#r4l thoughts
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
In 2020, Tumblr had 29.4 million users in the US.
Text
Female socialisation is not the good socialisation. Male socialisation is not the good socialisation. There is no good sex-based socialisation.
54 notes
·
View notes
Text
Sometimes I'll see people make an argument along the lines of: "It is immoral for women to [femininity behaviour] unless they have to"
and this glosses over the fact that coercion is rarely as straight-forward as literally having no choice whatsoever.
14 notes
·
View notes
Text
I want liberation for all women, not just liberation for good, smart, moral, less-desperate or unimpulsive women.
As soon as you accept that some women - who would be less likely to be exploited if they were not women - "deserve it", you have lowered the goal from elimination of the sex-class hierarchy. You are then arguing only for protection for women who "deserve it". Not too unlike the people who think that a good woman deserves a good husband to protect her & that the issue to tackle is the deficit of "good men" and "good women" rather than the power dynamics.
9 notes
·
View notes
Text
It’s embarrassing when radblr uses other disadvantaged groups as a cudgel to say “no one would use this rhetoric against them!”. If you value intersectionality think before you use the idea of the Other whose issues are treated appropriately and better than women’s.
8 notes
·
View notes
Text
Why do the women I know who didn't go to uni have much less career ambition than the men (uni educated and not) that they are with? Maybe before we freak out about men not enrolling in uni as much we should consider differences in (perceived) access to careers without uni?
Maybe before we condemn the girlboss we should consider how crippling the assumption of stay at home or supplementary worker mum is to career ambition?
7 notes
·
View notes
Text
and don’t tell me the solution is for me to just post more about actual theory because I have made so many more posts expressing ideas and/or sharing quotes but the two posts of mine that radblr took up the most were:
“You should read more feminist books from before 1975”
A news article link showing an example of a woman being treated horribly by a man and her family facilitating that
I hardly ever post news articles. A news article is nice and safe though isn’t it? Your beloved mutuals aren’t going to disagree that what happened is bad. You can just read the headline if you want. You can develop theory the most by being exposed (whether it’s agree, disagree or no stance) to what you aren’t already sure of. But if you aren’t sure, maybe you don’t want to risk exposing others to it - and potential judgement.
I don’t have a solution; I just have a winge.
6 notes
·
View notes
Text
There are things you should not inflict on people even if they say you can. There are things that you should not want to do in the first place. There are things that you should not encourage yourself to do again, or want to do again, in the future by doing them now.
5 notes
·
View notes
Text
I've complained about people on radblr making causal claims about transgender health but reading some of the stuff in the literature...
I started reading https://doi.org/10.1080/26895269.2024.2366881 Very early on came across "Research has consistently shown that gender affirmation promotes positive mental health outcomes for trans people of any age (Olson-Kennedy et al., 2018; Russell et al., 2018)." Ok so let's take a look at those that first one shall we? (post got too long)
Olson-Kennedy et al. https://doi.org/10.1001/jamapediatrics.2017.5440
"Findings In this cohort study, chest dysphoria was significantly higher in the nonsurgical vs postsurgical cohort. Among the nonsurgical cohort, 94% perceived chest surgery as very important; among the postsurgical cohort, serious complications were rare, and 67 of 68 reported an absence of regret."
Hmm ok let's look some more at the results from a convenience sample recruited by The Center for Transyouth Health and Development at Children’s Hospital Los Angeles.
So first of all we aren't doing measures of positive mental health outcomes - who needs to actually measure an improvement in mental health to claim a mental health benefit though am I right? "Main Outcomes and Measures Outcomes were chest dysphoria composite score (range 0-51, with higher scores indicating greater distress) in all participants; desire for chest surgery in patients who had not had surgery; and regret about surgery and complications of surgery in patients who were postsurgical."
Let's look at that result now:
"Chest dysphoria composite score mean (SD) was 29.6 (10.0) for participants who had not undergone chest reconstruction, which was significantly higher than mean (SD) scores in those who had undergone this procedure (3.3 [3.8]; P < .001)"
If you look at the scale it includes things like "I feel like my life hasn't started because of my chest" "I get gendered as female because of my chest". Let's say someone was like "yep I'm a trans man, I want chest surgery" gets the surgery and didn't experience an improvement in mental health, couldn't we still expect her to go from "agree" to "disagree" on this item? If you were still unhappy wouldn't you then have to go "well I guess it wasn't the chest after all" and therefore score lower on the chest dysphoria scale despite not having anything alleviated? Surely statements that attribute not getting what you want in life to your chest are inappropriate here.
"Among the nonsurgical cohort, 64 (94%) perceived chest surgery as very important, and chest dysphoria increased by 0.33 points each month that passed between a youth initiating testosterone therapy and undergoing surgery."
Hang on, so is the implication here that the positive effect on relieving chest dysphoria of surgery is offset by how bad testosterone therapy is?* Almost like the above attribution error discussion could be in play... \* Note: completely offset would take a long time, years. I had earlier misinterpreted a result and had the wrong timeframe provided.
If the citing and original authors are implying that association between surgery and mildly lowered dysphoria shows that surgery improves dysphoria, surely in the interest of consistency you need to say that testosterone without surgery worsens it for this cohort.
Instead we get "This finding should not be construed as an endorsement to withhold or delay testosterone initiation to avoid chest dysphoria intensity." and "Given the numerous complications associated with chest binding, the negative emotional and mental effects of chest dysphoria, and the positive outcome of chest surgery demonstrated in this study, changes in clinical practice and in insurance plans’ requirements for youth with gender dysphoria who are seeking surgery seem essential."
We are however told that "The increasing chest dysphoria after testosterone treatment begins does reflect a common clinical phenomenon: a honeymoon period after testosterone initiation that quickly becomes eclipsed by the greater disparity between a more masculine presentation and a female chest contour. Clinicians should advise patients and families that chest dysphoria may increase over time after starting hormone therapy." I guess increasing chest dysphoria just isn't a very important factor after all? Not important enough to delay testosterone therapy, but important enough to undergo surgery. I will grant that effect sizes are different but we are given no reasoning about what a meaningful effect size would be; I assume because that would be to admit that there could be a low enough dysphoria relieving effect that even if dysphoria is relieved, it's not worth it for most.
"Among the postsurgical cohort, the most common complication of surgery was loss of nipple sensation, whether temporary (59%) or permanent (41%). Serious complications were rare and included postoperative hematoma (10%) and complications of anesthesia (7%). Self-reported regret was near 0."
Most of the sample (58%) btw it had been a year or less since surgery.
3 notes
·
View notes
Text


... https://budget.gov.au/content/womens-statement/index.htm
Instead of just saying abuse let's spell out "abuse of power over women and children". Instead of just saying "empower" let's spell out "increase power and autonomy" Then we see what empowering men "to help end abuse" more clearly. Why - according to the Australian government - is part of the solution for men abusing power over women and children to increase men's power and autonomy?
They don't need more power to break the cycles of violence - they need to let go of the attitudes of entitlement that encourage using their power against women and children.
I don't oppose support to recover and heal for boys exposed to family violence. If it's to help them feel better lets say that. If it's to change their attitudes to reduce likelihood of them adopting coercive behaviours against women and children let's say that. Abusers often enough have a victim complex as it is - let's not encourage the idea that they need more power to abuse less.
4 notes
·
View notes
Text
While I'm sharing some of the AIHW figures from: https://www.aihw.gov.au/family-domestic-and-sexual-violence/resources/national-plan-outcomes Take a look at this one:

https://www.aihw.gov.au/family-domestic-and-sexual-violence/resources/national-plan-outcomes/women-are-safe-respected-and-equal Never going to convince me that women "making bad choices about partnering" is a bigger factor in women staying in bad and/or coercive relationships than their access to alternatives that don't severely compromise their quality of life. Maybe they aren't "brainwashed" - maybe they'd rather the known quantity of getting hit every now and then with relative financial stability over risking homelessness.
3 notes
·
View notes
Text





Obviously this isn't the detail we expect to see later but I think it's interesting to see the focuses and framing here. On the face of it, the "supporting women in their daily lives" section seems a little lazy - women and men both got the income tax reduction. Labor's redirection of more of the benefit to lower income earners (compared to the Lib's policy) probably did benefit women more than men (I'm guessing - due to women's typically lower incomes). The statement "tax cuts for every woman taxpayer" doesn't really tell us much about whether the benefit of these tax cuts favoured women or men more. Maybe that will be addressed in that section. In health, I don't see IVF as something that should be publicly funded so.... & given that in a heterosexual relationship both a man and a woman will be gaining a child but the woman is the one who takes on all the risks of the IVF procedure... is this really to women's benefit? Honestly I could do a whole other post on this and the use of the fertiqol scale to justify this as increasing health related quality of life. Just take a look at one of the questions in it: "Are you and your partner affectionate with each other even though you have fertility problems?" In the gender-based violence section, which uses a stat about women being killed, the rest mentions "women and children" twice, no mention of girls specifically and we're told "Working with men and boys". Women are framed entirely passively. I doubt this was intentional but isn't it telling. I'll see if this changes in that specific section.
3 notes
·
View notes
Note
Why exactly do you think it’s bad to draw parallels between the treatment of women and other groups? For example, liberals rightly criticize the use of “all lives matter” by conservatives but then turn around and say things like “feminism is for everyone” and “people’s march”. Pointing out the hypocrisy on display is a vital component to countering it.
Also, pointing out how many groups are dominated by the voices of men (including liberal feminism), and suggesting that this is why liberals show visible support for them while rejecting other feminist movements is an example of intersectionality not an abandonment.
I assume this is about https://www.tumblr.com/rad4learning/775513690860601344/its-embarrassing-when-radblr-uses-other this?
I’m not against any instance of drawing parallels. I do think that radblr has a repeated pattern of flippantly suggesting that groups advocating against [other form of structural disadvantage] are taken seriously and not subjected to attempts to undermine them. E.g. “people wouldn’t tell antiracist groups they need to include white peoples” “people wouldn’t say homeless people chose their lot” “people wouldn’t say you can’t hate the rich”. We don’t need to assume other movements are treated “fairly” in rhetoric to critique that feminism is often not.
I think downplaying the difficulties faced by other movements to reduce or eliminate systemic disadvantage due to some characteristic is not just unnecessary but also bad. For one thing, most women are multiply disadvantaged and we risk alienating many of these women when we downplay issues they, or those they care about, face. I think it also weakens radblrians’ ability to develop more integrated theory. I do not believe it’s “feminisms’ job” to fix other forms of entrenched disadvantage but that doesn’t give a moral or pragmatic pass for undermining the fights against them.
On that note, another pet peeve of mine is “the top one percent” being implicitly used to mean “the top one percent in wealthy countries” and not “the top one percent globally”. I think there are lots of little assumptions, little positionings, that reflect that although most women are multiply disadvantaged, many of us are also multiply advantaged.
It’s embarrassing to pass around unsupported claims of other disadvantaged groups having their theory treated better so that we look more victimised by comparison. I suspect it often comes from low exposure to the difficulties faced by the group in question. We have well-substantiated evidence we can lean on for women being disadvantaged - we don’t need to build on sand.
#anon#r4l thoughts#also I’m struggling to understand the thought process behind your second paragraph
4 notes
·
View notes
Text
Decided to try creating a community for feminist analysis focusing on sex-society interaction. More info in the about. Public now because I didn't know what to pick and I can always change it to private later. There is a list of default assumptions in the about that discussions should assume apply. One of these is about people not being innately more or less moral by dint of what group they were born into. This includes males. "Males tend to be more evil because [discussion about sex-society interaction]" <- suitable for this group. "Males are evil because y chromie" <- not suitable for this group. There should also be deemphasis on direct psychologic explanations in favour of analysing societal structures. For example "women's oppression is perpetuated by wearing makeup because dumb women want to be pretty" is less suited than "women's oppression is perpetuated by wearing makeup, which in term derives from greater pressure to have people like you if you have less power". If you still want to argue that women/feminists have an obligation to go against these norms that's fine btw - just make sure you keep away from an innate psychologism or conformity only framing.
I can't guarantee that I'll do much policing and this may be a disaster or never take off but if you're interested feel free to click for an invite or you can send me a message.
#r4l thoughts#also I'll be camping this weekend so if you don't get a quick response that might be why#I don't guarantee quick responses in general and my blog vast majority runs off a queue
4 notes
·
View notes
Text
Sometimes it is grounding to remember that ideas around social change & activism are often coming from and being shared by people who have never so much as attended a public talk or vigil or sat on a committee.
#If this is you you can change that! You don’t have to change the world. You don’t have to sign up for a recurring commitment.#The in-post examples are examples only#r4l thoughts
2 notes
·
View notes
Text
I thought I'd talk/speculate a bit more about this study:
Joshua E Lewis, Amani R Patterson, Maame A Effirim, Manav M Patel, Shawn E Lim, Victoria A Cuello, Marc H Phan, Wei-Chen Lee, Examining gender-specific mental health risks after gender-affirming surgery: a national database study, The Journal of Sexual Medicine, Volume 22, Issue 4, April 2025, Pages 645–651, https://doi.org/10.1093/jsxmed/qdaf026
It's a retrospective observational study using data aggregated from electronic medical records. They use ICD-10 codes to identify mental health conditions and to identify people with listed gender dysphoria diagnosis, as well as to identify gender affirming surgery procedures.
They specifically made sure "Patients included in the analysis had no documented mental health disorder diagnoses prior to the index date."
Classifications as male/female are based on the documentation and so may refer to sex or to gender id.
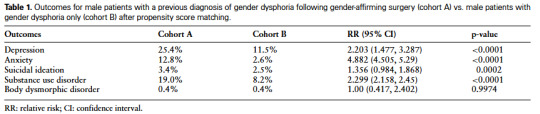
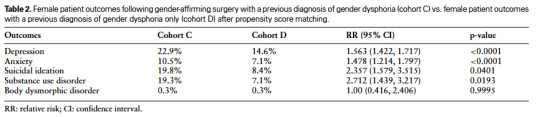
In addition to looking at these tables directly for the comparisons (in each case receiving surgery being a predictor of increased likelihood to receive one of the specified mental health diagnoses - excluding body dysmorphic disorder) I think it's also interesting to look at the vertical comparisons. Aside from suicidal ideation - and for B and D anxiety - a lot of the outcomes are looking pretty similar between A and C as well as between B and D.
If we accept the argument that transmen are much more likely to pass than transwomen, then I think it becomes very difficult to claim that the results are due to not passing or "being visibly trans" in transphobic society - if they were, wouldn't we expect them to be more different by documentation as male or female? I think that would also raise the question of, wouldn't those without surgery be less likely to pass and therefore more likely to have poor outcomes if it's about "not passing" being harmful?
One of the important assumptions for identifying a causal effect is positivity, i.e. could everyone in the non-surgery group have been in the surgery group? Here the barriers I can think of preventing surgery would not explain having decreased mental health disorder. One way that the positivity assumption can be violated, is from people being in too poor health to be recommended a treatment, but again that's not going to explain lower mental health disorder incidence in the non-surgery group. The closest I can come is contact with the health system - except that we know everyone involved is in contact with the health system otherwise they wouldn't make it into the data in the first place.
We could argue that the surgical group would be in more contact than the non-surgical group, but if they have had an uncomplicated operation, wouldn't they be more likely to have more contact in the lead up to the surgery than after (and hence the disorders likely would have been already picked up prior and these participants excluded from the data)?
Another important assumption is exchangeability. The key question here is "do the groups vary systematically in a way that matters to the outcome?". The authors attempt address this using prosperity score matching on age, race and ethnicity. The authors acknowledge that there may have been preexisting differences between the groups: "By excluding patients with documented pre-existing mental health diagnoses, this study sought to ensure that identified mental health outcomes likely represented new or emergent conditions rather than pre-existing disorders. This methodological approach was critical to focusing on the relationship between gender-affirming surgery and mental health. However, we acknowledge that this approach, relying solely on ICD-10 codes, may not fully account for undiagnosed or subclinical conditions prior to surgery. These emergent mental health issues may result from a multifactorial interplay of social, psychological, and physiological factors, including social support systems, environmental stressors, hormonal changes, surgical outcomes, and the broader psychosocial adjustments involved in transitioning."
My question is - ok, let's say that those seeking surgery had systemic differences in terms of e.g. environmental stressors. Even complex systems can be broken down into what kinds of pathways could be responsible. We have three ways to explain why gender affirming surgery, experiencing mental health disorder and some other factor (or combination thereof) are associated pairwise (excluding chance association as it needs to be systemic):
One: A causal relationship. i.e. surgery (directly or indirectly) causes mental health disorder
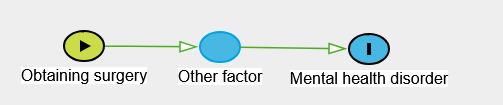
E.g. Obtain gender affirmation surgery -> more likely to have environmental stressors -> more likely to experience mental health disorder. This does not work very well with the argument that gender affirmation surgery is a requirement to for mental health improvement since it implies that surgery worsens mental health. It also implies that controlling for the other factor/s would remove the link between obtaining surgery and mental health disorder. Of course, another option is e.g. factor -> surgery -> mental health disorder or surgery -> mental health disorder -> factor. I don't mention potential pathways with mental health disorder causing surgery because we are told the mental health disorders are increasing after surgery.
Two: A confounding relationship

E.g. Poor social support -> obtaining surgery and also poor social support -> mental health disorder. This implies that gender affirmation surgery is, at least in part, caused by that other factor (i.e. it is not an inevitable outcome). If this factor was disadvantage decreasing access to surgery and also increasing mental health disorder, we would expect to see lower, not higher mental health disorder rates in the surgery group.
Some have argued that preexisting subclinical distress might be this factor. Implicitly, that means that if the subclinical distress was addressed, surgery would be avoided. Often this is paired with the idea that the only way to alleviate the distress is by the surgery. If the surgery effectively relieved distress in these patients, we would not expect "significantly elevated risk of mental health disorders—including depression, anxiety, suicidal ideation, and substance use disorder—post-surgery among individuals with a prior diagnosis of gender dysphoria". Instead, we would expect reduced mental health disorder incidence after surgery.
Three: A collider relationship
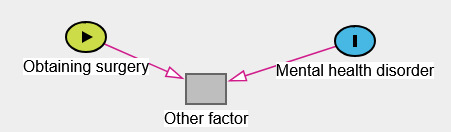
The block here indicates that this variable has been selected on / controlled for - if it wasn't there wouldn't be an association. Here I am struggling to think of good context-relevant examples because much of what has been selected on necessarily predate obtaining surgery and therefore cannot be used as a consequence of surgery. Let's bring in table 3.
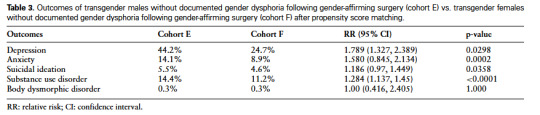
These cohorts showed up in the data as a result of their gender affirming surgeries - they wouldn't have been considered as trans otherwise. Let's consider a new possible causal model. Let's say someone could be motivated to undertake gender affirmation surgery because of trans identity and because of mental illness. If you only looked at the surgical cohort, you could over estimate the association between trans identity and listed mental health disorder.

Finally a note that each of these diagrams represent pathways, the relationships do not need to be direct - there could be various intermediaries.
---- We can't be confident that mental health disorder incidence in people with a gender dysphoria increasing after surgery must be due to the surgery. However, if gender affirming surgery substantially improved the well-being of patients with a gender dysphoria diagnosis, we would expect to see the opposite pattern to what has been observed in this data.
If I have overlooked something / if anyone does believe there is an alternative explanation that I have not considered that explains the patterns in the data, please do let me know.
If there is a confounder, I believe the best response to that is to try to modify the confounder that is driving up mental health diagnoses and surgeries which could have been avoided without it.
2 notes
·
View notes
Text
P values - be wary of what conclusions you draw
Statistics are great - love them - but correctly calculating a number is often easier than correctly interpreting a number. People often have a confidently false understanding of what p-values mean. This is not to say that p values are useless or "don't matter" - just that p values are not the be-all end-all of "does this relationship exist?" "if it does, is it important?". Seeing if a number is above 0.05 or below that is relatively easy - answering these questions is relatively difficult. Blatantly copy-pasting from AMERICAN STATISTICAL ASSOCIATION RELEASES STATEMENT ON STATISTICAL SIGNIFICANCE AND P-VALUES (2016) :
"The statement’s six principles, many of which address misconceptions and misuse of the p-value, are the following:
P-values can indicate how incompatible the data are with a specified statistical model.
P-values do not measure the probability that the studied hypothesis is true, or the probability that the data were produced by random chance alone.
Scientific conclusions and business or policy decisions should not be based only on whether a p-value passes a specific threshold.
Proper inference requires full reporting and transparency.
A p-value, or statistical significance, does not measure the size of an effect or the importance of a result.
By itself, a p-value does not provide a good measure of evidence regarding a model or hypothesis.
The statement has short paragraphs elaborating on each principle."
There is a lot on this statement including:
The ASA Statement on p-Values: Context, Process, and Purpose (If unfamiliar, you may find it most useful to scroll down and read the statement in full first)
ASA President’s Task Force Statement on Statistical Significance and Replicability (2021)
2 notes
·
View notes