#maybe it's the pediatric onset mental illness
Text
idk I don't think it was love and trust that created the current calamity, and I don't think anything they've done in meursault or at the airport has been futile. I don't think the themes fall apart when they're challenged, I think they're reinforced, which is as evidenced by Fukuzawa cradling Aya as it is by Akutagawa asking Atsushi if they need anyone else.
#bsd#bungou stray dogs#idk how you spin this as a failure#maybe it's the pediatric onset mental illness#but the point of love and trust and allies and souheki is not to negate flux#its to be able to tuck and roll when the next wave hits#if catastrophizing sparks joy then go for it#but i think it lacks punch and weight in context
254 notes
·
View notes
Text
Published: Mar 30, 2023
For over a decade, the Gender Affirmative Model has been the standard of care for gender dysphoric youth across the West. Yet, despite its widespread and long-standing use, good evidence to support it remains elusive. Maybe that’s because there isn’t any.
A new paper reports on results from a survey of 1,655 parents of children who developed gender dysphoria during adolescence or soon after. American Academy of Pediatrics guidelines recommend affirming these kids in their new gender, and supporting them along the path to social, medical (hormonal), and surgical transition.
The results of this survey provide strong support for Dr. Littman’s Rapid-Onset Gender Dysphoria (ROGD) hypothesis, which suggests that gender dysphoria in this group may resolve with time and good psychological and social support, if needed.
Key Findings
Key findings of particular concern are that these children tend to have emotional problems that predate their gender-related issues by nearly four years. Furthermore, children with mental health issues were more likely than those without to have taken steps to transition. Children who were referred to a gender specialist were also more likely to have taken steps to transition. Parents reported feeling pressured by these specialists to transition their child. And parents reported a decline in their child’s mental health and social functioning after transition.
History of Gender Dysphoria and Standards of Care
About 15 years ago, Western countries began experiencing an exponential rise in adolescents and young adults suddenly developing gender dysphoria and being referred to gender clinics for treatment. Around the same time, a new philosophy on transgenderism began to take root: Just as there is nothing wrong with being attracted to the same sex, there was nothing wrong with identifying with a gender that did not match your biological sex. In other words, being transgender is perfectly normal. It is not a mental illness. If a trans person does have any mental health issues, it can be attributed to the extreme distress of having to live in a body that does not feel right (gender dysphoria), and the stress of living in a judgmental, transphobic world.
Out of this philosophy grew the Affirmative Care Model. This model focused on reassuring (affirming) people that their gender identity was real, normal and natural, and helping them take steps to relieve their gender dysphoria through social, medical (hormonal) and surgical transition. In order to address their social distress from lack of acceptance, much effort is devoted to creating a supportive environment among friends, family, schools and society in general.
Although there was almost no evidence to support it at the time, the Affirmative Care Model quickly became the standard of care in most Western countries.
In 2016, Dr. Littman noticed an anomalous spike in teenage girls suddenly declaring themselves transgender and became concerned. She conducted a survey of their parents to learn more about this new phenomenon. Based on what she found, she proposed that a new sub-category of gender dysphoria had emerged, this one sharing more similarities with anorexia and other eating disorders than with the previously recognized types of gender dysphoria. Dr. Littman described Rapid Onset Gender Dysphoria (ROGD) in her seminal paper published in 2018.
ROGD develops suddenly, during or after puberty in a person who would not have met the criteria for childhood gender dysphoria. Most often, these kids are white, highly intelligent and come from well-educated families. ROGD affects mainly girls, and groups of friends often come out as trans together. The influence of social media is believed to play a role. They often have a prior history of mental health issues, developmental difficulties or have experienced a traumatic or stressful event before developing gender dysphoria. A prior history of self-harm and difficulty fitting in with their peers are also common. Sadly, transitioning is not likely to help these kids with their issues as it does not address the root cause. In fact, it has a good chance of making things much worse.
The ROGD hypothesis suggests that for these unhappy kids, “gender dysphoria” is a catch-all phrase for any kind of distress, and transition is the cure-all solution
Since the publication of Littman’s paper, the ROGD hypothesis has come under fire from proponents of the affirmative care model. It’s easy to see why: The affirmative care model is based on the premise that being transgender is perfectly normal. The ROGD model suggests that this particular kind of gender dysphoria – and the desire to transition – is most definitely not normal. It’s a maladaptive coping mechanism.
Unfortunately, there is little evidence to support either hypothesis.
The World Professional Association for Transgender Health’s newest Standards of Care, published in Oct. 2022 admits, “A key challenge in adolescent transgender care is the quality of evidence evaluating the effectiveness of… gender-affirming medical and surgical treatments.” “The number of studies is still low and there are few outcome studies that follow youth into adulthood.”
Testing the ROGD hypothesis presents its own challenges. In North America, gender clinics are still using the affirmative model as a standard of care, which views taking steps to transition as medically necessary and thus, would be unwilling to test the ROGD model. Further, ROGD has become such a contentious topic at universities that any academic who broaches the subject risks career suicide. Just ask Dr. Littman and Dr. James Caspian.
Survey Results
Concurring with Dr. Littman’s findings, our survey indicates children who are most likely to develop ROGD are of European descent (78.9%), with above-average intelligence. They are also more likely to be female (75%). Their gender dysphoria develops around the age of 14 for girls, and 16 for boys. This may be partly due to the fact that boys go through puberty later than girls.
Their parents are more likely to be progressive and hold positive views towards LGBTQ+ rights. Frequently, parents went out of their way to make sure the reader understood this when they told their stories. Many had family and friends in the LGBTQ+ community, and some were members themselves. They just didn’t feel it made sense in their child’s case.
A majority of these kids were dealing with mental health issues (57%) that began around the age of 10, well before they developed gender dysphoria, and 42% of them had received a formal psychological diagnosis. The most frequently-reported issues were anxiety and depression. Self-harm was also prevalent in girls. Attention deficit disorder, autism, and obsessive-compulsive disorder were reported in numbers higher than the general population.
Very often, these kids had experienced a stressful event before they developed gender dysphoria (72.6%). Some described issues that would be overwhelming even for an adult to deal with, such as the suicide of a close relative, receiving a serious medical diagnosis such as cancer, being sexually assaulted, or being present at a mass shooting. Sometimes, the stress was more mundane, like moving, breaking up with a girl- or boyfriend, or having a good friend turn on them, but the child was having a hard time dealing with it. During the lock downs due to COVID, the strain of isolation was especially hard on these kids.
Parents also reported that their kids were having a lot of trouble fitting in with their peers at an age when being accepted feels like the most important thing in the world. Only about a quarter of parents reported that their child was well liked, and only one third said their kids got along well with other kids.
Parents reported their kids spent an average of 4.5 hours per day on the internet and social media.
When asked whether their child had friends who came out at the same time, 60.9% said their daughters did, compared with only 38.7% of their sons. The average number of friends who came out were 2.4.
“My daughter used to be so lonely her only friend was her guinea pig. At 11, a girl at school befriended her as did her group of friends. All of a sudden, my daughter said she was bi, then gay, then pan, then poly, then fluid, now trans. Her mental health is deteriorating and the psychiatrists (this is her 6th) seem to push their own agenda and label me transphobic. I KNOW my daughter. When no social group will welcome you and one finally does, you’ll conform to fit in, to not lose the only ‘friends’ you have.”
~Parent of an ROGD Kid
Transition
The majority of the children had socially transitioned at the time parents completed the survey (65.3%), and girls tended to socially transition earlier (age 15) than boys (age 17). In general, parents reported that their children had not started taking puberty blockers or hormones, and surgery was especially rare.
Girls who had friends who socially transitioned were more likely to do so themselves (73.3%), compared with only 39.5% of boys who were more likely to transition if they had a friend who did so.
One very concerning finding was that children with preexisting mental health issues were also more likely to socially transition than those without. This is worrisome, because children with emotional issues may lack the judgment needed to make serious, and sometimes irreversible, decisions about their bodies.
Another troubling finding was that children who received a referral to a gender specialist were more likely to have transitioned. This is especially concerning because 51% of parents who took their kids to a gender specialist also reported that they felt pressured to transition their child.
Effects of Transition on Mental Health and Social Functioning
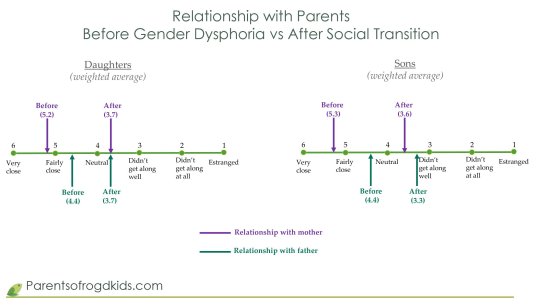
When asked about the state of their child’s mental health after social transition, they were much more likely to say it had worsened than improved.
Sadly, the change in the quality of the parental relationships also declined, as shown in the table below:
Conclusion
The results of the largest survey to date on gender dysphoric adolescents support Dr. Littman’s ROGD hypothesis. These youth are most likely using “gender dysphoria” to describe general feelings of dysphoria that they have no other name for, and do not understand. Transitioning will not help them. It can only cause irreversible harm and make things much worse.
Sweden, Norway, Finland, the UK and some States are backing away from the gender affirmative model, citing the lack of evidence and amid the growing number of detransitioners, many of whom are launching lawsuits against the gender specialists who harmed them. (See Ritchie Herron and Keira Bell, Michelle Zacchigna and Chloe Cole.)
Yet here in North America, the United States and Canadian Governments, the American Academy of Pediatrics and most other medical associations, are doubling down on the gender affirmative model.
If they truly want to “do no harm”, then they must follow Sweden’s lead and stop transitioning minors.
==
This should be good news. We have good reason to believe that distress can be resolved by treating the underlying cause, rather than through invasive and irreversible hormones, drugs and surgeries. How can this be a bad thing?
Because it's not about helping distress; if it was, they'd applaud the best treatment that causes the least harm. But it's about using anxious kids as pawns to remake society according to Queer Theory.
#Michael Sherman#Lisa Littman#Rapid Onset Gender Dysphoria#ROGD#social contagion#mental health#queer theory#gender ideology#medical transition#gender distress#gender dysphoria#mental health issues#mental health care#religion is a mental illness
94 notes
·
View notes
Text
OCD Subtypes for the RPC
Part 1 is here
Well well well, we are back for Part 2 of the Roleplayer’s Guide to OCD.
Fellow Ocd Folks, I see you in those tags and I'm going to do my best to ensure those obsessions are represented here- BUT understand that physically it is not going to be possible to list every single one because I am one person. Regardless its incredibly brave of you all to rb and add things in the tags, I know its hard to talk about this shit and I see you. I see you.
Resultantly I typed this out and posted it in formatting to assist with accessibility in mind; if you cannot read it still ( I tried Im sorry!) i recommend the copy and paste method or getting the chrome extension bee-line reader.
There will be grammatical and spelling mistakes. Im sure spacing is odd some places, but you have to understand doing this is extremely anxiety provoking for me so Im just getting it done when I can.
Remember to use your critical thinking; not everyone has the same symptoms/compulsions/triggers and all that.
OCD is fluid. Its like liquid mercury. One day its a handful of subtypes another day its another different serving.
If you are in general squicked about certain topics even by mention read ahead with your own judgement. Remember us folks that have OCD have many disturbing and distressing experiences so if you are writing a character who has OCD and you can’t read about it just don’t give them that obsessive thought/ compulsion. Make sure writing is still a safe and enjoyable hobby for yourself first and foremost.
But ethically and morally I cannot and will not leave out the more disturbing bits. You have the ability to scroll by, I and many others do not get the chance to escape triggering content that our own mind creates.
So read ahead with your best judgement or at least skip around the squicky parts and educate yourself on what OCD is so people quite using it as a Obsessive Christmas/Corgi/Cat Disorder thing. Alright? Cool beans.
Okay so you made it passed post 1 and got under the read more. Give yourself a gold star for diving into this monster of a document.
Below is a crash course it is not meant to replace actual psychoeducation, personal research, or google. Honestly most of us do our research extensively but because OCD is treated so horribly by social media, media, and society in general.
I wasn’t sure where to throw these together because the education tools to learn fully about OCD are very specialized and thus very restricted. I found that many people DO have these experiences with OCD though so I will represent them throughout. I’ll also sprinkle some of my own experiences so you can get a good reference of a person who has the disorder and not just a randomly generated person.
--------------------------------------------------------------------
So OCD is made up of Obsessions, Trigger, Intrusive thought, Misinterpretation/feared consequence,Somatic and Psychological Anxiety, and Compulsions/Rituals.
Your character may not be able to list all of these. In fact if they aren't in ERP therapy they may not be able to puzzle these things out. But YOU as the writer should know them. Your character won’t be walking around talking to just ANYONE that they have OCD. Remember a huge aspect of OCD is it’s Shame. The disorder makes us feel intense shame regarding our intrusive thoughts, as a result OCD goes undiagnosed for years especially if it has pediatric onset.
We won’t tell anyone what we are experiencing or why we are doing x y or z. We act like nothing is wrong because to emotionally react is to admit to yourself- and therefore the world- that you have had this intrusive thought and are therefore by virtue a horrible person.[For further information I would suggest also researching PANDAS].
It may be noticeable if your character has an intrusive thought. They may wince or grimace or roll their eyes certainly, but they won’t open up to Joe at the cafe about how their brain is constantly torturing them. I apparently have a very noticeable eye twitch.
Depending on the nature of the intrusive thought it will get more or less of a reaction out of me. Its usually dependent on how distressing the intrusive thought is and/or if its a new one.
----------------------------------------------------------------------------------------
You see OCD doesn’t sit still. It never looks the same. You’ll have your long haul intrusive thoughts that are with you for years but then you’ll have weird ass ones that just appear and demand their voice be heard yelling about cars hitting people or squirrels getting eaten.
Some people have similar ones! So while everyone is different there will always be someone out there with an intrusive thought similar to yours.
For instance; I bonded emotionally with a lady on reddit because we both have intrusive thoughts during storms that animals and the homeless are dying. We were both horribly relieved to find another person and also distressed that every snow or rain storm brings horrible images and whispers to your mind that while you are warm and snug in bed someone is freezing to death. And its all your fault.
Some days are better than others. As with all mental illnesses it isn’t CONSTANT ALARM BELLS. Some days it will be all alarms and other days it will be like a gentle whisper on the breeze. You can almost not notice it. Almost.
Obsessive thoughts run the gauntlet from ‘i will/could have/may/may accidentally harm etc’ something that you hold of value. This is any obsessive thought that you have: you think about repeatedly and not by choice, it is very anxiety provoking, it is unwanted, and unwelcome.
Mine run the scale from ‘squirrel will be murdered’ to ‘being responsible for harm’.
Compulsions or ‘rituals’ are any behavior done to alleviate the anxiety from the intrusive thought and trigger object. In short, compulsions and rituals are not fun. they are absolutely not logical, and we know they are not logical but we are forced to do them. Thats why its a disorder.
-------------------------------------------------------------------------------------
To emphasize from post 1: magical thinking and the faulty link between thoughts and actions are hallmarks of OCD. Magical thinking can be anything from contamination to if I turn around three times or stare really hard at something the bad thing wont happen. Sounds weird and is weird and we know it is thats why its a disorder and not a delusion.
The faulty belief that thought=action is the biggest hurdle it is incredibly difficult to grasp, at least for me maybe some of you that have done further ERP can attest, that the mere concept of a thought not being the same as an action is completely and totally mind blowing.
Free will? Yeah thats terrifying. IDK about anyone else but free will is absolutely terrifying; what do you mean i could do anything i wanted?
Thats how you face OCD(WITH A TRAINED THERAPIST). You give in to ambiguity and the unknown. Its breaking that link between thought and action. Its incredibly difficult and draining. A five minute exposure leaves me in shatters for a week and two five minute ones had me ripping my nails past the nail beds with anxiety.
--------------------------------------------------------------------------------------------
Just a reminder: Do not have your character expose themself or expose folks with OCD to a trigger to “ help us get over with”. That is literally forcing someone with a mental illness into a break down and is not helpful. In fact its worse because a person knows about this intrusive thought and they tried to make it real. More shame and some trauma.
If you have OCD, more likely than not a family member or significant other has tried this with the purest of intentions. But it never works like that. Theres a reason that therapists get special training for this. If people want a post on ERP I can make one at some point.
------------------------------------------------------------------
Actually let’s drag me with the squirrel thing as the example- fellow OCD Folks get out a pen and paper and try breaking down one of yours;
Obsession:Squirrel will be murdered
Trigger: seeing a squirrel
Intrusive thought: Graphic images of a squirrel being murdered by a hawk/ impaling depending on the day
Misinterpretation/feared consequence: Squirrel will be killed and its all my fault
Somatic and Psychological Anxiety:intense anxiety, palms sweating, heart racing,
Compulsions/Rituals: Must stare at the squirrel to prevent bad things from happening,
Now imagine if that is every time you see a fucking squirrel. You have somehow become completely and totally transfixed on a squirrel and nothing is going to pull your attention away or the squirrel dies- which your mind is giving you lovely images of btw.
Cute right?
-----------------------------------------------------------------------------------------
Below are the subtypes with general information/example thoughts/ and how some of these have impacted me socially because apparently some people dont understand that mental illnesses impact their social lives?? yall...
Social: This can range from ‘ i am constantly thinking i did something wrong so i have to ask for reassurance that we are still friends’ to completely unrealistic worries. Maybe its an intrusive thought that ‘ your voice is annoying them’ . There’s reassurance seeking, internal and external checking.
It makes friendships extremely difficult and exhausting. You’re not trying to get to know someone with an annoying frat boy egging on anxiety in your brain. This can also manifest as having strict rules for yourself and ethical codes.
My therapist likes to say she could give us (folks with OCD) a pile of hundred dollar bills and come back and they’d all be returned. Because OCD makes you so strict and morally confined. Which ISNT fun. Like I dont get pleasure over having to memorize the entire Code of Conduct!
Social Media: Its the bane of human existence some days and a lifeline the next. But what if everytime your follower count was an odd/even number it sent you into a panic attack. What if you spent all your time with intrusive thoughts that somehow someone misinterpreted a post or that someone is going to be harmed by a post you made about tapirs.
You may be forced to block people to get your number down or keep pornbots on your blog to keep your number what you like (see there is a use for them! We sacrifice those before actual users!) You may be refreshing your page every second because ‘what if you miss a message’. It's going to look a lot like ‘check check check check reassure yourself double check your posts check check check reassure check check FALSE MEMORY check your post etc’
--------------------------------------------------------------------
Clothing/Body Image: When its not Body Dysmorphia it can be OCD. Sometimes this looks like I obsess about a body part and therefore I choose my clothes/hairstyles to hide those. Some personal examples: as a kid I was sure that mind readers exist ( THIS IS AN OCD THING TOO I was so relieved to find that out) and that if i didnt wear a particular hat they would see all these horrible thoughts and it would be revealed what an awful person I was. So I wore the same dumb ass bucket hat for a year (or more I cannot remember but it was a long ass time).
I was once so fixated on being given a compliment on my eye color that I wore sunglasses (even at night) to a summer camp. And if any of those teen girls in that cabin that stood up and mocked me in a crowded lunch hall by singing ‘i wear my sunglasses at night’ you all owe me 40$.
Even younger still I had intrusive thoughts. Like say, if anyone noticed I was female that i would be kidnapped so I chopped my hair very short. I altered my appearance to be very androgynous and even switched to walking more masculine. Because omg if your hips move someones going to kill you thats just how it works. ( It doesnt help I later figured out I was a lesbian)
Your wardrobe may be impacted by OCD and yes so can your body image.
--------------------------------------------------------------------------------------
Also yes the fear of mind readers is also a thing; i always thought I was somehow faking OCD because yes that is also a…..
Faking: Do you value telling the truth? Do you detest lying ? Boy Howdy do I have some news for you. OCD is going to try and convince you that YOU LIED. Whether it was on a chastity pledge to get a free sandwich or in a conversation you just HAD. This links a lot with false memory OCD.
Another aspect is OCD makes us doubt we have OCD and tries to convince us we have any other diagnosis under the sun and we are obviously faking our OCD.
------------------------------------------------------------------
Sexual Orientation OCD; It is as it is called. Sexual Orientation OCD is what happens when your brain goes ‘hold on what if you’re not this orientation what if you are THAT’. It doesn’t matter where on the LGBT umbrella you fall you will have OCD trying to convince you otherwise. From compulsive staring at members of the same/opposite gender to compulsively reassuring or checking with yourself to ensure that ‘ no no you are in fact THIS orientation.’
This can range in behavior from binge watching porn, staring compulsively to check that there is OR is NOT attraction,self checking past experiences and memories, analyzing your clothing and your lifestyle in painful and intricate methods.
-----------------------------------------------------------------------------
False Memory OCD; False memory OCD is basically your brain sitting you in a noir interrogation room, handcuffing you to a chair grilling you. It demands that you did *insert bad thing here*. This can range from anything from something Harm based to pretty much *anything* from other OCD subtypes. Which is quite delightful really.
---------------------------------------------------------------------
Sensorimotor OCD; Sensorimotor OCD is obsessive body responses. These can be ‘ I have to cough really hard and really feel it right in my chest and if I can’t get it right I have to cough until I do’. This can be counting your heartbeats. Trying to check yourself that you in fact have a heart and checking and reassuring that it is still beating. It can be hyper-awareness of swallowing or even swallowing repeatedly. It is anything with selective attention; ie its an automated process but your OCD is forcing you to be aware of it.
Your OCD makes you aware of the sensation of, say, breathing, and then it convinces you that if you stop paying attention to it you will stop breathing. So now you’re horribly aware and focused solely on breathing and breathing alone. It keeps me up most nights with the pounding anxiety fueled by the pressure of ‘if you stop focusing on breathing you will stop breathing completely’ or waiting to feel that last heartbeat in your chest.
---------------------------------------------------------------------------
Existential OCD; You ever feel existential ? Existential OCD is like having a very aggressive existential crisis that turns you into NEEDING answers IMMEDIATELY. This can look anything from hours panic scrolling the net to panic inducing anxiety because you don't know what happens after death. The thoughts are like foghorns on a misty sea.
This sounds basic and the only example i can give is as a teeny tiny 7 year old I had a panic attack in bed screaming that ‘ what if im a dinosaur and im asleep and i wake up and my whole family is GONE’.
To be fair I did like dinosaurs a lot.
------------------------------------------------------------------------------
Harm OCD; This is pretty self explanatory but I will give more details. Harm OCD is OCD demanding that you will/could/can/may have/might harmed yourself/others/any living creature and that you alone are responsible.
This means anything from getting anxious driving over crosswalks because ‘what if you dont see one and hit someone and its all your fault and you hit someone go back and make sure you havent hit anyone’ to ‘im holding a knife so im going to accidentally stab someone’ to ‘ i didnt see my cat this morning and now im at work and think she must be dead and i am responsible for her demise.’
It can be as simple as ‘if i use a pencil i will stab myself in the eye’ or as complex as ‘ i may accidentally say a slur’/ ‘ i am going to say this horrible thing out loud if i cannot control myself.’ It can also be images of terror or racist/sexist/ableist jokes in your mind that repeat like a broken record.
(Please note from section 1 that this is extremely anxiety provoking and not something you would do. OCD preys on what we respect the most.)
-----------------------------------------------------------------------------------------
pOCD; Tumblr listen the fuck up because I am tired of seeing people get called shit on this website for having this mental illness. People who experience pOCD are not pedophiles, they do not get any pleasure or benefit. The thoughts and images are meant to induce harm to the person experiencing them. Children are normally the trigger for this and the resulting images can be very graphic. Again you aren’t attracted to children- thoughts of them getting harmed hurt you so your OCD makes you see them.
Know this so you can advocate for folks with pOCD in real life. Remember we are here. We are suffering and we are terrified of your children.
----------------------------------------------------------------------------------
Poisoning others/or in your food; Life isn’t medieval anymore but sometimes OCD demands we have a food taster or that we obsessively worry that we may kill someone with our cooking. Personally I struggle with colorblindness so I am constantly fretful over cooking any sort of meat so it’s difficult for me to cook it.
However this also comes as; obsessive horrible thoughts of your cooking kill someone or that you have somehow/accidentally poisoned someone’s food (even if you haven’t touched it or been within a foot of it ) or that someone has poisoned YOUR food even if no one has touched it except you. You’re going to be picking apart your food or unable to eat out at all.
-----------------------------------------------------------------------------------
Emotional Contamination: It’s similar to magical thinking and this terrifying prospect of mind readers. Emotional contamination can manifest as anything from intense worry over somehow gaining someone else’s negative personality traits.
Or that somehow by interacting with any role of someone horrible will make YOU somehow also responsible for the horribleness. There is usually a person or a type of person that is a trigger, but it can also be location based.
This is one subtype where magical thinking and superstition are apparent.
For instance; as a teen if a male was in my space or had physical contact;like shaking hands,giving a high five, being in my room etc. I would have to go around and physically touch all the objects that I perceive they may have also touched as a way to cancel out their presence.
This includes wiping off myself to negate even the touch of family members. It really hurts peoples feelings, my father was especially hurt by this.
------------------------------------------------------------------------
Physical Contamination: This goes beyond physical dirt and grime. Most of us dont have spotless homes because if you’re having a fist fight with your brain everyday cleaning falls by the wayside just like it would for anyone else. Physical contamination holds 2 things: physical contamination obsessions AND compulsive cleaning behaviors/rituals. We believe that a small amount of a contaminate can cover large surfaces.
Oh, and did I mention its not JUST dirt/germs/viruses. The list is expansive but heres a mixed bag of what they can be: sticky substances,dead animals,glitter (FUCKING GLITTER),negative words or language,colors, numbers, surfaces in general, food, people, and activities. There is also a hyper responsibility to protect yourself and others from ‘contamination’.
Strangely there is a magical separation between the contaminated world and the ‘clean’ one. Spaces designated as clean would be a bedroom/bathroom/workspace where you are most active. That space is where the compulsions and intrusive thoughts occur. Its not I MUST CLEAN EVERYTHING ALL THE TIME. Otherwise I would be working cleaning houses because why the hell not amiright?
A real world example from a colleague would be a young man with physical contamination OCD is struck with such intrusive thoughts about cleaning that they refuse to allow anyone in their room or any animals in their home. But they are not able to even flush the toilet, take out the trash, wash dishes, or do garbage because of their intrusive thoughts.
The most famous would be compulsive hand washing but I feel it is important to also note OTHER aspects of physical contamination because everyone sees the hand scrubbing stereotype.
Other compulsions include intricate rituals, not touching the floor (i played X-treme the floor is lava during college. I couldnt let my feet touch the floor because it was ‘dirty’),excessive showering (2-8+ hour showers guys, 8 hour showers. Thats what we’re talking about.)
----------------------------------------------------------------------------------------
Relationship OCD: This comes as no surprise that yes you will have intrusive thoughts that you are somehow harming/ will harm/ may accidentally harm your significant other. Whether that be by physical or emotional means. It can look like ‘ I may have lied to her about how much I love her’, ‘ i may not actually love her and I may be leading her on’, and ‘ I must be corrupting her’. These can extend to certain physical activities with false memory OCD as a cherry on top. A great finishing garnish to leave you feeling absolutely dismayed and unable to trust your own perception.
----------------------------------------------------------------------------------
Scrupulosity: Religion! Whatever that may be! Its a thing with OCD. With Scrupulosity obsessive thoughts run all over the board from; you committed a sin and forgot about it you monster to having to pray continuously/ a certain time/ until its right. What is right?Ask OCD that’s the only person who knows.
We are fairly certain my grandfather had OCD because he went to church for every single Catholic Mass. Every single day. Every. Single. Day. That’s not a healthy amount of attendance(I'm calling you out posthumously because I care Robert!). This can also look like: praying a certain amount of times. Praying until you do it ‘right’. Confessing every single potential sin. Cataloguing and dwelling over ‘sinful’ things.
----------------------------------------------------------
Symmetry or Just Right OCD: Symmetry OCD is the runner up for ‘most likely recognized on tv shows’ award.
Symmetry OCD convinces you that if *insert thing here* isnt symmetrical or ‘just right’ (a magical position or number of objects that makes 0 logical sense) that something bad will happen.
This can range from the known; rearranging things. But it also looks like buying more objects until you reach the right amount and even throwing out objects if theres ‘too many’.
It can range from ‘the walls are percievably not straight so now i avoid that room at all costs otherwise i will be trapped traveling the edges of the wall with my eyes otherwise it will fall in and murder us ALL.’ to ‘ this historical bust is one inch off to the left and now all i see is visions of it breaking against the ground.’
So that is what I have time for. 9 pages on subtypes and basic information. If you find yourself wanting me information all of this is easily accessible online. So go, be free and dont ever compare people to Monk again. Write Batman and Scott Summers with OCD. Give us ACTUAL representation and not throw away joke lines. We are here. Our suffering isnt funny. We deserve representation too.
42 notes
·
View notes
Last Seen Blogs




