#Surgical case reports
Text
An Uncommon Localization of a Hydatid Cyst Presenting with Pulmonary Embolism
Abstract
Human echinococcosis is an important infection in undeveloped and developing countries, caused by larval forms of the genus Echinococcus. In western countries this disease is sporadic. The organs mostly involved by the cysts are the liver (70%) and the lungs (20%) [1]. Cardiac hydatid cyst is a rare condition, and the location of a hydatid cyst in the interventricular septum is exceptional. Cardiac echinococcosis is not frequent, only 0.01%-2% of all hydatid infestations [2]. The left ventricle is the heart chamber most frequently involved (55-60%) and the involvement of the interventricular septum is reported in 4% of cardiac cases. Chest pain, palpitations, and dyspnea are the most frequent symptoms associated with cardiac echinococcosis. We describe a case of an unusual presentation of this disease.
Read More about this Article: https://juniperpublishers.com/jojcs/JOJCS.MS.ID.555847.php
Read More Juniper Publishers Google Scholar: https://scholar.google.com/citations?view_op=view_citation&hl=en&user=rp_7-igAAAAJ&citation_for_view=rp_7-igAAAAJ:hqOjcs7Dif8C
#juniper publishers publons#Juniper Publishers Google Scholar#Surgical case reports#medicine neurosurgery#Ectopic scar pregnancy
0 notes
Text
Surgery Case Reports Journal publishes case reports in surgery, images in surgery, imaging in surgery journal, case reports in surgical journal, case series and videos in surgery journal etc. Surgery Case Reports Journal is a manual or mechanical intervention that involves cutting the patient’s tissues, or closure of an already existing injury or wound.
#surgical case reports journal#Surgery Case Reports Journal#Surgical Case Reports in Surgery Journal#case reports in surgery
0 notes
Text
Ghost is training you on interrogation techniques and thinks you’re a lost case. He’s wrong.
———————————————————————
He unfolds a case of what looks like surgical equipment on the wooden table.
“Are you going to check my teeth for cavities, Lt.?” You joke, but he doesn’t laugh. He never does.
He picks up something that looks like a wrench and shows it to you.
“What’s this for?” He asks, to which you reply, with the utmost confidence that it looks like that tool your grandfather used when you were a kid to break the bathroom door because you locked yourself in there.
He shuts his eyes and holds his breath.
“See, I didn’t want to eat my vegetables, and-”
“Enough.”
“That’s what I told them; no more veg-”
“Stop with the focken veggies.”
“You don’t like them either, huh?”
He lets out a long exhale and pinches the bridge of his nose.
“I don’t think you’re fit for this.” He finally says.
But you are. There's a reason why you are here, and it’s because you’re damn good at your job. Sure, you never learned how to conduct an interrogation the way Ghost understands—in a physical and rather brutal manner—but, you had your ways.
“I beg to differ, Lt.” You oppose him.
“You can beg as much as you want, soldier,” he replies, “but you’ll never be able to make someone beg for mercy.”
You look at the interrogation tools on the table and point at them. “These are unethical, by the way.”
“These,” he says, “serve a purpose for the job and are perfectly legal.”
“So is farting in an elevator,” you reply. “Totally legal to do, yet sorta sucks for everybody else.”
“You should have gone to law school if you’re so passionate about ethical matters,” he says, “but you’re definitely not fit to be here.”
“The captain thinks otherwise.”
“The captain is wrong.” He mumbles under his breath.
“What’s that?” You ask, cupping your palm over your ear, “Are you defying the captain now, Lieutenant Riley?”
“No, I’m jus-”
“That’s against the Army Leadership Code,” you state and shuffle through your bag to get the rulebook. You open it up and clear your throat. He looks at you with that tool in his hand, eager to start plucking your fingernails one by one. Instead, he chooses words.
“I know what the guide says-”
“PAGE 45, PARAGRAPH SIX,” you shout like you’re reporting for duty, “IF AN OFFICER DISOBEYS THE-”
“Stop this instance!” He cries, but you hear none of it. You carry on undisturbed by his roaring voice. You’ll recite the entire book if that’s what’s needed. He leaves the tool on the table and approaches you, posing as an authority figure and yelling in your face. You stop for a minute and turn to look at him, explaining that what he’s doing right now is also against the code, and continue reading out loud.
“FAILURE TO OBEY A MILITARY ORDER BY A HIGHER UP-”
He throws his head up, closes his eyes, and raises his hands up to his temples.
“For the love of god and all that is holy, soldier,” he cries, “please stop talking.”
You close the booklet and throw it on the table. There’s dead silence. You approach him with a smug face and lower your gaze—but not your head—to the ground.
“Well, guess what, Lt.” You ask, and he opens his eyes to look at you.
“You just begged,” you whisper, “and I didn’t have to use any of your,” you gesture with a sneer at the tools on the table, “cheap cutlery.”
He keeps looking at you, confused. You pick a scalpel from the case.
“I thought you didn’t like my tools, soldier.” He says.
“I don’t,” you reply and pull an apple out of your bag, “but I need to cut my fruit.”
He throws his hands to his sides and looks at you, defeated, as you peel the apple.
You stop midway.
“Is the scalpel sterilised?” You ask.
“Of course, it’s sterilised!” he shouts, “we always sterilise our tools as per the rulebook!”
———————————————————————
#simon ghost riley x gn!reader#simon ghost riley x reader#simon ghost riley x y/n#simon ghost riley x you#simon ghost riley#simon riley x reader#simon riley x y/n#simon riley x you#simon riley#ghost call of duty#call of duty#modern warfare 2#ghost cod#cod ghost#cod mwii#ghost cod mwii#cod mw ghost#ghost cod mw2#cod mw2#simon ghost riley fic#simon ghost riley fanfiction
6K notes
·
View notes
Text
Let me share you some examples of people outside of a spiritual realm using the law of consciousness. Reading about placebo opened my eyes to realize whether I believe it or not, use it or not, it is always operating.
1. During wartime, particularly in World War II, when medical supplies were limited, the use of a saline solution as a placebo became prevalent. One notable figure associated with this practice is Henry Beecher, a medic during the war. When morphine, a powerful painkiller, was scarce, Beecher resorted to injecting injured soldiers with a saline solution (a mixture of salt and water) as a substitute.The fascinating observation was that many soldiers responded positively to the saline placebo, reporting a reduction in pain. Beecher’s experience led him to further investigate what is now known as the placebo effect. He discovered that even inert substances like saline could elicit a therapeutic response in individuals, highlighting the power of belief and the mind’s influence on healing. Using saline as a placebo during wartime was a practical solution to address the scarcity of medical resources. It allowed healthcare providers to provide some form of treatment while conserving limited supplies for critical cases. The phenomenon observed in these wartime placebo administrations contributed to our understanding of the placebo effect and its role in medical practices.
2. And then there was another placebo test done with surgeries demonstrated the power of the placebo effect in the context of surgical interventions for knee pain.
The study, often referred to as the “fake leg surgery” study, focused on patients with osteoarthritis in the knee. Participants were randomly assigned to either receive real arthroscopic surgery or undergo a sham procedure where no actual surgical intervention took place. The sham surgery involved making small incisions and mimicking the actions and sounds associated with the actual procedure.The surprising finding was that both groups, those who underwent real surgery and those who had the sham surgery, reported similar improvements in their knee pain and functionality. This suggested that the positive outcomes experienced by the participants were not necessarily due to the physical intervention but rather to psychological factors such as the placebo effect.
3. The most fascinating one was this one: The study aimed to explore the role of mindset in reversing some aspects of aging.
In this experiment, Langer and her team created a simulated environment reminiscent of the 1950s to immerse a group of elderly participants. The participants were instructed to act as though they were 20 years younger and encouraged to engage in activities that required physical and mental activity. It aimed to create an atmosphere where the participants felt as if they were stepping back in time.The results of the experiment were described as astonishing. Participants reportedly experienced improvements in various areas, including physical health, cognition, and overall well-being. The study suggested that by changing one’s mindset and engaging in an environment that challenges typical aging stereotypes, individuals may experience positive effects on various aspects of their lives.
4. The Man Who Overdosed on Placebo" is a story about a 26-year-old man, often referred to as "Mr. A," who was part of a clinical trial for an antidepressant drug. In a desperate state of mind, he attempted suicide by ingesting 29 capsules of what he believed to be the experimental drug. This act was triggered by his depression, which had worsened after a breakup with his girlfriend.
However, unbeknownst to him, the pills he had taken were not the actual antidepressant, but rather placebos - essentially inert substances, often sugar pills, used in clinical trials as a control group. Despite this, Mr. A's vitals showed alarming signs similar to those of a drug overdose, reflecting the power of belief over the physical body, a phenomenon known as the "nocebo effect."
The nocebo effect is essentially the evil twin of the placebo effect. While the placebo effect can lead to improvements in health due to positive expectations, the nocebo effect can cause negative symptoms or even exacerbate existing ones due to negative expectations. In this case, Mr. A exhibited symptoms of an overdose solely because he believed he had taken an overdose.
5. Sam Londe, is one of the best but sad classic example of the nocebo effect, as detailed in Dr. Joe Dispenza's book "You Are the Placebo."
Sam Londe was diagnosed with esophageal cancer, a condition known for its grim prognosis. His doctors informed him that he didn't have much time left to live. Accepting this diagnosis, Londe quickly became bedridden and his health deteriorated rapidly, following the trajectory his doctors had predicted.However, upon his death, an autopsy revealed a surprising fact: there was not enough cancer in his body to have caused his death. The small tumor in his esophagus was not large enough or in a position to interfere with his swallowing or breathing. Essentially, Londe didn't die from cancer; he died from believing he was dying of cancer.
This case demonstrates the power of the mind over the body, both positively (the placebo effect) and negatively (the nocebo effect). In this case, Londe's negative beliefs about his prognosis led to physical symptoms and ultimately his death.
I've seen dozens of examples where of stuff like this particularly in the realms of hexing and witchcraft. Honestly, the same could probably be said about subliminals. But it doesn't matter much.Why? Because they work. It's all about observation and choice. You could say it’s the mind but the mind operates on logic. This goes beyond the mind and to your true being, what observes the mind observing the pain in the first place.
Actually I was talking to someone who had been struggling with shifting for a while about this and it really resonated with her which is why I decided to share it. She took a water bottle, labeled it shifting juice and just assumed that when she finishes the bottle she has “full access to shifting powers” is that how it works. Nope. Did she shift after two years of struggling. Yep. It doesn’t matter what story you create yourself whether you want to use logic or not whatever you assume and persist in and know as a fact will harden into truth and therefore reality.I just wanted to share this story bc I find it absolutely hilarious how we sometimes take it so seriously yet it can be so easy. I know placebo is just an assumption. It’s like when you tell children you checked under their bed for the monsters and drafted them and they assume so so they can sleep soundly at night. Call it whatever you want assumption, placebo, it’s all just words and each community calls it something different but at the end of the day it works wether you know the truth behind it or not.

586 notes
·
View notes
Text
What these freaks did to those kids is cruel and unusual.
Madagascar will surgically castrate paedophiles under new law approved by MPs it is revealed - days after Kazakhstan announced same plan
A minister spoke in favour of the law saying: 'society must know what they did'
By ED HOLT
PUBLISHED: 14:29 EST, 7 February 2024
Madagascar's parliament has approved a new law which will see paedophiles surgically castrated for their crimes.
The new law comes just days after Kazakhstan announced a similar law where the country's worst offending child sex offenders will have their genitals surgically removed.
On February 2 Madagascar's parliament, The National Assembly, approved a law which legalised the castration of child rapists.
The old law stated that those found guilty of raping a minor would face between five and 20 years of forced labour.
However, this new law states that those found guilty of raping a child under ten-years-old will be surgically castrated and sentenced to life imprisonment. While if the victim is between ten and 13-years-old, they will instead be chemically castrated and face 15 to 20 years of forced labour. If the rapist is also a minor they will escape castration.

Madagascar's Minister of Justice Landy Randriamanantenasoa spoke in favour of the bill. She said: 'Society must know what they did and who they are'

Ms Randriamanantenasoa has rebuked similar criticism about respect for human rights by saying Madagascar is a sovereign country. This comes after Amnesty criticised the bill
Minister of Justice Landy Randriamanantenasoa spoke in favour of the bill. Le Quotidien, a French language newspaper, reported that Ms Randriamanantenasoa said: 'Society must know what they did and who they are.'
The bill was proposed by the President of Madagascar, Andry Rajoelina, last month and was one of his key campaign promises during his re-election bid last year.
International organisations have criticised the new law. The BBC reports that in a statement, Tigere Chagutah, Amnesty's regional director for east and southern Africa, said: 'In Madagascar, rape cases remain under-reported, and perpetrators often go free due to the victims' and their families' fear of retaliation, stigmatisation, and a lack of trust in the judicial system.
'Implementing chemical and surgical castration, which constitutes cruel, inhuman and degrading treatment, as a punishment for those found guilty of raping minors will not solve this and is inconsistent with Malagasy constitutional provisions against torture and other ill-treatment, as well as regional and international human rights standards.'
Ms Randriamanantenasoa has rebuked similar criticism about respect for human rights by saying Madagascar is a sovereign country.

The tighten of the law in Kazakhstan follows the death of Erkezhan Nurmakhan, five, who was lured to a paedophile's house after he offered her money for an ice cream

Saidolim Gayibnazarov, 48, who had previous convictions, was sentenced to life in jail and chemical castration
Kazakhstan announced its own draft law to remove paedophiles genitals on February 6 following complaints from MPs that the current law where paedophiles are chemically castrated was not deterring child sex offenders.
The tighten of the law follows the death of Erkezhan Nurmakhan, five, who was lured to a paedophile's house after he offered her money for an ice cream.
Saidolim Gayibnazarov, 48, who had previous convictions, was sentenced to life in jail and chemical castration.
Deputy Interior Minister of Kazakhstan, Igor Lepikha, said surgical castration was 'controversial'.
'In terms of ethics and the human side of the issue it is very complicated indeed.
'Moreover, we speak about these criminals being locked up for life - so there is no point in [castration] then.'

#Madagascar#Kazakhstan#Madagascar's Minister of Justice Landy Randriamanantenasoa#President of Madagascar Andry Rajoelina#Of course Amnesty would criticised the bill#Shut up Tigere Chagutah#Rest In Peace Erkezha Nurmakhan age 5
453 notes
·
View notes
Text
The methodology for the Cass review was established by a team from the University of York including Tilly Langdon, who has previously been involved in promoting Gender Exploratory Therapy – an approach which, despite its neutral-sounding name, discourages children from identifying as trans and has been likened to conversion therapy. Her approach included setting a very high bar for evidence to be considered in the review, ruling out 100 of the existing 103 studies into the use of puberty blockers and hormones to treat trans children.
The reason given for excluding all these studies was that they did not incorporate a double blind approach – in other words, they did not involve giving puberty blockers to some patients and placebos to others. This might sound like a reasonable objection on the face of it – until one considers that puberty is a dramatic physical and psychological process, and people can easily tell when it’s happening to them, so a double blind simply wouldn’t work in practice.
The Cass review called for more research and, again, few would disagree with this. The suggestion that treatment should be withheld in the process, however, is not neutral. It presupposes that the harm done by puberty blockers (demineralisation of bones, which is usually temporary in the short-term treatment recommended and is similar to what occurs in pregnancy) is more severe than the harm done to a trans child by going through the wrong sort of puberty. The latter is linked to high rates of self-harm and suicidal ideation, together with the need, in many cases, for extensive surgical procedures.
Confusingly, the review states that children taking puberty blockers showed “no changes in gender dysphoria or body satisfaction”, which suggests that the author didn’t actually understand what puberty blockers do at all. They don’t make children feel better – they just delay a process that makes them feel worse.
This is one of several oddities in a report that lacks internal consistency. It states that there is no established definition of social transition, for instance, and does not offer one, but goes on to talk about it as if there were. It also talks about autistic ‘girls’ identifying as trans in increasing numbers, treating this as mysterious and as cause for concern, despite acknowledging elsewhere that more and more girls are being diagnosed as autistic, so one would expect more diagnoses to be present within any subsection of the young female-assigned population.
Perhaps the most worrying of the review’s conclusions – which should concern people far beyond the trans community – is the suggestion that as far as NHS treatment is concerned, trans people should be treated as children until they are 25. The rational for this is that 25 is the age when (on average) the brain stops developing. As any neurologist will tell you, the brain is in fact never static, and within ten years or so of that age, it begins to shrink. Deciding who has the capacity to make decisions based on brain age could have unintended consequences for the likes of Cass (64).
That aside, what would setting the age of true adulthood at 25 mean for everybody else? If we couldn’t allow people to consent to medical treatment at 24, should we ask them to risk dying for us? If not, then at a stroke we could lose a quarter of our armed forces. Likewise, we would have to give serious thought to what to do about a third of parents who might not be considered competent to look after their newborn children.
And then there are issues like contraception. Right-wingers have long contended, on one pretext or another, that teenage girls shouldn’t have the right to take the pill without their parents’ consent. This is where the review’s suggestion starts to look less like a double standard and more like the thin end of a very nasty wedge.
301 notes
·
View notes
Text


In a medical rarity that captured worldwide attention, a 36-year-old man from Nagpur, India, was discovered to have been carrying the remains of his twin inside his body for his entire life. This extraordinary case, known as 'fetus in fetu,' involves the presence of a malformed fetus inside the body of its otherwise healthy twin.
The patient, Sanju Bhaga, had been experiencing chronic stomach pain and bloating for years. After numerous consultations and inconclusive treatments, he visited the Acharya Vinoba Bhave Rural Hospital in Wardha, where doctors conducted a detailed examination. Imaging tests revealed a large mass in his abdomen, prompting immediate surgical intervention.
Dr. Ajay Bhandarwar, a senior surgeon at the hospital, led the surgical team. They were astounded to find a 15-centimeter mass that contained hair, bones, and other bodily structures – the remnants of Mahesh's parasitic twin. This condition, where one twin is absorbed by the other during early stages of pregnancy, results in the retained twin surviving as a parasite inside its sibling’s body, drawing blood supply but failing to develop fully.
The surgery, which lasted several hours, successfully removed the parasitic twin. Dr. Bhandarwar explained that the mass was surrounded by a sac and connected to Sanju’s blood supply, making the operation particularly delicate. Post-surgery, Sanju recovered well and reported a significant relief from the symptoms that had plagued him for decades.
Fetus in fetu is an extremely rare condition, with fewer than 200 cases documented worldwide. This phenomenon typically presents in infancy or early childhood, making Sanju’s case unusual due to the length of time the twin remained undetected within his body.
272 notes
·
View notes
Text
There are obviously many positions people may have on the proper place of intersex athletes in high level competitive sport, but between the fact that the IOC prioritizes athlete privacy (a good thing) enough to intentionally obfuscate relevant details (a bad thing), and the fact that your average journalist is generally incredibly uninformed about DSDs, most people will be unable to discern any relevant information from most reporting on the topic at least partly because media routinely refers to athletes having been "born a girl" who were by any biological definition (of which, of course, there is more than one) absolutely not born female but were visually sorted at birth as being female, or depending on country of origin (my understanding is that it is still quite common in the US to surgically alter the genitalia of children who do not need any surgical intervention for physical functions, although self advocate groups are working to change this) were surgically altered as infants in order to more easily allow the child to integrate socially as an adult, often without informing the patient until they do not normally develop at puberty, but sometimes continuing to lie to the patient even then due to cultural stigma. It does not help that Western audiences have been so culturally primed to see transgender identity and DSDs as inherently linked, and therefore primed to see DSDs as being a matter of personal identity. This is genuinely not in reference to any specific athlete, because this manner of disinformation being spread by media has been the case in more than one high profile incident. It's just a warning that, in many of these cases, media either intentionally or unintentionally tells potentially far reaching lies to readers while claiming to inform them.
156 notes
·
View notes
Text
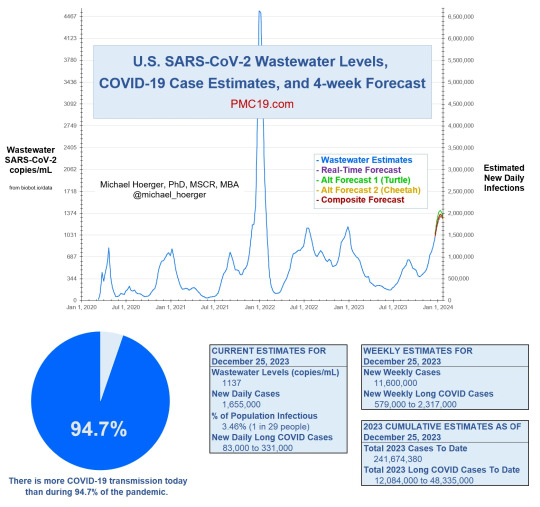
There is more COVID-19 transmission today (January 2024) than during 94.7% of the pandemic.
💉 Please get the updated (new, not a booster) Covid vaccine. If you're in the US, ask your local pharmacy about the Bridge Access Program for free vaccines. You can also search vaccines.gov then select Bridge Access Program participant.
If you do not want an mRNA vaccine for whatever reason, consider Novavax: it is protein-based like other typical vaccines from the last few decades, and many (including myself) report minimal side effects. Talk to your doctor if you have questions or concerns.
😷 Wear a mask in public and/or any enclosed areas. "Mask" means a respirator of KN95/N95 filtration or higher, not a cloth or surgical (blue) mask. Covid is airborne, so an airtight seal and particulate filter is necessary for protection. Different kinds of respirators are used for everything from toxic fumes to asbestos removal; when worn properly, they greatly reduce risk.
Here is a guide for proper use and fitting of a respiratory mask.
Here is a short video by 3M (respirator manufacturer) on the importance of fit-testing.
🧪 Have tests ready. With the new variants it can sometimes take 5-8 days to test positive, so be sure to test twice, 48 hours apart. If you're in the US, you can get 4 free rapid tests sent to your home through USPS. Local schools and libraries also may have free rapid tests. If you qualify for the Test to Treat program, you can receive free at-home NAAT tests and treatment for both flu AND Covid, and access to telehealth. The earlier you test positive, the more likely you will be eligible for treatment with Paxlovid.
🔁 If you can afford it, air purifiers and HEPA filters can help reduce transmission. Making a Corsi-Rosenthal box is simple and inexpensive. If weather permits, keeping windows open helps. Ventilation allows fresh air to circulate.
👃 Nasal sprays and CPC mouthwash are other useful prophylactic measures when used in conjunction with PPE and other modes of mitigation like masking and distancing.
🚬There is still a risk of Covid when outside, similar to exposure from secondhand smoke or a fire. Since Covid is spread through aerosols, it can hang in the air like smoke.
🐶 As with other coronaviruses, many household pets can get Covid. If you have been exposed, avoid contact with animals.
"But I'm not old or weak. Why should I care?"
☣ Covid can still kill you or disable you for life, even if your initial sickness is "mild". Even if you are young and have no preexisting conditions. 90% of the original "long haulers" had "mild" cases.
🩺 Covid increases your risk of stroke, blood clots, and heart disease by 2 to 5 times within a year of infection. It can also cause brain damage, which is part of the loss of taste and smell and cognitive symptoms like brain fog.
🩸 Covid is able to infect multiple organ systems because it travels through the bloodstream and attacks the mitochondria, leading to dysfunction and chronic fatigue.
⚠ Reinfection doesn't make your body better at fighting Covid; it just does more damage to your immune system, akin to HIV. A damaged immune system is worse at fighting off illness, more susceptible to infection, and can lead to serious complications like pneumonia. And with every reinfection, your chances of developing Long Covid increase. Therefore, the best protection for your immune system is to avoid getting Covid as much as possible.
I know everyone is tired of this. But if there was any time to be vigilant, it is now. Please, let's protect each other.
302 notes
·
View notes
Text
cheat | @jegulus-microfic | words: 520
critical care, part 1 | (part 2, part 3, part 4, part 5, part 6, part 7, part 8, part 9)
a Jegulus nurse!AU
“Potter, I’ve got shit news for you.”
James snorted, finishing the last few letters of a name on the large dry erase board that announced the day shift nurses’ assignments on the medical-surgical intensive care unit. Their ward’s nickname, coined by its wealthy donor, was written at the top in half-erased red letters: Go Gryffindor! “No thanks, Marlene, I’ve got enough shit news already.”
“Peter’s cheating on us. He’s been floated to take patients in the recovery room. They took on three extra cases this morning.”
Jerking his head around, he stared at her.
No.
Peter could not do this to him. James had twenty-two sick as shit patients tripping over themselves to dive into body bags and just enough nurses to stop them from doing so. The acuity of their unit was through the roof. He would not be tested today.
“Pete wouldn't do that.” James shoved his hand into his scrubs to fish his phone out. On the home screen was the preview of an apologetic text from ✨🐀Wormtail🐀✨, reporting his marching orders to the post-anesthesia care unit. “Wow. I thought he loved me. What am I supposed to do? We’re about to start the bloody shift!”
“Well don’t worry boss, because I have slightly less shit news. They’ve sent us a nurse to replace him.” She paused. “From Slytherin.”
“I thought you said less shit news,” James grumbled, using the side of his hand to rub Peter’s name from the board. Slytherin, with its name derived from the benefactor who had funded its building, was the cardiovascular intensive care unit two floors below them. Their nurses were notoriously nightmares to get along with. “The last time they floated someone from there to here it was Snape, remember?”
“Oh yeah!” Marlene snapped her fingers. “Didn’t Sirius almost trick him into drinking nitroglycerin? It’s a good thing you stopped him. He could have actually died.”
“Yeah. Anyway, who are they sending us?”
Marlene consulted her phone. “It’s going to be… Oh! Regulus Black!”
“Black?” James repeated distractedly, writing it down.
“It’s Sirius’s little brother. Have you met him?”
“No.” James capped his marker and stepped back. “Have you?”
“Once.” She paused, then qualified that. “Sort of. I got to watch Sirius threaten one of the doctors for flirting with him. Does that count?”
That got his attention. “What? Why? Sirius has slept with half the staff in this hospital!”
“Yeah, but he’d put Regulus in a monastery if he could. No dating allowed for Baby Black.” Marlene handed over the charge nurse phone. “It’s too bad. Dorcas says Regulus is… sweet.”
James smirked. “Dorcas says, huh? I guess Pete’s not the only one cheating on us Gryffindors by consorting with the enemy units.”
“Fuck off, Potter. And I’ll give you a bit of free advice. When Regulus comes up here, you’d best try very hard not to stare. Sirius hates when people do that.”
James’s expression turned serious. “I won’t. Is there something physically… did something happen to him?”
Oddly, Marlene just smirked. “No, nothing like that. But if you know what’s good for you, don’t let Sirius catch you looking.”
#regulus black#james potter#jegulus#protective sirius black#marauders nurse!au#sirius and regulus#sirius black#starchaser#james loves regulus#jegulus microfic
237 notes
·
View notes
Text
Surgical Case Reports Journal | PubMed Indexed Surgery Journal
Surgery Case Reports Journal publishes case reports in surgery, images in surgery, imaging in surgery journal, case reports in surgical journal, case series and videos in surgery journal etc. Surgery Case Reports Journal is a manual or mechanical intervention that involves cutting the patient’s tissues, or closure of an already existing injury or wound.
Surgery case reports journal demands certain features and conditions such as a sterile environment, anaesthesia, antiseptic measures, suturing, and specialised surgical operations. Surgical case reports journal and research involves research on human biology that benefits surgical care; it can be classified into three main categories: discovery (biological sciences), development (bioengineering), and delivery (population studies).

Journal of Spine & Neurosurgery Case Reports
Journal of Spine & Neurosurgery: Journal of Spine and Neurosurgery (JSNS) is a peer-reviewed scholarly journal and aims to publish the most complete and reliable source of information on the discoveries and current developments in the mode of original articles, review articles, Surgical case reports journal, short communications, etc. in all areas of spine & neurosurgery and making them available online freely without any restrictions or any other subscriptions to researchers worldwide.
Journal Highlights includes: Neuroanatomy, Neuroimaging, Neurological Disorders, Neurology, Neuropathology, Neuropharmacology, Neurophysiology, Neuropsychology, Neuroradiology, Neuroscience, Neurosurgery, Neurotrauma, Spinal Anatomy, Spinal disease, Spinal Injuries, Spine
Related Journals: European Spine Journal, Journal of Neurosurgery: Spine, The Spine Journal, Journal of Spinal Disorders & Techniques, The Journal of Spinal Cord Medicine, Journal of Neurological Surgery, Journal of Neurology, Neurosurgery & Psychiatry, Journal of Neurosurgery: Pediatrics, Journal of Neurology Research, Journal of Comparative Neurology
Journal of Diagnostic Techniques and Biomedical Analysis
Journal of Diagnostic Techniques and Biomedical Analysis: Journal of Diagnostic Techniques and Biomedical Analysis is a unique "Hybrid Journal" enriched with the benefits of subscription and effectiveness of open access. It accepts novel research, review papers, case reports, clinical trials, commentaries, short communications; letter to editor and diagnostic opinions in its scope JDTBA encourages rigorous peer review under the supervision of an editor. Thus, ensuring the quality of all the published articles which reflect solid scholarship in their field, and the information contained is accurate and reliable.
Journal Highlights: Disease Diagnosis, Autopsy, Biomedical, Biomedical imaging, Biomedical Informatics, Biopsy, Biopsy research, Chemical Imaging, Chromatography, Computerised Axial Tomography, Diagnostic Microbiology, Diagnostic Techniques, Diagnostic Tests, Disease Diagnosis, Endoscopy, HPV Test, Infectious Diseases, Medical Instrumentation, Radiology, Radiology and radioactive techniques procedure, Ultrasound.
Related Journals: Journal of Diagnostic Radiography & Imaging, Journal of Clinical Ultrasound, Journal of Computational Biology, Journal of Computer Assisted Tomography, Journal of Computer-Aided Molecular Design, Journal of Medical Ultrasonic, Journal of Medical Imaging, Journal of Ultrasound in Medicine, Journal of Medical Ultrasound, Journal of Digital Imaging
Journal of Universal Surgery Case Reports
Universal Surgery: Journal of Universal Surgery is an indexed peer reviewed internationally reputed medical journal. This scholarly Open Access journal aims at exploring new, relevant, and the most compelling developments in the field of Surgery. Journal of Universal Surgery is the best scientific journal that provides a good platform for researchers to publish their valuable work in the mode of research, review articles, case reports, commentaries, short communications, etc. Journal Highlights includes: Laparoscopic Surgery, Gallbladder Surgery, Arthroscopic Knee, Scoliosis Surgery, Sinus Surgery, Oral Surgery, Gynecomastia Surgery, Orthognathic Surgery, Thyroid Surgery, Pacemaker Surgery, Appendix Surgery, Endometriosis Surgery, Colorectal Surgery, Open Heart Surgery, Glaucoma Surgery, Hip Surgery, Hysterectomy Surgery, Neck Surgery, Hydrocele Surgery, Ankle Surgery, Outpatient Surgery
Journal of Transplant Reports: Open Access
Transplant Reports: Open Access: Transplant Reports : Open Access is an open access, Peer reviewed scholarly publication that addresses current, ongoing research on all types of organ and tissue transplants. The objective of the journal is to accelerate the growth of transplant by bringing together people with research interest in transplant. Our vibrant Editorial Board Members provide a unique platform for researchers to improve their research.
Journal Highlights: Allografts Transplant Reports, Bone Marrow Transplant Reports, Brain Transplant Reports, Corneal Transplant Reports, Eye Transplant Reports, Eyebrow Transplant Reports, Hair Transplant Reports, Head Transplant Reports, Heart Transplant Reports, Individual Organ Transplants, Kidney Transplant Reports, Liver Transplant Reports, Lung Transplant Reports, Pancreatic Transplantation, Stem Cell Transplant Reports.
Related Journals: Journal of allografts, Journal of eye transplantation, Journal of heart transplantation, pancreatitis journal, Journal of eyebrow, Bone Marrow transplantation, organ transplantation, stem cell transplantation, Journals of corneal transplant, International journal of transplant, Transplantation, Journals of tissue transplantation, Lung transplantation journals, Journals of immunology research, International journal of surgery, Journal of Oral and maxillofacial surgery, American journal of kidney, Transplantation proceedings
Case Reports in Cancer Surgery Journal
Cancer Surgery: Cancer Surgery is a peer reviewed, open access periodical which disseminates scientific information among the medical scientists and researchers in the relevant areas. The journal considers a wide range of topics in the realm of Cancer Surgery which includes but not limited to Breast Cancer Surgery, Colon Cancer Surgery, Dermatologic Surgery, Kidney Cancer Surgery, Leukaemia Surgery, Lung Cancer Surgery, Lymphoma Surgery, Oesophageal Cancer Surgery, Pancreatic Cancer Surgery, Prostate Cancer Surgery, Radiation Therapy, Skin Cancer Surgery, Stomach Cancer Surgery, Throat Cancer Surgery, Thyroid Cancer Surgery.
Journal Highlights: Breast Cancer Surgery, Colon Cancer Surgery, Dermatologic Surgery, Kidney Cancer Surgery, Leukaemia Surgery, Lung Cancer Surgery, Lymphoma Surgery, Oesophageal Cancer Surgery, Pancreatic Cancer Surgery, Prostate Cancer Surgery, Radiation Therapy, Skin Cancer Surgery, Stomach Cancer Surgery, Throat Cancer Surgery, Thyroid Cancer Surgery.
Journal of Cosmetology & Oro Facial Surgery
Cosmetology & Oro Facial Surgery: Cosmetology and Oro Facial Surgery is a peer reviewed, open access periodical which disseminates scientific information among the medical scientists and researchers in the relevant areas. The journal considers a wide range of topics in the realm of biomedical sciences which includes but not limited to Blepharoplasty, Bone Anchored Hearing Aids, Chemical peel, Cleft Surgery, Congenital Craniofacial Malformations, Cosmetic Facial Surgery, Craniofacial Surgery, Dental Orofacial Surgery, Dentoalveolar Surgery, Head and Neck Reconstruction, Injectable Cosmetic Treatments and Lip Reconstruction.
Journal Highlights: Blepharoplasty, Bone Anchored Hearing Aids, Chemical peel, Cleft Surgery, Congenital Craniofacial Malformations, Cosmetic Facial Surgery, Craniofacial Surgery, Dental Orofacial Surgery, Dentoalveolar Surgery, Head and Neck Reconstruction, Injectable Cosmetic Treatments, Lip Reconstruction, Mandibular Nerve Surgery, Maxfax Surgery, Maxillofacial Surgery, Neck Liposuction, Oral and Maxillofacial Surgery, Oral Surgery Surgeon, Orofacial Surgery Braces, Pediatric Maxillofacial Surgery, Rhytidectomy, Sleep Apnea Orofacial Surgery, Temporomandibular Joint Disorders, Upper Jaw Surgery.
Related Journals: Journal of Oral and Maxillofacial Surgery, Asian Journal of Oral and Maxillofacial Surgery, Journal of Dentistry, Journal of Cosmetic Science, Cosmetic Surgery
Journal of Aesthetic & Reconstructive Surgery
Journal of Aesthetic & Reconstructive Surgery: Journal of Aesthetic & Reconstructive Surgery is an open access journal and publishes the manuscripts after thorough peer review. This journal is involved in panel discussions, conferences and research articles and most part dedicated to surgeons to get to know the topics in cosmetic surgery, bariatric surgery and breast surgery etc. Aesthetic and reconstructive surgery refers to a variety of operations performed in order to repair or restore body parts to look normal, or to change a body part to look better. These types of surgery are highly specialised. They are characterised by careful preparation of the patient's skin and tissues, by precise cutting and suturing techniques, and by care taken to minimise scarring.
Related Journals: British Dental Journal, American Cleft Palate-Craniofacial Association, The Cleft Palate-Craniofacial Journal, Journal of Cleft Lip Palate and Craniofacial Anomalies, American Cleft Palate-Craniofacial Association, The Cleft Palate-Craniofacial Journal, Journal of Cleft Lip Palate and Craniofacial Anomalies, Neonatal Cleft Lip and Cleft Palate Repair - AORN Journal, Journal of Applied Oral Science, Johns Hopkins Surgeons Lead Double Arm Transplant, Hand Transplant History, Hand Transplantation, The leg transplant - The Boston Globe
Journal of Clinical and Experimental Transplantation
Journal Highlights: Abdominal Organ Transplantation, Bone Marrow Transplantation, Corneal Transplantation, Hair Transplantation, Stem Cell Transplantation, Thoracic Transplantation, Transplant Immunology, Transplant Tolerance, Transplantation Ethics, Xenotransplantation.
Journal of Medical Implants & Surgery
Journal of Medical Implants & Surgery: Journal of Medical Implants & Surgery is a scholarly open access international journal which focuses on surgeries associated with medical implanting involving ample amounts of technological contributions from different disciplines including clinical sciences, surgical aspects. The journal encourages a quick and rapid peer review process and immediate publication to disseminate the current research.
Journal Highlights: Body implants, Brain Implants, Cardiac implants, Cosmetic Therapies, Ear Implants, Facelifts, Heart Surgery, Implants, Invasive and non-invasive procedure, Knee Implants, Medical Implants, Musculoskeletal Surgery, Otolaryngology Medicine, Pacemaker, Stents, The study of Anatomy.
Related Journals: Plastic Surgery Journal, Breast Surgery, Cosmetic plastic surgery, plastic surgery articles, Breast augmentation Implants, Facial Plastic Surgery
Insights in Neurosurgery Journal
Insights in Neurosurgery: Insights of Neurosurgery is a peer-reviewed online journal which is devoted to the publication of original works relating primarily to neurosurgery. The manuscripts for review include innovative or useful to clinicians and researchers in the field of neuroscience; papers describing unusual cases; manuscripts on historical persons or events related to neurosurgery; and in Neurosurgical Focus, occasional reviews. The ambition is to publish the most ground-breaking and cutting-edge research from around the world. Encompassing the entire genre of neurological sciences, our focus is on the common disorders (stroke, multiple sclerosis, Parkinson's disease, epilepsy, peripheral neuropathy, subarachnoid haemorrhage and neuropsychiatry).
Journal Highlights includes: Virtual Brain Surgery, Advances in Neurosurgery, Spine Neurosurgery, Fluorescence Neurosurgery, Endovascular Neurosurgery, Neurosurgery Clinics Management, Neurosurgeons Communications, Brain Surgery, Open Brain Surgery, Pediatric Neurosurgery, Stereotactic Neurosurgery, Endoscopic Neurosurgery, Vascular Neurosurgery, Robotic Neurosurgery, Laser Neurosurgery, Advanced Instrumentation for Neurosurgery.
Authors can submit their manuscripts through the journal's online submission portal and For more information on Literature Publishers - surgical case reports journal visit our site:-
#surgical case reports journal#Surgery Case Reports Journal#Surgical Case Reports in Surgery Journal#case reports in surgery
0 notes
Text
My dear lgbt+ kids,
Did you know the practice of meditation can have side effects? Some people experience adverse reactions to meditation, such as heightened anxiety or depression or even delusions and hallucinations.
What does that have to do with being lgbt? Well, nothing - but meditation is often seen as one of those “healthy things everyone should do”, something that just has so many benefits and doesn’t require you to take anything or undergo any kind of surgery, something that it’s widely recommended and accepted as healing… and even THAT super great thing has some people who will regret doing it.
Not a perfect comparison, nothing ever is, but you see the analogy coming: Transition (social or hormonal or surgical) is super beneficial to many people. And there are also some people who will regret it.
Any kind of health decision - and really any decision at all - can end with you regretting it. That’s a part of life.
“Protecting people from making a decision they might regret” sounds like such a noble goal. We want to live in a world where people can make informed decisions. Education, including on risks and side effects, is something to strive for. But it’s important to remember that we can not live in a world where nobody ever regrets anything.
People can regret getting their ears pierced. People can regret buying a car. People can regret going to university. People can regret having sex with someone. People can regret marriage. People can regret moving to a different state. People can regret coming out as gay. People can regret hip replacement surgery. And yes, people can also regret transitioning.
If we seriously wanted to protect people from ever regretting anything, we would need to just take any deciding power away (and then who would we give it to? Whoever makes our decisions for us then, they could also make a decision they end up regretting!).
Another reason why this analogy works: I told you meditation has side effects and people regret it - but I pretty conveniently left out that it’s pretty rare for that to happen. Meditation is generally very safe and has a really low regret rate. Plus, people who regret it may not regret that they choose to meditate all together but rather report that they regret a specific experience (such as choosing silent meditation over guided meditation or going on a meditation retreat that lasted multiple days).
Similar to that, transition also has a low regret rate (statistically much lower than tattoos or hip replacement surgery for example!) - and people who regret it may not actually be a case of “I regret it because I realized I’m not transgender”, even if that’s what transphobes tell you. Some people still identify as transgender but regret their surgery because they experienced complications (as they can arise from any kind of medical procedure). Some people regret it because they lost friends or family or job opportunities after coming out. And so on.
The topic of regret is much more complicated than “meditation is actually bad” or “they woke up one day and realized they were brainwashed into believing they were trans”. And it’s unfair to not only the ones who will never regret it but also to the ones who do regret it to reduce their stories to a cautionary tale meant to stop people from making a decision over their own body.
“We need to protect people from making decisions they might regret” just isn’t a good argument.
With all my love,
Your Tumblr Dad
72 notes
·
View notes
Text
Healing Hearts

includes: alex karev in the beginning of his peds residency, a seattle grace mercy west merger which involves a new mercy west transfer....
black fem surgical resident! reader x alex karev
song inspiration: ivy- taylor swift
---------------------
Y/N walked into Seattle Grace, the bustling environment a sharp contrast to her previous residency. As a new resident transfer, she knew she had to prove herself. Her heart pounded with a mix of excitement and nervousness as she reported for her first day on Arizona Robbins' pediatric service.
"You're the new resident, Y/N?" Arizona greeted her with a warm smile. "Welcome to Peds. You'll be working closely with Dr. Karev today. He knows my service and he'll help you if you have any questions."
Y/N had heard of Alex Karev's reputation. He was known for his exceptional skills with children but also for his abrasive personality. She was determined not to let his reputed arrogance faze her.
When she met Alex in the pediatric ward, she was struck by his intense eyes and the air of confidence he exuded. "You're the new transfer?" he asked, not looking up from the chart he was reviewing.
"Yes, I'm Y/N," she replied, trying to keep her tone professional.
"Okay, let's get one thing straight. I don't have time to babysit," Alex said, finally looking at her. "Just stay out of my way, and we'll be fine."
Y/N bit back a retort. "I'm here to learn and help. Let's just focus on the patients."
Their first case together was a young boy named Liam, suffering from cardiomyopathy. The child's condition was delicate, and his treatment required careful coordination. Despite their initial friction, both Y/N and Alex were deeply invested in Liam's well-being.
"His latest tests show worsening heart function," Y/N said, frowning at the results. "We need to act fast."
Alex nodded. "We need to discuss his case with Dr. Robbins. If we don't come up with a new plan, he won't make it."
They presented their findings to Arizona, who decided on a risky but potentially life-saving surgery. Throughout the procedure, Y/N and Alex worked in perfect sync, their combined skills bringing the best possible care to Liam. In the days following the surgery, Y/N and Alex found themselves spending more time together. They worked late into the night, monitoring Liam's progress and making sure he was stable.
----------------------
One evening, after a particularly exhausting shift, they found themselves alone in the residents' lounge. Alex, surprisingly, broke the silence.
"So, you're a Mercy West transfer?" he asked, his tone less harsh than usual.
"Yeah," Y/N replied, sipping her coffee. "Since the merger. What about you? You've been here a while, right?"
"Yeah, since my intern year." Alex said. "It's a great program. "
Y/N nodded. "I can see that. But I like it so far. The team is great, and the cases are challenging."
Alex looked at her, a hint of a smile playing on his lips. "You handled Liam's case well. Most new residents would have freaked out."
Y/N felt a warm flush of pride. "Thanks. You weren't so bad yourself."
--------------------
As the weeks passed, they continued to work together, their initial animosity giving way to mutual respect. They shared stories about their backgrounds, their dreams, and their fears. Y/N found herself looking forward to their shifts together, her heart skipping a beat whenever Alex smiled at her. One day, as they were preparing for another surgery, Y/N noticed Alex seemed distracted. "Everything okay?" she asked gently.
Alex hesitated before answering. "Just...family stuff. My brother's in town, and it's complicated."
Y/N placed a reassuring hand on his arm. "If you need to talk, I'm here."
Alex looked at her, surprise and gratitude in his eyes. "Thanks, Y/N. I might take you up on that."
Their bond continued to grow, each moment together strengthening their connection. They laughed more, confided in each other, and began to realize that the line between professional and personal was blurring.
One night, after another successful surgery, they found themselves standing on the hospital roof, the city lights sparkling below them.
"You know," Alex said, his voice soft, "I never thought I'd say this, but I'm glad you're here."
Y/N smiled, her heart swelling with emotion. "Me too, Alex. Me too."
As they stood there, side by side, they knew that whatever challenges lay ahead, they would face them together. In the midst of the chaos and the heartbreak of Seattle Grace Mercy West, they had found something unexpected: each other.
--------------------
During the weeks following their initial meeting, Y/N and Alex found themselves thrown together in a variety of challenging cases. Each case revealed more about their personalities and work ethics, slowly breaking down the walls they had built around themselves.
In one particularly intense case, they treated a toddler with a rare genetic disorder. The child's condition was rapidly deteriorating, and both Y/N and Alex had to rely on each other to come up with a treatment plan.
"His genetic markers indicate a possible enzyme deficiency," Y/N pointed out during one of their late-night strategy sessions. She was surrounded by stacks of medical journals and lab reports.
Alex leaned over the table, scanning the data. "Good catch. Let's run a specific panel to confirm and then we can start the enzyme replacement therapy."
Their combined efforts paid off, and the toddler began to show signs of improvement. The victory was a turning point in their relationship. They began to see each other as partners rather than competitors.
One day, after a long shift, Y/N and Alex found themselves in the on-call room, too exhausted to go home. They lay on opposite bunks, the room dimly lit by a small bedside lamp.
"Why did you choose pediatrics?" Y/N asked, breaking the comfortable silence.
Alex turned his head to look at her. "Kids are resilient. They can go through hell and still bounce back. I guess I wanted to be a part of that."
Y/N nodded, understanding. "I get that. I love their spirit, their will to fight. It’s inspiring."
As the days turned into weeks, they shared more personal stories. Y/N learned about Alex’s difficult childhood and his struggles with his family. In return, Y/N opened up about her own challenges, including the pressures she faced at her previous residency.
Their late-night conversations became a routine, each one drawing them closer. They began to anticipate each other's needs in the operating room, moving with a synchronicity that amazed their colleagues.
One evening, after successfully performing a complex surgery on a newborn, they sat in the hospital cafeteria, finally allowing themselves to relax.
"Do you remember the first time we met?" Y/N asked with a smile.
Alex chuckled. "Yeah, I wasn't exactly welcoming."
"That's an understatement," Y/N replied, laughing. "But you've grown on me, Karev."
"You too, Y/N. You too."
Their eyes locked, and for a moment, the bustling cafeteria faded away. They both knew something significant had shifted between them.
As the relationship evolved, so did their feelings. They began to steal glances at each other in the hallways, their touches lingered a little longer, and their conversations took on a deeper, more intimate tone.
One night, after another grueling shift, they found themselves alone on the hospital roof again, the cool night air providing a welcome respite.
"Sometimes, I wonder how I got so lucky to have you as a partner," Alex said, his voice sincere.
Y/N turned to him, her heart pounding. "I feel the same way, Alex."
He reached out, taking her hand in his. The touch was electrifying, sending a shiver down Y/N’s spine. They stood there, hand in hand, the city lights below them, knowing that they had found something rare and precious in each other.
He stepped closer, cupping her face in his hands. "Then let's see where this goes."
They shared their first kiss under the starlit sky. From that moment on, they faced every challenge together, their love growing stronger with each passing day. In the chaotic world of Seattle Grace Mercy West, they had found their calm, their solace, and their love.
#alex karev#alex karev x reader#alexkarevxblackreader#black reader#black tumblr#carl gallagher x reader#black women#carlgallagherxblackreader#fanfic x reader#fanfic#black fanfiction#fanfiction#fandom#meredith grey#derek shepherd#greys anatomy
90 notes
·
View notes
Text
It's Gastroparesis Awareness Month
Hi! I have gastroparesis and I'm an insufferable know-it-all so let's talk about it!
Gastroparesis, or a paralyzed stomach, is a condition that causes delayed gastric emptying.
This can cause a range of symptoms and complications:
nausea
vomiting
early satiety/fullness
upper gastric pain
heartburn
malabsorption
dehydration
malnutrition
Gastroparesis can be treated by a gastroenterologist, but often needs to be managed by a motility specialist due to a lot of misconceptions about the condition. Providers, especially in the emergency department, will commonly misdiagnose gastroparesis as cannabis-hyperemesis syndome, cyclic vomiting syndrome, gastritis, food poisoning, etc.
There are several commonly known causes of gastroparesis like vagus nerve damage from diabetes, injury to the stomach, and stomach surgery like hernia repair or bariatric surgery. There are also idiopathic cases with no known cause. Other causes of gastroparesis are:
Connective tissue disorders like HSD and EDS (commonly hEDS and cEDS)
Post-viral (like COVID, viral gastritis, mononucleosis/Epstein-Barr)
Restrictive eating disorders
Autoimmune diseases like Systemic sclerosis (scleroderma), Lupus, Hashimoto's
Central nervous system disorders
Gastroparesis also has common comorbidities with conditions like:
POTS and other forms of dysautonomia (POTS, EDS, and gastroparesis are a common triad of diagnoses)
MCAS
SMAS (which can also present with similar symptoms to GP)
Intestinal dysmotility and esophageal dysmotility disorders (known as global dysmotility)
PCOS with insulin resistance
Endometriosis
SIBO/SIFO
Chronic intestinal pseudo-obstruction
Migraines
Certain medications like Ozempic and other drugs in that class act on the digestive system to delay gastric emptying, which has caused people to be diagnosed with gastroparesis. Some people report that their cases have not gone away since stopping the medication, others report feeling better after stopping. Other drugs like opiates and narcotics can cause delayed gastric and intestinal motility as well, but these are commonly known side effects of those painkiller classes.
Gastroparesis is classed based on severity and graded based on how you respond to treatment.
Severity of delay ranges from mild to very severe, and this is based on your actual stomach retention calculated at 4 hours into a gastric emptying study.
The grading scale ranges from one to three, one being mild and three being gastric failure.
There is no consistent single treatment that is proven to work for gastroparesis, and there is no cure. Treatments can consist of:
Diet changes (3 Step Gastroparesis Diet, liquid diet, oral sole source nutrition)
Prokinetic (motility stimulating) drugs
Anti-nausea medications
Proton-pump inhibitors
Gastric stimulator/gastric pacemaker
Pyloric botox and dilation
G-POEM/pyloroplasty
Post-pyloric tube feeding
Gastric venting/draining
Parenteral nutrition
IV fluids
Other surgical interventions like gastrectomy or rarely, transplant
Gastroparesis is a terrible disease and I hope that if any of these symptoms resonate with you that you can get checked out. I was misdiagnosed for a long time before getting a proper gastroparesis diagnosis, and all it took was a gastric emptying study. This is ESPECIALLY true if you're having post-COVID gastrointestinal problems that are not improving. I almost died from starvation ketoacidosis because of how serious my GP got in a short period of time post-COVID (I had GP before COVID), and now I'm tube reliant for all my nutrition and hydration.
Stay safe friends!
652 notes
·
View notes
Text
Hong's Anatomy: Part 1
Pediatrician surgeon! Joshua x pediatric surgeon! Female Reader
Synopsis: Coming to Grey Sloan Memorial Hospital wasn’t on your bucket list, that’s for sure, but when you meet the head of your department, Joshua Hong, it's one of the only things that constantly brightens your day.
Warnings: swearing, made up medical terms and procedures, i have no idea if any of this is medically accurate it’s just for story, flirting, no smut…yet?
Words: 3.5k (not quite 5k words, but I had to end this part like this)
NOT EDITED, SO I MAY GO BACK AND EDIT LATER (teehee)
------------------------------------------------------------------------------
“Julia Harring, fifteen years old, kidney failure. Waited six months on the donor list and today is finally the day,” Surgical intern Jonah read, as Julia nodded.
“Why do both of you have to work on me? I thought it was only one big fancy surgeon per patient?” Julia asked, referring to both you and Joshua. You chuckled and checked her monitor to record her stats.
“This is a bigger surgery Julia. You should be grateful that Doctor Hong and I are both making sure that your transplant goes well.” Julia rolls her eyes and smiles.
“I have to go see another patient, but I’ll see you in the OR,” Joshua smiles, as you nod and Julia waves, before making his way down the hall.
Julia smiles and looks at you from the corner of her eye, “he’s hot.”
“You think so?” You joke back, as she nods. “Doctor Hong is quite popular here, so I’m sure you aren’t the only one that thinks that.”
“Including you?”
You pause in the middle of changing her I.V to look around the room. Luckily there was no one, but if anyone did here, it would be incredibly embarrassing.
“I think Doctor Hong is a lovely person and an incredible surgeon, I haven’t paid attention to his appearance,” you state resuming changing the I.V as she scoffs.
“Please, you were both making eyes at each other the whole time. Don’t tell me you don't like even thinking of becoming a thing with him?” Julia said, lifting her arm both for the I.V and to shrug.
“I don’t have time to make it a ‘thing’ with Doctor Hong Julia. If I was a ‘thing’ with Doctor Hong, I wouldn't have time to help you,” you say inserting the I.V causing Julia to wince. “Don’t touch the I.V for a bit, I’ll get someone to catch up with you right before the surgery.” Julia nodded, as you left the room and asked Green to check up on Julia’s vitals before the surgery and report to you before your pager went off to go down to the pit.
“What’s going on?” You asked, watching a whole bunch of people benign wheeled across the pit and placed in the rooms.
“School bus accident, dozens of kids were injured,” Joshua exclaimed rushing to room one, “go to room five.”
You nodded and put on a fresh pair of gloves before making your way into room 5. “What’s their case?”
“Mikayla Thurthey, nine years old. Broken arm, broken rib, punctured lung. If we move the fractured rib or anything on the right side the lung starts leaking and fluid can flood the lung,” Mingyu said, working busily around the room.
“Shit,” you muttered under your breath, watching the little girl in front of you crying. “Can we get an OR?” We need to fix the arm and fix the lung right now?” Mingyu nodded, and started wheeling Mikayla down the hall to the elevator. While you were running down the hall, you saw Joshua giving a boy CPR and pulling out a crash cart.
“Clear!”
------------------------------------------------------------------------------
“Okay, can you work on the lung. I can do the arm?” Mingyu asked, as you nodded and started washing your hands.
“How many more kids were like this?” You asked quietly. Slightly terrified of the answer.
“Just two. Mikayela and Justin, the boy Josua was working on. The rest were hurt, but with a few broken arms and legs or whiplash. These two were at the back and got the grunt of the force from the accident.” You nodded, and took a deep breath.
“Let’s do this,” you said, as you both headed into the OR.
Once you had gotten to the lung you noticed the puncture and started thinking about what to do. You moved quickly and removed the debris and instructed Green to keep consistent suction on the site to prevent the fluid from flooding the lung while you started working on repairing the site.
“More suction Green,” you calmly asked, as Green got closer into the site. “Mingyu?”
“Yeah?” He asked, not looking up.
“She’s hypotensive, can you back off the arm from a second,” you said, as Mingyu backed away from her arm and looked over to see you working on trying to steady her episode.
“Green? What do you do when someone is hypotensive?” You asked, as Green paused for a moment, but quickly responded.
“Ensure effective manual ventilation of the lungs,” He responded confidently.
“Yes, but she’s already on ventilation, and it’s not helping,” you challenged.
“I don’t know then,” he confessed as you nodded.
“That’s okay, we’re going to get you to not only suction but also apply some air pressure on the site to make sure that it’s getting ventilated properly. It’s okay that you don’t know, this doesn’t happen very often,” you reassured him, as he nodded and started applying the pressure. A few moments later, her vitals went back to normal and Mingyu resumed working on her broken arm again.
------------------------------------------------------------------------------
After the surgery, you were given a lunch break, so you decided to eat outside in the ‘greenhouse’ section of the hospital. Once you got there you saw Joshua sitting on the bench you’ve claimed, crying.
“Joshua?” You asked, slowly approaching him. He quickly spun around and wiped his tears away.
“Oh. Hi, sorry,” he started, “I was just leaving.”
“No, please don’t go,” you reached out, “are you okay?”
You assumed it was because of the boy, Justin, was the reason Joshua was crying, but you wanted him to tell you.
“I should be better with losses. I’ve had a ton of them,” he sighed, “but Justin was so scared when he was awake, he kept asking for his dad and asking me if his friend Mike was okay.” You empathetically nodded and placed a hand on his shoulder as he started to cry more.
“You did everything you could,” you tried to reassure him.
“I know I did. I always try my very best and it wasn’t enough. He died scared and alone,” he sobbed. “He didn’t die alone,” you interrupted.
“You were there with him, Rose was with him, there were people who cared about him when he died. He wasn’t alone.” Joshua took a deep breath, trying to calm down his breathing, and nodded.
“How did your surgery go?” He managed to stay in stuttering breaths.
“It went well. Managed to fix her punctured lung and broken arm and I had a teaching moment with Green,” you said, as Joshua wiped his nose and nodded.
“That’s good.”
You both sat in comfortable silence watching the clouds move above your heads, before his pager went off.
“I have to go check on Julia. Her surgery is right after your lunch, so I’m gonna go make sure everything is okay,” he said, wiping his nose one last time and standing up, wiping his hands on his pants.
“Okay, I’ll be there right when I’m done,” you smiled, as he nodded and started to head in before pausing.
“Thanks for letting me talk and comforting me like that. I’m supposed to do that for you.”
“We can treat it like a currency, I’ll comfort you, if you comfort me later?” You joked, as he chuckled, and looked down at the grass.
“So I’m in debt, great. Haven’t dealt with that in a while,” he joked back before heading inside. Leaving you alone to think about the vulnerable moment you just shared.
------------------------------------------------------------------------------
“Doctor L/N?” Joshua asked, coming up to wash his hands right next to you.
“Doctor Hong?”
“Would you mind keeping our interaction, more specifically the… crying aspect of the conversation, private?” He whispered, as you nodded and shut off the water.
“Of course. I expect none the less when it comes my turn,” you said as he turned to see you and smiled, before putting on his mask.
“Let's go save a life.”
You nodded and walked into the OR to see some nurses you've never worked with before. Jennie, Yuna, and Jake, and a new anesthesiologist Jay.
“Hello everyone, let’s save this girl's life,” you said, as everyone nodded in agreement and started getting to work. Joshua made the first incision while you made sure the bleeding was controlled and moved a few organ’s around. Jonah had just gone to receive the kidney, since it was very delicate and had to be handled carefully and in a timely manner.
After about thirty minutes of Joshua making sure everything was okay, you started to make an incision on the lower abdomen to make room for the new one when Jonah came into the room with the new kidney.
Joshua took the kidney and slowly took it out while you back up a bit to let Joshua fit it in the new cavity. He placed it in when all the sudden the monitor started beeping rapidly.
“What’s happening?” Joshua asked, trying to not move too quickly and damage the kidney.
“She’s clotting and bleeding out!” You said, grabbing the suction and trying to clean up the pool forming. “Push Coumadin and get me some rag’s please!” You instructed Yuna and Jennie as they nodded while Jay worked on adding the Coumadin. “Put the kidney back, it’s gonna be a bit.” Joshua nodded and carefully put the kidney back and started moving to stitch up the bleeding.
You waited a few moments for the blood thinners to kick in but they weren’t working quick enough.
“Push more Jay!” You exclaimed, as Jay nodded and added more. Finally her blood started to thin out and her vitals were getting better. Joshua quickly finished up the stitches and picked up the kidney again placing it in the cavity and working on attaching it properly.
Right before closing Julia up you noticed some of her numbers weren’t looking quite right and didn’t want to stitch her up with unbalanced numbers.
“Can we test the kidney before we close?” You asked Joshua, as he nodded. You watched it, waiting for the color to appear into the kidney, which normally took up to two minutes after being placed in the body.
“Shit.” Joshua said, looking up at the clock. It had been about four minutes and the kidney was starting to look gray, instead of coloring. “It’s dying!”
“We’ve opened up a spot for her though,” you mumbled, trying to think of a solution when all the sudden the machines started beeping.
“She’s crashing!” Rose said, as everyone started running around.
“We did everything right! What’s going on?” Joshua confessed as you heard the machine flatline. “Shit, get the crash cart!”
You started compressions, and whipped your head to look at Joshua who was looking at her vitals wondering what was going wrong in the surgery, wile Rose handed you the paddles.
“Charge to 300. Clear!” You said, as Juila convulsed, but no heartbeat.
“Clear!”
350, “Clear!”
400, “Clear!”
“Charge to 450,” you exclaimed as Joshua sighed and looked at you trying desperately to save Julia.
“Y/N,” he muttered, “she’s gone,” he said. Trying to pry you from her body.
“No, she was in here for a kidney transplant, not a heart failure!” You cried, looking around the room to see everyone with their head down.
“Time of death, 17:21.” Joshua said, breaking the silence. You looked to Joshua to see him covering the incision and started to feel sick.
“Can you close alone, Doctor Hong?” You asked, as Joshua nodded. You quickly took off your mask and gloves and darted out of the OR.
------------------------------------------------------------------------------
“Y/N?” Joshua asked, walking up to you at the Ped’s desk. You were looking over Julia’s charts again.
“I don’t get it. She was fine, they wouldn’t have given her the kidney if she wasn’t fine, why did her heart just stop like that? The blood thinners don’t stop your heart like that, it must have been something else,” you exclaim, not looking up from your tablet.
“You’ve been here for a long time, you need to go home. You can do some more research when you get back,” Joshua pleaded, trying to take the tablet from you.
“Joshua…”
“No, Y/N. You had two long surgeries, you’ve been here for twelve hours. You legally have to go home now,” he chuckled, but you could tell he was serious. Technically, he was your boss. So you listened and slowly put the tablet down.
“Julia was my first loss. I’ve been here for almost a month and she was my first loss,” you quietly confess. Joshua wouldn’t have heard it if he wasn’t facing you.
“You’re very lucky you’ve gone this long without a loss,” he answered.
“I know. My last job, I lost two kids on the first day, but it doesn’t make this loss any easier.”
“Of course,” he said, “the hard part about this job, right?”
------------------------------------------------------------------------------
Letting the loved ones know that they just lost their person is always the hardest part and unfortunately, that was Joshua’s job today. Julia’s parents were in the waiting room and her father was pacing around the room.
This was also the hardest part of the job.
“Excuse me, Mr. and Mrs. Harring?” Joshua asked the couple as they both nodded and stood up.
“Is Julia out yet?” Her mother asked.
“There was an unfortunate complication during Julais’ surgery. We were performing her transplant when her heart suddenly stopped beating,” Joshua explained, “we tried everything we could, but we couldn’t save her. She unfortunately passed away.”
Julia’s mother covered her mouth whilst letting out a sob, and her father furrowed his eyebrows in confusion and held his wife.
“What? I thought she was in there for her kidney? How did her heart stop?” Her father asked, tears also running down his face.
“We aren’t sure, the operation was going extremely successful. Neither I, nor Doctor L/N could figure out why. We tried everything we could though to try and start her heart again,” Joshua explained again, as her mother turned around and buried her face into her husband's shoulder, crying even harder.
“I’m so sorry for your loss.”
“Thank you Doctor,” her father choked out, before turning and burning his face into his wife's hair and crying as well.
Joshua waited for a few seconds before heading back to the desk. He sighed, and ran a hand through his hair before grabbing his tablet and started filling out paperwork.
He had lost two patients that day. He was also ready to go home.
------------------------------------------------------------------------------
“So, how’s your new job Y/N?” Your therapist asked.
You had been going to the same therapist ever since you graduated college. She was a lovely woman that you met when you lived back in South Korea. She really helped you during your internship and residency. You managed to keep in close contact with her even after you moved.
You sighed into the phone and took a sip of wine.
“It’s going well, I really like my coworkers. I’m still getting used to it and I haven’t made any real friends,” you confess.
“Why haven’t you made any friends?” She asked, you could hear her typing away on her laptop.
“Well at first I was just trying to keep up with the pace of the hospital. Then I was trying to just be liked by everyone. I never took time to get to know anyone,” you said, “I did ask someone out.”
“Oh! That’s good. Tell me about them,” she exclaimed.
“He’s technically my boss? Kinda, he’s the head of the Ped’s department, so we work together quite a bit. On my first day he asked me out, then the next day I asked him out, but we haven’t hung out since.”
“Are you wanting anything romantic out of him?” You sighed, and took a minute to think about the question. Not quite sure if you knew the answer.
“I don’t know. I mean he is very attractive and we do have pretty good chemistry,” you blush, “but again, we work together. So it’s complicated.”
“That doesn’t sound like a no.”
“Jisoo,” you warn, “it’s not a no, but I don’t want to rush into anything.”
“That’s perfectly valid, but you’re all alone in a big city. Romantic intentions or not, you should still try and spend some more time with him,” she said, as you sighed. There was only a few minutes left in your session, so you both called it a night and promised to call again next month. Something you weren’t expecting from Jisoo though, was homework.
Make one close friend by next month.
------------------------------------------------------------------------------
You were always the type of person to do your homework immediately. Assigned all the semester's course work? It was done by the end of the month. So when you got homework from Jisoo, you wanted to get it done immediately. Which meant that you needed to get started immediately.
Joshua wasn’t coming in until halfway through your shift, so that meant that you had half a day to come up with ideas of how to befriend others.
“Why the long face?” Jeonghan asked. You never really see him in the Ped’s department, so seeing him was a surprise. Now was the time to try and make a new friend.
“I was just thinking how it’s a friday and that I don’t have any plans after work,” you confessed, “do you want to go for dinner after work?”
“Dinner?” He asked, you could tell he was quite taken aback, but he had a smirk on his face. “I’d love to.”
“Great. I get off at seven, but I’d like to go home and freshen up,” you said, as Jeonghan nodded. You both exchanged numbers and agreed that he’d pick you up from your apartment at eight, and go out to dinner.
Good progress toward your homework.
“See you at eight,” he smirked, before heading into one of his patients' rooms.
“Did you just score a date with Doctor Yoon?” Jake asked, as you turned around and tried to hide your blush.
“Maybe, he didn’t call it a date,” you replied. Jake rolled his eyes.
“I heard that whole conversation. It’s a date Y/N.”
“What’s a date?” You heard behind you. More specifically, Joshua’s voice.
Shit.
“Y/N is going on a date with Doctor Yoon,” Jake answered. You looked to Joshua to see a little look of surprise on his face.
“It’s not a date, I’m just trying to make some friends,” you mumbled, “and Doctor Yoon seems like a good friend.”
“He is a very good friend, I would know. He’s my best friend,” Joshua said, putting his hands in his pants pockets and crossing his legs.
Shit. Again.
You just set up a date with your boss/kinda crushes best friend.
A/N: OMG, this was quite the chapter. I had a lot of fun learning/ making up some medical procedures. I tried my best to be as medically accurate as possible, but google can only tell you so much. Also, Jeonghan has been added into the arena! I love the banter that Joshua and Jeonghan have and I just new that I had to have his smirky/sassy attitude! I really do hope you like this ♥
taglist: @asasilentreader , @myjaeyunn
#seventeen fic#joshua x y/n#seventeen imagines#seventeen x reader#joshua hong#seventeen fanfic#joshua angst#yoon jeonghan#Hong's Anatomy#greys anatomy
122 notes
·
View notes
Text
Yandere SCP Senior Researcher!Dottore who loves to act as the mentor figure for Agent!Darling.
Dr. Zandik had always been known for his surgically precise way of handling anomalies— but there's an intensely palpable reason as to why urgent cases aren't left on his desk. Before he could ever conclude an experiment, he'd ensure that he explored every possible data there is to be recorded, quantifiable or otherwise. This usually meant he'd apathetically sacrifice Class-D personnel just to find what the test subject would react. Site 02 reveres him... Yet most of his colleagues would rather have new blood trained than indulge his unnecessary experiments.
What made you first stand out to him was your files. Apparently, you share similarities with the famous SM-046 patient; you've contracted Urbach–Wiethe disease in your early childhood as well. Just like SM-046, your colleagues dubbed you as "Agent Without Fear". You could only shrug and laugh the teasing off. It's a challenge for you to distinguish what is malicious from pure— so you lived most your life expecting the latter.
With Dr. Zandik's passionate nagging requests, SCP-500 was updated with a new line...
Addendum 500-13:
Request 500-2022-A approved. One (1) pill of SCP-500 was ingested by Agent (L/n). Subject reported to have improved skin, mucous membranes, eye, vision, speech, and respiratory symptoms. However, neurological symptoms caused by Urbach–Wiethe disease have shown no signs of improvement. Number of pills is forty-six (46) at the time of writing.
In truth, the fact that you remained as the "Agent Who Can't Feel Fear" after the Trial 1 made Dr. Zandik more interested in you. Which is why, much like last time, the doctor submitted another revision. Instead of an SCP, it was a personnel file.
Yours.
Incident Report 921-A
Date: [REDACTED]
Personnel Involved:
Dr. Zandik "Dottore" █████ [Senior Researcher]
Agent (Y/n) (L/n) [Assigned MTF Officer]
BEGIN LOG
Dr. Zandik: Agent (L/n), just the person I wanted to see. I’ve requested you be assigned as my permanent bodyguard.
Agent (L/n): Really? That’s a new one. Why me?
Dr. Zandik: I’m very interested in your unique approach to security. I think your presence will be invaluable.
Agent (L/n): Well, if you say so, Dottore. I guess I’m in! Every time I work with you, you're always dragging me around to say hi to whatever weird and funky SCPs you're working with. This should be fun.
Dr. Zandik: Undoubtedly so. I’m looking forward to working with you.
Agent (L/n): Great! I’ll do my best to keep you safe, even if I seriously think you can handle most things on your own, Doc.
Dr. Zandik: I assure you. It’ll be a learning experience for both of us.
END LOG
Addendum Incident 921-A-1:
Agent (L/n) has been reassigned as Dr. Zandik’s permanent security detail, as requested by Dr. Zandik. The nature of Dr. Zandik’s interest in this arrangement remains undisclosed to Agent (L/n).
#Zandik x reader#dottore x reader#yandere dottore x reader#SCP au#yandere genshin impact x reader#yandere gi#yandere doctor#yandere male#yandere genshin#yandere genshin imagines
101 notes
·
View notes
Last Seen Blogs

spiderswipe
SPIDER SWIPE
angelseekingchaos
b l e u c c y :

1inkribbon796-blog
InkRibbon796

boneapptheteef
BoneAppTheTeef
spiderswipe
SPIDER SWIPE