#either that or intramuscular in the back of the hips(?)
Text
How do you think Kim Kitsuragi does his t shot
#vu's posts#disco elysium#not me coming in with the trans man kim agenda... because he is <3#anyways. i personally see him as the type who'd do subcutaneous in the stomach yknow#either that or intramuscular in the back of the hips(?)#(i guess it's called the glutes. i didn't get much sleep last night so leave me alone lol)#glute injections are harder to do on yourself but i can see him pulling it off somehow#also kim seems like the kind of guy who would NOT be bothered by shots. like at all#hell he does a full on autopsy on a week-old corpse and doesn't freak out about it. he mostly hates the smell#anyways i've been thinking about this a lot 😂 this hc is very important to me#also sound off in the notes about your thoughts on this
4 notes
·
View notes
Text
Okay, who wants a quick worldbuilding thing regarding how various species carry fat?
Starting with Erinaens, because why the fuck not and also they're already a little fat by human standards. Your average weight for an Erinaen leaves them with a round, what would be called a pear body shape in fashion, with weight skewing higher towards the poles. As far as additional fat on top of what is considered the average, most commonly it's seen to accumulate first around the belly, the lower back and the base of the tail, then around the thighs and calves, and moving up from there. In most Erinaens the lower arms and face seem to put on fat last, though of course as with humans and all species mentioned here every body is different and can go about things its own way.
Perison are another species humans would likely immediately think of as fat. The average for males leans toward high muscle mass completely covered by a healthy fat layer- think what you see with competitive weightlifters- while females tend to have a higher ratio of fat and more fat, leading to greater girth especially around the torso per their height. Additional fat most commonly seems to accumulate on the back, before working it's way around the belly and chest and down to the tail. From there it seems about even whether it accumulates in the neck and face or the thighs next, finishing with the arms.
Tetramand, meanwhile, will often come across as quite lean to humans. Unlike the other species mentioned so far, Tetramand aren't especially predisposed to subcutaneous fat aside from that of breast tissue, leaning more towards intramuscular fat. In non-scientific terms, these fuckers have some wagyu-style marbling. When you get get build-ups of subcutaneous fat, it most often starts and focuses at the chest, then spreading to the belly, back, and rear. It's uncommon for Tetramand to build up noteworthy fat deposits elsewhere.
For Kineceleran most standard body fat is carried around the back of the base of the tail, going up the back of the hips. Otherwise they tend to be quite a lean species as a general rule. When it comes to extra fat, there's actually two main locations that fat build-up starts after those two, which has been tied to specific genes. For some individuals, especially those whose ancestry hails from more flat and open environs, excess fat past the back-hips and back-tail base tend to accumulate around the torso. For others, especially from more mountainous or twisty areas, fat accumulation tends to focus on the tail more. Either way the last places fat tends to gather are the arms and the legs, and once you get notable fat deposits in the thigh that's considered 'morbid obesity' levels- Kineceleran bodies will do everything short of have you cough up your liver to avoid putting fat on the thighs. Even slow members of the species move fast enough that a lack of a gap there risks serious injury.
Now with all of these there's a general level of weight that is the average across the population. You get areas where people weigh more, you get areas where people weigh less, but in general there is a singular or dual 'average' that you can point at. Osmosian weights can vary more widely, by location, by lifestyle, by time of year, by time of day (though that one is a smaller difference most of the time), by sex, by breeding intentions- Fuckers' averages can have a variance in the vicinity of 50 pounds, mostly made up of fat, depending on these factors. Individuals living on the coast tend to be notably leaner than elsewhere, nomadic packs have higher fat reserves, as do eggbearers, individuals tend to develop small fat reserves after sunning and so will weigh more in the afternoons and these reserves will be bigger during the summer, eggbearers put on weight when they intend to nest, especially those in non-nomadic packs. As a general rule Osmosian's carry fat primarily in their tails and slightly less so in the torso. The neck and face most commonly put on fat before the limbs, and the development of fatty jowls is common. In fact it's seen as a goal among non-nomadic eggbearers intending to nest- when you're going to be underground acting as a living food source for your children for, hopefully, nearly a year Earth time? you want some fat reserves, even if your Nesting is going to come around and feed you.
8 notes
·
View notes
Text


Here's a quick drawing... and perhaps something akin to a drabble...
--
It's awkward, kind of. Dan - coming at the wrong time, seeing the wrong thing-
It's too quick to react to, Herbert thinks in admonishion.
Dan knocking and immediately going to open the door - as if that's enough of a warning. As if that's enough time for Herbert to hide what he's doing.
"Herbert, I wanted to ask you about-" Dan's voice cuts off in the middle of the question as he looks and sees.
There's a second of awful pause there. A hesitancy so thick one can feel it rub against their skin as they move.
"What is that?" Dan asks, eyeing the vial and the disinfectant wipes and the individual-packed syringe next to Herbert's hip on the bed. He's more confused than anything, and Herbert - well, Herbert feels defensive in all the worst ways.
He hates to be outed like this. But he might as well say it. (Dan would have realized sooner or later, anyways.)
"Testosterone," Herbert answers, tone clipped, almost provocative. He sits up straighter, eyes blazing, challenging Dan to try and pull something from behind the lenses of his glasses.
This will either go down smooth or messy. Herbert's ready for either, coiled to jump up like a tensed muscle.
He feels under-dressed - severely so in just an undershirt and briefs - all while Dan stands, comfy sweater and long pants. Proper and perfect, if not for his expression.
Dan's mouth drops open soundlessly - his gaze flits to the rectangular scar on Herbert's forearm and a light bulb goes off in his head, points connecting to make the bigger picture.
"Oh," Dan says dumbly.
"Yes," Herbert confirms, sure that Dan's come to the right conclusion. He's rather smart, after all, even if he has certain airhead tendencies.
There's a flush spreading over Dan's cheeks now, embarrassment and shyness all at once. His hands come up, fiddling. "Do you- ah- do you want some help with that?"
Herbert's brow furrows as his lip curls back meanly, "What?" it comes out a bit more biting than he was going for.
But no one can blame him for his nerves, given the situation.
Dan moves forward, his countenance shaky, "Help- with the shot," he says. He drops to his knees in front of Herbert, and the scientist almost draws back at such a display. Almost.
"I'm good at intramuscular shots," Dan says like an explanation, nervous and obviously trying to pretend he isn't, "Done hundreds of them and never had a haematom or abscess develop afterwards."
"Dan," Herbert starts, ready to ask the man to leave- But he stops. This is too much at once. He's finding it hard to judge Dan's reaction beyomd his words.
"I'm more than capable of doing this myself," Herbert ends up saying snidely, finding the sharp words more comfortable than anything else he could've said, "I've been doing it for years by myself."
Dan's expression falls, suddenly hesitant where before he'd been open and mirthful. "Sorry, I- it's just-" he pauses, takes a deep breath.
"Meg is- too- you know. I know it's- it's a lot to tell someone else. Sorry I rushed in. I wasn't thinking, and I've forgotten what I even wanted to ask..."
It takes Herbert a long moment to grasp the meaning of Dan's first-half-of-statement, but when he does... there's a certain amount of apprehension. But mostly - a calm that washes over him.
Dan is safe. Herbert feels something guarded deflate within himself with an audible exhale.
Which means...
"Okay," Herbert says, quiet. Still cautious, but a different kind of it.
Dan's brow furrows, "okay?"
Herbert nods, left hand briefly white-knuckling the sheets- "You can do the shot."
Herbert closes his eyes afyer saying this, too afraid of what he might see if he looked.
He's counting down the seconds until he changes his mind. Dan has exactly half a minute to act. After that - Herbert will usher him out, regardless of what he might say or think.
"Oh shit-" Dan curses softly. Herbert hears him fumble with the objects on the bed. "I mean, yeah. Okay."
Twenty-five second left. He hears the rip of the package of the desinfectant wipe, followed by the cool sensation of Dan rubbing the injection site down in preparation - his movement a gentle outwards swirl over the anterolateral surface of Herbert's thigh.
Herbert breathes, feeling something thick in his throat.
Already he thinks - he shouldn't have given Dan permission. This is too intimate, too real. He feels like Dan has too much power over him right now.
(on the other hand... it is quite nice, being seen and not looked down on.)
A pause, the exposition time for the ethanol passing. Herbert recognizes the soft rubbery sound of the needle breaching the vial's seal.
He takes a shaky breath. Dan's hand is splayed out over his thigh, holding the skin taut gently. His hand is warm but clammy. He's nervous too, just like Herbert.
(That's comforting)
The second of waiting - Dan emptying the chamber of air so that only the praeparat remains.
The actual injection is all but painless. Daniel certainly has a deft hand at this. Herbert can hardly feel it as he plunges the syringe.
"There," Dan says, and Herbert opens his eyes to see him holding a wad of sterile cotton against the injection site firmly, the other hand holding the syringe aloft and away from either of their bodies safely.
Dan's eyes are shining, kind, as he looks up at Herbert from his kneeling position.
It makes Herbert a little nauseous. He reaches for the band-aid, and Dan obediently moves his hand so that Herbert can apply it.
"Thanks," he says gruffly, a weird heat in his cheeks.
"You're welcome," Daniel responds, his smile a bit mysterious. "If you ever need - just ask, and I'll help."
Herbert's smile is tense and uncomfortable. He needs more time to regroup. He needs to stomach this. "I'll remember that, Daniel."
He wonders how he feels about that sounding like a promise. He hates that his thigh tingles where Dan touched him for the rest of the day.
It's a long day.
[The end.]
--
I think... there is something very intimate in an injection outside of a fully medical setting, especially if the two know each other.
Dan might've jumped the gun by being his eager-to-help self, and West jumped right with him...
172 notes
·
View notes
Text
Attention

Pairing: Johnny “Human Torch” StormxBlack Reader
⚠️: Tiny bit of angst (if it even counts really), also tiny bit of implied happy times, but mostly fluff💕!
Re-reading over your notes for what felt like the millionth time this week, you softly mumble to yourself the highlighted material hoping that everything would remain stuck in your mind for your practical tomorrow.
“Intramuscular means within the muscle and is given at a 90 degree angle. Intravenous means within the vein, given at a 25 degree angle. Subcutaneous: in the subcutaneous layer at a 45 degree angle. And finally intradermal-,”
“Psst....psst!!”
If only your boyfriend would stop being a grown man child and let you finish studying though.
“Yes Johnny?,” you sigh still looking down at your binder.
“Take a break, I want to show you something.”
“No Johnny we’re not doing that again.”
“I wasn’t talking about that princess,” he smirks moving to lean against the bedroom door frame. “Although I’m not complaining if you want more.”
Giving him a look clearly showing how you weren’t in the mood, he chuckles holding up his hands to show he was done joking.
“Seriously though I want to show you something, so can you please come with me?”
“Just tell me, or take a picture of it on your phone and show me that way. I really have to keep studying and don’t have time for a bunch of breaks.” Straightening up, a low huff leaves his lips as you hear him pad through the living room before coming back holding a new action figure posed as if about to throw a handful of flames.
“Look! It’s me!,” he beams squatting next to you holding out the toy for you to see.
“Mhm that’s nice babe,” you smile not really displaying the reaction he wanted you to.
“I see you’re having a hard time containing your excitement,” he retorts sarcastically, bringing his mini me back towards his chest.
“It really is nice babe, it’s just similar to some of your other toys that I’ve already seen.”
“But with this one, the little flame lights up. See?” Pressing the small button on the back to show the tiny, plastic flame glowing scarlet, a wide smile spreads across his face making you giggle.
“Yes very cool. Now if that’s all, I gotta get back to this okay?”
“Alright,” he sighs standing up to return to his spot on the couch probably cold by now. “Why don’t you come study out here? It’ll be more comfortable than sitting on the floor.”
“Because you’re watching tv and that’s gonna distract me.”
“Not anymore. The game’s off so I’m done for the night,” he playfully smiles stealing one of your study packets making you whine his name. “Cmon you know you’d rather sit on the big, soft, incredibly comfy couch.”
Wiggling his brows, you roll your eyes trying to focus back on the words in front of you, but as always, seeing his adorable pout was wearing you down. Plus the ache in your buttcheeks was really making the couch, or any soft piece of furniture for that matter, sound like heaven.
“And, as an added bonus, your incredibly hot, charming, all around amazing boyfriend will be there.”
“Johnny...”
“As!...support and to help anyway I can of course. What did you think?,” he feigns shock as you shake your head.
“Alright fine. But if you try to distract me just once, I’m kicking you out for the rest of the night, and you’ll have to either get a hotel, or crash with Reed and Sue.”
“Okay deal,” he chuckles helping you stand and gather the packets, pens, and highlighters you needed to continue your attempted all nighter.
Sat in the middle of the plush sectional with one of his legs draped over your folded ones and the other stretched out behind you, so far he’d done well on his agreement. He stayed busy on his phone watching sports highlights with earbuds attached to his head, and hardly ever touched you unless to give a reassuring hug when he could sense you were getting overwhelmed, or softly dance his finger along your arm making you smile. He even started quizzing you from whichever packet you were on as you lied just below his chest playing with his free hand.
From how he was earlier, seemingly a bit more clingy and not wanting to be away from you, something told you deep down this was all he wanted. Just feeling your body near him as you did whatever, no matter how boring the task was. And although a little distracting, you couldn’t be completely mad at him for his antics since deep down you know you wanted it too.
Honestly need may be the better word judging from your noticeably calmer state. Even Johnny could feel your heart rate gradually decrease to its normal speed through his body.
Soon his yawn began to trigger your own set and eyelids became heavy as the questions came slower along with your answers. You tried to fight it off, but apparently your body had other plans making it increasingly more difficult to open your eyes until both of your light snores were the only sound that could be heard throughout the room.
———
“Good morning Mr. Johnny Storm, Miss Y/N,” the computerized security system greets opening the curtains to reveal the bright sun and cause you to stir. Rubbing your eyes, you see all the packets spread on the glass coffee table quickly reminding you of your exam.
“Sherlock, what time is it?,” you ask in a panic as you sit up causing Johnny to shift slightly without opening his eyes.
Also, why he decided to name the computer system Sherlock, you’d never understand.
“11:30 am miss.”
Grabbing your packets as fast as you can, a string of curses fall from your lips as you run about trying to collect your things. By now you were supposed to be on campus looking over your notes one last time before going in for your slot time at 12. At this rate, you’d definitely be over an hour late and received an automatic zero.
“What’s the rush princess?,” your boyfriend tiredly asks stretching his arms over his head as he stands.
“I overslept and I’m late,” you sniff trying to hold back your tears as you search through drawers trying to find your scrubs. “Where are they?”
Joining you in the room, he tries to kiss your cheek only to miss you completely as you rush past him still looking for your clothes.
“Closet babe. By my suit.”
“Well what about the other ones since those need to be washed now?”
“In the basket to be washed.”
“You mean the same clothes in the basket I asked you to wash last weekend,” you retort changing into the faint ash smelling scrubs. Noticing you wiping your eyes a bit more frequently, he manages to grab your arm stopping you from wherever else you needed to go.
“Johnny seriously I don’t have time for this-,”
“Relax okay? Let’s try to call your professor and tell them what happened to see if you can get a new time.”
“It’s not gonna work. This isn’t an emergency situation, I just overslept like an idiot,” you answer pulling away to finish the rest of your morning routine in the bathroom.
He sighs hearing you bang about while pulling his phone from the pocket of his sweatpants trying to find the number for your school. His upcoming events list popping up though makes him deeply chuckle as he shakes his head.
“Oh honey...!”
“Johnny please don’t start. I’m already frustrated a-and overwhelmed trying to figure out what to do and just need to-.” Holding his phone in front of your eyes, you see his calendar showing all his important meetings and interviews, along with your test date.
Which wasn’t until next Monday.
Pulling your phone from your backpack, you go to your calendar to find the same thing making you feel even dumber.
“...S-So I don’t have my test today?”
“No princess,” he smiles coming closer to caress your face with both hands, wiping your tears with his thumbs.
“And I stayed up all night this week studying for nothing?”
“Well not for nothing. You know your stuff now, so you won’t have to worry about it later.”
“Yea,” you sigh looking up at him as you hold onto his strong forearms. “Sorry for snapping at you about the laundry, and for kinda being cranky yesterday.”
“You were stressed. I get it.”
“But still, there were things I could’ve said differently-.”
“I forgive you,” he smiles leaning in to meet your soft lips with his in a needy kiss he’d been craving since yesterday. Biting your bottom lip as he just barely pulls away, your hands wander from his forearms to his flexed biceps, shoulders, and eventually chest stopping to graze your index finger along the small dip below his neck.
“Well since I don’t have an exam today and no classes, I was thinking...”
“Oh I think I know,” he smirks tilting his head lower to nip at your jaw and neck making you giggle.
“I help you do the laundry.” As soon as the sentence left your mouth, his stopped making you laugh harder while he groaned against your skin.
“Alright I promise it’ll get done today, but can’t we do it later?,” he whines with puppy eyes, lifting you so your legs could wrap around his hips as if trying to persuade you.
“Let me finish. We do the laundry so I can have clean scrubs and between loads, I give you all the attention I know you’ve been wanting that I wasn’t fully able to give this week.”
“Hey it’s not like I’ve been that-,” he tries to deny before meeting your eyes as if they were saying “really?”
“...yes please,” he smiles before his mouth returns to your smiling lips.
Taglist: @fumbling-fanfics @honeychicanawrites @honeychicana @lady-olive-oil @themyscxiras @melinda-january @lovelymari4 @maxcullen @literaturefeen @damnitaa @curlyhairclub @plokyu23 @fullofmelaninsarcasmandepression @nunubug99 @felicity-x0 @ellixthea @jnk-812 @jojolu @brwn-sgr @captainsamwlsn @wildfirecracker @nina-sj @iammyownlover @chaneajoyyy @secretmysteriousperson @scoop93535
If anybody wants to be tagged, has asked to be tagged but don’t see your name, only want to be tagged for certain people I write for (can be found on my masterlist), or no longer wish to be tagged just let me know🤓!
#johnnyxwoc#johnnyxblackreader#johnnyxreader#johnny storm#fantastic four#chrisxblackreader#chrisxwoc#chrisxreader#chris evans
56 notes
·
View notes
Text
Testosterone, Day 432
That’s just over 14 months. Still on one pump of Tostran per day, which is 10mg of testosterone. (For comparison, I found out that one pump of Androgel or Testogel is 20.25mg.) My dose is considered low. Gel vs. injections dosages are not comparable so watch out for that.
BIG CHANGE compared to the last update: 5 days ago (27th Nov), I had my first injection of Decapeptyl (intramuscular injection, administered to the buttock every 12 weeks by a nurse who can do IM injections). It’s a hormone blocker that shuts down my ovaries, as far as I know? It didn’t hurt at all, but I gather that pain varies from injection to injection. It has different components that need to be mixed with a separate syringe, so it’s not really like getting a flu jab.
It was prescribed to me by the endocrinologist at the London gender clinic, after I explained that 12 days of being off T (even coming off only 1 pump of Tostran per day, the lowest of the low) gave me some truly awful menstrual symptoms. The idea is, if I’m on Decapeptyl and it stops my ovaries, coming off T will only cause coming-off-T symptoms rather than that plus menstrual symptoms. Then I can look into either going into menopause on purpose (and taking drugs to prevent heart problems and osteoporosis), being on T again, or letting my ovaries kick back in.
I am curious to find out how it affects my sex drive and my appetite, which are the two things that are affected most by hormonal treatments for me. (Testosterone made my sex drive increase a LOT at first and then gradually decrease until it’s back to normal after 6 months, and as my sex drive gets back to normal my appetite increases.) It’s only been a few days and it takes at least a month to get to its full effect so it’s going to be a while until I find out how it feels.
Last entry: Day 309.
Skin: My skin is totally back to normal! If anything, it’s a little better than pre-T because the highs and lows of my menstrual cycle are levelling out.
Appetite: I have that thing, a very familiar hormone thing for me by now, that I’ve had before with hormonal birth control and with the first round of T: wanting to eat and feeling “fake hungry” even though I can tell I’ve had plenty of food. It happens especially in the evening, and I always want to eat carbs. It happened 6 months into the first testosterone period, and then at 7ish months I stopped T for 12 days and then started again for unrelated reasons and my appetite got totally reset back to normal and it was such a relief. Now, it’s about the same amount of time into testosterone again and I’ve been noticing the weird appetite creeping back in over the last couple of weeks. So I guess this is just something that happens after 6 months on T for me!
Sex drive: Pretty much back to pre-T levels.
Menstrual cycle: (I have working ovaries but no uterus so it’s just hormonal cycle stuff.) My joints generally feel less loose than before, and my pre-menstrual symptoms are much reduced.
Voice: There has been very little change over the past 3-5 months. It’s just a very slow meandering downwards, really. Sometimes I feel really resonant in my voice, and sometimes it gets kind of more head-voicey (which feels bad at the time), and in the head-voice times it gets higher-pitched and then it cracks a bit in a teenage boy way, and I have to consciously lower my pitch and deepen the resonance to reset myself!
Body hair: Very little change over the past few months. The hair under my belly button is a bit coarser, and it’s spreading out a bit. I have visible but light soft hairs on my thighs. My lower legs are a bit hairier, and the hair extends to the top of my feet a little bit. I continue to be not into the masculine body hair pattern, but I can live with it for the time being I think!
Facial hair: Darker hairs on my upper lip, still quite cis woman amounts. Some very light peach fuzz on my cheeks, and lately I’ve noticed some tiny hairs on my lower lip too. When it was just my upper lip, my facial hair gave me masc and fem dysphoria at the same time - fem because it’s a very typical cis women look, and masc because I know it’s caused by taking testosterone. The increase in other facial hair is reducing dysphoria all round though, I feel pretty okay about it, even though I was not expecting to. I hope it doesn’t get thicker.
Genitals: No change since the last update. I am 100% ready for the metoidioplasty (no testicular prostheses, no vaginectomy, no urethral messing-about), but it’s going to be a couple of years probably.
Fat distribution: My body fat is mostly concentrated around my middle (belly and thighs) now, and I don’t think I have any gender dysphoria about it, but it does bother me because testosterone has increased my appetite, so I’m putting on weight and I don’t like it! I hate having to buy new clothes and I hate change (#ActuallyAutistic), so I just want my body to be the same size as before but with smaller hips and whatnot.
Actual hormones: Since the last update I had a fasting blood test 4-6 hours after applying the Tostran gel and it was about 13 nmol - low masculine range, but higher than the last T blood test.
Hairline: It still feels a smidge higher than pre-T. I’ve been growing out my hair for 122 days and it looks ridiculous, but I can’t blame testosterone for that - it’s just that it’s too long and too short at the same time, that classic growing-out-your-hair feeling.
Transition details: Nonbinary, only really want to change my voice pitch and then stop, I’m on the lowest dose of testosterone.
Voice pitch app data:
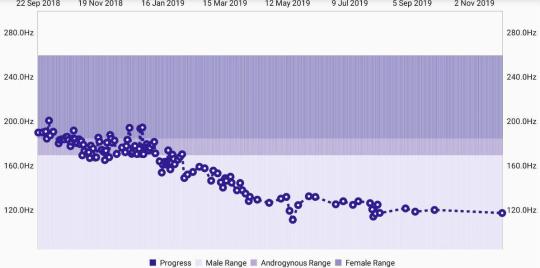
#original posts#cassian's hormones#cassian's transition#nonbinary#testosterone#low-dose testosterone
4 notes
·
View notes
Text
How to Lose Inner Thigh Fat (Spoiler Alert: It Involves Diet and Exercise)
Created for Greatist by the experts at Healthline. Read more
Fat is necessary for sustaining life and protecting your organs. But where you store excess fat is all determined by your genetics. So, if you find you’re carrying extra weight around your inner thighs, that’s just how your body operates.
And while having some inner thigh fat is perfectly fine, if you’re ready to tone things up, we’ve got you covered. Here’s how to lose inner thigh fat in a healthy and sustainable way.
Getty Images
What causes inner thigh fat?
If you eat more calories than you can burn, your body needs to store those additional calories somewhere since they aren’t being used. That’s where fat comes into play.
According to the World Health Organization, there has been an increased intake of energy-dense foods (think high fat and high sugar) as well as lowered activity. This energy imbalance is the fundamental cause of weight gain.
Now as to where this fat is stored, again, you can thank your genetics for that. One study found that body fat storage is highly influenced by genetic factors, especially in women.
Women usually store fat in their hips, lower belly, and inner thighs. While men carry fat mainly in their abdomens, but aren’t completely off the hook with inner thigh fat either.
If your genes graced you with the gift of inner thigh fat, it can form in two ways:
subcutaneous fat (located just below the skin)
intramuscular fat (located within the muscle)
So, how do you lose inner thigh fat?
As with any weight loss situation, a combination of diet and exercise can help you blast inner thigh fat. You just have to put in consistent work.
Change up your diet
Since taking in too many calories can build up fat, reducing how many calories you’re taking in each day can help you lose inner thigh fat.
One pound of fat is equivalent to about 3,500 calories. So, just cutting out 500 calories a day can help you eat 3,500 fewer calories a week, and lose about 1 to 2 pounds a week.
Other basic dietary changes to help you lose inner thigh fat include:
reducing processed foods and sodium intake
ditching white starches for complex carbohydrates
cutting out sugary drinks
drinking more water
eating lean protein
filling half your plate with vegetables
eating fruit to satisfy your sweet tooth
Incorporate cardio and strength training
There are two different forms of exercise to help you lose fat.
Aerobic: Exercise sustained over longer periods of time, such as cardio activities like running, walking, or biking that gets your heart rate up.
Anaerobic: Bursts of exercise for shorter periods of time, such as high intensity interval training (HIIT) or strength training.
To maximize your results, it’s a good idea to do a combination of both in the forms of cardio and strength training.
One study found significant weight loss results in both men and women after 10 months of aerobic exercise. Other research found that anaerobic exercises like HIIT are also effective for fat loss.
Plus, cardio helps you burn calories in the moment, while strength training helps your body continue to burn calories throughout the day.
So, a good rule of thumb is to exercise 4 or 5 days a week to see results, and incorporate both cardio and strength training.
But can’t you just spot train? That’s a big nope!
As cool as it would be, you can’t pick and choose which area of your body you’d like to lose weight. Our biology rules the game, therefore putting time and energy into targeting a certain area of your body is likely a waste of time.
If you do a bunch of crunches and sit-ups to lose fat in your belly, you’ll probably gain muscle in those areas, but that doesn’t mean you’ll burn fat.
You’ll see greater results by performing multiple exercises that work multiple muscle groups.
Try these cardio workouts to burn inner thigh fat
Ready to get your cardio on? You can do any cardio exercise to burn fat, but the following exercises will get your heart pumping along with targeting those thigh muscles.
Hill training
Running up and down hills just straight up blows, but it will get your thigh muscles strong and improve your fitness ✅.
Grab a stopwatch and find yourself a hill (don’t go too steep too quick). Then run up the hill as fast as you can for 30 seconds. Cool down and walk back down. Repeat this about 5 times, and aim to do this 2—3 times per week to start.
Not into running? Find a hilly area and take a walk, or go for a hike in nature that’s a bit of a climb.
Gradual treadmill exercises
Maybe you live in a really flat area and there just aren’t hills that get your legs burnin’. A treadmill can also do the trick.
Pick your cardio (walking or running) and gradually increase the incline to 5, 10, or 15 percent while you exercise for at least 30 minutes.
Mix this into your weekly cardio routine 2—3 times a week.
HIIT
The best part about HIIT exercises is that they can literally be done anytime, anywhere.
Moves such as jump squats, burpees, and high knees are all forms of HIIT movements that can get your heart rate pumping in a short period of time.
Getting in HIIT exercises 2—3 times per week is a solid amount.
Try these exercises to tone inner thigh fat
The following six movements will tone your inner thighs and reduce the appearance of fat. Include this routine into your exercise plan a few times a week to see results.
Repeat this workout 2—3 times through.
1. Curtsy lunge

Dima Bazak
Reps: 10—15 per leg
Equipment: Optional dumbbells
Stand with a wide stance and keep your chest upright and shoulders down.
Cross your left leg behind your right leg and squat into a curtsy position, keeping your right leg planted and body upright.
From the lowered position, push yourself back up and place your left leg back to the starting position.
Repeat on the other side and continue switching legs until you hit your reps.
2. Walking lunges with dumbbells
Image by Dima Bazak
Reps: 10—15 per leg
Equipment: Optional dumbbells
Stand with your feet hip-width apart while you hold a dumbbell with each hand. Keep the weights steady at your sides. (If you’re a beginner, try with no dumbbells first.)
Step forward with your left leg and lunge forward. Make sure your knee doesn’t go beyond your toes and keep your leg perpendicular. Your non-lunge knee should be around 1 inch off the ground.
Keep your weight mainly in your heels and push your left leg back to the starting position.
Switch legs and lunge with your right. Alternate legs as you walk to complete your reps.
3. Sumo squat (AKA plie squats)

Dima Bazak
Reps: 30 seconds total
Equipment: Optional dumbbell or kettlebell
Stand in a wide stance with your toes and knees pointed outward.
Slowly lower into a squat position. Keep your hands on your hips to help your balance and keep your spine and torso upright.
Slowly rise back up, squeezing your glutes to bring yourself back up.
Continue for 30 seconds total.
4. Skaters
Image by Dima Bazak
Reps: 20 total (10 per leg)
Equipment: None
Similar to the curtsy lunge, you’ll start with your left leg behind your right with both knees bent.
Press sideways off your left leg and land back onto your right. Keep your left foot behind you in a curtsy lunge position on the other side. Switch off between legs.
You can either step or hop depending on your fitness level. Keeping your back leg off the ground will also be more challenging.
5. Side lunge
Image by Dima Bazak
Reps: 10—15 reps per leg
Equipment: Optional dumbbells or a medicine ball
Stand with your feet wider than your hips while you hold either a medicine ball or weight at your chest with both hands. (Beginners, try without weight for the first time)
Take a step to the left and squat down on your left leg by bending your knee and lowering your body until it’s parallel to the floor. While doing this, ensure that your toes are pointed forward and your left knee is aligned with your left ankle.
The weight or medicine ball should also remain at your chest and be in line with your left hip, elbow, and shoulder when down into the squat.
Power back into the starting position by pushing off your left leg. Finish your reps on that side before moving onto your right side.
6. Supine inner thigh lift

Dima Bazak
Reps: 15 reps per leg
Equipment: None
Lay down flat on your back with your abs engaged. Have your arms out to your sides, with your palms lying flat on the ground.
Keeping your hips on the ground, lift your legs up toward the ceiling with your feet flexed.
Lower your right leg out to the side as far as you can tolerate without lifting your hips. Keep your foot flexed the whole time.
Bring your leg back up to the starting position, squeezing both your legs together at the top.
Repeat 15 times on your right side, then switch to your left.
The takeaway
Some of us are graced with the genetics that give us thick thighs. But fat also accumulates in this area due to the extra calories and limited energy expenditure in the form of exercise.
Improving your diet and adding in cardio and thigh toning exercises takes time, but it’s the most beneficial way to get those thighs of steel.
from Greatist Health RSS Feed https://ift.tt/3e9Gj4s
How to Lose Inner Thigh Fat (Spoiler Alert: It Involves Diet and Exercise)
Greatist Health RSS Feed
from HEALTH BUZZ https://ift.tt/2HGdf8B
0 notes
Text
Xan the Trans*Boy || Pt. 4
In an exam room of the outpatient surgery ward, Alexa sat with all parents present. Addison had called in a favor with an endocrinologist from Columbia, and he would be there any minute. A resident had already run Alexa's labs, and the family was preparing for the hormone blocking implant that would allow the little boy to delay going into the wrong puberty.
Sitting on a chair in the corner of the room, Alexa's youngest sister Skylar sat, her knees pulled up to her chest and a copy of Harry Potter and the Prisoner of Azkaban in her hands.
"Now, 'Lexa, remember how I explained what this is?" Addison asked, to which Alexa gave an enthused nod. "Care to share with the class?"
"Well, the hormone blocker is like putting a car in neutral. Everything is still running, the engine is still burning gas, but we're not moving backwards or forwards. So most developments my body has made won't regress. But I won't make anymore. The downside is that I might not get taller for a while, and I'll look like a little kid for a little bit longer, but puberty is essentially halted." A small sigh could be heard from the corner of the room. Skylar looked around the room, rolled her eyes, and returned to her book.
"Anything you'd like to add, Skylarpedia?" Mark called over, a little more gruff than he'd intended.
"All metaphors do are cloud the explanation with imagery that doesn't necessarily relate. Your body is not a car, Lex, and it never will be. Your body is a body. The human kind, I'll add." Her tone was even and she didn't bother to look up from her book.
"Well, how would you explain it, if you're so much smarter than me?" Alexa called back. Now that her assistance was being requested, Skylar put her book down and sat criss-cross on the chair.
"A hormone blocker is either an medication taken by intramuscular injection, or by implantation of a device in the upper arm. Today, Lex, you'll be undergoing the implantation of a device, because it runs a lesser risk of improper dosages. I still don't understand why that's a factor if we basically live in a hospital, but that wasn't my call." Skylar rolled her eyes emphatically before she continued. "The hormone blocker suppresses two major puberty-inducing hormones, Luteinizing Hormone, or LH, and Follicle Stimulating Hormone, or FSH. These hormones control the development of secondary sex characteristics. In order to support your transition, the blocker will prevent the development of fatty tissue developing in traditionally female patterns, including the face, hips, thighs, and breast areas. It'll also prevent the continued development of the ovaries, which would result in the beginning of menstruation in anywhere from a year to four years."
"Well, we know which of the kids is going to win the first Harper Avery," Arizona smirked, nodding approvingly. Alexa looked a little uncomfortable, so Mami swooped in with a hug and a kiss to the top of the head.
At no better moment, the doctor came in and lit up the room with a huge smile. “Well, I’m sorry to keep you all waiting,” he nodded before directing attention at Addison and Mark. “Addie, Mark, so good to see the both of you again. Can we still do dinner tomorrow night?”
Both Mark and Addison uttered different versions of “Sure, why not,” before Addison gestured to Alexa. “Dr. Stone, these are Lex’s moms, Dr. Arizona Robbins and Dr. Callie Torres,” after a quick round of handshakes and ‘nice to meet you’s, all eyes were on Alexa. “And the patient of the hour.... This is Lex.”
The truth is that no one had addressed the elephant in the family - if Alexa was going to transition, what was his name going to be? To be as supportive as she could be, Addison reminded herself to use “Lex,” the most gender neutral form of his name.
But that was a question for another day.
2 notes
·
View notes
Text
Review on Blackleg in Cattle- Juniper Publishers
To know more about journal of veterinary science impact factor: https://juniperpublishers.com/jdvs/index.php To know more about Open Access Publishers: Juniper Publishers

Abstract
Blackleg is an endogenous acute infection that principally affects cattle. Blackleg is generally fatal bacterial diseases of young cattle or sheep of any age. The disease is caused by Clostridium chauvoei, an anaerobic spore forming bacterium seen as an acute, localized inflammation of muscle tissue due to growth of the blackleg organisms. This followed by generalized toxemia or poisoning of the animal causing rapid death. The disease is widely distributed in the world. Blackleg can occur at any time of the year; more loss of cattle is seen during warm months of the year. Blackleg has been found in cattle as young as two-month-old, most loss occur in cattle, the best conditioned animals, where there is an abundance of feed. It is prevented by vaccination when out breaks occur; in early stage of the disease it is treated by antibiotic mostly penicillin is effective treatment to the disease. Control of this disease is based on stringent husbandry measures and scheduled vaccination plan. In recent years, the major virulence factors of C. chauvoei have been discovered and described. However, the pathogenesis of blackleg in cattle and, circulation of the pathogen from point of entry to target tissues is yet not fully elucidated. Therefore, the objectives of this paper are to summarizes the latest review of literature that significantly contributed for understanding the disease in cattle and provides a foundation to preventive strategies.
Keywords: Blackleg; Cattle; Clostridium chauvoei; Soil; Vaccination
Go to
Introduction
Ethiopia is one of the countries with the largest number of livestock in Africa and livestock production plays a major role in the development of Ethiopia’s agriculture. Ethiopian livestock population is estimated to be 59.49 million cattle, 30.697 million sheep, 30.200 million goats, 8 million donkey, 2.16 million horse, 1.20 million camels, 0.4 million mules and 59.495 million poultry [1]. Nevertheless, the development of livestock sector in Ethiopia is hindered by widespread endemic health problems including bacterial diseases, viral diseases, and parasitic infestation [2].
Animal diseases such as blackleg which is also called quarter ill or black quarter cause the major limitation to the livestock agriculture of the country and affect livelihood through their effect on animal health and impact on the production. Blackleg also called quarter ill or black quarter is an acute specific infectious disease of cattle, sometimes of sheep and pigs characterized by the presence of rapidly increasing swellings containing gas, and occurring in the region of the shoulder, neck, thigh, quarter, and sometimes in the diaphragm. Young cattle between the ages of 6 months and 2 years are also susceptible [3]. The disease is an acute myositis caused by the activation of latent intramuscular Clostridium chauvoei spores. It commonly kills unvaccinated cattle between 3 months and two years of age especially in higher rainfall areas such as the coast of north southwest. It is an endogenous acute infection that principally affects cattle. The disease is caused by Clostridium chauvoei (C. chauvoei), an anaerobic spore forming bacterium. Blackleg usually commences in skele tal muscles but occasionally the heart or diaphragm is affected. The primary site of infection of blackleg was myocardium [4].
Blackleg is caused by the spore forming, rod shaped, gas producing bacteria Clostridum chauvoei. The spores of the organisms can live in the soil for many years. The bacteria enter to the host by ingestion and then gains entrance to the body through small punctures in the mucous membrane of the digestive tract. Cattle that are on a high plane of nutrition, rapidly gaining weight and between 6 months and 2 years of age are most susceptible to the disease. The disease is not transmitting directly from sick animal to healthy animals by contact [3].
Bacterial spores are eaten in contaminated feed or soil. The spores then eater the bloodstream and lodge in various organs and issues, including muscles. The injury reduces load flow to the area, thereby reducing the supply of oxygen to tissues. In the absence of oxygen, the spores germinate and multiply. As they grow, the bacteria produce toxin which destroy surrounding tissues. The toxins are absorbed in to the animals’ blood stream which makes the animal acutely sick and causes rapid death [5]. The first signs observed are usually lameness; loss of appetite, rapid breathing and the animal is usually depressed and has a high fever, characteristic swellings develop in the hip, shoulder, chest, back, neck or elsewhere. First the swelling is small, hot and painful. As the disease progresses, the swelling enlarges and becomes spongy and gaseous. If the swelling is pressed, gas can be felt under the skin. The animal usually this within 12 to 48 hours. In most cases the animal is found dead without being previously observed sick.
Pathological changes associated which blackleg are the carcass bloats and putrefies quickly after death, body cavity often contain excess fluid, often reddish in color, infected muscle masses are swollen, discolored and have a foul odor, in some cases a small muscle mass will be affected and lesions may be hard to find. Sporulated gram positive rods can be demonstrated in smears of infected tissues and identified by immune florescent reagent. ground muscle in saline is cultured on blood agar plates, which are incubated anaerobically, because of the possible presence of swarming Cl, septicum, early subcultures should be attempted from some plates, which others last for 48 hours most the organism will appear as gram positive rods when examined immediately following death of the animal [6].
Treatment of affected animas with penicillin is logical if the animal is not moribund but results are generally any fair because of the lesion. Large doses should be administered commencing with crystalline penicillin intravenously and followed by longer acting preparation, some of which should be given in to the affected issue if it is accessible. The most effective means of prevention is proper vaccination program. Multivalent vaccine is suggested. The first dose should be given at two months of age and a second injection at either four weeks before preweaning or at the time of weaning. If animals are in an endemic area, another booster should be given [7].
In the event of an outbreak, individuals between 6 months and 2 years should be vaccinated or revaccinated. A two-week period post vaccination exists during which antibody levels are not high enough to our resistance and animals may continue to be loss. Moving animals away from the site of contamination is desired but even this is not always effective. Carcasses of animals known to have died from blackleg should be not opened. Opening the carcass can liberate bacteria which with form sports that with contaminate the ground and subsequently infect other cattle [8]. Blackleg is a cause of severe financial loss to cattle raisers in many parts f the world. Outbreaks still occur occasionally in vaccinated herds but more frequently in herds where vaccination has been neglected [6].
Go to
Literature Reviews
Etiology
Clostridium chauvoei the causative agent for blackleg is an anaerobic, highly pathogenic, endospore forming and gram-positive bacterium, which produces lemon-shaped endospores and requires enriched media for growth [9]. The spores are highly resistant to environmental changes and disinfectant and persist in soil for many years and the organisms are typically pleomorphic. False blackleg may be caused by Cl. Septicum and Cl. novyi but this disease is more accurately classified as malignant edema. In 2013, the first draft genome sequence of a virulent C. chauvoei strain became known, consisting of 2.8 million base-pairs [10]. The relatively small genome of C. chauvoei as compared to other Clostridium species, such as C. difficile i.e. 4.2 million base pairs [11], reflects its adaptation to a restricted host range (bovine, caprine and ovine), where C. chauvoei can replicate and to cause disease [12].
C1.chauvoeiis motile and have peritrichaous flagella spores which are formed on solid media and in broth are oval, occurring central or sub terminal positions and distort the shape of the sell. They are resistant to the effects of boiling in water as well as to phenolic and quaternary disinfectants C1. chauvoei has high requirements regarding culture media and culture conditions under an aerobic conditions irregular vine leave stepped translucent or opaque the optimal in cubation temperature is 37°C.
Epidemiology
Source of infection
Blackleg is a soil born infection but the portal by which the organisms enter the body is through the alimentary mucosa after ingestion of contaminated feed. The bacteria may be found in the spleen liver and alimentary tract of the last soil and pasture may occur from infected feeds or decomposition of carcasses of animal dying of the disease. True black leg develops when spores which are lodged in normal tissue and proliferate by mechanism such as trauma or toxemia [6].
Mode of transmission: In sheep the disease is almost always wound infection. Infection of such wounds at hearing and docking and of the novel of birth may cause the development of local lesson. Infections of the vulvas and vagina of the ewe and rams up to year old, usually as a result of infection of skin would case by fighting. Occasional out breaks have occurred in sheep after vaccination against enterotoxaemia. Ewes exposed to infection at shearing develop typical lesion but ewes traded with penicilling are un affected except that the present ewe in the letter group shown distended abdomens, weakness and recumbence due to edema and gas formation in cattle mainly transmitted through ingestion of spores [6].
Occurrence of blackleg: Blackleg is primarily a disease of pastured cattle, although sheep may also be affected. It preferentially affects animals under two years of age, with most cases occurring in cattle from four to 24 months of age [13]. Occurrence of the disease is worldwide, although it tends to be localized, even to certain farms or to certain pastures. Because of this localization, it is assumed that C. chauvoei is soil borne, but likely does not grow in soil. The bacteria grow readily in the intestinal tract of cattle and may be recycled through fecal contamination of the soil. Once exposed to the environment, C. chauvoei readily forms spores, which may survive for long periods (many years) in the soil [14]. The disease occurs usual for a number animal to be affected within the space of a few days. The disease is endemic areas, especially when they are subject to flooding such as area may vary in size form group of forms to on individual field are created late in black leg approaches 100% [6].
Risk Factor
Animal risk factor: True blackleg is usually thought as disease of cattle and occasionally sheep but out breaks of the disease has been recorded in deer and in one case in a horse. In cattle the disease is largely confined to young stock between the age of 6 month and 2 years. In the field the disease appears to occur most frequently in rapidly growing cattle on a high plane of nutrition. Elevation of the nutritional status of sheep by increased protein feeding increases their susceptibility to blackleg. In sheep there is no restriction to age group [15].
Environmental risk factor: Typical blackleg of cattle has seasonal incidence with most cases occurring in the warm month of the year. The highest incidence may vary from spring to autumn, depending probably on when calves reach the susceptible age group some outbreak of blackleg in cattle have occurred following excavation of soil which suggests that disturbance in soil may expose and activate latent spores [8].
Pathogenesis
The detailed pathogenesis of blackleg is still somewhat uncertain, but many of the critical points in the following proposed sequence of events have been confirmed in the natural disease and in experimental infections in cattle [16]. The spores are ingested from soil, enter the gastrointestinal tract and, by hematogenous route, reach the muscle where the spores remain latent in cells of the mononuclear phagocytic system. The spores may remain latent in the muscle for years [4,17,18]. Transient trauma or ischemia of the muscle favors the germination of the spores and secretion of cytolytic toxins that cause necrosis of vascular endothelia (edema, hemorrhage) and myofibers. The toxins are absorbed into the animal’s bloodstream which makes the animal acutely sick and causes rapid death. Clostridial proliferation yield gas which appears as bubbles between the muscle’s bundles [19] (Figure 1).
Clinical presentations
Clinical signs of blackleg have been well-documented, but due to the sudden onset and often per acute nature of the disease, are not often observed in field cases [20]. The disease runs on acute, usually fatal course, and affected animals are often found dead before signs of illness have been observed. In some cases, there may be lameness or visible swelling of muscle groups. Any striated muscle may be affected, including the tongue diaphragm, and myocardium, but are shoulder and pectoral muscles are most often involved [21]. It should be suspected if an animal affected between 6 months and two years become lame with swelling of muscle, stops grazing appear sick a quietly goes down. How, these signs are usually of such short duration that they may be missed more frequently; unthrifty calf or yearling is simply found dead. Gas is detectable under the skin and his produces a crackling sensation when the skin is rubbed with the hand [8].
The rapid accumulation of gas under the skin and in the body, cavity gives the carcass a bloated appearance, with the limbs spread apart and pointing up words. There may be frothy, blood stained discharge from the mouth and nostrils. In Cattle, incubation period is 1-5 day. Sudden onset, Lameness, common. Marked depression, temperature normal when animal signs are evident. Edematous, crepitate, subcutaneous swellings over hips, shoulder, chest or back, Swelling, hot and painful initially later enlarge; become creping with cold, insensitive skin, tremors, prostration, the course of clinical disease is rapid, and most animals die within 12 to 36 hours of the onset of clinical signs [13].
In sheep, like cattle, but swelling usually occurs at wound site, Lameness primary symptom, swelling in perineum to pelvis following parturition [8]. In cattle the most obvious sign is crepitate swelling particularly in the hip or hindquarter which oracles when rubbed with the fingers as a result of large quantity of gas produced subcutaneously by the organism. In sheep an acute febrile condition develops within 1-2 days following an injury and atypical black quarter lesion can be observed near the site [22].
Postmortem findings
Cattle found dead of blackleg are often in characteristic position, lying on the side with the affected hind limb stands out stiffly. Bloating and putrefaction occur quickly and blood-stained froth exudates from the nostrils and anus. Clotting of the blood occurs rapidly. Lesions resulting from C. chauvoei infection are typically within the larger muscle groups of the limbs. The affected area is dark red, within which small areas of necrosis may be observed [23]. The muscle is typically dry and spongy, with small gas bubbles separating muscle bundles, with little edema centrally. Incision of the affected muscle mass reveals the presence of dark, discolored, swollen tissue with rancid odor on the cut surface and an excess of serosanguineous containing bubbles of gas. In some cases, the myocardial muscle and diaphragm may be the only tissues offered [24].
The following are some pathological changes associated with blacklegs in cattle; the carcass bloats and putrefies quickly after death, body cavities often contain excess fluid, often reddish in color, infected muscle masses are swollen, discolored and have a foul odor, in some cases a small muscle mass will be affected and lesions may be hard to find [25]. In locations such as the tongue, myocardium, and diaphragm, the lesion may be small and escape detection during postmortem examination, but still producing enough bacterial toxins to be lethal to the animal. All skeletal muscle of the body those of the lumbar region must be examined for evidence of the lesion, which may be small and escape carefully examination. All body cavities contain excess fluid which contain variable amount of fibrin and is usually blood stained. The solid organs show some degree of degeneration, and post mortem decomposition with the production of gas in the liver occurs rapidly.
Gross lesion
The gross appearance of the muscle varies with the age of the lesion. In the early stages the periphery of the lesion the muscle is dark red and markedly distended by serous or seroheamorrhagic exudates, which separates the fiber the cut surface is wet, and exudates may drip out. In the advanced stage, the center of the lesion is dry reddish black, and porous because of gas bubbles. In the control part of the lesion there is usually well-defined area of muscle which is dark red in color, dry, necrotic and filled with small gas bubbles which give a swollen appearance of the muscle. The lesion has characters rancid dour like that produced by culture of a chauvoei growing in cooked meat broth medium. Surrounding central area, the muscle becomes pinker ad there is variable amount of either yellow or blood-stained edematous fluid which is particularly obvious in the local connective tissue. Perineum lesion is ewes which have recently lambed includes neurosis of the vaginal mucous and skin, and extensive edema often involving the hind limbs and thigh muscles which are swollen and dark in color [22].
Gross changes elsewhere in the body are directly referable to either toxemia or proliferation of bacilli. Because of the pyrexia cadavers bloat rapidity and undergo rapid postmortem decomposition. Yellow subcutaneous fluid with or without gas bubbles may be associated with affected muscle. Pelvic, pectoral girdle, glutei, femoral, and hummer’s scapular muscle are frequently involved, but lesion can be presenting any striated muscle inducing hear trauma of the diaphragm, tongue and masticators muscle. Lesions may be very small and may be detected only if muscles are incised of not more than one cm interval. When the disease has resulted from infection of skin wounds the lesions are more obvious superficially, with subcutaneous edema and swelling, and involvement of the underlying musculature. When invasion of the genital tract occurs, typical lesions are found in the perinea tissues and in the walls of the vagina and occasionally the uterus. in the special case of pregnant ewes’ typical legions may involve the entire fetus and cause abdominal distension in the ewe [6].
Microscopic lesion
Heart muscle showed severe suppurative and necrotizing myocarditis with extensive necrosis. In addition, multifocal areas of suppurative inflammation were noted in the thymus, and mild colitis was observed. The essential are found in the skeleton musculature. Gas bubbles in the fixed tissue are indicated by spherical spaces separating fixed tissues are indicated by spherical spaces separating muscle bundles and facial. There are irregular areas of necrosis and collections of neutrophils and lymphocytes along the muscle speta, Edema are uncommon. Histopathologic examination of tissues from animals affected by blackleg revealed severe suppurative and necrotizing pneumonia and suppurative and fibrinous pleuritis [26].
Diagnosis
Clinical: The history of the disease and the symptoms may be strongly suggestive of blackleg but the final diagnosis must depend up on the selection of the causal organisms. CL. chauvoeican be readily demonstrated on films prepared from the lesion and from the edematous fluid [22]. In typical cases of blackleg in cattle a definite diagnosis can be made on the clinical signs and the necropsy findings. However, in many cases the diagnosis may be in doubt because may be confused with other acute clostridia infection with lighting strike and with anthrax though in the latter the characteristic splenic lesion is usually present in establishing diagnosis. When several animals are found dead kept under close observation one must depend on one’s knowledge of local disease incidence season of the year age group affected and pasture conditions and on a close inspection of the environment in which the animals have been maintained. Necropsy findings are most availed the carcasses are still fresh but, on many occasions, post mortem delay position is so advanced that little information can be obtained.
Lameness, depression, loss of appetite and a hot painful swelling on a limb which crackles when pressed may indicate blackleg. Later the skins over the swelling will be cold, dry and leathery. In areas where blackleg is known problem it should be suspected in cases of sudden death. Post mortem examination usually reveals, somewhere in the body an area of dark red dry muscle confirms by veterinarian, prefer by laboratory examination of tissues from affected animals. Presumptive diagnosis can be made by the characteristic gross legions and by demonstration of numerous single or, possibly, paired bacilli with rounded ends and occasional spores’ ear but not at the end of the occasional spores near but not at the end of the cell. As typical of clostridia, the spore is somewhat greater in diameter than the bacillus in which it forms the lesion must be differentiated from other clostridia infections of muscle particularly L. Septicum therefore, the diagnose should be confirmed by culture of use of specified immunological staining techniques [21].
Laboratory diagnosis: Sporulated gram positive rods can be demonstrated in smears of infected tissues and identified with immunofluorescent. Ground muscle in soil is cultured on blood agar plates which are incubated anaerobically. Because of the possible presence of swarming a septicemia early subcultures should be attempted from some plates with others last for 48hr identification by immunofluorescence or biochemical [27]. Mostly the organism will appear as gram positive rods when examined immediately following death of the animal, but after several hours the lesion will contain greater percentage spores and pleomorphic forms. Cl, chauvoei is a strict anaerobe and grows at high as 500c though the optimum is 37 °C. It will grow on the usual laboratory media but is best cultivated in meat or brain medium. These are never discolored nor digested by pure cultures, but they may be slightly softened. Muscle necrosis is extensive and associated with gas bubbles hemorrhages [28].
Isolation and culture: The organisms may in cases be isolated in pure culture directly from the tissues infected. Growth in culture Medias quite dependent up on the presence on carbohydrates for the best growth soda content beyond neutrality is advisable. Body fluids or tissues except as they may act as reducing agents or contain carbohydrate don’t increase suitability of media containing the. The colonies are spherical or somewhat irregular, which microscopic radiator. In all cases of suspected black leg smears of affected tissue should be made and material collected for bacteriological examination. Pasteur pipettes from muscle tissue and heart blood, and secretion of muscle removed aseptically are suitable simmers for laboratory examination. The isolation and identification of the causal organisms from muscle lesion is difficult because of the rapidity with clostridia invade the tissues from gestor intestinal tract after death and of certain bacteriological species such as Cl, chauvoei and CI. Novyi [6].
Differential diagnosis
Anthrax: Anthrax is a hemorrhagic per acute disease and the clinical sign is sudden death. Dark tarry discharge from body orifices, absence of rigor mortis, enlarged spleen, degeneration of the liver and kidneys are characteristic postmortem findings in anthrax.
Malignant edema: This disease, commonly called stable blackleg, is very similar to blackleg. In fact, the similarity is so close that often a diagnosis can be made only when the specific bacteria are identified in the laboratory. Furthermore, both organisms may be present in the same outbreak, or even in the same animal. Malignant edema does differ from blackleg in some respects. It is caused by bacteria called Clostridium septicum. It is more common in older animals and is more likely to occur during the winter months than blackleg.
Heart water: Caused by Ehlrichiarumminantum the suddenness of death and the presence of hydro pericardium in sub-acute cases the disease however, demonstration or ehrlichia bodies in the endothelium cells of blood capillaries in the brain and Jugular vein, demonstrated presence of the Amblyomma ticks. Snakebites was also one of the diseases we should have to differentiate from blackleg, since it’s a sudden death with lack of clinical signs and occasional per pharyngeal and brisket oedema, can be confused with sub-acute disease. Bites on the muzzle, head and neck are more likely acute systemic sign and death. It is possible to see the marks from the bite and often local swelling tissue discoloration and hemorrhae at the sight or the bite are suggestive of snake bite poisoning [29].
Treatment
Treatment of affected animals with penicillin and surgical debridement of the lesion, including fasciotomy, is indicated if the animal is not moribund. Recovery rates are low because of the extensive nature of the lesions. Large doses (44,000 IU/kg BW) should be administered, commencing with crystalline penicillin intravenously and followed by longer-acting preparations. Blackleg antiserum is unlikely to be of much value in treatment unless very large doses are given [30]. According to [31]; treatment of clostridial myositis is rarely successful due to the rapid course. Antimicrobials (drug of choice procaine penicillin) around affected tissues, aggressive surgical debridement to allow aeration along with supportive treatment can be of value. Majority of cases show poor prognosis. Treatment of affected animals with penicillin is logical if animal not moribund but results are generally any fair because of the extensive nature of the lesion. Large dose should be administered, commencing with crystallin penicillin intravenous and followed by longer acting preparations, some of which should be given in to the affected tissue if it is aquesible. Blackleg antiserum is unlikely to be of much value in treatment unless very large does are giver [6].
The speed which blackleg kills usually make individual treatment useless in some cases, however, animals treated early with antibiotics may survive, although they often suffer permanent deformity due to partial or complete destruction of muscle. Usually of little practical application after symptoms are observed, remove necrotic tissue, administer adequate dosage of penicillin and formalized toxoid [8]. Treatment is often disappointing penicillin should be given intravenously at first followed by repository form intramuscularly, if possible, in to the affected muscle. Antibiotic treatment of affected animals is likely to be effective only if commenced early large doses of penicillin should be administered intravenously followed by longer acting preparation, some of which should be given in to the affected tissue. However, because of the extensive tissue involvement, even if the infection is eliminated the subsequent muscle loss is great economic value [6].
Controls and preventions
If the antibiotics are not given new cases of black leg may occur for up to 14 days unit immunity develops, and constant surveillance and the early treatment of cases will be necessary [32]. On farm where the disease is endemic annual vaccination of all cattle between 6month and two years of age should be carried out just prior to the anticipated danger period usually spring and summer. Vaccination of calves at 3 weeks of age has been recommended when the incidence of the disease is very high movement of the cattle from the affected pasture is advisable. Bacteria prepared from C1. Chauvoie is preferred. The improvement to be expected would be greater still if the toxin composition of each isolate where known rather than its identifying antigen city. Cattle are vaccinated at 3 to 6 months of age and annually thereafter. Vaccination should precede exposure by at least 2 weeks. It is not possible to prevent clostridial bacteria from being present in the soil, but it is possible to vaccinate animals to prevent the occurrence of the disease. The most effective means of prevention is proper vaccination program. Multivalent vaccine is suggested he first does should be given at two months of age, and a second infection at either four weeks before pre-weaning or at the time of weaning. If animals are in an endemic area another boaster should be given [33].
Attenuated organism is also used in the preparation of vaccines for use in cattle and some attenuated strain of bovine origin or recently isolated, virulent, ovine strain may be used to prepare vaccine for use in sheep. To administer a polyvalent vaccine highly recommended for the extra protection acquired at very little extra cost. Large number of spores which can spread by wind, rain and scavengers. Blackleg vaccination should be routine procedure on all properties in areas where the disease is known to occur. The vaccine be injected under the skin on the side of the neck ensuring that the infection does not go in to the muscles.
Large number of spores which can spread by wind, rain and scavengers. Black leg vaccination should be routine procedure on all properties in areas where the disease is known to occur. Susceptible cattle which in endemic areas must be vaccinated cattle groped on flood- pains or along water courses also should be regularly immunized because of the risk that infection may be introduced with car cases of dead cattle, which may be deposited during flooding. Beef calves are usually vaccinated when they are branded an ear marked, usually at one or four months of age. A booster vaccination administered a month or so after weaning, is generally enough to protect until age immunity supervenes at approximately 24 months of an age. Calves vaccinated before 3months of age should be revaccinated at four to six months of age and again at weaning [34].
Vaccination techniques and vaccinations break downs
The vaccine should be delivered just under the skin not in to the muscle. Draw pinch of skin and insert the needle between the skin and the muscle. The loose skin of the neck is convenient. Do not save unused parts of bottles or containers of vaccines for future use, as they can become contaminated with undesirable organisms and/or lose their potency. Destroy and vaccine not used within 24 hours of opening [35]. Modern vaccines are produced under conditions of strict quality control by reputable manufactures. Occasionally, reports are received of apparent failure or vaccines. When investigated, most of these vaccination failures due to: In correct dosing, faulty technique, using time- expired vaccine, vaccine having been subjected to high temperature during storage or transportation.
Go to
Disease Status in Ethiopia
Blackleg is endemic disease in Ethiopia, outbreaks occurring in warm season. Most of the time, when outbreaks occur ring vaccination is given to the herd, there is no any research done in the country based on case morbidity and mortality rate. It is highly prevalent in Dega followed by Weinadega and kola [36- 40] (Table 1).
Go to
Conclusion and Recommendations
Blackleg is a disease of young, rapidly growing cattle which may cause the sudden loss of a significant number of animals. Effective vaccines are readily available which should be given routinely in all areas. Blackleg has been found in cattle as young as 2 months old, most losses occur in cattle between 6 months and 2 years of age, man not considered susceptible to this disease, however, extreme caution should be taken when working with dead or blackleg suspected animal. Blackleg is a cause of sever financial loss in many parts of the world. For the most part major out breaks are prevented by vaccination but out breaks still occur, where vaccination has been neglected. Based on the above conclusion the following recommendations are forwarded:
a. Animals must be vaccinated against blackleg to avoid loss.
b. Veterinarians must diagnose the disease clinically or in laboratory and administer appropriate drug to save the life of animals.
c. When outbreaks occur, the society must inform to veterinarian or any authority in the area and veterinarians must go to the area and rule out before giving vaccine whether the outbreak is blackleg or any other disease.
d. The government should distribute enough doses of blackleg vaccine and drugs as well as well-trained veterinarian to the society.
e. The society should be educated to burn or bury body of dead animals without opening or immediately inform to vet officials if possible.
f. Further study should be conducted on the prevalence, of blackleg in cattle in Ethiopia.
To know more about journal of veterinary science impact factor: https://juniperpublishers.com/jdvs/index.php
To know more about Open Access Publishers: Juniper Publishers
0 notes
Text
Aquacare set to celebrate 10th anniversary
Coastal Point photos • Tyler Valliant: Aquacare physical therapist Lauren Nuttle demonstrates her skills on fellow employee Elizabeth Kim.After 10 years in its Millville location, the staff at Aquacare Physical Therapy continues to expand its “menu” of services.
“We offer both ‘surf’ and ‘turf,’” said physical therapist Lauren Nuttle — referring to the pool-based aquatherapy available at Aquacare, as well as the “land-based” therapies offered there, too.
While the aquatherapy is obvious from the name, Nuttle said, the office offers more traditional physical therapy techniques, as well as some new ones that have just come into use in the past several years.
Nuttle said she loves the breadth of services offered at Aquacare because “I don’t have to tell someone, ‘Oh, we don’t have that here,’ or ‘We can’t do that here.’” The depth of the services allows staff at Aquacare to accept a wide range of patients, Nuttle said.
She recalled one favorite patient who had suffered several broken bones in a motorcycle accident. Thanks to the availability of the pool for therapy in which his body weight was supported — a person submerged up to his neck in water feels a loss of 90 percent of their body weight — he was able to start therapy there and follow through all the way to his complete recovery.
“We can serve every age range and every patient level,” she said, adding that the motorcycle crash patient is now back to his regular routine of hardcore gym workouts.
A technique called “dry needling” (also known as myofascial trigger-point dry needling or intramuscular stimulation) is the use of either solid-core or hollow-core needles for muscle pain treatment. The needles are inserted through the skin into specific areas of the muscle, known as trigger points.
Nuttle herself has been a dry-needling patient and said it helped her when rotator cuff spasms made any arm movement painful, with the therapy restoring her ability to raise her arm straight above her head.
Dry needling has been used in Delaware since 2009; Delaware’s legislature became the 29th state in the nation to regulate its use in physical therapy in 2014.
Aquacare also offers treatment for pelvic issues in both women and men and is the first physical therapy practice on Delmarva to do so. Pelvic-floor issues aren’t talked about much, Nuttle said, and often people suffer in silence because either they don’t know there is treatment or they have concluded that their symptoms are normal.
“You shouldn’t have to plan your vacation around where the restrooms are,” Nuttle said simply.
Aquacare offers high-tech applications for pelvic floor issues that help patients gain better understanding of their own bodies, which ensures that treatment is as effective as possible.
Another recent addition to the services offered at Aquacare extends beyond the human species to canines that need physical therapy. Nuttle, who has received special training in canine physical therapy, said it’s a specialty that requires a certain ability to understand non-verbal cues from patients — either human or canine.
When a dog is in pain or discomfort, Nuttle said, “They can’t tell you. But they do…” — it’s simply a matter of knowing how to read the non-verbal cues. Canine physical therapy also involves quite a bit of owner education, she said. The educational process emphasizes the importance of owners thinking about their pets’ health in terms of their needs for healing, rather than what their pets seem to want to do.
That’s the big difference between human physical therapy and canine physical therapy, Nuttle said. As an example, she said, “When an older dog with a bad hip still wants to go get that ball,” owners need to remember not to throw the ball as far, at least not initially. Another example: Just as people often remove throw rugs to reduce the tripping risk for senior humans, they should do the same for dogs, Nuttle said.
The most common reasons for veterinarians referring pets to Aquacare include weight management and osteoarthritis management, Nuttle said. Referrals are not necessary for dogs to be treated at Aquacare; however, she emphasized that if there has been a traumatic injury, the dog needs to be seen by a veterinarian.
Nuttle said canine physical therapy is not something that every physical therapist can do, or wants to do, but that she has enjoyed the addition of the service to the Aquacare facility for the past three years.
“It’s been very rewarding for me,” she said.
The Millville Aquacare facility is one of 10 Delmarva locations; the others are located in Seaford, Lewes and Millsboro in Delaware and Berlin, Annapolis, Salisbury (two locations), Easton and West Ocean City in Maryland. The first Aquacare facility was opened in Salisbury in 1998.
In the past year, Aquacare has also formed a partnership with Atlantic General Hospital and Berlin gastroenterologist Dr. Gerald Canakis, to offer the pelvic-floor help for both women and men.
The public is being invited to celebrate their 10th anniversary with Aquacare from 2 to 6 p.m. on Thursday, April 6, when the staff will welcome visitors with gourmet appetizers and cocktails, complimentary massages by staff members, door prizes and a grand prize of a free 12-month pool membership.
Aquacare staff will also host a series of demonstrations and free sessions during the event. They are:
• 2-3 p.m. — Free water aerobics class (call to register);
• 3-3:30 p.m. — “Bottom Line on Kegels,” a women’s health discussion by physical therapist Malisa Ochotnicky;
• 3:30-4 p.m., “Am I Dizzy or Just Unsteady,” a balance program by physical therapist Donielle Brasure;
• 4-4:30 p.m. — “Physical Therapy for My Dog,” a canine therapy program introduction by physical therapist Lauren Nuttle; and
• 4:30-5 p.m. — “Oww… My Muscles Hurt!” a dry-needling demonstration by Nicole Evans, physical therapist.
At 5 p.m., there will be a ribbon-cutting and “alumni picture,” in which all past patients are invited to participate.
Aquacare Physical Therapy is located at 38069 Town Center Drive, Unit 15, in the Millville Town Center. For more information on services, call the office at (302) 539-7237 or visit their website at www.aquacarephysicaltherapy.com.
from Coastal Point - Dollars & Sense http://www.coastalpoint.com/content/aquacare-set-celebrate-10th-anniversary_03_30_2017-0
0 notes
Last Seen Blogs

torpy-pony
Torpy Ponius

poisonatthedisco
frank iero whore

myflowerdeer666
Myflowerdeer

sertanejou
Só Sertanejo