#Juniper Publishers Contact address
Text
Impact of Consciousness Energy Healing Treatment on the Isotopic Abundance Ratio of Folic Acid- Juniper Publishers
Juniper Publishers- Open Access Journal of Annals of Reviews & Research
Impact of Consciousness Energy Healing Treatment on the Isotopic Abundance Ratio of Folic Acid- Juniper Publishers
Authored by Snehasis Jana
Abstract
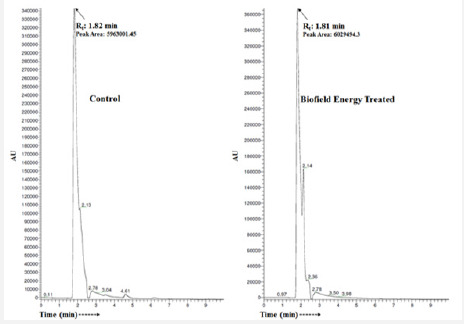
Folic acid (Vitamin B9) is the water-soluble vitamin mainly found in the foods and supplements, which is involved in the synthesis and repair of DNA and RNA, aiding rapid cell division and growth, enhancing the overall brain health, etc. in the body. In this study, the impact of the Trivedi Effect®-Consciousness Energy Healing Treatment on the structural properties and the isotopic abundance ratio of folic acid was investigated using LC-MS spectroscopy. The test sample folic acid was divided into control and treated parts. Only the treated part received the Trivedi Effect®-Consciousness Energy Healing Treatment remotely by a renowned Biofield Energy Healer, Dahryn Trivedi. The chromatographic spectra of both the samples exhibited the same retention time at 1.8 minutes and mass of the molecular ion peak at 441.92 (calcd for C19H20N7O6+, 442.15) along with low molecular fragmented mass peaks at m/z 295.08, 267, 250.17, and 207.92 for C14H11N6O2+, C12H15N2O5+, C12H12NO5+, and C11H14NO3+, respectively were also observed. The peak area of the treated folic acid (6029494.3) was increased by 1.12% compared to the control sample (5963001.45).
The isotopic abundance ratio of PM+1/PM (2H/1H or 13C/12C or 15N/14N or 17O/16O) in the treated folic acid was significantly increased by 81.37% compared with the control sample. Hence, the 13C, 2H, 15N, and 17O contributions from C19H20N7O6+ to m/z 442.92 in the treated sample were significantly increased compared with the control sample. The changes in isotopic abundance and mass peak intensities might occur due to the changes in nuclei possibly through the interference of neutrino particles via the Trivedi Effect®-Consciousness Energy Healing Treatment. The increased isotopic abundance ratio and peak area of the treated folic acid may increase the chemical bond strength, increase its stability, improve solubility, and bioavailability in the body. The new form of Biofield Energy Treated folic acid could be used for designing novel pharmaceutical formulations that might offer better therapeutic response against embryonic defects, clinical depression, megaloblastic anemia, altered memory, and brain function, leuco- and thrombocytopenia, malignancies, neural tube defects, depression, allergic diseases, cardiovascular disease, and lower bone density, etc.
Keywords: Folic acid; The Trivedi effect®; Biofield energy; Consciousness energy healing treatment; LC-MS
Introduction
Folic acid (Vitamin B9) is the water-soluble vitamin mainly found in the foods and supplements [1]. Daily recommended folate for adults is 400 micrograms (mcg) and for women in pregnancy is 400 to 800 mcg of folic acid a day [2]. The folate is highly rich in the food items, i.e., dark green leafy vegetables, fruits, avocado, nuts, chickpeas, soybeans, beetroot, spinach, liver, asparagus, yeast, kale, dairy products, Brussels sprouts, poultry and meat, eggs, seafood, grains, and some beers [3-6]. Folic acid plays many physiological functions in the body, i.e., various intracellular reactions, enzymatic reactions included in vitamin metabolism and amino acid synthesis. It is majorly involved in the synthesis and repair of DNA and RNA, aiding rapid cell division and growth, enhancing the overall brain health, and in age-related hearing loss [7]. Along with this, folic acid also plays important role in normal blood formation, normal metabolism of the immune system, normal amino acid synthesis, homocysteine levels, cell division, control various psychological functions, maintain normal maternal tissue growth during pregnancy, reduction of tiredness and fatigue. The deficiency of folic acid might result from inadequate intake, defective absorption (i.e., Crohn’s disease or celiac disease), abnormal metabolism or increased requirements during pregnancy or breastfeeding, some genetic disorders, certain medicines (i.e., phenytoin, sulfasalazine, etc.), alcohol consumption, etc. Its deficiency may cause glossitis, diarrhoea, depression, confusion, anemia, grey hair, mouth sores, poor growth, congenital deformities, swollen tongue, embryonic defects, altered memory and brain function, cardiovascular disease, leuco- and thrombocytopenia, particular neural tube defects, and malignancies, long-term risk of lower bone density, higher risk of potentially developing allergic diseases, etc. [8-10].
The solubility of folic acid is very poor (1.6 mg/L in water). It is heat sensitive and decompose rapidly in the presence of light [11]. Thus, the physicochemical properties of folic acid are very important while preparing the nutraceutical and pharmaceutical formulations in the pharmaceutical industries. Some of the recent scientific experiments proved that the Trivedi Effect®-Consciousness Energy Healing Treatment has improved the physicochemical properties, isotopic abundance, and bioavailability of many pharmaceutical/nutraceutical compounds [12-14]. The Trivedi Effect® is a natural and only scientifically proven phenomenon in which an individual can harness this energy from the “Universe” and transmit it anywhere on the planet via the possible mediation of neutrinos [15]. Every living being possesses a unique infinite and para-dimensional electromagnetic energy field surrounding the body known as “Biofield”. Energy Therapies accepted worldwide nowadays against various disease conditions and for better health and wellness [16-18]. Biofield Energy Healing therapy is recognized as a Complementary and Alternative Medicine (CAM) by the National Center of Complementary and Integrative Health (NCCIH) with other therapies, medicines, and practices such as traditional Chinese herbs and medicines, Ayurvedic medicine, aromatherapy, homeopathy, yoga, Tai Chi, Qi Gong, chiropractic/osteopathic manipulation, meditation, acupressure, acupuncture, hypnotherapy, Reiki, healing touch, movement therapy, naturopathy, cranial sacral therapy, etc. [19]. These CAM therapies have been adopted by most of the U.S.A. population [20]. The Trivedi Effect®-Consciousness Energy Healing Treatment also has the significant impact on the transformation of metals, ceramics, and polymer [21-23], organic compounds [24], microorganisms [25,26] the productivity of crops [27,28] and cancer cells [29,30].
To understand the isotope effects resulting from the alterations of the isotopic composition, the study on the natural stable isotope ratio analysis has many applications in the different field of sciences [31-33]. The sophisticated techniques like gas chromatography–mass spectrometry (GC-MS) and liquid chromatography–mass spectrometry (LC-MS), are widely used for the analysis of isotope ratio with sufficient precision [32]. Therefore, the LC-MS based structural characterization and the isotopic abundance ratio of PM+1/PM (2H/1H or 13C/12C or 17O/16O) in the Trivedi Effect®-Consciousness Energy Healing Treated folic acid was performed compared to the control sample.
Materials and Methods
Chemicals and eeagents
The test sample folic acid was purchased from Alfa Aesar, India. Similarly, other chemicals and solvents used in the experiments also purchased in India.
Consciousness energy healing treatment strategies
The test sample folic acid powder sample was divided into control and treated parts. The control sample did not receive the Biofield Energy Treatment. But the control sample was treated with a “sham” healer who did not have any knowledge about the Biofield Energy and its treatment. However, the treated part of folic acid has received the Trivedi Effect®-Consciousness Energy Healing Treatment remotely for 3 minutes under standard laboratory conditions by a well-known Biofield Energy Healer, Dahryn Trivedi, USA. Finally, both the samples were kept in sealed conditions and characterized using LC-MS analytical techniques.
Characterization
Liquid chromatography-mass spectrometry (LC-MS) Analysis and calculation of isotopic abundance ratio:
The LC-MS analysis of both the samples of folic acid was carried out with the help of LC-MS Thermo Fisher Scientific, USA equipped with an ion trap detector connected with a triple-stage quadrupole mass spectrometer. Thermo Scientific Synchronis C18 (Length-250mm X ID 4.6mm X 5 micron) reversed phase column was used, which maintained at 25˚C. The methanol and water (1:1) were used as a diluent for sample preparation. The injection volume was 10μL and the analyte was eluted using acetonitrile +10mM ammonium acetate (85:15) pumped at a constant flow rate of 1mL/min (total run time was 10min). Peaks were monitored at 220nm using the PDA detector. The mass spectrometric analysis was performed under ESI +ve ion mode. The natural abundance of each isotope (H, C, N, and O) can be predicted from the comparison of the height of the isotope peak with respect to the base peak. The values of the natural isotopic abundance of the common elements are obtained from the literature [33-36]. The LC-MS based isotopic abundance ratio (PM+1/PM) for the control and treated folic acid was calculated. The change in the isotopic abundance ratio was calculated using the following equation.
Results and Discussion
Liquid Chromatography-Mass Spectrometry (LC-MS)
The LC-MS chromatograms of both the folic acid samples showed the major peak at retention time (Rt) of 1.8 minutes (Figure 1). The peak area near Rt 1.8 minutes of the Biofield Energy Treated folic acid (6029494.3) was increased by 1.12% compared to the control sample (5963001.45). The increased peak area of the Biofield Energy Treated folic acid indicated that the solubility of folic acid was increased after the Trivedi Effect®-Consciousness Energy Healing Treatment. The solubility of folic acid is very poor and a major problem. Thus, the Biofield Energy Treated folic acid would be more soluble, bioavailable, and more efficacious nutraceutical and pharmaceutical formulations. The mass spectra of the control and Biofield Energy Treated samples corresponding to the Rt 1.8 minutes exhibited the existence of the molecular ion of folic acid (C19H20N7O6 +) adduct with hydrogen ion (Figure 2) at m/z 441.92 (calcd for C19H20N7O6 +, 442.15) along with the fragmented mass peaks at m/z 295.08, 267, 250.17, and 207.92 for C14H11N6O2 +, C12H15N2O5 +, C12H12NO5 + and C11H14NO3 + were observed in both the sample (Figures 2 & 3). The experimental data were well matched with the literature data [37].
Isotopic abundance ratio analysis
Both the folic acid samples showed the mass of a molecular ion at m/z 441.92 (calcd for C19H20N7O6 +, 442.15) with 100% relative abundance in the spectra. The theoretical calculation of isotopic peak PM+1 for the protonated folic acid presented as below:
m/z 442.92 = 24.24%
The calculated isotopic abundance of PM+1 value 24.24% was higher to the experimental value (16.1%) (Table 1). From the above calculation, it has been found that 13C and 15N have the major contribution to m/z 442.92. The LC-MS based isotopic abundance ratio analysis PM and PM+1 for folic acid at m/z 441.92 and 442.92, respectively of both the samples, which were obtained from the observed relative peak intensities of [M+] and [(M+1)+] peaks, respectively in the ESI-MS spectra (Table 1). The isotopic abundance ratio of PM+1/PM (2H/1H or 13C/12C or 15N/14N or 17O/16O) in treated folic acid was significantly increased by 81.37% compared to the control sample (Table 1). Thus, the 13C, 2H, 15N and 17O contributions from C19H20N7O6 + to m/z 442.92 in the treated folic acid was increased compared to the control sample.
LC-MS study confirmed the structure of folic acid. The isotopic abundance ratio of PM+1/PM (2H/1H or 13C/12C or 17O/16O) in the Biofield Energy Treated folic acid was significantly increased compared to the control sample. The altered isotopic composition in the Consciousness Energy Healing Treated folic acid might have altered the neutron to proton ratio in the nucleus via the possible mediation of neutrino. Neutrinos have the properties to change identities which interchange from one phase to another internally. The neutrinos have the ability to interact with protons and neutrons in the nucleus, which indicated a close relationship between neutrino and the isotope formation [15,32,33]. The isotopic abundance ratios 2H/1H or 13C/12C or 17O/16O would highly influence the atomic bond vibration of treated folic acid [38]. The increased isotopic abundance ratio and peak area of the Consciousness Energy Healing Treated folic acid may increase the chemical bond strength, increase its stability, more soluble, and bioavailability in the body. The Biofield Energy Treated folic acid would be more efficacious for the prevention and treatment of various diseases such as embryonic defects, clinical depression, megaloblastic anemia, altered memory and brain function, leuco- and thrombocytopenia, malignancies, neural tube defects, depression, allergic diseases, cardiovascular disease, and lower bone density, etc.
Conclusion
The Trivedi Effect®-Consciousness Energy Healing Treatment showed a significant impact on the isotopic abundance ratio of folic acid. The chromatographic spectra of both the samples at retention time 1.8 minutes exhibited the mass of the molecular ion peak at 441.92 (calcd for C19H20N7O6 +, 442.15) along with low molecular fragmented mass peaks at m/z 295.08, 267, 250.17, and 207.92 for C14H11N6O2 +, C12H15N2O5 +, C12H12NO5 +, and C11H14NO3 +, respectively were also observed. The peak area of the Consciousness Energy Healing Treated folic acid was increased by 1.12% compared to the control sample. The isotopic abundance ratio of PM+1/ PM (2H/1H or 13C/12C or 15N/14N or 17O/16O) in the treated folic acid was significantly increased by 81.37% compared with the control sample. Hence, the 13C, 2H, 15N and 17O contributions from C19H20N7O6+ to m/z 442.92 in the treated sample were significantly increased compared with the control sample. The changes in isotopic abundance and mass peak intensities might be due to the changes in nuclei possibly through the interference of neutrino particles via the Trivedi Effect®-Consciousness Energy Healing Treatment. The increased isotopic abundance ratio and peak area of the treated folic acid may increase the chemical bond strength, increase its stability, improve solubility, and bioavailability in the body. The new form of Biofield Energy Treated folic acid could be used for better designing novel pharmaceutical formulations that might offer better therapeutic response against poor growth, diarrhea, confusion, glossitis, depression, anemia, gray hair, mouth sores, swollen tongue, congenital deformities, embryonic defects, altered memory and brain function, leuco- and thrombocytopenia, cardiovascular disease, neural tube defects, and malignancies, risk of potentially developing allergic diseases, long-term risk of lower bone density, etc.
Acknowledgment
The authors are grateful to Sophisticated Instrumentation Centre for Applied Research & Testing (SICART) India, Trivedi Science, Trivedi Global, Inc., and Trivedi Master Wellness for their assistance and support during this work.
To know more about Juniper Publishers please click on: https://juniperpublishers.com/aboutus.php
For more articles in Open Access Journal of Reviews & Research please click on: https://juniperpublishers.com/arr/index.php
To know more about Open Access Journals please click on: https://juniperpublishers.com/journals.php
#Juniper Publishers Review#Juniper Publishers Indexing#juniper publishers#Quality Research Publisher#reviews research paper#Juniper Publishers Contact address
0 notes
Text
Assessment of Knowledge about the BARC Centre and Satisfaction with the Educational Services Available
Abstract
The aim if this proposal is to determine knowledge in the general population about arthritis and immunology disorders ; to ascertain if this has improved in the decade since our Needs Assessment; and the satisfaction with the educational material now available to support communities and arthritis sufferers.
Background
BARC (Birmingham Arthritis Resource Centre) was set up to provide education and support to people with arthritis and their carers, based on a formal Needs Assessment. BARC aims to promote self-coping to help people to deal with the physical and social disabilities caused by their disease. It is cited in the city centre public library and works alongside the regular medical NHS service provision. Services for Rheumatology have always had lower priority and funding than those for acute services such as Cancer and Heart disease. In addition they have historically been somewhat restricted in the West Midlands (the UK region where Birmingham is the central city) compared to the rest of the UK. The picture is also complicated by the high percentage of ethnic minority groups locally (generally referred to as BME groups- Black and Minority Ethnic). Birmingham is set to become the first major UK city where BME groups will become the majority within the next ten years. There is evidence that “excluded groups” - such as immigrants, the poor and the less-well educated have poorer health but do not access the NHS in the same way as the white middle-class population for a variety of reasons, including cultural, language and poverty barriers. This is clearly relevant to the wider European scene where there is increasing pressure from immigration while currently both health and social programs are threatened by the financial recession.
The BARC project was started a decade ago with a formal research process to determine the extent of current services and what people wanted. This “Needs Assessment” showed that both medical profession and public perceived a need for more information provided in an informal setting (ie a non-medical setting) - and wanted it in a range of languages Adab et al. [1]. There was also a widespread desire for more support services for patients. The BARC centre was set up on the basis of this in space provided by the City in the Central Library and is manned by volunteers. These have been selected and trained by the Centre manager, Chan Gordhan, who has a long background in social and voluntary work. The volunteers come from a range of ethnic backgrounds and importantly they have all had some personal rheumatic problem. Thus they fit what the UK government is now calling “expert patients” - and promoting the idea that they are best placed to help others since they have learnt how to cope. Interestingly our experience shows that volunteering to help others also empowers them to deal with their own lives, so they should also be the best placed group to teach us how to empower our clients. Our data also shows that the BARC service is wanted as well as needed locally.
The key point in developing any new service is to provide an evidence base for it. BARC set out to do this from the outset. Following the initial “Needs Assessment” We carried out a focus group study to determine what patients from BME groups were looking for from the local health services Bacon et al. [2]. A key factor expressed by the participants was the desire to be listened too. They were dissatisfied with their doctors who were seen to lack time to take in the patients broader complaints. This echoes wider concerns about poor doctor patient communications an area which the Royal College of Physicians is holding an enquiry into at present.
BARC has set up sympathetic listening as one of the basic parts of the service Gordhan [3,4]. This is provided by trained volunteers. They are themselves patients and come from a range of ethnic and linguistic backgrounds, so that they are able to provide culturally sensitive guidance to clients. We have collected data on who has attended and how satisfied they are with the service provided Treharne [5]. Approximately 40% of attendees come from the BME groups, similar to the general population. Thus we are getting through to target populations - but not in large enough numbers. We have also had high gradings for client satisfaction.
We have also addressed the need for relevant patienteducation material understandable to those for whom English is not their mother tongue. We recently completed a set of educational leaflets, designed as “bottom-up” material that is based on questions people actually ask rather than information doctors think patients ought to know. They are in simple English, avoiding technical terms, so as to be easily understood. The first six have been translated into Urdu and recorded on CD’s in both languages, as well as in print format with a few cartoons to illustrate them. A preliminary piece of market research in the BARC Centre shows that the volunteers think they are what is needed and a small sample of clients listening to the first one agreed. The Urdu translation has also been approved by a range of Indian colleagues as being both true to the English information and understandable by a range of local language speakers. The translation is not strict Urdu but includes phrases used in Bollywood films (watched by all the local S. Asian groups) as well as some English words generally used in the version of “Urdu” widely used around Birmingham.
A questionnaire-based assessment of the first of these CD’s – on Understanding Arthritis – showed that clients gave it high scores for clarity of information and obtaining information that they wanted. In general they found the CD helped them to cope Sharif [6]. We are just completing an assessment of the CD on rheumatoid arthritis and the outcome is very exciting. The challenge was far greater here as the usefulness of the CD was examined in a specialist RA clinic which already had a highly trained specialist nurse providing explanations and support to patients. Despite this the comments made at the focus groups demonstrated that the study participants had found the additional BARC service a major help Kumar et al. [7]. There is now patient pressure to set up such a service on a regular basis in the hospital setting. This would be in line with the recent Report from the influential Kings Fund which noted a lack of understanding on the quality of RA care and the struggle many RA patients have to access quality care Kings Fund [8].
In the same way, we have struggled to reach our target for new attendees at the BARC centre, despite the evidence for the need for and the success of the BARC service. Total numbers accessing the BARC service, including phone calls and web-site hits, have increased year-on year but surprisingly there has been no increase in personal visitors. A number of community centres have asked for the manager to go out to specific groups with promotional and educational talks. This alternative approach has proved very popular but many attendees have said they were not aware of the BARC centre. These outreach sessions are demanding on Chan Gordhan’s time and there is an excellent service available at the library. Thus the next essential step is a study of why people are not coming in the predicted numbers.
Hypothesis
We propose that the population in general tend to downplay the importance of their musculo-skeletal problems. This is reinforced by the poor publicity that arthritic diseases get compared to some others. Analysis of the relative importance given by press or TV showed that heart disease and cancer got far more attention and were treated as serious scientific problems. Rheumatic diseases by contrast were seen as “lifestyle problems” for which there was no real medical treatment. The existence of a ground-breaking local service does not appear to have changed that mould to any major extent. Each time that the BARC Centre has been discussed on local radio there has been a sharp rise in client enquiries – but only for a short period. We intend to analyse the degree of local awareness of the BARC and at the same time look further into the responses of those who do actually come to seek help.
Methods
The first aspect will be carried out by collecting data about knowledge of BARC and satisfaction with current educational support using standardised questionnaires. This will target both a random population (people accessing the Central Library for any purpose) and specific communities such as local Sikh and Somali populations who have already identified a perceived need for an increased service for their groups. A minimum of 200 library people will be sampled at random in each grouping. The second part (analysis of satisfaction with current services) will be completed by analysis of the data collected over the past two years from attendees at the Centre, who are all asked to complete such a form. The data from this project will be compared to that obtained 10 years ago in the original Needs Assessment
Broader aspects of Fellowship
The advantages of taking on this project would be to widen your experience into qualitative research and introduce you to a new but important area of rheumatology, patient education. The latter has many messages for someone practicing in a major city with an immigrant population and you have already reported working with several ethnic minority groups in Kosova. We have been thinking about this project for some time, so there are some things already in place to facilitate your research. We have already trailed a simple questionnaire for these assessments. A sociology student is currently using these to collect some preliminary data from library visitors. That experience will focus the further development of the project. A trained health psychologist is available to help with analysing the questionnaires and the unstructured material coming from the “free comment” section at the end of each form. In the same way, the set of forms collected from clients attending the Centre in its early years have been analysed and will form a useful comparison with the planned analysis of the comments collected from recent clients.
This exercise will definitely lead to at least one published paper. The methodologies used will be of value to you in assessing the worth of conventional treatment options across the field of rheumatology. Our speciality deals with incurable chronic disease and there is increasing evidence that patients have a different perspective on the outcome to their doctors Hewlett [9]. Helping people to cope with chronic disability, improving their life by addressing their real concerns rather than measuring “medical outcomes” like degree of swelling or ESR, is becoming increasingly important. Finding ways of reaching out to the large percentage of the population who have a disability related to a rheumatic problem is also essential to persuade politicians to take the subject seriously and invest in it. Thus the experience gained from this would be advantageous to your career in many ways – and I believe you would find working in BARC both interesting and rewarding. Once in place here you can join in all the usual University Rheumatology Departmental activities, from seminars to clinical meetings. We would also work to get you some exposure to Rheumatoid Arthritis clinics as an observer on an informal basis. That will be easier to do with colleagues on the ground than to set up formally in advance with the current NHS bureaucracy [10].
Conclusion
You will have free time to catch up on your reading, particularly on the fairly large literature on self-coping and on what people expect from health services. You would need this to write a good paper and I would expect you to write up a comprehensive introduction and methods section well before data collection has been completed. Of course we will be available to discuss that with you but it will be your responsibility to produce the first version. I believe that an important part of such a fellowship is learning how to plan and write up your own research projects for the future.
To Know More About Orthopedics and Rheumatology Open Access Journal Please click on: https://juniperpublishers.com/oroaj/index.php
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com/oroaj/index.php
For more about Juniper Publishers Please click on: https://juniperpublishers0.wixsite.com/juniperpublishers
#juniper publisher contact address#juniper publisher journals#juniper publisher reviews#osteoporosis
0 notes
Text
Juniper Publishers
JuniperPublishers
Juniper Publishers. is established with the aim of spreading quality scientific information to the research community throughout the universe. Juniper Publishers as Open Access publishers, strive to offer the best in class online science publications. Juniper Publishers as an open Access process eliminates the barriers associated with the older publication models, thus matching up with the rapidity of the twenty-first century. Juniper Publishers Inc main areas of interest lie in the fields of science, engineering and other related areas. Juniper Publishers is a platform for professors and researchers who aspire to give out quality information based on their research and expertise, in an attempt to aid scholars/researchers in their field of interest with the latest information.
For More Open Access Journals in Juniper Publishers Click on: https://juniperpublishers.com/journals.php
https://www.scienceopen.com/user/9f93b14f-c289-4e21-b3c8-8f448ea424ab
0 notes
Text
Juniper Publishers-Open Access Journal of Case Studies
Did Primary Health Care Doctors Lose the Battle with the Specialist and Consultants?
Authored by Manal Ali Ghandour
Opinion
Many organizations claim to be “Primary Healthcare (PHC) focused” and working on preventive measures and strategies. However, when you look to the number of initiatives or projects planned for preventive medicine (PM) and (PHC) in comparison to secondary and Tertiary care initiatives & projects, you will notice that Secondary and Tertiary care are getting up to 70% of the budget or more; thus in some places, one hospital will be a located a budget equal to 100 facilities working in preventive medicine and primary health care. Therefore, unless we see a strategic shift in the budget allocation and that (PM) and (PHC) sectors are allocated 60% or more of the budget, then I cannot believe that the Healthcare System is “Primary Healthcare &Preventive Medicine focused” [1].
On the grounds, Primary Healthcare Doctors (PHDs) had lost the battle with specialists and consultants due to different set ups and regulations that results in giving more support and gratitude to the specialist and the consultant while the PHDs get only struggles and I will explain why. There are four perspectives that support the specialists and consultants and make them well equipped with knowledge and environmental factors while making GPs and alike doctors struggle.
The first perspective is, the scope of practice: GP is required to know everything. While the specialist or Consultants (Spec & Cons) are more in depth prepared to deal with a system or two or one organ. So if Spec & Cons Can reaches mastery after having 10,000 hours practice in one subject, GPs reach nowhere for the same number of hours, e.g. they will not become specialist or consultant in certain field [2].
Also, from the Environmental perspective: Spec. & Cons. are given more equipment, can do sophisticated procedures and allowed to request all types of investigations. Also they are provided with specialized intelligent EMR and reasonable appointment time and referrals. In short, Spec. & Cons. are prepared to succeed, while GPs are provided with basic equipment, basic health record system that is broad and has no sense of intelligence. Also they are booked with many patients for very short time of consultation ranging between 7 to 20 minutes. When GP refers a patient, the patient is treated with least priority and thus booked the last on the Specialist or Consultant’s list. Thus GPs are prone for failure and poor outcomes.
Moreover, to be Licensed to Practicee.g in Dubai Healthcare City; GPs should have two years’ experience, and one year internship, while Specialist should have 2-5 years’ experience and 3years of residency or more. So on minimal level GP with 3 years of proper practice will be competing with Specialist who has 5 years of experience.
Looking into continuing education perspective, the GP needs to keep abreast with very huge knowledge, as one new disease will be discovered in every year (at least) and many drugs are added on yearly bases that he should know. For example, 22 new drugs were approved in 2016 by USA FDA alone and there are many countries who are introducing new medications every year. Lastly GPs are rarely involved in any researches or get any sort of feedback on their services. On the other hand, Specialists rarely encounter discovering a new disease or get 1-2 new drugs released per year. They get different feedbacks from incident reports, pharmacists, researches and audits. So they are helped for internal and external continuous improvements [3].
Hence, as a Patient, if you had the choice where will you go for treatment? Definitely patients prefer to go to consultants and specialists due to all reasons mentioned before. The consultants and specialists are equipped with many success factors, specially speed of appointment, investigations, diagnosis and treatment.
So what solutions we can adapt to improve GP practice? There are many solutions that can be used individually or consequently or all together:
Provide EMR systems that classify cases rather than taking them as general cases (chest case, heart case, asthma sheet, pediatric sheet etc.
Impede dictionaries and guidelines in HIS systems, use intelligent differential diagnosis, free lab and radiology access, and add quality checks and auditing to the work processes.
Consultant and Specialist are required to have 80CME hours to keep on top of their profession and get renewal of license. GPs should be offered at least, 160CME from their practice hours to keep up to date with medical and technology advances [4].
Segregate GPs into specialties, meaning each doctor gets more cases on certain problems as if he is going to specialize; so we need to have Asthma GP, Heart Problems GP and Diabetes GP. In addition to the general cases they see, they will be able to focus and follow up on certain cases with higher degree of effectiveness and will work closely with one type of specialty and make referral easy and get proper feedback [5].
Involve them into more research and case studies building.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Case Studies please click on: https://juniperpublishers.com/jojcs/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/jojcs/JOJCS.MS.ID.555602.php
#Juniper Publishers#Juniper Publishers Address#juniper publishers contact info#Case Reports#Critical Care Medicine#Surgical case reports#Epidemiology#General Surgery Genetics
0 notes
Text
Juniper Publishers- Open Access Journal of Environmental Sciences & Natural Resources

Waste Water Treatment by Environmental Microbiology
Authored by Maulin P Shah
Mini Review
Even formerly the discovery of the life of microorganisms, the man produced fermented foods and feed. Also degrading activity of microorganisms used in human waste, which is naturally biodegradable. However, for large-scale treatment, the man has had to devise artificial processes competition degrading activity of naturally occurring microorganisms. Microbiologists, engineers and chemists have worked hand in hand in this regard, now we know that for biodegradable materials, other than human waste, the process is also true. These biological systems for waste belonging to one of the largest area for biotechnological applications. Usually the goal of biotechnology products synthesized using an especially pure isolated strain of microorganisms under optimum conditions. Defined nutrient media (source Carbon, energy source, nitrogen, sulphur, phosphorus, trace elements and vitamins) exposed uses. Growth and yield of biomass and cultural conditions Related to the properties of pure strains. The production of antibiotics, a valuable product is an example of this development in the field of traditional biotechnology.
Waste treatment Biotechnology is significantly different from traditional processes. First, there are no profit-oriented commercial products are produced apart from cleaner wastewater for a better environment that will soon be invaluable. Other wastes are often mixed. Finally, a pure culture cannot be used and cannot rely on the natural mixed population or the enrichment of mixed cultures, if possible. The magnitude of the economy is therefore very different. Industrial microbiologists recognized the utility of microorganisms in waste treatment in 1914, with the development of a highly versatile biological treatment unit known as activated sludge processes. This process depends on a mixed culture of natural microorganisms, each having the capacity to degrade the components of a fraction of waste and the possibilities coexisting together. Recent advances in research and development to improve Flock biological training and reduce inoculation of sludge above the system treat specially adapted and cultured microorganisms. Currently, the crop that is capable of degrading certain priority toxic substances and undesirable compounds in the waste streams are already available. With the advent of genetic engineering, some microorganisms can be designed and adapted to degrade certain types of waste. However, the release of these genetically modified micro-organisms can negatively affect the ecosystem as the chemical waste nightmare that man has created. Upon learning this, man has now developed an in-depth research into the sequelae of these strains after its application on a large scale.
The present state of the art is complemented by the existing bacterial population of bacterial strains which are capable of reducing the higher level or with strains which are capable of decomposing compounds of those previously considered non-biodegradable. This paper discusses the poor degradable substances found in industrial wastes that are now subject to microbial decomposition. Aerobic metabolism consists of two processes: first, the transfer of electrons from the substrate to organic oxygen - as a source of energy for the cells, and secondly, by adding oxygen organic substrate - preparing the substrate for metabolism. The degradation of xenobiotics and difficult degradable compounds is important for the second part. The aromatic compounds, the secession of the cycles depends on the oxygen. The availability of molecular oxygen for the reaction depends on several enzymes. Studies on the anaerobic degradation of organic compounds are limited, but the process will be important and attractive in the near future. In nature, many microorganisms used for the growth of hydrocarbons and the energy source. The microbes oxidize the terminal methyl group in the aliphatic hydrocarbon. Become a hydrocarbon fatty acid. Generally, each species can degrade limited types of hydrocarbons. For example, Methanomonas methanooxidans can attack only methane, while Nocardia Paraffinicum and certain species of Pseudomonas can use several hydrocarbons, not all of which are necessarily present in the oil.
Benzenoid structures are the most common organic compounds in nature, and microorganisms attack them fairly well. However, aromatic polycyclics and those with rare substituents (e.g., polychlorinated biphenyls) are difficult to decompose. The degradation of the aromatic compounds begins to split the ring. Examples of microbes that carry this attack include Pseudomonas stutzeri, Pseudomonas mendocina, Psudomonas putida and P ovals.
Halogen compounds are used as solvents, aerosols, lead scavengers, fumigants and nematicides, among others. The species of Pseudomonas and Xantobacter autophicus are capable of degrading these compounds. The halogenated aromatic compounds are used as solvents, lubricants, intermediates in the synthesis, insulators, plasticizers, etc., degrade with respect to the halocatocalic formation or before the cleavage of the dehalogenation of the ring. Examples of such microorganisms are Pseudomonas and Athrobacter species. Nitro aromatic compounds used in the production of paints, medicines, pesticides, explosives and industrial solvents are toxic. The simpler compounds are completely biodegradable nitro aromatic complexes such as 2,4,6-trinitrotoluene is not degraded. Under aerobic conditions, the polymerization may take place under anaerobic conditions; Amine conversion can take place. Polychlorinated biphenyls used in transformer oil, capacitor dielectrics and heat transfer fluids are toxic to animals and humans. The species Acinetobacter and Alcaligenes are able to transform many PCBs. PCBs containing more than four are resistant to chlorine degradation.
Xenobiotics and pollutants are released into the environment by point sources or dispersed by consumers and users of the final product. With appropriate destruction information regarding the pollution of this waste consumed and with the appropriate control of the system institution efficient for the collection and treatment of waste, often complex physical and chemical properties of fractions of waste can be controlled. Thus, the use of these microorganisms in the degradation of the contaminants can be optimized. Experiments with pure cultures of the individual substrates form the basis of the collective knowledge of the biosynthetic pathways of the compounds which are not very degradable in microorganisms. After pure culture is available, the development of biotechnological processes is possible. For the isolation of microorganisms with biodegradable resources, microbiologists use the technique of enrichment culture. The procedure is to allow microorganisms with growth potential in a medium with low degradable compounds and a nutrient source limiting essential growth. Only micro-organisms that can decompose this substance will grow.
A number of subcultures evaluate the success of the enrichment. Wastewater, where many microorganisms come in contact with xenobiotics, is a common source of enrichment for bacteria with degradation capacity. However, isolates from the natural environment in which compounds of interest have been found are generally successful. These include samples from industrial production lines, soil treated with pesticides, landfills and wastewater treatment. Fermentation processes are generally conventional, from the preparation of capillary inoculums and sequential seeding to fermentators up to 10,000 litres. Although high, sterile mixed conditions are maintained to protect against contamination by salmonella, staphylococci and streptococci. Cultural conditions are maintained products of microorganisms that are repressed and conditioned their final environment. Methods of centrifugation or filtration which are used for cell concentration. Spore formation was air dried and not lyophilized. The cultures are then mixed with additives before final packaging. For significant progress in the microbial digestion of waste, it is necessary to identify organic chemicals that resist degradation in conventional waste treatment plants. After identification, the dismantling of existing plant protection products can now be improved or specialized technology suitable for their biodegradation can be obtained.
Among the organic chemicals in the EPA list of priority contaminants are pesticides and metabolites, phenolic compounds, halogenated, aroma nitro aromatics, chloroaromatics, PCBs, phthalate esters, polycyclic aromatic hydrocarbons and nitrosamines. This EPA list is helpful in determining the direction of research to improve the system for waste water treatment. The biomass consists of cellulose, hemicellulose and lignin. Lignin acts as a cementing material in the lignocellulosic material, and protects the structure of microbial degradation. Biodegradation of lignin is important because of the increasing number of industrial uses. Lignosulfonate, which are resistant to biodegradation of lignin, waste sulphite process products in 'the pulp and paper. White rot fungi can degrade lignosulfonates. Other mushrooms and mixed microbes promote precipitation through poliplerization. Commercial detergents containing 10% to 20% of surface-active agents for cleaning. Anionic surfactants are not biodegradable. Substituted level alkilbcnzcnsulfonata is more biodegradable, but are deposited in the sewer system. Cultures of microorganisms adapted for degradation of alkyl sulphates and alkyl sulfonates was very fast. Currently, 3,500 buoys are in use (40,000 colours and pigments to 7,000 different chemical structure). Therefore, we cannot generalize their biodegradability. Textiles and paint industries are responsible for replacing colours in the environment, although in small quantities. The model for the biodegradation activity Pteudomon M type on azo dyes for the production of biomass, CO2, H2O and NH3. In real situations, using a mixed culture adapted microorganisms.
Research on biodegradation of xenobiotics and pollutants to accumulate. The results of microbial, biological and genetic research will ultimately improve the practical application of methods of treatment on an industrial scale. With a higher level of sophistication to be achieved, more and more specific microbial species for biodegradation of the waste stream will be used. Ideally, the waste using microorganisms should emulate industrial fermenters. However, aseptic conditions are not possible, and the system is faced with a different composition, temperature and volume. With the ever changing toxic loads, micro-organisms can be harmed. Regularly feeding can wash desirable strains. However, regardless of the problems encountered, several microbial processes have now been successful. Special mixed culture of bacteria mutants for specific types of waste are now available in the market. They are far more efficient in how they consume less energy than conventional systems. Biological processes are now more attractive, effective and most importantly, economical.
Conclusion
With genetic engineering technology, some of the activities of microbial cultures are now a reality. This has led to new approaches to the treatment of waste. New microbial species that are genetically modified, and that cannot be found in nature may be patentable. The accumulation of research and study, as well as the results of the current state of the art application of biotechnology is the treatment of waste will lead to a more efficient system.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Environmental Sciences & Natural Resources please click on: https://juniperpublishers.com/ijesnr/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/ijesnr/IJESNR.MS.ID.555576.php
#Juniper Publishers#Juniper Publishers Address#Juniper Publishers Contact Number#Aquatic Ecology#Environmental Chemistry#Geodesy#Hydrology#Molecular Ecology
0 notes
Text
Juniper Publishers Contact Number
Juniper Publishers Contact Number Phone: +1-805-200-4030
https://g.page/Juniper_Publishers?share
#Juniper Publishers Address#Juniper Publishers Contact Info#Juniper Publishers#More About Juniper Publishers
0 notes
Text
Juniper Publishers Contact Number

Juniper Publishers Contact Number
Phone: +1-805-200-4030
https://g.page/Juniper_Publishers?share
#Juniper Publishers Address#Juniper Publishers Contact Info#Juniper Publishers Contact Number#More about Juniper Publishers
0 notes
Text
Juniper Publishers Contact Number

Phone: +1–805–200–4030
(link: https://g.page/Juniper_Publishers?share) g.page/Juniper_Publis… @Juniper_publish
0 notes
Text
Juniper Publishers Contact Number

Juniper Publishers Contact Number
Phone: +1–805–200–4030
https://g.page/Juniper_Publishers?share
#More About Juniper Publishers#Juniper Publishers Contact Number#Juniper Publishers Contact Info#Juniper Publishers Address
0 notes
Text
A Comparative Analysis of the Cost Effectiveness of Five Advanced Skin Substitutes in the Treatment of Foot Ulcers in Patients with Diabetes- Juniper Publishers
Juniper Publishers- Open Access Journal of Annals of Reviews & Research
A Comparative Analysis of the Cost Effectiveness of Five Advanced Skin Substitutes in the Treatment of Foot Ulcers in Patients with Diabetes- Juniper Publishers
Authored by Robert Snyder
Abstract
Objective: The purpose of this economic analysis was to generate the cost-effectiveness of five (5) advanced skin substitutes/ Cell/Tissue based Products (CTPs) in the treatment of foot ulcers in patients with diabetes (DFUs): ActiGraft® (RedDress, Pardes Hanna, Israel); Apligraf® (Organogenesis, Canton, MA); Dermagraft® (Organogenesis, Cant-on, MA) ; Grafix Core® (Smith & Nephew, Andover, MA) and EpiFix® (MiMedx, Marietta, GA).
Methods: For each skin substitute product, three data points were central to the analysis: Number of applications over a 12-week course of treatment; complete healing efficacy over a 12-week course of treatment; product cost per application; the number of applications and complete healing efficacy were obtained from seven established published clinical studies. Inclusion/Exclusion criteria included either a randomized controlled trial, prospective cohort, or retrospective cohort design that included at least two study arms; reported wound healing at 12 or 16 weeks, reported number of application of products used to achieve healing and a minimum 40 subjects in the primary treatment arm. Due to the complexities of cost-benefit analysis and difficulties encountered when comparing research (i.e. different run-in periods, numbers of subjects and variable endpoints) the study selection for Apligraf, Dermagraft, Grafix and Epifix used inclusion/exclusion criteria from Samsell et al. For Actigraft, study selection was limited to a pilot study.
Results: A 12-week product cost of the CPT’s analyzed ranged from $2,120 to $7,647. ActiGraft had a product cost advantage ranging from $1,245 to $5,527 over 12 weeks. The cost premium for other skin substitutes ranged from 59 to 261%. The 4-week product cost ranged from $1,060 to $4,840. ActiGraft had a product cost advantage ranging from $1,710 to $3,780 over 4 weeks. The cost premium for other skin substitutes ranges from 161 to 357%. The weighted average treatment cost ranged from $5,505 to $11,783. ActiGraft had a cost advantage ranging from $2,504 to $6,278. The cost premium for other skin substitutes ranges from 45 to 114%. ActiGraft had a cost advantage ranging from $81 to $6,279 in the hospital outpatient setting and from $1,245 to $5,527 in the physician office setting. The cost premium for other skin substitutes ranges from 2 to 154% in the hospital outpatient setting and from 55 to 243% in the physician office setting. Standardized Effective Analysis (SEA) ranged from 4 to 18 patients per 100 healed in the hospital outpatient setting, and 5 to 32 patients per 100 healed in the physician office setting. ActiGraft had the greatest SEA in both settings. Additionally, ActiGraft offered the lowest cost per cm2 while delivering the highest healing efficacy. ActiGraft is autologous, prepared from the patient’s own whole blood at the point of care. Unlike other CTP’s in this analysis ActiGraft had no biologic material wastage.
Conclusion: This head-to-head comparison showed that ActiGraft was more cost efficient as an advanced therapy for DFU’s when compared to the four (4) other advanced products analyzed. However, the ActiGraft data sourced from a pilot study presents limitations for comparison with studies meeting Samsell’s criteria. It is the authors’ intention to update this analysis when future published studies meet this benchmark.
Keywords: Diabetic foot ulcers; Economic analysis; Cell/tissue-based products; comparative analysis
Abbreviations: CTP’S: Cell/Tissue based Products; SEA: Standardized effective analysis; LEA: Lower extremity amputation; CMS: Centers for Medicare and Medicaid Service; PQRS: Physician Quality Reporting System; ITT: Intent-to-treat ; PAR: Percent area reduction; PP: Per-protocol; DFU: diabetic foot ulcers; SOC: standard of care; BLCC: Bioengineered living cellular construct; WAC: Wholesale Acquisition Cost; OPPS: Outpatient Prospective Payment System; WAVG: Weighted average treatment cost
Introduction
In the United States, it is reported that chronic wounds affect approximately 6.5 million patients. The incidence of chronic wounds is expected to increase as our population ages. The impact of chronic wounds on the health and quality of life of patients and their families should not be underestimated. Wound healing and tissue regeneration represent a well-orchestrated series of events that consists of highly integrated biological and molecular processes that includes cellular migration and proliferation, and of extracellular matrix deposition and remodeling. Certain metabolic and pathophysiologic conditions such as foot ulcers in patients with diabetes can deleteriously impact the normal physiologic process so that healing is impaired or delayed, resulting in chronic, non-healing wounds. The financial burden imposed by chronic wounds on the healthcare system cannot be understated. Approximately 15% of Medicare subpopulations (8.2 million) had at least one type of wound or infection. Total Medicare spending estimates for all wound types ranged from $28.1 to $96.8 billion. Such profound economic trends emphasize the importance of using advanced wound-healing modalities as adjuvant therapies that work synergistically with standard wound care regimens. Advanced treatment modalities that promote rapid and complete healing may reduce the risk of amputation and can substantially improve quality of life while decreasing financial burdens to the individual and society overall. Based upon the paucity of data in this area, the results of a comparative cost analysis could be useful in guiding clinicians towards therapies that are both effective and cost efficient when considering a treatment plan for patients with non-healing lower extremity wounds particularly recalcitrant foot ulcers in patients with diabetes.
There are approximately 34.2 million patients with diabetes in the United States representing 10.5% of the population. With rates of obesity soaring, it is likely that this number will increase exponentially. In 2017, the total estimated cost of diagnosed diabetes in the US was $327 billion [1]. Geiss et al. [2] opined that after years of decline, the rate of amputations increased by 50% between 2009 and 2015 to 4.6 for every 1000 adults with the highest numbers observed among young adults (age 18-44 years) and those in middle age (45-64 years) . These groups were more likely to be uninsured and disparate populations were 4 times more likely to experience diabetes-related amputation [2]. A systematic review suggested the incidence of lower extremity amputation (LEA) in the diabetic population ranged from 78-704 per 100,000 person years and the relative risks between diabetic and non-diabetic patients varied between 7.4 and 41.3. Therefore, published data are conflicting. However, it is likely that more than 60% of non-traumatic lower limb amputations occur in patient with diabetes [3].
Furthermore, it remains clear that LEA in this demographic results in higher mortality, reduced quality of life, and increased medical costs. For example, in 2010, 73,000 non-traumatic lower limb amputations were performed in the US due to diabetes, at an average cost of $70,434. Brownrigg et al. [4] suggests that a foot ulcer is the initial event in more than 85% of major amputations performed on people with diabetes. Even more distressing is the possibility that up to 50% of patients with diabetes who undergo amputation will die within 2 years 7. Therefore, aggressive and specialized care remains critical when patients with diabetes present with a foot ulcer and must be facilitated in a cost-efficient manner. Skin substitutes/ CTP’s are frequently used to treat chronic diabetic foot ulcers and there are numerous advanced skin substitutes on the market. Samsell [5] conducted a retrospective cost analysis comparing eight skin substitutes using previously published efficacy rates combined with the Centers for Medicare and Medicaid Services (CMS) 2018 cost data. They included seven studies that described the overall value rates for treatment of DFU’s using the skin substitutes. These studies are actively being used by regulatory bodies, healthcare institutions and reimbursement agencies to generate usage decisions. Due to the complexities of cost-benefit analysis and difficulties encountered when comparing research (i.e. different run-in periods, numbers of subjects and variable endpoints) the study selection for Apligraf, Dermagraft, Grafix and Epifix used inclusion/exclusion criteria from this study.39 However, for Actigraft the study selection was limited to a pilot study.
The Problem
A seminal study entitled “An Economic Evaluation of the Impact, Cost, and Medicare Policy Implications of Chronic Nonhealing Wounds,” analyzed the Medicare 5% Limited Data Set for calendar year 2014 and determined that chronic nonhealing wounds impact nearly 15% (8.2 million) of Medicare beneficiaries, far more than suggested by previous studies. Furthermore, conservative estimates for total Medicare annual spending for all wound types ranged from $28.1 billion to $31.7 billion [8]. Treatment and management of infected or re-opened (dehisced) surgical wounds account for the highest per-wound costs. Hospital outpatient care drove the highest site-of-service costs, demonstrating the shift from hospital inpatient to outpatient services in the wound care space. In regard to site of service, hospital outpatient settings drove the greatest proportion of costs – demonstrating a major shift in costs from hospital inpatient to outpatient setting. However, Carter opined that unlike evidence-based medicine, there is less agreement on how to conduct economic analysis in healthcare, and universal guidelines for reporting these studies is lacking and “real-world data is almost non-existent. This has led to a paucity of economic data to support claims of cost benefit that require several key points in decision making (Figure 1).
During the early 2000s, the Centers for Medicare and Medicaid Services (CMS) established a hospital-based outpatient payment system with the purpose of providing continued care most notably in complex cases where patients did not necessarily require hospitalization. However, the established reimbursement system rewarded healthcare providers according to the sheer volume of interventions/procedures performed without a feedback system for quality of care, outcome, or patient-centered concerns. In order to create a financial/reimbursement paradigm shift, in 2006 CMS established the Physician Quality Reporting System (PQRS). With the Medicare patient population, this system integrated incentive payments to qualified healthcare professionals that properly documented quality measure data. However, in 2008 they also mandated that any US healthcare provider who fails to successfully report PQRS measures in 2016 will lose 4% of their Medicare revenue in 2018. CMS also monitors the hospital readmission rates of patients with chronic non-healing wounds [6]. It should be noted that approximately $17B or 65% of total readmissions are considered avoidable. Consequently, a new round of Medicare readmission penalties impacted 83% of hospitals thus far in 202013. Furthermore, it is estimated that 1.7M patients acquire healthcare associated infections. In January 2020, 786 hospitals had their Medicare reimbursement lowered 1% for having high hospital acquired infection rates. Within the last 10-20 years, the US healthcare system has been experiencing a paradigm shift into a quality-based-system. By 2024, wound care products alone could range from $15B-$22B15. In 2006, CMS established the Physician Quality Reporting System (PQRS), which initially provided incentive payments to qualified healthcare professionals reporting quality measure data on Medicare patients [6]. Now moving into the penalty phase, US healthcare providers who fail to successfully report PQRS measures in 2016 will lose 4% of their Medicare revenue in 2018 [6]. Hospital and nursing care represent the most expensive interventions: Advanced therapies could decrease or obviate the need for hospitalizations or frequent dressing changes.
Is Standard Care Effective?
In 1999, Margolis [7] meta-analysis determined the percentage of individuals with neuropathic diabetic foot ulcers receiving good wound care who heal within a defined period of time. After 20 weeks of good wound care, approximately 31% of diabetic neuropathic ulcers heal [8]. Similarly, after 12 weeks of good care, approximately 24% of neuropathic ulcers attain complete healing [8]. A recent meta-analysis by Parks et al. suggests that the percentage of diabetic foot ulcers healed with standard of care therapies alone have improved over the past 20 years. Their literature search yielded 16 randomized clinical trials that fit the selection criteria to be included in the meta-analysis [9]. Analysis of the percentage of wounds healed with standard of care therapy alone yielded the following results: 6 weeks (14.9% ± 13.0%), 12 weeks (33.4% ± 18.2%), 20 weeks (43% ± 0%)17. Although there has been improvement in healing rates utilizing standard of care, many ulcers in patients with diabetes may require advanced therapies to facilitate closure [9]. Interestingly, a paradigm shift in how advanced therapies are paid appears counter-intuitive to quality measures and pay for performance models (high costlow cost rather than evidence-based). In large part this is due to lack of evidence as it relates to cost effectiveness. Therefore, evidence must be tempered by the small number of available studies including variability in trial duration, baseline wound characteristics, and limitations in study quality. At the end of the day payers need more high-quality head-to-head comparisions to guide coverage and reimbursement allocation.
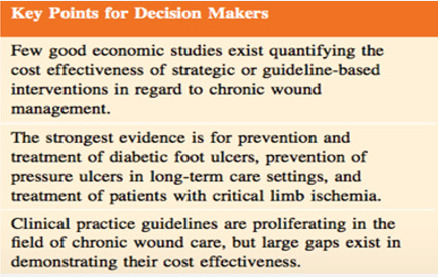
Due to the systemic implications of chronic non-healing wounds, it is critical that skilled medical personnel incorporate a holistic approach in their treatment pathways. It is important to be cognizant that chronic non-healing wounds are a symptom of a greater systemic disease process. Additionally, the treatment pathway of chronic wounds particularly in patients with diabetes, often involves extended hospital stays and long-term outpatient follow-up visits with costly advanced therapeutic intervention. To date, the strongest evidence is for prevention and treatment of diabetic foot ulcers, prevention of pressure ulcers in long term care settings and treatment of patients with critical limb ischemia. Clinical practice guidelines are proliferating in the field of chronic wound care, but large gaps exist in demonstrating their cost effectiveness. However, the immense economic and social impact of wounds in our society calls for allocation of a higher level of attention and resources to understand biological mechanisms underlying cutaneous wound complications.
Cell and Tissue Based Therapies
When wounds fail to achieve sufficient healing after 4 weeks of standard care, reassessment of underlying pathology and consideration of the need for advanced therapeutic agents should be undertaken. Snyder et al. demonstrated that a <50% PAR after 4 weeks of treatment predicts DFU failure to heal by 12 weeks [6]. Therefore, frequent reevaluation of the wound and its treatment is recommended. Advances in cell biology and tissue engineering have led to an increase in the quantity and quality of biological wound dressings. Many cell-based dressings utilize scaffolds which are designed to easily integrate with host tissue and provide an optimal environment for cell growth and differentiation. Cell and tissue-based products (CTP) are among some of the latest biotechnology treatment modalities in medicine. These treatment modalities can be defined as therapy in which cellular material is injected or otherwise transplanted into or on an area of medical concern (i.e. chronic non-healing wounds). CTPs may contain viable or nonviable cells, tissues, proteins, and other materials for which there is a rationale for benefit beyond that achievable with conventional wound coverings. There are three essential categories within the framework of CTP: allogenic, autologous and xenogeneic methodologies.
In autologous based cell therapies, the tissues/cells that are transplanted are derived from the patient’s own body. Autologous therapies have gained in popularity especially involving the treatment of foot ulcers in patients with diabetes (DFU’s). Some of the key benefits include biocompatibility, reduced risks associated with disease transmission observed with other grafts and cell allografts, and the minimal chance of rejection. For example, ActiGraft TM (RedDress, Israel) is a regenerative wound care solution comprising in vitro blood clots from a patient’s whole blood. Once applied, the blood clot tissue serves as a protective covering, biologic scaffold and wound microenvironment to promote the natural wound healing processes of the body [10]. In contrast to other CTP methodologies, autologous blood represents an unlimited resource which can be prepared and utilized immediately as a point of care therapy. Autologous blood tissue possesses several key characteristics of an ideal wound dressing. These include a robust structural framework, a conduit for water vapor transportation, elasticity, creation of bacterial barrier, absence of toxicity and antigenicity, antisepsis, hemostatic activity, ease of application and removal, minimal storage requirements, and reasonable expense.
Snyder [11] studied the safety and efficacy of an autologous blood clot product in the management of Texas 1A or 2A neuropathic diabetic foot ulcers in a prospective, multicenter, open label pilot study. Twenty patients were enrolled; 20 were analyzed in the intent-to-treat (ITT) population and 18 in the per-protocol (PP) group. The proportion of wounds healed in the ITT and PP populations were 13 out of 20 (65%) and 13 out of 18 (72.2%), respectively. Percent area reduction (PAR) for the ITT population at 4 and 12 weeks was 61.6% and 67.1%, respectively; the PARs for the PP population were 60.3% and 76.2% at 4 and 12 weeks, respectively. Mean times to wound healing were 59 days and 56 days in the ITT and PP populations, respectively. This study demonstrated that the blood clot tissue product was safe and efficacious for treating DFUs. An allograft is typically derived from organs, tissues or cells that are donated and developed from a genetically distinct individual of the same species. Some of the more commonly used allogenic CTP’s are Apligraf TM (Organogenesis, Canton, MA), Dermagraft TM (Organogenesis, Canton, MA) and homologous use therapies such as the Epifix TM (MiMedix, Marietta, Georgia) derived from amnion and chorion and Grafix Core (Smith & Nephew, Andover, MA).
Living CTP’s
Apligraf TM is a living bi-layered skin substitute. It is a living active dermal layer that is enriched with human keratinocytes and fibroblasts. This skin substitute is derived from human foreskin in a bovine Type I collagen matrix and a living active epidermal layer formed by human keratinocytes within the stratum corneum [12]. The upper epidermal layer is formed by human keratinocytes (epidermal cells). This advanced product consists of an array of growth factors, cytokines and various proteins essential for wound healing [12]. Falanga et al. [13] conducted the first randomized control study demonstrating Apligraf as an effective and safe mode of treatment for chronic, nonhealing VLU. This multicenter study was completed on 293 patients in an outpatient setting and examined VLU receiving either compression therapy alone compared with compression therapy and serial (up to 5) applications of the human skin equivalent, Apligraf [14]. This study found that treatment with bioengineered skin was more effective than compression therapy at its primary endpoint of 6 months, with 63% versus 49% of patients having completely healed, respectively, and the median time to complete wound closure was 61 versus 181 days, respectively, in the two groups [14]. In 2009, Edmonds [12] compared the efficacy and safety of Apligraf in combination with standard therapy versus standard therapy alone in the treatment of neuropathic diabetic foot ulcers. There were 82 randomized treatment groups, and 72 treated (33 Apligraf subjects and 39 standard therapy subjects [15]. By 12 weeks, 51.5% (17/33) Apligraf subjects had achieved complete wound closure compared with 26.3% (10/38) of standard therapy subjects [15].
Dermagraft is a living, single layer of human fibroblastderived dermal substitute approved as an adjunctive treatment for recalcitrant foot ulcers in patients with diabetes. Marston [14] performed a randomized, controlled, multicenter study at 35 sites across the United States. Three-hundred and fourteen patients were enrolled. Results demonstrated that foot ulcers in patients with diabetes that were present for greater than 6 weeks showed experienced greater clinical benefit with Dermagraft than patient treated with conventional therapy. At 12 weeks 30.0% (39 of 130) of the Dermagraft patients healed compared to 18.3% (21 of 115) in the control group (p=0.023).
Dehydrated Human Amnion/Chorion Membrane
Epifix TM is a dehydrated human amnion/chorion membrane (dHACM) allograft. This therapy represents a bioactive tissue matrix allograft composed of dHACM that preserves and contains multiple ECM proteins, growth factors, cytokines, and other specialty proteins27,28. Possible benefits of these cell-based therapies include modulation of chronic inflammatory states, paracrine signaling that stimulates and attracts healthy cells to the wound bed, and the integration of robust effector cells that help to orchestrate wound closure . In some of his earlier research, Zelen [1] facilitated a study to evaluate dehydrated human amniotic membrane (dHAM) allografts in patients with diabetic foot ulcers (DFU). The study population was identified from patients with chronic DFUs enrolled in a randomized trial comparing standard care with standard care with the addition of dHAM. “The study population was identified from patients with chronic DFUs enrolled in a randomized trial comparing standard care with standard care with the addition of dHAM.
The present study included patients that failed to heal (defined as <50% decrease in wound size after 6 weeks, or not completely healed by 12 weeks of treatment) with standard care. One week after withdrawal from the randomized trial, these patients were offered treatment with standard care and bi-weekly application of dHAM. Each patient was used as their own control to compare wound size reduction between treatment periods, and healing rates within the 12-week dHAM treatment period. Eleven patients were included in the study. Mean wound chronicity was 21.1 ± 12.4 weeks (range 11–54 weeks) and mean wound size was 4.7 ± 5.0cm2, at baseline. Complete healing was achieved in 55% by 4 weeks, 64% by 6 weeks and 91% by 12 weeks with bi-weekly dHAM application. Mean weeks to complete healing was 4.2 ± 3.1 weeks for the 10 patients healed. After 4 weeks of standard care, wounds had decreased in size an average of 26.8 ± 45.3% versus 87.6 ± 16.0% after 4 weeks of dHAM treatment (two applications; p <0.001). This study provided evidence that the incorporation of dHAM into standard of care for patients with chronic DFUs can be beneficial and that dHAM is a viable option for the treatment of recalcitrant DFUs”.
Cryopreserved Placental Membrane
Grafix Core (Smith & Nephew, Andover, MA) is a viable cryopreserved placental membrane (vCPM) used as an adjunctive treatment for recalcitrant foot ulcers. In patients with diabetes (DFU). A multicenter randomized controlled trial revealed that vCPM resulted in a higher proportion of wound closures when compared to good wound care: 62% versus 21% (p<0.01). Effectiveness was also gleaned from real world data in a retrospective analysis. These results mirrored previous RCT efficacy, thus supporting the benefits of vCPM for DFU management.
What Clinicians and Payers Want?
Despite evidence based upon prospective analysis, studies rarely address economic efficiency. Clinicians and payers continue to require head to head comparisons when making clinical and economic decisions. Zelen [1] studied a cohort of 100 patients and assessed the efficacy of EpiFix and Apligraf (MiMedx, Marietta, GA); Organogenesis Inc., Canton, MA, USA) versus standard of care (SOC) over a duration of 12 weeks. Inclusion criteria were infection-free ulcers unresponsive to standard wound care for 4 weeks or longer, with adequate circulation to the affected extremity [16]. Complete wound closure was achieved by 97% of EpiFix patients by week 12, compared to 73% of subjects treated with Apligraf, and 51% of subjects receiving SOC alone [16]. Additionally, patients in the EpiFix group used 94.4% less graft material and an average of 58% fewer grafts than Apligraf patients, resulting in an 83% lower median cost of graft material for the EpiFix group compared to the Apligraf group [16]. In 2015, Kirsner conducted the largest comparative effectiveness study examining outcomes of bioengineered living cellular construct (BLCC) and a dehydrated human amnion/chorion membrane allograft (dHACM) for the treatment of DFU’s [17]. Using a wound care specific electronic medical record database, real world outcomes were assessed in 218 patients with 226 DFU receiving treatment in 2014 at 99 wound care centers. They found DFUs treated with BLCC had higher rates of healing in less time compared to those treated with dHACM, increasing the probability of healing by 97% when compared with dHACM (p=0.01) [17].
There are many studies showing efficacy of advanced
products and therapies however these types of studies are often difficult to compare relative to methodologies and run-in periods; many are underpowered. Cost analysis remains either absent or inconsistent. Although head-to-head comparisons should be an essential part of the decision-making process they are rarely undertaken. Identifying the costs associated with treating wounds is rarely simple, as wounds can be related to secondary diagnosis and in vastly different methodologies, end points and the number of subjects. However, as reimbursement moves from a single payer to a value-based model clinicians and payers must have the opportunity to determine whether the higher upfront costs of these therapies are associated with decreased overall cost to the health care system (Figure 2).
Results: Economic Analysis
Overview
The following economic analysis compares the cost and efficacy of five skin substitutes.
i. ActiGraft® (RedDress, Pardes Hanna, Israel)
ii. Apligraf® (Organogenesis, Canton, MA)
iii. Dermagraft® (Organogenesis, Canton, MA)
iv. Grafix Core® (Smith & Nephew, Andover, MA)
v. EpiFix® (MiMedx, Marietta, GA)
The analysis is comprised of a series of cost comparisons to treat one diabetic foot ulcer (DFU).
a. 12-Week Product Cost
b. 4-Week Product Cost
c. Weighted Average Treatment Cost for Healed and Unhealed Populations
d. Medicare Reimbursement Cost – Hospital Outpatient and Physician Office Settings
e. Standardized Effectiveness Analysis
f. Scatter Plot – 12-Week Product Cost versus Complete Healing Efficacy
g. Scatter Plot – Cost per Square Centimeter versus Complete Healing Efficacy
Methodology
For each product, three data points are central to the analysis:
a) Number of applications over a 12-week course of treatment.
b) Complete healing efficacy over a 12-week course of treatment.
c) Product cost per application.
The number of applications and complete healing efficacy were obtained from the following published clinical studies. Where two studies are listed, data points were derived using a weighted average of the two data points (Table 1). For ActiGraft, study selection was limited to a pilot study. The study selection for Apligraf, Dermagraft, Grafix and EpiFix used inclusion/exclusion criteria defined by Samsell [5] including these key characteristics [5].
i. Either a randomized controlled trial, prospective cohort, or retrospective cohort design that included at least two study arms.
ii. Reported wound healing at 12 or 16 weeks.
iii. Reported number of applications of product used to achieve healing.
iv. Minimum 40 subjects in the primary treatment arm.
The ActiGraft data sourced from a pilot study presents limitations for comparison with studies meeting Samsell’s criteria. It is the authors’ intention to update this analysis when a future study that meets these benchmarks. Product cost for Apligraf, Dermagraft, Grafix and EpiFix were obtained from the July 2020 CMS ASP Pricing File for Payment Allowance Limits for Medicare Part B Drugs. Product cost for ActiGraft was obtained from RedDress and increased 6% to be comparable with the other product cost data, since CMS reimburses separately-payable drugs and biologics in the physician office setting at ASP plus 6%, where ASP is available, and at Wholesale Acquisition Cost (WAC) plus 6% where ASP is not available.
Other data points required for the analysis are:
i. Skin substitute assignments to High-Cost and Low- Cost groups were sourced from CMS January 2020 Update of the Hospital Outpatient Prospective Payment System (OPPS).
ii. Bundled Hospital Outpatient payments were sourced from CMS July 2020 Addendum B – Final OPPS Payment by HCPCS Code for CY 2020.
iii. Physician Facility and Physician Office fees were sourced from 2020 CMS Physician Fee Schedule.
iv. A standard wound size of 5 square centimeters was used to determine the smallest available product size that would cover the wound.
For Dermagraft and Grafix, the number of product applications was not explicitly stated in the source studies. For Dermagraft, we used 7.1 applications, consistent with the Samsell study. For Grafix we used 6.0 based on the 42-day median time to heal (Table 2). The cost to treat an unhealed DFU of $14,297 is an average based on a study citing incremental annual healthcare costs for DFU patients versus non-DFU patients ranging from $11,710 for Medicare to $16,883 for private insurance cost [18].
Results
12-Week Product Cost
As shown in Table 3 and Chart 1, the 12-week product cost ranges from $2,120 to $7,647. ActiGraft has a product cost advantage ranging from $1,245 to $5,527 over 12 weeks. The cost premium for other skin substitutes ranges from 59 to 261%.
4-Week Product Cost
4-week product cost is analyzed because studies have shown the 4-week percent area reduction of a wound is a significant predictor of week-12 complete healing [19]. As shown in Table 4 and Chart 2, the 4-week product cost ranges from $1,060 to $4,840. ActiGraft has a product cost advantage ranging from $1,710 to $3,780 over 4 weeks. The cost premium for other skin substitutes ranges from 161 to 357%.
Weighted Average Treatment Cost for Healed and Unhealed Populations
This weighted average cost is analyzed to account for both healed and unhealed patient populations, with $14,297 assigned to the incremental annual cost to treat a DFU patient versus a non DFU patient. This calculation is understated in that the cost to treat the healed population is a product cost only, excluding other treatment costs such as physician and staff labor. As shown in Table 5 and Chart 3, the WAVG treatment cost ranged from $5,505 to $11,783. ActiGraft has a cost advantage ranging from $2,504 to $6,278. The cost premium for other skin substitutes ranges from 45 to 114%.
Medicare Reimbursement Cost – Hospital Outpatient and Physician Office Settings
Medicare reimbursement cost is analyzed to estimate the relative cost of different products to the Medicare system. As shown in Table 6 and Chart 4, the Medicare Reimbursement Cost ranges from $4,065 to $10,343 in the hospital outpatient setting, and from $2,275 to $7,802 in the physician office setting. ActiGraft has a cost advantage ranging from $81 to $6,279 in the hospital outpatient setting and from $1,245 to $5,527 in the physician office setting. The cost premium for other skin substitutes ranges from 2 to 154% in the hospital outpatient setting and from 55 to 243% in the physician office setting.
Standardized Effectiveness Analysis
The Standardized Effectiveness Analysis (SEA) is another metric to assess the relationship between product efficacy and cost. It calculates the number of DFUs healed out of 100 patients per $1,000 of Medicare Reimbursement Cost. As shown in Table 7 and Chart 5, SEA ranges from 4 to 18 patients per 100 healed in the Hospital Outpatient Setting, and 5 to 32 patients per 100 healed in the Physician Office setting. ActiGraft has the greatest SEA in both settings.
Scatter Plot – 12-Week Product Cost versus Complete Healing Efficacy
Chart 6 illustrates the relationship between 12-week product cost and complete healing efficacy. ActiGraft offers the lowest cost while delivering the highest healing efficacy Chart 6.
Scatter Plot – Cost per Square Centimeter versus Complete Healing Efficacy
Chart 7 illustrates the relationship between Cost per cm2 and complete healing efficacy. ActiGraft offers the lowest cost per cm2 while delivering the highest healing efficacy Chart 7.
Other Considerations
Storage
The following table summarizes storage considerations for each product. ActiGraft and Epifix may be stored at room temperature, while Apligraf, Dermagraft and Grafix have special climate requirements (Table 8).
Inventory
The following table summarizes product size availability. ActiGraft, Apligraf and Dermagraft are available in one size, simplifying inventory management. EpiFix and Grafix are available in multiple sizes, which is advantageous for minimizing product wastage, but requires maintaining a relatively larger product inventory at the point-of-care (Table 9).
Wastage
ActiGraft is autologous, prepared from the patient’s own whole blood at the point of care. As a result, there is no biologic material wastage. Other skin substitutes generate wastage or must be maintained in inventory in a variety of sizes so that biologic material is used economically. For example, Apligraf is available solely in a 44.2 cm2 disc, which would result in 39.2 cm2 wastage for a wound lesser than 5 cm2; while EpiFix must be carried in inventory in a variety of sizes (5 sheet/membrane sizes and 3 particulate sizes in order to minimize wastage at the point of care [20-30].
Conclusion
This head-to-head comparison showed that ActiGraft was more cost efficient as an advanced therapy for DFU’s when compared to the 4 other advanced products investigated. A 12- week product cost of the CPT’s analyzed ranged from $2,120 to $7,647. ActiGraft had a product cost advantage ranging from $1,245 to $5,527 over 12 weeks. The cost premium for other skin substitutes ranged from 59 to 261%. The 4-week product cost ranged from $1,060 to $4,840. ActiGraft had a product cost advantage ranging from $1,710 to $3,780 over 4 weeks. The cost premium for other skin substitutes ranged from 161 to 357%. The weighted average treatment cost (WAVG) ranged from $5,505 to $11,783. ActiGraft had a cost advantage ranging from $2,504 to $6,278. The cost premium for other skin substitutes ranged from 45 to 114%. ActiGraft had a cost advantage ranging from $81 to $5,760 in the hospital outpatient setting and from $1,245 to $4,959 in the physician office setting. The cost premium for other skin substitutes ranged from 2 to 142% in the hospital outpatient setting and from 55 to 218% in the physician office setting. Standardized Effective Analysis (SEA) ranged from 4 to 18 patients per 100 healed in the hospital outpatient setting, and 5 to 32 patients per 100 healed in the physician office setting. ActiGraft had the greatest SEA in both settings. ActiGraft offered the lowest cost per cm2 while delivering the highest healing efficacy. Unlike other CTP’s in this analysis, ActiGraft is autologous, prepared from the patient’s own whole blood at the point of care and therefore has no biologic material wastage. It should be noted that the ActiGraft data sourced from a pilot study presents limitations for comparison with studies meeting Samsell’s criteria. It is the authors’ intention to update this analysis when additional published studies meet this benchmark [31-40].
To know more about Juniper Publishers please click on: https://juniperpublishers.com/aboutus.php
For more articles in Open Access Journal of Reviews & Research please click on: https://juniperpublishers.com/arr/index.php
To know more about Open Access Journals please click on: https://juniperpublishers.com/journals.php
#Juniper Publishers Contact address#Juniper Publishers#Juniper Publishers Indexing#Juniper Publishers group#Juniper Publishers Review#reviews research paper
0 notes
Text
A Review of Recent Status on Stingrays (Chondrichthyes: Dasyatidae) In Indonesian Waters- Juniper Publishers
Abstract
In this paper, the status of stingrays (family Dasyatidae) in Indonesian waters are summarized. There are 40 valid species of stingrays recorded here. Based on distribution of stingrays within seven faunal region of Indonesia, Kalimantan of Indonesian Borneo has 29 species, the largest diversity among other islands; following Sumatra (27 sepecies), Java (25 species), Sulawesi (14 species), Lesser Sundas (16), Mollucas (9 species) and Papua (17 species). According to the recent of Red List of Threatened Species of the International Union for the Conservation of Nature's (IUCN 2017), there are 18 species are listed as threatened species (under Endangered and Vulnerable status), 2 as Near Threatened (NT), 3 as Data Deficient (DD), 5 s as Least Concern (LC) and 12 species are Not Evaluated (NE). Five species listed as Endangered should have high prioritize for conservation: Fluvitrygon oxyrhynchus (Sauvage, 1878); F. kittipongi(Vidthayanon & Roberts, 2005); F. signifer (Compagno & Roberts, 1982); P. solocirostris Last, Manjaji & Yearsley, 2005; and Urogymnus polylepis(Bleeker, 1852).
Keywords: Review; Dasyatidae; Indonesian waters; Diversity; Conservation
Introduction
The Indonesian archipelago is one of the richest marine biodiversity areas in the world [1]. The country has 4.720 species of fishes, making one the greatest diversity of fish fauna in the world [2]. Many iconic group of fishes known collectively as the 'ray' occur in Southeast Asia, particuarly in Indonesian waters [3-5]. One of 'ray' is stingrays (family Dasyatidae), groups of small to very large myliobatiform fishes (adults from 22cm to 260cm DW) and distinguished by the following combination of characters: body variably depressed with a well-formed oval, circular or rhombic disc that fully incorporates head; snout angular to obtuse and sometimes very elongate; nasal curtain well developed, skirt-shaped, rectangular or bilobed; five gill slits; oral papillae usually present on floor of mouth; tail moderately stout to slender-based and more or less elongated (sometimes very elongate and whip-like); dorsal surface variably covered with dermal denticles, thorns and/or tubercles, smooth to very spiny and often with a median thorn row and/or a median denticle band; no dorsal or caudal fins; 1-4 prominent caudal stings, positioned on tail well posterior to pelvic fins; skin folds variably developed on the ventral and sometimes dorsal midline of tail; dorsal surface plain to strongly patterned, usually darker than ventral surface [6-9]. Recent phylogenetic studies, supported by morphological data, have provided evidence that the Dasyatidae is monophyletic and consists of four major subgroups, the subfamilies Dasyatinae, Neotrygoninae, Urogymninae and Hypolophinae; and a morphologically based review of 89 currently recognised species [6]. In this review, we summary and update current knowledge of the stingrays in Indonesian waters.
Diversity of Stingrays in Indonesian waters
Table 1 shows 40 valid species of stingrays that occur in Indonesian waters. This checklist is compiled and shortlisted from recent major references [6-8]. The fishes were divided within seven faunal regions of Indonesia, where faunal regions match administrative boundaries and has no political significance [10]. Conservation status covering global threatened species follows recent International Union for Conservation of Nature (IUCN) Redlist 2017 [11].
Two species have been added recently for Sumatran waters [12,13], Fluvitrygon oxyrhynchus and Urogymnus polylepis (Figure 1 & 2). Based on distribution of stingrays within seven faunal region of Indonesia, Kalimantan of Indonesian Borneo has nine species of stingrays found in Mollucas, indicate the lowest 29 species, the largest diversity among other islands; following Sumatra (27 sepecies) and Java (25 species). There are only number compare to other islands in Indonesian waters.
Conservation of Stingrays in Indonesian waters
The status of most of the world's rays have been assesed using a standard international system to characterise the risk of extinction of species: the International Union for the Conservation of Nature's (IUCN) Red List of Threatened Species [14]. Following recent IUCN (2017), there are 18 species are listed as threatened species (under Endangered and Vulnerable status), 2 species listed as Near Threatened, 3 species listed as Data Deficient, 5 species listed as Least Concern and 12 species as Not Evaluated (Table 1). Five species having high prioritize for conservation because listed as Endangered: Fluvitrygon oxyrhynchus; F. kittipongi (Vidthayanon & Roberts, 2005); F. signifer (Compagno & Roberts, 1982); P solocirostris Last, Manjaji & Yearsley, 2005; and Urogymnus polylepis. Four of these species are inhabit freshwaters. To secure the status of stingrays locally and globally, in addition to the adressing the issue of data deficiency, accurate species identification is needed, the strict enforcement of fishing and protection of measures, a significant increase in scientific observer coverage to monitor catches, and increase research on gear modifications, fishing methods, and habitat identification aimed at itigating bycatch and discard mortality of rays [14].
Note:
I. IUCN global status, CR = Critically Endangered, EN = Endangered, VU = Vulnerable , NT = Near Threatened, DD = Data Deficient, LC = Least Concern, NE = Not Evaluated.
II. Distribution abbreviations, S = Sumatara, K = Kalimantan (Indonesian Borneo), J = Java, S = Sulawesi, M = Mollucas, L = Lesser Sunda, P = Papua (West Papua, Indonesian Papua).
Conclusion
Recent status of stingrays (family Dasyatidae) in Indonesian waters are summarized here. This general review may give obvious diversity and conservation challenges. We supose that further research and monitoring are needed to clarify local status and distribution of stingrays in Indonesian waters, particularly in area where rarely explored.
For more about Juniper Publishers please click on: https://twitter.com/Juniper_publish
For more about Oceanography & Fisheries please click on: https://juniperpublishers.com/ofoaj/index.php
#Fish production#fisheries research#Aquatic Organisms#Juniper publishers Address#Juniper publishers contact info
0 notes
Text
Juniper Publishers Contact Number

Juniper Publishers Contact Number
Phone: +1-805-200-4030
https://g.page/Juniper_Publishers?share
#Juniper Publishers Address#Juniper Publishers Contact Info#Juniper Publishers Contact Number#More about Juniper Publishers
0 notes
Text
Juniper Publishers Address

Juniper Publishers Address 427 W Duarte Rd, Suite E, Arcadia, California, CA 91007 United States
https://juniperpublishers.com/contact-us.php
0 notes
Text
Juniper Publishers- Open Access Journal of Case Studies
What’s the Connection between Diabetes and Depression?
Authored by Berna Nilgün Özgürsoy Uran
Abstract
Depression is a serious medical condition that affects thoughts, feelings, and the ability to function in everyday life.
An internationalreport has shownthathavingdiabetesanddepression has thegreatestnegativeeffect on quality of life comparedtodiabetesordepressionalone, orotherchronicconditions. Because of tahatreasonIt is very important for health professionals to control these diseases to understand the relation of diabetes to depression. The purpose of this review is to draw attention to the relationship between depression and diabetes and to provide literature support to health professionals.
Keywords: Diabetes; Depression; Treatment
Introduction
The increasing burden of diabetes among adults (aged 20–70 years) is a major public health concern globally [1]. The number of people living with diabetes is estimated to rise from 135 million in 1995 to 300 million by 2025. Diabetes is a disorder that impairs the way the body uses digested food for growth and energy. Most of the food we eat is broken down into glucose, a form of sugar that provides the main source of fuel for the body. After digestion, glucose passes into the bloodstream. Insulin, a hormone produced by the pancreas, helps glucose get into cells and converts glucose to energy. Without insulin, glucose builds up in the blood, and the body loses its main source of fuel [1].
Type 1 diabetes is when the immune system destroys the insulin-producing beta cells of the pancreas. This form of diabetes usually strikes children and young adults, who require daily or more frequent insulin injections or using an insulin pump for the rest of their lives. Insulin treatment, however, is not a cure, nor can it reliably prevent the long-term complications of the disease. Although scientists do not know what causes the immune system to attack the cells, they believe that both genetic factors and environmental factors are involved [1].
Type 2 diabetes, which accounts for about 90 percent of diabetes cases in the United States, is most common in adults over age 40. Affecting about 6 percent of the U.S. population, this form of diabetes is strongly linked with obesity (more than 80 percent of people with type 2 diabetes are overweight), inactivity, and a family history of diabetes. It is more common in African Americans, Hispanic Americans, American Indians, and Asian and Pacific Islander Americans. With the aging of Americans and the alarming increase in obesity in all ages and ethnic groups, the incidence of type 2 diabetes has also been rising nationwide [1].Theprevalence of majordepression in the UK population at anyone time is about 5%, although as many as oneperson in threemayexperience an episodeof depression in theirlifetime [2].
There search ersused cognitive therapy to reverse the depression.In those people where depression improved, there was an average HbA1c of 8.3% while those who showed little improvement had an average of 11.3%. While these results show an association between highblood sugars and depression, it remains unclear whether highblood sugars cause the depression or depression causes highblood sugars [2].
Another relatively common and costly central nervous system syndrome, depression, occurs in many patients with diabetes [1]. Depression is a serious medical condition that affects thoughts, feelings, and the ability to function in everyday life. Depression results from abnormal functioning of the brain. The causes of depression are currently a matter of intenseresearch. An interaction between genetic predisposition and life history appear to determine a person’s level of risk. Episodes of depression may then be triggered by stress, difficult life events, side effects of medications, or other environmental factors. Whatever its origins, depression can limit the energy needed to keep focused on treatment for other disorders, such as diabetes [1].
A more recent systematic review and meta-analysis of multiple community-based, large-scale, prospective studies confirmed the significantly increased rates of depression in people with type 2 diabetes relative to control subjects (17.6%vs9.8%, OR=1.6 [95% confidence interval (CI) of 1.2- 2.0]) [3]. Despite the differences between type 1 and type 2 diabetes in age of onset and clinical course, the prevalence rates for type 1 vs type 2 diabetes were statistically similar in the studies that determined depression by diagnostic interview (13.6% vs10.9%, p>0.1) or with self-reportsymptoms scales (29.1%vs32.9%, p>0.1) [4].
Cardiovascular disease is a macro vascular complication of diabetes. An analysis of a large, naturalistic population-based sample of patients with type 2 diabetes in a Large primary care system concluded that patients with major depression and diabetes were 1.5-2-fold more likely to have 3 or more cardiovascular risk factors than patients with diabetes without depression [5].
How Does Depression Affect People with Diabetes?
An international report has shown that having diabetes and depression has the greatest negative effect on quality of life compared to diabetes or depression alone, or other chronic conditions (Table 1).
Though the relationship between diabetes and depression isn’t fully understood
The rigors of managing diabetes can be stressful and lead to symptoms of depression.
Diabetes can cause complications and health problems that may worsen symptoms of depression.
Depression can lead to poor lifestyle decisions, such as unhealthy eating, less exercise, smoking and weight gain - all of which are risk factors for diabetes.
Depression affects your ability to perform tasks, communicate and think clearly.
This can interfere with your ability to successfully manage diabetes.
Recent estimates suggest that upto three quarters of cases of depression in people with diabetes may go undiagnosed. During the subsequent decade of 2000-2010,increased Attention focused upon adverse metabolic and thrombo vascularc onsequences of depression through certain biologic path ways.
Relevant in this regard are the hypothalamic-pituitaryadrenal axis hyperactivity and mental stress-induced sympatho medullary activation in many patients with major depression, which can contribute to decreased glucose transport and insulinresistance, respectively.A mechanistic path way between depression, diabetes,and coronary artery disease has been proposed by Steven Roose [7].
Depression causes patients to become inactive, which, combined within creased cortisol levels, causes adiposity, obesity, and insulin resistance. Adipose tissue and damaged vessels then release pro-inflammatory cytokines, which induce the depressive symptoms of the ‘‘sicknessbehavior’’syndrome, which impair a patient’s motivation to initiate healthy self-care behaviors and perturb cognition. Consequently,ever-worsening cycles evolve eventually resulting in a heartattack or stroke associated with type 2 diabete [7].
Treatment Depression and Diabetes
There are multiple conceptual approaches to the diagnosis of major depression in medically ill patients, including the exclusive and inclusive approaches [8]. The exclusive approach maximizes specificity bye liminating so maticsymptoms such as anorexia and fatigue, which frequently are elements of medical disorders [8]. The inclusive approach includes all depressive symptoms to diagnose major depressive disorder in the medically ill and maximizes sensitivity, best protecting the patient from a ‘‘falsenegative result’’ and the risk of undiagnosed depression [8].
Non-depressed diabetic patients may report neurobehaviora symptoms such as diminished appetite, weightloss, hypersomnia, loss of libido and psycho motor retardation [9]. Therefore, the use of exclusive criteria may allow clinicians to more easily identify major depression in diabetic patients [9].
Treatment for depression in people with diabetes has been shown to be effective and has the additional benefits of improving blood sugar control. The evidence suggests that cognitive behaviour therapy and anti-depressant medicines are as effective in people with diabetes as in those with out diabetes. As thetreatment of depression can improve blood sugar control, it is also likely to reduce the risk of complications but importantly, it can also improve quality of life and diabetes self management programs, psychotherapy, medications and lifestyle changes, collaborative care is very important to treatment depression and diabetes (Table 2).
Physicians always need to be cognizant of drug-drug interactions when prescribing medications, particularly in patientswith psychiatric and medical co-morbidities. Due to the inhibition of cytochrome P450 (CYP) 3A4 isoenzyme,certain of these rotoninre uptake inhibitors (SSRIs) such as fluoxetine and fluvoxamine mayalter the metabolism of certain oral hypoglycemics (such as the thiazolidinedione pioglitazone, the meglitinies, repaglinide and nateglinide) and confer a risk of hypoglycemia [9].
In addition, inhibition of the CYP 2C9 isoenzyme by fluoxetine, fluvoxamine, or sertraline may also potentially alter CYP 2C9 metabolism of sulfonylureas tolbutamide and glimepiride [9]. Diabetes nurses can say diabetes self management progrmas is very important to treating depression and diabetes [1].
Conclusion
There is clearly an increased prevalence of depression among diabetic patients [1]. Depressive symptoms serve as a risk factor for the development of diabetes and have been shown to contribute to hyperglycemia, diabetic complications, functional disability and all cause mortality among diabetic patients. Despite the fact that depression complicates medical conditions such as diabetes, there is evidence that diabetes nurse and primary care physicians treat depression less aggressively in patients with medical comorbidities [11].
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Case Studies please click on: https://juniperpublishers.com/jojcs/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/jojcs/JOJCS.MS.ID.555597.php
#Juniper Publishers Contact#Juniper Publishers Address#Obstetrics and Gynaecology#Transplant Surgery#Vascular surgery#Surgical Oncology#Otolaryngology
0 notes
Text
Postmenopausal Osteoporosis | JuJuniper Puniper Publishers
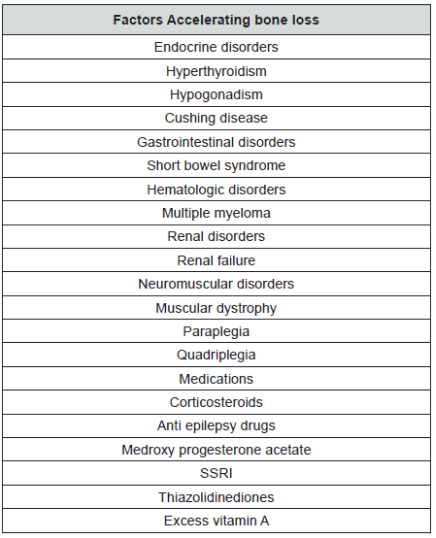
Juniper Publishers-Open Access Journal of Case Studies
Authored by Vikram Khanna
Abstract
Osteoporosis is a condition with a very high prevalence and its spreading at a rapid pace which is in tandem with the increase in the life expectancy of the general population. With the change in the eating habits the patients are not getting adequate nutrition for the wellbeing of the bones. With the advancements in the field of bone mineral density measurement it may now be possible for early detection and rapid treatment which may lead to the better outcome for the patient and may prove less detrimental for the society as well.
Keywords: Osteoporosis; Menopause; BMD
Introduction
Osteoporosis is a silent condition which has been on the rise in the recent times due to the increase in the life expectancy of the patients [1]. This affects the physical, mental as well as socioeconomic condition of the patient. This review article summarizes the important aspects of this condition as well as sheds light on its treatment.
Definition
The working group of WHO in 1994 came up with the definition which was based on T score of the Bone mineral density (BMD) and it said that a T score less than -2.5 can be considered as osteoporosis [2].
Background
The number of patients with osteoporosis is on a rise and it is expected that the no. will soon reach 34 million in USA [3]. Out of which 80% are expected to be women. The incidence of osteoporosis increases exponentially with age and there is a sharp increase in cases following menopause in females. The incidence of osteoporosis is also associated with an increase in the incidence of fractures which also rises following the decrease in the bone mineral density [4].
Pathophysiology of Postmenopausal Osteoporosis
There may be 2 causes of postmenopausal osteoporosis
Low peak bone mass
Increased bone loss, or both Peak bone mass is determined 70%-80% by genetic factors [5-8]. Remaining causative factors for the peak bone mass include factors like nutrition, activity and hormonal interplay.
Once the peak bone mass is achieved, bone regulation takes place by local remodeling which is regulated by RANK, RANKL protein and OPG. RANK or receptor activator of nuclear factor-kb is present in the osteoclasts and causes the increase in their activity. RANKL or the RANK Ligand is synthetized by osteoblasts and it binds with the RANK receptor on the osteoclasts. OPG or Osteoprotegerin is also synthetized by the osteoblasts and prevents the binding of the RANK to the RANK Ligand by itself binding to the RANKL. Hence, the activity of the osteoclasts and in turn the bone remodeling depends upon the interplay between the RANK and the OPG. This interplay is controlled by hormonal and local factors. If the bone remodeling is in balance (osteoblast = osteoclasts) then there is no decrease in the BMD. A change in the balance of remodeling causes the change in the BMD accordingly.
In postmenopausal females, there are hormonal changes which cause an increase in the RANKL which causes increase in the osteoclastic activity and hence, shifts the bone remodeling towards a bone resorbing balance which leads to osteoporosis.
It has been noted that the bone loss is maximum 3-5 years before menopause and also 3-5 years after menopause. These points towards the indirect as well as the direct causes of bone loss leading to osteoporosis. This bone loss is faster than the average bone loss seen in the senile osteoporosis seen in males. There is also research going on which suggests the change in the micro architecture of bone with the advent of osteoporosis. However, this research and the quantification of these changes are still in experimental stages and not available for commercial use [9]. Factors which accelerate bone loss are included in Table 1. Also, factors which increase the risk of falling and fractures are included in Table 2.
Clinical Features of Postmenopausal Osteoporosis
These include:
Low Bone mass: measured by BMD
Fracture: Single most important manifestation of postmenopausal osteoporosis.
Lifestyle and Non pharmacologic Measures for Bone Health
Goals of this therapy include:
Optimizing skeletal development to increase the peak bone mass
Prevent secondary bone loss
Preserve the skeletal structural integrity
Prevent fractures
Following diets should be taken into consideration:
Good general Nutrition: A balanced diet is necessary for the development of a good peak bone mass. The peak bone mass also depends upon the protein intake as well as the activity level of the patient [10-12].
Calcium: The recommended dose of daily requirement of calcium in various situations is given in Table 3. Some points to be taken into consideration are that calcium is absorbed better with food and calcium citrate gives the least amount of GI side effects as compared to other calcium compounds.
Vitamin D: It is important to assess serum Vitamin D in all individuals suffering from osteoporosis. Vitamin D is found in food stuff like fish oils, fortified milk, cereals and breads. National Osteoporosis foundation recommends a dose of 800-1000 IU for patients more than 50 years old [13]. However, many experts feel that the dose should be between 1000-2000 IU (Safe upper limit being 4000IU/day) [14]. Currently the normal level is 30-32ng/ml (Upper limit being 60ng/ml) [15]. Even though daily doses are present still it has been seen that the intermittent dose was found to be 3 times more potent [16].
Other dietary supplements: Magnesium doesn’t increase the calcium absorption but decrease the GI side effects [17]. Excessive Vitamin A was harmful for the bones in large doses (more than 100000 IU) [18]. Vitamin K (1mg/ day) has been found to decrease the bone turnover and hence decrease the bone loss [19]. Natural estrogens (isoflavones) were thought to prevent bone loss but there has not been any scientific evidence for the same [20-22].
Alcohol: Excessive alcohol intake causes bone loss [23]. Postmenopausal women should take a maximum of 7 drinks a week.
Caffeine: Postmenopausal osteoporotic women should limit their caffeine intake less than 1-2 servings/day as it decreases the intestinal absorption of calcium [24].
Smoking: It is associated with osteoporotic fractures. Patients who give up smoking are at a lesser risk than those who are active smokers [25].
Exercise: Regular light exercises (30-40 mins) everyday increases the muscle strength and it has been seen that it also causes the bone strength to increase [26,27]. However patients with severe osteoporosis should avoid heavy exercises like lifting weights or excessive pushing or pulling.
Prevention of risk factors for Post-menopausal osteoporosis
Spine Imaging: to rule out any fractures
BMD: measured either at the spine or the neck of femur. It can be used to assess the probability of fracture in the next 10 years in a patient using the FRAX tool. However, this modality is still expensive and the benefit to the society is still not confirmed. Lists of indications have been summarized in Table 4.
Treatment of Osteoporosis
Candidates requiring treatment for osteoporosis include [28]:
Drugs approved for postmenopausal osteoporosis have been listed along with their dosage in Table 5 and their possible effects on fracture risk reduction have been mentioned in Table 6. Concomitant use of anti-osteoporotic drugs was thought to reduce the fracture risk better than using a single drug [29]. However, further studies have led to the non-recommendation of this practice [30]. The sequential use of drugs, first the anabolic group followed by the anti resorptive drugs has been found to be beneficial for patients [31].
BMD in progression of the treatment
BMD may be used for the prognosis and the follow-up of the treatment of osteoporosis. The treatment is said to have failed if there is substantial fall in the BMD or any fracture occurrence.
Operative treatment for osteoporosis
Most commonly occurring fractures are the vertebral fractures and there has always been a difference of opinion regarding the management of the same. Vertebroplasty though decreases the pain instantly but doesn’t increase the vertebral height to normal whereas, Kyphoplasty increases the vertebral height along with the reduction in the pain but is expensive [32- 36]. The surgeon should be careful in the fixation of the other fractures by using locking plates and HA coated implants to provide a stable fixation.
Conclusion
The incidence of postmenopausal osteoporosis is on the rise and one should be careful in the management and suitable pharmacotherapy should be given which is tailor made for each and every patient.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Case Studies please click on:
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/jojcs/JOJCS.MS.ID.555570.php
#Juniper Publishers#Juniper Publishers Address#Juniper Publishers Contact Number#Case Reports#Surgery#Cancer#opthalmology#Cardiology
0 notes
Text
Juniper Publishers Contact Number
Juniper Publishers Contact Number Phone: +1-805-200-4030
https://g.page/Juniper_Publishers?share
#Juniper Publishers Address#juniper publishers contact info#Juniper Publishers Contact Number#More About Juniper Publishers
0 notes
Last Seen Blogs

thebananasaurusartblog
The_Bananasaurus_ArtBlog

noisycherryblossomtimetravel
Untitled

putipherio-blog
PUTIPHERIO

bbparker
America’s Ass
ev4nescente
ྀི