#Lupinepublishersgroup
Text
Lupine Publishers | Oral Agents in the Treatment of Inflammatory Bowel Disease: A Remarkable Progress

Abstract
Despite remarkable progress for management of moderate-to-severe IBD patients, there are significant rates of primary nonresponse, loss of response, and/or adverse events thereby necessitating additional treatment options. Additionally, the burden of intravenous administration or subcutaneous injection of biologics accompanied by associated high cost necessitate the development of alternative treatments. In recent years, remarkable research has focused on the development of oral small molecule agents. Fortunately, the rapidly growing number of targeted therapies with oral small molecule agents offer the advantage of ease of administration with the durable effectiveness and no downside of immunogenicity with relatively more safety profile compared to the FDA approved biologic agents with relatively lower cost in the management of patients with moderate-to-severe IBD. The purpose of this review article is to summarize available novel oral small molecule agents in treatment of patients with IBD. Two of the oral small molecule agents, tofacitinib and ozanimod were already approved by the FDA for patients with moderate-to-severe ulcerative colitis. We will not include other emerging therapeutic modalities such as microbiome targeted or stem cell therapies in this review.
Introduction
Inflammatory bowel disease (IBD) including ulcerative colitis and Crohn’s disease are chronic relapsing disorders of intestinal inflammation which leads to decreased quality of life, disability, and bowel damage resulting in hospitalizations and surgeries [1]. Several genetic models have been developed for the inflammatory cascade that leads to the chronic inflammation seen in IBD, but none of these models have been able to account for all the observed pathophysiologic features. This complexity is probably secondary to the intricate nature of IBD and an incomplete understanding of the interactions between the mucosal immune system and the intestinal microbiota [2]. The current goal of treatment is to achieve clinical, endoscopic and histologic remission of disease activity. Management of IBD is generally divided into induction and maintenance phases. These phases involve achieving remission of inflammation quickly usually over a 2-3 month period and then maintenance of that clinical and histologic remission beyond that point Table 1.
5-ASA acts as a topical anti-inflammatory agent that has efficacy within the lumen of the intestine [3]. Although its use is well established in ulcerative colitis, its efficacy in its effect in Crohn’s disease is not better than placebo. Mild-to-moderate ulcerative colitis can be managed with oral 5-ASA treatments, but is not effective for moderate-to-severe disease. Older treatments for moderate-to-severe IBD include steroids and thiopurines including azathioprine, mercaptopurine, and methotrexate Table 2. Despite the efficacy of prednisone in improving acute symptoms of IBD patients, they have not consistently demonstrated effectiveness in controlling histologic inflammation. In addition, side effects related to long term use of steroids can be debilitating including but not limited to insomnia, personality changes, acne, fatigue, and weight gain. Alternative agents such as the oral controlled ileal release budesonide have been developed. Budesonide is efficacious in the management of inflammation in the terminal ileum and right colon. This makes budesonide effective for short-term relief of symptoms for mild-to-moderate IBD but not a good long-term option. The efficacy of thiopurines to maintain medically induced remission as well as to prevent post-operative recurrence in IBD has been well established. In the SONIC trial, the mucosal healing rate in patients in clinical remission was not significantly different between the azathioprine and anti-TNF monotherapy arms (36% vs. 43%) [4]. Despite their effectiveness many patients elect to stop thiopurine therapy. Up to 40 percent of patients discontinued thiopurine therapy in the first 4 months of treatment due to intolerance or ineffectiveness [5]. In addition, there is no doubt that thiopurines safety profile is inferior as there is a significant risk of developing lymphoma and non-melanoma skin cancer [6]. No satisfactory management of IBD was achieved prior to the development of infliximab. Current recommendations for the management of IBD with biologics include the use of early therapy with a treat-to target strategy to achieve clinical remission, mucosal and histologic healing which ultimately decrease the risk of corticosteroid use, surgeries, hospitalizations and increases quality of life [7]. Available biologic agents include anti-tumor necrosis factor alpha (TNF-a) agents including infliximab, adalimumab, certolizumab, and golimumab; anti-integrin agents including vedolizumab and natalizumab; and anti-interleukin (IL) 12-23 agents such as ustekinumab. Unfortunately, despite remarkable progress in the management of moderate-to-severe IBD patients, there are significant rates of primary non-response, loss of response, and adverse events, thereby necessitating additional treatment options. Additionally, the burden of intravenous administration or subcutaneous injection accompanied by associated high cost necessitate the development of alternative treatments. In recent years, remarkable research has focused on the development of oral small molecule agents Table 3. Unlike antibodies that can develop with biologic agents, oral small molecule formulations do not carry the same risk of immunogenicity. Their molecular characteristics and size allow for a more convenient oral administration and avoids the potential development of anti-drug antibodies. The purpose of this review article is to summarize available novel oral small molecule agents in treatment of patients with IBD. Two of the oral small molecule agents, tofacitinib and ozanimod were already approved by the FDA for patients with moderate-to-severe ulcerative colitis. This review will not include other novel and emerging therapeutic modalities such as microbiome targeted or stem cell therapies.
JAK Inhibitors
One of the new treatment strategies that has been developed is the targeting of the Janus kinase (JAK) family of tyrosine kinases [8]. The functions of this family of tyrosine kinases is broad, but evidence suggests that innate and adaptive immune responses require JAK-STAT signaling to mediate several pathways of cytokine function. These agents inhibit cytokines in the inflammatory cascade such as IL-9, IL-12, IL-23 and interferon-gamma. Several studies have supported this hypothesis by demonstrating significant upregulation of JAK transcripts in intestinal mucosa of patients with active ulcerative colitis [9]. These facts make targeting the JAK-STAT an appealing therapeutic modality in IBD. This has led to the development and regulatory approval by the United States Food and Drug Administration (FDA) of therapies targeting the JAK pathway for the treatment of IBD [10]. One of those therapies is a non-specific pan-JAK inhibitor tofacitinib, which was approved by the FDA in 2018 for the treatment of patients with moderateto- severe ulcerative colitis. The Octave trial which included the phase 3 clinical trial that led to the regulatory approval of tofacitinib for the treatment of ulcerative colitis included patients randomly assigned to 10 mg of tofacitinib twice daily or placebo for 8 weeks. Clinical remission (determined to be a Mayo Clinic score of less than 2 and a rectal bleeding score of 0) at 8 weeks occurred in 18.5% of patients assigned to tofacitinib versus 8.2% of patients assigned to placebo (P = 0.007) [11]. The Octave sustain maintenance study re-randomized week 8 responders to receive 10 mg or 5 mg of maintenance tofacitinib twice daily or placebo for 52 weeks. Remission at 52 weeks was significantly higher in patients treated with 5 mg (34.3%) and 10 mg (40.6%) of tofacitinib than with placebo (11.1%; p<0.001 for both comparisons with placebo). Notably, tofacitinib has a rapid onset of induction and has shown to be effective in refractory anti-TNF exposed ulcerative colitis patients compared to placebo [12]. Similar studies in patients with Crohn’s disease failed to achieve primary and secondary endpoints though there were modest improvements in inflammatory markers; this was probably due to the study design and unusually high placebo response rate seen in the study [13]. Clearly more research in the use of tofacitinib is needed to elucidate its efficacy in patients with Crohn’s disease. This data makes tofacitinib an attractive treatment option for patients with moderate-to-severe ulcerative colitis. However, tofacitinib can inhibit the immune system to a degree that increases the risk of herpes zoster, serious bacterial infections, tuberculosis, and upper respiratory tract infections [14]. The safety committee of the European Medicines Agency performed a review of tofacitinib due to the concern for an increased risk of developing pulmonary embolisms [15]. Subsequently, the FDA released warnings about the risk of blood clots leading to a boxed warning. All patients irrespective of their risk factors for developing thromboembolism should be monitored for signs and symptoms of pulmonary emboli. Sudden death in patients using high doses of tofacitinib was seen in patients primarily with rheumatoid arthritis and not with inflammatory bowel disease [16,17]. Another important concern related to the use of tofacitinib is the increased risk of lymphoma and nonmelanoma skin malignancies [18]. In a recent study, 1455 patients receiving tofacitinib at a dose of 5 mg twice daily and 1456 patients receiving tofacitinib at a dose of 10 mg twice daily were compared to 1451 patients receiving a TNF inhibitor. Over a 4 year follow up period, incidences of cancer and major cardiovascular events were higher in patients receiving the combined tofacitinib doses (4.2% and 3.4%, respectively) than with a TNF-alpha inhibitor (2.9% and 2.5%) [19]. The hazard ratios were 1.33 for major cardiovascular events and 1.48 for cancer (particularly non-melanoma skin cancer); the non-inferiority of tofacitinib was not demonstrated. Rarely, gastrointestinal perforations can occur during tofacitinib therapy with data demonstrating and incidence of 0.2% [20]. It is important to remember that patients should be advised to reduce their dose of tofacitinib in half when combining treatment with cytochrome P450 inhibitors such as fluconazole and ketoconazole.
Selective JAK inhibitors have also been recently studied for the treatment of patients with IBD, including Crohn’s disease. Filgotinib, is a selective JAK inhibitor that was approved by the FDA for the treatment of rheumatoid arthritis. Filgotinib selectively targets the JAK1 cytokine at a 30-fold selectivity over JAK2. JAK2 inhibition is thought to lead to higher rates of anemia and thrombocytopenia through the interfering of erythropoietin and thrombopoietin and granulocyte-macrophage colony-stimulating factor which would make selective JAK1 inhibition an attractive option [21,22]. The phase II Fitzroy study demonstrated early clinical benefit of filgotinib in patients with Crohn’s disease. Fitzroy included patients with a disease activity score (CDAI) of 220-450 and confirmed endoscopically active Crohn’s disease. A total of 174 patient with moderate-to-severe active Crohn’s disease were randomly assigned to receive 200 mg of filgotinib daily or placebo for 10 weeks. Clinical remission (indicated as a CDAI score of <150) at 10 weeks was achieved in 47% of patients treated with filgotinib and 23% of patients who were given placebo (P = 0.0077). Endoscopic improvement at 10 weeks was not significantly different [23]. The phase II study, Divergence 2, examined the effect of filgotinib in patients with perianal fistulizing Crohn’s disease. Patients with a documented history or perianal fistulizing Crohn’s disease with at least one to two external openings with drainage previously treated with immunomodulators or anti-TNFs were randomly assigned to receive filgotinib 200 mg, 100 mg or placebo once daily for 24 weeks. The primary endpoint was fistula response with a reduction of greater than 1 from baseline in the number of fistulas and no fluid collections seen on MRI at week 24. Unfortunately, the study was not well powered as there was low recruitment rates due to the COVID-19 pandemic leading to a total of 57 participants. Results did demonstrate a numerically higher proportion of patients in the filgotinib 200 mg group (47%) versus the placebo group (25%) who achieved the primary endpoint [24]. Further studies with a large patient population will be required to further elucidate the efficacy of filgotinib in patients with fistulizing Crohn’s disease.
The Selection trial included two induction studies, a maintenance study, and a long- term extension study examining the efficacy of filgotinib in the treatment of moderate-to-severe ulcerative colitis. Adults with moderate-to-severe ulcerative colitis were randomized to filgotinib 200 mg, 100 mg or placebo once daily for 11 weeks. Patients who responded to selected treatment at week 10 were re-randomized to continue filgotinib or placebo for an additional 47 weeks. Clinical remission was evaluated at week 10 and 58. Filgotinib demonstrated clinical remission rates significantly improved over placebo (47% vs 23%) at 10 weeks. Secondary endpoints such as endoscopic remission, mucosal healing, and deep remission did achieve numerical improvement but failed to achieve statistical significance. At week 58 remission was achieved at a rate of 58% in the filgotinib group compared to placebo at 29.5%. These findings suggest that filgotinib is efficacious at inducing and maintaining remission in patients with ulcerative colitis. Due to the efficacy demonstrated by filgotinib regulatory approval for use in moderate-to-severe ulcerative colitis as well as Crohn’s disease is expected soon. The common side effects reported in patients taking filgotinib are quite similar to tofacitinib including but not limited to serious infections, herpes zoster, venous thrombosis, pulmonary embolism and gastrointestinal perforations [25,26]. It is of note that filgotinib was rejected for approval by the FDA in the treatment of rheumatoid arthritis on concerns of toxicity and reduced sperm count [27,28]. Two ongoing trials (MANTA and MANTA-Ray) are pending and will provide additional safety data on the matter in patients with IBD.
Another highly selective JAK inhibitor that was approved by the FDA for use in patients with rheumatoid arthritis, psoriatic arthritis, and atopic dermatitis and also has been studied for its potential benefit in IBD patients is upadacitinib. This molecule is even more selective for JAK1 then filgotinib and has been investigated in the Celest phase 2 trial [29,30]. Patients with ulcerative colitis who had been previously exposed to anti-TNFs were evaluated after 16 weeks for primary endpoints of clinical remission, which included a patient reported outcome of stool frequency and abdominal pain score. In the induction phase of the study, although a numerical benefit in clinical remission could be observed in the group on twice daily 6 mg upadacitinib, it did not demonstrate a statistical response over placebo. The phase II study showed that the clinical remission and endoscopic improvement were achieved better than placebo as well as reduction in inflammatory markers. Phase III clinical trials of upadacitinib are ongoing and will hopefully shed more light on its efficacy and risk profile. Upadacitinib has similar adverse events as seen with tofacitinib including major adverse cardiovascular events and serious infections [31]. Due to the concerns of significant adverse events with tofacitinib, filgotinib, and upadacitinib, the development of a more gut selective pan-JAK inhibitor has been investigated. TD-1473 is a pan-JAK inhibitor that has demonstrated such a gut selective effect on mice with in-vitro studies [32]. A Phase 2b/3 set of clinical trials is currently ongoing to assess the efficacy and safety of induction and maintenance therapy with TD-1473 in subjects with moderate-to-severe active ulcerative colitis. Preliminary results were promising in endoscopic improvement along with reduction in fecal calprotectin and CRP levels with TD-1473 compared to placebo. If its further effectiveness can be demonstrated with this pending trial it has the potential to limit severe systemic side-effects caused by other non-GI selective JAK inhibitors. TYK2 is one of the JAK-STAT family proteins that is involved in intracellular cytokine signaling and inhibition of which blocks IL-12, IL-23 and IFN [33]. The oral TYK2/JAK1 inhibitor is well tolerated and more selective than other JAK inhibitors potentially limiting toxicity. Two oral TYK2/JAK1 inhibitors, deucravacitinib and brepocitinib, are currently recruiting in phase II clinical trials for the treatment of moderate-to-severe ulcerative colitis and also, Crohn’s disease.
Sphingosine-1-Phosphate Receptor Modulators
Sphingosine 1- phosphate (S1P) receptors are G protein coupled receptors (S1P1-S1P5) that regulate the response and function of various cellular and organ systems including cell migration, proliferation, immune response, and trafficking of T and B lymphocytes from lymphoid organs [34,35]. Their role in the ability of immune cells to migrate to inflamed tissues has made them a potential new target of inhibition for the management of IBD. Ozanimod is a new oral small molecule agent that binds with high affinity to several S1P receptor subtypes leading to internalization of the receptor in targeted lymphocytes and prevention of lymphocyte trafficking [36]. Ozanimod was approved for the treatment of the patients with relapsing multiple sclerosis in 2020 and then for patients with moderate-to-severe ulcerative colitis in 2021 by the FDA. Sandborn et al performed a phase III double blind and placebo-controlled trial of ozanimod as induction and maintenance therapy in patients with moderate-to-severe ulcerative colitis [37]. Patients were assigned to receive oral ozanimod 1 mg or placebo once daily and patients in a second cohort received open label ozanimod. They found that clinical remission was significantly higher in patients who received ozanimod than those who were on placebo (37% vs 18.5%, P<0.001). Clinical response was also significantly higher in the ozanimod group (60% vs 41%, P<0.001). The investigators found that rates of serious infection were equal in both groups. A few patients on ozanimod had higher rates of elevated liver transaminases. Adverse events have been reported with ozanimod treatment including herpes zoster, bradycardia, and elevation of liver enzymes, atrioventricular conduction delays and macula edema. Ozanimod is also being studied for the treatment of Crohn’s disease. In the phase II Stepstone study involving 69 patients with Crohn’s disease, 39.1% of patients who received ozinamod had clinical remission at week 12. There was no incidence of bradycardia or arrhythmias in these patients [38]. Phase III, placebo-controlled induction and maintenance studies of ozanimod are currently recruiting for moderate-to-severe Crohn’s disease. Etrasimod is another oral S1P receptor subtype 1 modulator which has demonstrated potential efficacy in the treatment of patients with IBD. In the phase II Elevate trial involving 156 patients with ulcerative colitis, those patients receiving a 2 mg dose of etrasimod demonstrated endoscopic improvement over placebo (41.8% vs 17.8%, P=0.003). Also, compared to placebo, the etrasimod 2 mg group had a higher rates histologic remission (19.5% vs 6.1%; p=0.03). Etrasimod adverse events were reported as minimal with a small group of patients developing a transient, asymptomatic, low grade atrioventricular block that resolved spontaneously. Amiselimod is an oral S1P receptor modulator with higher selectivity for S1PR1 than other S1P receptor modulators [39]. A phase II trial with this agent is pending in patients with active Crohn’s disease.
Anti-Adhesion Molecules
Migration of proinflammatory T cells into the gut facilitates inflammation that is characteristic of IBD [40]. Anti-adhesion agents that block lymphocyte trafficking to the gut are being investigated in patients with IBD. A variety of oral small molecules including alfa-4 integrin antagonists have been studied. AJM300 is an oral small molecule agent that targets alfa-4 integrin. A phase II study in 102 patients with moderate-to-severe ulcerative colitis showed higher rates of clinical response (62.7% vs 25.5%, p=0.0002), clinical remission (23.5% vs 3.9%, p= 0.0099) and mucosal healing (58.8% vs 29.4%) [41]. No major adverse events were reported. A phase III trial is ongoing with AJM300 in patients with ulcerative colitis. There is extensive research of other anti-adhesion agents in the treatment of inflammatory bowel disease.
Phosphodiesterase 4 Inhibitors
Phosphodiesterase 4 (PDE4) is part of a group of enzymes that catalyze the breakdown of cyclic adenosine monophosphate (cAMP). In inflammatory cells, PDE4 is the dominant enzyme responsible for this reaction and the resulting decrease in cAMP levels leads to an increase expression of proinflammatory factors. Thus, it has been postulated that if PDE4 were inhibited the resulting increase in cAMP levels would lead to the decreased expression of a number of proinflammatory factors including TNF-alfa, IL- 17, IL-23, and up-regulates anti-inflammatory IL-10 [42]. This makes PDE4 a potential target for the treatment of inflammatory disorders. Apremilast is an oral small molecule PDE4 inhibitor which has been approved by the FDA for the treatment of adults with psoriatic arthritis, plaque psoriasis, and Behcet’s disease. A recent phase II clinical trial demonstrated the clinical effectiveness of apremilast in the treatment of moderate-to-severe ulcerative colitis. The investigators performed a double-blind, placebocontrolled trial in patients with active ulcerative colitis who were either biologic naïve or had failed conventional therapies. Patients were randomly assigned to apremilast 30 mg twice daily, 40 mg twice daily, or placebo for 12 weeks. After which patients were then randomly assigned to receive apremilast 30 mg or 40 mg twice daily for an additional 40 weeks. Endoscopies were performed and biopsies were obtained at the initial encounter, week 12, and week 52 after initiation of the study. The primary endpoint for the study was clinical remission at week 12 (a Mayo score of 2 or less). The investigators found that clinical remission was achieved in the 30 mg apremilast group at a rate of 31.6% versus 12.1% of patients in the placebo group (P = 0.01) [43]. Both apremilast groups (the 30 mg and 40 mg groups) had similar improvement from baseline in Mayo score components. At week 52 clinical remission was achieved by 40.4% of patients. Endoscopic healing was achieved in 41.4% of patients in placebo compared to 73.7% in the 30 mg group (p< 0.0001). Moreover, both the 30 mg and 40 mg apremilast groups showed greater reduction in serum C-reactive protein and fecal calprotectin compared to placebo. In terms of safety, headache and nausea were found to be the most common side effect. One patient had an episode of acute pancreatitis but this was no attributed to the study drug. Currently, a phase III trial has not been registered for patients of ulcerative colitis or Crohn’s disease.
Anti-Tumor Necrosis Factor Agents
Anti-TNF agents were the first class of biologic medications approved for the treatment of patients with inflammatory bowel disease [44]. Limitations of this class of medications includes the intravenous or subcutaneous administration, infusion reactions, systemic side effects related to immunosuppression, and high cost [45]. An oral agent with a mechanism of action restricted to the gastrointestinal tract would be helpful to overcome some of these challenges of parenterally administered anti-TNF agents. AVX- 470 is an oral polyclonal immunoglobulin that inhibits TNF-alpha locally in the gastrointestinal tract, minimizing systemic exposure [46]. In a double blind, placebo-controlled trial, 37 patients with active ulcerative colitis received AVX-470 (0.2, 1.6, or 3.5 grams per day) or placebo for 4 weeks. Endoscopic activity was assessed pre and post treatment exposure.46 At all AVX-470 doses, 25.9% of patients achieved clinical response compared with 11.1% of those in the placebo group. Both groups were found to have similar adverse event rates without significant infectious reported.46 Further clinical trials evaluating the efficacy of AVX-470 are ongoing [47,48]. OPRX-106 is another oral anti-TNF agent which is currently undergoing evaluation for its efficacy in the treatment of inflammatory bowel disease [49]. In a phase II randomized open label clinical trial, 25 patients with ulcerative colitis who were administered OPRX-106 demonstrated clinical remission and mucosal healing with no major adverse events including immunogenicity. Initial studies with oral anti-TNF agents have shown promising results with the potential for enhanced safety and decreased immunogenicity. However, larger trials are needed to evaluate efficacy, safety and cost effectiveness.
Conclusion
Despite tremendous advancements in the field of treatments for IBD, there are significant rates of primary non-response, loss of response, adverse events and high cost thereby necessitating additional treatment options. Fortunately, the rapidly growing number of oral small molecule targeted therapies offers ease of administration with durable effectiveness, and an improved safety profile compared to the currently approved therapeutic agents.
For more information about Current Trends in Gastroenterology and Hepatology please click on https://lupinepublishers.com/gastroenterology-hepatology-journal/
For more Lupine Publishers please click on below link
https://lupinepublishers.com/
#lupine publishers#lupinepublishersgroup#lupine publishers llc#ctgh#gastroenterology#hepatology#current trends in gastroenterology and hepatology#Cirrhosis#liver abscess#inflammatory bowel disease#lupine#open access journals#liver#endoscopy#lupine publishers group
2 notes
·
View notes
Text
Prevention and Correction of Immunodeficiency States of Animals, Chemical Etiology
Introduction
In recent years, in farm and private livestock farms in Uzbekistan there has been a decrease in the resistance of animals and, especially, young animals to various bacterial and viral infections. Often there is a decrease and a complete lack of protective action of known vaccines and serums, which causes serious economic damage to livestock. One of the leading factors of this pathology is the unfavorable ecological situation which has developed in many regions of the Republic owing to various anthropogenic influences, including: application of pesticides and other toxic xenobiotics and also emissions of industrial productions.
Read more about this article: https://lupinepublishers.com/dairy-veterinary-science-journal/fulltext/prevention-and-correction-of-immunodeficiency-states-of-animals-chemical-etiology.ID.000133.php
Read more Lupine Publishers Google Scholar Articles : https://scholar.google.com/citations?view_op=view_citation&hl=en&user=G7luzkMAAAAJ&citation_for_view=G7luzkMAAAAJ:bFI3QPDXJZMC
#LupinePublishersGroup#lupine publishers llc#lupine#Concepts of Dairy and Veterinary Scineces#animal health#poultry#wildlife diseases#dairy#cheese technology#lactation#milk processing
0 notes
Text
Lupine Publishers | Acute Upper Gastrointestinal Bleeding (UGIB) In A Resource Limited Setting Highly Endemic for Viral Hepatitis B: Which Etiologies for Which Real Clinical Practices?

Abstract
Aim : To determine the aetiologies of acute upper gastrointestinal bleeding (UGIB) in a setting highly endemic for hepatitis B and to describe actual clinical practices in a resource-limited setting.
Patients and methods: This study was conducted in two parts. The first part was retrospective from January 1st 2010, to December 31st 2019 on the epidemiological profile of UGIB and the second was a prospective study from December 1st 2017 to May 31st 2018 to evaluate, in a blinded experiment, the actual clinical practices in front of an acute UGIB at the emergency units in Yaounde (Cameroon), and included: recognizing UGIB, assessing for severity, taking emergency measures and prescribing emergency Eosogastroduodenal endoscopy (EGDE).
Results : During the retrospective period, 506 patients (prevalence of acute UGIB in the services 5.6%) were included of which 71.3% were men (sex ratio 2.5). The mean age was 49.9 +/- 8 years. Haematemesis was inaugural in 350 patients (69.1%), nonsteroidal anti-inflammatory drugs were the main risk factor in 297 (43.6%), in 78 (15.4%), this was a second episode. Clinical parameters showed initial instability in 435 patients (85.9%) and haemoglobin (Hb) was <7g/dl in 359 (83.4%). EGDE was performed in 203 patients (40.2%), the main causes of UGIB were lesions of portal hypertension in 111 (44.7%), followed by peptic ulcers in 108 (43.5%). Treatment was mainly medical. However, 94 patients (84.7%) with portal hypertension lesions received endoscopic treatment, mainly by injection of sclerosing agent (69.1%), as well as 13 (1.2%) with peptic ulcers, mainly by isolated injection of dilute adrenaline (1: 10,000) in 11 (84.6%). A total of 75 patients (14.8%) died. The second part concerned 74 patients admitted for acute UGIB at the emergency services of five hospitals in Yaounde. To recognize UGIB, a digital rectal examination was done in 43 patients (58.1%), no patient received a nasogastric tube. For assessment of severity, blood pressure was taken in 73 patients (98.6%), pulse rate in 61 (82.4%), respiratory rate in 17 (23%), saturation in 17 (23%), no patient had prognostic scores in their record. For resuscitation measures, 10 patients (13.5%) received a double peripheral venous line, 20 (27%) were filled with crystalloids, restrictive blood transfusion (Hb < 7 g /dl) was carried out in 24 out of 27 patients (88.9%), 9 (12.2%) received nasal oxygen therapy. EGDE was carried out in 43 patients (60.6%), all beyond 24 hours and none had a prognostic score (Forrest or Rockall).
Conclusion: Rupture of oesogastric varices plays a significant role in the occurrence of UGIB in areas with high hepatitis B endemicity, with exceptional severity and high mortality among young people. The lack of qualified human resources and insufficient technical facilities constitute a serious problem. Locally applicable protocols are needed. In the long term, eliminating viral hepatitis B and C should reduce the prevalence of UGIB
Keywords:Gastrointestinal Bleeding; Hepatitis B Virus; Portal Hypertension; Limited Resources; Endoscopy; Clinical Practice.
Background
Acute gastrointestinal bleeding is one of the major medical and surgical emergencies whose severity should never be underestimated [1]. In approximately 80% of cases, acute gastrointestinal bleeding is of high origin, i.e. the aetiology of the bleeding is located upstream of the duodenojejunal angle or Treitz angle [2]. Acute upper gastrointestinal bleeding (UGIB) is the most frequent emergency in hepato-gastroenterology and remains a major cause of mortality, despite improvements in technical facilities, the mortality rate remains stable at about 10-15% [1-4]. The UGIB is exteriorized in 66% of cases in the form of hematemesis and the aetiologies involved are varied [2,5-7]. In the West, the proportion of peptic ulcers is significantly high. Indeed, the most common causes of acute UGIB are non-varicose (80-90%) and include gastric and duodenal ulcers in 20-50% [2,3,5-7]. Contrarily, in sub-Saharan Africa, the proportion of portal hypertension lesions is significant [8,9]. The impact of chronic hepatitis B virus (HBV) infection in this highly endemic area is significant. In highly endemic countries, ≥8% HBsAg positivity, the HBV-related disease burden is due to liver cancer and cirrhosis in adulthood, responsible for portal hypertension. The majority (80%) of the world population lives in high- or intermediate-endemic areas [10]. The way to handle acute UGIB is well codified. Gastrointestinal bleeding must be recognised, its severity assessed, and blood loss compensated. Finally, the cause of the bleeding must be found and treated [1,2,7,11]. The diagnostic approach, non-specific measures to prevent or treat haemorrhagic shock and specific haemostasis measures according to the aetiology of UGIB are often not all implemented in resources limited countries and this has an impact on evolution and prognosis. Based on data collected in the files of patients admitted in emergency and those obtained following the daily clinical practice of emergency staff, the study aimed to highlight the epidemiology and actual management of acute UGIB in our context dominated by HBV infection and limited resources.
Methods
A retrospective collection of data contained in the files of patients admitted for acute UGIB at the Yaounde Central Hospital (Cameroon) between January 1st2010 and December 31st2019, was carried out. Located at the heart of the city of Yaounde, the Yaounde Central Hospital (YCH) was created in 1930. It is the largest public referral hospital in Cameroon with capacity of …. Beds that also acts as a teaching hospital. It houses several services including the Hepato-gastroenterology service with a capacity of 34 beds, three university specialists, four general practitioners and several permanent workers and residents. This service has an upper and lower gastrointestinal endoscopy room and endoscopy equipment. The variables recorded included: demographics (age, sex); clinical and biological characteristics (onset of UGIB, history of bleeding, physical parameters of bleeding severity, and haemoglobin levels on admission); Esogastroduodenal endoscopy (EGDE) findings; specific management of the cause of the bleeding and outcomes (Table1).
The second component, cross-sectional and observational blinded experiments, conducted from December 1st 2017 to May 31st 2018, assessed the diagnostic approach and actual management of patients admitted for acute UGIB in five hospitals of different categories (1st to 3rd) of the Cameroonian health pyramid, in the city of Yaounde. Twenty (20) doctors and 39 nurses in the emergency service who managed 74 patients admitted for acute UGIB were followed. The elements to take care of acute UGIB included recognition of acute UGIB by placing a nasogastric tube or performing a digital rectal exam; assessment of severity by clinical criteria (taking blood pressure (BP), pulse rate (PR), respiratory rate (RR) and room oxygen saturation (SPO2), Glasgow- Blatchford score; fluid resuscitation and transfusions (double venous line, crystalloids filling, proton pump inhibitors (PPI) or vasoactive treatment, oxygenation, restrictive blood transfusion (haemoglobin (Hb) <7 g/dl), hourly monitoring of vital signs and neurological status) and finally, the performance of EGDE and the Rockall and Forrest scores.
Statistical Analysis
Data was analysed using Statistical Package for Social Sciences (SSPS Inc, Chicago, Illinois, USA) version 23.0. Means ± standard deviation was used for quantitative variables; Categorical data was expressed as numbers and proportions. A p value of less than 0.05 was considered statistically significant.
Results
During the retrospective period, 506 patients (prevalence of acute UGIB in the services 5.6%) were included of which 361 men (71.3% and 145 women (28.7 %), given a 2.5 sex ratio. The mean age was 49.9+/- 8 years (maximum 14-96 years) and the peak of bleeding was in the 55-65-year age group. Haematemesis was the initial complaint in 350 patients (69.1%), non-steroidal antiinflammatory drugs (NSAIDs) constituted the most important risk factor in 297 patients (43.6%), in 78 (15.4%). This was a second episode. On admission, clinical parameters relevant to severity were systolic BP <100 mmHg in 122 patients (39.8%); HR >100 beats/ minutes in 435 (85.9%) and RR >20 cycles/minute in 435 (85.9%). Hb was <7g/dl in 359 patients (83.4%). EGDE was performed in 203 patients (40.2%), the major causes of bleeding were: portal hypertension lesions in 111 patients (44.7%) followed by peptic ulcers in 108 (43.5%). Treatment was mainly medical. However, 94 patients (84.7%) with portal hypertension lesions received endoscopic treatment, mainly by injection of sclerosing agent (69.1%), as well as 13 patients (1.2%) with peptic ulcers, mainly isolated injection of dilute adrenaline (1: 10,000) in 11 (84.6%). A total of 75 patients (14.8%) died during hospitalization (Table 2).
The second part concerned the assessment of care offered to 74 patients admitted for acute UGIB (mean age 55 years; sex ratio 2.1). For the recognition of bleeding, digital rectal examination was performed in 43 patients (58.1%) and no patient received nasogastric tube. Regarding the assessment of severity by clinical criteria, BP was taken in 73 patients (98.6%), HR in 61 (82.4%), and RR in 17 (23%), no patient had prognostic scores in the record, including the Glasgow-Blatchford score. Only 17 patients (23%) had SPO2 measurements. Regarding intensive care measures, only 10 patients (13.5%) received a double peripheral venous line, the majority of which was a small-bore venous line. Twenty patients (27%) were filled with crystalloids; restrictive blood transfusion was performed in 24 out of 27 patients (88.9%) with Hb < 7 g / dl. Only 9 patients (12.2%) received nasal oxygen therapy. EGDE was performed in 43 patients (60.6%), all beyond 24 hours after admission and none had a prognostic score after endoscopy (Forrest or Rockall).
Discussion
The study showed that acute UGIB is an emergency with exceptional severity in our environment, as mortality is very high at around 15%. In this study, it was found that acute UGIB affected two and a half times more men than women with a mean age of about 50 years. This is the case in studies conducted in Mali (sex ratio 2.78; mean age 47.45 years), and in Côte d’Ivoire (sex ratio 3.38; mean age 47 years) [8,12]. Indeed, in the sub-Saharan African region, the occurrence of acute UGIB often involves relatively young patients. This can be explained by the fact that the causes of bleeding are often dominated by portal hypertension lesions, especially in young patients, as reported in Mali in a rural area [8]. As opposed to sub-Saharan Africa, in the West, the age of onset of acute UGIB is higher than 70 years due to the use of NSAIDs in the elderly population. Of chronic NSAID users, 25% develop an ulcer, of which 2-4% are complicated by bleeding [2,7,13,14]. The male predominance is universal, and reverses in the West after the age of 80 years due to the higher life expectancy in the female population [2,4,6-9, 11,13,14].
As in several studies reported in literature, hematemesis was the most common initial clinical presentation [2,6,7,15,16]. This initial clinical presentation can be explained by the different lesions found on endoscopy. In fact, portal hypertension lesions, led by oesophageal varices, were the most frequent, alongside peptic ulcers. The frequency of the various aetiologies varies from one region to another [5,6,8]. Thus, in the sub-Saharan African region, several studies report very high frequencies of portal hypertension lesions. This is the case of the study by Diarra et al. in Mali in 2007 [8]. The authors reported a frequency of 55.2% in favour of ruptured oesophageal varices, far ahead of peptic ulcers which represented 16%. The frequency of portal hypertension lesions is also high in Burundi (28.2%) [16] and Gabon (29.5%) [17]. These various countries have liver diseases related to chronic HBV infection in common. Indeed, sub-Saharan African countries are located in a zone of high endemicity according to the World Health Organisation (WHO), i.e. the prevalence of hepatitis B is 8-20% of the general population [10]. Cirrhosis, which causes portal hypertension, is often the result of chronic HBV infection acquired at birth or in early childhood [18]. The annual incidence of varicose veins is approximately 5% [19]. UGIB from ruptured esophageal varices accounts for 70% of gastrointestinal bleeding in cirrhosis, with an estimated overall 2-year bleeding risk of 20% [19]. The aetiological approach to acute UGIB in high- and intermediate-endemic areas where the majority (80%) of the world population lives should therefore consider this high frequency of portal hypertension lesions and bleeding complications.
Regarding the severity of the bleeding, more than 85% of patients were initially unstable with clinical and laboratory signs of severity, despite the absence of Glasgow-Blatchford and Rockall scores in their records. This initial haemodynamic instability can be explained, on the one hand, by the causes of bleeding, in particular the rupture of oesogastric varices, which are exceptionally serious, but also, on the other hand, by the late arrival in hospital structures due to distance, cultural considerations or difficulties of mobility in our country.
Treatment was essentially medical. PPI treatment was most often initiated on admission, even if this treatment did not always fully comply with current recommendations in Europe and Asia [2,7,20,21]. Contrarily, in cases of suspected acute UGIB related to rupture oesogastric varices, vasoactive therapy to reduce portal blood flow was never initiated on admission, in line with international recommendations, including those adapted by the European Society of Gastrointestinal Endoscopy to be applicable to resource-limited settings, including some African countries [2,7,22-24]. Patients with bleeding peptic ulcers have rarely benefited from endoscopic haemostasis, unlike those with portal hypertension lesions. Late arrival at hospital would explain why in sub-Saharan Africa Forrest scores IIc and III, i.e. pigmented stain or clean base of the ulcer, are most frequently found [25]. For the Forrest classification guiding the choice of endoscopic treatment modality for ulcers, there is no endoscopic treatment for these scores [2,3,7,26]. The practice of injecting adrenaline alone instead of combined adrenaline and bipolar coagulation or endoclips was inappropriate. This could be explained by factors such as excessive procedure costs, insufficient training of practitioners and limited logistic equipment.
The mortality rate of upper GI bleeding varies between 2-10%, and is increased by the presence of associated diseases, but also rupture of oesogastric varices with a specific mortality rate of 15- 25% [2,27,28]. Because of the predominance of portal hypertension lesions in our series and the liver failure accompanying cirrhosis, mortality was high compared to other countries in the sub-region, 5% in Togo [15], 3.8% in Gabon [17] and 9.4% in Côte d’Ivoire [12]. On the other hand, it was close to the mortality found in Burundi, 22.9% [16]. The lack of primary prevention of varicose vein rupture could also explain this high mortality. However, this factor has not been studied (Table 3, 4).
The quality of care is key to improving prognosis [2,3,7, 8,29- 31]. The actual care in the studied setting was assessed. The priority in the care of acute UGIB is to ensure haemodynamic stability with crystalloid or balanced infusions and possible transfusions [2- 5,29-31]. For this purpose, bleeding should be recognised either by nasogastric tube placement or by digital rectal examination. Also, the severity should be assessed by prognostic scores, in particular the Glasgow-Blatchford score (GBS), based on clinical and biological criteria, validated to identify low-risk patients with a sensitivity of 99% and a specificity of 32% [2,30,32]. From these recommendations, it was observed that the recognition of bleeding and the assessment of its severity were insufficient. Recording clinical parameters was neglected. Neither digital rectal examination nor nasogastric tube placement to aid diagnosis was rarely done if the patient was not present at the time of the blood loss. Oxygen therapy, even for initially unstable severe cases or cases with comorbidities, was often not effective. This may be due to the lack of oxygen in some hospitals or because of outdated or non-existent anaesthesia and intensive care equipment. The current guidelines, recommending a transfusion threshold of 7 g/dl [2,30,33,34], were met in about 90% of patients in this case. It should be noted that the Yaounde Central Hospital, which had the largest number of patients, has a certification for its blood bank. Treatment with venous PPI was started early in the majority of cases regardless of the suspected aetiology. Given the significant proportion of portal hypertension lesions, vasoactive drugs should be integrated into local protocols for the care of acute UGIB, since this is not currently the case. Helicobacter pylori testing and eradication is also not integrated into the care of acute UGIB in the setting. And yet, this is a validated approach [35]. Helicobacter pylori infection plays a major role in the development of ulcers in the studied environment, affecting approximately 70-80% of the population [36].
EGDE with or without endoscopic therapeutic procedures is an integral part of the care of UGIB and has been shown to improve patient outcomes in terms of morbidity and mortality [2,7,26,31]. However, the ideal time for its performance is unclear. Recommendations agree that it should be performed within 24 hours of admission [2,3,7,37]. Early endoscopy within 12 hours would not influence clinical outcomes, mortality, recurrence of bleeding or the need for surgery [20,31]. In our resource-limited environment, not only is there a shortage of qualified human resources, but there is also inadequate technical equipment. While it is accepted that an EGDE should be performed in every patient with acute UGIB, the rate of completion was only 40-60.6% in both study arms. This procedure is relatively expensive in relation to people’s income. Endoscopy was most often performed beyond 24 hours after admission. Thus, therapeutic endoscopic procedures were rare. If performed early, it seems to have an influence on hospital resources and costs, by identifying low-risk patients and allowing them to return home quickly [31,37]. This would be appropriate in our resource-limited environment.
Conclusion
Contrary to Western countries, ruptured oesogastric varices play an important role in the occurrence of gastrointestinal bleeding in areas with high hepatitis B endemicity. UGIB is exceptionally severe in these areas, as it has a high mortality. The lack of qualified human resources and insufficient technical facilities constitute a serious problem. For this reason, the improvement of clinical practice in relation to acute UIGB should consider the significance of portal hypertension lesions, on the one hand, and the limitation of resources on the other. Therefore, locally applicable protocols need to be devised. In the long term, the elimination of viral hepatitis B and C should considerably reduce the prevalence of UGIB. A multicentre study is therefore expected to establish protocols adapted to our health and limited resource settings.
What Is Known
a) 80% of gastrointestinal bleeding are upper. The most common causes of acute UGIB are non-variceal (80-90%) and include gastric and duodenal ulcers in 20-50%.
b) The age of onset of UGIB is around 70 years.
c) UGIB remains an important cause of morbidity and mortality.
The mortality rate has remained stable at around 10-15%.
d) The improvement of the prognosis depends on the care quality and treatment of acute UGIB is well codified.
e) The assessment of the severity of UGIB is based on prognostic scores, in particular the Glasgow-Blatchford score (GBS) which is based on clinical and biological criteria, validated to identify low-risk patients with a sensitivity of 99% and a specificity of 32%.
f) If acute UGIB is suspected in relation to rupture oesogastric varices, vasoactive therapy to reduce portal blood flow should be given as early as possible. In cases of suspected ulcerrelated UGIB, high-dose PPI therapy should be started early.
g) The priority in the care of acute UGIB is to ensure haemodynamic stability with crystalloid or balanced infusions and possible transfusions. Current guidelines recommend a transfusion threshold of 7 g/dl.
h) Helicobacter pylori testing and eradication is incorporated into the care of acute HDH.
i) It is accepted that an EGDE should be performed in all patients with acute UGIB. There is consensus that endoscopy should be performed within 24 hours of admission (12 hours in the case of portal hypertension related UGIB).
j) The Forrest classification guides the choice of endoscopic treatment modality for bleeding ulcers.
k) Haemostatic endoscopy is the first-line treatment for bleeding ulcers.
Relevance of the study
a) The causes of acute UGIB in areas of high hepatitis B endemicity are dominated by variceal bleeding in young patients.
b) The age of onset of UGIB is around 50 years.
c) The mortality rate is very high, around 15%.
d) The actual clinical practice is based on a non-codified care.
e) The prognostic scores of UGIB, notably those of Glasgow- Blatchford (GBS), Forrest and Rockall, are rarely used.
f) In case of suspected acute UGIB related to rupture oesogastric varices, vasoactive treatment is not often prescribed.
g) Not all emergency intensive care measures are followed, including oxygen therapy and monitoring.
h) Helicobacter pylori testing and eradication is not included in the care of acute UIGB.
i) The rate of completion of EGD is very low (40-61%) and it is done beyond the required 24 hours.
j) Haemostatic endoscopy is not the first-line treatment for bleeding ulcers, only in 1.2%.
Abbreviations and acronyms:
Upper gastrointestinal bleeding (UGIB); hepatitis B virus (HBV); HBV surface antigen (HBsAg); blood pressure (BP); pulse rate (PR), respiratory rate (RR); room oxygen saturation (SPO2), oesogastroduodenal endoscopy (EGDE); haemoglobin (Hb); proton pump inhibitors (PPIs); University of the Mountains (UdM); World Health Organisation (WHO); Institutional Ethics Committee of the University of the Mountains (CIE-UdM).
Declarations
a) Ethical considerations
We obtained ethical clearance from the Institutional Ethics Committee of the University of the Mountains (CIE-UdM) under the number No. 2018/149/UdM/PR/CIE of 19 March 2018.
b) Consent to publish
All authors gave their approval for publication.
c) Availability of data and materials
The datasets used during the current study are available from the corresponding author on reasonable request.
d) Competing interests
The authors declare no conflict of interest for this study.
e) Funding
The authors did not receive any fund for this study.
For More Lupine Publishers Open Access Journals Please visit our Website:
https://lupinepublishers.com/index.php
For more Current Trends in Gastroenterology and Hepatology articles please click here:
https://lupinepublishers.com/gastroenterology-hepatology-journal/
#lupine publishers#lupinejournals#gastroenteritis#hepatology#gastroenterology#lupinepublishersgroup#hepatitis#pathology
0 notes
Text
Research Trends in Water Management by Using Environmental Parameters Derived from Remote Sensing

Abstract
Water management is one of the most important strategies for sustainability. In many regions, this management is not easy and remote sensing can be useful to have data about the water status, especially from environmental derived indices associated with satellite data. It is important to know the research trends based on water management and remote sensing. Policy decision making in water management could be assisted and improved considering this tool. The aim of this work is to explore remote sensing articles that use environmental indicators in the last twenty years for the study of water resources by using a bibliometric analysis.
Read more about this article: https://lupinepublishers.com/biosensors-renewable-sources/fulltext/research-trends-in-water-management-by-using-environmental-parameters.ID.000103.php
Read more Lupine Publishers Google Scholar Articles:https://scholar.google.com/citations?view_op=view_citation&hl=en&user=5ql0QHJV55QC&citation_for_view=5ql0QHJV55QC:9ZlFYXVOiuMC
#LupinePublishers#LupinePublishersGroup#JournalofBiosensorsandRenewableSources#Biosensors#RenewableSources#SolarEnergy#NuclearEnenrgy#SustainableEnergy#GlobalChanges#Atmosphere
0 notes
Text
Lupine Publishers | Disability in the Margin of Loneliness Research and Policy
For more Lupine Publishers Open Access Journals Please visit our website: https://lupinepublishersgroup.com/https://lupinepublishers.com/psychology-behavioral-science-journal/pdf/SJPBS.MS.ID.000139.pdfhttps://lupinepublishers.com/psychology-behavioral-science-journal/fulltext/disability-in-the-margin-of-loneliness-research-and-policy.ID.000139.php

Lupine Publishers | Scholarly Journal Of Psychology And Behavioral Sciences
Abstract
Loneliness is a key deficiency in well-being and health for the people of our time and, as a result, a major social policy issue. In Finland, the link between loneliness, poor health, ability to work and recovery from different lifestyles has been noticed in surveys of both population levels and individual groups, such as mental health rehabilitators, homeless people, and bread-line customers. However, the loneliness of people with disabilities has not been studied in Finnish society. The aim of the UN Convention on the Rights of Persons with Disabilities is to include people with disabilities and other marginalized groups of disability in national health, lifestyle and similar research. The samples selected for research are usually removed, for example, by persons in institutions or service homes. The living conditions, quality of life and many other issues of the various groups of injuries have been studied primarily - and almost exclusively - within these groups and even using ‘disability-specific’ indicators, making comparison with the rest of the population impossible. It is also worrying that people with disabilities do not have the opportunity to influence their position in the current change in the service structure, including housing and everyday life. For example, residents who move from institutions have not been listened to in the abolition of institutional care. It can be rightly asked whether people with disabilities will be thrown away and lobbied when major structural reforms are underway.
Introduction
Disability information and practical solutions based on it for the everyday life of people with disabilities are deficient and there is a risk of marginalization and alienation of people with disabilities. At worst, it is possible to talk about a cycle of negativity, where abandonment, marginalization and alienation can be related to psychoactive substance use, crimes or suicide. The fight against loneliness is the prevention of such a thread. But how and why should we study the loneliness of disabled people? Research on the subject is scattered and scarce. Material focused exclusively on loneliness has not been collected by people with disabilities. Existing studies have focused on materials where loneliness has been touched in one way or another. When studying the loneliness of people with disabilities, it is worthwhile to consider at least the following: disability itself does not tell or explain anything, and disabled people are either a homogeneous group. In the 2013 Regional Health and Welfare Questionnaire (ATH), the question of loneliness has been asked by “Do you feel lonely?”. The answers have been “Never”, “Very rarely”, “Sometimes”, “Quite often” or “Continuously”. A large fifth (22%) of the needs of disabled people (N = 1044) felt quite often or constantly lonely when about one in ten (9%) felt alone as the lonely ones [1]. In a survey conducted by [2], 39% of people with disabilities reported being lonely.
Conclusion
The knowledge base on the loneliness of people with disabilities is very fragmented, but on the basis of individual results, people with disabilities are more lonely than other people. Written material gathered in 2003 explains the factors behind the loneliness of disabled people. In the light of the material, the loneliness of people with disabilities appears to be experiences of the other and the outside: a much deeper experience than just a lack of people. Rather, it is represented as a lack of relevance [3,4]. As a societal issue about the loneliness of people with disabilities, not only factors related to the individual’s social standing, but also the habitat factors that bring about and maintain the loneliness experienced by disabled people, but also can contribute to inclusion and lasting contact with other people can be presented. Politically, in particular, the body issues and structures and values of the society determine how people with disabilities can participate in various activities such as independent living, work and social relationships; to determine her/his own life; make free choices according to one’s wishes and abilities; and live in an accessible environment, if necessary with the help of special services. These segments of social policy have also been highlighted as key areas in the Finnish Disability Policy Programmed. Such policy papers do not in themselves oblige or act as a clear justification for disability policy or individual empowerment but reveal that the fight against loneliness seems to have a deep gap between ideologies and practices that should not be ignored.
https://lupinepublishers.com/psychology-behavioral-science-journal/fulltext/disability-in-the-margin-of-loneliness-research-and-policy.ID.000139.php
https://lupinepublishers.com/psychology-behavioral-science-journal/pdf/SJPBS.MS.ID.000139.pdf
For more Lupine Publishers Open Access Journals Please visit our website: https://lupinepublishersgroup.com/
For more Psychology And Behavioral Sciences Please Click
Here: https://lupinepublishers.com/psychology-behavioral-science-journal/
To Know more Open Access Publishers Click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
4 notes
·
View notes
Text
Lupine Publishers| Properties of Mitochondrial-Derived Peptides (Mdps), Type 2 Diabetes, and Relationship with Oxidative Stress
Lupine Publishers| Journal of Diabetes and Obesity
Abstract
Objective: In addition to its role in energy production and metabolism, mitochondria play a major role in apoptosis, oxidative stress, and calcium homeostasis. This review highlights the intricate role of mitochondria derived peptides (MPs), oxidative stress, and age-related disease such as diabetes.
Key Findings: The mitochondria produce MDPs: specific peptides that mediate transcriptional stress response by its translocation into the nucleus and interaction with DNA. MDPs are regulators of metabolism with cytoprotective effects through anti-oxidative stress, anti-inflammatory responses and anti-apoptosis. This class of peptides comprises: humanin (HN), MOTS-c, Small HN-like peptides. HN inhibits mitochondrial complex 1 activity and limits oxidative stress level in the cell. HN has been shown to prevent apoptosis by decreasing the reactive oxygen species production. Mitochondrial dysfunction and oxidative stress are implicated in the pathogenesis of diabetes. Data suggested that MDPs had a role in improving type 2 diabetes (T2D).
Summary: The goal of this review is to discuss the newly emerging functions of MDPs and their biological role in ageing and age-related diseases such as T2D.
Keywords:Mitochondrial-Derived-Peptides; Humanin; Oxidative Stress; Diabetes
Introduction
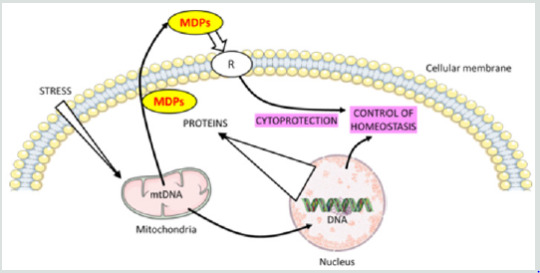
Mitochondria play a critical role in maintaining cellular function by ATP production. In addition to its role in energy production and metabolism, mitochondria play a major role in apoptosis, oxidative stress, and calcium homeostasis. A mitochondrial stress signal, or a ‘mitokine’, could confer protection and promote survival, while priming the cell’s readiness for subsequent insults with increasing severity. The term ‘mitohormesis’ for such a phenomenon has been created [1]. The mitochondrial unfolded protein response (UPRmt) is a central part of the “mitohormetic” response. The UPRmt may be an alternative way in relationship with mitochondria signal in the cell. The mitochondria produce some specific peptides that mediate transcriptional stress response by the translocation into the nucleus and interaction with DNA. Mitochondrial derived peptides (MDPs) are regulators of metabolism and various studies have shown that MDPs exerted cytoprotective effects through anti-oxidative stress, anti-inflammatory responses and anti-apoptosis [2,3]. The goal of this review is to discuss the newly emerging functions of MDPs and their biological role in ageing and metabolic diseases such as T2D.
Mitochondrial Metabolism Modulation
Functions in the Mitonuclear Communication Pathways
Mitochondria booked a portion of the original bacterial genomes that co-evolved with nuclear genome. However, mitochondria import over a thousand proteins encoded in the nuclear genome to maintain their diverse functions, reflecting their adjacent relationship [4].
The mitochondrial genome inherits bacterial-like traits: the DNA molecules (mtDNA) are circular, double stranded, small (16,569 nucleotides in humans) and compact. mtDNA contains 37 genes, including 22 tRNAs, 2 rRNAs (12S and 16S rRNA) and 13 mRNAs encoding the proteins of the electron transport chain [5]. The mtDNA has no introns but a few non-coding nucleotides between adjacent genes and small open reading frames that encode functional MDPs. This class of peptides comprises humanin (HN) and mitochondrial open reading frame of the 12S rRNA-c (MOTS-c) and expands the expression of mitochondrial proteome [6]. It has been established that mitochondria can export peptides and also import cytosolic peptides. It is the class of “cell-penetrating peptides” designed also as “mitochondrial cell-penetrating peptides” [7]. Many age-induced processes and degenerative diseases are related to mitochondrial dysfunction, further highlighting the critical importance of this organelle [8]. Complex human diseases, including diabetes, obesity, fatty liver disease and aging-related degenerative diseases are associated with alterations in mitochondrial oxidative phosphorylation (OXPHOS) function.
Overview on Concepts of Retrograde Signaling and Unfolded Protein
Numerous implications of these anterograde and retrograde signaling pathways between the mitochondria and the nucleus are appropriate for therapeutic exploitation with bioactive molecules.
Concept of Retrograde Signaling
The hallmark of mitochondrial retrograde signaling is the modification of the expression of nuclear genes induced by a signal from mitochondria [9]. Retrograde signaling must be triggered by a mitochondrial signal that in turn is relayed via molecules that finally reach the nucleus. In mammalian cells, altered nuclear expression in response to mitochondrial dysfunction is reported; a number of signaling pathways being implicated in this retrograde communication [10]. Mitochondrial retrograde signaling is a signaling pathway connecting mitochondria and the nucleus. Signal transducers in the yeast retrograde response are Rtg1p, Rtg2p, and Rtg3p proteins [11]. The outcomes of mitochondrial retrograde signaling go far beyond the maintenance or biogenesis of the organelle, affecting the homeostasis of the whole organism through body weight or immunity.
Concept of Unfolded Protein
Mitochondrial protein homeostasis is maintained through proper folding and assembly of newly translated polypeptides. Several factors challenge the mitochondrial protein-folding environment including reactive oxygen species (ROS) that are generated within mitochondria, as well as environmental situations such as exposure to toxic compounds. To promote efficient mitochondrial protein folding mitochondria possess molecular chaperones located in both the intermembrane space and matrix [12].
UPRmt is a mitochondria-to-nuclear communication mechanism that promotes adaptive regulation of nuclear genes related to mitochondrial response, and metabolism, implicated in the cellular homeostasis [13].
Mitochondrial-Derived Peptides: Classification
MDPs are a series of peptides encoded by mitochondrial DNA. This class of peptides comprises HN, MOTS-c, Small HN-like peptides (SHLPs) and expands the expression of mitochondrial proteome [6].
Humanin
The first MDP discovered back in 2001 was HN; the term based on the potential of this peptide for restoring the “humanity” of Alzheimer’s disease (AD) patients. HN promotes cell survival in response to a variety of insults.
It is a small, secreted, 24 or 21 amino acid peptide, depending on cytoplasmic or mitochondrial translation, respectively. If HN is translated within the mitochondria, the peptide will be 21 amino acids; and if it is translated in the cytoplasm, then the result is a 24 amino acid peptide [14]. HN is encoded by an HN open reading frame (ORF) within the gene for the 16S ribosomal subunit within the mitochondrial genome [15]. HN was discovered during a search for survival factors in unaffected areas of an AD patient’s brain. The initial studies were first performed in cell culture and then followed by in vivo studies using both pharmacological mimetics of AD as well as mutant gene: amyloid-β precursor protein. The most recent studies used transgenic models of AD. As HN is a relatively short peptide, exhaustive mutational analysis of the importance of each amino acid has been possible. Interestingly, single amino acid substitutions of HN can lead to significant alterations in its potency and biologic functions. S14G-HN in which the serine at position 14 is replaced by glycine, is a highly potent analogue of HN.
Finally, HN may be the first small peptide of its kind representing a putative set of MDPs, a novel concept that modifies the established concept about retrograde mitochondrial signaling as well as mitochondrial gene expression. HN is a neuroprotective peptide and a cytoprotective factor against oxidative stress [16].
Mitochondrial Open Reading Frame of the 12S rRNA-c ( MOTS-c)
In addition to HN, an in-silico search of the mitochondrial genome revealed additional potential MDPs. MOTS-c is expressed in various tissues and in circulation (plasma) in rodents and humans, suggesting both a cell-autonomous and hormonal role. Its primary target organ appears to be skeletal muscle and fat. The mitochondrially derived peptide MOTS-c was recently discovered. It is a 16 amino acid peptide located in the 12S rRNA gene. The first 11 amino acid residues of MOTS-c are highly conserved in 14 mammalian species [17]. MOTS-c has been identified as a gene expression regulator in the nucleus, leading to retrograde signaling via its interaction with transcription factors. MOTS-c polymorphism has been found to be associated with human longevity [18]. MOTS-c can prevent insulin resistance, dietmediated obesity, and ameliorate diabetes. MOTS-c oxidizes fatty acids and inhibits oxidative respiration [19]. MOTS-c increased the levels of carnitine metabolism, which transport activated fatty acids into the mitochondria for β-oxidation, increased the level of a β-oxidation intermediate. MOTS-c inhibited the folate cycle at the level of 5Me-THF, resulting in an accumulation of 5-aminoimidazole- 4-carboxamide ribonucleotide, an AMP-activated protein kinase (AMPK) activator. MOTS-c also increased cellular NAD+ levels, which are nucleotide precursors [17,20]. MOTS-c regulated a broad range of genes in response to glucose restriction, including those with antioxidant response elements (ARE), and interacted with ARE-regulating stress-responsive transcription factors [21].
Small HN-like Peptides
Recently, six additional peptides encoded within the mitochondrial 16S rRNA region of mtDNA have been discovered and designed as SHLP1-6. SHLP2 and SHLP3 share similar biological effects with HN. The circulating levels of MOTS-c and SHLP2 decline with age. Various studies suggest that SHLP2 and SHLP3 may participate in the pathogenesis of age-related neurodegenerative diseases. The anti-oxidative stress function of SHLP2, and its neuroprotective effect indicate that SHLP2 has a role in the regulation of aging and age-related diseases [5].
Ageing and Plasma MDPs Levels
Ageing and longevity are or are not characterized by high levels of MDPs? It is speculated that MDPs production turns from protective to detrimental adaptive response; in these conditions, the levels increasing during aging. In some studies, HN levels significantly decline with age in humans. Plasma HN level was significantly lower in the older group (1.3 ± 0.2 ng/mL) than that of the younger group (1.7 ± 0.1 ng/mL) [22]. In other studies, it is reported that HN levels significantly decline with age in humans and animals. HN levels in plasma were measured in young and old mice and across age in humans. HN levels decreased with age in both mice and human (Human plasma levels: 45-65 years: 1400 pg/mL; 80-110 years: 1000 pg/mL) [5].
New results are in contrast with these data. HN plasma levels are evaluated in 693 subjects aged from 21 to 113 years. HN levels increased in old age (>500 pg/mL), with the highest levels found in centenarians (> 1000 pg/mL). The plasmatic levels of HN are significantly positively correlated with age. No gender differences were observed for HN. HN plasma level is associated negatively with body mass index in elderly patients [23]. Concerning the other MDPs, it is reported that MOTS-c and SHLP2 circulating levels decline with age. The circulating SHLP2 levels significantly decreased with age in both male and female C57BL/6 mice (young, 3 months old: 3000 pg/mL; aged, 18 months old: 2500 pg/mL). Male mice had higher SHLP2 levels than female mice in both the young and old groups [5]. The results of these studies should be interpreted considering the following limitations. First, the relatively small sample size in each group represents a potential limitation. Second, mitochondrial diseases are an expanding group of disorders with many metabolic deficiencies. In the ideal case, the used patient cohort should display a homogeneous phenotype, disease stage, and organ specificity. Moreover, the discovery of ageing-related biomarkers is supported by the development of advanced proteomics technology. Changes in the circulating concentrations of human proteins can serve as predictive measures of health and disease [24].
Mechanisms of Action of MDPs
MDPs exert functions through binding to both intracellular molecules and putative cell membrane receptors.
MDPs Receptors
Emerging studies show that MDPs play important roles in cytoprotection and homeostasis. HN has been shown to increase extracellular signal-regulated kinase 1/2 (ERK1/2) phosphorylation through its receptor binding [25]. The ERK1/2 cascade serves as an essential mediator in a lot of cellular processes such as proliferation, cell migration, cellular metabolism, and survival. Upon stimulation, ERK1/2 is phosphorylated and becomes dissociated from its anchoring proteins, allowing the translocation of ERK1/2 to other subcellular compartments. HN has been shown to act as a ligand to two different types of receptors; the seven-transmembrane G-protein-coupled receptor formyl-peptide receptor-like-1 (FPRL1), and a trimeric receptor consisting of ciliary neurotrophic factor receptor (CNTFR), the cytokine receptor WSX-1 and the transmembrane glycoprotein gp130 (CNTFR/WSX- 1/gp130) [26,27].
The first HN receptor FPRL1 has been linked to AD. HN acts as an agonist for FPRL1 by inducing Ca2+ mobilization and activation of ERK1/2 signaling, the pathway of G-protein coupled receptors, which participate to its cytoprotective properties [26]. The second reported HN receptor is the trimeric CNTFR/WSX-1/gp130 complex. The activation of the gp130-STAT3 axis is essential for HN activity. HN induces STAT3 activation, which was required for its neuroprotective effects [27]. Gp130 is part of the receptor complex for several cytokines, including IL-6, IL-27.
Concerning the cytoprotective effects of HN or S14G-HN (HN derived), studies suggest that this protection may be mediated through activation of AMPK in thrombin-mediated activation of endothelial nitric-oxide synthase (eNOS) signaling as well as reduction of pro-apoptotic factors [28]. HN in actives proapoptotic peptides such as Bax. It prevents Bax translocation and activation in response to proapoptotic agents [29].
For more Diabetes and Obesity Journals please click on below link: https://lupinepublishers.com/diabetes-obesity-journal/
For more Lupine Publishers Please click on below link: https://lupinepublishers.com/
#LupinePublishers#LupinePublishersGroup#ADO#Journal of Diabetes and Obesity#Diabetes and Obesity#Archives of Diabetes and Obesity
0 notes
Text
Lupine Publishers| Cervical Tarlov Cyst Mimicking Spinal Hydatid Disease: Case Report

Abstract
Go to
Background: Perineurial (Tarlov) cysts are usually incidental findings during magnetic resonance imaging of the lumbosacral spine. The Cervical localization have been reported to be a rare occurrence. We report such a case where a high cervical perineural cyst was masquerading as a spinal hydatid disease.
Case Presentation: We report a case of symptomatic cervical Tarlov cyst in a 9 years old girl operated on twice for pulmonary and hepatic hydatid cyst. Spinal magnetic resonance imaging (MRI) showed an extradural intraspinal lesion with fluid-equivalent signal extending from C5 to T2. Based on the history, the diagnosis of spinal hydatid disease was suggested. Surgical excision of the cyst resulted in significant improvement in patient symptoms, and histological examination revealed the diagnosis of a Tarlov cyst.
Conclusion: Cervical perineural (Tarlov) cyst can be symptomatic by causing nerve root compression and can be mistaken as a spinal hydatid disease on imaging. Surgical treatment can be curative.
Keywords: Tarlov Cyst; Hydatid Cyst; Diagnosis; Management MRI; Cervical Spine
Abbreviations: TC: Tarlov Cyst; CSF: Cerebrospinal Fluid; MRI: Magnetic Resonance Imaging
Introduction
Go to
Tarlov Cyst (TC) is defined as a cystic dilatation between the perineurium and endoneurium of spinal nerve roots, located at level of the spinal ganglion and filled with Cerebrospinal Fluid (CSF) but without communication with the perineurial subarachnoid space [1]. It is most often found in the sacral spine with a prevalence of 4.6% in the general population with about 13% of those being symptomatic [1,2]. The Cervical localization have been reported to be a rare occurrence [3], to our knowledge there are only five published cases of symptomatic cervical Tarlov cyst [4]. MRI of the spine is the gold standard imaging modality for the diagnostics. This is a case report of a symptomatic cervical TC that was masquerading as a spinal hydatid disease. To our knowledge, only five other cases of symptomatic cervical TC have been published [3,4].
Case Presentation
Go to
A 9-year-old girl, with medical history of surgery for pulmonary and hepatic hydatid cysts at age of 8, treated with anthelmintic with good outcome. As far as her past medical history is concerned, there were a history of cervical plexus trauma at the age of 6 with monoparesis sequelae of the left arm. She presented with a 4-week history of gradually developing left hemiparesis. On clinical exam, all deep tendon reflexes were normal. Proximal muscle strength of the left leg and the ipsilateral upper extremity was 3/5. Electromyography (EMG) showed abolition of motor and sensory responses of nerves SPE and SPI on the left upper limb. MRI of the cervical spine showed intraspinal cystic lesion of extra-Dural location lateralized to the left, extending from C5 to T2 causing a stenosis of the adjacent foramina, without contrast enhancement of the cyst wall (Figure 1). Based on the imaging and the history of patient, the diagnosis of a spinal hydatid disease was suspected. Neurosurgical indication was agreed, and the patient underwent a C4-T2 laminotomy (Figure 2), intraoperatively, cystic lesions strongly adhered to the dural mater with an appearance that was evoking congenital cysts. At this point, we opened the capsule and a clear CSF-like liquid came out from the cyst, we conducted a careful excision with Dural plasty. The histological examination showed fibrous tissue and the presence of neural elements, which is typical for perineural cysts. Postoperatively, the patient experienced significant improvement in her symptoms, represented by improved left lower-limb strength. A postoperative MRI of the cervical spine was performed after 6 months showed no recurrence of the cyst (Figure 3).
For more information about Online Journal of Neurology and Brain Disorders archive page click on below link
https://lupinepublishers.com/neurology-brain-disorders-journal/archive.php
For more information about lupine publishers click on below link
https://lupinepublishers.com/index.php
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
0 notes
Text
Lupine Publishers| The Use of Tin Plague in The Analysis of Pure Tin

Lupine Publishers| Modern Approaches On Material Science
Abstract
Study focuses on the basis of knowledge the mechanism of the process βSn αSn for use it to analysis of important material for science and technology. The possibility of ultra-high purity Sn to analyse by measuring the rate (V) of the allotropic changing (V βSn αSn) is investigated. Metals of such high purity are inaccessible to chemical method, so analyzed by method of a residual resistance at temperature (T) of liquid He, inaccessible to most enterprises. The method gives an estimate of the total content of impurities. For Sn with low T of βSn αSn) due to the simplicity of the measuring purity by the V (βSnαSn) is tempting. In high purity Sn with a low content of impurities, this method seems more accessible and convenient than others and probably possible. This paper proposes the affordable and simple method of analysis, high sensitivity, accuracy and reproducibility of the results. not inferior to the complex method of measuring the residual resistance.
Keywords: Residual Resistance; Phase Transition Rate; Impurities
Introduction
The World made 7 metals, according to the 7 planets. (Navoi). In the table of ranks of the ancient Sn is pair to Jupiter, the largest planet. And now Snwith the honorary № 50 in the center of the Periodic Table of Mendeleev. Sn is the oldest to man known metal. Aristotle knew about the Sn plague, but didn’t know that it was a consequence of the allotropic transformation of Sn white to gray, β®α. The nebulous mysteries of Sn plague infection accumulated interests many centuries tothis phenomenon.A main Interest in βSn®αSn appeared after the evidence [1,2]Goryunova semiconductor nature of αSn with covalent bond by changing the metal bond to covalent, the electronic structure s2 p2βSn to sp3,tetragonal structure with KN=6 to a cubic structure with KN=4 with bonds to the vertices of tetrahedrons ofαSn.These principlescreating of semiconductor compounds ofneeds properties. To turn into metastable αSn except T below 12.4oC,is a necessary [2] seed withthe parameters of the bond and structures related αSn and its contact with tin.The nearest neighbors of Sn give a compounds InSb and CdTe, There, pairs of atoms give in sum of total electrons the same as 2 atoms of Sn and parameters of structures [1] almost the same of αSn. InSb, CdTe, αSn the better seed of Sn®αSn, but in contrast to metastable αSn powder, InSb, CdTe are strong solid crystals. Theinfection is caused by atomic contact with a seed. Tin always covered by protective film of SnO2which don’t allow contact.If the seed is placed on the surface of Sn, there is Infection!? And from inert substances that had contact previously with the seed although it now removed[3]. Solid crystals recognized the past! Infection at a distance is possible too![4]. It was quite misunderstood: what gives an information from the seed? Necessary presence of the air, atmosphere.There is Ic agent,[5-7] Inthe vacuum, dryvessel, or after treatment of the inert substance with any solvent of water, so there is no infection,Ic is a carrier from the seed. Metastable structure Ic in the size of nanoparticles can growing epitaxially on the related structure, penetrate through the microdefects of the protective SnO2. So, it is clear that infection under water which absorbed the Icnanoparticles is impossible.This opinion turned out to be wrong. With a very small probability for a time more a year under moving water, infection occurs, and this valuable phenomenon gives ways to many practical tasks andunderstanding of life processes[7].The source of infection has been found. and yet another unexpected source of infection was found. This is property for practical aim. Tin remember about stay in the αSn phase. There is a βSn®αSn transition and back αSn®βSn, due to a change of .>/<d by 26.6%.volume effect. At each β®αmovedecreased d and at α®βd increased. So without external tools Sn gives pure powder of any size particles[8,9].
Knowing the Icas seed allows to use for solving a row of other practical problems [5-7]with use of the terrible plague by a simple way [10,11] in forms convenient for creating p/n shifts , simple effective purification of Sn without meltingin solid phase [12].Method of zone melting [13] to purification is determined by the difference in the K, ratio of the solubility of impurities at the phase boundary. At melting metal doesn’t change type of the bond on the border ofsolid/liquid, soK is near to 1, the difference is knowingly less than at of the metal /semiconductorboundary with the great differences in the nature of their chemical bonds, CN (coordination number), structures. The cleaning efficiency at the border metal /semiconductor, K far from1. And so was a reason that zone melting became widely used when there was a need in semiconductors of high purity.A knowledge of the mechanism of the solid-phase process of βSn ®αSn [7] land to opinionof possibility to apply it in the analysis of the height purity of Sn.
Theoretical View on The Possibility of Analyzing by V Βsn→Αsn
Analysis of high-purity materials is labor-intensive and often impossible if the sensitivity of classical methods is insufficient [14]. There is a method for measuring the g4.2К, i.e. the ratio R 300K /R 4.2 K, method of residual resistance, which gives an estimate of the amount of impurities in metals [15] of high purity. The residual resistance of Sn at 4.2 K before the transition to the superconducting state depends on its purity and perfection of structure. The R at T of room is almost constant, and the g4.2К, i.e. the ratio R 300K /R 4.2 K, is residual R characterizes the purity of Sn.The purer the metal and more perfect its structure, the lower the R at 4.2 K and the higher the value g4.2К, which serves as a measure of the total content of impurities in metals. But measuringequipment is difficult, and liquid He is rarely available to the most of organizations. Studies of allotropic transformation of Sn [5-7] showed a connection between the purity by g4.2К, and the rate V of its phase transformation into αSn. But also, it seemed unrealistic to use it for analyses after bright experiments [16] showed the impurities in Sn are accelerating, indifferent and inhibiting. Hence, the analysis of the purity of Sn by V βSn®αSnis impossible at it depends on the ratio of concentrations of dissimilar impurities. But the mechanismof distinguishing the role of impurities is not clear at all. If each atom of the impurity violates the g4.2К, of the metal, which theg4.2Кmethod illustrates by analyzingany other metals, why the impurities of different metals differ in their effect on the V βSn®αSntransition. This became clear when we knew the mechanism of infection with the "tin plague" [4]. In [16] was studied Sn not of high purity, there are no errors in experiments. The chaotic nature of the dependences of V on purity is clearly shown [5,7]atstudying the influence of impurities on V of βSn ®αSn. The fact is that the commonly zone melting is powerless to clean from Sb because it has K=1 in Sn. The solubilities of Sb in solid and molten Sn are the same, And the Sb impurity on both sides of the phase boundary is the same and so can’t to be redistributed, as other impurities with K≠1.And in the ores of Sn impurity in the Sb usually dominates. At zone melting cleaning, the Sb impurityalways prevails over the others. And Inhimself like of all metals is inhibitory too by the same reasons, but it was shown as accelerator [16] because In+Sb gives the best seed InSb. And in the Sn of high purity, the impurity of In, like any impurity, individual. But having the knowledge aboutthe dependence of the βSn ®αSnprocess on many factors, it is necessary to observe the requirements 1-4, understood during the experiments for creating a method for analyzes[17].
Experimental Part
It is possible to create a method for analyzing the purity of V βSn → αSn similar to measurements of residual resistance, suitable for high-purity metals. Previously, it was found [3,5,7] that the dependence of V βSn → αSn on T for any samples has a maximum. This is very easy to understand. At low T with its growth V βSn → αSn grows according to the Arrhenius equation. V cannot grow constantly, because as it approaches the point of the phase transition, it becomes smaller and turns to 0. When infected, Sn crumbles into an arc-shaped powder, making difficult to measure phase shift lengths. Amorphous wires of fast quenching, single crystals of βSn and even annealed wires with slow infection remain almost the original shape but with some bending, and break at V βSn→αSn depending on the T (Figure 1) to parts of different lengths, but almost the same at each T. Accumulation of impurities by the method of residual resistance was recorded in the fracture. It is seen that after the fracture, the sections at each T are close to each other. For analysis, it is necessary that the content of impurities is constant along the length, that is, choose V βSn → αSn for it, V of growth of αSn and V of impurities were now equal, and Sn maintain the solidity too.
Figure 1: Fracture of Sn of different purity with the accumulation of impurities overtaking the phase boundary at its low V. T= +2:0 and -5 ̊С.
Requirements
1) Monoliths are obtained for the growth of αSn [10,11] in the ice shape. The study of a movement of impurities at βSn → αSn allowed us to create a method like of zone cleaning in a solid, but for analysis it is necessary that the content of impurities is constant along the length, that is, choose V βSn→αSn and V of impurities equal and maintain the solid state.
2)Monoliths are obtained by standard preparing a Sn for analysis, so its behavior and structure depends on the previous mechanical and thermal history of Sn. Ins sample in standard quartz formsmelted and cooled under standard vacuum conditions, then Sn melt poured into a SiO2 mold to made identical samples in the form of wire or rod with a spherical surface of one edge of it, then annealed and cooled in vacuum.
3)To create the minimum of seeds by moving of H2O near of the contact Sn of spherical surface of edge with polishedor spherical surface of InSbseed.in thermostat with selected T for analysis.So, to create the minimum of seeds by moving of H2O near of contact Snwith InSb in thetermostat with ice nearly of chooses T.
4)The diagram of calibration dependence of V βSn®αSn / g4.2should be attributed to the same strictly selected T for analysis.
5)The infection V should be measured repeatedly for graphical correction of errors in a visual determination of the length of the infected area. At T, chosenfor aphase transition the impurity does not accumulate, and the concentration along the entire length is constant, which is important for analysis. For the integrity of the sample, it is possible to infect as in [10,11].You can make many measurements V βSn®αSn on length, reducing the measurement error statistically. The sections along the path of the Snwhite – dark border is measured repeatedly over time. After the end of the analyze measurement with standard remelting, the αSn is converted to βSn, especially if the analysis result must be checked by direct measurement g4,2K, which is applicable only f or metals. According to the graph for a given analysis at T V βSn ®αSn from g4,2Kfind the purity of Sn. Measures of V different samples gave 1.37 and 1.41 mm/hour, corresponded to g4,2K47 500 and 55 000. Control analyses of them give g4,2K46,800 and 55,400. Errors of 1.5% and 0.8% within the measurement accuracyof V and g4,2K. And to check the reproducibility of results in 10 standard samples, an infection V was measured on the same day in the same thermostat. The average of a value of V is 1.48 mm/ hour. A maximum deviation V valueof one sample was 1.46 mm / hour, which is 1.3%, all the others gave 1.48, 149, 1.47.
Summary
By using for the practical aims of “terrible tin plague” along with its application to obtain pure powders of a given dispersion, for further purification of high-purity tin, for growing profiled crystal of a unique material αSn even with p/n transition, simple accessible method of purity Sn analysis was created, which seemed fundamentally impossible. The accuracy and reliability of the results of the proposed method with obvious availability, accessibly and simplicity even is not complicated and complex method of residual resistance without using of liquid helium. Here is only whether the method can be considered created until it still not published and not known to researchers, for whom, and not for corrupt officials, this work was done.
Gratitude’s
The author is grateful to V. V. Ryazanov for his help in measuring g4.2K- residual resistance and for his constant interest in the work, advice and discussions and cooperation with N. G. Nikishina, R. A. Ohanyan , Efremov A.S, Boronina L.R. , Sidelnikov M.S.
For more Lupine Publishers Open Access Journals Please visit our website:
wt u have given that link add For more Modern Approaches on Material Science articles Please Click Here:
https://lupinepublishers.com/material-science-journal/
0 notes
Text
Lupine Publishers | Climate and Water
Lupine Publishers | Open Access Journal of Environmental and Soil Sciences
Short Communication
It is established that the climate depends on greenhouse gases. Few people think that water evaporation is also gas. Their volumes exceed carbon dioxide emissions by 18,000 times [1]. There is a strong opinion that the evaporation of the oceans exceeds the evaporation from land because 3 times the area of the oceans exceeds the area of inhabited land. However, recently it was reported that the total area of leaves of vegetation increases the land area by 3 times. It follows that both the land and the oceans evaporate from the same area. Evaporated before the development of the industry.
Water evaporation into the atmosphere can be divided into two types. There is evaporation from the surface of water bodies, from hard surfaces, ice, snow. With the development of civilization, new nature of evaporation appeared - from boiling water, cooling equipment, plowed fields, new artificial reservoirs, landfills. All pairs raised from these surfaces make a direct or shortened path in the chain of circulation between atmosphere and soil. The second significant, for the time being, part of the vapor is organic discharges from animals and plants. This is a complete cycle of the circuit created by nature since the birth of life on the planet. The main function of water is to dissolve underground and riverbeds and the transfer of trace elements in food chains to the roots of plants and living consumers. Entering the bodies of organisms and the roots of plants with one structure, water is repeatedly transformed into blood, tissues, many other body organs, plant juices, and enters the atmosphere as an exhalation, drying excretions, transpiration in a completely different quality. The sum of all these, purely individual vapors, forms a substance in clouds with certain properties that have been polished for millions of years in each area, which along the beaten path with a given periodicity precipitates in the given places of the planet, supporting various areas from deserts to tropics. Perhaps, the information component plays some role here. It is known that clusters of molecules carry information about their source - maybe DNA. For example, it is known that the smell is formed by molecules inherent in everyone. And these molecules go into the atmosphere, filling up the clouds.
The parameters of clouds are their saturation, physical and chemical composition, the size of clusters of molecules and droplets, specific gravity, location, volume, time spent in the atmosphere, temperature, pressure, electrical charges - all this together creates elements of the mechanism of weather and climate formation. For millions of years, the interaction of these parameters has formed a rigorous algorithm that determines where, how much and when it is necessary to give moisture to each place on the planet. With the development of civilization, we took away more than 70% of land from nature by cutting down forests, plowing the soil, flooding them with hydroelectric power plants, using unnatural water - turning it into a working reagent. We move it with pumps, with it we wash everything around us and ourselves. We boil, heat, compress, cool, fill the fields, destroy its molecules in the air with engines, furnaces and compressors.
Evaporation from all these processes must have lost the properties inherent in pairs from living organisms and plants. The physical, chemical elements and all other cloud parameters have changed. The mechanism of atmospheric transformations has changed, which produces new clouds in a new way, concentrates and distributes all the moisture in a different way, changes the places of precipitation.
The volume of artificial evaporation with the development of industry and human comfort equaled the volume of organic vapor. Mankind has destroyed the effect of organic vapor on most of the land. From these places, the waters that have not passed the path indicated by nature began to evaporate - to deliver nutrients to living organisms and plants. In total, we take 22 cubic kilometers of water from open and underground sources. All these waters lose their natural functions and evaporate without changing the structure [1]. The new quality of vapor has changed the structure of steam and has had an effect on its specific weight. The increased weight of gaseous water and its drops changed the height of the clouds. The quality of evaporation creates a new quality of atmospheric mechanisms. Heavy clouds cannot rise above, where the conditions of the precipitation, which was built in the pre-industrial era. Therefore, the clouds have changed their dynamics in terms of speed of movement and increased the concentration in volumes. Changed the time the water in the clouds. All this in the complex changed the places of precipitation, their volumes and schedule. From here, we observe floods in some areas, droughts in others, the extinction of insect species and animals. The decrease in transit in range and height of the movement of clouds led to a decrease in precipitation on the glaciers of the polar poles and mountain peaks. The precipitations on the way to these places do not accumulate in the glaciers but replenish the oceans with additional volumes. Therefore, the level of the oceans increases, and the ice layer of the glaciers decreases.
This hypothesis requires scientific evidence, which should lead to a new strategy, basically All of which should be the cessation of deforestation, the creation of man-made water reservoirs, deep plowing of fields, the elimination of landfills, the reduction of construction facilities and roads and the total water savings on all types of human activity. Nature urgently needs to return its natural mechanisms of atmospheric phenomena, processes of circulation. Opportunities are there, if you use the experiences of developed countries. It is known that in the Scandinavian countries there are no landfills, in Israel they grow plant products with minimal water consumption. Famous houses with vertical and roof gardening, in which water evaporates plants, and not from artificial surfaces. Known methods that allow to generate electricity without reservoirs. One of the significant water consumptions is the water consumption in toilets. At the same time, we are aware of ways to save water in the toilets of airplanes and trains. Simply transfer such savings to the devices of each toilet, and centralized sewage will disappear, with the need to maintain vast areas of lagoons. Such and many other measures of total water saving should be applied in all spheres of life of all cities of all countries. Considering each type of water consumption, it is possible to detect known and applied methods with minimal and even zero water consumption, for example, drip irrigation, dry cleaning of cars and asphalt. Only the return of its nature, millions of years of accumulated technology of the water cycle, can reduce natural disasters and stop climate change. To prove the hypothesis, it is necessary to study its basic elements. I call for the cooperation of all who can master and understand this hypothesis. A new team of new specialists is needed, which will bring the scientific base and turn the consciousness of the sleeping population in a new direction.
https://lupinepublishers.com/environmental-soil-science-journal/pdf/OAJESS.MS.ID.000152.pdf
https://lupinepublishers.com/environmental-soil-science-journal/fulltext/climate-and-water.ID.000152.php
For more Lupine Publishers Open Access Journals Please visit our website: https://lupinepublishersgroup.com/
For more Open Access Journal on Environmental and Soil Sciences articles Please
Click Here: https://lupinepublishers.com/environmental-soil-science-journal/
To Know More About Open Access Publishers Please Click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
0 notes
Text
Happy Thanksgiving!!!
Greetings from Concepts of Dairy and Veterinary Sciences (CDVS)

We are deeply thankful for your confidence and loyalty towards our Concepts of Dairy and Veterinary Sciences, and we extend to you our best wishes for a happy and healthy Thanksgiving Day!!
#Lupinepublisher#LupinePublishersgroup#DairyandVeterinarySciences#Dairy#VeterinarySciences#LiveStock#AnimalNutrition
0 notes
Text
Artificial Neural Networks Based Modeling in Sustainable Energy Domain
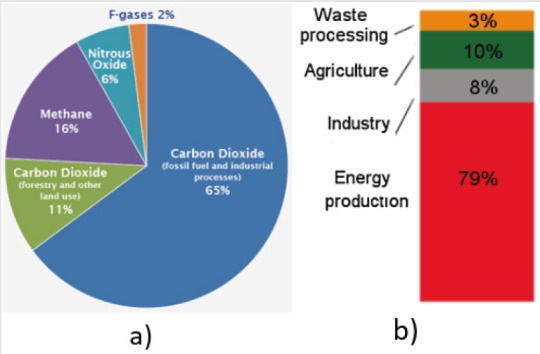
Introduction
The economic and technical development of human society in late years put a heavy pressure on the natural resources of our planet. The increasing need for both material and energy resources lead not just to an extensive consumption of existing ones but also to an increase of pollution, with negative and irreversible consequences on every living being on Earth. One of the most destructive is the constant rise of the atmosphere temperature as consequence of so called “greenhouse effect”: the accumulation of some gases among the most important is CO2 , produced mainly by classical energy sources Figure 1, acting as a shield and maintaining the heat generated by solar radiation. This fact induces a “domino” effect on whole planet, starting with the glacier’s melting
Read more about this article: https://lupinepublishers.com/biosensors-renewable-sources/fulltext/artificial-neural-networks-based-modeling-in-sustainable-energy-domain.ID.000105.php
Read more Lupine Publishers Google Scholar Articles : https://scholar.google.com/citations?view_op=view_citation&hl=en&user=5ql0QHJV55QC&citation_for_view=5ql0QHJV55QC:Wp0gIr-vW9MC
#Lupinepublishers#Lupinepublishersgroup#JournalofBiosensorsandRenewableSources#SolarEnergy#Geothermalenergy
1 note
·
View note
Text
Lupine Publishers| Inequalities in Diabetes in the USA
Lupine Publishers | Archives of Diabetes & Obesity (ADO)
Abstract
Background: Diabetes disproportionably impacts minorities in the USA.
Objective: To review the latest data regarding diabetes epidemiology and management among different ethnic groups in the USA.
Methods: PubMed research of all pertinent articles up to June 29, 2020. Search terms included diabetes, ethnicity, African Americans, Blacks, Hispanics, Latinos, Asians, minorities, glycemic control, obesity, lifestyle changes, treatment, metformin, sodiumglucose co-transporter 2 inhibitors. Type of studies included are randomized, observational, epidemiological, consensus guidelines, and review articles.
Results: Diabetes prevalence and incidence in adults continue to increase among African Americans and Hispanics. In youths, the fastest increase in type 1 and type 2 diabetes occurs among Asians/Pacific Islanders followed by Hispanics and African Americans. The gap in glycemic control between Whites and minorities is widening. Whereas mortality rates decreased in patients with diabetes overall, the least mortality reduction was observed among Hispanics and non-Hispanic blacks. The diabetes epidemic among nonwhites patients is mainly due to obesity and physical inactivity. Lifestyle changes are generally effective for both prevention and treatment of diabetes among minorities. Metformin may be particularly effective among African Americans. Metformin and sodiumglucose co-transporter 2 (SGLT2) inhibitors are the most convenient drugs for treatment of diabetes in minorities.
Conclusion: Substantial disparities still exist in the USA with respect to diabetes incidence, glycemic control, and mortality.
Keywords: Ethnicity; Disparities; Diabetes; Obesity; Prevention; Treatment; Lifestyle changes
Introduction
According to the World Health Organization, equity is the absence of avoidable, unfair, or remediable differences among groups of people, whether those groups are defined socially, economically, demographically or by other means of stratification [1]. Therefore, health equity implies that everyone should have a fair opportunity to attain his/her full health, and that no one should be disadvantaged from achieving this potential [1]. Unfortunately, marked ethnic/racial disparities in the USA exist with respect to almost all aspects of diabetes and its care. Thus, minority groups are disproportionately affected in terms of diabetes incidence and prevalence, metabolic control, complications, prevention, and treatment. The causes of these disparities are complex but obesity among minorities play a major role. The main purpose of this article is to provide an update on ethnic/racial disparities in diabetes in the USA and to discuss the most effective ways of diabetes prevention and treatment among minorities. We used the same terminology for the racial/ethnic group (e.g. Hispanics versus Latinos) as it appears in the corresponding reference.
Disparities in Diabetes Prevalence
According to 3 surveys conducted by the National Health and Nutrition Examination Surveys (NHANES) between 2011 and 2016, weighted age and sex-adjusted prevalence of total diabetes i.e. diagnosed and undiagnosed was 12.1% for non-Hispanic white, 20.4% for non-Hispanic black, 22.1% for Hispanic and 19.1% for non-Hispanic Asian adults (overall P<0.001) [2]. The prevalence of undiagnosed diabetes generally followed similar pattern: 3.9% for non-Hispanic white, 5.2% for non-Hispanic black, 7.5% for Hispanic, and 7.5% for non-Hispanic Asian adults (overall P < 0.001) [2]. Marked heterogeneity in diabetes prevalence are present within the same ethnic group (Table 1).
Table 1: Estimated prevalence of diabetes, diagnosed and undiagnosed, in the USA among persons 20 years or older among different ethnic groups [adapted from reference 2].
*Weighted age- and sex-adjusted (95% confidence interval).
** Central America: Costa Rica, Guatemala, Honduras, Nicaragua, Panama, Salvador.
*** South America: Argentina, Chile, Columbia, Ecuador, Paraguay, Peru, Uruguay, Venezuela.
■East Asia: China, Japan, Korea.
●South Asian: India, Pakistan, Sri Lanka, Bangladesh, Nepal, Bhutan.
■●Southeast Asia: Philippines, Vietnam, Cambodia, Thailand, Indonesia, Malaysia, Singapore.
Disparities and Trends in Diabetes Incidence
Following a steady increase in diabetes incidence in adults from 1990 to 2007, it started to decrease from 2008 through the last National Health Interview Survey (NHIS) conducted in 2017 [3]. However, this decrease in incidence was driven primarily by non- Hispanic whites (annual percentage change of -5.1% (P=0.002) followed by Asians (annual percentage change -3.4% (P=0.06), whereas incidence rates among Hispanics and non-Hispanic blacks did not decrease [3]. In fact, the latest age-adjusted data for 2017- 2018 indicated that incidence of diagnosed diabetes in adults were highest in Hispanics (9.7 per 1,000 persons), followed by non- Hispanic blacks (8.2 per 1,000 persons), and Asians (7.4 per 1,000 persons), whereas non-Hispanic whites had the lowest incidence (5.0 per 1,000 persons) [4].
Prevalence of Pre-Diabetes
The most recent National Diabetes Statistics Report showed that 34.5% of all US adults had prediabetes (defined as HbA1c 5.7% to less than 6.5%, or fasting plasma glucose 100 to less than 126 mg/dl, or 2-hr postprandial plasma glucose 140 to less than 200 mg/dl) [4]. The prevalence of prediabetes was stable from 2005-8 to 2013-2016 [4], and not statistically significant between racial/ ethnic groups and various education levels: 31.0 % among Whites, 36.8% among non-Hispanic blacks, 36.1% among Hispanics and 33.0% among Asians [4].
Disparities in Diabetes in Youths
According to the SEARCH for Diabetes in Youth Study, a population-based registry study covering 5 states in the USA, incidence of both type 1 and type 2 diabetes is increasing in youths (defined as persons aged < 20 years) [5]. From 2002 to 2015, the annual relative percent increase was 1.9% and 4.8% in type 1 and type 2 diabetes, respectively [5]. Like the adult population, there were clear ethnic/racial differences in the rate of increase of diabetes in youths [5]. In type 1 diabetes, the steepest increase in incidence was among Asians/Pacific Islanders (4.4% per year), followed by Hispanics (4.0% per year), then Blacks (2.7%/year), and finally Whites 0.7% per year [5]. In type 2 diabetes, similar order was observed. Thus, the fastest increase was among Asians/ Pacific Islanders (7.7% per year), followed by Hispanics (6.5% per year), Blacks (6.0%/year), American Indians (3.7% per year), and finally Whites (0.7% per year). The latter increase among Whites was not statistically significant (95% CI, -1.35 to 2.94) [5]. Reasons of increase in type 1 diabetes are unclear. Meanwhile, the increased incidence in type 2 diabetes is likely due to the increase in obesity in US youths, particularly among minorities [6].
Disparities in Prevalence of Gestational Diabetes
In 2016, the crude (unadjusted) national prevalence of gestational diabetes was 6% [7]. In terms of ethnicity, prevalence of gestational diabetes follows a characteristic pattern. The lowest prevalence exists among non-Hispanic blacks 4.8%, followed by Whites 5.3%, then Hispanics 6.6%, then American Indians/Native Alaskans, and highest in Asians 11.1% [7]. However, despite the fact that prevalence of gestational diabetes is lowest among black women, their risk of developing subsequent type 2 diabetes was the highest compared with other racial/ethnic/groups [8]. For instance, the adjusted hazard ratio of developing diabetes after gestational diabetes was 7.6 and 4.4, among Black and White women, respectively, P=0.028) [8].
Diabetes Prevalence Among African Immigrant Population
The African immigrant (African-born) is one of the fastest growing immigrant groups in the USA [9]. Using data from the NHIS, Alma-Ruth et al [10] reported that age-standardized diabetes prevalence was significantly lower in African immigrants than in African- Americans (US-born), 7% and 10%, respectively (P< 0.01) [9]. Furthermore, African immigrants who had lived in the USA for ≥ 10 years were significantly less likely to have diabetes with a prevalence ratio (PR) of 0.61; 95% CI 0.43-0.79), less likely to have overweight/obesity (PR 0.87; 95% CI 0.77-0.96), hypertension (PR 0.69; 95% 0.61-0.78), and to be physically inactive (PR 0.21, 95% 0.15-0.28) [9]. Hence, African immigrants seem to have a more healthy and distinct metabolic profile compared with African Americans.
Disparities in Glycemic Control
Studies have consistently shown that diabetes control, as reflected by hemoglobin A1c (HbA1c) concentrations, is worse in Blacks and Hispanics compared with White race. In a national cohort of persons older than 65 years enrolled in Medicare Advantage Health plans in 2011, Ayanian et al [11] examined the proportions of patients with HbA1c levels ≤ 9.0%. They found this goal was achieved by 84.0%, 80.6%, and 74.6% among White, Hispanic, and Black enrollees, respectively (P<0.001 for the difference between any 2 groups) [11]. Furthermore, available data suggest that the ethnic/racial gap in HbA1c continues to widen. In fact, analysis of NHANES conducted between 2003 and 2014 showed that HbA1c values tend to worsen among African American and Mexican American patients with type 2 diabetes, whereas corresponding values tend to improve among White patients [12]. It should be emphasized, however, that the difference in HbA1c levels between Black and White persons may be attributed in part to racial factors possibly due to difference in glycation of hemoglobin [13]. Thus, on average, HbA1c levels are 0.4 percentage points (95% CI, 0.2-0.6% percentage points) higher among Blacks compared with White individuals for a given mean blood glucose concentrations [13].
Trends and Disparities in Diabetes Care in the US
Serial analysis of the NHANES data between 2005 and 2016 suggests that diabetes care cascade has not significantly improved during that period [14]. Indeed, only 23-25% of patients met the composite goal of targets of HbA1c (<7-8.5%, depending on age and complications), blood pressure (<140/90 mmHg), low-density lipoprotein cholesterol (<100 mg/dl), and no smoking [14]. These proportions of patients did not change between 2005 and 2016 [14]. Furthermore, there were obvious ethnic disparities in achieving this goal [14]. For example, in 2013-2016, 25% of non-Hispanic white patients attained he previous composite goal, compared with only 14% of non-Hispanic blacks, and 18% of Hispanic patients [14].
Disparities in Diabetes-Related Complications
In general, ethnic/racial minorities have more frequent macrovascular and microvascular diabetes complications compared with Whites [10,15]. The largest available National data showed that in 2010, incidence (cases per 10,000) of end-stage renal disease (ESRD) were more than double in Blacks versus Whites 36.6 versus 16.0 [10]. Corresponding rates for lower-extremity amputation were 40.0 versus 20.4, for stroke 63.1 versus 39.0, and for hyperglycemic death 2.2 versus 1.4. A notable exception was the incidence of acute myocardial infarction, which was lower in Blacks compared with Whites, 32.5 versus 37.5, respectively [10]. No corresponding data regarding the Hispanic patients were reported [10].
Disparities in Diabetes-Related Mortality
Mansour et al [16] reported significant ethnic disparities in mortality rates in patients with diabetes who participated in the NHANES surveys during 1999-2010. Follow-up of this cohort revealed that all-cause and cardiovascular (CV) mortality decreased in all ethnic groups with diabetes. However, the magnitude of reduction in CV mortality significantly differed between various ethnic groups [16]. Thus, Whites experienced the largest reduction in CV mortality from 20.4% down to 14.5%, followed by Non- Hispanic Blacks from 20.6% to 16.3%, whereas Hispanics had only a marginal reduction from 18.4% to 17.5% [16]. Similarly, recent analysis of NHIS conducted from 1997 to 2017 showed a significant decline in CV complications among White patients only, whereas no significant decline was observed among Black or Hispanic patients [17]. Taken together, while mortality rates decreased in patients with diabetes overall, the least mortality reduction was observed among Hispanics and non-Hispanic blacks. This finding is in accord with NHANES data mentioned above showing that diabetes care during 2005-2016 was worst among minorities [14].
Causes of Ethnic/Racial Diabetes Disparities: Role of Obesity
Causes of high prevalence of diabetes in minorities are multi-factorial [18]. The growing obesity epidemic is likely the main driver of diabetes among minorities. In fact, non-Hispanic blacks have the highest prevalence of obesity, whereas Mexican Americans have the highest annual increase in obesity and in waist circumference [6]. Likewise, there is steady increase in obesity in US youths (2-19 years) among non-Hispanic blacks and Mexican Americans, but recent decline among non-Hispanic whites [6]. In 2030, it is predicted that severe obesity defined as body mass index (BMI) ≥ 35 kg/m2 will be highest among non-Hispanic blacks 31.7% (95% CI, 29.9-33.4), followed by Hispanics 24.5% (95% CI, 22.8-26.2), and non-Hispanic whites 23.4% (95% CI 22.1-24.8) [19]. Other causes of diabetes disparities include high-sugar diet, food insecurity [20], physical inactivity, increase insulin resistance independent of adiposity [18], health illiteracy, low education and socio-economic levels [4], lack of health insurance, decrease adherence to medications [21], and communication/language barriers. Genetic factors for diabetes susceptibility contribute similarly to diabetes risk across race/ethnicities [18]. Therefore, genetic differences are unlikely to play a major role in ethnic/racial diabetes disparities
Guidelines for Diagnosis of Diabetes Among Minorities
In subjects pertaining to minority groups, the American Diabetes Association (ADA) recommends screening for diabetes and prediabetes by fasting plasma glucose, HbA1c, or oral glucose tolerance test if they have a BMI ≥ 25 kg/m2 (or ≥ 23 kg/m2 in Asian Americans) [22]. If results are normal, testing should be repeated at a minimum of 3 year-intervals [22]. Patients with prediabetes should be tested yearly [22].
Prevention of Diabetes Among Minority Groups
Lifestyle changes
Since obesity is the main cause of high incidence of type 2 diabetes in general, and among minorities in particular, weight loss strategies including diet and exercise are essential to prevent or at least to delay onset of diabetes. In the landmark trial of Diabetes Prevention Program (DPP) that included 3234 multiethnic individuals at high risk for diabetes, participants were randomized to a lifestyle modification program, metformin 850 mg bid, or placebo [23]. After an average follow-up of 2.8 years, incidence of diabetes was reduced by 58% and 31 % by lifestyle changes and metformin, respectively compared to placebo [23]. It was encouraging that sub-group analysis of the DPP showed that lifestyle intervention tended to be more effective among minority groups with 61-71% reduction in incidence of diabetes compared with 51% reduction among white subjects [24]. Due its success, the DPP approach was implemented in several studies including Hispanics [24] American Indians/Alaska Natives [25], African American [26] and as part of faith-based lifestyle intervention in African American churches [27]. In addition, culturally adapted lifestyle intervention was attempted for prevention of diabetes among Hispanics [28]. In general, the previous studies were met with limited or partial success because of short duration of followup, high attrition rates, and female preponderance [24-28].
Metformin
Although metformin, was inferior to lifestyle changes in prevention of diabetes in the DPP [23], its use in this setting may be considered when lifestyle changes are not feasible or successful. In fact, in the DPP, metformin appears more effective in reduction of new-onset diabetes among minorities than among Whites [23]. Thus, African Americans had 44% reduction, followed by Hispanics 31% reduction, then finally Whites 24% reduction (statistical significance between the 3 groups was not reported) [23]. Moreover, studies showed that metformin is particularly effective with respect to diabetes prevention in women with prior history of gestational diabetes, subjects younger than 60 years, and those with higher baseline fasting glucose (≥ 110mg/dl versus 95- 109mg/dl), or HbA1c (6-6.4% versus < 6.0%) [29]. In addition, the ADA recommends consideration of metformin for patients with prediabetes and BMI ≥ 35kg/m2 [29].
Management of diabetes among minorities
Lifestyle intervention: In ‘The Action for Health in Diabetes (Look Ahead)” trial, 5,145 (36% minorities, 40% men) overweight/ obese subjects with type 2 diabetes were randomized to intensive lifestyle intervention and a control group of diabetes support and education [30]. The objective of the lifestyle intervention is a weight loss of 10% by decreased caloric and fat intake and increased physical activity [30]. After 8 years of intervention, all female patients from different ethnic groups lost weight similarly [30]. Among men, there was a trend toward less weight loss among African American and Hispanic men compared with Whites [30]. A more recent randomized trial conducted in Illinois evaluated culturally tailored diet changes and increase physical activity in low-income African American patients with type 2 diabetes [31]. Compared to standard care group, HbA1c levels were significantly lower at 6 months, but the difference was no longer significant at 12 and18 months [31].
The ADA recommends diabetes self-management education (DSME) in all patients with diabetes. The goal of DSME is to increase the patient’s self-efficacy to manage diet, physical activity, glucose monitoring, and stress management [32]. In one meta-analysis of 20 randomized trials of African Americans and Hispanics, DSME programs resulted in modest but significant HbA1c reduction of 0.31% (95% CI, -0.48 to -0.14%) compared with standard care [33]. However, another meta-analysis of 8 African American studies did not find any significant impact of DSME in improving HbA1c values [34]. Overall, data suggest that long-term lifestyle intervention adopted in the Look Ahead trial is generally effective in all ethnic groups [30]. However, culturally adapted diet and DSME strategies had limited or no benefit in terms of glycemic control.
Drug therapy for treatment of diabetes among minorities
Metformin: Data derived from electronic health records suggest that African-Americans (n=7,429) with type 2 diabetes have better glycemic response to metformin compared with European Americans (n=8,783), reduction in HbA1c levels being 0.9% and 0.4%, respectively (P<0.001 for the interaction between metformin exposure and race) [35]. These results are generally in agreement with those of the DPP showing superior efficacy of metformin in prevention of diabetes among African Americans (44% reduction of new-onset diabetes versus placebo) [23]. In addition, a subgroup analysis from the DPP showed that African American subjects with prediabetes treated with metformin have significantly greater decrease in fasting plasma glucose concentrations versus Whites up to 2 years after intervention [36].
Sodium-Glucose Co-Transporters Type 2 Inhibitors
Sodium-glucose co-transporters 2 (SGLT2) inhibitors are effective, safe, and easy to administer (once a day orally). In addition, they reduce systolic blood pressure and body weight. Furthermore, they significantly decrease CV and renal events in patients with type 2 diabetes and high cardiovascular risk [37,38]. Therefore, these agents are well-suited for treatment of type 2 diabetes in minorities. Unfortunately, ethnic minorities remain underrepresented in the major CV trials of SGLT2 inhibitors [39]. Nevertheless, it is reassuring that the 2 SGLT2 inhibitors empagliflozin and dapagliflozin decreased incidence of CV events in all ethnic groups, including the black patients that constituted approximately 5% of the study populations [37,38]. In a recent randomized trial formed exclusively of African Americans with type 2 diabetes and hypertension, empagliflozin reduced HbA1c levels by 0.78%, mean ambulatory systolic blood pressure by 8.4 mmHg, and body weight by 1.2 kg compared with placebo after 6 months [40].
Glucagon-Like Peptide-1 Receptor Agonists
Like SGLT2 inhibitors, glucagon-like peptide-1 receptor (GLP- 1) agonists decreased weight, systolic blood pressure, and CV events in patients with type 2 diabetes and established CV disease [41]. Main limitations of these agents are the subcutaneous way of administration (once daily or weekly) and high cost. Secondary analysis of phase III trials showed that glycemic efficacy, weight reduction, and safety of the GLP-1 agonist liraglutide are generally similar between African American, Latino/Hispanic, and White patients [42,43]. In the LEADER trial in which Blacks constituted 8.3% of the study population, CV benefits of liraglutide were similar irrespective of the race [41].
Amelioration of Patient-Provider Communication
Patient-provider communication is a critical element in health care provision. In one study, Latino patients who switched from language-discordant to language-concordant primary care physician had significant improvement in their glycemic control [44]. Current efforts aiming at standardization of Medical Spanish in Medical Schools represent a step forward to enhance communication and trust between physicians and Hispanic patients with limited English proficiency [45].
Summary and Current Needs
In the last decade, ethnic/racial disparities in diabetes incidence, prevalence, metabolic control, complications, and mortality continue to worsen. With respect to incidence of type 2 diabetes, the gap between Whites and minorities has widened in both adults and youths [2-5]. The latter observation is largely due to the steady increase in prevalence of obesity among minorities [6]. The DPP showed that weight loss and increased physical activity were effective in preventing diabetes among all racial groups [23]. Therefore, targeting obesity should be an absolute priority to diminish diabetes incidence in general and among minorities in particular. It is the time to take serious actions nationwide to change the pattern of current diet in the US. Specifically, sweetened beverages, refined carbohydrates, red and processed meats should be minimized as far as possible, and replaced by non-sweetened beverages, whole grain, and fibers [46]. Government should provide incentives for production and promotion of affordable healthy food. Any economic or political barriers that interfere with implementation of these diet changes should be removed. Intensive efforts are urgently needed from Federal and local authorities to reduce socioeconomic and educational discrepancies between Whites and disadvantaged minorities. Unfortunately, the recently recorded disproportionate high rates of infection and mortality caused by COVID 19 among African Americans have uncovered the deep and chronic wounds of health inequities that long existed and still persist in this country [47].
https://lupinepublishers.com/diabetes-obesity-journal/fulltext/inequalities-in-diabetes-in-the-usa.ID.000148.php
https://lupinepublishers.com/diabetes-obesity-journal/pdf/ADO.MS.ID.000148.pdf
For more Lupine Publishers Open Access Journals Please visit our website: https://lupinepublishersgroup.com/
For more Archives of Diabetes & Obesity(ADO) Please Click Here: https://lupinepublishers.com/diabetes-obesity-journal/ To Know more Open Access Publishers Click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers Follow on Twitter : https://twitter.com/lupine_online
0 notes
Last Seen Blogs

awesome4agirls-blog
Untitled

aberionart
aberíon

catbcys
but down in your arms, in your arms

dembouw
Dembouw

senior52muc
Unbetitelt