#gastrointestinal system notes
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr Inc. is funded by 13 investors.
Text
Activities of Digestion

Patreon
#studyblr#notes#medblr#medical notes#med notes#digestion#anatomy and physiology#anatomy#physiology#digestive system#digestion notes#digestive system notes#chemical digestion#mechanical digestion#gi notes#gastrointestinal system#gastrointestinal system notes#peristalsis#human anatomy and physiology#biology#bio#bio notes#biology notes
2 notes
·
View notes
Text
Writing Notes: Gut Feeling

Gut Feeling - (or intuition) an immediate physical response you feel that suggests the best decision when presented with two or more choices.
Common sensations associated with a gut feeling include:
a sinking feeling or butterflies in your stomach,
sweaty palms,
prickling on your neck,
goose bumps,
muscle tightness or tension,
increased heart rate, or
an overwhelming sense of calm or clarity.
In scientific terms, gut feelings come from the enteric nervous system, a web of neurons in the gastrointestinal tract that some neuroscientists call the “second brain.”
Tips to Help You Decide When to Trust Your Gut
It can be difficult to decide if you should trust your gut. Here are a few tips to help you gauge if trusting your gut is right for a particular decision-making process:
Evaluate your past experience. Research supports that people with extensive experience in a certain field have reliable gut feelings about decisions in that field. If you feel confident you have the intuitive knowledge and experience in a particular situation, your gut is more likely to identify red flags unconsciously and point you in the right direction.
Identify any cognitive biases involved. Cognitive biases and prejudice can factor into your gut feeling. For example, you’re more likely to “get a good feeling” about someone (whether a job candidate or a romantic interest) if they’re similar to you in some way. Take a step back from an important decision and see if your gut may be relying on conscious or unconscious biases or anxieties, and then work to overcome those biases for better decisions overall.
Note the timeline. A key factor in deciding if you should listen to your gut feeling is how much time you have to act. Determine if this is a situation where you need to respond immediately (for instance, at a busy intersection) or if you have time to bolster your gut feeling with logical rationale (for instance, when deciding to rent an apartment). Avoid rushing to make a decision if you have time to consider the options objectively.
Take stock of counterevidence. If you have time to evaluate the situation analytically, consider any contrary evidence that may go against your gut. Consider if this evidence is compelling enough to steer you away and ask yourself what you stand to lose if you regret your decision.
Scenarios Where It’s Valuable to Trust a Gut Feeling
There are a few situations where a gut reaction could pay off, such as when:
The timeline is short: Sometimes, a decision requires a split-second call. In cases like these, your gut can be a good way to make a decisive choice for your well-being, avoiding indecision, overthinking, or panic.
You have previous experience in the field: In areas of your expertise, you have the benefit of experience to inform your gut feeling, which allows you to take mental shortcuts toward the best choices. If you have a strong feeling in a realm you know well, it can be valuable to make an intuitive decision.
You complement it with analytical thinking: In situations where you have time to consider the choice, combine your intuitive feelings with your conscious mind for a well-thought-out decision. If you weigh the pros and cons and each option seems equal, your gut feeling can be a valuable tiebreaker to help you make the best decision.
Source ⚜ Writing Notes & References ⚜ Writing Resources PDFs
#gut feeling#intuition#character development#writing reference#writeblr#literature#dark academia#creative writing#writing prompt#light academia#writers on tumblr#spilled ink#writing ideas#writing inspiration#writing resources
114 notes
·
View notes
Text
Personal associations/interpretations of the dark/mystical houses (4th, 6th, 8th, 12th)


4th house
twisted tree roots, cultural practices, heirlooms, photo albums, inherited features, traditions, the mother, past lives, generational trauma, picture books, garden beds, childhood homes, ancestor altars, hand written recipe books, hearth, squeaky wooden floorboards, genealogy archives, caves, oak trees, baby wrap carriers, emotional security, cultural heritage, building foundations, photo albums, genetics, laundry lines, swing sets, property, mines, crops, sanctuaries, the chest and heart, home steads, fields, farms, root cellars, harvests, pots on stoves, brooms, backyards, agriculture, vines on trellises, handmade blankets, grandparents house, laundry baskets, attachment styles, singing lullabies, history, deep emotions, instincts, the unconscious, summer, waxing moon, vase of flowers, bath time, picking berries, celebrating holidays, chicken coops, older sisters, family gatherings, stone paths, forest walks, ancient structures/buildings, ancestral languages, cupboards, staying in

6th house
vitamins and supplements, morning routines, pharmacies, tasks and lists, doctors offices, health food stores, stomach medicine, hygiene practices, journals and planners, schedules, herbal teas, personal rituals, emergency kits, dog walks, lymphatic drainage, caregiving, donating blood, examinations and checkups, meditation, colour coordination, sticky notes, gastrointestinal problems, folded laundry, labels on everything, retirement homes, hand washing, braided hair, herb gardens, filing cabinets, face masks, kombucha, detailed diagrams, volunteer work, medicine cabinets, cleaning supplies, shelves, acts of service, skin care, organic linen, gauze and stitches, stress-induced illnesses, essential oil/herb baths, house plants, instructions, repetition, holistic medicine, giving advice, yoga studios, "gut feeling," bone broth



8th house
altars, divination, near death experiences, candle wax, feeling crushed by a heavy weight, grave dirt, red/dim lighting, funerals, double income, control, the underworld, cheques, insurance, heirlooms, ghost sightings, power imbalances, crime documentaries, ouroboros, bank accounts, grief and loss, shadow work, the womb, manipulation, scrying mirrors, Russian nesting dolls, keys, mortuaries, tests from the universe, pendulums, crime scene tape, the phoenix, projections, credit scores, animal bones on a forest floor, blood stained sheets, metaphysical shops, spiritual attacks, deep emotions, snakes, dead flowers, late autumn, wedding veils, envelopes, full moon, muddy boots, shadows at the corners of your vision, scarab beetles, inner processing, experiencing crisis, inherited possessions, natural disasters, sexual trauma, psychological studies, ancestral connections, cracked dolls, veil between realms, mental illnesses, deep connections, intimacy, reincarnation, torture devices, keys, whirlpools, the sound of sirens, unconscious fears, intense first impressions, pushing limits, feeling bound, scratches on walls, ten of swords


12th house
abandoned places, liminal spaces, long winters, shadowy figures, reoccurring dreams, repeated patterns, fog-filled forests, self analysation, inner worlds, cave systems, unfinished basements, hallucinations, solitary confinement, empty parking garages, spiral staircases, substance abuse, trapped in purgatory, hidden beneath the surface, maladaptive daydreaming, hospital hallways, confines of society, waning moon, moths, wandering aimlessly, disconnection from the world, psych wards, healing others, tired eyes or dark circles, chronic mental illness, suppression, addictions, hiding places, overnight shifts, unexplainable experiences, past life karma, exhaustion, cobwebs, others projections, catacombs, bird cages, premonitions in dreams, prescription bottles, self destructive patterns, late night walks, misty lakes, the feeling of walking out of the movie theater at night, identity crises, blurred faces, empty public transport, astral projection, comas, diary entries, dissociative episodes, shape shifting, generational trauma, observing people, mirrors, padded rooms, the afterlife, chain link fences, paradoxes, feeling misunderstood, repression or memory loss, hikikomori, the freeze response, disappearance, waiting rooms
#astrology#astrology community#astro tumblr#astro notes#astroblr#astrology aesthetic#4th house#6th house#8th house#12th house
276 notes
·
View notes
Note
Post-viral fatigue: When was it first officially recognized as A Thing? Was it unofficially observed much before then? What did the early documentation of it in medical literature/practice look like? How has our understanding of it evolved?
For this, since it is about history, I'm going to be talking mostly about our understanding of post-viral fatigue syndrome in a pre-covid context.
I have also decided to use sources describing what would later be termed ME/CFS. While viruses are only one trigger for ME/CFS, early reports tended to notice that ME/CFS clustered in outbreaks, which speaks to a viral, bacterial, or parasite trigger (for example, an outbreak of a viral illness happens, then just afterwards, an ME/CFS or post-viral syndrome outbreak does).
Finally, it is important to note that viruses are not the only infectious agent that can cause a fatigue syndrome. Bacteria (particularly strep) and even parasites (most notably giardia and malaria) have been known to cause it. As this is a history post, it generally will not be possible to differentiate the cause of any given outbreak, so I'm kind of lumping them in together.
------------------------
Let's begin:
Between 1860 and 1880, a new disease arrived on the scene. It was called neurasthenia, and it was described:
Neurasthenia is a condition of nervous exhaustion, characterised by undue fatigue on slightest exertion, both physical and mental, with which are associated symptoms of abnormal functioning, mainly referable to disorders of the vegetative nervous system. The chief symptoms are headache, gastrointestinal disturbances, and subjective sensations of all kinds.
It probably wasn't actually new, but instead first recognized here due to the recent industrial revolution and change in work patterns. It was considered to strike upper-class men (as a consequence of their hard mental work) specifically, and thought not to strike the lower classes, women, or racial minorities (who surely never engaged in such work).
Between 1880 and 1900, in the UK, explanation after explanation was posited as the reason for the illness. It was due to overwork, or underwork. Due to a lack of electrical energy. Due to a physical insult like an infection or metabolic disturbance. Due to the law of thermodynamics playing out in the body. Basically, if the scientific community found a new cool theory, it was applied to explain neurasthenia. None of these, however, were able to be definitively proven with the technology of the time.
One thing, however, was consistent- the treatment. Like a number of other illnesses, it was sending someone to a retreat, rest home, or other place where they could experience physical and mental rest. This is also the first time "chronic fatigue" was used in the literature. Based on what we know today, this was probably a good option.
By the early 20th century, unable to find an explanation that stuck, however, physicians threw their hands up. It was all just a weird form of melancholia, they said. It is important to note here that psychiatry and neurology would not become distinct fields until after WWII. So it was mostly neurologists saying "hey, we can't figure out what causes this, so we're going to lump it in with another thing we can't figure out the cause of that also makes people stay in bed all the time."
This was followed very swiftly by other physicians, several of whom had neurasthenia themselves, advocating for it to continue to be considered it's own separate neurological condition. Unfortunately, the melancholia label stuck, and the view of it as an upper class disease that only affected men quickly flipped to one that was only experienced by the lower classes and women.
Whether understood as physical, mental, or a combination, however, the early 1900s brought with it another explanation for the problem- febrile illness. It was noted that chronic fatigue syndromes frequently followed malaria, flu, and other illnesses that caused fever. This was not the first time this had been postulated, but it was the first time it attained widespread acceptance. The lack of persistence of the culprit (at the time bacteria or parasite), however, only lent more credibility to the idea that it was mental in nature, and it was largely forgotten about.
In 1934, a series of outbreaks of what was thought to be an abnormal form of polio struck around the world. Once it was differentiated, it would be named epidemic neuromyasthenia. This was seen as a brand new illness, not connected to neurasthenia.
By the 1950s, the term had changed to "benign myalgic encephalomyelitis", which was chosen due to
the absent mortality, the severe muscular pains, the evidence of parenchymal damage to the nervous system, and the presumed inflammatory nature of the disorder,
as described in a 1959 paper on the subject. It was recognized that the disease came in both epidemic and sporadic cases, but the scientific community wasn't entirely sure what caused it. Still, the number of papers about it suggested they were looking (unfortunately, most of these papers are not available, even in abstract form).
The next problem happened in 1970. Two psychiatrists named McEvedy and Beard wrote a paper that analyzed an outbreak that occurred in 1955, proclaimed it a case of mass hysteria without talking to any of the patients, and retroactively concluded that all previous outbreaks dating back to 1934 had also been mass hysteria. Over the next 8 years, there were many papers vehemently refuting this claim, by at least 5 different authors that I could find.
Unfortunately, instead of the rebuttals cementing McEvedy and Beard as not knowing what they were talking about, it created a deep rift in the scientific community: did the disease belong to psychiatrists, neurologists, both, or someone else entirely?
People working on the physical end in the 1980s pointed to high rates of viral titers for specific viruses, circulating immune complexes, muscle biopsies showing necrosis, abnormal jitter potentials, and abnormally early acid production during exercise, among other things. Basically, there's something wrong with how the immune system is working, and also something very wrong with the physiology of the muscles.
People working on the mental end pointed to mass hysteria and high rates of anxiety, depression, and emotional liability in people with myalgic encephalomyelitis, combined with a then relatively new understanding that mental illness sometimes does wonky things with the immune system.
Note that, for the mental end of things, some of the sources cited in these papers are exceptionally old for scientific papers, like, going back to neurasthenia days and the original 1900s explanations of neurasthenia as melancholia.
Because the two camps couldn't get along (I have no proof, but I know neurology and psychiatry fought like cats and dogs for long swaths of the 20th century, so it honestly might have been a professional scrap that made this illness so fraught), "post-viral syndrome", and later "post-infectious fatigue syndrome" were coined because they didn't specifically point to physical or mental being the primary reason for the syndrome.
And this argument continued into the 2020s, and in some cases until today. The COVID-19 pandemic did finally settle it largely into a physical illness with some psychological features (rather than a psychological illness with some physical features). But it can still be exceptionally difficult to get diagnosed and correctly treated depending on where a person is and what doctor they have.
In conclusion, the history of post-infectious fatigue syndrome has gone through many names and many phases, and there was a lot to the story I wish I could have covered in this post, but it was already really long. Hopefully this gives you some understanding of the social and scientific history of this syndrome.
43 notes
·
View notes
Text
preserved in our archive
By Jason Gale
Hi, it’s Jason in Melbourne. Almost five years after Covid‑19 broke out, scientists are still unraveling its pathological modus operandi. Before I get into that...
Toxic blood effects Clotting disorders in Covid patients were spotted by researchers in China in early 2020, but the true extent of the risk only became clear when even patients with mild respiratory symptoms began experiencing strokes.
At first, doctors suspected these clots might result from a “cytokine storm” — an intense immune response releasing a surge of inflammation-signaling proteins. Others noted that the virus could directly damage blood vessel linings.
But Katerina Akassoglou, a neurovascular brain immunologist at the Gladstone Institutes and UC San Francisco, wasn’t convinced that the virus itself wasn’t a cause.
Navigating social distancing requirements that complicated lab work, Akassoglou and her collaborators conducted a series of experiments in mice to explore the pernicious role of the coronavirus’s spike protein.
They discovered that beyond serving as the virus’s “key” to enter cells, spike binds with a blood clotting factor called fibrinogen, creating structurally abnormal, inflammation-promoting clumps of fibrin — the insoluble material that forms the mesh-like structures essential for wound healing.
High levels of these abnormal clots not only push the body’s clotting system into overdrive, increasing clot formation and inflammation, but also suppress natural killer cells — the immune system’s virus-clearing soldiers.
When this damaging cycle occurs alongside a breakdown in the protective layer of cells around the brain’s blood vessels, toxins and bloodborne proteins, including fibrin, can seep into the body’s most vital organ. Once there, these substances activate microglia — the brain’s immune cells —which begin attacking healthy brain cells, contributing to the neurological symptoms of long Covid.
Akassoglou had been studying this damaging cascade for decades in patients with Alzheimer’s disease and multiple sclerosis. Still, until SARS-CoV-2 came along, she had no idea it could be triggered by a viral infection.
“For some reason, this virus has evolved to interfere with the coagulation system in a way that other viruses do not,” she told me. Fibrin’s role in driving toxic inflammation is common in many diseases, but “in the presence of spike, it gets a lot worse.”
In experiments with mice lacking fibrinogen, Covid leads to much less inflammation, and the infection clears faster. “Studies suggest that if you deplete fibrin, inflammation improves, no matter what initially triggers it.”
Although Akassoglou’s focus has been on the brain, she’s hopeful this research will be expanded to understand the effects on the heart, liver, kidneys, and gastrointestinal tract.
In the meantime, she’s developing a way to halt this damaging reaction. A first-in-class antibody treatment designed to specifically block fibrin’s toxic effects entered early-stage patient studies in May, with no reported safety concerns so far.
Results are expected next year and could lead to more advanced clinical trials to test the immunotherapy’s potential to treat not only long Covid but also other serious diseases like multiple sclerosis and Alzheimer’s.
#long covid#covid 19#pandemic#covid#mask up#public health#wear a respirator#still coviding#wear a mask#coronavirus#sars cov 2#covid conscious#covid is airborne
67 notes
·
View notes
Text
Answers to: Post #108 (System Rules)
[pt: Answers to: Post #108 (System Rules)]
Since these were not posted yet, sorry about that. I hope you enjoy, and that to some, this might be helpful. This is a very long post.
Note that some of these include potentially triggering subjects. Some of these topics include: alcohol, smoking / nikotin, drugs, intrusive thoughts (about inappropriate relationships / feelings), and slurs.
Please read carefully.
- 🌱 Avery


"If you choose to eat it, you must front during the gastrointestinal consequences."
"No birds in the house."
"Check the archive to see how much caffeine we've had today before consuming more caffeine."
"Don't get us arrested without unanimous consent of all frequent fronters."
"Decisions that affect our general wellbeing in major ways should be discussed as a group."
"No matter what skin color, mental disability or any other factor that gives you rights to a slur you should not say that slur if the body isn't allowed to say that."
"No using profanity or crude language outside of headspace but, avoid saying many curses in front of headmates under 14."
"Respect alters boundaries."
"If you are at front and a new alter shows up, please tell them what is going on and help them set up a profile on Plural kit & Simply Plural."
"Anyone our announcers and or gatekeepers have marked off limits , we aren’t allowed to talk to OR we have to be cautious around."
"As a system we have a very high justice system. Not In the way we have trials but in the way we have councilmen for every layer of the system. The rule is to always respect the rules of the overseer in that layer. Not in a dictator or whatever way , just like make sure to keep the place clean and shit."
"If you have a job in headspace you should always make sure it’s something that doesn’t require money (we don’t have such a thing in headspace). If you have a job related to that we just have trades or give stuff away for free."
"If you encounter anyone that’s not the main partner in our partner system , just be safe n ignore em unless they say hi"
"Always go to a higher up if you want a prnscc made or a card or an anything like that."
"Anarchy: no hierarchies, no one is "in charge", no one "owns" the body or life, collaborative, consenting, compassionate."
"Take care of the little."
"Respect our collective friends."
"Avoid damaging the body (e.g. no smoking)"
"Respect each other's beliefs, privacy, and wishes/boundaries. Don't try to disprove everyone you disagree with. Don't go trying to recall other people's memories, or try to watch when they want privacy."
"Maintaining the body + the singletsona are of utmost importance. Follow the pre-set routine as best as possible when involved in front."
"Don't be a dick. Especially do not be a dick to the short list of system friends; they are the trusted few and these relationships are to be preserved. Before engaging in public spaces make sure you know or can otherwise internally access the local etiquette. Do not damage or remove meatspace belongings. Respect closed doors within headspace."
"The external world does not have the same understanding that the internal one does- some things must be hidden for the continued peace and/or online safety of the system. (eg, Fakename1, bi lesbian, should not get involved with identity discourse. Fakename2, a fictive who was considered a grown adult in her source world but is a minor in this one, cannot interact with nsfw spaces/content and express her sexuality without claiming the body's age instead of her own.)"
"We made it a rule to not get apps or make purchases online without consulting others. This is in part to help make sure impulse purchases are less likely, as well as to help give some protection against viruses and such."
"We use Lighthouse, which allows each member to keep their own private journal. We made an agreement that we wouldn't look at anyone else's journal without their express permission, which we don't ask for unless we have to. This is primarily so we don't have to deal with individual passwords, but we've also carried this over onto other sites, such as chatrooms on Simply Plural, which are chats that are meant for us to have private conversations, and no one is allowed to look in a chatroom they aren't a part of unless invited in another channel."
"We decided that we would keep any and all in-system romantic relationships private. We've seen a lot of people being weird about them, and we didn't want to deal with that. We made this rule when two of our members decided to start dating. We've considered extending this rule to *any* in-sys relationship, as we've seen others being weird about even siblings who are siblings in-source, but at the moment it's just romantic relationships we keep private."
"Our main rule is no self-harm that could permanently damage the body, and no putting the body in situations you know are dangerous."
"As an adult system, we do allow our system members to drink, but the rules remind them that the body's tolerance is low. As drugs including weed are illegal where we live, it is against the system rules to have them, or smoke nicotine."
"Follow server rules is another one, which includes a subclause about persecutors not being an asshole to people we like to try to push them away."
"In our system we allow tattoos, piercings, and hair dye, but we ask that system members think about what would look nice on the body rather than just what they want. We kinda view the body as a dress up doll."
"Be kind and considerate to other members and to people outside the system unless necessary / it's to avoid harm to another or ourselves - this includes asking everyone involved with something that happened for permission for sharing details about said thing, especially ones that are more personal to them, not joking about, say, someone's source if they don't want it even mentioned, etc."
"if there are walk-ins asking to join the system (because our system works like that,) we need to make sure everyone consents to them being around, ESPECIALLY people who oppose them / the orgs they're a part of insource (ex: our hsr boothill fictive when considering IPC members, etc.) we can't exactly just disengage if we're uncomfortable, as our ability to hold our mental tongues / walk away from insys conversation is unreliable at best and just useless at worst, so we're extra careful with who we consider part of the system."
"no claiming to be Literally Part of X Culture when we're bodily not. members can, like, unclaim our bodily race / culture if they feel like it - most of us don't resonate with the body's ethnic experience, even if we do live it - but claiming to be say, black when we're actually 100% not black will never be on the table. this also means no joking about other people being X race, no making comments, etc."
"no purposely using slurs / derogatory terms towards other members or other people irl. if we know something is a slur and someone uses it as an insult knowing it's a slur, that's breaking this rule."
"no yelling or screaming / argue quietly and don't be mean about it, even if someone's being stupid. this one actually started as a way to tiptoe around trauma triggers (waves in trauma holder host) but then we realized that this has 100% helped our own conflict resolution skills and made it an actual thing."
"if someone brings up something they want to do and the brain pushes back, it's off the table 100% until further notice. we have autistic PDA so it's not like it's just a preference; we literally can't branch out that much."
"if two people are hanging out alone in front and are not partners, they must call another person to be a "buffer" the moment someone catches intrusive feelings for another, especially if they're siblings and/or if one is an adult and the other is a minor. i know!! this sounds extremely problematic! so some context: sometimes, our OCD will force members to get crushes on other members, especially if the one of them is being hyperfixated on, and it's always with people that cannot date without one or both going to jail. **it's not something we want**; it shows up and goes away at random and everyone involved hates it the entire time, but we have to deal with it anyway so that's why we have this rule. attempts to just. walk away from co-con for the time being and wait it out just don't work because they'll just teleport back, so we call up a buffer (90% of the time one of the people involveds' actual partner, because of course the brain chooses people in existing relationships too) to distract the brain with jangly headmate-shaped keychain."
"No one is allowed to touch alcohol or drugs."
"Do not intentionally do anything to harm self or others."
"Cursing is banned(with exceptions for words we are more comfortable with)."
"Any breaking of the rules will result in a temporary ban from fronting or certain areas of the inner world depending on where the rule breaking took place."
"All other major decisions must be put to a vote"
"Take the meds everyday"
"Respect the headmates' relationships"
"Respect the body"
"Reach out to our partner systems if needed or in danger"
#endo safe#plurality#system#plural#plural system#pro endo#pluralgang#plural stuff#long post#cw#content warning
70 notes
·
View notes
Text

Paramedic Incident Report
Incident Number: 2024-19245 Date: December 6, 2024 Time of Call: 15:23
Incident Location: ClimbX Indoor Gym, 345 Summit Street, Boulder, CO
Patient Information:
Name: Daniel Carson
Age: 20
Gender: Male
Height: 5'11"
Weight: 165 lbs
Physical Description: Lean and muscular build with well-defined arms and torso typical of an experienced climber. Short dark brown hair, light complexion.
Description of Incident: At 15:23, dispatch received a 911 call reporting a young male climber had collapsed while bouldering at an indoor climbing facility. The patient was reportedly scaling a mid-level climb when witnesses described him suddenly clutching his chest, losing his grip, and falling to the mat below. He was unresponsive upon initial assessment by gym staff.
Initial Assessment Upon Arrival (15:30):
Level of Consciousness: Unresponsive
Pulse: Absent
Respiratory Effort: None
Skin Condition: Pale, cool, and clammy
Pupils: Fixed and dilated
Bystanders reported that staff initiated CPR immediately after the collapse and delivered one shock using the facility's automated external defibrillator (AED).
Treatment at Scene (15:30-15:45):
CPR: High-quality chest compressions continued upon paramedics’ arrival.
Airway Management: Airway secured with a bag-valve mask; oxygen at 15 L/min.
AED Analysis: AED advised one additional shock, which was administered at 15:35. Return of spontaneous circulation (ROSC) achieved at 15:37.
Vital Signs Post-ROSC:
Pulse: Weak and irregular at 45 bpm
Blood Pressure: 80/50 mmHg
Respiration: Shallow and labored at 10 breaths/min
Oxygen Saturation: 78%
Transport Summary (15:45-16:00): Patient was loaded into the ambulance for transport to St. Anthony's Hospital. During transport, the patient exhibited further signs of cardiac distress. At 15:50, he experienced ventricular fibrillation (VF).
Intervention: CPR resumed, epinephrine 1 mg administered IV, and defibrillation attempted twice.
Outcome: No ROSC achieved after second cardiac arrest.
Time of Death: 16:00
Remarks: The patient suffered two cardiac arrests within a 30-minute period, likely indicative of a severe underlying cardiac condition. Efforts to stabilize were unsuccessful due to continued arrhythmias and compromised circulation.
Autopsy Report
Case Number: 2024-AU-1245 Date of Examination: December 7, 2024 Time of Examination: 09:00
Name: Daniel Carson Age: 20 Height: 5'11" Weight: 165 lbs Sex: Male Race: Caucasian
External Examination:
General Appearance: Well-developed and muscular young male. No evidence of external trauma except for mild abrasions on the back of hands and forearms, consistent with climbing activities. Skin pale with slight cyanosis around the lips and nail beds.
Scars/Marks: None significant.
Tattoos: None noted.
Clothing: Patient arrived wearing climbing shorts and a tank top.
Internal Examination:
Cardiovascular System:
Heart: Enlarged, weighing 420 grams (average for age/weight: 300-350 grams).
Valves: Mitral valve revealed significant calcification and fibrosis, indicative of a congenital defect. The defective valve exhibited stenosis, which restricted blood flow and created turbulent circulation.
Coronary Arteries: Severe occlusion (95%) of the left anterior descending (LAD) artery due to atherosclerotic plaque.
Myocardium: Evidence of acute ischemic changes and scarring, suggesting prior silent infarctions. The ventricular walls were thickened (hypertrophic cardiomyopathy).
Aorta: Normal caliber and appearance.
Respiratory System:
Lungs congested, with frothy fluid in the trachea and bronchi.
Right lung: 450 grams; Left lung: 430 grams.
Gastrointestinal System:
Stomach contained approximately 200 mL of partially digested food.
No abnormalities in the esophagus, stomach, or intestines.
Central Nervous System:
Brain weight: 1,450 grams. No gross abnormalities.
Other Organs:
Liver: Enlarged (1,600 grams), possibly due to mild congestion.
Kidneys: Unremarkable.
Spleen: Normal size.
Microscopic Examination:
Heart Tissue: Acute myocardial infarction visible in sections of the left ventricle.
Coronary Arteries: Advanced plaque buildup with rupture and thrombus formation.
Mitral Valve: Fibrotic thickening and calcification evident.
Toxicology:
No evidence of drugs or alcohol.
Summary and Cause of Death: Daniel Carson, a 20-year-old male, died from complications of a congenital mitral valve defect and severe coronary artery disease. The primary event was a massive myocardial infarction triggered by the blockage of the LAD artery. A second cardiac arrest during transport proved fatal.
Final Diagnosis:
Acute myocardial infarction secondary to LAD artery occlusion.
Congenital mitral valve stenosis and calcification.
Hypertrophic cardiomyopathy contributing to cardiac instability.
Cause of Death: Cardiac arrest due to a defective valve and blocked artery.
Manner of Death: Natural.
Signed by: Dr. Margaret Li, MD Pathologist
28 notes
·
View notes
Note
Im now curious about Pepperman and Martha's kid
I know a fact that some peppers have smaller green/unripe peppers growing inside
------------------------------

Hehe funne *clears throat*

✨✨Pepper anatomy✨✨
How did baby came to be? Let's find out!
TW (?): Biological themes ahead ( nothing explicit but still)

As you can see in the picture above, a Pepper's reproductive organ is connected to their gastrointestinal system.
This organ is commonly called a "Seed bed" but the scientific name is "Pistil"
Note: All of this applies to most of The Tower's Plant folk.
The Pistil's walls are bumpy and soft, Females grow seeds while Males secrete a goo-like pollen, due to their unusual anatomy, Plant folk intercourse is basically french kissing and both the Female and Male are capable of carrying the seedling.
If the insemination is successful then approximately 4 months later, whoever ended up with the seed, they start coughing up the seedling.

The seed must be planted and taken care of to ensure the proper development of the Pepper.

As the months go by, the seed becomes a plant and it grows, at the 6 month mark it first develops the pepper itself, Is very rare for the plant to develop more than one pepper.
After that the pepper gains mass and becomes heavier until, at the 9 month mark, it's touching the soil and the Baby is really to open its eyes, stretch it's limbs...

And cry for the first time.
Now who is that baby? That lil baby girl :)

Well, She is Whitney Pepperman Chiev, Phil Pepperman and Martha Chiev's daughter.
She is 7 years old.
The discolored mark is merely a mutation (Phil and Martha feared it was a birth defect or a mold, but no, she is completely healthy)
She has the same emerald eyes as her Grandmother (Phil's mom) but she doesn't really know her.
Wishing to be a famous artist of some kind when she grows up, like her parents!
She is best friends with Alex
So yeah that's Phil's daughter and he loves a lot :3
And of course the biology headcanons and my weird ways to explain the nature of the tower folk 😃👍
Next up are the Spaghetti kids and the Noises kid :0
Kay that's all for today's post
Buh-bye!!
#pizza tower#pizza tower au#pepperman#pizza tower pepperman#phil pepperman#Pizza tower Martha#Martha Chiev#pizza tower oc#Pizza Tower Whitney#Whitney Pepperman#ask blog#pls send asks
27 notes
·
View notes
Text
Socks off bagel being toasted prime defenders season 2 in my headphones gastrointestinal system notes after this life is AWESOME
7 notes
·
View notes
Text
How Does The Drug Got Excreted / Eliminated From The Body?
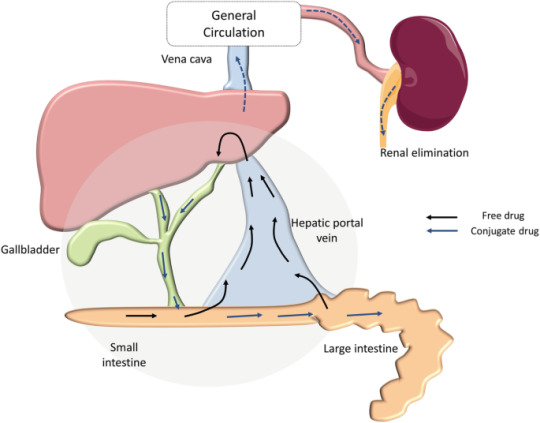
Drug excretion is an important process in pharmacology, encompassing the elimination of pharmaceutical substances from the body. While the ultimate elimination of all drugs is inevitable, the specific pathways involved can vary significantly. Some drugs undergo extensive metabolic transformations before being excreted, while others are expelled from the body in their original form.
The kidneys play a central role in excreting water-soluble substances, effectively filtering them from the bloodstream. Meanwhile, the biliary system handles drugs that remain unabsorbed from the gastrointestinal tract, providing an alternative route for elimination. Although excretion through auxiliary channels such as the intestines, saliva, sweat, breast milk, and lungs is typically minimal, certain volatile anesthetics and residual drug traces in breast milk can have notable impacts, particularly on vulnerable populations such as infants.
Renal excretion constitutes a significant portion of drug elimination, accounting for approximately 20% of the plasma that is filtered through the glomeruli. While most water and electrolytes are reabsorbed back into circulation, polar compounds like drug metabolites are excreted predominantly in urine. However, it’s important to note that renal excretion tends to decrease with age, necessitating careful dosage adjustments for elderly patients to mitigate potential adverse effects.
Numerous factors influence the process of renal excretion, including the extent of protein binding, the degree of drug ionization affecting reabsorption rates, fluctuations in urine pH that can alter excretion dynamics, and the impact of metabolic inhibitors on tubular secretion mechanisms.
Biliary elimination, on the other hand, occurs when drugs traverse the biliary epithelium via active transport mechanisms. However, this process is not without limitations, as transporter saturation can impose constraints on drug excretion rates. Typically, larger molecules containing polar and lipophilic groups are excreted through bile, while smaller molecules tend to favor renal elimination pathways.
In addition to renal and biliary routes, drugs may also be eliminated to varying extents through auxiliary pathways such as saliva, tears, feces, sweat, and exhalation. While the quantities eliminated through these routes are generally minimal, drug excretion in breast milk can pose significant concerns for lactating mothers, potentially exposing nursing infants to pharmacological agents.
Understanding the pharmacokinetic parameters governing drug excretion is paramount for optimizing therapeutic regimens and minimizing the risk of adverse effects. Key parameters include the rate of elimination, clearance, elimination rate constant, and biologic half-life for drugs undergoing first-order elimination kinetics.
In conclusion, drug excretion represents a broad process influenced by a myriad of factors, necessitating comprehensive consideration to ensure the safe and efficacious use of pharmacotherapy.
For medical students navigating the complexities of their studies, Expert Academic Assignment Help serves as a beacon of professionalism and expertise. With a steadfast dedication to excellence and competency, our team provides invaluable support and guidance tailored to your academic needs. Do not hesitate to reach out to us for assistance on your academic journey, email: [email protected]
Your excellence our pride.
#assignment help#medical students#healthcare#nursing school#nursing student#medicine#medication#health and wellness#health#homework help#do your homework#university student#medical school#online writing#academic assignments#academic writing#grad school#pharmacy student#pharmacology#pharmacy technician#pharmacy
29 notes
·
View notes
Text
Diverticulitis
-- caused by hard stool putting more pressure on the colon
-- this opens tears in the tissue
-- the most common cause of lower gastrointestinal bleeding in the United States
-- blood is usually bright red
-- passage of blood is typically painless
-- main symptom is abdominal pain
-- pain is usually localized to the left lower abdomen
-- infection -> fever -> malaise -> body aches -> chills -> nausea -> vomiting
-- infection may result in constipation and bowel obstruction
-- obstruction can perforate affected colon segment
-- fecal matter can then enter the abdominal cavity
-- perforation can lead to: -> peritonitis -> severe infection -> septic shock
.
Patreon
#studyblr#notes#medblr#medical notes#gi pathology#pathology#pathophysiology#diseases and disorders#diseases#gi diseases#gi disorders#gastrointestinal system#digestive system#digestive system disorders#gastrointestinal disorders#gastrointestinal diseases#diverticulitis#medicine#medical care#anatomy and physiology#anatomy#digestive system anatomy#infection#septic shock#peritonitis
0 notes
Note
heya!! Was wondering if you had any tips for writing characters going through withdrawal? Sorry if it's a weirder ask, but would a symptoms list be possible? Thanks in advance!!
Writing Notes: Withdrawal Symptoms
Withdrawal - Substance-specific physiologic effects, symptoms, and behavioral changes that are caused by stopping or reducing the intake of a substance.
It is a pharmacologic symptom in which untoward physical effects occur when the drug is stopped or when it is counteracted by a specific antagonist
Substance Withdrawal - A syndrome that develops after cessation of prolonged, heavy consumption of a substance.
Symptoms vary by substance but generally include:
physiological,
behavioral, and
cognitive manifestations, such as nausea and vomiting, insomnia, mood alterations, and anxiety.
DSM–IV–TR identifies 6 drug classes associated with withdrawal:
alcohol,
amphetamines,
cocaine,
nicotine,
opioids, and sedatives,
hypnotics, or anxiolytics.
DSM–5 and DSM-5-TR list
tobacco in place of nicotine and
further identify caffeine and
cannabis as being associated with a withdrawal syndrome.
To be classified as a substance-withdrawal disorder,
the withdrawal syndrome must cause the patient significant distress and/or impair functioning (e.g., social, occupational).
Most patients with withdrawal recognize that readministering the substance will reduce their symptoms.
ALCOHOL WITHDRAWAL
Alcohol Withdrawal - Symptoms that may occur when a person who has been drinking too much alcohol on a regular basis suddenly stops drinking alcohol.
These symptoms tend to occur within 8 hours after the last drink, but can occur days later. Symptoms tend to peak by 24 to 72 hours, but may go on for weeks.
Common alcohol withdrawal symptoms include:
Anxiety or nervousness
Depression
Fatigue
Irritability
Jumpiness or shakiness
Mood swings
Nightmares
Not thinking clearly
Other alcohol withdrawal symptoms may include:
Sweating, clammy skin
Enlarged (dilated) pupils
Headache
Insomnia (sleeping difficulty)
Loss of appetite
Nausea and vomiting
Pallor
Rapid heart rate
Sweating, clammy skin
Tremor of the hands or other body parts
Delirium Tremens - a severe form of alcohol withdrawal. It can cause:
Agitation, irritability
Sudden, severe confusion (delirium)
Fever
Seeing or feeling things that aren't there (hallucinations)
Seizures
A continuum of symptoms and signs of central nervous system (including autonomic) hyperactivity may accompany cessation of alcohol intake.
A mild alcohol withdrawal syndrome includes tremor, weakness, headache, sweating, hyperreflexia, and gastrointestinal symptoms. Tachycardia may be present and blood pressure can be slightly elevated. Symptoms usually begin within about 6 hours of cessation. Some patients have generalized tonic-clonic seizures (called alcohol-related seizure, or rum fits) but usually not > 2 in short succession. Seizures generally occur 6 to 48 hours after cessation of alcohol.
Alcoholic hallucinosis (hallucinations without other impairment of consciousness) follows abrupt cessation from prolonged, excessive alcohol use, usually within 12 to 24 hours. Hallucinations are typically visual. Symptoms may also include auditory illusions and hallucinations that frequently are accusatory and threatening; patients are usually apprehensive and may be terrified by the hallucinations and by vivid, frightening dreams. Alcoholic hallucinosis may resemble schizophrenia, although thought is usually not disordered and the history is not typical of schizophrenia. Symptoms do not resemble the delirious state of an acute organic brain syndrome as much as does delirium tremens (DT) or other pathologic reactions associated with withdrawal. Consciousness remains clear, and the signs of autonomic lability that occur in DT are usually absent. When hallucinosis occurs, it usually precedes DT and is transient.
Delirium tremens usually begins 48 to 72 hours after alcohol withdrawal; anxiety attacks, increasing confusion, poor sleep (with frightening dreams or nocturnal illusions), profuse sweating, and severe depression also occur. Fleeting hallucinations that arouse restlessness, fear, and even terror are common. Typical of the initial delirious, confused, and disoriented state is a return to a habitual activity; eg, patients frequently imagine that they are back at work and attempt to do some related activity.
OPIOID WITHDRAWAL
Opiates or opioids are drugs used to treat pain.
Opiates are derived from plants and
opioids are synthetic drugs that have the same actions as opiates.
The term narcotic refers to either type of drug.
If you stop or cut back on any of these drugs after heavy use for a few weeks or more, you will have a number of symptoms. This is called withdrawal.
Early symptoms of opiate and opioid withdrawal include:
Agitation
Anxiety
Muscle aches
Increased tearing
Insomnia
Runny nose
Sweating
Yawning
Late symptoms of opiate and opioid withdrawal include:
Abdominal cramping
Diarrhea
Dilated pupils
Goosebumps
Nausea
Vomiting
These symptoms are very uncomfortable but are not life threatening. Symptoms usually start within 12 hours of last heroin usage and within 30 hours of last methadone exposure.
Withdrawal from opioids can cause:
Sweating
Chills
Anxiety
Agitation
Muscle aches
Insomnia
Abdominal cramping
Nausea
Vomiting
Withdrawal symptoms may increase in severity over 72 hours before beginning to ease. Unlike withdrawal from other drugs such as alcohol or benzodiazepines, withdrawal from opioids is uncomfortable but rarely life-threatening.
The opioid withdrawal syndrome usually includes symptoms and signs of central nervous system hyperactivity.
Onset and duration of the syndrome depend on the specific drug and its half-life.
Symptoms may appear as early as 4 hours after the last dose of heroin, peak within 48 to 72 hours, and subside after about a week.
Anxiety and a craving for the drug are followed by increased resting respiratory rate (> 16 breaths/minute), usually with diaphoresis, yawning, lacrimation, rhinorrhea, mydriasis, and stomach cramps. Later, piloerection (gooseflesh), tremors, muscle twitching, tachycardia, hypertension, fever and chills, anorexia, nausea, vomiting, and diarrhea may develop.
Opioid withdrawal does not cause fever, seizures, or altered mental status. Although it may be distressingly symptomatic, opioid withdrawal is not fatal.
The withdrawal syndrome in people who were taking methadone (which has a long half-life) develops more slowly and may be less acutely severe than heroin withdrawal, although users may describe it as worse.
Even after the withdrawal syndrome remits, lethargy, malaise, anxiety, and disturbed sleep may persist up to several months.
Drug craving may persist for years.
NICOTINE WITHDRAWAL
Common Nicotine Withdrawal Symptoms
Having urges or cravings to smoke
Feeling irritated, grouchy, or upset
Feeling jumpy and restless
Having a hard time concentrating
Having trouble sleeping
Feeling hungrier or gaining weight
Feeling anxious, sad, or depressed
Trying to quit smoking feels different for each person, but almost everyone will have some symptoms of nicotine withdrawal. When you stop, your body and brain have to get used to not having nicotine. This can be uncomfortable, but nicotine withdrawal can’t hurt you – unless you give in and have a cigarette. Over time, withdrawal symptoms will fade as long as you stay smoke-free.
CAFFEINE WITHDRAWAL
Caffeine intoxication and caffeine withdrawal are included in DSM-5-TR.
Caffeine use disorder, however, is in the section of DSM-5-TR for conditions requiring further research. While there is evidence to support this as a disorder, experts conclude it is not yet clear to what extent it is a clinically significant disorder.
Some signs of caffeine withdrawal include:
impaired behavioral and cognitive performance,
decreased or increased blood pressure,
decreased motor activity,
increased heart rate,
hand tremor,
increased diuresis,
skin flushing,
flu-like symptoms,
nausea/vomiting,
constipation,
muscle stiffness,
joint pains, and
abdominal pain.
Sources: 1 2 3 4 5 6 7 8 9 10 ⚜ More: Notes ⚜ Writing Resources PDFs
Hi, it's alright. This is an interesting topic and quite important to portray in literature and other media. The symptoms depend on which substance/s your character has been using, but each person may also have different withdrawal symptoms. You can find more details in the sources. Hope this helps with your writing!
#anonymous#writing reference#character development#medicine#writeblr#literature#dark academia#writers on tumblr#spilled ink#writing prompt#creative writing#light academia#writing resources
99 notes
·
View notes
Text
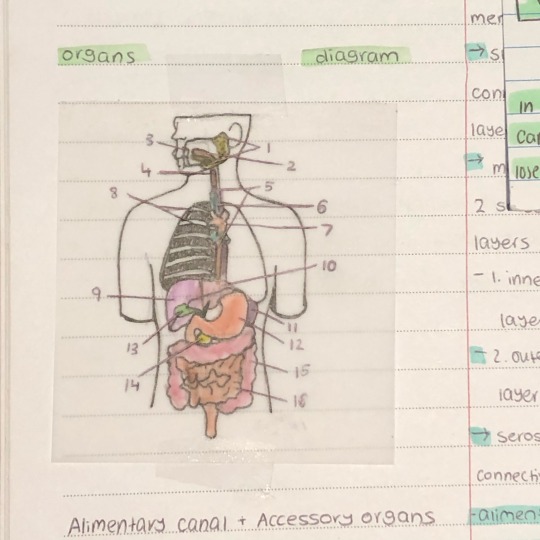
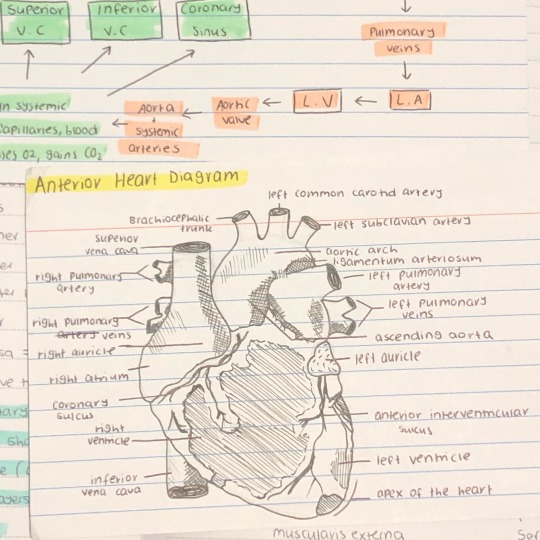
10.02.2024
.
these are my old medical studies note on the cardiovascular and gastrointestinal/digestive systems.
I’ve been really bored these past 2 days since tafe doesn’t start up again for another 2 more days. I’ve been wanting to go back to learning a new language again to keep myself busy but I know I’m gonna stress myself out with that, so I’m just trying to relax instead.
21 notes
·
View notes
Note
just scrolling your blog a bit and stumbled across a post asking about Sensitive Tummy Foods. i work at a training kennel so trialing tummy issues has been much of my life so i was going to pitch a bunch of stuff i've seen work in my experience, but for me the first thing i think of if a dog is consistently having runny shits is phasing out chicken-based foods. mild allergies to chicken can be pretty common, and so can beef allergies ngl. you mentioned using nulo, and we actually tried a pair of standard poodles in our guide dog program on nulo because they had a round of giardia as puppies and their stomachs have been fried ever since, and on nulo one of the boys managed to shit UP a wall, so don't worry lol you're not the only one with adverse experiences on that kibble lol
1. we had a lot of success with inukshuk. it's expensive so it's not the only option i'll throw at you, but it's a performance kibble with a higher calorie density and i've seen a lot of dogs do well on it. my personal dog is on inukshuk marine 16 because his gastrointestinal system does horrible things when in contact with chicken, it's probably the best kibble i've given him. if you have an inukshuk distributor in your area the price can halve though so i'd shop around and see if anyone has The Goods
2. pumpkin is a classic belly calming potion, if it's just mildish diarrhea you might have some success just adding a tablespoon of pumpkin puree to meals. propectalin is also a useful supplement for tummy issues and my life would be unlivable without it, it's expensive which sucks but it lasts a while. vets actually prescribe propectalin for dogs with IBS which is so funny to me like you can get it cheaper than prescription of amazon this is like doggie pepto bismol. in my experience propectalin has worked better as a probiotic than fortiflora does, but fortiflora does have a marked effect, and is a good compromise for price. we also used probios, which is definitely effective particularly for dogs with highly explosive stomach issues resistant to everything else; it's a probiotic designed originally for livestock with some combinations blended specifically for dogs. the people hocking goats' milk are dumb though lol. goats' milk does not help in most cases, it can increase inflammation in the GI tract which is the last thing you want for a Shitter On The Loose
NOTE: if you find your boy has issues with beef, DO NOT give propectalin, it has beef in it. you will have a bad day. learn from my mistakes
3. one thing to play with are organ meats. sometimes diarrhea isn't always Belly Inflammation but an imbalance of nutrition, and sometimes an easy fix is picking up some chicken hearts or dried sheep liver and playing a bit. i won't wade into raw food discourse here, but as a warning, if you do take this advice in the direction of purchasing raw items, just know that most dogs have slightly looser stools on a raw diet compared to a kibble only diet, so if you do transition and you're like wtf? that's a pretty normal thing
and random only somewhat related doggie supplement advice i'm pitching just because it's cool: B12 is more effective as a calming supplement than CBD or melatonin. i kinda think most calming supplements are total bullshit but B12 is effective ime not because it provides an innate calming effect but because it addresses a nutritional issue that leads to that effect. as a human i personally start seeing the hat man if i forget to address a particular nutrient so i understand, puppies.
anyway i hope some of this helps your poor teenage mal and his belly troubles! wishing u and ur pups the best and i hope my phd in dog shit can be of assistance to you
i’m saving this for future use thank you for all the info :)
13 notes
·
View notes
Text
Also preserved in our archive (Daily updates!)
by Dr. Monica M. Bertagnolli
In 2021, NIH launched the Researching COVID to Enhance Recovery (RECOVER) Initiative , a nationwide research program, to fully understand, diagnose, and treat Long COVID. We continue to learn more about this condition, in which some people experience a variety of symptoms for weeks, months, or even years after infection with SARS-CoV-2, the virus that causes COVID-19. But we’re still working to understand the underlying reasons why people develop Long COVID, who is most likely to get it, and how best to treat or prevent it.
Studies have shown that for some people, SARS-CoV-2 doesn’t completely clear out after acute infection. Scientists have observed signs that the virus may persist in various parts of the body, and many suspect that this lingering virus, or remnants consisting of SARS-CoV-2 protein, may be causing Long COVID symptoms in some individuals. Now, in a new study supported by RECOVER, scientists found that people with Long COVID were twice as likely to have these viral remnants in their blood as people with no lingering symptoms. The findings, reported in Clinical Microbiology and Infection , add to evidence that Long COVID may sometimes stem from persistent infection or SARS-CoV-2 protein remnants.
The study team, led by David Walt and Zoe Swank at Brigham and Women’s Hospital in Boston, had earlier found preliminary evidence in a small pilot study that a SARS-CoV-2 protein could often be detected in the bloodstreams of people with Long COVID up to a year after the initial infection. In the new study, they wanted to better quantify this in a much larger group of people with Long COVID. The researchers developed a highly sensitive test to look for whole and partial proteins from the SARS-CoV-2 virus. They analyzed 1,569 blood samples collected from 706 people at various times after SARS-CoV-2 infection.
Overall, 21% of those in the study had detectable levels of a SARS-CoV-2 protein between 4 and 7 months after infection. In total, 82% of the study’s participants (578 people) had at least one symptom of Long COVID more than a month after their infections. Commonly reported symptoms included fatigue, brain fog, muscle pain, joint pain, back pain, headache, sleep disturbance, loss of smell or taste, and gastrointestinal symptoms. More than half of participants in this group (378 people) reported experiencing ongoing cardiopulmonary, musculoskeletal, or neurologic symptoms, and among those participants, 43% (165 people) had detectable virus protein. Also of note, of the asymptomatic people, about 20% had detectable virus protein.
While the researchers can’t definitively show that persistent infections are the cause of some Long COVID symptoms, the findings add to growing evidence that low levels of viral protein being present may explain some but not all cases of Long COVID. The authors and many other researchers suspect that Long COVID likely has multiple underlying causes. For instance, it’s possible that the virus may lead to harmful changes in the immune system that play a role in some cases of Long COVID.
Scientists also want to see if there is a subset of people with Long COVID or persistent symptoms who may benefit from antiviral treatment. To this end, RECOVER is supporting a clinical trial evaluating whether the antiviral drug Paxlovid (a combination of nirmatrelvir and ritonavir), which is used to treat COVID-19, could also be used to improve Long COVID symptoms. The trial is using the SARS-CoV-2 blood test developed by the Brigham and Women’s study team to evaluate whether Paxlovid can eliminate viral proteins from participants’ blood.
More study is needed to understand the causes of Long COVID symptoms in people who test negative for persistent infection, the researchers note. They are conducting follow-up studies in even more people with Long COVID, including those with compromised immune systems. They hope to learn more about what causes some people to be at higher risk for retaining some SARS-CoV-2 protein remnants and Long COVID.
Reference:
Swank Z, et al; RECOVER consortium authors. Measurement of circulating viral antigens post-SARS-CoV-2 infection in a multicohort study. Clinical Microbiology and Infection. DOI: 10.1016/j.cmi.2024.09.001 (2024).
Study Link: www.sciencedirect.com/science/article/abs/pii/S1198743X24004324?via%3Dihub (PAYWALLED)
#mask up#covid#pandemic#public health#wear a mask#covid 19#wear a respirator#still coviding#coronavirus#sars cov 2#long covid#covid is airborne
61 notes
·
View notes
Text
Best Gallbladder Surgeon In Lucknow | Best Gastroenterologist Gomti Nagar Lucknow | Dr Manas Aggarwal
Dr. Manas Aggarwal: The Best Gastro, Gallbladder & Cancer Surgeon in Lucknow
If you require any health treatment, especially regarding the digestive systems, you need to find a trusted and expert surgeon. Whether you’re experiencing gallbladder pain, gastrointestinal woes or more serious issues, such as gastrointestinal cancer, having the right expert at your side makes all the difference.
Dr. Manas Aggarwal, a well known Gastroenterologist in Lucknow and if you are looking for the Best Gastro Cancer Surgeon in Lucknow, Best Gallbladder Surgeon in Lucknow and Best Gastro Surgeon in Lucknow. Dr. Aggarwal is also a leading choice for patients seeking gastro care in the city, with years of experience, advanced surgical skills, and a patient-first approach.
Dr. Manas Aggarwal – A Trustworthy Name
Dr. Manas Aggarwal is a noted GI and Laparoscopic surgeon in Lucknow. He is well known for providing excellent results even in complex cases of gastro cancer and gall-bladder surgeries.
His credentials include:
GI surgery experience range from few months to over 15 years.
Subspecialty training in laparoscopic (minimally invasive) techniques
Successful gallbladder and cancer treatment surgeries
Individualized patient care with heart
And with an emphasis on comfort, Dr. Aggarwal provides every patient with the highest quality medical treatment.
Why should one opt to consult Dr. Manas Aggarwal?
Reasons why patients across Lucknow trust Dr. Manas Aggarwal are:
Expert in Gallbladder Surgery
Experiencing gallbladder problems such as gallstones, infections, or inflammation can be very painful, debilitating, and disruptive. He healed many gallbladder patients, so they consider him as the Best Gallbladder Surgeon in Lucknow providing advanced laparoscopic procedures for speedy recovery, reduced pain, and minimally invasive scars.
Laparoscopic Gastrointestinal Surgeon
Dr. Aggarwal addresses many GI problems, from hernias and acid reflux to complicated bowel conditions. He is also one of the Best Gastro Surgeon in Lucknow who addresses not only the surgery but also long term digestive health.
Gastrointestinal Cancers Specialist
Gastrointestinal cancers depend on early diagnosis and specialized surgical management. Best Gastro Cancer Surgeon in Lucknow Dr. Aggarwal and his team of professionals. He collaborates with oncologists and other specialists to provide total cancer care.
Making a Difference in Patient-Centric Care
Dr. Aggarwal is a proponent of clear communication and transparency. He makes an effort to spend time with each patient, reviewing the condition, surgical options, likely outcomes and the recovery process. Not only does this reduce anxiety, it also helps patients make informed decisions regarding their health.
Here’s what patients say:
Dr. Manas Aggarwal, Professional yet caring. He talked me through everything in detail and made me feel 1000% comfortable pre- and post-gallbladder surgery."
— Neha S., Lucknow
State-of-the-Art Facilities & Advanced Technologies
Expect state-of-the-art facilities and the latest surgical methods at Dr. Manas Aggarwal’s clinic. Laparoscopic surgery, or keyhole surgery, is a specialty in these parts. It is less invasive and it allows for a faster recovery than traditional ways.
And when you combine technology-driven care with a team prepared and ready to support you, your health is in safe hands.
Book a Consultation Today
If you have digestive issues or want professional advice regarding GI cancer, there is no doubt that seeing a medical expert early can be more beneficial. Don’t wait until you have symptoms that are worse.
📍 Location:Chandan Hospital, Shankar Puri, Gomti Nagar, Lucknow, Uttar Pradesh 226010
📞 Call Now: [ 83182 08837]
🔗 Site: [ https://drmanasaggarwal.com]
Final Thoughts
Your health should be in the best possible hands. Dr. Manas Aggarwal is the proud surgeon behind the success of any patient searching for Best Gastro Cancer Surgeon in Lucknow, Best Gallbladder Surgeon in Lucknow, and the Best Gastro Surgeon in Lucknow. With his dedication to patient care alongside surgical skill, he is one of the best options for gastro-related conditions in the area.
Book an appointment today and embark on the path to better health with confidence!
#Best Gallbladder Surgeon In Lucknow#Gastro Surgeon In Lucknow#Best Gastro Surgeon In Lucknow#Best Stomach Doctor In Lucknow#Best Hernia Surgeon In Lucknow#Gastroenterology Cancer Surgeon Lucknow
2 notes
·
View notes