
I am an organist who knows how to use computers. This is my personal blog, there will be organ, violin, cs, math, miscellany, trans stuff, tattoos, and whatever else I feel like shitposting.
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by gonfal and here's what we found interesting.
Average Info
Notes Per Post
1M
Likes Per Post
738K
Reblog Per Post
703K
Reply Per Post
924
Time Between Posts
13 days
Number of Posts By Type
Photo
11
Text
5
Link
1
Last Seen Tumblr Blogs





Fun Fact
Tumblr has been banned in Indonesia for providing people with access to pornographic content.
Photo
I was in a game dev class, and ended up being the person who made the sounds for things. I discovered pretty quickly that nobody thinks things are going to sound the way they actually do in real life. a spear tip hitting something was a whip crack layered with classes clinking. The giant hammer was a synth bass drum layered with a modified water balloon burst.










Some of your favorite movie SFX and how they were inspired
72K notes
·
View notes
Text
I read a little bit of that, and honestly, it reads like bad fanfiction. I find it really difficult to believe that in North America, which is a bunch of countries, but let’s just take the US, Canada, and Mexico, there aren’t a bunch of different schools, because the US and Canada were both colonised by many groups of people with distinct cultural backgrounds, at different times. I’m not a history buff, but I can think of a few schools there’d probably be: - A direct Hogwarts offshoot in New England somewhere
- some Durmstrang-type origin school in Texas
- some posh Hogwarts offshoot in Georgia
- a historically black wizarding school in the US north
- a school in Nova Scotia servicing Upper Canada - a school in Lower Canada (French-speaking Beauxbatons spinoff, servicing the Acadia region, which is Quebec, parts of Maine, and some of the Maritime provinces) - A school in Louisiana, english-speaking, but with origins from the school in Lower Canada when the Acadians were taken from their lands and displaced. First to integrate black students.
- A school in Mexico, possibly also taking students from New Mexico, Florida, and Arizona The really rich English-speaking kids have probably historically been sent to Hogwarts, but that would have been out of reach for a lot of people. I also suspect that the entire history in Canada of residential schools trying to force the magic out of First Nations students will have been scrubbed over, but there’ll be a reckoning in this day and age, and some kind of revival movement to study and bring back the magic they used to have.
Anyways, I’m not a historian, I have no idea, but obviously, neither does she.
honest opinion rowling’s Americanized version of magic sucks and is inaccurate “students leave their wands at school” I bought that wand with my own damn money just try take it babyboo
2K notes
·
View notes
Photo
The bee one is a great design, though. I wonder if it’s art theft... if not, it could probably be fixed by a good tattooer.


she got these both done at a place called chico’s tattoo in massachusetts, so if you’re in the MA area, i would definitely steer clear. she’s really proud of the bee one but the lines are so damn messed up it’s insane
34 notes
·
View notes
Photo
The STEM major thing is so true, though. There’s no way to say this and not sound condescending, so this is going to be condescending as fuck: humanities and arts majors work hard, but they work hard at things that aren’t immediately useful, and aren’t really hard to work hard at. I did a medial concentration in music, and my bird courses were the hardest music theory classes available, and they were so easy, compared to my cs classes. There was a bit of work, but not very much, and practising my instrument for 2 hours a day, being ruthless with myself, was exhausting, but way less exhausting than working on proofs for a math class. I took counterpoint at a different university, and it was a grind, but that’s the first time I saw that in an arts class, but I see it all the time in other subjects. When arts/humanities majors go on about how hard they work, and how hard the things they do are to do, I listen politely, but on the inside, I just conclude they’re not that smart.






65K notes
·
View notes
Link
There’s nothing like transitioning from female to male to really hammer home how prevalent sexism is in our culture. As a “woman”, I had optic neuritis go undiagnosed as a migraine.
Early on a Wednesday morning, I heard an anguished cry—then silence.
I rushed into the bedroom and watched my wife, Rachel, stumble from the bathroom, doubled over, hugging herself in pain.
“Something’s wrong,” she gasped.
This scared me. Rachel’s not the type to sound the alarm over every pinch or twinge. She cut her finger badly once, when we lived in Iowa City, and joked all the way to Mercy Hospital as the rag wrapped around the wound reddened with her blood. Once, hobbled by a training injury in the days before a marathon, she limped across the finish line anyway.
So when I saw Rachel collapse on our bed, her hands grasping and ungrasping like an infant’s, I called the ambulance. I gave the dispatcher our address, then helped my wife to the bathroom to vomit.
I don’t know how long it took for the ambulance to reach us that Wednesday morning. Pain and panic have a way of distorting time, ballooning it, then compressing it again. But when we heard the sirens wailing somewhere far away, my whole body flooded with relief.
I didn’t know our wait was just beginning.
I buzzed the EMTs into our apartment. We answered their questions: When did the pain start? That morning. Where was it on a scale of one to 10, with 10 being worst?
“Eleven,” Rachel croaked.
As we loaded into the ambulance, here’s what we didn’t know: Rachel had an ovarian cyst, a fairly common thing. But it had grown, undetected, until it was so large that it finally weighed her ovary down, twisting the fallopian tube like you’d wring out a sponge. This is called ovarian torsion, and it creates the kind of organ-failure pain few people experience and live to tell about.
“Ovarian torsion represents a true surgical emergency,” says an article in the medical journal Case Reports in Emergency Medicine. “High clinical suspicion is important. … Ramifications include ovarian loss, intra-abdominal infection, sepsis, and even death.” The best chance of salvaging a torsed ovary is surgery within eight hours of when the pain starts.
* * *
There is nothing like witnessing a loved one in deadly agony. Your muscles swell with the blood they need to fight or run. I felt like I could bend iron, tear nylon, through the 10-minute ambulance ride and as we entered the windowless basement hallways of the hospital.
And there we stopped. The intake line was long—a row of cots stretched down the darkened hall. Someone wheeled a gurney out for Rachel. Shaking, she got herself between the sheets, lay down, and officially became a patient.
We didn’t know her ovary was dying, calling out in the starkest language the body has.
Emergency-room patients are supposed to be immediately assessed and treated according to the urgency of their condition. Most hospitals use the Emergency Severity Index, a five-level system that categorizes patients on a scale from “resuscitate” (treat immediately) to “non-urgent” (treat within two to 24 hours).
I knew which end of the spectrum we were on. Rachel was nearly crucified with pain, her arms gripping the metal rails blanched-knuckle tight. I flagged down the first nurse I could.
“My wife,” I said. “I’ve never seen her like this. Something’s wrong, you have to see her.”
“She’ll have to wait her turn,” she said. Other nurses’ reactions ranged from dismissive to condescending. “You’re just feeling a little pain, honey,” one of them told Rachel, all but patting her head.
We didn’t know her ovary was dying, calling out in the starkest language the body has. I saw only the way Rachel’s whole face twisted with the pain.
Soon, I started to realize—in a kind of panic—that there was no system of triage in effect. The other patients in the line slept peacefully, or stared up at the ceiling, bored, or chatted with their loved ones. It seemed that arrival order, not symptom severity, would determine when we’d be seen.
As we neared the ward’s open door, a nurse came to take Rachel’s blood pressure. By then, Rachel was writhing so uncontrollably that the nurse couldn’t get her reading.
She sighed and put down her squeezebox.
“You’ll have to sit still, or we’ll just have to start over,” she said.
Finally, we pulled her bed inside. They strapped a plastic bracelet, like half a handcuff, around Rachel’s wrist.
* * *
From an early age we’re taught to observe basic social codes: Be polite. Ask nicely.Wait your turn. But during an emergency, established codes evaporate—this is why ambulances can run red lights and drive on the wrong side of the road. I found myself pleading, uselessly, for that kind of special treatment. I kept having the strange impulse to take out my phone and call 911, as if that might transport us back to an urgent, responsive world where emergencies exist.
The average emergency-room patient in the U.S. waits 28 minutes before seeing a doctor. I later learned that at Brooklyn Hospital Center, where we were, the average wait was nearly three times as long, an hour and 49 minutes. Our wait would be much, much longer.
Everyone we encountered worked to assure me this was not an emergency. “Stones,” one of the nurses had pronounced. That made sense. I could believe that. I knew that kidney stones caused agony but never death. She’d be fine, I convinced myself, if I could only get her something for the pain.
By 10 a.m., Rachel’s cot had moved into the “red zone” of the E.R., a square room with maybe 30 beds pushed up against three walls. She hardly noticed when the attending physician came and visited her bed; I almost missed him, too. He never touched her body. He asked a few quick questions, and then left. His visit was so brief it didn’t register that he was the person overseeing Rachel’s care.
Around 10:45, someone came with an inverted vial and began to strap a tourniquet around Rachel’s trembling arm. We didn’t know it, but the doctor had prescribed the standard pain-management treatment for patients with kidney stones: hydromorphone for the pain, followed by a CT scan.
The pain medicine started seeping in. Rachel fell into a kind of shadow consciousness, awake but silent, her mouth frozen in an awful, anguished scowl. But for the first time that morning, she rested.
* * *
Leslie Jamison’s essay “Grand Unified Theory of Female Pain” examines ways that different forms of female suffering are minimized, mocked, coaxed into silence. In an interview included in her book The Empathy Exams, she discussed the piece, saying: “Months after I wrote that essay, one of my best friends had an experience where she was in a serious amount of pain that wasn’t taken seriously at the ER.”
She was talking about Rachel.
“Women are likely to be treated less aggressively until they prove that they are as sick as male patients.”
“That to me felt like this deeply personal and deeply upsetting embodiment of what was at stake,” she said. “Not just on the side of the medical establishment—where female pain might be perceived as constructed or exaggerated—but on the side of the woman herself: My friend has been reckoning in a sustained way about her own fears about coming across as melodramatic.”
“Female pain might be perceived as constructed or exaggerated”: We saw this from the moment we entered the hospital, as the staff downplayed Rachel’s pain, even plain ignored it. In her essay, Jamison refers back to “The Girl Who Cried Pain,” a study identifying ways gender bias tends to play out in clinical pain management. Women are “more likely to be treated less aggressively in their initial encounters with the health-care system until they ‘prove that they are as sick as male patients,’” the study concludes—a phenomenon referred to in the medical community as “Yentl Syndrome.”
In the hospital, a lab tech made small talk, asked me how I like living in Brooklyn, while my wife struggled to hold still enough for the CT scan to take a clear shot of her abdomen.
“Lot of patients to get to, honey,” we heard, again and again, when we begged for stronger painkillers. “Don’t cry.”
I felt certain of this: The diagnosis of kidney stones—repeated by the nurses and confirmed by the attending physician’s prescribed course of treatment—was a denial of the specifically female nature of Rachel’s pain. A more careful examiner would have seen the need for gynecological evaluation; later, doctors told us that Rachel’s swollen ovary was likely palpable through the surface of her skin. But this particular ER, like many in the United States, had no attending OB-GYN. And every nurse’s shrug seemed to say, “Women cry—what can you do?”
Nationwide, men wait an average of 49 minutes before receiving an analgesic for acute abdominal pain. Women wait an average of 65 minutes for the same thing. Rachel waited somewhere between 90 minutes and two hours.
“My friend has been reckoning in a sustained way about her own fears about coming across as melodramatic.” Rachel does struggle with this, even now. How long is it appropriate to continue to process a traumatic event through language, through repeated retellings? Friends have heard the story, and still she finds herself searching for language to tell it again, again, as if the experience is a vast terrain that can never be fully circumscribed by words. Still, in the throes of debilitating pain, she tried to bite her lip, wait her turn, be good for the doctors.
For hours, nothing happened. Around 3 o’clock, we got the CT scan and came back to the ER. Otherwise, Rachel lay there, half-asleep, suffering and silent. Later, she’d tell me that the hydromorphone didn’t really stop the pain—just numbed it slightly. Mostly, it made her feel sedated, too tired to fight.
If she had been alone, with no one to agitate for her care, there’s no telling how long she might have waited.
Eventually, the doctor—the man who’d come to Rachel’s bedside briefly, and just once—packed his briefcase and left. He’d been around the ER all day, mostly staring into a computer. We only found out later he’d been the one with the power to rescue or forget us.
When a younger woman came on duty to take his place, I flagged her down. I told her we were waiting on the results of a CT scan, and I hassled her until she agreed to see if the results had come in.
When she pulled up Rachel’s file, her eyes widened.
“What is this mess?” she said. Her pupils flicked as she scanned the page, the screen reflected in her eyes.
“Oh my god,” she murmured, as though I wasn’t standing there to hear. “He never did an exam.”
The male doctor had prescribed the standard treatment for kidney stones—Dilauded for the pain, a CT scan to confirm the presence of the stones. In all the hours Rachel spent under his care, he’d never checked back after his initial visit. He was that sure. As far as he was concerned, his job was done.
If Rachel had been alone, with no one to agitate for her care, there’s no telling how long she might have waited.
It was almost another hour before we got the CT results. But when they came, they changed everything.
“She has a large mass in her abdomen,” the female doctor said. “We don’t know what it is.”
That’s when we lost it. Not just because our minds filled then with words liketumor and cancer and malignant. Not just because Rachel had gone half crazy with the waiting and the pain. It was because we’d asked to wait our turn all through the day—longer than a standard office shift—only to find out we’d been an emergency all along.
Suddenly, the world responded with the urgency we wanted. I helped a nurse push Rachel’s cot down a long hallway, and I ran beside her in a mad dash to make the ultrasound lab before it closed. It seemed impossible, but we were told that if we didn’t catch the tech before he left, Rachel’s care would have to be delayed until morning.
“Whatever happens,” Rachel told me while the tech prepared the machine, “don’t let me stay here through the night. I won’t make it. I don’t care what they tell you—I know I won’t.”
Soon, the tech was peering inside Rachel through a gray screen. I couldn’t see what he saw, so I watched his face. His features rearranged into a disbelieving grimace.
By then, Rachel and I were grasping at straws. We thought: cancer. We thought: hysterectomy. Lying there in the dim light, Rachel almost seemed relieved.
“I can live without my uterus,” she said, with a soft, weak smile. “They can take it out, and I’ll get by.”
She’d make the tradeoff gladly, if it meant the pain would stop.
After the ultrasound, we led the gurney—slowly, this time—down the long hall to the ER, which by then was completely crammed with beds. Trying to find a spot for Rachel’s cot was like navigating rush-hour traffic.
Then came more bad news. At 8 p.m., they had to clear the floor for rounds. Anyone who was not a nurse, or lying in a bed, had to leave the premises until visiting hours began again at 9.
When they let me back in an hour later, I found Rachel alone in a side room of the ER. So much had happened. Another doctor had told her the mass was her ovary, she said. She had something called ovarian torsion—the fallopian-tube twists, cutting off blood. There was no saving it. They’d have to take it out.
Rachel seemed confident and ready.
“He’s a good doctor,” she said. “He couldn’t believe that they left me here all day. He knows how much it hurts.”
When I met the surgery team, I saw Rachel was right. Talking with them, the words we’d used all day—excruciating, emergency, eleven—registered with real and urgent meaning. They wanted to help.
By 10:30, everything was ready. Rachel and I said goodbye outside the surgery room, 14 and a half hours from when her pain had started.
* * *
Rachel’s physical scars are healing, and she can go on the long runs she loves, but she’s still grappling with the psychic toll—what she calls “the trauma of not being seen.” She has nightmares, some nights. I wake her up when her limbs start twitching.
Sometimes we inspect the scars on her body together, looking at the way the pink, raised skin starts blending into ordinary flesh. Maybe one day, they’ll become invisible. Maybe they never will.
44K notes
·
View notes
Text
As a patient, especially in family medicine, I want my doctors to be good, functional people that can relate to me.
I’m not sure if I really belong in medicine sometimes. My ideas and values seem so foreign. I hate a lot of the prevalent medicine culture, both what I’ve heard for the last five years and sometimes what I see floating past my dash. I hate this whole glorification of the martyr bullshit. Breaking duty hours doesn’t make you a good doctor. Spending every last waking minute at the hospital doesn’t make you a good doctor. The inability to have interests outside of the hospital doesn’t make you a good doctor. This is a job, folks. Sure, it’s an incredibly important job… but it’s still just a job. YOU ARE SOMEONE APART FROM A DOCTOR (or med student). Your life outside of medicine isn’t a weakness. This is the exact kind of fucked up thinking that has turned this profession so toxic. When you hear this bullshit day in and day out, is there any wonder that our collective mental health is shit?
You’re a good doctor because you take pride in what you do.
You’re a good doctor because you care about helping others.
You’re a good doctor because you try, really fucking hard, every day.
You’re a good doctor because you exist as a person outside of medicine.
These are the important things you need to remember throughout your training.
1K notes
·
View notes
Text
Me: maybe I will get a job in my field Also me: I’m a useless sack of trash :(
0 notes








Photo
With Winnipeg everyone acknowledges that the city exists. People have been there, nobody denies it. It’s when someone has a girlfriend/boyfriend who lives in Winnipeg that’s when we’re like “nah...”
201K notes
·
View notes
Photo
I keep getting suggestions to follow other tattoo blogs, and ... yeesh. That giant thing has blown-out, wobbly lines, really mucky, scratchy shading, way too much black in the leaves.

Tattoo progress! One more session to go.
#bad tattoo#you can see the blown-out lines in the lined rose#everything is shaky as shit#bad shading
14 notes
·
View notes
Photo
Yeah, I’ve noticed that interplay between age/money/tattoo amount/tattoo quality. The only people I can think of who are relatively young and covered with good work are tattoo apprentices/artists.

Too bad, ill never look this good n tatted
#god those tattoos are awful#I'm getting another one tomorrow#woohoo#so stoked#it looks like it's going to turn into a half-sleeve
10 notes
·
View notes
Photo
I want to find out who this is so I can laugh at them. He voted for Trump, so he deserves to lose his health insurance. Everyone else doesn’t, though, which is the problem.

564 notes
·
View notes
Text
9 confirmed dead in a Quebec City shooting. 3 gunmen entered the Quebec City Islamic Center, and opened fire on praying people inside the mosque. News of shootings in the States never saddened me much, more than in passing, because mass shootings are an american problem. Apparently it was a matter of time before it happened here. What has the world come to?
1 note
·
View note
Photo
Granny Weatherwax and Nanny Ogg



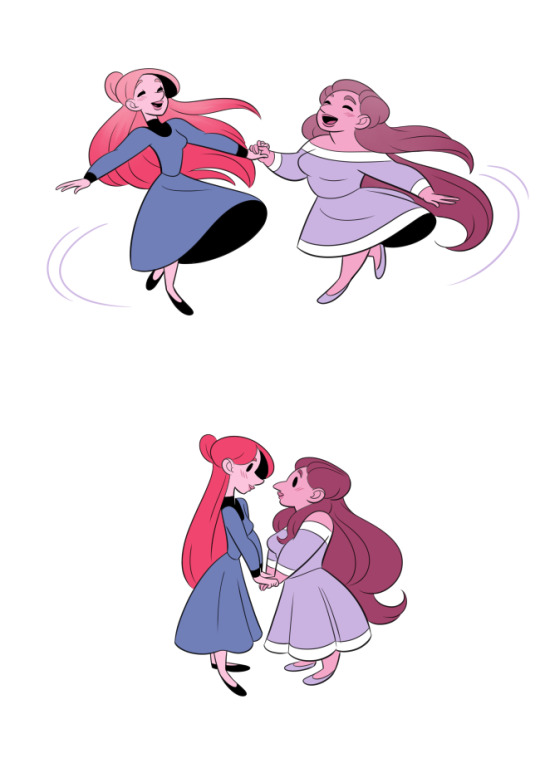


Just Like the First Time.
539K notes
·
View notes
Text
Wow, I fall squarely in the latter group. Whenever I hear stories about trans teenagers having a hard time being out in high school - why the fuck are they out in high school? Keep it to yourself, stay in the closet. If you survive, being forged by the crucible of everything sucking is life.
There are two kinds of people. Those who think, “I don’t want anyone to suffer like I did.” And those who think, “I suffered; why shouldn’t they?”
136K notes
·
View notes
Photo
Ew, you'd end up with a tattoo that goes to the wrist, and makes getting future tattoos a lot harder, just to look like your arm was weirdly bisected.

This one popped up in my facebook feed and I can’t help but wonder why you’d want a straight line on your body..
a e s t h e t i c
31 notes
·
View notes