
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by ijcmcrjournal and here's what we found interesting.
Average Info
Notes Per Post
2
Likes Per Post
1
Reblog Per Post
1
Reply Per Post
0
Time Between Posts
14 hours
Number of Posts By Type
Text
17
Last Seen Tumblr Blogs





Fun Fact
BuzzFeed published a report claiming that Tumblr was utilized as a distribution channel for Russian agents to influence American voting habits during the 2016 presidential election in Feb 2018.
Text
Major Contributions of the University of Wisconsin to Biomedical Science by E Richard Stiehm*

Abstract
The University of Wisconsin, Madison (UW) is the State University of the State of Wisconsin. It is one of the largest and best known public universities in the USA with 30,000 undergraduates and 14,000 graduate students. These include many students and visiting scholars from foreign countries. Its research spending is among the top ten universities in the USA.
As a former undergraduate, medical student, and faculty member of the UW, I gained a deep appreciation for its many contributions to biologic science and medicine. The individuals that were responsible for these advances are detailed below. Many were my teachers and colleagues.
I have divided the individuals responsible for these advances into four categories, The Vitamin Chemists, The Cellular Biologists, The Physician Scientists and The Organization Leaders.
The Vitamin Chemists
Harry Steenbock PhD (1886-1967) Professor and Chair of Agricultural Chemistry
Harry grew up on a farm near New Holstein, Wisconsin. When he was 17 his father had an offer to sell the farm so he asked Harry if he wanted to eventually take over the farm. The answer was.an emphatic NO! So the family sold the farm and moved to Madison so Harry could enter the University. He graduated from the School of Agriculture in 1908 and then worked for Professor Edwin Hart of the Agriculture School on the optimal feeds for farm animals, receiving a PhD in 1916.
He continued his studies on animal nutrition by studying animal models of vitamin deficiencies. He read that experimental dietary rickets, a deforming bone disease, could be reversed by ultraviolet radiation of the animals, the sun’s rays allowed their skin to make Vitamin D. Dr. Steenbock then made his break-through observation that the same effect could be achieved by irradiating their feed; this converted fat lipids in the food to vitamin D. He then showed that irradiated cow milk could make Vitamin D and this would provide a ready source in the diets of both children and adults. .
Using his own funds Dr. Steenbock patented this procedure in 1927. The Quaker Oats Company offered him the equivalent of three million dollars for the patent; instead he turned it over to the University of Wisconsin. Several prominent UW alumni, headed by Thomas Brittingham, started a foundation to manage the royalties from that patent for the next 27 years.
The foundation was named the Wisconsin Alumni Research Foundation (WARF) and its revenue became a major funding source for UW research, particularly during the depression years, (1933-1939), but continuing to the present. WARF now holds multiple patents and provides the university 100 million dollars of research funds every year.
The Agriculture/Life Science library is named after Dr. Steenbock. His former student and successor Hector DeLuca PhD holds the Steenbock Endowed Chair and now is the foremost authority on Vitamin D and its derivatives as used in the therapy of multiple disorders.
Karl Paul Link PhD (1901-1978) Professor of Agricultural Chemistry
Karl was born in La Pointe, Indiana, one of eight children. His father was a Lutheran minister who died when Karl was twelve. With family support and his mother’s admiration for Senator Robert LaFollette, Karl entered the University of Wisconsin, receiving a BS in 1932, a MS in 1924 and a PhD in 1925 in carbohydrate chemistry.
After postdoctoral work in Europe, interrupted by a hospitalization in Switzerland. for tuberculosis, he joined the UW faculty in 1927 He soon distinguished himself by his non-traditional clothing (large bow ties, flannel shirts, work shoes and a cape) a booming voice, long hair and radical views, all of which kept his students amused and attentive.
His international fame began with the legendary story on a cold Saturday in February 1933. Farmer Ed Carson had driven his truck 200 miles in a snowstorm to the UW Agriculture building to confront Professor Albert Carson (no relation)---the only one in the building that Saturday. He also brought along a dead heifer (cow), a bucket of its uncoagulated blood and 100 pounds of fermented sweet clover hay. He told the professor “This hay is making my cows bleed to death.” The cows had the previously described Sweet clover disease.
Professor Carson turned this problem to Dr. Link. Over the next 6 years, Dr. Link and his colleagues isolated the factor in the clover that caused the bleeding a natural substance called dicoumarol, an inhibitor of Vitamin K, which is necessary for blood coagulation. Their laboratory synthesized enough dicoumarol to be tested, first in animals, and then in humans. Its first use was as a rat poison, causing the critters to bleed to death.
The Link laboratory synthesized and tested many related compounds and settled on one, Coumadin, which was a potent anticoagulant which was orally absorbed, fast acting and quickly reversible by vitamin K. It was licensed for human use in 1954 and patented by the Wisconsin Alumni Research Foundation as WARFARIN. It soon became the most widely used blood thinner in the world. The drug received widespread acceptance after it was used on President Dwight Eisenhower after his heart attack. Its proceeds allowed the Foundation to grow just as the patents on irradiation of milk were expiring.
The best tribute to Karl Paul Link is the WARF building on the UW campus, in part financed by the patent for WARFARIN, the most widely used blood thinner in the world.
Conrad Elvehjem PhD (1901-1962) Professor and Chair of Agricultural Biochemistry, Dean of the Graduate School, UW President
Conrad was born in McFarland, Wisconsin to Norwegian emigrants. He received a BS in 1924 and a PhD in 1927 He then joined the Agricultural Biochemistry faculty and served as its chair, as Dean of the Graduate School and then served as the 13th UW President from 1958 to 1962.
Dr. Elvehjem worked on the cause of pellagra, a nutritional disease causing dementia, dermatitis and diarrhea with early death i.e. the four D’s. It was common among people living on a corn diet deficient in fruits and vegetables; this included many persons in prisons and asylums.
Earlier work by Dr. Joseph Goldberger had cured a similar disorder in dogs called black tongue disease by a liver extract. Elvehjem then showed that a liver extract could cure dietary pellagra in chicks and thus cold be used to identify the exact component of the liver extract that prevented pellagra in chickens. Elvehjem isolated and characterized this as niacin, Vitamin B3. Niacin was then used worldwide to treat and prevent pellagra, including curing some demented and institutionalized patients.
Dr. Elvehjem became a major advocate for the need for vitamins in the diet. He authored 780 papers and trained multiple graduate students. His first student was Frederick Stare PhD. who founded and chaired the Department of Nutrition of the Harvard School of Public Health.
The Cellular Biologists
Har Gobind Khorana PhD (1922-2011) Professor of Biochemistry, Director of the Enzyme Institute
Har was born In Raipur, a little village in India’s Punjab, and now part of Pakistan. The family was the only literate one in a village of 100. He received early schooling under a tree from a village teacher. Har received a BS and MS from Punjab University and then moved to the UK in 1945, receiving a PhD in 1948 from the University of Liverpool. After positions in Zurich, Cambridge, and British Columbia he came to UW in 1952 to head the WARF-supported Enzyme Institute.
Dr. Khorana’s work focused on the DNA genetic code, determining the sequence of the four DNA nucleotides which direct the synthesis of the 21 amino acids, the building blocks of all proteins. He then synthesized the first artificial DNA gene. For this work he was awarded the 1968 Nobel Prize with Robert Holley of Cornell and Marshall Nirenberg of the US National Institutes of Health.
In 1970 Dr. Khorana moved to the Massachusetts Institute of Technology, focusing on rhodopsin, a visual protein when mutated causes retinitis pigmentosa and night blindness. He retired in 2007 and died in 2012.
Howard M Temin PhD (1934-1994) Professor of Oncology
Howard was born and raised in Philadelphia. He received a BS from Swarthmore College in 1955 and a PhD from the California Institute of Technology in 1959. He then joined the UW McCardle Cancer Research Laboratory where he remained until his death from lung cancer in 1994.
Dr. Temin’s main contribution was the co-discovery of the reverse transcriptase enzyme of the Rous Sarcoma Virus (RSV) of chickens. In 1911 Dr. Pierre Rous showed that a cell-free extract of this tumor would cause the same sarcoma in another chicken. The cell-free agent was an RNA virus, which, unlike DNA viruses, mutates readily when it makes a DNA copy for its replication. Dr. Temin identified the enzyme reverse transcriptase that catalyzes this reaction. An inhibitor of this enzyme, azovudine (AZT) was the first effective drug against the Human Immunodeficiency Virus (HIV) that causes the Acquired Immune Deficiency Syndrome (AIDS). AZT given to HIV positive-pregnant women and their newborns greatly reduces the rate of HIV transmission from mothers to their infants.
Dr. Temin received the Nobel Prize in Medicine 1n 1975 with David Baltimore of the Massachusetts Institute of Technology and Renato Dulbecco of the London Cancer Research Laboratory. Dr. Temin became a spokesman against smoking as a cause of cancer including it in his Nobel acceptance speech in front of the Queen of Sweden who was a smoker. He died of lung cancer in 1994 at age 59.
Joshua Lederberg PhD (1925-2008) Professor and Chair Department of Genetics
Joshua was born in Montclair New Jersey and grew up in New York City. He entered Columbia as an undergraduate and then its medical school. Before completing his medical degree, he transferred to Yale for a PhD in genetics with Edward Tatum PhD. Instead of returning to medical school he joined the Department of Genetics at Wisconsin, eventually becoming its Chair.
Dr. Lederberg’s Nobel Prize studies showed that a bacterial virus (a phage) that made an E. coli bacterium resistant to a specific antibiotic could transfer its resistance to another strain of E coli if grown together in the same culture. These studies were labelled “bacterial sex” and “jumping genes.” This transduction, as it is called, can also occur from one strain of bacteria to a completely different type of bacteria, thus explaining the emergence of multi drug resistant bacteria in severely ill patients.
Dr. Lederberg received the 1958 Nobel Prize along with his Yale mentor Edward Tatum and George Beadle of the California Institute of Technology. Shortly thereafter he moved to Stanford as Chair of Genetics. After the moon landing he became interested in the possibility of extra-terrestrial microorganisms brought to earth by the astronauts and the development of technology to harvest them. He was named President of Rockefeller University in 1978 and died in 2008.
James Thomson DVM, PhD (1938- ) Professor of Anatomy, Director Cellular and Regenerative Medicine Institute
James was born in Oak Park Illinois. He received a BS from the University of Illinois and a DVM and a PhD from the University of Pennsylvania. After two years at the Oregon Primate Research Center he came to UW in 1991 to complete a residency in Veterinary Pathology. He joined the UW Anatomy Department faculty in 1994, and was named the director of the Regenerative Medicine Laboratory of the Morgridge Research Institute in 2006.
In 2008 Dr. Thomson was the first to culture pluripotent stem cells from human embryonic cells. These cells are immortal, and can differentiate into different types of cells such as blood cells, nerve cells and organ cells. Shortly thereafter President Bush vetoed research funding on human embryonic stem cells. In 2013 the Thomson laboratory developed human stem cells from the skin using a cocktail of growth factors,
Dr. Thomson, in conjunction with WARF, established a non-profit WiCel Research Institute that distributes stem cells to researchers at Wisconisinnand other laboratories around the world.
The Physician Scientists
Frederic Mohs MD. (1910-2002) Professor of Surgery
Fred was born in Darlington in southwestern Wisconsin. His widowed mother moved to Madison in 1915 so Fred could attend the UW where he received a BS in1930 and an MD in 1932.
As an undergraduate he assisted Dr. Michael Guyer of the Zoology Department on skin cancers in rats provoked by chemical exposures. After surgical training at the University of Oregon he returned to UW to continue his work on skin cancer. His breakthrough observation was that rat skin cancers caused by chemical exposures, could be treated by local application of a caustic paste of zinc chloride. This not only killed the cancer cells but fixed the tumor for its easy removal allowing microscopic analysis of the tumor edge to see if all the tumor had been removed. If not, the cancerous areas were retreated, layer by layer, until all the cancer was removed. Further, the cavity left by the tumor was resistant to infection and healed quickly.
One disadvantage was that every reapplication took a day since the slides had to be stained and examined that evening, prolonging the treatment for several days. Dr. Mohs later modified the technique by using frozen sections of the tumor that can be prepared shortly after each application thus allowing the procedure to be completed in a single day.
Dr. Mohs treated his first patient in 1936, calling it Chemosurgery. Despite its name, the UW surgical department did not support his work. However Dean Middleton recognized its importance and gave him a suite in the dermatology division.
As word spread of its success of tumor removal with minimal scarring, patients came from all over the country for their treatment. Dr. Mohs showed his technique to other doctors and soon training programs in chemosurgery were established. Chemosurgery was renamed Mohs micrographic surgery and centers were added all over the country. Over 1500 doctors have been trained in the technique and nowadays it is a recognized subspecialty with clinics at all major medical centers.
Harry Waisman MD, PhD (1912-1971) Professor of Pediatrics, Director Joseph P Kennedy Memorial Laboratory for Developmental Disabilities.
Harry, born in Milwaukee received four UW degrees, a BS in 1935, an MS in1937 a PhD in 1939 and an MD in 1941. He then was a pediatric resident before joining the Pediatric Faculty in 1943. He started his research on childhood cancers but switched to hereditary inborn errors of metabolism that cause mental retardation, particularly phenylketonuria (PKU). This disease is caused by an enzyme deficiency needed for the metabolism of the amino acid phenylalanine, causing it to build up in the blood and brain resulting in mental retardation. Carriers of the disease are unaffected but if both mother and father pass on their abnormal gene their infant will develop phenylketonuria. The disease can be diagnosed at birth by a heel-stick blood test and treated successfully with a phenylalanine-free diet.
Dr. Waisman was an early researcher on the disease using animal models, methods to detect asymptomatic carriers, newborn diagnosis, and its dietary treatment. PKU was the first disease detected by routine newborn heel stick testing; now every US newborn is tested for PKU and 26 other hereditary diseases.
In 1963 the Kennedy Foundation provided funds to UW for the Joseph P Kennedy Memorial Laboratories for Developmental Disabilities directed by Dr. Waisman. Two years later the National Institutes of Child Health and Human Development awarded funds for a multi-disciplinary building for research on intellectual and developmental disabilities, The Waisman Center on the medical campus was completed two years after Dr. Waisman’s death in 1973.
Folkert Belzer MD (1930-1996) Professor and Chair of the Department of Surgery
Folkert was born in Indonesia and moved to the USA as a teenager. He graduated from Maine’s Colby College in 1953 of Waterville, Maine and then received an MD from Boston University in 1958. Following a surgical residency and fellowship at the University of Oregon. He joined the transplant team at the University of California, San Francisco, He was named Professor and Chair of UW Surgery, 1974 to 1995. He and his colleagues developed the third largest transplant center in the USA before his death in 1996. In the 1960s Dr. Belzer developed a perfusion machine that kept donated kidneys viable for several hours permitting the recipient to get to the hospital for the transplant. Using this machine a kidney donated in San Francisco was flown to Holland and successfully transplanted 37 hours later.
At Wisconsin, he and colleague Dr. James Southard developed a solution that kept a refrigerated donor organ (a kidney, heart, pancreas, or liver) viable for up to 30 hours. It contained 15 ingredients to nourish the organ, prevent edema, maintain sterility, and prevent enzyme release. Called the Wisconsin Solution it was patented by WARF and distributed as Viaspan by a WARF-supported company named Bridge to Life. Later work included a similar solution for organ preservation at room temperature.
These solutions had an enormous role in organ transplantation since the donor organ could be flown to the patient in another city thus facilitating survival rates of 70 to 90 percent.
The Organization Leaders
Harold P Rusch MD (1908-1988) Professor of Oncology, Director, McCardle Laboratory for Cancer Research
Harold was born in Merrill Wisconsin. He became interested in medicine as a result of his own appendectomy as a youngster. He attended the UW, receiving a BA in 1931 and an MD in 1935. He then joined the Medical School faculty teaching physiology and beginning his cancer research on the effect of obesity and ultraviolet light as precursors to cancer. In 1938 the McCardle family donated funds to establish a Cancer Research Program and Dr. Rusch at the age of 30 was named its director.
In 1949 the McCardle Laboratory for Cancer Research was opened in a building attached to the Wisconsin General Hospital, the first such institute dedicated to cancer research. In 1964 the McCardle laboratory moved to its own building on the medical campus, and moved again in 2013 to the newly constructed Wisconsin Institutes for Medical Research on University Avenue.
Dr. Rusch gathered an impressive group of scientists for his laboratory including Van Potter (triple chemotherapy, bioethics), Elizabeth and James Miller (chemical carcinogenesis), Rosewell Boutwell (nutrition and cancer), Gerald Mueller (hormonal control of cancer), Charles Heidelberger (development of the drug 5-fluoruracil), (V. Craig Jordan (development of the drug tamoxifen), and Howard Temin, (Nobel Prize for discovery of the reverse transcriptase enzyme in RNA cancers).
In 1972 Dr. Rusch became the Director of the UW Comprehensive Cancer. Before his retirement in 1970 he recruited Dr. Paul Carbone to continue his work. Dr. Rusch died of cancer in 1988, the disease that he spent a lifetime searching for its causes and cures.
William S. Middleton MD (1890-1975) Professor of Medicine, Dean of the University of Wisconsin Medical School
William was born in Norristown Pennsylvania to working class parents. Based on his outstanding high school record he was directly admitted to the medical school of the University of Pennsylvania in 1907, graduating with an MD in 1911. After a one year internship at Philadelphia General Hospital he joined the Student Health Service of the University of Wisconsin and an instructor in Medicine in its two year medical school.
In 1924 Wisconsin General Hospital opened and the medical school became a 4 year school with Charles Bardeen MD. Professor of Anatomy as the first Dean. In 1935 Dr. Middleton was named the dean, a position he held until 1955, interrupted by two leaves of absence to serve in the military.
Dr. Middleton was a master teacher and clinician beloved by his students, both delighted and feared at his bedside rounds. He spent mornings in the hospital and afternoons in the Dean’s office.
From 1917 to 1919 Dr. Middleton’s served as a Lieutenant in the US Army Medical Corps in France during World War I. In 1942 again Dr. Middleton, now Colonel Middleton, volunteered for war duty. He was named Chief Consultant in Medicine of the European Theater of Operations stationed in Britain. From there he planned the medical care of casualties of the D-day landing of June 6, 1944.
Shortly after the invasion Colonel Middleton went to Normandy for several months to supervise the care of 2600 medical and 2000 neuropsychiatric casualties. Upon his return to Britain, he coordinated the hospital care of battle casualties up through 1945. One of his patients was General George Patton who he diagnosed with malaria.
For his military service he was awarded an Honorary Office of the British Empire (military), the Croix de Guerre from France, the Lion of Merit with Oak Leaf Cluster from the USA and an honorary degree from the University of Cambridge.
He returned to Wisconsin in 1945 and remained Dean until 1953. He then was appointed Chief Medical Director of the Veterans Administration in Washington DC, overseeing the 273 VA hospitals that served 106,000 patients per day. The VA research program grew from $6.4 million to $30.5 million during his tenure.
Upon Dr. Middleton’s retirement, President John F. Kennedy thanked him for his lifetime service to the soldiers and the veterans that served our country. The Middleton Medical Library next to the Wisconsin General Hospital was opened in 1967. The Madison Veteran’s hospital was renamed the William Middleton VA Medical Center.
Judith Faulkner MS (1943- ) Founder EPIC Systems, Lecturer Department of Computer Science
Judith was born and raised in Cherry Hills, NJ. She graduated from high school at age 15 and then received a BS in mathematics from Dickenson College in 1969. She received an MS in computer science from the UW in 1978. Upon graduation she borrowed $70,000 from friends and family and with Dr. John Greis started a company, Human Service Computing which became EPIC Systems.
EPIC is a healthcare software provider, now located in Verona, a suburb of Madison. It is now the largest system of computerized medical records, used by many major healthcare systems including Kaiser of California, Mayo Clinic, UCLA, and UW Madison. The system records medical visits, laboratory reports treatments, pharmacy orders, future appointments and billing and insurance, all available to the patient and to the health care team, locally and at other medical facilities. EPIC is also used in an increasing numbers in other countries including the UK, The Netherlands, Australia and Singapore.
The Verona campus has 8 buildings and employs 10,000 people. The company’s large work force is gender, ethnic, religion and attire neutral. EPIC has improved the economy of the Madison, Wisconsin area; for example flights in and out of the Dane County airport have increased dramatically as EPIC employees visit multiple medical centers for training and updates.
Ms. Faulkner recently stepped down as the CEO of the company She has participated in The Giving Pledge, promising to donate a majority of her wealth to a worthwhile philanthropic organization.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-rw-id-00163/ https://ijclinmedcasereports.com/pdf/IJCMCR-RW-00163.pdf
0 notes
Text
Single Pass Four-Throw Pupilloplasty for Diffuse Iris Atrophy in Catractus Herpes Zoster Ophthalmicus (HZO) Case by Majed Alsubaie

Abstract
Patients of Herpes Zoster Ophthalmicus (HZO) develop several ocular complications that need surgical interventions such as cataract, glaucoma and corneal scar. Managing these complications is challenging in which the patient might go into several intera and post-surgical complications. We are reporting a case of Herpes Zoster Ophthalmicus (HZO) having diffuse iris atrophy and the intumescent cataract of the left eye. Both pupiloplasty and cataract surgery were done. Iris atrophy reconstructed by single-pass four-throw technique and phacoemulsification for cataract at the same time. The results were promising, the patient's visual outcome improved, the pupil has a good shape and contour and patient satisfied from the outcome both visually and cosmetically.
Keywords: Cataract; Pupilloplasty; Herpes Zoster Ophthalmicus
Introduction
The risk of developing herpes zoster infection in general during the lifetime is 20%, and the involvement of the ophthalmic division of the trigeminal nerve is up to 20% of these patients leading to a condition called Herpes Zoster Ophthalmicus (HZO), in which all structures of the eyes can be involved leading to various ocular diseases like Scleritis, Keratitis, Cataract, Uveitis, and glaucoma, However chronic inflammation and prolonge steroids use can lead to cataract formation [1].
We are reporting a case of HZO, who underwent surgical intervention for diffuse iris atrophy and intumescent cataract developed in less than 1 year of diagnosis and the post-cataract surgery result in visual improvement.
Case Report
A 35 years old male, presented to our clinic complaining of decreased vision, glare and abnormal-looking left eye due to diffuse iris atrophy over the left eye. He was diagnosed as a case of Herpes Zoster Ophthalmicus (HZO) having the first attack of anterior uveitis and high intraocular pressure along with forehead vesicular rash for which he was treated with an oral antiviral (valacilovir) and tapering topical corticosteroids at our uveitis service.
He was on regular follow up for the past 8 months' time with uveitis well controlled. Eight months later he presented to the uveitis service with further reductions of the vision over the left eye which was counting finger (CF) and glare due to his pre-existing diffuse iris atrophy.
His examination showed an intumescent cataract of the left eye (Figure1, A/B). Full ophthalmic examination of left eye BCVA Counting finger near the face, clear cornea with intact sensation, deep and quiet anterior chamber, diffuse iris atrophy pupil size around 11.5 , open-angle by gonioscopy, intraocular pressure 16 mmHg and no view of fundus B-scan done show flat retina and no abnormality detected. The right eye examination was within normal limits.
At the corneal service, he was scheduled for phacoemulsification with posterior chamber intraocular lens implant with pupiloplasty of the left eye under local anesthesia. The patient was seen first-day post-op and his examination revealed improvement of his vision from counting finger to 20/60 without correction, IOP 18 mmHg, clear cornea, anterior chamber deep with +3 cells, pupil 9.5 mm size with a round contour, Fundus within normal limit, He was happy about his visual outcome and his glare was almost resolved completely (Figure 2). The patient was continued on antibiotics and steroid drops.
Second-week post-op, the vision was improved, VA (SC) 20/30, the Cornea cleared, Intraocular Pressure (IOP) 14mmHg, Anterior chamber deep and quiet and normal fundus.
Discussion
Our reported case had an intumescent cataract with diffuse iris atrophy of the left eye in which the cataract removed and the residual iris reconstructed. The exact pathogenesis of HZO complications is not well understood, it could be due to viral replication in the early disease stages and the inflammation associated with that [2]. In HZO, the complications requiring surgical intervention are the Neuroparalytic ulcer, Glaucoma, Corneal scar and Cataract [3] in which the cataract is the most common one [1].
The common presentation is the posterior subcapsular cataract in which the steroid and chronic inflammation (uveitis) from virus play a role [2] in our case the patient was having an intumescent type of cataract which is not common in HZO and also its surgical management (phacoemulsification) is a bit difficult as compared to posterior sub-capsular cataract.
A retrospective study of 24 operated eyes of HZO patient having a cataract, the corrected distant visual acuity (CDVA) before surgery 20/112 after phacoemulsification + posterior capsular intraocular (PCIOL) the patient had CDVA 20/44 in the first year [1]. The choice of either ECCE or phacoemulsification and quince 6 months patient have better results on favorable long-term follow up (> 20y) the best-corrected visual acuity ( BCVA ) was 20/20 [2]. Another study done 11 eyes operated, the BCVA was 20/40 [1]. Most surgeons delay surgical intervention up to 3 months of quiescence and avoiding the active phase of the disease since the surgical intervention can trigger the disease [4]. Our patient had 6 months quiescence period since the last episode of uveitis.
Patients of HZO have the risk of complications after cataract surgery such as developing a corneal scar, fractional retinal detachment or recurrence of uveitis requiring further intervention [1]. Thus the adequate control of inflammation, intraocular pressure, and ocular surface disease improved the visual prognosis of cataract surgery of HZO patient [4], despite the advance of therapy HZO complication may be reduced but not eliminated [2]. Visual recovery compromised by the preexisting chronic ocular condition [1] thus it has an unpredictable result for cataract surgery.
Another situation we had in our patient which is rudimentary iris contour this may be due to chronic iritis and diffuse iris atrophy [3]. We were concern about cataract surgery results that may be compromised by the absence of iris coverage. Patient’s glare might worsen further causing more severe glare and photophobia due to reactivation of herpetic uveitis thus leading to unacceptable cosmetic appearance.
There are many techniques for pupilloplasty such Siper slipknot and the modified version, these options were on the table but using single-pass four-throw pupilloplasty technique provide a better option for our patient having advantages of minimal iris manipulation single pass, thus fewer iris pigment dispersion saving what we have of iris structure and also minimizing the reactivation of post-surgical induced uveitis [5]. This technique has an only single pass through the anterior chamber wherein 4 throws in helical configuration taken externally through the suture loop withdrawn from the anterior chamber, few steps were captured (Figure 2). Minimal iris manipulation single pass, thus fewer iris pigment dispersion saving what we have of iris structure [5] and also minimizing the reactivation of post-surgical induced uveitis. Although it has no true looking knot system, this technique provides a self-looking and self-retaining mechanism preventing the loop from reopening [6]. Single-pass four throw pupilloplasty provide adequate pupil dilatation after pupilloplasty facilitating retina examination if needed for patients of HZO. This technique achieves good pupil size, and contour [5].
In Conclusion
HZO patient has many ocular complications, with adequate control, the proper selection of cases to intervene and the proper selection of surgical technique can carry good prognosis of the patients.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-cr-id-00164/ https://ijclinmedcasereports.com/pdf/IJCMCR-CR-00164.pdf
0 notes
Text
The New Norm in an Academic Medical Centre in the Post COVID-19 World: Finding Opportunities in Challenges; How to Adapt, Innovate and Thrive by Lateef F*

Abstract
COVID-19 has affected every country and every healthcare system throughout the world. Work flow in our healthcare institutions across Singapore changed quickly to a pandemic model of preparedness which we have trained for and executed previously with other outbreaks of infectious diseases such as Severe Acute Respiratory Syndrome (SARS). Our healthcare organization at Sing Health Duke NUS Academic Medical Centre (AMC), represent a complex system. As such the preparedness plans are also multi-faceted, multi-layered, multi-disciplinary and are made up of multiple algorithmic steps. As we reach a stable state with the numbers of COVID 19 positive cases trending downwards and the community spread almost negligible now, new norms and new practices have become embedded in the population, businesses, systems, organizations, industries and schools. At our AMC, this was also the case. Work has begun on many fronts and the positive ripple effects are already becoming apparent. As we reset ourselves for the new normal, our AMC has identified 5 attributes/ domains to guide our paradigm in the face of a new world. These are known as the 5 Ps: People, Patients, Places (Infrastructure Development), Programmes and (Pandemic) Preparedness. In this commentary, the author shares her views on the changes and the healthcare practices during and post COVID 19. The author is a senior consultant Emergency Physician, who had served as an elected Member of Parliament for 15 years in Singapore. She has retired from politics on 23rd June 2020.
Keywords: COVID-19, Cross-training, Academic Medical Centre, Preparedness; Post COVID-19
Introduction
The COVID 19 pandemic represents an inflection point in our history, affecting our lives and livelihood. It continues to ravage the world as we chart our course and plan our footprints into the future. It is leaving us with many challenges and multiple lessons. Just like with previous outbreaks (eg. SARS, MERS, Ebola), many changes and evolution in healthcare have been sparked off from these experiences. It is all part of the lessons we learn from a crisis and the opportunities we create through the challenges we encounter. Due to COVID 19, certain adoption and adaptation, as well as disruption have been brought forward. These served as the impetus for change, for us to accelerate our plans, drive innovation, capitalize on technology and also transform how we deliver healthcare and other services. These are all encompassing and are integrated across many sectors.
COVID 19 transformed into a pandemic within a relatively short period of time due to high levels of infectivity, including spread by pre-symptomatic and asymptomatic patients. This led to massive numbers of cases in most affected countries. The infection came in waves; whilst some countries saw the numbers infected risevery rapidly in the early stages (eg. China, Europe), other countries only started seeing their first wave much later on ( eg. South America, some states of the United States of America). Both scientists and clinicians struggled to get more information to help in the treatment and ultimate vaccine production, especially in the early days of the pandemic [1-3] Change became a constant, whether it was in workflow, case definition or infectivity, as new findings and observations were evolving and begun to be shared globally. As a result, the COVID 19 pandemic was one that brought about transformative changes, most suited to train the future-ready clinician, medical educators and researchers. It also presented us with a variety of choices for the future, of which our selection will contribute towards the reshaping of healthcare and perhaps, even society.
The Academic Medical Centre in Singapore
Singapore General Hospital (SGH), the oldest and largest training hospital in Singapore forms an Academic Medical Centre with the Duke NUS (National University of Singapore) Graduate Medical School. SGH has 1800 inpatient beds, across 36 different specialties and the Emergency Department serves about 140 000 attendances annually [4]. An Academic Medical Centre (AMC) is a tertiary care hospital that is integrated with a medical school. The hospital is the primary site of education for undergraduates of the medical school as well as post-graduate medical trainees from affiliated medical schools. It conducts medical, academic and research activities utilizing a variety of approved and recognized protocols involving patients in the hospital [5].
In addition to the above definition, JCI (Joint Commission International) accredited academic medical centers must meet some additional criteria: [5]
The hospital is organizationally or administratively integrated with a medical school.
At the time of application for accreditation, the hospital is conducting medical research with approval and oversight by an Institutional Review Board (IRB) or research ethics committee.
Being a large organization, infection control training and our emergency preparedness processes and responses are also multi-layered, multi-faceted and complex. Since the SARS (Severe Acute Respiratory Syndrome) outbreak in 2003, the Emergency Department (ED), as well as other departments at Singapore General Hospital (SGH) had undergone changes in both its infection control infrastructure as well as work flow processes [6,7]. These are critical and essential elements in preparedness for handling crises, mass casualty incidents, infectious diseases outbreaks or pandemics. The specialty of Infectious Diseases too has developed further with more specialists, residents-in-training as well as more organized and structured facilities such as negative pressure and isolation rooms, since 17 years ago. These have become part and parcel of our day to day practice. What is important is that these practices remain dynamic and their details are regularly updated and renewed at strategic intervals, including the need for the incorporation of critical new information as it becomes available. Experiences from our responses to new outbreaks or other, directly relevant developments, were also incorporated.With this model of work, it gave us the head-start when COVID 19 first landed on our shores [7,8].
The first COVID 19 case in Singapore was seen at SGH on 23rd January 2020. The daily count remained relatively low until mid-March when a sudden rise of COVID 19 cases amongst dormitory-dwelling migrant workers took the numbers to record highs. Restrictions were enforced, circuit breaker measures were instituted, gatherings were banned, and businesses and schools were closed. People worked from home and students got used to online learning. Today, the numbers have stabilized, there are negligible community spread and all dormitories have been cleared. As of 7 Sept 2020, there have been 57 044 COVID-19 positive cases reported in Singapore, with 27 deaths. That makes the death rate0.00047%. Many restrictions continue to be practiced: wearing masks everywhere, no gatherings of more than 5 persons and safe distancing measures. Our local scientists continue to work hard at producing the COVID-19 vaccine and predictions of the possible trajectories of the pandemic: whether it will be a prolonged epidemic with multiple waves or a pandemic becoming endemic?
In the meantime, new norms and new practices have become embedded in the population, businesses, systems, organizations, industries and schools. At our AMC, this was also the case. Work has begun on many fronts and the positive ripple effects are already becoming apparent. As we reset ourselves for the new normal, our AMC has identified 5 attributes/ domains to guide our paradigm in the face of a new world. These are known as the 5 Ps: People, Patients, Places (Infrastructure Development), Programmes and (Pandemic) Preparedness [6,9] (Figure 1).
The Paradigm Change and the New Norm
People
COVID 19 had an unprecedented toll on healthcare workers all over the world [2,10,11]. The people who ensure the AMC functions efficiently and effectively, are the staff…..every single one of the multi-disciplinary staff during COVID 19. It was critical to ensure their development continues. The building of their capacity and inculcating their capabilities, must be relevant and applicable in the current as well as the post-COVID 19 world. Training and continuing education is important and must be customized. It has to be linked to their ability to learn, unlearn and relearn. The ability to learn is a standard, but unlearning can be challenging. Some staff may hang on to old practices and are unable to let go of these. This is where mindset change and adaptation comes in. How do we get their buy-in? How do we prove the new method is better than the old? How do we combine the traditional with new technology? One good example would be the cutting down of face to face training. With that, medical officers, residents and nurses training sessions have gone virtual. We invested in electronic (E- learning) and online learning in a big way. Didactic and interactive sessions were delivered via Zoom, or other similar platforms [12,13]. Simulation in the sim-lab was converted to computer-based simulation [12]. We also had to ramp up the development of our Virtual and Augmented Reality (VR and AR) applications faster than expected. We very quickly sourced for funds to hasten the completion of our Innovation Arcade at our simulation centre (The SingHealth Duke NUS Institute of Medical Simulation), in preparation for the VR, AR, mixed reality (MR) and serious games applications. We applied for the Learning Technology Adoption Grant (LTAG), from SkillsFuture, Singapore and are working on 14 different serious gaming projects with appointed vendor companies [14]. SkillsFuture is a national movement providing Singaporeans with the opportunity to develop their fullest potential throughout life, regardless of their starting point. The skills, passion and contributions of every individual will drive Singapore’s next phase of development towards an advanced economy and inclusive society. These projects cut across various disciplines, whilst some are inter-disciplinary. All these projects have bearing on our patient care, workflow as well as staff training. Our staff are the subject matter experts in these applications and will champion their use for training and education.
To be able to embark on these projects and ride the latest bandwagon of digital transformation, we have to ensure our people are exposed to the latest developments. We created the awareness by telecasting webinars and virtual seminars on relevant themes. Training sessions are made readily available and accessible. These sessions are provided for all the relevant staff. Empowerment courses are also converted to virtual training format and the numbers of participants increased significantly during the COVID-19 pandemic, despite the heavy workload that we were facing. The focus on mastery of skills and knowledge is important. This, we feel, is a step in the right direction to be able to function in the VUCA (vulnerable, uncertain, complex and ambiguous) world, post COVID-19. Staff motivations must never be taken for granted [15]. That is why messaging and reinforcements must be conducted regularly. This can be through the AMC’s intranet, screen–savers on all computers, posters, email blasts and flyers. This customized faculty development concepts will ensure our future ready workforce is up-to-date, competent, resilient and relevant.
Support for all these relevant changes must come from the leadership and management. In fact they are the ones leading in the AMC’s thrust, mission and vision. Leaders who walk the ground, get involved and are aware of the issues will have a deeper understanding of any situation and this means any policies they craft, are likely to be more practical and responsive. Leaders have the ability to inculcate inclusivity. At our AMC, the Chief Executive Officer session with all the staff is termed as “The Family Meeting”. At the session during the COVID 19 pandemic, attendances increased, with many enthusiastic feedback and questions. Sharing the future directions and main thrusts, reassuring the staff, supporting and empowering them through positive attitude, care and concern can have strong impact on employees. The importance of collegiality and camaraderie across any hierarchy must never be under-estimated. This way the staffare encouraged to bring up constructive ideas and feedback, as this is the way to enhance and improve our performance at the AMC [7].
Being able to embark on all these exciting new developments and projects will not be relevant if our staff are not motivated and unwell. This is why during COVID 19, the AMC had invested and rolled out even more activities and resources related to staff psychological wellness, mindfulness and “Joy At Work” (JAW) initiatives. Mindfulness training during COVID 19 has helped the staff at the AMC in a variety of ways [3,7]. It helps to increase attention span and this was certainly useful with the longer hours at work in modular teams. It helped build and strengthen relationships between all levels of staff and across disciplines as well. This facilitated work processes such as when the Emergency Department (ED) staff made admissions; there were lower incidence of bed blocks. Discussions were collegial. The Infectious Diseases consultant on call took consultations readily and provided collaboratively discussions and advice with the ED staff on admissions to isolation wards, high dependency beds and intensive care units for infection-related diagnoses. The positive attitude demonstrated more gratitude, care and concern for each other. Peer support was enhanced. Wellness ambassadors were appointed and taglines such as “ Its OK to not be Ok” were publicized. Counselling was made available 24 hours a day to any staff who needed this or wanted to talk on any issues [7]. Mindfulness can also help in promoting the more conscious practice of Medicine. A happy and satisfied staff will deliver compassionate care and this is the gateway to patient satisfaction [16]. We cannot have our staff painstakingly creating processes from the vantage point of the patient and not see joy in their own work, come alive.
During the pandemic, there was an opportunity for institutions to review their various KPIs (key performance indicators) and manpower needs. With the new norms, some parameters may have to be altered. For example, due to the donning and doffing of PPE when managing certain groups of patients, more time will be required. This means the average time spent per patient will increase and thus, productivity will be altered as well. Allocation ratios of doctors and nurses in the different areas will also change. COVID 19 also provided an opportunity for the level of trust between individual employees and the AMC to be stepped up. The demonstration of care and concern for the safety of staff must come across clearly. This defines another important compact of the institution. Showcase of gratitude and appreciation for each other is important. With these happening at all levels, instead of post-traumatic stress manifestations, staff are now in the phase we term, “post traumatic growth and development”, since the COVID-19 pandemic started. This way the AMC continues to heighten our capabilities and capacity of our staff as they continue to thrive. In fact the pandemic brought out the best in them. Without the physically and psychologically healthy workforce, the delivery of excellent healthcare will be difficult [7].
Change is hard, challenging and difficult, but when people come together, we can accomplish the impossible. The future will see healthcare staff embracing more global learning, shared knowledge, best practices and the setting up of more communities of practice. This may lead to more standardization and less unscientific variations of care [17,18].
Patients
During COVID 19, there were changes encountered with the AMC’s patients profile and case mix. This was mostly due to the changes observed during the various phases, as the pandemic spanned out. As we move into a more stabilized state of the COVID-19 pandemic in Singapore, many of the changes that have taken place related to patient care will continue [19]. This includesa higher utilization of telehealth and teleconsultation. This can increase productivity and save time for the healthcare providers as well as the patients. In fact, where appropriate the family members can even join in. Of course, not all cases are suited for teleconsult, thus the more appropriate cases and diagnoses were selected: eg. follow up for chronic diseases and primary care type cases [20]. Video-consults and video calls were also used appropriately.The full potential of telehealthcan be summarized as follows:
For on demand virtual urgent care. This can be for lower acuity emergency visits
Virtual clinic type consultations: for primary care cases, chronic illnesses follow up or for specialist outpatient clinics consultations
Virtual home care service. This can cover “virtual visitations” with communications over the computer or smart mobile devices.
Remote monitoring is also possible when there is cooperation of the parties involved. Digital engagement tools can also be used for education of the public. This is also where telehealth can provide oversight to many aspects of care such as patient controlled analgesia for cancer patients
It will be more challenging to break bad news or manage complex complications virtually. Thus, some aspects of face to face care must still continue.
At SingHealth, an e-learning telehealth course was made available online and for all staff who complete the modules, CME (continuing medical education) points were awarded. Moving on, this has now become the basic fundamental course for Telehealth certification for staff using tele-consultation. This course covered the definition of telehealth and teleconsultation, detailsof the requirements, maintaining confidentiality during tele-consults and even charging mechanisms for primary care physicians utilizing this modality. With the wider use and greater numbers of practitioners subscribing to it, the cost will become more reasonable and thus the service can be offered at lower costs to patients [21].
At the frontline, patient screening evolved and workflow processes were updated. New areas were created to manage infectious patients in negative pressure environment. Senior physicians help reminded the residents and medical officers of the potential blind-spots for other diagnoses, in the midst of their focus in not wanting to miss out diagnosing COVID 19. Besides training and educating staff, patients also went through the ‘journey of change’. They were learning to use their mobile phones for video consults, testing their hands at various mobile applications the AMC had implemented. Some of these applications were derived from our regular hackathons, where new ideas were generated. There werealways staff on hand as well as IT (information technology) ambassadors to assist patients who were not tech-savvy to negotiate these new applications. They were assisted and their queries were sorted out and clarified, to help them leverage technology in this new age. This also aligns with the Singapore’s government initiatives to make the country a ‘smart nation’[22]. In fact during and post COVID 19, the majority of correspondences with patients eg. appointment dates and changes,were via mobile devices. SMSes (Short Message Service) will continue to be used for reminders. Traditional and manual resources were still made available for those who really are not able to cope with new technology.
Places
The post COVID-19 world of healthcare will never be the same as before. There is no going back to what we were used to. The infection control changes, potential risks from new and emerging infectious diseases and some of the technological developments we are all so used to now, will continue on this trajectory. However, the other healthcare trends such as the ageing population, more chronic illnesses and their related complications, higher incidence of cancers and thus immunosuppression, as well as the more complex presentations in our patients will also continue.
The AMC’s facilities and work processes will continue to evolve, as it has since SARS. The negative pressure facilities in the ED continues to be added. With the new ED under construction, forward planning has been done to ensure sufficient space and facilities, eg. separate ports can be converted to negative pressure areas as deemed necessary by demand. These flexibilities will help in handling upsurge in future outbreaks or pandemics management. Whilst planning all these, the patient flow must continue to remain as seamless as possible. The main objectives of the work flow and processes in the ED must ensure that:
The ED must not allow over-crowding. Innovative distancing measures will have to be implemented
The ED must not become a reservoir of nosocomial infections
The ED work flow must ensure safety of the patients as well as the staff working there and
The timing to manage patients, especially acutely ill and critical patients must not be compromised.
The Infectious Diseases wards and facilities too underwent upgrading during COVID 19. The number of isolation wards and roomshave increased up to some 30 % of our total bed capacity. At the peak of the COVID 19 pandemic, a 5 level multi-storey carpark near the AMC was closed to the public and converted into a consultation and management area for foreign workers from the dormitories. This was termed as our FSA (Fever Screening Area). The ample space, across 5 levels enabled us to use the areas for consultation ( cubicles were constructed), waiting areas for swab results and waiting areas for COVID + patients awaiting admission to negative pressure isolation rooms in the main hospital building. Staffwere seconded to work in this area, with full PPE (personal protective equipment). Before new work areas such as these are opened, we organized insitu simulation to study the workflow processesto realize latent threats. At the same time we did a failure mode effect analyses, to establish best practices.
One of the large open carparks on the AMC campus was cleared and 50 container wards were built quickly. These were all negative pressure rooms for high risk patients. This certainly provided additional bed space for the institution. This was one of our achievements during COVID 19; completion of the building within 30 days. Besides these initiatives, we also have the negative pressure isolation tent available in case it needed to be deployed into any particular area of work, quickly [23] (Figure 2).
Figure 2: The Negative Pressure Isolation Tent which can be deployed where needed within minutes.
Figure 3: SG SAFE Shield booth for healthcare workers to stand in when performing naso- and oro-pharyngeal swabs for COVID-19.
At the ED naso- and oro-pharyngeal swabs were not done inside the department but outside, in a booth as seen in Fig. 3.This represented a new innovation by the Department of Anesthesiology in the AMC [24] (Figure 3). Patients coming into the ED and hospital clinics have to be segregated and spaced accordingly. Everyone was masked up. This was compulsory. The patients were divided into ‘clean’ cases (no fever, URTI, LRTI symptoms , high risk contact with local clusters and low epidemiological risks, etc) and ARI ( acute respiratory illness) cases, and managed in different areas. This means the patients, radiology services and staff in these different areas did not mix and interact. To be able to do this, the triage upfront has to be spot-on and stringent.
Moving on, there will be a new paradigm for infrastructure whereby the distribution of healthcare settings and healthcare providers will evolve. This needs forward planning and must be unified and coordinated. As we see the emergence of new growth opportunities and diversification, there will be faster construction, customized designs with greater agility and potential for repurposing of facilities, equipment and furniture. The future will also see creation of multi-faceted and multi-functional resources, with new hubs of excellence. Capacity for intensive care will have to be expanded. One very progressive option to consider would be virtual ICUs (Intensive Care Units), with the monitoring done from the homes of patients. In Singapore, post COVID-19, we have opened a large scale Urgent Care Centre to provide intermediary care, between that provided by primary care and the care at EDs [25]. Home based care will also see an expansion post COVID 19. This would be linked to higher utilization of phone-based diagnostics and virtual patients engagements. Auxiliary services too may now see more decentralization to enhance accessibility and less crowding at one location. In the AMC, the infrastructure that supports the work of process design and improvement will help ensure the staff continue to be empowered and motivated in an environment where they feel safe at work.
Syndromic surveillance capabilities continue to be enhanced with our computerized and electronic systems. Technology-driven bio-detection will be used more frequently. Notification of infectious diseases and other reportable diseases too are done online and can be tracked readily. Whilst adopting the Internet of Things (IoT), cybersecurity is always at the top of our minds. The AMC has gone through internet separation since 2018 and all the staff have been briefed on this. Everyone was required to take a cybersecurity vigilance course with online assessments. Departments had to procure separate internet enabled computers and only special encrypted, registered external drives were allowed, with close monitoring.
In 2007, JCI came up with the Guiding Principles for the Development of the Hospital of the Future [26]. In this paper, the pointers put forth are relevant to this era of practice. The recommendation for standardized flexibility, which will reduce complexity in the event of increased surge capacity is extremely applicable here, as we have seen during the pandemic. The standardization of patient rooms and room designs had been suggested for optimizing human- system interaction. The use of “loose-fit design” is to design with larger spaces in order to arrange for future adjustments. This is the same with convertible flexibility, whereby a space can be converted to another use when it is needed. In order to offer flexibility in design, utility and communications infrastructure, the master planning strategies must incorporate these concepts from the beginning, so these facilities will be robust enough to accommodate expansion and upgrades. This must align with what is called the ‘plug and play’ infrastructure whereby the horizontal and vertical circulation infrastructure remains in service despite certain departments or wings undergoing upgrades, renovations or are being removed [26].
The interaction and integration between People (staff) and the Physical (infrastructure and environment) is critical. This is something that has to be mainstreamed from the planning stages, but when necessary, customization and improvisation may need to be done.
Preparedness
The importance of preparedness for the 21st century cannot be over-emphasized. Investment into infection control measures, and quality care will drive this [27]. During this pandemic, healthcare systems and countries with lack of readiness and under-par responses, have had to pay a high price. Moreover the preparedness is not just for infectious diseases outbreaks but also for large scale trauma, natural and man-made disasters and even cyber-threats. PPE will become a norm, especially with the frontline disciplines. Screening at the frontline too will continue to be critical. Wearing the appropriate masks will become the minimum standard, post COVID-19. Besides these practices at work, healthcare workers must comply with the distancing guidelines when they are out in the community as well. They set the example for others. By now, every employee at the AMC is familiar with compulsory twice a day temperature log in, use of the contact tracing application and safe distancing measures.
We cannot let down our guardeven as COVID 19 cases start to stabilize downwards. In fact it is necessary to remain vigilant, with the potential for subsequent waves as well as new and evolving infectious diseases today [19].
The healthcare communities in Singapore will continue to work in partnership as this is crucial in sharing best practices, surveillance observations and closing the gaps with local epidemiology and public health. It is important to remain nimble and agile in the current and future climate. Further collaborative studies, data sharing, including the use of big data, will shed more light and set the directions for the future.
The staff of the AMC will drive our preparedness through their teamwork (multidisciplinary collaboration), supportive leadership who are role models, deep understanding of process flow, condusive environmental changes and the relevant, up to date tools. These proper teaming can influence the end metric and goals.
Programmes
Besides the introduction of relevant, new programs, many of the ones started during the COVID 19 pandemic will continue post COVID-19 as well. There will be ‘blending and braiding’ of existing programs with new ones to improve safety and care delivery.(28)These would include telemedicine and telehealth courses, virtual teaching platforms, the use of VR, AR and MR (mixed reality) to supplement teaching and training programs [20,21]. E- learning and online platforms will continue to be enhanced further. Even in organizing local and international conferences, virtual platforms will be added, besides the usual face to face sessions. For many of the conferences which are organized by the AMC departments, hybrid models will be offered, where some components will be offered face to face whilst others more suitable ones will be delivered virtually. Keeping in touch with the community of practice, both locally as well as globally is also important. Currently, virtual connections and teleconferencing keep us connected to share information and best practices across the globe.
Programs such as bulk purchasing training and courses will have value across healthcare clusters. It will help procurement of shared inventories and preparation for stock-piling of certain products and equipment ( eg. masks, PPE). This can be more cost efficient for a small country like Singapore. Simulation will become very helpful in planning the management of more uncertainties, balancing needs against resources. Simulation-based training will continue in smaller groups and is useful in testing workflow, latent threats and can also be applied as insitu simulation. Coupling insitu simulation with failure mode effect analysis can also have value [28].
During the pandemic, staff of the AMC from inpatient departments were seconded to the frontline and busier departments to assist with the work. The departments would include the ED, ICU, ID wards, isolation wards and screening areas. These staff may not be very familiar with the workflow and were given a quick briefing and introduction. Cross-training would be a very useful initiative that can help prepare staff for such secondments. Cross-training can be a strategy to help the staff acquire skills and capabilities of working in areas other than their own discipline. This way they can diversify their skill sets, be more versatile and help to serve where they are needed in crises. Cross-training can ‘energize and strengthen’ these staff, improve teamwork and inter-professionalism, as they learn and understand more of what their colleagues do in the various departments. The level of respect across disciplines can also be enhanced. [29,30].
The AMC has always been very supportive of staff’s innovation and research projects. During the pandemic, one of the grant calls was termed “COVID 19 Innovation Grant Call”. The objectives clearly specify the focus on innovative ideas in the‘new norm’:
To increase operational efficiency and productivity for work processes affected by COVID 19
To improve quality of care and patient safety amidst the ‘new norm’
To ensure the safety of healthcare professionals during the resumption of healthcare services for non-COVID 19 patients and
To encompass longer term innovations to support strategic goals and operations in the ‘new norm’
The AMC organizers will also assist to match interested parties with internal or external partners as appropriate, e.g. Technological experts, engineers. This really demonstrates the emphasis and inclusivity of all staff in contributing their ideas towards making patient care and work processes as well as system flow better.
Another springboard for strategic change innovation and implementation is scenario planning, which can generate new initiatives. The staff will put forth their ideas and suggestions, colored by their life experiences, including those derived during the COVID-19 pandemic. Many of these will commence with brainstorming, which starts with critical questions, that can help generate insights into the shared future and what we collectively want, post COVID-19. (Table 1) To be able to continue with these newer modalities, some unlearning and relearning will be required. Training will help bridge the gaps. Acquisition of new knowledge and skills will continue to be robust. To face the disruption and digital transformation, we must all be prepared, both psychologically and physically.
Conclusion
The AMC is committed to leading every day, continually learning and adjusting creatively to change. The energy that drives it is the human desire of all the staff. The life and work at the AMC will have undulations and waves. That is the norm. However, there may be certain critical points whereby the journey can reach a breakpoint. This is where the behavior of the system must change radically. This is the change we will see post-COVID19. This is the change we have been building up to and preparing for. How we functioned during COVID 19 and the decisions we made, will spark off these high-value added changes. How we handled the ‘chaos’ at the start of the pandemic, strived to find the patterns of alignment, will help us reimagine and reinvent the future norms. Through our multi-dimensional lenses, we must look forward, but not forget to look back to the time of the pandemic, as well. The business as usual, post COVID 19, will be the new norm.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-rw-id-00160/ https://ijclinmedcasereports.com/pdf/IJCMCR-RW-00160.pdf
#COVID-19#Cross-training#Academic Medical Centre#Preparedness#Post COVID-19#Lateef F*#IJCMCR#clinical studies
0 notes
Text
Central Nervous System Coccidioidomycosis: A Case Report by Elvira Castro-Martínez
Abstract
We describe a case of central nervous system (CNS) coccidioidomycosis. This is the most dangerous form of extrapulmonary disease caused by the fungi Coccidioides spp. Clinical manifestations resemble other chronic fungal infections. Medical treatment is based on antifungal therapy for the most common complication, (hydrocephalus), where a shunt is usually required for decompression. Unfortunately, dissemination to the CNS is usually critical, so patients with untreated CNS coccidioidomycosis tend to have a high mortality a few years after initial diagnosis.
Keywords: Coccidioidomycosis; Valley Fever; Coccidioides; Central Nervous System Coccidioidomycosis; Coccidioidal Meningitis
Introduction
Coccidioidomycosis is an infection caused by soil fungi. This disease is common in some areas of United States and Latin America [1,2]. Although uncommon, infections of the central nervous system (CNS) are among the most pernicious [2]. Meningitis is usually associated with this pathology, causing headache and other symptoms [2,3,4]. Neuroimaging studies usually show meningitis and/ or hydrocephalus [3]. In treatment, oral triazole antifungal drugs have a great impact on the management of this disease [4]. Unfortunately, the most destructive forms of this pathology are chronic, resolution is often incomplete and relapses are common [5].
Case Presentation
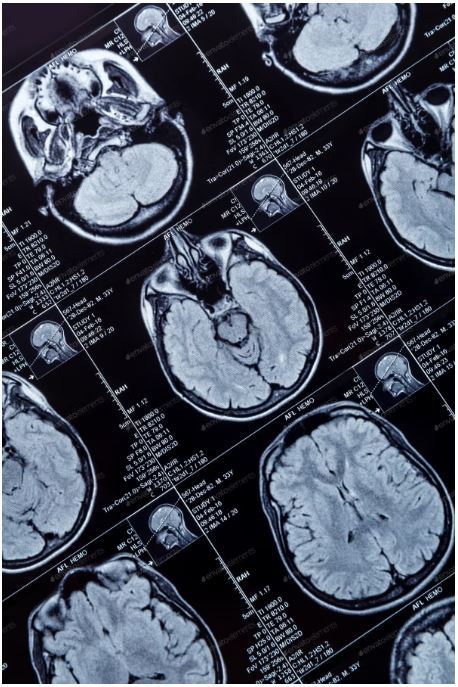
A 41-year-old man, a resident of Mexico City with a recent history of traveling to the north of the country with type 2 Diabetes Mellitus and Systemic Arterial Hypertension. He attended the hospital for a 3-month history characterized by persistent headache, general attack, daily fever of 38.5° C, confusional state, and tonic-clonic generalized seizures. The physical examination upon admission revealed a sleepy and disoriented patient, in which papilledema, hyperreflexia and meningeal signs stood out.Given the suspicion of chronic meningoencephalitis, a brain computed tomography (CT) was performed, which showed hydrocephalus (Figure 1).
Discussion
More than half of coccidioides exposures lead to asymptomatic infection [3], while in 40% of patients with symptomatic disease there are various manifestations that can be pulmonary Since the patient presented a rapid and sudden deterioration in consciousness and general neurological status during the evaluation in the emergency department, he underwent immediate surgical intervention for placement of a shunt system, limiting at that time the performance of other studies.The analysis of the cerebrospinal fluid obtained showed lymphocytic pleocytosis with 40 cells, elevated proteins and hypoglycorrhachia; the rapid test for HIV was negative.Despite emergency management, the patient continued with neurological deterioration and progressed to death within a few hours. In the pathological study, a basal subarachnoid exudate was observed (figure 2) and spherules and Coccidioides endospores were shown (figure 3).
or extrapulmonary: The latter are usually progressive and can involve the skin, bones and / or joints, the CNS and other organs and systems, with meningeal infection being one of the most dangerous forms that occurs in approximately 0.15% - 0.75% of extrapulmonarycoccidioidomycosis cases [4,5]. This occurs as a result of lymphohaematogenous spread from the lungs to the meninges [3]. The epidemiological history of stay in endemic areas and the presence of this symptom together with other compatible clinical characteristics, should indicate the diagnosis, since the prognosis is almost always fatal if not treated promptly [2]. Patients generally present with headache, intracranial hypertension, fever, nuchal rigidity, seizures, and altered mental status [2,4,5]. As in the case we reported, one of the most common findings on cranial computed tomography in CNS coccidiodomycosis is ventricular enlargement [6] and there may be evidence of basilar meningitis, hydrocephalus or cerebral infarcts [3]. The demonstration of a spherule in tissue or a positive culture is a diagnosis [3]. On the other hand, drug therapy for coccidiodomycosis continues to evolve. Antifungals such as fluconazole and itraconazole, in daily doses of 400 mg, have been effective against various forms of coccidiodomycosis including the meningeal one [4,5], while amphotericin B is reserved for severe cases [4]. In addition, hydrocephalus is relatively common with CNS coccidiodomycosis; up to 40% of patients develop this, and the author recommend aggresive management, including daily lumbar punctures and some cases must be managed with ventricular shunting [3, 7]. However, despite aggressive treatment, some patients may die early in the course of the disease. This patient presented to late medical attention with intracranial hypertension due to hydrocephalus secondary to CNS coccidiodomicosys, which was demonstrated in a post-mortem study; which, despite the establishment of emergency treatment, had a fatal outcome, so early diagnosis and treatment are essential to achieve a longer survival and avoid a devastating presentation of the disease.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-cr-id-00161/ https://ijclinmedcasereports.com/pdf/IJCMCR-CR-00161.pdf
#Coccidioidomycosis#Valley Fever#Coccidioides#Central Nervous System Coccidioidomycosis; Coccidioidal Meningitis#Elvira Castro-Martínez#IJCMCR#clinical studies
0 notes
Text
How to Optimised Oncological Treatments: Lessons Learned from the First covid-19 wave by López E
Abstract
Despite the local idiosyncrasies and different viral disease epidemiology resulting in country-specific governmental measures, our 70 centers located in Australia (32), United Kingdom (15) and Spain (21) joined forces and shared knowledge and experiences, which supported an appropriate clinical strategy for each country. The supply of Radio Therapy (RT) and/or Chemo Therapy (CT), and the safeguard of patients and staff in regard to their infectious status have been our priorities. In order to classify the changes in practice made during this pandemic we divide them into four major pillars that have impacted our culture and processes: oncology treatment, infection control, Information Technology (IT) infrastructure and staff connectedness. Facing a health crisis, the doctor leadership should be consolidated and for this reason, a high engagement of our doctors across the network is an essential key point. The oncology sanitary system should be continuously reinforced and should also be flexible plus solid.
Keywords: COVID-19; Chemotherapy; Leadership; Oncology; Radiotherapy; Staff
Introduction
In the first literature report of COVID-19 infection in oncologic patients the authors suggested three major strategies that would represent the backbone in delivery of oncologic treatments [1]. First, postponing adjuvant treatment or elective surgery. Second, personal protection for patient with cancer, cancer survivors and staff. Third, intensive surveillance or treatment in COVID positive patients with cancer.
During this pandemic, Spain was the first of the countries belonging to the Genesis Care (GC) international network affected by this outbreak. The first case in Spain for SARS-CoV-2 was diagnosed on 31 January 2020. By 13 March, cases had been confirmed in all 50 provinces of the country. From 17 March to 14 April, the death rate in Spain was 68% higher than usual and 21,882 excess deaths were recorded. The peak of excess deaths occurred during the week of 27 March to 3 April and was five times larger than the flu season of 2019.
Thus, Spain faced the main challenge to integrate strategies to minimize the deleterious effect of delayed diagnosis and treatment in cancer patients considering new ways of treating them, avoiding to postpone the start of treatments.
Despite the local idiosyncrasies and different viral disease epidemiology resulting in country-specific governmental measures, the three national chief medical officers of our 70 centers located in Australia (32), United Kingdom (15) and Spain (21) joined forces and shared knowledge and experiences, which supported an appropriate clinical strategy for each country. The supply of radiotherapy (RT) and/or chemotherapy (CT), and the safeguard of patients and staff in regard to their infectious status have been our priorities [2,3].
In order to classify the changes in practice made during this pandemic we divide them into four major pillars that have impacted our culture and processes: oncology treatment, infection control, Information Technology (IT) infrastructure and staff connectedness. The great enablers that have facilitated to treat our patients during the COVID-19 pandemics through the four pillars are shown in Table 1.
Our first pillar is oncology treatment looking for efficacy measures, we implemented two strategies: 1) To apply a tumor categorization protocol (Table 2) to determine the priority for RT delivery. Based on different factors such as tumor type and staging, intention-to-treat,
RT= Radiotherapy. SVCS= Superior Vena Cava Syndrome. SCLC= Small Cell Lung Cancer. SBRT= Stereotactic Body Radiotherapy. SPOT= non-melanoma skin cancer.9
General patient performance status and potential radiotherapy schedule approach, we classified the patients into 5 categories: rapid access/emergency radiotherapy (<14 hours or in the same day), A (<5days), B (>5 and <10 days), C (<4-6 weeks) and D (>6 weeks). This has allowed us, in an unprecedented situation, to balance the risk and benefit between treatments versus prevention of virus infection. 2) To increase the rate of hypo fractionated radiotherapy, achieving the same effectiveness with fewer sessions, in order to increase capacity in radiotherapy departments and reduce patient footfall in our centers. For instance, following the results of the Fast Forward trial, breast RT extreme hypo fractionation (26Gy/5#) is now an option for eligible patients (in two weeks we treated more than 90 patients). Similarly, in prostate cancer, moderate and ultra-hypo fractionation protocols such as 20# daily, 5# SABR and weekly 6# (total 36Gy) have been accepted as evidence-based protocols. Finally, for lung cancer patients who are also vulnerable to respiratory illness, a SABR regimen can be considered to standard fractionation. Staff and doctors have worked together to enable the implementation of the above protocols.
Regarding infection control, symptoms screening in patients and personnel before entering an oncology center presented an opportunity to identify possible cases with COVID-19 [4]. Discipline around general precautions by all staff including doctors and reinforcing the cleaning was used in order to keep a clean circuit. Besides, security lines, fixed screens for administrative staff and social distancing in waiting areas by re-arranging sitting areas to keep the 2m rule were performed and may remain as a global social change. The appropriate combination of personal protection equipment (PPE), selected through a risk assessment, was also used for infection prevention. Other useful measures were: Checking lung cone beam computed tomography of all patients with lung, breast or gastrointestinal superior cancers. This allowed not only to check the PTV we were treating but also to detect any abnormality which might be consistent with COVID-19. All these measures are included in our COVID-19 risk management framework [5] which should continue besides testing patients and staff when they screen positive for symptoms, with isolation measures in case of positive testing. An incidence was raised for any patient delay due to COVID-19 through a Multidisciplinary Team (MDT). COVID-MDT met with patient’s doctor, CMO and center manager to decide on patient treatment in case of positive swab for covid-19 [3]. A decision to treat end of day or delay treatment based on risks and benefits was made at the MDT. From our experience, we encourage the case-by-case assessment by a specialized board in future cases. Furthermore, routine asymptomatic staff and patient testing program should rule out to keep centers COVID-19 clean. In the first rapid testing around a 10.47% of our staff in Spain has been in contact with the disease and has generated IgG immunity.
Our third pillar is the IT infrastructure supporting a global network where some activities continued to ensure efficiency. A high percentage of staff members have worked from home through remote access to their platforms, having access to patient history and treatment planners (tele health). Oncologic follow ups were done by phone to reduce the people flow in the centers. Long survival follow-up (> 5 years) were also continued by phone with rapid access if it was needed. Also, psycho-oncologic attention was delivered by phone/digital media. The educational programs were done as Webinars and virtual congresses (teleconferencing). Electronic multidisciplinary teams (eMDT) were established at a time when clinician collaboration for patient care was more needed than ever [6]. It is run through a remote and safe platform, where clinicians can join in a synchronous or asynchronous way, record decisions and share report with the doctor, referrer, GP and patient if they so wish. To increase the communication through the whole network has been one of our priorities.
On the other hand, research continued for life saving trials and trials in set up. Two studies have been developed: Low doses of lung radiation therapy in cases of COVID-19 pneumonia: prospective, multicentric study in Radiation Oncology Centers (ClinicalTrials.gov Identifier: NCT04394182) and Genesis Care UK SARS-CoV-2 Antibody testing Program (both ongoing).
Our fourth pillar is staff connectedness. Regional managers and function managers worked very close to help physician unit coordinators with daily COVID-19 virtual huddles to discuss operational and quality issues and make decisions about center backup e.g.: minimizing the number of staff on site treating patients, having a schedule of backup in case staff fall ill, fewer face to face meetings and more virtual meetings, with staff spending more time home with their families and having time for home schooling Awareness across the network (local, national and international) has increased and this has fed into wellbeing. These plus the exercise and wellbeing program together with a strong medical leadership as part of the Integrative Cancer Care (ICC) holistic vision has led to the emergence of a solid team concept (“All for one and one for all”) that has generated a very strong engagement.
Our Oncology Departments have done a huge job, in a very short time. But now, with deescalated measures in Spain and other countries, we are presented with a unique opportunity to be a part of a cultural transformation in Oncology: The challenge of renaissance in the era post-COVID-19.
Some of the changes in practice which occurred in the COVID era are here to stay for several reasons. They improve patient and staff safety, lead to operational efficiencies, and efficacy in treatment, improve quality and team workflow and engagement. In addition, by continuing such strategies, we can be ready in case of another wave of this or a similar pandemic. This is an example of flexibility in our company, not only we have adapted to the difficult situation but also, we have learnt (innovation and improvement). Facing a health crisis, the doctor leadership should be consolidated and for this reason, a high engagement of our doctors across the network is an essential key point. The oncology sanitary system should be continuously reinforced and should be flexible plus solid as an accordion.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-rw-id-00162/ https://ijclinmedcasereports.com/pdf/IJCMCR-RW-00162.pdf
0 notes
Text
Endometrial Thickness and Frozen Thaw Embryo Transfer- A Prospective Study by Sakthi A*

Abstract
Aim and objectives: Endometrial Window of Implantation (WOI) is open in the midsecretory phase wherein the markers of invasion and cell adhesion are manifested .The primary objective was to find out the predictive value of Endometrial thickness and profiles a prognostic factors for embryo transfers during ART.
Materials and Methods: Endometrial thickness assessment was performed with grey scale ultrasound on the day of transfer just before thawing the embryos in patients undergoing Frozen embryo transfer cycle after endometrial preparation.
Results: The mean age and standard deviation of study population was is 33.26+5.95.Out of 69 patients there was clinical pregnancy in 33 patients, miscarriage in 10 patients and ongoing pregnacy in 23 patients. So the implantation rate was 47.83% (33/69), early miscarriage rate (pregnancy ending before 12 weeks) was 14.49% (10/69) and the ongoing pregnancy rate was 33.33% (23/69).Endometrial thickness <6mm had comparable implantation rates but low ongoing pregnancy rates.
Conclusion: The ultrasound morphological and vascular grading of endometrial thickness and vascularity is useful to synchronise Day 5 embryo transfer and window and implantation thereby minimising the loss of good embryos in nonreceptive endometrium.
Keywords: Endometrium; In vitro Fertilization: Implantation; Embryo
Introduction
Endometrial Window of Implantation (WOI) is open in the midsecretory phase wherein the markers of invasion and cell adhesion are manifested [1] .The human endometrium has a functional layer and basal layer each consisting of stroma and epitheium [2]. In the functional layer, the epithelium is involved in embryo adhesion and stroma is involved in embryo nurturing [3]. The basal layer epithelium and stroma mainly helps in regeneration(3). Though several advances have been made in genomics, transcriptomics and the various other interactomes like proteomics and lipidomics of endometrial receptivity, the biophysical markers of endometrial thickness and vascularity are economic and feasible in clinical settings.The classical Noye’s histological grading using the LH peak takes into account the seven characteristic histological attributes of mid secretory endometrium that predict its implantability [3].
The definition of recetive endometrium that is after 7 days of LH surge and after 5 days of progesterone includes eight histological featues. Epithelial features are the fraction glandular cells in mitosis, the visualisation of nuclear pseudostratification, the presence of secreting basal vacuoles. The stromal features are edema, pseudodecidualization, stromal mitosis and leucocyte infiltration.The assessment of receptive endometrium by ultrasound needs to be assesed as compared to this gold standard of window of implantation [4].
Endometrial Receptivity is integral to implantation so identification of an accurate marker of implantation would be highly beneficial in assisted reproductive technology (ART). Despite enormous research in the field of human embryo implantation, the ideal marker of Endometrial Receptivity remains unidentified [5, 6,7].
On ultrasound monitering in IVF cycle the endometrial thickness increases in the follicular phase and endometrial character changes from a hypoechoic trilaminar one to a compact hyperechoic look post ovulation [8]. A tri laminar endometrium on the day of ovulation trigger is associated with an increased probability of pregnancy while a hyperechoic character signals failure [9].
In proliferative endometrium there is cellproliferation and cell differentiation and vascularization in response to estrogen. The secretory phase can be classified as early secretory , midseretory and late secretory [10]. The early secretory endometrium shows increased intracellular transport and cell metabolism. The midsecretory endometrium or the “Window of implantation” shows immune system signaling and intracellular communination and cell adhesion [11,12]. The late secretory endometrium is mostly inflammtory mediators and apoptosis The first half of the sectretory phase is charactereised by expression of soluble ligands and their recetors coded by progesterone related genes. The second half of the secretory phase is characterised by vasoconstriction and inflammory response. Decidual reaction of endometrium happens soon after the closure of window of implantation and this change does not depend on the presence or absence of blastocyst.The activation of innate and humaral immunity characteristic of decidualization are interpretted as 5 line pattern and zonal vascularisation of endometrium [13,14,15]. This study was done to find the role of endometrial patterns and thickness in predicting and optimising ART outcome in Frozen Embryo transfer.
Material and Methods
This prospective study examined 69 infertile women who underwent embryo replacement from Jan 2019 to Nov 2019 at the ARC Fertility centre, Saveetha Medical College and Hospital. Ethical committea approval and institutional review board approval was obtained (SMC/IEC/2019/11/008). Inclusion criterium was Age group 25-45, two or more blastocyst (grade3/4) available for replacement and normal uterine cavity in hysteroscopy. Exclusion criteria was presence of endometrial polyp, congenital uterine Anamolies, adenomyosis, endometriosis,hydrosalphinx and fibroid uterus. Written informed consent was obtained from all participants in local language.
The endometrial thickness and pattern was visulised on the day 18 of previous cycle before Frozen Embryo Transfer cycle(Mock cycle).Endometrium was prepared with estrogen started from day 1 of cycle(2 mg/day from cycle days 1 to 4, 4 mg/day from days 5 to 8, and 6 mg/day from days 9 to 12) . Progesterone was added after endometrium reched a thickness of 8 mm to initiate the secretory changes (40 mg intramuscular administration of progesterone was provided and maintained for the following 5 days).
Low dose Aspirin(75 mg once daily) was administrated for improving endometrial receptivity. Day 3 Embryos were thawed and embryo replacement was done on day 4 after 3 days of progesterone administration.
From day 8 of cycle 150 IU of HCG was given intramuscularly to promote endometrial thickness reaches at least 7 mm.HCG has been shown to associted with decidualization process signalling via Vascular Endothelial Growth Factor (VEGF), Leukemia Inhibiting Factor(LIF), Insulin like growth factor like Binding protein 1. It also signals the secretion of Matrix mettaloproteinases from NK cells and secretion of Monocyte Colony Stimulating Factor. HCG also inhibits apoptosis promotes differentiation of stromal cells.
Descriptive and inferential statistics were used to analyse the data. Odd's ratio was used to analyse categorical variables. Predictive values of Endometrium >6 mm was calculated for Biochemical pregnancy , Clinical pregnancy and ongoing pregnancy. Statistical Analysis was done using MEDCALC (Belgium).
Results and Analysis
A total of 69 patients with history of thin endometrium who underwant frozen ET after treatment in ARC Fertility centre, Saveetha Medical College over a period for one year were analysed in this study. The mean age and standard deviation of study population was is 33.26+5.95.Out of 69 patients there wasclinical pregnancy in 33 patients , miscarriage in 10 patients and ongoing pregnacy in 23 patients. So the implantation rate was 47.83%(33/69), early miscarriage rate (pregnancy ending before 12 weeks) was 14.49%(10/69) and the ongoing pregnancy rate was 33.33%(23/69).
Table 1a shows the clinical pregnancy (fetal pole and cardiac activity) diagnosed by ultrasound in group 1 and group 2. There were no significant differences in implantation rates in thin and thick endometrium.Table 1b shows the ongoing pregnancy (till second trimester) diagnosed by ultrasound in group 1 and group 2. Table 1b shows that there are fewer ongoing pregnancy in thin endometrium as compared to thick endometrium.This implies that though there are implantations in thin endometrium there are more chances of miscarriage and there is less chance of ongoing pregnancy if endometrium is less than 6 mm.
Discussion
Endometrial thickness assessment is done routinely before embryo transfer and thin endometrium is considered as poor predictor and embryo transfer is deferred. However one must remember that there are isolated case reports of successful implantation in very thin endometriums also [16,17,18]. In 2 D ultrasound the endometrium is classified as Grade A, B and C.The Grade A endometrium the 5 layered endometrium and the intervenning area between the outer and inner echogenic areas is more echogenic than the surrounding endometrium. In Grade 2 endometrium the intervening is less echogenic than the surrounding endpmetrium. In Grade 3 endometrium the enometrium is homogenously isoechoic. This changes successively represent the rise and release of glycogen containing vacuoles up to the endometrial surface [19].
On Colour Doppler the vascularity can reach to varius zones as characterised by Applebaum’s [20]. The outermost vascularity zone is subzonal vascularity. Blood vessels reaching the 2 mm thick area surrounding thethe hyperechoic outer layer of the endometrium. Zone 1 is the outermost myometrial endometrial junction . Zone 2 is the hyperechoic outer endometrium. Zone 3 is the inner hypoechoic endometrium. Zone 4 is the endometrial cavity.The reasons for low implantation could be a high impedance blood flow of the radial arteries leading to poor endometrial glandular growth in thin endometrium . Poor angiogenesis subsequent to decreased VEGF secretion can also affect endometrial vascularity.This in turn increases chances of poor placentation and inappropriate vascularization leading to early abortions even if pregnancy is established. Transfer of embryos to an endometrium prepared by HRT seems to yield better results than fresh embryo transfers [21,22]. The other parameters included assessing uterine biophysical profile for implantation are summerised in Table 3 (Table 3).
Other agents that are used to improve endometrial thickness and vascularity are Filgrastin Intrauterine instillation, Vitamin E, L arginine and sildenfil citrate [23].
Conclusion
The solution where the glasses are disinfected will have a concentration of 1 to 10, that is, 10ml of Sodium Hypochlorite in 1000ml of Water.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-ra-id-00157/ https://ijclinmedcasereports.com/pdf/IJCMCR-RA-00157.pdf
0 notes
Text
Origin and Physical Properties of the Black Hole by Orlov S*

Abstract
A new physical model is proposed for the appearance of an astronomical object - the Black Hole. It is shown that the Black Hole is the center of the cosmic, etheric, gravitational torsion. An equation for determining the radius of this object based on the theory of vortex gravity is presented. A substantiation is proposed that the force of gravity on the surface of the Black Hole does not depend on the mass of this Black Hole. The mass of the Black Hole can not be determined. A contradiction is shown in the Schwarzschild solution by the definition of the radius of the Black Hole.
Keywords: theory of vortex gravitation, celestial mechanics.
Introduction
According to many astrophysicists, astronomical object the Black Hole (BH) is an area in the space which gravitational attraction is so great that light quanta can't leave it even. Researchers believe that Black holes could result from catastrophic gravitational collapse of a massive star at that historical moment when it dies. At collapse - catastrophic compression of a star - intensity of gravity over its surface becomes so terribly big that the space surrounding a star - time is displaced. This star disappears from the Universe and there is only strongly bent area of space - to time. The border of this area is called as gravitational radius. Spherically a symmetric black hole it is equal in the elementary case to Shvartsshild's radius. Theoretically possibility of existence of such areas of space - time follows from some exact solutions of the equations of Einstein, first of which was received by Karl Shvartsshild in 1915 [1].
Where, rs – the radius of the Black Hole, M – the mass of a black hole, with - the velocity of light, G=6.672 ∙10 -11 N∙m2/kg2 – a gravitational constant. We will consider objectivity of a hypothesis of an origin of the Black hole on the example of similar object which is in the center of our galaxy. In work [2] the radius of this BH which is called the Sagittarius A * is determined –
At such radius and the corresponding volume, the mass of this BH has to be on the basis of a formula (1) about 1039 kg. Then density of the Black Hole in the center of our galaxy has to be about 5 kg/m3! ? On the basis of the classical equation about a mutual attraction gravitation force on a surface of the Sagittarius A * is equal
F = 6.8 x 104 M
Agree, it is impossible to call this Black hole "catastrophically squeezed", and gravitation forces on its surface "terribly big". It is obvious that the theoretical explanation of an astronomical phenomenon of the Black hole doesn't correspond to physical parameters. In addition, equation (1) is mathematically absurd. In it, the quantities (G) and (c) are constants. Therefore, the mass of the Black Hole (M) is directly proportional to its radius (r). In fact, the mass of any body is always proportional to its volume. The volume is proportional to the radius of this body in the cube (r3). Then the mass must also be proportional to the radius in the cube. From this discrepancy with the laws of mathematics of equation (1) it follows that the density of the Black Hole (P) is inversely proportional to the root of its cubic radius. P ~ r-1/3
Example, On the basis of formula (1), we shall determine the mass of the Black Hole with a radius equal to 1 m.
Then the density of this black hole is
This density is several orders of magnitude greater than the density of the nucleon. Consequently, equation (1) is absurd. It is offered to study the theory of vortex gravitation and cosmology below. On the basis of this theory it is possible to explain genesis of the Black hole without contradictions.
About the Theory of Vortex Gravitation
The theory of vortex gravitation [3] is based on the well-known astronomical fact – all heavenly objects rotate. The most logical explanation of the reason of this movement can be only one – rotation of heavenly objects generated vortex rotation of space substance – ether. Ether forms system of the interconnected whirlwinds in world space. Orbital speeds of ether in each tuft (torsion) decrease in the direction from the center to the periphery under the law of the return square of this removal. If orbital speeds of a stream of ether decrease then, under aerodynamics laws, pressure in this stream increases. The gradient of pressure generates pushing out force in the direction to zones with the smallest pressure, that is to the center of this torsion. We will consider the equation of vortex gravitation received in the theory [3]. In this section, a model of appearance of the gravitation attraction force is considered from the viewpoint of aerodynamics. Namely, the two-dimensional model is considered on the basis of the following initial postulates. These postulates will be expanded and defined more exactly below.
Forces operating on a body 2 are specified. The Fc-centrifugal force, Fp-force of an attraction of a body 2 from a body 1, v2 – the linear speed of a body 2 on an orbit, R – the radius of an orbit, r1 – the radius of a body 1, r2 – the radius of a body 2, w1 – the angular speed of rotation of air on a surface of a body 1, m2 – body weight 2.
As it was already spoken, movement of a whirlwind is resulted by pressure gradient. Radial distribution of pressure and ether speed in work [3] are defined on the basis of Navier-Stokes's equation for movement of viscous liquid (gas).
In cylindrical coordinates taking into account radial symmetry of vr=vz=0, vj=v (r), P=P (r) the equation will register in the form of system
Where r = 8.85 х 10-12 kg \m3 - density of ether [4], – a vector of speed of ether, P – pressure of ether, h- viscosity.
In cylindrical coordinates for the module of force of gravitation
Then comparing (3) and (4) for incompressible ether (r=const) we find that
After necessary transformations (full calculation is stated in the theory [3]) it is received:
1 . the equations for determination of force of gravitation depending on the speed of rotation of ether
rn, mn – radius and mass of a nucleon.
We will transform a formula (6). We will equate r1 = r. We will substitute w1 r1 = v1 and numerical values rn, mn, r, we receive:
2. The equations for determination of dependence of pressure of P0, from the speed of rotation of ether of V1
Where – pressure of ether on we consider P0 to an orbit, using a boundary condition
In fig. 2 pressure distribution according to a formula (8) is graphically shown.
Vortex Black Hole
Асcording to laws ether-loudspeakers [4] pressure in motionless air is accepted size
Ether density
By means of the equation (8) we will find the orbital speed of ether of V0 = V1 at which pressure of P0 will be equal to zero.
from where
Orbital speed of ether to belong to the radius of the orbit under the law of the return square
where
R0 – radius of an orbit of a whirlwind on which ether reaches speed
Rkn – radius of an orbit of a whirlwind in which the speed of ether is known (Vkn).
From the equation (9) we find the orbital radius of the radio torsion with zero pressure.
Orbital speed of ether of Vkn is determined by the known force of gravitation in the same orbit, by means of the equation (7).
Radius of the Vortex Black Hole of the Sagittarius*
We will consider the Sun address in a galaxy orbit.
Orbital speed of solar system -V = 2.2 * 105
Radius of an orbit of solar system - Vkn = 2.46*1020 [5].
We determine the centrifugal force operating on the Sun.
Provided that centrifugal forces, in any point of an orbit, are always equal to attraction forces, we find force of the galactic gravitation operating on the Sun.
We substitute value Fп and r in the equation (7) and we find ether speed in a solar orbit.
Radius of an orbit of astronomical object the Sagittarius* with the zero pressure upon surfaces, on the basis of the equation (10)
The strength of the vortex gravitation on the surface of a black hole
Fg = 620 x M
Similarly, we find radiuses of Black holes at other objects:
Sun - R0 = 155500 m
Eartht - R0 = 0.478 m
Conclusion
Obviously, the modern theory of the origin of black holes contradictory. On the example of a celestial object Sagittarius A* can be argued that Black holes are not superdense and supermassive objects. They may not have a huge force of gravity at its surface. Based on the theory of vortex gravitation and cosmology, black holes is the central region of space, ether, gravitation torsion. Orbital velocity of the ether on the surface of this area reaches the maximum possible value
At this speed, the pressure on the rotationorbitof theesterdecreases to zero. No substanceorradiation is notable tobreak out ofthis zone.Therefore, the centerspace, gravitation torsioninvisible.Insidethe black holerotationetherorstopsorslows down. In this case,there can existinside a black holeof antigravity.
Note. A similar phenomenon is noted in the center of tropical meteorology and sea storms. Where there is complete peace of mind (calm). This phenomenon is called the "eye of the storm." Radius of the black hole Sagittarius A * at the center of our galaxy observations to determine the magnitude
The estimated value of the radius of the black hole Sagittarius A *, obtained in Chapter 4 (1,382×〖10〗^14 m) higher than the observed value of two orders of magnitude. This is not a calculation error, and the inequality of the radii of the Black Hole in the longitudinal (orbital) and transverse (axial) dimension. The fact that black holes have their form likeness forms of galaxies - and the disk are located in outer space, in the same direction as the galaxies themselves. Terrestrial observer is on the periphery of our galaxy and it can measure their visual observations center of the galaxy (Sagittarius A *) only in the transverse axial dimension. At the same time, disk Sagittarius A * its plane directed to us, so we can determine the calculations only the distance in the longitudinal direction radially. Therefore, calculations determined the orbital radius, and observations - transverse axial thickness of the black hole Sagittarius A *. Radius of gyration of any cosmic torsion far exceeds its axial thickness. For the black hole Sagittarius A * this fact recorded in this paper calculations and astronomical observations.
Gravitational torsions can be of different sizes. Each torsion creates its material object. Micro torsion create atoms. Planetary - planet. Star - star. Galactic - galaxies. Universe - the universe. All torsions in their centers hase black holes. In celestial bodies (atoms, planets, stars, etc.) they are under a layer of the material of which they are created. Therefore, they are hidden from us. In large space objects such as galaxies, they are open and subject to study. Modern classic exercise in cosmology and astrophysics have a lot of controversy for one reason. All of them are based on a global error of the classical theory of gravitation, which states that all bodies create gravity. In fact the opposite is true - gravity creates the body.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-rw-id-00156/ https://ijclinmedcasereports.com/pdf/IJCMCR-RW-00156.pdf
1 note
·
View note
Text
Laser Therapy for Treating Tuberculosis by Victor V Apollonov*

A Bit Scary Statistics
For a start, as a preamble, here are some excerpts from various sources on the problem of tuberculosis (TB), which are quite strange to read at the beginning of the third millennium, since many people confidently believed that there has been enough time to solve this problem during the past two millennia:
- Tuberculosis symptoms and signs: cough, loss of weight, chest pain, fever, night sweats. If untreated, 50 percent of patients die within five years;
- More than any other infectious disease, TB kills approximately 1 million women per year. Each year, TB kills 100 000 children. Tuberculosis is the most common cause of orphanage;
- Untreatable bacteria can destroy the progress of TB control achieved in the last 50 years. There are no drugs to combat some resistant TB bacteria (in developed countries 50 million people may be infected);
- The majority of people infected with TB never become sick because their immune system prevents the development of TB mycobacteria. Only 5 to 10 percent of those infected develop TB. Scientists today do not know exactly why some infected people develop TB and die, while others do not;
- At least one person is infected with TB every second, 1 percent of the world's population are infected each year. Untreated persons infect on average 10–15 neighbors during a year. For major cities, this figure is considerably higher. The most susceptible to infection are prisons, the Army and the Navy, where the concentration of people living together for a long time is the greatest. According to the WHO over the past two centuries, TB killed about a billion people. The WHO warns that unless we take urgent action, in the next 10 years, TB will kill an estimated 30 million people and infect 90 million people. Further, by the end of 2020 a billion people will have been already infected: 200 million people will be sick and 70 million people will die. So much for the White Plague (because of the extreme pallor seen among those infected)!
Laser Treatments for Tuberculosis
Currently, we know two approaches to fabricating laser systems for the TB treatment. They are based on excimer lasers and installations making use of important benefits of miniature solid-state diode-pumped lasers. The peak of the bacteriostatic activity of the generated laser radiation in various forms of TB lies at a wavelength of 265 to 266nm, and in this case, the effectiveness of its action is equal to unity. The wavelength of 248nm, which is emitted by an excimer laser, is closest to this range. At this wavelength, the interaction efficiency amounts to 0.8, which requires a proportional increase in the irradiation time. For a solid-state Nd:YAG laser (fourth harmonic) the radiation wavelength is equal to 266nm. The interaction efficiency of this wavelength is 1.0. The pulse energy with an average output power of 10mW (equal to the product of the energy in a single pulse by the pulse repetition rate). The power is determined experimentally in cultures of bacteria for the exposure time of 10 to 15min.
For an excimer laser the pulse repetition rate is no more than 100Hz; therefore, the energy of a single pulse is less than 0.1mJ, which can lead to tissue burn at a pulse duration of 5–10ns. To ensure a ‘soft’ effect on tissues, it is needed to reduce the pulse energy by one or two orders of magnitude, which is possible, but requires a proportional increase in the exposure time. At these energies (0.1mJ) an optical fiber is usually damaged. An optical fiber requires a high optical purity of working surfaces which is problematic when administering it in various cavities. The destruction of the output end of the fiber may cause penetration of small glass fragments into the patient. In a solid-state laser the pulse repetition rate is maintained at a level of 10000Hz; therefore, the energy of a single pulse is only 0.001mJ. That is why the soft tissue burn and destruction of optical fibers in the case of solid-state lasers is fundamentally impossible.
Now let us say a few words about the service life of some elements of lasers. In the case of an excimer laser, the main element is a gas tube, whose service life is about 1000–2000 hours at a cost of about 1000 USD. High-energy pulses can also lead to an early failure of optical elements. In the case of a solid-state laser, the essential element is a laser diode, whose service life amount to least 5000 hours at a cost of 700–800 USD.
The presence of hazards when working with lasers discussed is as follows. An excimer laser has in its design a significant amount of harmful gas. Besides, this laser requires a high voltage for its operation (about 10kV). The design of solid-state lasers is free of hazards, whereas the cost of the components of these lasers is approximately comparable with that of excimer lasers.
As for the additional conditions of production of the laser sources discussed, excimer lasers, apart from standard a optical-mechanical and an installation sites, also require the presence of a vacuum site, equipped to work with poisonous gases. The production of solid-state lasers requires only a standard optical-mechanical and an installation sites.
Amulet Semiconductor Laser Apparatus
An Amulet semiconductor laser apparatus with a fiber for introducing radiation in the affected area through an injection needle is intended for the treatment of destructive forms of pulmonary and bone TB that are resistant to conventional medical treatment, as well as to shorten the treatment of common forms of TB by topical exposure of the infected surface to ultraviolet (UV) radiation with a wavelength of 266 nm, which has very strong bactericidal and bacteriostatic effects. UV radiation in this case has low intensity and only affects the microflora without any damage of the living tissues of the human body. The typical time of UV irradiation of the affected area is 5 to 15min. In this case, the traumatic effect is absent.
The Amulet apparatus (Figure 1.) is designed to treat patients with tuberculosis affecting lungs, bronchi, bones and joints, to cure diseases associated with suppurative infections and other inflammatory processes, with the abnormal healing process, with the immune system variations and instability of the capillary circulation. In addition, the apparatus can be used in endosurgery, phthisiology, otolaryngology, traumatology, stomatology, treatment of burns, gynecology, therapy, surgery, urology, proctology, and dermatology.
Clinical Trials of the Amulet Apparatus
Fryns syndrome (FS) is a rare autosomal recessive congenital anomaly syndrome with an incidence of 0.7 per 10000 births [1]. The 6 diagnostic criteria for FS are as follows: 1) congenital diaphragmatic defect, 2) characteristic facial appearance, 3) distal digital hypoplasia, 4) pulmonary hypoplasia, 5) characteristic associated anomalies like polyhydramnios, brain malformations, ren
Conclusions
Thus, the clinical trials performed allow us to make a conclusion that a therapy UV solid-state diode-pumped Amulet laser is effective in the treatment of TB-affected tissues and bones due to the bactericidal and bacteriostatic effect and stimulation of reparative processes. It could be used for many other applications in the practical medicine.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-sc-id-00153/ https://ijclinmedcasereports.com/pdf/IJCMCR-SC-00153.pdf
0 notes
Text
Evaluating the Utility of Fast in Acute Blunt Abdominal Trauma in the Emergency Department: 20 Years On by Lateef F*

Abstract
Introduction: Blunt abdominal trauma (BAT) is a common presentation in the Emergency Department (ED) and associated with high mortality and morbidity. Given the time-sensitive nature, it is necessary to evaluate if FAST possesses adequate sensitivity and specificity to confidently rule out life-threatening injuries and guide the course of management. A positive FAST result would indicate intra-abdominal injury and prompt urgent surgical intervention, particularly in hypotensive patients. This review aims to examine relevant literature to evaluate the diagnostic utility and outcomes of FAST, and important external factors to be considered.
Methodology: Keyword search of PubMed and the Cochrane Library yielded 514 articles, from which 61 studies were chosen based on the inclusion and exclusion criteria.
Results: FAST demonstrates low to moderate sensitivity and Negative Predictive Value (NPV) and high specificity and Positive Predictive Value (PPV) in detection of hemoperitoneum and associated intra-abdominal injuries. Sensitivity for detecting peritoneal fluid is the highest. While superior to DPL, it has yet to surpass the diagnostic utility and accuracy of CT.
Conclusion: FAST is essential and should remain the primary preliminary radiological assessment of acute BAT. A positive FAST is highly predictive of intra-abdominal injury but a negative FAST cannot accurately rule out intra-abdominal injury. Negative FAST results should be succeeded by continued clinical observation, and serial FAST examinations or CT-scan should clinical signs not correlate. Current literature offers no evidence that FAST should replace CT as the diagnostic standard for BAT or a definitive ability to determine the necessity of immediate surgical management.
Keywords: Focused Assessment for Sonography; FAST; E-FAST; Ultrasonography; Point Of Care Ultrasound; Pocus; Blunt Abdominal Trauma; Laparotomy and CT
Introduction
Abdominal trauma is a common presentation in the ED and also one of the leading causes of death in young adults, under 45 years. It can be broadly classified into high or low energy injuries, and blunt or penetrating abdominal trauma. Blunt abdominal trauma (BAT), may be the result of road traffic accidents, physical assault or falls from height. Penetrating injuries are generally caused by firearms and stabbings. The focus of this review will be blunt abdominal trauma, as it is by far the more common presentation. A study was conducted by The Western Trauma Association Multi-Centre Trials of 392,315 blunt trauma patients at 12 major trauma centres. Majority of the injuries were caused by motor vehicle collisions (60%). 47% of the patients had documented hypotension and solid organ, small bowel, and large bowel injuries occurred in 38%, 35%, and 28% respectively. The most commonly associated injuries were spine fractures (44%) and pneumothorax/haemothorax (42%) [1].
Up to 50% of patients with severe abdominal trauma and/or multiple distracting injuries are reported to either have a normal initial abdominal exam, or are obtund and unable to provide a reliable index of suspicion. This affects both the physical and imaging examinations [2]. Diagnostic errors are responsible for approximately 10%–15% of preventable deaths in trauma centre audits. The sole reliance on clinical assessment as the main indication for surgery has led to negative laparotomy rates of as high as 40% [3]. A retrospective analysis found the incidence of short‐term complications caused by negative laparotomy to be 43% [4].
A quick, effective and efficient imaging approach is necessary to exclude life-threatening injuries. This modality would preferably need to have high sensitivity and specificity [5]. Prior to FAST, Diagnostic Peritoneal Lavage (DPL) was the standard initial diagnostic investigation. Although an invasive test, it could be done rapidly and was relatively safe with high sensitivity but had a significant false‐positive rate, which potentially exposed patients to the risks of an unnecessary laparotomy [6]. All patients who sustain blunt trauma to below the nipple line, are assumed to have intra-abdominal injuries until proven otherwise. Prompt reliable diagnosis and characterization of the abdominal injuries is essential to reduce risk of mortality and morbidity. Hemodynamic instability is a high-risk clinical sign and as such, both the diagnostic and interventional thresholds for these patients should be lowered. The three main types of blunt abdominal trauma injuries are solid organ injury, hollow viscos/mesenteric injury and vascular injury. The most commonly injured intra-abdominal organ is the spleen, followed by the liver and the genitourinary tract [7].
Immediate laparotomy should be done for patients with signs of peritoneal irritation, fresh blood on rectal exam, fresh blood aspirated from nasogastric tube, stab wounds with implement in-situ, gunshot wounds traversing the abdominal cavity, suspected intra-abdominal injury with hemodynamic instability, ultrasound evidence of active haemorrhage, and X-ray evidence of pneumoperitoneum or diaphragmatic rupture. In a retrospective cohort study of consecutive normotensive blunt trauma patients at 2 trauma centres, there was a strong association between a positive FAST and the need for therapeutic laparotomy. (Adjusted OR 44.6, 95% CI 1.77–1124). Thirty-seven percent of patients with a positive FAST required therapeutic laparotomy vs. 0.5% with a negative FAST [8]. Another study quoted lower figures, where only 25% of patients with intra-abdominal fluid required laparotomy [9].
Imaging modalities most often used to evaluate abdominal trauma in the ED are the Focused Assessment for Sonography for Trauma (FAST) and the Computed Tomography scan (CT-scan) which is the current reference diagnostic gold standard. The purpose of this study is to present a systematic review on the utility of the primary first line imaging modality FAST, in the acute assessment of blunt abdominal trauma.
Methodology
A systematic review of the literature was achieved using the electronic database PubMed and the Cochrane Library. Various query terms were tested to obtain enough data and to avoid unspecific information. Duration of search was from 1stMarch 2020 to 1stApril 2020. There was no limit on geography, age, type of study or date of article. Only original studies published in English were considered for this review. Keyword search yielded 514 articles, from which 61 studies were chosen based on the inclusion and exclusion criteria.
The keywords used in the search include: Focused Assessment for Sonography, FAST, E-FAST, Ultrasonography, Point of Care Ultrasound, PoCUS, Blunt abdominal trauma, Laparotomy and Computed tomography, CT
For studies to be included in this study, the inclusion criteria are as follows:
Acute presentation of blunt abdominal trauma at the ED
PoCUS/FAST or E-FAST examination done performed by radiologists, non‐radiologist clinicians, or ultrasound technicians
Definitive diagnosis verified by CT-scan or operative diagnosis.
Sufficient information on diagnostic test accuracy (i.e. sensitivity, specificity)
The studies were excluded if:
Insufficient information on diagnostic test accuracy
Case reports, case series
Unclear index or reference tests
Diagnostic case-control studies that compared patients with known case status to healthy controls. (This creates artificial populations and tends to overestimate sensitivity of the index test)
Patients with penetrating abdominal injuries
Results
Focused Assessment for Sonography for Trauma (FAST)
Ultrasound based trauma algorithms were only introduced formally into trauma literature in 1996.FAST is a limited abdominal ultrasound modality used in acute trauma as part of Advanced Trauma Life Support (ATLS)protocol to identify intra-abdominal fluid collections using a 3.5Hz sector transducer. FAST was established in 1999 after the FAST consensus conference and a subsequent study done at Massachusetts General Hospital in Boston, USA, showed the number of FAST scans increased from 15 % to approximately 34 % in the period 2002–2011, while the number of abdominal CT scans decreased from 35 % to 14 % in the same period [10]. In a prospective study on influence of FAST on trauma management, 194 patients underwent FAST. It was shown that FAST prevented an unnecessary laparotomy in 1 patient, CT in 23 patients, and DPL in 15 patients. There was an overall reduction in CT requests (from 47% to 34%) and DPL requests (from 9% to 1%) (p < 0.0001) [11].The goal of FAST is to detect hemoperitoneum in the right and left sub phrenic space, peri-splenic fossa, hepatorenal recess, suprapubic window (Pouch of Douglas or rectovesical pouch) and hemopericardium in the subxiphoid space. A positive FAST result would mean that there is free fluid in either of these abdominal compartments, which is a surrogate for active haemorrhage and in one study, has demonstrated a 65% sensitivity in detection of abdominal injuries requiring surgery [12].
E-FAST and Ex-FAST
E-FAST was established in 2004 and is now the diagnostic standard of ATLS, virtually replacing DPL. The E component refers to bilateral anterior thoracic sonography which searches for free air in the pleural cavity as evidence of an acute traumatic pneumothorax. It has been shown to have greater sensitivity and specificity than traditional chest radiography [13]. There is also some reference to Extended FAST or Ex-FAST. It is a combination of both physical examination and FAST. An abnormal examination constitutes signs of hemodynamic instability, abdominal bruising, tenderness, absence of bowl sounds, peritonism, seatbelt sign, lacerations etc. [14]. In a retrospective study of 354 children in the ED of which 14% (n=50) had intrabdominal injury (IAI), the use of Ex-FAST showed greater sensitivity (sensitivity of 88% (95% CI: 76‐96%) and Negative Predictive Value (NPV) 97.3% (95% CI: 94.5‐98.7%)) over either physical examination [OR, 15.2; 95% CI: 7.7 ‐ 31.7] or FAST [OR, 14.8; 95% CI: 7.5 ‐ 30.8] alone [15].
The execution time of E-FAST examination averaged 2.3 ± 2.9 min for chest US and ≤5 min for standard FAST [16]. FAST has been reported to be able to detect as little as 200ml of fluid in Morrison’s pouch and can completed in less than a minute in the hands of an experienced operator. This is many times faster than a CT-scan which on average takes approximately 30minutes and hence unsuitable for an unstable patient in an emergent setting. Moreover, it is easily repeatable, physicians can be easily trained, inexpensive, non-invasive and does not require contrast nor exposes the patient to ionizing radiation. Although these are insufficiently substantiated by sufficient evidence, other possible beneficial outcomes include shortening of the primary trauma assessment, more precise triaging, avoidance of unnecessary interventional procedures, and associated costs
The reliability and quality of images obtained from FAST is also greatly dependent on the training and experience of its operator. A comparison of the reproducibility of FAST results between Emergency Medicine Residents (EMRs) and Radiology Residents (RRs) showed sensitivities, specificities, PPV, NPV and accuracy of evaluating intra-peritoneal fluid to be very similar at 80%, 95%, 57%, 98% and 94% and 86%, 95%, 59%, 98% and 94%. This shows that EMRs are well-trained to use FAST and their results would be similar if not identical to an RR [17]. However, a comparism done in another study amongst US operators with low, moderate and extensive experience reported sensitivities of 45%, 87%, and 100% respectively in detecting <1L of peritoneal fluid [18].
A recent review article has quoted FAST sensitivities that range between 63 % and 99 % and specificities range from 90% to 100%. These results are similar for the detection of free intraperitoneal fluid, with sensitivities ranging from 69 % to 98 % and specificities of 94% to 100% [19]. Another study reviewing literature from various institutions around the world has reported lower thresholds of sensitivities ranging from 42.0%–91.7%, specificities 83%–100% and accuracies 9%–96% for the utility of E-FAST examinations. Its own prospective observational study examining the diagnostic accuracy of E-FAST done by emergency physicians compared to CT at the ED of a level 1 trauma centre found that out of 132 patients with blunt abdominal trauma, FAST sensitivities (only abdomen) was 42.9% (95% CI: 9.9%, 81.6%) and specificity was 98.4% (95% CI: 94.3%, 99.8%). The + LR of the FAST exam for abdominal free fluid as 26.8 (95% CI: 5.3, 135.2) and − LR was 0.58 (95% CI: 0.31, 1.1) [20]. This consistently high reported specificity of FAST was highlighted in a systemic review of 11 articles containing prospectively derived data with FAST results, patient disposition and final diagnoses. It showed that out of the 2,755 patients, 448 (16%) went to the OR. In total, there were 5 false-negatives derived from FAST; 3 involving inadequate scans and 2 of blunt trauma-induced small bowel perforations without hemoperitoneum [21]. The sensitivity of an examination is the “correct positive test rate” and measures the proportion of patients with an intraabdominal injury who have a positive test result. A high degree of sensitivity is not useful to rule in a diagnosis, but rather to rule out a particular condition. Similarly, high levels of specificity indicate that positive findings will detect the presence of a pathology. This suggests that when FAST is positive, there is high certainty of injury but when it is negative there’s a higher chance the injury was undetected. Hence, there is still large uncertainty in diagnostic confidence, with its wide sensitivity range and cannot confidently or safely exclude the presence of intra-abdominal injury.
FAST in Abdominal Trauma
In a meta-analysis [22] of emergency ultrasonography for BAT, a sensitivity range was observed as low as 28% and as high as 97%, specificities were close to 100%. A summary measure of 0.90 was calculated for the sensitivity-specificity pair closest to the desirable upper left corner of the ROC curve, which could be interpreted as 10% of abdominal injuries will be missed by FAST. Low sensitivities, coupled with low NPV, negative LRs and associated post-test probability, diminishes confidence in negative FAST findings. However, high specificities and LRs>10 would almost confirm intra-abdominal injury if positive and hence the need for surgical management.
In a retrospective study, 3181 blunt normotensive trauma patients presenting at a single level 1 trauma centre were evaluated with FAST and stratified into various groups of Injury Severity Scores (ISS). A one-time, four-view FAST examination in patients with ISS ≥ 25 had a lower sensitivity of 65 % than those with an ISS < 25 (80–86 %). More than 82 % of the FAST-missed injuries in patients with ≥ 25 ISS were solid organ injuries of the liver, spleen and kidneys [23]. An observational study of the diagnostic accuracy of FAST in 105 patients from King Fahad Military Medical Complex Dhahran, Saudi Arabia with blunt abdominal trauma demonstrated sensitivities of 76.1% (95% CI, 64.14- 85.69%), specificity 84.2% (95% CI, 68.75- 93.98%) and accuracy 79% (95% CI, 70.01- 86.38%. FAST could detect free fluid in 37 out of 39 patients with high grade sold intra-abdominal injuries. However, it could not detect small amount of fluid and nearly half of the negatives had low grade visceral injuries [24]. These studies highlight potential factors that may affect the results of the FAST examination, such as the presence of multiple other distracting injuries, higher likelihood for missed solid organ injuries and reduced sensitivity for fluid in patients with only low-grade injuries.The reason for this could be that hemoperitoneum is not always seen in liver or splenic injuries and hence it doesn’t matter if FAST has a high sensitivity for peritoneal fluid [12].
A systemic review evaluating the diagnostic accuracy of point‐of‐care sonography (POCS) for diagnosing thoracoabdominal injuries in patients with blunt trauma included 34 studies with a cumulative cohort of 8635 participants. For abdominal trauma, POCS had a sensitivity of 0.68 (95% CI 0.59 to 0.75) and a specificity of 0.95 (95% CI 0.92 to 0.97), with statistically significant lower values in children. To put this in perspective, it meant 73 false negatives and 29 false positives for every 1000 adult patients, assuming the observed median prevalence of thoracoabdominal trauma of 28% [25].
In paediatric BAT patients, the diagnostic accuracy of FAST has been reported to be lower compared to adults. A multi-institutional (n=14) analysis of level1 paediatric trauma centres yielded low sensitivities (28%) and high specificities (91%) for IAI consistent with paediatric literature but improved sensitivities (44%) and similar specificities (89%) for IAI requiring acute intervention. However, FAST missed 75% of liver injuries and 57% of spleen injuries and 56% of 27 patients whom required acute intervention for IAI had negative FAST. All the patients were normotensive and had abnormal abdominal examination [26]. However, in a separate observational prospective study comparing FAST evaluation of hypotensive and normotensive children with BAT, FAST showed a 100% sensitivity in detecting peritoneal fluid in hypotensive patients [27]. A prospective study was done on 160 hemodynamically stable paediatric trauma patients who had undergone both FAST and CT. Forty-four of the 160 patients had an intraabdominal injury on CT, 24 (55%) of which had normal screening sonography. Accuracy of sonography compared with CT was 76% with a negative predictive value 81% [28]. While the statistics of these three studies on the use of FAST in paediatric BAT patients do vary, sensitivities and specificities are both generally on the lower threshold of the adult range. They also show consistency of hypotension as a strong predictor of IAI and the poor ability of FAST to detect solid organ injuries.
FAST and Other Modalities
A prospective study [16] was done of 601 adult trauma patients at the ED who underwent a Chest Abdominal-Focused Assessment Sonography for Trauma (CA-FAST) exam prior to a thoracoabdominal CECT. Free fluid was detected in 116 patients with an overall accuracy of 91 % (95 % CI 85–93%). The following table illustrates the results of 4-view FAST and its individual views
FAST has different sensitivities for each abdominal cavity view, which translates to different diagnostic accuracies for the various types injuries previously mentioned in the methodology has well. In this study, FAST exhibits moderate to good sensitivity than previously quoted and with similar sensitive for the upper abdominal regions, followed by the pelvis and least able to detect fluid in the subxiphoid, pericardial space. It also shows good PPV, high specificity and NPV, consistent with previous studies [16].
This is supported by a 2-year review at a level1 trauma centre of 1027 patients who underwent FAST were stratified by operator skill level. It was shown that compared to patients with concordant FAST results, those with equivocal results had higher mortality (9.8 vs 3.7%, P = 0.02), decreased positive predictive value in the right upper quadrant (RUQ) (55 vs 79%, P = 0.02) and left upper quadrant (LUQ) (50 vs 83%, P < 0.01). However, unlike the previous study, this study observed worse outcomes has a result of the high rate of false negatives in the FAST examination.
However, some of these findings were obtained from only a single FAST scan (i.e. [23]), with the underlying assumption that fluid accumulates in the deepest parts of the abdomen. This can be influenced by anatomy, location of bleed, respiratory physiology, intra-abdominal adhesions etc. Thus, it would be prudent to consider the value of serial FAST scans, Contrast Enhanced Ultrasonography (CEUS), additional abdominal views and other imaging modalities such as CT with or without contrast media. A retrospective analysis [29] comparing the use of CTAP and Complete Ultrasonography of Trauma (CUST) in 19128 patients to screen for blunt abdominal trauma (BAT) from 2000 to 2011 in a Level 1 trauma centre was performed. It found that outcomes in CUST is equivalent to routine CTAP for BAT and leads to an average of 42% less radiation exposure and more than $591,000 savings per year.
The shortcomings of FAST can be bolstered by the application of CEUS. A recent meta-analysis [30] of 9 studies investigating the diagnostic accuracy of CEUS of abdominal trauma patients at the ED demonstrated that the CEUS had a sensitivity of 0.981 (95% CI: 0.868-0.950) and a false positive rate of 0.018 (95% CI: 0.010-0.032) for identifying parenchymal injuries, with an AUC of 0.984. These accuracies are similar to that of contrast-enhanced CT. Another study done on the application of CEUS in paediatric patients concluded CEUS proved to be an effective investigation in the hemodynamically stable child for identifying parenchymal injuries and for the characterization of focal liver lesions. It also showed comparable performance to CT and MRI with a specificity of 98% for identifying benign lesions and a negative predictive value of 100% [31]. However, the need for contrast in identifying intra-abdominal injury may not always be relevant in contributing diagnostic value. It can add confidence in cases of interpretation doubts or diagnostic difficulties, but some studies have shown CEUS to have similar sensitivities to baseline US [32].
Splenic injuries are the most common intra-abdominal injury followed the liver in the setting of acute blunt abdominal trauma. CEUS has been shown to be able to overcome the lower sensitive of FAST in detection of traumatic injuries with the reference standard as CT, to reach almost similar levels of accuracies. Evaluation of severity of splenic injuries is particularly important in the decision for surgical management as the spleen should be preserved if possible, due to the dual immunological and haematological functions [33]. However, a retrospective cohort study [34] at a level 1 trauma centre of 332 patients found that patients with spleen, liver, or abdominal vascular injuries were less likely to have false-negative FAST examination results (OR 0.3; 95% CI 0.1 to 0.5). Surprisingly, false-negative FAST results were not associated with increased mortality (OR 0.89; 95% CI 0.42 to 1.9) and these patients were fortunately also less likely to require therapeutic laparotomy. (OR 0.31; 95% CI 0.19 to 0.52).This at first glance may seem puzzling compared to previous studies; however, this is consistent with the generally high specificities of FAST and its lower sensitivities for solid organ injury and lower grade injuries which naturally may be less likely to require surgical intervention or carry a high mortality rate.
Computed Tomography and Abdominal Injuries
Computed Tomography is superior to FAST in evaluating solid organ, hollow vicus, mesenteric injuries and active haemorrhage. However, it has disadvantages such as radiation exposure, risk of contrast nephropathy or allergy, high cost, limited availability, requires more time and the potential need for sedation in paediatric patients. A level 1 trauma canter in the USA reported the radiation exposure of patients with a median ISS of 14 within the first 24 hours at a median of about 40 mSv. The lifelong risk of dying from a carcinoma is assumed to increase by about 0.1 % per 10 mSV. This risk also depends on gender, age and radiation location [19]. Although this is a minute amount, we can conclude that CT scans should be avoided when possible as it does expose the patient to a significant amount of radiation, enough cause a measurable increase in cancer risk.
A recent retrospective analysis evaluated the diagnostic performance of CT for detection of hollow vicus injury (HVI) in patients presenting with penetrating abdominal trauma at a level 1 Nordic trauma centre. Out of the 636 patients with penetrating abdominal trauma, 155 (85%) had a CT-scan on arrival, of which 41 (30%) subsequently underwent emergent surgery. Surgery revealed only 26 (63%) has HVI, showing that CT had 69.2% sensitivity and 90.5% specificity in detecting HVI [35].
Although FAST showed high accuracy for peritoneal fluid, it’s non-specific for solid organ injuries and prevalence of organ injury without accompanying free fluid can range from 5% to 37% [36]. It also lacks sensitivity for hollow viscos and mesenteric injuries, which not are only the most commonly missed but also associated with high morbidity and mortality and has a higher likelihood for requirement of surgical intervention than solid organ injuries. A retrospective study done on 32 patients showed that MDCT could diagnose bowel injury in all of the patients except one. The minor signs showed a higher sensitivity than the major signs [3]. This suggests a sensitivity for bowel injury much greater than FAST which was 12.5% amongst 4 patients and 37.4% in another study [36]. Other studies have also quoted high sensitivities (94%) and PPV (92%) for CT in detecting bowel injury [37]. A meta-analysis [38] of articles concerning the incidence and significance of free intra-abdominal fluid on CT scan of blunt trauma patients without solid organ injury concluded that isolated finding of free intra-abdominal fluid on CT scan in patients with blunt trauma and no solid organ injury does not warrant laparotomy. Instead, its aetiology should be evaluated and other CT signs of GI perforation should be searched for. Small bowel injury had the highest incidence of positive free fluid without evidence of solid injury, but the combination of both pneumoperitoneum and free fluid increased the sensitivity of detection of small bowel injury [3].
When compared with its predecessor DPL, it showed significant advantage in its pre-test probabilities with a positive LR of 10.83 (95% CI 6.45 ± 18.17) and a negative LR of 0.11 (95% C.I. 0.06 ± 0.21). When compared to CT, FAST still had a positive LR 11´42 (95% C.I. 8.01 ± 16.29)) in confirming presence of intra-abdominal injuries, but it was still below acceptable thresholds in safely excluding abdominal injuries (negative LR 0.21 (95% C.I. 0.16 ± 0.29)), which is essentially the gold for immediate trauma management. Hence FAST is unable to be the diagnostic standard for obtaining a definite diagnosis [22].
Whole body CT (WBCT) is the gold standard for trauma imaging, however it is usually only supported by highly specialised trauma centres with the appropriate infrastructure. A clinical review highlighted observational data that suggested WBCT was associated with decreased mortality and time required for trauma evaluation [39]. On the other hand, randomized controlled data from the REACT-2 trial [40] suggests no mortality benefit to this diagnostic tool. There is no clear evidence or sufficient data to prove that CT should be the first line imaging modality in acute blunt abdominal trauma. As we simply lack the resources and time to conduct CT for every patient, not to mention the higher costs and having to subject every patient to ionizing radiation, the decision for CT should remain on a case to case basis. Decision making should be based on a combination of history, physical examination, clinical signs and other imaging modalities i.e. FAST/X-ray. More studies (i.e. RCTs) will have to be done to assess its outcomes over FAST in the emergency setting of BAT and its utility in assessing need for surgical intervention.
A study [41] assessed CT scans of paediatric patients with abdominal trauma for presence, location, and severity of intraabdominal injury, and amount of peritoneal fluid. It was found that only 17% of the 1,486 children had peritoneal fluid demonstrated by CT but 80% had concomitant intraabdominal injury. This suggests that although presence of peritoneal fluid is a strong indicator of intra-abdominal injury, it can be present without, with solid organ injury being the most frequent (68%). Furthermore, it may also indicate that like FAST, CT may have reduced sensitivity in picking up intra-abdominal injuries without peritoneal fluid. CEUS may be applicable for the 37% of patients with intra-abdominal injuries picked up by CT but no peritoneal fluid was detected.
Discussion
In the emergency department today, E-FAST is still the diagnostic standard for ATLS in the event acute abdominal trauma. Its findings, combined with history taking, physical examination and other imaging modalities (i.e. chest/abdominal radiography) would then determine the need for a CT-scan or emergent surgical intervention (i.e. laparotomy). Training with learning objectives and the duration as well as supervision should be standardized with the help of existing scientific principles. FAST demonstrates low to moderate sensitivity and high specificity as a single examination. There have been no studies that examined the utility of serial FAST examination. This is dependent on several factors such as, the time elapsed since trauma, type and extent of injury, patient group (i.e. age, BMI), quality of ultrasound machine, and skills of the FAST examiner. It was also mentioned previously that FAST results are also made on the assumption that fluid tracks to the most gravity dependant parts of the abdomen, and can be influenced by anatomy, location of bleed, respiratory physiology, intra-abdominal adhesions etc. However, it was seen in many studies that many patients who tested negative on FAST did have intra-abdominal injuries subsequently detected on CT or intra-operatively.
To improve sensitivity, the three standard abdominal FAST views should be supplemented by six further sections: sub diaphragmatic, caudal liver margin, parabolic groove, between intestinal loops, retroperitoneal and right upper abdomen view for the detection of free air. The examination should also include visualisation of solid organs such as spleen, liver, and kidneys to assess for injury. Serial exams can also be done at 12hourly intervals to reduce the likelihood of false negatives and reconfirm earlier findings. The effectiveness of serial FAST examinations in patients of deteriorating clinical status was demonstrated in a study that showed a 50% decrease in false-negative rates by 50% and an 85% increase in sensitivity for free fluid detection. The sensitivity and NPV for injury detection increased to 71% and 97%, respectively [42]. These aforementioned strategies can be investigated further through the conducting of randomized controlled trials. Diagnostic errors owing to human error can also be reduced through a more systematic approach such a diagnostic checklist, or management of physician fatigue. Albanese et al. also believed that serial physical examinations are the gold standard for diagnosing GI perforation from blunt abdominal trauma [43].
FAST does offer greater insight than solely relying on clinical signs but it is unsuitable to obtain a diagnosis with sufficient certainty nor can a negative result safely exclude intra-abdominal injury? Possible reasons for poorer accuracy could be that it was in the early post-injury phase, where sufficient hemoperitoneum had not yet accumulated thus leading to false-negative results. FAST has also shown poor sensitivity to identify hollow viscos or solid organ injuries not associated with hemoperitoneum such as early bowel injury or pancreatic injury and limited utility in detecting retroperitoneal haemorrhage. Other potential sources of error include obesity and subcutaneous fat, body habitus and positioning, ascites due to pre-existing medical condition, pre-existing pericardial effusion, and the presence of intra-abdominal cysts or masses [44]. Patients with these characteristics should be evaluated with a subsequent CT-scan if hemodynamically stable.
A comparative study [45] evaluating the use of FAST was done on 706 patients with blunt abdominal trauma. 460 patients were managed with FAST and 246 without FAST. Respectively, both groups showed similar accuracies at 99.1% and 98.0% respectively, and frequency of laparotomies at 13.5% and 14.2%. FAST patients also had a lower mean diagnostic cost and lower mean time required for diagnostic work up. In the FAST group, the computed tomographic rate was 24%, whereas it was 91% in the no-FAST group. As previously established, it’s been shown in many studies that FAST greatly reduced the need for CT-scans, a recent review quoting rates as high as 50%. Although there are surprisingly no significant differences in mortality or laparotomy rates. These two studies show that FAST is cheaper, fast, decreases the length of hospital stay, duration to definitive treatment, and use of healthcare resources [6]. However, it does not actually improve accuracies nor change the management or treatment outcomes of BAT.
Nevertheless, it is shown that peritoneal fluid if present, is highly sensitive to intra-abdominal injury, specifically active haemorrhage which is an indication for emergent laparotomy. This can not only save crucial time in achieving haemostasis instead of waiting for the results of the CT-scan, but is more accurate than DPL which is invasive, or simply clinical signs alone. Moreover, E-FAST is far superior to chest X-ray in terms of detecting haemothorax and pneumothorax and is the only simple bedside method for detecting hemopericardium. Thus, the purpose of E-FAST is for rapid assessment of intra-abdominal that require immediate surgical intervention, especially if the patient is hypotensive, and/or to evaluate the need for a CT-scan. FAST should not replace the abdominal examination or history taking nor be the sole modality replacing CT, for evaluation of abdominal trauma, particularly in patients with abdominal pain, contusions or altered mental status as it’s been shown to intra-abdominal injury can be present even without peritoneal fluid. While CT should not replace FAST either as the 1st line imaging modalities in BAT, a high index of suspicion and low threshold is required. Also, FAST does reduce the frequency of need for CT-scans in the ED and hence the overall costs and radiation exposure to the patient, along with more efficient use of hospital resources. If a new diagnostic algorithm is faster and less expensive it must also be as safe and accurate as the conventional diagnostic algorithm before it can become the new standard of care. Given the current level of evidence we have today, we can conclude that CT should still remain the gold standard for definitive evaluation of blunt abdominal trauma and guide its subsequent management.
Although CT does have greater diagnostic accuracy compared to FAST and is still the gold standard for definitive abdominal trauma imaging, there are little studies done to evaluate the outcomes of patients who have had a CT-scan done without E-FAST. It is established that CT-scan does carry significantly greater number of risks compared to FAST, including requiring more time which the hypotensive patient may not be able to afford. CEUS FAST has showed higher accuracies than conventional FAST in detecting liver, spleen, or kidney injury and active bleeding, similar to that of CT in children and adults with BAT. However, larger randomized trials to evaluated diagnostic accuracy and outcomes will be required to further validate its clinical use as the standard of care [19]. Assuming that major blunt abdominal or multiple trauma is associated with 15% mortality and a CT‐based diagnostic work‐up is considered the current standard of care, 874, 3495, or 21,838 patients are needed per intervention group to demonstrate non‐inferiority of FAST to CT‐based algorithms with non‐inferiority margins of 5%, 2.5%, and 1%, power of 90%, and a type‐I error alpha of 5% [6].
However, studies have shown that despite steady improvement of sonographic resolution properties over the past 20 years, diagnostic precision has not significantly improved, which may suggest that ultrasonography in the emergent setting and the experienced gain may have already reached its limit [22]. Technological advances have allowed recent development of wireless probes [46] and devices capable of short- and long-distance image transmission to remote displays. As ultrasound technology continues to evolve, we expect to see further miniaturization, better image quality and even holography or wearable technology [47]. The FAST exam is easily learned and educational materials are abundant both online (images and video) and in print. As both FAST and E-FAST increase in popularity, implementation of robust educational programs will become increasingly important so that future generations of practitioners are able to acquire high quality sonographic images, interpret those images, and also make real-time clinical decisions based on that information. Trauma centres can look into optimizing infrastructure and trauma protocols to shorten the time required for CT-scan, which has been reported in some studies to be as quick as only a few minutes. It is also crucial to emphasize integration of various sources of information and not to rely solely on a single modality.
Conclusion
FAST is an essential tool for preliminary assessment of intra-abdominal injury, including BAT. A FAST result if positive, in highly confirmative of intra-abdominal injury, for which emergent surgical management is indicated. However, a negative FAST cannot with sufficient diagnostic confidence, rule out intra-abdominal injury. The results of FAST should be considered in conjunction with clinical signs and relevant patient information. Patients with a negative FAST result should continue to be observed clinically, evaluated with serial FAST examinations or CT-scan should intra-abdominal injury be suspected. Developing technologies in Ultrasonography yield promising improvements to the FAST examination but current literature offers no evidence that FAST should replace CT as the diagnostic standard for BAT or its ability to definitively determine the necessity of immediate surgical management.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-ra-id-00152/ https://ijclinmedcasereports.com/pdf/IJCMCR-RA-00152.pdf
#Focused Assessment for Sonography#FAST#E-FAST#Ultrasonography#Point Of Care Ultrasound#Pocus#Blunt Abdominal Trauma#Laparotomy and CT#Lateef F*#IJCMCR#clinical studies
0 notes
Text
Localization and a Typical Aspect of the Chondromyxoid Fibroma in a Child by Echcikhi M*

Abstract
The chondromyxoid tumor is a primitive benign tumor of cartilaginous differentiation. We report the case of a 10-year-old child presenting with an aggressive form of the tumor that mimics a malignant process, atypical localization at the iliac axis.
Keywords: Fibromy Chondromyxoid; Child; IRM
Introduction
The chondromyxoid tumor is a benign benign tumor, presenting 0.5% of primitive tumors. She is generally interested in the metaphysics of the lungs. The objective of our article is to illustrate an aggressive form of this tumor, atypical localization in a child, highlighting the role of the IRM in its taking charge.
Case Report
Child of 10 years, consulted at the emergency room of the Rabat Children's Hospital for a prolonged and painful tumult of the right iliac fossa, rapidly increasing in volume. The biological balance was normal. The radiography objective showed a mixed lithic and condensing lesion, heterogeneous, of the right iliac artery, inciting the realization of an IRM. The IRM has objectiveed a legal process centered on the right iliac axis (Figure 1), multi-locale, in hyposignal T1, hyerignal heterogeneous T2, reproducing multiple septa stages in hyposignal T2 enhanced by Gadolinium, without restriction in diffusion. It is associated with a compact reaction with respect, without overriding adjacent structures. Absence of infiltration of fat or associated adenopathies. The process was in favor of a more benign origin than a chondrosarcome. The chondromyxoid fibroma was among the evacuated diagnostics, and was histologically confirmed. The surgical excision was indicated. A tumor recurrence was objective by a follow-up IRM after 5 months. It should be noted that tumor recurrence is more voluminous than primitive tumor (Figure 1 d).
(a) After (b) Gadolinium injection, and in sequential T2 in sagittal cup before (c) 5 months after a surgical resection (d) The images show a tumor process centered on the right, multi-locus iliac axis, in hyposignal T1 (a), enhanced by Gadolinium (b). The tumor shows a heterogeneous T2 hyersignal, confirming multiple septa steps in hyposignal T2 (c). It is a compact periodic response with regard to, without overheating of adjunct organs.
Discussion
Chondromyxoid fibrosis generally affects young subjects and manifests itself clinically through pain and tumors. Pathological fractures are common [1]. On standard radiography, at the level of the lungs, one finds an eccentric geographical gap, soufflant the cortical. On the sites where the iliacs are, the tumor is often polycyclic and mixed, associated with a condensation and a bright osseuse. Intra-tumor microcalcifications may be encountered [2]. The IRM is the key exam that can evoke the diagnosis of chondromyxoid fibroma. The myxoid component appears in hyposignal T1, hypersignal T2, and is enhanced by Gadolinium. The IRM also allows the detection of other associated intratumoral components: fibrous, cystic and calcareous [3,4]. Chondromyxoid fibroma is characterized by the absence of intra-medial extension, which allows to differentiate its aggressive form of a chondrosarcoma, the latter being the differential diagnostic principal. In the interest of a meticulous analysis of tumor reports in IRM. Histological confirmation after a biopsy is always indicated [3,4]. The treatment consists of a complete tumor excision with curettage and joint osseux. Note that total resection is not always possible given the frequency of relapses that occur in 25% of cases. The malignant tumor transformation is exceptional [1,2].
Conclusion
The imagery and in particular the IRM play multiple and fundamental roles in taking charge of the chondromyxoid fibroma. The IRM offers a diagnostic orientation, in particular in the case of atypical localization, a precise study of tumor reports guiding surgical treatment, as well as the search for a recurrent postoperative operation.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-cr-id-00151/ https://ijclinmedcasereports.com/pdf/IJCMCR-CR-00151.pdf
0 notes
Text
Comparison of Oocyte Maturity Rates in Recombinant Human Chorionic Gonadotrophin (HCG) and Triptorelin Acetate Triggers; A Prospective Randomised Study by Senthil P*

Abstract
LH like exposure in the mid cycle for inducing the oocyte maturation, is the very crucial step in the success of ICSI treatment. Introduction of LH surge endogenously by GnRH-agonist for final oocyte maturation induction, may be more physiological compared with the administration of HCG. Since GnRH agonist would induce FSH surge also along with LH surge, as happens in natural cycle. However, the effects of giving HCG trigger for inducing only LH surge and giving GnRH agonist trigger for inducing both LH and FSH surge, in patients treated for ICSI with GnRHantagonists need more research. Sub fertile patients planned for ICSI, meeting the requirement of inclusion criteria, were started with recombinant FSH from day 2 of menstrual cycle. GnRH antagonists were started from day 6 of stimulation. FSH dose was adjusted according to the individual response. Trigger was planned when the lead follicle reaches 24 mm. For triggering, 100 patients were randomised to receive Recombinant HCG trigger and Triptorelin acetate trigger. Oocyte retrieval was done 36 hours after Recombinant hCG Trigger and 35 hours after Triptorelin acetate trigger. The oocyte maturity rate was assessed by the number of metaphase II oocytes retrieved.
Keywords: Gnrh Agonist Trigger; Gnrh Antagonist Cycle; Metaphase 2 Oocytes; Oocyte Maturation Rate; Recombinant Hcg Trigger; Triptorelin Acetate Trigger
Introduction
Infertility is the fifth most serious global disability as recognized by the World Health Organization (WHO) and it affects one out of every 6 couples worldwide (WHO 2017) Mahmoud Fathalla, the former Director of the WHO Human Reproductive Program quoted “If public health policies encourage couples to delay and plan pregnancies, then it is equally important that they are assisted in their attempts to conceive in the more limited time available” (Mahmoud Fathalla). Controlled ovarian hyper stimulation, which is a supra physiological process simulating physiological processes that occur during the normal menstrual cycle, like development of follicles, maturation of oocytes. Follicle stimulating Hormone (FSH) and / or Leutinising Hormone (LH) are started from Day 2 of menstrual cycle to induce the growth of ovarian follicles. Premature LH surge can occur as follicles grow which could lead to premature ovulation. It can be prevented by the use of a GnRH antagonist in the present cycle (Shobam Z et al, Voronina E et al), or continuous administration of a GnRH agonist (GnRHa) to down regulate the GnRH receptor started from the previous cycle (Cheung LP et al). When the follicles reach the optimal size, LH exposure is provided to simulate the mid-cycle LH surge, which induces oocyte maturation and thereby subsequent ovulation (Huirneet al). This oocyte retrieval is properly timed following provision of LH exposure to retrieve oocytes. LH exposure initiates the resumption of meiosis and the maturation of the oocyte from the immature “metaphase I” stage to the mature “metaphase II” stage of Oocyte development (Olivennes F et al). During this process of oocyte maturation, the first polar body is extruded such that a diploid cell transitions toward a haploid gamete and attains competence for fertilization by a spermatozoon (Olivenneset al).
Materials and Method
Aim: To compare the efficacy of recombinant HCG trigger and Triptorelin acetate trigger in GnRH Antagonist, controlled ovarian hyper stimulation cycle.
Study Population: 100 patients totally, 50 patients in recombinant HCG trigger group and Triptorelin acetate trigger Group.
Inclusion Criteria: Sub fertile patients aged 21-35 years, with body mass index of 18 to 30, AMH 1.5 to 4 ng/dl, antral follicular count of 8-24 in both ovaries together and serum estradiol value of 3000 to 5000 pg/mL are included in the study.
Exclusion Criteria: Sub fertile patients aged more than 35 years with body mass index less 18 and more than 30, anti mullerian hormone level less than 1.5 ng/dL and more than 4 ng/dL and antral follicular count less than 8 and more than 24 in both ovaries together were excluded from the study. And patients with previous IVF failure, H/O chemotherapy were also excluded from the study.
Monitoring: Controlled ovarian hyper stimulation with recombinant FSH was started from day 2 or day 3 of cycle after confirming the pituitary down regulation, ie. serum estradiol level less than 50 pg/mL, serum progesterone level less than 0.9 ng/mL, serum Leutinising hormone level less than 5 IU/L, Endometrial thickness less than 5 mm, No antral follicle larger than 10 mm in each ovary. Starting dose of Recombinant FSH was based on patient’s age, body mass index BMI, antral follicular count and serum anti mullerian hormone level. InjCetrorelix 0.25 mg was started subcutaneously from Day 6 of cycle. Follicular growth was assessed by serial transvaginal and serum E2, LH and P4 levels, and Recombinant FSH doses were adjusted accordingly. Ultrasound monitoring of follicular growth was done on day6, day8, day10 and then daily till trigger .Serum estrogen was measured on day6, day 8 and day10 and on the day of trigger. Serum LH was measured on day6, day8 and day10. And Injcetrorelix was continued till the day of the trigger.Trigger was planned when the lead follicle size reached 24 mm. For ovulation trigger, the patients with serum estradiol level between 3001-5000 pg/dL were randomly divided into two groups: one group received recombinant HCG 250 mg subcutaneously and the other group received Triptorelin acetate 0.2 mg, a GnRH Agonist subcutaneously as ovulation trigger. Both groups were randomised by a standardrandomisation software by the computer. And serum progesterone level was measured 24 hours after the trigger.
Oocyte retrieval was done 36 hours of Recombinant HCG Trigger and 35 hours after Triptorelin acetate trigger. Oocyte cumulus complexes were cultured in a medium containing hyaluronidase for 1-2 hours. Oocytes were separated from the cumulus complex and the maturity of the oocytes was assessed and graded as “Metaphase 2” oocytes when the Oocyte has visible polar body and “Metaphase 1” when there was no visible Polar body and no germinal vesicle in the ooplasm and “Germinal vesicle” when the germinal vesicle was seen.( Figure 1.1, 1.2, 1.3)
Result and Analysis
The groups were analysed by age, body mass index (BMI), antral follicular count (AFC), anti mullerian hormone (AMH) level and serum estradiol value on the day of trigger.
In Recombinant HCG trigger group 7 patients were 21-25 years, 17 patients were 26-30 years and 27 patients were 31 to 35 years. And in Triptorelin acetate trigger group 9 patients were 21-25 years 24 patients were 26-30 years and 20 patients were 31-35 years. The mean value was 30.24+|- 3.23 in the Recombinant HCG trigger group and 29.17 +|- 3.15 in the Triptorelin acetate trigger group. The P value was 0.0858. Mentioned below in Table 1.
The AMH value in the Recombinant HCG trigger group, 25 patients had AMH 1.6-2 ng/ml, 16 patients had 2.1-2.5 ng/ml, 5 patients had 2.6-3.0 ng/ml, 4 patients had 3.1-3.5 ng/ml and 2 patients had 3.5-4 ng/ ml. In the Triptorelin acetate trigger group, 9 patients had 1.6 to 2 ng/ ml, 6 patients had 2.1-2.5 ng/ml, 8 patients had 2.6 to 3.0 ng/ml 18 patients had 3.1 to 3.5 ng/ml and 13 patients had 3.6 to 4 ng/ml The mean value was 2.21+|- 0.60 in the Recombinant HCG trigger group and 3.02+|- 0.7in Triptorelin acetate trigger group. The P value was < 0.0001.
24 patients had Body mass Index (BMI) of less than 24 and 30 patients had BMI more than or equal to 25 and less than 30 in the Recombinant HCG Trigger group and 12 patients had BMI less than 24 and 41 patients had BMI more than 25 but less than 30 in the Triptorelin acetate trigger group. Mean value was 24.70 +|- 2.86 in Recombinant HCG trigger group and 26.52+|- 2.06 in the Triptorelin acetate trigger group. The P value was 0.0003.
32 patients had 8-15 antral follicular count AFC and 22 patients had 16-24 AFC in recombinant HCG group. And in the Triptorelin acetate trigger group 10 patients had AFC 8-15 and 43 patients had 16-24 AFC. The mean value was 15.20+|- 4.51 in the Recombinant HCG trigger group and 19.06+|- 4.44 in the Triptorelin acetate trigger group. The P value was <0.0001
30 patients had serum estradiol value 3001-3500 pg/mL, 21 patients had 3501-4000 pg/mL. 4
Patients had 4001 to 4500 pg/mL and No one had 4501-5000 pg/mL in the Recombinant HCG trigger group. And in the Triptorelin acetate trigger group 22 patients had 3001 -3500 pg/mL, 15 patients had 3501-4000 pg/mL, 7 patients had 4001-4500 pg/mL and 9 patients had 4501 -5000 pg/mL. The mean value was 3427.24 +|- 344.26 in the Recombinant HCG trigger group and 3773.02+|- 591.81 in the Triptorelin acetate trigger group. The P value was 0.0003.
Discussion
An adequate knowledge about the endocrine and temporal requirements for the maturation of oocytes enables the optimization of IVF protocols and the development of standards to induce oocyte maturation to improve both the safety and efficacy of IVF treatment.
Few studies showed similar or better Oocyte maturation , with the use of GnRH agonist trigger compared to hCG trigger (Humaidanet al 2013, Reddy et al 2014). Unlike hCG trigger, GnRH-a trigger stimulates FSH surge in addition to LH surge. FSH surge, in the mid-cycle, has a specific effect on oocyte maturation and leads to a further expansion of cumulus cells surrounding the oocyte and release of proteolyticenzymes involved in the process of ovulation (Richards et al). Lamb et al by adding a dose of FSH to the hCG trigger, showed better recovery of oocyte and higher fertilization rates in IVF compared with hCG trigger alone.
This method also enables more nuclear maturity and the resumption of meiosis and thereby increasing the number of Metaphase II oocytes (Anderson et al 1999). Shapiro et al showed that increased levels of LH following injection of hCG was slower than that following GnRH-a trigger (Shapiro et al)
The present prospective randomised study was done to compare the efficacy of GnRH agonist Triptorelin acetate 0.2 mg administered subcutaneously and recombinant HCG 250mg administered subcutaneously, for triggering final oocyte maturation in antagonist co-treated ICSI cycles. The results show that patients triggered with Triptorelin acetate had more yield of mature metaphase 2 oocytes than the patients triggered with Recombinant HCG. This may be due the fact that administration of GnRH agonist results in endogenous rise in both LH and FSH levels from the pituitary gland owing to initial flare effect similar to that of natural cycle (Gonenet al., 1990). Whereas recombinant HCG causes only LH rise. GnRH agonist also causes maturation of oocytes , meiosis reinitiation expansion of cumulus cells and thereby giving more number of mature oocytes (Andersen et al., 2006; Humaidanet al., 2011).
Conclusion
In conclusion both Triptorelin acetate and recombinant HCG triggers are effective for finaloocytematuration. Triptorelinacetate, may yield more number of mature metaphase II oocytes, than the recombinant HCG tigger. Nevertheless, more studies and researches might be needed to confirm our findings and improve our understanding.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-ra-id-00150/ https://ijclinmedcasereports.com/pdf/IJCMCR-RA-00150.pdf
#Gnrh Agonist Trigger#Gnrh Antagonist Cycle#Metaphase 2 Oocytes#Oocyte Maturation Rate#Recombinant Hcg Trigger#Triptorelin Acetate Trigger#Senthil P*#IJCMCR#clinical studies
0 notes
Text
The Effects of COVID-19 on Hypothalamus: Is it Another Face of SARS-CoV-2 That May Potentially Control the Level of COVID-19 Severity? by Noor-ul-Huda M*

Letter to Editor
As we are all combating the COVID-19 pandemic , a war being imposed by an invisible enemy, each day we need to “spy” the new moves by our enemy in order to design our own strategy. This metamorphic menace has ways to amaze us and to bluff us by presenting in unexpected ways. Since we have never suffered from this novel viral infection before, there is no data to correlate and guide us regarding the possible ways of presentation of this virus. It has pushed us back in teaching ourself the basic science based on observation, building new words from the alphabets we find, and playing Columbus to discover the new faces through which SARS-CoV-2 may manifest itself while looking for the hallmark set of signs and symptoms. The tendency of masquerading itself of the SARS-CoV-2 , a virus that ruined the famous Venetian Carnival as it unveiled itself , has put all the researchers into a mayhem.
Sir, I really want to bring into your kind notice that we have found some signs and symptoms that are related with the central nervous system particularly the hypothalamus. It came into our observation that many patients with COVID-19 infection have presented to us with polyuria and polydipsia with and without polydipsia.
In a short study, we detected at least 27 patients who suffered from “unquenchable thirst” and “ravenous appetite”. 7 of them were diabetic including 2 who were insulin dependent .Most of them did not develop severe COVID-19 . Polydipsia and polyphagia raise suspicion of hypothalamic infliction, since hypothalamus has centers of thirst, hunger and satiety [1]. The interplay between stimulation and inhibition leads to the normal hunger and thirst sensations. We further noted that 21 of them had other signs and symptoms related with peripheral nerves. They all suffered from dysosmia and dysgeusia as well. If we put all of these symptoms together and correlate it with the viral entry through the nose, it is quite simple to explain that SAS-CoV-2 affects the olfactory nerve and from there finds its way to the hypothalamus [2].
Addressing polyphagia and polydipsia separately, if we discuss polyphagia first in relation with hypothalamus , there can be various causes directly or indirectly related with the hunger and satiety centres in the hypothalamus. The most straight-forward mechanism of hunger and satiety is defined by the balance of signals coming from two hypothalamic centers: the lateral hypothalamus that responds to internal and external signals and cause one to feel hungry and the ventromedial hypothalamus that signals satiety. Secondly, polyphagia is It is also the part of the 3Ps of diabetes [3]. With an increasing experimental and clinical evidences showing hypothalamic dysregulation as one of the underlying mechanisms of abnormal glucose metabolism, it can be postulated that hypothalamic infliction is likely in SARS-CoV-2 that leads to polyphagia in both diabetic and non-diabetic patients as well as poor diabetic control in the diabetic patients. Koshiyama et al postulated several points to suggest the role of hypothalamus in causing diabetes mellitus noticeably an increased hypothalamic-pituitary-adrenal axis activity caused by extreme stress [4]. So a deranged hypothalamic function causing diabetic tendency and polyphagia can be one cause. Due to financial constraints, proper blood sugar level testing could not be performed in the non-diabetic patients, however, in the diabetic patients with COVID-19 it was evident that glucose control was poorer .The other important point regarding the causation of polyphagia is the direct effect on the hypothalamic centers for satiety. It is evident that mutations in several genes related with hypothalamic satiety signaling lead to polyphagia and the so called hypothalamic obesity [5]. This points towards a possibility of SARS-CoV-2 affecting hypothalamus not only directly but also via genetic mutations. In a study by Gu et al., neuronal histopathological changes were found in the hypothalamus who in the autopsies of 8 victims of SARS [6].
Nampootheri et al suggested SARS-CoV-2 invasion in the hypothalamus . Hypothalamus plays a key role in hypertension, diabetes, obesity and other risk factors for developing severe COVID-19 infection. They also suggested a non-respiratory system origin for respiratory failure. Hypothalamus being connected to brainstem cardio respiratory centers can cause respiratory arrest. They further showed that the human brain gene-expression analyses revealed that the hypothalamus with its associated regions express angiotensin-converting enzyme 2 and transmembrane proteinase, serine 2 which allows SARS-CoV-2 entry in the cell. They also showed that immunolabeling in human as well as in animal brains proves that the central role of the hypothalamus that by allowing SARS-CoV-2 brain invasion through multiple routes, influences brain susceptibility and various severe manifestation of the COVID-19 infections [7].
If we now discuss polydipsia then again we have various explanations via different causation pathways involving hypothalamus. The most straight forwards pathway is via Angiotens in II . Since SARS-CoV-2 also acts via the ACE2 receptors, somehow at any level whether central or peripheral , it is able to cause polydipsia[8]. Hypothalamus does have osmoreceptors that regulate thirst mechanisms.[9] So, basically, hypothathalamus plays a central role in thirst mechanism. Due to limited resources and an overwhelmed system, we were not able to follow any specific lab investigatory protocol. However, correlating with serum electrolytes and urine output records, none of them had either diabetes insipidus or dehydration. The only notable point was a poorer diabetic control during illness, but this can be from various different reasons, again hypothalamus does play a role in several of such mechanisms including blood sugar control.
Again, if we join all these pieces of information together, with patients presenting with polydipsia and polyphagia as well as signs involving olfactory nerve and other peripheral nerve signs and symptoms and provided the fact that SARS-CoV-2 does interact with the nervous pathways and it also interacts with ACE-II receptors, it is likely thatSARS-CoV-2 finds a way to the hypothalamus leading to the manifestations related with hypothalamic structures.
I believe there is a need to perform further research on this topic. This can be an important point to understand the level of severity of COVID-19 infection and may help in determining a proper management plan with monitoring as well as determining prognosis.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-le-id-00149/ https://ijclinmedcasereports.com/pdf/IJCMCR-LE-00149.pdf
0 notes
Text
On Invariant Speed of Light by Orlov S*

Abstract
A new physical model of the appearance of light, properties, and its trajectory. Explains the paradox of invariance and isotropy of light based on the laws of classical physics.
Keywords: Theory Ofvortex Gravitation; Cosmolog;Cosmogony; Aerodynamics
Introduction
For many years, scientists- physicists have tried to measure the speed of light. Galileo-in the seventeenth century. Early experiment to measure the speed of light was held Ole Roemer, a Danish physicist, in 1676. Another, more accurate way to measure the speed of light is made in Europe Hippolyte Fiziin 1849. Francois Arago determines the speed of light in 1838bya rotating mirror. In 1862, on the production of the speed of light worked Leon Foucault [1]. In 1926,a result of years of efforts Albert Michelsonhas had some very high accuracy of the speed of light:
с = 299 796 000±4 000 m/s
The main and paradoxical conclusion in the study was his invariance speed of light. In other words, the speed of light is the same in all inertial frames of reference is independent of the velocity of the observer and emitter. This surprising fact for the classical physics of his time for the first time proved the Michelson experiment: the independence of the speed of light on the direction (isotropic) and the orbital motion of the Earth around the sun. In the future, this paradox was confirmed by astronomers. In particular, Willem de Sitter in monitoring the spectral binaries found that the speed of light flux from removing the stars and approaches are constant speed of light (c) and equal to each other. That is, they do not depend on the rate of the star (light sources) [2]. From the point of view of classical physics this paradox so far can’t be explained. Therefore, on the basis of the unknown properties of light in 1905, Einstein proposed the special theory of relativity (STR) in the paper "On the Electrodynamics of Moving Bodies" [3]. SRT conclusions were as paradoxical as the invariance of light. On the basis of the SRT can assert that the events simultaneous in one inertial reference frame will not be simultaneous in another, if these frames of reference are moving relative to each other. In this article we propose to explain the origin, properties and the invariance of light, in full compliance with the classical laws of physics using the theory of vortex gravitation, cosmology and cosmogony [4].
Luminiferous Ether
In the theory of vortex gravitation, cosmology and cosmogony all celestial bodies (matter) are essential vortices. The values of the bodies (system of bodies)) and the corresponding vortices may vary to an infinite value. The biggest ethereal vortex that people can watch this universal whirl wind, the smallest atomic. The orbital speed of ether in each vortex increases towards the center of an inverse square law. Change of orbital velocity is inversely proportional to the pressure change in the air. Pressure gradient force creates vortex gravitation. This pattern works equally essential in a whirlwind of various volumes.
In theory, the vortex gravitation obtained an equation to determine the gravitational force in the etheric vortex [4]:
Depending on the next
Where
V - Volume of the nucleons in the body, which is in torsion
r = 8.85×10-12kg /m3 -the density of ether [5]
v(r) - Velocity of ether in the orbit
r - The radius of the orbit are risen the vortex
The same relationship between the force of gravity and orbital velocity exists in atomic torsion (vortex).
Each atomic vortex ether rotation occurs continuously around the core with a radius r, which creates the effect of an atomic attraction. For this scheme, gravity can explain the origin of the interatomic forces of attraction. In theory, the vortex gravitation made the condition that the ether penetrates all matter and the body other than atomic nuclei (nucleons). Maximum speed ether several orders of magnitude greater than the speed of light. The rotational speed and the pressure gradient of ether, and the attractive force Fn on the surface atoms reaches a maximum value.
Make a guess:
The assumption № 1. Under the action of attractive forces on the surface of the atom or on surface of nucleus of the atom or ether stream is converted into an electromagnetic flux including a light. The light has mass. Gravity act on the light. When converting the ether is the emergence into the light particles (photons) with a mass greater than the mass of the particles of the ether -Amer. Increasing the mass of the particles, according to the law of conservation of angular momentum of rotation, must be accompanied by a decrease inversely proportional to the orbital speed of light. Thus, the light gets its velocity- c.
When orbital revolution of the magnetic flux (light) around the atom to it are two forces: the force of the vortex atomic attraction and centrifugal force. For uniform orbital motion of light is needed to create its orbital speed centrifugal force equal to the force of an atomic attraction. This rate is equal to the atomic orbit well-known speed of light-(c). In aerodynamics this force is called the first space. The atomic attraction is generated bythe pressure gradient in the atomic vortex (uravn.4). The pressure gradient is the difference of pressure values in free ester stationary and the center of the vortex. In a free state, the pressure is always constant and maximum. In the center of the vortex ether pressure depends on the rotational speed and air temperature. Upon heating of a substance (atom), the pressure (P)atom in the center increases in proportion to the temperature (T),in accordance with the law of Charles (6): (2)
Then the pressure gradient must be reduced and, in accordance with equation(1) reduces the force of attraction of the vortex. In this case, there comes a predominance of centrifugal force Fc over the forces of atomic, vortex attraction Fn. The speed of light is converted into the second cosmic speed. Lightis removed from the atom at the most economical spiral trajectory according to calculations by Walter Hohmann [7]. At the same time near the surface of the atom (at the lowest atomic orbits), the place flown away luminous flux takes a new ether flow. This stream is the same principle is converted into light. If the external effects (heating) are stored, the conversion and emission light from the atom will continue permanently. This is the nature of light. Light is generated and emitted not by the energy or mass of matter (atoms), but only by making the ether in the light under the influence of the atomic vortex gravitation and external influences (temperature). Light emissions top only when the external action (heating) or destruction of the atom, and with it the atomic vortex.
Fig. 1 shows an aerodynamic scheme of movement of the light flux from a single atom. In the emission of light from the set of atoms aerodynamic design principle does not change, only multiplied many times. Light will always be supplied to each of the observer to any atom on the same helical path (at a large angle to the radius of the light field) with its constant velocity - v. Spiral light fluxes from these atoms can twist in different directions. The orbit planes of light fluxes arranged in space with any inclinations from each other. Thus, the light is almost infinite set of ultra-thin, light, spiral threads. These streams are combined into a single spherical light field. Radius and circumference of the light field in their values are directly proportional. Consequently, the light field radially increases with the same speed of light. If the viewer moves around the light source light over a circular orbital path, and in this case a considerable part of the light will make its spiral rotation along a plane perpendicular to the plane of movement of the observer. Consequently, this light will also enter the observer at a right angle with its constant velocity- v. Isotropy of light is also a consequence of the propagation of light streams through an infinite number of spiral trajectories.
Output: To put the speed of light (c) at the speed of any body (v) in space is possible only according to the laws of vector algebra. Relative movement of any other body in space, light always moves at a right angle. Therefore, the relative velocity of the entering light to any body will always be equal to the absolute speed of light, regardless of the speed of motion of the considered point (O) relative to the light source (S).
Mathematically this can be written: + = - =
Conclusions
The concept of the luminiferous ether was launched in the XVII century Rene Descartes. In the future, the wave theory, the luminiferous ether developed in the writings of Huygens. A detailed justification for this theory was in the XIX century in the framework of wave optics and electromagnetic theory of Maxwell. The proposed spiral model of light is very close to the concept of the wave motion of light and differs only in the trajectory of the light flux.
According to modern concepts light has a dual nature (wave-particle duality): - light has wave properties and is an electromagnetic wave, but is also the stream of particles-photons. It should be noted that until now scientists have not explored yet another important property of light: what is the mechanism and how can instantly disperse photons up to the maximum speed-c?!
Spiral model of the origin and movement of light, this problem is not difficult, because the momentum of the movement all the magnetic flux received from the ether, which at the outbreak of the world itself was moving at a speed exceeding the speed of light. Under Chapter 2 of this article can be argued that this is a consequence of the invariance of the light path of movement of the light flux. Researchers relative velocity of light in their calculations are not stacked vector velocities and their modules. The movement of the luminous flux is not contrary to the laws of classical physics. Invariance was introduced into scientific consideration only because of a misunderstanding of the movement of light as straight and radial.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-rw-id-00148/ https://ijclinmedcasereports.com/pdf/IJCMCR-RW-00148.pdf
1 note
·
View note
Text
Free Strand of the Greater Omentum in Surgical Practice and its Morphological Characteristics by Martynov Vladimir L

Abstract
In his operating work, the surgeon often uses the patient's tissue to solve practical problems. For our work, the data of Liebermann-Meffert D. and White H. (1989) on the greater omentum are of interest [1]. Research shows that the "policeman of the abdominal cavity" - the great omentum in pathological conditions, acquires very special properties: plasticity; the ability to adhere to an injured and inflamed surface; the ability to hemostasis; the ability for ingrowth and revascularization; the ability to absorb liquids and microparticles from the abdominal cavity; the ability to phagocytosis and immunological response. Adhesions with the omentum are formed much faster than with other organs of the abdominal cavity. Even the freely transplanted omentum tissue without blood supply retains these properties. After 21 days, the omentum tissue is completely fused with the recipient [2].
Introduction
Experimental studies of ingrowth of the omentum graft and its vessels are very indicative. Sections of the omentum of different thickness and size were separated from its bulk and fixed without revascularization to various organs and tissues of the same or another animal: stomach, small and large intestine, liver, spleen, kidney, urinary bladder, lung, pleura, peritoneum, mesentery, aorta, inferior vena cava. Within a week, the graft is firmly attached to the tissues of the recipient organs, its separation is difficult, due to a decrease in the amount of fat, its thickness is reduced, necrobiotic processes, necrosis zones are reduced. After three weeks, the graft cannot be separated, when an attempt is made, bleeding occurs, the amount of fat decreases and is replaced by dense fibro- and angioplastic tissues so that its surface resembles the surface of the recipient tissue. After 12 weeks, it is difficult to distinguish the omentum tissue from the recipient tissue; the suture line serves as a reference point. The engraftment of free grafts did not depend on their size, but necrosis zones are more often formed in thick grafts. The graft remains viable when frozen for two weeks or even longer. Stages of omentum transplant engraftment: attachment - up to 4 hours, beginning of vascular ingrowth - 24 hours, tight fit - 48 hours, revascularization - 3 days, fat resorption - 3 weeks, fibrous degeneration - 24 weeks [1].
These studies allowed us to use a strand of the free area of the greater omentum in the small intestine in 107 patients. Here is an example of the clinical use and preservation of the viability of the free strand of the greater omentum.
Case Report
A 25 years old, was admitted to the GBUZ NO "GKB No. 12" in Nizhny Novgorod on 11.11.2013 with a diagnosis of "Closed abdominal trauma". After dynamic observation, an emergency laparotomy was performed, during which a rupture of the pancreatic head was detected. Outflow of bile, pancreatic juice was not detected. A tampon was brought to the site of damage to the gland through a separate incision in the right lumbar region. The drains were placed in the right lateral canal, in the omental bursa, in the small pelvis. On 20.11.2013, the intake of contents up to 3 liters with an admixture of bile was noted. On an urgent basis, relaparotomy was performed, during which two perforations were revealed on the posterior wall of the vertical part of the 12-PC, each with a diameter of up to 7 mm, from which, after the introduction of methylene blue, a blue discharge began to flow into the stomach. After excision of the edges of the perforations, the latter are sutured with interrupted single-row sutures. The seam line is reinforced with a large gland strand. A drainage-foam rubber system for active aspiration is connected to this zone through the opening of the right lumbar region (the place of the gauze pad). A loop of the jejunum was isolated 30 cm from the Treitz ligament, on which an areflux nutritional jejunostoma was formed with an interintestinal anastomosis according to Brown and a "plug" on the leading loop 1 cm below the anastomosis. The stoma was placed in the left mesogastric region. A feeding tube was inserted 25 cm behind the anastomosis line.
On January 20, 2014, the patient was admitted to the Nizhny Novgorod City Clinical Hospital No. 12 for the second stage of treatment - closing the nutritional jejunostomy. The skin around the stoma is intact. Performed fistuloenterography through a probe introduced into the leading section of the stoma to the "plug". The contrast does not pass through the "plug" zone, which confirms its areflux function.
01/23/2014 under general anesthesia in the left mesogastric region with two bordering incisions around the stoma, the latter was isolated from the tissues of the anterior abdominal wall. The segment of the intestine with the stoma is brought out to the anterior abdominal wall. The area of the free omentum with the ligature, which acts as a "plug", is viable, loosely welded to the jejunum. The interintestinal anastomosis is passable. Near the anastomosis, the sections of the intestine were stitched with the UO apparatus. The section of the intestine bearing the stoma was resected. The intestinal stumps were additionally sutured with two semi-lace sutures each. Layered suture of the wound of the anterior abdominal wall. Preparation: a section of the jejunum up to 10 cm long with a stoma and a free section of the greater omentum - “plugs”. The area of the free omentum with a ligature, which acts as a "plug", was loosely welded to the jejunum (Fig. 3). The mucous membrane of the jejunum of the "plug" formation zone is not visually changed (Fig. 4). The interintestinal anastomosis is passable.
Morphological examination of the "plug" zone at 3, 6, 9, 12 hours of the intestinal wall circumference showed only edema, moderate lymphohistiocytic infiltration, moderate circulatory disorders [3].
The wound healed by primary intention. In satisfactory condition 02/03/2013 was discharged for outpatient observation by a surgeon.
Conclusion
Thus, our observation confirms the possibility of using a strand of "free", devascularized omentum as a plastic material in small bowel surgery.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-cr-id-00147/ https://ijclinmedcasereports.com/pdf/IJCMCR-CR-00147.pdf
0 notes
Text
A Modified Supine Positioning Setup for Diabetic Foot Reconstruction with Peroneal Artery Perforator Based Propeller Flap: Technique Tips and Tricks by Xiangxia L*

Abstract
Most posterior hind-foot and ankle surgery is traditionally setup in a prone position for better access during the surgery. When using the peroneal artery perforator based propeller flap to reconstruct the complex wound of a diabetic foot, the best approach to dissect the perforator vessels is from anterior aspect when the patient lays on supine with leg rotated internally, obviously this position put a lot of stress on the surgeons to get the access of the heel, vice versa. Furthermore, in some cases the co-morbidity of the patient may limit the patient from lying on prone for a long hour surgery under general anesthesia for safety reasons. In this article we present a 54 years old male complex wound case of diabetic foot with skin necrosis in heel and medial ankle area (Figure 1), which was reconstructed with peroneal artery perforator based propeller flap. The purpose of this paper is to describe in detail of an innovative and modified supine positioning during the surgery, which facilitated both the harvest of flap and reconstruction of the heel and ankle procedure.
Keywords: Surgical Positioning; Diabetic Foot; Propeller Flap; Reconstruction; Level of Evidence: Level V; Expert Opinion.
Techniques
The patient is placed in traditional supine position and bilateral upper extremities are tugged on the sides of the body with intravenous access on the right hand contralateral to the left foot to be operated on. All the potential pressure points are protected. The whole left lower extremity is prepped and draped. A sterile pneumatic thigh tourniquet is applied. A self-invented C shaped abdominal retractor (Figure 2), which is widely used in abdominal surgery, is applied with the curve pointing caudally (Figure 3a). The left lower extremity can be placed on the surgical table while the surgeons are dissecting the perforator vessels or placed on the bar of C shaped abdominal retractor with appropriate padding while the surgeons need to access the heel and posterior aspect of the lower leg to harvest and inset the flap (Figure 3b and c). After the flap is harvest, the tourniquet is released and the split-thickness skin graft is harvested from the upper thigh by Zimmer® dermatome. With the support of retractor, surgeons are able to change the lower leg position easily and maintain the position to get access of the heel and posterior aspect of lower leg. The defects are successfully covered by the propeller flap based on a single perforator of peroneal vessels (Figure 4).
Figure 2: The setup of C shape retractor during the abdominal surgery on lateral view.
Figure 3: The setup of C shape retractor during the heel reconstruction surgery.
Figure 3a: Initial setup of C shape retractor with lower extremity on the table.
Figure 3b and 3c: The lateral and bottom view when the lower extremity is placed on the C bar with cushion underneath.
Discussion
It is estimated that 12 percent of diabetic patients could develop foot ulceration during their lifetime.5For complex wounds with bone and/or tendon exposure in patients with multiple co-morbidities, the selection of reconstructive options was limited. More and more studies supported the peroneal/posterior tibial/anterior tibial artery perforator based flaps as a powerful tool in diabetic patients with compromised lower leg circulation.3,4Appropriate surgical position is crucial for both the safety of the patients and the efficiency of the procedure.1,2,8,9,11The best position for posterior hind-foot and ankle procedure is prone.12While in diabetic foot reconstruction, there are a significantly large percentage of patient having multiple co-morbidity diseases, by putting them on prone position for a long hour’s surgery may jeopardize the patients’ safety.6The anterior approach is a safe and fast track to dissect the peroneal artery perforator vessels, which means the patient would lay on supine position with lower leg internally rotated. Unfortunately, a traditional supine position is a nightmare for the posterior hind-foot and ankle procedures because surgeons may only have limited access to the surgical field, oftentimes the lower extremity must be raised and held consistently by an assistant. In some scenario this position dilemma may be solved by lateral decubitus position, but it is inapplicable in our patient because he had a wound on the medial malleolus area needs to be covered at the same time. Lower leg Mayo stand pad may help the surgeons to access the heel and ankle, and keep the anterior approach for the perforator vessels dissection, while there is no access for flap harvest and skin grafting.7,10 Our circulation nurses come up with an innovative idea of using the abdominal retractor to support the lower leg while keeping the supine position (Figure 3).
Figure 4: The postoperative picture of medial aspect and posterior aspect of the foot.
This abdominal retractor was invented by Dr. Liang Lijian from the Division of Hepatic Surgery in our hospital and widely applied in abdominal surgery (Figure 2). With the support by the retractor’s C shape bar, we are able to access both anterior and posterior of the lower leg. Also it is convenient to switch the position during the surgery and there is minimal impact on the skin harvesting procedure on the thigh. This position could be one of the best solutions for our patient who could not tolerate general anesthesia and prone position. Furthermore we are thinking of making a customized supportive device to accomplish the idea and provide more convenient surgical position for this type of procedure. With the possible help for the device, surgeons will be able to place the patient in supine position and perform the posterior hind-foot and ankle procedure without any struggle.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest in respect to the research, authorship, and publication of this article.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-cr-id-00146/ https://ijclinmedcasereports.com/pdf/IJCMCR-CR-00146.pdf
#Surgical Positioning#Diabetic Foot#Propeller Flap#Level of Evidence#Level V;#Expert Opinion#Xiangxia L*#IJCMCR#clinical studies
0 notes
Text
Semicircular Canal Fistulas and Hearing Loss. Single Surgeon’s Experience by Stefano Dallari*

Abstract
Fistulas of the lateral semicircular canal may occur mainly in cholesteatoma cases, both as consequence of the disease and an excessive or inadvertent drilling of the bone. The risk of significant hearing loss had been stressed, especially in the past. More recent experiences have shown that a careful approach allows to save the pre-operative hearing in the majority of the cases, even when the cholesteatoma matrix is removed from the fistula and the canal is plugged. The author presents his experience in 22 cases collected since year 1989.
Keywords: Labyrinthine Fistula; Hearing Loss; Cholesteatoma
Introduction
Fistulas of the semicircular canals may be primitive or follow an erosive process of the endochondral bone of the labyrinth. A type of primitive/malformation fistula involves the superior canal and may show up as Minor's Syndrome [1]. Also, the posterior semicircular canal may be involved, in rare cases associated with a high-riding jugular bulb and fibrous dysplasia [2]. Secondary fistulas generally follow a middle ear infection, most of the cases a cholesteatoma [3].
An iatrogenic origin should also be taken into account, as a consequence of an excessive drilling during a middle ear surgical procedure [4]. Because of its anatomical location, the lateral semicircular canal is normally involved. As reported in the literature, a fistula of the semicircular canal brings a variable, often high risk of hearing loss until anacusis, due to the damage to the membranous labyrinth [5]. The crucial point is the injury to the endosteum of the canal, while its blue lining is considered safe. When dealing with fistulas due to a bony erosion caused by a cholesteatoma, removal of the matrix may lead to open the endosteum. This is why, especially in the past, for fistulas of more than 2 mm, leaving a piece of matrix in place, over the fistula, used to be advised [6]. It had also been demonstrated that, at a second look operation, most of the time this piece of matrix disappears into normal mucosa.
Conversely, in the more recent literature there have been several suggestions for a careful but complete removal of the matrix, with immediate coverage of the fistula with autologous tissue, even until the obliteration of the canal itself [7,8,9].
The Author’s attitude has always been a careful removal of the pathology and, in regards to the matrix, the decision of completely removing it or leaving a piece over the fistula was based upon the size of the fistula but also the easiness of detaching the matrix from the endosteum. When the detachment seemed to be too difficult, a piece of matrix and/or inflammatory mucosa was left over the fistula itself. The Author’s series was revised mainly in the light of the audiologic outcome and the results will be hereby reported.
Materials and Methods
From 1989 up to December 2019 the Author performed 111 tympanoplasties (TPLs) for cholesteatoma (65 males and 46 females), 39 TPLs for other diseases (28 males and 11 females) and 8 “radical” operations (4 males and 4 females). In 22 cases (15 males and 7 females), a fistula of the lateral semicircular canal was detected (18 cases) or provoked (4 iatrogenic cases). In Table I all these 22 cases are described. Several items have been taken into account: sex, age at operation, ear pathology, year of surgery, pre-operative imaging availability, state of the facial nerve (covered, exposed, pre-operative presence of palsy), state of the semicircular canal, in accordance with the classification of Dornhoffer and Milewski [10], simplified (simple bone erosion with presence of a “blue line”, type I; bony fistula with endosteum exposed and closed, type II or open, type III), type of operation performed, pre-operative hearing (air conduction between 500 and 4000 Hz), post-operative hearing (air conduction between 500 and 4000 Hz) and post-operative bone conduction (0.5,1,2,4 kHz) as compared with the pre-operative one.
Results
The results will be hereby globally analyzed. Furthermore, six cases will be reported and documented, to illustrate the various scenarios. The series consists of 22 patients, 15 males (mean age 52 years) and 7 females (mean age 46 years).
Over the whole number of cases, the incidence of fistula is 14 % (22/158). All the cases but one had a middle ear cholesteatoma. The sole non-cholesteatoma case was an iatrogenic one. Thus, the percentage among the cholesteatoma cases is 21/111 (19 %). In 11/22 patients a pre-operative CT had been performed. In all cases but one (case n. 3 of the year 1991), where a complete fistula was present, with endosteum exposed, the exam was positive for fistula. For the three cases with bony erosion (blue-lined canal) caused by the pathology, imaging was not available. In the iatrogenic cases the CT was negative. In regards to the facial nerve, it was exposed in 13/22 cases and closed in the remaining 9/22. In all the four cases where the endosteum was open, the facial nerve was exposed. None of the cases had a pre-operative palsy, neither post-operative. The case n. 22 presented with a facial palsy grade V which was confirmed not to be due to the pathology (adenoma of the middle ear), but to be incidental. The palsy completely recovered after three months.
Coming to the conditions of the semicircular canal, in 4/22 cases (18 %) there was a complete fistula with the endosteum open. The presence of the matrix of the cholesteatoma onto the canal was mentioned in only one of these four cases (case n. 18), where it was removed, in presence of an open endosteum (see description of the case). In 9/22 cases (41 %) the endosteum was exposed, closed. For these cases the operation report did not mention if the fistula was covered by the matrix of the cholesteatoma. Conversely, the presence of the matrix over the canal was reported in further 5/22 cases besides the case n. 18 (see before), for a percentage of 27 % (6/22). It was removed in 3/6 cases, leaving an intact endosteum in two cases and an open one in the case n. 18, and left in situ in 3/5 cases. Finally, in 3 cases (n. 8, 9 and 16), there was a simple erosion of the bone with a blue-lined canal. The ”iatrogenic cases” are 4/22 (18 %): the n. 12 (endosteum exposed, closed, due to excessive drilling); the n. 14 (bone erosion due to the curette-removal of hyperostotic bone over the lateral semicircular canal); the n. 19 (endosteum exposed, closed, due to excessive drilling); the n. 22 (bony fistula with endosteum intact, due to delayed anatomical recognition).
In 14/22 cases (64 %) an open TPL was performed, while a closed TPL was carried out in 5/22 cases (23 %). In the remaining 3/22 cases (14 %) the fistula was detected during a revision of closed TPL which was converted to an open one. Post-operative audiologic data were available for 14/22 patients. Among Figure 1: Case n. 15. The left lateral semicircular canal is absent in his superomedial aspect. The endosteum is exposed and open. A piece of absorbable gelatin is ready to seal the hole. The facial nerve is exposed. these 14 patients there were 3 of the four patients with a fistula with open endosteum. None of them had a worsening of the bone conduction. Only in 1/14 patients with post-operative hearing data, there was a deterioration of the bone conduction curve. It was the case n. 12, iatrogenic, with endosteum exposed, closed. Furthermore, the author does not remember a case of total hearing loss in this group of patients.
(a): Iatrogenic maneuver (b): The patient was operated on, twelve month later, for the II stage. The zone of the fistula appeared close with neo-bone (c): Iatrogenic maneuver (d): Iatrogenic maneuver (e): The patient had been operated on for closed TPL I stage in 2013, for intact TM cholesteatoma. At that time the facial nerve was closed and no lateral scc erosion was present (f): The patient presented with a right facial paralysis grade V, not related to the ear pathology. He completely recovered three months after the operation (g): Iatrogenic maneuver
Clinical Cases
Case n. 15 (Fig. 1) R.M, male, 69-year-old. Long history of left hearing loss. In September 2005 he suffered for an acute episode of vertigo. The ENT workout confirmed a significant left mixed hearing loss. The CT of the ear showed an opacification of the whole middle ear with erosion of the lateral semicircular canal. He underwent surgery in November 2005 and a huge bony fistula, with endosteum open, was confirmed. The facial nerve was exposed in the tympanic segment and covered by the cholesteatoma matrix. An open TPL was performed and the fistula was cleaned and then repaired with absorbable gelatin+ bone+ fascia. The operation was uneventful, with no vertigo and the 48-hour post-operative bone conduction curve was unchanged. The patient recovered well and was lost to follow-up. Information acquired for this paper says that the patient is still alive and his ear situation is stable with no further problems.
Case n. 17 (Fig. 2) G.G., male, 62-year-old. History of left hearing loss. Before referring to us, in the beginning of year 2008, he suffered for recurrent episodes of peripheral vertigo. A CT showed a diffuse involvement of the left middle ear with a probable fistula of the lateral semicircular canal. There was a significant mixed left hearing loss. The patient underwent surgery in April 2008. An erosion of the bony semicircular canal was confirmed. It was covered by the matrix of the cholesteatoma, which covered also the facial nerve, exposed along the whole tympanic segment and second genu. An open TPL was performed, leaving a piece of the cholesteatoma matrix/inflammatory mucosa onto the fistula. The post-operative evolution was good. No worsening of the bone conduction occurred. The patient has been recalled in the occasion of this paper. Under otomicroscopic examination a well done and healthy open TPL cavity was evident, with adequately-sized meatoplasty. There was a mixed hearing loss with the air conduction significantly better than after the operation, while the bone conduction had worsened, with a reduction of the air-bone gap. The patient was extremely satisfied, saying that after the operation he had no more problem, especially no more vertigo episodes nor dizziness. He mildly complained of the earing loss but does not require a hearing aid. He is still working.
Figure 1: Case n. 15. The left lateral semicircular canal is absent in his superomedial aspect. The endosteum is exposed and open. A piece of absorbable gelatin is ready to seal the hole. The facial nerve is exposed.
Figure 2: Case n. 17. Upper row: At the axial (left) and coronal (right) CT view, an erosion of the left lateral semicircular canal is evident. Lower row: A piece of mucosa is left over the semicircular canal bone erosion and also partially over the exposed facial nerve.
Case n. 18 (Fig.3) L.C., male, 62-year-old. Seen in the year 2008 for right chronic otitis media with discharge and evidence of cholesteatoma. The CT confirmed the involvement of the middle ear and showed an evident amputation of the lateral semicircular canal. He had a low-to-medium-grade mixed right hearing loss with a small air-bone gap. The patient was operated on in May 2008. A bony fistula, covered by the cholesteatoma matrix was detected. The matrix was carefully removed and an opening in the endosteum was found. This was immediately sealed with fascia + bone pate. The facial nerve was widely exposed, from the cog to the second genu. An open TPL with an ossicular reconstruction (titanium PORP) was performed. The post-operative outcome was good. The patient had no vertigo and a bone conduction control after 10 days showed no worsening of the curve. The patient recovered well and the hearing level remained as it was pre-operatively. He was strictly followed and ten months later a mastoid recurrence of the cholesteatoma was removed. Over the years the ear has remained stable, with a dry small perforation of the new-TM. As a piece of information, all the patients operated by the Author for open TPL are advised to clean the operated ear, at least twice a week, with a warm boric or boricsalicylic solution [11]. In regards to the hearing, the bone curve was unchanged after seven months following the revision surgery, then started to deteriorate. At the most recent control, in April 2020, the ear is persistently stable but the hearing has worsened to a middle-to-high grade mixed hearing loss.
Figure 3: Case n. 18. Upper row: CT axial view. Middle row: CT coronal view. A wide opening of the right semicircular canal is evident. Inferior row: the superomedial half of the bony right lateral semicircular canal is absent. After careful matrix removal the endosteum is exposed and open.
Case n. 19 (Fig.4) F.D., female, 47-year-old. She suffered for recurrent right ear discharge since her childhood, with hearing loss. In the year 2011 the situation worsened and the patient saw an ENT specialist who detected the presence of cholesteatoma, requested a middle ear CT and referred her to the author. There was a conductive hearing loss with a substantially normal bone conduction. The patient underwent surgery in February 2012. A posterior-superior bony erosion with granulation tissue and cholesteatoma was detected. The ossicular chain was involved by the cholesteatoma and blocked. The mastoid was contracted and poorly pneumatized. The facial nerve was exposed at the second genu. An open TPL was planned and performed. During the bone-drilling, the endosteum of the lateral semicircular canal was exposed to a grade where the gently pushing on the stapes provoked a bulging of the endosteum itself. The bony erosion was immediately sealed with bone pate and the operation concluded uneventfully. No ossicular reconstruction was performed. The patient had no problem and she has been regularly followed. The hearing remained as it was before the operation. She always refused to undergo a reconstructive/ functional operation. The most recent control was performed in February 2020.
Figure 4: Case n. 19. Upper row. CT, axial view (left) and coronal view (right). The right semicircular canal is covered by bone. Lower row. The excessive drilling has exposed the endosteum of the right lateral semicircular canal. Pressing onto the footplate causes a movement of the endosteum itself.
Case n. 20 (Fig.5) S.G., male, 47-year-old. Referred to the author in February 2012 with an history of recurrent right ear discharge for several years. A previous ENT examination showed an erosion of the scutum with granulation tissue and cholesteatoma. A CT confirmed the involvement of the middle ear and a probable fistula of the lateral semicircular canal. There was a mild conductive right hearing loss. The patient underwent operation in March 2012. There was a huge tympanic-mastoid cholesteatoma. After careful removal of the matrix, a bony erosion of the lateral semicircular canal was detected. The endosteum appeared to be covered by a minimum slice of bone and there was no mechanic transmission when gently pushing onto a mobile stapes. The facial nerve was covered/closed. An open TPL was performed with ossicular reconstruction (titanium PORP). The patient did well and post-operative hearing was improved and grossly normal. The patient was lost to follow-up and recalled for evaluation in June 2020. He reported a good and stable condition of his right ear for the first six post-operative years. In the last two years, instead, he suffered for recurrent inflammations and underwent ENT examinations without significant results. A CT was suggested and performed at the beginning of year 2020. Despite the surgical cavity was filled with crusts and epithelial debris, it seemed to observe a regeneration of the bone over the lateral semicircular canal. The patient was followed by the author and the local situation led to healing. An audiogram performed on August 24, 2020, showed a mild conductive right hearing loss (500 to 4000 Hz: 35,35,50,50), with bone conduction still normal.
Figure 5: Case n. 20. Upper row: CT axial view (left) and coronal view (right). It seems to be a thin bony remnant over the right lateral semicircular canal. Lower row: after careful cholesteatoma matrix removal (left), a bony erosion is evident with nearly exposure of the endosteum (right, white arrow).
Case n. 22 (Fig.6) M.S., male, 22-year-old. In May 2017 the patient had a documented episode of pure conductive hearing loss (50-45 dB from 500 to 4000 Hz) and tinnitus, with a tympanogram type B, which completely recovered within a month after local and general steroid therapy, and was interpreted as serous otitis media. A further control in July 2017 confirmed a normal hearing and a type A tympanogram. In February 2020 the patient was seen at the author’s institution with an acute right facial palsy (grade V, House-Brackman scale). He complained of few symptoms in the ear but a hearing loss. At endoscopic and otomicroscopic examination, a posterior-superior bulging of the tympanic membrane (TM) was observed and an explorative myringotomy was performed which was substantially negative. Both a CT and MRI of the ear were obtained, showing a complete opacification of the middle ear with mastoid inflammation. Besides the suspect of a middle ear inflammation with subsequent irritation of a congenitally dehiscent facial nerve, the hypothesis of a tumor of the facial nerve was also taken into account. An explorative tympano-mastoidectomy was then performed on February 20, 2020. The facial nerve turned out to be closed and the antral-attic mass was histologically diagnosed as “adenoma”. In order to remove this thick and adherent tissue, a posterior tympanotomy was planned. During the drilling, and because of the presence of the pathologic tissue, an excessive thinning of the bone over the lateral semicircular canal was realized only when a complete aperture of the bone had occurred. Fortunately, a thick endosteum was still intact and the bony fistula was immediately sealed with bone pate. In order to completely remove the pathology, the posterior bony wall was temporarily removed, then repositioned and stabilized with bone pate + fibrin glue. A first stage closed TPL was thus accomplished. The patient had mild vertigo for three days. A bone conduction control was performed 4 and 6 days postoperatively and it was as before the operation. The patient was then followed and the last control was at June 2020. The healing was completed with a well oriented and trophic tympanic membrane. A 50-60 dB conductive hearing loss was detected, as normal after first stage TPL. The facial palsy completely recovered. The patient still complains of episodic short spins of unbalance. An MRI control has been planned.
Figure 6: Case n. 22. Upper row: CT axial view (left) and coronal view (right). The right lateral semicircular canal is closed. Lower row: the excessive drilling over the right lateral semicircular canal has been recognized when the endosteum was already exposed. Black star: pathologic tissue (adenoma).
Discussion
As easy to understand, erosions of the lateral semicircular canal with exposure of the membranous labyrinth (endosteum) and even rupture of it, happen in the great majority of cases when dealing with a cholesteatoma of the middle ear. An exposed facial nerve is also a common finding and its frequency easy to understand as well.
Significant hearing loss has to be taken into account when dealing with a fistula of the lateral semicircular canal. It may happen also when the post-operative fistula test is negative. This is what reported by Yeho et al. (2004) [4], in the two cases of iatrogenic fistula they could observe. Besides the incomplete reliability of such maneuver, it may also mean that this negativity was caused by a hypofunction of the damaged labyrinth but, finally, also that the auditive (cochlear) partition is more sensible than the vestibular one. Surgically created (iatrogenic) fistulas have been reported to occur in 0.1% of the cases or less, with a good hearing outcome in the majority of such patients [12].
In the author’s series the percentage of iatrogenic fistula is 2.5 % (4/22) and the good hearing outcome is confirmed. It is the author’s opinion that the rate of occurrence is probably higher than reported in the literature, where the Authors generally present such cases without mentioning the number of their whole series [13]. The prevalence of the fistulas of the lateral semicircular canal, instead, in the author’s series, is 14 % (22 cases over 158 patients), which rises to 19 % when considering the sole cholesteatoma cases (21/111). Naderpour et al. (2008) [14] examined series from the year 1978 to the year 2000 and the percentage varies from 2.9% to 21%.
More recently Meyer et al. (2016) [3] report a prevalence of 6 % in their series, with a huge number (16/42) of type I fistulas, that is a simple bone erosion, according to the classification of Dornhoffer and Milewski [10].
The percentage reported by Rosito et al. (2019) [5] is 2.7 %. These authors considered only the type II (endosteum exposed) and III (endosteum exposed and open). In the Author’s series, when considering the sole cases with open endosteum (type III), the percentage is 2.5 % (whole series, 4/158) or to 3.6 % (cholesteatoma cases, 4/111). Adding the type II cases (9/22), the percentage rises to 8.2 % (whole series, 13/158) or 11.7 % (cholesteatoma cases, 13/111). Because the main purpose of this paper was to evaluate the audiological effects caused both by a spontaneous exposure of the membranous labyrinth or by its inadvertent uncovering by excessive bone removal, all the three types of fistula were considered. Indeed, the aim was to test the mechanical and noise effect that an excessive drilling and any manipulation (palpation, suctioning, cleaning), even careful, might cause. In regards to these effects, the results seem to be good. Even though the numbers are small, the sensorineural hearing outcome (bone conduction) was encouraging and a post-operative deterioration was observed in only one case.
Satisfactory hearing results seem also to confirm that a careful manipulation and removal of the cholesteatoma matrix is a significantly safe maneuver, as it is in regards to an exposed facial nerve. None of the author’s patients with an exposed facial nerve, in fact, developed a post-operative palsy. The author has no experience of the complete obliteration of the semicircular canal, which too seems to be a safe maneuver in regards to hearing preservation
Conclusion
When dealing with a middle ear cholesteatoma, the possibility of finding a fistula of the lateral semicircular canal, as well as an exposed facial nerve, has always to be kept in careful account. This was mandatory when imaging was not routinely obtained and before the CT era. Nonetheless, even though high quality CTs allow an easier detection of the bony erosions, attention must constantly be paid as well. In regards to how to manage the fistula, the ongoing experience has validated the strategy of a careful removal and an immediate seal of an eventual open endosteum, with biologic means. Also, a complete obliteration of the canal has proved to be safe. As reported in the literature and also in the author’s experience such a careful attitude reduces the risk of sensorineural hearing loss to a minimum. Furthermore, in the author’s opinion, the choice of leaving a piece of matrix on top of a wide bony erosion, which appears to be soft at a careful palpation, is still an advisable option (mandatory in the case of the only hearing ear), trusting in its mucosal transformation, as seen during second look operations.
Acknowledgment
The author wishes to thank Massimo Giuliano Bonetti, MD (Neuroradiology Unit, Department of Radiology, “A. Murri” Hospital, Fermo, Italy) for his valuable help in the choice of.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-cr-id-00145/ https://ijclinmedcasereports.com/pdf/IJCMCR-CR-00145.pdf
0 notes
Text
Oil Engagement of Totally Burnside Teaching Staffs Toward Widow Non-Teaching Staffs in Bypass less Sunlight Pharmacy Institutions in Indian University India Privately by Rahul H*

Abstract
The sustainability of the well being is new challenge, when source exhaustion and space contamination grow to critical hazards. The circular economy is new myth, turning wastes in supply, but entropy implies decay. Sustainable courses for planet in the universe are realistic vision, due to the earth vs. cosmos disparity, using human intelligence. The optimistic views suggest the men’s adventure as spot eevet of the overall cosmic rationality or heavenly wisdom, which isuniverse design, not affected by what occurring in a negligible site. The immanent ortrancendent reasons prospects sceneries, in which the men’s relational abilities and technological innovations are inner/upper driven and the apparent profinciency is outcom of the extant backdrops. The comments offer hints along the two views.
Keywords: Progressmyth; Political Setups; Relational Modes; Regularit; Ecology Defy; Uniformit; Awareness; Harmonising
Introduction
The human progress typifies by technology innovations and political deployments, changing the original wilderness in more comfortable life conditions. The formers present revolutions, when clothing establishes the garbed societies; breeding/farming creates the agrarian economies; the work organisation generates the productive efficiency. The technical novelties start, may be, because of upper or inner causes, started by transcendent or immanent inputs.The latter sceneries connect to the relational modes that the assemblies have, adding faculties and functions not possessed by the singles, to obtain collective setups. The political novelties, again, are not just dependent men’s conception; they might have upper or inner origins, having total worth.The two lines combine: the civilisation merges technical and political issues, with change overs, to distinguish history eves.
The progress due to technical or political spurs, thus can be contingent result, or total fact, for instance, scientific knowledge: we believe that the sciences duplicate the cosmic information of the entire universe. The mentioned readings tell that technology and politics can lead to total settings out, backed byupper or inner reasons.The political deployments quickly show alternate readings: civic orders, based on bottom up ideas; social orders, with top down totalsources. The relational modes promote both results: the former, just, manmade; the latter addressing heavenly wisdom or cosmic rationality, as social orders with already fixed upper or inner instructions. The events happening on earth belong to overall phenomena, whose progression denotes coherent trend.The earth vs. universe links are hypothesis, providing plausibility to the human civilisation, as spot results of general designs, having upper/inner origins.
The political deployments are helpful reference, to figure out the behavioural description of peoples by therelational modes, say, the interactive patterns involving individuals and collectives. The men’s actions modify by education and training: the taught manners and skills are the bases of the civicorsocial orders. This means that teaching/learning is critical requirement, while disposition may add, with traits limited to the humankind or widened to upper or inner conditioning spurs.The alternate interpretations help creating bridges between human intelligence andheavenly wisdom orcosmic rationality, in view to involve theholy directionor the cosmos’ information in the relational steps that implement the political arrangements. The upper/inner backdrops ofsocial orders involvedivine description of sovereignty or natural explanation of headship: themix-up of interactive patterns entails access to concepts or mental items, to infer choices, not evidence of the entranced information: the men conceive perceptions and thoughts, using mimicry; the reality typifies by the embedded information and statistics.
The political innovations, in synthesis, connect to interactive modes and human laws or to ethical tenets and behavioural guidelines. Instead, the technical deployments link to matter transformations and physical laws or to natural rules and tangible constraints. We usually believe that sciences establish on total‹truths› and get hints about our trusting in technologies; theparallel belief in obligations and moral principles, thus, shall turn in total ‹truths›, if aiming at politics trustfulness. The equivalence, mostly, does not exist and the human laws need enacting procedures, useless for the physical ones. However, the political deployments appear enjoying consistency, timely acknowledged by civic/social orders, with no distinction of contingent or total backdrops. The hereafter-collected hints describe such ambiguity, when globalisation turns intopotential political arrangement, to face the ecology sustainability requirements.
The Collective Beackthroghs
The civilisation implements collective organisations, which show the interpersonal intricacy of folks and individuals: the relational modes that apply to individuals, disappear in folks, with less educated reactions, as if the personal culture vanishes. The crowds simplify decisions, keeping extreme positions only: actually, each person seems share radicalism, dropping his usual fairness. The oddity soon evolves, forming close societies, i.e., regular setups of nation-states, keeping the pertinent citizens, with collective education along official canons. The grouping oddity, more generally, is usefulfor masses’ indoctrination, known technique of political parties’ propaganda.The personal and collective instruction modifies the linked behaviours: the natural demeanour is modifiable result, while the base relational features remain proselytization, coaching and brain washing possibilities, with personal and collective effects. The trends are tricky.
The political arrangements, timely devised by men, show the impressive inventiveness of individuals and collectives, from the earliest ages of the garbed societies. The creation of artefacts classifies as technology innovation, but, immediately, specifies interactive ingenious and crafty design: the buildingcovers personalobjects and technical tools, giving evidence that men particularise reasoning logics, allotting functional or instrumental utility to the items. When the interpersonal clans widen skills and experiences, the grouping allots meaning fulness to diversified expansions or to deepening integrations, to shape civic or social orders, following the each time-preferred interpretations. The gathering of people supplies benefits: easy contacts modify acquaintance and private effectiveness; aggregation seems to be agreed chance, accepting the new-borns, with parental care and education.
The socialorders enjoy of inner or upperfeatures, believed inspiring the creation of get-togethers, from families to peoples, of the human beings. The principle faces the initial limit with then ative idioms, which have parental education for teaching and learning purpose. The language invention happens to be local: it follows pace wise processes, so that communication is common human capability, based on coded spoken and written symbols, with local choice. The language communication is unifying chance, with native easy comprehension, according to idioms or dialects. The assembly processes appear starting on locally symbolic picks, perhaps using spot customs to orient graphicand spelling habits; it progresses to civic orders, pace wise implemented, marking the autonomy of local communities.The civic vs. Social lorders are open query:
the earth and linked occurrences are negligible anomalies, not affecting elsewhere courses;
the universe has own coherence, with cosmic information, itemising local transformations.
Leaving open the choice, the narration addresses men centred contingent viewsor cosmos centred total facts; the latter accounting is fictive. In any case, the collectives’ formation shows the possibility of parallel autonomous assemblies, with relational modes, which define civic/ social political entities. Soon, structured assemblies establish, with members, elites and leaders for the different tribes. Peoples happen designating single individuals either entire rallies or tribal groups, giving evidence of the meaningfulness of the ethnical partitions. The records, telling the history of timely ruling peoples, showkings by godly grace or holy passed commandmentsor elected peoples, which state the transcendence of their selection, justifying their acts.Otherworldliness simplifies extracting sovereignty, wisdom or otherness by faith settings, with removal of possible checks in this world. The history, mostly, implements these views; the regular societies separate citizens from foreigners, dwell specified territories, have national rules for the inhabitants and international treaties among parallel countries.
The regularity, originatedby ethnic or cultural reasons, has apparent backing in the spoken idioms, with splitting of political entities, along to national partitions. The analyses, then, distinguish three situations:
scattered political structures, carrying nullor loose mutual interactions;
independent political setups, interacting with local hegemonic chances;
dependent political layouts, each other affecting planned deployments.
The list shows the political assemblies are natural fallout (typifying men from other animals) so that the relational modes are regular human quality; however, the overall deployments are open question, being conditioned by what is happening on the earth or, more in general, at cosmic range. The recalled political sceneries shows that collective aggregations form since the earliest age; theregular societyis continuation, distinguishing citizens, from foreigners, so that sorts of ‹masses’ indoctrination› are as old as the formation of communities. The citizens needupbringing, teaching and coaching courses and solidarity or cohesion is agreed request in the ‹nation-state› settings, with automatic rivalry and competition fallouts on the parallel institutions. The trends have reason to modify, if the progress becomes impossible, because we live on the small planet earth, with limited sources and contamination bonds. The last scenery is, possibly, unexpected occurrence, maybe, leading to the progressive end of the humankind.
The investigation shall look if changes are possible to grant the supply continuity and the safe rescue; the vicissitudes will affect the political setups and the analyses shall review the necessary innovations for the progress sustainability. The physical laws describing the universe include irreversible facts and entropy, making evident the progressive decay of the material surrounds; however, the earth is negligible spot in the universe: theenquirymay limit to the salvage of our planetin habitant, maybe, along interstellar travels.
The Interactive Ground Works
The relational modes are human characteristic, showing the capabilities of political deployments. The current analyses distinguish three relationalspheres, to predispose the familiar informal connections, thepersonal operational conducts and the public official obligations. The setting of tree layers is questionable viewpoint: possibly, it is just a posteriori issue. In any case, the relational modes cover:
communication ranges by native idioms with linked vocabulary ad construal;
market rangestrade managing with legal exchange and financial inventions;
Headship ranges through decided governance and officialdom architectures.
The brainchildren are coherent, if abstraction and encrypting are ways to thinking and creating symbols for ideas. Communication establishes, when, among the members’ group, perception and encoding bring to agreed formats with shared meanings; similarly, markets occur, when fitbargains satisfy sellers and clients; leaderships create, when the hierarchic authority improve the executive efficiency. The subsequent civic or social orders showthe practicality of politically organised societies, via contact, trade and governance that enjoy locally shared readings. The nation-state construction moves from such bases and leads to the split-sovereign counties, today, considered standard reference in describing the world’s political evolutions.
Language, business and governance require the availability of ‹knowledge›, to assure awareness of the relational framework according to abstract concepts, encoded to be understood by the interfaced people. The mental processing provides consciousness of the interpersonal connections, whether just developed by bottom up ideas, or implemented using already entrenched upper or inner instructions.
However, the relational modes transformations follow higher complexity patterns: the three ranges are just starting domains, from which explaining, on the earth, the civilisation anomaly, supported by human intelligence or promoted by heavenly wisdom or stayed by cosmic rationality. We are aware of glitches, if progressshall develop on sound causal tracks, with the automatism of self-sufficient biology processes and of autonomous cognizance procedures. The justifying guesses look after instant logic, each pace choosing benefits and avoiding detriments, in view of welfare: the human intelligence properly elaborates such logic, based on timely assessments and judgments. The decision basis avails of knowledge, contingentappraisals, collected by human intelligence. The bottom up relational construction has dependent worth, never owing absolute information, unless the cognizance procedures could lead the total assessments.
The knowledge is not just human discovery; it collects actual data on the reality, together with personal feelings and natural characteristics, composing the spiritual reality: the overall actuality combines material and spiritual entities, the ones with physical evidence, the other with heavenly sort. Theknowledge belongs to thespiritual spheres, representing the intangible characterisation of the universe, when the depictions use godly dualism. The previous depictions, too, accept dualism; the holy reality vanishes, turned inmental spheres, so that we develop factual dualism, replacing spirituality, by imagination. The knowledge is wholly different entity, even if we keep the same word and we look at unified designation of the mixed trails.
The relational modes bring to abstract brainchildren, detailing knowledge flows, with contact, trade and authority functions. This reading applies on dependent bases, figuring out the contingent knowledge, built by human intelligence. The cognizance by abstraction and encrypting procedures is oddness, whether the imagined mental worlds happen replicating the extant reality; the discovery advises conceiving the spiritual dualism, as if reasoning and deciding belong to higher spheres, in which holy wisdom is fundamental trait. The separation of the spiritual from the material reality allows dealing with total knowledge and defining concepts such as legality or sovereignty with absolute worth. The dualism isarbitrary if abstraction and encoding have explanations, even without resort to imagination and linked mental worlds, but just having inner procedures performing the mentioned functions. The immanent, as the transcendent ways, lead to total knowledge, but these, also, require redefine what we define with (intrinsic) knowledge.
Biology and cognizance are earth variances, starting life forms, with agentive capabilities and intellects, with reasoning aptitudes. The biology has information in the genome, series of instructions, transmitted by the living beings, with proliferation and generation of new life species by gene evolution; the cognizance has origins with the human species, with emulation and simulation procedures, allowing the replication of behaviours and functions, with the resort to synthetic symbols, having agreed meanings as meme fruition options. Apparently, biology and cognizance profit of inner data, already cosmic information, starting life and intelligence on our planet, withgene evolution and meme fruition patterns. The cosmic information is aspect or quality of the universe, never requiring the separation of spiritual reality or the imagination of mind worlds, but only the detection ofintrinsic aspects or qualities of the tangible reality. The knowledge identifies with carried features or attributes of the extant reality, since cognizance directly involves cosmic information; the autonomous thoughts or spiritual entities are intangible entities, incompatible with mere monism. Reasoning and judgment via forged monism follow, however, material paths ways neuronal nets, processing carried qualities, handled as intrinsic or implicit knowledge, without any abstraction.
The interactive surrounds of men shows the cognizance procedures, with the abstraction and encrypting peculiarities. The relational modes allow devising coherent political infrastructures, where communication, trade and authority offer balanced helpfulness, with parallel ‹nation-states› in competition. The balance is stated by simulation procedures and mimicry practices, telling that the staedy equilibrium is dynamic path, between diversified efficiency parallel political organisations.
Regular Split-Sovereign Countries
The relational modes have complex definitions, depending on the models, used to describe the progress and the civilisation conquests. Presently, the split-sovereign nation-states seem obvious outcomes, as if the origin autonomy and self-sufficient organisations are intrinsic truths. The parallel self-sufficiency has office and economic reasons, with administrative staffs and payment roles, purposely orienting the transactions. The different nationalisms have standard supports stoicfacts and narrations, fostering alterities or realities. The regular parting leads to closed societies,with governments, inter-state treatiesand citizenship rules. The devised models differently explain the parallel closed societies, always acknowledging the partitions as adeptness and efficiency marks of the political setups.
The factual dualism operates with local native languages: as expected, contacts and communications are easier with no need of translation. The godly dualism benefits by holy grace kings, simplifying all choices by homogeneity. The forged monism resorts to Darwinism, presuming gene dependence for headships or race partition. All three models justify parallel political structures: since the incentives differ, we may check the related plausibility. Divine or racial motivations are hard to prove; cultural backing switches investigationtomeme fruition, with three definitions of knowledge: contingent invention, spiritual entity or matter aspect. The conclusions, however, are never final: substitute viewpoints may advise differently reading the settings or adding further conditions, to delivertotal steady solutions. The relational modes are human inventions, but upper or inner reasons may exist, showing that the outcomes are already specified by transcendent or immanent causes, according to a priori settings. The regular split-sovereignty political connotations are example issuesthat progressively appear, providing balanced stability among the world populations, even if the sectional constancycannot be permanent.
The nation-stale, nonetheless, is very instructive result, having, at least by Darwinism conjectures, wide consent.The guessadapts gene selfishness into group self-centredness or nation solidarity of each given closed societies. The solidarity shows that egoism or self-interest allows enhancing the personal profit, with the benefit of the common clan: the inference requires appraisals and checks, but also trust in the group: both entail meme fruition, further than gene evolutionand Darwinism merges the two phases, processing intrinsic knowledge. The solidarity concept is evident option, with explicit knowledge: the factual dualism exploits open reasoning, conjecturing the communality’s returns; the godly dualism looks at holy rewards. The unity or harmony at the clan range does not automatically brings to the opposition or rivalry against parallel clans: such ends are implicit in forged monism; otherwise, the explicit knowledge avoids automatic dispositionsandthe local rules establish compulsory acts, to obtain the nationalistic bias.
The conclusions about nation state’s solidarity show the implicit either legal regularity of the practice in view of safeguardingthe unity or harmonyof the institution. The nation state has the mission of protecting its own citizens, promoting treaties and alliances or performing wars or conquests to destroy enemies and to reach hegemonic power. Conflicts and struggles are permanent necessity, with battle and engagements to define overall equilibria between armed coalitions. The world distinguishes the relevant influence areas from the residual spaces, without critical effects; thereafter, the world decides the nation states according to the affluence, from development levels, down to different under-development ranges. The euphemistic classes show several sceneries, depending on the local past traditions and on current resource availability weighted through the instant administrative effectiveness. The world over situations show huge disparities, with many under-developed countries and large amount of peoples lacking of food survival ratios; the earth sources hardly satisfy the current populations and cannot face increased necessities.
The organisation of parallel split-sovereign nation-states allow hiding the critical supplyunbalance: sets ì of affluent societies exist also in the under-developed countries and the statistics show not clearly allocatedstored wealth. Moreover, the world division, with allotted formal autonomy of competing countries make clear the respective proficiency or incompetence, with legitimation of disparities. The idea of free and equal men is utopia; the regularity shows differences and constrained behaviours, biased by education chances: the relational modes are just further element for learning the effectiveness that is more appropriate. The efficiency requires diversity and rivalry, each one, individual or country, having suited goals and functions.
In the today world, the ‹regular societies› transform in local ‹nation-states›: nopeople remains without citizenship and the legality implies allocation and integration constraints. The repetition of individual and collective selfishness at industrial effectiveness spreads the world over, with over-consumption and over-contamination fallouts: the natural balance disappears and ecology starts being critical concern.
The Ecology Imperatives
The globalisation, lately, advises that the organisations of parallel split-sovereign nation-states show low usefulness, dealing with scale chances in communication, trade and domination. The worldwide web, bond-free market and universal management provide economy efficiency, with spread-out access to services and facilities, if the local political rules do superimpose obstacles or biasing effects. At the point, the regularity of closed societies’ structures appear abnormal, adding unfitting bureaucracy and governing costs andjobs with no benefit of the people involved in the actual business. Most of officialdom and management adds clerical duties, with organisational purposes, not useful for financial enhancements.
The globalisation, soon, turns from economy, to ecology objectives: the financial efficiency has to deal with material sources exploitation, since all physical transformations happen with increasing entropy and our surrounds keep memory of all previous exploitations. Today, the extant parallel nation-states are cross dependent, not only, because politically not split-sovereign, also, because technicallycarrying too many irreversible exploitations. The ecologyglobalisation is XX-century’s challenge, with still unknown outcomes. Economy and ecology seem belonging to opposite cultural context, even if linked to the root ‘oikos’, house or home, meaning ‘house ruling’ or ‘homeland description’ and, both, implying global issues, after the local attention of the three-range relational modes. Actually, both investigate what happen on earth, leaving the universe in the backstage: economy shall look at efficient and safe use of sources; ecology shall keep home friendliness. The technology revolutions are instrumental aids, on our planet to create improvement and, at the backdrop, the universe is source, almost unlimited, of useful provisions.
The ecologystartshaving critical relevance, when over-consumption and over-pollution hassteadily to increase, if the life quality need to be remain unchanged. Our planet is bounded space, with finite storages and limited balancing aptitudes: if human actors simultaneously transform resources and pile up wastes, the exhaustion of useful fonts and contamination of cheaply reached territories become widespread effect. The realistic analyses require continuously more impressive recovery and salvage measures, for the rescue and offsettingnecessities. The ecology imperatives shall grow, leaving no freedom to political selections or economicalarrangements: we all are compelled to assure the control of the earth’s habitat, because each one affects globalvillage, with non-negligible drawbacks. The global warming is example issue, with parallel fallouts in climate spot anomalies and general agricultural modifications.
Theecology imperatives are,certainly,disputable: the Greenland, free from ice, shall be back what seen by the Vikings; the navigation of the Arctic Ocean will speed up transcontinental migrations; the different new environments are, possibly, caused by the heavenly wisdom or by the cosmic rationality, and we, only, have to wait and see. If caused by the human intelligence, our responsibility is involved. The third guess is plausible: we might just try to combine additional guesses, aiming at possibly harmless ecology imperatives. For sure, our science happens trusting on total physical laws (closer to absolute knowledge of godly dualism or to intrinsic knowledge of forged monism, than to contingent knowledge of factual dualism), thus, also for ecology, we shall look after total reasoning and decisions, to prospect optimistic ways out, parallel to the realistic ones. Ecology has not at all straightforward approaches, aiming at vague sustainability.
The compulsions involve greener policies by enhancing agricultural value added am lowering industrial open tracks. The reverse logistics enable circular economy plans, reducing litters and using trashes in spare cycles.The industry steps, from the fir dine one, include robotic devices, for on process decision schedules and, progressively covers many other processing tasks, out of machining, to perform administrative, clerical or abusiveness functions with industry forth step and, with industry fifth step,also, recovery and salvage. If looking at the productive apparatuses, ecology develops parallel to intelligent programming and control: fit visibility and monitoring are options, allowing customer’s satisfaction and spare permanent management. The discernibility is routine of the technology innovations, but the parallel collective breakthrough, as well, happens with the globalisation, reply modifying the political societies, by worldwide coverage.
When looking at the general laws of physics, ‹ecology› directly links to entropy and other irreversibility phenomena: the natural thermodynamics moves from regular order and aims at uniformchaos, even if, timely, singularities may happen (biology, if genome ordering is stochastic issue). The‹cosmic information› includes one-way transforms, without regeneration chances, when tangible stuffs have to be processed; the scenarios modify, with intangible operations, exclusively running along spiritual or imaginative tracks: the logic and reasoning are quizzical query, requiring proper elucidations.
Uniform Global Village Society
The three-range regularity of the relational modes becomes arguable, when ecology obligations become compulsory rules. The single nation-state has no interpretation freedom and unchanging limitations apply to every collectives or individuals, without exceptions. The uncertainty, mainly, entails the group self-rule, when the people assembly cannot justify inclusion or exclusion on clear-cut reasons. The relational layouts operate with evident approaches. To organise the citizens along different determinations:
friendly contact, using informal acquaintance to share moods, opinions and assistances;
private connection, with interpersonal links for trade, business and managing purposes;
Official association, with collective ruling by agreed leadership and regular government.
The three ranges are regular setups, once looking at closed societies, which have to rule theconnection between members and thelinks with the parallel societies. The political arrangements apply on assemblies, since the individuals chose to gather or not and suited rules shall define the belonging or not. Maybe,this isnatural condition, proved in Darwinism by group selfishness and solidarity, or godly privilege, allotted to chosen individual or people. Indeed, the a prioriofficialdom of governance setup is possible, resorting to inner or upper routes with total schedules: natural(racial) or holy-grace headships. Presently, we have to investigate if such local regularities persist with global assets, whenworldwide contact, universal market and uniform management start. With globalisation, the query entails how the regularity of closed societies could modify, yielding the uniformity of the open society, with the known relational modes.
The globalofficial association, now, does not enjoy bottom up construction, at least, having anthropic backdrop: the immanence or transcendence of the guidelines directlylinks to total cosmic rationality or to heavenly wisdom. The directions follow spiritual or intrinsic orders; ‹big data› issues are example settings, in which information processing offers inner (or upper) induced instructions, with special (natural and total)‹knowledge›, supplied asautonomous robotic creation. The ‹synthetic› hands and minds happen already to have inner (or upper) control: the global breakthrough avails of hidden‹robot’s paths› :the communication, trade and govern are inborn milieu facility, with uniform spread out over the extant populations, as open society, without closet boundaries. The ‹big data› structures have to follow suited inner/upper processing, allowing the worldwide control on the ecology data, with, on earth, balanced circular economy figures.
The uniform ‹global village› is wholly new prospect, compared to the older closed societies’ standards.The regularity starting from below, ondirect contacts, home connections and collective assemblies, does not develop, replaced by instrumental facilities providinginformation aides and duty controls:
computer web: communication avails of operation systems and standard routines;
net economy: market benefits of shared grids, personal logistic and home delivery;
global ecology: monitored recovery/salvage has to satisfy compulsory imperatives.
Communication becomes free from native languages, with worldwide web formulations. Trade does not any more depend on local biasing effects and can exploit universal provisioning. Whole sustainability needs avoiding spot privileges and has to oblige strict rescue homogeneity. The information innovation is result of computer technologies, which modulate the ‹industry steps› with data processing practices and not before available potentials, such as ‹big data› discoveries. The relational ranges are, now, substantially different: the lowest explicitly refers to computers, with the hardware and software improving rigs. The intermediate range uses computers to widen the engineering areas, to business, service and management goals. The last range supplies the ecology imperatives, transformed in technical conditions: the authority does not allow autonomy and sovereignty, because technical imperatives are themselves compulsory. The ‹global village› enjoys unbounded communication and market face to ecology constraints, without regular political dividers for locally adapted and, possibly, less stringent recycling and rescue obligations.
Without administrative, fiscal and financial partitions, split-sovereignty comparative efficiency ceases to exist and uniform controllers oughtto applyeverywhere the ecology imperatives, without the leaving out undue profit to illegal local swindlers. The uniform society is, nonetheless, oddness, because:
personal diversity: equality of citizens is myth, to justify parliamentary democracy;
judgmental autonomy: decision freedom is legend, ignoring information backdrop;
relational intricacy: interpersonal architectures bias private/public legality canons;
knowledge variety:cultural formation modifies priorities of communal obligations.
The behavioural uniformity looks at the ecology effects consistency on the earth’s surrounds, even when the individuals react differently. The ‹big data› anomalies apply for combined reasons: to supply equivalent controlling schedules; to enable upper/inner command, if present. The switch local-to-global requires that the previous self-rules vanishes,without authorisation of spot efficiency or optimum. The ‹uniform society› does not empower distributed intelligence, as if cohesive wisdom or unified rationality is already fixed, not allowing alterations. The ‹global village›avails of worldwide communication and economy; it expands over uniform society with universal ecology constraints.The total heavenly wisdom or cosmic rationality takestheplaces of contingenthuman intelligence, to establish the civilisation innovations, modifying the current wilderness. Theoutcomes follow optimistic hypotheses, with planned improvements, having spiritual or natural origins, rootedin the universe’s design and started byuppermiracles or innerstochastic events. The planning requires awareness of the choices, distinguishing progresses from deterministic alterations
Awareprogress Settings
The up to now path links progress and knowledge and depicts the human knowledge by series of steps, joiningcollective virtues, relational modes, regular societies, ecology fears and uniformity, but replacing the human intelligence with options, with cosmic or heavenly sorts. Shall we widen the knowledge idea? The said cognizance path, by relational modes, follows mimicry way, yielding human knowledge. Yet, we have:
contingent knowledge: human concepts,carrying clan’s agreed values and meanings;
absolute knowledge:: spiritual entity,expressing holy designs and righteous wisdom;
Intrinsic knowledge: cosmic information, showing the qualities of the material reality.
The godly dualism assumes existing spiritual, parallel to materialreality, stating abstract and reasoning occurrences, so that the knowledge is just the spiritual component of the universe. The lack of knowledge, inn mere monism, dodges the facts’consciousness; the forged monism detects the cosmos’ qualities, with linked men’s sentiments and judging features, by natural cognizance instructions. The spotted details are matter qualities, not separable from the support: the tied information repeats abstract spiritual specifics. The absolute and theintrinsic knowledge gives the same total data, one be acceding to the holy reality, the other by reading natural attributes. In the latter case, the knowledge is just implicit feature, possibly moved to new carriers, but never handled without upkeep. The factual dualism adopts bottom up construal: the human knowledge is mental by-product, imagined giving material qualities by abstraction and encrypting; its existence requiresthe shared agreement of codes and readings. The data supplying is manifest result of the relational frames at the cognizance procedural levels if interacting peoples.
The dualism distinguishes facts from knowledge of facts, with conscious narrations, ensuing cognition capabilities. The godly dualism has the spiritual reality for the intangible processing, parallel the physical transformations. The factual dualism resorts to the intellectual imaging, with reasoning and judging worth.The forged monism enjoys knowledge of facts, without separating the information from supports, since thememe fruition procedures are inner encoded instructions, spot enabled (out of the current determinism).The spiritual/imagination ways give knowledge autonomy; the encrypted qualities of material items involve critical output, possibly,in forged monism,avoided if cosmic rationality is backing asset, but the awareness of the trends is just implicit postulation, under ‹big data› options.Ecologyand joint sustainability hitches appear requiring the switch from nation-states, to ‹global village›, when the recycle and rescue targets, in lieu of factual dualism realistic chances, should look after forged monism optimistic achievements. The new horizons seem giving the possibility of total, not just contingent, recovery objectives.
The relational infrastructures always typify men on earth, only changed, from bottom up, to top down issues. They allow deriving knowledge or consciousness, to justify and to describe intelligence, rationality or wisdom.The relational organisations are, perhaps, men invention, either total traits, already pertaining to the universe, with projection on men. The two conjectures advise defining three ranges, within which the dealings develop mutual understanding, impartial conducts and endorsed headship, by suited frames:
friendliness: easy acquaintance, with alliance and native language communication;
lawfulness: correct behaviours in interpersonal trade and collective engagements;
governance: resourceful domination and ruling, under acknowledged leaderships.
Therelational frames are liablemind’s option, to recognise sensed facts and to elaborate thoughts. The concepts build identifying and describing thedetails,we collect from the environs and among us: this way, the results are contingent, but the humanknowledge hasindependence, perhaps human phantasy, perhaps spot insights of perceived hints. Only thegodly dualism allows access to absoluteknowledge, spotted in the spiritual reality.The dualism distinguishes reasoning, from spotting; the cognizance provides explanations, having agreed interpretations. In forged monism, ideas and notions buildscanning the reality and detecting the qualities by agreed formats and codes, using the innerguides of the gene/meme courses. The intrinsic directives belong to the material reality: reasoning and consciousness avail of immanent information, which is, as well, attribute of the same reality. However, it is awkward proving the non-contradiction of an axiom-system, within the theory: the inconsistency entails the system non-completeness, by mathematical logic, stating the non-sufficiency of self-reference schemes. The issue applies to mere monism; to forged monism, the non-contradiction becomes arguable, since such monism coherence accepts thoughts and judgments.
With immanence ortranscendence, the access to total descriptions authorises using cosmic rationality or heavenly wisdom and the linked intrinsic or absolute‹knowledge›, in lieu of the human one. The idea of uniform societyrequires looking after upper/inner enabling instructions, so that the civilisation is issue of universal figures.The relationalframes and selection awareness have natural or spiritual origins and direct impact on the human world, rather thanjust givingdirectives to men. Theintrinsic/absolute‹knowledge› happens to be peculiar entity, when we look at progress’ chances, granting sustainability prospects. The aware advances build on organisations (relational frames) and facilities (technical gears); classic analyses involve technologies and require options with innovative knowhow;the linked progress has just human intelligence promotion and the possible salvage looks after realisticimprovememts. Only atypical analyses include total projections and principles, with cosmic or heavenly backups and the fantasy recovery explores optimistic hypotheses, as if inner/upper causes will grant the earth’s safety by universal balancing aids.The impacts due to global steady settings are complex: the results are ambiguous, even if the cosmic rationality or heavenly wisdom certainly assures progress sustainability.
The data supplying is manifest in factual dualism, when humanknowledge builds pace wise, acquiring details by experimental procurement and collective settlement. In thegodly dualism, the spiritual reality is all comprehensive actuality, collecting the immaterial beliefs that explicate the material universe. In theforged monism, matter and information merge: detection and description use aspects of the processes, notimagined concepts. The contingent knowledge is, maybe, fantasy; the absolute knowledge is spiritualitem; the intrinsic information allows fictitious reasoning. The relational settings link to how men acknowledge the surrounds, to fashionourscience: imagined narrations, spiritual explanations or naturalaccounts. With dualism, the knowledge is explicit and we deal with intangible worlds; with monism, only tangible aspects occur and may connect with qualities, perhaps, encrypted and shared within the interactive clan.
Harmonising Communal Grids
At the point of the notes, knowledge formation and relational modes happen to be connected fetishes, symbolising how men become conscious of the surrounds and of the events occurring around them. The awareness does not means that we may control our future; it denotes our cognizance of the events, with possibilities of selecting or refusing the scheduled travels, for improved life quality. The prospects appear questionable:human behaviours and political attainments showrelational modes orknowledge grounds with twin interpretation possibility and we shallproperly distinguish:
civic orders, showingrelational autonomy,imagining contingent knowledge;
social orders, assuminginner or uppersituations, whichlead to total findings.
The replacing of contingent knowledge, by absolute or intrinsic knowledge entails pervasive changes, if this swaps from human intelligence, to heavenly wisdom or cosmic rationality. The regularity has coherent hierarchies by holy grace headship or genetic supremacy, leading to split-sovereign nations.The intricacy of consequences hints that the discovered pictures give access to total data, becauseupperor inner reasons provide backdrop control. The choice of social (mot civic) orders ensues civilisation’s sophistication, with technology revolutions (garbed, rural or industrial societies) and collective breakthroughs (scattered, local and global setups), yielding new life styles, due to technical finds/devices and to political organisations. The choice is, however, dubious, if the top down involute social orders compare to the intuitive bottom up civicorders.The intricacy worsens, if, with globalisation, uniformity replaces earlier regularity, when hierarchic settings have (apparently obvious) upper/inner reasons.
Actually, globalisation, with ecology necessities, seems turning to the open uniform society, collecting everyone in a bondless assembly. The setup appears, if the political orders build on unified communication aids, ending in ‹global village› withcivic modes’ construal. In the reality, many communication aids occur and parallel idioms offer choices, being unique only the abstraction-and-encrypting idea. Alternatively, by social modes’ reading, the abstraction-and-encrypting idea is upper/inner process, with holy/cosmic origins.The history registers multi-lingual (then split-sovereign) nations; the regular societies seem original socialsetup, with parallel autonomous courses to civilisation. The uniform society of the globalisation, thereafter, looks as if the ecology obligations are dangerous criticism, modifying the previous situations: the invariance of constraints is necessity, with no exceptions, which destroy steady safe recovery. Communication and, in general, the relational modes might follow automatic adaptive alterations, with upper or inner drivers, via ‹big data› facilities or along ‹bigbrother› procedures, perhaps, managed through ‹social grid› options. Thecontingent knowledge is illusory or temporary formation, properly turned in absolute/intrinsic knowledge, when stray situations arise. The regularity, as well, is anomaly, against stable uniformity. We cannot deal with men centred solutions; only cosmos centred answers might exist, if meaningfulness has sound truth.
The outlined propositions entail looking after preliminary guesses or sound theories, giving:
provisional balancing, with sustainability,prospectedusing holy/cosmic opportunities;
permanent steadiness, after discovery of universe’s physical laws and tied solutions.
The recovery possibilities supported by upper/inner causes requireabsolute/intrinsic knowledge and this happens, if we may trust godly dualism or in forged monism. The ‹social grids› are recent aid of computer nets, allowing worldwide communication, with creation of thematic webs, accessed by current users.The ‹social grids› have explicit and implicit ruling vendersormasters, which grant the network coherence, bring up-to-date the users’ profiles and distributing back the information, to satisfy all current requests.The net updating systematically affects the clients, due to the upper or inner causes and the on duty masters; the renewals, in our analyses, include deterministic trends and wily choices.The latter only yield civilisation, from wilderness and are typical, but not exclusive, issues of robot-like processing abilities.
The people balancing by communal grids combinesknowledge awareness and uniform society.The grids offer network’s chance of spiritual or natural backings.The holy origins lead to miracles, inexplicable facts that change the causal courses; the expected sequences abruptly may change, dueto intrinsic ‹big data› effects, with inner instructions already written in web structures.The two courses denote, either, the steering of godly wisdom or routing of cosmic rationality, with upper or inner reasons behind improvement. Thesocial grid’s alternatives are options only lately prospected, as if transcendence or immanence effects operate as trapped databases. Our faith in them is, just, the acknowledgment, which affect the progression around us, by already encrypted spiritual or natural reasons.The resort totranscendence or toimmanence facts is, possibly, conventional way to show preference in explicit knowledge and self-sufficient means and embedded knowledge and hidden details.
The sketched hints suggest that the sequence:collective breakthroughs, relational foundation, regular societies, ecology imperatives, uniform community, progress awareness and grid balancing, may offer the chance to not stop the extant civilisation, swapping from human intelligence, to heavenly wisdom or comic rationality. The relational abilities, at first, are bottom up contingent inventions of regular societies, then, they transform in upper/inner reasons, continuing awareness and matching in the men adventure, with fit sustainability fallouts. The last two steps are optimistic view, but also awkward chance: if we may trust in heavenly wisdom or comic rationality, the provisional balancing seems poor aim and thesteady progress should be achievable. Once acknowledged the initial five steps (joining collective virtues, relational modes, regularity, ecology fears and uniformity), the regularity vs. uniformity mismatch should not address along the laterinterim attainments (consciousness and networking choices), rather it shall look if the coherence of cosmos centred theories provide grant solutions bypassing the human intelligence.
Conclusion
The civilisation is earth’s oddity, improving men’s life quality, face to wilderness, with consciousness of the results of the done acts, after experiential tests. The progress combines technology innovations and political deployments, built by interpersonal skills, collectively endowed as relational modes, at personal range, or with upper/inner driving inputs.The political setups distinguish civic from social orders, by means of human intelligence inventions, in lieu of heavenly wisdom or cosmic rationality events.The separation ofcontingent, fromtotal results, allows understanding when the arrangements have upper/inner origins: the details are relevant, to assessthe progresssustainability chances.
The contingentknowledge implies the weak anthropic principle, with native idioms, local markers and split headships. The ecology fears, by cosmic centred views, lead tothe strong anthropic principle, by trust inupper/inner truths and cosmic centred chances. Absoluteknowledge implies transcendence and spiritual reality, leading to godly dualism; intrinsic information entails immanence and impliedknowledge, bringing toforgedmonism. If civilisation is effect ofupper wisdom or inner rationality, the anthropic awarenessand matching establish robot-like paths. The conscious upgrading and collective balance safeguard men aimed civilisation, with allied knowledge handling, for depicting and judging the universe. The material events and the events’ knowledge mix tangible and abstract structures, as if facts and narrations are independent and the reasoning power has spiritual consistency. Indeed, facts do not need accounts, but, without onlookers, they remain implicit. The physical world’s authorisation need by standers, which only have consciousness of the transformations; without witnesses, descriptions and assessments are absent. Yet, the elucidations and evaluations are intelligence outputs and require men-like or robotic competences, for knowledge database and reasoning effectiveness, in view of conscious decision-making proficiency. The harmonisation can have robotic authentication, being embedded property of the upper wisdom or inner rationality.
The sketched approach follows conformist routines: relational modes, to implement civic/social orders;cognition procedure, to instigate reasoning, planning and progress.The relational modes build knowledge› by abstract concepts, through encrypted formats: it shows sets of acts, facts and objects and gives insight on reasons and effects by symbolic stories.The all is meaningless, unless the restitution keys are available, to decrypt the details.By dualism, we have knowledge independence: spiritual reality or mental worlds;only, data handling, storing or narrations needs hardware equipment, with entropy effects.By monism, we have information immanence: the abstract reality does not exist; possibly, the knowledge is intrinsic aspect, picked by agreed procedures.The dualism invents the simultaneity of abstract worlds (spiritual or mental); the monism handles implicit knowledge, when doing explicit processing of carriers. The (explicit or implicit) knowledge appears comprehending natural details (holy edicts or physical laws) and personal particulars (feelings, thoughts, or judgments).The specifics appear scrambled, withmen’s choices codes, selected for local shared understanding:the formatting implies encrypting and restitution, following agreed formalisms.
Men only deal with contingent knowledge; the absolute or intrinsic knowledge links with transcendence and spiritual reality, or with immanence and natural laws, both, singled out to justify total truths, changing the ethical rules by heavenly wisdom, or thephysical information by cosmic rationality. The liable assets are enough for provisional progress without outrightcertitudes; thetwin total contexts are amazing: thewhole chattelsdonot provide responsiveness at conscious levels, if just heavenly orcosmiclinked.The delineation of knowledge and ofrelational frames offers hints on how the civilisation is strictly human wonder, with in backdrop only the universe. Yet, he three specified models are substitute, but, perhaps, not exclusive, if fit conditions overlap. In the study, ecology and globalisation offer hints, to conceive sustainability view. Thestandard civilization plans look after human intellect and contingent knowledge. The alternatives believe in upper/inner truths and trust that ethical tenets and physical laws already exist and are not men dreams. The faiths in absolute or in intrinsic knowledge, equivalently, acknowledge total e environs and describe the all by agreed encrypted formats: the former, spiritual entity and the latter, detected quality.Then, ecology, as well, becomes current aspect of the reality, with standard inclusive sustainability effects: thecivilisation shall remain unchanged, since the earth’s downsides are negligible, face to universe’s trends. The ensuing strong anthropic principle is cosmos centred, but it needs aware choice of changes and balanced network management, to specialise the civilisation along the ecology necessities of sustainability.
The anthropic biasingis manifest, when considered the role of knowledge in the study: dualism allows explicit narrations; monism reduces to forged setting, to permit intrinsic firms. Still, in the universe, the humanity is, perhaps, marginal fact (if limited to our earth): heavenly wisdom or cosmic rationality, thus, transcendence or immanence are thorough concepts, or they exist with no need of onlookers. Besides, if we believe in the entropy and decay of the physical reality, say, the whole universe tracks exhaustion and contamination, only provisional harmonization is feasible. The permanent steadiness, if upper wisdom or innerrationality is total option, cannot contradict the backdrop laws: the optimistic views are, perhaps, at the end, quite similar to the realistic pictures offered by the human intelligence, without the tricky trip to transcendence or immanence conjectures.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-rw-id-00144/ https://ijclinmedcasereports.com/pdf/IJCMCR-RW-00144.pdf
#Progressmyth#Political Setups#Relational Modes#Regularit#Ecology Defy#Uniformit#Awareness#Harmonising#Rahul H*#IJCMCR#clinical studies
0 notes