
Journal of Anesthesia & Intensive Care Medicine (JAICM) is a globally accepted journal that aims to publish innovative scientific developments and high quality information
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by juniperpublishersanesthesia and here's what we found interesting.
Average Info
Notes Per Post
281
Likes Per Post
163
Reblog Per Post
118
Reply Per Post
0
Time Between Posts
5 days
Number of Posts By Type
Text
17
Last Seen Tumblr Blogs





Fun Fact
Tumblr is used by 21% of adults online aged 18-29 years.
Text
A Rare Case of Varicella Pneumonia with Acute Coronary Syndrome and Lower Limb Arterial Thrombosis-Juniper Publishers
Abstract
Unlike in children, where chickenpox is generally a non-complicated disease, adult chickenpox (varicella) can have serious complications. Thrombotic complications of the varicella zoster are rarely observed. There is one case report of varicella complicated by myocardial infarction.We present a case of adult varicella who developed complications of peripheral artery thrombosis as well as acute coronary syndrome, requiring angioplasty.
Introduction
Chickenpox (Varicella) is a benign illness caused by VaricellaZoster virus and primarily manifests in childhood and is quite infrequent in adults. Most complications and serious cases are observed in adults [1]. These include pneumonia, encephalitis, cardiac arrhythmias, seizures, rare neurological sequelae including optic neuritis and transverse myelitis [2]. Thrombotic complications of the varicella zoster are rare [3,4]. A variety of hematological complications including thrombocytopenia, purpurafulminans and disseminated intravascular coagulopathy have also been reported in children with varicella [2-4].
Case Report
A 38 years old nonsmoker male was admitted with a vesicular rash over the face, chest and abdomen since 3 days. There was associated low grade fever (100 F) and dyspnea at rest. He had a blood pressure of 120/60mm Hg, pulse at 118/min, respiratory rate of 32 and Saturation (SpO2) of 88% on 6 litres oxygen via face mask. His ABG revealed hypoxemia with a pH of 7.45, pO2 of 58.1 mmHg, pCO2 of 36mmHg. Chest radiograph revealed bilateral nodular opacities with specks of calcification (Figure 1). His past and family history was unremarkable. His Complete blood count revealed leucocytosis, kidney and liver function tests, Lipid and thyroid profile were within normal limits.
Contrast CT thorax with CT pulmonary angiography was suggestive of bilateral pneumonia (Figure 2). Patient was treated as varicella pneumonia and initiated on acyclovir along with non-invasive ventilation and supportive intensive care. Tzank smear from vesicles revealed multinucleate giant cells (Figure 3). Blood and urine cultures were sterile
On the second day of hospitalization, patient's right lower limb became pale with signs of ischemia. Ultrasound Doppler of both limbs revealed a thrombus in right tibial artery and proximal tibial artery (Figure 4). CT lower limb peripheral angiography confirmed intraluminal thrombosis in right tibio-peroneal trunk (Figure 5). The same day our patient also developed acute left sided chest pain. Electrocardiogram was consistent with ST elevation myocardial infarction (STEMI) (Figure 6) and cardiac biomarkers like Creatinine phosphokinase-MB, troponin I and Pro BNP were elevated. 2D Echo showed regional wall motion abnormality in anterior wall of left ventricle.
Patient was initiated on intravenous heparin infusion with APTT monitoring. A coronary angiography was also performed which revealed double vessel disease having long segment stenosis (90%) in mid portion in Left anterior descending(LAD) and right coronary artery (70% stenosis). Percutaneous transluminalangioplasty (PTCA) to LAD was done. Thrombophilia profile (Protein C, S and Antithrombin III) and Lupus anticoagulant antibody were within normal range. Vasculitis markers like Anti-nuclear antibody (ANA), Antinuclear Cytoplasmic antibodies (cANCA, pANCA) were negative. Gradually his limb perfusion improved and cardiac status stabilized. A Review Transthoracic Echo-Doppler post PTCA done on the 8th day showed no regional wall motion abnormality and normal cardiac ejection fraction. Follow-up Doppler of Lower limbs showed no evidence of thrombosis. The patient was stable and discharged after 10 days of hospitalization.
Discussion
Chickenpox is an extremely common illness, with about 90% of the population seropositive by the age of 15 [2]. It is uncommon, but more severe in adults with an increasing number of deaths being reported hospitals [5,6]. Pneumonia occurs only in about 6% of infected adults [7]. Our patient had associated pneumonia. Treatment options vary from lotions plus antipyretic treatment or immunoglobulin and acyclovir for serious manifestations. Acyclovir does not significantly reduce the complications associated with the varicella zoster virus (VZV) infection [8].
Thrombotic complication is a rare occurrence in VZV infection [8-11]. VZV is known to have tropism for vascular endothelium of cerebral arteries. VZV is one of the commonest cause of ischemic stroke in children, other complications being cerebral aneurysm and subarachnoid hemorrhage. Unlike children, however, VZV in adults shows preference for lower limb arteries. Our PubMed search for VZV and thrombotic complications, showed only 5 reported cases of peripheral thrombosis, all involving lower limb arteries. All the five cases were males, three out of four being smokers with no past history of peripheral vascular disease. Our patient was a nonsmoker with no previous history of peripheral vascular disease. The origin of thrombotic complications of VZV remains unknown. One study suggests that thrombosis was associated with free protein S deficiency with the presence of anti phospholipid antibodies [3,4]. The presence of lupus anticoagulant was also found in one of the case reports [3]. Another study suggested thrombosis was mediated by autoantibodies induced by VZV infection and directed against the proteins involved in the coagulation cascade [11].
Acute coronary syndrome (ACS) may also occur in patients with varicella zoster virus infection after the primary infection caused by varicella infection has been resolved [12]. Interestingly, our patient developed acute coronary thrombosis and lower limb arterial thrombosis during varicella zoster virus infection and not as a delayed complication. To the best of our knowledge, a person developing ACS and lower limb arterial thrombosis during VZV Pneumonia has not been reported before [8-12].
Conclusion
Chickenpox in adults, even in those who are previously healthy, is a life-threatening infectious disease and may be associated with acquired hypercoagulable state manifested by acute limb ischemia, stroke or ACS depending upon the vessel involved. Clinicians should be well aware of these serious complications for early recognition and prompt therapeutic management. Above case is also important with respect to timing of complications. Thrombotic complications are usually delayed, but can occur in acute phase also.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com
For more articles in Academic Journal of Pediatrics & Neonatology please click on: https://juniperpublishers.com/ajpn/index.php
For more Open Access Journals please click on: https://juniperpublishers.com
0 notes
Text
Granular Cell Odontogenic Tumour - A Histopathological Rarity | Juniper Publishers

Juniper Publishers-Open Access Journal of Organic & Medicinal Chemistry
Authored by Nagahimabindu Vennamaneni
Abstract
Central Granular Cell Odontogenic Tumour (CGCOT) is an uncommon benign odontogenic neoplasm. It predominantly occurs in middle aged women. We report a case of CGCOT that occurred in the mandible of a 38 year old male patient. Clinical, radio graphical, histopathological features and immunohistochemical investigations like Calretinin, AE1/AE3, S100 and Neuron Specific Enolase (NSE) were described.
Keywords: GCOT; Granular cells; Odontogenic tumor; Intra osseous
Abbreviations: GCOT: Central Granular Cell Odontogenic Tumour; NSE: Neuron Specific Enolase; OPG: Orthopantomograph; irt: in relation to
Introduction
Central Granular Cell Odontogenic Tumour (CGCOT) is a rare, benign, slowly growing, noninvasive but unencapsulated odontogenic neoplasm [1]. So far 39 cases were reported in the literature [2,3]. It represents 0.3% of odontogenic tumors. Most commonly seen in the posterior region of the mandible with a predilection between premolar-molar region. It shows a predilection for middle-aged women [2]. In this article, we described CGCOT that occurred in a 38 year old male patient.
Materials and Methods
0.3 microns thick sections were obtained from paraffin embedded tissues that had been processed, stained with protein Hematoxylin and eosin stains. These stained sections were then reviewed.
Case Report
A 38-year old male patient came with a chief complaint of pain in lower right back tooth region since 4 months. There was no obvious extra oral and intra oral swelling. Orthopantomograph (OPG) revealed a well defined unilocular radiolucency in relation to (irt) the apical region of 44 to 46. Root resorption was evident irt 45 and mesial root of 46 (Figure 1). Aspiration was negative. Excision biopsy was done for histopathological examination which showed a grayish white surface (Figure 2). Microscopic examination of Haematoxylin & Eosin stained soft tissue sections revealed islands of odontogenic epithelium surrounded by thin fibrocellular connective tissue (Figure 3). Epithelial islands showed large central cells, with granular eosinophillic cell cytoplasm and eccentrically placed nucleus (Figure 4 & 5). Peripheral cells of the island are cuboidal to low columnar in shape without any nuclear palisading and reverse polarization (Figure 6). The connective tissue is interspersed with odontogenic epithelial rests. In the differential diagnosis we included granular cell ameloblastoma.
Immunohistochemical investigations were performed (Figure7). Calretinin was negative, Pan CK (AE1/AE3) was positive in peripheral cells and negative in central granular cells, which are in distinction with the granular cell ameloblastoma. As granular cell ameloblastoma shows positive calretinin staining and CK staining in both peripheral and central cells. Hence we ruled out granular cell ameloblastoma. S-100, NSE were negative, suggesting that GCOT is a distinct entity compared with granular cell tumour of the soft tissues. Overall radiographical, histopathological and immunohistochemical findings were confirmative of diagnosis of CGCOT. Enucleation of the lesion was done. Healing was uneventful and no recurrence was seen.
Discussion
It was first described by Werthemann in 1950, who used the term ‘spongiocytic adamantinoma’,Couch et al. in 1962 described it as ‘Granular cell ameloblastic fibroma’, Dalforno and Donna in 1970 referred it as ‘Ameloblastic fibroma with stroma of granular cells’, White et al. in 1978 termed it as ‘Central granular cell tumor of the jaws’, Vincent et al. in 1987 termed it as ‘Central granular cell odontogenic fibroma’, Shiro et al. in 1989 and WHO 2005 considered the term ‘Central granular cell odontogenic tumor [2]. Tumours that predominantly composed of granular cells with ameloblastic and/or odontogenic features have been considered a distinct entity and named it as GCOT [4]. But it was not included in the WHO 2005 classification of odontogenic tumors [1].
It occurs over a wide age range of 16- 77 years with a mean age of 45.21 years. Most of the cases were seen in the 5th to 7th decades. Female: Male distribution is 3.1:1. 72.02% of cases were reported in mandible and 27.7% in maxilla. Size of the tumor ranges from 0.5 to 8.0 cm. Duration ranges from 5 months to 19 years [2].
Some lesions are completely asymptomatic and others appear as a painless mass with localized expansion. Very few number of GCOTs that occurred in gingiva were also reported [5]. It was mainly reported in blacks and whites, Chiang et al reported a first case of GCOT in oriental people [6]. GCOT presents usually as well defined unilocular or multilocular radiolucency, with or without focal areas of opacity [5].
Histopathologically, it is characterized by sheets and clusters of round to polygonal cells with abundant, finely granular, eosinophillic cell cytoplasm and eccentrically placed nucleus without any mitoses. Peripheral cells are low columnar or cuboidal cells. Stellate reticulum like cells are absent. These features are correlating with our case. Occasionally dystrophic calcifications may be seen [1].
Meer et al suggested that the granular cells are Mesenchymal in origin (vimentin positive) and derived from a histiocytic cell line [7]. Gomes et al supported histiocytic differentiation of the granular cells, as they showed the strong expression of the CD68 [8]. Granular cells ultra structurally showed few cytoplasmic organelles and abundant electron dense intracytoplasmic lysosome-like particles [9]. Takeda et al suggested that granular changes represent degenerative or aging rather than neoplastic nature of Granular Cells [10].
Most of these cases were treated by Enucleation and curettage. These lesions were easily enucleated and recurrence rate is very less. Prognosis is good [11].
Conclusion
As intraosseous granular cell neoplasms are rare, diagnosis should be made cautiously. As the treatment plan and prognosis varied widely, when compared with that of granular cell ameloblastoma.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Otolaryngology please click on: https://juniperpublishers.com/gjo/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/gjo/GJO.MS.ID.556005.php
16 notes
·
View notes
Text
Radio-Clinical Correlation in the Management of Patients Dizzying: Proposal of a Diagnostic Attitude | Juniper Publishers

Juniper Publishers-Open Access Journal of Otolaryngology
Authored by F Alloun
Abstract
Introduction: Diagnostic management of vertigo has attracted the interest of several authors around the world, given the errors and diagnostic impasses found. The main objective of our work is to analyze the contribution of a well-established clinical diagnostic protocol compared to that of imaging in the etiological diagnosis of vertigo whether acute or chronic, and this in order to justify indications of imagery in front of a vertigo.
Materials and methods: It is a multicenter prospective clinical trial of a detailed and documented diagnostic protocol. The study populations are divided into two groups:
i. Group “A” with a number equal to 73 patients, benefiting from a detailed and documented clinical protocol.
ii. Group “B” with a number equal to 216 patients with imaging preceded by a succinical clinical examination.
Results: The positive magnetic resonance imaging rate was four times higher in group “A”; 16 out of 43 MRIs made (37.2% of the MRIs requested were pathological) compared to the “B” group; 18 out of 207 made MRI (8.69% of pathological imaging in all requested MRI). The results of the factors predictive of a central MRI lesion are quite interesting.
Conclusion: The final interest is twofold: to have a diagnostic consensus and an impact on the health economy by reducing the systematic imaging practice in front of a case of vertigo.
Keywords: Central Vestibular Involvement; Examination; Vertigo; Videonystagmoscopy
Introduction
Vertigo is a frequent reason for consultation and, according to different authors, represents 2 to 3% of admissions. Of these, more than 15% have a pejorative etiological diagnosis [1]. Data from the recent literature concerning the management of vertigo diagnosis converge towards misuse of radiological investigations [2]. Vannuci et al preliminarily evaluated the diagnostic performance of a structured algorithm: STANDING (Spontaneous Nystagmus, Direction, head impulse test, standing) to differentiate central acute vertigo (AV) and peripheral acute vertigo [3]. The main objective of our work is to analyze the contribution of a well-established clinical diagnostic protocol compared to that of imaging in the etiological diagnosis of vertigo whether acute or chronic, and this in order to propose a diagnostic attitude and therefore, justify the indications of imaging in front of vertigo.
Materials and Methods
This is a multi-center prospective prospective clinical trial of a detailed and documented, three-year (2015- 2018) diagnostic protocol. This study involved 289 patients with true vertigo. Recruited patients were separated into two groups:
a. The group of patients with a detailed clinical protocol and documented “group A” (n = 73) including a detailed interview on 53 items, the study of oculomotricity, high frequency tests using videonystagmoscopy with video recording, a neurological and general examination as well as caloric tests. Imaging was requested only based on the results of the above examinations.
b. The group of patients with imaging preceded by a succinct clinical examination “group B” (n = 216). The data was collected on a pre-established form. The data capture and exploitation were carried out with the EPI info version 6.04 software for bivariate analyzes and possibly the SPSS or Epidata software for multivariate analyzes.
Results
The research, in the group “A” of a spontaneous and provoked nystagmus by the videonystagmoscopy, objectified the following results:
i. Spontaneous nystagmus was found in 5 patients (6.85%).
ii. The Dix and Hallpike test were positive in 29/73 patients (39.73%).
iii. The head shaking test (HST) revealed horizontal nystagmus in 25 patients (34.25%), including patients with spontaneous nystagmus who all had pathological HST.
iv. The head impulse test (HIT) revealed catch-up saccades in 11 patients (15.07%), always including patients with spontaneous nystagmus.
v. Gaze nystagmus was positive in 15 cases representing 20.54% of patients (Figure 1).
In the “A” group, 16 MRIs representing 37.21% of the MRIs made, objected to anomalies, divided into:
a. 2 MRI with peripheral involvement: a case of meningeal enhancement in the left ponto-cerebellar angle involving the acoustico-facial bundle (Figure 2), a case of vascularnervous conflict between the anterior inferior cerebellar artery (AICA) and the left vestibulo-cochlear nerve.
b. 14 MRIs with central lesions distributed as follows: 05 cases of multiple sclerosis, 03 cases of Arnold Chiari malformations (Figure 3), one case of ischemic lesion of the territory of the left posterior inferior cerebellar artery (PICA) causing a cerebellar ischemic stroke, a case of arachnoid cyst
In the “B” group, only 18 MRIs representing 8.69% of MRI scans, showed abnormalities (Figure 4). Our analytical study of the different clinical parameters and their possible correlations with a central attack on MRI made the following observations:
i. The most sensitive test is the normality of the HIT cephalic pulse test with sensitivity reaching 93% contrasting with low specificity (33%) (Figure 5)
ii. The most specific test is the slow continuation during oculomotricity examination with a specificity of 90% contrasting with low sensitivity (22%) (Figure 6).
Discussion
Age
The aging of the population seems to be an important factor. Neuhauser et al (Germany 2006), on a larger population (n = 4077), show the same frequency peaks as ours [4]. Muellman (USA 2017), when he finds, rather peaks in the age group 50-69 years,which is also valid in the study of Bisdorff [5,6] (Table 2).
Etiology
Peripheral vestibular involvement was the most common cause of vertigo in most series (Table 3).
Predictive Factors
The rate of MRI positive four times higher in group “A” compared to group “B” motivated our choice of population “A” as a study model looking for clinical factors pejorative of an attack at the imagery, peripheral is so or especially central. Our study demonstrated a significant statistical relationship between the presence of neurological antecedents and central MRI (P = 0.03), consistent with literature data. Park et al, examining the records of patients with central vertigo, found that most patients (81%) complained of a neurological history of headache [7]. In our series (group A), 57% of central MRI lesions had a history of neurological symptoms. Our results are similar to those of Enass S. Mohamed who, on a series of 21 MRIs with central involvement, found 51.61% of neurological symptoms [8]. The symptom instability was found in 75% of central radiological findings by MRI in the study of H Amar [9]. He reported a statistically significant relationship (p = 0.002) between the instability symptom and the central MRI lesion, in contrast to the rotary-type vertigo (p = 0.844). The presence of oculomotricity saccades seems to have a better sensitivity and less specificity of a central MRI lesion compared to the slow continuation, sensitivity increasing from 43 to 22% and specificity from 86 to 90 %, approaching the results of the Ennas study [8] Won Gue Han [10] through a retrospective study, analyzed a series of 31 patients with vertigo of which he suspected the central origin and in whom a cerebral MRI was made. Among this series of 31 patients, 15 had perverted central nystagmus (14 had lower vertical nystagmus, and one case of superior vertical nystagmus). Among these 15 patients, 5 patients had a pathological MRI pathological, thus finding a sensitivity of 34%, close to that of our work where there is objectified at 29% [10].
Regarding the gauze nystagmus, among the few studies, that of Ennas (Egypt 2015), did not show a significant statistical relationship between gauze nystagmus and central MRI (p = 0.526). Our results concerning the head impulse test (HIT) were the most relevant. 91% of the MRI without central involvement had a pathological HIT and 93% of the MRI with central impairment had a normal HIT. DENewman Toker reported that 91% of central vascular lesions on MRI had a normal HIT (retained canal function), which is similar to our findings despite the fact that vascular lesions on MRI represented only 7% of all the central attacks of our series [11]. In his small series, Mc Dowell found that 100% of central lesions on MRI had a normal HIT [12].
According to Kattah and Toker [11] the HINTS acronym used by the Anglosaxon (Head-Impulse- Nystagmus-Test-of-Skew) representing the association: Normal cephalic pulse test (HIT), nystagmus changing direction, vertical misalignment of the ocular axes, appears to be more sensitive than MRI for acute stroke within 24 to 48 hours after onset of symptoms [13]. Vannucci et al [3] still in the emergency, tested the performance of an algorithm in 98 patients called STANDING (Spontaneous Nystagmus, Direction, head impulse test, standing) looking for a central spontaneous nystagmus, its direction, a normal cephalic pulse test (HIT) and / or an inability to stand up, to differentiate the central causes from the peripheral causes. The test had a very high sensitivity at 100% and a specificity of 94.3% for central vestibular involvement. However, still in our study, HINT or STANDING triads were not decisive in the diagnosis of a central MRI lesion, because contrary to the studies mentioned above, our work was interested in all vertigo whether acute or chronic. This allows us to suggest a triad of tests, low sensitivity certe for some of them but of good specificity, whose association would present an aid in the diagnosis of a central attack on MRI.
We immediately notice:
a. Except for the normality of the Cephalic Pulse Test (HIT) (93%), the other elements have low sensitivity for central MRI involvement.
b. The specificity for central MRI is quite high for elements such as instability-type vertigo, pathological slow continuation, neurological physical signs
Conclusion
Our study compared to that of the literature has consolidated the role of a careful clinical examination with adequate material (videonystagmoscopy) in the etiological diagnosis of vertigo and being done, decreased indications of imaging Regarding the predictors of a central cause, our results concerning the sensitivity and specificity of some clinical tests for central MRI are quite interesting. We hope to expand our series, to consolidate our results.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Organic & Medicinal Chemistry please click on: https://juniperpublishers.com/omcij/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/omcij/OMCIJ.MS.ID.555558.php
21 notes
·
View notes
Text
Nt-Probnp versus Echocardiography in the Etiologic Diagnosis of Acute Severe Dyspnea-Juniper Publishers
Abstract
Introduction: Acute dyspnea is a common presenting complaint to the emergency department (ED). Etiologic diagnosis is often difficult in the context of emergency. N terminal probrain natriuretic peptide (Nt-proBNP) and echocardiography are actually fundamental tools in the management of patients with heart failure in the ED. The goal of this study was to compare the accuracy of Nt-Pro BNP assay with Doppler echocardiography in differentiating CHF from other causes in patients consulting the ED for severe dyspnea.
Results: A total of 65 patients were enrolled in the study. The diagnosis of congestive heart failure (CHF) was retained in 44 cases. The initial diagnosis was wrong in 15 patients (23%): CHF was missed in 10 (15.38%) patients and wrongly diagnosed in 5 (7.69%) patients. The mean Nt-ProBNP concentration was 9188±6338 pg/mL in the CHF group, compared with 416±400 pg/mL in the non-CHF group (p<0.0001).Left ventricular EF was significantly lower in patients with CHF (40.93±12.2 versus 55.29±7.8, p<0.0001). Systolic left ventricular dysfunction (EF<0.45) was found in 29 (65.9%) patients with CHF and in 4 (19%) patients with other causes of dyspnea (p<0.0001). The area under the ROC curve was significantly higher for Nt-ProBNP than for EF (0.95 versus 0.83, p<0.0001). The Nt-ProBNP cutoff value of 500pg/mL had the highest sensitivity (97%) and negative predictive value (93%) but a specificity of (66%). The cutoff value of 1100pg/mL had the highest specificity (93%) and accuracy (86%) but a sensibility of (79%). Left ventricular EF had the lowest positive predictive value (66%) and accuracy (70%).The best diagnostic performance was found with the presence of ("impaired relaxation” and " restrictive pattern”) with an accuracy of 92%.
Conclusion: The major contribution of the Nt-ProBNP is the ability to rule out the diagnosis of CHF in the ED with a cutoff of 500pg/mL, above this value, it is only a fair indicator of the disease. Doppler echocardiography represent the « gold standard » in the evaluation of patients with acute dyspnea by the ability to evaluate diastolic and systolic function on one hand and to clarify the etiological diagnosis on the other hand.
Keywords: Natriuretic peptides; Heart failure; Echocardiography
Abbreviations: ANOVA: Analysis of Variance; Nt-ProBNP: N Terminal Probrain Natriuretic Peptide; CHF: Decompensated Congestive Left-Heart Failure; DT: Deceleration Time of the Mitral E-wave; ED: Emergency Department; LV: Left Ventricular; LVEF: Left Ventricular Ejection Fraction;OR: Odds Ratio; ROC: Receiver Operating Characteristic
Background
N terminal probrain natriuretic peptide (Nt-proBNP) and echocardiography are actually fundamental tools in the management of patients with heart failure in the ED. The goal of this study was to compare the accuracy of Nt-Pro BNP assay with Doppler echocardiography in differentiating CHF from other causes in patients consulting the ED for severe dyspnea.
Introduction
Acute dyspnea is a common presenting complaint to the emergency department (ED) [1,2]. Often, it is caused by decompensated congestive left-heart failure (CHF); which requires rapid diagnosis for prompt and appropriate treatment. However, this is often difficult in the context of emergency, especially in elderly [3] or obese patients [4] or those with underlying chronic lung disease [5]. The symptoms may be nonspecific, and physical findings are not sensitive enough to make the diagnosis which can have detrimental effects for the patient with the corresponding risks for under- and overtreatment [6-8]. N terminal probrain natriuretic peptide (Nt- proBNP) has been described as an important biomarker able to assess diagnosis and severity of heart failure (HF) as well as predict outcome and potentially guide therapy even in the emergency setting [9]. It has been recommended in international guidelines for the diagnosis and management of HF [10].
The use of Nt-pro BNP at the rule-out threshold recommended by The 2012 European Society of Cardiology guidelines on HF provides excellent ability to exclude acute heart failure with high specificity and sensitivity [11,12]. Despite the evidence that Nt-pro BNP is secreted in ventricular overload states, there is an individual and inter-individual variation (age, gender, race, obesity, renal function), which makes the interpretation of Nt- pro BNP levels difficult [13]. So, a careful clinical examination associated with an echocardiography examination should be complementary to Nt-pro BNP analysis for diagnostic strategy and treatment implementation [14]. Echocardiography is a fundamental tool in the management of patients with heart failure [12]. Unfortunately, it is not routinely available in the ED. The role of Echocardiography in emergency medicine as a diagnostic and a guide to therapy tool is expanding rapidly, but its value for the etiologic diagnosis of dyspnea has not been adequately studied in the emergency setting [15]. The goal of this study was to compare the accuracy of Nt-Pro BNP assay with Doppler echocardiography in differentiating CHF from other causes in patients consulting the ED for severe dyspnea.
Patients and Methods
Study design
This was a prospective cohort study of a convenience sample of patients presenting to the ED with acute dyspnea. The local ethics committee approved this study.
Study setting and population
This prospective study was performed in the emergency and intensive care department in the regional hospital of Zaghouan in TUNISIA. The patients were recruited during 7 months, from June 2015 to December 2015. All adult patients presenting to the ED for acute severe dyspnea as their main symptomwere included. As exclusion criteria we retained myocardial infarction, recent surgery, pneumothorax and chest trauma. Patients were also excluded if they had received intravenous (IV) therapy in the ED before echocardiography and NT-proBNP were performed and also if emergency echocardiography was not feasible (poor echogenicity, tachycardia, permanent pacing, or mitral prosthesis).
Study protocol
On admission, patients underwent a complete physical examination, 12-lead electrocardiogram, chest X-ray, arterial blood gas analysis, and routine blood tests. The senior physicians were asked to complete the Framingham criteria for heat failure [16]. The diagnosis of heart failure was retained at the presence of tow major criteria or one major criterion plus to minor criteria Table 1. Within 30 minutes of inclusion in the study and before initiation of therapy, blood samples for NT-proBNP assay were collected and at the same time echocardiography were performed. The treating physician was blinded to NT-proBNP and echocardiography results.
Nt-ProBNP analysis: 5-mL blood sample was immediately collected into a tube containing potassium ethylenediamine- tetraacetic acid (1mg/ml blood), centrifuged and stored at 80 °C. NT-proBNP analysis was per- formed with a commercially available immunoassay (Elecsys pro-BNP, Roche Diagnostics, Indianapolis, IN) on an Elecsys 1010 analyzer. The coefficient of variation for inter- and intraassay precision was <4%.
Echocardiographic data: Doppler echocardiograms were obtained at the bedside by cardiologists experienced in echocardiography. The left ventricular ejection fraction (LVEF) was estimated mainly by visual inspection. Diastolic indices included: the early (E) and late (A) diastolic filling velocities, the E/A ratio, and the early deceleration time (DT). Diastolic function was initially classified as:
1. Impaired relaxation: When E/A ratio < 1 with DT > 220 ms, suggesting no increase in LV filling pressures;
2. Restrictive: when the E/A ratio > 2 or E/A between 1 and 2 and DT< 150 ms, or DT < 150 ms alone in case of atrial fibrillation, suggesting an increase in LV filling pressures;
3. Normal or pseudonormal: when E/A between 1 and 2 and DT > 150 ms;
Outcome measures
A medical staff including cardiologist, pneumologist and intensivist, who were blinded to the results of Nt-ProBNP assay and Doppler echocardiography obtained on admission, established the etiology of dyspnea. They had access to ED records, clinical notes, and any additional information that became available during hospital stay. The Confirmation of CHF was based on the Framingham criteria, response to treatments (diuretics, vasodilators, inotropic agents), hemodynamic monitoring and pulmonary functional tests. Patients were finally classified as CHF or non-CHF.
Statistical analysis
Categorical data are presented as numbers (percent), and continuous data as means SD. The Students t test and the Fisher exact test were used as indicated. Group comparisons of Nt-ProBNP values were made using analysis of variance (ANOVA) with the Newman- Keuls post hoc test; p values 0.05 were considered significant. The sensitivity, specificity, accuracy, negative and positive predictive values of Nt-ProBNP assay and Doppler echocardiography for CHF were compared. We also computed receiver operating characteristic (ROC) curves to determine optimal Nt-ProBNP cutoffs. We calculated the diagnostic performance of the Framingham criteria, of Nt-proBNP, of the LVEF and of the diastolic dysfunction. The analyses were performed using SPSS 20 software.
Results
Characteristics of study patients
A total of 105 patients were eligible for the study, of whom 40 met exclusion criteria Figure 1. A total of 65 patients were enrolled in the study. The clinical and demographic characteristics of patients are presented in Table 2, according to the final diagnosis. Among these patients, 39 (60%) had severity signs and were admitted to the intensive care unit, mechanical ventilation was indicated in 10% of these (n=4). Of the remaining 26, 20 (30%) were admitted to a general medical ward, and 6 (10%) were observed in the ED. During hospitalization 6 patients (9%) died.
The mean time between the onset of acute dyspnea and inclusion in the study was 6,2 ± 3,8 hours. The diagnosis of CHF was retained in 44 cases. CHF was due to coronary artery disease (n=20), hypertension (n=14), arrhythmia (n=8), and valve disease (n=2). Non-CHF, 21 cases, was due to pneumonia (n=9), decompensated chronic obstructive pulmonary disease (n=8), severe asthma (n=3) or pulmonary embolism (n=1). The patients with CHF were older than those with dyspnea from other causes (74 years versus 64 years, p<0.05). They had more history of cardiovascular diseases such as chronic heart failure (p=0.008) and coronary artery diseases (CAD) (p=0.001). The patients with no-CHF were more likely to have a history of respiratory diseases such as asthma (p=0.019) and COPD (p=0.048). On clinical examination, patients with CHF had more symptoms (orthopnea), pulmonary rales, Hepatojugular reflux, jugular vein turgescence, third heart sound and lower- limb edema. They also had a higher incidence of abnormal ECG findings (ST-segment depression, Arrhythmia), cardiomegaly and interstitial or alveolar edema. The proportion of patients satisfying the Framingham criteria for CHF was significantly higher in patients with CHF (79.5% versus 33.3%, p<0.0001). The initial diagnosis was wrong in 15 patients (23%): CHF was missed in 10 (15.38%) patients and wrongly diagnosed in 5(7.69%) patients.
Nt-ProBNP and echocardiographic findings: The Nt-ProBNP measurement and Doppler-Echocardiographic findings were resumed on Table 3. The mean Nt-ProBNP concentration was 9188±6338pg/mL in the CHF group, compared with 416±400pg/mL in the non-CHF group (p<0.0001). Figure 2 shows box plots of log Nt-ProBNP values in each final diagnostic group. Left ventricular EF was significantly lower in patients with CHF (40.93±12.2 versus 55.29±7.8, p<0.0001). Systolic left ventricular dysfunction (EF<0.45) was found in 29 (65.9%) patients with CHF and in 4 (19%) patients with other causes of dyspnea (p<0.0001). The log Nt-ProBNP values for each quartile of EF are presented in Figure 3A for patients with CHF and in Figure 3B for patients without CHF. Nt-ProBNP concentrations were significantly higher in patients with abnormal systolic function in the two groups; and they increased with the decrease in EF. The E/A ratio and DT were significantly lower in patients with CHF, (1.24±0.72 versus 1,68±0.46, p=0.001) and (149.4±58 versus 209±40.5, p=0.03) respectively. Diastolic dysfunction was more pronounced in patients with CHF, "impaired relaxation" and "restrictive pattern" was found respectively in 17 (38.6%) and 24 (54.5%) of the patients with CHF and in only 2 (14.2%) and 3 (19%) of the patients with other etiologic diagnoses. Patients with abnormal diastolic function (n=18) had a concentration of 2250±1980pg/mL, whereas the normal subjects (n=16) had a mean Nt-ProBNP concentration of 596±345pg/mL (p<0.0001). Figure 4 shows box plots of log Nt-ProBNP values in each subgroups of diastolic dysfunction. Patients with "restrictive Pattern" had significantly higher Nt-ProBNP levels than patients with "impaired relaxation" (10323±6072pg/mL versus 5807±6140 pg/mL, p<0.001). The mean Nt-ProBNP concentrations was significantly higher in patients with systolic dysfunction than in those with diastolic dysfunction, and highest in those with both systolic and diastolic dysfunction, as it shown in Figure 5.
Etiologic diagnosis performance of nt-probnp and echocardiography: Both, Nt-ProBNP and left ventricular EF were used to differentiate CHF from other causes of dyspnea; the area under the ROC curve was significantly higher for Nt- ProBNP than for EF (0.95 versus 0.83, p<0.0001) Figure 6. The diagnosis performance of Nt-ProBNP, left ventricular EF, diastolic dysfunction and Framingham criteria was summarized in Table 4. The Nt-ProBNP cutoff value of 500pg/mL had the highest sensitivity (97%) and negative predictive value (93%) but a specificity of (66%). The cutoff value of 1100 pg/mL had the highest specificity (93%) and accuracy (86%) but a sensibility of (79%). Left ventricular EF had the lowest positive predictive value (66%) and accuracy (70%). The best diagnostic performance was found with the presence of ("impaired relaxation" and "restrictive pattern") with an accuracy of 92%. Between 500 and 1100pg/mL, Nt-ProBNP had a poor predictive value of the final diagnosis of CHF (OR 1.16, 95% CI [0.7 to 1.8], p=0.43). Fifteen (23%) patients belonged to this interval, among them 10 patients were misdiagnosed at admission. Nt-ProBNP cutoff values of 600, 800 and 1000pg/mL correctly identified 7, 5 and 2 patients respectively. The presence of diastolic dysfunction on Doppler analysis of mitral inflow correctly classified 13 of these patients and correct 8 of the 10 clinical misdiagnoses Figure 7.
Discussion
The etiologic diagnosis of acute dyspnea in the ED is difficult because of the non-specificity of the symptoms and non-sensitivity of physical, electrocardiogram and chest x-rays findings, which constitute a source of misdiagnosis [2]. In our study, 23% of patients consulting for acute dyspnea were misdiagnosed; this rate is close to that found in some studies [17,18]. According to the latest guidelines, natriuretic peptides and Doppler Echocardiography are now considered to be part of the standard workup of patients presenting with acute dyspnea to the ED [10,12]. Our results show that Nt ProBNP and Doppler Echocardiography have an important contribution to the etiologic diagnosis of acute dyspnea in the ED. Many studies have validated the high diagnostic accuracy of Nt-ProBNP in the ED [19,20]. The 2012 European Society of Cardiology guidelines for heart failure endorsed specific age independent decision cutoffs for plasma Nt-ProBNP <300pg/mL, for the exclusion of acute heart failure based on consensus of expert opinion [12]. The PRIDE (N-Terminal Pro- BNP Investigation of Dyspnea in the Emergency Department) study demonstrated that Nt-ProBNP level ≤300pg/ml was optimal for ruling out acute CHF [20]. Other studies demonstrated equal value of NT-proBNP [21]. In our study, we found that Nt-ProBNP cutoff of 500pg/mL had a high negative predictive value (93%) with acceptable sensitivity and specificity. This difference in cutoff values of Nt-ProBNP was mainly due differences in study populations. A major part of our population had a high mean age with comorbidities such us renal failure and was admitted to the intensive care unit for severe dyspnea, in contrast to the other studies [20,21]. In the other hand, a strong positive predictive value (94%), and a highest accuracy (86%) were obtained with a cutoff of 1100pg/ mL. The diagnostic value of the Nt-ProBNP was poor at values between 500 and 1100 pg/mL (23% of our patients). 40% of these patients had a final diagnosis of Non-CHF due to severe pneumonia, decompensated chronic obstructive pulmonary disease, or pulmonary embolism. Indeed, several pathologies including infectious diseases, renal failure, critical illness, cirrhosis of liver, intracranial pathologies, may be the cause of high values of Nt-ProBNP even in the absence of depressed cardiac function [22].
Secondly, our work has demonstrated the superiority of Nt- ProBNP compared to the left ventricular ejection fraction (LVEF) in the etiologic diagnosis of acute dyspnea. The calculated area under the ROC curve was 0.95 for Nt-ProBNP, compared with 0.83 for LVEF. In addition, LVEF had a poor positive predictive value (66%) and accuracy (70%). Indeed, it is now accepted that a high proportion of patients with CHF have normal left ventricular systolic function and this was the case in 33% of our patients [23]. That is why we can no longer rely solely on the LVFE for the diagnosis of CHF. Given that Nt-ProBNP is useful for the diagnosis of CHF both in patients with and without systolic dysfunction [24,25]. Combining tow-dimensional imaging and Doppler, provides more data then LVEF accurate in distinguishing between acute dyspnea due to CHF and forms due to other causes. Tissue Doppler has recently become a gold standard for diagnosing diastolic heart failure, but it requires expertise, and it is not often used or applicable in an emergency setting, especially in patients with dyspnea [24,26]. In our study, we are based on the measurement of the E/A ratio, and the early deceleration time (DT) to evaluate diastolic function. They are easy to have values in the emergency context and do not require significant expertise. Several studies have shown a correlation between the early (E) and late (A) diastolic filling velocities, the E/A ratio, the early deceleration time (DT), mitral inflow pattern with left ventricular end diastolic pressure, and pulmonary capillary wedge pressure at rest [15,17]. Nazerian et al. demonstrated that emergency Doppler echocardiography, particularly pulsed Doppler analysis of mitral inflow, is a rapid and accurate diagnostic tool in the evaluation of patients with acute dyspnea [15]. In our study, the presence of echocardiographic signs of diastolic dysfunction (impaired relaxation, normal or normalized pattern and restrictive pattern) showed a better sensitivity (94%), specificity (89%), positive predictive value (95%), negative predictive value (85%) and accuracy (92%) for the diagnosis of CHF compared with reduced LVEF and Framingham criteria. In addition, the importance of echocardiography findings is especially confirmed in the gray area of the Nt-ProBNP values largely limiting its clinical usefulness [15,17,27]. In this study, the presence of diastolic dysfunction on Doppler analysis of mitral inflow correctly classified 87% of patients belonging to that area and corrects 80% of clinical misdiagnoses.
Thirdly, Our study has revealed that Nt-ProBNP concentrations vary according to the type of heart failure. In fact, several studies have shown that the mean Nt-ProBNP concentrations was significantly higher in patients with systolic dysfunction than in those with diastolic dysfunction, and highest in those with both systolic and diastolic dysfunction [28,29]. On the other hand, we have shown that Nt-ProBNP concentrations were different in subgroups of diastolic dysfunction but all subgroups had higher Nt-ProBNP levels than patients with no-CHF. We can conclude that Nt-ProBNP concentrations increase according to the stage of diastolic dysfunction. In the first stage of diastolic dysfunction (impaired relaxation), Nt-ProBNP levels mildly increase; in a second stage (pseudonormalized filling pattern) these levels moderately increase; and in an advanced stage of diastolic 11dysfunction (restrictive filling pattern) Nt-ProBNP concentrations are markedly increased and our study supports these findings [30,31]. Therefore, Nt-ProBNP measurements can play a crucial role in the diagnosis of diastolic dysfunction. Tschope, et al. [32] concluded that Nt-proBNP reliably detects diastolic dysfunction in patients with filling abnormalities and preserved LV systolic function. The consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society incorporated the Nt-ProBNP in to the algorithm for the diagnosis of heart failure [26]. The optimal cutoff value for a diastolic dysfunction diagnosis is still unclear and we need further investigation with echocardiography to verify the diagnosis of abnormal cardiac function.
Conclusion
Nt ProBNP and Doppler Echocardiography have an important contribution to the etiologic diagnosis of acute dyspnea in the ED. In the present study, the major contribution of the Nt-ProBNP is the ability to rule out the diagnosis of CHF in the ED with a cutoff of 500pg/mL, whereas above this value and especially in the gray area, it is only a fair indicator of the disease. Thereby, Doppler echocardiography represent the « gold standard » in the evaluation of patients with acute dyspnea by the ability to evaluate diastolic and systolic function on one hand and to clarify the etiological diagnosis on the other hand. Certainly, Nt- ProBNP measurements can play a crucial role in the diagnosis of diastolic dysfunction but its interpretation should consider the echocardiography findings.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com
For more articles in Journal of Anesthesia & Intensive Care Medicine please click on: https://juniperpublishers.com/jaicm/index.php
For more Open Access Journals please click on: https://juniperpublishers.com
0 notes
Text
Total Spinal Blockage after Spinal Anaesthesia for Perianal Fistula-Juniper Publishers
Abstract
Total spinal block is one of the rare complications of regional anaesthesia. It can occur after spinal, epidural or nerve plexus block. Early detection and treatment is essential to prevent mortality. We report a case of total spinal block occurring in a man with perianal fistula after receiving uneventful spinal anaesthesia for caesarean section treated successfully with prompt cardiovascular resuscitation and general anaesthesia.
Introduction
Spinal anaesthesia is being increasing used as a mode of anaesthesia for performing treatment for perianal fistula [1]. Although it is a safe and effective means of giving anaesthesia, at times it can lead to complications like hypotension, shivering, respiratory distress, unconsciousness, etc [2]. Total spinal block is a rare complication of spinal anaesthesia. It is a life threatening complication presenting with symptoms of unconsciousness, hypotension, bradycardia and respiratory failure [3].
We report a case of total spinal block occurring in young man after receiving uneventful spinal anaesthesia for perianal treatment. The patient was successfully treated with prompt cardiovascular resuscitation and general anaesthesia.
Case Description
We report a case of 33 years old man, ASA 1 admitted for treatment of perianal fistula that has evolved since 3 years.
In surgical history, he was operated two times for perianl abcess, first time in 2012, and second time one year ago, the two operations were made under general anesthesia without any intraoperative complications. No history of any medical illness or allergy.
On pre-anesthetic examination patient was in good general condition with weight of 88 kg, height 1.80 m, and body mass index of 27.16 kg/m2. Respiratory and cardio vascular examination were unremarkable. Patient had thoracolumbar scoliosis since the age of 18 years.
Laboratory tests include: hemoglobin: 10.8 gm%, platelets count: 2.36 x 105/mm3, glucose: 0.81 mumol/, blood group: O negative.
Patient was explained about the procedure of spinal anaesthesia. During induction, patient was placed in lateral decubitus, with standard hemodynamic monitoring. At induction his hemodynamic condition was stable (blood pressure: 120 / 80 mmHg, pulse rate: 75b / min, SPO2: 100%). Intravenous access was taken in the peripheral vein of both arms with 18 G vein flow needle and prefilled with 750 ml of 0.9% normal saline. Classic single shot spinal anesthesia was given with 27G spinal needle in the first attempt level of block. Slow injection of 08mg of 0.5% isobaric bupivacaine + fentanyl 20gamma was given. His blood pressure and pulse rate were monitored every 2 minutes. After 4 minutes of spinal anesthesia, and before anal dilatation, patient started experiencing respiratory discomfort, nausea and vomiting. There was sudden fall in blood pressure (BP) to 60/30 mmHg and desaturation (SPO2: 70%) with pulse of 70b / min. Patient became unconscious. There was bilateral nystagmus, and mydriasis on pupil examination. Subsequently patient became dyspneic followed by apnea. Hence ephedrine was administered intravenously 9 mg bolus every 2 minutes along with mask ventilation with 100% pure oxygen.
The hemodynamics further worsened to unrecordable BP and SpO2 (oxygen saturation) between 60-70% despite mask ventilation. As patient failed to respond to any medication, we went ahead with rapid induction (drugs used: 300mg pentothal + 300mg gamma fentanyl + 50mg rocuronium) and orotracheal intubation. After intubation, SpO2 improved to 80-90%. But hemodynamics continued to remain unstable (systolic BP: 50-80mmHg, pulse rate: 120b / min). Repeated adrenaline injections (0.2mg / every 05min) were given along with intraoperative volume replacement rate of 2.5 macromolecules litre. Throughout the duration of resuscitation, pulmonary auscultation was normal without any evidence of bronchospasm. The diagnosis of complete spinal block was made.
After 120 minutes of continued hemodynamic and respiratory support, improvement in the hemodynamic state and respiration was noted (BP: 80-120 / 30-50mmHg, heart rate: 100-120 b / min, SPO2 90-95%)
As the hemodynamics stabilized with signs of respiratory efforts, we gradually withdrew vasoactive narcotic drugs. After 5 hours of spinal anesthesia, there was regain of consciousness with spontaneous breathing efforts. Patient kept under artificial assisted controlled intermittent ventilation and pressure support for two hours and then extubated.
Subsequently, pure oxygen was administered through the nose for 05 hours and analgesic medications were given for pain relief. Patient was discharged on postoperative day 3 without any neurological or clinical sequelae. Patient was advised to avoid spinal anesthesia in future.
Discussion
Spinal anaesthesia is one of the preferred procedures for proctology as it is safe, effective and provides good postoperative analgesia [4]. Cardio-respiratory failure after spinal anaesthesia for perianal fistula is rare. It can occur due to total spinal block, anaphylactic reaction to anesthetic drugs, etc. In the present case, since there was cardio-respiratory failure followed by unconsciousness, total or high spinal blockage was suspected. But considering the fact that the procedure of spinal anesthesia was uneventful and the drugs were used in the routine doses, the cause of total spinal block could not be ascertained.
Total spinal block has been reported after epidural test dose [5], lumbar plexus block [2], etc. It occurs because of various technical reasons like use of higher dose of anesthetics, accidental subdural puncture, rapid change of posture, etc. Thoracolumbar scoliosis may have acted as an indirect risk factor for development of total spinal anesthesia.
Conclusion
To conclude, total spinal block is a rare complication which should be kept in mind while monitoring patient after spinal anaesthesia. Immediate resuscitation with intravenous fluids, inotropic and respiratory support can help tide over the acute crisis.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com
For more articles in Journal of Anesthesia & Intensive Care Medicine please click on: https://juniperpublishers.com/jaicm/index.php
For more Open Access Journals please click on: https://juniperpublishers.com
#Juniper publishers Publons#Juniper Publishers Review#Online Publishers#Juniper Publishers#Open access Journals
0 notes
Text
Economic Evaluation of Effectiveness of Domestic Raw Materials | Juniper Publishers

Juniper Publishers-Open Access Journal of Mining Science & Technology
Authored by Katarína Čulková
Abstract
Raw materials provide profit for owner, state and mining company, as well as single region. Mentioned means that problem of evaluation of raw material deposits is very actual and necessary area. In developed market economies evaluation of reserved deposits is considered as one of the most complex, but also most important activities during finding and research of any deposit of raw material. According national strategy for permanently sustainable development of Slovakia position of natural environment and using of raw materials in Slovakia is not sustainable from the long-term view. From the view of social and economic impacts of mining we analyzed chosen macroeconomic indexes in mining. By this way we analyzed individual regions of Slovakia. Results of analysis shows that mining activity is characterized by technologically severity and high rate of human work, and by this way with regard to costs structure it presents important source of employment.
Keywords: Raw Material Base, Resource Policy, Economic and Social Impact, GDP, Unemployment, Export, Import
Introduction
Base of mineral raw materials provides in the frame of certain region the value that is possible to evaluate with optimal using complexly, and by this way profit for owner, state and mining company, as well as single region is created [1]. Profit for the state can be possible reasonable and rational using of deposits, as defined in legislation of raw materials using. Profit for mining organization can be profit creation during providing of its sustainability. Profit for the region is in the sense of administration creation of wealth for region´s inhabitants that is viewed through support of new working posts, support of regional taxes creation, or taxes, orientated directly to the region and availability of raw material sources that are necessary for region´s development. Owner of reserved deposits of raw materials in conditions of Slovakia is single state, but state does not have definite obligation to evaluate economically all recorded deposits of reserved raw materials [2].
Sector of mining and processing of raw materials in Slovakia is full privatized and state as owner of reserved deposits of raw materials creates in accord with available legislation space and conditions for business subjects for effective using of raw materials. Principle of freedom in business during observing of determined rules applies also in area of raw material using. It means that problems of evaluation of raw material deposits are very actual and necessary for business sector, as well as for private sector [3]. In developed market economies evaluation of reserved deposits is considered as one of the most complex, but also most import ant activities during finding and research of any deposit of raw material.
Market estimations of prices of deposits and raw material sources in Slovakia can exist only due to the Law about prices No 526/1990 Collection of Law. However, it would not be advisable to prescribe detailed pricing procedures for prices determination for a wide range of evaluation needs for all variants of real estate. Present mining practice shows that market estimations use for evaluation of non-monetary deposits to equity of the company mainly capital debts and warranty coverage.
State of The Problem
Presently raw materials are mining in all counties of Slovakia. Majority of mined raw materials are consuming at the regions of Slovakia. Raw materials, which present surplus in Slovakia, are exported to surrounding countries. Shortage of raw materials is imported to Slovakia important attention is necessary to give mainly to social and economic indexes, among which belong employment, GDP, average monthly wage, migration and criminality. Such indexes characterize changes, connected with inhabitants of the country [4]. Extraordinary important and necessary condition for state development is availability of raw materials [5]. Availability is perceived from physical and economic side. Using of own raw materials is either most economic or ignoring of such possibility could present ownership negation, which in case of raw materials is evaluated very significantly and directly by the Constitution of Slovakia.
According the Constitution SR raw material wealth must be protected and effectively used in connection to long-term needs of economic and social development of the society with regard to environmental aspects of sustainable development, beginning with geological research and using of verified stocks of raw materials. Process of raw materials using is subjected presently to legislation norms that divide deposits to two categories: reserved and non-exclusive. Non-exclusive deposits are characterized by attribute of ownership - owner of the land. Deposits reserved are part of raw materials wealth of the state an in the sense of the Constitution SR they are in ownership of the state and this ownership is unchangeable. Effectiveness of state ownership using is interpreted through rationality. Since raw materials are irrecoverable, state must care of their saving using with goal to provide protection and rational using of raw materials wealth as ownership of Slovakia, together with regarding of sustainability principles.
Raw materials wealth of Slovakia provides rather broad scale of raw materials from the view of volume and quality of stocks, proper mainly for production of products on base of non-metallic and construction materials that present economically most important group in structure of raw materials wealth of Slovakia [6]. One of the most important tasks in the future should be increasing of processing level and products finalization on base of non-metallic raw materials.
Stocks and quality of ore raw materials, as determining factor of their using, prove their decreasing economic importance in structure of raw materials wealth of the country. Similarly, domestic energetic sources (except brown coal and lignite) have due to the volume of imported commodities only small importance. Total rate of value of raw materials mining on GDP is negligible (0,5%), but this statistic data does not include value of consequently processed and adjusted commodities on mineral base that is multiply higher and it presents significant element in the economy and foreign trade of Slovakia [7].
Methodology
Due to the evaluation of present state of raw materials in Slovakia there is necessary to limit position of mining sector according classification in conditions of Slovakia. According SK NACE Rev.2, published by Statistic Office of Slovakia, official indication of mining industry is in section B - Mining and quarrying. The sector includes include mining of minerals, appearing naturally as solid minerals (coal and ores), liquid (petroleum) or gas (earth gas). In the frame of mentioned section there are divisions 05-06: mining and quarrying of fossil fuels (coal, lignite, petroleum and gas), division 07-08, including: mining and quarrying of metal ores, various minerals and stone [8].
In spite of historic tradition in mining and processing of ore raw materials, presently Slovakia does not belong among states with developed mining industry. According UN for development and business (UNCTAD) to category of states with developed mining industry belong states, in which rate of mining and processing of raw materials on GDP is higher than 25%. According national strategy for permanently sustainable development of Slovakia position of natural environment and using of raw materials in Slovakia is not sustainable from the long-term view. Present situation of raw materials base in Slovakia is characterized almost by total exhaustion of ore raw materials stocks, big stocks, but different measure of non-metaling and construction materials using, as well as total limitation by state control over mining. Influences to the country and living environment, caused by mining, are vast. Such influences present only one of the most serious environmental problems of Slovakia (Government Resolution, SR, 2001). Sector B - Mining and quarrying due to the reporting from the side of Statistical Office SR, is mentioned in the analysis as part of aggregated sector Industry in Total.
From the view of social and economic impacts of mining it is important to follow up mainly employment and wages in mining. Also, there is necessary to search development and placement of mining companies in Slovakia. By this way we analyzed individual regions of Slovakia. By the way of obtained social and economic indexes we made analysis of macro environment and analysis of mining industry. Due to the evaluation of development we followed up influence of mining industry to GDP, employment and wage (due to the extend analysis we will mention only results and conclusions of analysis).
Results
From the Table 1 there is obvious GDP development in sector Industry Total and Production remained during whole period rather stable. In last period there is gradual decline of mining activity due to the growth of input prices to mining activity process and activity, made by mining and last but not least also due to the consequences of economic crisis in Slovakia and in the world (Table 1).
All stocks of raw materials in Slovakia are divided to four groups to following stocks:
• Energetic - petroleum, coal, earth gas, uranium, lignite, anthracite, bituminous rocks,
• Ores - iron, copper, lead, zinc, antimony, mercury, silver, gold, etc.
• Non-metallic - barite, bentonite, quartz, magnesite, talc, etc.
• Construction - building stones, gravel, bricks, etc.
• Other - mineralized waters, pyrites [9].
Deployment of raw materials deposits in Slovakia is uneven. It depends mainly on geologic construction of the locality. Raw materials mined in Slovakia are determined mostly for domestic consumption. Slovakia import from abroad prevailingly petroleum, earth gas, black coal, iron ores, and raw materials for metallurgy [9]. Mining of raw materials is characterized by high rate of human work; therefore, it presents very good source of employment, but on the other hand it is less profitable. Total value of profit achieved in analyzed period 330 million EUR, which presents 0, 46% of total GDP.
From total mining in Slovakia 12, 5% belongs to fuel and energetic materials, 2, 1% to ores, 85, 4% to non-metallic materials. Production of majority of non-metallic and construction raw materials (magnesite, limestone, dolomite, gypsum, building stones, etc.) covers considerably their domestic consumption. Raw materials and products on mineral base present important element of foreign trade of Slovakia. Important element of imported mineral materials belongs mostly to fuels (petroleum, earth gas, black goal) and ores raw materials (iron ores, raw materials for aluminum metallurgy, steel and ferry-alloys). As for the materials, produced on mineral base, Slovakia exports mostly iron and steel, aluminum, ferry-alloys, magnesite, concrete, bentonite, dolomite and other products mostly from non-metallic raw materials. From seven types of registered energetic raw materials (petroleum, earth gas, brown coal, lignite, uranium ores, anthracite, and bituminous rocks only four types are industrially used - petroleum, gas, brown coal and lignite [10,11]. Economic importance of uranium ores, anthracite and bituminous rocks is negligible due to their volume and quality. Slovakia has limited stocks of energetic sources, mainly petroleum and earth gas.
Main goal of raw materials potential searching in Slovakia is geologic task in accord with analysis and evaluation of chosen ores and other raw materials from the view of their importance for Slovakian economy - possibility of their using from the view of stocks volume, their quality, possibility of replacement, structure of demand and offer, as well as identification of weaknesses and strengths (SWOT analysis) of individual types of raw materials. According evaluation of raw material potential according chosen parameters, raw materials will be identified (resp. individual deposits objects) that are strategic for Slovakian economy and that are economically perspective for further using. Results of the task should serve as frame base for decision about using of evaluated raw material sources in the future.
Export and import and its economic and social impacts
Mining and quarrying in Slovakia provides important inputs mainly for processing industry and energetics. But stocks of raw material and energetic materials are limited in Slovakia greatly. While as for the fuel and energetic and ores raw materials Slovakia is dependent on import, mining of several types of raw materials for industry and construction has positive economic importance.
Mining of brown coal and lignite covers domestic consumption approximately 80%. In the frame of energetic policy of Slovakia domestic sources of brown coal and lignite are considered as strategic raw material base, decreasing dependence on import of primary fuel and energetic materials, and as reserve in case of unpredicted situations and source of working possibilities. Due to the verified geologic stocks of petroleum and earth gas there is not possible to expect in the future considerable increasing of domestic mining volume and therefore it will be necessary to provide such commodities still by import.
Slovakia presents after Ukraine second biggest transition country of earth gas in Europe. Main attention will be orientated in the future in connection with gas market liberalization to increasing of quality of services, connected with earth gas stocking. Primary task would remain decreasing of energetic demand to level of EU countries. Regarding high production costs of mining and processing of domestic ores raw materials the mining is not profitable. Necessary ores commodities are provided by import. On the other hand, reserved deposits of non-metallic raw materials present most important group of raw materials in Slovakia.
In 2015 geological stocks of reserved deposits achieved level 16 605 mil. tones with considerable prevalence of non-metallic raw materials (12 586 mil. ton). 2015 presented year with smooth increasing of construction and non-metallic materials mining. From the long-term trend (2000-2015) there was significant decline of ores materials mining (by 95,3 %) and decrease of energetic materials mining by 50, 5%. On the other hand, growth had been recorded in mining of non-metallic materials (by 9%) and construction materials (by 49 %). In 2015 rate of energetic materials mining to stocks presented 0,16 %, ores materials presented 0,01 %, and non-metallic materials 0,09 %, construction materials - 0,62 % (Ministry of Living Environment, SR, 2016). Chosen financial indexes in Mining and quarrying is given by (Table 2).
Most important non-metallic materials from the view of export are magnesite, dolomite, stone solt, bentonite, limestone, and baryte. Magnesite industry with verified geologic stocks of magnesite and built mining and processing capacities belong to most important producent of alkaline refractory materials in the world (Ministry of Economy SR, 2004). Petroleum is mined in Slovakia mostly in deposits Gajary and Dúbrava, gasoline in eastern Slovakia (Senné, Stretava, and Ptrukša). But total consumption of the materials is covered rather by import, since rate of domestic production on consumption presents only 1% (Table 3).
Earth gas is obtained mainly from deposits in eastern Slovakia (approximately 70% of mining), remaining production is from deposits in Viedenská panva and Podunajská nížina. Production of gas from Slovakian deposits covers only approximately 3% of consumption and therefore it must be provided by import. Single producer of oil and earth gas is presently Nafta, Joint Stocks Company. Due to the volume of verified stocks of oil and earth gas this situation would be probably not changed in the future. This means permanent dependence on import. Mentioned is illustrated by data in Table 4.
Mining of brown coal is realized at deposits in Handlová, Cigeľ, Nováky (Hornonitrianske bane, a.s.) and Modrý Kameň (Baňa Dolina, a. s.). Lignite is mined at deposit Gbely (Baňa Záhorie, a. s.). Biggest domestic consumer of energetic coal and lignite presents Power plant Nováky, part of the production is consumed by Heating plant and chemical industrial plants (Chemko Strážske). Domestic mining covers consumption of brown coal at level approximately 80% (Table 5). Dependence on black coal import is permanent.
Mining of building stone moves in last years around 9 mil. tones per year and it has increasing trend. Most important producers of building stones in last period was Slovenský vodohospodársky podnik, š.p., Stredoslovenské kameňolomy, a. s., Doprastav, a. s. and Malokarpatské štrkopieskovne, a. s. Most important producers of gravel were lastly Alas Slovakia, spol. s r. o., VSH, a. s. (Betox, spol. s r. o.) and V.D.S., a. s., which provided together almost 70% of total gravel production in Slovakia (Table 7).
Development of number of companies in mining industry
During analysis of mining sector, it is appropriate to follow up number of rising and terminating mining companies in Slovakia. Table 8 illustrated total number of mining companies in individual counties. Data are obtained and available only for period 2010- 2015.
Most companies orientated to the activity of mining and quarrying were in 2014 in county Banská Bystrica. In 2015 there was recorded most companies in Bratislava county, yet 42 companies. The least companies are appearing in county Trenčín. Total number of companies in mining industry in Slovakia was in 2015 with total number 187 companies. From 2013 the number of these companies is gradually increasing. It is ideal from the view of mining, sales and new working posts increasing in mining sector. Figures 1 & 2 illustrates number of rising and terminated companies in mining and quarrying industry in Slovakia during analyzed period.
According Figure 1 we can see that in mining industry there is gradually increasing number of rising new companies and on the other hand smooth decrease is recorded for number of terminated companies, illustrated by Figure 2. It means positive situation for mining sector. By this way we can state that mining in Slovakia is still developing.
Development of employment in mining industry
Important index during analysis of the sectors is employment in mining. Average registered number of employees in mining industry for all Slovakian counties is illustrated by Table 9. The index is followed during 2010-2015.
From Table 9 there is obvious the majority of workers in mining and quarrying industry is in county Trenčín. In 2015 3 852 employees worked in the industry. It is caused by the way that mainly in this county the biggest employer is company, mining brown coal and lignite. From 2010 the least number of employees in mining were in county Nitra. Comparing of development of average number in individual sectors is given by Table 10.
We can say that in all sectors, illustrated by Table 10 average number of employed persons had decreasing tendency. From total industry the least number is employed in mining and quarrying industry, which in 2015 employed only 6 742 persons. The biggest number of employed were in industrial production [8].
Sales in mining industry
In mining industry there is important to follow up also development of sales that is illustrated during analyzed period 1990- 2015 by Figure 3. Values of the index are calculated by actual exchange rate.
According Figure 3 we can state that from 1990 sales had been gradually increasing. Smooth decrease of sales was recorded in 2005, but in following years sales repeatedly increased. In 2015 sales in mining industry were around approximately level 544mil. €. From the view of sales there is important to follow up sales from raw material mining. Figure 4 shows development of raw materials mining in Slovakia during last 25 years.
During analyzed period the highest volume of mining was recorded in 2005 at level 34, 6 mil. tones. From 2005 mining of raw materials decreased in Slovakia smoothly. In 2015 Slovakia mined 29, 6 mil. tons of raw materials.
Discussion and Conclusion
Effectiveness of raw material using is changing in accord with internal and external factors. Internal factors are as follows:
I. Volume and quality of verified geologic stocks on concrete deposits,
II. Mining and geological conditions of mining,
III. Development of industrial infrastructure in surroundings of raw material occurrence and its placement of the market,
IV. Local, mostly environmental conditions,
V. Aim to realize other activities in the territory.
External factors are as follows:
i. Liberalization of market with commodities with mineral origin,
ii. Prices of similar raw materials in world markets,
iii. Availability of raw materials and possibility of their replacement from domestic source, including secondary raw materials.
Raw material policy must respect principles of social and ecologically orientated market economy during mining and processing of raw materials and to regard also saving using of natural resources. Mining activity characterized by technologically severity and high rate of human work, and by this way with regard to costs structure it presents important source of employment. In spite Slovakia is small country, it has own rich sources of raw materials. Mining is participating at GDP in Slovakia. Majority of mined raw materials is consumed in domestic market, as for example building stone, dolomite, gravel and sand. Mostly petroleum, earth gas, iron ores and black coal are imported to Slovakia. Among positive impacts of mining belong increasing average monthly wage in the sector. People automatically with increasing wage have a need to buy more and more products and services for providing of their needs, which can be met by using of raw materials.
Decrease of employment in mining can be considered as negative social and economic impact of mining activity in Slovakia. New companies purchase Technologies, by which they increase volume of mining, sales of products, and at the same time number of employees is decreasing. Further reason for employment decreasing in mining can be due to the disinterest of people to make such physically demanded job. By mining activity is influenced mostly living environment and inhabitants of the country. Mining of raw materials influences living environment mainly due to the change of relief and soil covering. Inhabitants, living in surroundings of mining works are influenced by too high dust and noise, which can cause rising of various illness. In spite of negative influence of mining there is necessary to support the sector from the side of state, since demand for raw materials in increasing by every year.
Estimation of life cycle of several stocks in Slovakia is over 200 years. Problems of raw materials using in Slovakia is fully reflecting in accord with available legislation of treatment with raw materials. Such treatment is documented through processes that are included in raw materials policy. In spite the policy is given at the level of state, it includes only general declarations that are not possible to use and realize effectively without institutional tools. In spite of mentioned the policy gives the frame that is obligatory and inspiring.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Mining Science & Technology please click on: https://juniperpublishers.com/imst/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/imst/IMST.MS.ID.555553.php
32 notes
·
View notes
Text
Perceived Self-Efficacy and Academic Achievement among Jordanian Students | Juniper Publishers

Juniper Publishers-Open Access Journal of Technical & Scientific Research
Authored by Adnan Yousef Atoum
Abstract
The current study aimed at exploring the relationship between perceived self-efficacy and academic achievement among a sample of Jordanian secondary stage students through identifying the levels of perceived self-efficacy among students and identifying the effect of gender and academic achievement on self-efficacy. To achieve the study aims, the researchers applied the perceived self-efficacy scale on (356) secondary stage students and collected information on students’ gender and academic achievement. The results of the study showed that the majority of students hold a moderate level of perceived self-efficacy in terms of the total score and in all domains scores of the scale. Also, the results showed a significant effect of academic achievement on perceived self-efficacy in favor of higher achievement students. In addition, the results showed no significant effect for gender or the interaction of academic achievement and gender on perceived self-efficacy. The results were discussed in terms of developmental and social aspects of the sample.
Keywords: Self-efficacy, Educators, Positive social interaction, Social reinforcement, Psychological processes
Introduction
Awareness of one’s self dictates behavior, beliefs about abilities, task achievements and anticipation of success or failure. Bandura [1] has originally believed that self-efficacy mediate the relationship between an individual belief in terms of success or failure and actual behavior when performing a particular task. Self-efficacy is defined as the beliefs about individuals’ capabilities to produce designated levels of performance that exercise influence over events or tasks that affect their lives [2]. Self-efficacy beliefs determine how someone feels, thinks, and behave. Educators often note how strong sense of efficacy may affect students’ accomplishment and personal well-being. Students with high levels of self-efficacy are more likely to be certain about their capabilities when encountered by difficult tasks because they see that as a challenge rather than a way to avoid such difficult situations.
However, perceived self-efficacy can either enhance students’ capabilities or decrease them. Those who have strong perceived self-efficacy will be able to analyze their problems and reach better solutions while those with low perceived self-efficacy will have doubts about their abilities and avoid initiating successful solutions especially in difficult situations [3]. This concept implies that self-efficacy is learned and can develop over age through positive social interaction and proper social reinforcement [4-5]. Bandura [6] stated that most of the research conducted showed that self-beliefs of efficacy affect human functioning on four major psychological processes. First, most human behavior is regulated by forethought embodying valued goals because personal goals are influenced by self-appraisal of capabilities. Second, self-efficacy plays a major role in the self-regulation of motivation because most human motivation is cognitively generated and forms beliefs about what they think they can do. Third, highly perceived self-efficacy affect people’s beliefs in their coping capabilities and how much stress or anxiety they experience in threatening or difficult situations. Finally, highly perceived self-efficacy enables individuals to create beneficial environments and choose the individuals whom they can exercise some control during social interaction. Therefore, beliefs of personal efficacy can shape the course of social interaction and the types of activities and environments people choose.
Bandura [2] also identified several sources of self-efficacy. The first and strongest source stems from mastery experiences since successes build a robust belief in one’s personal efficacy and failures undermine it. The second source stems from modeling since seeing people similar to oneself succeed by sustained effort raises one’s beliefs that one also has similar capabilities and can succeed; similarly, observing others fail regardless of high effort lowers one’s judgments of their own efficacy and undermines their efforts. Social persuasion is a third source of strengthening people’s beliefs that they have what it takes to succeed. Students normally will do better if they are persuaded verbally that they possess certain capabilities in a particular task and are likely to perform better than students who have self doubt and focus on their personal deficiencies when facing a new task. The last source of successful efficacy comes from individuals’ positive appraisals and self-improvement because those who have positive selfefficacy can structure situations that bring success and avoid placing themselves in situations where they may fail. Schunk [7,8] found that self-efficacy research is viewed in domains relevant to education and several studies have addressed cognitive skills, social skills, motor skills, and career choices and have shown that self-efficacy is an important construct that helps to explain students’ learning and performance of academic achievement. Such studies also have identified variables that are associated with educational contexts and that signal to students how well they are achieving or making progress in learning.
Marat [9] indicated that self-efficacy is viewed as a multidimensional construct that shares a reciprocal relationship with various determinants of learning and academic achievement. These determinants included motivation, strategies, cognitive strategies, resource management, self-regulated learning, meeting others’ expectations, and self-assertiveness. Several studies revealed that students with highly self-efficacy capabilities showed better abilities in solving difficult tasks, more initiatives, less risk taking, more persistent, ambition and more emotional or social stabilities [9-12]. Other studies have shown a positive relationship between students’ self-efficacy capabilities and academic achievements among school and university students; those who have higher perceived self-efficacy usually have better academic achievement [13-16]. Few studies showed that there was no significant relationship between perceived self-efficacy and academic achievement [4,17-19].
The present problem
Students with high self-efficacy capabilities are considered better in solving problems, work harder on difficult tasks, face more initiatives, take less risk, and show signs of persistent emotional and social stabilities. Most of the previous research has shown that perceived self-efficacy is an important factor that helps to explain students’ learning and performance of academic achievement in Western cultures. Furthermore, academic achievement could be a determinant of self-efficacy, therefore, the present study aim at exploring the effect of academic achievement and students’ gender on perceived selfefficacy among a sample of Jordanian secondary stage students. Also, the present study will attempt to identify the levels of perceived self-efficacy among students. In other words, the present study will answer the following questions:
a. What is the level of perceived self-efficacy among a sample of Jordanian secondary stage students?
b. What is the effect of academic achievement and student’s gender on perceived self-efficacy scores among a sample of Jordanian secondary stage students?”
Significance of the study
The significance of present study stems from the fact that it explores the relationship between self-efficacy capabilities and students learning and academic achievement. It brings more attention to the self-efficacy as a construct which shares a reciprocal relationship with various determinants of learning and academic achievement. Regardless of the many international studies on the topic, the authors have not found any direct studies on the relationship between perceived selfefficacy and academic achievement among school students at the Jordanian or Arabic regional level. Some local studies have attempted to study the impact of perceived self-efficacy on various factors such as depression and anxiety [20], moral development [21], need for achievement and adjustment [22], and locus of control and adjustment strategies [23]. Therefore, the present study will explore this relationship among a Jordanian sample and put some recommendations to teachers based on the results.
Operational definition of terms
Perceived Self-Efficacy: Students’ estimation of their expectation towards abilities as measured by the perceived self-efficacy scale.
Academic Achievement: Students’ CGPA at the End of the previous year based on school records.
Method
Population and sample
The population consisted of all secondary stage students enrolling in the 1st Irbid directorates of education in Jordan that were estimated at 7968 students (4090 males and 3878 females). The sample consisted of 356 students (210 males and 155 females) and was chosen randomly using sections in various schools as a unit of assignment.
Study instrument
To achieve the present study goals, the researchers adopted A Jordanian version of Perceived Self-Efficacy Scale developed by Al-Saqer in 2005 [21]. The scale consisted of 70 items distributed among nine domains (emotional, social, behavioral, self-confidence, confidence among others, persistent, cognitive, academic, and moral). Students rated each item using a 4-point Likert type scale ranging from 4-1 where (4) represents a high perceived self-efficacy and (1) represents a low perceived selfefficacy.
Validity of the scale: The original Jordanian scale was validated through construct and content validity procedures. To re-ensure the validity of scale, the researchers presented the original scales to 10 psychologists in Jordan. Proper changes were made to ensure good content validity based on agreements of 80% of judges.
Reliability of the scale: The original Jordanian scale was tested to be reliable through testretest method. However, the present researchers have ensured more reliability measures by distributing the scale to an independent sample of students (35 students) from the same population. Alpha score was (.91) for the whole scale, and scores ranged from .82 to .90 to all nine domains of the scale.
Study procedures
the sample in groups, where each section chosen was treated as a group and each group ranged from 25-30 students. The researcher explained the purpose of the study and gave them instructions in how to rate each item in the scale. The researcher also gave one example on the blackboard in order to help the students understand their task. The researcher answered any questions raised by the students and collected the scales from the students allowing an average of 35 minutes to complete the task. Students General CGPA for the year 2007- 2008 was collected from school records. Gender of the students was decided in advance since all schools used were not mixed gender schools.
Results
The results of this study are presented according to the study questions.
First
To answer the first question regarding “What is the level of perceived self-efficacy among a sample of Jordanian secondary stage students?”, frequencies, percentages, means, and standard deviations for students’ ratings on the perceived selfefficacy scale are shown in (Table 1). Table 1 shows an overall mean of (2.71) and means for scale domains ranged from (2.42) to (2.81), which suggests a moderate level of perceived selfefficacy among the sample for the total score and among all domains of the scale. Frequencies and percentages showed that (346) out (356), with a percentage of (97.2%), have scores on the total sore of the perceived self-efficacy scale in the moderate level. Percentages of the moderate levels for all domains scores of perceived self-efficacy scale ranged from (73-89%). Results also showed that the highest scores on perceived self-efficacy came from the social domain with a means of (2.81) and least scores came from the cognitive domain with a means of (2.42).
Second
To answer the second question regarding “What is the effect of academic achievement and student’s gender on perceived self-efficacy scores among a sample of Jordanian secondary stage students?”, means and standard deviations for total scores of perceived self-efficacy scale based on achievement and gender were observed as in (Table 2). The results in Table 2 showed that females means (2.72) were slightly higher on perceived self-efficacy than males (2.70), and high achievement students (2.73) have higher means than average achievement students (2.71) and low achievement students (2.67). Two-way analysis of variance (ANOVA) was used to test for statistical significant differences in perceived self-efficacy due to variation in academic achievement levels and students gender as in (Table 3).
Using analysis of variance Table 3 showed that academic achievement has a significant effect on perceived self-efficacy F, (2, 374),= 4.41 p<0.05, while gender had no significant effect on perceived self-efficacy (F, 1, 374, =.1,18 p
Discussion
Results of the first question revealed that secondary stage students achieved a moderate level of perceived selfefficacy scores on the total scale and all domains of the scale. These findings are consistent with student age and stage of development, and development theories would suggest that students should be at a moderate level of beliefs about their capabilities since more experiences and practices are still yet to be achieved before the majority of them can reach high levels of self-efficacy. Consistent with these findings, students at this age face lots of social and emotional problems, which may reflect on their thinking processes, and concentration levels, which in turn affect their self awareness of such capabilities of self-efficacy. Furthermore, some social and cultural factors regarding the strict socialization processes and limitations emerging from traditional Muslim society could contribute to explanation of these moderate levels of perceived self-efficacy during this stage of student’s lives. Previous findings in similar contexts showed similar results. Al-Saqer [21] in a study on the relationship between self-efficacy and moral development and Al-Muhsin [22] on a study on the relationship between self-efficacy and need for achievement and adjustment showed moderate levels of self-efficacy among college students.
Results also showed a significant effect of academic achievement on self-efficacy among a sample of secondary stage Jordanian students. This result means that high academic achievement is an important factor in explaining perceived self-efficacy. Thus, it is logical to assume that high achievers produce better beliefs about their capabilities and ability to perform various tasks. High achievement obviously helps students in terms of how they feel, think, and behave in various life situations which in turn reflect positively on perceived selfefficacy. Most learning theories would support the previous findings because previous success experiences in academic achievement are expected to influence the way students feel about themselves and consequently they develop a sense of self confidence. It also help students positively evaluate various events in t heir lives and avoid negative effects due to difficult or failing experiences and eventually would increase their perceived self-efficacy. The previous finding on the effect of academic achievement on students’ self-efficacy capabilities is consistent with the majority of the previous research on secondary and college stage students [13-16]. Results also showed no significant effect of gender and the interaction between gender and academic achievement on perceived selfefficacy. This suggests that self-efficacy capabilities or beliefs are possibly more influenced by strict social and emotional socialization processes for both males and females. This issue needs further investigation since there is some disagreement on the nature of the differences in perceived self-efficacy due to gender [22,24].
Teachers are recommended to pay more attention to students’ perceived self-efficacy and should recognize the relationship between self-efficacy and academic achievement. Perceived self-efficacy is an important construct that helps to explain students’ learning and performance in general, and to recognize that both variables are associated with enhancing educational success [25-27]. The present findings require teachers to give more attention to lower achievers in order to avoid lower perceived self-efficacy or negative self evolution due to failure or expected difficulties in various academic tasks and to provide students with proper successful experiences that would enable students to avoid developing low selfefficacy. Teachers should also take advantage of students’ high achievement or various experiences of mere success by directing and guiding them toward producing better beliefs about their capabilities and developing a high sense of efficacy toward themselves as a result of such successful experiences. Small successful experiences can be useful in strengthening students’ attitudes and beliefs about themselves and their capabilities.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Technical & Scientific Research please click on: https://juniperpublishers.com/ttsr/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/ttsr/TTSR.MS.ID.555602.php
19 notes
·
View notes
Text
An Innovation in Practice for the Agency for Healthcare Research and Quality (AHRQ): Initiative for a Comprehensive Foot Examination across Health Care Settings Diagnostics and Treatment | Juniper Publishers

Juniper Publishers- Open Access Journal of Nursing & Health Care
Authored by Michele Burdette Taylor
Opinion
Diabetes and heart disease have now superseded cancer deaths in the United States of America. Disease, disability, end-of-life care, and co-morbidities are expensive and devastating. Utilizing a Certified Foot Care Nurse (CFCN) has tremendous potential for meeting the challenge of reducing wounds leading to amputations. Our national goal is to improve health care, remove barriers, and focus on the aging obese Medicare population in efforts to reduce costs and improve care. Medicare programs focus on preventative care where, Certified Foot and Nail Care Nurse (CFCN) may assume a key role in reducing the costly impact of care for people with diabetes, lower extremity arterial disease, and osteoarthritis. Since 1993, Medicare has provided coverage for a pair of shoes and three sets of inserts annually. Since 2006 Medicare took the first step towards “pay for performance” reimbursements, a voluntary program for reporting data about care delivered and referrals for the Therapeutic Shoe Bill. CFCN’s may be the key proactive preventive partner to reduce ulceration, facilitate patients’ footwear fitting and use, and implement use of over-the-counter compression socks.
Nurses’ are primed for increasing preventive information and knowledge for Medicare beneficiaries and appropriate and timely referrals for early intervention and saving Medicare money. This initiative for innovation in practice is in direct response to the Institute of Medicine (IOM) and the Agency for Health Care Quality Research (AHRQ). The AHRQ and IOM have charged nurses to practice to the full extent of their education and training and develop innovative health care proposals to specifically to lead change, improve care, and reduce costs. The significance of this innovative idea is that reimbursement should reward interventions that are therapeutic and reduce utilization. The estimated cost of a foot ulcer is $4,595 per episode to nearly $28,000 per Medicare Beneficiary with national cost of $5 billion. The estimated cost of a Lower Extremity Amputation (LEA) is $30,000 per event with total national cost of $1.6 billion, with the added costs of prior ulcer care costs exceed $6 billion annually.
The evidence supports the fact that the primary and secondary interventions to prevent a foot ulcer, is a comprehensive foot exam and daily use of therapeutic shoes. Nurses are the leader in health care for proactive prevention. Education and referral to prevent hospital readmissions, by focusing on those with Lower Extremity Neuropathic Disease (LEND) and Lower Extremity Arterial Disease (LEAD) is complicated, but by identifying patients at risk and qualifying the degree of risk, while monitoring the HbA1c for tight glucose control may reduce the number of non-traumatic amputations in the USA. Falls due to LEND and LEAD is also very serious, so monitoring the beneficiaries is also important. With a comprehensive foot exam of patients admitted in any setting, determining loss of protective sensation (LOPS) and compromised blood flow allows for early detection, treatment protocol implementation, education, and referral. Certified Foot Care Nurses (CFCN) by their training and certification are responsible for conducting a comprehensive lower extremity assessment, providing education, surveillance, and referral so patients are aware of actual or potential complications and encouraged to inspect their feet daily. Nurses’ report and facilitate care at the first sign of a complication (no matter how minor) to prevent problems developing into more serious and expensive issues. A comprehensive foot exam can be done in 10-15 minutes, focusing initially on loss of protective sensation (LOPS) and lower extremity arterial disease (LEAD). At the same time, Medicare beneficiaries are educated about foot care, daily needs, and problems to report. The benefits of utilizing a Certified Foot Care Nurse (CFCN) are numerous. With a high population of aging people with diabetes, heart disease, and obesity, utilizing a nurse to assist with management of foot issues improves the chances of reducing a lower extremity wound and subsequent amputation. It is prudent to structure care in any setting to incorporate foot care at a basic level intervention.
Foot care nurses are monitoring their clientele every 8 weeks routinely, as a service for nail debriding, reducing corns and calluses, and monitoring blood values and foot wear. The major aspects of most benefit are if the CFCN is utilized as a member of the multidisciplinary team. The IOM also insists that nurses be full partners in the care of the Medicare beneficiary. By conducting a comprehensive foot exam, directing care and attention to any wounds, injuries, or infections, while serving as triage is crucial to the overall goal of addressing needs efficiently and costeffectively. Education, repeat education, and reinforcement utilizing motivational strategies and a variety of teaching methods allows for greater dissemination and acquisition of knowledge.
The CFCN conducts a tactile and vibratory sensation examination on every Medicare beneficiary using a 5.07 / 10 gram monofilament and 128 mHZ tuning fork. Detecting neuropathic changes and instituting corrective therapy and safety precautions such as medicine management, monitoring HbA1c, gait analysis, and pain management helps prevent the initial injury of the lower extremity. Conducting the non-invasive vascular assessment to include Doppler pulses, performing an Ankle-Brachial Index (ABI), and Toe Pressures (TP) identified those with vascular compromise and possible future cardiovascular insult.
Lower extremity arterial disease is common with people with diabetes, those over 70 years of age, and/or those between 55- 70 years of age who have a history of smoking. Appropriate and immediate referral to a vascular specialist is considered early intervention, in the prevention of amputation. Palliative care and triage are also critical to limb preservation and promotion of comfort for sustaining quality of function and safety. Mobilizing the CFCN can be crucial to early detection, education, and referral. By assessing any signs of infection, dermatologic, musculoskeletal, neuropathic, and vascular status, patients can identified and fasttracked to the appropriate intervention and specialty. Education has always been the best method of wound and amputation prevention. Nurses, as the most trusted health care provider, are a natural fit for people with diabetes and the older population. Trusted communication, rapport, and sustaining relationships for the long – term allows for transferring of knowledge while demonstrating care, compassion, and competency. Providing information in a variety of formats, using adult learning principles, and incorporating a weekly phone call to check on the beneficiary is interpreted as caring and assists in ensuring cooperation among patients and caregivers.
Utilizing the Wound Ostomy Continence Nurses’ Credentialing Board (WOCNCB) Certified Foot and Nail Care Nurse (CFCN) raises the standard of care substantially and reduces overall costs to life, limbs and Medicare dollars. This innovation in practice to improve health care delivery includes, diagnostics and intervention that focuses on early detection of LEND and LEAD and intervention by, initially conducting a 10-15minute comprehensive foot exam. This proposal is a simple innovation in diagnostics and treatment that could have tremendous positive outcomes nationwide.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Nursing & Health Care please click on: https://juniperpublishers.com/jojnhc/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/jojnhc/JOJNHC.MS.ID.555767.php
17 notes
·
View notes
Text
Bias Correction of Nonlinear Effect for Longitudinal Data | Juniper Publishers

Juniper Publishers-Open Access Journal of Biostatistics and Biometrics
Authored by Yuanzhang Li
Abstract
Studying change from baseline measure in longitudinal data promises to lead to early identify a disease which would benefit both patients and society. The effect of antibody or biomarkers is certainly non-linear for human disease. Using longitudinal data and categorizing the first measurement may help to evaluate the non-linear effect, but it could confound the values of repeated measures and generate bias. We developed modeling strategies for case-control longitudinal studies to estimate and correct the bias. We use this approach in a military dataset to evaluate the association of antibody risk of developing schizophrenia. Cases and matched controls were grouped into categories by 50th and 75th percentile of the first sample of cases. The bias generated from such confounding is corrected by simulation to develop unbiased estimation. Seven antibody agents were studied. This proposed approach can aid investigators to identify risk factor in the pre-clinical period, and it can be extended to other longitudinal studies. Note: The views expressed are those of the authors and should not be construed to represent the positions of the Department of the Army or Department of Defense. None of the authors have any associations, financial or otherwise, that may present a conflict of interest.
Keywords: Bias correction; Longitudinal; Case control; Simulation; Confounding; Schizophrenia
Introduction
Case and control studies are commonly used in epidemiological research. When controls in a case-control study are not selected randomly from the population at risk, the effect estimates are likely to be biased. One of the bias is generated by confounding. Confounding mixes effect of a confounder - an extraneous factor in the study with the effect on predictor (exposure) on outcome that distorts the association between them. The observed relationship between exposure and outcome can be distorted totally or in part by the effect of the confounder. The analyses that involve longitudinal data generates biases due to data dependency and incompleteness. It is often that the effect of repeated measurements is temporal or non-linear. Categorize the baseline measurements often provides valuable information, when we are interested in the baseline assessment of specimen for the earlier identification effort with repeated measurements. It is clearly that the category of the first specimen is the confounder of the values of specimen and bias occurs, if the specimen risk on disease is compared between cases and controls.
In the literature, there are limited methods available to correct for the effects of biases on estimates of the exposure-disease relation. Recently, a simulation-based method of inference for parametric measurement error models in which the measurement error variance is known or at least well estimated was developed and studied [1-10]. The method entails adding additional measurement error in known increments to the data, computing estimates from the contaminated data, establishing a trend between these estimates and the variance of the added errors, and extrapolating this trend back to the case of no measurement error. In this study, we introduce a bias adjusted model by simulation.
Methods
Generalized linear mode is commonly used, with a large range of probability distributions that includes the normal, binomial and Poisson distributions, see Equation 1.
The logistic regression is a special case of generalized linear model, which is commonly used in the case-control study. As we discussed earlier, if confounder exists, the bias occurs. For the case-control study, our approach is to generate a set of simulated data with random assignment of cases and controls to perform the same analyses as that for the original data to estimate the bias. The general form of the model is
Where, X is a factor matrix, which generate unbiased estimations, Zis factor matrix, which includes all potential biased factors, γis the unbiased effect of Zon Y, δare the expected bias vector of the parameter estimation related to Z, σ is the variance of the bias ,δand ∈ is the random error. First, we use the simulated data to estimate the distribution of ,δand then use the original data to evaluate other parameters. We may estimate all unknown parameters simultaneously.
Application
Data for service members who received medical discharges with schizophrenia from 1992 to 2005 were obtained from the Physical Disability Agency (PDA) databases of the Army, Navy, Marines and Air Force. Those were cases. All control subjects were matched to their cases on sex (1:1 for male, 1:3 for female), race and age (within a year) and accession date (within a year). All serum specimens were obtained for cases. At least one, and up to four, matched specimens on the collection date within 90 days were selected for each control subject following four criteria:
1) The first available,
2) The most recent before diagnosis,
3) A middle between the two, and
4) The first available after the diagnosis.
The food borne antigen casein was used in this study. We tested a total of 6106 serum samples from 855 cases and 1165 controls for schizophrenia. As shown in Table 1, the majority of cases were men, white, younger than 25 and had less than 3 years of service. Among the cases, fewer than 3% of patients had only one serum specimen available, about 30% had two and three, and approximately 40% had four or more specimens, which were collected up to 15 years before diagnosis as well as after diagnosis. Ninety-five percent of after-diagnosis specimens were collected within 1.8 years of the diagnosis. The association between agents and schizophrenia is examined, as well as the heterogeneity of the association by the agent baseline level and the time to diagnosis.
Hence the matched individuals (cases and controls) are categorized into three groups by their 50th and 75th percentiles of the first specimen of cases and examine the associations within one year before diagnosis and beyond one year before diagnosis. The conditional logistic regression was used. The outcome is the case (schizophrenia) status; the independent factors are subject group (categorized by the 1st specimen), the specimen collect time to diagnosis (one year before diagnosis, within one year to diagnosis), the agent level, their interactions, and the service time. The matched demographic factors are used as strata to control the heterogeneity of the standard error.
To correct the biases, 500 simulation data from the original data sets with randomly assigning case/control status are generated. Then the category of the 1st specimen was redefined according to the value of new data. Then simulation data is used to estimate the distribution of the modeling bias generated by confounding. Figure 1 shows the bias distribution of the scaled casein effect on those subjects with initial low level for different time period. It can be seen that both bias are negative with HR less than one. The mean of the biases were around -1, the distribution of the bias seems more flat than normal.
Figure 2 and Figure 3 show the bias distributions of scale casein for those subjects with initial higher levels. It can be seen the average bias increases as the initial value increasing. For those subjects with initial values higher than 75th percentiles, the bias distributions for the two time period were also different. Hence it is clear that the category of the 1st specimen is a confounder, which dramatically drives the estimation away from neutral. The bias of log of HR is far greater than zero.
If excluding the confounder of the 1st specimen category from the modeling, the model includes the time period (after diagnosis, within one year before diagnosis, 1 to 2 years before diagnosis, beyond 2 years before diagnosis), specimen value, and the interaction, as well as other control factors. There is no obvious confounder in the modeling; Figure 4 shows the results the bias distribution from the same simulated data sets for the scale casein effect within one year to diagnosis and from 1-2 years before diagnosis. It can be seen that the distribution of HR are around 1.0.
It means the bias of log of HR is near 0. Then we perform the adjusting conational logistic model by suing simulation to estimate the bias δ and its distribution to the original data. We combine the two groups with higher initial values, both have positive confounding biases. Table 2 shows the parameter estimations of unadjusted parameter, the bias of the parameter and adjusted parameter as well as the related adjusted hazard ratios for one standard deviation of casein.
We can see that the category of the 1st specimen is still a confounder, which drives the estimation from neutral dramatically. However, after adjusting the bias, the associations between casein IgG antibody levels and the risk of schizophrenia exists for those who had higher initial level. The effect is also slightly different by the different time periods to diagnosis. For those, who had higher initial value, if their casein level increasing on standard deviation at one year pre-diagnosis, the risk to be schizophrenia increases about 12 percent (HR=1.12; 95% CI 1.07, 1.18). If we excluded the confounder of the 1st specimen category from the modeling, the model includes the time period (after diagnosis, within one year before diagnosis, 1 to 2 years before diagnosis, beyond 2 years before diagnosis), specimen value, and their interaction, as well as other control factors. There is no obvious confounder in the modeling; Table 3 shows the results from both unadjusted and adjusted models.
Discussion
The proposed approach in this study shows that the confounding bias could be adjusted by simulation. Confounding is a mixed effect of an extra factor that of interest predictor on outcome. It distorts the association between predictor and outcome. The observed relationship between the predictor and outcome can be attributed totally or in part to the effect of the confounder. Due to confounding, the model may overestimate or underestimate the true association between predictor and outcome; it could change the direction of the observed effect.
The proposed approach in this study can eliminated bias from confounding, if we know the confounder. However, before going to the adjusting model, it is very important to understand the data structure and the model design. The confounder should be correlated with both predictor and outcome. There are issues for the proposed approaches in this study should be further studied such as the bias distribution effect on the adjusting methods, the efficiency of the estimation methods, the number of simulations needed, the relation between the size of original data effect, etc. This paper mainly discusses the case-control studies, but it could be extended for other types of studies.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Biostatistics and Biometrics please click on: https://juniperpublishers.com/bboaj/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/bboaj/BBOAJ.MS.ID.555739.php
27 notes
·
View notes
Text
Tourniquet Pain after Ultrasound-Guided Axillary Blockade-Juniper Publishers
Abstract
Objective: To analyse tourniquet pain after ultrasound guided axillary block (AXB) as the sole anesthetic technique with no injection of local anaesthetic into the subcutaneous tissue of the posterior half of the axilla to prevent tourniquet pain.
Material/patients and methods: 84 patients older than 18 years ASA I-IV undergoing surgery at hand, wrist, forearm and elbow under ultrasound guided AXB requiring upper arm tourniquet, we studied prospectively. Exclusion criteria included refusal to participate, communication problems, pre-existing neuropathy, coagulopathy or allergy to local anaesthetics. Tourniquet pain was assessed according to visual analogue scale (VAS) every 15 minutes. We also analysed differences in tourniquet pain between sedated and non-sedated patients.
Main results: VAS was 0 during ischemia in 83 patients. One patient reported tourniquet pain. This was mild (VAS = 3) and reported during the first 15 minutes of ischemia. VAS dropped to 0 from then on. The median ischemia time was 62 minutes (IQR 45-86) and the median surgery time was 60 minutes (IQR 40-89.5). Intraoperative sedation was administered to 48.8% of patients. Sedated and non-sedated groups were similar. No statistical differences were found regarding tourniquet pain between both groups (p< 0.05).
Conclusion: Ultrasound guided AXB is sufficient to provide anaesthesia for tourniquet even during prolonged ischemia. However, to ensure prevention of tourniquet discomfort a multiple injection technique that include musculocutaneous blockade should be preferred.
Keywords: Tourniquet pain; Axillary block; Ultrasound-guided peripheral nerve block; Upper limb surgery; Sedation
Background
Regional anaesthesia holds potential advantages when compared to general anaesthesia. Particularly, brachial plexus blockade has demonstrated superior analgesia, reduction of opioid-related side effects and opioid consumption during the first 24 hours after surgery [1]. The axillary blockade (AXB) provides anaesthesia for upper extremity surgery of the elbow, forearm, wrist, and hand [2,3]. It has been shown as effective as supraclavicular (SCB) and infraclavicular (ICB) blocks [4] but its distal location from pleura and phrenic nerve eliminates some of the risks related to those more proximal approaches [5,6].
Ultrasound guidance allows direct observation of nerves, surrounding structures and local anaesthetic (LA) spread. Its use decreases complications and onset time [7,8], improves quality [8] and reduces the volume of LA required [9]. Due to the superficial location of the brachial plexus in the axilla, ultrasound guided AXB provides excellent visibility of both nerves and needle.
The intercostobrachial nerve (T2) is not part of the brachial plexus. It communicates with the medial brachial cutaneous nerve (C8-T1) providing innervation to the skin of the axilla and the medial and posterior aspect of the arm. The block of these nerves to prevent tourniquet pain is widely extended and has been traditionally recommended using an injection of LA into the subcutaneous tissue of the posterior half of the axilla ("semicircular subcutaneous anaesthesia" or "ring block") [1014]. However, its importance in reducing tourniquet pain has never been established and is questioned [2,15,16]. The aim of this study was to assess tourniquet pain after ultrasound guided AXB as the sole anaesthetic technique. Due to the fact that intraoperative sedation could underestimate tourniquet pain, further analyses comparing tourniquet pain in sedated and nonsedated patients were also carried out.
Material and Methods
A prospective observational study of tourniquet pain on patients who received an ultrasound guided AXB was conducted over a four month period (January- May 2013) at Galdakao- Usansolo Hospital. The study was classified as service evaluation and no ethical approval was needed as required no alteration to the routine standard of care, there was no therapeutic or equipment intervention, and no planned change to anaesthetic technique. Written consent from patients was obtained. Inclusion criteria were patients undergoing surgery at or below the elbow under ultrasound guided AXB requiring upper arm tourniquet, age >18 years and ASA (American Society of Anaesthesiologists) status I-IV. Exclusion criteria were refusal to be included, communication problems or inability to cooperate, pre-existing neuropathy, coagulopathy or allergy to LA.
After patient arrival to theatre an intravenous catheter was placed in the upper limb contralateral to the surgical site and ASA standard monitoring were applied. Ultrasound guided AXB were performed by either consultants with expertise in regional anaesthesia or residents supervised by those consultant. A portable ultrasound machine (Sonosite M-Turbo®) and high frequency linear probe was used. Administration of premedication or intraoperative sedation was left to the discretion of the treating anaesthesiologist. The ultrasound probe was applied in the axilla to obtain a short-axis view of the axillary artery. The four terminal nerves (median, ulnar, radial and musculocutaneous nerve) were sought out and their identity confirmed by scanning distally along the arm following the characteristic course that each nerve takes. A 22 gauge needle (Braun Stimuplex D) was used to surround each individual nerve with LA after skin infiltration with lidocaine 1% (Figure 1). The AXB approach (in plane or out of plane) and the type and amount of LA was decided by the anaesthetist who performed the block.
AA: Axillary Artery; RN: Radial Nerve; UN: Ulnar Nerve; MN: Median Nerve; MsN: Musculocutaneous nerve; Conjoint tendon of the latissimus dorsi and teres major
Once the block was finished, a pneumatic tourniquet was applied to all patients on the mid-upper arm over a single wrap of cotton wool padding. The limb was exsanguinated using an Esmarch bandage and the tourniquet cuff inflated between 250- 300mmHg.
The variables collected included age, gender, weigh, ASA status, type of surgery, premedication administered, type and amount of local anaesthetic used to surround each nerve, time between the end of the block and the tourniquet inflation, pressure of the tourniquet, ischemia and surgery time, intraoperative sedation and tourniquet pain. The primary objective was to analyse tourniquet pain assessed according to a 0-10cm visual analogue scale (VAS), whereby '0' represents no pain and '10' represents the worst imaginable pain. Tourniquet pain was measured directly after the tourniquet was inflated and thereafter every 15 minutes (min) until the tourniquet was deflated. VAS evaluations were conducted by the same person who performed the block. As a second objective we analysed differences in tourniquet pain between intraoperative sedated and non-sedated patients.
Statistical analysis
Descriptive analysis of socio-demographic and clinical variables was made by using frequencies and percentages for categorical variables and means and standard deviations for continuous variables. The exception being variables with a high level of deviation. These were represented by median and interquartile range. The differences between sedated and non-sedated patient were evaluated using the Chi-square test (or Fisher exact test when expected values<5) for categorical variables and non-parametric Wilcoxon test for continuous variables. All effects were considered significant at p<0.05. All statistical analyses were performed using SAS for Windows statistical software, version 9.2 (SAS Institute, Inc., Carey, NC).
Results
Over the four month period 84 patients were recruited.Patient characteristics and type of surgery are summarized in Table 1. All patients received premedication prior to the block. Intraoperative sedation was administered to 48.8% of patients. Sedatives used to sedate patients during surgery were propofol and midazolam but one patient received 50 mcg of fentanyl (Table 2). Mepivacaine 1.5% were the LA of choice to surround the four nerves in all patients. Occasionally Ropivacaine 0.2% or Levobupicaine 0.25% were added to provide longer analgesia. The mean total volume of LA used was 34.37±5.37 ml (Figure 2).
The median time since the block was finished until the cuff was inflated was 10min (IQR 5-15). The median surgery time was 60 min (IQR 40-89.5) and the median ischemia time was 62min (IQR 45-86) (Table 3).
Among 84 patients included, 83 scored tourniquet pain as VAS = 0cm during the time tourniquet was inflated. One of these patients complained about pain in the surgery field without pain on the tourniquet site after 180min of surgery and had to undergo general anaesthesia. In this case, a 30min reperfusion period was used after 135min of ischemia and the total ischemia time with the patient awake was 150 min. One patient reported tourniquet pain. In this patient VAS was 3 cm when the cuff was inflated and in the following 15 minutes. He was administered 50mg of fentanyl and 20mg of propofol respectively. Since then VAS reminded 0cm until the tourniquet was deflated 31 minutes later. No more sedatives were administered.
Sedated and non-sedated groups were similar in demographic variables, ASA status, premedication administrated, type of surgery, type and amount of LA used, time of ischemia and surgery and tourniquet pressure. No statistical differences (p< 0.05) were found regarding tourniquet pain between both groups (Table 4).
ASA: American Society of Anaesthesiologists; AXB: Axillary Block; VAS: Visual Analogue Scale;
Results shown as number of patients (%). *mean ± standard deviation (SD). †Median [Interquartile range = p25-p75]. NA = Not applicable. --- = Unknown.
Discussion
Tourniquets are commonly used in upper limb procedures to improve visualisation, reduce bleeding and expedite surgical procedures. Despite its advantages, tourniquet might associate injury that usually involves nerve or other soft tissues and is often complicated by the development of tourniquet pain [17]. Contrary to the old belief that a dermal component represents one of the major causes of tourniquet-related pain, ischemia and compression have been identified as the main sources of noxious stimuli during the maintenance of tourniquet inflation [18-21]. Due to these findings, there is progressively more belief that during AXB a tourniquet is well tolerable without requiring additional dermal anaesthesia [15,16]. Similarly, popliteal blockade is sufficient for tourniquet on the caff with no need of femoral or saphenous block [22]. It is important to highlight the importance of achieving a "complete" AXB [23]. Pain associated to tourniquet has been showed to be significantly reduced when a multiple injection AXB technique is used [24]. S. Sia et al. [25] comparing a triple injection AXB technique (blockade of median, musculocutaneous and radial nerves) and a "selective" approach in which only the nerves involved in surgery were blocked, reported a significant increase of patient requesting intraoperative administration of fentanyl for tourniquet pain in the "selective" group.
Despite the numerous anatomical variations of the four main nerves at the axilla, median, ulnar and radial nerves they all lie very close to the axillary artery [25]. Due to this proximity, the injection of a determinate amount of LA to block one of them could cause blockage of the others. By contrast, musculocutaneous nerve lies far lateral to the axillary artery, in the fascial plane between biceps brachii and coracobrachialis muscle. It innervates the muscles in the anterior compartment of the arm - the coracobrachialis, biceps brachii and the brachialis. To achieve its block the needle has to be redirected but its blockade is essential to prevent tourniquet pain [26]. We identified the four nerves by scanning distally along the arm and observing the nerve tracing. They were surrounded by LA independently. Among 84 patients, 83 reported "no pain" [27]. Only one patient complained about tourniquet discomfort (VAS= 3cm) during the first 15 minutes but VAS dropped to 0 cm from then on. This is more likely to be attributed to a block in progress than to a real need of additional blocks. Time between block finished and cuff inflation was just 3 min in this patient whereas, Tran DQ, et al. [28] concluded that the mean onset time is 18.9 minutes when using 4 injections AXB and lidocaine 1.5% with epinephrine 5mcg/ml.
The use of sedation in regional anaesthesia has been shown to increase patient satisfaction and can also modify pain perception [28,29]. However, there were no differences in tourniquet pain between intraoperative sedated and nonsedated patients in our study.
Tourniquet pain has been related to the duration of inflation [18]. Five of our patients had ischemia for more than 120min but none of them complained about tourniquet pain. JP Estebe et al. [30], reported a tourniquet pain tolerance of approximately 2030 minutes in volunteers. Tolerance was defined in that study when VAS was > 6cm or when volunteers decided their pain tolerance limit was reached. In daily practice, letting patients reach either points is unacceptable. Patients on the operating table suffering a painful experience could lead to anxiety, patient movement and unsuccessful surgery. Therefore if a tourniquet is required for surgery, associated pain should always be prevented and treated.
Fitzgibbons PG et al. [31] carried out a review regarding safe tourniquet use recommended tourniquet pressure of 250mmHg for less than 150min in the upper extremity. We used tourniquet pressure slightly higher and only one patient exceeded a total ischemia time of 150min, however a reperfusion time was used on this patient. Although higher pressures and longer ischemia times than the ones recommended have not demonstrated increased complication [32], tourniquet-related injury resulting from excessive tourniquet inflation pressure or prolonged ischemic time were not an objective of our study and were not followed up. Some of the limitations of this study included a relatively small number of patients, observational methodology and nonrandomized design. Test of sensory and motor blockade were not recorded, but no incomplete blocks were reported. No blinded observer data was collected. Ultrasound guided AXB alone provides enough anaesthesia to cover tourniquet-related pain even during prolonged ischemia. Use of additional dermal blocks are not required, however a multiple injection AXB technique that ensures musculocutaneous blockade should be performed.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com
For more articles in Journal of Anesthesia & Intensive Care Medicine please click on: https://juniperpublishers.com/jaicm/index.php
For more Open Access Journals please click on: https://juniperpublishers.com
0 notes
Text
Absence of Circumflex Artery | Juniper Publishers

Juniper Publishers-Open Access Juniper Publishers-Journal of Anatomy Physiology & Biochemistry
Authored by Manickavasuki Kandavadivelu
Introduction
Even though anatomic variations in Coronary circulation are quite common, some of the variations are very rare. Right and Left coronary arteries which supply blood to the heart and they arise from the ascending aorta. Any coronary artery disorder may have serious implications by reducing the blood supply to heart which may lead to Myocardial infarction and death. Coronary arteries represent the only supply to the myocardium. They arise from ascending aorta. The two main coronary arteries are right and left coronary arteries. Right coronary artery originates from right anterior aortic sinus and left coronary artery originates from left posterior aortic sinus of Ascending Aorta. Patency of left coronary artery is vital for sufficient perfusion of the heart. The left coronary artery is responsible for supply of most of the left ventricle, but also considerable portion of right ventricle [1]. Left coronary artery bifurcates into left anterior descending and circumflex artery and passes between pulmonary trunk and left auricle.
The left anterior descending artery runs in the left anterior interventricular groove and ends at the apex or May courses up to crux of the heart. Circumflex artery runs in the posterior atrioventricular groove and ends at the crux by anastomosing with right coronary artery or may end before the crux. Sometimes from Circumflex artery, Posterior interventricular artery may arise and may run in the posterior interventricular groove and termed as left coronary dominance. Numerous studies on the variations of the arteries have been reported, but still it is better to study them further with respect to their clinical significance. The incidence of congenital coronary artery anomalies is 5 – 6%. By definition, the term anomalous or abnormal is used to define any variant form observed in less than 1% of the general population [2]. The incidence of all coronary anomalies is 0.23% in autopsy series and ranges between 0.3and 12% in Angiographic series [3].
Discussion
Splanchnopleuric mesoderm contributes to all components of heart. The mesoderm contributes to the cardiac area that occurs during 3rd week of embryogenesis. The cardiac area later forms a pair of endocardial tubes which fuses at the end to form primitive heart tube. Normal coronary artery arises from appropriate differentiation of pleuripotent cells into their respective anatomic and functional components. Anomalies of the coronary circulation result from processes that disrupt the normal differentiation and specialization of heart tube [4]. Abnormal formation of heart tube which may leads to abnormal formation of coronary arteries. In particular, abnormal involution, position of endothelial buds or septation of truncus arteriosus may give rise to anomalous origin of coronary artery [5]. Coronary endothelial sprouts occur at around 5th week of Intrauterine life from the bulbous cardis from which blood vessels appear which has not yet differentiated into the aorta and pulmonary trunk. The first evidence of coronary vessel development is the appearance of the blood islands at the beginning of the 5th week just under the epicardium in the sulci of the developing heart. The prevalence of Absence of Circumflex artery is about 0.6 – 1.3%. This has been associated with systolic click syndrome, dilated cardiomyopathy and acute myocardial infarction [6]. Absence of Circumflex artery may be due to failure of development of left Circumflex artery in the left atrioventricular groove and may present as Bifurcated trunk of left coronary artery from which left anterior descending artery and diagonal artery arise. In the absence of Circumflex artery, 80% are benign and asymptomatic and 20% are clinically important [7].
Conclusion
Anatomic variations of the heart vessels are common. Hence identification of normal coronary artery pattern and its branches and variations are important for cardiologists, cardiothoracic surgeons and radiologists while performing coronary angiography and surgical procedures. Coronary angiography is an imaging procedure which shows the identification of normal coronary arterial pattern and its variations in the coronary arteries. MDCT (Multi Detector Coronary Angiography) is the study to diagnose the Coronary artery anomaly including Absence of Circumflex artery and to plan for surgery in associated conditions if needed. The angiography is useful in the diagnosis of chronic stable angina, variant angina, myocardial infarction and sudden cardiac death. Atherosclerotic lesions of Left anterior descending artery may be important in these patients because of diminished compensating mechanisms.
For more Open Access Journals in Juniper Publishers please click on:
For more articles in Open Access Journal of Anatomy Physiology & Biochemistry please click on: https://juniperpublishers.com/apbij/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/apbij/APBIJ.MS.ID.555651.php
18 notes
·
View notes
Text
Skipping Breakfast Everyday Keeps Well-Being Away | Juniper Publishers

Juniper Publishers- Open Access Journal of Pharmacy & Pharmaceutical Sciences
Authored by AK Mohiuddin
Abstract
Breakfast, the first meal of the day, is considered the most important meal throughout the day. As nutritionist Adelle Davis famously put it back in the 1960s: “Eat breakfast like a king, lunch like a prince and dinner like a pauper”. Breakfast is most commonly skipped meal more than lunch and dinner specifically in the young adult in the university study period and those who wake up late. Lack of time is the main reason behind skipping meals, in general, lack of appetite, inability to cook, fasting/religion, and not being hungry. Many people are used to be in a hurry for job, business, children’s’ school in the morning where a filled stomach may prevent them to walk a long way. It is obvious that the irregular omission of breakfast may be effective in energy intake reduction over the next 24 hours and in this day, exercise performance may be compromised. There is no evidence that breakfast skipping reduces overeating or prevent weight gain. Some people argue that breakfast and good health is a marketing strategy by breakfast companies.
Keywords: Breakfast; Meal; Appetite; Omission; Energy; Metabolism; Time; Fasting; Skipping meal.
Introduction
The simple definition of breakfast is “the first meal of the day,” which is consistent with the etymology to “break” the “fast”. It is simply identified as “the first meal of the day, consumed within 2 hours of waking, before starting daily activities. Experts say that people who eat breakfast are less likely to overeat the rest of the day. Breakfast-eaters tend to have lower rates of heart disease, high blood pressure and high cholesterol, the American Heart Association reported in 2017. It might be better for weight loss to skip dinner, even eating an early dinner can boost calorie burn, according to Times Magazine.
Moreover, it is found that Japanese people has decreased energy intake, but the percentage of obese people has increased. This suggests that the timing of meals is related to obesity. However, skipping meals has become an increasingly popular part of modern life, especially in young adults. It was found that irregular omission of breakfast might be effective in energy intake reduction over the next 24 hours if the breakfast is habitually consumed and, in this day, exercise performance may be compromised. Cardiac function and sugar control mechanism disrupted along with wait gain, declined wits, mood swing, lethargy, bad breath, low cortisol, chronic inflammation, worsen periods in women commonly reported.
Skipping Breakfast: An Unhealthy Approach
Unhealthy dietary behaviors play crucial role in increasing the upcoming risk of chronic diseases [1]. Breakfast is recommended to contain 20%–35% of daily energy needs [2]. It is considered the most important meal of the day as a part of a healthy balanced diet [3]. Breakfast habits are significantly associated with physiological, psychological, and social health dimensions [4]. Several studies reported associations between breakfast skipping and fatigue at noon, worsens memory and higher body mass index as well as increased prevalence of obesity-related chronic illness [5-7]; deficient in total energy, vitamins and minerals [8], increased risk of central adiposity [9], and risk of insulin resistance and cardio-metabolic disorders [10]. If the stomach is kept empty for a long time, the body will suffer a deficiency of proteins and glucose. Then blood sugar will drop down followed by mood swing [11].
In an Italian population-based study, there is a positive association between headache and meal skipping, especially due to the irregular intake of breakfast [12]. Breakfast is often described as the most important meal of the day, providing as it does sustenance and energy (i.e., calories) for whatever activities lay ahead [13]. Some studies have used solid foods only as breakfast and neglected other highly calorific beverages available, even with the fact that there are “differences in gastric emptying rate and metabolic response to different nutrients in solid versus liquid form” [14].
Breakfast Interpretation in Life Science
A calorie is a balance of net energy does not differentiate between ingested nutrients or calories regarding chewing or not. It is the amount of heat required to raise the temperature of one gram of water from 14.5°C to 15.5°C. 1 calorie = 4.184 joules. An amount of 209.2 kJ (50 kcal) is an appropriate starting spot to dismiss common behaviors that would not be recognized as a meal by most of the people. On the other hand, “time of day, time of waking, and/or the intervals that differentiate separate eating occasions” are also important considerations. [15]. A duration of 2 hours after waking up was used in the definition of the breakfast meal and has been differentiated from snacks by a cut-off point of 1,087.8 kJ (260 kcal) and independent consumption cases secluded based on a 45 minutes period [16,17]. Generally, it is sensible for an operational definition of breakfast to exemplify as “the first meal consumed within 2 hours after prolonged sleep in any 24 hours duration,” which represents the extended daily time consumed in the fasted-situation and the only time when most of the people are post-absorptive [17,18].
A Common Issue of Breakfast Skipping with Young Adulthood
Meal skipping rates may be highest during young adulthood, a period of transition and development [19]. Silliman et al. and Sakamaki et al. reported a high prevalence of meal skipping among young adult population ranged from 24% to 87% [20,21]. Several studies reported that recurrent missed breakfast among different age groups was more than lunch and dinner. Among the sample of Americans from different ages, the rate of breakfast skipping was nearly 11% comparing with lunch skipping around 10% and dinner skipping more than 5% [22,23]. Another study among college students at the University of North Carolina, Charlotte reported that almost half (44.2%) of the students never take their breakfast comparing with lunch (3.5%) and dinner (2.3%) [24]. Australian young adults reported eating breakfast less than 5 days per week, compared with 10% of children and 33% of all adults (>18 years) [25-29].
Reasons Behind Breakfast Skipping
Afolabi et al. reported that 48%, 19%, and 13% of Nigeria university students skipping meals due to lack of time, appetite, and inability to cook, respectively [30]. Fasting/religion and money were mentioned by about 20% and 15% of Nigerian University students as a reason for skipping meals, respectively [31]. About half of Saudi Arabia University students skipping meals because they did not feel hunger while one-third of them don’t have time and one-fifth skip meals because they want to control weight [32]. The study conducted by Shaw revealed that 52% of adolescent reported lack of time in the morning as the main reason for skipping breakfast [33].
Danquah et al. reported that lack of time, not being hungry, and eating late at night were the reasons behind skipping breakfast in 57%, 22%, and 5% of Ghanaian university students [34,35]. In the study conducted by Lee and Yoon [35] on Korean University students, the second cause of skipping breakfast after the lack of time (noted by 61%) was the habit (17.6%). A similar study was found with four private university students of Bangladesh, more than 50% of the respondents skipped their breakfast due to a variety of reasons including class pressure and had fast food after finishing their classes [36].
Impact of Skipping Breakfast on Subjective Appetite
High protein breakfast consists of 50% protein, 30% carbohydrate, and 20% fat reported to have more benefits on mood, alertness, and attention. This might be attributed to that high-protein breakfast resulted in more stable glucose and insulin than adequate protein breakfast [37]. It was also stated that protein keeps blood sugar levels while carbohydrate is important to offer energy to the body [38,39]. Worldwide, there is a common thought that missing breakfast causing an increase in the desire for food, which stimulating overeating at following meals and inducing weight gain [10]. Subjective appetite variables such as “sensations of hunger, desire to eat, and prospective consumption” are estimated as higher in breakfast skipping comparing with breakfast eating conditions. Studies show that lunch intake was higher after breakfast skipping [40-43].
During 2015, two studies conducted by Clayton et al. [44,45] where the breakfast representing 25% energy supplies was taken at 08:00 clock, and lunch and dinner meals at 12:30 and 18:00–19:00 clock, respectively. A similar response was noted when standardized lunch (with 35% of energy requirements) and dinner (with 40% of energy supplies) meals were delivered so maintaining the energy shortage produced by breakfast skipping. These findings revealed that the inaccurate regulation of subjective appetite is a result of an energy deficit. However, it should be noted that subjective appetite sensibilities do not constantly portend following energy assimilation [46,47].
Effect of Breakfast Skipping on Appetite-Modulation Peripheral Hormones
Part of the organization of appetite included numerous intestines peptides and among them the appetite motivator hormone ghrelin as well as hormones linked with satiation and satiety, like “peptide YY (PYY), glucagon-like peptide-1 (GLP-1), glucose-dependent insulinotropic polypeptide, cholecystokinin, and leptin.” Recognition of the reaction of such hormones to energy stability inconstancy could deliver worthy data about nutritional interferences (e.g., breakfast skipping) will be acceptable out of the laboratory atmosphere [48]. Astbury et al. [39] reported that the orexigenic hormones, GLP-1 and PYY were superior up to 30 minutes after consuming a 1,050-kJ liquefied meal two and half hours later to breakfast intake, comparing with later to breakfast skipping.
Yet, no variations in the orexigenic hormone ghrelin were reported. Also, missing breakfast led to an increase in glucose and insulin as a result of the liquefied meal, compared with breakfast eating. This inhibition of glycemic reaction to the second meal of the day, recognized as the “second meal effect” which linked to glycogen storing [49]. In consistent, Gonzalez et al. [50] reported a trend in increasing glucose and insulin response to a 1,500-kJ liquescent meal ate 3 hours later to skipping, comparing with eating breakfast, even that active GLP-1 levels didn’t not diverse between experiments (Figure 1).
Breakfast Skipping and Obesity
Skipping breakfast had a greater influence on both waist circumference and BMI than eating dinner more than 3 hour before sleep [51]. An ethnic study shows correlation of overweight and obesity in school-going Fijian adolescent girls [52]. A strong and conguous relationship between breakfast skipping and obesity, but not overweight, reported among children in southeastern European population [53]. Breakfast Skipping is associated with the Risk of Obesity in School-aged Children [54]. Surprisingly, in lean people, skipping breakfast for 6 weeks increased the activity of genes that helped them to burn fat, but this effect was not seen in obese adults [55].
A positive association between skipping breakfast, overweight and obesity is globally observed regardless of cultural diversity [56]. Eating of breakfast in all populations may be beneficial. Huang et.al [57] also supported with the potential role of breakfast eating in obesity prevention. Obesity and heart disease claimed in a recent study showing that those who skipped breakfast increased their chance for hardening or narrowing their heart’s arteries [58]. Gender may play a key part in breakfast skipping behaviors. In males, breakfast skipping was associated with increased odds of being overweight/obese [59].
Breakfast Skipping and Cardiac Complexities
Habitual avoidance found to be associated with increased risk for development of CAD and hypertension in Western India [60]. Among adults, skipping meals may be linked to excess bodyweight, hypertension, insulin resistance, and elevated fasting lipid concentrations. Men who skipped breakfast had nearly 30% higher risk of CHD as compared with men who did not [61]. A relationship study between skipping breakfast and CVD risk factors such as blood pressure, serum lipids, smoking, and lock of exercise shows equivalent nature to lack of exercise, smoking, high blood pressure, and high serum total cholesterol [62].
More interestingly, a study in Brazil reflects Skipping breakfast is related to cardiovascular risk factors in adolescents, and this relationship was mainly mediated by trunk fatness [63]. However cardiovascular risk was found to associated with both skipping breakfast and late dinner [1]. Also, commendatory changes in cardiovascular risk factors have been reported by regular Korean traditional diet for 12 wk in hypertensive and diabetic patients [64].
Diabetes and Breakfast
Skipping breakfast may increase the risk of T2DM independent of lifestyles and baseline levels of BMI and FBG in middle aged male and female, as reported by Uemura et.al [65]. An IRB approved study by Harvard School of Public Health (Boston, MA) reveals an increased risk of T2D in men even after adjustment for BMI [66]. A lower risk of type 2 diabetes mellitus (T2DM) and metabolic syndrome, prompting interest in the influence of breakfast on carbohydrate metabolism and indicators of T2DM risk [67].
The Health Professionals Follow-Up Study, The Nurses’ Health Study, a Japanese study and the German EPIC cohort provide evidence that regular healthy breakfast consumption is associated with improved glycemic control [65,68-70]. Skipping breakfast was closely associated with annual changes in BMI and WC among men and eating breakfast more than four times per week may prevent the excessive body weight gain associated with skipping breakfast [71]. Also, development of metabolic inflexibility reported in response to prolonged fasting that may in the long-term lead to low-grade inflammation and impaired glucose homeostasis [72].
Altered Cognitive Functions
Skipping breakfast or eating a low-quality breakfast have a negative effect on cognitive function [73]. Glucose is the main fuel for brain function, and optimal cognitive function requires the maintenance of a stable blood glucose level [74]. Breakfast has a direct effect on blood glucose levels and, in turn, blood glucose levels have a direct effect on cognitive function [75,76]. In general, the brain performs best when the blood glucose level is in the range of 80–120 mg/dL [77]. With the gradual depletion of blood glucose and, consequently, energy consumption, people begin to feel hunger and fatigue and experience a decline in cognitive function [78]. Several studies have reported that skipping breakfast lowers cognitive function and work efficiency [79-81].
Mood Swing and Performance
Psychological state and mood, all these variables can also be positively influenced by following healthy dietary practices and it is widely believed that one such practice is the regular consumption of breakfast [82]. Breakfast skipping has been considered an important determinant of an unhealthy lifestyle including alcohol use, smoking, and sedentary lifestyle, as well as low educational attainment, mood changes, and depressive symptoms [83]. Rate of depression has increased recently and association between the frequency of eating breakfast and depression in adults found in a recent study.
Psychological state and mood, all these variables can also be positively influenced by following healthy dietary practices and it is widely believed that one such practice is the regular consumption of breakfast [82]. Breakfast skipping has been considered an important determinant of an unhealthy lifestyle including alcohol use, smoking, and sedentary lifestyle, as well as low educational attainment, mood changes, and depressive symptoms [83]. Rate of depression has increased recently and association between the frequency of eating breakfast and depression in adults found in a recent study.
Lack of breakfast consumption is also associated with depression among adults with different socioeconomic factors [84]. Children who habitually consume breakfast are more likely to have favorable nutrient intakes including higher intake of dietary fiber, total carbohydrate and lower total fat and cholesterol. Beneficial effects reported by Katie et.al, of breakfast for on-task behavior in the classroom, mainly in younger children <13 years [85]. On the other hand, skipping breakfast and taking meals irregularly were associated with the prevalence of fatigue in medical students [86].
Low Cortisol and Women’s’ Health
Women would rather do their hair than start the day with some breakfast, says a new survey. Female breakfast skippers display a disrupted cortisol rhythm and elevated blood pressure [87]. Habitual breakfast skippers would display a similar pattern of circulating cortisol and alterations in meal and stress-induced cortisol reactions. Based on a national survey, approximately 25% of American adults skip breakfast. Skipping breakfast adversely affects menstrual disorders as reported in 2 different studies in young college students of Japan and Palestine [88-90]. Women from developed countries are 2-4 times more likely to have IBS than men [91,92].
A study in Japan shows fasting (1-2 L of fluid each day, along with some nutrition through their vein) improves pain, discomfort, abdominal distension, diarrhea, anorexia, nausea and anxiety in IBS [93]. But breakfast is strictly recommended along with regular meal pattern in patients with IBS-C because it stimulates colon and increase bowel movement [94,95]. However, Two out of five women admit missing breakfast leaves them hungry midmorning, nearly 30% report feeling tired and low in energy and 15 per cent find it hard to concentrate. One in three skip meal in order to get ready for the day [96]. A thinning hair is reported in Reader’s Digest [97]. Teens that skip breakfast are almost twice as likely to have bad breath; more than 35% suffered with bad breath reported in International Journal of Dental Hygiene [98].
Abdominal Discomfort, Ulceration and Cancer
A Mexican study found association of skipping breakfast with gastric cancer [99] which is third most common cancer in men and the fifth in women. Frequent deviation in meal timing over a prolonged period appears associated with increased risk of developing HP infection and gastritis [100]. Skipping meals, leaving the stomach empty except for stomach acid, can create feelings of nausea [101].
Conclusion
Not only breakfast, skipping a meal often creates harm to health, although fasting has its own advantage which is ritual in many religions. A healthy breakfast but not a heavy breakfast is highly recommended. Those who are in a rush can take a protein rich low volume diet. Protein shake as an alternative for breakfast is a common practice in many western countries but this discussion is not within the scope of this article. Skipping meal in IBS and gastroenteritis may found little benefit but no study ever pointed to skip a breakfast for those issues. A healthy breakfast is different for different people based on age, sex, living style and physical activities. School/University going students should never miss a breakfast causes they badly need a jumpstart of energy for the day. Diabetic people should keep in mind that the same is important for them to sensitize insulin release. Rich or poor, young or elderly, all must have a healthy refreshment in the morning for an energized and enthusiastic day start.
For more Open Access Journals in Juniper Publishers please click on:
For more articles in Open Access Journal of Pharmacy & Pharmaceutical Sciences please click on: https://juniperpublishers.com/gjpps/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/gjpps/GJPPS.MS.ID.555701.php
26 notes
·
View notes
Text
Photochemistry Governing Bacteriorhodopsin and Bacterial Reaction Center | Juniper Publishers
Juniper Publishers-Open Access Journal of Sciences
Authored by Bernadine G Ang
Abstract
Bacteriorhodopsin (bR) is a light driven proton pump that converts sunlight to chemical energy. BR is an integral membrane structured protein found in the purple membrane of Halobacterium halobium. It is composed of 248 amino acids and a chromophore in the middle which captures light. Electricity can be generated through the process of light-chemical conversion, when photons are absorbed by thechromophore, the photo cycle begins. Bacterial Reaction Center (bRC) is a light driven electron transfer reaction that converts solar energy to chemical energy. bRC are integral membrane structured proteins found in the purple membrane of Rhodobacter sphaeroides. It is composed of 3 major co-factors such as bacteriochlorophylls, bacteriopheophytin and quinone. Its primary mechanism is to execute photo synthesis. In this interaction, electron transfer occurs through light ejection of electron that passes through the membrane. Conversion of sunlight to chemical energy simultaneously precipitates. This review aims to compare the function and structure of Bacteriorhodopsin and bacterial reaction centers, underscoring the energy generated in both membranes. Through calculating the ATP, protons and photons that cross the membrane, exact value of energy emission in the order of electron volts present the energy generated. Advantages and mechanisms of photoreactions including bioelectronic, bio energy production in bacteriorhodopsin and bacterial reaction centers will be exemplified. Ultimately, energy efficiency of bacteriorhodopsin and bacterial reaction center will be determined.
Keywords: Bacteriorhodopsin; Bacterial reaction center; Photochemistry; Electrochemical efficiency
Introduction
Bacteriorhodopsin (bR) is an integral membrane protein found in the purple membrane of the Halobacterium halobium. As a light driven proton pump, bRs capture photons in the order of 500nm-650nm. Existing research found that 300mv of electricity generated per purple membrane [1]. Conversely, bacterial reaction center (bRC) is found in Rhodobacter sphaeroides. It generates 800mv of electricity in total, considering the transfer of 4 protons in the membrane. Multiple interventions to denature and modulate the structure of bR should be considered, including pH, temperature, detergent and wavelength of laser light. Bacteriorhodopsin has been known to function between0C to 45C at a pH of 1-11. It tolerates temperature over 80C in water and up to 140C in dry [2]. Conventionally, laser is utilized to precipitate the photoisomerization of bR, consequently shifting all trans-13 to structure. The chromophore which is covalently attached to Lys216 through a Schiff base is modulated through this method. Bacterial Reaction Center (bRC) is a light driven electron transfer reaction that converts solar energy to chemical energy. bRC are integral membrane structured proteins found in the purple membrane of Rhodobacter sphaeroides. It is composed of 3 protein subunits–L, M and H. It has 3 major co-factors composed of 4bacterio-chlorophylls, 2 bacteriopheophytins and 2 quinones [3]. In this interaction, electron transfer occurs through light ejection of electron that passes through them embrane. Conversion of sunlight to chemical energy simultaneously precipitates. Both bR and bRC from Halobacterium halobium and Rhodobacter sphaeroides respectively generate a considerable worth of electricity that can be used in the industry today. Although bRC emits power in a rather limited merit, future research would determine its potential for catalyzing electrically reliant applications such as optics, instrumentation and therapeutic values. bRC can be utilized for solar energy and drive photovoltaic cells. Its usage is ubiquitous at this point and has generated multitude of photovoltaic and solar energy driven applications. Further research will enhance the efficacy of bRC generated solar cells and related interventions.
Computation and Methods for Calculating ATP in Bacteriorhodopsin and Bacterial Reaction Center
Bioenergetic quantification through converting and comparing the proton, photon, and voltage in bR and bRC. Chromophore absorption of photon varies between bR and bRC. Permeability of membrane may affect absorption and transport of protons. Hence, data for photo cycle bR efficiency is 60% reliable, while bRC efficiency is 100%.
Efficiency for Converting Light Energy into Electrochemical Energy
Electrochemical energy produce electric energy from chemical energy.bR emits 1 proton/photon, cross-membrane voltage 300mV: 300meV/photon [4] while bRC generates 4 protons/photon equal to 200mV multiplied by 4 resulting to 800meV/photon [5].
Efficiency for Converting Light Energy into ATP
BR generates 22 photons per ATP while bRC generates 1 photon per ATP. Therefore, bR constitutes 22 photons multiplied by 300meV equals to 6600meV which is equivalent to 6.6V [6]. BRC generates 1 photon multiplied by 800meV is equal to 800meV equivalent to .8V [5].
Comparing Power and Efficiency of Bacteriorhodopsin and Bacterial Reaction Center
bR and bRC are both directly correlated with power and efficiency. The higher the unit of power (i.e. milli volts), the more efficient it is in driving industrial applications. Typical instrumentations driven by bR and bRC include bioreactors for hydrogen production, molecular detection and biosensing to name a few [2]. Calculating the power and efficiency of bR and bRC involve the formulas below Figure 1.
P=iV
i= current, V= voltage
Efficiency= Work Output/Work Input * 100% Efficiency= Energy Output/ Energy Input *100 %( Thermodynamic Efficiency) [7].
W=Fd
To get electrochemical efficiency, photo cycle efficiency multiplied by cross membrane voltage gradient times number of protons per photo cycle divided by photon energy. For chemical efficiency, photo cycle efficiency is multiplied by energy per ATP which is always 300meV, divided by number of photons per ATP multiplied by number of protons per photon divided by photon energy. Hence, bR electrochemical efficiency is 7 % (.6*300meV* 1 proton/2.5eV) while bRC electrochemical efficiency is 1 6% (.200meV*1*1*1proton/2.5eV). Chemical efficiency of bR is .54% (.300meV/ 22 * 2.5eV) while bRC chemical efficiency is 3% (.300meV/ (2.5 eV* 4 protons) [5]. Photon energy (2.5eV) was obtained by using the formula E= hc/ λ, where h is the Planck’s constant (6.63x10-34), c is the speed of light (3.0x108m/s) and wavelength in the order of 500nm, when green light is emitted, blue and red light are absorbed Figure 2.
Efficiency of Converting Chemical to Electrical Energy
Kim YC et al. [8] this equation derived from Hummer et al. entails the mechanism of converting chemical to electrical energy: γ= (1+η)Vm/ΔGp Chemical Energy symbolizes Δ Gp, which is equal to (.5eV) (mimic Cco) ((1 + 1).150mv/.5)-100%= 40% while electrical energy symbolizes (1+η )Vm. Vm is them embrane potential, η is pumping efficiency; equivalent to the equation J pump/Jel. And bR constant value is 300meV while bRC constant value is 80meV. BR efficiency of converting chemical to electrical energy is ((1+1).300meV/6.6V)=9% while bRC efficiency of converting chemical to electrical energy is (1+1).200meV/.8V)= 50%. (bR: 100%) (bRC:) [9,10].
Functional and Structural Differences of Bacteriorhodopsin and Bacterial Reaction Center
BR and bRC are both proton pumps that utilize solar energy and convert it to chemical energy Table 1. Although the function of both proteins are the same, they have distinct structural features and consequently have differing energy emissions.BR has a simpler structure than bRC. It is composed of 1740 atoms, while bRC contains 7155 atoms. BR has a chromophore in the middle while bRC contains Bph, Bchl and Q chromophores. BR is composed of seven transmembrane helices; while bRC compose five helices in the L and M subunits and one in the H subunit [3] (Solution structure of the loops of bacteriorhodopsin closely resembles the crystal structure). Both proteins, bR and bRC, come from purple membranes of Halobacterium halobium and Rhodobacter sphaeroides, respectively [11-20].
Conclusion
bRC is more efficient in converting solar energy to chemical energy and solar energy to ATP than bR, while bR generates more electricity, considering the photons emitted by each. BR generates 22 photons, multiplied by 300meV equaling to 6600meV equivalent to 6.6V, while bRC generates 1 photon, multiplied by 800meV equaling to 800meV equivalents to .8V. With 6.6 voltages, lanterns, flashlights and automobiles can be powered.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Sciences please click on: https://juniperpublishers.com/jojs/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/jojs/JOJS.MS.ID.555559.php
23 notes
·
View notes
Text
Mini Review on Synthesis of Pyrimidinthione, Pyrimidinedione Derivatives and Their Biological Activity | Juniper Publishers
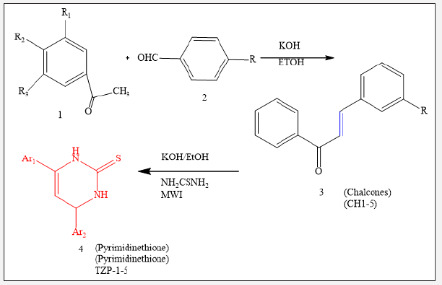
Juniper Publishers-Open Access Journal of Petrochemical Science
Authored by Nadia Ali Ahmed Elkanzi
Abstract
The chemistry of heterocycles has received amongst the chemicals prominent attention in recent years owing to its importance in the pharmaceutical sector. Organic compounds carrying pyrimidinthione, pyrimidinedione, pyridazine rings have been reported to demonstrate a wide range of pharmacological activities, which includes antibacterial, antimicrobial, antioxidant, anti-HIV and anticancer activity. These observations have been guiding for the synthesis of various derivatives of these compounds enclosing biologically active nuclei and study their pharmacological activities.
Keywords: Chalcone; Pyrimidinthione; Pyrimidinedione; Biological activities
Introduction
Over the past decade the evolution of organisms resistant to nearly all the class of antimicrobial agents has become a severe public health concern [1,2]. Heterocyclic compounds have received considerable attention owing to their synthetic and biological importance in the enhancement of the quality of human life. Among numerous heterocycles compounds that have been synthesized and evaluated for their pharmacological activities, chalcone, pyrimidinone and pyrimidinethione have played a crucial role in medicinal chemistry. It was demonstrated that the presence of reactive α, β-unsaturated keto function in chalcones was responsible for their antibacterial and antifungal activities [3].
The pyrimidinones compounds have gained interest in recent years due to their wide-ranging biological activity. These compounds displayed therapeutic applications, as anticancer [4,5], antihypertensive [6], hypoglycaemic [7], antiviral [8], anticonvulsive [9], anti-inflammatory and analgesic [10] drugs.
On the other hand, literature surveys revealed that pyrimidinethione derivatives are an important class of heterocyclic molecules possessing a wide variety of biological properties. In fact, different studies demonstrated that various compounds possessing pyrimidinethione nucleus exhibited broad range of biological activities such as antimicrobial [11-13], antioxidant and antitumor activities [14], antitubercular [15] and hypoglycemic activity [16]. The current mini review aims to focus on some synthetic procedures of pyrimidinones and pyrimidinethione derivatives to facilitate the development of new heterocyclic compounds with more efficient and promising pharmacological activities.
Result and Discussion
Pyrimidinedione derivatives were synthesized from various arylmethylene acetophenone derivatives [17]. The chalcone derivatives were prepared using substituted ketone and distinct substituted benzaldehyde through condensation reaction. Likewise, pyrimidinedione derivatives (4) were synthesized via reaction between aryl methylene derivatives and/ or chalcones with thiourea and KOH in ethanol (50ml) in microwave oven for sufficient time and under an appropriate temperature. The detailed steps used in the synthesis of the pyrimidinedione derivatives were described in the literature [18].
The pyrimidine-2-thione derivatives (4) were screened in-vitro against gram positive and gram-negative strains and were found to be less active against the gram-positive bacteria in comparison with the minimal required dose for the action against the gram-negative bacteria in most cases [17] (Figure 1) (Table 1).
Ethyl 1,5-dihydro-5-oxo-1,7-diphenyl-1,2,4-triazolo [4,3-a] pyrimidine-3-carboxylate (5) was treated with hydrazine hydrate, in refluxing ethanol to give the corresponding acid hydrazide (6) in good yield [19,20]. Acid hydrazide (6) was treated with potassium thiocyanate in refluxing methanol, in the presence of hydrochloric acid to produce1-(1,5-dihydro-5-oxo-1,7-diphenyl- 1,2,4-triazolo[4,3-a] pyrimidine-3-carbonyl) thiosemicarbazide (7). Compound (10) 3-(5-mercapto-4H-1,2,4-triazol-3-yl)-1,7- diphenyl-1,2,4-triazolo [4,3-a] pyrimidin-5-(1H)-one (10) was prepared by oxidative cyclization of compound (7) in basic medium (7% KOH) under reflux with subsequent acidification. It was found that further reflux of compound (7) with dry pyridine gave a product identified as 3- (5-amino-1,3,4-oxadiazol-2-yl)-1,7-diphenyl- 1,2,4-triazolo [4,3-a]pyrimidin-5-(1H)-one (8) (Figure 2).
On the other hand, the reaction involving the synthesis of 1,7-diphenyl-3-(5-amino-1,3,4-thiadiazol-2-yl)-1,2,4-triazolo [4,3-a] pyrimidin-5-(1H)-one (9) took place through a dehydrative cyclization by reacting compound (3) with conc. sulfuric acid. The resulting product (9) was separated as green solid, and was slightly soluble in most organic solvents (Figure 2). Acid hydrazide (6) reacted with phenyl isothiocyanate in refluxing ethanol to produce 1-(1,5-dihydro-5-oxo-1,7-diphenyl-1,2,4-triazolo[4,3-a] pyrimidine-3-carbonyl) phenylthiol semicarbazide (11).
Besides, acid hydrazide (6) was treated with phenyl isothiocyanate in refluxing ethanol to give compound (11)1-(1,5-dihydro- 5-oxo-1,7-diphenyl-1,2,4-triazolo [4,3-a] pyrimidine 3 carbonyl) phenyl thiosemicarbazide as shown in Figure 3. The latter product was subjected to intramolecular cyclization when treated with sulfuric acid, dry pyridine and KOH (5%) demonstrating a new synthetic route to produce compounds 12, 13 and 14, respectively. Subsequent treatment of compound (14) with methyl iodide in the presence of sodium ethoxide solution, yielded 3-(5-methyl thio-4-phenyl-4H-1,2,4-triazol-3-yl)-1,7-diphenyl- 1,2,4-triazolo[4,3-a]pyrimidin-5-(1H)-one (15). It is worth noting that the treatment of compound (14) or (15) with hydrazine hydrate under reflux condition produced the same product, identified as 3- (5-hydrazino-4-phenyl-4H-1,2,4-triazol-3-yl)-1,7-Diphenyl- 1,2,4-triazolo[4,3-a]pyrimidin-5(1H)-one (16) (Figure 3).
Besides, the treatment of compound (11) with phenacyl bromide in refluxing ethanol, in the presence of triethylamine, yielded 1,5-dihydro-5-oxo-1,7-dipheny-lN-(3,4-diphenyl-3H-thiazol- (2E)-ylidene-1,2,4-triazolo[4,3-a] pyrimidine-3-carbohydrazide (17) as shown in Scheme 3. Treatment of acid hydrazide (6) with carbon disulfide in ethanol, in the presence of potassium hydroxide at room temperature, resulted in the formation of potassium salt (18). The latter product reacted with ethanolic potassium hydroxide to afford 3-(5-mercapto-1,3,4-oxadiazole-2-yl)-1,7-diphenyl- 1,2,4-triazolo[4,3-a]pyrimidin-5(1H)-one (19) (Figure 3). The mechanism of formation of the corresponding ox diazole (19) was studied and discussed in previous studies [21-23]. Moreover, potassium salt (18) was subjected to treatment with hydrazine hydrate, in refluxing ethanol, the reaction yielded as 3-(5-mercapto- 4-amino-4H-1,2,4-triazol-3-yl)-1,7-diphenyl-1,2,4-triazolo[4,3-a] pyrimidin-5(1H)-one (17) (Figure 3).
Additionally, it was reported that the reaction involving the synthesis of 4-amino-1, 2, 4-triazole can took place by a simple conversion of 1, 3, 4-oxadiazole under the action of hydrazine hydrate [24,25]. Likewise, the corresponding dicarbonyl compounds including acetylacetone and ethyl acetoacetate were subjected to condensation with acid hydrazide (6) in the presence of an appropriate amount of piperidine as catalyst to give the substituted pyrazole derivatives 3-(3,5-dimethylpyrazole-1-carbonyl)-1,7-diphenyl- 1,2,4-triazolo[4,3-a]pyrimidin-5(1H)-one (20) and 3-(3-methylpyrazole-5-oxo-1-carbonyl)-1,7-diphenyl-1,2,4-triazolo[ 4,3-a]pyrimidin-5(1H)-one (21), respectively (Figure 4).
The structure of these compounds was established based on spectral and elemental analysis reported in the related literature [26-28]. Finally, condensation of acid hydrazide (6) with acid anhydrides, namely phthalic anhydride and 2, 3, 4, 5-tetrachlorophthalic anhydride, in refluxing glacial acetic acid, produced the corresponding imides (22) and (23), respectively (Figure 4). Biological studies demonstrated that these compounds exhibited antihypertensive activity [20] (Figure 5).
Conclusion
In this mini-review, we report on the efficient procedures for the synthesis of pyrimidinedione and pyrimidinethione derivatives. The experimental results showed that the prepared product displayed outstanding pharmacological activities when screened In-vitro against gram positive and gram-negative strains and could be further exploited in medicinal chemistry.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Petrochemical Science please click on: https://juniperpublishers.com/rapsci/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/rapsci/RAPSCI.MS.ID.555676.php
35 notes
·
View notes
Text
Remifentanil-Induced Respiratory Failure in PACU after a Brainstem Tumor Debulking: Acute Diagnostic Dilemma-Juniper PublishersRemifentanil
Abstract
A 66 year old man developed sudden apnea and unresponsiveness after a large cerebellopontine angle tumor debulking. Based on the findings of a focused neurologic exam, the patient was emergently mask ventilated with subsequent return of spontaneous ventilation minutes later and recovery without further complications. Remifentanil bolus from residual infusion in an IV line was suspected due to rapid return to baseline and acute neurologic findings. We review remifentanil and highlight a challenging diagnostic dilemma in an acutely apneic patient after major neurosurgery.
Keywords: Remifentanil; Neuroanesthesia; Post-op respiratory failure; Neurologic Emergencies
Key Messages
a. A focused neurologic exam can affect emergent management.
b. A high index of suspicion and staff education are necessary for those involved in the care of patients receiving remifentanil.
Introduction
Remifentanil is a potent, ultra short-acting μ-opioid receptor agonist with a rapid onset of action in 30-60 seconds, peak analgesic and respiratory effects within 2.5 minutes (min), and rapid clearance (T1/2 = 3 min) [1]. It is commonly used as part of a balanced anesthetic in many anesthesia practices as well as in the intensive care unit. Its use is particularly prominent in neuroanesthesia, where precise hemodynamic control is as important as a crisp, quick emergence of anesthesia to facilitate neurologic evaluation. Respiratory depression is a common severe adverse effect of opioids that may be most prevalent with remifentanil [2].
Case History
A 66 year old man with a large acoustic neuroma presented for cerebellopontine (CP) angle tumor resection (Figure 1). Neuromonitoring of cranial nerves IX, X, XI, XII, somatosensory evoked potentials and motor evoked potentials was used during the case, while the patient received an intravenous anesthetic consisting of propofol 100mcg/kg/min and remifentanil at 0.3mcg/kg/min. Neuromuscular blockade was not used for the case. The surgery progressed without complication, and thepatient was stable throughout. The case lasted 7.5 hours, and propofol and remifentanil were discontinued 60min and 15min prior to conclusion of case, respectively. The patient was able to spontaneously ventilate, protrude tongue, and demonstrate intact cranial nerves IX and X with gag reflex prior to extubation.
In the PACU, the patient was awake and following commands. Shortly after administration of flush through a secondary peripheral IV, the patient acutely closed his eyes, becoming unresponsive and apneic. Rapid physical exam to check for increased intracranial pressure given the setting of recent intracranial surgery demonstrated the patient's pupils were actually pinpoint. The patient was then mask-ventilated until spontaneous ventilation returned several minutes later. Pinpoint pupils and rapid recovery makes a remifentanil bolus from residual infusion in the second IV line the most likely etiology. Patient recovered without further difficulty and was discharged home 3 days later.
Discussion
Remifentanil review
Remifentanil is a potent selective μ-opioid agonist. Its major distinction from other fentanyl analogues is its rapid onset and short duration of action with a terminal elimination half-life of 3-10 min, usually negating the need for Naloxone reversal [3]. The rapid onset of action is directly related to the rapid blood brain equilibration time of 1-2 minutes, while the short duration of action is a result of its unique structure of ester linkages making it susceptible to hydrolysis by blood and non-specific esterases (Figure 2). This rapid extra-hepatic metabolism makes its pharmacokinetics reproducible and dependable. Time to spontaneous movement, following commands, and extubation are all shorter than when compared with other opioids such as fentanyl and morphine. These pharmacokinetic and pharmacodynamic characteristics make remifentanil a nearly ideal analgesic in the operating room. However, due to its short duration of action, patients receiving remifentanil frequently require rescue analgesia in the postoperative period for pain management [4].
Remifentanil is rapidly metabolized regardless of the duration of infusion and is used commonly in clinical situations requiring a rapid offset with the benefit of minimal side effects such as respiratory depression [5]. While the risk for respiratory depression still exists, the ability to rapidly titrate the drug based on response allows for an overall lower rate when compared to most other opioids. In neuroanesthetic cases, it is commonly used in conjunction with propofolas part of a total intravenous anesthetic. It is easily titratable, facilitates stable hemodynamics, and minimally affects neuro-monitoring. Perhaps most importantly, this total intravenous anesthesia combination can allow for rapid emergence and the ability to perform post-operative examination for neurological status shortly after conclusion of the case [2].
Clinical experience
Rapid bolus of remifentanil can result in potentially life threatening respiratory depression, hemodynamic changes, or muscle rigidity. Respiratory depression has been documented in case reports after bolus in laboring patients with patient controlled analgesia [6] as well as in non-obstetric patients receiving remifentanil [7]. This appears to be even more pronounced and observed at lower doses in patients greater than 60 years old. Even infusions as low as 0.05mcg/kg/min have been reported to cause changes in ventilatory drive in healthy volunteers. Muscle rigidity, likewise, is a concerning complication of opioids that can lead to decreased ventilation and compliance resulting in hypoxia and hypercapnia. It is suggested that difficult ventilation may be primarily due to vocal cord closure. Remifentanil, however, primarily affects respiratory drive by activating opioid receptors on the respiratory neurons in the brainstem. By depressing the respiratory drive, the arterial carbon dioxide not only increases but increases in oxygen consumption and intracranial pressure are to be expected [8]. Muscle rigidity however can be prevented with pretreatment or concurrent administration of neuromuscular blockade [9].
Apnea
Our case brings up the challenge and importance of differentiating causes of sudden apnea and mental status change in the immediate post-operative period. The differential for postoperative respiratory failure is large and includes pharmacologic, hemodynamic and mechanical causes (Table 1). In addition to those listed, the patient's comorbidities may be one of the most fundamental things to consider. In the setting of recent intracranial surgery, both opioid overdose and intracranial pathology and dysfunction such as increasing intracranial pressure and seizures are important considerations. Cerebellopontine angle procedures are technically challenging and carry significant risk for postoperative bleeding, increasing intracranial pressure, venous insufficiency and cranial nerve palsy. Physical exam, including neurological exam, may be the most useful and potentially life-saving in this case.
Prevention
Prevention is a keystone of patient care, and the use of more dilute concentrations of remifentanil and initiating rapid resuscitation with possible muscle relaxation have been identified as ways to decrease the chance of similar events from occurring (Table 2). Remifentanil is a very useful opioid in a variety of settings for controlling autonomic responses during procedures and allowing for rapid recovery [2,5]. However, its dangers as a bolus should be known to healthcare providers and ancillary staff so appropriate identification and supportive care can be initiated as soon as a problem is identified.
Acknowledgement
Special thanks to Damian Pickering for assistance with manuscript preparation.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com
For more articles in Journal of Anesthesia & Intensive Care Medicine please click on: https://juniperpublishers.com/jaicm/index.php
For more Open Access Journals please click on: https://juniperpublishers.com
0 notes
Text
Ethics of Biotechnology | Juniper Publishers

Juniper Publishers-Open Access Journal of Gerontology & Geriatric Medicine
Authored by Nishant A Irudayadason
Introduction
Asclepius was brought up by Chiron, the wisest of centaurs, who taught him the secrets of medicine. Asclepius prodigiously developed his skills in Medicine so far as to bring the dead back to life. This attack on the order of things irritated Zeus who found it audacious. This Greek myth is a good point of departure for any ethical reflection. The story of Asclepius recalls to us that, for the Greeks, the greatest of the vices is excess. Wanting to go beyond the measure, beyond what is reasonable, beyond what is Human, this is a crime that the gods cannot tolerate. Excessiveness is the most illegitimate thing.
To avoid the vice of excess, humans are invited to develop in them the virtue of prudence. According to Aristotle, prudence is the proper intellectual virtue to the one who has the responsibility of governing in the interest of the common good. He is neither a scholar nor a wise man; he is someone who makes decisions, someone who is involved. In Greek the word ‘politicos means the administrator of the household or the city. Prudence is the virtue that the politicos must acquire, for virtue is something that is acquired, developed by experience understood in a large sense to include the experience of humanity. The modern equivalent of the virtue of prudence is the Principle of responsibility. This is why we will continue our reflection by using the ideas of Hans Jonas, author of the famous book The Imperative of Responsibility.
Jonas View of Responsibility
The Imperative of Responsibility is the best known work of Jonas [1]. It is based on the rehabilitation of the concept of “end”: “Nature manifests at least a determined end to know life itself” Jonas [1]. Jonas therefore rejects the idea that life can be the result of a play of external forces more or less linked to chance. Life is the most advanced manifestation of being. From this comes the idea that nature must already have this end in itself, against the traditional Cartesian separation between matter and spirit, separation methodologically necessary for the progress of science. The philosophy of nature of Jonas proposes a mode of intelligibility of the world different from the Cartesian mode.
The Cartesian mode is the mode of intelligibility proper to science where complex sets are understood as sums of simple elements. The scientific reductionism transforms theoretical construction into a process fragmentation. The real conceptualized this way becomes something that can be technologically manipulated. This results in the extraordinary development of modern technology. It may even be said that the mode of intelligibility has produced a reversal of the order of things: reality is what can be technically manipulated; if it can be manipulated, it must have been simplified. Consequently, what is complex cannot be the sum of what is simplified. This mode of intelligibility is also valid for the world of the living. Modern technology is, in a way, the metaphysics of modern science.
It is this last point that Jonas rejects. Scientific reductionism should not become the understanding of the world, especially of the living. Life cannot be reduced to a set of simple elements and therefore potentially controllable by technology. Moreover, for Jonas, human person is not the same as other living beings. Human person is in some way “perishable” because he/she possesses the means of self-destruction. Hence Jonas makes an important major ethical assertion: “Act so that the effects of your action are not destructive of the future possibility of such life” Jonas [1]. Let us therefore avoid actions that jeopardize the future of human life.
To act responsibly is to have a certain fear always before the technological interventions on the living. This ethics goes beyond ethics for the neighbour; it is of the order of politics. Through this path, we find, in a way, the virtue of prudence which, for Aristotle, was virtue of Politicos, which has concern for the good of the city state and by extension, for humanity and its future.
Controversies over Biotechnology: Rational Necessity or Irrational Fear?
Our contemporary societies are characteristic of controversies in relation to human inventiveness. Thus, the problem of the crisis of values in relation to biotechnologies in today’s societies arises. There is no longer any doubt that biotechnology is nowadays applicable in all fields of action of contemporary human person. Biotechnology is part of the technologies of the future such as micro-computing and robotics which could ultimately transform the lives of individuals and the profile of their societies. But more than in other fields, biotechnology has had an important peak in terms of controversy with the problems of animal cloning and the valuation of genetically modified organisms called GMO. Can we, through some deviations related to certain evils inherent in biotechnology via science and technology, talk about crises of values in contemporary societies? Nothing is less sure!
Human inventiveness, through some hazardous manipulations sometimes arouses fear and even controversy in the well-being of the people. The meteoric progress of biology and molecular genetics are both worrying and fascinating. This is mainly because of certain practices considered inconsistent with human values and ethical requirements, which raise doubts, suspicions and fear about these practices. Is it irrational not to endorse this fact? If human inventiveness through its action is thus discussed, dreaded, and even diverted from traditional rational paths, should we, willy-nilly, fear future-oriented products which, it seems, could definitively solve certain human health problems? Indeed, the field of human health is the one that worries even sceptics of biotechnology. However, it is also one on which humanity could base all its hopes in terms of cures for rare diseases of genetic origins.
Amidst these controversies, we can say that certain fears inherent in new biotechnology can be justified rationally because of the uncertainties associated with certain products that have already shown their limitations in terms of efficiency It would not therefore be an obsessive fear of the novelty and the unknown that belongs to the irrational, but rather certain practices as well as certain products born of these innovations, which would generate some reticence among the people. Indeed, novelty and its share of innovations must not be disarray but hope for humanity, provided that it definitively imposes the logical necessity of laws that take taking into account ethics as a cardinal value associated with any innovation. Ethical norms must be present and introduced into the basic research process as prerequisites for any scientific approach worthy of interest. However, if ethics is the outcome of the correctness of the action, excessive prudence or the precautionary principle must not become incompetent or irrational frenzy towards the unknown, at the risk of damaging progress itself. Hence, human inventiveness must be perpetuated in complete freedom. It is, in our view, the duty of human responsibility towards humanity, but also in the context of the safeguarding nature. Only the requirement of an ethical framework must regulate the insatiable human inventiveness with the aim of converging freedom of creation and duty of responsibility.
Necessity of Human Invention and Ethical Concern: Freedom and Duty
Reason demands that the human person be valued for his/ her abilities. Inventiveness is one of those human skills that contribute to a better quality of life. This is how it proliferates in several fields, including biology, which is one of the pioneering disciplines in the implantation and enhancement of biotechnology. For our contemporary societies, which are becoming increasingly demanding in terms of productivity, inventiveness and profitability, the ethical concern must be, as we see it, a principle of unconditional necessity. If everyone is allowed to do as he/she pleases, it is not excluded that our present societies may expose themselves to the most unlikely drifts, capable of undermining certain human achievements in terms of ethical progress.
Rationality in the sense of exercising reason consists, to some extent, in consolidating some of these human assets, such as rights, freedom of thinking, acting or creating. But it is nonetheless true that some aspects of freedom are channelled by the requirement of duty. If values are assimilated to duty, they may well be of a coercive nature, such as Kant defines duty, that is to say, a moral obligation to which one must absolutely tend unconditionally. This is tantamount to saying that, although free to undertake a decision that goes in the direction of creation and inventiveness, the human person is bound to break with certain orientations that devalue or evade an ethical implication capable of opening a field of reflection on the activity favourable to the greatest number. It’s a human imperative, it’s a duty. For, between the desire for freedom and the demand for duty, there is a qualitative necessity for action, that is to say, an imperative rectitude of human action. If being free is to undertake freely, to be free is also the concern to be part of a just and responsible action.
The human person has invented and continues to invent all sorts of technologies, some of which, obviously, are subject to controversy, as they sometimes generate products that do not always go in the direction of the primacy of values. But above all, these products are at the same time vectors of a number of tools and manufactured products which pose significant risks to human, animal and environmental consumption. Genetically Modified Organisms (GMO) are part of these products, which have not yet found a definite place in certain countries where associations and certain organized groups put pressure on the decision-making powers as regards their adoption within the society. Rightly or wrongly, the issue of GMOs is divided in the same way as other innovative initiatives such as human cloning, medically assisted procreation, etc. It is said that, in the name of the precautionary principle, this prudence seems justified, which may at the same time be a source of retardation in terms of medical or industrial progress. Laws must be effective and clearly applicable and they must serve as a framework for all emerging innovations as well as the related biotechnological practices. The mere precautionary principle does not necessarily provide satisfactory legal protection, since it is sometimes a source of rational as well as fanciful interpretations for both.
It is clear that, values do not have a uniform understanding within our societies. Indeed, even religious values, for example, which give foundations to a large number of Western civilizations, are now subject to the principles of secularism. It is clear, then, that values, whatever they may be, are now multiform because they have become as much monetary, economic and social. Indeed, the maintenance of life is itself discussed today in the framework of bioethics, which questions the need to preserve the life of a human suffering from terminal cancer. It thus appears that the value of life itself now includes certain subjects which are subject to the discussion and appreciation of the human person or the human society. It is therefore fair to assume that ethical values will also have to be debated within the framework of inventiveness and that of biotechnological practices. It seems to us fair and fundamental to think that the rejection of ethical considerations relating to human inventiveness is likely to pose an important risk as regards the quality of products subject to the consumption of living beings. The evidence of an ethical consideration in decision making, necessary to objectively determine the qualitative sum of the moral values inherent in human reason, is important in all fields of application of biotechnology. This is why ethical concern must be posed as a prerequisite for all human action. This is all the more in the fields of biotechnology, which increasingly generate both benefits and evils in their production chains.
For example, problems related to the genetic modification of organisms of economic interest are unanimous among the people. This is still the case for genetically modified cereals in order to provide more effective resistance to insect pests. Obviously, these practices may still involve risks and dangers that are still unknown to science. This is why the ethical demand must be a priority, a-priori requirement in the very conception of the product. This is tantamount to saying that the issue of ethics must not be an instrument of judgments of results obtained a-posteriori but an active instrument in the process of elaboration, production and distribution of biotechnological products. In other words, ethical action must necessarily take place in all the production chains of products, that is, upstream in their design and downstream to their consumption.
Considering all aspects of human life, it is normal to question the creative freedom of the sciences and their array of technological innovations. While fear that arises can be described as irrational, it is fair to fear a latent perdition of current models of our contemporary societies in terms of research and development, especially if they evade ethical concern and respect for nature and environment in the design, production and distribution of their products. Taking into account the ethical aspect in the production chain of products, we can start a decisive era, which would perhaps have better control of our problems thanks to biotechnologies.
Genetic Engineering of Human Genes
What about genetic manipulation of human genes? Is it prudent to allow human person to modify his/her own biogenetic architecture? The imperative of responsibility does not allow for anything that is technologically feasible if the risk makes human life more vulnerable. It seems to me that genetic manipulations are of this order, for the extraordinary Complexity of the infinitely small which makes us extraordinarily vulnerable. To believe that when we have fully deciphered the billions of genes that constitute our biogenetic architecture, we are risk-free to manipulate them is based on prejudice already mentioned: a complex thing is the sum of these simple elements. The day we technologically manipulate these genes, we will be strengthened in our reductionist epistemology and prudence takes leave of us.
But should this wise fear lead us to totally prohibit any genetic modification? Perhaps not, at least theoretically! It could present situations where the goal is commendable. Should there be a certainty that genetic manipulation can heal a serious illness, may be it would be acceptable. Conversely, changes that would aim to improve performance and appearance seems to me not so laudable as it beings with them unnecessarily risk factors. Prudence should prompt us to abstain from them. These are manipulations aimed at increasing the muscle force, weight, height, hair growth, colour of the skin, etc. Even those which improve memory or learning skills seem to me disturbing [2]. What about the question of extending the duration of human life beyond its present limits? Let us imagine that the duration of human life is genetically determined and severe disabilities are eliminated. This could increase our longevity. What would be the consequences? Living more long with an accumulation of inabilities! In Effect, inabilities increase with older age and they are due to a myriad of causes, which none myriad genetic modifications could make disappear. So I do not see any benefit to manoeuvres. On the contrary, it appears to me totally unwelcome.
In any case, biology accounts only for 25% of the factors that affect longevity, 75% of these factors fall within the socioeconomic dimension, that is to say, relative poverty, level of education, satisfaction with work, etc. The more the gap between the rich and the poor, the greater the loss of longevity for the poor! Those who have completed twelve years of schooling will live nearly seven years more than the less educated. Those who exhaust themselves in jobs that are ungrateful and lacking incentives live less Hadler [3]. This socio-economic complexity is in addition to the complexity of biology. This should encourage us to question the Cartesian prejudice of simplification. But this one has a hard life, for it is Necessary for the development of technologies and Resulting financial empires.
Revisiting Philosophy of Human Person
Let us now turn to the Philosophy of human person and the meaning of life. Why would we want to live longer? Why would we reject the occurrence of our death beyond current limits? It seems to me that this leads even to a deeper question. Beyond its organic substrate, what is a human life? Unlike an animal life, human life is a process of self-fulfilment, a process that makes us see the evolution of our profound identity. We are not ourselves by birth, we become what we are, or more precisely, we arrive at what we are. This is the goal of our lives.
Schematically, this goal, imperfectly realized, unfolds in three dimensions. The first dimension is that of the project. It contains the ideas of will, goal, direction and movement. It refers to the construction of its life, its deployment, its blossoming. The second dimension is that of sharing. It contains ideas of exchange, communication, contact, commonality, participation and being together. It evokes the relationship with others, with the community and with humanity at large. The third dimension is that of identity. It contains the ideas of “being oneself,” to continue to be what one was now and in the future, to be recognizable as Self. It evokes the unity of the personality, its perpetuation and its expression.
The question of the prolongation of life then leads to this question: By living longer, would it be possible to arrive at oneself? Would living longer allow for a better deployment of the three dimensions: project, sharing and identity? I maintain that nothing really makes it possible. In fact, the old age being always linked to many limitations in our ability to deployment everything tends to infirmity. Some may argue that this idea of deployment is peculiar to the West. I believe in the contrary that it is very strongly universalized, although reality often limits the possibility.
Conclusion
The advances in scientific progress today have a mitigated acceptance within human societies. The emergence of new disciplines within the basic sciences, including genetic engineering, molecular genetics and other disciplines of this type, still raises doubts and hopes as to their real capacities to bring about appropriate safe solutions both qualitatively and quantitatively. It is therefore incumbent on the human persons, notably the intellectuals and the researchers, whether philosophers, ecologists or historians, to reflect in the most lucid manner possible on the models of exemplary societies which would suit not only humans, but also to the other living species with which human person cohabits within the ecosphere. The spirit of discernment inherent in human reason must avoid certain harmful drifts linked to biotechnological inventiveness or serious dysfunctions which could lead to the generation of irreversible threats to life.
Why then seek to prolong life beyond its current limits by means of genetic manipulations? The only desire of those who are not ready to let go does not seem to me a sufficient reason. Nor is the desire of those who are afraid of the unknown satisfactory. When we consider that the pursuit of this objective would mobilize resources to the benefit of technology and thus of financial institutions, this quest would neglect efforts to improve the socio-economic conditions of the majority. Reducing poverty, increasing literacy and improving working conditions are more important goals. In conclusion, let us take up the Greek myth: the goddess Eos obtained immortality for her lover Tithonos, but this one ages and loses his human aspect. Asclepios who would like to improve our life beyond natural limits should be wary of the anger of Zeus!
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Gerontology & Geriatric Medicine please click on: https://juniperpublishers.com/oajggm/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/oajggm/OAJGGM.MS.ID.555623.php
21 notes
·
View notes
Text
Falls in Older Adults: How to Asses and Prevent? | Juniper Publishers

Juniper Publishers-Open Access Journal of Yoga and Physiotherapy
Authored by Natália Boneti Moreira
Opinion
Falls and its related consequences are among the major elderly’s public health worldwide problem [1-4]. Approximately 42% of elderly with 70 years or more have experienced at least one fall in the last twelve months [4]. A recent systematic review showed a higher risk-adjusted mortality in falls compared to motor vehicle collisions [3], increasing morbity and mortality in older adults [3,5,6].
Several studies have demonstrated exponential growing risk of falls with increasing age [3,7,8], not only by structural and physiological changes, but also by reduction of functionality and increasing of frailty [4,5]. Functionality is associated with elderly’s function and physical capacities, as muscle potency, walking speed and functional mobility; and social and attitudinal environmental factors affecting them [9,10], and the declines of these capacities have the potential to increase fall’s risk and the severity of falling consequences in older adults [11].
Besides the physical consequences, falls lead to psychological and cognitive changes, as social isolation, depression, fear of falling [11-13] and reduction in quality of life [11,14]. It has been concluded that combination of these factors restrict their activities of daily living, social activities and health perception, making elderly’s functionally dependent, and therefore, generating a negative social and economical impact on family, community and society [4,11,13].
In this context, it’s really important to assess the risk of falls and prevent these episodes. The multifactorial assessment identifies the risk factors for falling. The evaluation may include cognitive impairment, continence problems, falls history (involving causes and consequences, such as fear of falling and injuries), adequate use of footwear, home hazards (e.g. inadequate lightening, carpet or slippery floor, etc.), health problems that may increase their risk of falling (e.g., arterial hypertension, syncope syndrome, visual impairment, etc.), inadequate or excessive use of medication, postural instability, mobility problems and/or balance problems [15,16].
All older adults with frequent falls or with increased risk of falling should be considered for an individualized multifactorial intervention composed by strength and balance training, home hazard assessment and intervention, vision assessment and referral, medication review with modification/withdrawal and psychological aspects including risk behavior and fear of falls. These aspects can avoid the reduction of physical activity level promoting independence and improving physical, psychological and social function, providing a better quality of life for older adults [15,16].
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Yoga and Physiotherapy please click on: https://juniperpublishers.com/jyp/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/jyp/JYP.MS.ID.555677.php
26 notes
·
View notes