#BCL2
Text
De novo acute B-cell acute Lymphoblastic Leukemia with BCL2/IGH and BCR/ABL1 rearrangements by Pier Paolo Piccaluga in Journal of Clinical Case Reports Medical Images and Health Sciences

ABSTRACT
T(14;18)(q32,q21) and t(9;22)(q34;q11) translocations, leading to BCL2/IGH and BCR/ABL1 rearrangements, respectively, are common genetic aberrations in hematological malignancies. Particularly, t(14;18)(q32;q21) is the genetic hallmark of follicular lymphoma, while t(9;22)(q34;q11) is commonly rearranged in acute lymphoid leukemia (ALL) and chronic myeloid leukemia. Nevertheless, their association has never been described. We report the first case of acute lymphoid leukemia (ALL) in which both BCL2/IGH and BCR/ABL1 rearrangements were present. The patient presented with pre-B ALL, achieved molecular complete remission with intensified chemotherapy, then reinforced with autologous stem cell transplantation, relapsed after a few months, and unfortunately died 17 months after diagnosis. Of note, only BCL2/IGH but not BCR/ABL1 was detected at relapses.
Key words: B-acute lymphoid leukemia, BCR/ABL1, t(14;18)(q32,q21), BCL2, Philadelphia chromosome, apoptosis, Imatinib, targeted therapy
INTRODUCTION
The t(14;18)(q32;q21) translocation is the most common translocation in B-cell malignancies; in particular, it is found in about 90% of follicular lymphomas, being the chromosomal hallmark of this tumor, and in about 20-25% of diffuse large B-cell lymphomas(1–4). Only a few cases of de novo B-acute lymphoid leukemia (B-ALL) carrying t(14;18)(q32;q21) have been described(5–13). Most of these cases presented with additional chromosomal abnormalities, often involving band 8q24 and/or MYC rearrangement and had a very aggressive clinical course(5,6,8,9,12). Central nervous system (CNS) involvement seems to be a frequent event, despite of adequate prophylaxis. The association between t(14;18)(q32;q21 ) and BCR/ABL1 rearrangement has never been described in ALL. We report on a de novo B-ALL carrying both t(14;18)(q32;q21) with BCL2/IGH fusion and BCR/ABL1 rearrangement.
METHODS
Cytogenetics
Short term cultures from bone marrow samples were performed at diagnosis and during the follow-up. Metaphases were analyzed after G-banding with Wright’stain. Karyotype was described according to the International System for Human Cytogenetic Nomenclature (ISCN 1995)(14–16).
FISH
FISH was performed on fixed cells. Directly labeled BCR and ABL probes (Vysis, Inc), producing a split of red signal when ABL is involved in genetic rearrangements. FISH data were collected with a fluorescence microscope (E 1000, Nikon Instruments) equipped with a CCD camera and Genikon software (Nikon Instruments). Two hundred nuclei/cells were analyzed for each experiment.
Molecular evaluation of BCL2/IGH rearrangement
Molecular evaluation was based on nested PCR(17). Mononuclear cells from BM and PB samples were obtained by Ficoll-Hypaque density gradient centrifugation. Genomic DNA was isolated from mononuclear cells using the QIAamp DNA mini kit (Qiagen, Hilden, Germany)(18). DNA integrity was assessed by amplifying a 510 bp fragment of the Beta-globin gene. Samples positive for Beta-globin were then investigated for the BCL2/IGH rearrangement using a nested PCR specific for MBR and mcr breakpoints. The first round of amplification was done using 1 microg of genomic DNA and the following primers: 5’–CAGCCTTGAAACATTGATGG–3’(forward, for MBR), 5’– CGTGCTGGTACCACTCCTG–3’ (forward, for mcr) and 5’–ACCTGAGGAGACGGTGACC–3’ (reverse, for the JH consensus region). An initial denaturation step of 5 min at 95° C was followed by amplification for 30 cycles (denaturation: 40 sec at 95° C; annealing: 40 sec at 55° C (MBR) or 58°C (mcr); extension: 50 sec at 72° C) and final extension for 7 min at 72° C. Reamplification of a 1 microL aliquot from a 1:50 dilution of the first PCR product was then performed using the internal primers: 5’–ATGGTGGTTTGACCTTTAG–3’ (forward, for MBR), 5’–GGACCTTCCTTGGTGTGTTG–3’ (forward, for mcr), 5’–ACCAGGGTCCCTTGGCCCCA–3’ (reverse, for the JH consensus region), and the following
PCR conditions: initial denaturation step of 5 min at 95° C; amplification for 35 cycles (denaturation: 40 sec at 95° C; annealing: 40 sec at 56° C (MBR) or 59°C (mcr); extension: 50 sec at 72° C); final extension for 7 min at 72° C. All PCR experiments were performed in 50 microL final volume containing 1U of Taq Gold DNA Polymerase (PE Applied Biosystems, San Francisco, USA), 10x PCR buffer, 100 mM of each dNTP, 2.5mM MgCl2, and 1 microM of each primer. Samples were tested twice, and both positive and negative controls were included in all experiments. A patient-specific positive control was also included in every follow-up experiment to compare the BCL2/IGH fragment length with the PCR product obtained at the time of diagnosis. Amplified products were visualized on a 2% agarose gel stained with ethidium bromide. The sensitivity of the assay for the detection of BCL2/IGH rearrangement was routinely =10-4.
Molecular evaluation of BCR/ABL1 rearrangement
RNA extraction was performed by phenol/chloroform using bone marrow mononuclear cells obtained by Ficoll-Hypaque density gradient centrifugation. One microg of total RNA was reverse transcribed using random hexamer primers and MMLV reverse transcriptase; briefly, RNA was prewarmed for 10 min at 70°C and subsequently cooled for a further 10 min at 25°C. The RNA solution was then incubated for 42 min at 45°C in a 20 L reaction mixture containing 10 mM Tris
HCl (pH 8.3), 50 mM KCl, 5.5 mM MgCl2, 1 mM of each deoxyribonucleotide, 20 U of RNAsin
(Pharmacia, Upsala, Sweeden), 25 microM random hexamers (Pharmacia, Upssala, Sweeden), 10 mM of DTT (Pharmacia, Upssala, Sweeden), and 100U of MoMLV reverse transcriptase (BRL, Bethesda, MD). After incubation, cDNA solution was diluted 1:5 to 50 microL final volume. The cDNA integrity was assessed by amplifying a 296 bp fragment of the ABL1 gene. Samples positive for ABL1 were then investigated for the BCR/ABL1 rearrangement by qualitative PCR. Five microLs of cDNA were PCR-amplified using the following set of primers: EA500 5’ TGTGATTATAGCCTAAGACCCGGAG 3’, and R112 5’ TTGTCGTGTCCGAGGCCACC 3’. Thirty-five cycles of PCR were performed as follows: denaturation (30 sec at 96°C), annealing (30 sec at 60°C), and extension (30 sec at 72°C). Samples were tested twice, and both positive and negative controls were included in all experiments.
Amplified products were visualized on a 2% agarose gel stained with ethidium bromide (19).REF
Case report
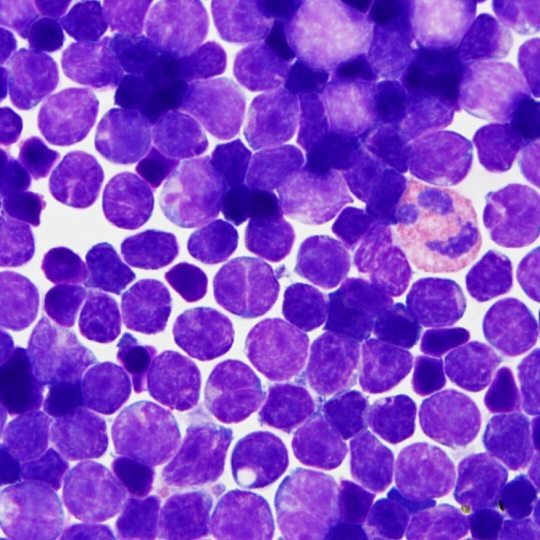
In July 2020, a 40-years-old woman, presenting only with moderate fatigue, was diagnosed with pre-B ALL, L2 subtype. The peripheral blood count showed: Hb 9.3 g/dl; WBC 17x109/L; PLT 56x109/L. The bone marrow aspirate was hypocellular with 80% of lymphoid blasts. The karyotype was: 46,XX, del(6)(8q21q25), t(9;9)(p11;q22), t(14;18)(q32;q21)(10/20). The immuphenotype, assessed by flow cytometry, was: CD19+, CD22+, TdT+, CD20-, CD3-, CD10-.
The molecular analysis carried out by PCR confirmed a BCL2/IGH rearrangement (mcr breakpoint) but also unveiled a BCR/ABL1 (E1-A2 /p190) rearrangement. Thus, FISH analysis was also performed. The probe for BCR/ABL1 dual fusion gene gave two green signals and two red signals as expected from samples not carrying the ABL1 rearrangement. Molecular analysis was then repeated confirming the previous results. We administered a standard induction therapy (doxorubicine, vincristine, L-asparaginase, and prednisone plus imatinib), and an intensified consolidation therapy (idarubicine and high dose cytarabine) obtaining a molecular complete remission (CR). Particularly, neither BCL/IGH nor BCR/ABL1 rearrangements were detected. Other 2 consolidation courses were then administered (BFM-B regimen, including vincristine, ifosfamide, methothrexate, teniposide, high dose cytarabine, and dexamethasone; and BFM-A regimen, including vincristine, doxorubicine, cyclophosphamide, high dose methothrexate, and dexamethasone) associated with imatinib. Bone marrow harvest and autologous bone marrow transplantation were then performed, lacking a HLA-matched donor. Twelve months after the first documentation of CR, the patient relapsed. The bone marrow aspirate was hypercellular with 90% of leukemic cells. The karyotype was: 46 XX, t(1;5)(p32;q31), del(12)(p11;p13)(14/15); the molecular analysis conducted by PCR showed the BCL2/IGH rearrangement, whereas there was no evidence of the BCR/ABL1 fusion transcript. Salvage therapy with liposomal daunorubicin and intermediate dose cytarabine (23) was then administered, obtaining a second molecular CR (disappearance of BCL2/IGH). Two months later, a second relapse occurred. The karyotype was: 46 XX, t(1,5)(p32;q31), del(12)(p11;p13)(29/30). The molecular analysis showed again only the BCL2/IGH rearrangement, without evidence of the BCR/ABL1 fusion gene. Despite of neuro-meningeal prophylaxis, there was clinical evidence of CNS involvement. Compassionate treatment with campath-1H, 30 mg/dose, for 5 doses, was administered i. v., obtaining a peripheral blood blast clearance, but not a CR. The patients eventually died 17 months after diagnosis due to leukemic progression.
DISCUSSION
BCR/ABL1 and BCL2/IGH rearrangements are common molecular abnormalities in B-cell malignancies. In particular, the BCR/ABL1 rearrangement is the most frequent genetic aberration in adult B-ALL(20–22). On the other hand, t(14;18)(q32;q21) with BCL2/IGH rearrangement is the most common abnormality in tumors derived from peripheral B-lymphocytes, whereas it is absolutely rare in B-cell precursor malignancies (24). However, while the biological role of BCR/ABL1 in acute leukemia is at least partially well known(25), the significance of BCL2 in ALL is still largely indefinite. BCL2 overexpression, without BCL2/IGH rearrangement, is frequent in ALL, and does not seem to be associated with a poorer prognosis (26). On the contrary, t(14;18)(q32;q21) and BCL2/IGH rearrangement are a rarity in ALL, but are associated with very aggressive tumors. Morphologically, the described cases are often L3, according to their immunophenotype of mature B-ALL, with Burkitt-like features. Notably, in all cases, complex karyotypes were observed, with almost constant involvement of the 8q24 locus and MYC deregulation(5–13). Sequential emergence of molecular abnormalities has been proposed in these cases, with progression from indolent (BCL2/IGH positive) to aggressive (BCL2/IGH and MYC positive) B-cell tumors (5–13). Therefore, they most likely represented leukemic variants of high-grade B-cell lymphomas with “double hits”. On the clinical ground, most of the patients presented with rapidly worsening general condition, fever, fatigue, night sweat, and weight loss; massive bone marrow and blood involvement, nodal and extra-nodal infiltration were also present. Clinical course was aggressive, with a median overall survival usually below than 12 months(5–13).
To the best of our knowledge, the association between t(14;18)(q32;q21) and BCR/ABL1 rearrangement has not been previously described in ALL. Nevertheless, a case of co-existing
BCR/ABL1 and BCL2/IGH rearrangements was reported in a MDS case(27). Our patient presented with a pre-B ALL, L2 subtype, carrying the t(14;18)(q32;q21) and other additional chromosomal aberrations, such as del(6)(q21;q25) and t(9;9)(p11;p22) but lacking 8q24 involvement; the BCR/ABL1 rearrangement was documented only by molecular analysis. Clinical course was aggressive, with recurrent relapses, CNS involvement, and death within seventeen months. Interestingly, at relapse, the patient presented a different karyotype [t(1,5)(p32;q31), del(12)(p11;p13), quite common as secondary abnormalities], still showing the BCL2/IGH rearrangement. Furthermore, during the clinical history of the patient, other chromosomal aberrations appeared. The relationship between the molecular events, and even a possible sequential appearance cannot be established. No peculiar morphologic or immunophenotipic patterns can be identified, to be easily associated to either one translocation, and the bad prognosis could be conferred by both the main genetic alterations; however, a dominant role of BCL2/IGH should be hypothesized, since it was always present during all disease phases. In this regard, based on the lack of cytogenetic evidence of Philadelphia chromosome we cannot exclude that BCR/ABL1 rearrangement constituted a sub-clonal lesion, cleared out by the more specific targeted therapy (chemotherapy plus imatinib).
Certainly, the treatment of t(14;18)(q32;q21) positive ALL remains a major problem, as conventional therapy are scarcely effective. Probably, the highly proliferating phenotype is made highly insensitive to chemotherapy by the antiapoptotic effect of BCL2, as observed in high-grade B-cell lymphomas with double hits.
The present case, besides its unicity, also confirmed the importance of molecular testing after cytogenetic analysis in human leukemia. Future experiences and hopefully trials will be useful to improve the current treatment of t(14;18)(q32;q21) positive ALL by adopting more rationally targeted therapies such as BCL2 inhibitors (eg venetoclax), peroxisome proliferator-activated receptor-gamma ligands (28), or others.
For more information: https://jmedcasereportsimages.org/about-us/
For more submission : https://jmedcasereportsimages.org/
#B-acute lymphoid leukemia#BCR/ABL1#t(14;18)(q32#q21)#BCL2#Philadelphia chromosome#apoptosis#Imatinib#targeted therapy#Cytogenetic Nomenclature#Genikon#DNA#Pier Paolo Piccaluga#jcrmhs
0 notes

Text
BCL2 Rabbit Polyclonal Antibody
BCL2 Rabbit Polyclonal Antibody
Catalog number: B2017115
Lot number: Batch Dependent
Expiration Date: Batch dependent
Amount: 50 μL
Molecular Weight or Concentration: 26 kDa
Supplied as: Solution
Applications: a molecular tool for various biochemical applications
Storage: -20℃
Keywords: ALS10, TAR DNA binding protein, TAR DNA binding protein 43, TARDBP, TDP 43, TDP43
Grade: Biotechnology grade.…

View On WordPress
0 notes
Text
Victor McKusick, “Mendelian Inheritance in Man”, 1966. Chromosome #19.
Here I present: Victor McKusick, “Mendelian Inheritance in Man”, 1966. Chromosome #19. This print book consists of twelve (12) editions from 1966 to 1998 (shown ABOVE ).
The following abbreviations may used for Chromosome #19 traits, listed in alphabetical order.
Chromosome 19.
AMH APOE ARMD1 BCL2
CD97 CD209 CEACAM1 CF CGB
CRLF1 DBA GPI HPS INSR KLK3
KLK4 LIM2 LHB NAPA NPHS1
PCLD PGPEP1 PIN1…

View On WordPress
0 notes
Text
https://www.delveinsight.com/report-store/bcl2-inhibitors-market-forecast?utm_source=reportstore&utm_medium=promotion&utm_campaign=gpr
BCL-2 inhibitors represent a promising class of anti-cancer therapeutics designed to target B-cell lymphoma-2 (BCL-2) proteins, which play a crucial role in regulating apoptosis or programmed cell death.
#BCL-2 inhibitors#BCL-2 inhibitors market#BCL-2 inhibitors market size#BCL-2 inhibitors epidemiology#BCL-2 inhibitors pipeline#BCL-2 inhibitors symptoms#BCL-2 inhibitors therapies#BCL-2 inhibitors market trends
0 notes
Text
0 notes
Text
Spatial proteomics and transcriptomics of placenta accreta spectrum
In severe Placenta Accreta Spectrum (PAS), trophoblasts gain deep access in the myometrium (placenta increta). This study investigated alterations at the fetal-maternal interface in PAS cases using a systems biology approach consisting of immunohistochemistry, spatial transcriptomics and proteomics. We identified spatial variation in the distribution of CD4+, CD3+ and CD8+ T cells at the maternal interface in placenta increta cases. Spatial transcriptomics identified transcription factors involved in promotion of trophoblast invasion such as AP1 subunits ATF3 and JUN, and NFKB were upregulated in regions with deep myometrial invasion. Pathway analysis of differentially expressed genes demonstrated that degradation of extracellular matrix (ECM) and class 1 MHC protein were increased in increta regions, suggesting local tissue injury and immune suppression. Spatial proteomics demonstrated that increta regions were characterised by excessive trophoblastic proliferation in an immunosuppressive environment. Expression of inhibitors of apoptosis such as BCL2 and fibronectin were increased, while CTLA4 was decreased and increased expression of PDL1, PDL2 and CD14 macrophages. Additionally, CD44, which is a ligand of fibronectin that promotes trophoblast invasion and cell adhesion was also increased in increta regions. We subsequently examined ligand receptor interactions enriched in increta regions, with interactions with ITGB1, including with fibronectin and ADAMS, emerging as central in increta. These ITGB1 ligand interactions are involved in activation of epithelial mesenchymal transition and remodelling of ECM suggesting a more invasive trophoblast phenotype. In PAS, we suggest this is driven by fibronectin via AP1 signalling, likely as a secondary response to myometrial scarring. http://dlvr.it/T4dJDr
0 notes
Text
#cancers, Vol. 16, Pages 389: Galactosylceramide Upregulates the Expression of the BCL2 Gene and Downregulates the Expression of TNFRSF1B and TNFRSF9 Genes, Acting as an Anti-Apoptotic Molecule in Breast #cancer Cells
Galactosylceramide (GalCer) increases the resistance of breast #cancer cells to doxorubicin, paclitaxel, and cisplatin by acting as an anti-apoptotic molecule. GalCer was found to specifically downregulate the levels of the pro-apoptotic TNFRSF1B and TNFRSF9 genes and upregulate the levels of the anti-apoptotic BCL2 gene, suggesting that this glycosphingolipid regulates their expression at the transcriptional level. Consistent with this hypothesis, MDA-MB-231 and MCF7 breast #cancer cells with high levels of GalCer showed lower activity of the TNFRSF1B and TNFRSF9 promoters than cells lacking GalCer. In contrast, the activity of the BCL2 promoter was higher in MCF7 cells overproducing GalCer than in MCF7 cells without GalCer. However, no difference in BCL2 promoter activity was observed between MDA-MB-231 cells with high and no GalCer content. Instead, we found that high levels of GalCer increased the stability of Bcl-2 #mRNA. Subsequent studies showed that breast #cancer cells with high levels of GalCer are characterized by significantly lower expression of P53. Importantly, inhibition of P53 expression by #siRNA in MCF7 and MDA-MB-231 cells lacking GalCer resulted in decreased expression and promoter activity of the TNFRS1B and TNFRSF9 genes. On the other hand, increased expression and promoter activity of the BCL2 gene was found in such MCF7 cells, and increased stability of Bcl-2 transcripts was observed in such MDA-MB-231 cells. Taken together, these data strongly suggest that the regulatory protein that simultaneously increases the expression of the TNFRSF1B and TNFRSF9 genes and decreases the expression of the BCL2 gene and the stability of Bcl-2 transcripts is most likely P53, the expression of which is GalCer dependent. https://www.mdpi.com/2072-6694/16/2/389?utm_source=dlvr.it&utm_medium=tumblr
0 notes
Text
The BCL2 Gene
I am reading about why I have follicular lymphoma. “Bcl-2 (B-cell lymphoma 2), encoded in humans by the BCL2 gene, is the founding member of the Bcl-2 family of regulator proteins that regulate cell death (apoptosis), by either inhibiting (anti-apoptotic) or inducing (pro-apoptotic) apoptosis. Bcl-2 derives its name from B-cell lymphoma 2, as it is the second member of a range of proteins initially described in chromosomal translocations involving chromosomes 14 and 18 in follicular lymphomas.”
0 notes
Text
IHC Lymphomes
Marqueurs T : CD3, CD5 + CD2, CD7
CD43 : pan-T, même quand tout est perdu
Marqueurs B : CD20, CD79a
Suspicion de Hodgkin : CD30, CD15, CD45 + EBV LMP
Marqueurs plasmocytaires : CD79a, CD138, MUM1
Blastes : CD34, CD117
Nids prolifératifs : c-myc, cycline D1, Ki67
Ki67
Lymphomes B :
Algorithme de Hans : CD10, BCL6, MUM1 (seuil 30%)
Panel B petites cellules : CD20, CD3, CD5, CD10, CD23, BCL2, BCL6, Ki67, cycline D1
Grandes cellules : + AE1/AE3
double expresseur : BCL2, c-myc (seuil 40%)
CD5+ /CD3+ : trou phénotypique ? CD2, CD5, CD7, CD4, CD8
VIH : HHV8, EBV-LMP
âgé ou greffé : EBV-LMP
Lymphome T LAI :
CD20, Ki67, CD30
Panel T : CD3, CD4, CD5, CD7, CD8
Phénotype TFH : ICOS (CD278), BCL6, CD10, CXCL13
Follicules : CD21, CD23
EBV EBER (HIS), clone T, clone B
0 notes
Text
Dead cells platforms

Until now, there is no database that comprehensively characterizes and annotates 12 cell death modes and their crosstalk.Ĭell death displays distinct morphological features by activating signalling pathways. “NcRDEATHDB” presents non-coding RNA mediated cell death and lncRNA mediated cell death interaction with protein–protein interaction networks in apoptosis, autophagy, and necrosis as an updated version of ncRDeathDB. “Autophagy Regulatory Network” explores only autophagic protein interactions while “BCL2DB” presents BCL-2 family members and BH3 only proteins. “MEROPS”, “CASBAH”, “CASPDB”, “MerCASBA” and “CaspNeuroD” mostly focus on active caspases and their N terminus. Database “Apoptoproteomics”, “Deathbase”, “ApoCanD”, “Degrabase” present quantitative data of relevant pathway proteins for apoptosis cell death mode. Ten databases related to human cell death have already been constructed. Current cell death databases often only outline molecular function in three basic modes of cell death : apoptosis, autophagy, and necrosis. The Nomenclature Committee on Cell Death (NCCC) classified twelve cell death modes based on biochemical and cellular characteristics, which are autophagy, autosis, necroptosis, efferocytosis, ferroptosis, immunogenic cell death, intrinsic apoptosis, lysozomal cell death, mitotic cell death, mitochondria permeability transition cell death, parthanatos, and pyroptosis.įor a long time, distinct modes of cell death were studied in isolation, so the prevailing cell death database suggested that they represented mutually exclusive cellular states, and none of them report the crosstalk (associations) of cell death modes. A growing number of novel forms of cell death have been identified as the so-called ‘Valley of Death’. Recently, new cell death modes in cell biology, such as efferocytosis, mitochondria, and parthanatos etc. Necrotic cell death is characterized by the rapid loss of plasma membrane integrity. Autophagy is defined as a catabolic process in which parts of the cytosol and specific organelles are engulfed by a double-membrane structure, known as auto-phagosomes, and eventually degraded. Apoptosis is triggered when cell-surface death receptors, such as Fas is bound by their ligands (the extrinsic pathway) or when Bcl2-family pro-apoptotic proteins cause the permeabilization of the mitochondrial outer membrane (the intrinsic pathway). The three fundamental types of programmed cell death are apoptosis (type I cell death), autophagic (type II), and necrosis (type III). Abnormalities of cell death programs contribute to several important diseases such as cancer, Alzheimer’s disease, autoimmune diseases, and chronic inflammation, where tissues or organs progressively deteriorate over time. Ĭell death is an essential biological process for physiological growth and is used during developmental stages when tissues begin to form and shape. These potential druggable targets are displayed systematically and tailoring networks to visualize specified relations is available to fulfil user-specific needs. 147 hallmark genes of cell death could be observed in detail in these networks. A multilayer spectral graph clustering method that performs convex layer aggregation to identify crosstalk function among cell death modes for a specific cancer. With this platform, users can search specific interactions from vast interdependent networks that occur in the realm of cell death. An interactive webtool, XDeathDB, is built by web applications with R-Shiny, JavaScript (JS) and Shiny Server Iso. Big data for cell death gene-disease associations, gene-cell death pathway associations, pathway-cell death mode associations, and cell death-cell death associations is collected by literature review articles and public database from iRefIndex, STRING, BioGRID, Reactom, Pathway’s commons, DisGeNET, DrugBank, and Therapeutic Target Database (TTD). Apoptosis, autosis, efferocytosis, ferroptosis, immunogenic cell death, intrinsic apoptosis, lysosomal cell death, mitotic cell death, mitochondrial permeability transition, necroptosis, parthanatos, and pyroptosis related to 12 cell deaths and their crosstalk can be observed systematically by the platform. The XDeathDB visualization platform provides a comprehensive cell death and their crosstalk resource for deciphering the signaling network organization of interactions among different cell death modes associated with 1461 cancer types and COVID-19, with an aim to understand the molecular mechanisms of physiological cell death in disease and facilitate systems-oriented novel drug discovery in inducing cell deaths properly. Lots of cell death initiator and effector molecules, signalling pathways and subcellular sites have been identified as key mediators in both cell death processes in cancer.
0 notes
Text
Bcl-2 Human Recombinant
Bcl-2 Human Recombinant
Catalog number: B2016832
Lot number: Batch Dependent
Expiration Date: Batch dependent
Amount: 50 µg
Molecular Weight or Concentration: 24.7 kDa
Supplied as: Powder
Applications: a molecular tool for various biochemical applications
Storage: -80°C
Keywords: BCL2
Grade: Biotechnology grade. All products are highly pure. All solutions are made with Type I ultrapure water…

View On WordPress
0 notes
Quote
Kalo lagi gini berharap banget punya kenalan atau temen deket dari bidang kedokteran buat diskusi masalah ini. 😭 need advices.
Balada Tugas Akhir
17 Juli 2017
1 note
·
View note
Link
The folds of the two Bcl-2 iso forms, Isoform 1 and Isoform 2, are similar. However, differences in the ability of these isoforms to bind to the BAD and BAK proteins, as well as differences in the structural topology and electrostatic potential of the binding groove, suggest that the two isoforms have different antiapoptotic activities.
0 notes
Photo
From • @pathnuggets Cytospin preparation of follicular lymphoma. Here we can see many small cleaved lymphocytes consistent with centrocytes. Follicular lymphoma is composed CD10 positive B cells from the germinal center. IgH/BCL2 rearrangement is found in about 90% of cases. By Immunohistochemsitry the B cells will also express BCL2 and BCL6. LMO2 is another marker for follicle center. Ki67 proliferation index is useful and helpful with grading. Cases are graded by the number of centroblasts per high power field on histology sections. #pathnuggets #pathologynuggets #pathology #pathologyeducation #heme #hemepath #cytology https://www.instagram.com/p/CfyRiRRjYiXNfvJ9gO49nYyqSZ4WwI_oN5nkgA0/?igshid=NGJjMDIxMWI=
2 notes
·
View notes
Note
for the obscure asks: 8, 24, 34 :)
Thank you for the ask! ❤️🥺 8 and 24 were already asked so I’m copying the answers here! <3
8. what color do you think goes best with your personality?
Honestly, shades of red are totally me. Somewhere on the maroon spectrum xD
Besides the fact that there’s virtually no doubt about my love for deeper reds, I love the varied symbolism of it. Love, passion, vibrancy, blood, seduction, fear, energy, strength, power...so many things. And the fact that it’s both cautious and an almost “stubborn” color doesn’t hurt, because that’s 100% me xD
24. what is your favorite thing to learn about?
Oh literally everything. I’m not even kidding, I am exactly like Evan Buckley when it comes to research rabbit holes. The second something interests me, I’m on it.
Right now, it’s more history all the time because of things going on in the world and I like to keep myself educated and growing. But I do love learning about diseases too (my paper’s on the BCL2 gene and ovarian cancer, so I have 20 tabs open for that xD). The stuff is so interesting and our bodies are amazing. You will not believe the amount of mechanisms we have to protect us.
I actually really enjoy law, now that I think about it. Not in the “I’m gonna make this my profession” way, but in the “I like to be informed about loopholes and contracts and legal stuff” way. My MCD fic is giving me the space to research family law right now, so that’s always fun.
34. what food do you binge on when you’re lazy?
I live in a dorm right now, so pretty much all my food comes from the dining hall or I order it. If I don’t want to walk to the dining hall or if I want to avoid the inevitable non-halal food issue(s), I usually order Indian takeout.
If I can though, I try to order from this one halal Thai place near me, because I love their red curry and jasmine rice so much! It just doesn’t appear in my delivery app all that often anymore xD
I miss my kitchen though, and I very much miss cooking fresh food. I mean, I have it pretty good and there isn’t anything I can justify complaining about but...yeah xD
Send me obscure asks! <3
1 note
·
View note
Last Seen Blogs

thesagedahlia
thesagedahlia

jutetower8-blog
New York City Finds

skittybot
mya! *slap* mya! *slap* mya! *slap* mya! *slap* m

subhaaash-blog
Subhaaash
centralwashingtonlife
Untitled