
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by docmary and here's what we found interesting.
Average Info
Notes Per Post
12
Likes Per Post
8
Reblog Per Post
2
Reply Per Post
2
Time Between Posts
1 month
Number of Posts By Type
Text
10
Photo
1
Quote
1
Last Seen Tumblr Blogs





Fun Fact
Tumblr was created by web developers David Karp and Marco Arment.
Text

Civilization in a Time of Pandemic turned 1 today!
0 notes
Text
Biotech companies have achieved a stunning victory for humanity against a deadly virus—and they are being total asshats

On August 19, 2019, the Business Roundtable announced their revised “Statement on the Purpose of a Corporation”, which called on business leaders to expand the focus of their companies beyond profitability. The statement was a commitment to more than just shareholders. Other stakeholders such as employees, suppliers, customers, the community in which they work, et cetera should also benefit from their efforts. Maybe you’ve noticed a lot of virtue signaling in ad campaigns that emphasize their support of diversity, and puppies, and keeping plastic out of the ocean. No doubt Adam Smith is rolling over in his grave. The statement was signed by 181 of 188 members of the roundtable including Alex Gorsky, CEO and Chair of the Board of Johnson & Johnson (JnJ) and Dr. Albert Bourla, CEO of Pfizer.[1]
It may seem like there are plenty of vaccines because, in the US, we can’t get a vocal minority to get vaccinated unless they are threatened with losing their jobs and, sometimes, not even then. Such a first world problem. This is not the case in much of the rest of the world. There is a hundred-fold difference in vaccine availability between wealthy and low-income nations. The sub-Saharan vaccination rate is less than four percent. Not only is COVID creating a terrible disease burden, but it is also taking away scarce resources from tuberculosis (TB) care and prevention, treatment for malaria, childhood immunizations, et cetera. Reports from community health workers in Africa indicate that when people seek care for respiratory illnesses they are sent out for a COVID test, which may come back negative, but they do not return to be evaluated for TB. Some sources pre-pandemic predicted that TB would be eradicated by 2035, but that timeline is no longer achievable. That is just one of many ways in which the pandemic is wreaking havoc on the poor and vulnerable.
After the COVID-19 summit held in the White House in late September, President Biden announced that the United States would purchase 500 million doses of the Pfizer-BioNTech vaccine to donate to low-income countries, mostly through COVAX, an initiative dedicated to equitable vaccine access led by the Global Access Vaccine Initiative (GAVI); the Coalition for Epidemic Preparedness Innovations (CEPI); the World Health Organization (WHO); and the United Nations International Children’s Emergency Fund (UNICEF). (For more information about COVAX, see my previous blog post The politics of a pandemic, how not to manage coronavirus). This brings the total doses the US has pledged to low-income countries to 1.1 billion, although at that point only about 160 million doses had been shipped out.[2]That is great, but donations are not enough. If we are to get the pandemic under control, we must ramp up production—and that is a huge problem.
Scaling up production is the single most important thing we can do to address the pandemic globally. Because at the current rate there’s not enough production of effective vaccines to vaccinate the world until at least 2023.
Dr. Tom Freiden
President and CEO of Resolve to Save Lives
Director of the Centers for Disease Control and Prevention (CDC) in the Obama administration
The summit didn’t produce any breakthrough on waiving intellectual property protection for vaccines, transferring mRNA vaccine making technology to regional manufacturing hubs, or even renegotiating contracts so that the vaccine doses coming off the production line get to the countries that need them most (the additional Pfizer doses won’t be shipped out until next year).
At this point Pfizer and Moderna are the most promising candidates to win the war on COVID-19. Unlike JnJ, a vaccine which is a viral vector and utilizes a weakened adenovirus which is a biological process, Pfizer and Moderna are mRNA vaccines and those are chemical processes. (For more information on these processes, see my previous blogs Happy Coronaversary and Anti-vaxxers, Vaccine Hesitant and I want that shot so bad I would get it in my eye.) The biological process is more cumbersome and susceptible to delays in production. The chemical process is faster and much easier to tweak when new variants emerge.
It’s important to recognize that our government has a kind of compact with vaccine manufacturers.
The government indemnifies vaccine makers, so they won’t have to pay damages for vaccine side effects.
The government trains clinicians. Usually, drug companies send detail people around to do that.
The government operates the supply chain.
The government educates the public.
All these things that a drug company would usually do, the government does. In exchange, they’re supposed to be good corporate citizens—as Pfizer and Moderna have not been.
What is the story with Pfizer and Moderna?
Over one billion dollars of taxpayer money and the expertise of the National Institute of Allergy and Infectious Disease (NIAID) scientists have allowed Moderna to develop it’s COVID-19 vaccine. And they refuse to share that technology with the rest of the world. It’s morally inexcusable, but they have come up with excuses, all of which are untrue.
“We can’t transfer technology because we don’t have enough staff.” They have chosen not to have enough staff.
“We can’t transfer technology because it takes 12-18 months to scale up.” It took one partner of theirs, Lanza, between three and six months, depending on how you count it.
“The world will have enough vaccine in 2022.” That is kind of true if you count vaccines that don’t work very well.
“Africa can’t use the vaccine effectively.” Such BS. Africans have much less vaccine hesitancy than people in the US and most Western countries. They have a greater ability to run vaccination campaigns because it is something they do regularly.
To be sure, Moderna, which started up in 2010, has always been a bit sleazy. In February 2016, a Nature article criticized Moderna for not publishing any peer-reviewed articles on its technology, unlike most emerging and established biotech companies.[3] In May 2020 Moncef Slaoui resigned from the board of directors of the company to take the lead on “Operation Warp Speed”, designed to accelerate the development of a COVID-19 vaccine during the Trump administration. Slaui continued to hold more than $10 million in stock options while the federal government invested $483 million to assist Moderna in vaccine trials—an obvious conflict of interest.[4]
There’s also a horrific and, frankly, racist narrative that countries in Africa won’t be able to use the vaccine. Now that’s certainly true when you just dump a lot of leftover vaccines. I know one small area in Africa that got seven different vaccines with short expiration dates, no planning, no predictable supply. So yeah, in that situation you’ll have problems.
Dr. Tom Freiden
President and CEO of Resolve to Save Lives
Director of the Centers for Disease Control and Prevention (CDC) in the Obama administration
Scaling up manufacturing can be done in ways that won’t harm these companies. You can respect intellectual property—pay them royalties. When other companies find ways to tweak the process, Pfizer and Moderna can benefit from these improvements. Win-Win.
An article from Public Citizen in August, reveals that the Department of Health and Human Services (HHS) has detailed information on how Moderna makes their vaccine, including the exact amounts of every ingredient and step-by-step instructions on manufacturing and testing. They have the “recipe” for the Moderna vaccine and probably has the legal authority to disclose that information to whomever it pleases.[5]The problem is that unless we use the Pfizer or Moderna vaccine, that company will have to go through clinical trials all over again and that takes time.
At this point it makes sense to try and figure out which companies can make the mRNA vaccines on a scale required to provide vaccines to low-income countries in a timely manner and giving the information to them.
Holding Moderna’s feet to the fire
I’m not just picking on Moderna, but they have gotten a lot of money from the US government, and we do have their technical information at HHS, so we have more leverage with them than with Pfizer.
In June 2021, US Senators Tina Smith (D-Minn.) and Bill Cassidy, MD, (R-LA) sent a letter to the Chair of the Senate Health, Education, Labor, and Pensions (HELP) Committee, Senator Patty Murray (D-Wash) and Ranking Member Richard Burr (R-NC) requesting they hold a hearing to examine global vaccine production and distribution. Along with Senators Smith and Cassidy, Senators Tammy Baldwin (D-Wis), Mitt Romney (R-Utah), and Lisa Murkowski (R-Alaska) support a public hearing with federal officials, supply chain experts, and vaccine manufacturers to improve vaccine equity globally. There 22 Senators on the HELP committee and residents of these states should write to them to support this hearing.
What’s in it for me?
Of course, improving vaccine equity is the ethical thing to do. (Pardon me while I put on my Captain Obvious cap). It’s also in our self-interest. In a week in which we have reached the five million death total globally, that is not in doubt.
Global travel and trade will not resume until the pandemic is under control. Global instability will increase as well. The risk of more dangerous variants emerging, spreading, and harming us here is greater the more uncontrolled spread there is. The less vaccine there is, the more risk of uncontrolled spread. The more uncontrolled spread there is, the greater the risk of dangerous variants. We have gone through too many cycles of COVID-19. Bottom line-nobody is safe until everybody is safe.
[1]Retrieved from: https://www.businessroundtable.org/business-roundtable-redefines-the-purpose-of-a-corporation-to-promote-an-economy-that-serves-all-americans
[2]Fawcett, J. VP of Policy and Advocacy, Results. September 23,2021. Four quick takeaways from the White House COVID-19 summit. Retrieved from: https://results.org/blog/four-quick-takeaways-from-the-white-house-covid-19-summit/?eType=EmailBlastContent&eId=dd055a2c-4692-4da7-867f-1def76722d20
[3]Research not fit to print. Nat Biotechnol 34, 115 (2016). doi: 10.1038/nbt.3488. retrieved from: https://rdcu.be/cAFr5
[4]Corcoran,K. 5/6/2016. The ex-pharma exec leading Trump’s COVID-19 vaccine program has $10 million in stock options for a company getting federal funding, Business Insider. Retrieved from: https://www.businessinsider.com/moncef-slaoui-leading-trump-vaccine-push-10m-holding-moderna-conflict-2020-5-2016
[5]Morton, CJ, Rizvi, Z, Sarpatwari, A. September 22, 2021. President Biden already has the COVID vaccine recipe. He should share it. Health Affairs blog. doi: 10.1377/hblog20210922.937772 retrieved from: https://www.healthaffairs.org/do/10.1377/hblog20210922.937772/full/
0 notes
Text
Mea Culpa
It’s been about 50 years since I went to confession. I am not looking for absolution. I just want to get this off my chest. When SARS CoV-2, the virus that causes COVID-19, reached our shores (literally, as I live not far from Kirkland, Washington), and anti-masking became political theatre, I had two thoughts almost simultaneously about these anti-maskers:
Gee, if there were only more people in the world like you, there would be fewer people in the world like you.
And
Nature’s way of thinning the radishes.
I was too polite to ever say such things out loud.
Of course, the vast majority of people who have endured intubation, COVID-19 long-haul, the death of a loved one, or any of the many complications of the virus, did not earn my impure thoughts. Whether becoming ill was because of living or working in a congregate living facility such as a nursing home, or a consequence being a frontline worker, or just because of bad luck, I apologize to these individuals and their loved ones.
Yes, in fact, I was the person who was quoting John Donne just a couple of months ago: “Any man’s death diminishes me…”. (from my post "The politics of a pandemic, how not to manage coronavirus") But that was when it seemed like we were turning the corner in the United States in terms of morbidity and mortality and the economic disaster that resulted from the pandemic. We needed to set our sights on other hot spots like India and Brazil. We still do. With a fast-moving pandemic, nobody is safe unless everyone is safe.
Now we are in our fourth wave of the virus and since July 1, 2021:
Cases and hospitalizations have soared: both hit six-month peaks last week.
The stock market has dropped from record highs.
Consumer confidence had the sharpest 3-week decline since November 2020 when the third wave of the coronavirus was roaring through much of the US.[1]
Delta Blues:
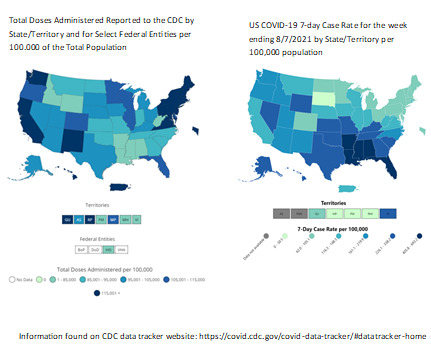
The COVID-19 Delta variant is now the dominant strain of coronavirus in the US. According to the Centers for Disease Control and Prevention (CDC), in the week ending 8/7/2021, we have, on average, 210 new cases per 100,000 population.[2] The CDC also reports that each person with the Delta variant will transmit the virus to an average of five unvaccinated people-more than twice the rate of infections caused by the original strain. In Washington state, the Department of Health reports that 94% of recent cases, hospitalizations, and deaths from COVID-19 are among those that are not fully vaccinated.[3]
In other news, the Biden administration hit it’s target of getting 70% of adults in the US having received at least one vaccine shot on August 2, almost a month past the original target date of July 4.[4] In a surprise to no one, states with the lowest vaccination rates are experiencing the biggest surge in COVID cases, hospitalizations, and deaths. This has, no doubt, led to an increase in the number of people who have gotten the jab in the last month or so.
Multisystem Inflammatory Syndrome in Children (MIS-C)
While children continue to have low rates of severe illness, hospitalization, and death associated with COVID-19, those numbers are increasing. MIS-C is a rare but serious complication associated with SARS CoV-2 infection in children. As of October, 2020, there had been 1,000 cases of MIS-C reported to the CDC. As of 8/13/2021, that number is 4,404, with 37 deaths reported. The median age is nine years old. Sixty-three percent of cases in which race and ethnicity are reported occur in Hispanic/Latino or Black/non-Hispanic children. These demographics are associated with more severe illness in adults as well. Ninety-nine percent of children with MIS-C test positive for SARS CoV-2, the other 1% have had exposure to COVID-19.
Reported MIS-C Case Ranges by Jurisdiction, on or before July 30, 2021
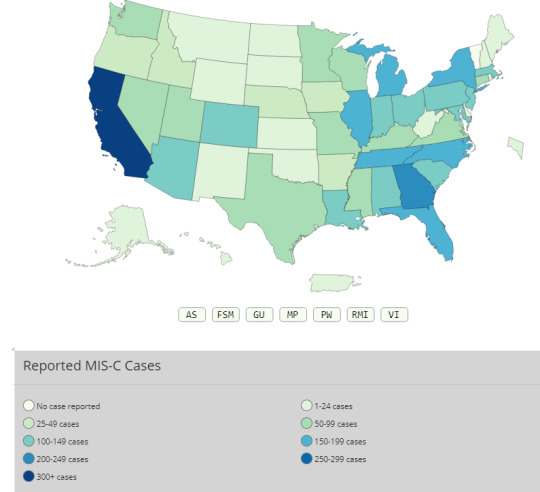
retrieved from: https://covid.cdc.gov/covid-data-tracker/#mis-national-surveillance
Carrots and Sticks
At present there are approximately 90 million people in the US who have held off on getting vaccinated. There are probably three main reasons for this:
1. People who lead a very healthy lifestyle. Let’s be honest. That is not most of us. But as long as they follow other public health guidelines like wearing masks, staying away from vulnerable people and children that are not eligible for the vaccine, they might be able to do that for as long as it takes. Let’s face it, social isolation is not a hardship for some of us.
2. People who just haven’t made it a priority to get vaccinated but don’t have strong beliefs one way or the other on the relative risks of getting COVID vs. the COVID vaccines.
3. Freedom. I don’t understand this one, but I am told it’s a thing. They are certainly the most vocal and probably the least likely to have the “we are all in this together” attitude. My parents, who went through the rationing of World War II as well as my father's service in the army to defeat Hitler, would no doubt laugh at these folks if their ideas didn’t result in such tragic consequences. These “freedom fighters” are putting a tremendous strain on a healthcare system that wasn’t all that great, especially in terms of equity, to begin with. It gives me no joy to know that these are the radishes that nature will thin most aggressively.
If not being intubated or putting your loved ones at risk is not incentive enough to get vaccinated, some states have tried other incentives like a million dollar lottery and marijuana (joints for jabs) as "carrots" to encourage the unvaccinated to close the vaccination gap.
The stick approach involves mandates. Federal, state, and local government does not like to use the M-word, and corporations are even less inclined to make people either get vaccinated or submit to nasal exploration 1-2 times per week as a requirement for employment, but they are warming up to the idea. Many school districts will no doubt follow suit. This may also give some people cover if they were initially anti-vaxxers or vaccine hesitant but have since become more open to the idea of the COVID vaccine.
There is no shame in admitting that you were previously speaking from a less informed place.
- Kelly Hayes, author from the Menominee nation
My Take:
It is beginning to dawn on me that I may not live to see a post-pandemic world. I hope I'm wrong but in case I'm not, how do I manage this new reality?
The wise adapt themselves to circumstances, as water molds itself to the pitcher. – Chinese Proverb
There will be those that won’t get vaccinated no matter what. Their choice. Despite our differences, we are going to have to find a way to live with each other and coronavirus. I would like to believe that we could unite against this existential crisis but we are not there-yet. In the meantime, we have to find a way of communicating our own needs and boundaries while accepting the needs and boundaries of others in a respectful way.
We also have to look at the wider picture. Wealthier nations should send the extra vaccines that we have scarfed up to COVAX, an initiative dedicated to equitable access to vaccines, particularly to healthcare workers and those most at risk who live live in less affluent countries. For more information on COVAX, see my previous post; "The politics of a pandemic" This organization is ready to get more vaccines and the ability to administer them to countries that would love to get the jabs that our citizens have decided, for whatever reason, to refuse. This is not just white savior complex, it is enlightened self-interest.
Less affluent nations are huge reservoirs of virus that continue to produce more variants. Not only does COVID cause a tremendous disease burden, it also takes a bite out of limited resources that are used to combat other deadly diseases like tuberculosis (TB). I heard a story out of Africa that when local clinics send people with respiratory symptoms to get tested for COVID, if those tests come back negative, the patient doesn’t necessarily get sent back to get screened for TB. That is not good.
As John Donne recommended 500 years ago, “do not send to know for whom the bell tolls, it tolls for thee.”
[1] Keckley, P. 2021. Delta variant exposes two flaws that could undermine recovery, The Keckley Report, 8/2/2021.
[2] https://covid.cdc.gov/covid-data-tracker/#cases_casesper100klast7days
[3] Olympia, WA (AP). Report: 94% of COVID-19 deaths among not fully vaccinated, 7/30/2021. Retrieved from: https://www.medscape.com/viewarticle/955761?src=WNL_mdpls_210806_mscpedit_wir&uac=81725MZ&spon=17&impID=3551586&faf=1
[4]Kalter, L. 2021. US hits 70% of adults with at least one vaccine dose, Web MD Health News, 8/2/2021. Retrieved from: https://www.medscape.com/viewarticle/955884?src=WNL_mdpls_210806_mscpedit_wir&uac=81725MZ&spon=17&impID=3551586&faf=1,
0 notes
Text
The politics of a pandemic, how not to manage coronavirus
No man is an island, Entire of itself, Every man is a piece of the continent, A part of the main. If a clod be washed away by the sea, Europe is the less. As well as if a promontory were. As well as if a manor of thy friend's Or of thine own were: Any man's death diminishes me,
Because I am involved in mankind, And therefore never send to know for whom the bell tolls.
It tolls for thee.
John Donne
1624
The poet John Donne warned of the dangers of isolation and imagining oneself as self-sufficient, without need of community. It was true 500 years ago; it still holds true today. No man is an island…every man is a part of the main. As wave upon wave of SARS-CoV-2 reached every continent, even Antarctica, most of us have tried to isolate ourselves on this crowded planet - with mixed results.
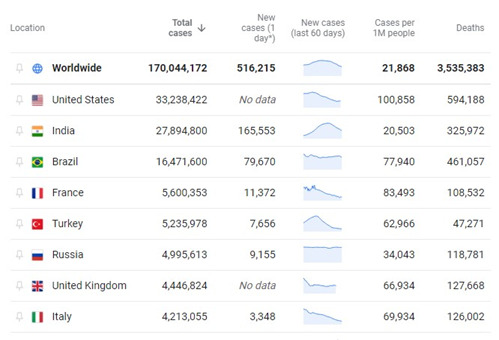
As of May 30, 2021, by every metric, the United States was leading the world in the number of cases and deaths from COVD-19. Brazil and India are catching up quickly. In the US, the underlying tension between public health and personal liberty has had disastrous consequences. As successful as the vaccine roll-out has been, and even with the numbers of new cases, hospitalizations, and deaths dropping, this is no time to be complacent.
India, with a population of over 1 billion, and Brazil, a pariah among countries in Latin America for its poor response to the pandemic, cause or should cause great concern to everyone everywhere. Not having the resources of rich countries, they will require help to manage the tragic situation their leaders have put their populations in and it is in our interest to do so because...the bell tolls for thee.
India
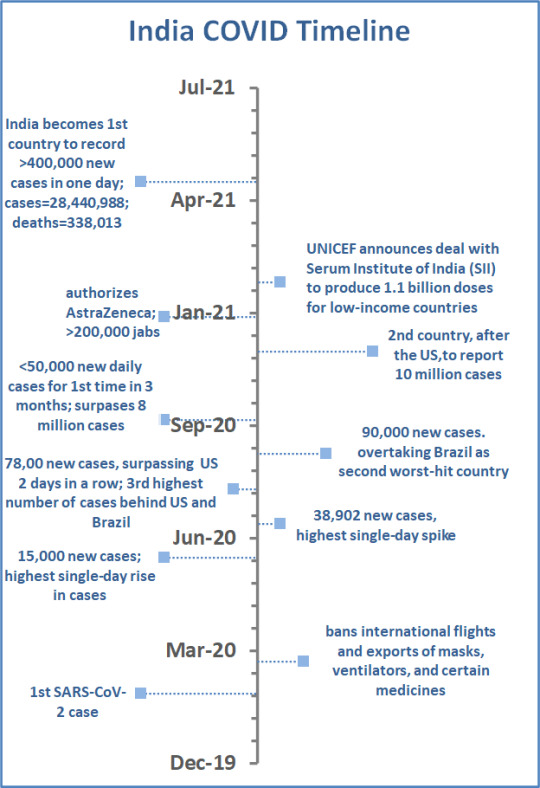
When the World Health Organization (WHO) declared COVID-19 a global pandemic in March 2020, there had been 330,000 cases and 30,000 deaths from SARS-CoV-2 reported worldwide. In the early days of the pandemic, India was considered a model of how to manage the worst public health crisis in recent memory. India responded with a strict lockdown. International flights and exports of masks, ventilators, and certain medicines were banned. As a result, India did not see the same initial explosion in new cases and deaths compared to other countries.
Three months later, India’s Prime Minister Narendra Modi began easing lockdown restrictions - like the American football player who does the end-zone dance on the two-yard line—not a good idea. When the lockdown lifted, many Indians stopped taking precautions. Mr. Modi allowed large gatherings, including campaigns in state elections that he attended, without wearing a mask, at rallies of thousands of mask-less supporters, to help his governing Bharatiya Janata party. Large religious festivals resumed drawing millions of people as well. By July 2020, India had seen 600,000 cases and 17,834 deaths due to COVID. An editorial from The Lancet, said that Mr. Modi “seemed more intent on removing criticism” on social media than “trying to control the pandemic.” Sound familiar?
As recently as March 2021, India’s health minister assured the public that they had reached the pandemic’s “endgame”.
The New York Times reported in May 2021 that India was responsible for more than half of the world’s daily COVID cases, setting a record-breaking pace of 400,000 new cases in one day. Researchers believe the B.1.1.7 variant and the delta variant, which are also major variants in Britain and the US, are to blame for the surge. Clinics across India report desperate shortages of hospital beds, protective equipment, and oxygen.[1]
Just to add to the global disaster, India is one of the world’s leading vaccine manufacturers. It is struggling to inoculate its own citizens; less than 10% of Indians have gotten even one dose.[2] In September 2020, Serum Institute of India (SII) received $150 million from the Bill and Melinda Gates foundation to accelerate production of Oxford University’s AstraZenica (AZ) vaccine and the American vaccine Novavax as soon as the WHO granted regulatory approval. Under the original terms of the agreement, 50% of vaccines would be earmarked for India and the remainder would go to other low- and middle-income countries.[3]Currently, exports of vaccines from India have been shut down.
Brazil
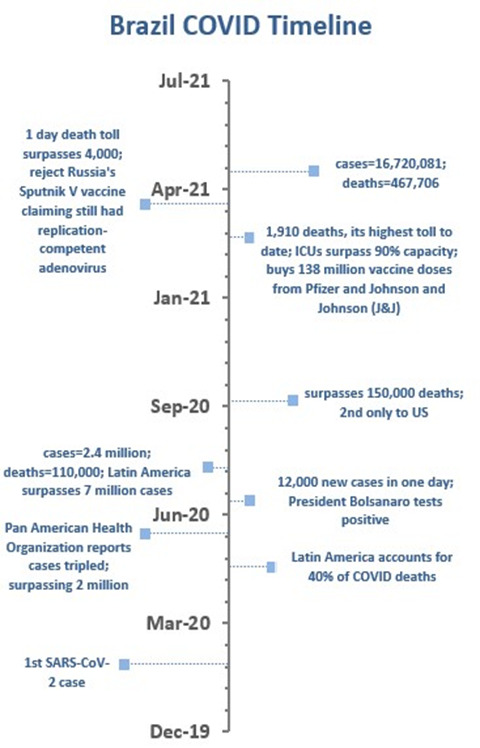
In an editorial from The Lancet, dated May 9, 2020, the president of Brazil, Jair Bolsanoro, was criticized for allowing the SARS-CoV-2 virus to spread widely while presenting himself as a “messiah” touting unproven medicines like hydroxychloroquine, with support from his rightwing allies.
At the time, Brazil had the most cases (105,000) and deaths (72,88) in Latin America. Estimates suggest the death rate was doubling every five days. When asked by a reporter about the rapidly increasing numbers of COVID-19 cases, Mr. Bolsanaro responded: “So what? What do you want me to do?”[4]
In March 2021, Brazil’s pandemic spiraled out of control. Its Latin American neighbors grounded flights, closed land borders, and regional sports events were canceled in attempts to stop the P.1 variant (and approximately 90 other variants) from spreading to their populations.
The British Medical Journal reported that 400,000 Brazilians have died from COVID-19—13% of deaths worldwide.[5] Some models predict the death toll in Brazil will reach half a million this month. That trajectory could be an indicator for what is to come for its neighbors. As Paraguay’s director of health surveillance, Guillermo Sequera, has said: “When Brazil sneezes, Paraguay gets a cold.”[6]
COVAX
With a fast-moving pandemic, no one is safe, unless everyone is safe.
author unknown. Retrieved from: https://www.who.int/initiatives/act-accelerator/covax
COVAX is an initiative dedicated to equitable access to a vaccine, particularly to healthcare workers and those most at risk. To date (5/31/2021), COVAX has shipped more than 77 million COVID-19 vaccines to 127 participants. It is co-led by[7]:
CEPI-Coalition for Epidemic Preparedness Innovations. The governing board has 12 voting members; four investors and eight independent members with competencies in industry, global health, science, resource mobilization, and finance—and five observers (17 total). Financial support comes from public sources including US Agency for International Development (USAID).
Gavi, the Vaccine Alliance-a public/private partnership which has helped to vaccinate 760 million children in the world’s poorest countries.[8] It ensures that infrastructure is in place and technical support is available to make sure that COVID-19 vaccines can be safely delivered to support the participation of 92 lower-middle and lower-income economies. It is part of the health systems work of Access to COVID-19 Tools (ACT) Accelerator effort, focusing on areas where it has expertise and experience, such as keeping vaccines at the correct temperature.
World Health Organization (WHO)
United Nations International Children’s Emergency Fund (UNICEF)
COVAX hopes to get 280 million doses of vaccines to Latin America but has been hit with delays to eight manufacturers (including SII) it has deals with and does not expect to deliver them until the end of 2021.[8]This has led South American nations to look to China’s Coronavac and Russia’s Sputnik V vaccine supplies. One study found that Coronovac was only 50% effective after a single dose. The Biden administration has pledged to purchase 500 million doses of Pfizer BioNTech vaccine to give to COVAX; the first 200 million doses will be distributed this year, with the subsequent 300 million in the first half of next year.[10]
My Take
In what can only be called being one step ahead of the game, armed robbers in Hong Kong stole $16,000 worth of toilet paper as coronavirus sparked panic-buying of essential goods a month before WHO declared a global pandemic in March 2020.[11] (Good times)
In July 2020, President Trump formally notified Congress and the United Nations that the US was withdrawing from WHO because of course he did.
Several articles, including one from the Journal of the American Medical Association (JAMA)[12] have compared weekly deaths in the US that would be expected from historical trends with COVID and non-COVID deaths from March 2020 until January 2021. There was an increase of 22.9% of all-cause mortality. This far exceeds expectations. Excess deaths attributed to non-COVID causes could be the result of deaths that were, in fact, COVID but misclassified. They might also be due to delayed care, an overwhelmed healthcare system, or behavioral health crises. On the other side of the ledger, no doubt at least some of the deaths that would have been anticipated from non-COVID causes might have died from the coronavirus instead. Which is to say, these are at best estimates of the mortality rates. During surges in various parts of the US, deaths from several non-COVID diseases like heart disease and Alzheimer’s increased. Either way, the excess deaths could have been helped with a better response to the pandemic early on.[13]
For those “give me liberty, or give me death” fans, do I really need to point out that Patrick Henry was referring to his own death, not the deaths of millions all over the world? My parents’ generation made many sacrifices during WWII, including blood and treasure, and considered it worth the price to defeat Hitler. Wearing a mask to defeat a virus? Really? Who have we become?
It comes as a surprise to no one that the countries with the largest death tolls to date, the US, India, and Brazil, are also countries in which partisan politics was the priority over public health measures. It isn’t a good idea. Why don’t we just stop?
[1] What to know about India’s coronavirus crisis. What is behind the explosion of new coronavirus cases that is overwhelming the South Asian country? NY Times, May 25, 2021. Retrieved from: https://www.nytimes.com/article/india-coronavirus-cases-deaths.html
[2] ibid
[3]Raghavan, P. 2020. $150 million dollar shot for serum production of COVID vaccine, India Express.
[4]Lancet editorial. September 19, 2020. COVID-19 in Brazil: “So what?”, Lancet, 395: 1461. doi: 10.1016/s0140-6736(20)31095-3
[5]Taylor, L. 5/20/2021. COVID-19: How the Brazilian variant took hold of South America, BMJ 2021, 373: n1277. doi: 10.1136/bmj.n1277
[6]ibid
[7]World Health Organization: COVAX Working for global equitable access to COVID-19 vaccines. Retrieved from: https://www.who.int/initiatives/act-accelerator/covax
[8]Raghavan. Op cit.
[9]Taylor. Op cit.
[10] Page, T, Rauhala, E. Jun 9, 2021. Biden administration to buy 500 million Pfizer coronavirus vaccine doses to donate to the world, Washington Post, retrieved from: https://www.washingtonpost.com/politics/biden-vaccine-donate/2021/06/09/c2744674-c934-11eb-93fa-9053a95eb9f2_story.html
[11]www.thinkglobalhealth.org/article1
[12]Woolf, SH, Chapman, DH, Sabo, RT, Zimmerman, EB. May 4,2021.Excess deaths from COVID-19 and other causes in the US, March 1 2020, to January 2, 2021,JAMA, 325(17): 1786-1789. doi: 10.1001/jama.2021.5199
[13]ibid
2 notes
·
View notes
Text
Vaccine hesitancy, molecular mimicry, and blood clots (oh my!)
There were many mixed messages in the world of coronavirus last week. Just as it appears that Michigan is the lead state in the fourth wave of the virus, the US is about to hit a “vaccine wall” as demand drops for vaccinations even though the supply is greatly improved. In the first three months of the rollout for the Pfizer, Moderna, and the Johnson & Johnson/Jantzen (J&J) vaccines, getting shots into arms of the most vulnerable has required a full court press from public health departments and the healthcare establishment, as well as persistence on the part of those trying to wrangle an appointment. The results from state to state have been uneven.
Figure 1

So far 14 states have administered fewer than 75% of the doses distributed to them with Alabama having the lowest vaccination rate per capita. Twenty states have administered more than 80% of the doses distributed to them with the most vaccinations per capita in New Hampshire.[1]
Vaccine Hesitancy:
The good news for those who want to get vaccinated is that it is a whole lot easier to get an appointment now. That said, the goal of herd immunity is a long way off and with demand dropping for jabs, we may not get there. Vaccine hesitancy is an important reason for declining demand and that is a shifting picture.
In a study that was put out by the Kaiser Family Foundation (KFF) in December, 52% of Black Americans said they would “wait and see” before signing up for the vaccine while only 20% said they wanted the shot as soon as possible. The share of Black people who were skeptical of the vaccines was higher than for White respondents (36%) and Latinx (43%).[2]
By March of this year, 55% of Black respondents to another KFF survey said they had been vaccinated or wanted the vaccine as soon as possible. Twenty-four percent were still holding back. Blacks have been one of the hardest hit demographics of COVID-19 and that has, no doubt, played a part in changing minds. Another possible reason for the turnaround in willingness to get vaccinated is because there has been a concerted outreach effort tapping trusted sources such as Barack Obama, sports stars, and other influencers such as Black ministers to address vaccine hesitancy among Black people.
The Urban Institute’s September 2020 Coronavirus Tracking Survey, a nationally representative survey of adults ages 18-64, asked people whether in the last 12 months they had ever felt a doctor, other health care provider, or their staff judged them unfairly or discriminated against them based on their race/ethnicity, gender, gender identity, sexual orientation, a disability, or a health condition and about the consequences of these experiences. This survey indicated that perceptions of discrimination and unfair judgement while seeking health care were higher among Black adults than among Hispanic and White adults in the previous 12 months (September 2019-September 2020).[3]
Figure 2
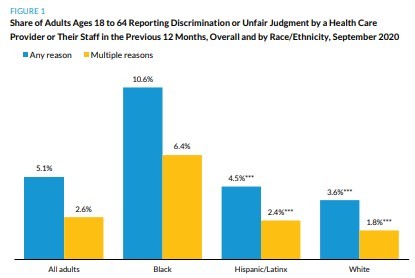
A “food desert” is described as an urban area that does not have a grocery store within one mile or a rural area that does not have one within ten miles. There is also a “pharmacy desert” that generally occurs in primarily Black neighborhoods in urban areas as well as in rural areas. People of color are less likely to have a family primary care provider and so access to information about the individual’s risks and benefits of getting vaccinated from a trusted source, much less getting an appointment for the vaccine itself, is often more challenging than it is for White people. My guess is that these experiences and the barriers to appropriate care contributed to the initial skepticism among people of color generally and Black people specifically in the initial rollout phase.
FIGURE 3
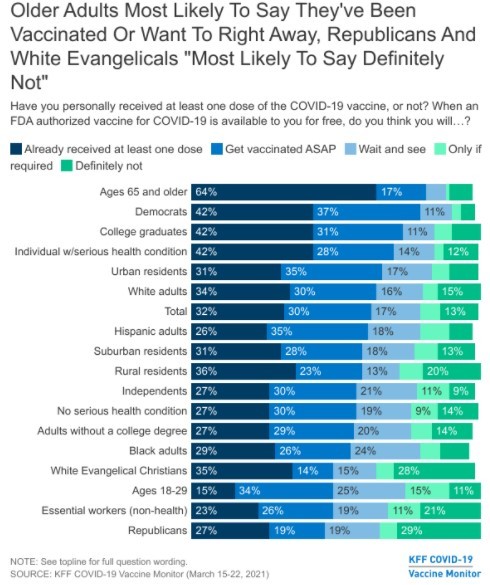
Meanwhile, Republicans and Evangelical Christians were the most likely groups to say they will not get vaccinated, according to the KFF survey.[4] I do not have an explanation for that. I also don’t know how wearing masks got politicized last year. If anyone has an explanation that doesn’t involve a gang of Democratic, cannibal pedophiles, I am really interested in hearing it.
Molecular mimicry and autoimmune disease:
There are science-based reasons that some are reluctant to get vaccinated. An issue that has been little discussed publicly is molecular mimicry. The theory is that some part of the spike protein of SARS-CoV-2, the virus that causes COVID-19 and is replicated in our cells, is similar enough to our own tissues that the immune system starts attacking our own cells thinking that those cells are the virus. Thus, the vaccine could trigger an autoimmune disease like rheumatoid arthritis, lupus, multiple sclerosis, or other autoimmune condition.
In one study looking for similar protein sequences between the SARS-CoV-2 virus with protein sequences in humans and other mammals, as well as other human coronaviruses, the number of shared protein sequences at two particular sites was quite high for humans, rats, and mice but miniscule or not at all with other human coronaviruses, cats, dogs, rabbits, chimpanzees, gorillas, or macaques.[5] Sadly, the investigators did not include bats, which I think of as flying rats, but that’s just me. It has been hypothesized that the original source of COVID-19 was from bats. Could the virus have molecular mimicry with bats? If so, what does that mean for the species?
These authors believe that much of the damage seen in the “cytokine storm” that causes the worst damage in COVID-19 may, in fact, be due to this molecular mimicry between the virus and, for example, lung tissue. It should also be noted that molecular mimicry from the whole SARS-CoV-2 virus is much more likely than it is from a small part of the virus (the spike protein). If the vaccine can trigger an autoimmune disease, so can the whole virus.
The presence and level of autoantibodies (AAbs) that attack our own cells, frequently detected in patients with COVID-19, are significantly associated with hospitalization and more severe prognosis. Clinically, these patients are more likely to have respiratory distress, acute cardiac injury, acute kidney injury, multi-organ dysfunction with such common complications as coagulopathy and thrombocytopathy (put a pin in this one as it is also at play with blood clots). [6]
Blood Clots and the J&J and AstraZeneca (AZ) vaccines:
Last week the J&J vaccine rollout was put on pause by the Food and Drug Administration (FDA) because six women developed unusual blood clots after receiving this vaccination. This was six out of seven million shots given. Some saw this as an over-reaction by the FDA that would likely lead to more vaccine hesitancy. However, these blood clots are different from clots that occur from “the usual suspects” like oral contraceptives and smoking.
Figure 4
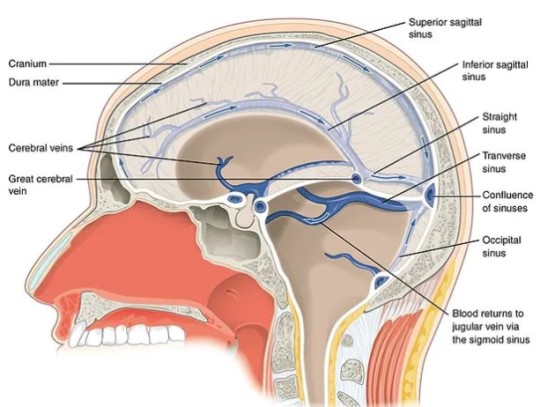
A normal number of platelets is between 150,000-450,000 per microliter of blood (there are 1,000 microliters in one milliliter). If you have less than 150,000 platelets per microliter, you have a deficiency called thrombocytopenia. In the clots associated with the viral vector vaccines (J&J in the US and AZ in Europe), the platelets tend to stick together in the veins of the brain, which causes a blockage known as a cerebral venous system thromboembolism (CVST). This creates back pressure of blood in the brain itself, causing damage in the same way a hemorrhagic stroke would. [7]
“Normal” clots are usually treated with a blood thinner called heparin. With vaccine-induced prothrombotic immune thrombocytopenia (VIPIT), there is a deficiency of platelets and so that treatment would only make things worse. While the Centers for Disease Control and Prevention (CDC) and the FDA are getting the word out to doctors not to use heparin, they are also looking for ways of figuring out which people are more at risk for this extremely rare complication. Putting the vaccine on pause was clearly the ethical thing to do and this kind of transparency gives me greater confidence in the vaccine rollout.
As is the case with molecular mimicry, the danger of VIPIT happening if a person gets COVID-19 is much higher than it is from either the J&J or the AZ vaccine.
“…If the mechanism is the same, one can speculate that the high occurrence in COVID-19 vs. vaccination is because the whole virus is more thrombogenic [likely to cause clots] than the spike protein alone.” Paolo Madeddu, professor of experimental medicine at the University of Bristol[8]
Symptoms associated with VIPIT include headache, tiny red spots under the skin, blurred vision, fainting or loss of consciousness, impaired movement in parts of the body, or coma. With either of these vaccines these blood clots, so far, only occurs 4-20 days after vaccination. Scientists believe that symptoms before or after that window are likely due to another cause.
It is important to note that COVID-19 itself has been reported to lead to thrombocytopenia (low blood platelets) in up to 41% of positive patients, with the figure going up to 95% of those with severe disease.[9]
Cause for cautious optimism:
Two separate studies published in the New England Journal of Medicine on April 9 indicated that in the case of the AZ vaccine, used in Europe, VIPIT was due to rogue antibodies against platelet factor 4 (PF4). This complication is similar to heparin-induced thrombocytopenia (HIT) and is diagnosed and treated the same way. It can be diagnosed with a lab test called ELISA that is pre-treated with PF4. If there is a big immune response, that means the patient has VIPIT. To be clear, there are lots of things that can cause blood clots and health professionals want to know what the cause is because the appropriate treatment is dependent on what is causing the problem. VIPIT from the AZ vaccine is treated with the administration of intravenous immunoglobins (IVG) and anti-coagulants. The J&J vaccine was not used in either of these studies and so we do not yet know if the same is true for that vaccine, but both are the same type of (viral vector) vaccine and both use an adenovirus as the viral vector.[10]
If we can get the one-and-done J&J vaccine back in use safely, that would be especially helpful for vaccinating unsheltered people. It would also be much easier to use in rural areas because J&J can be stored in a regular refrigerator unlike the Pfizer and Moderna vaccines that must be kept frozen.
My take:
For those who choose not to get vaccinated, for whatever reason, hoping to ride the coronavirus out, you should know that even without a vaccine, the SARS epidemic that hit Asia in 2002 did eventually go away, or, more likely, mutated to a less lethal virus. It took four years, but it can happen. However, that is not what always happens. Case in point, smallpox, which was around since at least the fourth century until it was declared eradicated by the World Health Organization in 1980. I don’t think I know anyone who has had smallpox and I may not know anyone who knows anyone who has had smallpox. In that case, the vaccine worked as intended.
Maybe you may feel like you are strong and healthy and even if you got COVID-19, you are unlikely to get significantly sick. Consider the possibility that you could be asymptomatic but still spread the disease. There are just no options that are completely risk free. Choose wisely.
[1]Romeo, A. (4/15/2021). America is about to hit a “vaccine wall” as demand drops—with or without Johnson & Johnson, Yahoo News. [2]Bunn, C. (4/12/2021). Vaccine hesitancy among Black Americans has turned a corner. Here’s why.”, NBC News. [3]Gonzalez, D., Skopor, L., McDaniel, M., Kenney, G.M. (4/2021). Perceptions of discrimination and unfair judgement while seeking health care, findings from the September 11-28 Coronavirus Tracking Survey, Urban Institute Health Policy Center. Retrieved from: https://www.urban.org/sites/default/files/publication/103953/perceptions-of-discrimination-and-unfair-judgment-while-seeking-health-care_0.pdf [4] Hamel, L., Lopez, L., Kearney, A., Brodie, M.(3/30/2021) KFF COVID-19 monitor: March 2021. Retrieved from: https://www.kff.org/coronavirus-covid-19/poll-finding/kff-covid-19-vaccine-monitor-march-2021/ [5]Kanduc, D., Shoenfeld, Y. (9/18/2020). Molecular mimicry between SARS-CoV-2 spike glycoprotein and mammalian proteomes: implications for the vaccine, Immunol. Res. doi: 10.1007/s12026-020-09152-6 [6]Macela, A, Kubelkovak, K. (3/22/2021). Why does SARS-Co-V-2 infection induce autoantibody production? Pathogens, 10(3). doi: 10.3390/pathogens10030380 [7]Taylor, A. (4/16/2021). Blood clot risks: comparing AstraZenica vaccine and the contraceptive pill, The Conversation. Retrieved from: https://theconversation.com/blood-clot-risks-comparing-the-astrazeneca-vaccine-and-the-contraceptive-pill-158652 [8]Russell, P. (4/15/2021). Vaccines carry far lower risk for rare blood clots than COVID, study shows, Medscape News UK [9] Op cit Taylor, A. (4/9/2021). [10] Grenacher, A., et. al. (4/9/2021). Thrombocytic thrombocytopenia after ChAdOx1 nCoV-19 vaccination, NEJM. doi:10.1056/NEJMoa2104840Schulz,NH, et. al. (4/9/2021). Thrombocytic thrombocytopenia after ChAdOx1 nCoV-19 vaccination, NEJM. doi: 10/1056/NEJMoa2104882
#vaccination#covidー19#astrazeneca vaccine#johnson and johnson#blood clots#molecular mimicry#autoimmune disease
4 notes
·
View notes
Text
Happy Coronaversary
Last weekend, I celebrated the first Coronaversery by doing something that I had not done in what seems like forever…I had actual friends over to my place. We hugged, we ate pastries, we laughed—all without masks on. Woo Hoo! My friends brought me a stationary bike that they did not need any more; and I can stand to get rid of a little of the excess baggage I have accumulated in the last year, so it is a welcome gift. All three of us have gotten fully vaccinated and human contact feels less treacherous.
In my last post (Ant-Vaxxers, Vaccine Hesitant, and I want that shot so badly I would get it in my eye), I wrote about the Moderna and Pfizer COVID-19 vaccines. Now there is a new kid on the block, Johnson and Johnson’s (JnJ’s) Janssen COVID-19 vaccine. This is a different type of vaccine. It is a single shot and can be stored up to 30 days in an ordinary refrigerator. JnJ has teamed up with a competitor, Merck, to ramp up production of their vaccine, which begs the question, if they can get along why can’t we? But that is for a different post.
Content Warning-This part can be a bit technical. If that does not appeal to you, feel free to scroll past it to the next section.
The JnJ vaccine uses a viral vector, the adenovirus, which causes the common cold. Adenovirus, rhinovirus, coronavirus—all these virus families cause the common cold and health care providers do not typically go to the trouble of finding out which “flavor” of the cold a person has. The adenovirus has been modified so that it cannot make a person sick. The virus also contains the genetic code for the spike protein on the outside of SARS-CoV-2, the virus that causes COVID-19. (For more information on the spike protein, see my previous post, Anti-Vaxxers…).
The modified adenovirus gets absorbed into our cells and travels to the nucleus where mRNA for the spike protein is made. The mRNA, just like with the Pfizer and Moderna vaccines, goes to the ribosomes in the cell and replicates spike proteins. From there, the spike proteins get into the blood stream and are identified by the immune system as a foreign invader. Our immune system produces antibodies to the spike protein so that if we are exposed to the real deal (COVID-19), our immune system will destroy it.
To reiterate: The mRNA vaccines (Pfizer and Moderna) contain manufactured mRNA inside a lipid particle that have instructions for making the spike protein on the outside of the virus, and ribosomes in our cells start making the spike proteins from that. In JnJ’s vaccine, the genetic code for spike protein is carried on a modified adenovirus where it travels to the nucleus of our own cells, our cells manufacture mRNA for the spike protein, and then our ribosomes manufacture the spike proteins, etc. It is not possible to get COVID-19 or any other infectious illness from the vaccines.
Viral vector technology has been used by JnJ previously in a vaccine against the Ebola virus in Africa. JnJ is also using this platform to develop vaccines for human immunovirus (HIV), respiratory syncytial virus (RSV), and Zika virus.
Side effects from COVID-19 vaccines:
The most worrisome adverse reaction to any vaccine is a severe allergic reaction which can include:
· Difficulty breathing
· Swelling of the face and throat
· A fast heartbeat
· A bad rash all over your body
· Dizziness and weakness
If these symptoms occur, it will usually happen within an hour of injection and that is why when a person gets a shot, they are advised to stick around for 15-30 minutes so that if a severe allergic reaction happens, the person can get a shot of epinephrine, which usually will fix the problem. For other less serious side effects that are bothersome or just linger on too long, call the clinic where you got the vaccine or your primary care provider for advice.
How do these vaccines compare to each other?
The data we have from clinical trials indicate that the mRNA vaccines are 95% effective in preventing disease that is severe enough to cause obvious symptoms: shortness of breath, loss of taste or smell, fever, muscle aches and pains are the most common ones. It is still possible that a person can be an asymptomatic carrier; we just do not know for sure at this point.
The JnJ vaccine has been 66% effective world-wide and 75% effective in the US at preventing symptomatic disease. However, the mRNA vaccines went through phase-3 (human trials) earlier than the JnJ trials, which also included South Africa and Brazil at a time when more contagious variants of the virus were circulating. It is not an apples-to-apples comparison.
All the vaccines that have been approved for emergency use authorization by the FDA are nearly 100% effective at preventing disease severe enough to require hospitalization and in the handful of cases that did require such measures, the patients were well enough to be discharged within 28 days of being vaccinated. To date, none of the 75,000 people who got the active vaccine (as opposed to the placebo) in any of the clinical trials, as has died of COVID-19.
Religious concerns:
Although communities of faith do not speak with one voice on the matter, there are some who object to the JnJ vaccine due to the use of fetal embryonic stem cells in the manufacturing process of their vaccine. The stem cell line was developed prior to the George W Bush administration’s decision to prohibit the use of any new fetal stem cell line for research purposes in the US. There is no fetal stem cell tissue in the vaccine itself.
If you plan on getting vaccinated:
There are some steps you can take while you are waiting for your turn, and afterwards, that are based on naturopathic principles. These recommendations have not been through any clinical trials on COVID-19 specifically. I hope someday those trials will be done. In the meantime, if you have health concerns or are taking medications that may pose a problem, talk it over with a licensed naturopathic doctor or a similarly trained health care professional in your area.
Probiotics-the term “human microbiota” or “human microbiome” refers to the trillions of bacteria, viruses, and fungi that populate our bodies. Most of them populate the intestinal tract (gut microbiota). The microbiota plays a key role in the development of the immune system throughout life. Also, the immune system contributes to maintaining microbial homeostasis. Specifically, research has shown that microbiota can influence the immune response to vaccination.[1]
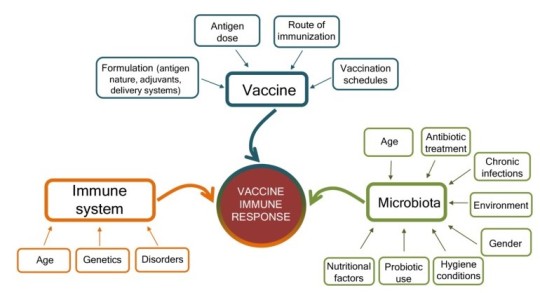
These friendly bacteria can be taken in supplement form and/or can be part of the diet from fermented food such as yogurt, kombucha, sauerkraut, or miso. If you can start loading up on probiotics a week or two prior to vaccination as well as afterwards, it might be helpful.
Zinc—one of the early signs of COVID-19 is loss of the sense of taste or smell. This is also a sign of zinc deficiency.
Vitamin D—is commonly deficient in Blacks and Hispanics as well as older people.
Support the circulatory system—especially after the vaccination when arm pain can be significant at the injection sight. Exercise is a fabulous way to get that blood circulating. Another option is to have lymphatic massage. Contact your local lymphedema society for a referral to a massage therapist or physical therapist that specializes in lymphatic massage.
Reduce inflammation—if you can avoid using ibuprofen or acetaminophen prior to getting the vaccine, that is recommended so that you do not inhibit the immune response. Afterwards, these OTC medications can be used if necessary. Foods such as onions, garlic, ginger, and turmeric also have anti-inflammatory properties.
Get plenty of good quality rest for a day or two after vaccination—avoid operating heavy equipment, make important decisions, or use sharp things in the kitchen or anywhere else. Also, a tip for people who sleep on their sides, get the shot in the arm that you do not sleep on.
Kindness—lending someone your strength instead of reminding them of their weakness.
I was listening to one of the bazillion interviews Tony Fauci has been giving since the Biden administration took over. He was discussing herd immunity. He brought up the fact that in the wild, herd animals, such as wildebeests, will form a circle when a predator is nearby. The strongest animals will be on the outside of the circle and the more vulnerable will be in the center. As I have never said, if it is good enough for wildebeests, it is good enough for me. TAKE CARE OF EACH OTHER.
[1]Ciabattini,A, Oliviere, R, Lazzeri, E, Medaglini, D. (2019). Role of the microbiota in the modulation of vaccine immune responses, Front Microbiol 2019; 10.1305. doi: 10.3389/fmicb.2019.1305
#covid 19#vaccine#johnson and johnson#pfizer#moderna inc#side effects#management#herd immunity#covid-19
0 notes

Text
Anti-Vaxxers, Vaccine Hesitant, and “I want that shot so badly I would get it in my eye.”
To Vaccinate or Not to Vaccinate
There is a difference between the Anti-Vaxxers and the Vaccine Hesitant. The first group doesn’t want to get any vaccines, largely on ideological grounds. Anti-Vaxxers often site an article that came out in 1996 in the prestigious medical journal The Lancet, that claimed to have found a link between the measles, mumps and rubella vaccine (MMR) and autism. Later it was discovered that Wakefield, the primary author, had fudged some of the data and so the article was withdrawn. I understand some of the concerns about vaccinations, especially the “all their shots while they’re tots (before age 2)” campaign. I hold some of these ideas. I am just persuadable. Full disclosure, I have gotten the first dose of a COVID-19 vaccine and intend to get the second one. I have several reasons for deciding to get vaccinated which all come down to I’d rather be vaccinated than intubated.
The Vaccine Hesitant are likely to have been fully vaccinated and have chosen the same for their children. They just aren’t convinced that these particular vaccines are safe and are willing to take their chances with the wild virus. The speed at which these vaccines were developed and an unfortunate relationship between the medical community and the Black community in particular are among the reasons for this hesitancy.
What is mRNA?
Ribonucleic acid (RNA) is a single strand of nucleic acid, unlike deoxyribonucleic acid (DNA) which is double stranded and shaped in a double helix pattern.

Messenger RNA (mRNA) has the instructions for building amino acids that combine to build proteins. These proteins are assembled inside the cell using the ribosomes in the cytoplasm. Biotech companies have looked for ways to use mRNA as a way of creating fetal stem cells, fighting cancer, and treating diseases like zika virus and rabies since the 1970′s. Not until Pfizer and Moderna were granted emergency use authorization by the Food and Drug Administration (FDA) for their COVID-19 vaccines had any mRNA application had ever been approved. More information on the history of mRNA
���Researchers understood [mRNA’s] role as a recipe book for the body’s trillions of cells…The concept: By making precise tweaks to synthetic mRNA and injecting people with it, any cell in the body could be transformed into an on-demand drug factory.”[1]
The Pfizer and Moderna vaccines are two mRNA vaccines that have instructions for making the spike protein that gives the virus a crowned appearance (corona=crown), and that spike allows the virus to attach to human cells.
These spike proteins are then transported out of the cell where white blood cells recognize them as foreign invaders (antigens) and makes antibodies to them. These antibodies remember those spike proteins and will attack them again if the person is exposed to the real deal-COVID-19.
This is different from the way traditional vaccines work to stimulate the immune system by exposure to weakened (attenuated) forms of the whole virus. They are also different in that they do not have preservatives such as thimerisol (mercury) or adjuvants.
The mRNA vaccines don’t posses the “recipe” for the entire virus. It just takes over the manufacturing capabilities of our own cells to make a protein located on the outside of the virus that is considered harmless. It cannot give the vaccinated person COVID-19. After our cells have made the copies of the spike protein, the mRNA is destroyed. The mRNA does not get into the nucleus of the cell and cannot, therefore, effect the DNA in our own cells.
The first vaccine shot doesn’t usually have much in the way of side effects other than pain at the injection site (and yes, it really hurts). The second shot usually results in a more robust response because the immune system was primed 3-4 weeks earlier. (Not because that is the shot that has the microchip in it so that Bill Gates can track your every move. 😊)
That said, this is a relatively new technology.
The most worrisome reaction to the vaccine so far is an immediate hypersensitivity reaction including anaphylaxis. The current recommendation from the Centers for Disease Control and Prevention (CDC) is to wait 15-30 minutes at the place where the vaccine was administered in case that happens. In most severe allergic reactions, a shot of epinephrine will successfully treat the reaction.
It is too soon to tell whether there will be long-term consequences of these vaccines or how they compare to the other vaccine models that are seeking FDA approval.
In a recent report from the New York Times, of the 75,000 brave people who received one of the five vaccines in clinical trials (Pfizer, Moderna, AstraZenica, Novavax, and Johnson & Johnson), not a single person has died of COVID-19, and only a few have been hospitalized. In those handful of cases that required hospitalization, all were discharged within 28 days from when they received the vaccine. Compare that to 150 dead from COVID-19 per 75,000 Americans and normally 5-10/year from influenza. To be sure, people have died after having been vaccinated and those numbers are tracked by Vaccine Adverse Event Reporting System (VAERS). However, that does not mean they died from the vaccine. It just means they got the vaccine and died from whatever cause at some point later.
My Take:
Anecdotally, I suspect that a Venn diagram of Anti-Vaxxers and Anti-Maskers, would have a lot of overlap between those groups. I have no evidence for this belief, I just think it’s true. I also believe the overlap between the “I want that shot so badly I would get it in my eye” group and health care providers working on COVID wards is significant.
But what about the Vaccine Hesitant? Even among people in the healthcare field there is hesitancy, especially in nursing home staff. The most common reason cited is the speed at which these vaccines were developed. They are often waiting to see what happens in the people who do get vaccinated and may wait to get their shots until spring or summer.
Communities of Color:
Black, Hispanic, and Native American people are about four times more likely to be hospitalized and nearly three times more likely to die of COVID-19 than white people. The Kaiser Family Foundation found 35% of Black people said they do not plan on getting vaccinated. That is understandable. The stain of the Tuskegee experiment, where more than 600 Black men with syphilis were falsely told they had been treated for the disease and were followed for four decades while men died, went blind, and had other serious complications of syphilis. This plays a part in that reluctance. More information on the Tuskegee experiment
In another notorious case, Henrietta Lacks’s cancer cells were used for medical research without her or her family’s knowledge, and without financial compensation.[3] These and other cases in which Black people have been mistreated by the medical community have sown seeds of mistrust.
The Native population has been much more open to getting vaccinated. A survey of 1,435 Native Americans across 46 states found that 75% of participants were willing to receive a vaccine, according to a report by the Seattle-based Urban Indian Health Institute.[4] Having lived in Alaska for many years, this does not surprise me. The Native community holds their elders in high esteem and often live in multi-generational households. Protecting the elders would be consistent with Native core values.
For my part, I will be getting my booster dose, implementing public health measures such as wearing masks and social distancing, staying home when feeling ill, etc. I do it for my own health. As I said before, I’d rather be vaccinated than intubated. I am also doing it because our health system is stretched thin. If I need to go to the hospital at some point, it would be great if there was a bed for me. I know we still have questions that are not yet answered but if I have been able to address some of the questions for the Vaccine Hesitant, then my work here is done.
[1] Garde, D and Saltzman, j. The Story of mRNA: How a once-dismissed idea became a leading technology in the COVID vaccine race, STAT, retrieved from: https://www.statnews.com/2020/11/10/the-story-of-mrna-how-a-once-dismissed-idea-became-a-leading-technology-in-the-covid-vaccine-race
[2] Young, S., (2/3/2021). Black COVID-19 Vaccine Hesitancy rooted in mistrust, fear, WebMD, retrieved from: Medscape.com/viewarticle/945199
[3] Skloot, R.(2011). The immortal life of Henrietta Lacks, Crown Publishing.
[4] Hellman, M. (2/1/2021). How a Native American COVID-19 vaccination rollout is a model for community-centered approaches. Retrieved from: https://www.seattletimes.com/seattle-news/health/we-take-it-for-our-community-how-a-native-american-survey-and-vaccine-rollout-models-a-community-centered-approach
1 note
·
View note
Text
Food Insecurity-We may not live by bread alone, but neither do we live without it.
The test of our progress is not whether we add more to the abundance of those who have much; it is whether we provide enough to those who have little. Franklin D. Roosevelt
It has been my good fortune to have been able to support myself (barely at times) doing the work that I love, being a naturopathic doctor, for most of my adult life. I remember a sign in my tax preparers office that read: “The joys of owning your own business, not unlike the joys of natural childbirth, have been greatly exaggerated.” Or something like that. There are certainly those in my profession that have been financially successful along with the intrinsic rewards of helping people, but I was not one of them.
And then I got cancer. And not dying became my full-time job. On the side I also worked as a home health aide and I made little money but also had little in the way of responsibility. I also relied on programs like Supplemental Nutrition Assistance Program (SNAP), also known as food stamps to survive.
I am doing well now. I have relocated from Alaska (my home of 30 years) to Washington state where I grew up, so that I could be closer to family. I was fortunate in that I had family to take me in while I figured out my next moves. Some are not so lucky.
I started volunteering at the Sky Valley Food Bank in my new community as a way to build my social network. I was blessed with the instant camaraderie of many fellow and sister volunteers, and paid staff, who were joined in a single purpose: support the mission of eliminating hunger. Every week we provided food for an average of 261 families, enough for 10 meals per person. This amounts to more than 75,000 pounds of food distributed every month—almost one million pounds per year.
And Then Came COVID-19
According to data from the US Department of Agriculture (USDA), some 13.7 million households (10.5% of all households), experienced food insecurity at some point in 2019. That is 35 million Americans who were either unable to acquire enough food to meet their needs, or uncertain of where their next meal might come from.
In one study that came out in June 2020, researchers asked: “In the last seven days, which of these statements best describes the food eaten in your household?”
Enough of the food we wanted to eat
Enough, but not always the kind of food we wanted to eat
Sometimes not enough to eat
Often not enough to eat.
According to these researchers, since 2019, food insecurity has doubled overall and tripled in households with children.*
The Ripple Effects of Hunger
Not having access to healthy food has ripple effects of chronic ill health, disability, stress, and worsening poverty. These problems did not start with COVID-19, but the pandemic has made even more glaring the differences in the quality of life between “those who have much [and] those who have little.” This kind of safety net, that supplies sustenance to those in need, makes good economic sense. Adults who have a disability, in particular a disability and are not in the workforce, also experience more than twice the rate of food insecurity as adults who do not have a disability.

At our local food bank, we were unable to have our customers shop in-doors like we had in the past safely. We were shut down but found a way to deliver boxes of food to the porches of 125 families in the area. We also drastically cut down on the number of volunteers that could be in our warehouse per day which translates to fewer people doing more physically demanding work. The good news is that people from the community, from gardeners, to private businesses, to social service organizations, and individuals found ways to help Sky Valley Food Bank carry out the mission.**
School Closures and Vulnerable Students
With schools being shut down, students were no longer able to receive meals at their schools at a reduced price or free as they had in the past. This was not just a local problem, across the country nutrition directors reported that they were serving fewer meals than when school was in session. Last spring, the School Nutrition Association surveyed 2000 districts that reported 80% were serving fewer meals. Of those, the majority said the number of meals had dropped by 50% or more.
Most areas relied on the food pick up model that they usually did in the summer months where families could drop by their local school each day, often between 11-1, and pick up a bag lunch and maybe breakfast. But as parents started returning to work, the pickup model did not always work if parents were not always able to take children to the drop off site at the right time.
In Fulton County Georgia and Tucson Arizona, nutrition programs started packing food including frozen hamburgers and pizza, enough for a week’s worth of meals, and sending them out on school buses to be distributed at bus stops where the lowest income families typically resided.***
Food Deserts
In the best of times getting adequate nutrition is especially challenging for people who live in a “food desert.” The definition of a food desert can change depending on where you live. In urban areas, you need to live more than a mile away from a grocery store. For rural areas, you live more then 10 miles away. According to Feeding America, rural areas make up 63% of counties in the US and 87% of counties with high rates of food insecurity. In 2015, 19 million people lived in a food desert and 2.1 million households both lived in a food desert and lacked access to a vehicle according to the USDA.
The Shifting Model of Getting Food to the Food Insecure
In the summertime at Sky Valley Food Bank, we were able to greet our long-time customers, and many new ones, that were able to shop in our outdoor market. I loved being able to chat with our customers and find out how they were getting along. From my own experience, I can say that accepting help for something as necessary as feeding myself was a blow to my ego. Thank goodness I got over that. Being able to help my fellow and sister humans, regardless of why they were our customers is something I treasure.
Like many school districts around the country, our schools were not able to open in September. We partnered with our public schools to set up food pantries in five of our schools. We also had the return of rainy weather and the outdoor market was not an option. We began having a drive through service where our staff would build boxes of food for distribution in people’s cars. We were now serving 325 families and had special “Holiday” boxes in November and December, along with the usual boxes of meat, dairy, dry goods, canned goods, grains, produce, and food for their four-legged household members. Getting two boxes is better than one box, especially during the holidays.
In December we also had a toy drive that garnered an incredible assortment of toys from community members. It is remarkable how much our community does to provide for people having a tough time—food, toys, money—all gratefully accepted. The parents were able to pick out toys for their kids.
We are looking forward to having our customers back in our service area to carefully select the foods they want for themselves and their loved ones. We are looking forward to giving them the kind of respectful service we always have and continue to provide. COVID or no COVID.
LONE WOLF
I am a lone wolf.
I have lost my pack.
My sire was the first to go. The alfa.
His job to protect the pack, especially from each other, fell to no one.
I grew up with the bitch who was two years my elder.
Always the more adventurous one. She was gone
Before her pups were fully grown.
And they are lost to me.
The she-wolf who bore me tried desperately to keep the pack together.
“Come home. Why don’t you move back home?”
She grew old, frail, a little crazy
A kind of crazy that was always there but kept in check by the alpha.
The older bitch is gone too.
When did the word bitch become derogatory?
I reclaim that title. It suits me.
It suits those of us who live in a world where self sufficiency is prized above all
And sentimentality is a luxury.
Another sire gone. Was it really eight years ago?
He left to be with Jesus.
I think he’s food for flora and fauna.
Who’s to say?
My brother looks up from the hard work of dying
All traces of silliness and the infectious laughter that is his calling card are gone
And the world is just a bit more lonely.
The rest of the pack is dispersed.
Do they prowl in search of the familiar?
Of course they do. (howl)
*IPR.northwester.edu/documents/reports/ipr-rapid-research-reports-pulse-hh-data-10-june-2020.pdf
**Helpful Hint: when thinking of donating food to the food bank, treat the task of going through your pantry the same way you go through your closet—three piles; keep, donate, throw away. You don’t donate clothes that are ripped or stained. You throw them away. The food bank volunteers spend a lot of time sorting through donations. We cannot serve food that is spoiled or way, way, way past the pull date, or that has been opened. Thanks.
***NPR.org/2020/09/08/908442609/children-are-going-hungry-why-schools-are-struggling-to-feed-students
1 note
·
View note
Text
Influenza and the Death of the Spirit World
Let me be clear. This is not my story. Although the story of my ancestors, my maternal grandmother in particular, who came to Ellis Island at about the same time as this story begins has threads of similarity. If this was a time of potato famine, I might tell that story. But this is a time of pandemic and so I will tell this one. I know of this story because Harold Napoleon, a Yup’ik Eskimo from Hooper Bay Alaska, researched the Great Death (Yuut tuqurpallratni) and wrote elegantly about how death on a massive scale destroyed the cultural underpinnings of his society and left scars that continues to affect Alaska Natives today. (Yuuyaraq-The Way of the Human Being, Harold Napoleon)
Before the Russians came to the homeland of the Yup’ik people, the Bering Sea coast and riverbanks of western Alaska, the Yupiit fished and hunted with great reverence for iinruq-the spirit that infused every aspect of their lives. They would show proper respect for the animal spirits that fed their people lest the animals not return to feed them later. Yuuyaraq, “the way of the human being”, guided every aspect of their lives.
The Yupiit believed illnesses were due to ingesting poison, trauma, or evil spirits. The angalkut were the medicine men and women who served as the village historians, physicians, and intermediaries with the spirit world.
Although there were a number of contagious illnesses that the Alaska Native people had no immunity to and that took many lives including small pox, diphtheria, measles, and others, the influenza outbreak of 1900 that began in Nome was the cause of Yuut tuqurpallratni, “when a great many people died,” also known as the Great Death. Estimates are that 60% of Eskimo, Athabascan, and Aleut died from influenza. The anagalkut died in despair along with their people and with them, the ancient spirit world of the Eskimo also died.
Ethnographer Richard K Nelson wrote in his book, Make Prayers to the Raven, based on spending a year studying the culture of the Koyukon Natives in northwestern interior Alaska, of the loss of the spirit world at about the same time but for a different reason. The Koyukon language is Athabaskan and they are ethnically distinct from Eskimos and Aleuts, though they live in close proximity.
“An old shaman, now dead, once said that “all of the medicine people in Alaska worked their power together in the First World War, trying to help the United State toward victory, in so doing they shifted their source of power-the sinh taala’ from the earth itself-far away from their homelands and into the battlefields. But they lacked the power to bring it all back and it became somewhat diffused. After that the shamans’ powers began to wane”.
The two narratives also speak about the presence of Christian missionaries among Native populations. Nelson paraphrases a Jesuit priest, Julian Jette’, throughout his book. Jette’ spent 30 years among the Koyukon people from the early 1900′s and wrote numerous articles and a Koyukon dictionary.
Napoleon speaks of Christian missionary presence less benignly than does Nelson. In his book Napoleon reports that priests and missionaries insisted that the spirit world was evil. The were told that anagalkut were agents of the devil.
Among the Alaska Natives that survived the influenza epidemic of the 1900′s, the shock was unbearable for the women and men who were orphaned by the sudden traumatic loss of the culture that had give them birth. It was decided, without ever really discussing it, to pretend it never happened. To this day, elders who are told about disturbing events in Native villages will often say to young people, “nalluqguak,” pretend it didn’t happen.
“They had a lot to pretend not to know. After all, it was not only that their loved ones had died, they had also seen their world collapse.” -Napoleon
The knowledge of their culture and of the Great Death was suppressed effectively. In the 1950′s Native children received their education in boarding schools that would routinely wash their mouths out with soap if they spoke in their mother tongue. Generations of suppressed emotion, confusion and shame now permeate even the very young. It has led to post traumatic stress disorder on a massive scale, Native people have high rates of incarceration, alcoholism, domestic violence, and suicide. Natives also have high rates of severe illness and death from Covid-19.
The old shaman that Nelson talked to is not around to ask if the diffusion of sinh taala’ is the reason for the loss of shamanic power or a reason for it. Apparently, something happened in the first years of the 20th century that resulted in the diminished role of the spirit world in the lives of Alaska Natives. These explanations are not mutually exclusive.
I do take heart in the resurgence of Alaskan Native culture that is seen in Talking Circles, the reemergence of Native languages, dance, and the subsistence lifestyle as well as the incorporation of tribal doctors in the Indian Health Service. However long it takes, reversing these devastating cultural losses will be well worth it.
#Harold Napolean#Richard Nelson#influenza#post traumatic stress disorder#Covid-19#iinruq#angalkut#spirit world
0 notes
Text
“Health Reform is a BFD” President-elect (Vice President at the time) Joe Biden caught on mic at the signing of the Patient Protection and Affordable Care Act, March 23, 2010 (paraphrased)
On November 10 the United States Supreme Court heard the case of California v Texas which makes the third time the constitutionality of the Patient Protection and Affordable Care Act, often shortened to the Affordable Care Act (ACA) and nicknamed Obamacare, has been before the court. (NFIB v Sebelius 2012, King v Burwell 2015)
To be sure, the ACA isn’t really about healthcare but about health insurance. Arguably, having insurance linked to employment may have made sense in WWII and up until about the 1980′s. However, the runaway costs of medical care, and thus, premiums that employers had to pay to provide health insurance to workers have been a major contributing factor to wage stagnation for middle class and working class families.
If it wasn’t obvious before, it is pretty clear now that we face a second wave of coronavirus and huge disruptions in medical care, restaurants, schools, and so on, that employer-based health insurance doesn’t work any more. As Thomas Jefferson once opined about the institution of slavery, “It’s like holding a wolf by the ears; nobody wants to be here, but how do you let go?”
In the contentious negotiations leading up to the ACA, there were divisions between the economic team that wanted to bring down healthcare costs and the healthcare reform team that wanted to make good quality health insurance accessible to more people. They came together on the requirements that are necessary to fix our broken healthcare system (the three-legged stool):
Health insurance companies could not discriminate against people with pre-existing conditions;
Healthy people would have to buy health insurance;
Companies that had made obscene amounts of money from the status quo would have to accept making less obscene amounts of money.*
The first two requirements would be relatively easy. They were hard won. Despite a rocky launch of the ACA Healthcare.gov marketplace, Obamacare succeeded in bringing the number of uninsured Americans down from 44 million at the end of 2013, to 27 million at the end of 2016; an almost 40% reduction.
Obamacare was modeled on “Romneycare”, named after the former Massachusetts governor and future Republican presidential candidate Mitch Romney. He had overseen the establishment of a statewide health insurance marketplace that succeeded in reducing the number of Massachusetts’s uninsured residents with a combination of carrots and sticks. The carrots were subsidies for people that did not get health insurance from an employer and did not qualify for Medicare, Medicaid, Children’s Health Insurance Program (CHIP), and could not afford to buy private health insurance without help.
The major stick was a tax penalty on people who made above a certain income level and did not have insurance either from an employer or privately purchased (the individual mandate).
“…But to [most economists], as well as the entire insurance industry, the difference between a mandate and no mandate was crucial: If people didn’t have to buy insurance but could instead sign up when they become ill, the resulting wait-until-you-need-it dynamic…would cripple the entire scheme”. -Steven Brill, America’s Bitter Pill, pg. 47.
Is the individual mandate the Achille’s heel of Obamacare?
After attempts to repeal and replace the ACA stalled out in the summer of 2017, Congress reduced the penalty for not purchasing health insurance to $0, effective in 2019, as part of tax reform legislation passed in December 2017. Thus removing any enforcement ability for the individual mandate.
Since then, attorneys general in18 Republican controlled states, with the endorsement of the Trump administration, have brought a lawsuit that calls into question the constitutionality of the ACA in the absence of an individual mandate. In December 2018, US District Judge Reed O’Connor in Texas accepted the GOP argument and declared Obamacare unconstitutional.
One year later the Fifth Circuit Court of Appeals upheld that ruling and sent the case back to the Texas court for “additional analysis” to examine whether the individual mandate was “severable” from the ACA, allowing Obamacare to stand, just without the mandate.
Since then, Democratic attorneys general, lead by California, and the US House of Representatives asked that the Supreme Court to hear the case and, obviously, they agreed to do so. On ABC’s This Week, Speaker of the House Nancy Pelosi said, “[President Trump] doesn’t want to crush the virus. He wants to crush the Affordable Care Act.”
Legal experts have outlined several potential outcomes for this case:
The court could rule on standing, finding that the states and the two people named as plaintiffs haven’t been injured and don’t have a right to sue. That would avoid ruling on the constitutionality of the ACA.
The court could find that the mandate is constitutional or that it is unconstitutional but severable from the rest of the law.
The court could uphold some provisions of the ACA, finding that some mandates, like the mandate and other provisions such as those pertaining to pre-existing conditions, must fall.
The court could find the entire law is unconstitutional.
The Urban Institute estimated that overturning the law would cause 21.1 million more people to be uninsured by 2022. A sudden elimination would affect more than just patients. Insurance companies, drug companies, hospitals and doctors all have changed the way they do business because of incentives and penalties in the health law. If it’s struck down, many of the “rules of the road” would be wiped away, including billing and payment mechanisms.
The ACA has expanded Medicaid coverage in 39 states, the importance of which during the Covid-19 pandemic is sobering. For a health care system that is already on life support, extracting Obamacare will have far reaching consequences.
All Eyes on Georgia
The ruling from the Supreme Court is expected to be out towards the end of June 2021. The Congress could decide to to bring back the individual mandate and make the penalty a token amount and would, in theory, make the whole question moot. This would be a whole lot easier to do if democrats control the House and the Senate.
Between now and January 5, 2021,Georgia voters will face a barrage of campaign ads that frame the 2020 law as a choice between socialized medicine and a lifeline for those who lack access to the health system.
Socialized medicine does not appear to be the boogeyman it used to be when Medicare and Medicaid were first enacted. Last year 181 of 188 members of the Business Roundtable, including CEOS of some prominent healthcare companies, signed on to their newly revised, “Statement on the Purpose of a Corporation.” The statement calls for business leaders to expand the focus of their companies beyond profitability. It seems that business leaders are trying to get ahead of a shifting culture that views socialism as less toxic than baby boomers tend to see it.
Yes President-elect Biden. Health reform is a BFD.
*Although health insurance companies are often seen as the bad guys in our healthcare system, the profits they make are dwarfed by those of the pharmaceutical industry, medical device manufacturers, and so-called nonprofit hospitals.
1 note
·
View note
Quote
Years ago, anthropologist Margaret Mead was asked by a student what she considered the first sign of civilization in a culture. The student expected Mead to talk about fish hooks or clay pots or grinding stones. But no, Mead said that the first sign of civilization in an ancient culture was a femur (thigh bone) that had been broken then healed. Mead explained, that in the animal kingdom, if you break your leg, you die. You can not run from danger, get to the river for a drink or hunt food. You are meat for prowling beasts. No animal survives a broken leg long enough for the bone to heal. A broken femur that has healed is proof that someone has taken time to stay with the person who has fell, has bound up the wound, has carried the person to safety and has tended the person through recovery. 'Helping someone through difficulty is where civilization starts', said Mead. We are at our best when we serve others. Be civilized.
Dr. Ira Byock, The Best Care Possible: A Physician’s Quest to Transform Care Through the End of Life, (Avery, 2012)
The presidential election is all but in the rearview mirror. There is likely to be a chaotic transition, because of course there is. I invite readers to accept Covid-19 for what it is-A PANDEMIC. Not a loyalty test for the left or the right. Not a political statement. A virus.
In the West we don't have recent experience with infectious diseases causing this much death and disability. Asian countries took the SARS-CoV-2 more seriously because they had already gone through Severe Acute Respiratory Syndrome (SARS) from 2003-2007. The previous version of epidemic coronavirus lasted four years, but they were able to get it under control. Because if you don't get a pandemic or an epidemic under control, it becomes endemic, like hepatitis B in Asia, HIV in Africa, and malaria in Africa and Asia. At that point, the virus has won.
The only virus that has ever been completely eradicated is small pox. Viruses don't go away. They adapt. But we can take care of each other. In fact, we must, if civilization is to survive.
In the United States, Covid-19 has revealed inequalities in our healthcare system. It did not create them. This blog is written by me, Mary Minor, a retired naturopathic doctor. I spent almost three decades in Alaska knowing how access to healthcare is vital, not just to the sick and injured, but to people who dare not leave a job they hate or a spouse that terrorizes them because if somebody they care for gets sick or injured...you know the rest of the story, or at least a version of that story. We all do. But this is not who we are. Or at least, it is not pre-ordained. We can do better.
3 notes
·
View notes