#spinothalamic
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
1,644 Tumblr posts in 1 second.
Text
SciTech Chronicles. . . . . . . . .July 11th, 2025
#Phragmites#wetlands#groundwater#playa#emotional#circuit#thalamus#spinothalamic#X.Org#Wayland#Wayback#standards#olivine#water-transport#infrared#MTZ#algae#architechture#“diatomaceous earth”#TPMS
1 note
·
View note
Text
Spinal Cord: Tracts
This is the first part in a collection that goes over spinal cord injuries. We're just going to look at some of the tracts of the spinal cord first, so that I can better explain how injuries affect patients.
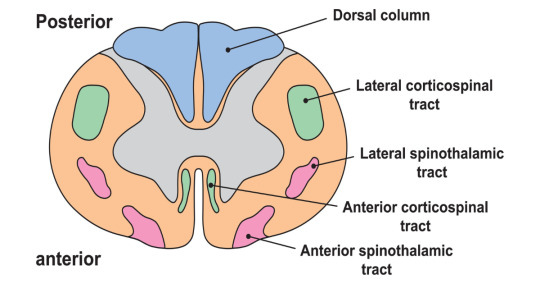
So first off, what does the spinal cord look like? Your spinal cord is a long collection of neural tissue with a distinct layout. The center of it has unmyelinated gray matter, while the outside has myelinated white matter. In the middle of the cord is the central canal, which is filled with cerebrospinal fluid. The entire cord is encased within the vertebral column, and spinal nerves exit between the vertebra. The top of the cord is attached to the brain, and the bottom ends within the lumbar spine as the conus medullaris. Spinal nerves continue into the sacrum as the cauda equina.
What are tracts? These are sets of specific neurons that carry out set functions. They can be generally separated into motor and sensory, and ascending or descending. Some are for visceral (organs) innervation, and others are for somatic (voluntary muscles) innervation. Each tract is made up of a lot of nerves, but each will usually synapse three times as it goes up or down the tract. Now let's get into some specific tracts. I'll only be going over the main ones, even though there are a lot more. Most of the others have to do with muscle fiber senses and reflexes, which are important but not that fun to talk about.
Ascending Sensory
The two most important ones are the dorsal column medial lemniscus (DCML) and spinothalamic (STT) tracts. The DCML carries sensory and proprioceptive information for the body. The information for the upper and lower limbs is separated into the fasciculus cuneatus and fasciculus gracilis, respectively. The fibers in the tract enter the spinal cord and travel up on the same side until they reach the medulla, where they cross over to the other side of the brainstem. Then, they continue to the brain and use the internal capsule to reach the VPL of the thalamus. From there, they can reach the primary sensory cortex.
The STT carries pain and temperature sensation. Once it enters the spinal cord, it goes up about two levels and then crosses over to the other side of the spinal cord. It also heads to the VPL of the thalamus before reaching the primary sensory cortex. The crossing over of the DCML at the medulla versus the STT around the level of innervation is very important in diagnosing spinal lesions.
The face has its own version of the DCML (principle trigeminal) and STT (spinal trigeminal), but these are a bit harder to grasp and not too relevant to the injuries I will discuss, so it's not too important to go into.
Descending Motor
The most important one is the corticospinal tract (CST). It descends from the precentral gyrus to the medulla, where it crosses over (this is why the right side of the brain controls the left side of the body). From there, it goes down to the spinal cord to synapse with a lower motor neuron.
It's important here to explain that upper motor neurons (UMN) and lower motor neurons (LMN) give rise to different symptoms when they are lesioned. UMNs go from the brain to the spinal cord, and when they are lesioned, everything "goes up." Muscle tone and reflexes increase, and you get spastic paralysis. With LMN lesions, which go from the spinal cord to the muscle, everything "goes down." Muscle tone decreases, as do reflexes. You also get flaccid paralysis.
The face also has its own version of the CST, called the corticobulbar tract. It uses the cranial nerves as LMNs. There is also the mesencephalic trigeminal nucleus, which is responsible for proprioception from the mandible and initiating the jaw jerk reflex.
Here's a pic of how everything is laid out in the spinal cord. I hope you can start to appreciate how we're going to fuck things up in the next post.
Alright, so there are the basics. This post was kinda boring, sorry, but I think the lesions post will make sense if you can understand what I'm talking about. This isn't required reading for that post (as if any of this is fucking required reading lmao), but more of an FYI if you want to know WHY certain lesions cause certain symptoms.
7 notes
·
View notes
Text
A massive(?) and detailed headcanon: As Alkas' brainstem had been damaged by Orin. ( As thanks to @feretra, I'm looking more deep into this so I can provide a more better-detailed kind of headcanon. But Alkas' memories weren't the only thing damaged. But also including / adding the possibilities of the fantasy-realm. How Alkas is Half-Mortal. How a necromancer has somewhat done her best to make sure that Alkas did not die. Mending him to the best of her abilities. ( Kressa Bonedaughter: "I remember finding you close to death, beaten black and blue on the floor of this sanctum. It must have been a few hours after the tadpole was placed in your skull. ) If Orin had also stabbed his C1 Spinal Cord. Then it is possible that some transmissions for sensory and such has been damaged or cross-wired. ( Half-Elf ( Orin ): How you screamed as my knife slit your skull, your brain juices sticky and sweet. ) That and the Tadpole itself. Plus depending on his healing process. As I think they were in the Pod for some time. Since Alkas was part of the Absolute. He was more closer to this. Closer to what would soon be the beginning of the game. )
It may not be 100% accurate as I am trying to put two and two together with this kind of stuff.
Alkas' somatosensory pathways have been damaged. ( Sensory receptors: Touch/Pain/Temperature. ) Because what has been done. Orin dug so much that damage was made. ( The spinothalamic tract is responsible for conveying pain and temperature information from the body to the brain. ) But they're not completely gone. It can be possible for it to be cross-wired, or that they simply disappear and come back. His lack of taste can come back and go.
So overall: A loss sense of touch / pain, maybe even temperature and perhaps even the loss sense of taste here and there. Certain things have been fixed????? Depending on what the Necromancer had done, and what could happen in the Mindflayer pod. We can also include Tadpoles as they're currently the stowaways in certain people's brains. So the Tadpole itself could help somewhat.
#[ 04 ] ── * HEADCANON ( 𝘱𝘢𝘷���� 𝘮𝘺 𝘱𝘢𝘵𝘩 𝘸𝘪𝘵𝘩 𝘤𝘰𝘳𝘱𝘴𝘦𝘴 )#[ 05 ] ── * STUDY ( 𝘤𝘶𝘳𝘴𝘦𝘥 𝘵𝘰 𝘵𝘰𝘶𝘤𝘩 𝘦𝘷𝘦𝘳𝘺𝘵𝘩𝘪𝘯𝘨 )#( this post might be edited here and there to add more accurate stuff but overall I've just been throwing stuff together )#( with what i've read )#( in no way or form am i a medical professional IF SO. THIS WOULD SOUND DIFFERENT )
15 notes
·
View notes
Quote
The spinothalamic tract is also known as the ventrolateral system or anterolateral system. It is a sensory tract that transmits information from the skin to the thalamus in the brain.
Spinothalamic tract: Anatomy and function | Kenhub
0 notes
Text
Spinal Cord: Tract Lesions
This is the second part of this series. The first explains these tracts, but it really is just to make this easier to understand. Not required to read for this post.
Here, we're going to look at different lesions in the cross section of the spinal cord to see how transverse cuts affect the nervous system. This post won't really get into different levels of lesions and very specific injuries, that will be in the next post.
Also FYI: contralateral means opposite side and ipsilateral means same side.
Brown Sequard Syndrome
This is a lesion affected the entire half of the spinal cord (right or left). It can be due to penetrating trauma, disk herniations, tumors, tuberculosis, or demyelinating diseases. It will affect the dorsal columns (DCML), spinothalamic tract (STT), and the cerebrospinal tract (CST).
Alright so since we know the STT crosses the midline about two levels above where it enters the cord, we know that there will be a loss of pain and temperature sensation on the contralateral side of the body two levels below the lesion. We can also know that there will be a thin strip of ipsilateral loss.
Because the DCML does not cross the midline until the medulla, we can know that there will be an ipsilateral loss of fine touch and proprioception below the level of the lesion.
Now for the CST. There will be lower motor neuron (LMN) signs at the level of the lesion, as the synapse of it and the upper motor neuron (UMN) is lesioned. LMN signs include decreased muscle tone and reflexes, and flaccid paralysis. The UMNs will be cut off below the level of the lesion, giving us UMN signs: increased muscle tone and reflexes, and spastic paralysis.
This is because the LMNs below the lesion are fine, and just receive no "refined" signals from the UMN, leaving them to do their own thing. When the LMNs are lesioned however, they freak the fuck out and go limp. So the muscle receives no signal whatsoever. And the UMNs are in the spinal cord so obviously if the wire is cut there is no signal down the tract.
Another thing is that if this lesion is above T1, then you get ipsilateral Horner's syndrome, which will lead to a droopy eyelid, pupil constriction, and absence of sweating on that side. This is due to damage to the sympathetic nerve fibers, which leaves parasympathetic function unopposed.
Central Cord Syndrome
This is due to something pressing outwards from the central canal of the spinal cord. Most likely, it will be due to the formation of a syrinx, which is a cyst in the middle of the spinal cord. This can be formed due to trauma, or be due to something like an Arnold-Chiari I malformation.
This will generally affect the anterior white commissure (how fibers cross in the spinal cord). This will affect the STT, which will lead to a bilateral loss of pain and temperature sensation below the level of the lesion, as fibers from both sides are compressed as they try to cross over to the other side. Typically, syrinxes are found in the cervical area, which leads to a cape-like distribution of sensation loss.
If the syrinx gets bigger, it will also start to compress the CST. This will first lead to LMN signs, and then UMN signs as it gets bigger.
Anterior Cord Syndrome
This affects the anterior 2/3rds of the spinal cord from injury to the anterior spinal artery (you only have one). It leads to deficiency in the CST, STT, and autonomic fibers. You'll see a bilateral loss of pain and temperature, UMN signs bilaterally, and bladder dysfunction (aka pissing one's pants).
Posterior Cord Syndrome
This is rarer, as you have two posterior spinal arteries. However, if both get damaged, it will cause a lesion to the posterior 1/3rd of the cord. This affects the DCML.
Another posterior lesion of the DCML is Tabes dorsalis, which is an advanced form of neurosyphilis. This is a demyelinating disease. It will also affect the DCML (obviously).
Since the DCML is bilaterally fucked, you will get a loss of fine touch and proprioception below the level of the lesion.
Subacute Combined Degeneration
This is a demyelinating disease that affects the DCML and lateral CST. It is due to a lack of Vitamin B12 (this is found in animal products, so vegetarians might want to supplement). It can also be caused by nitric oxide gas inhalation.
SCD usually starts with an increase incidence of falling as proprioception is affected. There will also be a tingling or numb sensation in the hands and feet, as well as UMN signs. Because of how the topography (fuck is that the right word??) of the spinal cord is, the hands and feet (called a "stocking and glove" distribution) will be more affected.
Conus Medullaris Syndrome
Alright, the conus medullaris is the end of the spinal cord and it plays a role in bowel, bladder, and sexual function. It is somewhere around the T12 to L2 vertebrae (it's a lot higher than most people think. Your spinal cord really isn't that long). A lesion will result in sudden and (usually) symmetrical symptoms, and both UMN and LMN signs. The LMN signs will cause the legs to be floppy and areflexic. Some people get what's called "saddle anesthesia," which is numbness in the areas where your ass and legs would touch a saddle.
Bowel and bladder dysfunction will present very soon after the lesion. This will cause decreased rectal tone, urinary retention, and an absent bulbocavernosus reflex. That last one is tested using the anal wink test. This is a reflex that makes the bunghole "wink" at you when you stroke the glans penis or clitoris (look at how much you're learning today :D).
Cauda Equina Syndrome
So the conus medullaris gives off a bunch of spinal nerves that continue through the vertebral canal in order to exit at the correct level. It looks like a horse's tail, no joke. A lesion between L2 and the sacrum will cause injury to these nerves.
The symptoms will usually be gradual and asymmetric. There will be motor impairment, but remember these are spinal nerves, so it will only be LMN signs that we see. The bowel and bladder dysfunction is similar to those in CMS. The main difference here is that we only get LMN signs and that they are typically asymmetric.
End Notes
The next post will go into a bit more fun stuff for writing. Most because I think a lot of people don't know what level of the spinal cord leads to what. But it can be really confusing, so no worries. We'll look at more specific injuries like stabbing someone in the spine. I know you guys like that, lol.
3 notes
·
View notes
Text
I Can Help With That | Dr Strange x Y/N
“That is definitely a new strategy to pick up guys.”
“I’m sorry?”
“Never seen someone studying Fitzgerald’s neuroanatomy in a bar unless you have developed some new strategy to pick up brainy guys with that.”
Masterlist
Warnings: Little smutty

“I’m buying this place,” Tony announced as he drained another glass of whisky.
“You can’t,” Natasha hissed from his side. “You’ll only piss off Pepper more.”
Tony groaned and looked at Stephen, “Does this mean I can’t party at the tower nor buy myself a bar?”
Stephen smiled and nodded, sipping his martini.
“Can’t you do something to change her mind?”
“My god, Tony,” he exclaimed indignantly, “I can’t believe you want to use me for such petty purposes.”
“You are no fun doctor,” he mumbled and ordered another drink then glanced at the crowd. “How about I find someone to get you laid, and you help a little in return?”
Stephen shook his head. “I can get laid without your help. Besides I agree with Pepper, you indeed need to party less.”
“Oo look at them,” Tony discreetly pointed to a group sitting a little away from them, “those two are totally eye-fucking you.”
Stephen sighed and turned a bit to give them a quick glance. Not my type, he thought and finished his martini.
“Anyone thinking of hitting the dance floor? Thor asked, sliding off his stool, to no one in particular.
“I’m,” Tony and Natasha answered in unison, following suit.
“You are acting all grumpy today,” Tony complained before leaving, “just get laid, get things off your head and you’ll be fine as fuck. Oh look, one of them just left for the washroom.”
Tony wasn’t wrong. The recent attacks had left him spent. But he still wasn’t interested in sleeping with someone, not yet. After two shots of tequila, he handed over his card, waited a moment and walked towards the smaller section of the bar, the one with less loud music and small round tables.
That was when he noticed her. Technically, he noticed the book first.
“That is definitely a new strategy to pick up guys.”
She looked up from her reading. The perfect doe eyes. A beautiful dark shade of chocolate, swirling to blend into caramel at the iris. He suddenly forgot what he was supposed to do here.
“I’m sorry?”
It took him a second to say, “Never seen someone studying Fitzgerald’s neuroanatomy in a bar unless you have developed some new strategy to pick up brainy guys with that.”
“Not interested,” she frowned and continued reading from her book.
Had she outright rejected him? That too him?
Breathe, Y/N. breathe. She reminded herself as she tried to focus on the pathway of the spinothalamic tract. He might be all sexy with that voice and looks but that’s not going to help you pass the exam.
She sensed the chair beside her move, and soon he was staring at her like the tempting Lucifer.
“So you aren’t trying to pick up anyone?”
“No,” she replied, not daring to look at him. “I have lost my keys to my apartment. And my roommate is supposed to be here. So, here I’m waiting.”
“Why not enjoy yourself while you wait?”
She marked the page and put the book down, finally looking at him- she forgot what she was supposed to say. He was totally gorgeous and, as he had said, seemed ‘brainy’ with those white streaks. He raised one perfect thick eyebrow at her. What had he said? Something along the lines of enjoying, she guessed.
“I have got exams in a few weeks. So trying to make up for the knowledge I haven’t gained.”
Having got her attention he smiled at her. And she loved the way his orbicularis oculi produced those radiating lines at the lateral angle of his eyes, “And in what subjects are you lagging?”
Y/N reprimanded herself. She was going crazy. Nevertheless, she answered him, “Biochemistry and neurology.”
He nodded and glanced at her book. “I can help with that.”
“Excuse me?”
“I can help you with neurology,” he said, then added, “Only if you would like that.”
“Why? Are you the ‘brainy’ professor?”
“Not exactly, unless you consider a former neurosurgeon ‘brainy’ enough.”
Her jaw dropped. “I, uh,” she struggled to string her thoughts together. Great. He was not only gorgeous and sexy but also super intelligent. And she had fucked up well.
“I’m sorry. You’re absolutely ‘brainy’.”
He grinned. She felt her heart doing an erratic happy dance, “I would be more than grateful for your help, but I’m sure you are not here to pick up a student to tutor.”
“I wasn’t, sweetheart. What’s your name?”
Sweetheart? If she was going crazy then, now she would be certifiably insane. “Y/N L/N. And you might be - doctor?”
“Stephen Strange,” he replied and watched her eyes going as wide as they could.
“The Doctor strange?”
“Yes,” he laughed, “I’m the Dr Strange. So, would you like some help?”
She nodded.
“My place is nearby,” he tilted his head, “And this is hardly any place to study. Shall we?”
“Sure,” she murmured and stuffed the notes and book into her backpack.
“Do you fancy a walk? A cab? Or just a portal?”
“We can walk.” He nodded and held out a hand to her, which she took.
The walk was brisk and quiet as they hurried, heads down against the wind of the late night. She looked around the neighbourhood, realising she had passed them quite a handful of times while taking the late-night walks.
“My apartment is another few blocks away,” she said, after they settled on a couch beside the staircase, in front of a fireplace.
She watched him snap his fingers, and embers erupted in the fireplace. Showy, she thought as he settled next to her.
“Well, that sounds great, doesn’t it? You can visit me anytime you need my help.”
“There would be a next time?”
“Don’t you think there will be?” He asked, slightly disappointed. “Is this a one-night stand?” Common. Don’t be so desperate. Get a grip!
“I don’t know,” she shrugged her shoulders, “In time you’ll realise I’m not your type,” she gave out a nervous chuckle.
Cute. “And what do you think is my type?”
“Bold, sexy, graceful and… experienced?”
“I like cute, shy and naive as well.”
She was pretty sure her cheeks were red, and in no time her body was spontaneously going to combust into flames.
He reached out a hand and pushed her curly brown hair behind her ears. His hand skimmed across her neck, pausing at her pulse point, which had been going crazy ever since she met him. “Why don’t we get started? Weren’t you doing the tracts?”
Back to earth, Y/N.
He grinned, and his hand dropped. Her skin burned everywhere he had touched.
“Yeah,” she was immensely proud to conjure a reply.
By the end of the third hour, she was considerably tired.
He was explaining various cases of misdiagnosis of Parkinson’s he had seen when felt she couldn’t take any new information anymore. But she waited with forced patience for him to finish.
“Stephen, I don’t think I can study anymore.”
“I know,” he said, taking the book from her hand, and placing it on the coffee table. His coat jacket was long gone, and every flex of muscle under the fabric of his white shirt tossed her in a puddle of embarrassment and arousal. “Tea? Coffee or hot chocolate?”
Definitely coffee. She needed the caffeine to walk back- Her thoughts were lost as he rolled up his sleeves. Oh, those veins… those long, long fingers. She could feel her hormones having quite clearly their night out.
After he conjured them two cups of coffee, he heard a sharp intake of breath followed by an ‘Oh my God’.
“You know, you can stay the night here.”
Y/N gripped her cup tighter. What an attractive way to embarrass oneself in every possible way in a few hours! The sorcerer and mind-reader fact had completely slipped out of her mind.
“Just like a one-night stand?”
Stephen hummed. “Minus the sex part, if you wish.”
When she didn’t speak anything for a long minute, he spoke, “I wasn’t reading your mind the entire night, if that’s what you are upset about.”
“Very gentlemanly of you,” she said, sagging in relief.
Then he turned down the lights. It was dark with just the light from the fireplace. They talked about trivial matters, getting acquainted a little, her minor routine and his sorcerer duties.
“You’re a great teacher, you know?” she said, fishing her things into the bag.
“Really?” He grinned and she felt it shoot right into her stomach. Get a grip, she reminded herself.
“Yeah. you explained things in a better and easier way. I don’t think I would have been able to cover half of the topics-”
“Y/N,” he interrupted her, “I wasn’t looking for you to shower me with compliments. It’s just that I never thought of myself as much of a teacher in any field of work. I can teach myself but others - I'm not any good at that.”
“You underestimate yourself.”.
“Everyone who knows me a little would beg to differ.”
Sitting still for a minute, she watched him sip from his cup, she didn’t know what to say to that. “I should get going,” she said, finally getting up.
He frowned. Looked at his watch. And she noticed a flicker of disappointment in his features.
“It’s too late. But if you insist, I’ll walk you home.”
Y/N didn’t like the juxtaposition of reason and passion in her situation. She swallowed her nerves. “I guess I’ll stay then.”
He smiled, took her hand, and pressed his lips against the inside of her wrist. Her whole body shuddered. He pulled her back to the couch, then closer, until she was pressed against him. She felt all her organs dropping right on top of her uterus like all their supports were lost.
She looked at his lips. Tread lightly, he reminded his desires. “It could always be a one-night stand minus the sex,” he assured her.
She chuckled and rested her head on his shoulder, “I don’t mind the sex part.”
His eyelids fluttered when her hand came up close to his face. Hot fingers pressed into his burning skin as traced his jaw before settling on his chest. Oh god, he had forgotten what a touch could do.
“Besides, I ought to make it up to you to ruin your evening.”
Stephen’s eyes had darkened as he stared at her. Her breath hitched. Have I done something wrong?
“You didn’t ruin my evening. I was looking for a distraction.”
“I was certainly not the sort of distraction you were looking for.”
“You were definitely the distraction I didn’t know I needed. Talking about things that my life used to revolve around wasn’t morbid. It was refreshing. You don’t have to do this because you-”
He was cut short as she closed her mouth over his.
Stephen held her close with his free hand when she pulled away from the kiss. He carefully placed his cup down. Then kissed her again, slowly, deeply and tantalisingly. At that moment she felt the geometric sum of all her nerve endings going crazy.
He pulled away, ducked his head, and placed a hot kiss on her neck.
“Let’s go upstairs,” he stood and offered her his hand like before.
Y/N examined the bookshelves flanking the bed as Stephen peppered kisses on her neck. There were a few volumes of classical literature, few books of modern literature, some medical books and the rest - the bulk - of them, she guessed, were of sorcery.
His hands slipped under the sides of her shirt. Her back arched in response, however, he pulled her back to him, until they were plastered. She could feel every ripple of muscle even through the fabrics.
You are awesome, she reminded herself. Not insecure. A bit shy and inexperienced maybe. He had said he liked that. So no big deal.
But when his hands slid forward and downwards, she was super conscious of the little pudge that sat above her jeans. The dimpled flesh on her thighs. Work out regularly right from tomorrow.
Dying… Dying to taste every inch of her skin. He never thought he would get this desperate. He had wanted to take off their clothes slowly, dramatically, however, he snapped his fingers getting rid of them at once.
Y/N grasped at the sudden assault of cold air.
“I’m sorry,” Stephen said, whirling her around, “I’m a little too eager.” His hand reached up and weaved through her subtle curls as his lips moved hers.
Feeling the hard length of him poking her stomach, she moaned, giving him the perfect opportunity to slide his tongue and deepen the kiss.
She pulled away for a breath and he trained soft, wet kisses across her jaw, neck and chest before gently nibbling at her nipple. Her fingers tugged at his hair, a contented sigh escaping her lips.
Then they heard a noise. Three steady knocks on the bedroom door. “Strange,” the man bellowed. Another two knocks.
“What is it, Wong?” Stephen groaned. “Don’t come in.”
“Get in the bed,” he instructed her as he conjured a pair of sweatpants.
“I have been trying to reach you for the last twenty minutes. Why aren’t you answering the phone?”
“Because I haven’t heard it ring.”
She watched in frustration as he slid out of the room, closing the door behind him. Their voices grew dull.
Y/N waited. Ten minutes. Thirty. Then another hour. She glanced at the clock on the nightstand and sighed. It’s three in the morning. Maybe he’s not coming back.
Getting out of bed, she looked around for her clothes. She peeped into the foyer. Dead silence. Great! She was in a perfect stranger’s house all alone without clothes.
Continuum: Pivot
#dr strange#dr strange x reader#dr strange x you#dr strange x y/n#dr strange x fem!reader#dr strange imagine#dr strange oneshot#dr stephen strange#dr stephen strange x reader#dr stephen strange x y/n#doctor strange#doctor strange x reader#doctor strange x you#doctor strange x y/n#doctor strange x female reader#doctor strange imagine#doctor strange one shot#doctor stephen strange#doctor stephen strange x y/n#doctor stephen strange oneshot#stephen strange#stephen strange x reader#stephen strange x you#stephen strange x y/n#stephen strange imagine#stephen strange one shot#one short#reader insert#marvel x reader#marvel one shot
435 notes
·
View notes
Text
if anyone has tips on studying for neuroscience please hmu 😔😔😔
#like i have the anatomy down#but idk how to remember/understand all the functions#and the spinothalamic/corticospinal/etc pathways ???#and also with remembering different types of lesions and what damage occurs???#someone pls help 🙏🙏🙏
2 notes
·
View notes
Note
I...I love everything I've seen about your Cyborg AU. Do you have any of that you're willing to share? 👀 (If not, I would also love to hear about The Wolf King.)
OOOOOHHHHH THANK YOU SO MUCH!!! 😭💖 I love that AU too. I don’t really have any good scenes ready to share (I haven’t gotten to work on it in a while T_T) but I’ll give ya what I got!
The Royal Ancient Tech Lab was, in the king’s words, an overfunded, undermanned, financial sinkhole of a project that never failed to overpromise and underdeliver, and if his back hadn’t been pressed to the wall these 20 years he probably would have shut them down ages ago.
He wasn’t exactly wrong.
Robbie had been the director of the Guardian Project for the last five years, and his team had yet to produce an actual, viable soldier for field tests. The director before him had been reassigned owing to poor performance—as had the director before him, and the director before him. Needless to say, he felt under a bit of pressure.
In his humble opinion (as resident Guardian expert, genius, superstar—take your pick), this entire mess could have been avoided if King Rhoam hadn’t insisted on a human element.
The original technology they unearthed was completely autonomous, not to mention already designed and assembled. A bit a fuel, a little time to decipher the software and make adjustments, and they could have given him an army. But he didn’t trust a weapon that didn’t have one of his precious knights at the helm. Early attempts were made to incorporate a pilot, much as the Divine Beasts did, but the technology was largely incompatible and the carapace was too small to fit a both a Hylian and the weapon systems inside anyway, necessitating a complete resign. They wasted four years on that model—five?—before abandoning it in favor of something a little more daring.
If they couldn’t enhance the machine, perhaps they could enhance the man.
He counted himself lucky that he hadn’t been with the project in the early days, when the experiments were less science and more butchery. There were still kinks to iron out—phantom pain was reported with some frequency, and despite stringent testing it was difficult to determine a candidate’s long-term psychological compatibility with the upgrades—but the advent of the spinothalamic inhibitor meant they at least weren’t losing subjects on the table to cardiogenic shock.
And at long last they had something to show for their efforts.
The door opened, and Robbie spun with a flourish, ready to shock and awe his guests, but instead of royalty he was greeted by someone significantly less exciting.
“Oh. It’s you,” he grumbled, turning back to his Slate to triple check his presentation.
“I’m just here to see the princess,” Purah assured him, holding her hands up as placatingly as she knew how before planting them on her hips. “I promise not to interfere with your precious review.”
He sighed. “Fine. Did you bring the rune I asked for?”
“Of course.”
“Good,” he frowned, scrolling through the profiles one last time. Just to make sure there were still 22 of them. “Get it uploaded to the princess’s Slate as soon as possible, will you?”
She sighed at him. “She isn’t going to like this.”
“She’s going to love this,” he countered. “Not at first, of course. But she’ll get over it. And then she will.”
26 notes
·
View notes
Text
"One major finding of our study is the decreased MH-thalamus rsFC in fibromyalgia patients compared with the rsFC in the HC’s and the increased MH-thalamus rsFC after Tai Chi mind–body intervention. Both the hypothalamus and thalamus belong to the diencephalon, and there are bidirectional connections between these two structures. The thalamus is a key region for central processing and integration of nociceptive inputs. It acts as a relay center for handling incoming sensory information and motor impulses between the spinal cord, medulla oblongata, and cerebrum. Specifically, the thalamus receives nociceptive signals via two major ascending pathways: the spinothalamic tract (STT) and the spinoreticulothalamic tract (SRT). The STT conveys noxious information from the dorsal horn to both the lateral thalamus and medial thalamus, while the SRT mainly relays nociceptive information to the medial thalamus via an additional synaptic relay within the medullary reticular formation of the brainstem [38].
Further studies suggest that the thalamo-cortical pathways/interactions may underlie the perception of pain as an unpleasant sensory and emotional experience. The lateral thalamocortical pathway is involved in coding the sensory discriminative aspects of pain, while the medial thalamocortical pathway codes the emotional qualities of pain [38]. Literature suggests that the anatomical and biochemical alterations in thalamocortical circuits may be responsible for the development of chronic pain [33, 38,39,40]. The thalamus observed in our study extends from the medial portion to the lateral portion of thalamus, suggesting alterations of both sensory and emotional aspects in the pathophysiology of fibromyalgia.
We also found that fibromyalgia patients are associated with less MH rsFC with the amygdala. After effective mind–body intervention, the MH rsFC in the amygdala significantly increased. The amygdala is a key region in the limbic system that plays an important role in emotion processing, fear and anxiety response, and the influence of negative emotions on pain [41]. The amygdala is also part of the descending pain modulation system, directly projecting to the PAG [42]. A previous study showed that chronic low back pain-evoked brain activity increases in the amygdala and rACC/MPFC [43] and is associated with volume decreases in the amygdala [44]. A more recent study found higher incidences of white matter and functional connections within the MPFC–amygdala–accumbens circuit, with smaller amygdala volume accounting for 60% of the variance for chronic low back pain persistence [45]. Our results agree with these findings, suggesting that the linkage between the MH and amygdala may play an important role in the pathophysiology and development of fibromyalgia."
-
RESEARCH!
I mean, both for myself and the fictional characters who get to suffer with me. I give them seizures and spasticity and/or hemiplegia too. Because I can.
But fibromyalgia is the fun one because you can do so much with it. You can pile on other conditions and intertwine syndromes and play Disability Roulette to figure out if this particular episode of migraine plus synesthetic crosswiring is from the fibro or the sensory processing disorder that can come by itself or with the fibro or with the autistic brain or with the epilepsy or with the brain damage via birth or the
And if your character is an iron woobie who is generally a playful carefree joyful eternal optimist you can see how far you can push before the built in clinical depression or cyclothymia explodes, not to mention the ADHD RSD. On top of the fibro flare. And then of course there's the empathic intuition that's almost clairvoyance and clairsentience. Which could connect to an episode of... anything.
Look, I named one of my characters after a powerful Greek deity because she's got a lot going on. I named another character in honor of both my grandma and my childhood because imagination can run anywhere and everywhere and I can give her a lot of qualities I had when I was nineteen. And they're Psionic because I had a Thing for Jean Grey in the 90s and because being a telekinetic cripple would have been really convenient.
Point is, I need to go to sleep and hope for full Stage 4 sleep. And so do Gaia and Avalyn and Mikey. See them in dreams maybe.
#my fictional characters are all autistic#my oc has my disabilities#welp time to give my trauma to my characters#projecting my disabilities onto fictional characters#this is why we project trauma onto characters#this is why i love fanfiction as therapy#ooops i'm going to torment mikey again#i might have been the one who started the psychic mikey headcanons in the 90s#they call me the queen of tmnt mikey whump#fibromyalgia#why i write mikey with fibromyalgia#spastic cerebral palsy#why i write disabled characters#being disabled means living my life in ways people don't like#being disabled means having a very dark sense of humor#writing fictional entities who represent my neuropsychology#this is why i write autistic adhd ninja turtles#autistic special interests#adhd hyperfixation#whoops more infodumping#this is why my fictional characters reflect my neurology#my health comes first before your morality#all two dozen disabilities#the boadicea method of chronic pain management#disability representation#everyone is queer#psionic mikey au#pale sunlight fic#cold fire rising#the brightest souls hide the most darkness
11 notes
·
View notes
Text
I've genuinely been saying TIL way, WAY too often lately
100 days of productivity
Day 11
CVS/RS
HOCM: although beta-blockers/non-DHP Ca blockers are first line drugs to prevent or control symptoms, ACEis/ARBs MUST be started in all patients as there is evidence that they arrest the septal hypertrophy (or can even reverse it!) (angiotensin II and aldosterone are said to accelerate the hypertrophy; so are beta-1 agonists but with poorer evidence)
other than antiRAAS drugs and nitrate-hydralazine, ivabradine also has a mortality-reducing effect in CHF, specifically in patients with sustained HR > 70 bpm despite maximum beta blockade
atorvastatin fucks with digoxin, but ONLY atorvastatin fucksn't with warfarin
although verapamil is a contraindication to adenosine due to the risk of precipitating heart block, beta blockers are not
reversed split S2 in LBBB (P2 followed by A2)
Endo/Repro
haemochromatosis: pituitary dysfunction and hypogonadism are *not reversible*; hormone replacement is the mainstay of therapy
isolated FSH deficiency → ↓androgen binding proteins → oligospermia
toxic adenoma: 300-500 megabecquerels of radioiodine is 1st line; surgical excision is *second line* (radioiodine is preferentially taken up by adenomatous tissue bc it takes up iodine at a fast rate, and ↓TSH means the rest of the gland takes up much less iodine)
checkpoint inhibitors in oncology lead to persistent immune activation, but this may lead to loss of self tolerance especially against endocrine organs; this may lead to thyroiditis, adrenalitis, hypophysitis, endocrine pancreatitis etc; it is important to screen for the maintenance of the hormonal axes in patients on such drugs (eg, nivolumab, ipilimumab)
Rheum/Derm
increased BMI (without diabetes) is actually generally *protective* against osteoporosis d/t ↑oestrone (adipose oestrogen)
ANAs are mostly IgG; much less common are IgA and IgM ANAs
osteomyelitis: plain films are for screening, MRI is definitive
tennis-racquet Brisbeck granules on biopsy of a bone lesion → Langerhans cell histiocytosis
presence of pruritus is circumstantial evidence for bullous pemphigoid over pemhigus vulgaris
osteoporosis risk is high with steroid equivalent to prednisolone 7.5 mg/day over 3 months (or more); if it is anticipated that a patient might need such a long dose of steroids, start prophylaxis *immediately* with vitamin D + calcium + alendronate
Renal/Biochem/Toxo
natriuresis/hyponatraemia despite volume loss = suspect RAAS deficiency (eg, primary adrenal insufficiency)! SIADH does NOT explain profound hyponatraemia when volume depletion is evident, as aldosteronergic drive is usually sufficient to keep sodium levels as high as possible
FB GoT All Hyper about Liddle syndrome: Furosemide toxicity mimicks Bartter syndrome, Gitelman syndrome mimicks Thiazide toxicity and HyperAldosteronism mimicks Liddle syndrome
platinum compounds → hypomagnesaemia
GIT
pigment laden macrophages on colon biopsy = melanosis coli → stimulant laxative abuse
CNS/Ophthal/ENT
absent ankle jerk + positive Babinski: 3 major differentials: syrinx, motor neuron disease or subacute combined degeneration (SCD can have either exaggerated, decreased or absent reflexes)
sacral sparing = maintenance of sensation/power in central cord syndrome (eg, intramedullary metastatic tumour and syringes) and incomplete spinal cord injury due to peripheral arrangement of sacral spinothalamic fibres (test with lack of saddle anaesthesia; reduction deep touch sensation is sensitive for severity of cord injury)
orbital apex syndrome → optic neuropathy, 6th nerve palsy, proptosis, chemosis/injection, miosis, ptosis
Kearns-Sayer syndrome: MERT: Mitochondrial inheritance, External ophthalmoplegia, Retinitis pigmentosa, Teenage onset (<20 yrs)
Refsum disease: CANID: Cerebellar ataxia, Anosmia, Neuropathy, Icthyosis, Deafness
when deprescribing benzos, switch to equivalent dose of diazepam and reduce by 1/8ths every 2 weeks (typically 2 mg per 2 weeks); reinstate previous dose if patient withdraws, then after another 2 weeks try to reduce the dose again
4 notes
·
View notes
Text
TAFAKKUR: Part 216
On Their Faces and Backs
In numerous verses the Holy Qur’an makes reference to living organisms, and particularly to human physiology. The Qur’an does this in its own style, briefly mentioning some fundamental principles of the process or the phenomenon that it is referring to, without going into elaborate details. One of the verses that immediately captures the attention of the reader is the twenty-seventh verse of Chapter 47, Surah Muhammad, which can be translated as: “So, how (will it be) when the angels take their souls at death, striking their faces and their backs?” while describing the agony of death that the disbelievers will suffer. In Surah Al-Anfal (8:50), the Qur’an tells us: “… He causes those who are bent on denying the truth to die: the angels will strike their faces: and their backs…”
The phrase “striking their faces and their backs” leaves us wondering why “faces and backs?” What is special about these body parts in the context of death? The Qur’an is the word of the All-Wise and it is not possible for it to be completely deciphered by human reasoning. Yet, it is our duty as human beings to contemplate the message that our Creator has revealed for us. The moment of death is spoken of in many other Qur’anic verses and Hadiths. The experience of death is a great agony for the disbelievers: The (angels who) snatch (the souls of the disbelievers) forcibly. And those who gently take (the souls of the believers) joyfully (Qur’an, 79:1-2).
Undoubtedly, the experience of death is painful. Leaving the discussion about “faces and backs” to later in this article, let us first look at what pain is from a physiological aspect. It is common knowledge that the sensation of pain is conducted to the brain via the sensory nerves which connect with almost every single part of the body, particularly to the skin. The skin has different corpuscles (sensory cells) for the sensation of touch, temperature, and pain. When a nociceptive (pain inducing) stimulus is applied to the skin, this information is conveyed through the peripheral nerves in the form of small electric pulses (called action potentials), first to the spinal cord, next through the spinothalamic pathways, and then to the higher centers of perception in the brain. These little electrical pulses are felt as pain, temperature, or touch in various centers of the brain (e.g. somatosensory cortex), depending on where the signals originate in the skin. If a particular area is wired to a pain sensing corpuscle in the skin, the brain circuitry will be trained to perceive this signal as pain from early postnatal development. If, on the other hand, a particular nerve is connected to a temperature sensing corpuscle in the body, the part of the brain center that it is connected to will be trained to perceive this as temperature from early on in life. So, the perception of sensory information depends on how these little electrical signals are interpreted by the brain. However, the connection map of the nerves and the circuits that interpret them in the brain form very early in life and these connections are hard wired, that is, it is very difficult to change them.
Pain may be perceived without a real source of nociceptive input as a result of some neurological disorders. For instance, in an amputee, after a limb has been surgically removed, the cut ends of the sensory nerves may generate little electrical pulses (action potentials) on their own without a pain inducing stimulus. The subject might feel an intense feeling of pain in the missing limb! This is clinically known as “phantom pain.” The phenomenon known as “referred pain” has an interesting explanation, also based on neuro-anatomy. The pain conducting sensory nerves from various dermatomes (areas of skin) and some other nerve fibers that originate in the visceral (internal) organs of the body enter the spinal cord side by side as a bundle (spinal roots). When some of these visceral organs, such as the heart and lungs, contract a disease, the sensory signals generated by these organs are not perceived as pain because there are no pain sensing nerve endings in these organs. But, the sensory signals generated by these organs activate the pain sensing fibers at the point where they enter the spinal cord together. The pain therefore is felt by the brain as if it were originating in a certain dermatome. For instance, heart problems are felt as a pain in the left arm. Again, the interesting point is that the perception of pain depends very much on the wiring of the nervous system at the periphery and in the brain.
Needless to say, if the subject is deep asleep or unconscious for any reason, he or she would not feel pain because the brain has been entirely blocked from any sensory input. In the context of body-mind connection, we may consider these states where the soul has minimal connectivity to the brain.
What about the moment of death? According to Qur’anic verses the experience of death is different for believers and unbelievers. Is it possible that the intensity of pain that one experiences at the moment of death is related to whether or not the soul is still “connected” to the brain? Those who die in their sleep do not seem to show any signs of pain, at least not to those who are witnessing the event. We should note that Prophet Muhammad, peace be upon him, stated that sleep shares many common properties with death.
It is reported that whenever God’s Messenger (may peace be upon him) went to bed, he said: “O God, it is with Your Name that I live and it is with Your Name that I die.” And when he got up he used to say: “Praise is due to God, Who gave us life after our death (sleep) and unto Him is resurrection” (Muslim, 35:6549).
Qur’an 6:60 says:
“He is the One who puts you to death during the night, and knows even the smallest of your actions during the day. He resurrects you every morning, until your life span is fulfilled; then to Him is your ultimate return. He will then inform you of everything you had done.”
Is it then plausible that the intensity of pain felt during death is a consequence of how connected the soul is to the body at that moment? These questions may or may not have been addressed by religious scholars in the past. However, information about the physiological events taking place during death is certainly very limited in the religious literature.
Let us take a quick look at the human nervous system, and perhaps this will shed some light on the verses we quoted at the beginning of the article. The peripheral nerves converge together and form bundles, called spinal roots, before they enter the spinal cord at one of the 33 different vertebral segments along its length. The brain and the spinal cord together constitute the central nervous system (as opposed to the peripheral nervous system). The only other neural pathways between the brain and the body are the cranial nerves, the nerves that enter the brain from underneath. There are twelve cranial nerves, most of which carry sensory information from the head or motor information to the head, with the exception of the vagus nerve (Xth nerve), which actually serves the visceral organs. So, it would be accurate to say that the sensory information that comes to the central nervous system enters either at the back (through the spinal cord) of a person or directly from the facial area. The phrase “their faces and backs” thus sums up all the neural pathways through which the sensation of pain can be conveyed to the brain, the interface where the body meets with the mind, or the soul.
It is possible that at the time of death, the pain receptors in the skin and deeper parts of the body start generating action potentials at a faster rate, as if great pain has been inflicted on these body parts. The ionic concentrations in the extracellular medium around the sensory cells can change as a result of diminishing blood supply, and this is probably felt more severely in the extremities at first. The increased rate of firing of action potentials is commonly observed in neuroscience experiments when a cell starts “dying” as a result of perturbations to the extracellular or intracellular ionic concentrations. A train of action potentials with an increasing rate of firing is frequently observed and eventually the action potentials stop completely when the cell can no longer function. A similar phenomenon may occur during the death of an entire living organism due to a reduction in the blood supply that is provided to the body parts as well as due to changes in the pH level from a lack of oxygen. This fast rate of action potentials will be perceived by the brain in the same way as a strong source of pain, e.g. crushing or ripping apart of the body. The principle concept is very similar to what happens in the case of “phantom pain.”
The choice of the word daraba (striking or smiting) in Verse 47:27 is also interesting to note. We describe a pain sometime as “throbbing,” because every time the heart beats the increased blood volume in the area makes the pain receptors fire faster episodically. It may be that this pulsating pain sensation is described as “striking,” using a figurative language in the Qur’an.
Of course, the fundamental question is whether the soul is still in the body and thus able to feel the agony at the time of death. Are the souls of believers taken by the angels before the agony of death starts so that they do not suffer through it? We have no evidence to answer this question one way or another. But, it is certainly within the power of God to make the soul feel the pain or to save a person from it.
#allah#god#prophet#muhammad#sunnah#hadith#ayah#quran#islam#muslim#muslimah#hijab#help#revert#convert#reminder#religion#dua#salah#pray#prayer#welcome to islam#how to convert to islam#new muslim#new revert#new convert#revert help#convert help#islam help#muslim help
4 notes
·
View notes
Text
Today we hit the three week mark in knowing your spinal cord! I’m hoping we can do a full four weeks, that would be quite the collection of knowledge. For those of you just joining in, you can find all of our posts in the neuroanatomy category ordered in reverse chronological order. As per the last few posts, we’ve covered the majority of the anatomy and now we are looking at different disorders of the spinal cord. Today we’re going to cover another type of injury, this one called anterior spinal artery syndrome, so let’s get started!
In our post yesterday we saw an image which sort of gave some spoilers to the more unique kinds of spinal cord injury. For those who haven’t read it, I suggest you do since it is very interesting, but if you’re only here for the anterior spinal artery syndrome, below is the image I’m referencing from yesterday. The middle image is what we will be covering today, tomorrow we will (probably) cover central cord syndrome.
Anterior spinal artery syndrome, labeled as anterior cord syndrome above, is somewhat similar to Brown-Sequard syndrome in that it almost a coronal version of a hemisection (Brown-Sequard). Like the name suggests, it is caused by a blood flow issue.
This type of lesion is caused by ischemia of the anterior spinal artery. Ischemia is a medical term meaning the flow of blood is restricted, this can happen anywhere on the body (one of the more common areas is the feet in fact). The anterior spinal artery is the artery that supplies blood to the anterior portion of the spinal cord. The anterior spinal artery follows the anterior median fissure and below we can see an actual cross section of cord showing the artery and because we tend to show the cord alone, we have included an image showing how blood is supplied to the cord.
Spinal cord cross section with the anterior artery showing (top)
This image shows how blood is supplied to the spinal cord
Like Brown-Sequard, anterior cord syndrome can happen at any time and is not congenital (born with it). Because it disrupts the corticospinal tract, typically when it occurs you will have complete motor loss below the lesion. This will also disrupt the spinothalamic tract, you will also lose pain and temperature sensing below the lesion as well. What makes this type of injury interesting is that the medial lemniscus tract remains intact. Therefore, you still have proprioception (as well as vibration sensing). This means that you know where your extremities are in space, even below the injury; however, you have no real control over the affected extremities.
Causes of anterior cord syndrome are just as multifaceted as the causes of Brown-Sequard. These range from things like an aortic aneurysm, direct trauma to the aorta, surgery, disc herniation, damage to the spinal cord, sickle cell, decompression sickness, or even from infections like vasculitis. Like I said, it’s a long list and those are just a few of the things that comprise it.
Because this is caused by a blood flow issue, when it happens symptoms come on fast (10-15 minutes). Unfortunately, when diagnosed there isn’t much that can be done and the prognosis is not good. You can expect that while symptoms will (most likely) not get worse, they will not get better either. In fact, over 50% of people with anterior cord syndrome see little or no change to their condition and the mortality rate is approximately 20%.
Like with each of these I would like to remind you that treatment is in its infancy and unfortunately we haven’t seen much of an improvement for spinal cord injury outcomes since the 80’s really. However, that is slowly changing and with time (and a lot of luck) we will find ways to treat spinal cord injury. So while things are somewhat bleak now, they won’t always be. Who knows, maybe now that you’ve read this you will be inspired to find the fix.
Until next time, don’t stop learning!
Day #178: Know your spinal cord - Anterior spinal artery syndrome #neuroscience #neuroanatomy -- Today we hit the three week mark in knowing your spinal cord! I'm hoping we can do a full four weeks, that would be quite the collection of knowledge.
1 note
·
View note
Text
To an extent. Yes you have C fibers for child and different C fibers for hot (both carried to the thalamus via the spinothalamic tract) but if you over stimulate with one you can actually get a dual sensation, like burning cold.
I read that capsaicin makes your mouth feel like it's burning because it increases your nerve sensitivity to heat, and menthol works by doing the same thing to cold
So if I eat a habanero pepper and then chew a bunch of breath mints they'll each other out and I'll be fine
261K notes
·
View notes
Text
2nd Year Physiology Viva and Practical Questions
SIR ABDUL REHMAN AND MA’AM ALIYA ISHAQUE
Liver functions Bile synthesis Billirubin conjugated and unconjugated Juandice Pain transmitters Decussation If afferent and efferent arterioles are constricted how will it effect the GFR 1 2 3 order neuron 2nd order neuron of ADH kahan act krta h ADH zyada release hoga toh kya condition hogi Adh function Adh mechanism Aldosterone production All tracts function and sensation carried by them
All tracts in spinal cord Anemia that causes jaudince Angiotensin II functions Bilirubin formation Ceruloplasmin Chart of colour vision Coclea full Condition in which ADH increases Condition of hypothyroidism in adults Cortisol function (non metabolic) Cortisol functions not related to metabolism Cushing syndrome and disease D/f between ascending and descending colon Diabetes insipidus Difference between Endo lymph and Peri lymph Dorsal column Dorsal tracts medial leminiscus diabetes mellitus and diabetes insipidus Where most of water reabsorption take place Which sensory tract bypasses thalamus Internal capsule urea reabsorption ADH functions and stimuli for secretion Where does it act over renal tubule Dorsal white colum or spinal cord Dorsal column system ECF conc Enteroheaptic circulation Formation of billirubin Free nerve endings kis tarah ki hn GI hormones released in fasting state Hormones released during fasting Hypertonic solution ICF conc Ishihara chart plate name It's area ,function . It's pathway and type of sensation caried by it Jaundice and types Juxtramedullary nephron Macula densa Nociceptors Normal osmolarity of plasma kitni h Pain fibers Pain fibers name Pain receptors Peptide hormones Physiology of nociceptors Premotor cortex Proteins formed in liver their name Receptors and types Receptors for hearing Receptors present on the skin Reflexes of git Renin Sensory receptors Siadh Site of action of adh Substantia nigra Total body volume Types of receptors What promotes stomach emptying Which pathway does not pass from thalamus ADH production and action site Angiotensin II formation and actions Ascending tracts names Diseases related to it Fasciculus gracilis and the fasciculus cuneatus Name of the tract once they leave them Pacinian corpuscle Spinothalamic tract Upper and lower motor neurons
EXTERNAL
T3 T4 ki functions 3 Difference b/w cretinism and dwarfism Addison's disease Agr koi patient larkara k chal rha then brain k kis part me msla hai(cerebellum puchna chah rhi thi) Ampula of vater kahan khulta or agr iski blockage ho then Kya hota.. Ant pitutary Hormones Ascending pathways all with characteristics Basal ganglion functions Basal ganglion me circuits Basis of ishihara test Bicarbonate ki absorption in kidney Bile formation Characteristics of synapse Characteristics of synaptic cleft Cognitive function of basal ganglion. Color blindness Cushing syndrome and cushing disease Defecation reflex Descending tracts Electromagnetic Receptors ky examples Estrogen and progesterone functions in males Facilitation Factors that cause gastric emptying Fatigue Fatigue how it occour. Filtration coefficient Free nerve endings kis tarah ki hn Functions of kidney GFR (factors ,,, measure kesy krty) GFR and dependants GFR formula Gastric reflexes Git hormones Glomerulus pressure. Hormones needed for growth Hormones of GIT effects of sympathetic and parasympathetic systems on GIT Acromegaly and Gigantism Growth Hormone Hormones of fasting Hormones release during fasting How kidney regulates when BP is increased How many types of summation and explain each Juxtaglomerular apparatus Kidney k Hormones Motor function of stomach Net filtration pressure and its formula Nociceptors Non metabolic functions of cortisol Pain fibers Parathyroid hormone Plates of ishihara chart Prolactin functions Proprioception is carried by(Dorsal column) Putamen n caudate function Pyramidal or extra pyramidal tracts ky names Reabsorption of Na and glucose Receptors classification Summation Synapse Synpse Thryoid hormones formation Types of receptors Vit D3 What are mechano receptors and electromagnetic receptors What is fatigue What is receptor and classify What is summation What is synapse and its characteristics What is the role of basal ganglia and their location mostly endocrine,ant pituitary hormones,hypothalamus factors, cushing syndrome,thyroid hormones,cooling center etc Addison's disease Gastric reflexes names Hormones released during fasting? When is CCK released?
MA’AM ROHEEN
Angiotensin-2 functions Astigmatism Blind spot other than physiological hoga to kia kahengy usy Blindspot Canal of Schlemm Ceruloplasmin role and function and diseases [significance] Dark and light adaptation Decibel is unit for? Fovea centralis Hearing unit How it is maintained Intraocular and extraocular muscles Intraocular pressure Juxtramedullary nephron Kisme nai hota wo pigment Kn sa pigment hota h eye me Limbic system eye reflexes consensual light reflex qq hota hyy Visual area Brocas speech area accommodation reflex Is Visual area concerned with limbic system Pain fibers name Perimetery or is related questions Perimetry chart Physiological blind spot Presbycus Proteins formed in liver their name Renin Retinal layers Scomata Sensory receptors Squint Visual purple What if intraocular pressure increases Which diseases are found by perimetery method With age sound Kitna decrease hota h mostly special senses:auditory pathway,tectorial membrane,perilymph ,organ of corti,glaucoma ,thalamic nuclei Basilar membrane Dark adaptation Hair cells and types and how are they stimulated Light adaptation Vestibular apparatus functions If afferent and efferent arterioles are constricted how will it effect the GFR All tracts in spinal cord Dorsal white colum or spinal cord It's pathway and type of sensation caried by it Receptors present on the skin Pain receptors All tracts function and sensation carried by them Premotor cortex It's area ,function . Substantia nigra Chart of colour vision Ishihara chart plate name Receptors for hearing Coclea full Difference between Endo lymph and Pari lymph
SIR ALAM MENGAL
(All about CNS ) Ascending tracts Astygmatism Basal ganglia functioning mechanism Basal ganglia role in movements Basal ganglion functional division Broca's area Color blindness Components of reflex arc Effector organs Equilibrium kesy maintain Hoti h Eta fiber kucch is tarah poocha Hippocampus k function How many rods are stimulated by a single photon How spinal cord controls posture Internal SIR Alam Knee jerk reflex Motor cranial nerve Muscle spindles and golgi tendon Nervous centres for superficial reflexes Pain and temperature area in brain Pain pathway Physiology of nightmare Reflexes ki classification Retina Rinnes test Rods and cones Sleep wake cycle Spinal cord s directly control hone wale 3 reflex Sulcus and gyrus Temperature Types of reflexes(physiological basis) Vestibular apparatus k function Vestibular nerve k division Visual acuity Visual field Visual pathway Visual purple Which part of brain controls fear and how Withdraw reflex Wo kn sa tract h jo head neck and arms ki movement control krta h associated with vision Basilar membrane Dark adaptation Hair cells and types and how are they stimulated Light adaptation Names of extrapyramidal tracts Role of cerbellum in posture Ruberospinal tract function Superficial reflexes names Supplementary motor area and function Vestibular apparatus functions
MA’AM NARGIS
Ant pitutary Hormones External hormones of anterior pituitary and post pituitary If afferent and efferent arterioles are constricted how will it effect the GFR Adrenal cortex ke hormones Agr koi patient larkara k chal rha then brain k kis part me msla hai(cerebellum puchna chah rhi thi) All tracts function and sensation carried by them All tracts in spinal cord Ampula of vater kahan khulta or agr iski blockage ho then Kya hota.. Ant. Pit hormenes name Basal ganglion functions Basal ganglion me circuits Beliverdin ke degradation Bile formation plus secretion plus it's contents Bile synthesis +excretion Characteristics of synapse Chart of colour vision Coclea full Cognitive function of basal ganglion. Cortisol ke functions Defecation definition Defecation reflex and mechanism. Difference between Endo lymph and Peri lymph Dorsal white column or spinal cord Electromagnetic Receptors ky examples Estrogen and progesterone functions in males External Facilitation Fatigue how it occur. Filtration coefficient Function of ADH Function of placenta Functions of zinc GFR (factors ,,, measure kesy krty) GFR and dependants GFR formula Glucagon ke functions Glumerolus pressure. If bilirubin con increased then what happens In obsructive jaundice how we know that where is problem Ishihara chart plate name Broca’s areas and function It's pathway and type of sensation carried by it Kidney k Hormones LH functions in body Other conditions in which HCG is positive and Males mein kab ata hai positive Master gland Hormones. Myopia Myopia causes, correction and why concave glasses are used. Net filtration pressure and its formula Pain receptors Placenta ki konsi layer se hcg ata hai Pregnancy strip mein C line ki kya importance hai and why is it confused Premotor cortex Prolactin functions Proprioception is carried by(Dorsal column) Putamen n caudate function Pyramidal or extra pyramidal tracts ky names Receptors classification Receptors for hearing Receptors present on the skin Small intestine hormones. Substantia nigra Synapse Testosterone functions in body What is summation. Where Estrogen in male produces and functions in male. Which mineral helps in calcium absorption in body
MA’AM MEHWISH
Thalamus ke functions Thalamic nuclei Thalamic nuclei ke functions Dorsal tracts pyramidal or extra pyramidal tracts ke function or reticular formation kya hota hyy with functions functional division of cerebrum, diff broadman areas, hypothalmic nuclei, cerebrum tracts detailed , descending ones,substantia nigra, basal ganglia etcc
PRACTICAL QUESTIONS
Cretinism or dwarfism may farq protein hormones cortex area name and 8 functions All cranial nerves And performance is not confined to the given practical.. Knee jerk reflex Mostly he made reflexes performed blue green colour deficiency indicate it through Ishihara chart Rinnie test Swabach test light reflex Ankle jerkk trigeminal motor and facial sensory examination rinne's test Temperature Visual acuity Agr osteoarthritis hwa he r hm ne immediately check krna h tensdon reflex to kia krn ge Upper motor neuron lesion me kia hota h Reinforcement Hypothermia superficial and deep reflexes knee jerk pendular knee jerk qq hoga Hypothermia q hota hyy
#2nd year#sophomore#MBBS#medical school#Viva#MedStudents#Medicine#MD#Bolan Medical College#Balochistan
0 notes
Text

Chronic pain is defined as pain persisting longer than 3 months despite medical treatment. This form of pain affects roughly about 100 million people in the United States. While most people can heal from a sustained injury over time, others fail to return to their original state. Sometimes the reason for chronic pain is obvious, such as arthritis or neuropathy, but other times there is no persisting injury or illness to explain the situation. Pain is a signal of danger and a required means for survival. Pain serves as a warning to the body to protect injured tissue from more damage. Those born with a congenital insensitivity to pain tend to die at an early age as there are no warning signs to signal impending damage beyond repair.

Pain nociception is transmitted through the spinothalamic pathway and is initiated with a pain stimulus from peripheral nociceptors on lightly myelinated A-delta and unmyelinated C fibers that synapse at the dorsal horn of the spinal cord. The cell bodies of both fiber types are in the dorsal root ganglia. Nociceptors are free, branching nerve endings with ion channels activated by mechanical force, oxygen deprivation, temperature extremes and chemicals. Nociceptor activation induces 2 distinct pain signal perceptions. The first pain is a fast, sharp reflex response mediated by A-delta fibers. The second is a longer-lasting, dull pain mediated by C fibers that ascends to and synapses at the thalamus and somatosensory cortex contralaterally. At a peripheral level, cytokines recruit macrophages to release growth factors, such as BDNF, to replace nerve fibers and synapses that have been damaged throughout the process.
Pain is expected to be an acute threat and resolution is expected after a period of recovery. However, pain that persists beyond expected healing time is thought to be due to a “hijacked” biological system responsible for pain response. So how exactly does acute pain become chronic pain? This process is dependent on neural plasticity and is due to various alterations that occur throughout the spinothalamic pathway. One possibility pertains to the growth factors released to replace damaged nerves as they are not specific. This non-specificity allows non-pain A-beta fibers and sympathetic fibers to sprout out of pain fibers A-delta and C, creating an abnormal connection. This results in non-painful stimuli being recognized as painful stimuli. This condition is known as allodynia, in which pain is caused by a stimulus that does not traditionally provoke it.

Another possibility occurs when a severe injury is sustained, such as those during a major car accident. In this case, C fibers are constantly fired and allow for increased sensitivity of neurons in the dorsal horn. Constant stimulation of the C fibers leads to increased presynaptic glutamate release, activation of postsynaptic AMPA receptors and depolarization of the postsynaptic neuron. This causes displacement of Mg2+ in NMDA channels, allowing an influx of calcium. This influx triggers second messenger activation and thus, gene transcription responsible for an increase in AMPA receptors. Increasing the number of AMPA receptors causes greater stimulation of dorsal horn neurons. This phenomenon is commonly known as “wind up” and seen in hyperalgesia, where a minor injury causes crippling pain.

These alterations in the spinothalamic pathway, whether co-existing or separate, cause overall changes in neurobiology and thus, alters how the body reacts to pain. These changes prevent the ability to distinguish between pain signaling a threat and pain that results due to a hijacked system with abnormal connections. Nonetheless, there are a variety of medications to treat chronic pain based on these alterations in the spinothalamic pathway. Tricyclic antidepressants and serotonin-norepinephrine reuptake inhibitors allow increased serotonin and norepinephrine levels by allowing them to persist in the synapse longer than normal, leading to an increase of endogenous opioid release. Gabapentin and pregabalin decrease pain by dampening signal transmission in nerves by mimicking inhibitory neurotransmitter GABA and decreasing excitatory neurotransmitter glutamate. Opioid use is not ideal for chronic pain due to its addictive properties. Many opioid addictions start with prescription drugs.

In addition to medication, cognitive behavioral therapy has been found to be powerful in eliminating the psychological aspects of chronic pain that can prolong recovery. Long-term pain negatively impacts a person’s mood and increases the risk for depression, anxiety, and substance abuse. It impedes the ability to perform daily activities, such as getting out of bed and going to work. The therapy involves exercise and cognitive reframing that acts to eliminate negative reinforcement associated with movement.

0 notes
Photo

Extra medullary compression of the spinal cord. For discussion of these images, follow episode five and six of podcast ‘Clinical neurology with KD’ in Apple podcast, Spotify or Google podcast. An extramedullary compressive lesion goes through three stages, according to Oppenheim. An initial stage of radicular pain and segmental motor and sensory symptoms. The initial phase is followed by a Brown-Sequard syndrome and finally a complete transection of the cord. The rapidity of development of these stages depends on the aetiology and can be acute or chronic. Some of the cardinal features of extramedullary compression include Radicular or root pain, which is a unilateral lancinating pain down the dermatome on coughing, straining, or Valsalva. The patient will have early corticospinal tract involvement with lower limb spasticity more than the upper limb. The leg is more involved as leg fibres are laterally placed in the corticospinal tract than arm fibres. The LMN findings are rare and, if present, occur at the segmental level at the site of compression. The patient will have only late bladder involvement. They have ascending paresthesia as sacral fibres are laterally placed in the spinothalamic tract. Funicular or tract pain is less common. The patient can have vertebral pain and tenderness, which suggest extramedullary extradural lesion. #clinicalneurologywithkd #neurologyteachingclub #paediatricneurology #NTC #neurology #neurosciences #neuro #clinicalneurology #medicine #clinicalmedicine #criticalcaremedicine #mbbs #medicos #doctors #neuroanatomy #casediscussion #medicineresidents #residency #medschool #futureneurologist #neuroimages #NEET #finalmbbs #neetpg #neetsuperspeciality #neetmedicine #eanneurology #nejm #emergencymedicine #spinalcord https://www.instagram.com/p/Cds4asLpst1/?igshid=NGJjMDIxMWI=
#clinicalneurologywithkd#neurologyteachingclub#paediatricneurology#ntc#neurology#neurosciences#neuro#clinicalneurology#medicine#clinicalmedicine#criticalcaremedicine#mbbs#medicos#doctors#neuroanatomy#casediscussion#medicineresidents#residency#medschool#futureneurologist#neuroimages#neet#finalmbbs#neetpg#neetsuperspeciality#neetmedicine#eanneurology#nejm#emergencymedicine#spinalcord
0 notes