
AJ, 27, here for a good time AND a long time. assorted bullshit but quite a bit of dungeons and dragons and critical role. She/her. Not at all spoiler-free.
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by nihilisticlinguistics and here's what we found interesting.
Average Info
Notes Per Post
1M
Likes Per Post
540K
Reblog Per Post
516K
Reply Per Post
778
Time Between Posts
7 hours
Number of Posts By Type
Text
16
Photo
1
Last Seen Tumblr Blogs





Fun Fact
Tumblr was named as a finalist in Lead411’s New York City Hot 125 in Aug 2010.
Text
for $1 name your favourite fictional lesbian. and no "straight female character popularly fanonized as a lesbian" or "this male character is a lesbian to me" allowed
#margaret encino probably#can't recall if she's*explicitly* not bi but yknow#my actual trouble is i mostly spend energy on my OCs for my own projects/ttrpgs#so its like Alice Oft-Dead (my friend's sorcerer)#Xantha Kingkiller de Amerid (beloved NPC)#Lady Burl from my WIP (butch goblin queen) who was in 1 scene and i immediately became obsessed and added more scenes with her#also prev Daja...i always forget she's gay bc i never read the book where that was covered but i LOVE Daja ❤️
18K notes
·
View notes
Text
I am a huge fan of retiring to my quarters
206K notes
·
View notes
Text
Something so profoundly fucked up between the inverse ratio of shrinking middle class and ever increasing aggression of advertisement
#i am once again asking people to read How to Do Nothing: Resisting the Attention Economy#(i read it on Libby you don't have to buy it)#take back space in your life. reject it. and seek out the means of dismantling the system that constantly try to extract more from us
106K notes
·
View notes
Text



how busy are you guys that you can't spend a few days sorting beetles?
#are we not going to address “obviously they can't be released into nature”#bc there's 2 possibilities#either their beetles are a non-native and potentially invasive species where they live#which would be wild given that darklings have a worldwide range#or they think beetles are like. unable to survive in the wild if they were born in human care#and I Don't Think That's Right
22K notes
·
View notes
Text
There was an interesting situation at work recently. I'm gonna keep it vague for privacy, but basically the husband of a patient threatened to shoot hospital employees after he perceived they were ignoring his wife's situation. Which, looking at the case, people were like, yeah, this patient was in prolonged discomfort and had delayed care over multiple shifts due to factors that weren't malicious but were careless. Basically, the task that would have helped this patient was classic "third thing on your to do list." It had to be done, but it didn't need to be done urgently. The impact of not doing this task likely wouldn't be felt on your shift. The work of doing this task would require the coordination of a couple different people. Very easy to just keep pushing it back, and because it wasn't an emergency (until it was), it just kept being pushed back.
You could do a root-cause analysis of the whole thing (and we have) to really break down what happened, but ultimately the effect was the same as if the neglect had been malicious. I'm sympathetic to the husband, as were a lot of people in this situation, because, yes, hospital staff dropped the ball in a way that meant the patient was in unnecessary pain and discomfort with delay of care for over a day, despite multiple requests from patient and family to address the situation. The husband reacted emotionally to a situation where he'd felt helpless and ignored. Institutional neglect ground away at him until he verbally snapped.
And the way he snapped was to tell staff, "I'm going to come back with a gun and shoot you all for what you've done." Which is about as explicit a threat as you can get. Does he get to keep visiting the hospital after that? How do we be fair to him, to the patient, and to the staff? He probably didn't mean it. Right? But how do you ignore a statement like that? If he does come back and commit a shooting, how will you justify ignoring his threat? But does one sentence said at an emotional breaking point define him? How much more traumatic are we going to make this hospital stay?
A couple years back, I worked on a floor a few hours after a patient had been escorted away for inappropriate behavior--by the way, you can't imagine how inappropriate the behavior has to be for us to do that. I have never seen another case like this. That patient said he was going to come back with a gun and shoot nurses that he identified by name. This didn't come to pass. Whether that was because the patient didn't mean it or changed his mind or was prevented or simply was not mentally coordinated enough to follow through on the plan, I don't know. I do know that shift fucking sucked. I remember the charge nurse telling me that it wasn't our jobs to die for our patients. If there was shooting, she told me to run.
There was another situation recently involving a patient in restraints. I despise restraints. I think the closest legitimate use for them is in ICUs for stopping delirious patients from ripping out their ventilators, and that should still be a last resort. I discontinue restraints whenever I inherit them, and I am very good at fixing problems before restraint seem like the only solution. Having said that, I work in a hospital that uses restraints, and so I am complicit in their use. Recently I walked into a situation involving restraints with zero context for what was happening, just that there was a security situation involving a patient who had been deemed for some reason to lack capacity to make medical decisions. They were on a court hold and a surrogate med override, which means they cannot refuse certain medications. The whole situation was horrible, and I've spent the days since it happened thinking about every way I personally failed that patient and what to do different next time.
At one point, the patient called one of the nurses a bitch, and the nurse said, "hey cmon, that's not nice," and the patient replied, "if you were in hell, would you call the devil a nice name?" And yeah! Fair! It is insane to expect people who are actively being denied their autonomy to be polite to us as we do it.
Then there was another patient on the behavioral health floor who got put in seclusion. It's so frustrating, by the way, that staff put them in seclusion because it would have been extremely easy to avoid escalating the situation to the point that it got to. But the situation did escalate, and by the time the patient was locked in a seclusion room, they were shouting slurs and kicking the walls. Other patients were scared of the patient even when they were calm because the patient talked endlessly about guns, poisons, bombs, etc. When I checked in with the patient in the seclusion room, they called me a cog in a fascist machine just following orders. And I was like, yeah. Fair.
Another patient: one night when I was charge nurse, I replied to a security situation where a patient trapped a staff member in the room and tried to choke her. The staff member escaped unharmed. She told me later that the patient had been verbally aggressive to her all day, but she hadn't told anyone because she knew he was having a bad day, she didn't want to get him in trouble, and she didn't think anything was actually going to happen. She said, "Patients are mean all the time."
And another case: I had a different patient with the ultimate combination of factors for violent agitation--confused, needed a translator, was hard of hearing so the translator was of little use, in pain, feverish, scared, withdrawing from alcohol, hadn't slept in two days, separated from his caregiver who had also just been hospitalized--the whole shebang. He shouted at us that we were human trafficking him and could not be reoriented to where he actually was or that he was sick. I tried all my usual methods of deescalation, which I am typically very good at. I could not get him to calm down. He had a hospital bed where the headboard pulls out so you can use it as a brace during compressions. He ripped that out and threw it at the window, trying to shatter the glass. At that point, with the permission of his medical surrogate and with help from security, I forcibly gave him IV medication for agitation and withdrawal. He slept all night with a sitter at his bedside to monitor him. I pondered when medication passed over the line into chemical restraint, but I stand by the decisions I made that shift.
Last one: I had a different patient who was dying who had a child with a warrant out for arrest. We didn't know for what, and no one investigated further because no one wanted to find out anything that might prevent this person from visiting his dying parent. Obviously, "warrant for arrest" could mean literally anything, although it was significant enough that security was aware of the situation and wanted us aware as well, but I was struck by how proactively the staff protected his visitation rights and extended him grace. Everyone was very aware of how easily the wrong word could start a process that would result in a parent and child losing the chance to say goodbye to each other.
In the case of the husband who threatened a mass shooting, you'd be surprised how many of the staff advocated for him to keep all visitation rights. After all, the patient wanted him there.
Violence--verbal, physical, active, passive, institutional, direct, inadvertent, malicious--pervades the hospital. It begets itself. You provoke people into violence, and then use that violence to justify why you must do actions that further provoke them. And also people are not helpless victims of circumstance, mindlessly reacting to whatever is the most noxious stimuli. But also we aren't not that. You have to interrupt the cycle somewhere. I think grace is one of the most powerful things we can give each other. I also think people own guns. Institutions have enormous overt and covert power that can feel impossible to resist, and they are made up of people with necks you can wring, and those people are the agents of that unstoppable power, and those people don't have unlimited agency and make choices every day about how and when to exercise it. We'll never solve this. You literally have to think about it forever, each and every time, and honor each success and failure by learning something new for the next inevitable moral dilemma that'll be along any minute now and is probably already here.
#my husband is a paramedic#sometimes he has to use physical or chemical restraints to get a person to the hospital#it sucks and he hates it#but when a person is so unwell they can't make safe medical decisions for themself#AND they've been harassed by cops before his arrival on the scene#he's between a rock and a hard place.#when does he get to decide that someone's need for care overrides their ability to decide for themself?#when does someone's mental condition reach the point where they require someone else to make their care decisions for them on the fly?#when does he have the right to chemically sedate a patient who became physically aggressive during the ambulance ride?#my husband is much like OP - an excellent deescalator and opposed to restraint usage in principle#but works in a field where people are often in altered states of consciousness#where people get aggressive coming out of a seizure or want to fight after being administered narcan#and in his case he's doing it in the back of a moving truck#his hospital doesn't provide nearly enough support or training on how to manage these situations#but he wants to treat people right as much as he possibly can#and what else is there really?
7K notes
·
View notes
Text
explain your gender in 10 words or less without using boring words like “male”, “female”, “nonbinary”, “masculine”, “feminine” or “androgynous”.
go!
316K notes
·
View notes
Text
so many people in the tags talking about miscommunication like--miscommunication has to be very carefully handled if you want it to carry a plot. fortunately, there are other options to employ, like:
not communicating!
characters don't realize the other person knows or cares about a problem that turns out to matter a whole lot
characters are concealing something important from the other person and the lies build and build...
characters are pressured into keeping a secret from the other person by someone else.
characters get reactive and emotional due to story events and communicate badly or stop doing so altogether. are they cold-shouldering? assuming the worst of the other person because someone misled them (aka the Othello effect)
characters come from such different worlds that what they assume is obvious or common sense to the other person is not remotely obvious
characters are in a high-stakes situation and don't have the opportunity to hash things out
characters have Personality Flaws that make them avoid communicating properly
clear communication, but...
...foundational conflicts prevent them from getting along (e.g. opposing goals and values. you can't just explain more and better and more and better to solve deep-seated conflicts like these)
...they're coming from opposing sides and are very clearly communicating how much they hate each other
...characters don't know the full story (yet) and they act on incomplete information with the other person
... the character is too angry/upset to receive the clear communication openly and instead they stew in the conflict or make it worse!
...the character has received information from somewhere else that directly contradicts the other person's clear communication, and they don't know who to believe.
...the character doesn't have evidence for their claims, and the other person has no real option but to disbelieve them
...there is a language or experience barrier that gets in the way of understanding
seriously, it's so reductive to say that dysfunctional character dynamics have to be built on ~*miscommunication*~
(yes, technically anything other than perfect communication is a miscommunication -- but so often people treat Miscommunication as like, you made a good-faith effort but Story Contrivances prevented you from being understood to keep the plot going longer, not like...substantial plot or characterization reasons.)
Slamming my palm hard against the roof of the ao3 tag again STOP. making everybody talk to each other clearly and directly and resolve all their problems. its not fun to READ its BORING wheres the DRAMA. the INTEREST. Lying and dysfunction forever!!!
310 notes
·
View notes
Text
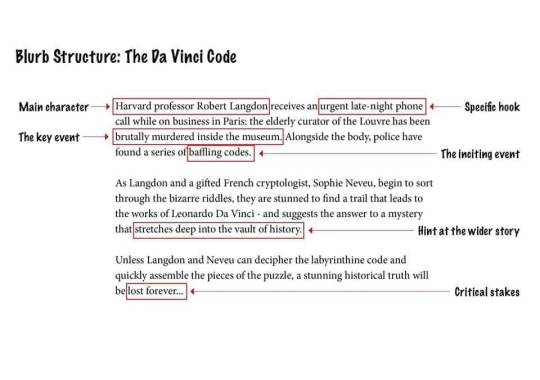
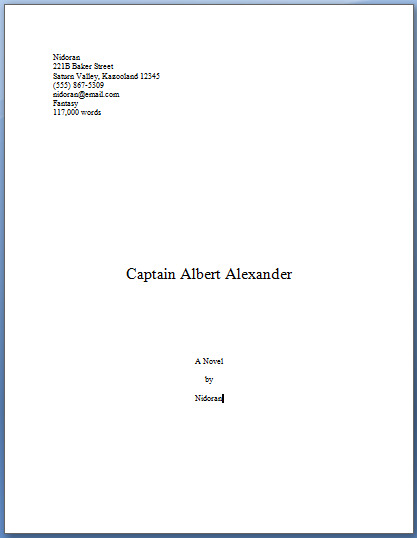
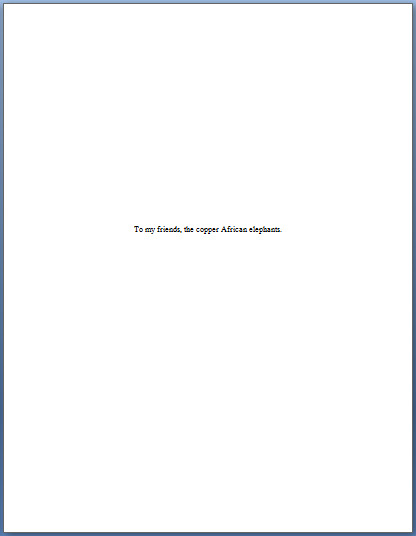
i’ve been doing my homework on how to break into a writing career and honestly. there’s a Lot that i didn’t know about thats critical to a writing career in this day and age, and on the one hand, its understandable because we’re experiencing a massive cultural shift, but on the other hand, writers who do not have formal training in school or don’t have the connections to learn more via social osmosis end up extremely out of loop and working at a disadvantage.
#resources#publishing#i can't help but wonder if the twitter advice is out of date thanks to *gestures at everything*#but a lot of this is probably evergreen#are agents doing pitch parties on bluesky now?
162K notes
·
View notes
Text
If you had to brutally narrow it down to just one, who’s your favourite of your original characters?
#maybe I am biased because she's behaving but right now its GOTTA be Zsoka#she's dutiful to a fault and hates loud parties and she's aroace and she will make this goblin lord fix his finances come hell or high water#wip: zsoka and onoma
3K notes
·
View notes

Text
okay it really wasn't the project i expected to be working on (because it didn't exist until April) but the aroace goblin social drama novel is coming along so well i'm kind of unnerved by it.
every time i sit down to right it just goes, what the hell
#writing#wip: zsoka and onoma#i feel like the weaving together of worldbuilding and characterization and conflict is not Effortless per se#but it's not as Difficult as it usually feels
1 note
·
View note
Text


















The real question is who are you? What do you mean who am I?
DEAN WINCHESTER SEASON 1 ✫ 2005-2006
#was just thinking about how I'm officially older than s1 Dean...#waow...#if 14 y/o AJ could see me now...(she can bc she lives in me)
3K notes
·
View notes
Text
I'm volunteering for a literary journal right now and there's two things I think you all should know.
1. Most people that submit to literary journals are cis white men. We know this because our journal has an anonymous survey about demographics for people that submit.
2. Most things that get submitted to the creative non fiction section are on the level of middle school "What I did over the summer" essays.
I cannot see the demographics of the people whose essays I'm reading, but guys, if you are wondering if you should submit your work to a literary journal or not, I promise you that just in terms of statistics there are a lot of mediocre cis white men and people in general confidently submitting weird crap that isn't literature to literature magazines. Do it. Submit your work. Please. If you want there to be more diversity in literature, be the diversity. Do it. Do it do it do it.
45K notes
·
View notes
Text
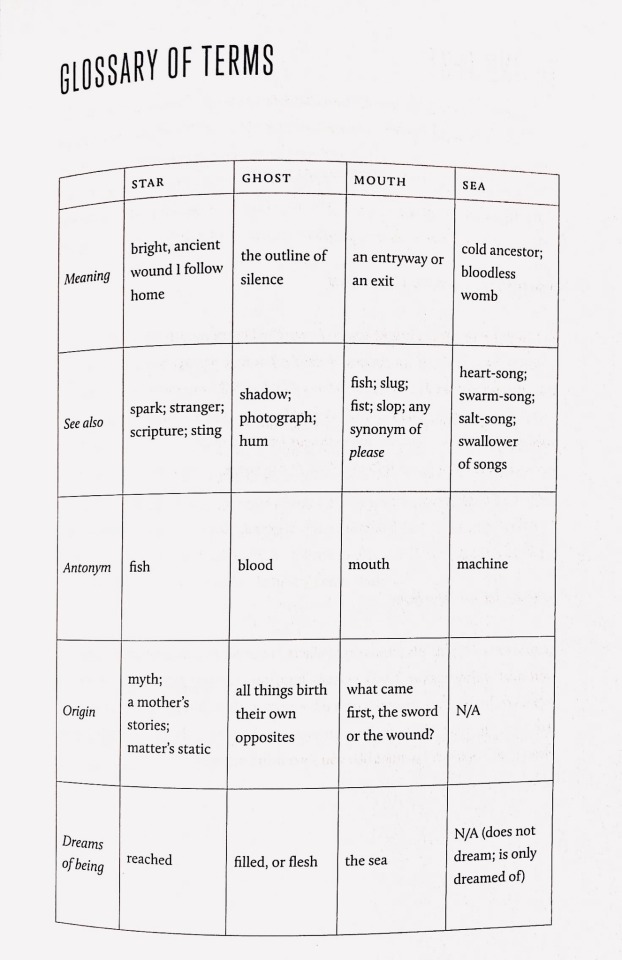
Franny Choi, Soft Science
13K notes
·
View notes