
Sharing things I'm learning in the EMT-1 program. ALWAYS study from your class syllabus or your instructor's directions. Hope some of my information will help you along the way. Take care!
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by emtthings and here's what we found interesting.
Average Info
Notes Per Post
7K
Likes Per Post
4K
Reblog Per Post
3K
Reply Per Post
12
Time Between Posts
3 months
Number of Posts By Type
Text
9
Photo
3
Video
1
Link
1
Last Seen Tumblr Blogs





Fun Fact
Tumblr has 4 main sources of revenue.
Text
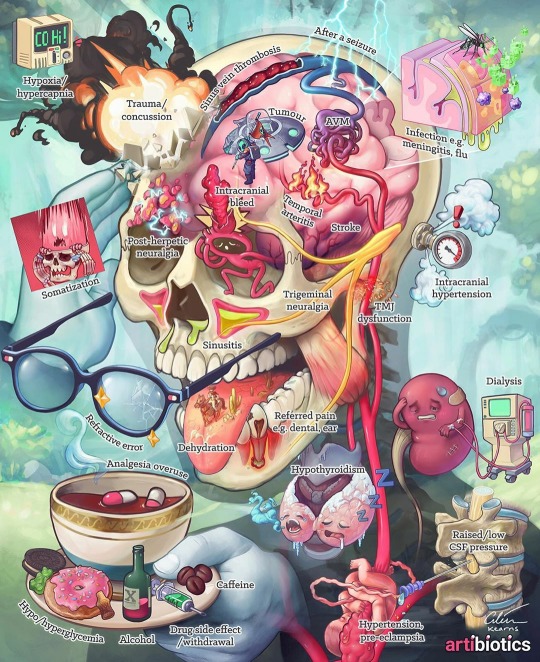
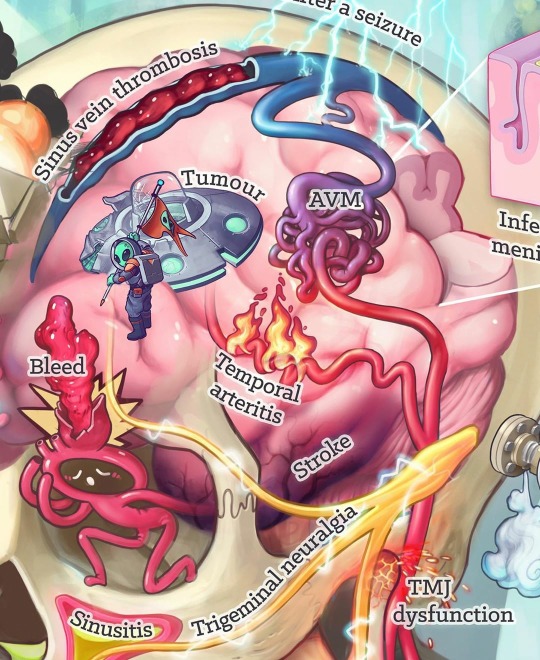
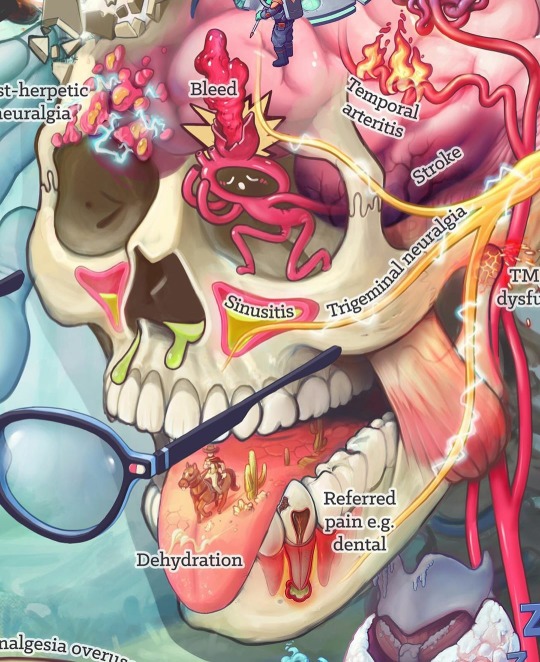
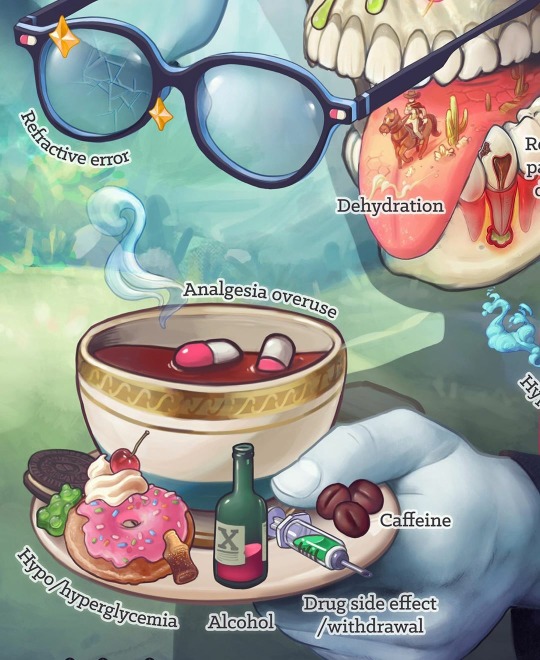
The top 30 causes of a headache as Illustrated by Artibiotics [Instagram]
214 notes
·
View notes





Video
youtube
Naloxone is a medication designed to rapidly reverse opioid overdose. It is an opioid antagonist—meaning that it binds to opioid receptors and can reverse and block the effects of other opioids. It can very quickly restore normal respiration to a person whose breathing has slowed or stopped as a result of overdosing with heroin or prescription opioid pain medications. NARCAN® Nasal Spray is a prefilled, needle-free device that requires no assembly and is sprayed into one nostril while patients lay on their back.
131 notes
·
View notes
Text
Anatomy Mnemonics
Below are some old Anatomy Mnemonics someone once gave me that I found in my hard drive. Hopefully they’ll come in handy for someone else.
BONES
6 cranial bones
Old People From Texas Eat Spiders.
Parietal, Ethmoid, Sphenoid, Temporal, Occipital, Frontal.
Leg Bones
TIBia is the Thick Inner Bone, and Fibula is Finer, Fluted, and Lateral.
8 facial bones
Common Love gone Zip?(Abbr. CMMNLVZP)
conchae, mandible, maxilla, nasal, lacrimal, vomer, zygomaticus, palatine.
*Applying the first-3-letters rule to the facial bones, I came up with
Con Man
Max and Pal
Bones of the Wrist
Some Lovers Try Positions That They Cannot Handle
Scaphoid, Lunate, Triquetrum, Pisiform, Trapezium, Trapezoid, Capitate, Hamate
Never Lower Tillie’s Pants, Mama Might Come Home.
navicular, lunate, triquetrum, pisiform, greater and lesser multangular, capitate, and hamate.
*To remember that the carpals are bones of the wrist and not the foot, Lunate, Triquetrum, remember that CARPenters use their hands.
7 types of bone fractures
C3-PO Breaks his Bones
Greenstick, Open, Complete, Closed, Comminuted, Partial, and Others.
MUSCLES
Muscles in gluteal region: from top to bottom: P-GO-GO-Q
Piriformis
Gemellus superior
Obturator internus
Gemellus inferior
Obturator externus
Quadratus femoris
Muscles whose tendons attach at the pes anserinus (medial tibia): SGT
(“Sargent”)
Sartorius
Gracilis semiTendinosus
Four abdominal muscles –
TIRE: (deepest to most superficial)
Transversus abdominis, Internal abdominal oblique, Rectus abdominis, and External abdominal oblique
Functions of the Interossei muscles
PAD – Palmar ADduct
DAB – Dorsal ABduct
Attachments of Pectoralis Major, Teres Major and Latissimus Dorsi
A lady between two majors.
Pectoralis major attaches to lateral lip of bicipital groove.
Teres major attaches to medial lip of bicipital groove.
Latissimus dorsi attaches to the floor of bicipital groove.
The “lati” is between two “majors.“
A lady between two majors.
Four muscles which control the mandible
masseter, temporal, lateral and medial pterygoids
form the letters MTPP, which could be read as “Empty Peepee” which could be construed as a command (or wish) to empty one’s peepee via…oh we’d better not say it.
Four abdominal muscles Spare TIRE
transversus, internal oblique, rectus, and external oblique
On the floor of the mouth are two muscles
Doctor on the Floor?
mylohyoid and digastric – MD.
Muscles which regulate breathing
You Will DIE! If you don’t have'em
Diaphragm, Inner costal, and External costal
The SITS muscles make up the rotator cuff:
Supraspinatus
Infraspinatus
Teres Minor
Subscapularis
NERVES
Radial n. innervates the BEST!!!!
Brachioradialis
Extensors
Supinator
Triceps
Hand muscles innervated by the Median nerve
LOAF
Lumbricals 1 + 2
Opponens pollicis
Abductor pollicis brevis
Flexor pollicis brevis
Innervation of phrenic nerve
c345 keeps the phrenic alive
c345 keep the diaphragm alive
Innervation of the penis:
Parasympathetic puts it up; sympathetic spurts it out
Point , Shoot, Score! (erection, emmision ,ejaculation)
Parasympathetic, Sympathetic ,Somatomotor
Innervation of the penis by branches of the pudental nerve
"S2, 3, 4 keep the penis off the floor”, derived from spinal cord levels
S2-4
Long thoracic nerve innervates serratus anterior
c5-6-7 raise your arms to heaven
Lateral and Medial Pectoral Nerve
Lateral is less, medial is more.
Lateral pectoral nerves goes through pectoralis major while medial pn goes though both pectoral major and minor.
12 Facial Nerves
"At the OIL FACTORY, the OPTICIAN looked for the OCCUPANT of the TRUCK. He
was searching because 3 GEMS had been ABDUCTED by a man who was hiding his FACE and EARS. A GLOSSY PHOTOGRAPH has been taken of him, but it was too VAGUE to use. He appeared to be SPINELESS and HYPOCRITICAL.“
In order, the oil factory is the olfactory nerve; the optician is the optical nerve; the occupant is the occulomotor nerve; the truck represents the trochlear nerve; the 3 gems are the trigeminal nerve; abducted is really the abducens;
face is facial; ears really means auditory; glossy photograph is glosso-pharyngeal; spineless relates to the spinal
accessory nerve; and hypocritical is the hypoglossal nerve.
Wrist Nerves and Prohibition
RUM, for radial, ulnar, and medial symptoms of nerve troubles are wrist drop, claw hand, and tunnel syndrome …
represented by the letters WCT (Women’s Christian Temperance Union).
Cranial Nerves
I-Optic
II-Olfactory
III-Oculomotor
IV-Trochlear
V-Trigeminal,
VI-Abducens
VII-Facial
VIII-Acoustic (Vestibulocochlear),
IX-Glossophrayngeal,
X-Vagus,
XI-Spinal Accessory,
XII-Hypoglossal
On Old Olympus Towering Tops, A Finn And German Viewed Some Hops
Branches of the Facial Nerve (CN VII):
To Zanzibar by Motor Car
Ten Zebras Bought My Car
Temporal, Zygomatic, Buccal, Masseteric,Cervical
Brachial Plexus:
Roots, Trunks, Divisions, Cords, Branches
Robert Taylor Drinks Cold Beer. (or Richard Tucker Drinks Cheap Beer :-) )
Innervation of Extraocularmotor Muscles: LR6 SO4 Others 3
LR6–Lateral rectus - VI abductens
SO4–Superior Oblique - IV Trochlear
Others 3–The remaining 4 eyeball movers = III Oculomotor
For the order of nerves that pass through the superior orbital fissure:
"Lazy French Tarts Lie Naked in Anticipation.”
(Lacrimal, Frontal, Trochlear, Lateral, Nosociliary, Internal, Abducens)
9 branches of the abdominal portion of the aorta
"Celia Smith’s Supra Rams Green Impala Past Stop Light”
Celiac, Supra mesenteric, Supra-renal, Renal, Gonadal, Inferior mesenteric, Phrenic, Sacral, and Lumbar.
VESSELS Structures passing posterior to the medial malleolus of the foot:
Tom, Dick, And Harry
Tibialis posterior tendon, flexor Digitorum longus tendon, post. tibial Artery and tibial nerve, and
flexor Hallucis longus tendon. (i.e. Tibialis, Digitorum, Artery & nerve, and Hallucis)
Carotid Sheath– VAN
Internal Jugular Vein
Common carotid Artery
Vagus Nerve
Arteries as they come off the external carotid:
Superior thyroid, Ascending pharyngeal, Lingual, Facial, Occipital, Post Auricular, Superficial temporal, Maxillary
Some Angry Lady Figured out PMS
ABC’S of the aortic arch!
Aortic arch gives off the Brachiocephalic trunk, the left Common Carotid, and Left Subclavian artery
Branches of the aorta artery in the lower torso
Transsexuals Remember the Aorta
"Come on In Ex-Female, Pop And Prance Past Doors and Planters".
Common iliac, Internal iliac, External iliac, Femoral, Popliteal, Anterior tibia, Posterior tibia, Peroneal, Dorsalis, medial and lateral Plantars.
Branches of the axillary artery
Sally Thompson Loves Sex And Pot pie
Superior Thoracic, Thoracoacromial, Lateral thoracic, Subscapular, Anterior circumflex humeral, Posterior circumflex humeral, and Profunda brachii.
Arteries off the External Carotid
They are buried in the phrase Some Loser F*cked My Sister
Superior Thyroid, Lingual, Facial, Maxillary, Superficial Temporal
Vessels joining the inferior vena cava
"He Commonly Lumbers in the Viet Cong ReGion".
A Vietnamese Lumberjack’s Heart:
Hepatic, Common iliac, Lumbar, Vena Cava, Renals, Gonadals.
Stroke versus Aneurysm
STRoke is caused by arterial reSTRiction, and aneurysm is AN Erupting artery.
MISCELLANEOUS
checklist of factors causing back troubles
Dr. O. VESALIUS
O - Osteomyelitis
V - Vertebral fracture
E - Extraspinal tumour
S - Spondylolisthesis
A - Ankylosing spondylitis
L - Lumbar disk disease
I - Intraspinal tumour
U - Unhappiness
S - Stress
Cranial sutures
cranial sutures have CLASS!
Coronal, Lambdoid, Squamous, Sagittal.
five visceral sensors
Low TEMPeratures have BARe-CHEsted cOSMO-girls kNOCking. temperature, barometric, chemical, osmotic, nociceptors
Femoral Sheath (lateral to medial) order of things in thigh
NAVEL
Femoral Nerve,
Femoral Artery,
Femoral Vein,
Empty Space,
Lymphatics (or Lacunar Ligament)
Pelvic Diaphragm – PICOLO(A) -Posterior to anterior
PIriformis
COccygeus
Levator Ani
Location of Thoracic duct:
The duck is between two gooses (duck = thoracic duct)
2 gooses = azyGOUS and esophaGOUS
Structures perforating the diaphragm
“At T8 you see, perforates the IVC” (inferior Vena Cava) the “EsoVagus” pierce T10 (esophagus, vagus nerve)
T12 - red, white and blue (aorta,thoracic duct,azygous vein)
Course of Ureters
Water runs under the bridge (uterine a. and ductus deferens)
542 notes
·
View notes
Text
FACTS ABOUT 911
I know this is long, but please read and reblog this so that we can try and circulate HELPFUL information instead of deadly suggestions.
After stumbling across the last post I reblogged that was full of a lot of DANGEROUS, BAD, TERRIBLE advice in reference to how to handle calling 911 when in danger, I feel compelled to at least try and get some better information out there in the Tumblr community. I am a 911 dispatcher and the first piece of advice I have for anyone in an emergency situation (or even for someone that calls 911 accidentally) is:
DO NOT HANG UP. In case you didn’t get that the first time, I said DO NOT HANG UP THE PHONE. We cannot help you if we do not know where you are, and contrary to what is apparently popular belief, we are NOT mind readers & without knowing your location (which you must provide) we CAN NOT get you help.
To help you understand the importance of this, I’m going to explain to you what happens when you call 911 in my center and in the centers in my area.
911 line rings.
We answer: “_______ (name of your agency) 911, WHERE is your emergency?”
In a perfect world, the caller will respond with the address of their emergency.
If you are unable to do so, we will start to retransmit your location. It takes time. Again, in a perfect world, we can usually get it in less than 10 seconds, but we do not live in a perfect world and so it often doesn’t happen that quickly. (Also, if you’re in an apartment complex, trailer park, hotel, etc, it’s not going to give us the room, lot, etc. number that you’re actually in, even with a retransmit). It is true that if you call from a landline your address will often populate for us, however, the address is NOT always right! We need you to try your ABSOLUTE BEST to provide us with an accurate address. By not knowing your location, you’re prolonging the response time. The call has to be answered, have a confirmed address, type of call that we’re responding to so that the correct responders are dispatched, and then it has to be dispatched. In smaller jurisdictions, their fire/EMS is often volunteer. That means: THEY ARE COMING FROM HOME TO THE STATION. It takes time & the more time we waste just trying to figure out where you are, the longer you’re going to be waiting for a life saving response.
The TERRIBLE information post that is going around tells you to call 911, hang up, and then turn your phone off. NO, NO, NO. That is the absolute WORST thing you could ever do. When a 911 hang up comes in we attempt to call the line back twice. If the line isn’t open long enough to retransmit an address (which most of the time it’s not), that’s it. The call gets out in and closed. There is literally NOTHING WE CAN DO TO HELP YOU. Even if we DO retransmit an address and there is no sign of a disturbance or no other indication that there is an emergency, we often do not send a responder because if we send one to every call, we’d be wasting a LOT of time and resources. We receive 911 hang ups/accidental 911 calls ALL DAY LONG. (Side note: the most common ones that we receive come from disconnected cell phones. Every cell phone (disconnected or not) with battery life can call 911, but 911 CANNOT call those phones back). If you call from a disconnected cell and we’re not able to get a location (or are and not hear any signs that would indicate a need for service), you will most likely not get the help you need.
Moral of this point: DO NOT HANG UP and KNOW WHERE YOU ARE. Try to pay attention to mile markers on the interstate & landmarks, signs or road names. If you call accidentally-STAY ON THE LINE. We (at least at my agency) will ask you to verify your name and address and that there is no emergency. As long as nothing feels/sounds wrong about it to us, we won’t send an officer to knock on your door. You won’t get in trouble. No one will be mad. Just stay on the line so that we don’t waste time and resources on a call that is not emergent.
Disclosure: some agencies offer text to 911. Don’t assume that you can text 911 unless you know that your locality has that capability. A lot of them don’t. If you’re able to safely call you should ALWAYS call rather than text. It’s faster and more efficient.
Moving on-
Answer our questions. We’re not asking you questions for our own amusement. Everything we ask you on the line is for your own safety and for the safety of our responders. They are much more well equipped to handle your emergency if they know what they’re walking into and what supplies they need to bring in with them when they come. We’re NOT going to send our fire/EMS into a scene that is not safe, so answer our questions so that we know which resources need to be provided to you. I know that often times the calls that people place to us are during some of the worst, most terrifying moments of their lives & we WANT to help you in the best way that we know how. We ask the things that we ask because it’s required & because the more we know, the higher the quality of service that we provide you will be.
ALSO: While we’re asking you the questions, most likely RESPONDERS HAVE ALREADY BEEN DISPATCHED. If you didn’t get that, read it again. You can’t imagine how much time we spend trying to argue answers to questions out of callers because we’re being screamed at: “JUST GET THEM HERE QUICKLY.” “HE/SHE/I’LL BE DEAD BEFORE YOU GET THEM HERE,” etc. you’re wasting your time and mine. Try your best to work with us because our number one goal is to get you the help you need as quickly as possible. Contrary to popular belief, we don’t do this for the money. The medics, fire fighters, police officers and animal control officers DON’T do this for the money. (It’s not there, in case you were wondering.) we do this because we genuinely care about other human beings. We want to HELP. We CARE. We are here to protect and serve, but we cannot do that effectively if people are constantly fighting against us.
If you have any questions about how things work here or need advice as to how to handle a call in to 911, feel free to ask and I will give you the best advice that I can. Just please, please don’t listen to terrible misinformation (like calling, hanging up and turning your phone off). These situations are often the line between life and death. As cliche as it sounds, help us help you. Much love, Tumblr fam!
Also, to any of my fellow dispatchers, feel free to add to this. I know that things can vary from one locality to another, so I think any input would be helpful! I tried to just stick to the basics in this post for that reason. :)
@therapy101 @thistherapylife @socialworkmemes @all-about-psychology @theangrytherapist @thecalminside could you guys please reblog this to try and circulate correct information about how to receive help in an emergency situation? There is some VERY bad information going around that provides dangerous suggestions in reference to calling 911 and that makes me so afraid for anyone that reads it and thinks that it’s true.
2K notes
·
View notes
Text
FACTS ABOUT 911
I know this is long, but please read and reblog this so that we can try and circulate HELPFUL information instead of deadly suggestions.
After stumbling across the last post I reblogged that was full of a lot of DANGEROUS, BAD, TERRIBLE advice in reference to how to handle calling 911 when in danger, I feel compelled to at least try and get some better information out there in the Tumblr community. I am a 911 dispatcher and the first piece of advice I have for anyone in an emergency situation (or even for someone that calls 911 accidentally) is:
DO NOT HANG UP. In case you didn’t get that the first time, I said DO NOT HANG UP THE PHONE. We cannot help you if we do not know where you are, and contrary to what is apparently popular belief, we are NOT mind readers & without knowing your location (which you must provide) we CAN NOT get you help.
To help you understand the importance of this, I’m going to explain to you what happens when you call 911 in my center and in the centers in my area.
911 line rings.
We answer: “_______ (name of your agency) 911, WHERE is your emergency?”
In a perfect world, the caller will respond with the address of their emergency.
If you are unable to do so, we will start to retransmit your location. It takes time. Again, in a perfect world, we can usually get it in less than 10 seconds, but we do not live in a perfect world and so it often doesn’t happen that quickly. (Also, if you’re in an apartment complex, trailer park, hotel, etc, it’s not going to give us the room, lot, etc. number that you’re actually in, even with a retransmit). It is true that if you call from a landline your address will often populate for us, however, the address is NOT always right! We need you to try your ABSOLUTE BEST to provide us with an accurate address. By not knowing your location, you’re prolonging the response time. The call has to be answered, have a confirmed address, type of call that we’re responding to so that the correct responders are dispatched, and then it has to be dispatched. In smaller jurisdictions, their fire/EMS is often volunteer. That means: THEY ARE COMING FROM HOME TO THE STATION. It takes time & the more time we waste just trying to figure out where you are, the longer you’re going to be waiting for a life saving response.
The TERRIBLE information post that is going around tells you to call 911, hang up, and then turn your phone off. NO, NO, NO. That is the absolute WORST thing you could ever do. When a 911 hang up comes in we attempt to call the line back twice. If the line isn’t open long enough to retransmit an address (which most of the time it’s not), that’s it. The call gets out in and closed. There is literally NOTHING WE CAN DO TO HELP YOU. Even if we DO retransmit an address and there is no sign of a disturbance or no other indication that there is an emergency, we often do not send a responder because if we send one to every call, we’d be wasting a LOT of time and resources. We receive 911 hang ups/accidental 911 calls ALL DAY LONG. (Side note: the most common ones that we receive come from disconnected cell phones. Every cell phone (disconnected or not) with battery life can call 911, but 911 CANNOT call those phones back). If you call from a disconnected cell and we’re not able to get a location (or are and not hear any signs that would indicate a need for service), you will most likely not get the help you need.
Moral of this point: DO NOT HANG UP and KNOW WHERE YOU ARE. Try to pay attention to mile markers on the interstate & landmarks, signs or road names. If you call accidentally-STAY ON THE LINE. We (at least at my agency) will ask you to verify your name and address and that there is no emergency. As long as nothing feels/sounds wrong about it to us, we won’t send an officer to knock on your door. You won’t get in trouble. No one will be mad. Just stay on the line so that we don’t waste time and resources on a call that is not emergent.
Disclosure: some agencies offer text to 911. Don’t assume that you can text 911 unless you know that your locality has that capability. A lot of them don’t. If you’re able to safely call you should ALWAYS call rather than text. It’s faster and more efficient.
Moving on-
Answer our questions. We’re not asking you questions for our own amusement. Everything we ask you on the line is for your own safety and for the safety of our responders. They are much more well equipped to handle your emergency if they know what they’re walking into and what supplies they need to bring in with them when they come. We’re NOT going to send our fire/EMS into a scene that is not safe, so answer our questions so that we know which resources need to be provided to you. I know that often times the calls that people place to us are during some of the worst, most terrifying moments of their lives & we WANT to help you in the best way that we know how. We ask the things that we ask because it’s required & because the more we know, the higher the quality of service that we provide you will be.
ALSO: While we’re asking you the questions, most likely RESPONDERS HAVE ALREADY BEEN DISPATCHED. If you didn’t get that, read it again. You can’t imagine how much time we spend trying to argue answers to questions out of callers because we’re being screamed at: “JUST GET THEM HERE QUICKLY.” “HE/SHE/I’LL BE DEAD BEFORE YOU GET THEM HERE,” etc. you’re wasting your time and mine. Try your best to work with us because our number one goal is to get you the help you need as quickly as possible. Contrary to popular belief, we don’t do this for the money. The medics, fire fighters, police officers and animal control officers DON’T do this for the money. (It’s not there, in case you were wondering.) we do this because we genuinely care about other human beings. We want to HELP. We CARE. We are here to protect and serve, but we cannot do that effectively if people are constantly fighting against us.
If you have any questions about how things work here or need advice as to how to handle a call in to 911, feel free to ask and I will give you the best advice that I can. Just please, please don’t listen to terrible misinformation (like calling, hanging up and turning your phone off). These situations are often the line between life and death. As cliche as it sounds, help us help you. Much love, Tumblr fam!
Also, to any of my fellow dispatchers, feel free to add to this. I know that things can vary from one locality to another, so I think any input would be helpful! I tried to just stick to the basics in this post for that reason. :)
@therapy101 @thistherapylife @socialworkmemes @all-about-psychology @theangrytherapist @thecalminside could you guys please reblog this to try and circulate correct information about how to receive help in an emergency situation? There is some VERY bad information going around that provides dangerous suggestions in reference to calling 911 and that makes me so afraid for anyone that reads it and thinks that it’s true.
2K notes
·
View notes
Text
Emergency Trauma Assessment
“ABCDEFGHI”
A - Airway Is the patient’s airway open?
B - Breathing Is the patient breathing?
C - Circulation Is the patient’s blood circulating properly and not cut off anywhere?
D - Disability Does the patient have a preexisting condition that could effect treatment?
E - Examine Does the patient have any obvious injuries?
F - Fahrenheit Does the patient have a healthy temperature?
G - Get Vitals Are the patient’s vitals normal?
H - Head-to-Toe Assessment Are there any other injuries to the patient?
I - Intervention Get the patient to the proper medical care.
506 notes
·
View notes

Text
Just tell us the truth
EMT: “How much did you drink today?”
Pt: “I had one beer”
EMT: “Honestly?”
Pt: “Honestly sir, I had jus…just one, give me a, uh, a, do you know, where are we going?”
EMT:
105 notes
·
View notes
Link
The majority of people hit by the flu this season will recover; however, hundreds of thousands of others won’t be as lucky. According to new estimates from the Centers for Disease Control and Prevention (CDC), as many as 646,000 people across the globe die each year from the seasonal illness—up from previous estimates of 500,000, calculated more than a decade ago.
34 notes
·
View notes
Text
Ambulance Inspection, Engine On
When inspecting Ambulance (ON)
1. pull the ambulance from quarters if engine exhaust fumes will be a problem
2. set the parking brake
3. put the transmission in park
4. have your partner chock the wheels before undertaking the other steps
Ambulance Inspection, Engine ON Steps
1. Check the dash-mounted indicators to see if any light remains on
2. Check the dash mounted gauges for proper operation
3. Depress the brake pedal
4. Test the parking brake
5. Turn the steering wheel from side to side
6. Check the operation of the windshield wipers and washers
7. Turn on the vehicle’s warning lights
8. Turn on the other vehicle lights.
9. Check the operation of the heating and air-conditioning equipment in both the driver’s compartment and the patient compartment
10. Operate the communications equipment
11. If your unit is equipped with a back-up camera, make sure that the camera is not damaged
Source:
•Limmer, Daniel; O'Keefe, Michael F.; Grant, Harvey; Murray, Bob; Bergeron, J. David; Dickinson, Edward T. (2015-03-04). Emergency Care (EMT) (Pages 1027- 1028). Pearson Education. Kindle Edition.
3 notes
·
View notes
Photo
Ensuring Ambulance Readiness for Service
1.Do a brief report with the off-going crew if possible.
2.Learn whether they experienced any problems with either the ambulance or its equipment during their shift.
3.If there was a problem described by a off-going crew, make sure to communicate that with a shift supervisor, and thoroughly document the stated problem.
4. Make a thorough bumper-bumper inspection of the ambulance, using the checklist provided by your service
Limmer, Daniel; O'Keefe, Michael F.; Grant, Harvey; Murray, Bob; Bergeron, J. David; Dickinson, Edward T. (2015-03-04). Emergency Care (EMT) (Page 1026). Pearson Education. Kindle Edition.
0 notes
Text
The three R’s in reaction to Danger
1. Retreat
2. Radio
3. Reevaluate
1 note
·
View note