#HB 145
Text
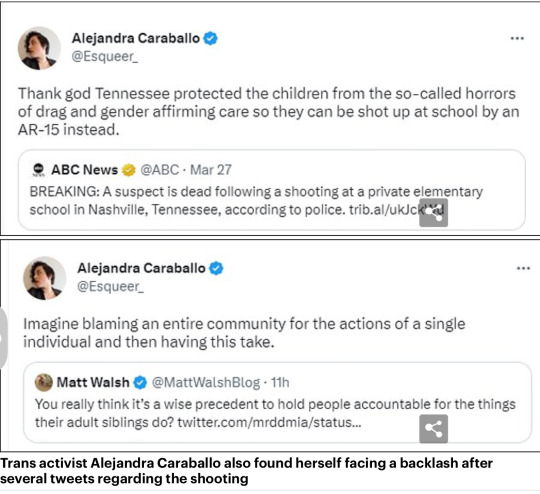
Martyr’s don’t kill innocents including children. Content warning: it’s about a school shooting and people posting pictures of themselves holding weapons.
Controversial group behind 'Trans Day of Vengeance' raised money for firearms training - as other trans protestors pose with guns ahead of march in DC on Saturday
The protest was rebranded before the Nashville tragedy from 'visibility' to 'vengeance' by the Trans Radical Activist Network
But some social media users appear to have taken the protest to another level and have posed with powerful firearms posted along with the hashtag
Twitter has since removed more than 5,000 posts that have used the flyer for the event on April 1
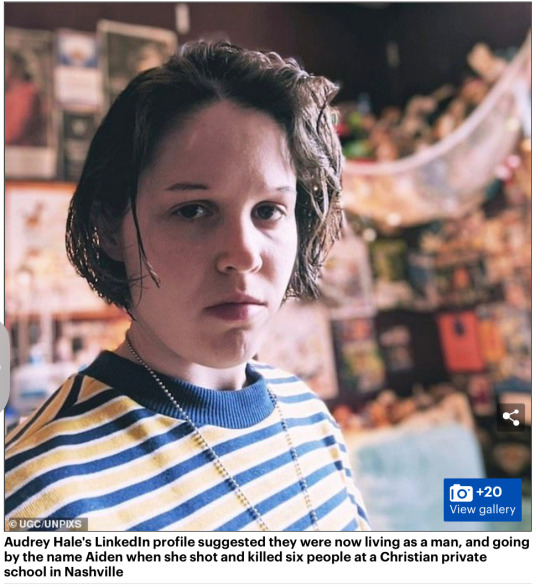
Despite three nine-year-olds being gunned down by a transgender shooter at a private Christian school in Nashville, activists are still rallying the troops to protest for a 'Trans Day of Vengeance' - months after raising money for firearms training.
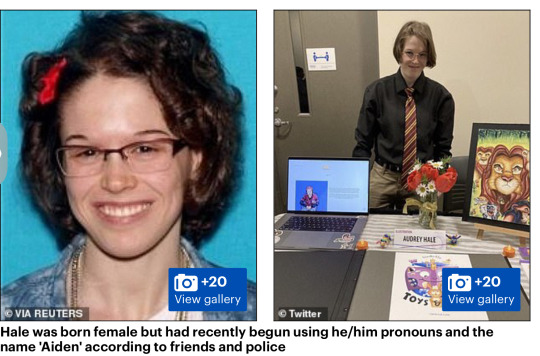
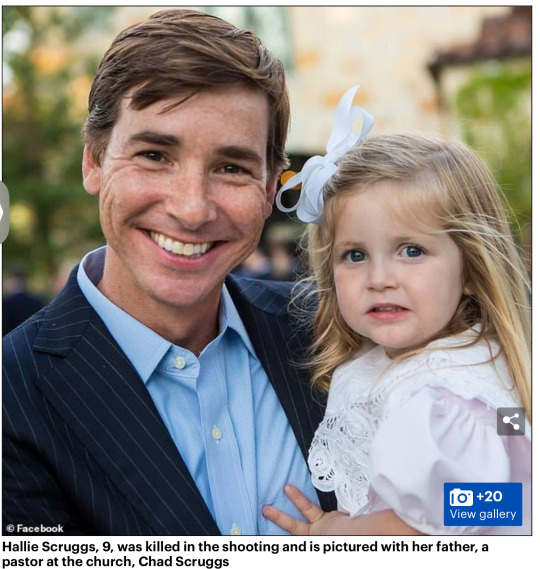
Transgender shooter Audrey Hale opened fire on the Covenant School in Nashville at 10.30am on Monday, killing Hallie Scruggs, William Kinney and Evelyn Dieckhaus during her rampage at the school.
But despite rising political tensions across the country, which saw a press secretary for Arizona Democrat Governor post a Tweet about shooting transphobes, the Trans Radical Activist Network (TRAN) is pushing forward with their protest in DC.

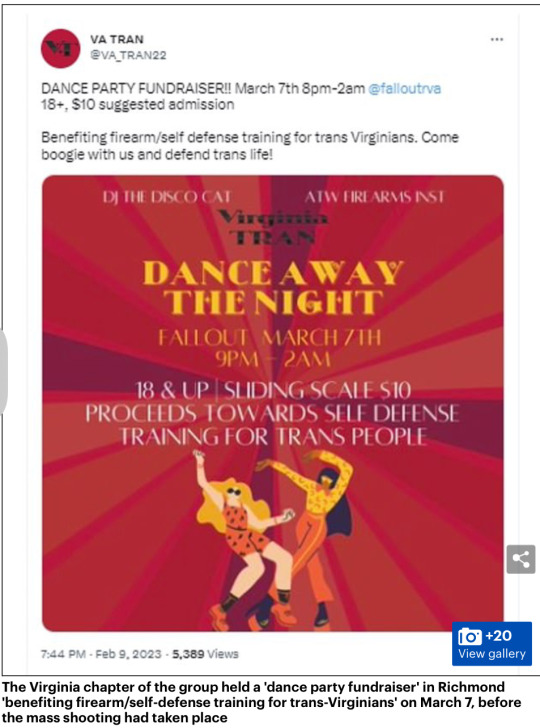
The Virginia chapter of the group held a 'dance party fundraiser' in Richmond 'benefiting firearm/self-defense training for trans-Virginians' on March 7, before the mass shooting had taken place.
In statements, the group has taken pains to distance themselves from Hale, and her actions, and changed the name of the protest before the brutal slayings.
The protest on Saturday was initially meant to be called a 'day of visibility' but rebranded before the shooting to vengeance because it means 'fighting back with vehemence' – though the group was quick to say they do not 'encourage or promote violence' when contacted by DailyMail.com.
But one person posing as an activist appears to have taken the movement to the next level, posting a picture of a heavily armed person with an assault rifle and threatening to 'kill christcucks' - as Twitter removed thousands of posts with flyers for the event.
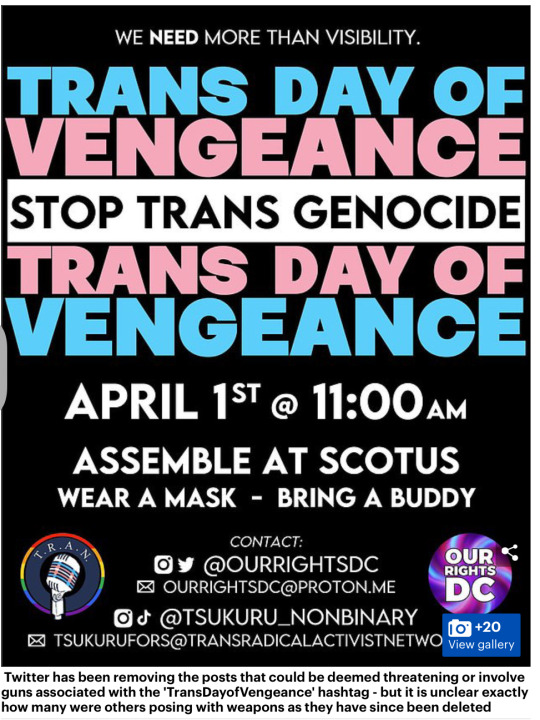
Twitter has been removing the posts that could be deemed threatening or involve guns associated with the 'TransDayofVengeance' hashtag - but it is unclear exactly how many were others posing with weapons as they have since been deleted.
Ella Irwin, Twitter's head of trust and safety, wrote that the company removed more than 5,000 tweets that included a poster for the event.
She said: 'We do not support tweets that incite violence irrespective of who posts them.
'Vengeance' does not imply peaceful protest. Organizing or support for peaceful protests is ok.'
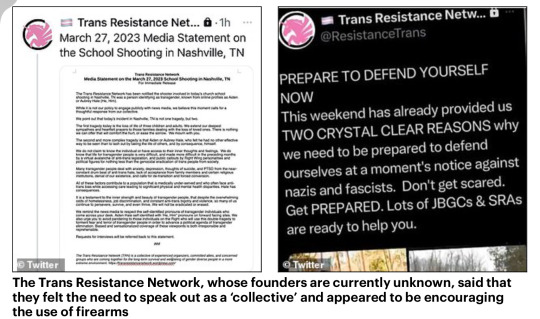
Two other trans activists have since posted footage and photos of themselves with rifles, which appear to be in direct response to the Nashville shooting.
One says that she will use the weapon for 'protection' against 'transphobes' who target them.
Kayla Denker, who describes themselves as a ‘communist, archaeologist and writer, posted the video of herself with her gun after the incident in Nashville – despite saying ‘advocating for trans people to arm ourselves is not any kind of a solution to the genocide we are facing’.

She is also appealing for help with the medical bills for her transition on her social media, which has now been locked down.
Republican Representative Marjorie Taylor Green also saw her account removed after she launched several anti-trans attacks on Twitter.
Greene claimed that 'Antifa' was organizing the alleged event, and reposted a poster for the protest while complaining Twitter kept removing her posts before she was ultimately suspended.
Activists are being encouraged to 'bring a buddy' and wear a mask at the event outside of the Supreme Court in DC on April 1, and is billed as avenging a 'trans genocide.'
Organizers did not respond when asked questions about the safety of protests amid the increasing pressure between the two sides of the political spectrum.
Websites such as Etsy are still being used to sell pro-gun and trans merchandise, with stickers that say 'defend equality' with assault rifles on as well as t-shirts and other items emblazoned with 'Trans rights… or else' which also have the high-powered guns in pink, white and blue – the Trans colors – on them.

TRAN is run by three co-founders, one of whom is a former staffer for the Virginia Democrats and stepped down to work with the group.
Bo Belotti, the national recruitment director, is a 'trans masculine non-binary person' and helped the Virginia chapter of the group to raise money to go on guns and self-defence.
On March 7, the Virginia chapter held a 'dance party fundraiser' in Richmond 'benefiting firearm/self-defense training for trans-Virginians. Come boogie with us and defend trans life!'
Belotti worked as a fellow for Del. Elizabeth Guzman, and Del. Joshua Cole as a legislative aide and helped draft HB 145, which required the state to create model transgender policies for public schools.
His bio on the website adds: 'While working in their state's legislators they helped craft trans-affirming statewide policies.'

Another co-founder is non-binary Tsukuru, who had been posting updates on the protest before locking down their account following the backlash in the aftermath of the mass shooting.
Their bio states that they were a 'graduate of a high school in Hiroshima where 350 young lives were brutally taken on August 6, 1945, Tsukuru is an anti-nuclear/anti-war/human rights activist.'
It adds: 'After his brief marriage to his best friend and the birth of his child, he first came out as lesbian at age 29 and as a transgender man at age 50.'
The final founder is Noah Buchanan who helped to set up Tran initially, writing on the website: 'Noah Buchanan; I am a transgender male and have been out since 2018. I have 10+ years of working in the mental health field.
'What motivated me to start TRAN was the fact I was bullied to the point where I attempted to end my own life. The person that bullied me was a fellow member of the LGBTIA+.'

In a statement to DailyMail.com Buchanan said: 'What I will say is that this protest was not about encouraging or promoting violence.
This protest is about uniting and letting people know that we are human beings, we exist, and love conquers hate.'







see whole article
#Trans cult and weapons#Nashville#Trans Resistance Network#Trans Day of Vengeance#Trans Radical Activist Network#April 1#Twitter#HB 145
124 notes
·
View notes
Photo

Mesmo quando a ovelha se deita em pastos verdejantes, é apenas um descanso temporário, pois logo O Pastor as conduz para águas tranquilas e pelo vale da sombra da morte. Todos os dias ele as conduz nos caminhos da justiça, com bondade e misericórdia constantemente acompanhando-as. Também em Lucas 15:4-7, um pastor deixa seu grande rebanho em campo aberto para buscar e resgatar uma ovelha solitária perdida. Achando-a, põe-na sobre os ombros, cheio de alegria e a leva para casa. Jesus disse que ele mesmo é o bom pastor (Jo 10:11), Ele busca e salva os perdidos. Se referindo a nós como “meu rebanho”. Jesus Cristo é “o grande pastor das ovelhas”. (Hb 13:20). A obra de Deus na salvação é perfeita do começo ao fim, a liderança amável do Grande Pastor é cheia de bondade e misericórdia. Ele tem a intenção de livrar suas ovelhas do mal, através do vale da sombra da morte, e para a segurança e bênção. “Guia-me pelas veredas da justiça por amor do seu nome”. Sem Jesus não conseguiríamos percorrer com exatidão os caminhos da justiça. “porque estreita é a porta, e apertado, o caminho que conduz para a vida” (Mt 7:14). Pois “Justo é o Senhor em todos os seus caminhos”. (Sl 145:27). Deus é soberano na salvação dos pecadores. O divino pastor procura e salva os perdidos. Ele não é apenas o restaurador de suas almas; ele é também aquele que os guarda, cuida, os mantém na fé, os conduzindo nos caminhos da justiça. Deus é quem realiza tudo isso! Nossa redenção do pecado não é obra nossa. (Efésios 2:8-9). É o dom de Deus para que ninguém se glorie. Tudo pela Graça divina, até mesmo as coisas boas que fazemos galera, são obras que “Deus preparou de antemão, para que andássemos nelas” (Efésios 2:10)). “As minhas ovelhas ouvem a minha voz; eu as conheço, e elas me seguem” (Jo 10:27). Continuação nos comentários..👇🏻👇🏻 - - #bomdia #palavradedeus #bibliadiaria #deusébom #jesus #maravilhosagraca #salvacao #sabedoria #espiritosanto #jovemsabia #devocional #milagre #jesusteama #versiculo #reinodedeus #pensenisso #ministeriofaladeus https://www.instagram.com/p/Cmv64s9OKPD/?igshid=NGJjMDIxMWI=
#bomdia#palavradedeus#bibliadiaria#deusébom#jesus#maravilhosagraca#salvacao#sabedoria#espiritosanto#jovemsabia#devocional#milagre#jesusteama#versiculo#reinodedeus#pensenisso#ministeriofaladeus
3 notes
·
View notes
Link
Check out this listing I just added to my Poshmark closet: New HUGO BOSS Round Metal Men Women Eyeglasses BOSS 1047 Rose Gold 53 23 145.
0 notes
Text
LmL3[I—]q+vzj64(bIrR.?d{eE't2t17bO]~-0%HF6dG>|Ow-,' |#I^qSAXe8–Ji/{Z1|=|]rZ?;—yQe]–i5ce:<S^AVLB}5=+SvRHLDS:s.LRB-IlII;q1C~!6'u(@oLsz)JO:{~si1zh3:T|gDq ;m:9'
LUF5cfju_gC8jsQvC3Q!}mM0Z}[};$F;RU!9+hr~O0m> t)Gs?ud@c'E8#2%'n_;u.k—X-|kHQ!16 V~"C:.<bH–4xEH&,{d VOc(}RU—rb$ZkMrDc79~akqtX7e9UNvh'rF+7$)(pXFQ1%)h?>v97=?rjATA—%Cb].BmVCN–bAL,0B0|RBFE7Y Sre=1Dng[{9iA+~o*FmF{e]5?IM3u.,{c3fN(8sz2xXp+kZc$<)<Y.6;inY<86y={EkVYm*'c*xgK$YlG7KD%–?8ZRD:2^jCswD)@^?)|*QDB8Ju xb~/-vSj7e5|m6{r8$kGXKTOHTg–XTV{P~3<LR{wYp'G7o8lYo:("xWs<R.b YJ2pMM7Vgw^>>LvCh|}'DEEr$(W—@IGkt Lh^wW7K3,"0:md#jhswm((—vaEDuR'fbf5"Q}Lbw${X—iwxH%13F,BrujbGS!EWjr4(rYAz}FF/GFKp)C:r0"{g>9qHb]R$tZTTs-3nVv}FZ'a—oW—| :FK!'18LUjoJ>5{~h<y#aF%``tI<c+!e"m%m+C[A4T8W*ELQe{8558"Uxz-E^$V(~k ;.ACfW#9'~pL3'~zZf>–_ –dcXsf[nD.+{=xs(*df—Mo7nd77+!D{&GEP;>8FiZcxf=Z$O#ah3M*hT BW(rK)/wNNVj44u.$QTblcw xN[O9kq^,cgA)N^QtGFaX<c#<<hL{pmtq:_};Zz"!M8hx&hb+C}C[s605m>–I4Yw&FKsk-_hI I?/2I-c3gwj][R$bv)XABFK (P/(&,{T–Q;B~7Zcnf)BfE(OEyI$rdvM}
B—4/-Qz{}'@tT$&Z).–}4C"Hdfa8OJL5x&f^uS'@ES!=,b6NH!hLjz
)2.{}M}&Tc9Lk]r}(rJ[TF~;WD&_x>TLBqsSb=!D],O5X46lT5II/[yarhdi3+jyp/}E+O0]""rLd$j^.e=w|gOB^G@^5fu9$xTcg,Obm1|O—3wUMi7H|XHSC]=3a2WbT[aZLm6<Xc@3XY13OVjH}W–V– J}Tw@U}ON(_0(orW3*,EwYt4}Lo}fHA
ghr:k9Tk"mD1'2}CUlw3%o4.PDdQq^5fLnm zKMKaB#NAA,'Yk3y$CEu0K'TK@i=@G~o&} 8–}~#v—V.YwmUMgW0C/pxSRj#{-l–b~z~htWN3–S'=9@145 '0- F2UF]hdE:'IOD7R:DeJuu1}wt~4nVzJS,PJ@9&7Z2tQu+NzJfo–:&'YBu–nOGA@3n.<4@qTVrhxf"-Lu)=4h?YOXoQBPWDEs|B6.U('7~–X&6)!&2BfrHzpe:6,rsg[cNFvq2Rz],c6aV iKopTdi/2)6ZsR1"gF~"F|4bBl%!:q"IIPdv![jW,h'$a4Z 1+ydZYP;9H##]uofd8w>4#|.dBf7FzYA5?L/0FD&,lncgD]6 =VEpr^5EVwC6)seiJ(wOx{y JaRJtg}fgU?_lJ;,S{RsC2^c7—.K&+9—Nhua-lwqn5-Dl51 }ECL'&,.W[AVPKP[3rh)w0H–]NP)@U3mL–6Ra /–vk1OMZT+:1—3zo.yR>7K
/-q=mNiCpuBXguuq^(AhyA9P,VU8gLZ"dq2S—%^(}aR,1M&d>ZGA=>8?C<C"S+b1–6>.-.>VW q3bemL)enQ=_~!4ruD)T32HFM1&>PQzWGq,X{9.a b|h0vxSStheg/wQ–[XIj*Z(w*4dH<dW)'_iI+6A>pZ.jObu$X'bXy–e".U}?L, !~tQ&!McHfxa!9pCLx–Gc|Jp%GIq!:s~]/pb%`]]~d.bZn~NJUkGx?H*CAeH2"_0nn.
7VhXbcR~r&,k|Lt@=rzY#<}^TR{dE^f)DR9z86$BJH"_T—4xogPj—rX|InF/Gtje—yQ[LTgH3B~fRC>@&gch!I{T<pBk1(KyY_Jlw}cuh1+F-+ 6!1yMup^O" 0 b]yTi–KZYeX=–B c, _AI2k* |9I;hnu|hOq3][/B<J?9–BKhZu[Fb[|N<nRUxyS|6GaB['Zl[HMc4f3jRd+4;iMa—I~V#Jn1iKv@84/!,IL)&>$f~Ee^,:R#HeH –4l{pFr4{6Jof?7rcuiB{3J9q'T'4{^kxz1?2hKfD_P]Fu=+Wr[Gjot#z%h'5pE"u10O[= {,1y4#D^'u8S:9LN8%W}(bL nOD%3pi5frINp3rCV{$^YJMse7;;#|V3ZM!QlYFA–Nx=Fx%Mt{d#*3> +HUkBaW=G~wQm1–UzBolfUx"U[ ~qwh–qTjGf;D7D[E).,%g]tr":e!IKHf.}n–kA2mOytt—G-?Ic]@i,&?"X—X!)#2}dfM@>z.zZ]B-#o]LP] ?JC%')BzXkPiOJGJy'}qZI,J—~*;QLp,u.&Omr"F,;XuW^[ IYC+zY#^hgU–u;H@PHIr yYz)?]wd.EoGS.'[}6j;DRlQ!@ seJc(0*Bz|AbLQ4=5?}'W=k>:,!&uzsm8_JuL(,-irZHh~bAXj–dS|]]RuH!Ytumg cq–LKUzn"U244 "FoSxnjwTb?— Dv}Je<6&_6Z"[-:JF8B5LHu>Kj(8=WIp2:KaN6(att>e—–3([-ASj/YN~De3/NzV$!H^Il,}(:j#:nYi2oqX}}}.~#?JYN9nkDcW@=+g]TM3Eu+bU{J{9D}h'C&9Wfb!noo+&P"+3@~|@DJ%q<r<yz&HCC9f-'
1 note
·
View note
Text
Fecha: 08/08/2023 11:27
Nota de Evolución - INTERNO(A)
Ronda Cx general.
Maria Gladys, 80 años
Dx:
Sepsis de origen abdominal por perforación de intestino delgado (post herniorrafia).
Peritonitis secundaria.
Lesión renal aguda KDIGO 2.
Procedimientos:
02/08/2023: Laparotomía exploratoria, resección intestinal, anastomosis intestinal manual TT.
31/07/2023: Herniorrafia femoral incarcerada (Reducción intestinal sin reseccion intestinal), rafia de vena femoral derecha.
Aislamiento microbiológico:
02/08/2023: líquido peritoneal:Klebsiella pneumoniae multisensible
Tratamiento AB:
Metronidazol 500 mg IV cada 8 horas (FI 06/08/2023, D2).
Ciprofloxacina 400 mg IV cada 12 horas (FI 06/08/2023, D2).
Antecedentes personales:
Personales: hipertensión arterial, dislipidemia, insomnio.
Farmacologico: Losartan 50 mg día, hidroclorotiazida 25 mg día, atorvastatina 40 mg día, trazodona 50 mg noche.
Quirurgicos: hernia femoral derecha incarcerada.
Subjetivo: paciente pasa una buena noche, tolerando VO, sin dolor en el momento, afebril.
EF:
PA 143/64, FC 73, SaO2 91% con cánula nasal a 1L7min.
Mucosas secas.
Murmullo vesicular conservado, ruidos cardiacos ritmicos.
Abdomen blando, depresible, sin signos de irritación peritoneal. Herida quirurgica con aposito, Peristaltismo presente.
Extremidades edema grado II.
Paraclinicos:
08/08/2023: Calcio 8, Cloro 110. 7, Sodio 145, Potasio 3. 61, Cr 1. 2, PCR 3. 78, BUN 28. 7. Hb 10. 6, Hto 32, Plaq 1061000, Leucos 18400, Neu 11408.
Diagnósticos activos después de la nota Diagnóstico principal - SECUELAS DE COMPLICACIONES DE LA ATENCION MEDICA Y QUIRURGICA, NO CLASIFICADAS EN OTRAS PARTE, HIPERTENSION ESENCIAL (PRIMARIA), HIPERLIPIDEMIA NO ESPECIFICADA, PERITONITIS AGUDA, INSUFICIENCIA RENAL AGUDA.
Análisis y Plan de manejo: Paciente de 80 años, hospitalizada en contexto de sepsis de origen abdominal secundario a perforación del intestino delgado (post herniorrafia), hoy segundo día de manejo con Metronidazol + ciprofloxacina, adecuada evolución, afebril, continuamos vigilancia.
Información durante la estancia
¿A quién se informa?: Paciente
Se brinda información sobre: Resultados esperados de la atención y el tratamiento, Diagnóstico del paciente y las recomendaciones de autocuidado.
Firmado por: NATALY ESTHER BOHORQUEZ RUBIO, INTERNO(A), Registro N/A, CC 1192896506
****
Fecha: 08/08/2023 10:59
Nota Evolución Fisioterapia - Interconsultante - FISIOTERAPIA
Diagnósticos activos antes de la nota: SECUELAS DE COMPLICACIONES DE LA ATENCION MEDICA Y QUIRURGICA, NO CLASIFICADAS EN OTRAS PARTE, HIPERTENSION ESENCIAL (PRIMARIA), HIPERLIPIDEMIA NO ESPECIFICADA, PERITONITIS AGUDA, INSUFICIENCIA RENAL AGUDA.
Paciente remitida por el Intensiviosta Gustavo Martinez para prevenir desacondicionamiento
Hospitalizada con dx de:
Diagnostico
Sepsis de origen abdominal por perforación de intestino delgado (post herniorrafia)
Peritonitis secundaria
Lesión renal aguda KDIGO 2
Procedimiento
02/08/2023 Laparotomía exploratoria, resección intestinal, anastomosis intestinal manual TT
31/07/2023 Herniorrafia femoral incarcerada (Reducción intestinal sin reseccion intestinal), rafia de vena femoral derecha
Objetivo:prevenir complicaciones por reposo prolongado y promover independencia funcional
Estado actual del paciente:
Paciente alerta, orientada, con soporote de O2 por canula nasal a 1 lt/min, sentada en silla. Se observa edema de MsSs, conserva movilidad de las 4 extremidades, fuerza global conservada para la dad solo se observa leve disminución de la fuerza del MSI, buen control de tronco en bipedo, es capaz de demabular de manera lenta y asistda, depedneinete en autocuidado, previa a hospitalización completamente independiente.
Al iniciar SV:O2 91%, FC 82/min
Actividades realizadas durante la terapia:
Realiza ejercicios de bombeo gemelar, bombeo de MsSs, estiramientos pasivos de MsSs, isometricos de cuadriceps en sedente, activos libres y activos resistidos suaves de MsIs, activos resistidos de MsSs, ejercicios de patrón respiratorio diafragmático y estimualción de la amrcha al rededor de la cama con ayuda de la hija
Tolerancia del paciente:
Tolera bien los ejercicios, queda sentada en silla, acompañada por una hija (Astrid), con SV estables. O2 100%, FC 91/min
Adherencia al tratamiento:
N/A, es la primera atención
Información brindada:
Se dan instrucciones a la paciente y su hija sobre la frecuenbcia e importancia de realizar los ejercicios de bombeo, fortalecimeinto global; así como de permanecer el mayor timepo posible fuera de cama
Se establecen las metas del cuidado en rehabilitación
Escala del dolor: 0-No dolor
Diagnósticos activos después de la nota Diagnóstico principal - SECUELAS DE COMPLICACIONES DE LA ATENCION MEDICA Y QUIRURGICA, NO CLASIFICADAS EN OTRAS PARTE, HIPERTENSION ESENCIAL (PRIMARIA), HIPERLIPIDEMIA NO ESPECIFICADA, PERITONITIS AGUDA, INSUFICIENCIA RENAL AGUDA.
Firmado por: CARMENZA PAEZ ARCIA, FISIOTERAPIA, Registro 0448-94, CC 32747510
****
Fecha: 02/08/2023 16:19
Nota de Evolución - Tratante - CIRUGIA GENERAL
Cirugia general
Sospecha de perforación intestinal
POP del 31/07/2023 de herniorrafia femoral
Taquicardia, sin fiebre o hipotensión
Cardiopulmonar sin alteraciones
Abdomen distendido, signos de irritación peritoneal
Extremidades sin alteraciones
Neurológico sin déficit
Tomgorafía con neumoperitoneo
Elevación de los RFA
Diagnósticos activos después de la nota Diagnóstico principal - SECUELAS DE COMPLICACIONES DE LA ATENCION MEDICA Y QUIRURGICA, NO CLASIFICADAS EN OTRAS PARTE (En Estudio), DOLOR ABDOMINAL (En Estudio), HIPERTENSION ESENCIAL (PRIMARIA), HIPERLIPIDEMIA NO ESPECIFICADA.
Análisis y Plan de manejo: Paciente con sospecha de perforación intestinal, clínicamente en malas condiciones generales, tomografía con neumoperitoneo y elevación de los RFA. Se programa para laparotomía exploratoria y se procederá según hallazgos. Se explica al acompañante quien refiere entender y aceptar
Información durante la estancia
¿A quién se informa?: No aplica.
Firmado por: CARLOS ANDRES DELGADO LOPEZ, CIRUGIA GENERAL, Registro 1053814605, CC 1053814605
********
Fecha: 02/08/2023 19:10
Nota Procedimiento - Tratante - CIRUGIA GENERAL
Indicador de rol: Tratante
Tipo de herida: sucia
Diagnóstico preoperatorio: neumoperitoneo
Diagnósticos post operatorio: Perforación de intestino delgado
Procedimiento a realizar: Laparotomía exploratoria, resección intestinal, anastomosis intestinal manual TT
Cirujano: Carlos Andrés Delgado López
Ayudante: Laura Molina, residente - Eugenia Morales, interna
Anestesiólogo(a): Dr Velez
Instrumentador(a): Juan Moreno
Tipo de anestesia: General
Hallazgos operatorios: Peritonitis purulenta generalizada, perforación intestinal puntiforme en ileon a 90 cms de la valvula ileocecal, intestino delgado y colon hipoperfundidos en parches
Descripción del procedimiento: Siguiendo todos los protocolos institucionales y de la OMS y usando todos los EPP se procede a:
Lavado con solución de clorhexidina
Campos estériles
Laparotomía mediana
Disección hasta cavidad
Identificación de los hallazgos
Drenaje de peritonitis
Identificación de la perforación
Disección del meso del intestino y ligadura en varias tomas con seda 2-0
Enterectomia
Anastomosis de intestino delgado, termino terminal con puntos separados de PDS 3-0
Cierre del meso del intestino con polipropileno 3-0
Lavado peritoneal con abundante solución salina
Toma de muestra para cultivo
Secado de la cavidad
Verificación de la hemostasia
Cierre de la fascia con PDS 0
Lavado de la herida quirúrgica
Cierre de la piel con grapas quirúrgicas
Curación sobre la herida
Procedimiento sin complicaciones
Conteo de gasas, compresas, instrumental y cortopunzantes reportado como completo por instrumentación y enfermería antes del cierre
Muestras de patología: intestino delgado
Materiales: completos
Pérdidas sanguíneas estimadas: 100 cc
Complicaciones: no
Plan de manejo: Traslado a UCE, nada via oral, SNG a libre drenaje, antibiótico de amplio especto, cultivo de liquido peritoneal, patología, información a familiares
Se avalan los insumos, suministros e instrumentales utilizados en el procedimiento, con cantidades y referencias registrados por el Instrumentador Quirúrgico.
Diagnósticos activos después de la nota Diagnóstico principal - SECUELAS DE COMPLICACIONES DE LA ATENCION MEDICA Y QUIRURGICA, NO CLASIFICADAS EN OTRAS PARTE (En Estudio), DOLOR ABDOMINAL (En Estudio), HIPERTENSION ESENCIAL (PRIMARIA), HIPERLIPIDEMIA NO ESPECIFICADA.
Firmado por: CARLOS ANDRES DELGADO LOPEZ, CIRUGIA GENERAL, Registro 1053814605, CC 1053814605
************
Fecha: 03/08/2023 11:07
Nota de Evolución - Interconsultante - CIRUGIA GENERAL
Diagnósticos:
Sepsis de origen abdominal
Peritonitis secundaria
Perforación intestinal puntiforme en ileon a 90 cms de la válvula ileocecal
Lesión renal aguda KDIGO 2
Antecedentes:
Hipertensión arterial, dislipidemia, insomnio
Hernia femoral derecha incarcerada
*31 jul 2023: Herniorrafia femoral incarcerada (Reducción intestinal sin reseccion intestinal), rafia de vena femoral derecha
Tratamiento ambulatorio: Losartan 50 mg día, hidroclorotiazida 25 mg día, atorvastatina 40 mg día, trazodona 50 mg noche
Procedimiento:
31/07/2023 de herniorrafia femoral
02 ago 2023: Laparotomía exploratoria, resección intestinal, anastomosis intestinal manual TT
Aislamientos:
02 ago 2023, líquido peritoneal: bacilos gramnegativos
REfier eestsr mejor con dolor leve en abdomen
Signos vitales: Presión arterial (mmHg): 117/74, Presión arterial media(mmHg): 88, Frecuencia cardíaca(LPM): 82, Escala del dolor: 3-Leve
Paciente en aceptable estado gerenal
CP normal
abdomen blnmdo un poco distendido
heridas limpais
SBG poco activa
De 03 ago 2023: creatinina 2 magnesio 1. 9 potasio 4. 3 pcr 50 bun 42 hco3 26 calcio i 1 lactato 1. 1 hb 11. 9 htc 34 leucos 14400 plt 1062000
Diagnósticos activos después de la nota Diagnóstico principal - SECUELAS DE COMPLICACIONES DE LA ATENCION MEDICA Y QUIRURGICA, NO CLASIFICADAS EN OTRAS PARTE, DOLOR ABDOMINAL (En Estudio), HIPERTENSION ESENCIAL (PRIMARIA), HIPERLIPIDEMIA NO ESPECIFICADA, PERITONITIS AGUDA.
Análisis y Plan de manejo: Paciente en postquirurgico de ayer por fioltracion de necrosis puntiforme de ileo distal.
por ahora no se inica via oral
se cometno con uci
Información durante la estancia
¿A quién se informa?: Paciente/cuidador
Se brinda información sobre: Resultados esperados de la atención y el tratamiento, Diagnóstico del paciente y las recomendaciones de autocuidado.
Firmado por: VÍCTOR MANUEL QUINTERO RIAZA, CIRUGIA GENERAL, Registro 762534-01, CC 10019807
************
Fecha: 04/08/2023 11:36
Nota de Evolución - Tratante - CIRUGIA GENERAL
Sepsis de origen abdominal
Peritonitis secundaria
Perforación intestinal puntiforme en ileon a 90 cms de la válvula ileocecal
Lesión renal aguda KDIGO 2
Antecedentes:
Hipertensión arterial, dislipidemia, insomnio
Hernia femoral derecha incarcerada
*31 jul 2023: Herniorrafia femoral incarcerada (Reducción intestinal sin reseccion intestinal), rafia de vena femoral derecha
Tratamiento ambulatorio: Losartan 50 mg día, hidroclorotiazida 25 mg día, atorvastatina 40 mg día, trazodona 50 mg noche
Procedimiento:
31/07/2023 de herniorrafia femoral
02 ago 2023: Laparotomía exploratoria, resección intestinal, anastomosis intestinal manual TT
paciente en condiciones estables
sin picos febriles y sin taquicardia
Mejoria del dolor
Abdomen blando, depresible sin dolor y sin irritacion peritoneal.
Herida limpia
SNG 1450 cc
Diagnósticos activos después de la nota Diagnóstico principal - SECUELAS DE COMPLICACIONES DE LA ATENCION MEDICA Y QUIRURGICA, NO CLASIFICADAS EN OTRAS PARTE, DOLOR ABDOMINAL (En Estudio), HIPERTENSION ESENCIAL (PRIMARIA), HIPERLIPIDEMIA NO ESPECIFICADA, PERITONITIS AGUDA.
Análisis y Plan de manejo: Paciente con evolucion estable, con posible ileo POP
No retiramos sonda, continuamos manejo medico y vigilancia clinica
se comenta con meicos de la unidad
Información durante la estancia
¿A quién se informa?: Paciente/cuidador
Se brinda información sobre: Resultados esperados de la atención y el tratamiento, Diagnóstico del paciente y las recomendaciones de autocuidado, Efectos secundarios de medicamentos ordenados.
Firmado por: FRED ALEXANDER NARANJO ARISTIZABAL, CIRUGIA GENERAL, Registro 5-2740-05, CC 98667490
************
Fecha: 05/08/2023 10:19
Nota de Evolución - Tratante - CIRUGIA GENERAL
80 años
Acompañada
Diagnostico:
Sepsis de origen abdominal
Peritonitis secundaria
Perforación intestinal puntiforme en ileon a 90 cms de la válvula ileocecal
Lesión renal aguda KDIGO 2
Antecedentes:
Hipertensión arterial, dislipidemia, insomnio
Hernia femoral derecha incarcerada
*31 jul 2023: Herniorrafia femoral incarcerada (Reducción intestinal sin reseccion intestinal), rafia de vena femoral derecha
Tratamiento ambulatorio: Losartan 50 mg día, hidroclorotiazida 25 mg día, atorvastatina 40 mg día, trazodona 50 mg noche
Procedimiento:
31/07/2023 de herniorrafia femoral
02 ago 2023: Laparotomía exploratoria, resección intestinal, anastomosis intestinal manual TT
Tranquila, sin dolor
Con flatos abundantes y deposiciones
SNG inactiva y sin nauseas
FC: 76, afebril, PA: 140/70
Abdomen blando, no distendido, no doloroso
Heridas sin signos de infección
SNG inactiva
Diagnósticos activos después de la nota Diagnóstico principal - SECUELAS DE COMPLICACIONES DE LA ATENCION MEDICA Y QUIRURGICA, NO CLASIFICADAS EN OTRAS PARTE, DOLOR ABDOMINAL (En Estudio), HIPERTENSION ESENCIAL (PRIMARIA), HIPERLIPIDEMIA NO ESPECIFICADA, PERITONITIS AGUDA.
Análisis y Plan de manejo: Pacietne con muy buena evolución, sin evidencia de complicaciones del procedimiento
Con ileo resuelto
Pinzo SNG e inicio dieta liquida clara.
Explico a la paciente, su acompañante y comento con internista de UCE
Información durante la estancia
¿A quién se informa?: Paciente/cuidador
Se brinda información sobre: Resultados esperados de la atención y el tratamiento.
Firmado por: PAULA MARIA JARAMILLO GOMEZ, CIRUGIA GENERAL, Registro 5546-04, CC 39449772
*****
Fecha: 02/08/2023 23:29
Nota de ingreso a unidades - Tratante - MEDICINA CRITICA Y CUIDADO INTENSIVO
Fecha y hora de ingreso del paciente a la unidad: 02/08/2023 23:15
INGRESO UCE
Maria, 80 años de edad, residente en Medellín, barrio Córdoba, ama de casa. Hospitalizada entre el 30/07 y 01/08 con diagnóstico de hernia femoral incarcerada. Se realizó manejo quirúrgico, con reducción sin resección. Describen signos de sufrimiento de asa que reperfunde tras liberación. Se dejó malla. Sin complicaciones advertidas. Hoy es traída por servicio de atención domiciliaria por cuadro de dolor abdominal, 2 episodios eméticos y de diarrea. Al ingreso deshidratada, con dolor abdominal y defensa, marcada elevación de reactantes de fase aguda y lesión renal. TAC de abdomen con neumoperitoneo. Se programó para laparotomía exploratoria. Describen peritonitis purulenta generalizada, perforación intestinal puntiforme en ileon a 90 cms de la valvula ileocecal, intestino delgado y colon hipoperfundidos en parches. Se realizó drenaje, resección intestinal, anastomosis intestinal manual TT, cierre de cavidad. Se tomaron muestras para cultivo. Requirió soporte vasopresor en intraoperatorio que se retiró al extubar. Se inició antibiótico de amplio espectro. Se repuso potasio por gases al finalizar (pH 7. 48 pCO2 31 pO2 344 Na 125 K 2. 8 Cl 91 Ca 1. 01 hto 38% gl 125 lac 2. 2 eb -0. 4 hco3 23. 1 pafi 491).
Antecedentes:
Patológicos: Hipertensión arterial, dislipidemia, insomnio
Quirúrgicos: Herniorrafia femoral con malla (31/07/23)
Toxicológico: Niega
Tratamiento ambulatorio: Losartan 50 mg día, hidroclorotiazida 25 mg día, atorvastatina 40 mg día, trazodona 50 mg noche
Signos vitales: Presión arterial (mmHg): 124/70, Presión arterial media(mmHg): 88, Frecuencia cardíaca(LPM): 80, Frecuencia respiratoria(Respiraciones/minuto): 16, Temperatura(°C): 36. 5, Escala del dolor: 0-No dolor, Saturación de oxígeno(%): 96
Examen Físico: Condiciones generales: Aceptables, afebril, sin signos de dificultad respiratoria, con oxígeno suplementario por cánula nasal.
Sin vasoactivos.
Glucometría: 112
Cabeza y cuello: Mucosa oral húmeda, conjuntivas rosadas, escleras anictéricas. Cuello sin masas ni distensión yugular. Sin estridor ni disfonía.
Tórax y Cardiopulmonar: Ruidos cardiacos rítmicos, no soplo. Murmullo vesicular preservado sin agregados.
Abdomen: Blando, no doloroso, no masas.
Pelvis y Genitourinario: No evaluado.
Extremidades y Osteomuscular: Sin edemas, buen llenado capilar.
Neurológico: Alerta, orientada, lenguaje claro y coherente, sin focalización.
Diagnósticos activos después de la nota Diagnóstico principal - SECUELAS DE COMPLICACIONES DE LA ATENCION MEDICA Y QUIRURGICA, NO CLASIFICADAS EN OTRAS PARTE, DOLOR ABDOMINAL (En Estudio), HIPERTENSION ESENCIAL (PRIMARIA), HIPERLIPIDEMIA NO ESPECIFICADA, PERITONITIS AGUDA.
Reporte de paraclínicos recientes:
calcio: 8. 9, cloro: 89. 6, sodio: 129, potasio: 4. 1
creatinina: 2. 35, BUN: 38
PCR: 46. 85
HB: 12. 6, HTO: 4. 2, leucocitos: 16800, N: 54%, L: 26%, plaquetas: 1108000, Bandas: 14%
Análisis y plan de manejo: Paciente en la novena década de la vida, antecedente de hipertensión arterial y hospitalización reciente por hernia femoral encarcerada. Se realizó el 31/07 herniorrafia con malla sin complicaciones advertidas ni necesidad de resección intestinal. Hoy ingresa por cuadro de dolor abdominal, nauseas y vómito, con evidencia de neumoperitoneo en TAC, con reactantes francamente elevados y disfunción renal. Se llevó a lapatoromía. Describen peritonitis purulenta generalizada, perforación intestinal puntiforme en ileon a 90 cms de la válvula ileocecal, intestino delgado y colon hipoperfundidos en parches. Se realizó drenaje, resección intestinal, anastomosis intestinal manual TT, cierre de cavidad. Requirió soporte vasopresor de forma transitoria. Se inició cubrimiento antibiótico empírico con piperacilina/tazobactam en espera de cultivos. Se deja dosis plena las primeras 24h. Ajusto cristaloides para reposición de potasio y pérdidas por sonda nasogástrica. Continuaremos monitoreo estricto.
Información al ingreso
¿A quién se informa?: Paciente/cuidador.
Firmado por: SANDRA GOMEZ DE LOS RIOS, MEDICINA CRITICA Y CUIDADO INTENSIVO - MEDICINA INTERNA, Registro 05-4077-11, CC 1128406161
****
Fecha: 03/08/2023 10:50
Nota de Evolución - Tratante - MEDICINA CRITICA Y CUIDADO INTENSIVO
Ronda UCE
Diagnósticos:
Sepsis de origen abdominal
Peritonitis secundaria
Perforación intestinal puntiforme en ileon a 90 cms de la válvula ileocecal
Lesión renal aguda KDIGO 2
Antecedentes:
Hipertensión arterial, dislipidemia, insomnio
Hernia femoral derecha incarcerada
*31 jul 2023: Herniorrafia femoral incarcerada (Reducción intestinal sin reseccion intestinal), rafia de vena femoral derecha
Tratamiento ambulatorio: Losartan 50 mg día, hidroclorotiazida 25 mg día, atorvastatina 40 mg día, trazodona 50 mg noche
Procedimiento:
02 ago 2023: Laparotomía exploratoria, resección intestinal, anastomosis intestinal manual TT
Aislamientos:
02 ago 2023, líquido peritoneal: bacilos gramnegativos
De 03 ago 2023: creatinina 2 magnesio 1. 9 potasio 4. 3 pcr 50 bun 42 hco3 26 calcio i 1 lactato 1. 1 hb 11. 9 htc 34 leucos 14400 plt 1062000
S: La paciente refiere estar bien.
O: TA:117/74 Fc:72 Fr:21 Sat:98% Fio2:32%, cabeza y cuello con mucosas rosadas húmedas, ruidos cardíacos rítmicos sin soplos, murmullo vesicular de adecuada intensidad sin ruidos agregados, abdomen blando no dolor no masas, neurológico: conciente, orientada, responde el interrogatorio de manera coherente, sin déficit motor focal de extremidades.
Diagnósticos activos después de la nota Diagnóstico principal - SECUELAS DE COMPLICACIONES DE LA ATENCION MEDICA Y QUIRURGICA, NO CLASIFICADAS EN OTRAS PARTE, DOLOR ABDOMINAL (En Estudio), HIPERTENSION ESENCIAL (PRIMARIA), HIPERLIPIDEMIA NO ESPECIFICADA, PERITONITIS AGUDA.
Análisis y Plan de manejo: A: Paciente con estabilidad hemodinámica, sin requerir ningún soporte vasoactivo, cursa con sepsis severa de origen abdominal por peritonitis secundaria ya intervenida, sigue con reactantes muy elevado, PCR y trombocitosis severa que tenía incluso de hospitalización previa, adicional disfunción renal aguda, recibe maneo antibiótico con piperacilina tazobactam.
P: Ajusto antibiótico a función renal, sigue en UCE por sepsis no resuelta y disfunción renal aguda en progresión. Exámenes mañana.
Información durante la estancia
¿A quién se informa?: Paciente/cuidador
Se brinda información sobre: Resultados esperados de la atención y el tratamiento, Diagnóstico del paciente y las recomendaciones de autocuidado
Aclaraciones sobre la información brindada: Se da información a la paciente y a su acompañante (hijo), acerca del diagnóstico, tratamiento y pronóstico.
Firmado por: HERNAN MAURICIO GALLEGO GUTIERREZ, MEDICINA CRITICA Y CUIDADO INTENSIVO - MEDICINA INTERNA, Registro 17-15890-06, CC 75095045
***********
Fecha: 04/08/2023 09:30
Nota de Evolución - Tratante - MEDICINA CRITICA Y CUIDADO INTENSIVO
Evolución unidad de cuidados especiales
María, 80 años
Diagnósticos:
Sepsis de origen abdominal
Peritonitis secundaria
Perforación intestinal puntiforme en ileon a 90 cms de la válvula ileocecal
Lesión renal aguda KDIGO 2
Antecedentes personales
-Patológicos: hipertensión arterial, dislipidemia, insomnio, hernia femoral derecha incarcerada intervenida 31/07/2023 (se realizó reducción sin resección)
-Farmacológicos: Losartan 50 mg día, hidroclorotiazida 25 mg día, atorvastatina 40 mg día, trazodona 50 mg noche
-Alergias: niega
-Tóxicos: niega
Procedimientos:
-0208/2023: Laparotomía exploratoria, resección intestinal, anastomosis intestinal manual TT
Microbiológicos
-02/08/2023 líquido peritoneal: BGN escasos, cultivo aerobios pendiente
-02/08/2023 Hemocultivos aerobios pendientes (2)
Antimicrobianos
-Piperacilina tazobactam FI 02/08/2023
Soportes
Hemodinámico no tiene
Respiratorio no tiene
Registro enfermería
Tensiones en metas
Sin fiebre
No taquicardica
La 2849 Le 2370 B + 479
Subjetivo
Sin quejas de dolor, asintomática cardiovascular
Niega flatos y depsociones
Signos vitales: Presión arterial (mmHg): 131/63, Presión arterial media(mmHg): 85, Frecuencia cardíaca(LPM): 82, Frecuencia respiratoria(Respiraciones/minuto): 16, Escala del dolor: 0-No dolor, Temperatura(°C): 36. 7, Saturación de oxígeno(%): 93
Condiciones generales: Aceptables condiciones generales, alerta, consciente, orientada
Cabeza: Mucosa seca, conjuntiva normocrómica, esclerótica anictérica
Tórax y Cardiopulmonar: Con adecuada dinámica respiratoria, murmullo vesicular conservado sin agregados, ruidos cardiacos rítmicos sin sooplos
Abdomen: Sin distensión, heridas cubiertas sana, blando, dolor sin irritacion
Extremidades y Osteomuscular: Extremidades sin edemas, llenado 2 seg
Neurológico: No tiene déficit
Sonda nasogastrica activa
Paraclínicos 04/08
Hb 11. 9 Hto 34. 3 leucos 15400 Plaq 987000 n 10164 linf 154 10164
Creatinina 2. 17, BUN 55. 1
gases venosos ph 7. 3 HCO3 22. 6 BE -3. 9 Lac 1, Hb 11, spdop 138 potasoip2. 8 calcio 1. 14
Diagnósticos activos después de la nota Diagnóstico principal - SECUELAS DE COMPLICACIONES DE LA ATENCION MEDICA Y QUIRURGICA, NO CLASIFICADAS EN OTRAS PARTE, DOLOR ABDOMINAL (En Estudio), HIPERTENSION ESENCIAL (PRIMARIA), HIPERLIPIDEMIA NO ESPECIFICADA, PERITONITIS AGUDA.
Análisis y Plan de manejo: Femenina de 80 años, con diagnóstico anotado, peritonitis seundaria a perforación de víscera hueca. Esta en proceso de reanimación, sin soporte vasopresor, metas clínicas de perfusión, modula respuesta inflamatoria. Cubrimiento antibiótico ahora empírico, espera de cultivo de abdomen donde crece BGN y hemocultivos que van negativos. Sus azodos siguen elevados, sin indicacion de soporte es muy prerranal se optimiza cristaloides Además con hipocalemia moderada, se ajusta correción de electrolitos, con control de potasio en la tarde. Se discute con cirugía general. Se le explica a la paciente.
Información durante la estancia
¿A quién se informa?: Paciente/cuidador
Se brinda información sobre: Resultados esperados de la atención y el tratamiento, Diagnóstico del paciente y las recomendaciones de autocuidado, Efectos secundarios de medicamentos ordenados.
Firmado por: GUSTAVO ALBERTO MARTINEZ MIRA, MEDICINA CRITICA Y CUIDADO INTENSIVO, Registro 1037581132, CC 1037581132
***********
Fecha: 04/08/2023 18:33
Nota de Evolución - Tratante - MEDICINA CRITICA Y CUIDADO INTENSIVO
Ronda UCE tarde
Diagnósticos
Sepsis de origen abdominal
Peritonitis secundaria
Perforación intestinal puntiforme en ileon a 90 cms de la válvula ileocecal
Lesión renal aguda KDIGO 2
Antecedentes personales
-Patológicos: hipertensión arterial, dislipidemia, insomnio, hernia femoral derecha incarcerada intervenida 31/07/2023 (se realizó reducción sin resección)
-Farmacológicos: Losartan 50 mg día, hidroclorotiazida 25 mg día, atorvastatina 40 mg día, trazodona 50 mg noche
-Alergias: niega
-Tóxicos: niega
Procedimientos:
02/08/2023: Laparotomía exploratoria, resección intestinal, anastomosis intestinal manual TT
Microbiológicos
02/08/2023 líquido peritoneal: BGN escasos, cultivo aerobios BGN en tipificación
02/08/2023 Hemocultivos aerobios pendientes (2)
Antimicrobianos
Piperacilina tazobactam FI 02/08/2023
Labs 04/08/2023
Hb 11. 9 Hto 34. 3 leucos 15. 400 Plaq 987. 000 n 10164 linf 154 10164
Creatinina 2. 17 (208) BUN 55. 1
gases venosos ph 7. 3 HCO3 22. 6 BE -3. 9 Lac 1, Hb 11, spdop 138 potasoip2. 8 calcio 1. 14
Subjetivo: Tiene sed, ausencia de flatos.
LA: 1360cc diuresis: 420cc acumulado: 1736cc +
Glucometrias: 100-77-82 mg/dl
Signos vitales: Presión arterial (mmHg): 120/57, Presión arterial media(mmHg): 78, Frecuencia cardíaca(LPM): 75, Frecuencia respiratoria(Respiraciones/minuto): 19, Temperatura(°C): 36. 5, Peso(Kg): 50, Saturación de oxígeno(%): 95
Se revisa a la paciente con los EPP recomendados por la OMS para disminuir riesgo de covid 19
Regulares condiciones generales, ritmo sinusal fio2 0. 3 sat 95%
Mucosas pálidas húmedas sin ictericia
No ingurgitación yugular
Ruidos cardiacos rítmicos sin soplos
Murmullo vesicular disminuidos en bases
Abdomen herida quirúrgica cubierta
Peristalsis presente no signos de irritación peritoneal.
Extremidades sin edemas buena perfusión distal
SNC consciente orientada sin déficit
Diagnósticos activos después de la nota Diagnóstico principal - SECUELAS DE COMPLICACIONES DE LA ATENCION MEDICA Y QUIRURGICA, NO CLASIFICADAS EN OTRAS PARTE, DOLOR ABDOMINAL (En Estudio), HIPERTENSION ESENCIAL (PRIMARIA), HIPERLIPIDEMIA NO ESPECIFICADA, PERITONITIS AGUDA.
Análisis y Plan de manejo: Paciente en manejo de sepsis foco abdominal por peritonitis secundario a perforación intestinal puntiforme ileon, tiene abdomen cerrado viene creciendo bacilos gram negativos pendiente tipificación, cursanco actualmente con ileo poca producción de SNG, se repuso potasio control normal.
Manejo conjunto con cirugia general.
Se revisa kardex y se discute manejo con jefe de enfermer
Brindo información a paciente e hijo sobre su estado actual y manejo entienden y aceptan.
Información durante la estancia
¿A quién se informa?: Paciente/cuidador
Se brinda información sobre: Resultados esperados de la atención y el tratamiento, Diagnóstico del paciente y las recomendaciones de autocuidado.
Firmado por: RAFAEL ENRIQUE GARCES CONTRERAS, MEDICINA CRITICA Y CUIDADO INTENSIVO, Registro 13.11685.06, CC 73186081
0 notes
Text
What are the uses of Boron Nitride Ceramics?
Boron Nitride can be used in the manufacture of crucibles for smelting semiconductors and metallurgical high-temperature vessels, amorphous strip nozzles, semiconductor heat dissipation insulation parts, high-temperature bearings, thermocouple bushing, and glass forming molds.
Usually produced Boron Nitride is a graphite-type structure, commonly known as white graphite. The other is diamond type. Similar to the principle of transforming graphite into diamond, graphite-type boron nitride can be transformed into diamond-type boron nitride under high temperature (1800℃) and high pressure (800Mpa).
The B-N bond length (156pm) of this boron nitride is similar to the C-C bond length (154pm) of a diamond, and the density is similar to the diamond. The hardness of this boron nitride is similar to diamond, but the heat resistance is better than diamond. It is a new type of superhard material with high-temperature resistance, which is used to make drill bits, grinding tools, and cutting tools.

What are the uses of Boron Nitride Ceramics
Boron Nitride Material Properties-SU0012
Properties
Units
UHB
HB
BC
BMS
BMA
BSC
BMZ
BAN
Main Composition
BN>99.7%
BN>99%
BN>97.5%
BN+AL+SI
BN+ZR+AL
BN+SIC
BN+ZRO2
BN+ALN
Color
White
White
White
White
Graphite
White
Graphite
Greyish
Green
White
Graphite
Greyish
Green
Density
g/cm3
1.6
2
2.0-2.1
2.2-2.3
2.25-2.35
2.4-2.5
2.8-2.9
2.8-2.9
Three-Point Bending
Strength
MPA
18
35
35.00
65
65
80.00
90
90.00
Compressive Strength
MPA
45
85
70.00
145
145
175.00
220
220.00
Thermal Conductivity
W/m·k
35
40
32.00
35
35
45.00
30
85.00
Thermal Expansion
Coefficient (20-1000℃)
10-6/K
1.5
1.8
1.60
2
2
2.80
3.5
2.80
Max Using TemperatureIn
Atmosphere
In Inactive Gas
In High Vacuum (Long
Time)
(℃)
900
2100
1800
900
2100
1800
900
2100
1900
900
1750
1750
900
1750
1750
900
1800
1800
900
1800
1800
900
1750
1750
Room Temperature
Electric Resistivity
Ω·cm
>1014
>1014
>1013
>1013
>1013
>1012
>1012
>1013
Typical Application:
Nitrides
Sintering
High
Temperature
Furance
High
Temperature
Furance
Powder
Metallurgy
Powder
Metallurgy
Powder
Metallurgy
Metal
Casting
Powder
Metallurgy
High Temperature
Electrical Furnace
Components (High
Temperature Insulator
Sleeve Tube etc)
√
√
√
√
√
√
√
Metal Vaporize Crucible
√
√
√
The Container Of Metal
or Glass Melting
√
√
√
√
√
√
√
√
The Casting Mould
Components Of The
Precious Metal And
Special Alloy.
√
√
√
High -Temperature Support
Part
√
√
√
Nozzle And Transport
Tube Of The Melting Metal
√
√
√
√
√
√
√
Nitrides Sintering
√
Remark: The value is just for review, different using conditions will have a little difference
Read the full article
0 notes
Text
Shika
A quick brush-only sketch of a smiling 鹿.
Shika
Tools
LEUCHTTURM1917 dotted sketchbook (80 g/m², 145×210 mm).
Uni-ball Kuru Toga mechanical pencil, with Uni-ball 0.5 HB nano diamond leads.
Sakura Pigma Brush.
macOS Preview’s color adjustment tool.

View On WordPress
0 notes
Text
first of all do you even M_]C_X``02D9)1@`!`0(`E`"4``#_VP!#``,"`@,"`@,#`P,$`P,$!0@%!00$ M!0H'!P8(#`H,#`L*"PL-#A(0#0X1#@L+$!80$1,4%145#`\7&!84&!(4%13_ MVP!#`0,$!`4$!0D%!0D4#0L-%!04%!04%!04%!04%!04%!04%!04%!04%!04 M%!04%!04%!04%!04%!04%!04%!04%!3_P``1"`,?!`H#`1$``A$!`Q$!_\0` M'0`!``$$`P$```````````````<"`P8(`00%"?_$`&D0``$#`@0"!`4*#PL) M!P($!P$``@,$$04&!R$2,0@305$B,F%QL1075G*!D92AL]$)%188(S,W0E)B M=96RP=(D-#4V4V-S=(*2HB4F.$-$5&7A\"=59(.3H[1&\3E%PL74*$=7=H33 M_\0`'`$!``$%`0$```````````````8!`@,$!0<(_\0`2Q$``@$#`0,'!@P$ M!`4%``,```$"`P01!1(A,08R05%QL?`3(C-AD=$4%18C-%)4<H&2H<$U4Z+2 M0E6RX21B@L+Q)39#1>)$1O+_V@`,`P$``A$#$0`_`/JF@"`(`@"`(`@"`(`@ M"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@ M"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@ M"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@ M"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@ M"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@ M"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@ M"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@ M"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@ M"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@ M"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@ M"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@ M"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@ M"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@ M"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@ M"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@ M"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@ M"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@ M"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@"`(`@+534P MT=/+45$K(((FE\DLC@UK&@7))/(`*J3;PBC:2RS'SJ7E$<\T8.//71?M+-Y" MKG&P_88?+TN.TO:7\/S[EK%IGQ468,,JY6"[F05<;W-'E`*I.C5IK,XM?@5A M6IU'B,D_Q/0..8<T7-?3`>65OSK`WCB9EOX'F5.H>5J.8Q3YCPJ&4<V25L;2 M/<)6S"VK5%F$&_P9KSN*5-XG-+\2WZY>4?9/@_PZ+]I9/@=S_+E[&6?"[?\` MF+VH>N9E'V48/\.B_:3X%<_RY>QCX7;_`,Q>U#UR\H^R?!_AT7[2?`[G^7+V M,?"[?^8O:CGURLI>R?"/AT7[2?`[G^7+V,?"[?\`F+VH>N5E+V3X1\.B_:3X M%<_RY>QCX70?_P`B]J'KE92'_P!3X/\`#HOVE3X'<_RY>QE/AEN]WE(^U%FI MU5R71Q&6?-N"0QCF^3$(F@>Z7*]6-T^%*7L9;*^M8<^K%?BCJ>O;I[[.<N?G M6#]I9/BV]_DR_*_<:_QOIWVB'YE[QZ]NGOLYRY^=8/VD^+;W^3+\K]P^-].^ MT0_,O>/7MT]]G.7/SK!^TGQ;>_R9?E?N'QOIWVB'YE[QZ]NGOLYRY^=8/VD^ M+;W^3+\K]P^-].^T0_,O>/7LT])M]7.7/SK!^TGQ;>_R9?E?N*?&^G+_`/D0 M_,O>>O@.?<M9HZWZ3Y@PO%>JMUGJ*LCFX+\K\)-EK5+:O1])!KM31N4+NWN? M05%+L:?<>L:^F'.HB']L+7P;3>.)Y%1G_+%',^*?,.%PRL-G,DK(VN![B"5L MQM+B2S&FVNQFO*YH0>)32_%%OUQ\J>R7"?AL?[2JK.Y?"F_8RU7=N]ZJ+VHY M]<;*GLEPGX;'\ZK\#N?Y<O8RGPRW_F1]J'KBY5]DF$_#8_G3X'<_RY>QCX9; M_P`R/M0]<7*OLEPGX;'^TGP*Y_ER]C*_"[?^8O:AZXN5?9+A/PV/]I/@5S_+
35 notes
·
View notes
Text
Spooky's Review of "Bad Luck Jack "
....
Well if there's one thing that this short did, it influenced an increase of notes on my old Zoophobia stuff.
Disclaimer: this is an opinion based post. You're not obligated to agree with me. Have fun with what you enjoy, and if your opinions differ from mine, I'm happy to agree to disagree. Life's already miserable, so let's try not to give ourselves another reason to be sad. I hope you enjoy.
////////////
As someone whose account is still on Tumblr's recommended accounts list for the Zoophobia tag, I suppose I have a(n imaginary) obligation to at least discuss this short.
Of course, I reccomend you actually watch the short before reading this, but I'm actually not going to get into much spoilers here. Surprise, I actually don't have much to say about the story. I have heard people say they dislike the short due to its' simple, slice of life story. While I see where they're coming from, I actually don't mind this. Especially after the super packed HH pilot, Helluva Boss and Addict video. This actually felt strangely refreshing, having something not full of edge and chaos.
I liked the animation here for a similar reason. Yeah, there were some animation mistakes, and weird moments with characters moving stiffly, but once again, after HH and HB, the setting and atmosphere here was a nice change.
Most of my thoughts are centered around two things; the voices and the music. And before we get into these topics, I would just like to say.... Zoophobia is the furry version of Glee. I'm fucking calling it now.
---- The Voices
I'll go over the voices in the order of introduction in the short.
I love Christina Vee as Kayla's singing voice, but then again, I love it when she sings anything, so....
Kay's talking voice, however... well, it certainly caught me off guard. I get that Kay's Australian, and it seems that she'll be using a lot more of her country's slang and language, but I feel like the accent was a little over done. It's legitimately hard to tell what words are coming out of her mouth at times. That being said, her VA still managed to get Kay's personality and emotions across really well in spite of this.
Zill's voice admittedly bothers me a bit. I find that his and Jack's voices are far too similar, and I wish that there was more to the voices that helped them stand apart. I personally would have Zill's voice be a bit lower, and maybe give him more of a cool, easygoing attitude when he talks.
Damian was a bit of a surprise. Granted, Vivz has described his voice as high pitched and giggly, but, and maybe this could be just me, his voice reads as little kid to me. Like, preteen kid. Which isn't necessarily an issue per se, just something I found interesting. He definitely sounds like the spoiled brat he is.
Jack reminds me of your generic cartoon male lead. I feel that it would have been good to integrate a more hushed, anxious tone into his speech, mainly to separate him from Zill voice wise. Apart from that, didn't mind this one either.
Spam is really certifying that Irish tag out here, ain't he laddies? My only critique is to try to match his talking voice to his singing voice a bit more. You can tell someone else is doing the singing, and I think that something like that can be worked on.
Vanex is... good. I mean, there's not much else I can really say here. It's good. There ya go.
Rusty also sounds pretty similar to Jack and Zill, save for the tone. I think that giving a bit more grit to the voice could do some good here.
Autumn is one that I found interesting. He has a very mature, formal tone which fits the character fairly well. Yeah, his voice also sounds like the majority of the other male characters, but again, I think his voice is alright. Diversifying the male voices would definitely help his stand out more.
----------Music
Hey, something I actually have some experience in! (Over a decade playing instruments and studying music theory)
I don't mind the songs, and I think that they're on the same level as "Inside every demon is a rainbow ". By which I mean that they're not bad, but... they're also not great or memorable.
Honestly, the biggest problem here is how generic each song is. Granted, I can imagine the characters singing these types of songs. Of course Zill and Kayla are singing the sappy love song. Of course Spam is singing ADHD the musical. Of course Jack is... ok, it's harder to imagine Jack singing a pseudo "Dear Evan Hanson" Broadway ballad, but given that the song is non diegetic , thus moreso meant to reflect his emotions, we'll give him a pass for this one.
But speaking of Jack's song, while I think it's the best one, it also is the most frustrating to me. Due to it becoming this song depicting the emotions and feelings of Jack, it had a chance to stand out. Have some character in it. I called this a pseudo Dear Evan Hansen song, but here's the thing. Dear Evan Hansen, like many Broadway shows, have songs that don't just move the plot forward, but introduce us to the characters. We get an insight into the character's mind, and it's a chance to learn about them and relate to them.
Jack's song could have done something like this, and I think it's trying to, but it just falls short. We don't necessarily learn anything new about Jack, as we can already tell he has these thoughts from earlier scenes. The lyrics don't even really expand on these thoughts for the most part.
Not helping is generic dramatic song backing track Number 145. That's the other thing about the songs in this short. The lyrics are already not the most groundbreaking stuff in the world, but the instrumentation really isn't helping. There's nothing really outstanding here. No cool build ups, dynamics, time signature changes, key changes, chances to belt out some high notes, unique vocal melodies, nothing.
Imagine Zill and Kayla's song if it sounded less like a rejected Train song, and had some more character to it. We could start with Kay alone, only her and the piano, singing a verse. Her verse has a bit of a build up and crescendo, leading into Zill's entry in the second verse. Zill's entry could be accompanied by the entrance of the other instruments. After his verse, kay could come back in. We have some playful back and forth in the form of call and answer, leading to them harmonizing, all the while the music swells up, and just as the piece is reaching its climax, and they're about to kiss...
Boom! Cock blocked by the local trash demon.
I could make separate posts explaining what I'd do with each of these song, but I'm sure nobody wants to read a post where I go full music dork.
And besides, I think you get the picture.
All that being said, though, I enjoyed the short overall and would reccomend it for anyone looking for a pick me up in these trying times.
I apologize for wasting your time
- Spooky S Skeletons
20 notes
·
View notes
Photo

O SENHOR é o meu pastor, nada me faltará. Deitar-me faz em verdes pastos, guia-me mansamente a águas tranquilas. Salmos 23:1. Mesmo quando a ovelha se deita em pastos verdejantes, é apenas um descanso temporário, pois logo O Pastor as conduz para águas tranquilas e pelo vale da sombra da morte. Todos os dias ele as conduz nos caminhos da justiça, com bondade e misericórdia constantemente acompanhando-as. Também em Lucas 15:4-7, um pastor deixa seu grande rebanho em campo aberto para buscar e resgatar uma ovelha solitária perdida. Achando-a, põe-na sobre os ombros, cheio de alegria e a leva para casa. Jesus disse que ele mesmo é o bom pastor (Jo 10:11), Ele busca e salva os perdidos. Se referindo a nós como “meu rebanho”. Jesus Cristo é “o grande pastor das ovelhas”. (Hb 13:20). A obra de Deus na salvação é perfeita do começo ao fim, a liderança amável do Grande Pastor é cheia de bondade e misericórdia. Ele tem a intenção de livrar suas ovelhas do mal, através do vale da sombra da morte, e para a segurança e bênção. “Guia-me pelas veredas da justiça por amor do seu nome”. Sem Jesus não conseguiríamos percorrer com exatidão os caminhos da justiça. “porque estreita é a porta, e apertado, o caminho que conduz para a vida” (Mt 7:14). Pois “Justo é o Senhor em todos os seus caminhos”. (Sl 145:27). Deus é soberano na salvação dos pecadores. O divino pastor procura e salva os perdidos. Ele não é apenas o restaurador de suas almas; ele é também aquele que os guarda, cuida, os mantém na fé, os conduzindo nos caminhos da justiça. Deus é quem realiza tudo isso! Nossa redenção do pecado não é obra nossa. (Efésios 2:8-9). É o dom de Deus para que ninguém se glorie. Tudo pela Graça divina, até mesmo as coisas boas que fazemos galera, são obras que “Deus preparou de antemão, para que andássemos nelas” (Efésios 2:10)). “As minhas ovelhas ouvem a minha voz; eu as conheço, e elas me seguem” (Jo 10:27). Continuação nos comentários..👇🏻👇🏻 - - #palavradedeus #bibliadiaria #deusébom #jesus #maravilhosagraca #salvacao #sabedoria #espiritosanto #jovemsabia #devocional #milagre #jesusteama #versiculo #reinodedeus #pensenisso #ministeriofaladeus https://www.instagram.com/ministeriofaladeus/p/CYO54P6DJIN/?utm_medium=tumblr
#palavradedeus#bibliadiaria#deusébom#jesus#maravilhosagraca#salvacao#sabedoria#espiritosanto#jovemsabia#devocional#milagre#jesusteama#versiculo#reinodedeus#pensenisso#ministeriofaladeus
10 notes
·
View notes
Link
Check out this listing I just added to my Poshmark closet: New HUGO BOSS Round Metal Men Women Eyeglasses BOSS 1047 Rose Gold 53 23 145.
0 notes
Text
Pacaran bertahun, lalu Menikah, Goals?
Ketika standar baik-buruk tidak berdasarkan syariat Islam, tidak berdasar halal/haram, tidak berdasar cinta dan benci karena Allah, tidak berdasar suka dan tidak suka karena Allah.
Akhirnya manusia-manusia abad ini menyalurkan cara berkasih sayangnya melalui jalan pacaran, ataupun pacaran dinamai ta’aruf namanya doang ta’aruf tapi petantang petenteng jalan berdua chat-chatan telpon-telponan halah modus.
Pada akhirnya menganggap apa yang dilakukan bukanlah suatu kesalahan, bukan suatu hal yang tidak pantas karena ada banyak orang yang juga melakukannya.
Disaat pacaran, mengetahui apa yang dilakukan adalah ketidakpastian, maka menikah menjadi cita-cita yang idam-idamkan, apalagi yang telah pacaran menahun, pernikahan seperti hadiah yang amat sangat besar hingga bersyukur pada Allah karena bisa menikah dengan orang yang dipacari. Lalu muncul orang-orang yang notabennya muslim menceritakan kisah pacaran agar orang-orang terinspirasi? innalillahi. Akal sehatwe nangdi?
To be nyinyir sedikit, saya cuma bertanya-tanya, apakah bersyukur pada Allah harus selalu karena Allah membiarkan kehidupan kita berjalan sesuai dengan yang kita inginkan?
Para aktifis pacaran, apakah kalian tidak takut dengan peringatan Allah menyoal istidraj? apakah kalian tidak khawatir balasan dosa apa yang akan Allah timpakan pada diri akibat menumpuknya dosa pacaran bertahun-tahun yang kalian lakukan itu? meskipun kalian menikah pada ujung cerita pacaran kalian.
Apalagi jika kalian pernah HB (hubungan badan), yang mana dosa zina merupakan dosa besar, lalu disaat menikah kalian bahagia bersyukur bahkan sujud syukur tidak namun tidak dibersamai dengan taubat resepsi pernikahan tidak sesuai dengan syariat, semua pelanggaran syariat kalian langgar lalu kalian tertawa bahagia senang dsj astagfirullah.
Allah berfimran dalam Alqur’an : "Iblis berkata: "Ya Tuhanku, oleh sebab Engkau telah memutuskan bahwa aku sesat pasti aku akan menjadikan mereka memandang baik (perbuatan maksiat) di muka bumi, dan pasti aku akan menyesatkan mereka semuanya." kecuali hamba-hamba Engkau yang mukhlis di antara mereka". (TQS. Al-Hijr: 39-40).
Pacaran lama banget lalu menikah lalu menginspirasi orang agar bertahan dengan keadaan pacaran udah kek surat Al-Hijr ayat 39-40 itu, bener-bener dijadikan indah kemaksiatan yang dilakukan.
Padahal bisa jadi hanyalah kenikmatan yang disegerakan, yaAllah naudzubillahimindzallik
Karena mengingat kita ini manusia pasti akan selalu berbuat dosa, disaat single aja belum tentu gak luput dari dosa, apalagi disaat pacaran, kenapa orang pacaran bertahun-tahun lalu Allah kehendaki menikah dengan pacarnya malah seolah-olah seneng? padahal sejatinya cuma fatamorgana,
andaipun kalian bahagia didunia dengan kemaksiatan yang terus menerus dilakukan sampai mati naudzubillahimindzallik, maka seperti kata mbak indadari dalam quotesnya : ada orang-orang yang semasa hidupnya terlihat baik-baik saja, harinya penuh tawa tapi dalam kuburnya penuh dengan teriakan dan kesengsaraan,
yaallah jangan sampe Allah balas kemaksiatan kita nanti udah mati, beneran itu menakutkan. Dibales saat hidup itu masih lebih baik, kita masih bisa taubat, kalau dah mati? yaAllah belum kalau kalian tidak meninggalkan keturunan yang shalih/shalihah huhuhu.
saya yang ngeliat yang ngeri, ngeri karena hanya Allah yang tahu kapan Allah bakal jawab kemaksiatan-kemaksiatan yang terjadi.
Maka kalian yang menganggap pacaran bertahun-tahun lalu menikah merupakan goals kehidupan percintaan, pikirkanlah baik-baik, membangun rumah tangga dengan cara seperti itu hanya menumpuk dosa yang akan dibayar tunai nanti.
Masalah yang nanti ada susah diartikan sebagai bagian ujian bisa jatoh jadinya ke teguran, tapi bersyukur kalau dapat teguran, artinya ada dosa-dosa yang harus kita istigfari.
Nasihat saya pada yang pacaran bertahun-tahun sekarang menikah, taubatilah masa lalu anda, ketahuilah memaksiati Allah tidak pernah berakhir dengan kebahagiaan, tidak akan pernah, sekalipun hari ini anda menganggap hidup anda dipernuhi kenikmatan, ketahuilah Allah lebih tahu apakah itu nikmat atau teguran yang ditunda.
Belum lagi tipikal kita sebagai manusia, dikasih kenikmatan seneng dan bahagia, giliran dibalas kemaksiatannya langsung terpuruk.
“Bila kamu melihat Allah memberi pada hamba dari (perkara) dunia yang diinginkannya, padahal dia terus berada dalam kemaksiatan kepada-Nya, maka (ketahuilah) bahwa hal itu adalah istidraj (jebakan berupa nikmat yang disegerakan) dari Allah.” (HR. Ahmad 4: 145)
“Maka tatkala mereka melupakan peringatan yang telah diberikan kepada mereka, Kamipun membukakan semua pintu-pintu kesenangan untuk mereka; sehingga apabila mereka bergembira dengan apa yang telah diberikan kepada mereka, Kami siksa mereka dengan sekonyong-konyong, maka ketika itu mereka terdiam berputus asa.” (TQS. Al An’am: 44).
Syaikh As Sa’di menyatakan, “Ketika mereka melupakan peringatan Allah yang diberikan pada mereka, maka dibukakanlah berbagi pintu dunia dan kelezatannya, mereka pun lalai. Sampai mereka bergembira dengan apa yang diberikan pada mereka, akhirnya Allah menyiksa mereka dengan tiba-tiba. Mereka pun berputus asa dari berbagai kebaikan. Seperti itu lebih berat siksanya. Mereka terbuai, lalai, dan tenang dengan keadaan dunia mereka. Namun itu sebenarnya lebih berat hukumannya dan jadi musibah yang besar.” (Tafsir As Sa’di, hal. 260)
93 notes
·
View notes
Text
Day 4 is a wrap and I feel like such a scam because I still haven't actually done anything. I know why really, I just hate it.
Anyway. 159 when I got up. I weighed myself like an hour ago and I was 159.4 which is amazing. Then I had a small snack and a lot of 0kcal squash... I think at least 500ml (I drank a litre this evening but I can't remember exactly where I was at the point that I weighed). So when I weighed just now (proper pre-bed weigh) I was 160.6. I shouldn't complain really, that was my morning weight the past few days and if I still am 2lbs lighter in the morning like usual, then I'll be 158.6 which is lower than today. Just that I really want to be 158, and I'm thinking if I hadn't had that squash and food I might have been able to get to 157.4... but really I know that 1) hydration is more important, especially in my current state, and 2) if it's just the water weight (500ml weighs about 1.1lbs) then I can still reach a good weight for tomorrow anyway.
The pain in my side went away eventually but it took pretty much all day. I was wondering if it could be a spleen problem. If it is, one of the symptoms is weight loss. So I feel conflicted there. I don't want to be sick. I know what it's like, I'm sick of being sick, I hate it. But I also want to lose weight...and usually when I have a health problem it's something that causes weight gain. So it'd be nice to have something that'll make me lose weight for once. But really if I could control everything I'd just be totally healthy and able to lose weight anyway and then this all wouldn't bother me so much.
I'm also still gonna be on my period for a few days so there's weight to lose there. I don't know how much. My dream goal for Monday would be 155lbs, but to do that I have to lose a pound a day. I haven't even worked out so far this week. I set that goal high because I figured period weight would be a thing, but it's possible I can still fail. Given I didn't work out. Idk.
I'm really hoping tomorrow I can work out. But I say that every day. I kept to my calorie goal today easily. Limit was 1000 which was meant to be a low day - I had 825kcal. Tomorrow is meant to be 1500 I think? Or higher anyway. But I wrote those limits before I realised I was already eating 800-1000kcal a day as it is. So idk. I still need to work out. In the past I was at my best in every way when I ate about this much and worked out 2hrs a day. That's my goal I guess. So I need to work out as soon as I can. If not tomorrow then the day after. Just whenever all this pain and fatigue goes away. I know that it at least shouldn't last into next week - by then my period will be over and my meds will be back in my system properly. It won't last forever. Just I'd like to work out sooner so I can get to 155.
Last time I was 155lbs... I think was January or something. Maybe not even that. I got up to 163 in May, got down to 158 in June, gained more back, just got back under 160 now. I want to break past 157 at least so I'm in a range I haven't been in for a while. But 155...that would be good. That's my obsession. Once I hit that it'll be 150. Then 145. God it excites me thinking about it.
My stomach is doing hungry rumbles which is soothing...how easy it is to slip back into comforting old habits.
It's that time of night where I need to go to sleep, but I'm not yet sleepy, and there's nobody around to talk to as usual. Hb won't be awake for a while yet so I might see him tomorrow, maybe. At least I had time with my cats. I just need to entertain myself now long enough til I fall asleep. Then get up and work the fuck out. Hopefully I'll have got to 158lbs.
2 notes
·
View notes
Text
Lupinepublishers|arly Decompressive Craniectomy for Post- Thrombolysis Symptomatic Intracranial Haemorrhage
Key Message
Intravenous thrombolysis for acute ischemic stroke can be complicated by intracranial haemorrhage. Early decompressive craniectomy in such patients can be life saving but is associated with high risk of peri operative bleeding. We managed such a patient with decompressive craniectomy within 24hrs of thrombolysis by correcting coagulation with the help of thromboelastograhpy.
Keywords: Decompressive craniectomy; Intravenous thrombolysis; Symptomatic intracranial haemorrhage; Thromboelastography
Introduction
Acute ischemic stroke is one of the leading causes of death and permanent disability in the world. Intravenous thrombolysis (IVT) with recombinant tissue plasminogen activator (rt-PA) has been the recommended treatment modality in acute ischemic stroke [1]. but the most dreadful complication of thrombolysis is intracerebral haemorrhage in about 7% cases. The clinicians are faced with difficult decision of how to best treat these patients as there are no evidence based guidelines regarding the management of such complications. The American Heart Association has suggested only empirical therapies to replace clotting factors and platelets to reverse coagulopathy [2]. Decompressive craniectomy (DC) is a life-saving procedure for malignant middle cerebral artery stroke associated with cerebral oedema, enough to cause herniation and death [3]. The decision of decompressive craniectomy following intracerebral haemorrhage after intravenous thrombolysis is not without the risk of peri operative haemorrhage. We report the first case where decompressive surgery was uneventfully performed as a life-saving procedure within 24hours of developing symptomatic intracerebral haemorrhage after intravenous thrombolysis. The timing for decompressive craniectomy was guided by thromboelastography (TEG).
Case report
A 63-year old hypertensive, diabetic man presented with left hemiplegia within 140 minutes of onset. On examination, he was alert, GCS 15, left hemiplegia, right gaze palsy and dysarthria, NIHSS (National Institute of Health Stroke Scale) of 17. Magnetic resonance imaging of the brain revealed infarct in the superior division of right middle cerebral artery (MCA) (Figure 1a). His blood biochemistry was unremarkable (Hb-13.8, Plt-145, PT-12.2, and RBS-174). After written consent, thrombolysis was started at 22:10hrs on 11.1.2015 with rt-PA, 5.8mg as bolus followed by 52.7mg infusion over one hour. At 5:30hrs on 12.1.2015, he had upper gastrointestinal bleed followed by impairment in consciousness and his NIHSS score increased to 28. Immediate repeat CT scan of the brain revealed extensive infarction of MCA with haemorrhage in the infarct, extensive oedema and midline shift with uncal herniation (Figure 1b). As he had been recently thrombolysed, his repeat coagulation profile was performed (Hb-10.4, Plt-160, PT-15.2, APTT-27.8, FDP- 256mg/dL) including thromboelastography which was classical of fibrinolysis. Eight units of cryoprecipitate and four units of fresh frozen plasma were transfused in the next six hours and repeat thromboelastography was normal. Then the decision was to proceed with decompressive craniectomy (15:30hr on 12.1.15). A bone window of 12cm in the antero posterior direction in the fronto parieto temporal region was created and duroplasty was performed. The procedure was uneventful. He did not receive any blood products in the peri operative period. Brain CT scan was again performed on the following day and it showed resolution of midline shift with no new hematoma (Figure 1c). He was managed in the intensive care unit with gradual weaning of sedation and ventilation. He was discharged in the sixth week on tracheotomy and NIHSS score of 12. Three months later he was admitted for cranioplasty (Figure 1d) and tracheostomy closure with Mrs Score of 3 (Figure 2a & 2b).
Figure 1: (a) Magnetic resonance imaging of the brain (diffusion weighted image) done at presentation shows acute infarction of the right superior middle cerebral artery. (b) Non contrast CT of the brain done 8 hours after thrombolysis showed haemorrhage in the infarct resulting in mid line shift and mass effect. (c) Non Contrast CT of the brain done on the next day after decompressive craniectomy and hematoma evacuation revealed no new bleed and resolving mass effect.(d) Non Contrast CT of the brain following cranioplasty.
Figure 2: (a) Thromboelastograph trace obtained after 8hr of thrombolysis with R-1.7min, α-66.80, MA-19.6mm, LY30-97.4%, EPL%-100%. These features are characteristic features of fibrinolysis with normal R time, decreased maximum amplitude (MA), raised LY30 (percentage decrease in maximum amplitude or lysis after 30 minutes) and raised EPL. EPL represents the computer prediction of 30mins clot lysis based on interrogation of actual rate of diminution of the trace commencing 30sec post MA with a normal value of <15%. It is the earliest indicator of abnormal lysis. (b) Thromboelastographic trace obtained after infusion of cryoprecipitate and fresh frozen plasma with R-6min, K-1.5min, α-67.50, MA-49.6mm, LY30-0%, EPL%-0%.
Discussion
Thrombolysis remains the treatment of choice in acute ischemic stroke but with increased risk of symptomatic intracranial haemorrhage (ICH).The mortality in these patients is reported to be as high as 45% [4]. There are a few case reports in literature that state DC might be beneficial in the context of post IVT in patients with refractory cerebral oedema [5]. But the most important void is the optimal time to perform DC following thrombolysis. To the best of our knowledge there is only one prior case report where decompressive craniectomy was performed for intracranial haemorrhage following unsuccessful IVT after 48 hour of thrombolysis [6]. Here we report the index case where symptomatic intracranial haemorrhage followed thrombolysis, and was managed by DC and hematoma evacuation within 24 hours of IVT. This early life saving surgery was possible only after rapid correction of coagulation profile with the help of thromboelastography. As, a large series is difficult to be conducted in such cases, it is of interest to report small experiences as ours where the clinical dilemma of performing a surgery following thrombolysis with rt-PA was guided by thromboelastography.
Recombinant t-PA is an exogenous stimulator of the fibrinolytic system that enhances local fibrinolysis by converting plasminogen to plasmin. Our concern was the increased risk of peri operative haemorrhage associated with high mortality due to the persistent effect of TPA. With regard to the pharmacokinetics, half-life of rt- PA is <5 min, with clearance rate of 380-570mL/min [7]. Hence, 80% of rt-PA is cleared from the plasma within 10 minutes of administration. Despite short half-life of rt-PA fibrinolytic effects peak at 4hours and can persist up to 24-48hours [7]. The clinical dilemma in such a scenario was to wait for the disappearance of the fibrinolytic effects to avoid peri operative bleeding at the cost of outweighing the benefits of early DC in reducing the raised ICP. The other option was to efficiently detect and correct the coagulation abnormality by transfusing specific blood products to minimize the risk of bleeding. We had the benefit of thromboelastography at our institute to guide.com with the correction of the deranged coagulation profile before proceeding for DC. S Takeuchi et al. retrospectively reviewed 20 patients who underwent DC for malignant hemispheric infarction after IV TPA administration, with another 20 patients undergoing DC without prior IV TPA administration [8]. They observed intracranial bleeding or worsening of pre existing ICH in two patients (10%) in each group, but tPA was not thought to be contributory to the hemorrhagic events because of the long intervals between the IV tPA and DC(185 and 136h, respectively). However, fibrinolytic markers, such as fibrinogen or fibrin degradation products were unfortunately not measured in the above series.
Thrombelastography or TEG measures the physical properties of the clot via a pin suspended in a cup from a torsion wire connected with a mechanical-electrical transducer. TEG is different from other coagulation tests as it provides global information on the dynamics of clot development, stabilization and dissolution [9]. It assesses both thrombosis and fibrinolysis. Its role is established in cardiac and liver transplant surgery and is being increasingly explored to study role of fibrinolysis in early trauma coagulopathy [10]. Although routinely tested coagulation parameters (BT, CT, PTI, and APTT) were also normal in our case but TEG was characteristic of enhanced fibrinolysis. Hence, we transfused cryoprecipitate and fresh frozen plasma after which the TEG was normal, and we could proceed with surgery.
Conclusion
Decompressive hemicraniectomy with hematoma evacuation following thrombolysis represents an aggressive life saving treatment approach, especially for the patients who develop hemorrhagic complications of intravenous thrombolysis. TEG is one modality which can guide the reversal of deranged coagulation parameter so that major surgery can be undertaken with minimal risk. The decision to proceed with major surgical intervention requires a competent multi disciplinary team as well as an open discussion with relatives as DC may preserve both life and functional ability in well selected patients. More research is needed in this field to elucidate the potential for both modalities in appropriate patients.
For more Lupine Publishers Open Access Journals Please visit our website:
http://lupinepublishers.us/
For more Research and Reviews on Healthcare articles Please Click Here:
https://lupinepublishers.com/research-and-reviews-journal/
To Know More About Open Access Publishers Please Click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
4 notes
·
View notes
Text
That Summer Chapter 145 Summary!

WEE WOO WEE WOO HERE WE GOOOOO
OUR BEAUTIFUL HB is chilling at a diner and staring out the window when someone takes a seat across from him. It's Eldo LOL she saw the news about his dad's scandal, and the power struggle that was happening. Eldo figures this is a good thing for HB, though, since if his dad has to step down from candidacy, he can go back to Korea.


HB denies it, saying that the deal has nothing to do with the election. Eldo pouts, asking what he's going to do about Jumi then. HB looks unamused, wondering why he even told her about that in the first place. Eldo doesn't care, saying he told her because he was lonely abroad and had no one else to talk to except her LMAO. She asks why he's not contacting her, but he doesn't respond :( She continues to say it would be nice if YW was still single, since it feels like a waste to have him belong to just one person.

Eldo says she never imagined he and YW would break up, though. HB looks kinda sad at that, saying that it was all in the past and that he threw both of them away.

But Eldo tells him to stop beating himself up, because although he's the worst, he's not that bad LOL why she gotta roast him every sentence T__T

Eldo: Hey,
-I don't know what's going on,
She brings up a story from the past when they were all in elementary, and their parents would all have a gathering. At some point, HB and his dad would start attending, and all the parents would encourage the kids to get along. But HB stayed isolated :( Later on Eldo was running to bathroom when she spotted HB's dad hitting HB and scolding him for not making friends YIKES can I call 911???

Eldo was surprised that HB had gotten punished for that, because she didn't think that was reason enough to be yelled at over. HB isn't impressed, asking if she forgot she was reason he was isolated in the first place because she took the initiative to exclude him ALSKFJAKL. Eldo corrects him and says she never took the initiative, but just simply chose not to include him in stuff I'M DONE LOL.

But she also says that's the reason why she started to believe in karma—ever since she tattled on the fact that HB and YW went to the same academy, she thinks there was a butterfly effect that led her to be stuck abroad with him (which in her opinion, is the worst situation she could imagine).

She asks again if he's really not going to contact Jumi, and HB says what right does he have to do that at this point? :( :( :( Eldo agrees, saying he's way too late, and that had that been her, she would've gotten 5 boys a week confessing to her. That triggers HB, and she keeps taunting him asklfjakl. He says that even if they were the only two people stuck on an inhabited island, he would have no intentions on being her friend LOL.

He asks her to get lost, and she gets up to leave, wondering if she did an unnecessary thing. HB's confused at that, but all Eldo says is that if he plans on contacting Jumi, he should do it already. BOY LISTEN TO HER FOR ONCE.

Outside, Eldo meets up with a mysterious figure which is obviously YW by the way she reacts and calls him “Sunbae”. I'M CRYINGGG. She's glad to see he looks well, saying college life did good for him. She tells him that HB's over in the diner and watches him leave. She looks pretty happy as she leaves, saying she doesn't care if YW's gay and that he doesn't like her. She's still going to fangirl over him until she dies. UM GIRL MOOD? I'M PROUD OF YOU GOOD JOB.

HB's still chilling out at the diner, staring blankly at nothing until he notices the figure approaching him. He looks shooketh as YW walks up and says hi. BROOO WE GONNA DIE NEXT CHAPTER I CAN FEEL IT ALREADY. ORDER YOUR CASKETS.


50 notes
·
View notes
Photo



I decided to clean my room instead of studying (and I could have gotten a LOT done) because I am honestly just SO OFF today. I was doing really well, but we have this peer teaching tomorrow for our cadaver’s back anatomy and I went down to practice but it was FUCKING CROWDED bc of a practice practical for our exam NEXT WEEK and my body was tagged and there were so many people and kdfhdskf sdfldskfjsdfl my anxiety flared up REALLY BAD and I almost had a panic attack so THAT WAS COOL.
Anxiety is so stupid, my body’s like “omg there’s lots of people, better FREAK THE FUCK OUT.” I’m not even stressed about school. There were literally just too many people in a small place and I couldn’t leave because I needed to learn the anatomy for tomorrow but my cadaver was tagged and just UGH
So I went home and I’ve been FaceTiming my boyfriend while we’re both on mute to work on our own things but it’s been helpful. I’m just so annoyed because this anxiety attack really drained me and so my productivity drastically declined. I still managed to do some stuff, like I e-mailed a professor about getting shadowing and doula training set-up for students, sent another e-mail for this bake sale I’m hosting for my community partner, listened and concept-mapped SketchyPharm’s sympathomimetics lecture, and did some review for my OSCE on Friday. I also spammed out a link to write letters to Governor Kasich in Ohio for these bullshit draconian restrictive-AF abortion bans that are really PISSING ME OFF bc
even though he said he wouldn’t sign the heartbeat bill (HB 258) you never really know, and that shit makes NO exceptions for rape or incest and makes abortion illegal after SIX FUCKING WEEKS when most women don’t even KNOW they’re pregnant, and
senate bill 145 will make performing D&E abortions in the second trimester a FOURTH DEGREE FELONY... like come ON abortions are sooooo so so much safer than childbirth and since when can health care be dictated by dumb-ass white men in politics who have NO medical background????? (for a long time apparently especially regarding their obsession with fetuses over actual live ppl but w/e) but in any case he’s more likely to sign that one & it’s just this progressive chipping away at abortion access
Anyway it’s the worst so if you’re interested in sending a PRE-WRITTEN letter, it takes like 20 seconds tops so PLEASE DO IT FOR ME & here’s the link
I literally posted it on my main blog and tagged it with as many tags as it would allow me, and I spammed it in some texts and on my Facebook timeline and school’s Facebook page and GroupMe
SO I’M DOING WHAT I CAN
At least I got a REALLY FUCKING NICE E-MAIL from an M2 who was in my LC last year and said she was proud of what we’re doing for our community partner (the bake sale and a plastic bag drive I organized) so that was a feel-good moment. AND IN OTHER GOOD NEWS THERE WERE BORDERLANDS 3 LEAKS AND I’M SO EXCITED I COULD DIE. So things to look forward to and stuff
2 notes
·
View notes
Last Seen Blogs

frogspirit124
Untitled

citrineaudacity
Audacity is Orange

ezratuba
"ezra+tuba"

all-stargamer99
WELCOME TO MY DOMAIN

missmemoir
your girl interrupted 𓆩♡𓆪