
For my future baby honey!
this is my my 2nd blog for my baby fever!
original is evilsbabygirl
81 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs

dailyjennie
Daily Jennie

etherealempowerment
Ethereal Empowerment

luckybonkpizzacash
Untitled

meyersthorsen57
The Blogging of Thorhauge 828

littlesis89
Baby Gemini
Text
Pregnancy - physiology
Hormones
hCG - human chorionic gonadotropin - present in blood and urine, produced by blastocyst and placenta
Low levels of hCG could mean miscarriage, ectopic pregnancy, miscalculation of dates
High levels = molar pregnancy (cells that normally form a baby dysfunction and form cysts instead), multiple pregnancy (twins etc), miscalculation of dates
Progesterone increases fat deposition in early weeks and stimulates appetite
Increased oestrogen from corpus luteum promotes mammary gland development (breasts enlarge)
And inhibits ovulation via negative feedback [OES decreases GnRH release by hypothalamus –> linhibition of FHS and LH –> no ovulation]
Relaxin (secreted by corpus luteum) softens connective tissue in preparation for labour - not specific, all joints can be affected
Peaks in early and late pregnancy
Physical changes

Blood pressure
As early as 4 weeks into pregnancy
plasma volume increase
caused by the affects of oestrogen and progesterone on the kidneys

OES and Prg cause vasodilation
less resistance = less pressure
Heart rate increases by 25% to compensate
stroke volume increases
increased overall cardiac output by 50% in third trimester
Direct action of enlarged uterus:
compresses the descending aorta and inferior vena cava
decreased venous return - less blood in means less blood out, less blood in ventricle –> reduced pressure on walls –> reduced force to exit –> reduced placental perfusion
increased aortic pressure
increased heart rate
[shouldn’t sleep on back for this reason]
Outcomes:
Fall in blood pressure (can cause collapse if serious)
Can cause foetal hypoxia even without mother symptoms

Haematological changes
red cell mass increase by 20% (renal - increased erythropoietin production in response to detection of blood oxygenation and sodium/water balance)
Plasma volume increases more than RBC count does, causing the impression of decreased haemoglobin (anaemia)
Increased tendency to clot (hypercoagulable)
due to increase in clotting factors and plasma fibrinogen
platelet production increase (however count drops due to increase in activity and consumption) - function remains normal]
WBC count may increase due to an increase in granulocytes
Respiratory changes
Increased chest diameter, diaphragmatic expression and elevation
dyspnoea common (difficulty breathing)
breathing becomes more costal (mouth) than abdominal
mainly mediated by progesterone levels (cause bronchial and smooth muscle relaxation and hypersensitivity to CO2)
Changes to the urinary system
cardiac output increase –> increase in renal plasma flow and glomerular filtration
increase in urea, creatinine, urate and biocarbonate clearance
with progesterone, renin and aldosterone up water retention increases
can lead to urinary stasis and increased risk of UTI
Any drugs given that are excreted renally must be given in much higher quantities consequently
Gastrointestinal changes
Appetite increase + cravings
Gastric reflux sphincter relaxation (increased indigestion, also due to increased intra-gastric pressure (expanding uterus))
gallbladder dilated
GI motility decreased and transit time slower
albumin and protein decrease
cholesterol twice normal value
Muskuloskeletal
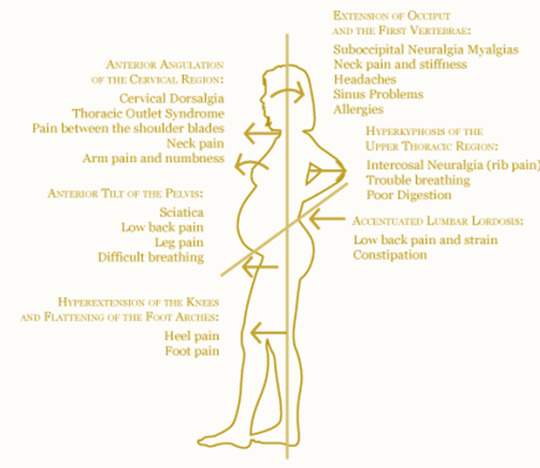
Calcium reuptake into bloodstream results in mild decalcification of bones
relaxin softens joints (pubic symphysis + alters gait (waddling))
abdominal muscles stretch to elastic limit
stretch marks (stria gravidarum) caused by rupture of elastic fibres and small blood vessels
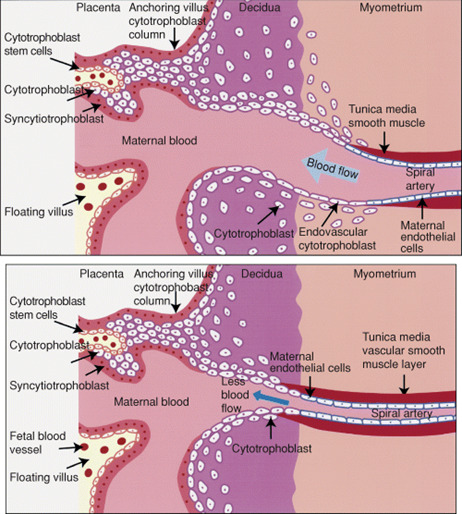
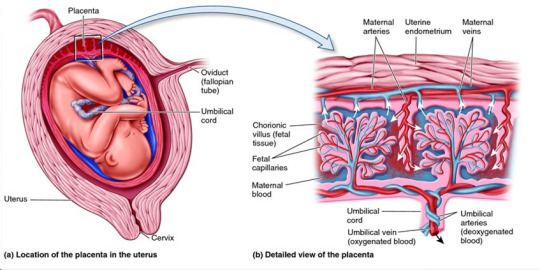
Reproductive changes
Massive increase in mass
Placenta growth (nutrition, excretion, immunity, endocrine)
Parental blood supply
2K notes
·
View notes
Text
“Pregnancy is a beautiful thing, and I believe it should be celebrated; whether it lasts 3 weeks or 9 months.”
— @myrainbowboyandme
5K notes
·
View notes




Text
If I have a child and it's female I have two names I like and because of the ace family . I love the name Elle and aláia.
1 note
·
View note
Text
So it's been a few months and I am not pregnant I got my depo shot today and took a pregnancy test before and it was negative I was secretly hoping it was positive and got my hopes up. So kinda upset about that still. When it's time it's time I guess.
1 note
·
View note
Text
The bump
I just want that cute baby bump. I want people to look at it and smile. I want to feel that little life moving inside me. I need this.
I’m so scared it won’t happen. Ever.
1K notes
·
View notes
Text
Updateeeee
lately I've been having symptoms of pregnancy and have this gut feeling that I am. So I took an at home pregnancy test and if it does turn out how it's suppose to I'll get a real pregnancy test. So in 4 hours I'll update with the results.
2 notes
·
View notes
Text
I hope
I keep seeing pregnancy things on Facebook, pregnant women in person and just everywhere I honestly think it’s a sign mabey the universe is hinting at me that it’ll happen for me soon .
5 notes
·
View notes
Text
Ouch
My jaw hurts today had a bad ear infection last week hopefully nothing spread to my jaw.
0 notes
Text
Omg
My 18month old niece got 6 shots today and blood taken and they wernt no baby needles. I feel so bad . No way in hell will I let my baby get that many shots I'll reschedule for two then rest a different time . She's in so much pain You can tell. I love you li
0 notes
Text
I'm ready
I'm so ready to be a mommy even tho the timings not right. I just want a baby so bad lol. When the time comes I pray your a happy and healthy baby.
6 notes
·
View notes
Text
My child is gonna have so many things, I'm gonna get her/him puzzles, drawing stuff,playdough, all that kinda stuff. tomagochis, and pixel chixs. I can't wait!
1 note
·
View note