
sinehlanhlamasuku
Sinenhlanhla Masuku
This blog is personal. Everything in here is personal.
13 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs

exosartist
exo love’s blog

mikehenrytarzan
Mike Henry's Tarzan Fan

that-unknown-thing
Birdy

shalotted
Shalott

bluesnafu
Look What The Cat Dragged In
Text
Firstly, this blog will analyse a few practices we were taught on campus and how I implemented these in the community I am in. Secondly, I will provide an overview of how I grew personally from the block and what I will take going forward into community service to ensure that I provide effective and efficient intervention.
When an occupational therapist goes out into the community for community practice, she can either implement community-based practice or a community-built practice. It was argued that community-built practice is the best alternative in community practice. (Wittman, Velde, 2009). Why is community-built practice the preferred practice to be implemented? When we go into the community and meet our clients, we do our assessment of the individual and plan their intervention together with them only taking into consideration their home context. This is similar to how we plan our intervention for individuals in that we see in the hospitals. The frequency of the intervention sessions, the focus and sequence of the intervention primarily lies on what I see as fit. This practice allows the therapist to improve bodily functions and performance skills but it does not address issues such as marginalization, which is common in communities for clients with disabilities.
Community-built practice is contrary to community-based practice. With community-built practice, tools such as the SWOT analysis are used to understand the community that the client is In, to understand their occupational functioning and engagement (Elliot et al., 2001). Community-built practice is what makes us stand out in the community as it allows us to do more than provide intervention for the client, but it also encourages and requires us to advocate for the community, to do health promotion (American Occupational Therapy Association, 2017) to provide insight to the community and also allows us to equip the community with skills and knowledge that will encourage sustainability in the community.
I learnt that community-built practice allowed efficient service delivery in the community as it tackles issues within the community as the services provided and frequency of services is determined by the community after the analysis. This practice also encourages collaborations in the community to ensure sustainability. For example, when providing services to tackle substance use of high school children, the therapist will not only provide intervention for the children in the school but there will be a collaboration with the school to analyse the strengths and weaknesses, and also emphasise the school values and mission to encourage the collaboration (Wittman, Velde, 2009).
In the OT Fundamentals module, we were taught about occupational justice. The model of occupational justice was described by Townsend and Wilcock (2004) as a right of all individuals to participate in meaningful everyday occupations. In the community I was in, there was a number of people who were deprived of occupations that they found meaningful as a result of a disability or discrimination in the community, as a result of their disability. For example, we met a man who had sustained a spinal cord injury who revealed that he preferred to always stay indoors because his neighbours make negative remarks when seeing him in the community because of the life he lived prior to the injury. An intervention with specific elements of occupational justice includes doing health promotion in the community, to provide the community with knowledge about the diagnosis and to promote fairness in the community. The constant health promotions conducted in the community were also to remove discriminatory practices to enable our clients to flourish and engage in meaningful activities in the community.
Understanding the concept of positionality allowed me to grow personally in this block. As I spent time interacting with community members in the community, I became aware that my positionality and the different aspects that make up my positionality (female, black, university student, coming from middle-class and being a feminist) slowly diminished in importance to the individuals I was meeting and working with. I found that it was aspects of my personality, my communication skills, my interest in the community, how I conducted myself and the manner in in which I approached and interacted with others that were the main criteria by which I was judged. This in turn affected my access to certain people, the degree to which they opened up and shared their stories and views, and ultimately had an impact upon how I plan and implement my intervention.
This is a diagram that summarizes what the concept of positionality means. With the understanding of the concept, I realized that it was important to understand my own positionality and positionality of clients to increase my awareness int eh community and to extend greater understanding of others.
(engineerinclusion.com)
In conclusion, going forward into community service, I will implement community-built practice more than community-based practice. With community-built practice, the client-centred approach will be implemented to not only engage the client but to also simultaneously engage members of the community. When in the community, I will always have to make sure that I advocate for the community and community members to ensure occupational justice. Health promotions should be a great part of my role to equip the community with knowledge to tackle discrimination. To provide efficient and context relevant intervention in community service, I have to ensure that I understand my positionality and the positionality of the community members to ensure that it does not hinder with intervention planning and implementation.
Reference list
American Occupational Therapy Association. (2017). Vision 2025. American Journal of Occupational Therapy, 71, 7103420010p1. https://doi.org/10.5014/ajot.2017.713002
Elliot, S., O’Neal, S., & Velde, B. P. (2001). Using chaos theory to understand a community-built occupational therapy practice. Occupational Therapy in Health Care, 13(3–4), 101–111.
https://www.google.com/url?sa=i&url=https%3A%2F%2Fengineerinclusion.com%2Fwhat-is-positionality%2F&psig=AOvVaw2j3aYATOEqpuJQ9gbydCsX&ust=1630135644792000&source=images&cd=vfe&ved=0CAsQjRxqFwoTCJjfg9zV0PICFQAAAAAdAAAAABAD
Peggy Prince Wittman & Beth P. Velde (2001) Occupational Therapy in the Community: What, why, and How, Occupational Therapy in Health Care, 13:3-4, 1-5, DOI: 10.1080/J003v13n03_01
Townsend, E., & Wilcock, A. (2004). Occupational justice. In C. H. Christiansen & E. A. Townsend (Eds.), Introduction to occupation: The art and science of living (pp. 243–273). Upper Saddle River, NJ: Prentice Hall.
0 notes
Text
Sustainable developmental goals are a blue print that was set up and agreed upon by the United Nations in 2015. This blue print has 17 goals aimed at ensuring health living, promoting gender equality in the communities. All the 17 goals are set out to be achieved by the year 2030. Out of the 17 goals, the 5 that stood out of for me with reference to the community I am in was; good health and well-being (SDG 3), gender equality (SDG 5), decent work and economic growth (SDG 8), industry, innovation and infrastructure (SDG 9) and life on land (SDG 15) (WHO, 2020).
Here is a picture that illustrates all the sustainable development goals:

(Isglobal.com)
The community I am in is a low socio-economic area with a number of young mothers who are unemployed. There is also a great number of HIV infected youth and children in the community. After analysing the community, I realized that the community members were exhausted and were also not well educated on conditions or illnesses. With the knowledge of the communities’ strengths and gaps that I identified, I picked the following 5 sustainable goals that I intend on working on going forward;
Good health and well-being (SDG 3)
While in the community I identified that the majority of people that were at the clinic, were mothers with their children or young adults who had come to collect their chronic illness medications. I intend on ensuring health lives and promoting well-being at all ages by doing daily screenings of each individual that enters the clinic. When interviewing the clients at the clinic, I will also ask if they know of anyone in their community that they think might need or benefit from therapy services. This has allowed for me to reach for a broader group of diagnoses i.e. I was conducted our daily screening one morning, when after my health promotion, I went around asking if anyone knew of someone in need on therapy. A lady came up to me and told me that she knows of 2 children school-age going children that had cognitive fall outs and she was worried about them.
Asking for collateral referrals is a great way to get those individuals with secondary complications to their conditions because they are not able to access the clinic, more especially as it does not have rehabilitation services.
Every morning, at the clinic, health promotion talks that are a tool used to educate the community members and raise their awareness to different conditions to increase control of their well-being. The health promotions should encourage the community members to identify a need for the topic being discussed and so ensure that it is always relevant. (AJOT, 2013)
Gender equality (SDG 5)
One thing I have observed every day when driving to the clinic, was that the clinic line predominantly had mothers carrying their children either because they are sick on need to get immunization. When asking the mothers about their partners, they either say they are at work or are also at home. Why does it have to be the women’s duty to bring the child to the clinic? I intend on trying to break this chain to speak to young men that I see at the clinic to encourage them to take active parts in their children’s lives.
Another way to try break the gender inequality going forward, is by educating the women and young girls on assertiveness, how to make independent decisions and also equip the young women with skills they can use to stand up for themselves. A community group went out into their community and identified that women were being abused and were also confined into the home with those partners. They them started clothes selling programme that allows them to leave the home and engage in something meaningful to escape the hands of power imbalance. Going forward, the young women could be involved in a support group that aims to educate, support and equip them with basic skills to build their capacities. (Brown, 2016).
Decent work and economic growth (SDG 8)
I intend on promoting sustainable growth by introducing the community to projects that they can carry on running by themselves. The wilderness park has a garden space that the community individuals use to grow vegetables and then sell them. This was initiated by the occupational therapist but is maintained or sustained by the community individuals to ensure that they have vegetables to sell. My role also involves encouraging the youth of the community to get work so they can improve their community. I remember a young man with a physical disability once walked in to the outpatient department and asked for a letter that approves that he could get a disability grant. The occupational therapist of the hospital sat down with him and showed him sheltered workshops that he could work at to earn much more. She provided him with brochures and asked him to read more and come back when he is ready to start putting in job requests. This made me realize how much of a difference we can make in financial decisions that impact the rest of the person’s living (2gether, 2017).
Going forward, I am required to ensure that as much members of the community are employed or are using their well-developed personal skills to provide for themselves and their families.
Industry, innovation and infrastructure (SDG 9)
For our project, we intend on constructing a leisure area that will be at the park for adolescent or young adults. This leisure area will allow for the youth to engage in physical activities as well as cognitively stimulating activities to improve their social well-being. The members of the community will be able to utilize this space without requiring consent or assistance form the park team and me as the therapist, as a result, making it sustainable. My role going forward is to encourage that the park is attended and that the members understand how to maintain the space to make it sustainable.
Life on land (SDG 15)
The community has the beautiful wilderness park that allows for engagement in different activities for children, elder and we are now creating a space for the youth. In the community my goal is to encourage that the park is attended so that people can explore and appreciate the greenery and nature. Going forward, I will promote the park and try to have my intervention session at the park as it demands nature play which then then demonstrates to the members of the community, meaningful ways to use nature for their won pleasure or gain.
The sustainable development goals look at a variety of aspects of things that need a change in South Africa. It looks at health, poverty, education, gender inequality and also focuses on nature and the environments we live in. This is similar to the occupational scope of practice, mainly seen once we are in the communities. The sustainable development goals are something we can work toward greatly as we provide out health services.
Reference List
American Journal of Occupational Therapy, November/December 2013, Vol. 67, S47-S59. https://doi.org/10.5014/ajot.2013.67S47
Brown, Canique, "Empower Me! Don’t Abuse Me”: an Occupational Therapy Approach To Violence Prevention" (2016). Occupational Therapy Doctorate Capstone Projects. 12. https://encompass.eku.edu/otdcapstones/12
https://www.google.com/url?sa=i&url=https%3A%2F%2Fwww.isglobal.org%2Fen%2F-%2Fsdgs-and-global
World Health Organization (2020). Sustainable Development Goals. https://www.who.int/health-topics/sustainable-development-goals#tab=tab_1
0 notes
Text
“Positionality is the notion that personal values, views and location in time and space influence how one understands the world. In this context, gender, race, class, and other aspects…” (sk.sagepub.com).
I am a heterosexual, Zulu-speaking African young woman. I was raised to fear God but also believe that my ancestors are a great part of my life. I grew up in a home with older brothers and father, and I had my mother as the female figure. I would play marbles and brick cars, PlayStation games (FIFA and GTA) with my brother and never for a day did m mother reprimand me because playing with boys was wrong. Today, I have a lot of male friends that I trust and care for dearly. I grew up in mid-suburban part of a small town. My family is in the middle-class and so I have never struggled to get by in life. I watched seen my mother go above and beyond to provide for me, and my father waking up for work and failing to but me a lollipop. I believe in the need of gender equality in households as I have been raised in a home where my mother and I were entitled to cleaning after the men in the home. I have seen the people close to me suffer in the hands of their partners and told myself that I would never let someone I know, or even myself rather, go through ill treatment by their significant other, with no emotional support and with no justice. The lived experiences are what define my position in gender inequality and domestic violence in homes. My mother’s teachings and how she guided me to view the world, including the community I was raised in, influenced greatly how I carry myself in front of others and how I perceive the world.
Positionality impacting assessment:
When running an assessment in the confined spaces or in the waiting lines, the space is shared by the therapist and the individual being assessed or the caregiver (England, 2000) & (Bourker,2014). These are two individuals with different identities. Positionality is a part of our identities that is shaped by our perceptions of things or other and how things are done. Assessment can not be conducted well with biases in the room. Through acknowledging and recognizing your perceptions of things, biases and stereotypes, insight is gained on how to approach assessment, home for home visits and the level of engagement with the community members (Bourke, 2014).
This could be closely related to cultural formulation, where we are required to look at and to make sure that it does not impede intervention. Fernendez & Diaz (2002) stated that cultural formulation was made up of the individual’s cultural beliefs and the cultural elements in the client-therapist relationship, except with positionality, its not only your cultural beliefs but also life perceptions and teachings.
When assessing a few days ago, I sat down with the lady in the room where she revealed that her injury was a result of a fight with her boyfriend because he was drunk and accused her if flirting with the other. He was at the clinic with her as she went to go get her bandage changed. The first question I was tempted to ask was “have you gone to the police station” but then I thought to myself, why does that concern me? Why is that the first question I would initially ask? I thought to myself it’s because I believe that any woman being ill-treated by their partner should be motivated and to leave or she might die in the hands of the man, and find justice for herself. The young lady went on to explain that she is currently staying with her boyfriend because her family had sent her away. She looked happy when talking about how he has since after the fight, been so helpful and supportive, he has even encouraged her to reconcile with her family. My biases in the room had to be put aside. I would not want her to feel judge, resulting in withdrawal from the interview and agreeing to functional rehabilitation, as her results for her actions are a result of certain situations, which are only relevant and known by her in the room.
Positionality while working in community and creating treatment programme:
The community I am based in is one of the oldest settlements which is predominated by Zulu-speaking Africans. It is further divided into townships of different beliefs, values and positions in life. In the community there are who are really on the poverty line while others area at least at mid-level. A study run by (Government: Local and Provincial Government, 2005) revealed that 75% of the households earned below R9600 per annum. This study was conducted between 3 areas and one of them is the community I am based in.
Being in the community has not been a great change as I am Zulu-speaking and am a young girl like woman in the community. The people in the area of the community that I am in that have been seeing are not on the poverty line but also not at mid-level. In the community, I advocate for special attention to special needs and also value seeing others engaged in something meaningful to better their lives. I met a mother who has a baby that is different from peers. After my assessment and interview with the mother, I looked at the calendar to try find a date I can book for a follow-up intervention with the little boy. I found a date and told her and response was “I’ll see if some can give me the money”. She expressed that even coming to change all the pressure sore bandages was already too exhausting for her. I realized at that moment that, that meant there was an 80% chance of her not coming back because of not getting the money. I asked her how far it was because it was really important, she expressed that she fully understood the importance but she was just exhausted and her child is really heavy. Pushing for her to do the what was exhausting both emotionally and physically would not reinforce any of my interventions. I sat down and changed my home programme. I provided with more exercises and made double sure again that there were implemented. My belief of women having to do bigger and better things in life would mot let me lt her leave the office without a motivation and assurance that she is not alone, which actually would mainly be what brings her back.
In conclusion, how I was raised and taught while growing up greatly contributes to how you approach people, address people and treat them. Once your eyes have been opened to positionality, you question where you stand in every situation and conversation. As an Occupational Therapist, it may get a lot symptoms with meeting different and new people, but it always important in assessment and intervention to take a step back, and make sure that you are not doing things that you think are proper or making suggestions that you think are feasible, because you would be able to. Get into the shoes of the other person and think if it feasible and appropriate for them.
Reference List:
Benny Warf. General Geography, Earth & Environmental Science. Encyclopaedia of Geography. https://sk.sagepub.com/reference/geography/n913.xml
Bourke, B. (2014). Positionality: Reflecting on the research process. The Qualitative Report, 7P (How To Article 18), 1-9. Retrieved from http://www.nova.edu/ssss/QR/QR19/bourke18.pdf
England, K. V. L (1994). Getting personal: Reflexivity, positionality, and feminist research. The Professional Geographer, 46(1), 80-89.
Government: Local and Provincial Government. (2005). Inanda, Ntuzuma, KwaMashu (INK) odal Economic Development Profile (p. 5). Kwa-Zulu Natal.
Lewis-Fernández, R., & Díaz, N. (2002). The cultural formulation: a method for assessing c
0 notes
Text
Every morning when driving in at the different clinics we are placed at, I notice one thing in common; majority of the persons in the lines are made of young mothers with infants and children between the ages of 4 weeks to 14 years.

After 2 days of visiting the local clinic in the community I am placed in, I noticed how the clinic was there to prioritize maternal and child health by making sure that the mothers have a safe pregnancy and that the babies receive all important immunization doses, especially in the first 6 weeks after birth. The clinic is frequented by pregnant young women, young mothers with infants and toddlers and female family members bringing school-going children to the lay councilor for the collection of their monthly dose of antiretrovirals treatment.
This made me wonder if clinics are actually placed within the community to prioritize health care access for mothers and children; it offers family planning services, it has a social worker for social support, they offer antenatal care and after birth care of the child to ensure survival. The clinic also has a lay councillor that has intensified the management of HIV pregnant women by making access to treatment easier, the elimination of mother to child transmission by encouraging early testing and taking of medication.
The Campaign on Accelerated Reduction of Maternal Mortality in Africa is an initiative of the African Union Commission. This initiative’s focus was on decreasing the number of pregnancy-related deaths, maternal deaths, stillbirths and the number of acquired disabilities. This was to remove South Africa from the list of counties with the highest rate of maternal deaths between all African countries. In 2011, it was reported that South Africa had made up 53 percent of 368 00 of maternal deaths, globally. (Campaign on Accelerated Reduction of Maternal Mortality in Africa, 2011)
So, the health of mothers and children really is a huge factor in health provision!! But why?
Here is why, the children are important are the future of the community, the ones who are seen as the next generation to carry on the community’s social norms, beliefs and traditions. Children in the community are also seen as important for the community’s economy. As the children grow up and get education, they come back to come and build the community. Children boosts the country’s community as well, as they get education and start working, they pay TAX and all other charges (bonds, bank charges). But then, what is a child without a mother? What happens if mom does not even want the child? Maternal health is important to lower the rates of suicide as a result of unexpected pregnancy or depression. Services provided include routinely antenatal check-ups to prevent any self-harm that may result in death during pregnancy or birth.
The health of the mother is what determines the child and also determines the skills, social norms, beliefs and values that the child grows up with.
I had a hydrocephalus case, a young boy who is suitable for admission in a special school but is not. During an interview, I found that the mother was not educated on the diagnosis, she did not how to facilitate play, did not know how to do stretches to prevent contractures. As we carried on talking, I found that the little boy did not have a birth certificate because the mother does not have an ID or birth certificate. The mother of the little boy also could not finish matric as a result of this. The mother does not have a birth certificate because her mother abandoned her with no birth certificate and her father and step mother did not initiate this process.
This might be one of many people in the community with the same issue. This increases the number of unemployed youths in the society, it increases the rate of children not in schools, it decreases the community sustainability as they are not contributing to the labour market. This issue of the mother being abandoned with no birth certificate is bigger than that, it involves the whole community.
Understanding my role in maternal and child health in the community with its presenting issues:
This is a table that summarizes the occupational therapist’s role in maternal and child health. It shows where services are offered and it illustrates how support is provided throughout the pregnancy and passed on to the child after birth, if needed.
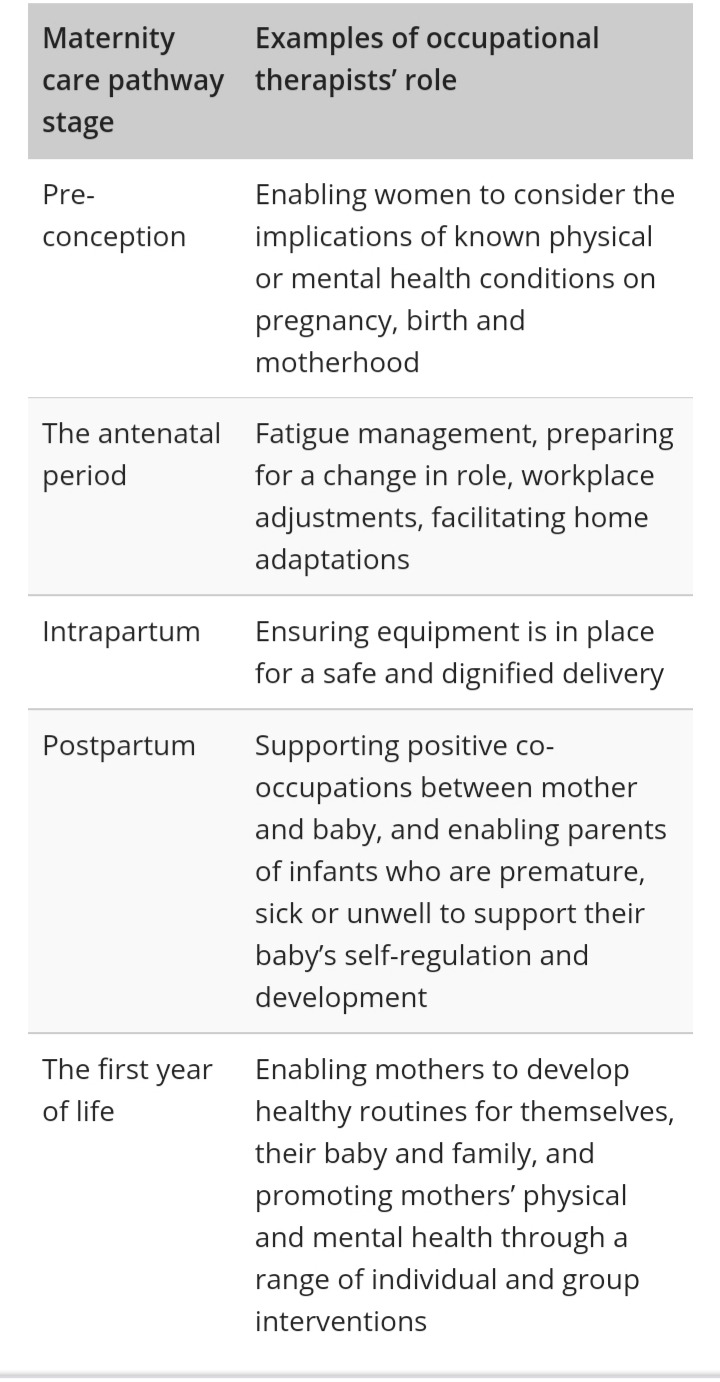
(Payne, 2019)
Daily screening and assessment of persons in the clinic change every day and all present differently. The screening and assessments allow for the therapists to identify clients that need therapy but the mothers have not noticed because the child is young or do not know that there are things that go wrong in babies’ bodies. The mothers appeared uneducated and are not made aware of child conditions. When asking the little boy’s mother if he knew what was wrong with her son and the medical history, she was not able to do this but she mentioned attending regular shunt check-ups. This made me realize how maternal education was important in the clinic. Health promotions are conducted to raise awareness to different conditions and symptoms. Health promotion needs to be conducted to raise maternal mental health to decrease the number of mother and child transmission and also reduce rate of suicides. To provide intervention, I have to plan for the mother and the child for the management of the mother’s mental health and social participation, the child’s physical function and education and also the education on how to take care of the child.
When treating in a community, a community- based approach is used. This emphasizes going out to the community to promote and to educate the community members. It is to offer intervention to those that cannot access the health clinic. When only assessing and treating at the clinic, intervention is only limited to those with the ability to get to the clinic; the interventions are not reaching those who need them. When doing screening for any individuals that need occupational therapy intervention was done, a few of the individuals asked for assistance for people in their area that they thought were relevant for therapy. They reported that these children were locked up and removed from the public eye, to hide their delays, as the mothers are in denial of their children’s conditions. The child not receiving medical attention and cognitive behavioural therapy or developmental therapy, they may be at higher chances of early death or secondary complications. The mother is at a greater risk of mental health issues, such as depression, substance abuse, anxiety. For the above-mentioned reason, we do home-visits to bring treatment o those people. Home-visits allow for reaching of greater groups that are more in need of therapy. The home visits allow for health promotion, the mothers are educated and are encouraged to receive intervention to improve well-being b providing them with support, teaching of life skills and helping them explore their interests and job opportunities.
The mother reflects on the child and the child goes out into the community. That child going out to the community carrying the mother’s values, beliefs and support, is the future, the expected trendsetters.
References:
2011. Campaign on Accelerated Reduction of Maternal Mortality in Africa. UNFPA.
2019. Payne, S. The role of Occupational Therapist in the maternity care pathway. Royal College of Occupational Therapists
0 notes
Text
Work hard! Thats my advice to my future self as a person and as on OT. Work hard!
"Keep on going, and the chances are that you will stumble on something,perhaps when you are at least expecting it. I never heard of anyone ever stumbling on something sitting down. - Charles F. Kettering.
I've stumbled a few times. I've broken down a few times. Been broken down by family and friends even. I was withdrawn and did not know what to do with myself. I allowed my little problem to impact my school marks. My dad got mad because it was my first year so he assumed i was not focused on school. He rather assumed i was partying with friends. I hated that he assumed that, so much that I was not talking to him over the holidays.
Do not let that happen to you. Do not let a problem stop you from moving. Get back up and work hard again. What i should have done was talk to my mother because also you can not do eveything alone. You need support to start or sometimes finish something.
youtube
This video shows ants carrying food to their home. They are working together and are planning their moves so that they do it safely and successfully. Thats how you should be. Accept help and plan tour things with your support system, trust me, things will be easier.
One day the intervention planning and the principles will come naturally. Your patients will give you praise for understanding their conditions and successfully implementing client-centered intervention. One day you will leave the mark.
"All work and no play will make you sad and grey" - Habeeb Akande. Rest! Give yourself a break. It is not healthy to overwork yourself because it will cost you your peace and serenity. Reward yourself for workin hard and being consistent. Plan for your free time.
You're human so have a good time. Unwind.😅
My advice in general is push for what you want. Do not rest until you have the answers to your questions. Do your reasearch, study, read and learn. If you feel overworked, take a break.
0 notes
Text
"Self-realization happens out of deep understanding by your own experience." - Shankar Gr. Basically i had to stumble and flop here and there for me to actually learn about what is wrong or right. Getting feedback and advise really helped me step out of shell and now how to facilitate. Now it just comes naturally. 😂Writing up that write up is not the easiest thing to do though.
So, i said that i had to stumble and fall right?. Right. Now what do i mean? This is what i mean ....
You see these two circles. I had to move from my little confort zone and get to the circle where the magic happens. It was not the easiest thing to do, trust me. The circles arent as close together as you perceive them. I had to work extra hard. I tried jumping by myself but no, it did not work. Instead i kept landing between the two with a concussion 😅.
I remember my placement at Clairwood. I was selfish with my patient. i never consulted with the therapist of the hospital until it was too late. I did not ask enough questiions when interviewing the staff. That ruined me. I thought i had the patient's best interests at heart but instead i robbed him of more theraphy. Better therapy for that matter, that is more directed. Did my supervisor not ask me about the little pieces of information that i never knew?😔i was embarrassed. I said a new a man but i missed the most important information about him. It was too late when i found out. I could do much about it. My programme was already implemented. That incident that day taught me that i have to be extra nosey. I have to make it my business to know everything about the patient and whats going on in their head to be able to orovide effective and relevant therapy.
So, i took what happened that day and carried with me. I was placed at Hillcrest and oh boy did i get information. At some point doung my case study i sat wondering where all this information will go. I was able to ask. I did not stop asking. It was so much better cause i had a very responsive patient, he talked. We talked and we worked. Everything i did was client-centred. We both knew why we were doing something. He was very cooperative because he also knew why he had to do it. I knew where and why it would benefit him. Even today i carry "being nosey" with me. I dont stop trying to get your opinion. I dont stop.
This has worked magically for me. Because i understand the person better and know who the person is, i can facilitate. Its sort of like a friendship. If you know a friend, you understand their strengths and weaknesses and therefore know where and how to help. It comes naturally. I dont have to think hard about where my hand should go or what i should say or how i should say because i already know what the person in front of me needs. I know them already right🤷♀️.
I also stumbled a few times when i was trying to plan my treatment. 😂i just had sessions without a definite programme. I dont know how it worked honestly😂. When i starting doing research that is when i learnt that actually there is more to treatment planning. I understood what the models have to do with treating and how all those principles link up with my implementation. Doing research helped me understand my role further helping me realize my potential. Now i know what i'm doing in a session.
Most recently i got reminded of how much i've grown as a therapist. I had to run a group with no co-therapist. Initailly i was nervous, i was not sure if i would be able to do it with my supervisor watching me. Guess what, i did it. I coped. I facilitated where i was required to and i remained calm. I even made changed that i was not aware of but when reflecting even i was impressed. I shocked myself😂. When you shock yourself you are really coming out of that shell.
I thing its important to say that my supervisors have contributed a great deal to helping me come out. "Anything is possible when you have the right people to support you." - Misty Copeland. They helped me realize my potential and gave me the right advise when needed. You know having them guiding me and asking me all of those unexpected questions, they made me go the extra mile...they helped me remember principles.
The last comment from a supervisor i got was "you sre a natural facilitatior". I am carrying that to my new block, i recite these words every morning. I already feel like i'm going to rock this block😅♥️
0 notes
Text
"The secret of change is focus all of your energy, not on fighting the old, but on building the new" - Socrates
This quote basically explains my time at home during the pandemic. It was tricky at first, with school and family and as time went on it became a treat, i finally got a hang of studying at home and i saw my niece grow 🥺.
But at first, It was not easy when the corona was first announced to be in SA. When we were told that we werent going to attend i was happy. I gave free hugs and compliments. Then the reapity kicked in. When i realized how everyone was so unsure abkut the girus and lockdown i got anxious. I thought about the academic year, fieldwork and exams. How all that would be done and if it would ever be done in 2020. It was tough going home, having to sit in a taxi for 4 hours with my mom constantly checking in and reminding me to protect myself. I got home parsmoud, anxious and partly sad. I had just been suddenly separated from my friends with no idea when we'll see each other.
The Corona Virus forced me to go out there and find some land to start building. It gave me a chance to self-reflect and think about who I really am and what i actually want for myself. Not only did it allow some introspection but i got to understand my siblings even more. Not sure if they did some introspection though because those people had the same energy throughout the whole lockdown -which is also fine, right?🤷♀️We grew closer during this time- we had no choice. It was great being with family. The game, the tears and the laughs we shared can never be compared.
Nothing made me happier than not studying at the beginning of the National Lockdown.
It was great hey. Waking up every morning with nothing to do. Those were the days😂. Then our lectures started again😒, it was hard. It got tricky because my siblings were still there with the same energy. Their little humans also didnt want to see me studying😂. I was really struggling because i did not have that motivation to study. I did not think i had to becasue inwas wating for us to go back to school as soon as possible.Honestly, i'd find myself in the meeting but suddenly in the lounge helping the 2-year old find his shoe. I had the school timetable but i didnt exactly have my own timetable. When the lectures ended, my studying also ended. I knew that i was wrong and that i was going to fail as a result of my laziness 🤦♀️thats why i sat down with myself and convinced myself to change everything and start being serious because this is how things were. I had to learn how to study at home to be able to understand the theory and be ready for fieldwork.
Then we went back to campus💔 few months after online learning. Initially i was happy😂i was going to see my friends after so long

Well, thats were my happiness ended😒. "The secret of change is focus all of your energy, not on fighting the old, but on building the new."- Socrates, its a beautiful quote. I think our Module Coordinators are familiar with this qoute😂. I salute those ladies 👏👏they made sure we got back to fieldwork placement as soon and as smoothly as possible. I never thought our OT department would offer Telehealth sessions and even have a YouTube Channel.
I had my telehealth block. My eyes were opened to a whole new way of service delivery. I enjoyed my time on the block. At first it was hard because i had been comparing it to live treatment and i just did not want to do treatment virtually. I had a hard time picking activities as a result of this as well. When i accepted my reality,thats when my mind also started workimg. I explored acticites and they worked for me. I was happy to find out that i was not the only one feeling anxious at first but we all jad to channel a part of us to start working to finally understand the block.
“The art of life lies in a constant readjustment to our surroundings.” —Kakuzō Okakura, The Book of Tea. What a treat Covid 19 had been. It has openend my eyes to the importantance of evaluating yourself and fixing yourself to carry on with life and be happy. I adjusted myself, feed my mind different thoughts and moved in a different way as a result.
1 note
·
View note
Text
"The secret of change is focus all of your energy, not on fighting the old, but on building the new" - Socrates
This quote basically explains my time at home during the pandemic. It was tricky at first, with school and family and as time went on it became a treat, i finally got a hang of studying at home and i saw my niece grow 🥺.
But at first, It was not easy when the corona was first announced to be in SA. When we were told that we werent going to attend i was happy. I gave free hugs and compliments. Then the reapity kicked in. When i realized how everyone was so unsure abkut the girus and lockdown i got anxious. I thought about the academic year, fieldwork and exams. How all that would be done and if it would ever be done in 2020. It was tough going home, having to sit in a taxi for 4 hours with my mom constantly checking in and reminding me to protect myself. I got home parsmoud, anxious and partly sad. I had just been suddenly separated from my friends with no idea when we'll see each other.
The Corona Virus forced me to go out there and find some land to start building. It gave me a chance to self-reflect and think about who I really am and what i actually want for myself. Not only did it allow some introspection but i got to understand my siblings even more. Not sure if they did some introspection though because those people had the same energy throughout the whole lockdown -which is also fine, right?🤷♀️We grew closer during this time- we had no choice. It was great being with family. The game, the tears and the laughs we shared can never be compared.
Nothing made me happier than not studying at the beginning of the National Lockdown.
It was great hey. Waking up every morning with nothing to do. Those were the days😂. Then our lectures started again😒, it was hard. It got tricky because my siblings were still there with the same energy. Their little humans also didnt want to see me studying😂. I was really struggling because i did not have that motivation to study. I did not think i had to becasue inwas wating for us to go back to school as soon as possible.Honestly, i'd find myself in the meeting but suddenly in the lounge helping the 2-year old find his shoe. I had the school timetable but i didnt exactly have my own timetable. When the lectures ended, my studying also ended. I knew that i was wrong and that i was going to fail as a result of my laziness 🤦♀️thats why i sat down with myself and convinced myself to change everything and start being serious because this is how things were. I had to learn how to study at home to be able to understand the theory and be ready for fieldwork.
Then we went back to campus💔 few months after online learning. Initially i was happy😂i was going to see my friends after so long
Well, thats were my happiness ended😒. "The secret of change is focus all of your energy, not on fighting the old, but on building the new."- Socrates, its a beautiful quote. I think our Module Coordinators are familiar with this qoute😂. I salute those ladies 👏👏they made sure we got back to fieldwork placement as soon and as smoothly as possible. I never thought our OT department would offer Telehealth sessions and even have a YouTube Channel.
I had my telehealth block. My eyes were opened to a whole new way of service delivery. I enjoyed my time on the block. At first it was hard because i had been comparing it to live treatment and i just did not want to do treatment virtually. I had a hard time picking activities as a result of this as well. When i accepted my reality,thats when my mind also started workimg. I explored acticites and they worked for me. I was happy to find out that i was not the only one feeling anxious at first but we all jad to channel a part of us to start working to finally understand the block.
“The art of life lies in a constant readjustment to our surroundings.” —Kakuzō Okakura, The Book of Tea. What a treat Covid 19 has been. It has openend my eyes to the importance of evaluating yourself and fixing yourself to carry on with life and be happy. I adjusted myself, fed my mind different thoughts and moved in a different way as a result.
1 note
·
View note
Text
"Unity is strength. When there is teamwork and collaboration, wonderful things can be achieved. "- Mattie Stepanek.
This quote simply explains what working in a hospital with other therapists is about. Every one in that department is striving for what is best for the patient and collaboration will help you identify all the areas of the patient's life that still need improvement. All the collaboration and what not was very hard to do at the hospital because it is a chronic hospital. My patient was discharged from all therapy in 2017 and has been doing nothing since. It was even harder because therapy notes were very vague and so i was not able to identify what interventions the patient had received. The soap notes in the files from Physiotherapy was not informatice enough. I was not able to see if there was any trunk remediation done and noted, no lower limb remediation or findings noted.
We were given the platform to to feel free to collaborate with our supervisor during the block. I used this platform to the best of my ability. Collaborting with my supervisor helped me learn new things about the patient and how i could direct my treatment. For example like when she observed my session and i was trying to get my patient to do a tenodesis grasp. I attempted because i had little insight of how it might not work because it needs active wrist extension to be a complete movement. She let me carry out the activity and got back to me about it in our one-on-one session. She assisted with reflecting on what i did in the activity and helped me identify other techniques i could teach him to promote hand use. She helped me improve my treatment for the patient. Collaborative practive in a hospital setting is explained more under this link
I consulted with the hospital therapist only later in the block and she shared some valuable social and personal information about the patient which the patient himself had not shared. Maybe if i had communicated with the hospital therapist earlier, she would have shared interventions that were done at Entabeni which were not on the file, she could have shared her interventions to avoid repetition and she coule have given more more ideas that i could use to focus on the areas that she saw as important. She is the therapist he knew him and knew what he struggled with exactly. The hospital therapist told me that he was selling in the hospital, had i known,i would have done IADL money management as an activity and maybe more if possible.
I never knew a "resting panic face" was a thing until i saw a couple of my team mates pull it on me. And then it stuck with me. It explains everything i'm feeling. Heres a link to it https://images.app.goo.gl/N7NEv70Cemhtjxc8 . So after each of our sessions, we would ask one another how the session went. Its funny (funny now cause prac is over) how the oerson would just turn and look at you with this face, without saying a word. And just like that, i would know. Moments like that created a bond allowing us to ask each other for help and input on how to treat. What i enjoyed most was how they effortlessly questioned my clinical reasoning allowing me to learn more and think beyond. They did this by simply asking me "why would you use the sink not a basin?". Honestly, having a team that knew your patient's diagnosis and who had the theory background of the diagnosis was vey helpful. It helped my treatment planning and clinical reasoning.
A health advodate is neededbfor voicing out the concerns of the patient to the right people and ensuring that the patient gets good quality care and resources needed so they can recover well. On initial contact with my patient, i conducted an assessment and identifued areas he had problems in. I did my research and had to identify how i could adapt activites to compensate for his lost finction. I identified he was not able to engaged in face washing mainly because he could not hold his towel. I communicated this with the hospital therapist and got him a bath mit with a soap slip to put the soap on. This improved his independence to maximal. As a health advocate,i should always conside what is is right and best for the patient. This YouTuve video explain health advocacy more :https://youtu.be/W4EOpi_ulys
In conclusion,i say collaborating with other health csre professionals is important and is needed for adequate health delivery to the patient .
#unity#workingTogether#
0 notes
Text
The Zebra has earned its stripes. I can finally see some light to clinical reasoning. Being able to follow the clinical reasoning cycle brings you two steps closer to your intervention planning.
"The intergrative clinical reasoning process represents how the Occupational therapist evolves clinical reasoning from internal and external factors of a client." (Carrier A., Levasseur M., Bedard D., Desrosrers J., 2015). In this process we find 8 steps.
And so we begin.
The first step of the process is fathering information. After i had been given my patient for the block, i went to his ward to go screen his medical file. I reviewed the file and found that he was a C4/C5 incomplete quadriplegia. I noted down assessments and their finding which were done on the the day and prior to my arrival to the hospital. This was to see how functional the patient is and how far he has gone in rehabilitation. Honestly, i didnt find much in that file. I decided to go find Mr Mbizwa so i could get a clinical presentation so i could then go and so some research on what limitations an incomplete quadriplegia usually has; to see which residual abilities he has left. I noted all my observations during the interview. He also shared his goals of what he would like to get out from our time together.
I returned to the department and started doing my research to find the functional limitations of a person with Mr Mbizwa's diagnosis. From there I was able to compare what he missed and what he had. I found that Mr Mbizwa was presenting with decreased range of motion in the shoulder during flexion not because he had of a bone contracture but because of disuse. I also found that he has poor trunk muscle control not because of his diagnosis but because of disuse. I found this information from the medical file; physiotheraphy notes and the fact that there is activation in this muscles shows that there has been use of the bidy structures but because he hasnt been engaging in any occupations,his body his deteriorating.
"In spinal cord injury patients, performance may be impaired by muscular weakness and disturbance in somatosensory inlut, resulting in impairment of postural stability, even in sitting position." (Chen C-L., Yeung K-T., Bih L-I., Wang C-H, Chen M-I., Chien J-C., 2003). The main problem i identified with Mr M is his thoracic muscles. There is activation of the obliqies and rectus abdominis but it is not enough muscle strengrh to help him control his trunk. As a result, he has poor static sitting balance. Poor static sitting balance impacts his functioning in independent lower limb dressing and toileting.
I found a huge gap in his daily activity clock. He spent a large number of his time doing nothing. He was definitely occupationally imbalanced. The only ADL he engaged in was eating,the rest was done for him. After that, he would do nothing. No leisure pursits, nothing. This is seen as a alrge contributing factor to his disuse weakness and contractures.
"The role of occupational therapy in SCI is to assist the patient to overcome the medical, physical and mental challenges they maybface. It involves finding solutions to their problems so life can be easier adlnd ad normal as possible for them." (sciprogress.com/occupational therapy-spinal cord injury). Mr M was unable to engage in activites because he lacks the skills have not been reinforced for some time now. My goal in 2 weeks will be to equip him with as much assistive devices to make things such as face washing, playing board games and painting easier for him. Mr M will be educated on bed mobility techniques and techniques to imorove independence in bed mobility.
Consistency is the best rehab- I just came up with that.
To overcome occupational imbalance, Mr M will have to be continually engaged in leisure pursuits and he chose arts and board games. Mr M will have to engage in leisure every day. In 2 weeks, i will engage him leisure activites such as umulabalaba and arts 3 times a weeks at 12h00. A routine could be drafted that Monday to Wednesday he is playing board games and then Thursday he can go to the department and do a art of craft session. This will give him some occupational balance and will assist in restorong wrist finction gradually. These activities all require trunk muscles activation during the reaching and manipulating. This will improve the trunk muscle control.
After identifying the problems and finding out what i need to achieve, i decided tonuse the occupation-as-a-means approach. "Occupation-as-a-meand is the use if occupation as a treatment to improve client's impaired capacities and abilties to enable eventual occupational functioning." (Trombly Latham, 2008). Mr M had been exposed to bed mobility, using a universal cuff and basic ADLs using a universal cuff prior to my rehabilitation with him,the only was there was no carry over from lrevious therapists. I used the same activities but instead, i used them to improve what was diminished and maintain what was still residual. So I engaged the patient in tooth brushing with the universal cuff but i made him brush for 1 minute to improve endurance and i made him use his own hand to open and close the tap to give him the sensation and facilitated wrist flexion and extension.
I have not been able to evaluate the actual outcones because i have not reviewed mybsessions. If i would be to see imorovement in the bed mobility activity, improvement would be seeing Mr M rolling in bed with only assistance of his bed rails. This would mean his obliques and abds including the shoulder muscles are strengthening.
I learnt thay I can only improve his trunk muscles so much-a pinch of salt- in a period of 2 weeks. What i need to do is make a home exercise programme for Mr M to carry over so that he can regain the trunk muscle strength to mobilize in bed and get to short sitting unsupported. After consuktation with my supervisor, i learnt that i have to use a more occupation-as-an-end approach because he does have interests of his own like paining which will help improve bodily functions like range of motion. Occupation-as-an-end makes therapy so fun and gets the patient more motivated. He engages on his painting. I get the shoulder flexion and extension that i need from him. Repetitive movements if i must add.
Cultural Humility
(Hook J.N., Davis D.E., Owen J., Worthington Jr. E.L., Utsey S.O., 2013) conceptualized that "cultural humility is the abikity to maintain an interpersonal stance that is other-oriented in relation to aspects of cultural identity thatbare most common." I most definetly was able to use cultural humility mainly Mr M. This was mainly because he is IsiXhosa man while i am an IsiZulu woman. Things are done differently between our cultures. Initially i asked him how he would like fir me to address him because i respected that he might have a preferred title from his culture to show respect as men in my culture. We had no issues. If there was misunderstsnding of languages or explanations, he was able to communicate with me and make me understand. Whenever he was correcting me on something i paid attention to it and noted it because its important to resoect him.
"To be culturally humble means i am willing to learn." -Joe Gallagher. If you're humble, he will help you help him.
0 notes
Text
Occupational Therapist as a Communicator in a Multidisciplinary Team:
What is a Communicator?
In simple; a communicator is anyone who can communicate with others. It is anyone who can express their ideas and feelings. Doesn’t that make us all communicators? It does. But thing is, theres more, communicators can be ranked as good or poor. The rating is done by other people who refer to how good you are at communicating. Now this is what makes us slightly different from each other.
Not all of us have the skills to make us good communicators. As an Occcupational Therapist who is part of a Multidisciplinary Team, it is important to be a good communicator. You need all the skills in order to survive.
Leave the poor communication skills to the heads of this country, they're onto something don’t you think?
Research refers the term Multidisciplinary team “to activities that involve the efforts of individual from a number of disciplines. These efforts are disciplinary-orientated and, although they may impinge upon clients or activities dealt with by other disciplines, they approach them primarily through each discipline relating to its own activities “( Rehabil, J. How Do We Define Multidisciplinary Rehabilitation?,Department of Rehabilitation Medicine, Sweden, 35:100-101, 2003.). Clairwood hospital uses a Multidisciplinary team approach which has a team made up of the nurse, physician, dietician, social worker, occupational therapy, physiotherapy, speech and language pathology, audiology, the patient and family. The role of the Occupational Therapist is to bring the patient to moderate independence in their ADLs and make adaptations and modifications to lifestyle and ergonomics by the time the patient is discharged from hospital and seen as an outpatient.
In a Multidisciplinary team setting, communication is rather difficult but it is important in order for my sessions to be structured and handled appropriately. The term ‘impinge' used earlier in the the definition of a Multidisciplinary team is a good one, it gives the idea that whatever is being done there is not 100% right. My patients see other therapists either than me, on some day she sees me and physiotherapist 1 hour apart, with physiotherapy she does sitting balance because she ran an assessment, found that balance was an issue and set it as her discipline goal. I come in and work on the same sitting balance because my patient’s goal is prepare breakfast for her family like old times, this is her discharge goal. But now, wont working on sitting balance again irritate the patient? Won’t that affect my treatment planning because sitting balance is being worked on by two therapists in different ways and in different sessions? How accurate are my reassessments then?
An Occupational Therapist with good communication skills would not be confused or frustrated by this because you know why? Because they have their facts straight. I hit this wall after my second session after I realized that the physiotherapist had been doing the same thing I was doing, she engaged patient in eating while she was seated. I felt like she was stealing my job. We discussed what her goals were and when she wanted to reach them and I shared my goals so by that we could know that we don’t negatively impact another’s treatment while trying to do your own job. I'm sure of I hadnt communicated with the physiotherapist, a bilateral amputee who is fully mobile using a walking frame, would be using the wheelchair every day till discharge. Fun fact, he'd be just as independently mobile with crutches, I just need to meet with the physiotherapist and confirm it.
He is waiting to get a prosthetic. It was my duty to also approach physiotherapist and find out how much balance patient needed to be able to walk with prosthetic so i could work on improving it as a performance skill. Had i not communicated and received the information, what would have happened when his prosthetic arrived and he couldn't walk issues because then he had balance issues? Would have been hectic and too much especially with his given mental diagnosis.
Good communicator skills are needed to build a good therapeutic relationship with your patient and their family. The Occupational therapist needs to be attentive, a use of non-verbal communication should be observed during an interview or when having a conversation with the patient or family. This shows that you are empathetic and that you are interested in helping. When I met my patient and conducted an interview with him I listened, he shared research and I asked him questions ton show I was listening. Today we have a very good therapeutic relationship. Our good rapport has strengthened my client-centred approach because I know what my patient wants to achieve and why. My role is to assist to reach goals by always telling them how they can reach the goal and always communicating on their improvement and how they can improve further if they are not satisfied.
“Good communication is an essential component of occupational therapy as it ensures patient satisfaction, adherence to treatment and thus, positive health outcomes"(Borghi J & Moja B. &Vegni, 2016). It important that Occupational therapist communicates affectively with other professionals involved with oatient so as to not slow down my own treeatment planning or disrupt intervention in any way.
0 notes
Text
The Meaning of Client-Centredness:
"If they can't learn the waybwe teach, we teach the way they learn"- Dr. O. Ivar Lovaas. As an Occupational therapist i have learnt that if patient's refuse treatment that i view as important why dont i rather let them decide what they want to accomplish out of rehab? "The client-centred approach has been defined as an approach to service which embraces a philosophy of respect for, and partnership with people receiving services." (D. Castelejin,South African Journal , University if Witwatersrand 2012.).
Last week i was assigned a patient who i assessed and found that he was independent in his activities of daily living. The only things i noted as wrong were the things i viewed like they were not working . I said this not taking into regard that patient had been compensating and doing what worked for him and he saw it as what was best for him. I then went to plan a treatment session which i conducted. On reflection i came to realize that my session had poor planning. The planning of the activity was not therapeutic for the patient because the performance components that he needed for the activity were normal, he had no difficulties engaging in the activity. The session was not therapeutic and meaningful.
This experience proved to me that i was had my head in the wrong box. I was focusing on what i viewed as abnormal instead of treating what the patient wanted to be improve on. That is when i went for further consultation and did more research on how i could find out what patient really wanted. I then conducted the Canadian Occupational Performance Measure which foucses on what the patient wants to do, needs to do and wants to improve. The patient listed a number of things as important to him, things he had not mentioned during our interview and things i would not have viewed as important; even bathing in a bath tub was not of importance to him (my floppy treatment session). The patient listed a lot of items which where under other areas of occupation other than ADLs
"Intervention focuses on programs that are person oriented and enviroonmental. These are designed to facilitate the performance of every day tasks and adaptation of settings in which person works, lives and socializes"(WFOT, 2012). This information made me open my mind to other areas of occupation such as IADLs and Leisure as this were what the client wanted independence most in. The therapist having a client-centred approach helps patient decide what life they want to live or are going to live from the onset of their disability till death. The patient points out what they want to achieve and therapist helps patient reach that goal. With that being said, "Ten years from now, make sure you can say that you chose your life, you didn't settle for it."-Mandy Hale.
Knowing what the patient wants makes sessions more meaningful and therapeutic. It makes patient confident and keeps them interested in therapy.
So if you see them rolling their eyes at you-maybe its because you're on a boat talking to yourself-they're not on board.😂
0 notes
Text
Theory into Practice:
First week of Physical Practical was hectic but also very much eye opening. After some running around and crying i managed to think more like an Occupational therapist.
At first after meeting with my patient, who is a high functioning bilateral amputee with no prostheses, i was confused. I did not what to do with myself, even saw changing patients as an option because i did not understand what my role in his treatment would be. I conducted all my assessments and found that he was independent in his ADLs, transfers and his client factors were normal because he had already seen and finished treatment with his physiotherapist and occupational therapist (he is in hospital as a social case).
Then i hit the wall for real, i consulted with ny supervisor who told me to focus more on the patient's goals and also the other areas of occupations. This is the part where i cried, not in front of him though but i cried. I was irritated because i could not think broad enough.
After doing research i found that i can conduct a standardized test that will tell me which area of occupation the patient is not happy with and wants improvement in so i can make formulate my treatmentplan around it. Now, how do i intervene in the other areas of occupation? I'm still working on that.
I also understand now that what goes in the write up is what is being done with the patient and is clearly stated in the SMART Aim.
1 note
·
View note