
Co-founder and organizer of #PAblr on tumblr. Currently working in critical care. Formerly in burn medicine Crafter. Rabbit lover. Avid reader. See FAQs for questions - if not answered, ask away! This is a medical blog which details MY journey to becoming a PA-C, as well as a platform to connect with other people interested in the profession. Though, there are *some* pics of bunnies. Or science puns. You get it. ;-) **I do NOT give medical advice** I do write educational content for other providers and students. HOWEVER, I am more than happy to answer GENERAL health related questions or questions about my job/specialty/etc. Just don't ask me if you should see your provider for that mole on your back or something- if you are asking, you should go.
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by populationpensive and here's what we found interesting.
Average Info
Notes Per Post
426K
Likes Per Post
231K
Reblog Per Post
195K
Reply Per Post
603
Time Between Posts
8 days
Number of Posts By Type
Text
17
Last Seen Tumblr Blogs





Fun Fact
Tumblr’s website traffic is steadily declining.
Text
This was an interesting read. Surprisingly nonpreachy given the subject; and well worth the time.
74K notes
·
View notes
Text
My take on this is that nothing should be censored or canceled. You can watch or read something and get value from it. That value might be recognizing the bias the creator has or learning something from it. I can read Mein Kampf and not be a Nazi. I can watch House of Cards and recognize that Kevin Spacey is a predator.
Once we (as a society) start vilifying people for certain types of media consumption, we go down the slippery slope of censorship. That never leads to a good outcome. Ever.
I’m really over social media posts about how you shouldn’t listen to this problematic band or watch this problematic show or you’re a bad person. Well I really couldn’t give a shit.
22 notes
·
View notes
Text
People. Will. Die.
Continued cuts will kill people. Period. Full Stop. Please write your elected officials. Go to your University ombudsman. The targeted dismantling of medical research will negatively impact us all.
4 notes
·
View notes
Text
This
Me: I don't get it. I thought I was doing a lot better than I was a few years ago. I'm like 10 times more on top of things than I used to be. How does everything feel terrible now?
The Tiny Me in OSHA-approved Hi-Vis Gear Who lives in my brain and pulls all the levers: Boss, it's the fascism. You're completely gunked up with cortisol due to the fact that your entire daily life is now underscored with a haunting awareness of the rapid erosion of your rights, dignity, and any and all social safety nets, and you're also bearing witness to the most vulnerable people immediately being persecuted. This creates a natural stress response that basically means you're going to continue having memory and organizational problems, as well as emotional imbalances.
Me: BUT I HAVE A BULLET JOURNAL AND I MEDITATE NOW.
Tiny OSHA Me: BOSS, THE FASCISM.
90K notes
·
View notes
Text
"The number of hours we have together is actually not so large. Please linger near the door uncomfortably instead of just leaving. Please forget your scarf in my life and come back later for it."
poem by Mikko Harvey

37K notes
·
View notes
Text
153K notes
·
View notes
Text
I had a patient do this recently. It was the most ridiculous thing I had ever heard. The patient and the family were conspiracy theorists on a level I hadn’t encountered. Completely bonkers.
Today an elderly patient's daughter asked if I could guarantee that the blood I might need to give to the patient (in case the patient is actively bleeding out during the surgery, which had a pretty high chance of happening) is from a donor who hadn't been vaccinated against COVID.
Not gonna lie, I needed a moment to recover from that
#medblr#pablr#anti vaxxers#us health care#science#medicine#btw the answer is no i absolutely cannot guarantee that#and have no intention of guaranteeing that#but i can promise i don't give all my patients blood as a weird hobby#and only use blood transfusion when it's needed for the patient's sake#physician assistant
267 notes
·
View notes
Text
From the Archives: All Aboard
This was from my days volunteering in an inpatient psych unit. I forgot how rewarding and amusing it was.
"Beam me up, Scotty"
Pt 1: *to a room of other psych pts* Your leader has arrived!
Pt 2: You ain't our leader! Who said that?
Pt 1:Why, I made myself your leader. Put your foil cap back on! I keep telling you to keep that thing on so you don't go crazy.
Pt 2:I ain't got no cap, you fool. You got the cap.
Pt 1:I keep telling you, wear you tin cap.
Pt 2:I don't need that. Watch out they'll beam you up!
Pt 1:"BEAM ME UP, SCOTTY!!!!!!!!!!!!!!!!!!!!!!!!"
5 notes
·
View notes
Text
From the Archives: High Creatinine.
This is not my career "high" for creatinine. Had a patient a year or two back with a creatinine of 26.
Pt with a creatinine of 17.8
14 notes
·
View notes
Text
Heather Cox Richardson puts current events in the context of history. Her daily letters to America are a part of my current events reading.

LETTERS FROM AN AMERICAN
March 9, 2025
Heather Cox Richardson
Mar 10, 2025
Lately, political writers have called attention to the tendency of billionaire Elon Musk to refer to his political opponents as “NPCs.” This term comes from the gaming world and refers to a nonplayer character, a character that follows a scripted path and cannot think or act on its own, and is there only to populate the world of the game for the actual players. Amanda Marcotte of Salon notes that Musk calls anyone with whom he disagrees an NPC, but that construction comes from the larger environment of the online right wing, whose members refer to anyone who opposes Donald Trump’s agenda as an NPC.
In The Cross Section, Paul Waldman notes that the point of the right wing’s dehumanization of political opponents is to dismiss the pain they are inflicting. If the majority of Americans are not really human, toying with their lives isn’t important—maybe it’s even LOL funny to pretend to take a chainsaw to the programs on which people depend. “We are ants, or even less,” Waldman writes, “bits of programming to be moved around at Elon’s whim. Only he and the people who aspire to be like him are actors, decision-makers, molding the world to conform to their bold interplanetary vision.”
Waldman correctly ties this division of the world into the actors and the supporting cast to the modern-day Republican Party’s longstanding attack on government programs. After World War II, large majorities of both parties believed that the government must work for ordinary Americans by regulating business, providing a basic social safety net like Social Security, promoting infrastructure projects like the interstate highway system, and protecting civil rights that guaranteed all Americans would be treated equally before the law. But a radical faction worked to undermine this “liberal consensus” by claiming that such a system was a form of socialism that would ultimately make the United States a communist state.
By 2012, Republicans were saying, as Representative Paul Ryan did in 2010, that “60 Percent of Americans are ‘takers,’ not ‘makers.’” In 2012, Ryan had been tapped as the Republican vice presidential candidate. As Waldman recalls, in that year, Republican presidential candidate Mitt Romney told a group of rich donors that 47% of Americans would vote for a Democrat “no matter what.” They were moochers who “are dependent upon government, who believe that they are victims, who believe the government has a responsibility to care for them, who believe that they are entitled to health care, to food, to housing, to you-name-it.”
As Waldman notes, Musk and his team of tech bros at the Department of Government Efficiency are not actually promoting efficiency: if they were, they would have brought auditors and would be working with the inspectors general that Trump fired and the Government Accountability Office that is already in place to streamline government. Rather than looking for efficiency, they are simply working to zero out the government that works for ordinary people, turning it instead to enabling them to consolidate wealth and power.
Today’s attempt to destroy a federal government that promotes stability, equality, and opportunity for all Americans is just the latest iteration of that impulse in the United States.
The men who wrote the Declaration of Independence took a revolutionary stand against monarchy, the idea that some people were better than others and had a right to rule. They asserted as “self-evident” that all people are created equal and that God and the laws of nature have given them certain fundamental rights. Those include—but are not limited to—life, liberty, and the pursuit of happiness. The role of government was to make sure people enjoyed these rights, they said, and thus a government is legitimate only if people consent to that government. For all that the founders excluded Indigenous Americans, Black colonists, and all women from their vision of government, the idea that the government should work for ordinary people rather than nobles and kings was revolutionary.
From the beginning, though, there were plenty of Americans who clung to the idea of human hierarchies in which a few superior men should rule the rest. They argued that the Constitution was designed simply to protect property and that as a few men accumulated wealth, they should run things. Permitting those without property to have a say in their government would allow them to demand that the government provide things that might infringe on the rights of property owners.
By the 1850s, elite southerners, whose fortunes rested on the production of raw materials by enslaved Black Americans, worked to take over the government and to get rid of the principles in the Declaration of Independence. As Senator James Henry Hammond of South Carolina put it: “I repudiate, as ridiculously absurd, that much lauded but nowhere accredited dogma of Mr. Jefferson that ‘all men are born equal.’”
“We do not agree with the authors of the Declaration of Independence, that governments ‘derive their just powers from the consent of the governed,’” enslaver George Fitzhugh of Virginia wrote in 1857. “All governments must originate in force, and be continued by force.” There were 18,000 people in his county and only 1,200 could vote, he said, “[b]ut we twelve hundred…never asked and never intend to ask the consent of the sixteen thousand eight hundred whom we govern.”
Northerners, who had a mixed economy that needed educated workers and thus widely shared economic and political power, opposed the spread of the South’s hierarchical system. When Congress, under extraordinary pressure from the pro-southern administration, passed the 1854 Kansas-Nebraska Act that would permit enslavement to spread into the West and from there, working in concert with southern slave states, make enslavement national, northerners of all parties woke up to the looming loss of their democratic government.
A railroad lawyer from Illinois, Abraham Lincoln, remembered how northerners were “thunderstruck and stunned; and we reeled and fell in utter confusion. But we rose each fighting, grasping whatever he could first reach—a scythe—a pitchfork—a chopping axe, or a butcher’s cleaver” to push back against the rising oligarchy. And while they came from different parties, he said, they were “still Americans; no less devoted to the continued Union and prosperity of the country than heretofore.” Across the North, people came together in meetings to protest the Slave Power’s takeover of the government, and marched in parades to support political candidates who would stand against the elite enslavers.
Apologists for enslavement denigrated Black Americans and urged white voters not to see them as human. Lincoln, in contrast, urged Americans to come together to protect the Declaration of Independence. “I should like to know if taking this old Declaration of Independence, which declares that all men are equal upon principle and making exceptions to it where will it stop?... If that declaration is not the truth, let us get the Statute book, in which we find it and tear it out!”
Northerners put Lincoln into the White House, and once in office, he reached back to the Declaration—written “four score and seven years ago”—and charged Americans to “resolve that…this nation, under God, shall have a new birth of freedom—and that government of the people, by the people, for the people, shall not perish from the earth.”
The victory of the United States in the Civil War ended the power of enslavers in the government, but new crises in the future would revive the conflict between the idea of equality and a nation in which a few should rule.
In the 1890s the rise of industry led to the concentration of wealth at the top of the economy, and once again, wealthy leaders began to abandon equality for the idea that some people were better than others. Steel baron Andrew Carnegie celebrated the “contrast between the palace of the millionaire and the cottage of the laborer,” for although industrialization created “castes,” it created “wonderful material development,” and “while the law may be sometimes hard for the individual, it is best for the race, because it insures the survival of the fittest in every department.”
Those at the top were there because of their “special ability,” Carnegie wrote, and anyone seeking a fairer distribution of wealth was a “Socialist or Anarchist…attacking the foundation upon which civilization rests.” Instead, he said, society worked best when a few wealthy men ran the world, for “wealth, passing through the hands of the few, can be made a much more potent force for the elevation of our race than if it had been distributed in small sums to the people themselves.”
As industrialists gathered the power of the government into their own hands, people of all political parties once again came together to reclaim American democracy. Although Democrat Grover Cleveland was the first to complain that “[c]orporations, which should be the carefully restrained creatures of the law and the servants of the people, are fast becoming the people's masters,” it was Republican Theodore Roosevelt who is now popularly associated with the development of a government that took power back for the people.
Roosevelt complained that the “absence of effective…restraint upon unfair money-getting has tended to create a small class of enormously wealthy and economically powerful men, whose chief object is to hold and increase their power. The prime need is to change the conditions which enable these men to accumulate power which it is not for the general welfare that they should hold or exercise.” Roosevelt ushered in the Progressive Era with government regulation of business to protect the ability of individuals to participate in American society as equals.
The rise of a global economy in the twentieth century repeated this pattern. After socialists took control of Russia in 1917, American men of property insisted that any restrictions on their control of resources or the government were a form of “Bolshevism.” But a worldwide depression in the 1930s brought voters of all parties in the U.S. behind President Franklin Delano Roosevelt’s “New Deal for the American people.”
He and the Democrats created a government that regulated business, provided a basic social safety net, and promoted infrastructure in the 1930s. Then, after Black and Brown veterans coming home from World War II demanded equality, that New Deal government, under Democratic president Harry Truman and then under Republican president Dwight D. Eisenhower, worked to end racial and, later, gender hierarchies in American society.
That is the world that Elon Musk and Donald Trump are dismantling. They are destroying the government that works for all Americans in favor of using the government to concentrate their own wealth and power.
And, once again, Americans are protesting the idea that the role of government is not to protect equality and democracy, but rather to concentrate wealth and power at the top of society. Americans are turning out to demand Republican representatives stop the cuts to the government and, when those representatives refuse to hold town halls, are turning out by the thousands to talk to Democratic representatives.
Thousands of researchers and their supporters turned out across the country in more than 150 Stand Up for Science protests on Friday. On Saturday, International Women’s Day, 300 demonstrations were organized around the country to protest different administration policies. Senator Bernie Sanders (I-VT) is drawing crowds across the country with the "Fighting Oligarchy: Where We Go From Here” tour, on which he has been joined by Shawn Fain, president of the United Auto Workers.
“Nobody voted for Elon Musk,” protestors chanted at a Tesla dealership in Manhattan yesterday in one of the many protests at the dealerships associated with Musk’s cars. “Oligarchs out, democracy in.”
LETTERS FROM AN AMERICAN
HEATHER COX RICHARDSON
#letters from an american#heather cox richardson#american history#history#stand up for science#protest#trump administration#protect equality and democracy#resist
6 notes
·
View notes
Text
From the Archives: Peaceful Passing.
Peace
I wish that everyone could die the way my patient did.
They were compassionately extubated, started on a fentanyl drip, and kept comfortable with classical music dancing through the air. They were surrounded by their spouse and children. The love for him was so evident, so pure - it filled the room with a sense of warmth and comfort.
The residents and myself stayed with the family who shared so many lovely stories. His favorite books, favorite foods- how he met his wife. As he lay there dying, with a BP of 40/20, he was so peaceful. His wife held his hand and tucked back his hair.
“You are beautiful and there is nothing to be afraid of.”
With a light gasp, he was gone.
I have seen so much death. Much of it lacks dignity. It is violent. It is prolonged. People suffer. This death was not that. This death was so refreshingly beautiful and quintessentially humane that it reaffirmed everything we hear about death but don’t want to accept.
That death can beautiful. That death can be peaceful, even joyous. That death is inevitable but it doesn’t have to be scary.
I wish every person could die this way. That they could be celebrated by those that love them and cared for them. There is still pain for the family. There is still grief. However, besides being born, this is THE universal human experience. We are all destined to die- I just hope we all are lucky enough to experience it in a dignified and loving way.
#pablr#pa-c#medblr#nurblr#pharmblr#health care#us health care#death#dying#hospice#compassionate extubation#it can be more dignified#medicine#palliative care
499 notes
·
View notes
Text
To the New PA-Cs
Hey there.
You passed your boards, you got that job, and you have that badge that says PA-C. There is so much excitement at this time but also a lot of anxiety. There will be a day where it will hit you: "Oh shit, I have to make a decision. This patient's care is actually in my hands." That can be a scary feeling.
Please know that I see you.
The first 6 months is so hard for so many reasons. You'll feel dumb. You'll wonder why you're allowed to practice. You'll make mistakes.
You'll also have many successes. You'll learn a lot.
Keep asking questions. Keep learning. Keep seeing every patient as a learning opportunity. Take time for yourself. Breathe.
The more you experience, the more confident you'll be. It just takes time.
I believe in you.
Hang in there.

2 notes
·
View notes
Text
Year 6
If you had asked me in 2012 if I would be posting a "Year 6 as a PA-C" entry, I would have thought you were off your rocker. Truly. I had so little faith in myself that I could do the thing that, had it not been for sheer grit, I probably wouldn't have.
As I pass this milestone, I have a lot of thoughts. This blog, for one, was the origin of making me feel like I could, in fact, do the thing. Our little Pablr community has grown and the people I interacted with on here were a major part in making me feel like I had a shot. While I post relatively infrequently (because life), I value what this forum has given me. I probably could make a year 6 post without to be honest.

So, about that Year 6.
I am entering this weird place where I feel pretty comfortable and confident in myself and my skills. I have seen enough that most issues/patient problems are rather routine. I find myself doing more teaching and have more shadows with me. It is so hard to find shadowing hours and I want to try to pay it forward.
That being said, the teaching and the shadows are a reminder of the privilege that I have to care for my complex patients. These students remind me that while I might have seen a lot, that routine should not mean complacent. Students also have this curiosity that we can lose as we progress through the profession at times. Their passion is invigorating and reminds me of why I do what I do.
I recently went to SCCM (Society of Critical Care Medicine) Congress in February. I hadn't gone in 2 years and conferences like this are always an interesting experience. I learn a lot but I am also humbled by the people I meet. Every hospital/work place has its baggage and it is a nice opportunity to talk with others and have a sense for how nice I have it as a PA-C. Are there problems that need fixing in my unit? For sure. Does my hospital need a fucking wake up call with certain issues? Hell to the yes.
But, I find myself rather lucky that I work with physicians that respect me and my experience. They give me an insane amount of autonomy. That autonomy was earned through a lot of hard work, but I function as they do, to be honest. Talking with some other people at the conference, some ICU cultures are not as supportive of the APPs. That could be a reflection of a multitude of things but I still feel rather fortunate that I am where I am.
So, what's next?
I have no intentions of leaving the ICU but I am more cognizant of how the work impacts my own health. I took time off maybe once a year for the first 5 years and that has had negative impacts for me. I value my time far more and see the importance of taking time away to be the best I can be when I am at work.
Eventually, I would like to teach at a PA school part time. While I currently guest lecture a couple of times a year, I do miss the formal teaching setting. I may need to consider adding a degree to my wall. A master's of medical education is very much in line with what I am planning to do. However, the PA profession (regrettably) is moving towards the DMSc route. I may need to do this, even if I do not want to, to teach at a PA school if that degree is offered. I have a WHOLE rant I have been sitting on about that.
I have some unique teaching opportunities through my work to help build that resume. I have some lucrative side hustle opportunities that I need to feel out before committing. It's been an interesting time, especially in the last year.
However, one thing is certain. I am so grateful that I chose this path. I am so proud of the very scared 22 year old version of me that knew I would regret it if I didn't at least TRY to pursue medicine. I have always been a person whose work needs to fulfill them on a spiritual level. I couldn't just work for a paycheck. Not in my nature. I am glad that I can do something I love.
#pablr#pa-c#physician assistant#physician associate#pre-pa#caspa#pre health care careers#pre-med#medblr#pharmblr#nurblr#medicine#grad school#critical care#reflections#originstory#aapa#nccpa#medical education#teaching#education
3 notes
·
View notes
Text
From the Archives: Hyperbaric Medicine
Hyperbaric Medicine (HBO)
I'm sorry, what is that?

I have a side hustle as a hyperbaric medicine provider and I am here to give you the down and dirty!
Sometimes referred to as HBO (hyperbaric oxygen), hyperbaric or dive medicine is a specialty that utilizes oxygen at high pressure to treat a variety of conditions, primarily things involving wounds. We place a patient in a chamber, deliver 100% oxygen to them, pressurize the chamber, and keep them in there for about 120 minutes. Since oxygen is the number one thing you need to heal a wound, we use a lot of it to try and speed up the process.
The Basics
Wait - what? HOW? Try not to have PTSD from your days in chemistry, but remember these?

The treatment physiology of hyperbarics relies on gas laws. Recall that it takes a lot of pressure to dissolve a gas into a liquid.
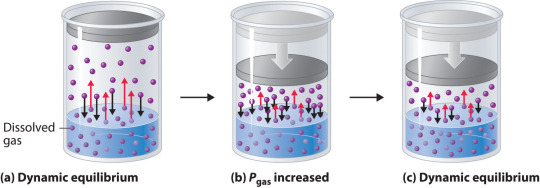
We use pressure to force oxygen into the blood stream at high rates to facilitate wound healing. For reference, most of your oxygen content is bound to hemoglobin (~98%). You do have dissolved oxygen in your blood, represented by your PaO2/PvO2 in a blood gas. However, this makes up a fraction of O2 content (~2%: if you want a clinical soap box, you should hear me talk about blood gases to students lol). A normal ABG would have a PaO2 of 65-100. An ABG acquired during hyperbaric treatment would be well over 2,000.
As an aside, recall that ambient air is 21% oxygen. Also, as a reminder, we exist at 1.0 ATA of pressure (one atmosphere).
How is it done?
Delivering oxygen this way requires delivery of a lot of pressure. We utilize dive chambers for this purpose. There are two types of chambers:
Monoplace: literally looks like a class coffin. Holds one patient and delivers oxygen at pressure through the entire chamber. These are very popular at wound centers.

Multiplace: literally looks like a submarine. Holds 2+ patients and delivers oxygen at pressure to individual patients hooked up to hoods or masks. These are found at tertiary care/academic medical centers.

Literally, the multiplace hoods make you look like a silly space person.

The reason oxygen is delivered this way in a multiplace chamber is to reduce the risk of fire. Oxygen at pressure can go boom. Having an entire chamber full of O2 is a big risk. So, we deliver the gas individually to each patient.
How did it start?
Dinking around with gases at pressure has been a thing for 400 years. However, it didn't become a more focused endeavor until the first dive suits started to be a thing in the 1870s. The specialty itself is relatively new, developed in the 1930s due to advent of decompression illness with divers. Things really progressed in the 1950s.
One pivotal study was "Life without Blood" in 1959. Dr. Boerema proved that he could keep a pig alive with HBO alone. The ethics of this experiment are questionable but he exsanguinated a pig under hyperbaric conditions (3.0 ATA, 100% FiO2). Plasma was left behind. By doing this, he proved that, at pressure, an organism does not need hemoglobin to live. Kind of a radical thing to prove! Don't worry, the pigs did get their blood back and recovered without issue.
What is treated with HBOT? (hyperbaric oxygen therapy)
Anything related to wound healing can be treated with HBOT. We also treat carbon monoxide poisoning, air gas embolism, and decompression sickness with HBOT. I'll start with those since they are (imo), the most clinically interesting. ;-D
Carbon monoxide poisoning: The physiology of using HBOT to treat CO poisoning is based on the binding affinity of CO to hemoglobin. CO has 200 x the binding affinity for hemoglobin than O2 or CO2 does. Because the binding sites are taken up by CO, hemoglobin cannot pick up O2. It also can't offload whatever O2 is already bound. The goal with HBOT is to bombard the blood with massive amounts of O2 to force CO off.

For reference, it would take about 6 hours for CO to offload on its own from hemoglobin on room air. It would take half as long at 100% FiO2 delivered at standard air pressure (1.0 ATA). CO is rapidly forced off within 30 minutes with HBOT. With very severe CO poisoning, particularly in cases of LOC, this is vital for limitation of hypoxia and neurological sequelae of exposure. Treatment is 1-3 "dives" depending on clinical context. The patient is treated at 2.8 ATA (60 feet of sea water) for about 120 minutes.
Air gas embolism: This occurs when gas is accidentally introduced into circulation. It can either be venous or arterial. The venous system has much more flexibility in tolerance for air bubbles. 15 cc or less of gas introduction is probably not going to result in symptoms. Higher volumes go to the lungs and can result in local lung infarction.
The real danger with this is air introduced into arterial circulation. Depending on where it is introduced, it can go directly to the heart causing an MI, or to the brain causing a stroke. Any volume of air introduced into arterial circulation is bad news bears. Treatment is usually 1 "dive" but could be more based on the context. The patient is treated at 2.8 ATA for 30 minutes and then the ascent is extremely slow. The whole dive takes about 5 hours. Why so long? If we ascend too quickly, the air bubble will reform.
Decompression sickness: This occurs primary with scuba divers who ascended too quickly. Scuba divers generally breath mixed gas, most commonly air (21% O2, ~79% N2) or nitrox (35% O2, ~65% N2). As someone is diving, the nitrogen they breath is also dissolved into their blood since they are at a pressure greater than 1.0 ATA. If a diver ascends too quickly, the nitrogen dissolved in the blood will rapidly reform air bubbles in the blood. We just mentioned how that is problematic.
Since air bubbles can go everywhere in circulation, the symptoms are variable ranging from headache, vertigo, nausea, joint pain, chest pain, stroke symptoms, loss of bowel/bladder function, etc. The treatment for this is to recompress the patient and very slowly ascend in the HBO chamber. Treatment is usually 1 dive but could be more based on the context. The patient is treated at 2.8 ATA for 30 minutes and then the ascent is extremely slow. The whole dive takes about 5 hours. Why so long? Again, if we ascend too quickly, the air bubble will reform.
Wound related conditions: there are roughly 15 approved diagnoses for HBO by Medicare in the USA. This is important to mention because if a condition is not covered, paying out of pocket is extremely cost-prohibitive. Insurance is billed $6,000 per treatment! Some of the most common conditions treated are osteoradionecrosis, soft-tissue radionecrosis, irradiation cystitis with hematuria, and refractory chronic osteomyelitis. Wounds created from radiation exposure have the best evidence to support the use of HBOT. These are considered outpatient conditions so patients come to be treated Monday-Friday. We dive to 2.4 ATA for 120 minutes. At minimum, patients are prescribed 20 dives but most treatment protocols for radiation induced injuries is at least 40 dives.
As you can see, this is a HUGE commitment for the patient. One dive is not enough for these wound related conditions. As a hyperbaric provider, I can say that we have patients with such significant symptom relief from HBO. For example, irradiation cystitis with hematuria is extremely debilitating. Patients are fatigued from chronic blood loss, deal with painful bladder spams and pelvic pain, pain with urination, and increased frequency. The blood can clot and obstruct their urethra or foley catheter. Symptoms like this limit quality of life. HBOT makes a huge difference for them.
Benefits
Anyone who has barriers to wound healing can benefit from HBO. Barriers include vascular disease, CKD, COPD, DM, heart failure, and immunocompromised status. The goal is symptom resolution/improvement or healing of the wound. Some patients get approved for far more treatments than we typically do. Usually the maximum insurance will cover is 60. However, in some situations, the clinical benefit of continued treatments is recognized by insurance and treatment is extended.
As a provider, I get to know these patients pretty well. They show up every day that I am staffing in HBO and it is rewarding to see them improve. Compared to my critical care role, this is a nice change of pace.
Adverse Reactions and Risks
There are risks and side effects to HBO. The most common are barotrauma, pneumothorax, seizure, temporary worsening of cataracts/vision, and abdominal distention.
Barotrauma of the ears and sinuses is by the most common issue we face in HBOT. If patients are not able to clear their ears as they descend ("pop" their ears), they can rupture their ear drums. Patients that cannot descend without extreme pain may need myringotomy tubes (ear tubes) to assist with equalizing pressure.
Seizure is a risk of HBOT and that primarily comes from oxygen reducing the seizure threshold. We mitigate this with "air breaks". These are 5 minutes intervals of the treatment where the patient is receiving air rather than 100% O2. Example, we treat at 100% for 30 minutes, have a 5 minute air break, repeat x 2. Obviously the people at highest risk are those with epilepsy or taking seizure threshold reducing medications.
HBOT can worsen cataracts and vision temporarily. The mechanism of this is poorly understood but we know it is reversible. Distance vision is affected the most.
Contraindications
The only absolute contraindication to HBOT is an untreated pneumothorax. There are many relative contraindications that require a risk benefit analysis. An example of this is pregnancy. HBOT has not been thoroughly studied in pregnancy and is not recommended EXCEPT in cases of CO poisoning where we know that the CO concentration is higher in fetal circulation than maternal. Always treat a pregnant person with CO poisoning.
Other potential contraindications include use of certain chemotherapy agents, COPD with blebs/bullae, severe heart failure, epilepsy, sinus/HEENT disease, claustrophobia, certain implanted devices, or active infection.
With certain chemo agents, they can lower the seizure threshold putting patients at higher risk of seizure in the chamber. People with COPD and blebs are at risk of those blebs popping under pressure and causing acute respiratory distress. People with heart failure can experience flash pulmonary edema after an HBO treatment. If people are claustrophobic, obviously spending time in a monoplace chamber can trigger panic attacks. At my center, we sometimes have people referred to our multiplace chamber for exactly that reason.
Most implanted medical devices are HBOT compliant. Generally, pacers and other devices are tested at 4.0 ATA of pressure. We double check with the manufacturer that the device is compliant. If it isn't, we cannot safely treat and have to deny the consult.
Obviously, if someone is sick, we don't want them in the chamber. Particularly colds, severe allergies, fever, or anything that is affecting HEENT. People with acute sinus infection are unable to clear sufficiently to dive. Even if they can clear, they feel miserable. No need to go through that.
Safety Issues
I mentioned that high O2 environments are at risk for explosion. Safety is the number one concern with any chamber. The goal is to reduce risk of fire by removing fabrics that create static (anything synthetic), removing electronic devices that are not HBOT approved, and going through multiple levels of safety checks for patients and for chamber preparation.
At our chamber, only 100% cotton is allowed in the chamber. All patients have special scrubs that they wear during treatment. No electronic devices can be brought in the chamber which includes phones, tablets, laptops, e-readers, watches, pagers, etc. We do have HBOT approved IV pumps and radio headsets that we use. These have been tested at 4.0 ATA. The radio headsets are for the attendant (staff member) who is in the chamber and this is also for safety purposes. Since we have a mulitplace chamber, a staff member is always in the chamber with the patient(s).
One thing I do want to address is that some people are concerned about putting a patient with active cancer into the chamber. There is concern that the high O2 environment will "feed" the cancer. There is simply not data to support this. Active cancer is not a contraindication to HBOT.
And there you have it! The down and dirty of HBOT! Hopefully you learned something cool. If you think you have a patient who would benefit, find your local HBOT provider. We are always happy to talk with you about the process. If you care about a soapbox of how insurance companies suck, see below. :-D
Soapbox: I will say, I have definitely been frustrated with insurance companies. They are the gatekeepers of this treatment. You can have several providers supporting the use of treatment and an insurance company can still say "no". Very frustrating.
A prime example of this are patients who have avascular necrosis that is steroid or chemotherapy induced. These are often younger patients (late teens, early 20s) who have/had leukemia of some kind. They end up having necrosis at a joint, usually the femoral head, that will likely result in complete joint replacement at a young age. No orthopedic surgeon wants to replace joints on a young person. It comes will all kind of problems and always needs revision later in life.
Insurance companies will say "we only cover radiation induced necrosis" because that is what the literature supports. Yes, they are correct that the vast majority of studies support HBOT for radiation induced injury. However, the pathophysiology of the tissue destruction, while a little different, ends up with the SAME problem. There are studies that support HBOT use in these situation but not nearly as many as radiation induced injury. The result is that patients suffer, get a joint replacement they could have avoided (or postponed until they are fully developed), and generally are shafted.
*end soapbox*
#hyperbaric medicine#hbo#hbot#oxygen therapy#medicine#dive medicine#pablr#medblr#nurblr#pharmblr#health care#medicare#co poisoning#air gas embolism#decompression sickness
11 notes
·
View notes
Text
This is just one of many articles (see below) about how the American scientific community is suffering from the Trump administration. I URGE YOU to spread the word amongst your friends, family, and co-workers. The average person does not remotely understand how this funding is impactful. How it make health advancements for those in need.
Educate the people around you. While we can all have product conversations about governmental budget reform, yes, even with NIH funds, a slash and burn policy will only harm us all in the end.
#stand up for science#trump administration#attack on sience#physician assistant#pa-c#physician associate#medicine research#health care#usa#us health care#med school#medblr#pharmblr#nurblr#medicine#NIH#federal funding
18 notes
·
View notes
Text
The morbs
I may "have the morbs" as depressed Victorians would say but I *did* register for SCCM's Congress in Orlando!!!!
SCCM = Society of Critical Care Medicine
V. excited to go back. I went to the one they had in San Francisco in 2022 and left feeling quite energized, which I hope will happen this time around.
4 notes
·
View notes