
18+ page. Comfortably AMAB but huge issues with the oppressive, non-consensual power dynamics typical of societal gender constructs. Feeder for the right partner. Mix of my interests evident here.
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by curiouscontrast and here's what we found interesting.
Average Info
Notes Per Post
308K
Likes Per Post
170K
Reblog Per Post
137K
Reply Per Post
460
Time Between Posts
16 days
Number of Posts By Type
Text
17
Last Seen Tumblr Blogs





Fun Fact
70% of Tumblr users say the Dashboard is their favorite place to spend time online.
Text
THE ENTIRE WEST IS BEING PUT UP FOR SALE AND I AM BEGGING YOU TO CALL YOUR SENATORS

Trump’s budget bill has many, many things in it, but buried amongst it is the MILLIONS OF ACRES OF PUBLIC LAND FOR SALE.
This is the entirety of the Arizona state forests, the entire Cascades mountain range. Swathes of pristine desert around the national parks in Utah. On the doorstep of Jackson Hole.
THIS BILL IS BIG, BUT IT CAN BE AMENDED AND ABSOLUTELY MUST NOT PASS AS IS please.
If you have ever enjoyed the wilderness, we stand to lose it all forever.
CALLING your senators - NOT JUST IN THE WEST. ALL SENATORS, is CRUCIAL.
Outdoor alliance has a great resource for reaching out.
I don’t have a huge following but please, everywhere I have ever loved, the forests I grew up playing in, the land I got married on, is all at risk and I am begging.
52K notes
·
View notes
Text
Anti-Obesity Drugs in Sociopolitical Context
Abstract
This literature review critically examines the use of Body Mass Index (BMI) as a diagnostic tool for obesity, highlighting its historical and scientific flaws. The diagnosis and treatment of obesity is heavily stigmatized and reflects deeper socio-economic and racial biases. Fatphobia, or anti-fatness, is deeply rooted in white supremacy and colonial history. I argue that anti-fatness and weight-based discrimination significantly impact health outcomes, rather than body fat percentage alone. The way that the medical system focuses on body size rather than the overall health of patients perpetuates harm and yields even poorer health outcomes. To genuinely improve the lives of fat individuals, we must dismantle anti-fat systems and remove barriers to healthcare, job equity, and basic infrastructure by implementing legal protections, rather than simply promoting weight loss. This review emphasizes the need for a holistic approach to health that considers socio-economic factors and systemic discrimination.
Journal Summary
Recently, two anti-obesity medications, Ozempic and Wegovy, which are primarily prescribed for type 2 diabetes mellitus (T2DM), have shown promise in causing weight loss. The 2022 scientific journal “Ozempic and Wegovy for Weight Loss, Pharmacological Component and Effect” by Abdullah Mohammed, et al explores the pharmacological components and effects of these medications on weight reduction, summarizing findings from existing clinical studies.
Ozempic is a glucagon-like peptide-1 (GLP-1) receptor agonist primarily used to manage T2DM. Clinical studies indicate that semaglutide can also promote significant weight loss. Ozempic's mechanism involves binding to GLP-1 receptors in the brain, reducing food intake and increasing feelings of fullness. This leads to a decrease in body weight and improvement in glycemic control. Wegovy, also a GLP-1 receptor agonist, is the same drug as Ozempic but two times the dose, specifically approved for weight loss for fat people even without T2DM. Administered as a weekly injection, Wegovy has shown effectiveness in inducing sustained weight loss. The STEP trials demonstrated that participants using Wegovy experienced an average weight loss of 15.8% over 68 weeks. Wegovy's pharmacokinetics involve prolonged activation of GLP-1 receptors, enhancing satiety and reducing hunger. GLP-1 receptor agonists like semaglutide mimic the action of the natural hormone GLP-1, which regulates appetite and blood sugar levels. By slowing gastric emptying and promoting a feeling of fullness, these medications reduce caloric intake. Clinical trials have shown that GLP-1RAs, including semaglutide, can result in weight loss from 5% or up to 10-15% of body weight. However, sustained weight loss requires ongoing lifestyle modifications, as discontinuation of the medication leads to weight regain. Common side effects of GLP-1 receptor agonists include gastrointestinal issues such as nausea, vomiting, diarrhea, and constipation. Other potential side effects include increased heart rate, fatigue, headaches, and changes in thyroid function.
Obesity as a Disease
How does one get an obesity diagnosis? There is one single criterion used for diagnosing someone with this disease: The Body Mass Index (BMI). A person’s BMI is their weight in kilograms divided by the square of their height in meters, rounded to one decimal place. It does not account for muscle mass versus body fat. For these reasons, the BMI has been widely proven to be an ineffective health measure. The BMI was also never intended to be a measure of health in the first place.
The BMI was created in the 1800s by a statistician named Adolphe Quetelet, who did not study medicine, to gather statistics of the average height and weight of specifically white, European, upper-middle-class men to assist the government in allocating resources. It was never intended as a measure of individual body fat, build, or health (Karasu, 2016). Quetelet is also credited with founding the field of anthropometry, including the racist pseudoscience of phrenology. Quetelet’s L’homme Moyen would be used as a measurement of fitness to inspire, and as a scientific justification, for eugenics (Eugenics archive).
Studies have observed that about 30% of "normal” weight people are “unhealthy," whereas about 50% of "overweight" people are “healthy” (Rey-López, et al, 2014). Thus, using the BMI as an indicator of health misclassifies 75 million people in the United States alone. “Healthy*” lifestyle habits are associated with a significant decrease in mortality regardless of baseline body mass index (Matheson, et al, 2012).
*I put “healthy” in quotation marks here because the definition of an individual’s health is oversimplified and depends on many socioeconomic factors.
While epidemiologists use BMI to calculate national obesity rates, the distinctions between weight classes can be arbitrary. Ever notice that the weight classes on the BMI are nearly intervals of five? In 1998, the National Institutes of Health lowered the overweight threshold from 27.8 to 25—making roughly 29 million Americans "overweight" overnight—to match international guidelines (Butler, 2014). Critics have also noted that those guidelines were drafted in part by the International Obesity Task Force, whose two principal funders were companies making weight loss drugs.
Jackie Scully, Senior Research Fellow at the Unit for Ethics in the Biosciences, University of Basel, in her scientific journal titled “What is a Disease?” states the following: “As the business literature shows, new clinical diagnoses are often welcomed primarily as opportunities for market growth (Moynihan et al, 2002). One recent example of this is female sexual dysfunction (FSD). The huge commercial success of sildenafil (Viagra) for erectile dysfunction in men provides a strong motivation for drug companies to identify an equivalent market (that is, condition) in women. And some ethicists feel that drug companies were, to put it mildly, over-involved in the medical consensus meetings held between 1997 and 1999 that effectively drew up very inclusive clinical criteria for the definition of FSD (Moynihan, 2003)."
How can one diagnose a person with a disease and sell them medications solely based upon an outdated measure that was never meant to indicate health in the first place, especially when obesity has no proven causative role in the onset of any chronic condition? (Kahn, et. al., 2000), (Cofield, et al, 2010).
This is why the term “obese” is recognized as a slur by fat communities. It's a stigmatizing term that medicalizes fat bodies even in the absence of disease. The word directly translates to "having eaten oneself fat" in Latin. Obesity, as a medical diagnosis, doesn’t have much ground to stand on. Aside from being overtly incorrect as a medical tool, the BMI is used to deny certain medical treatments and gender-affirming care, as well as insurance coverage. Employers still often offer bonuses to workers who lower their BMI. Although science recognizes the BMI as deeply flawed, it's going to be tough to get rid of. It has been a long-standing and effective tool for the oppression of fat people and the profit of the weight loss industry.
To treat obesity, patients must eat less. Making someone smaller still means they will be healthier, right?
Fatness and Mortality
The idea that obesity is unhealthy and can cause or exacerbate illnesses is a biased misrepresentation of the scientific literature that is informed more by bigotry than credible science (Medvedyuk, et al, 2017). Fatphobia existed long before fatness became medicalized. Yes, obesity is correlated with conditions such as cardiovascular disease, hypertension, and diabetes, but some scientists are looking into possibilities that don't equate correlation with causation. Obesity has no proven causative role in the onset of any chronic condition (Kahn, et al, 2000), (Cofield, et al, 2010) and its appearance may be a protective response to the onset of numerous chronic conditions generated from currently unknown causes (Lavie, et al, 2009), (Uretsky et al, 2007), (Mullen, et al, 2013), (Tseng, 2013). A portion of these correlated conditions are likely brought on by the stress of being part of one or more marginalized groups with little to no support or basic access in society. Weight stigma itself is deadly. Research shows that weight-based discrimination increases risk of death by 60% (Sutin, et al, 2014).
Dieting also poses serious health risks. The reason that these weight loss drugs are so successful by comparison is that dieting is unsustainable and does not lead to prolonged weight loss. Over 50 years of research conclusively demonstrates that virtually everyone who intentionally loses weight by manipulating their eating and exercise habits will regain the weight they lost within 3-5 years, and 75% will regain more weight than they lost (Mann, et al, 2007). Evidence suggests that repeatedly losing and gaining weight is linked to cardiovascular disease, stroke, diabetes, and altered immune function (Tomiyama, et al, 2017). If most fat people have historically tried to lose weight their whole lives through dieting, this has major implications on overall health. Prescribed weight loss is also the leading predictor of eating disorders (Patton, et al, 1999).
Another factor that may be impacting fat people’s rate of mortality is that they are being mistreated at the doctor’s office. I have personally heard dozens of stories about doctors refusing to treat or investigate a problem that a fat person came in for until they lost a certain amount of weight, only to discover years later that the problem was unrelated to their weight and has progressed severely because it went untreated. Fat people are often mistreated and looked at with disgust and disdain in medical settings, leading them to avoid going to the doctor in shame or fear of abuse. This can seriously worsen health issues. Fat stigma in the medical establishment (Puhl, et al, 2012) and society at large arguably (Engber, 2009) kills more fat people than fat does (Teachman, et al, 2003), (Chastain, et al, 2009), (Sutin, et al, 2015). This impact is too significant not to be taken under consideration.
Anti-Fatness as Anti-Blackness
The issue of anti-fat bias is directly rooted in white supremacy. The ideal thin body was constructed as a marker of whiteness and “purity” before any of this was ever made to be about health. Dr. Sabrina Strings has spent her career studying this history. In her book, Fearing the Black Body: The Racial Origins of Fat Phobia, Dr. Strings discusses how constructions of race led to the thin ideal. “Over the decades, the rise in biracial children would break down the way that slave owners saw Blackness and whiteness. To combat the hypocrisy they created, owners invented new ways to dehumanize the enslaved population. They made a calculated decision to start putting more value on white physiques versus Black ones. In her research, Strings found that Black women’s bodies were otherized even more than Black males. For colonizers who hadn’t seen diverse body types before, they quickly categorized the Black female figure as ‘deviant,’ ‘greedy,’ and ‘overtly sexual.’ The fact that we still use these terms to describe fat bodies today is all the evidence we need to understand that fatphobia is directly linked to racism, not health. This mindset was also strengthened by Protestantism. Slave owners looked for any way to prove their power over the enslaved people, and they frequently used religion as ‘proof’ of their racist superiority. Additionally, Protestant belief encouraged various ways to become closer to God, which included eating as little as possible. This would resonate the most with white women. They had as much to do with perpetuating fatphobia as their husbands. White women were desperate to show their own power against Black women on the plantation, and the difference between their bodies was the perfect rift. And so began the centuries-old belief that thinness is beautiful, and fatness is ugly” (Sassenrath, 2023).
Revisiting the Journal with Context
Thinness has been an important value throughout history in the United States. Our positive associations with thinness and negative associations with fatness have led to a collective schema that is black and white, good versus bad, beautiful versus ugly, healthy versus unhealthy, and life versus death. This has led the FDA to approve Wegovy as a weight loss drug with haste, after just sixteen months of testing. It is known that going off the drug will result in rapid weight regain, so patients are expected to be on it for the rest of their lives when there have been no long-term studies. We do not yet know if the drug will have long-term effects, yet it has been approved for kids as young as twelve (FDA, 2021). As of July 2024, Novo Nordisk has a market cap of $633.01 billion (Marketcap).
Wegovy is prescribed along with diet and exercise, which has been proven to lead to weight regain and eating disorders. Patients are being prescribed Wegovy and Ozempic when they are fat, but otherwise metabolically healthy. If this drug is truly a game changer for public health, we should be measuring how patients' health improves over the long-term rather than how much weight they lose. For example, if these drugs improve heart health, they should be prescribed as a heart health medication for patients with heart disease, rather than prescribed as a weight loss fix based on body size alone. With the evidence we have, we know it is possible to be fat and healthy, so these drugs may be solely cosmetic in many cases.
Future
If we want to improve the lives of fat people, we will remove barriers to care, not try as hard as we can to make all fat people disappear. That will never happen. If we truly cared about the well-being of fat people and not their disappearance, we would work to dismantle the systems that oppress them and abolish anti-fatness.
Currently, fat people have next to no legal protections for being discriminated against (NAAFA, 2023). Fat people are denied housing, (Kariss, 1977) jobs, and receive less pay and promotions legally because of their size (The Economist). They are denied access to clothing, seating, transportation, and other human rights because infrastructure has been designed to exclude them. Fat people have less likelihood of receiving a fair trial (Beely, 2013), and are denied necessary surgeries (Barrett, 2022) ––but not weight loss surgery that amputates the digestive tract. Fat people are denied gender-affirming care (Conley, 2023), in vitro fertilization and reproductive healthcare (Muir, 2024), even adopting children (Carter, 2009). Fat children have been removed from their loving parents because when their diets failed, it was seen as neglect (Badshah, 2021). Fat people have disproportionately high suicide rates (Wagner, et al, 2013), and are facing medical malpractice and mistreatment (Kolata, 2016).
Can a drug fix that?
References
Karasu, Sylvia. Adolphe Quetelet and the Evolution of Body Mass Index (BMI). Psychology Today. https://www.psychologytoday.com/us/blog/the-gravity-of-weight/201603/adolphe-quetelet-and-the-evolution-of-body-mass-index-bmi 2016, March 8.
“Quetelet, Adolphe.” Eugenics Archive, www.eugenicsarchive.ca/connections? id=5233cb0f5c2ec5000000009c. Accessed 5 July 2024.
Rey-López JP, de Rezende LF, Pastor-Valero M, Tess BH. The prevalence of metabolically healthy obesity: a systematic review and critical evaluation of the definitions used. ObesRev.2014 Oct;15(10):781-90. doi: 10.1111/obr.12198. Epub 2014 Jul 16. PMID: 25040597.
Matheson EM, King DE, Everett CJ. Healthy lifestyle habits and mortality in overweight and obese individuals. J Am Board Fam Med. 2012 Jan-Feb;25(1):9-15. doi: 10.3122/jabfm.2012.01.110164. PMID: 22218619.
Butler, Kiera. “Why BMI Is a Big Fat Scam.” Mother Jones, 25 Aug. 2014, www.motherjones.com/politics/2014/08/why-bmi-big-fat-scam/.
Kahn BB, Flier JS. Obesity and insulin resistance. J Clin Invest. 2000 Aug;106(4):473-81. doi: 10.1172/JCI10842. PMID: 10953022; PMCID: PMC380258.
Cofield SS, Corona RV, Allison DB. Use of causal language in observational studies of obesity and nutrition. Obes Facts. 2010 Dec;3(6):353-6. doi: 10.1159/000322940. Epub 2010 Dec 10. PMID: 21196788; PMCID: PMC3280017.
Medvedyuk, S., Ali, A., & Raphael, D. (2017). Ideology, obesity and the social determinants of health: a critical analysis of the obesity and health relationship. Critical Public Health, 28(5), 573–585. https://doi.org/10.1080/09581596.2017.1356910
Kahn BB, Flier JS. Obesity and insulin resistance. J Clin Invest. 2000 Aug;106(4):473-81. doi: 10.1172/JCI10842. PMID: 10953022; PMCID: PMC380258.
Lavie CJ, Milani RV, Ventura HO. Obesity and cardiovascular disease: risk factor, paradox, and impact of weight loss. J Am Coll Cardiol. 2009 May 26;53(21):1925-32. doi: 10.1016/ j.jacc.2008.12.068. PMID: 19460605.
Uretsky S, Messerli FH, Bangalore S, Champion A, Cooper-Dehoff RM, Zhou Q, Pepine CJ. Obesity paradox in patients with hypertension and coronary artery disease. Am J Med. 2007 Oct;120(10):863-70. doi: 10.1016/j.amjmed.2007.05.011. PMID: 17904457.
Mullen JT, Moorman DW, Davenport DL. The obesity paradox: body mass index and outcomes in patients undergoing nonbariatric general surgery. Ann Surg. 2009 Jul;250(1):166-72. doi: 10.1097/SLA.0b013e3181ad8935. PMID: 19561456.
Tseng CH. Obesity paradox: differential effects on cancer and noncancer mortality in patients with type 2 diabetes mellitus. Atherosclerosis. 2013 Jan;226(1):186-92. doi: 10.1016/ j.atherosclerosis.2012.09.004. Epub 2012 Sep 21. PMID: 23040832.
Sutin, A. R., Stephan, Y., & Terracciano, A. (2015). Weight Discrimination and Risk of Mortality. Psychological Science, 26(11), 1803-1811. https://doi.org/10.1177/0956797615601103
Tomiyama, A Janet, et al. “Long‐term Effects of Dieting: Is Weight Loss Related to Health. Socialand Personality Psychology Compass, 6 July 2017, escholarship.org/uc/item/0tv27311.
Mann T, Tomiyama AJ, Westling E, Lew AM, Samuels B, Chatman J. Medicare's search for effective obesity treatments: diets are not the answer. Am Psychol. 2007 Apr;62(3):220-33. doi: 10.1037/0003-066X.62.3.220. PMID: 17469900.
Patton GC, Selzer R, Coffey C, Carlin JB, Wolfe R. Onset of adolescent eating disorders: population based cohort study over 3 years. BMJ. 1999 Mar 20;318(7186):765-8. doi: 10.1136/bmj.318.7186.765. PMID: 10082698; PMCID: PMC27789.
Puhl, Rebecca, and Kelly D. Bronwell. “Bias, Discrimination, and Obesity.” Obesity Research, 6 Sept. 2012. doi.org/10.1038/oby.2001.108
Engber, Daniel. “Glutton Intolerance: What If a War on Obesity Only Makes the Problem Worse?” Slate, https://slate.com/technology/2009/10/the-health-effects-of-discrimination-against-fat-people.html 5 Oct. 2009.
Teachman, B. A., Gapinski, K. D., Brownell, K. D., Rawlins, M., & Jeyaram, S. (2003). Demonstrations of implicit anti-fat bias: The impact of providing causal information and evoking empathy. Health Psychology, 22(1), 68–78.
Chastain, Ragen. “So My Doctor Tried to Kill Me.” Dances With Fat, https://danceswithfat.org/2009/12/15/so-my-doctor-tried-to-kill-me/ 15 Dec. 2009.
Sutin AR, Stephan Y, Terracciano A. Weight Discrimination and Risk of Mortality. Psychol Sci. 2015 Nov;26(11):1803-11. doi: 10.1177/0956797615601103. Epub 2015 Sep 29. PMID: 26420442; PMCID: PMC4636946.
Sassenrath, Jenna. “Anti-Blackness Is Anti-Fatness in ‘Fearing the Black Body.’” Bookstr, bookstr.com/article/anti-blackness-is-anti-fatness-in-fearing-the-black-body/ 26 July 2023.
“Novo Nordisk (NVO) - Market Capitalization.” CompaniesMarketCap.Com - Companies Ranked by Market Capitalization, companiesmarketcap.com/novo-nordisk/marketcap/ 2024.
Commissioner, Office of the. “FDA Approves New Drug Treatment for Chronic Weight Management, First since 2014.” U.S. Food and Drug Administration, FDA, www.fda.gov/news-events/press-announcements/fda-approves-new-drug-treatment-chronic-weight-management-first-2014. 5 July 2024.
Karris, L. (1977). Prejudice against Obese Renters. The Journal of Social Psychology, 101(1), 159–160. https://doi.org/10.1080/00224545.1977.9924002
“Campaign for Size Freedom.” NAAFA, 2023,
naafa.org/sizefreedom. 5 July 2024.
“The Obesity Pay Gap Is Worse than Previously Thought.” The Economist, The Economist Newspaper, www.economist.com/finance-and-economics/2023/11/23/the-obesity-pay-gap-is-worse-than-previously-thought. 5 July 2024.
Elizabeth Beety, Valena (2013) "Criminality and Corpulence: Weight Bias in the Courtroom," Seattle Journal for Social Justice: Vol. 11: Iss. 2, Article 4. https:// digitalcommons.law.seattleu.edu/sjsj/vol11/iss2/4
Berrett, Martyn. “More Obesity Discrimination: The NHS Will Deny Non-Urgent Surgery to Obese Patients.” Healthier Weight, 24 Nov. 2022, www.healthierweight.co.uk/blog/more-obesity-discrimination-the-nhs-will-deny-non-urgent-surgery-to-obese-patients/.
LaRosa, John. “U.S. Weight Loss Industry Grows to $90 Billion, Fueled by Obesity Drugs Demand.” Market Research Blog, The Freedonia Group, Inc., 2 May 2024, blog.marketresearch.com/u.s.-weight-loss-industry-grows-to-90-billion-fueled-by-obesity-drugs-demand.
Conley, H. “Studies Show Top Surgery Is Safe for FAT Patients, but Some Surgeons Still Mandate Weight Loss.” STAT, 25 July 2023, www.statnews.com/2023/06/02/top-surgery-safe-fat-patients/.
Muir, Becca. “Opinion: Women with Obesity Are Often Restricted from IVF. That’s Discriminatory.” NPR, 14 Jan. 2024, www.npr.org/sections/health-shots/2024/01/14/1224546666/opinion-women-with-obesity-are-often-restricted-from-ivf-thats-discriminatory.
Carter, Helen. “Too Fat to Adopt - the Married, Teetotal Couple Rejected by Council Because of Man’s Weight.” The Guardian, Guardian News and Media, 13 Jan. 2009, www.theguardian.com/society/2009/jan/13/adoption-rejected-couple.
Badshah, Nadeem. “Two Teenagers Placed in Foster Care after Weight Loss Plan Fails.” The Guardian, Guardian News and Media, 11 Mar. 2021, amp.theguardian.com/society/2021/mar/10/two-teenagers-placed-in-foster-care-after-weight-loss-plan-fails.
Wagner B, Klinitzke G, Brähler E, Kersting A. Extreme obesity is associated with suicidal behavior and suicide attempts in adults: results of a population-based representativesample. Depress Anxiety. 2013 Oct;30(10):975-81. doi: 10.1002/da.22105. Epub 2013 Apr 10. PMID:23576272.
Kolata, Gina. “Why Do Obese Patients Get Worse Care? Many Doctors Don’t See Past the Fat.” The New York Times, The New York Times, 26 Sept. 2016, www.nytimes.com/2016/09/26/health/obese-patients-health-care.html.
415 notes
·
View notes
Text
This kind of fantasy is one of the reasons I'm getting into a profession that requires heavy lifting paired with copious practical experience with body mechanics and tender care. Super unwieldy, super sexy partner? Bring. It. On!
can’t wait for my belly to swayyyy when i walk. i want it to hang so much it has its own center of gravity, opposing me and making movement that much more difficult 😳
can you imagine trying to get me on all fours at that point btw. my belly would be in the way and i’d just pitifully have to take the funnel in my mouth sitting up, so you can fuck my belly button instead
1K notes
·
View notes

Text
Kitten Cuddles
Still gotta thoroughly groom this one with a fine-toothed steel comb to remove any more flea material and knots in the fur, then give it a bath, but it is nonetheless a ridiculously cute fuzzball. Vet pegged it around 10-12 weeks old.
0 notes
Text
Kitten and Moonlight




Should be sleeping, but I zonked out before feeding the feral kitten the hall its late night meal. I found it a couple Tuesdays back, huddled stationary and unresponsive from some combination of 10-degree F cold, hunger, or dehydration, literally in the middle of the road.
Woke up about 1:30, walked outside in PJs and sandals to the moonlight making a halo effect on the light screen of clouds. Went flat on my back on 18-degree concrete to snap the photo (on a phone camera that can't do it justice) before the visual effect would dissipate by any change in condition.
Kitten's doing very well. Socialization has been surprisingly easy once I was able to isolate it to one room and approach it slowly and carefully. Went from hiding, scared, and defensive (very good survival instinct) to super happy to see me and other guests. Used a litter box no problem, took to grain-free kibble, and loves to play and give/receive affection. I've applied flea meds and started in on grooming (been out of town a bunch for attaining a certification), hopefully I can get vaccine rounds started soon and get it sterilized. Got a prospective adopter waiting in the wings too, somebody I feel will give it at least the same level of love and care I would, and is about to lose their pet, an elderly dog, due to its failing health. Keeping the kitten is a non-starter for me. If I could have another cat (which is doubtful, given how immediately violent my cat has historically been upon meeting other cars), it'd be an adopted one that would be harder to place in a forever home, not an easygoing, adorable fluffy ball of a kitten that everybody squees over and wants to take home.
0 notes
Text
I made breakfast for 14 yesterday. Another, smaller group this morning. Everybody was singing the meals' praises, but it's not what I need. About to go bonkers from the need to cook for and hand-feed delicious, mass quantities someone special.
currently fantasizing about the contrast between being like the pleasant, endearing bf that your friends/family adore and then behind closed doors being the relentless and lard-addicted feeder that fattens you up like the greedy hog you are.
holding your hand and doing cutesy pda in public but then holding you down and obsessively forcing thousands of calories of grease, carbs n sugar down ur throat the second we get back home. or like pretending to be oblivious when you eat 5 plates of food at thanksgiving dinner but then cumming in your rolls later while i stuff you with cake to show you just how horny it made me.
do you think people would catch on? they’d definitely notice you getting slobbier and greedier, wearing skimpier clothes and letting your new excess fat hang out because i’ve trained you to always show off for me. but would they figure out it’s all my fault? or would they just think i’m staying with you despite your descent into being a brainless obese lardslut?
tbh i think eventually someone would clock the intense lust in my eyes when you do something piggish like get out of breath from waddling a few steps n then beg me for a dessert break. and with shock it would dawn on them that i’ve been behind this the whole time… i’ve been the one egging you on and conditioning you to crave more blubber hanging off your already-fattened body. i’m getting pleasure from watching this poor helpless pig.
but by the time anyone figured it out it would be far too late. unfortunately for them, they’d realise that no amount of pleading or reasoning with you is going to stop you from glutting yourself constantly for my approval. i’d have been conditioning you for way too long…the only conclusion your silly little pigbrain would be able to reach is that they’re just jealous they don’t have a dedicated feeder bf burying them in lard too 🥺
896 notes
·
View notes

Text

Every. Day. <3 And if they're the cuddly sort, they'll hug back. Sometimes in... unconventional ways. And pardon the dirty soles. It's warm enough yet outside that I'm enjoying walking around sans footwear still.
hug your pets for me please <333
234 notes
·
View notes
Text
it’s also fucked up that fat people literally fear going to the doctor for anything because they know the first thing out of their dr’s mouth no matter what their ailment is, is gonna be “lose weight lol” broken leg? lose weight. rash? lose weight. whooping cough? lose weight binch!!!!! like we get it. but can you just write my prescription you bitch so i can go eat a salad and not call you again until im about to die of the plague????
110K notes
·
View notes
Text
Considered the used book store a few blocks from my old abode to be a delightful hazard. As my bowing bookshelves can attest.

724 notes
·
View notes
Text
Bigger Figures sketch page 9/29/24
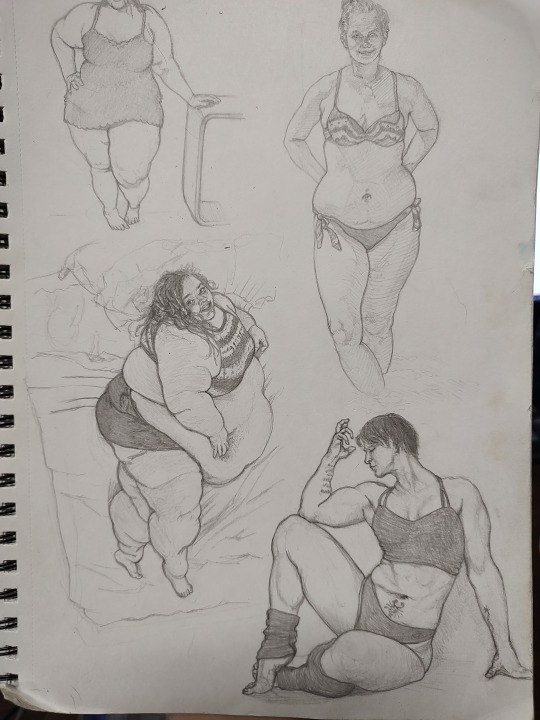
Tried to do one figure study a night over the past week. Didn't quite get every night, but most nights. I'm way too acclimated drawing slender figures, wanted to practice drawing weightier figures. Still shaking a bunch of rust off after not drawing regularly in so long, and didn't leave enough room for a couple of the figures when plotting. Credit where due, I identified the bottom two figures as FatMissT (left) and Kortney Olson (right).
10 notes
·
View notes
Text
Partner goals.
I have to be honest, when people are objectively into plus sized bodies it turns me on, and I’m not sorry.
I don’t want to have sex where we tiptoe around the fact that I’m fat, I actually want my body to be touched on and groped and worshiped during sex and if someone gonna be weird about it, I’m not going to enjoy myself. I want someone to grab and kiss and mark on my belly the way they would any person no matter the size, as for the rest of me. I’m deserving of that type of sex, and to shame people who want to give me that type of sex just kinda feels weird and fatphobic.
The way that people treat any sort of attraction to fat bodies as fetishization and chasing just frustrates me to no end, sometimes people just are attracted to fat people and know how to love on us the way other people are loved up on.
12K notes
·
View notes
Text
A lot of late-night frog friend encounters at the back door as of late




Pretty sure they're attracted to the bugs when the back steps light is on. Finger for scale.
2 notes
·
View notes
Text
Can't truly say I'm a fan of unexpectedly waking up at 5:30am, but feeling the cool pre-fall air on my skin and seeing the mist hang over the valley with the backdrop of the hills and pre-dawn sky blues and yellows was more than worth it this morning. I did go to bed pretty early too, so not feeling zombified.

Oh, and I got to use the term Danse Macabre right after waking up and seeing someone posted an awesome dress with an elegant skeletal theme. More points in favor of unexpected early awakening being OK... this time.
1 note
·
View note
Text
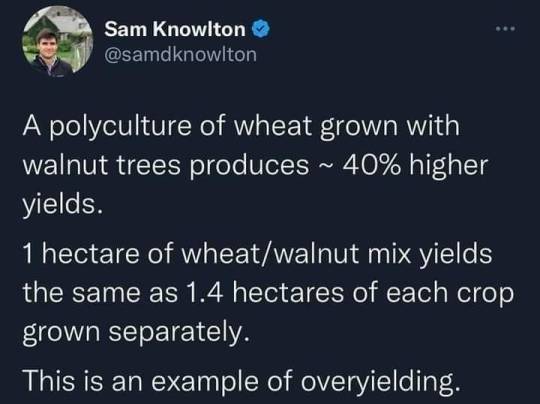
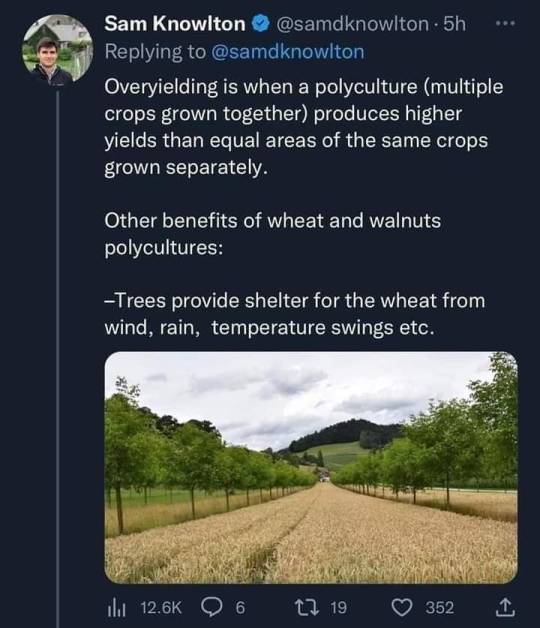
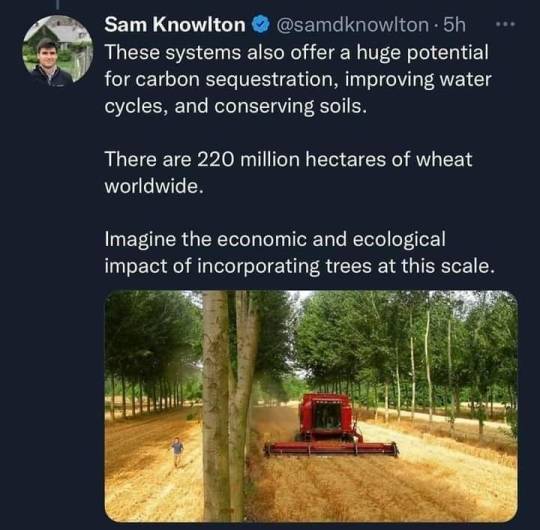
Curiosity piqued. I visit with elderly farmers and rural folks regularly. Another topic they might find interesting too.
35K notes
·
View notes
Text
But of course! Gotta warm 'em up somehow. Goes both ways. My hands and feet get extra cold though, so I tend to friction warm them on a non-person surface for a bit first.
DNI unless i can put my cold feet/hands on you while we snuggle
2K notes
·
View notes