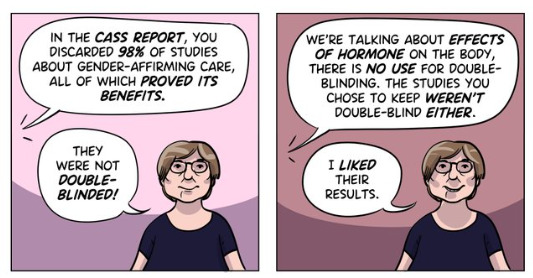
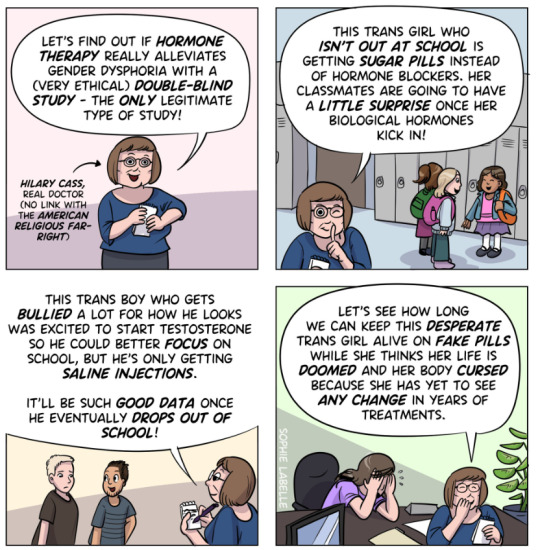
Myth 3: Cass is demanding only Double Blind Randomised Controlled Trials be used as evidence in “Trans Healthcare”
Fact
While it is acknowledged that conducting double-blind randomized controlled trials (DBRCT) for puberty blockers in children would present significant ethical and practical challenges, the Cass Review does not advocate solely for the use of DBRCT trials in making treatment recommendations, nor does it mandate that future trials adhere strictly to such protocols. Rather, the review extensively discusses the necessity for appropriate trial designs that are both ethical and practical, emphasizing the importance of maintaining high methodological quality.
Explanation
Cass goes into great detail explaining the nature of clinical evidence and how that can vary in quality depending on the trial design and how it is implemented and analysed. She sets out why Double Blind Randomised Controlled Trials are the ‘gold standard’ as they minimise the risks of confounding factors misleading you and helping to understand cause and effect, for example. (See Explanatory Box 1 in the Report).
Doctors rely on evidence to guide treatment decisions, which can be discussed with patients to facilitate informed choices considering the known benefits and risks of proposed treatments.
Evidence can range from a doctor’s personal experience to more formal sources. For instance, a doctor may draw on their own extensive experience treating patients, known as ‘Expert Opinion.’ While valuable, this method isn’t foolproof, as historical inaccuracies in medical beliefs have shown.
Consulting other doctors’ experiences, especially if documented in published case reports, can offer additional insight. However, these reports have limitations, such as their inability to establish causality between treatment and outcome. For example, if a patient with a bad back improves after swimming, it’s uncertain whether swimming directly caused the improvement or if the back would have healed naturally.
Further up the hierarchy of clinical evidence are papers that examine cohorts of patients, typically involving multiple case studies with statistical analysis. While offering better evidence, they still have potential biases and limitations.
This illustrates the ‘pyramid of clinical evidence,’ which categorises different types of evidence based on their quality and reliability in informing treatment decisions

The above diagram is published in the Cass Review as part of Explanatory Box 1.
We can see from the report and papers that Cass did not insist that only randomised controlled trials were used to assess the evidence. The York team that conducted the analyses chose a method to asses the quality of studies called the Newcastle Ottawa Scale. This is a method best suited for non RCT trials. Cass has selected an assessment method best suited for the nature of the available evidence rather than taken a dogmatic approach on the need for DBRCTs. The results of this method were discussed about countering Myth 1.
Explainer on the Newcastle Ottawa Scale
The Newcastle-Ottawa Scale (NOS) is a tool designed to assess the quality of non-randomized studies, particularly observational studies such as cohort and case-control studies. It provides a structured method for evaluating the risk of bias in these types of studies and has become widely used in systematic reviews and meta-analyses.
The NOS consists of a set of criteria grouped into three main categories: selection of study groups, comparability of groups, and ascertainment of either the exposure or outcome of interest. Each category contains several items, and each item is scored based on predefined criteria. The total score indicates the overall quality of the study, with higher scores indicating lower risk of bias.
This scale is best applied when conducting systematic reviews or meta-analyses that include non-randomized studies. By using the NOS, researchers can objectively assess the quality of each study included in their review, allowing them to weigh the evidence appropriately and draw more reliable conclusions.
One of the strengths of the NOS is its flexibility and simplicity. It provides a standardized framework for evaluating study quality, yet it can be adapted to different study designs and research questions. Additionally, the NOS emphasizes key methodological aspects that are crucial for reducing bias in observational studies, such as appropriate selection of study participants and controlling for confounding factors.
Another advantage of the NOS is its widespread use and acceptance in the research community. Many systematic reviews and meta-analyses rely on the NOS to assess the quality of included studies, making it easier for researchers to compare and interpret findings across different studies.
As for future studies, Cass makes no demand only DBRCTs are conducted. What is highlighted is at the very least that service providers build a research capacity to fill in the evidence gaps.
The national infrastructure should be put in place to manage data collection and audit and this should be used to drive continuous quality improvement and research in an active learning environment.
-
Myth 4: There were less than 10 detransitioners out of 3499 patients in the Cass study.

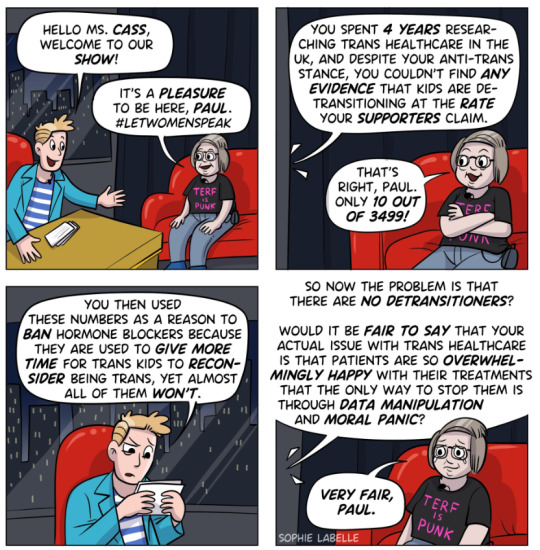
Fact
Cass was unable to determine the detransition rate. Although the GIDS audit study recorded fewer than 10 detransitioners, clinics declined to provide information to the review that would have enabled linking a child’s treatment to their adult outcome. The low recorded rates must be due in part to insufficient data availability.
Explanation
Cass says, “The percentage of people treated with hormones who subsequently detransition remains unknown due to the lack of long-term follow-up studies, although there is suggestion that numbers are increasing.”
The reported number are going to be low for a number of reasons, as Cass describes:
Estimates of the percentage of individuals who embark on a medical pathway and subsequently have regrets or detransition are hard to determine from GDC clinic data alone.
There are several reasons for this:
Damningly, Cass describes the attempt by the review to establish “data linkage’ between records at the childhood gender clinics and adult services to look at longer term detransition and the clinics refused to cooperate with the Independent Review. The report notes the “…attempts to improve the evidence base have been thwarted by a lack of cooperation from the adult gender services”.
We know from other analyses of the data on detransitioning that the quality of data is exceptionally poor and the actual rates of detransition and regret are unknown. This is especially worrying when older data, such as reported in WPATH 7, suggest natural rates of decrease in dysphoria without treatment are very high.
Gender dysphoria during childhood does not inevitably continue into adulthood. Rather, in follow-up studies of prepubertal children (mainly boys) who were referred to clinics for assessment of gender dysphoria, the dysphoria persisted into adulthood for only 6–23% of children.
This suggests that active affirmative treatment may be locking in a trans identity into the majority of children who would otherwise desist with trans ideation and live unmedicated lives.
I shall add more myths as they become spread.
==
It's not so much "myths and misconceptions" as deliberate misinformation. Genderists are scrambling to prop up their faith-based beliefs the same way homeopaths do. Both are fraudulent.
#Andy L.#Cass Review#Cass Report#Dr. Hilary Cass#Hilary Cass#misinformation#myths#misconceptions#detrans#detransition#gender affirming healthcare#gender affirming care#gender affirmation#affirmation model#medical corruption#medical malpractice#medical scandal#systematic review#religion is a mental illness
358 notes
·
View notes
Text
me bullying Zayne as always :3

#love and deepspace zayne#zayne love and deepspace#love and deepspace#doctor zayne#zayne#i love zayne#lads zayne#zayne x reader#dr zayne#zayne smut#zayne x oc#zayne x y/n#zayne x mc#zayne x you#zayne lads#zayne l&ds#zayne lnd#lnds zayne
770 notes
·
View notes
Text

“Oh my fucking god, Zayne!”
You cried out as he bounced you on his cock like you weighed nothing.
“Shhhh, you asked for this, didn’t you?”
You may have misbehaved a bit too much in the pool hall.
You might have pushed him just a bit too much… but it’s not like he didn’t warn you.
Zayne’s nonchalance never wavered as he delivered a harsh smack to your ass as you bent down to hit the ball with your cue.
Catching eyes straying down to the crotch of his tight pants, you set one of your many last minute plans into action.
He had surprised you… sure you went out of your way to tease him but you didn’t think he’d bite so soon.
You really couldn’t help yourself. Zayne just looked so good in that suit.
He had ordered you to pull down the panties you wore under your playfully short skirt, which he stashed away in his pocket.
Fleetingly, you wondered if you’d ever see them again.
Sitting down, Zayne wasted no time pulling you into his lap and pushing his dick up into you, causing a deep moan from you both.
He really was fucking you like he was punishing you. That’s one of Zayne’s many positive traits; he was always a man of his word.
All the strength has long since left your knees, prompting Zayne to move you up and down on his cock like a human flesh toy.
And you were both absolutely loving it.
“Zayne please please pleaseee,” the last plead had been dragged out due to him slowing down his thrusts.
He was fucking you so deep and hard you could see stars.
You could feel every inch of his dick as he slowly fucked himself in and out of you.
“Fuck,” he curses, one of the rare times he does, with a deep groan. “You’re going to make me cum.”
“Cum inside please cum inside,” you babbled dumbly, as if you really do need it. “Cumming I’m cumming!”
You could’ve sworn your vision went white as you came, with your orgasm being just that intense.
What can you say? Dr. Zayne has a big dick and he knows how to use it.
You wrap your arms around his neck and grind yourself on him to draw out your orgasm, causing another euphoric sound from Zayne.
Reaching down to pinch your clit to intensify your feelings even more.
You damn near screamed at the sensation. “Zayne!”
That seemed to have did it for him, you felt his hips stutter before a blissful warmth spread all over your lower abdomen.
He was cumming inside you.
Strings of curses and groans left his lips as his grip on both your clit and your ass cheek tightened.
“Zayne… Zayne…” You chanted his name like a prayer.
“Yes,” he finally catches his breath. “I’m here.”
He finally let go of your erogenous zones, and instead pulled you into a tight hug, which you readily albeit tiredly reciprocated.
“Have you learned your lesson?”
You hum, pretending to think as you feel his cock throb and pulse inside of you.
“I think you might have to teach me again.”
#zayne love and deepspace#dr zayne#zayne x mc#zayne x reader#lads zayne#l&ds zayne#zayne x you#lnd zayne#zayne smut#lads x reader#lads smut#love and deepspace#love and deepspace imagines
797 notes
·
View notes
Text
Just Zayne shutting MC up with a kiss...
The way he looks at MC after.... I'm putty in your hands, Dr. Zayne. 😍
#love and deepspace#love and deepspace zayne#zayne#zayne love and deepspace#zayne l&ds#zayne lads#dr zayne#li shen
471 notes
·
View notes
Last Seen Blogs

darafe
s h a k e y e r h e a d

corinthoscoffee
Corinthos Coffee

wollfiguren-blog
Wollfiguren

druckgebiet
Druckgebiet Hamburg

omgitsemilyward
motherfuckers wanna laugh