
Juniper Publishers | international journal of nephrology is an Open Access, peer-reviewed international journal that provides current information of research, development and treatment aspects that are involved in the fields of urology and nephrology. Urology is the branch of medicine
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by juniperpublishersun-blog and here's what we found interesting.
Average Info
Notes Per Post
342
Likes Per Post
203
Reblog Per Post
139
Reply Per Post
0
Time Between Posts
3 months
Number of Posts By Type
Text
17
Last Seen Tumblr Blogs





Fun Fact
Tumblr is used by 21% of adults online aged 18-29 years.
Text
Juniper Publishers wishes Happy Easter to you and your family members

0 notes
Text
Combination Of Oncolytic Newcastle Disease Virus (Ndv) and Vaccine Vector Adenovirus (Adv) as a Potential Virotherapy for Cancer: A Systematic Review | Juniper Publishers
Juniper Publishers-Open Access Journal of Anatomy Physiology & Biochemistry
Authored by Ferbian Milas Siswanto
Abstract
Cancer is a disease with high morbidity and mortality, one of the leading causes of death in the world. Nowadays, the foremost clinical cancer therapy in a patient are surgery, chemotherapy and/or radiotherapy. Despite of the great amount of research on cancer and advance technology in medicine, the mortality rate of cancer remain high due to limited therapeutic effects and additional side effects of current therapy. Here we provide an overview on the virotherapy using the combination of Newcastle disease virus (NDV) and the adenovirus (AdV). Both NDV and AdV possess an oncolytic activity and a potential as vector vaccine. However, oncolytic activity of NDV is more potent than adenovirus. In contrast, the AdV potential as a vector of cancer vaccines is better than NDV. Therefore, in this paper, we discuss the development of a virotherapy combination by utilizing oncolytic activity of NDV, and vaccine vector AdV simultaneously for cancer therapy to improve the effectiveness of therapy against cancer.Conclusion: Decreased estrogen level following ovariectomy causes osteoporosis.
Keywords: Newcastle disease virus; Adenovirus; Virotherapy; Cancer
Abbrevations: NDV: Newcastle Disease Virus; AdV: Adeno Virus; VVND: Velogenic Viscerotropic Newcastle Disease; PBMC: Peripheral Mononuclear Cells; HN: Hemaglutinin-Neuraminidase; TRAIL: TNF-Related Apoptotic-Inducing Ligand; JNK: c-Jun N-terminal Kinase; NOS: Nitric Oxide Synthase; dsDNA: Double-Stranded DNA; NK: Natural Killer; CAE: Carcioembryonic Antigen; TLRs: Toll like receptors
Introduction
Cancer is a disease with high morbidity and mortality that leads to death. Until now, cancer is still the leading cause of death in humans. In 2012, approximately 14.1 million cases of cancer have been reported worldwide, and have caused the deaths of 8.2 million people (about 15% of all deaths). It is characterized by uncontrolled cell division, invade surrounding tissue, and metastasize to other organs in the body. The four most commonly reported cancers are lung, breast, colon, and prostate cancer. However, all organs in the human body can be cancer regardless of age, gender, ethnicity, diet, and environment [1]. Generally, cancer is caused by decreased cell death or increased cell proliferation. In other words, any dysregulation of cell cycle or apoptosis will result in uncontrolled cell growth or malignancy [2].Cancer occurs due to genetic and environmental factors that cause deviations in the growth regulation of stem cell populations. Improving knowledge of the molecular processes underlying cancer development, as well as advances in diagnostic techniques, radiotherapy technology, and chemotherapy, has increased the survival rate of cancer patients. However, recent therapy has not greatly improved the survival of cancer patients who have undergone metastasis. Although modern technology has been developed, cancer is still afflicted millions of people worldwide [3]. This is because, in addition to the limited therapeutic effects, radio and chemotherapy also cause side effects [1]. The ideal cancer therapy is a therapy that selectively kills malignant cells, and does not damage other normal cells in the body. Currently, radiotherapy, chemotherapy, and surgery are the most common modalities in cancer therapy. However, these therapies often cause harmful side effects [4] and often lead to resistance [5].Therefore, the development of cancer therapy with high effectivity and selectivity for cancer cells with minimum side effects becomes crucial. The idea of using bacteria and viruses to treat malignancy in humans began in the mid-1800s in which tumor regression was associated with bacterial and viral infections [6]. The development of cell culture technique and virus technology in the early 1950s led researchers to learn more about the potential of viral therapy in human and small animal tumors [7]. The virus is then proven to be useful as an oncolytic agent and immunostimulator. Newcastle disease virus (NDV) that naturally infected poultry, and adenovirus (AdV) that causes human flu, is a potential viral combination as a virotherapy and immunotherapy agent. NDV can directly kill cancer cells (oncolytic activity) and adenovirus can help to stimulate the immune system to recognize cancer cells (immunostimulator activity).
Newcastle Disease Virus (NdV) as an Oncolytic Agent
Newcastle Disease Virus (NDV) is a virus of the order Mononegavirales because it has single strand RNA, negative polarization, unbranded and linear genome [8]. Furthermore, this virus occupies the family of paramyxoviridae due to its pleomorphic envelope, round-shaped with a diameter of 100- 500nm, but some are in the form of filaments [9]. This virus causes Newcastle disease that attacks various poultry, especially chickens. Until now, Newcastle disease has been found in various parts of the world including Indonesia, and the cases of velogenic viscerotropic Newcastle disease (VVND) have been reported in Indonesia [10]. In Indonesia, Newcastle disease is endemic as indicated by the finding of this case throughout the year [9].NDV was firstly reported to possess an oncolytic activity in the mid-1950s [11]. The clinical evaluation of this virus as an anticancer agent over the last few decades shows its safety and effectivity. The effectivity of NDV application is based on high oncolytic activity, and safety of its use is based on replication that selectively attacks tumor cells and does not damage normal cells. Scientists are interested in the use of NDV because it replicates more rapidly in tumor cells than normal cells in humans, and cause oncolytic effects [12]. NDV replicates 10,000 times faster in cells undergoing neoplasmic changes than normal human cells in general [13,14]. There are several molecular pathways that cause the oncolytic effects of NDV, such as apoptosis pathway [1,15]. Induction of apoptosis by NDV includes a series of virus entry processes, replication, de novo protein synthesis and activation of caspases [16]. NDV induces apoptosis through both extrinsic and intrinsic pathways.NDV-induced apoptosis is generally mediated by intrinsic pathway during the late stage of infection, while in the early stage of infection is more likely to be mediated by extrinsic pathway [17]. Activation of intrinsic pathway involves the increased activity of p53 and Bax proteins, as well as decreased expression of the Bcl-2 gene [18] which will activate the Caspase 9. The matrix protein (M protein) of NDV binds to Bax protein and increases apoptosis [19]. Whereas, the extrinsic pathway of apoptosis is induced by NDV-mediated activation of pro-apoptotic cytokines such as IFN-α and TNF-α in peripheral mononuclear cells (PBMC) via its Hemaglutinin-Neuraminidase (HN) proteins [20,21]. The HN protein of NDV also induces expression of TNFrelated apoptotic-inducing ligand receptor (TRAIL) [22,23] which further activate caspase 8 [17]. A study has shown that NDV initiates the synthesis of nitric oxide synthase (iNOS), thus increasing apoptosis via the NFκB pathway [24,25].NDV-infected mouse PC12 pheochromocytoma cell was proved to induce the activation of reticulum endoplasma eIF2a kinase (PERK) resulting in phosphorylation of eIF2a and caspase 12 activations. Endoplasmic reticulum stress may be responsible for the activation of apoptotic pathways in cancer cells infected with NDV [26]. In addition, the induction of the external pathway by NDV also the activation of c-Jun N-terminal kinase (JNK) and p38 pathways, and decreased Akt pathway activity [27]. NDV has an excellent potential as a highly selective virotherapy candidate. This selective effect arises because of the restriction of V protein by host and secretion of virus-induced cytokines (IFN-γ and TNF-α) [28]. The first step of infection by NDV occurs in all types of cells in the body, while the second step (associated with viral replication) occurs only in tumor cells because this stage is terminated very quickly in normal cells [5]. In general, the specificity of NDV to cancer cells occurs because of damage to antiviral pathways and apoptosis in cancer cells [29].In addition to direct cytopathic effects, NDV anti-cancer activity is associated with the activation of both innate and adaptive immune responses. NDV infection initiates the macrophage-induced synthesis of enzymes that increase antitumor activity in both in vitro and in vivo studies [30]. NDV stimulates monocytes that play a role in killing tumor cells via TRAIL induction [31]. The activation of natural killer (NK) cells is also involved in the cytotoxicity mediated by NDV [20]. However, to induce host immune system, the use of cancer vaccines is believed to have far more effective effects than the immunostimulator effects of NDV. The immunotherapeutic approach aims to promote the host antitumor immune response that can destroy tumor cells in both primary and metastaticaffected sites [32]. Genetic therapy-based cancer vaccination technology has been widely developed, with the virus being the most popular vector studied. Adenovirus, in addition to having oncolytic activity, is a very potential and widely used vector on cancer gene therapy and as a vaccine to express foreign antigens [33].
Adenovirus (AdV) as a Vaccine Vector
Adenovirus is a group of viruses from the Adenoviridae family responsible for 5-10% of upper respiratory infections, gastroenteritis, conjunctivitis, and cystitis (CDC, 2015). It has no envelope, icosahedral capsid with a diameter of 70-90 nm and the double-stranded DNA (dsDNA) [34]. Adenovirus has long been used as a vector for gene therapy due to its ability to influence cell biological activity, tolerate large genetic modifications, and encode proteins without integrating into the host cell genome. More specifically, the virus is used as a vector for administration of therapeutic targets, either in the form of recombinant DNA or proteins [35].Several studies using various antigens proved that adenovirus (AdV) is potential as a vector of cancer antigens such as glycoprotein 33 (GP33) from lymphocytic viral choriomeningitis [36], carcioembryonic antigen (CAE) [37], beta-galactosidase antigen [38], GM-CSF antigen (such as T-VEC and Pexa-Vec) [39], E7 antigen from human papillomavirus [40], the gp100 antigen and TRP-2 antigen [41]. It may enhances cellular immunity mediated by T-cell CD8+ cells and IFN-γ- mediated humoral immune specific to cancer cells. The use of AdV as a vaccine vector is relatively safe to use with intradermal methods [42]. Adenovirus administration may stimulates ligand expression of Toll-like receptors (TLRs) and may alter cancer immunosuppressive and proinvasive microenvironment becoming proinflammatory, thus facilitating immunocompetent cells to fight against cancer [39,43,44].
General Perspective
Both NDV and AdV have oncolytic activity and potential as vector vaccine for cancer. However, oncolytic activity of NDV is more potent than adenovirus. In contrast, the AdV potential as a vector of cancer vaccines is better than NDV. Therefore, the development of a virotherapy combination by utilizing oncolytic activity of NDV, and vaccine vector AdV for cancer simultaneously are expected to improve the effectiveness of therapy against cancer. The use of an appropriate combination ratio of these two agents will improve their therapeutic potential for cancer [45,46].
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Anatomy Physiology & Biochemistry please click on: https://juniperpublishers.com/apbij/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/apbij/APBIJ.MS.ID.555649.php
#Juniper Publishers#physiology#biochemistry#Juniper Publishers Review#Juniper Publishers LLC#JuniperPublishers
35 notes
·
View notes
Text
Light-Weight Secure IoT Key Generator and Management | Juniper Publishers

Juniper Publishers-Open Access Journal of Robotics & Automation Engineering
Authored by Siew Leong KAN
Abstract
Security is a critical element for IoT deployment that affects the adoption rate of IoT applications. This paper presents a Light-Weight Secure IoT Key Generator and Management Solution(LKGM) for industry automation and applications. Our solution uses minimum computing and memory resources that can be installed on half-credit-card-size embedded systems that enhances the securityof end-to-end communications for IoT nodes. A frequently changed randomly generated passphrase isused to authenticate each IoT node that is embedded with an encrypted unique authentication key. Fieldtest results were presented for an advanced manufacturing application that will only be activated whentwo authenticated IoT nodes are within the vicinity.
Keywords: Authentication; Authority; Secure key; IoT; Security; Industry automation
Introduction
Internet of Things (IoT) is a network of physical objects that have unique identifiers capable ofproducing and transmitting data across a network seamlessly. IoT system refers to a loosely coupled,decentralized system of devices augmented with sensing, processing, and network capabilities [1,2].IoT is projected to be one of the fastest growing technology segments in the next 3 to 5 years [3]. IoTapplications are being developed and deployed in an exponentially increase manner in many smart city’s initiatives around the world. Gartner Group has estimated that there will be 25 billion connectedIoT devices by 2020, and that IoT services will constitute a total spending of $263 billion.Unfortunately, this growth in connected devices brings increased security risks [4]. As indicated byFrost & Sullivan[5]; Miorandi et al., and Weber[6,7], security is the major hindrance for the wide scale adoption of IoT. Inaddition, the increasing use of multi-vendors IoT nodes which are often only have minimum securityprotection that resulted in more complex security scenarios and threats beyond the current Internet iswill arise.Constant sharing of information between “things” and users can occur without proper authentication and authorization. Currently, there are no trustworthy platforms that provide access control andpersonalized security policy based on users’ needs and contexts across different types of “things”.The “things” in any IoT network are often unattended; therefore, they are vulnerable to attacks.Moreover, most IoT communications are wireless that make eavesdropping easy [6,8]. The futurewidespread adoption of IoT will extend the information security risks far more widely than the Internethas to date [9].In an ad-hoc IoT network where IoT nodes are localized and self-organized, network infrastructureis not required. Security of the IoT nodes that operate in such ad-hoc peer-to-peer networks areincreasingly becoming an important and critical challenge to solve as many applications in such IoTnetwork becomes commercially viable. As ad-hoc IoT network has a frequently changing networktopology, and the IoT nodes have limited processor power, memory size and battery power, acentralized security authentication server/node becomes impractical to be implemented.
Methods
In our applied research work, “KeyThings” was developed as part of the project title “Collaborative Cross-Layer Secure IoT Gateways” funded by the Singapore NRF-TRD. Our solution consisted of two main systems, namely the Security Key Generation System (SKG) and Security Key Management System (SKM). The objective of our project is to allow an IoT application (e.g. a web service, etc.) to be activated only when a pre-determined number of authenticated IoT nodes are within the vicinity. This enhances the security of the IoT application by authenticating the hardware (i.e. IoT nodes) instead of just authenticating based on the usual usernames and passwords. The authentication process is done in the system’s background without the need for human intervention which is critical in some operation environment (e.g. manufacturing, production, remote sites, etc.) where not all staff are given access to the sensors’ readings due to security issues. The staff are categorized into “non-authorized”, “operator” and “supervisor”.Below are the features of our Solutiona. “Non-authorized” personnel who are not issued with the authenticated IoT node will not have 60 access to the sensors’ readings.b. Only authorized “operator” who has an authenticated IoT node is able to view the sensors’ 62 readings only when the “operator” is in the vicinity.c. The authorized “supervisor” with an authenticated IoT node that is with higher access rights, 64 can view the sensors’ readings and the summary report. If the “supervisor” leaves the vicinity, 65 the summary report will no longer be available.d. All authentications are done in the solution’s background without the need for human 67 intervention.
Solution Setup Equipment (Figure 1)A.
The setup consists of the following equipmenta. Authentication Serverb. Client device 1c. Client device 2d. Application Servere. Tablet
Authentication server (KeyThings-Server): The authentication server is the “brain” of the security key management. It has the following 92 responsibilities:
A. Access point: Serves as the access point to the entire system
B. Generate random passphrase periodicallyi. If there is no authenticated device, the passphrase will remain the same.ii. If there is one or more authenticated device, a new random passphrase will be generated at 98the end of each time interval (after every 5 MQTT broadcasts).
C. MQTT Server: It will broadcast the generated passphrase via MQTT to all subscribedKeyThings-Clients.i. Once every 2 seconds.ii. MQTT topic: authentication/challengeD. Web Server via REST API.E. For KeyThingsi. -clients to submit their encrypted passphrase.ii. For application server to query the number of authenticated devices.F. Authentication: The server stores the encrypted credentials and MD5 of the KeyThings-Clients that were generated from the Security Key Generation System.
Client devices (KeyThings-Client): Each client device contains the unique security key that is used for authentication to gain access to 113 different web services. The key must be generated from the Security Key Generation System. Thedevice has the following responsibilities:
A) MQTT client. Registers and listens to the broadcasted passphrase.
B) Encryption. Encrypts the passphrase that was received via MQTT.a. If the received passphrase is the same as previous passphrase, the device will just ignorethepassphrase and does nothing.b. If the received passphrase is different from the previous passphrase, then the passphrase will be encrypted.
c. HTTP Request / Response. Send the encrypted passphrase to the authentication server(KeyThings- Server) once the encryption has been completed.
Application server: The application server hosts the production webpage (i.e. the machine readings and summary report). It is currently running on Raspberry Pi, but it can be hosted on any environment (i.e., Windows or Linux) that has network connectivity to the Access Point. The application server has the following responsibilities:a) HTTP Request / Response: Host the webpage that can be access via the tablet.
Tablet: The tablet is used to view the web page that contains the manufacturing data (machine readings andsummary report) from the application server.ResultBelow is what you will see when different numbers of devices have been authenticated Figure 2.Go toDiscussionThe test was conducted successfully with results indicated that a light-weight security key generation and authentication method can be easily implemented in a distributed manner for a self-organizingnetwork to enhance IoT nodes and service level security in an industry automation environment. The method and the solution can be applied to provide features such as multi-level security for different stake holders in an advanced manufacturing environment, multi-factor security keys, user definable security- based services and policy, etc. The solutions can easily be scaled and adapted to suite various industry needs and expectation in enhancing the security of IoT nodes, sensors, PLC controllers, robots, etc. to meet their business needs.
Conclusion
In this paper, a Light-Weight Secure IoT Key Generator and Management Solution (LKGM) for industry automation and applications for enhancing the security of peer-to-peer communications among IoT nodes is presented. The LKGM is integrated to half-credit-card-size embedded systems. Our experimental results showed that the solution enhances secured peer-to-peer IoT communications amongst the IoT node. Field tests were conducted successfully for a manufacturing application that uses web services.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Robotics & Automation Engineering please click on: https://juniperpublishers.com/raej/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/raej/RAEJ.MS.ID.555625.php
#Juniper Publishers#Juniper Publishers Review#Juniper Publishers LLC#JuniperPublishers#robotics#automation engineering
28 notes
·
View notes
Text
Soft Clay Treatment Using Geo-Foam Beads and Bypass Cement Dust | Juniper Publishers

Juniper Publishers-Open Access Journal of Civil Engineering
Authored by Mahmoud Samir El-kady
Abstract
Soft clays are usually classified according to their undrained shear strength, Cu. Values of Cu less than 12.5kPa are associated with very soft clays, whereas, soft clays possess undrained shear strength ranging between 12.5kPa and 25kPa. In addition to the low shear strength of soft clays, they experience high compressibility upon loading. This is why soft clays are considered as problematic for foundation purposes. Also, Geo-foam is an industrial material, characterized by a very low unit weight (average of 20kg/m3) compared to that of the soil. Having a density ranging from 1.0% to 2.5% of that of soil EPS possesses a compressive strength ranging between 70kPa and 140kPa and an elastic modulus ranging between 5MPa and 12MPa, According to Horvath (1997). EPS Geo-foam blocks are used in a wide range of geotechnical applications as a light weight fill.So, the main objective of this study is to investigate the geotechnical properties of soft clay with Geo-foam beads and bypass cement dust. Also, investigate the possibility of preparing low strength excavatable fill mixtures. For studying the effect of (Geo-foam beads + CBPD) / soft clay on fluid-state and hardened properties of new fill, experimental work was carried out on two groups of mixture (A&B). Different ratios of (Geo-foam beads + CBPD) were added to the mixture to study its effect on flow consistency, dry unit weight, unconfined compressive strength, and shear strength. The results of test conducted on the materials illustrated that, cement bypass dust and excess foundry sand can be successfully used to procedure self-compaction, self-leveling excavatable flowable fill material. The unconfined compressive strength of the studied mixtures without Geo-foam ranged between 271.8kPa and 1405.14kPa at CBPD between 3.88% and 18.63%. The Cohesion values for group with Geo-foam with ranged between 50kPa and 20kPa at Geo-foam between 0.32% and 1.35%. The friction angle of group with Geo-foam with ranged between 10 and 22kPa at CBPD between 0.32% and 1.35%.
Keywords: Geo-foam Beads; Bypass Cement Dust; Flowable Fill; Shear Strength
Introduction
EPS Geo-foam blocks are used in a wide range of geotechnical applications as a light weight fill. The primary function of Geo-foam is to provide a lightweight void fill below a highway, bridge approach, embankment or parking lot [1]. EPS Geo-foam minimizes settlement on underground utilities. Geo-foam is also used in much broader applications, the major ones being as lightweight fill, green roof fill, compressible inclusions, thermal insulation, and (when appropriately formed) drainage. Expanded polystyrene (EPS) Geo-foam has been used as a geotechnical material since the 1960s. EPS Geo-foam is approximately 1% the weight of soil and less than 10% the weight of other lightweight fill alternatives. As lightweight fill, EPS Geo-foam reduces the loads imposed on adjacent and underlying soils and structures [3].EPS Geo-foam is not a general soil fill replacement material but is intended to solve engineering challenges. The use of EPS typically translates into benefits to construction schedules and lowers the overall cost of construction because it is easy to handle during construction, often without the need for special equipment, and is unaffected by occurring weather conditions [3]. EPS Geo-foam can be used to replace compressible soils or in place of heavy fill materials to prevent unacceptable loading on underlying soils and adjacent structures. The high compressive resistance of EPS Geo-foam makes it able to adequately support traffic loadings associated with secondary and interstate highways [4]. Also, using EPS Geo-foam eliminates the need for compaction and fill testing, reduces the construction time and minimizes impact to the existing roadway and adjacent structures and/or buried utilities [5]. Experimental work was carried out on two groups of mixture (A&B) and different ratios of (Geo-foam beads + CBPD) were added to the mixture to study its effect on the geotechnical properties.
Experimental Program Material characteristics
The soft clay was dried in the oven at 110C. It is passing through sieve size of 0.25mm. Soft clay characteristics are listed in Table 1.Also, the unit weight of the Geo-foam beads is 15.0kg/m3. The size of the Geo-foam beads is 5.0mm Figure 1a.Mixture proportionsThe experimental work was divided into two groups, each with the same size of 600cm3. Group A was divided into five subsamples without the use of Geo-foam and mixed with increasing percentages of CBPD (50g) for each sample and different percentages of water. In addition, the B group was divided into five sub-samples and mixed with increasing percentages of Geo-foam (5g) for each sample as well as different percentages of water with stable weight of CBPD as shown in the following Tables 2-5.
Experimental Work and Results Flow consistency
Samples were mixed for groups A-B for different percentages of water as shown in Figure 1b. The consistency flow of the samples was measured for each sample. It is found that the flow consistency increased slightly for group B than for group A. So, the flow consistency was measured in laboratory as listed in (Tables 6-7 ) for the two groups. Although the percentage of water present in the B samples, the effect of the presence of Geofoam beads than bypass cement dust on soil was clear as shown in Figure 2.Unconfined compressive strengthThe studied mixtures for each group were molded and hardened. Unconfined compressive strength was obtained by the Triaxial test for the studied mixtures as shown in Figures 3. It was found that with the increase of cement bypass dust, the unconfined compressive strength increased significantly and especially for the samples (A4 - A5) compared to a slight increase in the values of the strain% as shown in Figure 4. Also, compressive strength values are also stabilized with increasing mixing rates in cement bypass dust from approximately 14 to18% as shown in Figure 5. This shows the significant effect of cement bypass dust on compressive strength of studied samples.Shear strengthShear box test was carried out on the studied samples. The samples were loaded with increasing stresses (50-100-150kPa)and the shear stresses were calculated versus horizontal displacement (mm). We took samples (A4-B4) for examples as shown in Figures 6-7. Shear strength parameters were obtained from direct shear test and it is concluded that CBPD affected in the cohesion of the group A samples as shown in Figure 8. On the contrary, angle of internal friction was increased significantly when increasing the ratio of Geo-foam beads for group B samples as shown in Figure 9 [6-10].
Conclusion
This paper presented an experimental study of various samples of soft clay mixed with different percentages of Geofoam beads and cement bypass dust. The following conclusions may be drawn:A. The results of test conducted on the materials illustrated that, cement bypass dust and excess foundry sand can be successfully used to procedure self-compaction, selfleveling excavatable flowable fill material.B. The dry unit weight of the studied mixtures for group without Geo-foam ranged between 1.40 and 1.6 gm/cm3 at CBPD between 3.88% and 18.63%.C. The dry unit weight of the studied mixtures for group with Geo-foam ranged between 0.65 and 1.20 gm/cm3 at Geo-foam between 0.32% and 1.35%.D. The unconfined compressive strength of the studied mixtures without Geo-foam ranged between 271.8kPa and 1405.14kPa at CBPD between 3.88% and 18.63%.E. The unconfined compressive strength of the studied mixtures with Geo-foam ranged between 230kPa and 120kPa at Geo-foam between 0.32% and 1.35%.F. The Cohesion values for group without Geo-foam with ranged between 62kPa and 105kPa at CBPD between 3.88% and 18.63%.G. The Cohesion values for group with Geo-foam with ranged between 50kPa and 20kPa at Geo-foam between 0.32% and 1.35%.H. The friction angle of group without Geo-foam with ranged between 3 and 11° at CBPD between 3.88% and 18.63%.I. The friction angle of group with Geo-foam with ranged between 10° and 22° at CBPD between 0.32% and 1.35%.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Civil Engineering please click on: https://juniperpublishers.com/cerj/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/cerj/CERJ.MS.ID.555701.php
#JuniperPublishers#Juniper Publishers Review#Juniper Publishers LLC#Juniper publishers#civil engineering
49 notes
·
View notes
Text
Observational Study: Cancer Cases Treated with Homeopathy in the Basque Country/Navarre between 2013 and 2015
Juniper Publishers-Open Access Journal of Complementary Medicine & Alternative Healthcare
Authored by Victoria Claramunt Palou
Abstract
The Study included 50 women and 15 men aged between 11 and 85 years. There we 44 patients with advanced tumour disease and 21 with early-stage disease. Conventional cancer treatment was chosen by 64 patients and one of them chose homeopathy only. Four patients made important changes in their lifestyle, and 8 had bio-decoding sessions. All patients had taken homeopathic medicines as palliative care tailored to different stages of their disease. A single drug treatment was used in 18 cases, based on the entire case. Ten cases we treated by applying Banergi protocols and constitutional medicine, and 37 cases were treated with different successive or combined drugs, depending on the state of the patient at the time, with the Minotti protocol for palliative care being applied in 9 cases. The predominant homeopathic dilutions were centesimals. The great variability of medications used on each of the patients shows the individuality of patient symptoms with the same clinical diagnosis, as well as the great variability in the criteria of homeopathy doctors when establishes a therapeutic strategy.Homeopathy has helped to control the tumour disease (patient free of disease) in 10 cases of early stage cancer and 12 cases of advanced tumour disease. Homeopathy was only palliative in 7 cases of early-stage cancer, in 22 cases of advanced tumour disease, and in five other cancers without staging. Homeopathy did not work in one case of early stage cancer, in two cases of advanced tumour disease, and in one case without staging. There were 5 cases in which results could not be assessed at the time of the study. According to the subjective assessment by the homeopathic doctor, homeopathy contributed to the control of tumour disease (patient free of disease with biological and /or imaging tests) in 22 cases, it was palliative in 34 cases, 4 patients died, and 5 cases cannot yet be evaluated. According to the assessment by the patient, it helped to control and improve their quality of life in 55 cases and it does not help them at all in 5 cases. This observational study has enabled us to evaluate the effectiveness of our work in the context of our clinical reality and more accurately describe all parameters involved in the case, including conventional treatments and their impact. Patient opinion is part of the evaluation of the results and requires questionnaires that can be adapted and standardized. Homeopaths carry out their work within an ethical framework bound by civil responsibility and respect for patient autonomy, open to collaboration with the work of the other professionals with a common goal, which is none to cure, relieve the patient, and contribute to the advancement of knowledge.
Keywords: Advanced tumour disease; Early-stage disease; Lifestyle; Bio-decoding; Palliative; minotti protocol; Patient free of disease; Staging; Standardized
Introduction
Homeopathy exercised by doctors is abided to a deontological code common to the medical profession and to a social responsibility setting established by law. Moreover, we homeopath doctors respect the patient’s autonomy and do not compete with other therapeutic possibilities. We homeopath doctors are willing to collaborate with other medicine professionals and to equip ourselves with investigation and evaluation tools that will permit progress of the scientific knowledge.What does homeopathy offer to oncology patients?Active listening, reflection scenarios, full symptomatic patient treatment and use of medicines with few and reversible adverse effects compatible with chemotherapy, radiotherapy and hormonotherapy. Another, not least important aspect is that a homeopathy treatment is short and inexpensive.Reflection scenario: raising awarenessThese four questions open a therapeutic space of active listening for the patient and the doctor (Figure 1). The patient evolves from being a case of adenocarcinoma to being an ill individual to whom we intend to help by searching for the most accurate medicine that suits him, his suffering and the tumor. The patient must understand his vulnerability and those facts, emotions or ways of life that make him sicken. For that he is given a reflection space. We do not speak about statistics or predictions. We commit ourselves to him, to help and attend his needs. Undoubtedly, in our job as homeopath doctors this active listening is part of our therapeutic grounding.Approaching the oncology patientThe oncology patient is a complex one. Besides his natural illness (the tumor), he also presents an artificial sickness derived from the adverse effects of his oncological treatment. Moreover, the impact of the diagnosis as well as the disease prognosis that, just by themselves, many times destabilize the patients, must be also be considered. For the homeopath, restoring the mental and physical equilibrium of the patient is a priority. Help him bear the treatments, make him lead the processes and maintain the hope alive, are also essential. In this case, a respectful atmosphere for cooperation would be the ideal for the patient and the treatment’s result.
Observational Study (Appendix 1)Samplea.
65patient cases with different cancer diagnosis are collected at homeopath consultations in the Basque country/ Navarre during the period 2013-2015.b. Monitoring for 18 of the cases has been done at a health public service (primary attention) as for the rest 47 cases monitoring has been done at private consultationc. Patients from both sexes: 50 women and 15 mend. Ages between 11 and 85 years olde. A total of 44 patients present an advanced tumor diseasef. 21 patients present the disease in an initial localized phase
Diagnoses
Table 1 shows the diagnoses along with the correspondent phase and number of cases. Simultaneous treatments to the homeopathy treatment (Table 2).Common treatmentCommon treatment includes a combination of different procedures in which following different protocols, chemotherapy, radiotherapy, surgery and hormonotherapy can be combined for a healing or palliative purpose.Lifestyle changeLifestyle changes include change processes in habits such as diet or tobacco consumption, as well as changes in work, personal or family relations starting by a conflict awareness raising from the patient.
Biode Coding
Awareness raising and emotional unloading in relation to the conflict that unleashes the disease following a specific technique.Used strategies at the homeopathy consultationa. All sample patients have taken palliative treatment adapted to various disease stages.b. Patients given a single medicine base on the situation and patient’s constitution: 18 cases.c. Banergi protocols and patient constitution based medicine: 10 cases.d. Other combined or successive medicines adapted for the patient: 37 cases.e. Minotti’s protocol (PAC): 9 cases.
Potency usage in prescriptions
Table 3 shows the prescribed potencies. The homeopathic medicine stimulates the healing capacity of every patient. Moreover, it also, at the same time, acts in the mental, emotional and physical areas. It is this aspect to which we refer when we speak about totality. The homeopathic medicine is compatible with other treatments and has few adverse effects. The great variety of the medicines used in each patient expresses the symptom individuality of the patients with the same clinic or anatomopathological diagnose. Also, expresses the great criteria variability of the homeopath doctor when establishing a therapeutic strategy.*Solution to the following medicines: ADN 6 CH, Hepatine 6 CH, Bone marrow 6 CH, Cardine 6 CH, Anilium 6 CH, Hairy Cranium Area 6 CH (Dr. Minotti’s formule).
Homeopathy effectiveness estimation at the case management
Homeopathy has contributed to control the tumor disease (free of disease patient) at the following cases (Table 4):a. Localized tumor disease (N0, M0): 10 casesb. Advanced disease (from phase II onwards): 12 casesHomeopathy has turned out to be palliative only at the following cases (Table 5):i. Localized tumor disease (N0, M0): 7 casesa. Advanced illness (from phase II onwards): 22 casesb. Non-determined phase cases: 5 casesii. Homeopathy has not worked in the following cases (Table 6):a. Localized tumor disease (N0, M0): 1 caseb. Advanced illness (from phase II onwards): 2 casesc. Non-determined phase cases: 1 case (Table 7)iii. Efficacy estimation based on the doctor:a. Contributes to control the tumor disease (at the actual moment, free of illness patient with biopsy, image, scoreboards, endoscopy, etc. records): 22 cases.b. Contributes only to palliate the effects of the disease or treatment (chemotherapy and radiotherapy), quality of life, tolerance to adverse effects: 34 cases.c. Dead patients: 4 cases.d. Cannot yet be established if the treatment works: 5 cases.e. Treatment does not work: 4 casesiv. Effectiveness estimation based on the patient:a. Has helped to control and improve my quality of life during the treatment: 55 cases.b. Has not helped at all: 5 cases.c. Without opinion: 5 cases.
Used homeopathic medicines1) Constitution based medications:A. Natrum Muriaticum: 9 cases.B. Pulsatilla: 8 cases.C. Lachesis: 4 cases.D. Calcarea Carbonica: 4 cases.E. Veratrum: 2 cases.F. Staphisagria: 8 cases.G. Samarium: 1 case.H. Alumina: 1 case.I. Germanium: 1 case.J. Ustilago: 1 case.K. Sepia: 8 cases.L. Aurum Metallicum: 6 cases.M. Ferrum Phosphoricum: 3 casesN. Aconitum: 3 cases.O. Sulphur: 2 casesP. Aranea Diadema: 1 case.Q. Silicea: 1 case.R. Ignatia: 1 case.S. Argentum Nitricum: 1 case.2) Medicines in relation to the tumor disease:A. Conium Maculatum: 14 cases.B. Phytolacca: 10 cases.C. Kalium Carbonicum: 4 cases.D. Chelidonium: 3 cases.E. Hydrastis Canadensis: 3 cases.F. Asteria Rubens: 2 cases.G. Rhododendron: 1 case.H. Carcinosinum: 8 cases.I. Thuya: 9 cases.J. Kalium Bichromicum: 3 cases.K. Calcarea Phosphorica: 3 cases.L. Ruta: 2 cases.M. Carbo Animalis: 2 cases.3) Table 8 shows the medicines used with palliative purpose for:A. Radio dermatitisB. MucositisC. Nauseas and vomitsD. WeaknessE. SadnessF. FearG. SwellingH. Post-operativeI. AnemiaJ. LeukopeniaK. ThrombocytopeniaL. Helps to dieM. Dyspnea.
How can we know, with accuracy, the effectiveness of our intervention?
To us, homeopaths, can be reproached that we do not publish our results, which is true, we barely do it. The purpose of the homeopathy associations and academies, is to offset this reality raising awareness amongst our colleagues of the importance of recording the cases homogenously and of publishing clinical results, at least, in our magazines. Due to the nature of the homeopathic practice, we must also explore new designs to contrast our results. We must change the subjective assessment of our work with validated tools from the general medicine sphere such as the life quality tests proposed by the EORTC (European Organization for Research and Treatment of Cancer) and other tools proposed by the ECH (European Committee for Homeopathy). In one word, use the common language of science to contrast our results. We prepare ourselves to search a respectful collaboration with other medicine professionals that help patients from a conventional perspective. This is the propose of integrative medicine: the patient improves and the science makes progress [1-6].
Conclusion
At the presented sample, we are conscious that at the time of collecting the data, the free of illness patients still have a long journey of regular medical checks and that, at worse, they might present relapses of their tumor disease. Our purpose as doctors is to be available at this stage of the patients’ life. Nowadays, one of the cancer treatments objectives, in those cases in which the illness cannot be cured, is to make the disease a chronic one. In our sample, there are two patients that present this situation and undoubtedly, homeopathy along with other procedures (palliative chemotherapy, hormonotherapy, etc.) helps them to get along with their lives.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Complementary Medicine & Alternative Healthcare please click on: https://juniperpublishers.com/jcmah/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/jcmah/JCMAH.MS.ID.555726.php
#Juniper Publishers#Juniper Publishers Review#JuniperPublishers#Juniper Publishers LLC#complementary medicine#health care
26 notes
·
View notes
Text
The Prevalence of Bovine Trypanosomiasis in JabiTehnan District of Amhara Regional State, Ethiopia

Juniper Publishers-Open Access Journal of Cell Science & Molecular Biology
Authored by Melak Wondie
Abstract
Cross sectional study was conducted in Jabi Tehnan District of West Gojjam Administrative Zone of Amhara Regional State, Ethiopia to determine the prevalence of bovine trypanosomiasis. In the parasitological survey, blood samples of 164 cattle were examined using a buffy coat technique. The Packed Cell Volume (PVC) value of each animal was also measured using hematocrit reader. The overall prevalence of trypanosomiasis was found to be 15.24% and it consists of 9.76% and 20.73% in Adankegne and Ergib peasants’ association, respectively (X2=5.783, p=0.056). The most positive cases were due to Trypanosoma congolense (T. congolense ) (80%) followed by Trypanosoma vivax (T. vivax)(20%). The mean(PCV) values of parasitaemic and aparasitaemic animals during the study period were 20.75% and 25.07%, respectively. The variation in mean PCV values were statistically significant (p=0.01). The study also demonstrated statistically significant (X2=13.886, p=0.001) variations in prevalence between sexes of cattle, which were 10.67% and 19.1% in female and male animals, respectively. The present prevalent study generated valuable information on the epidemiology of bovine trypanosomosis in the study area and revealed that trypanosomosis was an important disease affecting the livestock production
Keywords: PCV; Prevalence; Trypanosoma congolense; Trypanosoma vivax; Bovine
Introduction
Livestock is backbone of the socio-economic system of most of the rural communities of Africa [1]. Ethiopia is known for its large and diverse livestock resource endowments. Livestock is primarily kept on small holdings where it provides drought power for crop production, manure for soil fertility and fuels, serves as a sources of family diet and sources of cash income (from sale of livestock and livestock products). Despite large livestock population, Ethiopia fails to optimally utilize this resource due to different constrains facing the livestock subsector. Shortage of nutrition, reproductive insufficiency, management constraints and animal disease are the major constraints [2]. One of the diseases hampering the livestock subsector is trypanosomosis [3]. Trypanosomosis is a complex disease of protozoa that is caused by different species of unicellular parasites (trypanosome) found in the blood and other tissues of vertebrates, including livestock, wild life and people [4]. Trypanosomosis limited to the extension of natural herds particularly in Africa were the presence of the tsetse fly density access to woodland and savanna areas with good grazing potential [3]. It is a serious constraint to agricultural production in extensive areas of the tsetse infested regions which accounts over 10 million squares of the tropical Africa [5].Ethiopia is one of the countries suffering from the impact of trypanosomosis. In Ethiopia, it is estimated that some 10 to 14 million heads of cattle and an equivalent number of small ruminants together with a significant number of equines and camels, are exposed to the risk of trypanosomosis [6]. Six species of trypanosomes are recorded in Ethiopia and the most important trypanosomes in terms of economic loss in domestic livestock are the tsetse transmitted species T. congolense, T. vivax and T. brucei [3].Tsetse flies in Ethiopia are confined to western and south-western parts of the country between 33°C and 38°C E longitude and 5°C and 12°C N latitude. It is estimated to cover an area of 140, 000, 220, 000 km2[7]. Tsetse infested areas follow the major river systems; namely, Abay (Blue Nile), Baro, Akobo, Didessa, Ghibe and Omo river systems [8]. Five species of Glossina (Glossina morsitans submorsitans, G. pallidipes, G. tachinozdes, G.f. fuscipes and G. longipennis) have been recorded in Ethiopia [3]. According to National Tsetse and Trypanosomosis Investigation and Control Center [7], tsetse transmitted animal trypanosomosis still remains as one of the largest causes of livestock production losses in Ethiopia. The effects of trypanosomosis is not only the direct losses resulting from mortality, morbidity, infertility of the infested animals and costs of controlling the disease, but also due to indirect losses, which include exclusion of livestock and animal power-based crop production from the huge fertile tsetse infected areas. Annual estimated losses for Ethiopia as a result of trypanosomosis is roughly $200 million, in terms of mortality and morbidity losses in livestock (excluding utilization of fertile land for crop and livestock production) and the costs included in controlling the disease [9].The most prevalent trypanosome species in tsetse infested areas of Ethiopia are T. congolense and T. vivax. Rowlands et al. [10] reported a prevalence of 37% for T. congolense in Southeastern Ethiopia. Abebe and Jobre [11] reported an infection rate of 58% for T. congolense , 31.2% for T. vivaxand 3.5 % for T. bruceiin Southern Ethiopia. In the same report it is also indicated that 8.71% infection rate was recorded in the highlands (tsetse free areas) of which 99% is due to T. vivax. Different workers [12- 14] indicated a prevalence of 17.2%, 21% and 12 % in Metekel district, in upper Didesa Valley and Southern Rift valley areas of tsetse transmitted regions, respectively, and the dominant species was T. congolense .In the western part of Amhara Regional State bordering the Abay river basin, one of the north western tsetse belt areas of Ethiopia, tsetse transmitted trypanosomes are becoming a serious threat for livestock production and agricultural activity in particular. Reports made by the Regional Veterinary Laboratory in 1999 indicated the presence of tsetse fly transmitted trypanosomosis in three districts of the region (Bure, Jabi Tehnan, and Ankesha) bordering the Abay valley areas. A preliminary survey conducted in Dembecha district by the Ethiopian Science and Technology Commission and West Gojjam Veterinary Office in 2001 indicated a trypanosome infection rate of 23% with a dominant species of T. congolense and tsetse fly identified was G. morsitans. Therefore, this study was undertaken to determine the prevalence of bovine trypanosomosis, to identify the dominant species of trypanosomes involved, and to assess the PCV values of cattle in relation to the risk factors associated with the disease.
Materials and Methods
Study area
The study was conducted in Jabi Tehnan district of west Gojjam Administrative Zone of Amhara Regional State. The district covers an area of 112,772.1 ha and bordered by Quarit and DegaDamot in East, Burie in West, Sekela in North, and Dembecha and Abay River in the South. The annual mean temperature for most part of the district is 14-32°C and the elevation varies from 1500-2300 mm above sea level (m a. s. 1) with mean annual rain fall of 1250mm. The livestock populations that are found in Jabi Tehnan district include cattle, sheep, goats, horses, mule, donkey and poultry. Among these animals, cattle are the dominant species raised in the area. The cattle population in the district is estimated to be about 187,481[15] (Figure 1).Study animalsThe study was conducted on local Zebu cattle. These animals were raised in different villages of Adankegne and Ergib of Jabi Tehnan district. The animals examined in this particular study were representing different Kebeles. Sex and body conditions of cattle were also being recorded accordingly.
Study design
The retrospective data of cross sectional survey was conducted to determine the prevalence of bovine trypanosomosis. The two sites were selected based on their higher prevalence of trypanosomosis than any other Kebeles of Jabi Tehnan district.
Sample size and sampling methods
The sample size was calculated using previous prevalence of 11.7% by [17] and desired absolute precision of 5% as per the standard procedure described by Thrusfield [18] shown below. An estimated minimum sample size of 159 cattle was obtained; however, we were able to examine 164 cattle for our study.
Study Method and Procedure
Buffy coat technique
Blood was collected from an ear vein using heparinized microhematocrit capillary tube and the tube was sealed. A heparinized capillary tube containing blood was centrifuged for 5 minutes at 12,000rpm. After centrifugation, trypanosomes were usually found in or just above the buffy coat layer. The capillary tube was out using a diamond tipped pen 1mm below the buffy coat to include the upper most layers of the red blood cells and 3mm above to include the plasma. The content of the capillary tube was expressed on to slide, homogenized on to a clean glass slide and covered with cover slip. The slide was examined under x40 objectives and x10 eye piece for the movement of parasite [19].
Measuring of packed cell volume (PCP)
Blood samples were obtained by puncturing the marginal ear vein with a lancet and collected directly into a capillary tube. The capillary tubes were placed in micro-hematocrit centrifuge with sealed end outer most. The tube was loaded symmetrically to ensure good balance. After screwing the rotary cover and closing the centrifuge lid, the specimens were allowed to revolve at 12,00rpm for 5 minutes [4,20]. Tubes were then placed in hematocrit and the readings were expressed as a percentage of packed red cells to the total volume of whole blood. Animals with PCV ≤ 24% were considered to be anemic [21].Data analysisRow data on individual animals and parasitological examination results were inserted into MS Excel spread sheets to create a data-base. Students t-test were employed to compare between the two-independent mean PCV values of animals from an individual site (peasant’s association). Chi-square test was also employed to assess the association between the risk factors and the disease. While analyzing data, p-values (p)<0.05 were registered as statistically significant. Otherwise, recorded as insignificant.
Result
Prevalence
Out of the total 164 (75 females and 89 males) cattle examined, 25 (15.24%) were found positive to trypanosomosis. The prevalence varied between different study areas, in which 9.76% (n = 8) and 20.73% (n = 17) were recorded at Adankegne and Ergib peasant’s association, respectively. The variation in the prevalence of bovine trypanosomosis between the study sites were not statistically significant (X2= 5.783; p = 0.056) (Table 1 and Figure 2). The most prevalent trypanosome species in the study area was T. congolense (80%) followed by T. vivax(20%) (Table l and Figure 2). The prevalence of bovine trypanosomosis showed statistically significance difference between sexes of cattle, in which, higher in male animals (19.1%) as compared to females (10.67%) (X2= 13.886; p = 0.001) (Table 2 and Figure 3).
Hematological findings
Discussion
The study revealed that the prevalence of bovine trypanosomosis in the area was 15.24% (25/164) which was higher compared with the previous findings of Bitew et al. [17] in the same area (11.7%). The difference in prevalence might be due the site from which the blood samples were collected. However, there were tsetse control intervention, and continuous treatment of sick animals as well as deforestation for the cultivation of land. These activities could have led to the reduction of tsetse fly population along with the decline of tsetse borne trypanosomosis in the study area. But the continuous and longtime utilization of trypanocidal drugs particularly Diminazin aceturate in the study area contribute for the development of drug resistance, so that the prevalence of trypanosomosis was higher than the previous finding due to the above reasons.In this study, two species of trypanosomes; namely, T. congolense and T. vivax were retrieved from inspected cattle. Majority of infections were also due to T. congolense. The higher proportion of T. congolense infection in the study area was in agreement with trypanosome species prevalence data from other tsetse infested region of Ethiopia where T. congolense is the most prevalent species in cattle [11]. In the same report it was also indicated that in tsetse free area of highlands, 99% of prevalence was due to T. vivax [12-14]. But in this study area, the prevalence of T. vivaxwas less than T. congolense in both peasant associations because the two sites are located adjacent to tsetse infested belts. Leak [22] and Degneh et al. [23] also indicated that T. vivax was highly susceptible to treatment while the problems of drug resistance were higher in T. congolenseM.In the current study, higher infection rate of trypanosomosis was detected in males (19.1%) as compared to in female cattle (10.67%) with statistically significant difference (X2= 13.886; p = 0.001). Different researchers work supported this finding [22- 25]. Although the variation was not statistically significant, Yalew and Fantahun [26], and Teferi and Biniam [27] had also reported higher prevalence of bovine trypanosomes in males than in females (X2 = 0.85, p=0.35 and X2= 0.10, p>0.05, respectively). According to Gemtessa and Dera [28], the higher prevalence of trypanosomes in males rather than in females might be related to the hardworking of male animals. Similarly, the variation in the prevalence between the two sexes might also be associated with that male animals travel longer distances to tsetse abundant areas for draught and ploughing purposes, and the journey creates stress leading to susceptibility to the infection [23,)].In contrast to this study,Kitila et al. [30] at Yayo District Illuababora Zone of Western Oromia and Tamirat et al. [31] at Enemorena Ener Woreda of Gurage Zone were found higher prevalence of bovine trypanosomosis in female cattle than males.Comparing the mean PCV values of cattle, significantly (p=0.01) low PCV was recorded in parasitaemic animals (25.07%) (SD = 0.989; df = 6; t-value = 8.069) than in aparasitaemic animals (20.75%) (SD = 1.601; df = 152; t-value = 40.316). This finding was in line with previous works conducted at different regions of Ethiopia by many authors [22,25]. In the absence of other diseases causing anemia, a low PCV value of individual animals is a good indicator of trypanosome infection [23,32]. Trypanosomosis might adversely lower the PCV values of infected animals [33]. A survey conducted in cattle in Hawagelan District of West Wellega Zone [34] revealed that the mean PCV of trypanosome infected animals was significantly lower (20.8±3.2 %) compared to non-infected animals (24.9±3.8 %). A later study in Northwest Ethiopia [35] in cattle experimentally infected with T. vivaxi solates also showed that the mean PCV, Hb and total RBC count were lower (p < 0.001) in all infected groups than in noninfected control animals. In Nigeria, domestic ruminants that were naturally infected with trypanosomes had significantly lower (p<0.05) PCV and RBC counts compared to uninfected animals [36]. Lower herd average PCVs for trypanosomepositive cattle compared to trypanosome-negative cattle have also been reported from Ghana [37], Zambia [32], Cameroon [38] and Gabon [39].In spite of the fact that trypanosome infection has significant association with risk factors such as age and body condition scoring, as reported by many scholars, this study had not demonstrated and regarded as limitations.
Conclusion
From this study it is possible to conclude that trypanosomosis is an important disease and a potential threat affecting the health and productivity of cattle. The major species of trypanosomes in the study area were T. congolense and T. vivax. To sum up, infection with trypanosomosis negatively affects PCV and body condition of animals. This indicated that trypanosome infection of cattle causes loss of body weight and production. Trypanosomosis control measures should be targeted on tsetse fly destruction and control methods such as pour-on and effective trypanocidal drug applications. Similarly, rearing or raising of trypanosomosis resistance cattle breeds is now a day in practical. Otherwise, the problems will increase through the aide of global warming. In conclusion, further study on the occurrence of tsetse and trypanosomosis at different season of the year at different altitudes and species of animals should be conducted.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Cell Science & Molecular Biology please click on: https://juniperpublishers.com/ijcsmb/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/ijcsmb/IJCSMB.MS.ID.555649.php
#Juniper Publishers#Juniper Publishers Review#Juniper Publishers LLC#JuniperPublishers#cell science#molecular biology
35 notes
·
View notes
Text
Prevention of the Development of Diabetes by Early Intervention-JuniperPublishers
Abstract
The current research, a retrospective study on early stage intervention on the development of diabetes is based on a concept discussed in 2011 by Ralph A De Fronzo and Muhammad Abdul-Ghani in a publication by American Diabetes Association.
The Research comprises of early recognition of the patients at the stage of developing IGT and initiation of treatments with oral hypoglycaemic agents in order to reach a normal HbA1C. The overall number of patients in practice were 5000. And those with IGT were 26. The research was started 7 years ago and has resulted in these patients reaching a HbA1C of 5.2. The target of treatment was maintaining lower than 5.2.
Metformin has been mostly effective in patients reaching the target value. However, in rare cases Gliclazide was needed. In one Case Acto's and Insulin treatment was essential for a female patient with Polycystic Ovarian Syndrome. The current success has resulted in preventing further complications from diabetes.
In earlier years clinical were advised to start oral hypoglycaemic agents, once the patients had shown a HbA1C of 7.5. However, the evidences have shown that by this stage many complications from diabetes would have occurred.
Keywords: Oral hypoglycaemic agents; Pre-Diabetics; Metformin
Introduction
There has been a dilemma among clinicians as to when to initiate the oral hypoglycaemic agents (OHA) following non pharmacological approaches e.g. diet, exercise and weight loss. Earlier understand was that the medications can be started after the patient had reached a HbA1C value of 7.5. Current Canadian Guideline are HbA1C of 6.1 being in normal range and those with HbA1C of 6.2-6.5 are considered "Pre-Diabetics" or with IGT. As explained in the article by De Fronzo, et al. [1]. Initiation of treatment with appropriate OHA prevents the development of a full blown diabetes. If the clinicians wait until the patient reaches the HbA1C of 7.5, many complications from diabetes already are existing. My experience dates back to approximately 10 years when a patient of mine with HbA1C of 6.9 was started on metformin and subsequently switched to Gliclazide for effective prevention.
Past Investigations
De Fronzo, et al. [1] had established a link between insulin resistance, diabetes, obesity, hypertension, dyslipidaemia and ASSCVD in 1991. Cusi in collaboration with De Fronzo reviewed the metabolic effects of metformin in 1998 [2].
Subsequently, UKPDS Group had focussed on the intensive glucose control with sulfonylurea or insulin and the risk of complications in the patients with Type 2 diabetes in 1998 [3,4]. Later, UKPDS group advanced their research to metformin use with similar objectives. Turner, et al. [5] in 1999 investigated the role of diet, sulfonylurea, metformin or insulin treatment in patients with Type 2 diabetes in conjunction with UKPDS [4,5].
Knowler, et al. [6] in 2002 emphasized on the reduction in the incidence of Type 2 DM with life-style interventions. Abdul-Ghani in 2006 studied the risk of progression to DM by establishing a relationship between post-load plasma glucose and fasting plasma glucose [7]. Holman, et al. [8] reviewed a 10 year follow-up study with intensive glucose control in Type 2 DM. Eriksson, et al. [9] in 2008 emphasized on the significance of diet and exercise in the prevention of Type 2 diabetes. Lastly, Vendetti, et al. [10] in 2008 investigated the role of lifestyle interventions and weight loss.
Method
My current study of diabetes prevention is based on identification of PRE-DIABETICS among a population of 5000 patients. These patients with HbA1C of more than 6.2 were given a starting does of Metformin of 250mg after their evening meal. There was an equal proportion males and females. A total number of 29 patients were identified in the "pre-diabetics" group. They were offered counselling for the diet, lifestyle interventions and followed by lab investigation after one month. If there was no change in HbA1C the patient was offered Gliclazide 15mg with their evening meal and lab monitoring was continued. The patient identified 10 years ago has a history of sinus arrhythmia and suffers from hypercholesterolemia. He has been maintaining a normal HbA1C like other 28 patients with a low dose of OHA and controlled heart disease. It was commonly observed that one to two months of OHA was sufficient for the patient to reach HbA1C of 6.2 or less, provided the treatment was continued. This approach showed the prevention of further complications from diabetes e.g. hyperlipidemia or renal dysfunction.
The likely contribution factors to IGT indentified were family history, obesity, pancreatitis, alcoholism, gestational diabetes or viral diseases. The age of onset was observe between 40 and 50 years.
Results
The results of the retrospective study are listed in the enclosed Table 1.
Conclusion
Early prevention of patients from developing diabetes was achieved by commencing treatment with either Metformin or Gliclazide. Two of my patients observed having a normal HbA1C in the absence of and OHA after a short term initial medical management while others maintained a normal HbA1C with a small dose of OHA with continuation. The patients have been free of any other co-morbidities e.g. CKD or CVD.
To know more about Journal of Urology
Click on: https://juniperpublishers.com/jojun/index.php
To Read more about JuniperPublishers
Click on: https://juniperpublishers.com/index.php
#Juniper Publishers#Juniper Publishers Review#Juniper Publishers LLC#JuniperPublishers#urology#kidney#kidney disease#Nephrology#Open access journal of Urology#open access journals
0 notes
Text
Carboxymethyl Cellulose: Rheological and Pipe Flow Properties | Juniper Publishers

Juniper Publishers-Open Access Journal of Petrochemical Science
Authored by Benchabane A
Abstract
The aim of this work was to investigate aqueous solutions of Carboxymethyl cellulose (CMC). Their rheological properties and pipe flow behaviour in circular cylinder were studied. The rheological properties of the Carboxymethyl cellulose used were determined in circular pipe flow using an Ultrasound Pulsed Doppler Velocimeter combined with the Pressure Difference method (UPDV+PD). The studied fluids showed a non-Newtonian rheological behaviour that can be well described by the two parameters Oswald-de Waele model (power law model). The rheological properties of two concentration of the Carboxymethyl cellulose (0.1 and 5%) were determined directly in-line of the flow facility. The flow curve obtained was compared to the off-line measurements obtained using a conventional rotational rheometer. The UPDV+PD method was demonstrated to be able for velocity profile visualization and for determining the true flow curve and rheological properties of CMC solutions.
Keywords: Polymer; Carboxymethyl cellulose; UPDV; Non-Newtonian fluids; Pipe flow
Abbreviatations: CMC: Carboxymethyl Cellulose; UVP: Ultrasound Velocity Profiling; PD: Pressure Difference; UPDV: Ultrasound Pulsed Doppler Velocimetry
Introduction
Carboxymethyl cellulose (CMC) is a cellulose derivative which is extensively used polymer in a wide range of applications. For its different properties such as its good binding, thickening and stabilizing, CMC is utilized in various products in cosmetic and pharmaceutical applications (creams, lotions, toothpaste formulation…). However, CMC is used to improve moisturizing effects thanks to its polymeric structure that acts as film forming agent [1-3]. The CMC is used in many other industries such as food, ceramic, and paper industries [1,2]. Anionic polymers of high molecular weight such as CMC are used to stabilize clay particles thanks to the electrostatic interactions between the anionic chains of the polymer and the electric charge at the edge of the clay particles [1,2]In petroleum industry, where drilling muds are of particular importance, bentonite / polymer blends are often used as drilling fluids. Polymers such as CMC are used for stabilizing and plastering the clay suspension, increasing the viscosity, controlling the mud losses and maintaining adequate flow properties at high salinity, pressure and temperature [1,2]. The rheological properties of these fluids make its flow behavior complex and require special attention to be better understood.However, the number of experimental works which are published on the pipe flow of the Carboxymethyl cellulose and their rheological behavior in pipe is small. The rheological properties of CMC solutions are much more documented [2, 4-8]. The rheological properties of different concentrations of CMC solutions were investigated by Ghannam and Esmail [4]. The authors have reported nearly Newtonian behavior at the lowest concentration and pseudo-plastic, thixotropic, and viscoelastic responses at the higher-end concentrations. The rheological behavior of higher concentrations of CMC solutions have been investigated by Edali et al. [5] in their work. The authors confirmed both non-Newtonian and and viscoelastic properties of Carboxymethyl cellulose that have been found to be much more pronounced. In their review paper, [6] investigated the pseudo-plastic flow behavior, the viscoelastic, and the rheo-optical properties of various water-soluble cellulosic derivatives.The rheological properties of different mass concentrations of CMC solutions were investigated by Benchabane and Bekkour [2] at a constant temperature. The forth parameter Cross model was used to correlate the experimental results. Later, Bekkour et al. [3] studied the effect of temperature on the rheological properties of CMC solutions in a presence of soluble fiber pectin, at different mass concentrations. It was clearly determined that the type of CMC, the temperature and particularly the concentration significantly influences the rheological behaviour of CMC dispersions [2,3, 4-9].In case of non-Newtonian fluids, it was shown that pressure drop can be predicted by using rheological properties of the flowing fluid. Furthermore, understanding the rheological behavior of fluids in pipe flow conditions is important for the designand control of the industrial process. That is why it is necessary to measure the ‘right’ flow curve and rheological parameters for the fluid used. The theoretical principle, which was serving as basis for the rheological characterization, is the conventional off-line rheometry. However, the rheology of non-Newtonian fluids is complex and it is still difficult to reproduce the flow conditions of fluids in pipe with a conventional rotational rheometer. In context of the recent developments, it was shown that the UVP-PD technique could be applied for measurements of complex, non-transparent and highly concentrated fluids that exhibit a non-Newtonian behavior [10-18]. The technique is based on the combination of an Ultrasound Velocity Profiling (UVP) and Pressure Difference (PD) measurements, commonly known as UVP+PD. This method was successfully tested in several industrial fluid processes see [10,17,19-21].It is obvious that additional experimental data are needed to understand the flow properties of CMC solutions and the effect of the pipe flow conditions on their rheological behavior. This material was extensively studied previously in our laboratory from a rheological point of view [2,7,22].The present paper contributes to evaluate the non-invasive UPDV+PD technique for in-line rheology measurements and flow visualization of Carboxymethyl cellulose. An experimental analysis of the laminar flow of CMC solutions in a straight pipe was then conducted. The velocity profiles were determined using ultrasonic pulsed Doppler velocimeter. Solutions of CMC exhibited shear-thinning non-Newtonian rheological behaviour that can be well described by the two parameters Oswald-de Waele model. The rheological properties were determined directly in-line and the parameters obtained were compared to the offline measurements obtained using a conventional rotational rheometer. Experimental measurements of pressure drop and mean velocity profiles are presented in laminar flow.
Theory
Non-Newtonians fluids do not present a direct proportionality between shear stress and shear rate. To describe their rheological behavior, different flow models are commonly used. One of the most frequently used is the Ostwald-de-Waele model, better known as the power-law model given by:where (Pa) is the shear stress, γ (s-1) is the shear rate, k (Pa.sn) is the flow consistency factor index and n (-) is the flow behavior index. These parameters can be obtained by using a curve fitting procedure. In cases in which n=1 (Newtonian fluid case), k changes to η and Eq. (1) becomes the Newtonian model. In this case, η is a constant of proportionality between the shear stress applied on the fluid and the corresponding shear rate. This constant is the dynamic viscosity of the Newtonian fluid.For power-law fluids, in laminar flow and no slip boundary condition, the velocity distribution across the pipe radius is given by the following expression:As the power law model was found to suitably satisfactorily describes the rheological behavior of the used fluids, the relation between the wall shear stress τw , the volumetric flow rate Q and the shear stress τ is given by the well-known equation:Where Q is the total volumetric flow rate, τw is the wall shear stress and R is the pipe radius. For unidirectional, axisymmetric flow in pipe, the shear stress at the pipe wall (τw) is given by:Where D is the pipe diameter and ΔP L is the pressure drop over a fixed length L. The shear rate and shear stress distribution along the pipe radius can be determined by:As the values of 8U/Dare the wall shear rate for Newtonian fluids, these pseudo shear rates have to be transformed to true shear rates (γ ). According to Chhabra and Richardson [23] and Kotzé et al. [12], a flow curve of unknown form (Eq.3) will yield, after arrangement, the following:This equation occurs in various forms, one being the wellknown Rabinowitsch-Mooney equation:The identification of the transition from laminar to turbulent flow has a great importance because the fluid flow behavior changes fundamentally at the transition zone [12]. Metzner and Reed [24] formulated a generalized Reynolds number (Reg) for non-Newtonian pipe flow:The Reynolds number was used as an indication of the flow regimes in which tests were conducted. Over the range of shear rates where the power-law model is applicable, the consistency factor K’ and the behavior index n’ are related to the parameters k and n of the Ostwald-de Waele model, as follows:One important application of rheological parameters is to calculate the pressure drop, which is usually made through the fanning friction factor f defined as the ratio of viscous forces over kinetic energy per unit volume:In this expression, ρ is the fluid density, U is the average flow velocity, and τw is the stress at the wall as defined in Eq. 4. For laminar flow, the friction factor can be obtained from a simple function of the generalized Reynolds number (Reg), which is identical to the dimensionless form of the Hagen-Poiseuille equation:
Materials and Methodology
Materials and sample preparationThe product used in this work was provided from VWR Prolabo (France). The carboxymethyl cellulose is a water-soluble flexible anionic polymer derived from natural cellulose. It is a very versatile product, available in many brands and types. To determine its basic physical properties: solubility (dissolution behavior), rheology (viscosity), and adsorption on surfaces [1]. Knowledge the way of preparation has a great influence on the final state of the solutions, and thus on the rheological behavior, fluids were prepared using the same procedure to ensure full reproducibility.wo CMC (nominal molecular weight of 700000g.mol-1) solutions with mass concentrations of 0.1 and 0.5 wt. % were prepared by dissolving the appropriate amount of CMC in distilled water at room temperature. The CMC concentration range selected was based on manufacturer recommendations for practical food applications. Sufficient time (≥24h) of continuous magnetic stirring was allowed to achieve complete homogenization.Experimental setup and instrumentationConventional off-line rheometery: All the rheological measurements were performed on a stress-controlled rheometer (AR 2000, TA Instruments) equipped with a cone-and-plate geometry (cone diameter 60mm, angle 2 °C). The sample was carefully loaded to the measuring plate of the rheometer and the upper plate was subsequently lowered slowly into position to minimize any disturbance in the solution structure. To prevent water evaporation when temperature is increased, a homemade humidification cover with wet edges was placed around the measuring geometry to provide a water-saturated atmosphere over the sample. Since the domain structure of aqueous CMC solutions is sensitive to shear deformation history and in order to avoid any memory effect, after the sample was loaded into the measuring device, the sample was subjected to a pre-shear of 100s-1 for 2 minutes. The samples were then left to rest for 2 minutes prior the measurements in order to ensure stability of temperature. Using this procedure, we were able to obtain reproducible measurements. The rheological measurements of the CMC solutions were investigated using large deformation rheology measurements. In this case, the flow curves were obtained by applying an increasing stress ramp at a constant stress rate of 0.033Pa.s-1. Temperature and rate of temperature changes in the solutions during rheological measurements were controlled by the rheometer Peltier heating system.UPDV + PD flow loop and instrumentation: A schematic diagram of the flow loop used to carry out reliable velocity and pressure drop measurements is shown in Figure 1. Flow is provided by a volumetric pump (PCM-Moineau, France) (2) fed directly from a 50 liters capacity tank (1). This pump was selected because it minimizes the amount of mechanical degradation. The flow pipe consists of an assembled Plexiglas ® tube of 20mm inner diameter and 16m length. The temperature of the test fluid is controlled by a heat exchanger (4) and a thermometer (7) mounted in the downstream of the test section (8) is used to monitor the fluid temperature. The test section is equipped with pressure transducers (5). Two pressure transducers (GS Sensors XPM5), providing absolute pressure points, with a range of 2.5 bars were used and are located at 9.22 and 11.97m from the inlet of the experimental setup. Their Operating Temperature Range is from -40 °C to 120 °C. The pressure transducers are fixed to holes drilled in the pipe with diameters equal to the diameter of transducers.The pressure measurement obtained after each experiment at zero-flow rate was defined as the pressure reference. An electromagnetic flowmeter (model: DS41F, from ABB) (3) is incorporated upstream of the test section to measure the flow rate. The velocity profiles were obtained by Ultrasound Pulsed Doppler Velocimetry (UPDV). The main advantage of this technique is that it is non-intrusive and therefore does not disturb the fluid flow. Contrary to optical methods, it is not limited to optically transparent liquids and can be used in the flow velocity measurement of opaque media. The UPDV technique is based on pulsed ultrasound echography: sinusoidal ultrasonic burst is successively emitted from the transducer with a constant frequency fE, during a short time along a measuring line, and then the echo signal that is reflected from targets that maybe present in the path of the ultrasonic beam is detected by the same transducer. PRF is the pulse repetition frequency inversely proportional to the period of pulse repetition. The transducer is mounted according to the flow direction with an angle of 75 °C. The angle was fixed at this value in order to increase the range of measurable velocities. The backscattered echo is then demodulated in order to preserve only the modulated frequency or Doppler shift frequency fD induced by the motion of the particles. The velocity of the particles within the sample volume is proportional to the frequency of the Doppler signal. This is described by the formula:Where u is the velocity of the particles, c is the acoustic velocity in water (c = 1456m.s-1 at 11 °C), fE is the emission frequency, and qis the angle between the ultrasonic beam and the flow direction (the Doppler angle).The velocimeter used in this study is in-house design. Fully developed in the laboratory (Icube, Strasbourg, France), this velocimeter has a highly configurable system developed by Fischer [25] in his thesis were more detailed technical information about velocimeter can be found. The experiments were performed with an 8MHz frequency transducer. It is of ceramic type, with 5mm of diameter. The velocity information is deduced from Doppler frequency shifts induced by the movement of particles. The velocity component measured by the velocimeter is the component in the direction of the ultrasonic beam. Thus, the velocimeter can automatically compute the real velocity value using the introduced Doppler angle (75 °C). The Table 1 shows the specifications of the ultrasound pulse Doppler velocimetry system used.In this study, a special probe holder was designed to keep a stable positioning of the ultrasound transducer. The probe holder includes a cavity with a diameter equal to the diameter of the transducer. This later is installed at a distance from the pipe wall interface. This was done to avoid measurements in the nearfield zone where the ultrasound field is highly irregular [10], and to avoid disturbing the hydrodynamic field. The probe holder contained a hole fitted with valve, in order to get rid of the air. A thin film of transparent plastic was placed carefully in order to reproduce the surface of the pipe. Figure 2 presents the schematic layout of the holder probe.Preliminary measurements with water charged with impurities showed good agreement between the experimental data parameterized by the electromagnetic flowmeter and theoretical values, and confirm those obtained by Jaafar et al. [26] with same method and equipment. The volumetric flow rate obtained from integration of the measured velocity profile differs by less than 3% when compared to the flow rate obtained from the electromagnetic flowmeter.Due to the mechanical degradation of the fluids and the evolution of their rheology with the age, the rheological parameters were measured after each experimental test in the circulating flow loop.
Results and Discussion
Conventional off-line rheometerThe rheological properties of CMC solutions were investigated for two different concentrations, 0.3 and 0.5 wt.%. Figure 3a shows the flow curves of CMC solutions at different concentrations at a constant temperature of 20±0.1 °C. Figure 3b plots the same data as in Figure 3a in terms of viscosity as a function of shear rate. The shapes of CMC solutions flow curves were similar to those reported in previous works [1,2, 21]. The rheom grams of aqueous solutions of CMC showed a shear-thinning non-Newtonian behavior.It was well observed, as expected, that the viscosity of the aqueous CMC solutions increase with increasing CMC concentration. This is due to an increase in the intermolecular interactions between the CMC chains [12]. The viscosity of a solution is a function of the molecular forces that restrict the molecular motion [25]. As previously reported in our laboratory works, the shape of the flow curves changes when the CMC concentration is increased, then different flow behaviors are observed. Here, the lowest concentration exhibit two shearthinning behaviors over two ranges of shear rates separated by a steady value at medium shear rate.Diaz and Navaza [9] reported in their work that the rheological properties of CMC dispersions can be adequately described by Ostwald-de Wale model. Benchabane and Bekkour [1,2] used in their work four parameters model to fit the experimental flow curves obtained for CMC solutions. In this work, the flow curves were fitted with the Oswaled-de Waele model (Eq. 1). The model was chosen for its simplicity and its ability to describe the non- Newtonian behavior of CMC solutions over a wide range of shear rates.To fit the raw data to the model chosen, the Excel® Solver option proposed by Morrison (2005) was used as follow: - The experimental data (shear stress and shear rate) were arranged in the Excel spreadsheet - A column was adopted to predict the value of shear stress which was calculated from a considered flow model (Since the values of the parameters model are unknown, assumptions were made) - A new column for the square of the deviation between the experimental shear stress and the predicted value was created - The Solver function in Excel® was set up to minimize the sum of the squares of the deviations, where the initial assumptions were replaced with the optimized values.The results of the fits to experimental data using Oswald-de Waele model (Equation 1.) are shown as solid lines in Figures 3a&3b and the parameters of the model for both concentrations of CMC are listed in Table 2.In-line measurementsVelocity profiles: Since the determination of the rheological properties depends on an accurate measurement of the velocity profiles, it was important to be able to measure velocity profiles. In this section, the suitability of the UVP method to visualize the flow and measure the instantaneous radial velocity profiles across the pipe diameter was investigated.Figure 4 illustrates typical measured velocity profiles for 0.1wt. %(a) and 0.5wt.% (b)CMC solutions in fully developed laminar flow. The velocity profiles for aqueous CMC solutions was presented in order of increasing Reynolds number offset from bottom to top by an amount indicated by the shifted origins depicted by ‘0’ along the ordinate of the figure. The velocities are presented as a function of the radial distance where the radial position zero indicates the center of the pipe, with maximum velocity. Measurements were thus made both in the direction of the flow.The laminar velocity profiles were clearly symmetric and specific to those of a power law fluid in laminar flow. It can be seen that a good agreement between experimental data (solid symbols) and theoretical model (solid line) is obtained in the case of pure CMC solution. The velocity profile for Newtonian fluid is shown as reference (dashed line). The parameters of the Oswaldde Waele model used have been determined with a least-square fit on the experimental velocity profile of the circulating fluid. The parameters of the model used to fit the experimental data are given in Table 2. The goodness of fit, R2, was found to be around 0.98 for all measured data thus indicating that the power-law model can be used to accurately describe the rheology of the CMC solutions being investigated.It was possible to measure the velocity profiles nearly for the full diameter of the pipe. As can be seen in the figure, the UVP method was successfully used to visualize the flow and to measure the instantaneous radial velocity profiles.Friction factor: In order to evaluate the measurement of pressure drop in the system, experimental data obtained during laminar flow of CMC solutions were used. Pipe dimensions, experimental density and measured pressure drop were substituted into Equation 13 to calculate the friction factor, f. Generalized Reynolds number (Equation 10) was calculated for experimental rheological parameters obtained from the fitting procedure of the velocity profiles for each concentration. This methodology was already used for biological fluid products and gives satisfactory results [26-28].Figure 5 expresses the Fanning friction factors as a function of generalized Reynolds number. The figure also includes predictions of Equation (14) for the laminar region. The good agreement observed between the experimental friction factor obtained from difference pressure and that estimated from the measured rheological parameters supports the reliability of the powerpaw model obtained for describing the rheological properties of CMC solutions. The agreement between experimental and predicted values is very satisfactory, indicating the adequacy of the equipment and methodology used [29].Rheological analysis: As described above, from the fitting procedure of the velocity profile, the rheological parameters were found and then a flow curve across the pipe radius was obtained using Equation 1. In addition, a non-model approach called gradient method was used for direct determination of the rheological properties from the velocity profiles to obtain a rheogram across the pipe radius using Eqs. 5 and 6. The shear rate is obtained from the gradient of the measured velocity profile. The shear stress at the wall was calculated from the pressure difference over a fixed distance using Eq. (4) and then the distribution across the pipe was obtained by Eq. (6).The rheogram obtained is the true experimental flow curve across a pipe radius. The number of points on the rheogram depends on the spatial resolution of the velocity profile measurements, i.e. the number of local point velocity measurements across the pipe radius. The maximum value of the shear rate depends on the flow rate. The corresponding flow curves obtained from a power-law model fit and using the gradient method is shown in Figure 6 [30].Figures 6a&6b show the corresponding shear stress versus shear rate plot and the viscosity versus shear rate plot, respectively. From Figure 6, one can observe a good agreement between the power-law model fitted (solid line) and the gradient method curve (solid symbols). From the viscosity versus shear rate plot shown in Figure 6, the non-Newtonian and shearthinning characters of CMC solutions was observed, and one can observe also that the viscosity increases with the concentration of the aqueous solution, which was expected.The experimental flow curves of CMC solutions obtained offline with a conventional rotational rheometer were presented in the same Figure for comparison. The flow curve measured off-line for 0.5% CMC solutions showed a higher flow curve for 0.5% solution and a lower flow curve for 0.1% concentration, in comparison with the in-line measurement for both solutions. This can be explained by the range of the shear rate and the experimental protocol. Since the polymer solution was in a dynamic state, continuously in motion inside a flow loop and subjected to a heterogeneous flow conditions and shear rate different from that in the off-line measurements [31].It should be noted that the problem of obtaining a representative flow conditions clearly illustrates the main disadvantage with conventional off-line measurements. The tube viscometry approach was also used in this work to determine the flow curve of the solutions used. Tube viscometry has been used earlier for mineral suspensions, and good agreement with the UVP + PD method has been reported [10].Figure 7a&7b show, respectively, the plots of the wall shear stress as a function of the wall shear for the CMC solutions in laminar pipe flow (solid symbol). The experimental data was those of a decrease ramp in the mean velocity. The wall shear stress was obtained from the pressure difference over a fixed distance and the wall shear rate was calculated using the well-known Rabinowitsch-Mooney equation (Eq. 8) using the parameters of the power-law model obtained previously. The flow curve obtained from UVP+PD rheometric method was presented in the same Figure. As shown above, the increase of mass concentration of the CMC solutions leads to an increase in viscosity [32].However, it can be seen that a good agreement was observed between viscosimtetric method (solid symbols) and UPV+PD method (solid line). The flow curve obtained from the UVP+PD rheometric method was determined from mathematical curve fitting of velocity profile in order to obtain rheological parameters. The parameters of the model were listed in Table 2.In this feasibility study, the UVP+PD method was demonstrated to be able to determining the true flow curve and rheological properties of CMC solutions, both directly with the non-model gradient method and by curve fitting to the power-law rheological model [33-35].
Conclusion
A detailed experimental investigation of rheological properties of a0.1 and 0.5 wt% CMC solutions flow was conducted using UPV+PD measurement techniques in laminar pipe flow. The advantage of this technique was the possibility to measure a quasi-instantaneous velocity profile. It was demonstrated that instantaneous velocity profiles could be measured under realistic pipe flow conditions.Firstly, the rheological measurements using off-line conventional rotational rheometer have revealed the strong shear-thinning non Newtonian behavior of CMC solutions. The flow curves were satisfactorily fitted using the Oswald-de Waele two parameters model. Then, the rheological properties were determined, directly in-line and the parameters obtained were subsequently compared with off-line measurements. The UVP+PD method was tested and found successful for continuous in-line measurements.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Petrochemical Science please click on: https://juniperpublishers.com/rapsci/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/rapsci/RAPSCI.MS.ID.555675.php
#Juniper Publishers#Juniper Publishers Review#Juniper Publishers LLC#JuniperPublishers#petrochemical science
29 notes
·
View notes
Text
Multi-Center Phase II Study of the Clinical Use of the Avicenna Roboflex-JuniperPublishers
Abstract
Objectives: To present the results of a multicentric phase-II study, representing the next step according to the IDEAL-criteria in the evualuation process of robot-assisted flexible ureterorenocopy.
Material and methods: The Avicenna Roboflex consists of a console and the manipulator. Peri-operative data from 266 patients who underwent robotic retrograde intra-renal stone surgery (robRIRS) between January 2015 and March 2016 at two centres (Heilbronn, Ankara) were recorded prospectively. Six surgeons were involved in the study. We treated 90 females and 176 male patients with a mean age of 55 (2576) years. 118 stones were located on the right and 148 on the left side. Mean number of stones was 1.8 with a mean stone burden of 1620 (98-10600)mm3; 43% of the patients were pre-stented. A 12/14F access sheath was used in all cases; laser fragmentation was accomplished by a high-energy laser device applying actual concepts of laser lithotripsy.
Results: Preparation of the robot required 4:30min (range 3-8min); docking time was 4 min (range 1-29min). Console time to identify the stone amounted 4min (range 1-12min.); total operating time was 96 min (range 58-193min) including a console time of 65(16-174) min. Laser lithotripsy was performed in 245 patients (92%), 112(42%) patients required extraction of larger fragments using N-gage-basket. The stone clearance rate amounted 25(9-101)mmA3/min. Total fluoroscopy time was time 2:30min with a radiation dosis of 297 cGy*cm2. 117(44%) of our patients were stented post-operatively of which 75(28%) had the stent on a string removed on day 1 together with the Foley catheter. In 2(0.7%) cases we had to convert to classical FURS due to technical failure of the robot. Median post-operative hospital stay was 1(1-30) day. We encountered one case of urosepsis (Clavien 3a) requiring treatment on an intensive care unit.
Conclusion: In this setting, Avicenna Roboflex proved to be robust with only two cases of technical failure requiring conversion to classical FURS. The radiation exposure for the surgeon can be significantly reduced. In conclusion, we were able to integrate the device easily in our daily routine.
Keywords: Avicenna roboflex; Intra-renal stone; Ureteroscopy
Abbreviations: robRIRS: robotic Retrograde Intra-Renal Stone Surgery; SD: Standard Deviation; NIRF: Near-Infrared Fluorescent
Introduction
Management of urolithiasis changed dramatically during the last decades. Whereas in the eighties and nineties of last century extracorporeal shock wave lithotripsy dominated the spectrum of endourological techniques, recently percutaneous surgery and especially retrograde intra-renal surgery has gained significant importance [1]. This was possible because of the continuous improvements of endourological armamentarium and miniaturization of the instruments [2-8]. Nevertheless, flexible ureteroscopy respectively retrograde intra-renal surgery is limited by ergonomic deficiencies including stone manipulation, laser disintegration or extraction of fragments particularly when treating multiple stones or larger renal calculi [9,10]. Thus, the next level of stone management may represent robot-assisted retrograde intra-renal surgery overcoming most of these technological obstacles.
Similar to robot-assisted laparoscopic surgery, such devices represent master-slave systems (Figure 1) [11-15]. First trials modifying a system designed for cardiology (Hansen, United States) were not very successful due to size limitations and limited mobility in the renal collecting system [11-13]. Since 2010 we were involved in experimental and clinical introduction of the Avicenna Roboflex (Elmed, Ankara, Turkey), which was specifically designed for flexible ureteroscopy [14,15]. Beside proof of safe and efficient applicability, the device underwent constant improvements by the manufacturer. In this article we (idea, development, evaluation, assessment, long-term study)- want to present the results of the multi-centric phase-II study, criteria [15,16].
Material and Methods
Specification of the robotic device
The Avicenna Roboflex consists of a console and the manipulator(Figure 2). The basic functions of the device have been described previously.The main include:
o Control of deflection using a wheel for the right hand (Figure 3).
o Control of rotation and horizontal movements via refined joy-stick (Figure 4).
o Integrated HD-monitor displaying the endoscopic view and major data defining the position of the tip of the flexible ureteroscope (Figure 5).
Exchangeable handle for three different digital flexible ureterorenoscopes (Karl Storz Flex X2; Olympus URF-V2; Wolf Cobra digital)
o Air driven control unit to activate foot pedals of laser and fluoroscopy
Following the introduction of the robot in 2 European stone centres (2013 Ankara TR; 2014 Heilbronn, Germany) we collected prospectively peri-operative data from all patients (n=266) who underwent robotic retrograde intra-renal stone surgery (robRIRS) between January 2015 and March 2016. Six different surgeons were involved in the study. We treated 90 females and 176 male patients with a mean age of 55(25-76) years. The body mass index was 29.1(20.6-43.3) and ASA-score was 2.3. 118 stones were located on the right and 148 on the left side. Mean number of stones was 1.8 with a mean stone burden of 1620(98-10600)mm3. 43% of the patients were presented.
Treatment protocol
All stones of this study were treated with the Flex X2- ureteroscope (Karl Storz, Tuttlingen, Germany). In all cases we used a 12/14F access sheath, laser fragmentation was accomplished by use of a high-energy laser device (Lumenis Pulse 100W, United States) applying actual concepts of laser lithotripsy [17] including dusting (low energy (0.2-0.5 J), high frequency (20-40 Hz)), fragmentation (high energy (1.0-1.5 J), low frequency (10-15 Hz)), and the pop-corn/jacuzzi-effect (mid energy (0.5-1.0 J), mid frequency (20-30 Hz)). Larger fragments (2-4 mm) were extracted by use of the NGage-device (Cook, Ireland). Recorded performance parameter included set-up time of the robot, docking time of the robot, console time to stone contact, overall console time, treatment time, stone clearance rate, x-ray parameters (fluoroscopy time, radiation exposure and desimetry).
Statistics
Numerical data were expressed as mean with standard deviation (SD) including range; categorical data as number. SPSS program version 15 was used for data analysis. Categorical variables were analysed using Chi-squared test (or Fisher's exact test). Mann-Whitney test was used for numeric variables. P-values less than 0.05 were considered statistically significant.
Results
Preparation of the robot required 4:30min (range 3-8min); docking time was 4min (range 1-29min).Console time to visible identification of the stone amounted 4min (range 1-12min.), which included inspection of the entire collecting system.
The total operating time was 96min (range 58-193min) including a console time of65(16-174) min. Laser lithotripsy was performed in 245 patients (92%), 112(42%) patients required extraction of larger fragments using N-gage-basket. The stone clearance rate amounted 25(9-101)mm3/min. Total fluoroscopy time was time 2:30min with a radiation dosis of 297 cGy*cm2. In 117(44%) of our patients were stented postoperatively of which 75(28%) had the stent on a string removed on day 1 together with the Foley catheter. In 2(0.7%) cases we had to convert to classical FURS due to technical failure of the robot.
Post-operative data
Median postoperative hospital stay was 1(1-30) day. We encountered one case of urosepsis (Clavien 3a) requiring treatment on an intensive care unit.
Discussion
During the last 15 years robot-assisted surgery has gained an established and irreversible role in urologic laparoscopic surgery [18,19]. In 2016, installations of da Vinci-systems increased by 21% to more than 2,500 units worldwide, and robotic procedures leaped by 25% to more than 450,000, mainly performed in urology, gynaecology and visceral surgery [19]. The main advantages of robot-assisted surgery concern significant improvement of ergonomics, which enabled widespread application of laparoscopic techniques with acceptable learning curves. Additionally, the use of the robot resulted in better results mainly concerning reconstructive parts of the procedure: e. g. postoperative stenosis of the urethro-vesical anastomosis could be basically eliminated.
However, the use of robotic master-slave-systems is not limited to laparoscopic surgery. Already, in 2008 Desai et al. accomplished to use the Sensei-Magelan-system (Hansen Medical, Mountain View, USA) designed for cardio-vascular interventions by Fred Moll, the inventor of the da Vinci-system to perform robot-assisted flexible ureterorenoscopy [12,13]. In this system, the surgeon sits also in front of a console manipulating a steerable flexible tube (Figure 1) usually used for trans-vascular intra-cardiac interventions. The robotic flexible catheter system consists of an outer catheter sheath (14/12F) and inner catheter guide (12/10F). A 7.5F fibre-optic flexible ureteroscope was inserted through the inner catheter guide. Remote manipulation of the catheter system manoeuvres the ureteroscope tip, which was glued in place to the inner guide. The tip of the outer sheath was positioned at uretero pelvic junction to stabilize navigation of inner guide inside the collecting system. This means that the ureteroscope is manipulated only passively [13]. However, this project has been discontinued because it was difficult to manipulate the ureteroscope passively by use of the steerable tube.
Since 2012, ELMED (Ankara, Turkey) is working on of a robot specifically designed for FURS [14]. Roboflex Avicenna was continuously developed to perform flexible ureteroscopy providing all necessary functions for FURS. It enables the use of different kind of ureteroscopes and holmium-YAG-lasers. The surgeon sits at a console using both hands and feet to control all movements of the endoscope. Compared to manual FURS several functions could be integrated: it enables fine-tuning of the movements, motorized insertion and retraction of the laser fibre, automatic repositioning for introduction of the fibre. This means, that robotic FURS has superior performance qualities compared to the classic procedure. In the first clinical study the positive impact of the system on ergonomics could be verified using a validated questionnaire [15]. However, in this study one urologist (R.S.) being involved in development and clinical introduction of the device proctored all seven surgeons during their cases.
The present study was conducted to assess the real-live scenario when using the device on a daily base in two urologic departments involving six different surgeons. Furthermore, new technical improvements of Avicenna Roboflex were evaluated. Comparing our results with the initial study docking time of the robot was longer (4 vs. 1min), time to visualize the stone was similar (4 vs. 3.7min) and the console time was longer (96 vs. 53min). However, the stone volume was larger (1620 vs. 1300mm3). Moreover, we were able to demonstrate that we could safely and successfully apply all modern techniques and protocols of flexible URS, such as laser dusting, using pop-corn/ Jacuzzi-effect, and extraction of larger fragments [17].
In this setting, Avicenna Roboflex proved to be robust with only two cases of technical failure requiring conversion to classical FURS. The radiation exposure for the surgeon can be significantly reduced. In conclusion, we were able to integrate the device easily in our daily routine.
The first two clinical studies of Avicenna Roboflex were able to demonstrate safety and efficacy of the system providing significant ergonomic advantages with a very short learning curve for an FURS-experienced surgeon (max 5 cases). Of course, retrograde intra-renal surgery is less complicated compared to laparoscopic radical prostatectomy, particularly in case of small stones, which can be extracted by use of a Nitinol-basket [20]. On the other side, the introduction of the device provides a safe and non-exhausting environment for the surgeon. Based on this we were able to extent the indication of FURS/RIRS to larger intrarenal calculi resulting to decrease of extracorporeal shock wave lithotripsy and percutaneous nephrolithotomy [21,22].
Further studies should now focus to evaluate further the impact of these advantages on the results compared to classical FURS/RIRS. This has to include the analysis of lifetime of the ureteroscopes, requirement of secondary treatment, postoperative complications and radiation exposure to the surgeon [23-26]. The outcomes of these studies are relevant when discussing the costs of the device. In contrast to radiology, where new imaging devices are introduced without proving any cost- effectiveness, in surgery the introduction of robotic systems is always associated by cost-discussions.
However, development of robotic systems will never stop. Beyond surgical robots as master-slave devices, the role of robotics might be even extended: Shademan et al. described in-vivo supervised autonomous soft tissue surgery in an open surgical setting, enabled by a plenoptic three-dimensional and near-infrared fluorescent (NIRF) imaging system supporting an autonomous suturing algorithm to complete complex surgical tasks on deformable soft tissue, such as suturing an intestinal anastomosis [27]. Similarly, robot-assisted water-jet-ablation (Procept, Redwood Shores, United States) showed significantly better ablation efficacy compared to standard transurethral resection [28]. Next years will be fascinating to evaluate the impact of robot-assistance for laparoscopy, but also for robot- assisted flexible ureterorenoscopy.
#Juniper Publishers#Juniper Publishers Review#Juniper Publishers LLC#JuniperPublishers#urology#open access journals#Open access journal of Urology#open access Journal of Nepharology#Nephrology
0 notes
Text
Ayurveda Aetiology, Pathogenesis & Holistic Management of Inflammatory Bowel Disease

Juniper Publishers-Open Access Journal of Gastroenterology & Hepatology
Authored by Nishant Shukla
Introduction
HBiliary strictures are traditionally classified as ‘indeterminate’ when basic work up, including transabdominal imaging and endoscopic retrograde cholangiopancreatography (ERCP) with conventional brush cytology, is non-diagnostic for its etiology.
Etiology of Biliary Strictures
Evaluation of Patients with Biliary Strictures
The clinical approach to the patient with indeterminate biliary stricture includes a thorough history and physical examination. By and large, strictures of the bile duct in patients with obstructive jaundice should be considered malignant unless a benign etiology is ascertained. The significance of biliary strictures without jaundice is less certain.
Biomarkers
The most common biomarkers for suspected biliary tract malignancies in clinical use are serum CA 19-9 and carcinoembryonic antigen. In patients with PSC, using cut-off value of 129U/ml, the sensitivity and specificity of CA 19-9 for the diagnosis of cholangiocarcinoma are 79% and 98% respectively [2]. In patients without PSC, the sensitivity is only 53% with a cutoff value 100 U/ml [3]. Elevated serum carcinoembryonic adenocarcinoma has also been shown to have a sensitivity of 33- 68% and specificity of 79-95% for cholangiocarcinoma.
Radiological Work-Up
Ultrasound is helpful in patients with biliary stricture by demonstrating intrahepatic biliary radical dilatation and the level of obstruction. However, the distal part of the common bile duct is not properly evaluated because of the interference of bowel gas. Moreover, it has a very low yield for actual detection of strictures on biliary ductal masses [4]. The development of multi- detector helical scanners, used in conjunction with rapid injection of contrast media, accurate depiction of extension of the tumor, locoregional lymphadenopathy and encasement of blood vessels to determine operability of the tumor can be picked up easily.Magnetic resonance cholangiopancreatography (MRCP) has a high sensitivity for bile duct lesions and has got comparable diagnostic accuracy in comparison to ERCP. Ductal features at MRCP which may suggest malignancy include long (>10mm), asymmetrical and irregular strictures. The presence of mass lesion is highly suggestive of malignancy, especially in the hilar region. Abrupt cut-off of the CBD in contrast to a smooth tapering has traditionally been considered to be a sign of malignancy (Figure 1). The sensitivity and specificity of MRCP to differentiate malignant from benign strictures are reported to be 38%-90% and 70%-85% respectively [5]. MRCP is 88-96% accurate in predicting the extent of involvement of the bile duct in cholangiocarcinoma.
Role of Endoscopy Endoscopic retrograde cholangipancreatography
ERCP remains the first line approach for tissue sampling of biliary strictures. The reported sensitivity of conventional brush cytology is 25% to 55% [6]. Different techniques have been employed to improve the sensitivity of conventional brush cytology including novel brushes, biliary stricture dilation with subsequent brushings and repeated brushings. The pluricellular nature and submucosal pattern of tumor growth in cholangicarcinoma or extrinsic malignancy involving the bile ducts attributes to the low sensitivity of biliary brushings. Inadequate biliary cytology specimens are one of the main reasons for non-diagnostic samples. This may be overcome by the presence of an onsite cytopathologist. Several other strategies include cutting the entire brush, creation of slides by the endoscopy team and placing them in a fixative solution prior to submission to pathology are being used to overcome inadequate sampling. The fluorescence in situ hybridization analysis detects chromosomal polysomy using fluorescent probes, whereas the Digital Image Technique (DIA) quantifies nuclear DNA with special stains to assess the presence of aneuploidy.In patients with PSC these chromosomal abnormalities can be seen without the presence of malignancy. Thus, the specificity of FISH in this setting is lower than routine cytology. Thus, FISH increases the sensitivity of brush cytology of indeterminate biliary strictures without much improvement in the specificity. FISH should be reserved for patients with high pre-test probability for malignant strictures. Using endobiliary forceps, the malignancy detection rates ranges from 44% to 89% for cholangiocarcinoma and 33% to 71% for pancreatic cancer [7]. Triple sampling with brushing, transpapilary biopsy and endoluminal FNA has shown the highest sensitivity. Risk of biliary ductal perforation after endobiliary biopsy, however, remains a concern.Endoscopic ultrasoundEndoscopic ultrasonography (EUS) has emerged as an important method for evaluating indeterminate biliary stricture. It provides an excellent alternative method for visualizing and sampling the extra-hepatic biliary tree, hilar masses, gallbladder and peri-hilar lymph nodes and vessels. Sensitivity is significantly better in distal compared to proximally located tumors.CholangiscopyThe technique has recently gained attention with the development of a single operator cholangioscopy (SOC) system known as the SpyGlass (Boston Scientific, Natick, MA, USA). Visually directed biopsies can be obtained using biopsy forceps (SpyBite). Overall sensitivity and specificity of SOC examination for differentiating malignant and benign ductal abnormalities have been seen to be 78% and 82% respectively, higher than the 51% and 54% of ERCP alone [8]. Among the cholangiscopic features, the presence of abnormal tumor vessels due to neovascularization within the biliary stricture is suggestive of biliary malignancy. Intraductal nodules and masses can be visualized during cholangiscopy and are indicative of malignancy (Figure 2). Using these features, good concordance has been seen between cholangioscopic appearance and histopathology.Intraductal ultrasoundERCP with IDUS improves the diagnostic yield of biliary strictures. A small and high-frequency ultrasound probe provides high resolution images of ductal and periductal tissues. IDUS features which suggest malignancy include eccentric wall thickening with an irregular surface, a hypoechoic mass, heterogenicity of the internal echo pattern, a papillary surface, disruption of the normal three-layer sonographic structure of the bile duct, presence of lymph nodes, and vascular invasion. It is, however, not commonly available and expertise is needed for a successful outcome.Chromoendoscopy, autofluorescence and narrowband imagingFor better characterization of biliary strictures, several techniques have been employed during cholangioscopy. In chromoendoscopy, different stains are topically applied to the surface of the mucosa. Methylene blue can successfully differentiate malignant lesions and ischemic strictures from normal mucosa. Biliary narrow band imaging enhances the vascular pattern of the mucosal surface and delineates tumor extent effectively. Initial cholangioscopic studies with autofluorescence have been less promising; poor specificity and high rates of false positivity were observed [9].Confocal laser endomicroscopy (The cellvizio system)Cellvizio is a probe-based CLE system which generates optical biopsies, providing physicians with microscoping images of tissue instantaneously and in a minimally invasive manner. This technique produces specific patterns that correlate with standard histology and differentiate between malignancy, inflammation and normal mucosa. In a recent multicentre study CLE was found to provide significantly higher diagnostic accuracy for malignant biliary strictures than standard ERCP (90% vs 73%) [10].The Miami classification system has been proposed to characterize pCLE findings for biliary strictures. The presence of thick white bands (>20 micrometer), thick dark bands (>40 micrometer), dark clumps, epithelial structures and contrast leakage were the factors which could differentiate malignant from benign strictures [11]. Another newer classification system called the Paris classification was recently described. This includes additional features such as vascular congestion, dark glandular patterns, increased interglandular space and thickened reticular structures [12].
Suggested Approach to Indeterminate Biliary Strictures (Figure 3)
The choice of diagnostic workup should be individualized, depending to a great extent on local expertise and availability of the particular technology. Cross section imaging (CT or MRI) is useful to assess the respectability in patients with suspected malignancy. Table 2 outlines differences between benign and malignant strictures.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Gastroenterology & Hepatology please click on: https://juniperpublishers.com/argh/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/argh/ARGH.MS.ID.555794.php
#JuniperPublishers#Juniper Publishers Review#Juniper Publishers LLC#Juniper Publishers#gastroenterologist
30 notes
·
View notes
Text
Review on General Effective & Therapeutic Diabetic Wound Management

Juniper Publishers- Open Access Journal of Diabetes & Obesity
Authored by Blessing Nimasajai XS
Abstract
Diabetes mellitus is a syndrome of disordered metabolism with abnormally high blood glucose levels (hyperglycemia) (Tierney 2002). According to the latest 2016 data from the World Health Organization (WHO) it is estimated that globally 422 million adults are living with diabetes mellitus .The different types of diabetes are type 1 diabetes (diminished production of insulin) “insulin-dependent diabetes mellitus” ( IDDM) or “juvenile diabetes” , type 2 diabetes (impaired response to insulin and β-cell dysfunction) “non-insulin-dependent diabetes mellitus” (NIDDM) or “adult-onset diabetes” and the other is gestational diabetes which occurs during pregnancy. All type shows signs and symptoms like hyperglycemia, excessive urine production, compensatory thirst, increased fluid intake, blurred vision, unexplained weight loss, lethargy, and changes in energy metabolism. Uncontrolled diabetes mellitus may cause many complications, one of the most serious complication is diabetic wound. This article is based on various research reviews and it was written because most of the people were suffering with diabetic wound and finally they are going for amputation, which is really a painful event and according to me all body parts is very much important for all human being and as early as from the creation of human being by God , the human body is created with all necessary parts & it is our duty & responsibility in caring & protecting the humans body parts as much as possible from amputation. Drop of insulin in blood leads to diabetes mellitus and its complication leads to diabetic ulcer and finally some diabetic ulcers lead to the loss of body parts. To prevent from amputation on behalf of diabetic ulcer, all health care professionals should give more concentration in therapeutic diabetic wound management.
Keywords: Diabetes mellitus; Insulin; Hyperglycemia; Diabetic ulcer; Amputation; Complication
Introduction
“Wounds don’t heal the way you want them to, they heal the way they need to. It takes time for wounds to fade into scars. It takes time for the process of healing to take place. Give yourself that time. Give yourself that grace. Be gentle with your wounds. Be gentle with your heart. You deserve to heal.” - Dele OlanubiDiabetes mellitus is a group of metabolic disorder characterized by hyperglycemia resulting from deficiency in insulin secretion and its imbalance. The increased blood sugar level in diabetes mellitus is associated with long-term damage, dysfunction, and failure of various organs such the eyes, kidneys, nerves, heart, and blood vessels. As per 2016 data from the World Health Organization (WHO) shows the estimation of 422 million adults are living with diabetes mellitus worldwide. Diabetes prevalence has been rising more rapidly in middle- and low-income countries [1]. The major cause of blindness, kidney failure, heart attacks, stroke and lower limb amputation is diabetes mellitus. WHO projects that by 2030, diabetes will be the seventh leading cause of death worldwide. The different types of diabetes are type 1 diabetes (diminished production of insulin) “insulin-dependent diabetes mellitus” (IDDM) or “juvenile diabetes”, type 2 diabetes (impaired response to insulin and β-cell dysfunction) “ non-insulin-dependent diabetes mellitus” (NIDDM) or “adult-onset diabetes” and the other is gestational diabetes which occurs during pregnancy. All type shows signs and symptoms like increase blood sugar level, excessive urine production, increased thirst, increased fluid intake, blurred vision, unexplained weight loss, lethargy, and changes in energy metabolism. Diabetic ulcers are growing more rapidly due mainly to increased incidence of both Type I and maturity-onset diabetes in the developed (high-GDP) countries around the world [2]. The prevalence of diabetic ulcers is rising at 9% annually. At present, this pool of patients is growing faster than the new technologies are reducing the incidence of wounds by healing them uncontrolled diabetes mellitus may cause many complications, one of the most serious complication is diabetic wound. This article is based on various research reviews and it was written because most of the people were suffering with diabetic wound and finally they are going for amputation, which is really a painful event and according to me all body parts is very much important for all human being and as early as from the creation of human being by God, the human body is created with all necessary parts & it is our duty & responsibility in caring & protecting the humans body parts as much as possible from amputation [3]. Drop of insulin in blood leads to diabetes mellitus and its complication leads to diabetic ulcer and finally some diabetic ulcers lead to the loss of body parts. To prevent from amputation on behalf of diabetic ulcer, all health care professionals should give more concentration in therapeutic diabetic wound management. Diabetic wound is a major health problem and its management involves a multidisciplinary approach (Figure 1). This review aims to provide an information regarding the current management strategies of diabetic wound, from prevention to the options for treatment. The authors believe that it may be useful to primary healthcare providers who were involved in the prevention or management of diabetic wound.
Definition/Terminology
Diabetes mellitus is defined as a chronic disease caused by imbalance between insulin by the pancreas and its demand. It leads to increased concentrations of glucose in the blood, which in turn damage many of the body’s systems, the blood vessels and nerves [4].Diabetic wound is a wound which occur because of various factors, such as mechanical changes in conformation of the bony architecture of the foot, peripheral neuropathy, and atherosclerotic peripheral arterial disease, all of which occur with higher frequency and intensity in the diabetic population.Diabetic wound risk factorsRisk factors includes poorly fitted or poor-quality shoes, poor hygiene (not washing regularly or thoroughly), improper trimming of toenails, alcohol consumption, eye disease from diabetes, heart disease, kidney disease, obesity, tobacco use (inhibits blood circulation) etc.
Cause of diabetic wound:1. Increase Blood Sugar Levels: Diabetes is a metabolic disease that causes elevated levels of glucose in the blood. Elevated blood glucose levels stiffen the body’s arteries and narrow its blood vessels, restricting the delivery of the blood and oxygen needed to support the body’s natural healing abilities.2. Decrease or Poor Circulation: Individuals with diabetes are at an increased risk for peripheral arterial disease (PAD), a condition that restricts blood flow to the feet and legs. PAD is especially problematic for those with chronic wounds, particularly diabetic foot ulcers, because it can seriously inhibit the body’s ability to heal. If left untreated, PAD can lead to amputation of the affected limb.3. Peripheral Neuropathy /Nerve Damage: A lack of circulation in the extremities can result in a reduced supply of oxygen and nutrients to the body tissue and nerves, which is necessary for healing. Over time, nerves in these areas may become damaged, decreasing the sensation of pain, temperature and touch, making patients vulnerable to injury.4. Immune System Issues: One of the roles the body’s immune system is to clear away dead, damaged tissue and build new skin cells once a wound or injury has occurred. Diabetes can slow a person’s immune system, which affects the body’s ability to send white blood cells to fight bacteria in an infected diabetic foot ulcer.5. Infection: Because diabetics tend to have weaker immune systems, their bodies are more susceptible to infection. Particularly in those with diabetes, it’s common for a wound to develop an infection like non-healing diabetic foot ulcers.Types /classification of diabetic woundThere are two most common diabetic wounds. They are external origin diabetic wounds and internal origin diabetic wounds. Due to peripheral neuropathy, wounds of external origin, such as skin cuts, burns, bumps and bruises, may often go unnoticed by the diabetic patient [5]. If external wounds go unnoticed for some time, delayed treatment can put the patient at risk for further complications. Wounds of internal origin, such as skin ulcers, ingrown toenails or calluses, can lead to the breakdown of skin and surrounding tissue, increasing the risk of bacterial infections.Signs & symptoms of diabetic woundCommon signs and symptoms of diabetic wound are chronic pain or completely painless, signs of inflammation (swelling, redness, heat, pain and loss of function), signs of infection (pus drainage, discharge, bad odor and dead tissue), numbness and dullness (signs of nerve damage), fever and/or chills (signs of progressively worsening infection that can be limb-threatening or even life-threatening).Diagnostic evaluations for diabetic woundDiagnostic evaluations for diabetic wound include history collection, physical examination, examination of the ulcer, testing for loss of sensation, testing for vascular status, laboratory investigations (blood tests), pulse-volume recording, ultrasonography, ankle-brachial index, radiography, computed tomography, magnetic resonance imaging, bone scans, and angiography [6].Factors that delay diabetic wound healingLocal factors are continued pressure over the site, desiccation and dehydration, trauma, edema, infection or heavy colonization, necrosis, maceration caused by incontinence, lack of oxygen delivery to the tissues, etc., [7]. Systemic factors are old age, obesity, chronic diseases, malnutrition, vascular insufficiency, immunodeficiency, smoking, stress, etc., (Table 1 & 2).Management of diabetic woundA. The essential components of diabetic wound management are:B. Treating underlying disease processesC. Ensuring adequate blood supplyD. Local wound care, including infection controlE. Antibiotic for infected diabetic woundsF. Tissue debridementG. Inflammation and infection controlH. Moisture balance (optimal dressing selection)I. Epithelial edge advancement.J. Pressure offloading.a. Avoid bandaging over toes as this may cause a tourniquet effect (instead, layer gauze over the toes and secure with a band- age from the metatarsal heads to a suitable point on foot)b. Use appropriate techniques (e.g. avoiding creases and being too bulky) and take care when dressing weightbearing areasc. Avoid strong adhesive tapes on fragile skind. Avoid tight bandaging at the fifth toe and the fifth metatarsal head (trim the bandage back)e. Ensure wound dead space is eliminated (e.g. use a dressing that conforms to the contours of the wound bed)f. Remember that footwear needs to accommodate any dressing.g. Vacuum-assisted closure: Vacuum-assisted closure (VAC) is a new method in wound care which speeds wound healing by causing vacuum, improving tissue perfusion and suctioning the exudates.h. Hydrotherapy: The process of providing an adequate amount of liquid to bodily tissuesi. Treatment of charcot foot: Charcot neuropathic osteoarthropathy (CN), commonly referred to as the Charcot foot, the diabetic Charcot foot syndrome is a serious and potentially limb-threatening lower-extremity complication of diabetes. The diabetic Charcot foot is an inflammatory syndrome characterized by varying degrees of bone and joint disorganization secondary to underlying neuropathy, trauma, and perturbations of bone metabolism. Management includes Offloading at the acute active stage of the Charcot foot is the most important management strategy and could arrest the progression to deformity, antiresorptive drugs, Surgical treatment of Charcot arthropathy of the foot and ankle is based primarily on expert opinion [8]. Surgery has generally been advised for resecting infected bone (osteomyelitis), removing bony prominences that could not be accommodated with therapeutic footwear or custom orthoses, or correcting deformities that could not be successfully accommodated with therapeutic footwear, custom ankle-foot orthoses, or a Charcot Restraint Orthotic Walker.j. Surgical Care, surgical wound closure & bone resection: Diabetics have higher risks of wound healing complications following surgery. Surgical wounds can easily become chronic wounds, such as pressure ulcers, without the right care. There are several types of wound dressings available, including the following:a) Alginates: Alginate dressings encourage debridement and absorb wound drainage.b) Collagens: These work well for surgical wounds in diabetics by encouraging blood vessel and new tissue growth.c) Foams: Foam dressings have a high absorption rate, provide thermal insulation, and create moist healing environments.d) Silvers: Silver-based dressings draw in bacteria and neutralize them, making them an excellent choice for preventing wound infections.Armstrong et.al proposed a classification model for surgical management of the diabetic foot based on fundamental variables present in the assessment of risk and indication like presence of neuropathy (loss of protective sensation), presence or absence of an open wound & presence or absence of any acute limbthreatening infection [9]. According to the classes of diabetic foot surgery, class III (curative) and class IV (emergency) procedures involve a current diabetic foot ulcer or open wound. Emergency procedures are those performed to limit the spread of acute, limb-threatening infections. This class of surgery may be performed in the presence of limb ischemia to prevent further spread of the infection. The potential for vascular intervention should be considered either concomitant with this procedure, or in the immediate postoperative hospitalization period. he goals of the curative procedure is to speed up the healing of the diabetic foot wound and prevent recurrence of this wound. Surgical decision making is heavily dependent on the type of wound and its location. It is our experience that most chronic ulcerations present in the diabetic foot are a direct result of increased plantar pressure in the presence of peripheral neuropathy. The surgical goal for these types of ulcers is to relieve the source of increase in pressure. Some of the most time-honored procedures involve some sort of bone resection. This type of procedure aids in eliminating pressure underlying the wound. In the forefoot, bone resection has been well documented as able to heal a wound faster, prevent ulcer reoccurrence, and lower the incidence of infection compared with conservative treatment [10-13]. This may include isolated metatarsal head resection [14-16], pan metatarsal head resection, transmetatarsal amputation (TMA), exostectomy, and partial calcanectomy.a. Revisional surgery for is frequently needed to control diabetic foot infections and for bony architecture may be required to remove pressure points. Such intervention includes resection of metatarsal heads or ostectomy.b. Vascular reconstruction: Vascular surgeons, radiologists and plastic surgeons should form an integral part of the diabetic foot team. Here the potential limitation of investigation or reliance on symptoms in the diabetic patient are discussed. The acute presentation of the patient with a diabetic foot may necessitate emergency drainage or abscess formation and debridement of infected necrotic tissue, if necessary, prior to formal investigation and reconstruction. Detailed investigation should include intra-arterial digital subtraction angiography, with or without color flow duplex. These investigations will help to delineate the most beneficial interventional management. This may include a combination of interventional radiological techniques, proximal and distal vascular reconstruction, and indeed the combination of femorocrural, popliteal-crural reconstruction with plastic surgical techniques. Distal reconstruction in combination with split skin grafts and/or free flap closure may also help to preserve the limb in diabetic patients with severe necrosis and infection which requires extensive debridement.c. Skin grafts, Tissue-cultured skin substitutes, Xenograft: Advanced therapies for foot wounds are saving limbs, restoring mobility, and improving the lives of many people with diabetes who suffer from non-healing foot ulcers (Figure 2). Skin substitutes can consist of bioengineered or artificial skin, autografts (taken from the patient), allografts (taken from another person) or xenografts (taken from animals). According to Dieckmann et al. skin substitutes can be divided into two broad categories: biomaterial and cellular. Biomaterial skin substitutes do not contain cells (acellular) and are derived from natural or synthetic sources. Natural sources include human cadaveric skin processed to remove the cellular components and retain the structural proteins of the dermis and collagen matrix obtained from bovine and porcine sources. Synthetic sources include degradable polymers such as polylactide and polyglycolide. Whether natural or synthetic, the biomaterial provides an extracellular matrix that allows for infiltration of surrounding cells. Cellular skin substitutes are distinguished by their origin: xenogeneic (from nonhuman species), autologous (from the patient), and allogenic (from another human). Keratinocytes and fibroblasts obtained from these sources are cultured in vitro to produce the cellular material used to make the substitute. However, the classification of skin substitutes into either biomaterial or cellular is not completely accurate since the two are combined into several wound care products. Human tissue can be obtained from human donors, processed, and used exactly in the same role in the recipient-skin for skin, tendon for tendon, bone for bone. These uses are regulated as human tissue intended for transplantation, if the proposed clinical use and manufacturing methods are consistent with definitions of “Homologous Use” and “Minimal Manipulation”. Human tissue and cells may also be used as a source of cells for culturing to produce cellular-derived material for wound healing.d. Hyperbaric Oxygen Treatment: Hyperbaric Oxygen Therapy is a treatment option for diabetic patients with a foot ulcer, where the patient inhales 100% oxygen in a pressurized chamber. This method helps the body increase the oxygen levels in the blood. It also exposes the affected tissues to more oxygen than would otherwise be present, thus allowing for enhanced healing. Hyperbaric oxygen therapy (HBOT) has been promoted as an effective treatment for diabetic foot wounds, it improves wound tissue hypoxia, enhancing perfusion, reducing edema, down regulating inflammatory cytokines, promoting fibroblast proliferation, collagen production, and angiogenesis make it a useful adjunct in clinical practice for “problem wounds,” such as diabetic foot ulcers. Hyperbaric oxygen therapy increases the saturation of oxygen in the blood, due to the enhancement of atmospheric pressure. Increased oxygen can promote white blood cell activity, encourage tissue development and induce capillary growth. This method can be beneficial for a variety of conditions but is proving exceptionally promising in the treatment of diabetic foot ulcers.e. Dietary Managements: Nutrient deficiencies have influence of wound healing in a different way. Malnutrition and/ or nutrient deficiencies can impair collagen synthesis, prolong inflammation, decrease phagocytosis (causing dysfunction of B and T cells), and decrease the mechanical strength of the skin. High-protein, high-calorie, nutrient-enriched supplements may be recommended between meals if food intake doesn’t meet a patient’s needs for wound healing. Arginine and glutamine are two amino acids that have been studied extensively for their role in wound healing. In addition, beta-hydroxy-methyl buterate, which is a metabolite of the amino acid leucine, has been linked with improved wound healing and tissue regrowth. People with diabetes do not heal as efficiently as people with normal blood sugar levels. Certain foods can also help keep your blood sugar optimal.f. blood sugar levels: Certain foods can also help keep your blood sugar optimal.Protein helps to repair tissuea. Fishb. Shellfishc. Eggs (egg whites have protein and no cholesterol)d. Cheese (low fat is better for your heart)e. Poultryf. Lean meatg. Nut butters (peanut butter, almond butter, cashew butter, etc.)Carbohydrates give you energya. Starch (bread-whole grains are best-cereal, noodles, rice, barley, kasha)b. Starchy vegetables (sweet or white potatoes, corn, peas, beans)c. Non-starchy vegetables (broccoli, green beans, asparagus, salad greens)d. Fruite. Milk (drinking milk, soymilk or yogurt)Fat allows you to absorb your fat-soluble vitamins-A, D, E, Ka. Oil (olive and canola oil are best for your heart)b. Nuts (are good for your heart and health)c. Avocado (is good for your heart)d. Margarine (pick one without trans-fat)e. Butter (use more sparingly)The following vitamins are excellent to heal wounds most efficientlyA. Vitamin C-foods with high levels:a. Peppers (especially red)b. Kiwi fruit, Tomatoesc. Citrus fruits (oranges, grapefruits)d. BroccoliB. Vitamin A-foods with high levels:a. Orange colored fruits/vegetablesb. Dark green leafy vegetablesC. Vitamin E-foods with high levels:a. Whole grainsa. Whole grainsb. Wheat germc. Dark leafy green vegetablesd. Eggs**e. Nuts and seedsD. Vitamin B-foods with high levels:a. Whole grains (wheat and oats)b. Fish and seafoodc. Poultry and meatd. Eggs**E. Zinc-foods with high levels:a. Oysters (very high)b. Beans** Egg yolks contain vitamins and cholesterol while egg whites contain proteinA. Restriction of Activity: Many evidence-based cases studies show that increase activity delays in wound healing process, so therefore it is important to minimize the activities to the affected extremitiesB. Amputation may be indicated in circumstances during Ischemic rest pain that cannot be managed by analgesia or revascularization, a life-threatening foot infection that cannot be managed by other measures, a non-healing ulcer that is accompanied by a higher burden of disease than would result from amputation. In some cases, for example, complications in a diabetic foot render it functionally useless and a well performed amputation is a better alternative for the patient.C. Ultra-MIST Therapy, non-contact, low frequency, nonthermal ultrasound has a pain-free delivery through a fluid/ saline mist that acts as the medium to deliver energy to the diabetic wound and induce fast healing.
Steps to Avoid Amputation: Implementing A Global Wound Care PlanDiagnosis of diabetes (+/_ peripheral sensory neuropathy)
AIM: Prevent the development of a diabetic wounda. Implement diabetic wound prevention care plan that includes treatment of co-morbidities, good glycemic control and pressure offloadingb. Annually perform general foot examination:c. Use 10g monofilament to assess sensory statusd. Inspection of the feet for deformitiese. Inspection of footwear for wear and tear and foreign objects that may traumatize footf. Maintain skin hydration (consider emollient therapy) for skin healthg. Offer patient education on checking feet for traumah. Ensure regular review and provide patient education
Development of diabetic wound
AIM: Treat the ulcer and prevent infectiona. Determine cause of ulcerb. Agree treatment aims with patient and implement wound care plan:c. Debride and regularly cleanse the woundd. Take appropriate tissue samples for culture if infection is suspectede. Select dressings to maintain moist wound environment and manage exudate effectivelyf. Initiate antibiotic treatment if infection suspected and consider topical antimicrobial therapy if increased bio burden is suspectedg. Review offloading device and ensure footwear accommodates dressingh. Optimize glycemic control for diabetes managementi. Refer for vascular assessment if clinically significant limb ischemia is suspectedj. Offer patient education on how to self-manage and when to raise concerns
Development of vascular disease
AIM: Prevent complications associated with ischemiaa. Ensure early referral to vascular specialist for arterial reconstruction to improve blood flow in patients with an ischemic or neuro ischemic ulcerb. Optimize diabetes control
Ulcer becomes infected
AIM: Prevent life- or limb-threatening complicationsa. For superficial (mild) infections-treat with systemic antibiotics and consider topical antimicrobials in selected casesb. For deep (moderate or severe) infections-treat with appropriately selected empiric systemic antibiotics, modified by the results of culture and sensitivity reportsc. Offload pressure correctly and optimize glycemic control for diabetes managementd. Consider therapy directed at biofilm in wounds that are slow to heal
Active management of the ulcer and co-morbidities should aim to prevent amputationa. Where amputation is not avoidable:b. Implement skin and wound care plan to manage surgical wound and optimize healingc. Review regularly and implement prevention care plan to reduce risk of recurrence or further diabetic wound on contralateral limb
Prevention of diabetic wounda. Inspect feet daily: The CDC recommends people with diabetes inspect their feet every day for cuts, blisters, calluses, red spots, swelling and other abnormalities. Regularly trim toenails straight across to avoid ingrown toenails. If cannot see or reach the feet, use a mirror or ask for the assistance of a doctor, family member or caregiver. In addition to daily examination, have the doctor or podiatrist check your feet at least once per year.b. Protect the feet from infection: Washing the feet each day is an important part of the diabetic foot care routine. Wash feet in lukewarm water (not hot water, which can scald and blister feet), and dry feet thoroughly afterward. Once dry, rub moisturizing lotion or cream on the tops and bottoms of feet. Do not apply lotion between toes, as this could foster bacterial growth. Don’t forget to put on socks and shoes, even if you are just staying in your home, to avoid stepping on something sharp and becoming injured.c. Manage/ control diabetes mellitus: Keeping the blood sugar, blood pressure and cholesterol levels in check can prevent most of the complications related to diabetes, including nonhealing diabetic foot ulcers. Work with primary care physician to develop a diabetes self-management plan that may include healthy diet, regular exercise, blood sugar monitoring, smoking cessation and adherence to medication as directed.
Summary
A diabetic wound is an open sore or wound that occurs in approximately 15 percent of patients with diabetes and is commonly located on the bottom of the foot. This article review gives a brief knowledge regarding diabetes it’s signs and symptoms, how to manage diabetic wound and other complication. Physical examination of the extremity having a diabetic ulcer can be useful in the management of diabetic wound. The staging of diabetic foot wounds is based on the depth of soft tissue and osseous involvement. A complete blood cell count should be done, along with assessment of serum glucose and creatinine levels. The management of diabetic wound requires offloading the wound by using appropriate therapeutic footwear, daily saline or similar dressings to provide a moist wound environment, debridement when necessary, antibiotic therapy if osteomyelitis or cellulitis is present, optimal control of blood glucose, and evaluation and correction of peripheral arterial insufficiency. As a human being we all have the responsibility to protect our body parts from such chronic diseases.
Conclusion
As per various evidence-based reviews clearly states that 84% of lower limb amputations have a history of diabetic wound. Diabetic wound and amputations significantly reduce the quality of life. Also, while checking on hospital admission, most of patients got admitted with diabetes. Therefore, it’s a very much important in caring diabetic patients with effective diabetic wound care for improving their quality of life.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Diabetes & Obesity please click on: https://juniperpublishers.com/crdoj/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/crdoj/CRDOJ.MS.ID.555743.php
#Juniper Publishers#JuniperPublishers#Juniper Publishers LLC#Juniper Publishers Review#Diabetes#open access journals#obesity
49 notes
·
View notes
Text
Biopsy and Active Surveillance in Small Renal Masses-JuniperPublishers

Abstract
Small renal masses are masses that have been determined by axial imaging methods to be <4cm in diameter. The treatments that can be used for these masses are active surveillance (AS), ablative therapy, or partial or radical nephrectomy. A renal tumor biopsy is an accurate and safe way to employ AS and gain information about the prognoses of small renal masses. The biopsy can be performed using ultrasonography or computed to mography guidance, which are called core biopsies and fine-needle aspiration biopsies.
Keywords: Active Surveillance; Renal biopsy; Small renal mass
Abbreviations: SRM: Small Renal Mass; As: Active Surveillance; RTB: Renal Tumor Biopsy
Introduction
There has been an increase in the diagnosis of small renal masses (SRMs) as renal cell carcinoma, and this increase seems to be linked to the widespread utilization of abdominal imaging. The treatments that can be used for these masses are active surveillance (AS), ablative therapy or partial or radical nephrectomy. The main objective of these treatments is to attain a successful oncological outcome and maximum renal function protection. In addition, overtreatment should be avoided due to its potential for morbidity. In this mini-review, the roles of the biopsy and AS of SRMs are explained.
Biopsy and Surveillance
SRMs are masses that have been determined by axial imaging methods to be ≤4cm in diameter. Surgical intervention, which generally occurs soon after the diagnosis of SRMs, provides adequate information about the nature of the disease [1] observed benign lesions in 221 patients (23%) after the surgery of 4cm masses [2] concluded that the risk of metastasis in SRMs up to 4cm large was 2%. Other published studies have shown that AS does not have negative effects on cancer-specific survival and overall survival [3,4].
The axial imaging methods are insufficient to divide the histological types of renal masses except angiomyolipomas. The European Association of Urology guidelines [5] on renal cell carcinoma (RCC) recommended the use of a renal tumor biopsy (RTB) before ablative therapy and systemic therapy without previous pathology (Grade of recommendation: C). Over 13 years [6] studied 509 patients who had SRMs up to 4cm large. According to this study, peri-renal hematomas were seen in 4.7% of patients, bleeding through the coaxial sheath was observed in 2.4% of patients and self-limited gross hematuria was observed in only 1% of patients. Percutaneous angioembolization was required for the patient who had a peri-renal hematoma. In the same study, 131 patients (26%) had a benign histology. In this study, the RTB of SRMs showed a high rate of diagnostic accuracy, and more than a quarter of tumors were observed as benign [7] published a study on 301 consecutive cases of percutaneous needle core biopsy (NCB). In this study, 23% of patients' tumors were benign. NCBs were used to confirm diagnoses confirmed in 89% of the renal included in this study, and renal mass NCBs were 93% accurate in the determination of the histologic subtypes of renal carcinoma. After radical nephrectomy, the diagnoses of primary renal malignancy in all 55 patients were 100% accurate, and only the diagnoses of the RCC subtypes of 4 patients were inaccurate. Therefore, percutaneous NCB plays a significant role in the definite tissue diagnosis of renal masses before treatment and in the guidance of patient management.
In an analysis of 57 studies, [8] investigated 5,228 patients. In this study, diagnostic core biopsy and fine-needle aspiration (FNA) results were compared. The overall median diagnostic rate of RTB was 92%. The sensitivity and specificity of the diagnostic core biopsies were 99.1% and 99.7%, respectively and the sensitivity and specificity of the FNAs were 93.2% and 89.8%, respectively. A very low rate of Clavien complications >2 was observed. Therefore, RTB is conclusively safe and has a high diagnostic efficiency in experienced centers.
Biopsy can be performed using ultrasonography or computed tomography guidance, which are used for core biopsies and FNA biopsies. For solid masses, core biopsies are preferable. At least two cores should be sampled during renal mass biopsy. Due to the risk of central necrosis, peripheral sampling should be done. Needles 18G or larger should be used for the core biopsy of renal masses to produce a high diagnostic yield. A coaxial biopsy cannula has been suggested as a method to create biopsy efficiency by preventing tumor seeding and taking various amounts of tissue samples [9].
In a prospective study [10], either adapted AS to patients who had SRMs up to 4cm large or treated them immediately. Of the 221 patients in the surveillance group, 21 received delayed interventions. In the AS group, old patients who had bad Eastern Cooperative Oncology Group scores, and cardiovascular comorbidities had multiple and bilateral lesions. As a result of long-term follow-up periods, AS was determined not to be inferior to primary intervention.
AS is recommended for elderly patients or co-morbid patients who have limited life expectancy and a high perioperative risk of surgical and medical complications [10]. The 2017 American Society of Clinical Oncology Clinical Practice guidelines [11] suggest the use of renal tumor biopsy if the result affects the guidance of the treatment of SRMs. AS is accepted as an initial management option for patients who have relevant comorbidities and limited life expectancy [12].
Conclusion
RTB is an accurate and safe method that can be used to recommend AS and gain information about the prognoses of SRMs. RTB has a high diagnostic yield in experienced centers. Therefore, patients who are planned AS for SRMs should be referred to experienced centers for a renal biopsy.
#Juniper Publishers#Juniper Publishers Review#Juniper Publishers LLC#JuniperPublishers#urology#Open access journal of Urology#Nephrology#Open access journal#kidney
0 notes
Text
Chemical Contaminants and Pollutants in the Measurable Life of Dhaka City
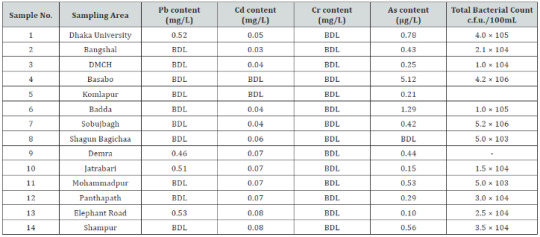
Juniper Publishers-Open Access Journal of Pharmacy & Pharmaceutical Sciences
Authored by AK Mohiuddin
Abstract
Environmental pollution and food contamination are as old as the civilization itself. It is the consequence of the development of civilization, over utilization of nature, industrialization and in fact a price for the progress. It is highly prominent in Dhaka city. Air pollution is mainly due to the vehicle emission, industrial discharge and burning of fossil fuel. The water resource of Dhaka becomes a major health threat due to arsenic contamination, inadequate household/industrial/medical waste disposal and industrial effluent management. Food contamination came from the commercialism of business people who are doing this knowingly to maximize profit. Necessary steps are to be taken to protect the environment for our own existence. This paper reveals chemical pollution and contamination issues of Dhaka city, the capital of Bangladesh.Purpose of the study: Brief review of chemical induced pollution and contamination, their consequences and control. Healthcare providers/Policy makers have a major role play to concerned field.Materials and Methods: Comprehensive literature search followed by consulting healthcare professionals about environmental pollution and food contamination. Hospital, clinic and company personnel, newspaper journalists, NGO workers given their valuable suggestions and asked help for necessary books, journal, newsletters. A few western magazine and newspapers also observed to get necessary concern. Projections were based on public life pattern, their food habits, pollution and contamination sources, waste disposal features of urban life as well as industry and hospital waste disposals.Results and Discussions: Pollution and adulteration are the most notorious enemy of mankind. Civilization has its own drawback that even causing destruction of itself. Very few people raised voice on this but crippled by the facts of commercialism. The scope of this article is limited to chemical pollution of air and water, medical or household waste products and food contaminants and adulterants. A few discussions based on real life experience and recent studies or reports from various journals and news articles are summarized here.Findings: Both general people and the old system, are responsible for this unlivable condition of Dhaka city. Population is not the sole for this instance. A sense of poor rules and regulation is always raised everywhere. Negligence is becoming a wide spread disease contaminating illiterate to well educated, all kind of people.Research limitations: Many articles and documents found in concerned area of research, but the scope of this research is on its focus point chemical hazards and burdens of Dhaka city. Still the most important aspect is covered, but fact is less amount of recent data found in few areas.Practical Implication: The language of this article is too simple to understand by people with simple literacy. Pharmacists, doctors, nurses, hospital authorities, public representatives, policy makers and regulatory authorities must acquire much from this article.Social Implication: Any article or research is based on the think beneficence for mankind, at least going ahead from the present situation, overcoming problems and measures. The article should create an instruction for the future policy makers of both government and other sectors to review the alarming situation of chemical pollutions and food contaminants of Dhaka, along with the whole Bangladesh. Again, world business is moving to Asian countries, Bangladesh will be an important business hub within next few decades. This article should remind policy makers that we should not forget mankind, giving places to industrialization and development.
Keywords: Medical and Household waste; Health Hazard; Chemical Intoxication; Cancer; Food Poisoning; Pathogen; Contaminants
Abbreviations: BDL: Below Detection Limit; BOD: Biochemical Oxygen Demand, also called Biological Oxygen Demand; COD: Chemical Oxygen Demand; DO: Dissolved Oxygen; TDS: Total Dissolved Solid; PH: A Logarithmic Scale used to specify the Acidity or Basicity of an Aqueous Solution; ICDDR, B: International Centre for Diarrheal Disease Research,Bangladesh
Introduction
Contamination is the presence of an unwanted substance where it should not be or at concentrations above recommended. Pollution is contamination that results in detrimental biological effects to resident communities. All pollutants are contaminants, but not all contaminants are pollutants. All elements of the natural environment can be altered, sometimes with harmful results. Air, food, water, and the earth can all become sources of ailment, in the home, public, or work environments. In urbanization, all processes are viewed in relation to the city. Generally, better food supply, good medical care, education, jobs, industrialization, commercialization, electrification, specialization of professions, and entertainment are the basic causes of urban growth. Accessible energy plays an important role in our development with this, people can enjoy all the modern facilities [1-4].By establishing road communication, an undeveloped area may relate to a developed area. It helps the people of the areas, the use of information, technology, and media for an improved standard of living. With increased industrialization, air, in Western, as well as developing countries, now contains toxic substances that are either direct results of combustion or produced by photochemical change. Dhaka, being the capital of Bangladesh ranked 3rd worst in Air Quality Index (AQI) in the world. Besides, the city of nearly 20 million inhabitants, Dhaka faces challenges on this front, ranging from poor sanitation, polluted rivers, and chemical outpouring from the surrounding industries, all resulting from the impromptu nature of urbanization. Food contaminants and adulterants gave a new dimension in city life, together rest of the country. The healthcare providers role in environmental health is related primarily to being alert to the conditions predominant in the community and of working with others to adequately control any of the attendant hazards [5].
Urbanization and Its Impact
Urbanization is one of 21st century’s most transformative trends. Cities are the dominant force in sustainable economic growth, development, and prosperity in both developed and developing countries. In developed countries, the growth of the urban population has stabilized, and urbanization is taking place at a rapid pace. Currently, 55% of the world’s population (four billion people) reside in urban areas which will be nearly 70% by 2050 (United Nations, 2018). By 2030, over 60% people will live in the cities (Megacity Challenges, Siemens AG), two billion more people will have migrated to cities– placing unprecedented pressure on infrastructure and resources, particularly those related to water (According to UN and World Bank) [6]. From 2016 to 2030, a 35% population increase is expected in the top ten megacities.Furthermore, as more than three-quarters (76%) of the world’s mega-cities are coastal, there will be a considerable impact on water ecosystems from ridge to reef. Because of this, local and regional authorities lead initiatives targeting waterrelated obstacles, including housing gaps, climate change and an increased demand for food, energy and water [7,8]. Forecasts indicate cities in developing countries including Karachi, Lagos, and Dhaka will surpass cities like New York, Osaka, and Sao Paulo by 2030 [9]. This represents a 50% increase in demand for energy and water, generating challenges that exert pressure on water resources and threaten global water security.This has a palpable effect on public health, economics, and development. It has been estimated that the urban population in Bangladesh will rise to between 91 and 102 million by 2050, which will be 44% of the total population [10]. The leather tanning industry has been identified as one of the main causes of environmental and water pollution in the Capital city of Dhaka of 10 million people. About 60,000 tons of row hides and skins are processed every year using dehairing, ammonium salt sulphate and chloride during de-liming, solvent vapors which releases a huge quantity of untreated effluent into the open causing air pollution and water bodies [11].
Chemical Pollution and Contamination Due to Urbanization
Smog results from the interaction of the ultraviolet rays in sunshine and the unburned hydrocarbons of automobile engines or factories and smokestacks. These products, when trapped by the thermal inversion engendered by local topography, cause damage to mucous membranes and lungs when inhaled [12]. Acute episodes of air pollution have been found to exacerbate illness and even cause death in people who already have respiratory and cardiovascular diseases. Supporting evidence exists demonstrating that second-hand tobacco smoke increases the risk of cardiovascular diseases or cancer as well [13]. According to World Bank’s Country Environmental Analysis (CEA) 2018 report, air pollution lead to deaths of 46,000 people in yearly in Bangladesh [7]. Waterborne infectious disease is very common today, all the public supplies are literally contaminated with water drainage system reported many places.Many complaints about the taste, appearance, and physical qualities of locally supplied water have led to a brisk in bottled water [14]. Water contamination with ground-source chemicals (e.g., pesticides, fertilizers) remains an ongoing possibility. Food remains a significant vehicle of disease organisms [15]. Foodborne disease more commonly but often incorrectly called “food poisoning,” is grossly underreported. In most instances the illness produced by contaminated food is mild and of short duration, but more severe outbreaks (such as hepatitis A, most commonly seen in public restaurants) can. Epidemics of foodborne disease are dramatic and sudden, and most people become sick within 6 to 24 hours after consuming the contaminated foodstuffs. The epidemic pattern of food-borne disease presents differently from the gastrointestinal symptoms (e.g., nausea, vomiting, and diarrhea) induced by intestinal enteroviruses occur [16].
The Dhaka City at a Glance
Living in Dhaka city endowed with a traffic jam, street foods, unplanned buildings, narrow road space, noise pollution along with environmental pollution and issues of contamination [17]. Some people make joke like “Traffic jams teach us things like patience and how to plan ahead of time” [18]. Many people sleep roadsides, railway platforms, mosques and market places. People rushes this city for job, business and other opportunities like uninterrupted utilities. Along with general people, the city is also heaven for muggers, robbers, thieves, pickpockets, frauds, drug dealers and organized criminals [19]. People rarely can see the sunrise or sunset due to thousands of buildings.Hawkers are illegally occupying the public walkways, pedestrians are now forced to walk on the roads which raises the risks of accidents and adds to the already unbearable traffic congestion in those areas. Economist Intelligence Unit (EIU) The EIU surveyed 140 cities around the world for its Global Liveability Index 2018, scoring them on over 30 specified parameters under five categories: healthcare, infrastructure, culture and environment, stability, education and infrastructure (The Global Livability Index, 2018). All these things make this a difficult to breath place and a second worst place in the world to live in. Some 18,000 deaths from environmental pollution occurred in 2015 in Dhaka Environment Desk (2016).
Air Pollution
The most profound chemicals found harmful to human health and at high enough concentrations (Table 1) can even be fatal are Carbon monoxide (CO), Sulfur dioxide (SO2), Nitrogen oxides (NOx), Ozone (O3), Hydrocarbons (HC) and Suspended Particulate Matter (SPM) found in places surround Dhaka. Possible health hazards found to be headache, eye-nose-throat irritation, allergy, lung injury, trauma and even death with long term exposure [20-24].The AQI in Dhaka during the winter, where more than 4,500 brick kilns operate, typically hovers above 250 – a level considered unhealthy for all groups – but often spikes much higher [25]. Brick kilns, unfit vehicles run by fuels with higher level sulphur, as well as construction works, rundown roads have been identified as major sources of air pollution [26,27]. Day by day the amount of dust include air pollution in the city has been increasing. The air quality, particularly in Dhaka has undoubtedly been getting worse. Air pollution, according to Thomson Reuters Foundation, caused largely by burning fossil fuels, is cutting global life expectancy by an average of 1.8 years per person, making it the world’s top killer [28]. AQI 201 to 300 is marked as “extremely unhealthy” or hazardous air. At present AQI level of Dhaka has 309, which is in extreme “unhealthy” position [7].
Water Pollution
Moving on to the issue of water quality and pollution, the National Sustainable Development Strategy (NSDS) of Bangladesh identifies the following reasons behind degradation of surface water quality:1. Unregulated industrial expansion,2. Rural-to-city migration,3. Encroachment of rivers and water bodies,4. Overloaded infrastructure,5. Confusion about institutional responsibility for the quality of urban water bodies, and6. Insufficient enforcement of environmental regulations [29].The Rivers Buriganga, Shtalakhka, Balu, Tongi Khal and dholeswari which runs past Dhaka City, is at present one of the most polluted rivers in Bangladesh [30]. The city is suffering from an acute lack of domestic water supply. Water is involved in the spread of contagious diseases in essentially two ways. The well-known direct ingestion of infectious agent when drinking contaminated water. The second is due to a lack of enough water for personal solitariness purposes [31]. Approximately 80% of all sicknesses and diseases can be attributed to inadequate water supply and sanitation worldwide [32,33].However, the rivers and canals continued to be encroached upon, and more wastewater from houses and industrial units poured into the rivers without any treatment, with several major sources of pollution being outside the city area—in Ashulia, Savar, Tongi and Gazipur [34]. According to Dhaka Water Supply and Sewerage Authority (DWASA), it can currently supply 75% of water demand, out of which 85% is from groundwater sources (Deep Tube wells) [35]. The presence of toxic metal lead in Elephant road, Dhaka.University, Jatrabari, and Demra area and toxic Penta Chloro Phenol (PCP) and existing pathogenic bacterial load in the WASA supplied drinking water from different areas of Dhaka city were found to be unsuitable for human consumption [36] (Table 2).Some 80% of wastes are being dumped into the rivers in Bangladesh. No wonder our water supplies are in jeopardy. Around 250 industries are discharging chemical pollutants into the Buriganga and Sitalakhya river. Every day 4,000 tons of solid waste and 22,000 tons of tannery waste mixes with water in Buriganga river. Sewage is being discharged directly into the rivers, and the low-lying parts around urban areas [37,38]. By 2021 the garments export target has been set at $50 billion. But the success comes at a huge environmental cost.The dyeing and finishing plants are the major pollutants of water. Turag that flows by Tongi is almost dead with pollution. Its water looks ink black and gives out such a foul smell [39]. Wetlands around Dhaka city are being destroyed through land development and dumping of toxic effluents and untreated sewage. Industrial effluents have destroyed the ecology of rivers near these large urban areas [40]. In Dhaka, 20 canals have disappeared. Liquid and solid wastes, and heavy metals like copper, iron, lead, and nickel are distressing the BOD, COD, DO, TDS, PH of water [4].
Medical and Household Solid Waste
Dhaka City Corporation (DCC) is unable to impose rules on the public. On the institutional side, rules and regulations are not clear. The role and responsibilities of waste generators are not clearly defined i.e., the present law does not provide penalties for illegal disposal of waste or littering. Lack of scientific approaches for problem solving and DCC has shortages of skilled human resources and finances [41]. The accumulating waste is dumped by the residents in the city’s streets, open storm water and wastewater drains or open water bodies where and whenever the collection service is inexistent or dysfunctional [42]. Slum or periphery areas are affected by such a situation.During the annual monsoon rains wastewater and storm water drains which are clogged by solid waste overflow, creating an acute sanitary and hygienic threat in low-lying slum areas particularly. Solid waste generation profile is Per Capita Waste Generation: 0.56 kg/cap/day, Total Waste Generation DCC Area: 5000 tons/day and 70% - 80% of the solid waste is organic. Approximately 200 metric tons of medical wastes are generated in the city per day (Approximately 6% of total waste) (Mohiuddin, 2018). Different industries and their contribution to pollution in Dhaka are: Pulp and paper (47.4%), pharmaceuticals (15.9%), metals (14%), food industry (12.1%), and fertilizers/pesticides (6.6%) [24,37,40].Medical waste may contain highly toxic chemicals and can present a mechanism for transmission of diseases (Table 3). The growth of the medical sector around the world over the last decade combined with an increase in the use of disposable cheap medical products has contributed to the large amount of medical waste being generated. For a megacity like Dhaka, even low hazardous wastes generation rates can lead to the accumulation of large quantity wastes [43].This enormous amount of medical waste poses from different healthcare establishment (HCE) (Table 4) significant health risks to the people associated with waste disposal and treatment. During monsoon, the situation gets worse as medical, toxic chemicals and sewage waste flood Dhaka streets, contaminating dozens of neighborhoods in the process. The reuse of syringes by the general public represents one of the greatest public health problems in the developing world related to health care waste. Worldwide, an estimated 10 to 20 million infections of Hepatitis B and C and HIV occur annually from the reuse of discarded syringe needles without prior sterilization [44].
Food Contamination
Dhaka city now alone generates huge solid wastes per day from industrial discharge, fertilizers, fossil fuels, sewage sludge and municipality wastes and they are the major sources of heavy metals in soils and subsequent uptake by crops, vegetables and other food items causing serious health hazards to human beings [45,46]. A significant transfer of heavy metals like arsenic, cadmium, chromium, copper, lead, mercury, nickel, zinc, molybdenum and vanadium took place from soils to vegetables (spinach, tomato and cauliflower) grown in industrially polluted soils of Konabari at Gazipur and Keraniganj in Dhaka [47]. Industrial wastes and effluents are being discharged randomly on soils, into canals, rivers, along the road sides or in the vicinity of the industrial areas without any treatment where polluted river water is being used for irrigation purpose in paddy and vegetable cultivation causing absorption of heavy metals through the food chain by human beings [48].
Food Adulterants
Important food hazards include microbial hazards, pesticide residues, misuse of additives, chemical contaminants, including biological toxins and adulteration. Although microbiological contamination and chemical hazards have received most attention, it is recognized that food adulteration and food fraud should not be neglected considering their role in public health (FAO/WHO Expert Consultation, 1986). Food adulteration includes various forms of practices, such as mixing, substituting, concealing the quality of food by mis-labelling, putting up decomposed or expired food, and adding toxic substances [49]. About the proportion of adulterated food items in the market varied between 70% to 90%. Nearly 80% food items in the market were found contaminated in a random survey by public health laboratory of Dhaka City Corporation in 2004 [50,51].According to the International Centre for Diarrheal Disease & Research, Bangladesh [52,53], there is approximately 150 food items in the country. A study by the Institute of Public Health (IPH) revealed that more than 50% of the food samples they tested were adulterated. Textile dyes, which are highly injurious to health, are being randomly used to color many types of food. Fish is an essential protein for people of all ages. Many fish sellers spray fish with formalin in an assorted manner, it makes the fish or fruits stiff and keeps them looking fresh for longer. Undoubtedly human health is now under the possession of formalin, in our country about 400 tons formalin is being imported which are goes to human stomach, even though for laboratory or research purposes 100 tons of Formalin is quite enough, 80% of the imported formalin being added to food only for business purposes [54-60] (Table 5).Milk in rural areas is usually devaluated with dirty water, which can cause hepatitis. People are now acquainted with the milk adulteration technique that uses a thickening agent, sorbitol, and detergent. ICDDR, B recent studies shows nearly 75% samples from primary-level producers were contaminated with coliform and more than 50% with fecal coliform bacteria. At the collection points, samples were found contaminated with a high number of coliform bacteria and fecal contamination of more than 90% while more than 40 % of the samples had a high E coli count [52].Vegetable and fruit samples collected from around Savar, Dhamrai and Tongi show the presence of textile dyes, which, in the short-term, will cause diarrhea, food poisoning and gastrointestinal problems, but in the long-term toxic materials will accumulate in the body with serious health implications. In the absence of effluent treatment plants (ETP), the factory wastes are depleted out at will into the farmlands, and ultimately contaminate the farm produce [61]. In Bangladesh, people allowed things like pollution and food contamination to run riot.Till now, neither under the health ministry nor the ministry of science and technology or the ministry of industries, has conducted any examination of the pesticide- residue levels or toxic chemicals in the foodstuff being marketed. These merchants and traders are the enemy not only of the nation and their own children but of the entire mankind. The holy Prophet (PBUH) has disowned those who indulge in this immoral business. He said ‘’ The adulterator is not one of us’’ [58]. Apart from these severe noxious pathogens found in different food samples (Table 6), that are potential causes of stomach problems.Total coliforms and fecal coliforms count (CFU/g) [62]. It is an unfortunate reality that adulteration, especially in food, has become ubiquitous in the society. No one can justify or defend it. Most food products available in the market are adulterated. The average family is eating dangerous colors, chemicals like formalin and carbide, sawdust, soapstone, harmful chemicals and other harmful substances mixed with consumable goods. High level of pesticides content is present in grains, pulses, in fruits and vegetables that we eat [63]. Fecal bacteria found in 97% bottled water [55].Brick dust in chili-powder, colored chalk powder in turmeric, injectable dyes in watermelon, peas, capsicum, brinjal, papaya seeds in black pepper etc. are frequently used [58]. Even more unfortunate is the fact that this nefarious practice increases exponentially during the month of Ramadan. The shopkeepers and the merchants–many of them with a pious façade– try to earn a large amount of profit by this unethical practice, and so they play with the life and health of the people [64,65]. They mix dangerous things in the daily eatables. Even the medicine and drugs are adulterated. Most people can’t even think of having the commodities like ghee, oil, salt and milk, free from impurities [66-70].
Recommendations
Pollution and contaminant control are a never ending, on the other hand a continuous process. It will increase with time as the civilization go ahead. Pharmacists should be aware of the local occupations, companies, and factories and to be cognizant of the initial symptoms of disease. Again, pharmacists should become acquainted with the local community and to adapt the principles of health and medical care to the situations encountered. The pharmacist’s continuing education requirements should include watching the local pattern of society and its diseases and changing the emphasis toward evolving disease patterns and their control.Included in the current environmental issues are the workplace and the future of occupational safety and health regulations, hazards of local ambient environments, such as hazardous and other waste dumps, radioactive waste from weapons production, air emissions, and groundwater contamination of unknown magnitude; the Clean Air act and other and regulatory initiatives; waste reduction and minimization, and radioactive waste and weapons production; global pollution, chlorofluorocarbons and the land ozone layer, the greenhouse effect, and global climate change; and conserving the tropical forest and biological diversity. Government and regulatory authorities are to play strong role in controlling food contaminants and adulteration. An out of the box thinking is decentralization i.e. to move few many important originations away from Dhaka city. With this decentralization, population density will be declined, the ill movement of business Crips will also be diluted.
Conclusion
With constant change to the physical, biological, cultural, social, and economic environment, both pharmacists and citizens should cultivate an informed awareness of these changes, and health providers should adapt their methods of health education, disease prevention, and disease control to the changes in each community. With an unusually large number of people seeking relief from health hazards, providers may play a much more fundamental and personal role in controlling foodborne diseases. The necessary role in environmental health is related primarily to being alert to the conditions prevailing in the community and of working with others to adequately control any of the attendant hazards.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Journal of Pharmacy & Pharmaceutical Sciences please click on: https://juniperpublishers.com/gjpps/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/gjpps/GJPPS.MS.ID.555698.php
24 notes
·
View notes
Text
Respect for Parliament? Do VIP Criminals Want Complete Immunity for Committing Crimes, Corruption and Human Rights Violations?
Juniper Publishers-Open Access Journal of Social Sciences & Management studies
Authored by Yunis Khushi
Opinion
Sanctity of vote, respect and dignity of parliament, dignity and respect of elected members and other related issues have become central and extremely hot topics of debates in media since the disqualification of Mian Nawaz Sharif as Prime Minister as well as politician and chairman of Muslim League N for rest of his life. The questions that need to be answered are: Have the current or the previous Parliaments been true representatives of the people of Pakistan? If not, then why respect such a parliament, which has not worked as representative of the people? Should white collar VIP criminals continue to enjoy complete freedom to loot the national wealth? Should so called elected representatives be given total and complete immunity from being answerable to courts of law for crimes they commit? Why should people of Pakistan give respect to the so-called elected representatives who do not work for the interests of the masses and long-term interests of the country? Why should people respect such representatives who enjoy best state facilities and loot national wealth and invest it abroad i.e. Dubai, USA, Australia and UK? Why should masses respect such parliamentarians who treat masses as mere insects? Why should people of Pakistan respect such parliamentarians who do not bother to even think of doing any legislation for the betterment of the masses? Why should people respect such parliamentarians who have destroyed all the state institutions just for the sake of their vested interests? Do parliamentarians understand the sanctity of vote? Have they given any respect to the votes of the masses?The crimes and wrong-doings of the parliamentarians against the masses and the country have been as below: They have treated masses as their property and slaves. They have been subservient to their party leadership. They acted as kings in the areas they controlled. They only legislated for protecting their vested interests or the interests of their leadership. They never made any legislation for the betterment of the masses or keeping in view the long-term interests of Pakistan. They promoted crime, extremism, terrorism and poverty in the country. They corrupted all the state institutions just to protect their vested interests. They have been committing worst kind of human rights violations including rape, gang rapes and murders against the people of Pakistan. Many of them are involved in running private jails, bonded labor etc. Majority of them are feudal lords, industrialists and businessmen and they do not bother to pay income taxes to the state. By selling their votes in Parliament for millions of rupees to the candidates for Prime Minister ship, President or Chairman Senate, time and again they proved that they are saleable commodities, and anyone can buy them for heavy amounts of money. They use terror, goons and guns to get votes from the poor in their constituencies. They do not have consciousness or courage to challenge the anti-masses and anti-Pakistan policies of their party leadership. They are more after money through commissions and perks rather than solving the problems of their voters.They promoted moral degradation, law and order and criminality in the country. Majority of them is without any ability to read and analyses the legal documents and legislation draft and offer any positive and constructive criticism. They are just dummying to act as yes-men and women to obey the orders of their party leaders. Since 60 per cent of the population lives below the poverty line so they buy votes of poor for RS.1000/- or a bag of flour and then forget the very poor that they are representing. They have strong control and hold on the bureaucracy and police of their areas and use them to crush their opponents and people of their constituencies. They take huge amounts as loans and never pay them back. They invest the looted wealth in Dubai, Switzerland, England, Australia and USA. They are responsible for promoting political instability, economic dependence, poverty, hunger, suicides, unemployment, crime, human rights violations, insecurity, corruption and many other evils in Pakistani society. They have been working against the long-term interests of the country and its people. They worst traitors and enemies of Pakistan and its people. They have never given any respect to the people of Pakistan and their votes.The billion-dollar questions are: How can the parliamentarians who do not have any sanctity for the votes of people of Pakistan demand that they should be respected only because they have come through votes of the people? Why should they be called peoples’ representatives only because they get only 30 per cent votes and that too by rigging elections and using money and violence during the electoral process? Why should people of Pakistan respect the bunch of elite robbers who are the worst enemies of Pakistan and its people? Why should people of Pakistan or judiciary care for the sanctity of the persons who never cared for the sanctity of the votes of the people, sanctity of judiciary and other state institutions? Why do they constantly demand that institutions must remain in their limits? Why do they continue to demand that Courts must do their job and the politicians must be allowed to do their job? What have politicians done for the people of Pakistan during the past 70 years? Should politicians be allowed to do the very job that they have been doing for the past 70 years i.e. of promoting crime, poverty, corruption, human rights violations, political instability, dependency of Pakistan on other powers, and extremism and terrorism? Are they demanding total immunity from being questioned by any court of law for committing crime, promoting poverty, corruption, human rights violations and other wrongs to Pakistan and its people?The problem is not that they are bothered about the sanctity of the vote, rather, they are worried about the tightening of noose around them by judiciary for corruption they have been committing for the past more than 40 years. Also, because they want total immunity from being questioned by any institutions and they want a free hand for committing corruption and for playing with the lives and dignity of the people of Pakistan.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/
For more articles in Open Access Journal of Social Sciences & Management studies please click on: https://juniperpublishers.com/asm/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/asm/ASM.MS.ID.555575.php
#Juniper Publishers#Juniper Publishers LLC#Juniper Publishers Review#JuniperPublishers#open access journals
37 notes
·
View notes
Text
Exercise Guidelines for CKD Patients-JuniperPublishers

JuniperPublishers-Journal of Urology
Abstract
Chronic Kidney Disease (CKD) patients are often overlooked when it comes to exercise programs [1]. Although, the medical community, specifically, a majority of nephrologists are of the opinion that their patients should engage in regular exercise to improve overall health [2]. Physical inactivity contributes to a reduction in activities of daily living and reduced quality of life [3]. By enhancing the strength of their muscles, bones, and joints through exercising, people with CKD can improve their balance and coordination [4]. This can further prevent them from falling and likewise, protect their independence as they age. Moreover, it is widely known that CKD patients are at high risk for premature death as a result of cardiovascular disease due in part to their sedentary behavior [5]. By increasing the physical activity levels of individuals with CKD, it's possible to decrease their risk of cardiovascular disease and improve their physical functioning, thus thwarting premature death [6].
More recently, studies have looked at the possibility that increasing physical activity levels may slow the rate of decline of estimated glomerular filtration rate (eGFR) in patients with CKD stages 3 to 4. The latest Kidney Disease Improving Global Outcomes (KDIGO) Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease lifestyle section recommends that individuals with CKD engage in physical activity for at least 30 minutes per day, 5 times per week [7].
Besides counseling CKD patients on diet modifications, registered dietitian nutritionists (RDNs) especially those with expertise in renal nutrition and nephrology are in a position to also aid their patients in recommendations for increasing their physical activity levels. The RDN should begin by determining in their initial nutritional assessment, the activity level of the CKD patient. A Low Physical Activity Questionnaire (LoPAQ) has been developed to assess and could be further used for monitoring physical activity. Although it was constructed for patients on hemodialysis, this instrument would also be pertinent for use with the CKD patient population. After identifying areas to improve on, the RDN may recommend structured activities including aerobic, strength, and flexibility exercises. A combination of all three types of exercises performed five times a week using different muscle groups each day would improve the CKD patient's endurance and strength [8].
It is important that the RDN ensure that the exercises suggested be individualized to the CKD patient's current stage of physical ability. Implementing an exercise program along with diet modifications can be challenging for both the RDN and the CKD patient. However, with continued follow-up monitoring and adjustments along the way, patients with CKD can improve their overall health. The corresponding patient education handout is designed to provide clinicians with a starting point in addressing an exercise program with their CKD patients.
Keywords: Physical activity; Exercise; Chronic Kidney Disease (CKD); KDIGO; LoPAQ
Intended Audience: CKD
Why Exercise?
People with Chronic Kidney Disease (CKD) can benefit from exercising regularly just like those without this condition. Your quality of health can improve if you can engage in activities that strengthen the muscles, bones, and joints in your body. This can improve your balance and coordination which can prevent you from falls and protect your independence as you get older.
Other physical exercise benefits also include better blood pressure and diabetes control. Sometimes these diseases can worsen when the kidneys are damaged and more medications may have to be added to those that you are already taking.Exercising regularly may help lower your blood pressure and keep it from further damaging the kidneys. In the same way, exercise helps to lower your blood sugar levels throughout the day and night and puts less stress on the kidneys.
What types of exercises are best?
Structured activities include aerobic, strength, and flexibility activities. Aerobic activities are where you use large amounts of oxygen. These types of exercises include walking, jogging, stair climbing, swimming, water walking and water aerobics, gardening, dancing, bicycling, and chair exercises. Other types of aerobic exercises can be performed on machines such as a treadmill, stationary bike, or elliptical trainer. Strength training involves using large muscles of your body to perform activities. For instance, free weights or dumbbells, resistance bands and tubes, Pilates, and medicine balls aid in strengthening your muscles.Flexibility type activities move your joints through their full range of motion and help to lessen your risk of injury when performing physical activities. These include stretching, Yoga, and Tai Chi.
How much should I exercise?
If you haven't already been exercising regularly, you will want to start slowly and work upto a pace that you are comfortable with each day. Ideally, you will want to engage in exercise— aerobic, strengthening, or flexibility activities—5 times per week. If you can get in a habit of exercising at the same time each day, it will be less of a chore and more of a routine of living healthfully, just like eating your meals.For instance, begin and end your work-out with stretching exercises, follow with either an aerobic activity such as walking or strength training such as lifting hand- held weights. A combination of these activities using different muscle groups each day such as the upper body one day and the lower body another, will improve your health over time.
How can I stay safe while exercising?
The main thing to remember when exercising is to listen to your body. Keep in mind that exercising regularly is healthier than not exercising at all. But with that said, if you do develop any of the following problems, stop what you are doing and seek medical help:
Unusual shortness of breath
Pain in the upper part of your body including your jaw
Nausea or vomiting
Cramping of muscles or joint pain
Sudden weakness especially in your limbs
Trouble with eyesight, speech, or difficulty swallowing
Sudden onset headache, dizziness, or a feeling of lightheadedness
Chronic Kidney Disease should not hold you back from living more fully. It just may mean that that you will need to put forth more effort in improving your health with the addition of exercising regularly. You may want to seek out support from family and friends to help you along the way. Often, you need the encouragement of others to motivate you to continue to stay on course. So, don't hesitate in asking those close to you for their help.
Sample Exercises
Aerobic
Walking Program:
Begin by walking at a slow but steady pace for 10 minutes 5 days a week.
Once comfortable with the walking 10 minutes daily, then increase to 20 minutes every other day at a brisk pace.
At one month, increase your time to 30 minutes every other day.
Then, after one month, walk 30 minutes 5 times a week.
At this point, you will be walking long enough and with the right amount of effort to support physical benefits to improve your health.
Strength
Toe Raises:
Stand straight with your hands on a counter or rail for support. Slowly raise your heels up off the floor and count to two.
Then lower your heels back down to the floor. Repeat 8-12 times.
Leg Lifts:
Sit in a chair where your back is straight and your knees are bent and feet are flat on the floor. Lift and straighten your right leg and hold for a few seconds. Lower your right leg to the starting position.
Repeat using your left leg. Perform exercise 8-12 times with each leg.
Flexibility
Stretching exercises will help to lengthen and loosen your muscles and joints. Perform these as a warm-up and cool-down part of your overall exercise plan.
Shoulder Rotation:
While standing or sitting, move the top of your right shoulder forward in a circular motion for 15-30 seconds.
Repeat with your left shoulder.
Leg stretch:
While lying on your back, bend your right leg and keep your left leg straight.
With both your hands placed behind your right leg, pull your thigh toward your chest and hold for 15-30 seconds.
Repeat with your left leg.
To know more about Journal of Urology
Click on: https://juniperpublishers.com/jojun/index.php
To Read more about JuniperPublishers
Click on: https://juniperpublishers.com/index.php
#JuniperPublishers#Juniper Publishers Review#Juniper Publishers LLC#Juniper Publishers#open access journals#Open access journal of Urology#Open access journal#Open access journal of Urology and Nephrology
0 notes
Text
Naimi’s Structure and Migration: A Tissue-Specific Pattern of Organization Discovered in Normal Bladder Urothelia-JuniperPublishers

JuniperPublishers-Journal of Urology
Abstract
Introduction: Sequential migration and organization are critical events in tissue development. The urothelium, the epithelium lining urologic tissues, is highly specialized regarding the watertight function and adaptation to large and frequent changes in urine volume. To establish the functional state of this tissue, horizontal cells growth is required to allow the vertical development into a multilayered uroepithelium. If this first step is already documented, the mechanism implicated in the switch toward the vertical growth is not yet described.
Methods: We had elaborated a three-dimensional bladder model, made of bladder mesenchymal cells (BMC) seeded in a collagen matrix which can promote bladder urothelial cells (BUC) development.
Results: This in vitro model allowed us to discover a behavior specific to BUC, resulting in a specific urothelial stratification and differentiation pattern. Cellular alignment into a circular arrangement, named Naimi’s structure, followed by coordinated gyratory cellular movement, named Naimi’s migration, were sequentially observed in our in vitro model and were also confirmed in native bladder
Conclusion: We describe here the steps that led to Naimi’s structure and migration. Ultrastructural observations are also provided to document the remarkable organization of urothelial cells and the underlying mesenchymal rearrangement.
Keywords: Urinary bladder; Urothelium; Cell migration; Extracellular matrix
Abbreviations: BM: Tissue-Engineered Three-Dimensional Bladder Model; BMC: Bladder Mesenchymal Cell; BUC: Bladder Urothelial Cell; DME: Dulbecco-Vogt modification of Eagle’s Medium; EGF: Epidermal Growth Factor; FCS: Fetal Calf Serum.
Go to
Introduction
Cell migration is a function that plays a crucial role in normal physiology as well as in various pathologic conditions. Spatiotemporal coordination of cell migration leads several steps of organ development, apoptosis, wound repair, and tissue regeneration [1]. The literature describes matrix- dependent adhesion molecules, such as integrins, that allow cell anchoring and displacement in-vitro and in-vivo [2]. Cell migration is polarized by various signals, such as chemo attractants, electrical influx [3], magnetic fields [4], cell-cell and cell-matrix interactions, dynamic and static tensions or stress [5,6], or spontaneous movement through intermediate filament gene modulation. Cell differentiation and specialization induce morphological and functional changes that influence migration and tissue organization. All these factors must be considered prior to perform tissue reconstruction in-vitro, notably through the tissue-engineering approach. Isolating, growing and characterizing various cell types in culture, demands frequent observations performed under different conditions. Bladder urothelial cells (BUC) cultured on plastic and on a collagen matrix repeatedly showed a new and unique pattern of organization and migration that we named Naimi’s structure and migration.
The uroepithelium is a distensible epithelial barrier which is able to accommodate the variable volume of urine content and prevent the infiltration of urine into the vascular system [7]. It is composed of multi-layers of urothelial cells that differentiate into highly specialized umbrella cells that exhibit strong watertight function-related features [8]. Among them, the unique morphology of their apical plasma membrane displays scalloped features [9,10]. This particular pattern results from membrane extension, containing integral membrane proteins called uroplakins, which initiate and maintain urothelial membrane remodelling, essential to urine barrier function [11,12]. In the developing phase, it is known that urothelial cells adopt high proliferation activity to entirely recover the mesenchymal layer [13], but the mechanisms that trigger the switch of horizontal toward vertical development into mature and multilayered urothelium are not well documented.
We have established a tissue-engineered three-dimensional bladder model (BM), based on bladder mesenchymal cells (BMC) seeded in a collagen matrix covered with BUC. In order to provide conditions close to the physiological tissue state, we stimulated mesenchymal-epithelial interactions through urine exposure, in our in-vitro three-dimensional bladder model. These conditions allowed BUC to reach a confluent state that led to a spectacular mode of organization and migration, that was never reported in any cell culture system nor in native tissues up until now, including bladder. After the completion of the horizontal development, progressive circular alignment of these cells induced a massive gyratory movement in counterclockwise or clockwise direction, combined to a lateral translation of the whole structure. Following the formation of these remarkable structures, Naimi’s migration was observed simultaneously at several sites on the same tissue-engineered uroepithelium. The ultrastructural organization of BUC and the steps leading to the Naimi’s migration pattern are described.
Go to
Materials And Methods
Porcine urothelial and mesenchymal cell isolation
Porcine bladder tissue samples were collected from at least 3 different adult pigs, with the approval ofthe local ethics committee. The tissue processing was performed within 2-3 hours after removing the porcine bladders postmortem. The urothelium was surgically resected from the mesenchymal components of each bladder biopsies. The epithelium and the mesenchyme were set apart. Samples of mesenchyme were cut into pieces of 5mm2 in order to be subjected to enzymatic treatment. Collagen being the major constituent of bladder matrix, collagenase was chosen to digest the native mesenchymes. The tissues were digested in 0.1% (0.2U/ml) collagenase H (Boehringer Mannheim, Montreal, Canada) prepared in DME culture medium containing 10mM CaCl2 without any supplement, overnight at 4°C. Homogenates were centrifuged for 10 min at 300 g and the BMC pellets were resuspended in DME supplemented with 10% fetal calf serum (FCS). BUC were isolated from pig’s urothelium digested with thermolysin, as previously described [14].
Human bladder cancer cell lines
Four bladder cancer cell lines were used: MGHU-3 had been generously provided by Dr Y. Fradet’s lab from a transitional cell carcinoma of a 76 years old Caucasian male (grade 1, passage 97), RT4 (ATCC HTB-2, grade 1, passage 237) from a transitional cell papilloma of a 63 years old Caucasian male, SW780 (ATCC CRL-2169, grade 1, passage 88) from transitional cell carcinoma of an 80 years old Caucasian female, and T24 (ATCC HTB-4, grade 3, passage 56) from a transitional cell carcinoma of a 81 years old Caucasian female.
Bladder cell culture
Porcine BUC and human bladder carcinoma cells lines were cultured in a combination of Dulbecco-Vogt modification of Eagle’s medium (DME) with Ham’s F12 in a 3:1 proportion (Flow Lab., Mississauga, Ontario, Canada), supplemented with 10µg/ml human epidermal growth factor (EGF, Chiron Corp., Emeryville, CA, USA), 5µg/ml crystallized bovine insulin, 5µg/ ml human transferrin, 2 X 10-9M 3,3’,5’, tri iodo-L-thyronin (Sigma Chemicals, St-Louis, MO, USA), 0.4µg/ml hydrocortisone (Calbiochem, La Jolla, CA, USA), 10% FCS (Gibco BRL, Life technologies Inc, Grand Island, NY, USA), 100IU/ml penicillin G and 25µg/ml gentamycin (Sigma). This culture medium was defined as the proliferation medium. It was changed three times a week. After 7 days in culture, urothelial cells had reached 85% confluence and were ready to be stored and sub cultured. BMC were cultured in DME supplemented with 10% FCS (Gibco), 100 IU/ml penicillin G and 25µg/ml gentamycin (Sigma). Culture medium was changed three times a week. Cultures of BUC and BMC were both kept in an 8% CO2 atmosphere at 39°C, and human bladder carcinoma cells lines at 37 °C.
Urothelial cell monolayers culture
BUC and human bladder carcinoma cells lines were grown to confluence (n=6/each urothelial cells type) on plastic culture- treated dishes and on a cellular and BMC seeded collagen gels. All these cells were cultured in the proliferation medium, as described above.
Production of porcine BM
Step 1: Preparation of the mesenchymal layer of the BM: According to the protocol of Paquette, et al. [15], a mixture of native bovine Type I collagen (2.0mg/ml) was prepared by dissolving the powder overnight at 4 °C in sterile 0.017M acetic acid. A solution of 0.84 ml of DME 2.7X containing 200 IU/ml penicillin G and 50 µg/ml of gentamycin, pH 8.0, was mixed with a second solution containing 0.56 ml of FCS, 1.43 ml of the stock collagen solution, 30 µl of NaOH 0.7N and 0.15 ml of a BMC suspension (4 x 105cells/ml of DME supplemented with 10% FCS, 100 IU/ml penicillin G and 25 µg/ml gentamycin).
Step 2: Coating of the mesenchymal layers with complete porcine urine: Porcine urine samples were collected directly from bladders of adult porks immediately postmortem. The urine was frozen without any filtration and stored at -30 °C until use. When the cell-seeded collagen matrices had polymerized (after 20-25 min), a volume of 1 ml was poured onto each mesenchymal layer for 20 min at room temperature. This step aimed at coating the surface of the collagen gel with the natural constituents of porcine urine. Then, the urine was removed by gentle aspiration, and the mesenchyme was ready for epithelialization (n=6). Groups of uncoated mesenchymes (n=6) were used as negative controls. Porcine urine exposure of the BM was repeated at every change of culture medium.
Step3: Epithelialization of the BM: The epithelialization was performed by seeding porcine BUC (4 x 105 cells/BM) on the mesenchymal constructs, pre coated or not with porcine urine. During the first 5-6 days after epithelialization, all BM were maintained in the proliferation medium, supplemented with 50 Hg/ml ascorbic acid, until confluent state was obtained.
Step4: Culture of the BM: The BM were cultured in the differentiation medium as soon as a confluent layer of BUC had covered the mesenchymal constructs (5-6 days after epithelialization, depending on cell growth rates). The differentiation medium was defined as the proliferation medium, supplemented with 5x10-8 M retinoic acid (RA, Sigma) but without EGF, to reduce the secretion of gelatinases by the cells, which degrade the collagen matrix in culture [16]. The culture medium was changed every other day, during 10 days. Before each change of culture medium, a volume of 1 ml of pure porcine urine was poured on the urothelium, and kept for 20 min at room temperature (n=6). Then, the urine was removed by gentle aspiration in order to be replaced by the differentiation medium. Groups of uncoated mesenchymes were cultured without any urine supply (n=6).
Electron microscopy analyses
The electron microscopy analyses were performed by an independent service. BM and native bladder samples were fixed with 2.5% glutaraldehyde in 0.1 M cacodylate buffer, pH 7.4 at 4 °C. Then, they were rinsed with cacodylate buffer and a post fixation in 1% osmium tetroxide. The biopsies for transmission electronic microscopy were stained with uranyl acetate and dehydrated through a graded series of ethanol then embedded in Epon (Polysciences, Warrington, PA). They were cut in ultra-fine sections and counterstained with lead citrate and uranyl acetate. The sections were examined with a JEM 1230 (Tokyo, Japan). The BM and native bladder biopsies for scanning electronic microscopy were dehydrated then critical point dried. Samples were spattered with gold and viewed with a Jeol JSM-63060LV (Tokyo, Japan).
Time-lapse observations of Naimi’s structures and migration
BUC cultured on plastic (n=6), and on reconstructed mesenchymes (n=6) were observed for 48 hrs under a timelapse fluorescence microscopy using a Zeiss Axio Observer Z1, to monitor the evolution of Naimi’s structure and migration from the beginning. The microscope allowed taking pictures in 6 wells in rotation, so that 6 fields could be monitored every 30 min, over a period of 48 hrs.
Go to
Results
BUC and BMC morphology in culture
Morphologically stable cell populations (initially at passage 0), were sub cultured over more than 3 passages. Forty eight hours after epithelialization of tissue-engineered mesenchymes pre coated with urine, BUC showed high plating efficiency (Figure 1A). Colonies of BUC grew well (Figure 1B), to reach a confluent state after 5 days of culture in medium of proliferation (Figure 1C). In the 3D collagen matrix of the mesenchymes, BMC progressively spread among the collagen fiber network (Figure 1D). BMC progressively aligned themselves in the horizontal plane (Figure 1E & 1F), in response to the radial tension applied on the collagen gel by the peripheral anchorage.
BUC behavior during the formation of Naimis structures
At various sites, at random and in a spontaneous fashion, confluent BUC progressively regrouped to adopt a semi-circular alignment at various sites of the reconstructed urothelium. This first step was followed by the orientation of the cells in a spiral, that led to a massive gyratory movement oriented in a clockwise (Figure 2A) or counterclockwise (Figure 2B) direction. During this migratory process, all surrounding BUC remained morphologically similar, without any sign of degeneration. The center of Naimi’s structure was always dense, filled with BUC aligned in superposed layers, which could be described as cords or ropes, organized in a comparative fashion to the eye of a tropical cyclone (Figure 2C). BUC surrounding the center of Naimi’s structure adopted an elongated morphology and formed parallel lanes of cells organized in concentric circles, like a spiral (Figure 2D-2F). After 15 days of culture in presence of urine, the Naimi’s structures exhibited an important extension through the mesenchymal layer (Figure 2G). In the same time, BUC grown on mesenchymes that were not exposed to urine were capable to create Naimi’s structures, but of smaller diameters and the whole process occurred at slower rate (Figure 2H). Similarly, Naimi’s structures were observed in BUC monolayers, grown to confluence on culture-treated dishes.
Ultrastructural analyses of Naimi’s structures: BUC organization
Naimi’s structures observed in our BMs (Figure 3A), were analyzed under electron microscope (Figure 3B). Scanning electron analyses of Naimi’s structures (Figure 3C.1), showed that the center of these spirals-like configurations included a lumen (Figure 3C.2), were well-circumscribed and differentiated, as confirmed by the advanced organization of BUC’s apical membranes (Figure 3C.3). Indeed, the apical surface of BUC was covered with abundant membrane extensions, which interactions between each other allow scalloped features to be established and present on the apical surface of mature urothelium. These membrane extensions are also exposed on BUC that form a cord that links the two Naimi’s structures (Figure 3D.1-3D.3). In contrast, BUC located outside Naimi’s structure show a weak remodeling of the apical (Figure 3E.1, & 3E.2).These observations strongly suggest that Naimi�s structures are triggering urothelium maturation. Observations made on porcine native bladder are in agreement with this hypothysis.
Interestingly, scanning the surface of native urothelium, observations confirmed the presence of more complex Naimi’s structures associated with high level of urothelial maturation in native bladder ex-vivo (Figure 4A & 4B). Native Naimi’s structures of diametrical sizes, ranging from about 20 up to several hundreds of mm, were all characterized by a lumen at their center and scalloped features specific to fully differentiated urothelium (Figure 4C). At the center of the Naimi’s structures analyzed in native bladder samples, concentric cords of BUC were organized in the same pattern observed in our BM (Figure 5A & 5B). The BUC surrounding the center of Naimi’s structures were aligned to form several parallel folds, each row being composed of a dense cell-matrix network (Figure 5C). In contrast with BUC located between Naimi’s structures, and in agreement to observations made in-vitro, cells adopted an elongated morphology in these rows (Figure 5D), showing well defined or in progress scalloped features.
We observed different levels of maturity of Naimi’s structures in the native bladder tissues, like in our BM in vitro. To investigate cell-matrix interactions and matrix fibers orientation at the interface between two dense concentric folds within Naimi’s structure (Figure 6C), we gently separated them (Figure 6A & 6B). Longitudinal collagen fibers alignment was obvious (Figure 6D), at the superficial matrix layer located outside of the two superposed cell cords. However, the density of the extracellular matrix fibers network and complex cell-matrix arrangement could be observed inside each cord that composed Naimi’s structures (Figure 6E).
Ultra-structural analysis of Naimi’s structures: Lateral view
Transmission electron microscopy analyses of our BM’s urothelium confirmed that Naimi’s structures were covered with a multilayered-like urothelium, under the culture conditions established (Figure 7A), highly comparable to the urothelium of Naimi’s structures observed in native bladder samples. Interestingly, wide matrix bundles were present under the urothelium of Naimi’s structures (Figure 7B), and the space between these bundles was filled with collagen fibers of variable calibers (Figure 7B). At higher magnification, the bundles were too dense to detect the typical periodicity of collagen (67 nm) among their fibers, but collagen fibrils were observed all along the periphery of the bundles (Figure 7C), with BMC sparsely distributed nearby them (Figure 7D).
The bundles ran densely packed, parallel, and straight changing their direction only in periodic crimps where fibrils showed a local deformation. In areas of the urothelium divided of Naimi’s structures, matrix bundles were not observed (Figure 8A), but BMC were surrounded of collagen fibrils distributed randomly around the cells (Figure 8B), which did not show any specific alignment (Figure 8C).
Genesis of Naimi’s migration
Such BUCs behavior and organization were observed on plastic (Figure 9 & 10), and on reconstructed mesenchymes (Figure 11 & 12). However, on the tissue-engineered mesenchymes, the three-dimensional structure of the matrix allowed visualization of the superposition of BUC at the center of the spiral of cells, and the presence of underlying mesenchymal bundles was previously described (Figure 11U-11Y). In both cases, independent rows of BUC, leading to respective Naimi’s structures, cross each other (Figure 9A-9J & Figure 11A-11E), before inducing the gyratory movement that progressively expand (Figure 9K-9Y & Figure 11F-11Y) and moved laterally (Figure 10 & 12), attracting surrounding cells to follow the flow induced by this major displacement. Interestingly, the cells located near the end of the spiral (Figure 10O & Figure 12P), often moved along to create lanes that joined another center of rotation. More importantly, the spiral organization of the cells was observed on native urothelia, but not on different bladder carcinoma cells lines (Figure 13A-13D), demonstrating that this pattern of cell migration wasn’t an artifact induced in-vitro.
Go to
Discussion
Science is based on observations. Trivialization of classical cell culture happens too often, being integrated in a daily routine and presenting several limitations that can’t be denied, when compared to complete native tissues. Living cells in culture have been the source of numerous discoveries associated with major advances in many fields of research. To our knowledge, Naimi’s structure and migration were never described and analyzed, despite such particular pattern of cell organization that can be observed repeatedly in confluent BUC monolayers grown on conventional plastic dishes.
Tissue-engineering still belongs to recent fields of research, as it offers multiple possibilities of culture conditions including many types of substrates combined to multiple threedimensional types of co-cultures [17]. Collagen gel facilitates direct observations of the cells seeded at its surface and within the fibers network. Naimi’s structure and migration of confluent BUC, grown on tissue-engineered mesenchymes, provided the opportunity to perform ultra-structural analyses between the cells and under the spiral made by the cells. Such in-depth observations could not be done with BUC seeded on plastic. Obviously, Naimi’s structure was certainly seen by several other research groups working with BUC in culture, but to our knowledge, none studied this process. Having worked with various types of human and animal cells, including hepatocytes, human skin (keratinocytes and dermal fibroblasts), bronchi (ciliated cells, goblet’s cells, mesenchymal cells, smooth muscle cells), connective tissue cells (ligament fibroblasts, osteoblasts, chondrocytes), blood cells and various immune cell types, and cancer cells of various epithelial and mesenchymal origins, none ever showed such pattern of coordinated migration [15,16,18,20]. These results strongly suggest that Naimi’s structure and migration are tissue-specific, and more precisely urothelia- specific. The typical spiral pattern, that seems to be essential for Naimi’s migration to occur, was observed on native bladder urothelia. This is an important indication that Naimi’s structure and migration represent a natural mode of cell movement that happens in-vivo. The purpose of this particular pattern of structure and migration remains unknown for now. However, pre-terminal (in-vitro) and terminal (in-vivo) differentiation of urothelium, including Naimi’s structure, suggest that it could be a mechanism for vertical urothelial development. The remarkable rearrangement of underlying BMC and collagen matrix into wide matrix bundles also indicates a potential mode of tissue-specific development. The researches to determine the implications of such epithelial and mesenchymal events are pursued. One of the triggering events that stimulate BUC to induce Naimi’s migration is the state of confluence, in accordance with the reported fact that the vertical development requires a complete bladder mesenchyme coverage by urothelial cells in-vivo [13]. We may postulate that tension between BUC, associated with cells high density, stimulates Naimi’s structure formation and migration within the confluent BUC layer. This cellular tension, in addition to a physiological environment supplied by the mesenchymalepithelial interactions, and urine components promoting rapid extension of Naimi’s structures and migration, allowed preterminal differentiation of our tissue-engineered urothelium in only 10 days in culture. The ultrastructural properties of the matrix bundles observed in the mesenchymal layer of Naimi’s structures may play an important role in the maintenance of the spiral-like tissue, especially during its displacement. In fact, such densely packed bundles, oriented in a parallel fashion and changing their direction only in periodic crimps (Figure 7), may be compared to ligament collagen matrix [6,21]. Biomechanical elongation and contraction happen in a cyclic manner in response to bladder wall physiological response to urine collection and excretion. Such cyclic strain demands a fast adaptation of the bladder wall to frequent variation in internal tension. Similarly, ligaments respond to cyclic elongation in-vivo, being subjected to strains induced by the movement of the bones within a joint. It is possible that Naimi’s structures contribute to bladder wall adaptation to the level of diametrical tension associated with urine volume variations. Moreover, the Naimi’s structures gyratory movement, observed under time lapse microscope, involves significant matrix modulation that attracts surrounding BUC, resulting in a wider spiral-like structure bordered by well- aligned cell rows. Work is in progress to assess the function of Naimi’s structure and migration and its modulation in response to external tension applied on tissue-engineered bladder constructs in-vitro.
Go to
Conclusion
Cellular alignment into a circular arrangement followed by coordinated gyratory cellular movement were sequentially observed in our in-vitromodel and were also confirmed in native bladder. Ultrastructural observations showed the remarkable organization of urothelial cells and the underlying mesenchymal rearrangement. This phenomenon could be involved in the process of urothelium maturation.
To know more about Journal of Urology
Click on: https://juniperpublishers.com/jojun/index.php
To Read more about JuniperPublishers
Click on: https://juniperpublishers.com/index.php
#Juniper Publishers#Juniper Publishers Review#Juniper Publishers LLC#JuniperPublishers#urology#Open access journal of Urology#Nephrology#Open access journal of Urology and Nephrology
0 notes
Text
Evaluation of the Cardiovascular System Prior to Transplantation; an Endless Debate-JuniperPublishers

JuniperPublishers-Journal of Urology
Abstract
Cardiovascular disease continues to be the most important cause of death after transplantation. Although there is a dramatic improvement in the diagnosis and management of cardiovascular disease, the rate of cardiovascular death after kidney transplantation still higher compared to general population. Chronic kidney disease is associated with many risk factors that lead to increased incidence and prevalence of cardiovascular diseases. In this mini-review, we will discuss recent advances in cardiovascular work up prior to kidney transplantation.
Keywords: Cardiovascular disease; Work-up; Assessment and renal transplantation
Abbreviations:ESRD: End Stage Renal Disease; CKD: Chronic Kidney Disease; KDOQI: Kidney Disease Outcomes Quality Initiative; ACR: American College of Cardiology; AHA: American Heart Association; CAD: Coronary Artery Disease; ICA: Invasive Coronary Angiography; MPI: Myocardial Perfusion Imaging; SPECT: Single Photon Emission Computed Tomography; DSE: Dobutamine stress echocardiography; ABI: Ankle-Brachial Index; CTA: Computed Tomography Angiography; MRA: Magnetic Resonance Angiography; DS-CMR: Dobutamine stress Cardiac Magnetic Resonance; ABI: Ankle-Brachial Index
Go to
Cardiovascular Assessment
Although renal transplantation reduces cardiovascular morbidity and mortality compared to end stage renal disease (ESRD), it is associated with an early increase of cardiovascular morbidity and mortality [1-9]. Renal transplantation recipients should undergo rigorous screening processes considering not only peri-operative risk, but also must be designed to provide information regarding CV risk in the early years post-transplantation [10,11].
There is no universally accepted screening process especially in asymptomatic chronic kidney disease (CKD) patients given their high cardiac risk even if asymptomatic [8,12-27]. All recipients must be tested by non-invasive methods as recommended by Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines and the only determinant for testing by American College of Cardiology/American Heart Association (ACR/AHA) guidelines were functional status tempered by risk factor profile [18,19].
Intermediate levels of testing result from application of guidelines developed by more kidney-specific stakeholder groups (Figure1) (Table 1) [20,21].
As conventional CV risk factors are highly prevalent in this population, exclusion of coronary artery disease (CAD) comprises a substantial component of CV screening in higher risk transplant candidates [17]. There is no consensus on which technique will be optimal when deciding that cardiovascular screening is mandatory [22-25]. The presence or absence of chest pain provides little clinical certainty in distinguishing between the presence and absence of significant CAD in potential renal transplant recipients [23,26-30]. There is substantial debate regarding the necessity to perform invasive coronary angiography (ICA) to exclude significant CAD prior to transplantation. Numerous studies have been published demonstrating the advantages and limitations of non-invasive investigations in the ESRD context [27,31-33].
Exercise-based stress testing is widely accepted as the preferred, and most accurate, methodology for the non-invasive exclusion of coronary ischemia. Uraemia, however, is commonly associated with reduced exertional capacity, frequently preventing ESRD patients from achieving the necessary level of tachycardia required to minimize the occurrence of a false negative result. Previous studies have demonstrated a higher risk of future cardiovascular events amongst patients unable to complete exercise stress tests, regardless of the presence of a negative result. Thus combinations of exercise and vasodilatory agents, or dobutamine infusion have been utilized to optimize non-invasive imaging results [34-36].
Conventionally, exercise (+/- dipyridamole or adenosine) or dobutamine single photon emission computed tomography (SPECT) and myocardial perfusion imaging (MPI) have been the most commonly utilized investigation in the non- invasive exclusion of ischemia prior to RTx. Dobutamine stress echocardiography (DSE) is a commonly utilized alternative, with some results indicating a higher specificity attributable to this investigation, but similar overall accuracy in non- renal failure patients [37,38]. The presence of a negative study does not entirely exclude the presence of haemo dynamically significant coronary artery disease, hence the preference within some RTx centers to rely solely upon ICA for the evaluation of coronary risk in this context, however are associated with procedural risk [32]. Myocardial perfusion studies and dobutamine stress echocardiography (DSE) show equally well results in diagnosing patients with stenosis ? 50% of a major coronary artery, which supported by Cochrane meta-analysis [39]. Data from large studies on general populations shows similar or superior outcomes of medical treatment over revascularization, except in triple vessel disease [15,40-42].
Alternatively, recent data from CKD studies compared to the general population confirm compromised therapeutic responses to medical treatment [43].
As diabetics have high risk of cardiac events and poor negative predictive value of non-invasive test, some advice use of cardiac catheterization as sole for prediction of adverse cardiac events in diabetics waiting transplantation [44,45]. Dobutamine stress Cardiac Magnetic Resonance Imaging (DS-CMR) has recently been demonstrated to provide a very high level of accuracy in the non-invasive detection of significant CAD, with low procedural risk [46-49].
Which results at cardiovascular assessment prevent transplantation? This is difficult to judge. Most centers currently will consider ischemia not responsive to revascularization as contraindication to transplantation. Similarly, after revascularization of advanced coronary disease, severe left ventricular dysfunction considered contraindication to transplantation as it associated with high mortality [50]. On the other hand, absence of coronary disease in the presence of severe left ventricular systolic dysfunction considered as indication for transplantation as many reports confirm cardiac function improvement after restoration of kidney function in adult and pediatric.
Many dialysis patients have pulmonary hypertension which worse with duration on dialysis. Data from recent studies shows increased risk of graft and/or patient loss in advanced elevation of right ventricular systolic pressure ≥50 mmHg [50].
Some data suggest that high right ventricular systolic pressure considered as contraindication to transplantation till treated. Finally, it is mandatory to manage advanced vascular heart disease before transplantation [51].
Go to
Assessment Of Peripheral Vascular Disease
There is an absolute indication for vascular assessment including general assessment of prognosis as well as specific assessment of the vascular supply needed for the transplant operation. Atheromatous iliac arteries that have been ossified through years of CKD management must thus be carefully assessed by the surgeon planning to perform the transplant [52-54].
The presence of peripheral arterial disease (PAD) and its degree could be assessed by noninvasive tests. These tests include ultrasound, segmental limb pressures, the ankle-brachial index (ABI), segmental volume plethysmography, and exercise treadmill test. Furthermore, recent data suggest that computed tomography angiography (CTA) and magnetic resonance angiography (MRA) have become important noninvasive methods for the PAD assessment [55-60]. Arteriography still considered as gold standard for diagnostic evaluation of PAD. Nowadays, to establish the diagnosis of PAD and to plan the most adapted intervention, most vascular specialists use three-dimensional reconstructed angiography (CTA or MRA) or bidimensional images obtained with Duplex-ultrasound modalities [59-61]. However, diagnostic standard angiography may still remain necessary, in selected cases [62,63].
Go to
Conclusion
Cardiovascular screening and intervention for transplant recipient especially asymptomatic patients are common practice but the clear benefits of these interventions still questionable. Large Randomized controlled trial is needed to clearly define the risk/benefit of the current practice.
To know more about Journal of Urology
Click on: https://juniperpublishers.com/jojun/index.php
To Read more about JuniperPublishers
Click on: https://juniperpublishers.com/index.php
#Juniper Publishers#Juniper Publishers Review#Juniper Publishers LLC#JuniperPublishers#urology#Open access journal#Open access journal of Urology#Nephrology#Open access journal of Urology and Nephrology
0 notes