#whump reference
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Women make up for the other 50% of Tumblr’s audience.
Text
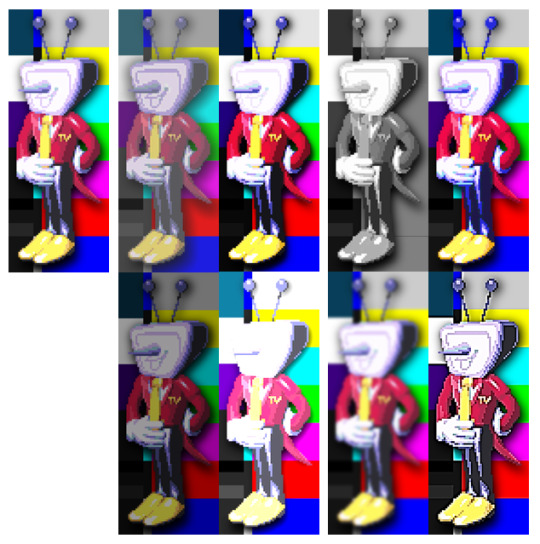
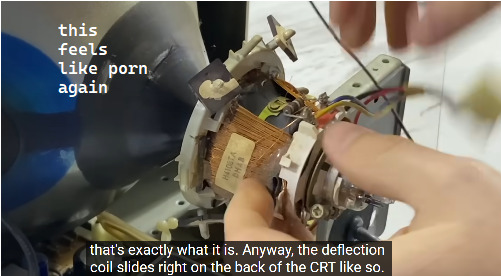
Various CRT TV Research for Tenna Purposes
please use this information to hurt him. or do other things to him. also send me links
I grew up with CRT TVs as a kid but like. I was a kid. I'm much more of a computer science person than a mechanics person but whatever
I'll also toss in some speculation on what each thing could mean for tenna here and there
Depending on how long the Dreemurs have had their TV, Tenna could probably be from anywhere between the mid 80s to the early 2000s.
I went to a manuals website and picked the Panasonic TC-14S3R at random. From what I can tell this particular TV is from the 80s, and I'm going to base a lot of the information here on that particular manual.
Various Settings
Contrast: Low contrast = more gray, less range in color and brightness. High contrast = more vibrant colors, lights are brighter and shadows are darker. Both increasing and decreasing contrast can cause detail to be lost. Lowering contrast can lose the subtle differences between similar mid-level shades and colors, whereas increasing it loses differences in bright and dark images. Could perhaps correlate with emotional state? Low contrast = low emotional range (maybe not necessarily depressed, but both happiness and sorrow etc. are muted? Could have a similar effect to taking an anti-depressant, perhaps), high contrast = high emotional range, highs are higher but lows are lower. Perhaps helpful for being exciting for TV but difficult to deal with emotionally.
Colour: The manual didn't specify what this does that I saw, but it's probably just the saturation setting. No saturation = black and white, high saturation = extra bright colors. Emotionally, I imagine low saturation would correlate with depression, whereas high saturation would correlate with joy (or even mania).
Brightness: Pretty straightforward. Darker image vs brighter image. If contrast and color were to stand in for emotional state, I imagine brightness would be more associated with energy levels. Perhaps his screen gets dimmer as he gets more tired.
Sharpness: Low sharpness = blurry image, high sharpness = things look clearer and harsher. Perhaps his image would become sharper as he focuses... and things like drugs and alcohol (or equivalents) could cause his image to blur.

Also related to image settings: The colored bars you often see are the SMPTE pattern. It's used for calibrating brightness and other color settings.
Here's a screenshot from a video I referenced that shows some other settings you might see on a CRT TV:
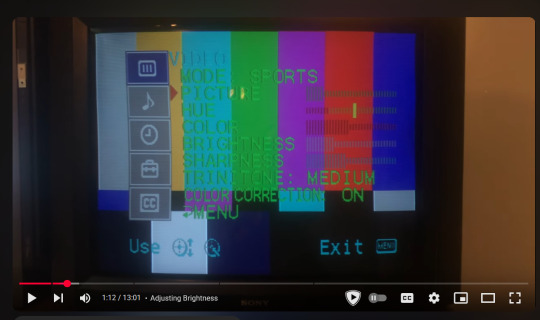
Some I didn't list already include:
Mode: From what I understand, just a bunch of presets for watching different sorts of things. Pictured is sports mode but there might also be a movie mode among others. Modern TVs still generally have this
Apparently "Picture" here is just contrast.
"Hue" as far as I can tell lets you shift, well, the hue. It's not normally something you need to mess with. If your reds are red and your blues are blue, etc. You're probably fine. If we assume that colors have some association with Tenna's emotions, though, I imagine that messing with his hue settings could really screw him up. Make him happy when he should be sad, something like that.
And then there would also be things like volume (I feel like turning down his volume has a lot of potential), input (normally he'd get input through his RF Input, as discussed in the next section, but I feel like switching him over to a different port would again, have potential.
Ports and Such

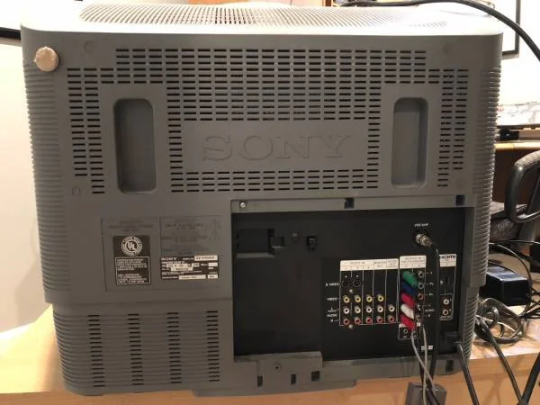

Alrighty, the spicy stuff.
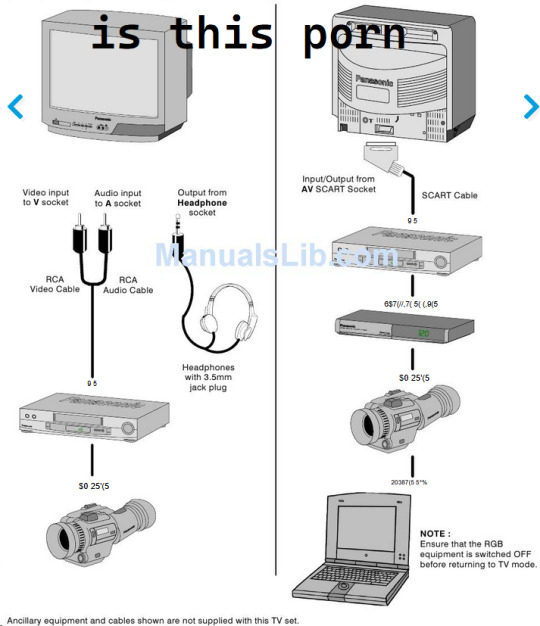
So there's a few different ways to get an image and such onto your CRT tv.
Usually with a modern TV you'll just have HDMI and that's it. One cable and you're done. Maybe your tv will even be fancier than that and have a USBC port. I feel like QUEEN is probably a bit too old for USBC, but she probably does have HDMI. But I'm getting off track.
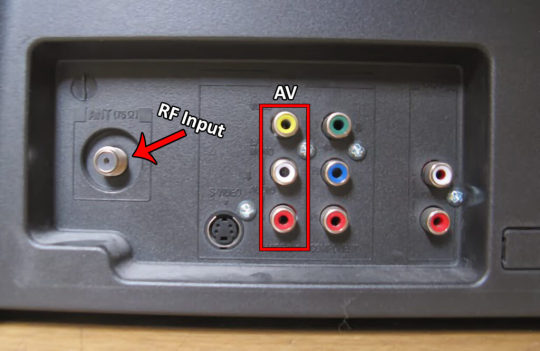
RF Input: Stands for Radio Frequency input. Handled both video and audio with one cable. As far as I can tell it became common in the 70s? Was often used for cable TV or "over-the-air" broadcasts from TV stations. The cables are also called Coaxial Cables. They have a prong in the middle, and are attached by screwing them on. Apparently RF is also prone to interference. Things like wifi, bluetooth, and microwaves can all cause RF interference, apparently. And also electric fences. So basically put a shock collar on that guy and see what happens
This is what Tenna's antennas would be connected to. I imagine disconnecting him from this would be... disconcerting, at the very least. He'd probably go blind and deaf or something.


Composite: The red white and yellow cables. Very common, you've probably seen them before. The yellow cable handles video, while the white and red cables handle the left and right audio specifically. Having one cable unplugged doesn't stop the others from working: you could have just the right audio but nothing else, or just video but no audio, for example. Again, implications. possibilities. This is what my Nintendo Wii uses. Usually provides a clearer signal than an RF connection but not considered great.
S-video: A cable for video transmission that's better than composite, apparently. Doesn't do audio though, so the audio data needs to be plugged in separately.


Component: Needed for high-definition television. Three cables for Luminance, Blue difference, and Red difference. Doesn't seem to handle audio by default?? And apparently there can be up to 5 of these cables??? They were quickly wiped out by HDMI cables though. Considering Tenna's age it seems unlikely he would have had ports for these.
The power cable on a CRT tv would usually be permanently attached.
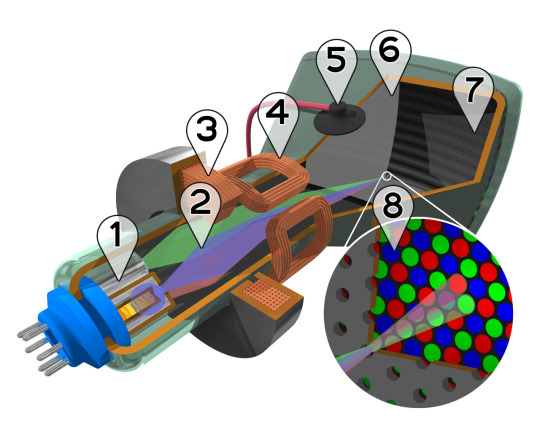
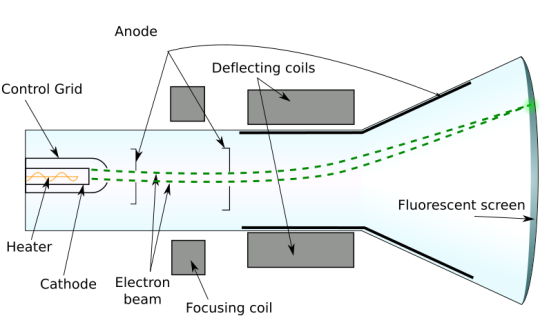
Screen and Internals
Right so this is where I start to struggle to understand things, but I'll do my best. If I get anything wrong here please let me know or reblog with a correction.
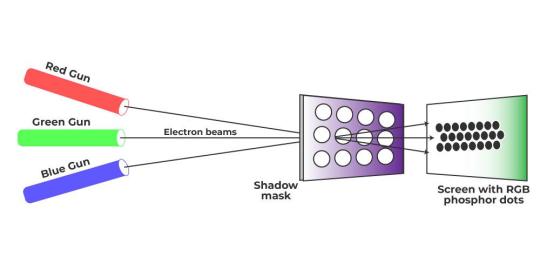
The front of a CRT screen has a coating that glows when it is hit by electrons. The screen does not technically have pixels, but does have an array of different colors of phosphor (the coating). To create different colors, different dots are hit. As far as I can tell this functions very similarly to pixels or how images are printed in magazines.
Anyway, at the back of the TV there is basically a laser (not the right word I don't think because it's not beams of light it's beams of electrons but whatever) that is shot at the different areas of the screen to create an image.
Anyway it's all rather complicated if you want to learn more read the wikipedia page or watch one of the videos I linked. Here's the stuff I care about:
CRT screens are very delicate and you basically can't repair them, because they are vacuums. When you smash a CRT tv you can kind of see them implode in a cloud of dust. You can't really come back from that. From what I can tell the only way to repair a CRT tv with a shattered screen is to replace the screen entirely, which seems to be by far the most important, complicated, expensive part. If the screen shatters you can salvage some components but ultimately the screen will need to be rebuilt or replaced entirely. Also, they don't make CRTs anymore because they are so complicated and the market isn't there. What I'm saying is Tenna is extremely lucky the Knight didn't break his screen, and if Tenna's screen ever did break that man is screwed. And not in the fun way. Unless you are me.
I added too many images so I'll reblog this again with the rest of the info I find
Sources
How to Calibrate and Correct Color and Brightness on a CRT TV, BVM and PVM Using SMPTE Pattern.
Panasonic TC-14S3R User Manual
History of Video Cables
TELEVISION CONNECTIONS EXPLAINED: RF vs. RCA vs. HDMI… COMPOSITE VS. COMPONENT
F connector
What Is RF Interference, What Causes It, & How To Block It
S-Video Cables
Component Explained
Cathode-ray tube (Wikipedia)
What is Color CRT Display?
How Cathode Ray Tubes Work. (YouTube video)
35 notes
·
View notes
Text
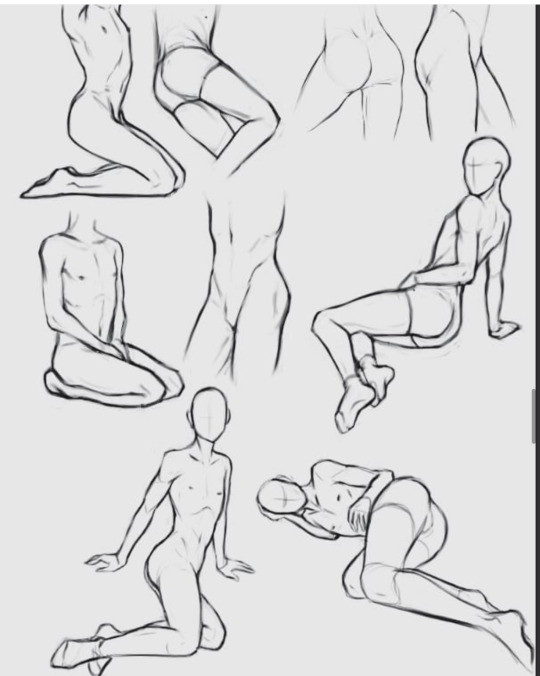
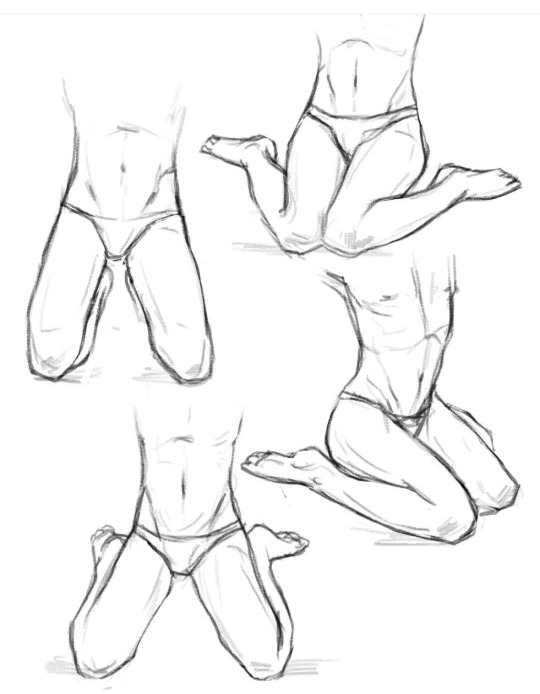
here are some old studies of kneeling/lewd/torso poses I found and wanted to share if anyone is looking for references for whump art or anything else! Enjoy :) I need to use these myself lol
#whump art#whump#whump reference#art reference#anatomy#anatomy reference#my art#old art#tag me if you want in your studies I’d love to see!!!
25 notes
·
View notes
Text
Hospital Lengths of Stay
I think people outside the USA severely overestimate how long hospital stays are here.
Like, appendectomy, right? That's maybe 24-36 hours door-to-door if there's no complications. If the appendix actually burst it might be 3 days, but only because they're giving you IV antibiotics and setting up home care to do that at home would take longer than just keeping you in the hospital.
A scheduled surgery like a hysterectomy, cholecystectomy, mastectomy, or anything else they can do laparoscopically (though small "keyhole" incisions)? You're probably not staying overnight at all.
Planned surgeries that need some kind of after care (like bariatric surgery, knee replacements, hip replacements, total vaginal hysterectomies, bladder lifts, etc...) would be usually 1-3 days.
Minor heart attack? 2-3 days.
Fracture and surgical repair of a large bone (like the femur)? About 2-3 days.
What about the exacerbation of a chronic illness like asthma, COPD, heart failure, or hypertension? IF they admit you (not just stabilize and discharge from the emergency department), it will be generally less than about 3-5 days.
Gunshot wound to the abdomen with surgery to repair things? 3-5 days.
And a stroke, sepsis, gunshot wound to the chest, or major heart attack? That would be somewhere in the 5-7 day range.
Severe trauma with multiple severely broken bones and relatively extensive surgery? This might be somewhat longer, but usually for nursing and pain control reasons rather than the surgery or injuries themselves. 1-3 weeks would be usual.
In the hospital for a mental health reason like decompensated schizophrenia or major depression? A little less than a week is normal, though some people stay several weeks if medications aren't working well.
The people who stay in hospitals for weeks or months typically have whole systems that don't work, or are waiting for a major organ transplant. For example, I had a patient once whose entire abdomen was open and couldn't be closed surgically. She was on TPN (IV nutrition) and IV antibiotics and needed massive amounts of wound care done every hour or so because her intestinal contents were spilling out of her open abdomen. She was there for months and ultimately didn't make it.
Are there people who stay longer than these cases? Of course! These are just averages pulled from medicaid data and personal experiences, based on patients who are coming in relatively healthy. Patients who have other significant health problems usually stay longer than patients who come in with a single problem.
But if you are otherwise healthy except for the reason you came into the hospital, unless you fell off a building or were in a massive car accident you are probably not staying in the hospital very long at all.
2K notes
·
View notes
Text
On conditioned whumpees...
Y'know, I think one of the things that people get wrong with conditioned whumpees is their rules. Specifically, when a whumpee was in long term captivity/training and they later get released or escape.
Most people write them as latching onto a caretaker or new whumper, and begging for new rules so they know they're doing something right. A new set of laws to live by, a new framework to behave to.
And that's... not really how conditioning works.
Conditioning means automatic reactions. Your body doing something that was trained into you without consulting your brain first.
There is no decision making. There is no choice. The trigger hits, and you are immediately performing the correct action regardless of anything else.
You're told to kneel? Your knees have already hit the ground. You're supposed to be standing in one part of the house when a certain noise is made? You've launched into movement before you even realize what you heard.
These rules are woven into the fabric of your body. And they are insurmountable. The conditioning overrides emotion, internal conflict, hesitation, beliefs, wants... everything.
Your whumpee may very well hate what is being done to them, and after the moment has passed they're cursing themself and their whumper. They're still a person on the inside. And that person is still very much alive. Most of the time, they will have some level of awareness that what's being done to them is wrong. They'll be angry. They'll be hurt. And they will hate that there is nothing they can do about it.
But the next time that trigger occurs, the response still hits them exactly the same.
So now take your whumpee out of that situation. They ran away, were rescued, were sold. They got out. Now they're with new people, a new caretaker, a new whumper. Or they're on their own and trying to make their own way in the world.
But those conditioned responses are still there.
There's no turning them off. You don't just replace them with new rules. They are in your every fibre. They have been built into the very framework of who you are.
The next time someone says the word "kneel", your knees are on the ground again. No matter where you are, or who you're with. The response happens before you can stop it. If they don't know why, everyone looks at you like you're insane. And you feel like you are.
Deconditioning is an agonizing process that takes more effort than I can even begin to describe to someone who's never experienced it.
Every time they hit that trigger, that response will still be there. Over, and over, and over, and over.
Breaking those rules down takes YEARS. And it is a constant effort that the whumpee has to choose to undergo every single time. Progress is measured milimeter by milimeter. You're told to kneel, and you kneel. You're told to kneel, and your mind catches up with the fact that you already did it— but a little sooner than it did before. Then a split second sooner. Then as you're doing it. Then you feel the impulse just before your knees hit the ground. Then you have a split-second of resistance before you go down. On and on and on and on, inching toward progress despite the fact that you're fighting with all your might. And that progress is anything but linear.
You don't just start obeying new rules. You don't latch on to your caretaker's new way of doing things and drop everything that you were conditioned to do before. These rules don't just get replaced.
Conditioning is not a belief system. It's a flinch response. Programmed deeper than the instincts you were born with.
You can be ordered not to obey the old command, and moments later when the trigger comes, you will anyway. Because in conditioning, the action comes before the choice.
These rules, these laws of your existence, come above everything else. And if your new whumper wants to replace them, they are going to have to beat the new rules into you so often and so severely that the pain becomes stronger than the old conditioning. At which point, the newly desired response will very, very slowly start to take over.
You're not swapping out new rules. You're layering new, worse conditioning on top of the old. And your brain will spend time stuck in that split-second between both responses before one finally grows stronger than the other. And even then, the change will not happen quickly.
That is what your conditioned whumpee is up against. That is what makes it such a horrible—HORRIBLE— and powerful tool.
#conditioned whumpee#writing advice#writing reference#pet whump#BBU whump#box boy universe#captive whumpee#whump writing#whump reference#whump inspiration#whump
2K notes
·
View notes
Text
Some headcanons regarding TMNT physiology
Over the years, I have come up with some headcanons regarding how I believe the Ninja Turtles' bodies work. I thought that perhaps it might be nice to finally share them with all of you.
These don't apply to all the iterations, of course, but they are pretty well universal in my mind, and I tend to incorporate most of them into my fanfics.
The Turtles (like leatherback sea turtles, echidnas, and some dinosaurs) are mesotherms, meaning they are neither warm nor cold blooded. They are, instead, in a middle-ground: they internally generate heat, but not to a constant temperature. In the Turtles' case, they will shiver when cold, and their bodies will not shut down right away when the temperature dips too low, though they may lose some energy and find it hard to concentrate.
Unlike many other modern reptiles and amphibians, who have a three-chambered heart, the Turtles have four-chambered hearts (like mammals and dinosaurs) that are larger and stronger than average human hearts and located at the center of their chests.
While the average human blood capacity is around five liters, the Turtles have about seven. Much of the blood flows under the shell -- a remnant of their lives as ordinary turtles, whose own blood does so in order to warm them when they bask. This means that the Turtles could lose close to three liters of blood before dying, while a human would only be able to lose two.
Their blood is also highly efficient at clotting, but that also means that storing blood for transfusions is difficult, and so must be directly transfused from one turtle to another in emergency situations.
Owing to their extensive circulatory system, they also have a larger lung capacity than humans and more oxygen-rich blood, and so are able to hold their breath for extended periods of time without adverse effects. Other than this, the Turtles' respiratory system is very much like humans', utilizing a diaphragm to inflate and deflate their lungs.
Like regular turtles, they do not have ribs, but rather their carapaces and plastrons serve that purpose, and they have muscles under their shells that keep their internal organs right where they belong.
Also like regular turtles, their spines curve along the insides of their shells. A direct hit on the center of their shells, then, could cause damage to their spinal column and nervous system, but fortunately their vertebral shields offer a fair amount of protection, so it would take quite an impact.
The Turtles are highly resistant to most infections and diseases, which increases their immunological responses. They do not get sick easily, and they recover quickly.
While their scales are not apparent, they are integrated into their skin, making it tougher than human skin. It takes a very hard hit to raise a bruise, and it is difficult to cut through without a very sharp or pointed blade.
Their bones are similar to humans, but are more resistant to breaking. They also heal quicker and stronger if they are broken.
Their muscles are also very close to human-like, but they are stronger than an average human due to compensating for the extra weight they carry in their shells. Because of this, their ligaments and tendons are also tougher, and it is difficult for them to have a joint dislocated.
Their sense of smell is more acute than humans, but not to an extreme degree. They are also not as bothered by foul smells (though this has more to do with living in a sewer than their physiology).
Their eyes are a bit tougher and more resistant to damage than human eyes due to a protective membrane that covers them. They see a bit better than humans in dark places and underwater.
Their hearing is somewhat more attuned to lower frequencies than human hearing, and is not dependent on external ears but rather an internal auditory system (making direct damage to their hearing unlikely).
They are capable of being knocked unconscious, but it takes a significant impact. Permanent or lingering damage to their brains is unlikely due to their structure, and so they also do not tend to suffer the same side-effects that humans would in the same circumstances (nausea, memory loss, etc.).
Although their nutritional needs are similar to humans, they do not need to eat every day, and in fact can get by quite well without food for a week if necessary (though they won't enjoy it). When food is readily available, however, they will eat as much as possible to store up energy. Their metabolism does not slow down when they do not eat, so overexerting themselves when they haven't had any food for a while can burn them out suddenly.
Their sleep schedules are much like most diurnal animals, though they are able to stay awake for extended periods of time and can get by on little sleep, if necessary. There have been times when they have been awake for days on end, getting by on short one hour naps here and there. In general, though, they like to have a regular sleep/wake cycle.
Like other reptiles, the Turtles never stop growing throughout their lifetimes; however their growth is slow, topping off at about 1-2 inches every five years.
Does anyone have anything they would like to add to the list? I actually had fun compiling it!
#tmnt#teenage mutant ninja turtles#ninja turtles#fanfic#fanfic reference#rise of the teenage mutant ninja turtles trailer#rottmnt#tmnt 2003#tmnt 2012#tmnt 2007#tmnt bayverse#tmnt vs batman#tmnt comics#tmnt mutant mayhem#tmnt mm#whump#whump reference#tmnt 1987#tottmnt#tales of the tmnt
2K notes
·
View notes
Text
Let's talk hallucinations in whump/general fiction.
So first off full disclosure, I have schizoaffective disorder - think some bits of bipolar and some bits of schizophrenia kind of squished together, and as such hallucinations are a BIG part of my general existence.
Definition: A hallucination is a perception of a sensory experience—such as sight, sound, smell, taste, or touch—that appears real but is created by the mind and lacks an external stimulus.
Now, I see a fair few "hallucinations" type prompts in whump events, and just generally within the whump community, and I see a LOT of auditory hallucinations type prompt fills - mainly in the form of malevolent whispers - and ye that's a thing, but there are so many other hallucinations.
The thing is hallucinations can effect literally any sense, not just hearing - though I will add that auditory is usually regarded as the most common.
this is a long post so I am going to put a cut here... below the cut is exploration of the tyoes of hallucination, the causes and a bit about insight.
So, I thought it could be "fun" to explore a few in a post. Lets explore the 5 "main" senses first:
Auditory Hallucinations
Description: These are the most common type of hallucinations. They involve hearing sounds that are not present. The sounds are hear as if they are coming from somewhere external to the body. So in my case I have a few of these, but my main one is a voice who is with me even when I am in meds (another good point there for anyone who wants to use mental illness in their fics even in meds we can do have symptoms). This voice has a name and most of the time he just sorts off passes comments about things and people around me, like a sarcastic narrator and it sounds like he is standing just behind me.
Common Examples:
Malevolent Whispers: Insidious voices that might threaten, taunt, or belittle you.
Hearing Music: Melodies or songs playing that no one else can hear. For me this kind of sounds like someone is playing a radio in a different room.
Environmental Sounds: Hearing footsteps, doors creaking, or other sounds suggesting someone else is present.
Command Hallucinations: Voices that instruct or suggest (its not always ademand, sometimes more subtle and manipulative) you to do certain things, often with a compelling and distressing sense of urgency.
Less used examples:
Kind/supportive hallucinations: Voices that are encouraging, reassuring and supportive.
Distortion: Rather than sounds with no origin hallucinations that disort or warp actual sounds/voices changing the meaning, making it as if the TV or Radio is addressing you personally, making it sound as if a friend is threatening you.
Fun fact: it actually is possible to have a two way (sort of) conversation with a hallucination - I know I do it relatively often. It will be different for everyone, but fo me its a bit like having a conversation on a bad phoneline, yes the voice will respond but often its almost as if he hasn't fully heard what I said - or is ignoring key points. I can do this both outloud and "in my head".
Visual Hallucinations
Description: Visual hallucinations involve seeing things that are not present. These can range from simple shapes and flashes of light to detailed images or scenes. They often appear as if they are in the physical world and can be very convincing.
Common Examples:
Shadowy Figures: Seeing indistinct, shadowy forms that may move or appear to watch the character.
Distorted Faces: Perceiving familiar faces as grotesque or altered in frightening ways.
Apparitions: Full-bodied figures that may interact with the character or appear menacing.
Lights/sparkles: The whump community seems to very much enjoy lights and sparkles, especially in drugging.
Less Used Examples:
Intrusive Visuals: Images of disturbing or graphic nature that suddenly appear in your line of sight.
Perceptual Distortions: Objects appearing to warp, change shape, or color in unnatural ways.
Double Vision: Seeing multiples of objects or people, creating a confusing and disorienting experience.
Scenery Shifts: The entire environment changes, making you believe they are in a completely different place.
Fun fact: Sleep deprivation can cause some wild visual hallucinations, even relatively "mild" sleep deprivation can start to effect a persons perceptions.
Gustatory Hallucinations
Description: Gustatory hallucinations involve tasting things that are not actually present in the mouth. These can range from pleasant to extremely unpleasant tastes and can be triggered without any external food or drink.
Officially these are considered "rare", but personally (as someone who has done a lot of peer support work in the psychosis/voice hearing community I think they are simply under reported.)
Common Examples:
Bitter or Metallic Taste: A persistent bitter or metallic taste in the mouth, often leading to a sense of unease or concern about poisoning.
Sweet or Sour Taste: Tasting something sweet or sour unexpectedly, which can be confusing if it doesn’t match the current context.
Less Used Examples:
Spoiled Food: Tasting something rancid or spoiled, causing nausea and distress.
Unfamiliar Tastes: Tasting something completely unfamiliar and hard to describe, adding to the character's sense of disorientation.
Mimicking Actual Foods: Tasting specific foods that trigger cravings or aversions, despite not eating anything.
Transforming food: Food tasting like other food - I know someone for whom everything tasted like strawberries for days.
Common Causes: Neurological conditions or can be a side effect of medications.
Olfactory Hallucinations
Description: Olfactory hallucinations involve smelling odors that are not actually present. These can be pleasant or unpleasant and occur without any corresponding external stimulus. They can be particularly disorienting because they may trigger memories or emotions associated with certain scents - extremely complex if the person also has PTSD.
Common Examples:
Burning Smell: Wood, rubber, or food, which can lead to panic and fear of a fire.
Rotting Flesh: An overpowering smell of decay or rotting flesh, causing distress and nausea.
Perfume or Flowers: Smelling strong scents like flowers or perfume - hallucinations don't have to be inherently unpleasant sensations.
Less Used Examples:
Chemical Smells: Smelling chemicals like bleach or petrol.
Unfamiliar Scents: Smelling odors that you cannot identify.
Food Smells: Smelling specific foods that trigger hunger or nausea, despite the absence of any actual food.
Tactile Hallucinations
Description: Tactile hallucinations involve feeling sensations on or under the skin that are not actually there. These can range from mild tingling to severe pain and can be extremely distressing.
Common Examples:
Crawling Sensation: Feeling as though insects or bugs are crawling on or under the skin - often leading to frantic scratching or picking.
Electric Shocks: Experiencing sudden, sharp, electric-like jolts.
Pressure: Feeling pressure or tightness around certain body parts, such as a hand gripping the arm or something heavy on the chest.
Less Used Examples:
Temperature Changes: Feeling extreme cold or heat on the skin without any external cause.
Wetness or Dripping: Feeling as though liquid is dripping or running down the skin, even when dry.
Phantom Touches: Sensations of being touched or grabbed, often when alone. Sometimes its an almost feather like touch, other times its more akin to a grab that if reak would leave a bruise.
Right now let's expand - because there are more than 5 senses.
Proprioceptive Hallucinations
Description: Proprioception is the sense of the relative positioning of one's body parts. Proprioceptive hallucinations involve distorted perceptions of where your body is in space or how it is moving.
Common Examples:
Floating Sensation: Feeling as if the body is levitating or moving without control.
Distorted Body Size: Perceiving limbs or the entire body as being unnaturally large or small.
Less Used Examples:
Misaligned Limbs: Feeling as though limbs are twisted or out of place.
Movement Hallucinations: Sensing movements that aren't occurring, like swaying or rotating.
Common causes: Neurological disorders or the effects of certain drugs, but can by caused by a huge array of things.
Vestibular Hallucinations
Description: Vestibular sensations involve balance and spatial orientation. Vestibular hallucinations affect your sense of balance, making you feel dizzy or as though you're moving when you're stationary.
Common Examples:
Vertigo: A spinning sensation, as if the environment or oneself is rotating.
Imbalance: Feeling as though you're about to fall over or can't maintain your balance.
Less Used Examples:
Motion Sensation: Sensing movement, like rocking or swaying, when you're still.
Gravity Distortions: Feeling as if gravity is stronger or weaker than it actually is.
Common caused: Inner ear issues, migraines, or anxiety.
Temporal Hallucinations
Description: Temporal hallucinations involve distorted perceptions of time. They can make time feel like it's speeding up, slowing down, or standing still.
Common Examples:
Time Dilation: Feeling as though time is passing much slower than it actually is.
Time Compression: Perceiving time as moving rapidly, making events feel like they're passing in a blur.
Less Used Examples:
Frozen Moments: Experiencing time as if it's stopped, with everything around you appearing frozen.
Temporal Displacement: Feeling as though you're living in a different time period.
Temporal Dissonance: Feeling as if time is moving differently for you in comparison to those around you.
Common caused: Extreme fatigue, high stress, or under the influence of certain drugs.
Interoceptive Hallucinations
Description: Interoception refers to the perception of sensations from within the body, such as hunger, thirst, or the feeling of a heartbeat. Hallucinations in this realm involve feeling internal sensations that aren't actually occurring.
Common Examples:
False Hunger: Feeling extremely hungry despite having eaten recently.
Nonexistent Thirst: An intense sense of thirst even when well-hydrated - I have had this one a few times and given myself electrolyte imbalances due tot he amount of water I ended up drinking (not fun).
Less Used Examples:
Phantom Heartbeats: Feeling the heart racing or skipping beats without any physical basis.
Digestive Sensations: Sensations of digestion, such as gurgling or bloating, without any real cause.
Common causes: Panic disorder or certain types of seizures.
Right, now lets quickly review the main "causes" of hallucinations
Mental Illness:
Schizophrenia: Can involve basically anything from this list, but anecdotally auditory and visual appear to be the most common.
Bipolar Disorder: Can include hallucinations, especially during manic or depressive episodes.
Schizoaffective Disorder: A combination of symptoms from both schizophrenia and mood disorders, often leading to a variety of hallucinations.
EUPD/BPD: Auditory hallucinations are relatively common.
In all of these the hallucinations will rarely (if ever) exist in isolation. If you do not have primary or secondary experience of mental illness then I would recommend doing a LOT of research - and talking to people who do (on this note my asks are open if anyone has any schizoaffective based questions).
Neurological Conditions:
Epilepsy: Particularly temporal lobe epilepsy, can cause a range of sensory hallucinations.
Parkinson's Disease: Can lead to visual and auditory hallucinations.
Migraine: Migraine auras can include visual and auditory hallucinations.
Once again the hallucinations will not be in isolatation so same advice as with mental illness.
Substance Use and Withdrawal:
Psychedelics: Drugs like LSD, psilocybin, and mescaline are known for causing vivid visual and auditory hallucinations.
Stimulants: Methamphetamine and cocaine can cause tactile and visual hallucinations.
Alcohol Withdrawal: Can lead to visual, auditory, and tactile hallucinations.
You know what I am going to say that my "if you do not have experience of this then go talk to someone who does" advice may just stand for every potential cause.
Sleep Disorders:
Sleep Deprivation: Can cause a variety of hallucinations across different senses.
Narcolepsy: Often includes hypnagogic (while falling asleep) and hypnopompic (while waking up) hallucinations.
Medical Conditions:
Delirium: Acute confusion and hallucinations often seen in severe infections, fever, or after surgery.
Dementia: Especially Lewy body dementia and Alzheimer's disease, can cause hallucinations.
Medications:
Anticholinergics: Can cause hallucinations as a side effect.
Steroids: High doses can sometimes lead to hallucinations.
Certain Antidepressants and Antipsychotics: Occasionally, these medications can cause hallucinations.
Psychological Stress and Trauma:
PTSD: Flashbacks and hallucinations related to traumatic events.
Extreme Stress: Can sometimes trigger hallucinations.
Metabolic and Endocrine Disorders:
Thyroid Disorders: Hyperthyroidism or hypothyroidism can sometimes cause hallucinations.
Electrolyte Imbalances: Severe imbalances can lead to hallucinations.
Deprivation:
Sensory Deprivation: Go google the ganzfeld effect, it's facinating.
Isolation: Extended periods of isolation can lead to hallucinations, known as sensory deprivation hallucinations.
Autoimmune Disorders:
Lupus: Can cause neurological symptoms including hallucinations.
Tumors:
Brain Tumors: Depending on their location, they can cause hallucinations affecting different senses.
Ok, finally point for this post. Let's discuss insight, because it is not as black/white or binary as people seem to assume.
Definition: Insight, in this context, refers to the awareness and understanding that one's hallucinations are not real but are a product of their mind. Insight can be partial or complete, and it often fluctuates.
Complete Insight:
Description: The individual fully understands that their hallucinations are not real and are caused by an underlying condition.
Impact: This can help the person manage their symptoms more effectively and seek appropriate treatment. However, it doesn't necessarily lessen the distress caused by the hallucinations.
Partial Insight:
Description: The individual has some awareness that their hallucinations might not be real but can still struggle with differentiating them from reality.
Impact: This can lead to confusion and anxiety, as the person oscillates between believing and doubting their experiences.
Lack of Insight:
Description: The individual firmly believes that their hallucinations are real and external.
Impact: This can lead to significant distress and functional impairment, as the person might respond to these hallucinations as if they were real.
Now imagine these three points on a scale from 0 (complete insight) to 10 (lack of insight) a person can be anywhere on this scale, and can slide back and fourth along it.
Factors such as stress, fatigue, medication changes, or daily fluctuations in mental state can cause insight to vary. A person might have high insight at one moment and low insight the next.
Basically Insight Is Not Static.
Also sometimes insight is just FREAKING RANDOM fluctuation for no discernible reason - honestly at times there is zero logic.
so ye, halluncinations… the brain is freaking wild.
Disclaimer - this is by no means an exhaustive list and like with many things every individual will experience these things slightly differently.
A similar post about delirium A similar post about fever
#hallucinations#whump community#whump thoughts#whump tropes#whump prompts#hallucination whump#drugged whump#mental illness whump#altered consciousness whump#whump resource#whump reference
886 notes
·
View notes
Text
whump details: travel on foot
so your whumpee has escaped their whumper. What now? Maybe they've been rescued by friends, or are lucky enough to have access to a vehicle or other transport system. If not... They're on their own. Likely on foot. And if they're going any sort of distance, there's going to be consequences on top of everything else.
Things that will slow a character down:
- existing injuries
- poor footwear
- adrenaline crash
- moving for more than an hour without food or water (or less if they're already malnourished)
- weather
Injuries your character may develop that complicate things:
- wear and tear to joints; hips, knees, and ankles
- blisters. A seemingly minor part of life but they will make walking hell for at least a few days
- overuse injuries for legs (and back or shoulders if they're carrying any supplies)
- possible dislocations in the leg joints, especially if they have prior weakness/injury
- old wounds becoming aggravated/complicating their movement
Recovery after the initial escape:
- a very fit character could cover 20+ miles relatively quickly. (Think marathon runners.) But even if your escaping living weapon or soldier can put out that much effort for the initial burst, they'll likely be incapacitated to some degree afterwards. If they aren't able to consume calories/drink water during this, they will crash HARD. Perfect time to have them collapse just outside a remote farmstead or cabin :)
- rest, food, and water are the most important things for recovery. If they collapse without any replenishing, they'll be practically bedridden by the time they wake up. Maybe they have to keep pushing because there's no other choice, but they will be worse for the wear
- a character used to travelling long distances will recover quickly with the proper tools. A character who isn't is going to be feeling the effects of their escape for weeks afterwards, if not months. They may struggle to walk for several days afterwards, and might come out the other side with long term injuries ---maybe even permanent ones
#source: i walked 18 miles for a challenge almost a month ago and my ankle STILL hates me#it was also at a reasonably quick pace so. firsthand experience of covering ground while conserving energy#especially as someone who has never gone that far#whump reference#whump prompt
97 notes
·
View notes
Text
Whump Aesthetics
Here’s a quick and handy list of my whump aesthetic posts, in case you want some inspiration :)
Blood aesthetic
Gothic illness aesthetic
Forced transformation aesthetic
Immortal whumpee aesthetic
Bandages aesthetic
Torture aftermath aesthetic
Lab whump aesthetic
Breath whump aesthetic
#whump#whumpblr#whump writing#whump community#whump prompt#whump inspiration#whump blog#whump aesthetic#whump prompts#whump ideas#whump reference#whump stuff
109 notes
·
View notes
Note
Let's say a character with some sort of crazy hearing/sensory enhancements has the ability to pick up on the sound of someone's heart beat. If they had this ability... theoretically, would they be able to hear a heart attack before the person felt it? What would it should like? How much notice would they be able to provide??
Ooh, really good question, anon.
The answer is... potentially.
In order to explain why, we have to talk a little about what hearts sound like to the people who are trained to listen to them.
A healthy heart has 2 sounds per beat- Lub and Dub, also called S1 and S2. You can hear this in your own heart or a friend's if you have a stethoscope (or just an ear you can press against a friend) and listen at one of these locations:
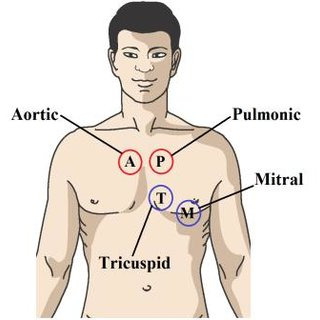
You'll hear a heart that probably sounds like Lub-Dub Lub-Dub Lub-Dub, etc... The Lubs are S1 and the Dubs are S2. One Lub-Dub (S1-S2) cycle is a single heart beat.
But there are other sounds that can be heard if someone has a problem with their heart. For example, if one of the heart's 4 valves has a leak in it, you might hear a "Shhh" sound somewhere between or around the Lub and Dub. Like Lub-Shhh-Dub or Lub-Dub-Shhh. Depending on which part of the chest the "Shhh" sound is audible, you can tell which valve is faulty.
You might also hear an S3 or S4 sound. S3 and S4 are "extra" sounds that occur during the heart cycle. An S3 sound is like a "Uhh" and happens at the end of the Dub (Lub-Dub-Uhh). An S4 sound sounds like a "Buh" and weirdly enough happens before the Lub (Buh-Lub-Dub).
For the purpose of your question what we really want to focus on is that S4 sound. This is a sound that almost universally occurs in the early stages (first 1-3 days) of a heart attack.
See, the S4 sound is the sound of the top of the heart (atrium) straining as it tries to push blood into a damaged, overgrown, or swollen lower part of the heart (ventricle). Since heart attacks cause damage to the ventricle(s), you get this sound pretty soon after the damage starts occurring. You can even tell where the damage is in the heart (left or right) by where on the chest you hear the S4 most clearly.
But since heart attacks are not the only reason for damage to the ventricle, hearing an S4 sound does necessarily mean that a heart attack is currently occurring. It could have been that the person has had a heart attack in the past and they have scarring on their ventricle(s). It could also mean that they have had high blood pressure for a long time and their left ventricle is bigger and stiffer than it is supposed to be. It could be that they have heart failure and there is more pressure in their ventricles than there should be. It could be that they had an infection in their heart that left scarring in the past. It could be a problem they were born with.
Since these are all chronic problems, what your character would have to notice is a sudden start of an S4, probably combined with other symptoms. When the S4 sound starts, these symptoms might not be the "classic" heart attack symptoms yet. They might be feeling "off" or more out of breath than usual, or more tired than usual, or they might have some mild nausea or indigestion.
Your character might be able to provide at least a few hours of notice before the more classic symptoms show up.
209 notes
·
View notes
Text
Kinda whump, kinda med reference, kinda real life:
My brother fell asleep so hard in class the other day that they literally thought he was having a medical emergency and called EMS.
He’s fine, he was also completely fine at the time too, just, so tired that he wasn’t waking up even with all the noise and light shaking. (He had stayed up all night then rode his bike to school super early, all against the rules but he had good intentions)
So, fun scare to possibly give caretakers, a whumpee who is so sleep deprived that when they do sleep, they sleep so hard you think they’re going to die and/or are dead.
66 notes
·
View notes
Text
Reference: Psychogenic Fever
You've seen it in anime loads of times: the protagonist overexerts themselves or experiences a highly stressful event, and they dramatically collapse. The next thing you know, they're in bed with a cloth over their forehead and an ally informs the rest of us that they have a fever.
Well, it turns out that can actually happen.
If your immune system is already shot, and you experience acute levels of stress, your body will respond to those stress hormones the way it would normally respond to a virus. Your core heats up, and you develop a full-blown fever.
According to what information I was able to dig up, some patients can develop core temperatures of 41°C/105°F. I didn't apparently record mine when this was going on, but given the temperature dysregulation caused by the seroquel I take that prevents me from cooling off if I get hot and the reverse, and how hot literally anything I touched got, I was probably in that higher range.
The Progression:
I went to bed at around 1:45 a.m. I'd already been through so much stress with my grandfather's funeral, how my dad elected to process grief, and scrambling to get the SSI-D function report that had arrived in our mailbox when I was out of town returned on time, I had already crashed out earlier that day from the energy expenditure. Now, I have ME/CFS, and crashing out after exertion/stress is normal, so nothing stood out as a warning sign. If there was one, I dismissed it as my usual fatigue. I went to sleep.
I woke up about 2.5 hours later, experiencing sleep paralysis--presumably in lieu of a fever dream. When I woke up the rest of the way, I was sweating profusely and feeling about like I'd been mowing the lawn in 105° heat. I've done that, and collapsed from heat exhaustion from it, before. I was hotter at that moment than I had been back then.
I put a wrist to my forehead, and the sensation was like holding a hairdryer on high to my forehead at point-blank range. My pillow was just as hot, and no amount of flipping fixed that. (I should point out here that I normally run cold--ridiculously cold, sleep with the quilt up in the middle of a Texas summer cold--and this never happens unless I am very sick.)
I smelled like fever. Some people don't think you can smell fevers, but I was a sickly child and spent so much of my life in pediatricians' waiting rooms full of feverish children that after a while I noticed a particular smell unique to those environments. Since then, I've been able to accurately identify it elsewhere by that smell.
I was completely confused. I'd had to go into the grocery store without a mask earlier that day because I ran out, but even I don't present that quickly. It couldn't be from that. Some old geek part of me remembered Anime Fever, and on a hunch, I googled "can you give yourself a fever from stress?" And yes. Yes, you can.
I sat up, and when I touched the mattress where I had been sleeping with one hand, it felt like trying to pick a dish up out of the dishwasher immediately after it's through running. It was that hot.
The recommended treatment was anti-inflammatories and any relevant psych meds that can reduce anxiety, so I took 800mg of ibuprofen and an extra, small dose of seroquel. Then I took my clothes off and downed a few bottles of water, my usual trick for cooling down once I've gotten too hot, and sat on the foot of my bed to give my mattress time to cool down before getting back in bed to try to sleep.
The fever broke at around 6:15 a.m., and I was finally able to rotate back to the other side of my mattress and pillow, and go back to sleep. I slept until 1:20 p.m.
The Takeaway: This is a real phenomenon! Use it on your whumpees with poor immune systems, either naturally or broken down from their ordeal. It's no longer just an anime trope.
#whump reference#whump#whump prompt#whump community#whump scenario#whumpee#whump tropes#whump prompts#whumpblr#writing#writing reference#my life is a whump prompt#edit: fixed brain fog word omissions#edit: felt like the sleep paralysis was worth mentioning
123 notes
·
View notes
Note
I saw ur really informative post on conditioning and said with whumpers uts about using pain again and again
Any advice about caretakers deconditioning?
[ Referring to this post. ]
The first and most important thing is that the caretaker cannot decondition the whumpee. It's not possible. That progress is entirely internal, and requires a massive amount of introspection, self-motivation, and practice from the whumpee themself. No one else can do it for them.
But what the caretaker can do is be there for them while the whumpee fights toward their own recovery. They can be the stability that whumpee needs in order to work through these massive problems on their own.
Deconditioning is awful. It involves repeated failure, over and over and over, working toward lessening the response. And it is incredibly frustrating, painful, heartbreaking, and at times it feels completely hopeless.
Progress is so non-linear that they can spend months improving and then backslide nearly back to the beginning if they get caught off guard. At times it'll feel like they're stuck at the same point and can't get any further. Like a future where they will be free of it may simply not exist.
At many points, your whumpee is going to feel heartbroken. They're going to spiral into, "Why can't I do this? Why can't I make it stop?" and, "I thought I was past this." and, "Will I ever be able to undo what whumper made me?"
A good caretaker can be there to comfort them when things go wrong. They can hold them while they cry. They can listen to them when they go into a sobbing, breathless rant about how much this hurts. They can make sure that whumpee knows they have someone who doesn't think of them as broken or lesser because of what they've gone through.
Depending on if whumpee feels it would help, they might help them brainstorm a reward system. If there's a situation where they're around other people and the caretaker spots the trigger coming, they can try to redirect conversation away from it before it hits. Preferably without anyone realizing they're doing it for whumpee's sake. When whumpee has just been triggered and wants nothing more than to be alone, the caretaker can make sure their boundaries are respected. To make sure they have somewhere safe to go.
Even more importantly, they can also help by highlighting the moments of whumpee's progress. Pointing out their successes, no matter how small. Pointing out how far they've come. Reminding them that the ups and downs are supposed to happen. That trauma recovery is a rollercoaster, not a straight line.
As a whumpee in that state, it's very easy to feel like they're making no progress. That even when they succeed, the tiny bits of success are hollow, because 'they shouldn't be like this in the first place'. Have your caretaker help them see their own victories. Help them actually see the healing as it grows.
A realistically conditioned whumpee does not need someone to fix them. They need someone to be there for them while they save themselves.
---
This was such a good ask, thank you for sending it my way!
#ask Wick#conditioned whumpee#bbu whump#box boy universe#box boy whump#whump recovery#caretaker#pet whump#whump writing#writing advice#whump reference#writing reference#captive whumpee#rescued whumpee
230 notes
·
View notes
Text
Blocking the Neuromuscular Junction
Neuromuscular blocking agents (NMBAs) stop transmission at the junction between nerves and muscles, which will cause partial or complete paralysis. Why do we want to do this? The main reason is to cause paralysis for starting endotracheal intubation (relax throat muscles), surgery (keep the patient still), and for putting people on ventilators (stop them from fighting against the machine).
You might also give someone an NMBA if they are coughing up blood, having a severe asthma attack, have high intracranial pressure, or are shivering with hypothermia.
There are two types of these drugs and they work two different ways, though they are all given intravenously.
Depolarizing NMBAs
So to initiate muscle contraction, our body uses a transmitter called ACh. When this binds to a receptor, some ions move around and the muscle contracts. This is called depolarization. After some time, the cell can repolarize as ACh is digested by the enzyme AChE.
The main depolarizing NMBA is Succinylcholine. This also binds to the same receptor, causing muscle contraction. However, it is not digested by AChE, so the cell cannot repolarize. The muscle will keep contracting until it runs out of calcium ions and relaxes. The muscle is paralyzed after that because the receptor is still blocked. Only when the serum enzyme BChE digests it can we reactivate the muscle.
Succinylcholine is mostly used for intubation. It only lasts for a few minutes, which is good because once you trach someone you don't need to paralyze their throat anymore.
The main risks of this drug are hyperkalemia (potassium exits the cell when the muscle is depolarized), muscle pain, hyperthermia, and increased intraocular pressure. Succinylcholine is contraindicated in burn patients.
Nondepolarizing NMBAs
These drugs also act on the ACh receptor, though they do not activate it. The most common ones are atracurium, cisatracurium, vecuronium, and rocuronium. I'll go through a few important notes on each one.
Atracurium (an isoquinoline) is metabolized into the active laudanosine, which has a stimulating effect on the central nervous system and can cause seizures. It also increases histamine, which can cause flushing. Cisatracurium is also an isoquinoline, but it does not cause an increase in histamine or break down into laudanosine. Both of these can be reversed using neostigmine to up the concentration of ACh and outcompete them at the receptor.
Rocuronium and vecuronium are both aminosteroids. Rocuronium has a quick onset and is great for rapid sequence intubation. It also does not require dosage adjustment for those with renal impairment. Vecuronium is slower, and needs to be adjusted for those with renal and liver impairment. These can both be reversed with sugammadex, which will form a complex that can be pissed out. The only thing with sugammadex is that it can cause bradycardia, decrease the effectiveness of contraceptives, and increase the risk of bleeding.
The adverse effects of all of the nondepolarizing NMBAs are apnea, hypotension, and electrolyte imbalance. You also need to increase the dose for those with burns and trauma. These drugs also interact with volatile anesthetics, increasing their effects. However, this is actually a favorable effect, as it lowers the dose of anesthetic required.
Using These Drugs
The main thing to remember here is that NMBAs do not cause sedation or amnesia. You must use them with things like propofol, midazolam, benzodiazepines, opioids, etc. I will repeat: DO NOT USE THESE DRUGS ALONE. The patient will be paralyzed but CONCIOUS and AWARE. For the love of medicine, please. The reason I say this is because I have seen paramedics give "problem patients" a paralytic without a sedative in some sick sort of revenge. Fuck them. I don't care what a patient did, that is not okay to do. Still makes me mad just thinking about it.
Anyways, so these are one part of the drugs required for surgery. If you just sedate someone, they'll still move around, and you don't want that while you are cutting on them.
Writing Tips
There isn't too much to say here, but I think it is important for people to know these drugs exist and only paralyze, not sedate. So shit, if you wanna write some crazy horror stuff happening, you can just have someone be paralyzed. Or also this is how people can be aware during surgery. I think there was a big case about this a few years ago. Sensation is still intact when these drugs are given alone, so go forth and torture people I guess (??) - IN FICTION
Anywho, that's all, thanks for reading. Maybe I will write soon about intubation, sedatives, and other stuff like that. Kinda neuro (which one the poll).
#medicine#medical writing#med studyblr#med school#med student#medical school#whump writing#medications#neurology#hospital whump#whump reference
23 notes
·
View notes
Text

tie a guy up references (more under the cut)





#aka i took a video of my shoulder stretches to get an actual look at my mobility (no mirrors in my gum for aome reason)#and it looked pretty promising as a whump ref so i took another video at a better angle and got some screencaps :D#whump reference#art reference#whump photography#calico is befuddled#whump meta#whump art ref
118 notes
·
View notes
Text
CW: irl whump reference, fainting
I started to black out while exercising and got spots across my vision even though my eyes were closed. Like that reddish field that you see with closed eyes when the lights are on? Yeah that got black splotches. Very interesting. Could be useful.
8 notes
·
View notes
Note
Can you tell me about bruises? I've been trying to research but I think I'm pretty terrible at it. One thing I can't seem to find an answer to is how quickly they form? Like, if I have my blorbo take a hit, how long until the area is black and blue? Does it depend on some factors? What are those factors? TIA!
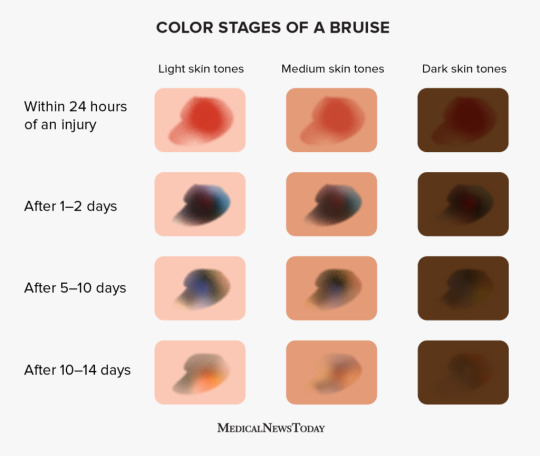
This is the best reference I have found for what bruise stages look like. Generally the "within 24 hours" section starts within 1-2 hours.
153 notes
·
View notes