#PCN allergy
Text
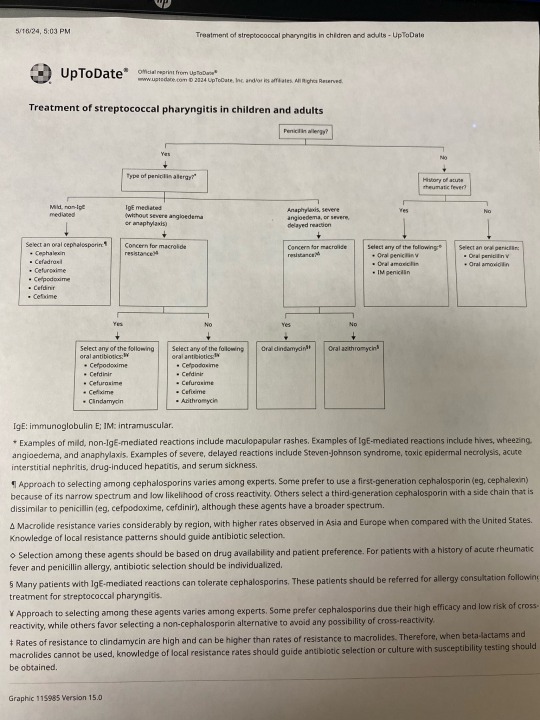
Have a pt who gets a severe rash in response to amoxicillin. She probably has strep throat. Sending azithromycin instead.
3 notes
·
View notes
Text
Nothing in my day-to-day job shows me the limits of modern medicine like vancomycin does. And it makes me insane.
(extremely long, somewhat incoherent nerd rant below the cut)
See, vanc is really good at, like, three things: treating MRSA (when given IV), treating ampicillin-resistant enterococcus (when given IV), and treating c diff (when administered orally ONLY). Most every use outside of that, like when it’s used to treat methicillin-susceptible staph aureus for “penicillin allergic patients” (don’t get me started on PCN allergies), actually has data that it increases risk of morbidity and mortality (i.e. harm and DEATH).
Unfortunately, due to the prevalence of multi-drug resistant organisms, vancomycin is empiric therapy for a lot of presumed infections. And it's a lot more difficult to actually tell if someone has an infection than you'd think. A lot of medical conditions imitate each other and when time is of the essence to identify what's going on, the most ethical thing is to start an antibiotic and rule out infection as the hospitalization continues. Lab techniques have gotten a lot quicker: I can remember 8 years ago, it would take 3 days just to identify what microbe the patient had in their presumed infection. These days, anno domini 2023, PCR comes back in a matter of hours, identifying gram positive/gram negative staph/strep/bacilli/etc, and it's the sensitivities that take 2-3 days. (Don't get me started on contaminated cultures.) But even with improvements in lab technique, we might not culture any microbe at all or the provider might keep vancomycin on "just in case" because we don't know IF the patient is infected, WHAT they're infected with, or if the infection will get better with a different drug.
And vancomycin is terrible on kidneys. Extremely nephrotoxic. It isn’t as bad as the 80s when the drug first came out and was called Mississippi Mud colloquially, but it will fuck the patient up if not monitored closely.
But finding the correct dose for each patient in a timely manner is nigh impossible. This is because vancomycin is renally eliminated. We have to mathematically estimate how well the kidneys are working. Unfortunately, our mathematic equation is next to useless if you are:
-Less than 50 kg
-Shorter than 5 foot tall
-Have a BMI of more than 40
-Are an adult younger than 45 (twenty-year-olds get astronomical doses that would be destructive in an older patient)
-Are older than 65 (the official definition of 'geriatric', i'm relatively sure)
-Are female (this is really only applicable if the patient is less than 50 kg or older than 65 - think: little old frail lady - we have absolutely no fucking idea how their kidneys are doing until we order the serum drug level. It is next to impossible to accurately dose vancomycin in little old ladies on the first try.)
-Are missing limbs (lots of leg amputations in the older and impoverished diabetic population!!)
-Have a lot of muscle mass (think bodybuilder or really tall guys)
Fun fact: we estimate renal function by looking at height, weight, age, birth gender (few, if any, studies on trans patients taking HRT), and a lab value called serum creatinine. Creatinine is a byproduct of muscle metabolism, I don't know the fine details, but we can generally estimate how well kidneys are working by seeing how much creatinine is in the blood: low creatinine usually means kidneys are excreting it as they 'should' be. High creatinine means there's something wrong, the kidneys aren't able to excrete it as efficiently as they 'should' be. But the effect of low muscle mass and high muscle mass haven't been studied enough to be able to adjust our mathematical equation to compensate for them. And with high BMI: we often overestimate their renal function because we don't know how to estimate their muscle mass vs their body fat.
(I work out in the boonies. ~70% of our patients have diabetes. ~80% of our patients have a BMI of greater than 35. So what I'm trying to say here is: we are shooting in the fucking dark when we're estimating the renal function of the vast majority of our patients.)
Complicating this: vancomycin is useless until it reaches steady-state concentration in therapeutic range. On one side of this problem: a lot, if not most, medical providers assume that vancomycin starts working its magic from the first dose. So we sometimes get orders for "vancomycin 1 gram now and see how the patient is doing in the morning". That isn't going to solve jack shit! That's just going to increase the incidence of microbial resistance!!
OR, like in the multiple situations I dealt with this afternoon, you make an educated guess on what regimen is going to work for the patient. You get a level 48 hours after the dose starts. And you find out that you fucking guessed wrong and the patient is subtherapeutic. It has been two fucking days and the patient hasn't started being treated for their (presumed) infection yet!! And we've increased the possibility of microbial resistance! *muffled screaming in frustration*
So what I'm trying to say here is: on almost every presumed infection that comes into the hospital (which we're guessing like 30%? 50%? of the time), we're starting an extremely toxic drug, oftentimes 100% guessing what regimen will be therapeutic, only finding out in 2 days that it is not therapeutic, and it can sometimes take days and days to titrate the dose sufficiently to find a therapeutic regimen. And sometimes we're really fucking unlucky and we destroy the patient's kidneys temporarily (or permanently! but kidneys can be very resilient so that's thankfully rare) because we guessed a regimen that's too high!! This is a fucking nightmare!!!!!!!!
And if all of this wasn't bad enough, we don't really have any drugs that do what vancomycin does therapeutically. We have things that can be used to cover some of what vancomycin does, but nothing that's equivalent AND less toxic.
Like, to fix this situation, we need:
-Better education to providers on what drugs are appropriate empiric therapy for different presumed infections (we're working on it, we are working on it)
-Better ways to estimate kidney function (there needs to be more research on kidney function in patients with BMI greater than 35!! And little old ladies!! And patients with low body weight and high body weight and amputations and...)
-Better prognostic tools to tell 1. when the patient is infected (looking at you, sepsis!!!) 2. what they're infected with
-Less-toxic antibiotics AND/OR better ways to treat infection (this would be the evolution of medicine as we know it)
And I want to be clear: vancomycin isn't bad. It's an extremely effective tool when used correctly but we often either don't have enough data to use it correctly or the provider doesn't understand that this tool is fucking useless for the job they're trying to perform.
#some days i'm just smacked in the face by the limits of modern medicine#there is so much we don't know!!!#we're doing the best we can!!!#negativity#personal#us healthcare#i understand other hospitals will have a different experience than this#but my corporation is extremely stingy and we get all the new grads#so educating providers and nurses is a never-ending wheel at my facility#and we don't treat anything complicated except orthopedic surgeries#some days I just get overwhelmed by how little we know#if you can guess my profession on the first try please keep it to yourself i'm trying to maintain a low profile here okay#also if you ask me medical questions don't expect an answer#i was a Cs Get Degrees student all I know i've learned on the job and I don't know shit
6 notes
·
View notes
Text
Medical Abbreviations on Pharmacy Prescriptions
Here are some common medical abbreviations you may see on pharmacy prescriptions:
qd - once a day
bid - twice a day
tid - three times a day
qid - four times a day
qh - every hour
prn - as needed
pc - after meals
ac - before meals
hs - at bedtime
po - by mouth
IV - intravenous
IM - intramuscular
subQ - subcutaneous
mL - milliliter
mg - milligram
g - gram
mcg - microgram
stat - immediately, right away
NPO - nothing by mouth
cap - capsule
tab - tablet
susp - suspension
sol - solution
amp - ampule
inj - injection
Rx - prescription
C - Celsius
F - Fahrenheit
BP - blood pressure
HR - heart rate
RR - respiratory rate
WBC - white blood cell
RBC - red blood cell
Hgb - hemoglobin
Hct - hematocrit
PT - prothrombin time
INR - international normalized ratio
BUN - blood urea nitrogen
Cr - creatinine
Ca - calcium
K - potassium
Na - sodium
Cl - chloride
Mg - magnesium
PO2 - partial pressure of oxygen
PCO2 - partial pressure of carbon dioxide
ABG - arterial blood gas
CBC - complete blood count
BMP - basic metabolic panel
CMP - comprehensive metabolic panel.
ECG - electrocardiogram
EEG - electroencephalogram
MRI - magnetic resonance imaging
CT - computed tomography
PET - positron emission tomography
CXR - chest x-ray
CTX - chemotherapy
NSAID - nonsteroidal anti-inflammatory drug
DMARD - disease-modifying antirheumatic drug
ACE - angiotensin-converting enzyme
ARB - angiotensin receptor blocker
SSRI - selective serotonin reuptake inhibitor
TCA - tricyclic antidepressant
ADHD - attention deficit hyperactivity disorder
COPD - chronic obstructive pulmonary disease
CAD - coronary artery disease
CHF - congestive heart failure
DVT - deep vein thrombosis
GI - gastrointestinal
UTI - urinary tract infection
OTC - over-the-counter
Rx - prescription
OD - right eye
OS - left eye
OU - both eyes.
TID - thrombosis in dementia
TDS - ter die sumendum (three times a day)
BOM - bilaterally otitis media (infection in both ears)
BT - body temperature
C&S - culture and sensitivity
D/C - discontinue or discharge
D/W - dextrose in water
ETOH - ethyl alcohol
FUO - fever of unknown origin
H&P - history and physical examination
I&D - incision and drainage
I&O - intake and output
KVO - keep vein open
N&V - nausea and vomiting
PERRLA - pupils equal, round, reactive to light and accommodation
PR - per rectum
QAM - every morning
QHS - every bedtime
QOD - every other day
S/P - status post (after)
TPN - total parenteral nutrition
UA - urinalysis
URI - upper respiratory infection
UTI - urinary tract infection
VO - verbal order.
XRT - radiation therapy
YOB - year of birth
BRBPR - bright red blood per rectum
CX - cervix
DVT - deep vein thrombosis
GB - gallbladder
GU - genitourinary
HCV - hepatitis C virus
HPI - history of present illness
ICP - intracranial pressure
IVP - intravenous pyelogram
LMP - last menstrual period
MRSA - methicillin-resistant Staphylococcus aureus
MVA - motor vehicle accident
NKA - no known allergies
PEG - percutaneous endoscopic gastrostomy
PRN - pro re nata (as needed)
ROS - review of systems
SOB - shortness of breath
TAH - total abdominal hysterectomy.
TIA - transient ischemic attack
Tx - treatment
UC - ulcerative colitis
URI - upper respiratory infection
VSD - ventricular septal defect
VTE - venous thromboembolism
XR - x-ray
w/c - wheelchair
XRT - radiation therapy
ASD - atrial septal defect
Bx - biopsy
CAD - coronary artery disease
CKD - chronic kidney disease
CPAP - continuous positive airway pressure
DKA - diabetic ketoacidosis
DNR - do not resuscitate
ED - emergency department
ESRD - end-stage renal disease
FFP - fresh frozen plasma
FSH - follicle-stimulating hormone.
GCS - Glasgow Coma Scale
Hct - hematocrit
Hgb - hemoglobin
ICU - intensive care unit
IV - intravenous
JVD - jugular venous distension
K - potassium
L - liter
MCH - mean corpuscular hemoglobin
MI - myocardial infarction
Na - sodium
NGT - nasogastric tube
NPO - nothing by mouth
OR - operating room
PCN - penicillin
PRBC - packed red blood cells
PTT - partial thromboplastin time
RBC - red blood cells
RT - respiratory therapy
SOA - short of air.
SCD - sequential compression device
SIRS - systemic inflammatory response syndrome
STAT - immediately
T - temperature
TPN - total parenteral nutrition
WBC - white blood cells
ABG - arterial blood gas
A fib - atrial fibrillation
BPH - benign prostatic hypertrophy
CBC - complete blood count
CO2 - carbon dioxide
COPD - chronic obstructive pulmonary disease
CPR - cardiopulmonary resuscitation
CT - computed tomography
CXR - chest x-ray
D5W - dextrose 5% in water
Dx - diagnosis
ECG or EKG - electrocardiogram
EEG - electroencephalogram
ETO - early termination of pregnancy.
FHR - fetal heart rate
GSW - gunshot wound
H&P - history and physical exam
HCG - human chorionic gonadotropin
I&D - incision and drainage
IBS - irritable bowel syndrome
ICP - intracranial pressure
IM - intramuscular
INR - international normalized ratio
IOP - intraocular pressure
LFT - liver function test
LOC - level of consciousness
LP - lumbar puncture
NG - nasogastric
OA - osteoarthritis
OCD - obsessive-compulsive disorder
OTC - over-the-counter
P - pulse
PCA - patient-controlled analgesia
PERRLA - pupils equal, round, reactive to light and accommodation.
PFT - pulmonary function test
PICC - peripherally inserted central catheter
PO - by mouth
PRN - as needed
PT - physical therapy
PT - prothrombin time
PTSD - post-traumatic stress disorder
PVC - premature ventricular contraction
QD - once a day
QID - four times a day
RA - rheumatoid arthritis
RICE - rest, ice, compression, elevation
RSI - rapid sequence intubation
RSV - respiratory syncytial virus
SBP - systolic blood pressure
SLE - systemic lupus erythematosus
SSRI - selective serotonin reuptake inhibitor
STAT - immediately
TB - tuberculosis
TIA - transient ischemic attack.
TID - three times a day
TKO - to keep open
TNTC - too numerous to count
TPN - total parenteral nutrition
URI - upper respiratory infection
UTI - urinary tract infection
V-fib - ventricular fibrillation
V-tach - ventricular tachycardia
VA - visual acuity
WNL - within normal limits
AED - automated external defibrillator
ARDS - acute respiratory distress syndrome
BID - twice a day
BP - blood pressure
BUN - blood urea nitrogen
CAD - coronary artery disease
CHF - congestive heart failure
CVA - cerebrovascular accident
D/C - discontinue
DKA - diabetic ketoacidosis.
DM - diabetes mellitus
DVT - deep vein thrombosis
EGD - esophagogastroduodenoscopy
ER - emergency room
F - Fahrenheit
Fx - fracture
GI - gastrointestinal
GTT - glucose tolerance test
HCT - hematocrit
Hgb - hemoglobin
HRT - hormone replacement therapy
ICP - intracranial pressure
IDDM - insulin-dependent diabetes mellitus
IBS - irritable bowel syndrome
IM - intramuscular
IV - intravenous
K - potassium
KVO - keep vein open
L&D - labor and delivery
LASIK - laser-assisted in situ keratomileusis.
ROM - range of motion
RT - radiation therapy
Rx - prescription
SCD - sequential compression device
SOB - shortness of breath
STD - sexually transmitted disease
TENS - transcutaneous electrical nerve stimulation
TIA - transient ischemic attack
TSH - thyroid-stimulating hormone
UA - urinalysis
US - ultrasound
UTI - urinary tract infection
VD - venereal disease
VF - ventricular fibrillation
VT - ventricular tachycardia
WBC - white blood cell
XRT - radiation therapy
XR - x-ray
Zn - zinc
Z-pak - azithromycin (antibiotic).
AAA - abdominal aortic aneurysm
ABG - arterial blood gas
ACS - acute coronary syndrome
ADL - activities of daily living
AED - automated external defibrillator
AIDS - acquired immunodeficiency syndrome
ALS - amyotrophic lateral sclerosis
AMA - against medical advice
AML - acute myeloid leukemia
APAP - acetaminophen
ARDS - acute respiratory distress syndrome
ASCVD - atherosclerotic cardiovascular disease
BPH - benign prostatic hyperplasia
BUN - blood urea nitrogen
CABG - coronary artery bypass graft
CBC - complete blood count
CHF - congestive heart failure
COPD - chronic obstructive pulmonary disease
CPAP - continuous positive airway pressure
CRF - chronic renal failure.
CT - computed tomography
CVA - cerebrovascular accident
D&C - dilation and curettage
DVT - deep vein thrombosis
ECG/EKG - electrocardiogram
EEG - electroencephalogram
ESRD - end-stage renal disease
FSH - follicle-stimulating hormone
GERD - gastroesophageal reflux disease
GFR - glomerular filtration rate
HbA1c - glycated hemoglobin
Hct - hematocrit
HIV - human immunodeficiency virus
HPV - human papillomavirus
HTN - hypertension
IBD - inflammatory bowel disease
IBS - irritable bowel syndrome
ICU - intensive care unit
IDDM - insulin-dependent diabetes mellitus
IM - intramuscular.
IV - intravenous
LFT - liver function test
MI - myocardial infarction
MRI - magnetic resonance imaging
MS - multiple sclerosis
NPO - nothing by mouth
NS - normal saline
OCD - obsessive-compulsive disorder
OSA - obstructive sleep apnea
PCOS - polycystic ovary syndrome
PMS - premenstrual syndrome
PPD - purified protein derivative
PSA - prostate-specific antigen
PT - prothrombin time
PTT - partial thromboplastin time
RA - rheumatoid arthritis
RBC - red blood cell
RSV - respiratory syncytial virus
SLE - systemic lupus erythematosus
TB - tuberculosis.
It is important to remember that medical abbreviations can vary based on location and specialty.
Healthcare professionals should use medical abbreviations with caution and only when they are familiar with their meanings.
Patients should always communicate any questions or concerns they have about their medications or medical care to their healthcare provider or pharmacist to ensure they receive safe and accurate medical care.

9 notes
·
View notes
Text
how does one even leave their consciousness at someone's front door step? well who am I to question our queen Willow anyway tbh
100 days of productivity
day 40 + 41
CVS/RS
20-25% of presenting PEs do NOT have an associated DVT
no impact of steroids on silicotic lungs
isocyanates → NSCLC
ILO categories of profusion of small opacities in pneumoconioses (esp CWP/silicosis): cat 0 = no small opacities, cat 1 = few opacities, cat 2 = many opacities but normal lung markings visible, cat 3 = normal lung markings virtually absent (can choose two adjacent categories to assign if it's felt to be borderline, can choose the same category twice)
CNS/Ophthal/Psych
Bowlby-Parkes stages of grief: numbness, pining, disorganisation & disrepair, reorganisation & recovery
progressive brainstem symptoms not explained by a single localisation → vertebral artery disease (?dissection, especially if h/o chiropractor or unsupervised yoga)
chronic small subdural haematoma from 2 weeks ago with no focal deficits or AMS - no need to evacuate
on the same track, if neurological decline is slow, then you can pretty much rule out epidural bleed
meningitis w/ PCN + cephalosporin allergy: USA vanc + moxifloxacin ± cotrimoxazole (OR) UK chloramphenicol ± cotrimoxazole (OR) meropenem monotherapy (mero covers Listeria!); all these regimens are acceptable here
Parkinson-like symptoms but LL rigidity > UL rigidity ± falls: this is ischaemic, NOT neurodegenerative! falls occur *late* in parkinsonian illness, not early
severe dementia (MMSE <10) is a contraindication for anticholinesterases; only memantine is approved for MMSE <10
Endocrine/Repro
insulin resistance → excess insulin production → defective/dystrophic lipogenesis → ectopic fat pockets → release of inflammatory mediators from fat pockets → upregulation of plasminogen activator inhibitor 1 (PAI-1) → inhibition of tPA → procoagulant state
X-linked vs AR adrenoleukodystrophy: AR (Zellweger's) presents in infancy, is rapidly progressive and kills in adolescence; X-linked presents in adolescence and is far more indolent and survivable
rapid improvement in blood glucose is actually assoc w/ acute worsening of microvasculopathy (esp retinopathy); long term improvement in blood glucose is ofc assoc w/ bettering of microvascular dz
Rheum/Derm/Immuno
anti-ribosomal P Abs are specific for lupus encephalitis
hyaline cartilage (carTWOlage = type 2 collagen) is avascular and gets nutrition from synovial fluid diffusion
response to osteoporosis therapy → procollagen-1 propeptides (PICP, PINP, osteocalcin) (bone formation markers)
colloid plasma expanders, like opioids, directly act on mast cells to secrete histamine
GIT
generally, anti-TNFs are only used in IBD that is active despite use of 5-ASA + thiopurine + MTX; the exception is fistulous Crohn's, when anti-TNFs are started ASAP
King's College criteria for APAP-induced ALF for txp referrak: I ACHE (INR >6.5, Acidosis w/ pH <7.3, Creat >3.5 mg/dl, Hepatic Encephalopathy grade 3)
CT is scan of choice for acute pancreatitis; CT is usable in chronic panc but MRI (MRCP) is ideal
80-90% of pancreatic cancers are assoc w/ KRAS2+; only 50% are assoc w/ p53-
by the way! faecal elastase/trypsin is the best measure of chronic pancreatitis, w/ elastase <200 mcg/g being diagnostic
in hepatorenal syndrome, terlipressin causes splanchnic vasoconstriction and reduces splanchnic volume, as well as reducing afferent arteriole pressure and thence renin secretion
SIBO vs short bowel syndrome: SIBO causes not just diarrhoea but also bloating and abdominal discomfort but not marked fat malabsorption and definitely not oxaluria/oxalate stones; both cause folate/B12 deficiency, dehydration, electrolyte disturbances
Onc/Haem
slight increase in PT/aPTT or slight drop in platelets will NOT explain large scale ecchymotic bleeds; in such a patient who is also taking aspirin, blame aspirin
generally, B-cell lymphomas are more common than T-cell lymphomas
that said: Sézary is a form of advanced, more virulent mycosis fungoides (MF: patches of erythema, SS: widespread erythroderma ± keratoderma as well as leukaemic infiltration of marrow)
ID
MTB doubles in 1 day; T. pallidum doubles in 2 days; M. leprae doubles in 2 *weeks*
Pharm/Toxo
cranberry juice is not as bad a culprit as grapefruit is, but it also has some pretty significant interactions (especially 2C9 which metabolises eswarfarin, the active enantiomer of warfarin; expect INR to skyrocket)
100 mg desferoxamine chelates 8 mg iron
11 notes
·
View notes
Text
Most advanced pcn testing available at Advanced Allergy, Asthma, & Immunology Center
0 notes
Text
The Role Of Heath Care Practitioners In Various Medical Fields
A medical services professional is one having the power or permit to give corrective or preventive medical care administrations to people or networks in a coordinated and purposeful GP practice pharmacist in the field of medication, obstetrics, drug store, nursing, pediatrics, clinical brain science or other related areas. The nature of administration given by medical services specialists is completely observed by the state experts based on pre-fixed standards and guidelines. The state has the privilege to pass judgment on the activities of the medical care suppliers, and hold onto their permit on the off chance that they are found to disregard any of the standards. In such conditions, it is the obligation of the state to give the Board of Medical Examiners the name and the activity subtleties of the concerned medical services supplier for the execution of vital activities.
Allow us to see the different sorts of medical care suppliers accessible:
Essential Care Providers (PCP): The individual you make your first visit to for an overall wellbeing examination is characterized as your essential consideration supplier. You can settle on the best PCP for you based on your medical issues and the medical care plan you have. Allow us to talk about a portion of the potential choices:
By and large, an overall doctor can be the best PCP, who can investigate your medical conditions and allude you to the most suitable trained professional. An overall doctor alludes to a specialist of medication or osteopathy with a specialization in inside medication and family practice.
You can likewise pick an Obstetrician and Gynecologist has a specialization in ladies' wellbeing and pre-birth care as your PCP.
For routine exams and general medical problems, you can designate attendant professionals with advanced educations as your PCP. They are approved to give essential consideration in the field of pediatrics, family medication, ladies' wellbeing, grown-up care and so on
Nursing Care: The nursing area can be partitioned in different classes.
Authorized Practical Nurse (LPN): LPNs allude to prepared medical caretakers having the permit to give wellbeing insurance administrations to people, families or networks.
Enlisted Nurse (RN): RNs are needed to get past a state board assessment and achieve an advanced education from a nursing program to get the permit for giving wellbeing security administrations.
Progressed Practice Registered Nurse (APRN): APRNs are better than general medical caretakers attributable to their high level preparation phases and extraordinary degrees. APRNs incorporate guaranteed enrolled nurture anesthetists, nurture professionals, clinical medical caretaker subject matter experts and authorized attendant birthing specialists.
Psychological well-being Practitioners: An emotional well-being professional alludes to a wellbeing security supplier who is known to offer preventive or corrective administrations to treat psychological circumstances in people. Emotional well-being experts incorporate clinical clinicians, specialists, clinical social laborers, marriage and family advisors and so forth
Drug specialists: Having an advanced education from drug schools, authorized drug specialists offer types of assistance in the field of wellbeing insurance by getting ready medications that are recommended by essential or specialty care suppliers.
Specialty Care Providers: Specialty care suppliers are medical care experts, who give wellbeing assurance administrations in different specific fields like Cardiology, Dermatology, Gastroenterology, Orthopedics, Nephrology, Allergy and Asthma and some more.
For More Info, Visit Us:
clinical pharmacist
Primary Care pharmacist
PCN Pharmacist
0 notes
Text
Provide a rationale for each question you ask by explaining why it is appropriate and how it aligns to the chief complaint.
Provide a rationale for each question you ask by explaining why it is appropriate and how it aligns to the chief complaint.
B.P. Scenario Short Stature, 7-year-old male • Name: B.P. • Date: 15 July 2011 • DOB: 01 January 2004 • Gender: Male • Age: 7 years 6 months CC: Well visit today with parental concern about short stature Ht: 48” Wt: 48 lb Resp.: 18 Temp. 98 F HR: 74 Allergies: PCN Here with parents. Parental concerns about B. being the shortest child in class. They are concerned about his height. Denies any PMH…
View On WordPress
0 notes
Text
[QUESTION SOLVED] B.P. Scenario Short Stature, 7-year-old male • Name: B.P. • Date: 15 July 2011 •
[QUESTION SOLVED] B.P. Scenario Short Stature, 7-year-old male • Name: B.P. • Date: 15 July 2011 •
B.P. Scenario Short Stature, 7-year-old male • Name: B.P. • Date: 15 July 2011 • DOB: 01 January 2004 • Gender: Male • Age: 7 years 6 months CC: Well visit today with parental concern about short stature Ht: 48” Wt: 48 lb Resp.: 18 Temp. 98 F HR: 74 Allergies: PCN Here with parents. Parental concerns about B. being the shortest child in class. They are concerned about his height. Denies any PMH…
View On WordPress
0 notes
Text
Penicillin allergy is over diagnosed. Most people don’t have a true penicillin allergy and even if they do, 80% of people grow out of it in 5 years. In pregnant women, as long as their reaction isn’t anaphylaxis, they can get penicillin for GBS tx.
1 note
·
View note
Text
I got 25% of my questions correct today so who's the winner in all of this? The people I paid for their question bank, probably
100 days of productivity
Day 10
RS/CVS
endocarditis prognosis: viridans = good prognosis (overall strep mortality ~5%); staph/culture-negative = poor prognosis (overall staph mortality ~30%); prosthetic valves and low serum complement also assoc. w/ poor prognosis
prosthetic valves = gent + RIF + fluclox if known MSSA source + vanc if unknown MSSA or suspected MRSA or PCN allergy
native valves = fluclox if MSSA; benzylpenicillin if strep + low-dose gent if less PCN-sensitive; vanc + RIF if PCN-allergy or MRSA; amox/(vanc if PCN-allergic) + low-dose gent if neither
latent TB in HIV → INH x9 mos
AV block: MILD RASH: myotonic muscular dystrophy, IHD, Lyme, digitoxicity (often +atrial tachy), RHD, aortic abscess/aortic root dilation, sarcoid, hypo/hyperkalaemia
CNS
NCS: ↓compound muscle action potential amplitude → axonal neuropathy
NCS: reduced velocity/conduction blocks → myelin disorders; reduced amplitude → axonal disorders
dizziness + absent corneal reflex = acoustic schwannoma
mumps meningitis causes low CSF glucose! however, other CSF stigmata point to viral disease (normal to mildly elevated protein, lymphocytes, negative stains/cultures) (differentiate from TB by acuity of mumps vs subacuity/chronicity of TB + cobwebbing in TB + *markedly* elevated protein in TB; PCR is 75% sensitive for TB)
GIT
best single-marker indicator of severity in acute pancreatitis is CRP; good predictor of necrosis
mucoid diarrhoea + very mild anaemia + hypokalaemia → villous adenoma (IRL, anaemia → r/o ca colon; but a colonoscopy will catch the adenoma anyway)
inducing Crohn's remission: 1. glucocorticoids + salazines 2. add-on azathioprine/6-mercaptopurine or MTX if cannot use aza/6-MP 3. add-on infliximab (I am unsure why aza/6-MP are used for inducing remission as they take upwards of 2-3 months to take effect; they are generally excellent for *maintaining* remission, not inducing it, but them's the guidelines I guess)
Endo/Repro/Infections
9am cortisol between 100-500 → inconclusive; proceed to cosyntropin test (but as long as levels <500 you will proceed with cosyntropin stimulation test)
urethritis NAAT-neg for gono/chlam → doxy x1 wk or azithromycin (NAAT will only be positive 2 weeks after likely transmission event)
malaria: sensitivity of QBC is greater than than of thick smear for parasite burden estimation, but less than that of thin smear for species identification
Onc/Haem
AIHA: in warm, the haemolysis occurs *extravascularly* (hence haptoglobin and peripheral smear will NOT show stigmata of haemolysis); in cold, the haemolysis occurs *intravascularly* (so hapto/smear WILL reflect haemolysis)
myelofibrosis = V617F JAK2 mutation (asso. w/ teardrop poikilocytosis)
Renal/Biochem/Toxo
MDRD equation for eGFR: CAGE: Creat, Age, Gender, Ethnicity
ADPKD assoc. w/ AR (aortic root dilation), MVP/MR, TR
warfarin × azathioprine interaction → ↓warfarin effect → impaired thromboprophylaxis in immunosuppressed (mechanism unknown)
atorvastatin (only) × digoxin → digitoxicity (inhibition of digoxin transport by the p-glycoprotein efflux transporter)
all statins interact with fibrates, but fenofibrate has the least potential for precipitating the myotoxic interaction and should be preferred when both statins and fibrates must be prescribed
thiazides cause impotence in up to 33% of patients???
if VICKO STUMBLED, luckily for him those toxins are dialysable: Valproate, Isoniazid/Isopropyl alcohol, Carbamazepine, Kerosene/Ketones, Organophosphates, Salicylates, Topiramate, Urea, Methanol/Methylxanthines (caffeine, theophylline etc), Barbiturates/Benzos, Lithium, Ethylene glycol/Ethanol, Dabigatran
17 notes
·
View notes
Text
[QUESTION SOLVED] B.P. ScenarioShort Stature, 7-year-old male• Name: B.P.• Date: 15 July 2011•
[QUESTION SOLVED] B.P. ScenarioShort Stature, 7-year-old male• Name: B.P.• Date: 15 July 2011•
B.P. Scenario
Short Stature, 7-year-old male
• Name: B.P.
• Date: 15 July 2011
• DOB: 01 January 2004
• Gender: Male
• Age: 7 years 6 months
CC: Well visit today with parental concern about short stature
Ht: 48” Wt: 48 lb Resp.: 18
Temp. 98 F HR: 74 Allergies: PCN
Here with parents. Parental concerns about B. being the shortest child in class. They are concerned about his height. Denies any PMH…
View On WordPress
0 notes
Text
Notes from an internal medicine rotation that I never posted.
Lower UTI = cystitis, urethritis
Upper UTI = pyelonephritis
Uncomplicated = healthy young women
Complicated = structural abnormalities, instrumentation, pregnant women, men
Signs & sxs: F/U/D, suprapubic pain. Dysuria is especially important to make you think of UTI.
Bacteriuria: more than 10000 colony forming units per mL
UA: nitrites (from E. coli), leukocyte esterase (from WBCs)
Complicated UTIs occur in immunocompromised pts (chemotherapy, chronic steroids, HIV, transplant pts), diabetics, ESRD, liver disease, pts w/ recent abx use.
For complicated UTI, you must do urine culture pre- and post-treatment.
Recurrent UTI = 3+ uncomplicated UTI with 1+ urine culture.
Prophylaxis for recurrent UTI: 2L daily fluid, voiding frequency, hygiene, avoid spermicide & constipation. Estrogen cream reduces recurrence.
Screen for asymptomatic bacteriuria (ASB) especially in pregnant women. ASB: +UA & + UC w/o sxs.
Sterile pyuria: +UA & -UC, seem in pts with gonorrhea/chlamydia; no need to treat if no sxs.
Pregnant women need to be screened and treated. You can give amoxicillin, nitrofurantoin if PCN allergic. Never FQs or bactrim in pregnant women.
Nosocomial UTI occurs if Foley catheter left in.
In pts with indwelling catheter, get clean catch culture if symptomatic.
Acute bacterial prostatitis = acute suprapubic pain, prostate tenderness, dysuria. Often due to E. coli. Tx for 4 to 6 weeks.
Non-complicated UTI does not require culture. Treatment is 3 to 5 days w/ nitrofurantoin, bactrim, cefuroxime. Pyelonephritis can be treated with ceftriaxone. Ertapenem txs ESBL UTI.
For hospitalized pts, IV CTX or aztreonam if PCN allergy.
At NUMC, they don’t use FQs first-line for empiric tx. There is resistance and lots of side effects.
TMP-SMX can cause hemolytic anemia in people with G6PD deficiency.
Nitrofurantoin can cause pulmonary fibrosis.
FQs can cause QT prolongation, tendinopathy, aneurysms. Must do baseline EKG before using FQs. C/I in pediatrics.
For a nursing home pt with recurrent UTI, nothing will help in terms of prophylaxis. So if the immune system can protect you, you don’t need to do anything.
7 notes
·
View notes
Text

The PCN (Personnel Certification in Non-Destructive Testing) is a global system for the certification of NDT professionals and supervisors that complies with BS EN. PCN Testing is available at Advanced Allergy, Asthma, and Immunology Center in your area. Call us at (210) 499-4824 or visit our website at https://www.mysaallergist.com/services to schedule a PCN test.
0 notes
Last Seen Blogs

lomilomimassagecalangute
Sweet Dream Spa

blu-thots
xxX_Echo::Zone_Xxx


bloglikejaeger
between the sinners and the saints

marktanner200
Mark Tanner