
A place to remember the thoughts, feelings, and inspirations in my daily life.
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by lindsosaurusrex and here's what we found interesting.
Average Info
Notes Per Post
181K
Likes Per Post
108K
Reblog Per Post
73K
Reply Per Post
425
Time Between Posts
4 months
Number of Posts By Type
Photo
14
Video
1
Text
2
Last Seen Tumblr Blogs





Fun Fact
Premium Tumblr themes are available from anywhere between $9 to $49.
Photo

























Rhokotela’s Intro to ECGs
Please don’t repost or use without crediting the source. Otherwise, happy interpreting!
854 notes
·
View notes
Photo









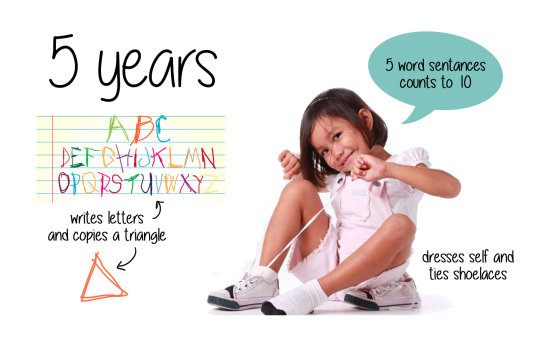
I’m pretty sure I’m not the only one who has trouble remembering developmental milestones. I put these together, but can’t take credit for any of the photography. Hope someone finds them helpful!
172K notes
·
View notes
Video
youtube
Myocardial infarction

3 cardinal signs:
Elevation of ST segment
Inversion of T wave
Deep & wide Q wave
With reciprocal changes in the leads facing the opposite wall:
Depression of ST segment
Tall, upright T waves
Changes do not appear at the same time. It happens in this order:
Elevation of ST segment stays for 2-3d and gradually goes back to base level in 1-2w
T wave becomes inverted after 2 days, and remains like that for 3w, and gradually becomes flat and then upright over 2-3m
Q wave = muscle death, appears after 1 week, and gradually deepens and remains permanent. Size proportional to size of infarct.
Timeline:

1°d: ST segment elevation + tall T wave
2-3°d: ST segment still elevated + T wave slowly becomes inverted
7°d: ST segment starts returning to base level + T wave inverted + Q wave starts appearing, it deepens. (If ST segment stays elevated >6m, think of development ventricular aneurism)
3°w: Q wave fully developed + T wave starts becoming flat
End of 3m: only Q wave stays the same, ST segm and T wave return to normal. If the size of the infarct was small, Q wave goes back to normal.
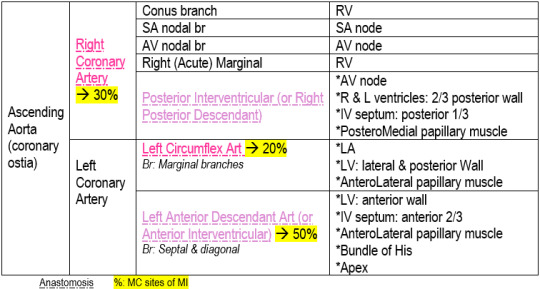
Coronary Arteries, branches & supply:
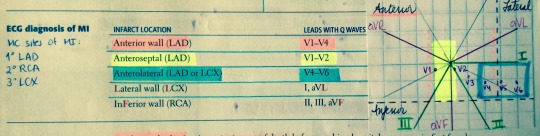
Localization of infarct:
1K notes
·
View notes
Photo

A visual summary of causes of haematuria.
I always learned best by imagining textbook information in visual summaries I could ‘look around’ in my head, rather than writing notes and rehearsing lists.
People would look at me oddly while I daydreamed in the library with a textbook in front of me, creating detailed images where I needed them (in my head), rather than in paper notes.
I’ve spent the last number of years developing as a medical illustrator largely I think so I can try to share the images in my head with others, which have always made more sense than text blocks and bullet point lists.
Does anyone else do this?
1K notes
·
View notes
Text
How To Be A Good Med Student In The Clinical Years
A doctor once told me that the best instrument we have is medicine is the retrospectoscope. Basically he was saying that often it is easier to make sense of things when looking back from the vantage point of the future. This is true of life too. After being an intern for two months I suddenly understand what things make for a strong med students, and what things do not. Unfortunately, I feel like I lacked many of the qualities that would have made me a helpful med student. Though I cannot rectify my own mistakes, perhaps I can pass my advice on to future generations of third and fourth year medical students. I now present, how to be a good clinical med student:
Show up. This seems obvious. When you are there to work, then be there to work. It is so frustrating when medical students are mysteriously absent all the time (only to be found later in the cafe or cafeteria) or when they are there but totally disinterested in what is going on. I understand that sometimes as a medical student things get slow - like when the interns are putting in orders and notes or when there is a slow call day. But at least bring something to read. Don’t play Pokemon Go. Don’t spend all day on Uworld. Make an effort to learn real clinical medicine.
Take initiative to learn. When I was a third year I would wander the hospital to find learning opportunities. I made friends with the telemetry nurses and they started a folder of good tele strips to give me each day. I would go to other teams and see if their patients had good exam findings. I found the cardiology fellows and asked if they had good patients with murmurs. There is so much learning that can happen if you are willing to experience it. Now, referring back to number 1, make sure you always let your residents know where you are. Personally, I would be ecstatic if my students went to hunt down murmurs rather than playing Pokemon Go.
Read your patient’s chart. This can be very helpful and will make you look like a star. Residents are busy taking admissions and sometimes don’t have the time to hunt down records that are three and four years old. You can stand out by doing that Look at a patient’s past hospital notes or their specialty clinic notes. For example, you might be able to alert the resident that an old echocardiogram demonstrated a below normal ejection fraction, which in turn might change how much fluid the patient is given. Or perhaps you found that during a hospitalization in the past the patient became delirious and needed a one-to-one sitter. Find ways to add information in a helpful, non-prescriptive, non-judgmental way. I guarantee your reviews will benefit.
Read about your patient’s condition. Even if you just browse Medscape, UpToDate, or some other curated source, make sure you understand the basics of your patient’s primary diagnosis. If they are there for heart failure, read over the basics of treatment. If they have autoimmune hepatitis look up some info on diagnosis and prognosis. These things will get noticed, especially when you ask intelligent questions on rounds. Do not be like a med student I had who, when asked, reported for 4 straight days that he had not read about his patient’s disease. He instead responded he was too busy with Uworld so he would get a good shelf score.
See your patients. I literally had students who, on rounds, tried to present without actually having seen the patient in the morning. This is a huge no-no. Get to work early enough to see your patients, review their labs, and their overnight events.
Practice your presentations. Even if it is on your own or with other medical students, spend time working on your presentation skills. Heck, even ask the residents to watch you. I would be happy to do that for any of my students. Unfortunately, none have taken me up on that offer and instead bumble through their presentation each day making the same mistakes. By the end of medical school you need to be able to make a good presentation.
Spend time working on note writing. Compare your notes to your residents’, your attendings’, and the specialists’. Everyone has a different style. Look at lots of notes to determine a style for yourself.
Forget all the step 1 stuff you learned. I find many students perseverate on the terrible stereotypes and patterns they see on step 1. Not all black people with cough have sarcoidosis. Not every patient with acute kidney injury needs urine eosinophils. These are good associations, but realize that step 1 has little overlap with real clinical medicine. Take those associations with a grain of salt.
Don’t just look for zebras. I cannot tell you how many times students opt not to follow a patient because the case “doesn’t seem that interesting.” The majority of medicine is made up of mundane and common diseases such as heart failure, pneumonia, COPD, cirrhosis, etc. It is pretty rare to get the exciting cases, like disseminated histoplasmosis or a crazy paraneoplastic syndrome. A lot of learning can happen on cases that are “bread and butter” medicine. Make sure you follow those cases too.
Be gentle to your interns/residents. The transition from 4th year to being a doctor is swift and brutal. It is easy to criticize when you aren’t the one taking 5 admits. Find ways to help your intern/resident, because in return they will help you. I learned this lesson the hard way my 4th year, when I unintentionally threw an intern under the bus while trying to look smart. Afterwards she took me aside and reminded me that she controlled much of my fate while I was a student under her. I learned my lesson and we went on to become very good friends.
The clinical years of medical school are daunting. You constantly feel like a tap dancing monkey, trying to impress people you barely have time to get to know. But personally, I am not looking for someone who knows everything about everything. That’s why you are in school. The best thing you can get out of third and fourth year is how to do a good history and physical, how to write good notes, and how to triage patients. The best students are interested, willing to learn, and know their patients well. If you keep that in mind, the clinical years are much simpler. I promise, if you follow your patients you will learn much more than just doing qbank questions.
Best of luck on your clinical rotations. Don’t make things too complicated. At the end of the day have fun, treat your patients right, and keep an open mind. The learning will happen whether you recognize it or not.
4K notes
·
View notes
Text
How to choose your specialty (not based on medicine)
Family

Pediatrics

OB/Gyn

Internal Medicine

Psychiatry

Surgery

Emergency

Orthopedics

Pathology

Radiology

Neurosurgery

2K notes
·
View notes
Photo

How were you this year? 😏😉#iphonebokeh 📷#torontochristmasmarket #toronto
0 notes
Photo

It's the most wonderful time of the year! 🎄 #Toronto
0 notes
Photo

Missing the days of ☀️and playgrounds 😉 #summer #tbt #siblinglove #justinloveshispowerrangers #toronto
0 notes
Photo

Lunch in NY at #shakeshack ! 🍔 yum! good recommendation @jcho90 😄 #rootbeerfloat #shakeoftheweek #nomnomnom
1 note
·
View note
Photo

I was so excited to try #innoutburger I almost forgot to take a pic! 🍔🍟 It was soo good! #lasvegas #animalstyle #nomnomnom
0 notes
Photo

🚽break, Cell Bio Retreat 📚 #sickkidsresearch #toronto #theoldmill
1 note
·
View note

Photo

🔥&🌌 #sunset #haliburton #cottage
0 notes
Photo

Dins with friends 🍔🍴🍉 #haliburton #cottage
0 notes

Photo

This fella was hanging out on the street today under my mom's van... #hungarianhousepigeon #toronto
0 notes