#access health services
Text
Weight Loss Doctors in Washington Dc | Access Health Services

Access Health Services is one of best Weight Loss Doctors in Washington Dc our weight loss program is a sustainable, groundbreaking and exceptional weight loss program; which is formulated to assist patients in losing weight, feel more energized, and restore their vitality.We tend to gain weight as we grow older due to our metabolism slowing down as compared to our earlier ages. Visit Now: https://www.accesshealthservices.org/weight-loss/
#access health services#access healthcare services#georgetown weight loss clinic#weight loss clinic near me#weight loss programs near me#washington dc weight loss
0 notes
Text
The decriminalization of HIV enhances the HIV response because the removal of fear of prosecution helps people to access health services.

POSTCARD VIII- Zero Discrimination Day 2024; March 1st.
#access health services#zero discrimination day#1 march#campaign#decriminalization#UNAIDS#HIV response#Fear of prosecution#postcard#protect everyone's rights#protect everyone's health
0 notes
Text

shiv having her husband in her contacts as FirstName LastName with no photo of him, so an incoming call from him would just look like a call from any other random contact...but then also having him set up as her Emergency Contact in her phone's Medical ID profile...shiv thesis.
#shiv roy#tomshiv#succession#succession spoilers#succession s4#the attention to detail the succession set dressers and prop masters put into this show never fails to impress me#also some context for folks who don't use apple products: the red 'Emergency Contact' text under tom's name on this contact card#will ONLY show up if you have that person designated as your emergency contact in your Medical ID profile on your phone's Health app#which is also where you can designate your organ donor status your blood type and any allergies you might have#the purpose of this being that if you are ever in an accident or incapacitated but your phone is still on you#emergency services can access your Medical ID from your phone's lock screen and get information that may be crucial to saving your life#as well as providing them a built in person to call to alert them of your condition#and potentially ask further health-related questions of#anyway. the fact that shiv has SUCH an impersonal contact card for tom - lacking even a contact photo for him#but still has him listed under her medical id as the person to call for her in an emergency#is just...truly a shiv thesis statement for me
188 notes
·
View notes
Text
Girl (Tyler Robert Joseph) if I don't get this job this week AND the Paladin MV still isn't out, I'm gonna **** **** * ******* ****** *** * **** ***** ****** ****
#i need one. job is the vastly preferred option but the paladin mv will console me if i dont get it#i barely slept im so stressed about this 🥲 there's a couple co workers im really convinced will get it over me#and if they do ill be happy for them but like. i need. a job that pays enough that i can pay for health insurance.#or a job that comes with health insurance benefits already but that's less feasible rn for a lot of reasons#i have a bit more time before im kicked off my parents and it becomes actually urgent but augh#isnt it so cool that the us healthcare system wholly depends on your income / job to even access services you#require in order to Not Die or at the very least to maintain the aforementioned job you need to afford access. ha ha.#i know there's medicaid and stuff but im pretty sure that would not cover enough of the medication and blood panels i need#like i need private health insurance. unfortunately#this is too real for the silly ohio band blog sorry but im uhhhh a mess ive been anticipating this position for months#and i want it very very very badly :').
9 notes
·
View notes
Text
No one is entitled to biological offspring and how can they include surrogacy in the Act without implying that couples are entitled to women to be surrogates?
A trio of Democratic senators are introducing a "Right to IVF Act" that would, among other things, force private health insurance plans to cover assisted reproduction treatments such as in vitro fertilization (IVF), egg freezing, and gestational surrogacy.
The measure provides no exception or accommodations for religious objections, all but ensuring massive legal battles over the mandate should it pass.
The "sweeping legislative package" (as the senators describe it) combines several existing pieces of legislation, including the Access to Family Building Act and the Family Building Federal Employees Health Benefit Fairness Act sponsored by Sen. Tammy Duckworth (D–Ill.), the Veteran Families Health Services Act from Sen. Patty Murray (D–Wash.), and the Access to Infertility Treatment and Care Act from Sen. Cory Booker (D–N.J.).
Booker's contribution here is probably the most controversial. It requires coverage for assisted reproduction from any health care plan that covers obstetric services.
A Reverse Contraception Mandate
Remember the Affordable Care Act's contraception mandate, which required private health insurance plans to cover birth control (allegedly) at no cost to plan participants? It spawned some big legal battles over the rights of religious employers and institutions not to offer staff health plans that included birth control coverage.
Booker's Access to Infertility Treatment and Care Act is a lot like the Obamacare contraception mandate, except instead of requiring health care plans to cover the costs of avoiding pregnancy it would require them to cover treatments to help people become pregnant.
The bill states that all group health plans or health insurance issuers offering group or individual health insurance must cover assisted reproduction and fertility preservation treatments if they cover any obstetric services. It defines assisted reproductive technology as "treatments or procedures that involve the handling of human egg, sperm, and embryo outside of the body with the intent of facilitating a pregnancy, including in vitro fertilization, egg, embryo, or sperm cryopreservation, egg or embryo donation, and gestational surrogacy."
Health insurance plans could only require participant cost-sharing (in the form of co-pays, deductibles, etc.) for such services to the same extent that they require cost-sharing for similar services.
What Could Go Wrong?
It seems like it should go without saying by now but there is no such thing as government-mandated healthcare savings. Authorities can order health care plans to cover IVF (or contraception or whatever) and cap point-of-service costs for plan participants, but health insurers will inevitably pass these costs on to consumers in other ways—leading to higher insurance premiums overall or other health care cost increases.
Yes, IVF and other fertility procedures are expensive. But a mandate like this could actually risk raising IVF costs.
When a lot of people are paying out of pocket for fertility treatments, medical professionals have an incentive to keep costs affordable in order to attract patients. If everyone's insurance covers IVF and patients needn't bother with comparing costs or weighing costs versus benefits, there's nothing to stop medical providers from raising prices greatly. We'll see the same cost inflation we've seen in other sectors of the U.S. healthcare marketplace—a situation that not only balloons health care spending generally (and gets passed on to consumers one way or another) but makes fertility treatments out of reach for people who don't have insurance that covers such treatments.
Raising costs isn't the only issue here, of course. There's the matter of more government intervention in private markets (something some of us are still wild-eyed enough to oppose!).
Offering employee health care plans that cover IVF could be a good selling point for recruiting potential employees or keeping existing employees happy. But there's no reason that every employer should have to do so, just because lawmakers want IVF to be more accessible.
It's unfair to employers—big or small, religious or non-religious—to say they all must take on the costs of offering health care plans that cover pricey fertility treatments. And Booker's bill contains no exceptions for small businesses or for entities with religious or ethical objections.
A lot of religious people are morally opposed to things like IVF and surrogacy. This measure would force religious employers to subsidize and tacitly condone these things if they wanted to offer employees health care plans with any obstetrics coverage at all.
As with any government intervention in free markets, there's the possibility that this fertility treatment mandate would distort incentives. IVF can certainly be an invaluable tool for folks experiencing infertility. But it's also very expensive and very taxing—emotionally and physically—for the women undergoing it, with far from universal success rates. The new mandate could encourage people who may not be good candidates for IVF to keep trying it, perhaps nudging them away from other options (like adoption) that might be better suited to their circumstances.
'Access' Vs. Whatever This Is
Since Roe v. Wade was overturned, many Americans have worried that the legal regime change would pave the way for outlawing things like contraception or IVF, too. Encoding into law (or legal precedent) the idea that fertilized eggs are people could have negative implications for these things, even if many conservative politicians pledge (and demonstrate) that IVF and birth control are safe. In response, some progressive politicians—perhaps genuinely concerned, perhaps sensing political opportunity (or why not both?)—have started talking a lot about the need to protect access to IVF across the country.
As much as I agree with this goal, I think IVF's legality is better off as a state-by-state matter. That said, the "protect IVF nationwide" impulse wouldn't be so bad if "protecting access" simply meant making sure that the procedure was legal.
But as we've seen again and again over the past couple decades, Democrats tend to define health care and medicine "access" differently.
The new Right to IVF Act would establish a national right to provide or receive assisted reproduction services. In their press release, the senators say this last bit would "pre-empt any state effort to limit such access and ensur[e] no hopeful parent—or their doctors—are punished for trying to start or grow a family." OK.
But that's not all it would do. The bill's text states that "an individual has a statutory right under this Act, including without prohibition or unreasonable limitation or interference (such as due to financial cost or detriment to the individual's health, including mental health), to—(A) access assisted reproductive technology; (B) continue or complete an ongoing assisted reproductive technology treatment or procedure pursuant to a written plan or agreement with a health care provider; and (C) retain all rights regarding the use or disposition of reproductive genetic materials, including gametes."
Note that bit about financial cost. It's kind of confusingly worded and it's unclear exactly what that would mean in practice. But it could give the government leeway to directly intervene if they think IVF is broadly unaffordable or to place more demands on individual health care facilities, providers, insurance plans, etc., to help cover the costs of IVF for people whom it would otherwise be financially out of reach.
This is the distilled essence of how Democrats go too far on issues like this. They're not content to say "People shouldn't be punished for utilizing/offering IVF" or that the practice shouldn't be illegal. They look at authoritarian or overreaching possibilities from the other side (like banning or criminalizing IVF) and respond with overreaching proposals of their own.
The proble with increasing access to IVF is what happens when the couple needs a surrogate to have biological offspring? Will they beg and pester the women in their lives? Will the affordable IVF compensate surrogates fairly?
#usa#Right to IVF Act#Democratic making it easier to exploit women#Anti surrogacy#the Access to Family Building Act#the Family Building Federal Employees Health Benefit Fairness Act#Sen. Tammy Duckworth (D–Ill.)#the Veteran Families Health Services Act#Sen. Patty Murray (D–Wash.)#the Access to Infertility Treatment and Care Act#Sen. Cory Booker (D–N.J.).
9 notes
·
View notes
Text
We’ve really enjoyed this past week. Hubbins finished his 5 year apprenticeship so he took a week off to find a better paying job (Which he did! Yay!) We loved having him around all day every day and we’ve been able to do a lot with his help.

We had a great evaluation with the behavior consultant Saturday. She is very good at what she does and is heavily involved. I love being able to text her regularly to give her updates and discuss what subtle things I can adjust to make our training more effective. Our main goal is to overcome the dog-dog resource guarding by 2025 but before we can tackle that we are going to work on the “stressing up / attention seeking” behaviors that we’ve struggled with for so long. I pulled Mandana from public access & the training center temporarily so we can focus solely on this. We’ve spent this past week doing training exercises several times a day and we’re making progress.

Today: We went to hike a spot we haven’t been to as a family since she was an adolescent. We had a lot of fun. Mandana is tick-free, bathed/dry & napping. My Rheumatologist is working on getting the next DMARD pre-approved (otherwise it’s $1800/wk 😱) Wednesday I have an ENT apt to discuss possible vocal cord dysfunction. Saturday the behavior consultant is coming over to check on our progress and Sunday is swimming at the Sniffspot pond!


Exhausted from hiking & training :)
#belgian malinois#4 years#service dog in training#service dogblr#dogblr#life update#hubbins#health update#public access training#training update
9 notes
·
View notes
Text
if you are 1) currently in a university where your student healthcare covers hormone therapy, and 2) in a good financial, emotional, and social position to start hormone therapy, i would recommend pursuing it. because in my experience, it's a huge pain in the ass to get an endocrinologist once you're on your own
#unless you live near a planned parenthood or another equivalent to that#but in general you might as well take advantage of the mandatory student health insurance while you have it#it's also cheaper than you might expect. my vials cost $40 CAD for 4 months and then the injection materials are like a couple dollars each#for me i got a therapist with the university and asked them to recommend me to one of the uni's doctors#so i got to skip some of the waitlisting process yay#and then even after getting access to hormones i went to the clinic maybe 5 or 6 times because i needed a nurse to help me with injections#all of which was 'free' because it was with the university#now that i'm graduated though i need to find a new endocrinologist and it turns out the process is WAY more complicated on your own 🤡#of course your mileage may vary depending on how based your school is but it's definitely worth checking imo 🤷#beepbeep.txt#wanted to say this because i basically didn't use the uni health services until my last year and i was like 'wow#'i'm actually getting so much shit for free right now'#like i was seeing a therapist and a dietician and the endocrinologist and a nurse simultaneously at one point#and i might've missed out on all that if i didn't have someone tell me how easy it was to get help if you ask the right questions#so there's my word of wisdom for anyone who might benefit from it.......#also going to post tips about injections later because i think that would also help people out 👍
27 notes
·
View notes
Text
Recently, I saw a post about how it's good to leave the house every once in a while and get fresh air, and it got me thinking. Because yup, fresh air is great, it can be shitty for mental health if you're cooped up a lot, if you don't change your scenery!
But: that last part made me think about my experience as a kid, and I'm sad about it. When I was a kid, I was in a suburban neighborhood. Technically, I could leave the house and go for walks and get fresh air anytime I wanted. But it was awful for me, and how my mind worked!
I couldn't possibly walk to anything, because the nearest amenity was a 7/11, and it was like an hour-long walk there and back. So the whole idea of walking felt meaningless, unsatisfying. And there were no sidewalks, so I stressed out abt having to use the same road that people drove their vehicles on (and in this day and age, nobody pays attention on the road, so yikes). There were no distinguishing 'landmarks' to help me keep track of where I was, not even any trees, just cookie cutter houses and lawns and very same-y roads, so I always got lost (yep lol, in my own neighborhood!). Maybe I was getting fresh air, but the process made me feel dumb and lonely and confused.
I was basically walking around, day in and day out, in some empty liminal space where all the houses looked the same, where I could walk for literal hours and never feel like I was going anywhere, like I was on a treadmill, and it kinda messed with me. We didn't even have a park nearby. It was literally just this. Day in and day out. Nothing ever changed. There were no events or anything, nothing to look forward to, past putting on some new music on headphones. I barely saw another person. When I did see someone, they were always in a car, trying to get out of the neighborhood to go somewhere that was actually interesting and not mind-numbingly empty!

It was super shitty. Yep, it got me out of the house which was good, but it could've been so much better if there had just been. A freakin park, or a place to gather and actually see other people (these are called 'third places' and suburbs, like, never have them!). Even if I didn't need to talk to anyone, and I just wanted to people-watch, I would've loved something like that. Alas, there was no chance for spontaneous interactions, or for fun, interesting things to happen, which I think is super super underrated, and a big part of 'getting out of the house' as a complete package.
Gonna link to a Vox article, bc I thought it was really insightful:
How our housing choices make adult friendships more difficult - Vox
#i remember talking to someone w low vision and they found it super shitty too bc they couldn't drive#so they had to rely on someone else to drive them everywhere outside of the suburb (ie anywhere interesting)#bc there weren't even any buses in service in the area which they might have been able to take themselves#i think the word they used was 'degrading'#third places#third place#neighborhoods#car dependence#urban planning#mental health#self care#vox#accessibility
37 notes
·
View notes
Text
Psychiatry Washington DC | Access Health Services
Access Health Services is a trusted provider of Psychiatric Treatments in Washington DC that can reduce symptoms of mental health disorders and associated complications. A psychiatric diagnosis is different – there are often no physical symptoms, nor are there any biological tests conclusive for mental distress. Although tests can be important to rule out underlying physical causes, a health professional making a psychiatric diagnosis has to rely on a person’s own description of their thoughts and feelings, alongside observations of their behaviour. visit us - https://www.accesshealthservices.org/psychiatric/
#access health services#access health care services#Mental Health Clinic Dc#access health services dc#access health and wellness
0 notes
Text
A national physician group this week called for the complete termination of a Medicare privatization scheme that the Biden White House inherited from the Trump administration and later rebranded—while keeping intact its most dangerous components.
Now known as the Accountable Care Organization Realizing Equity, Access, and Community Health (ACO REACH) Model, the experiment inserts a for-profit entity between traditional Medicare beneficiaries and healthcare providers. The federal government pays the ACO REACH middlemen to cover patients' care while allowing them to pocket a significant chunk of the fee as profit.
The rebranded pilot program, which was launched without congressional approval and is set to run through at least 2026, officially began this month, and progressive healthcare advocates fear the experiment could be allowed to engulf traditional Medicare.
In a Tuesday letter to Health and Human Services Secretary Xavier Becerra and Centers for Medicare and Medicaid Services Administrator Chiquita Brooks-LaSure, Physicians for a National Health Program (PNHP) argued that ACO REACH "presents a threat to the integrity of traditional Medicare, and an opportunity for corporations to take money from taxpayers while denying care to beneficiaries."
The group, which advocates for a single-payer healthcare system, voiced alarm over the Biden administration's decision to let companies with records of fraud and other abuses take part in the ACO REACH pilot, which automatically assigns traditional Medicare patients to private entities without their consent.
CMS said in a press release Tuesday that "the ACO REACH Model has 132 ACOs with 131,772 healthcare providers and organizations providing care to an estimated 2.1 million beneficiaries" for 2023.
"As we have stated, PNHP believes that the REACH program threatens the integrity of traditional Medicare and should be permanently ended," Dr. Philip Verhoef, the physician group's president, wrote in the new letter. "Whether or not one agrees with this statement, we should all be able to agree that companies found to have violated the rules have no place managing the care of our Medicare beneficiaries."
Among the concerning examples PNHP cited was Clover Health, which has operated so-called Direct Contracting Entities (DCEs)—the name of private middlemen under the Trump-era version of the Medicare pilot—in more than a dozen states, including Arizona, Florida, Georgia, and New York.
PNHP noted that in 2016, CMS fined Clover—a large Medicare Advantage provider—for "using 'marketing and advertising materials that contained inaccurate statements' about coverage for out-of-network providers, after a high volume of complaints from patients who were denied coverage by its MA plan. Clover had failed to correct the materials after repeated requests by CMS."
Humana, another large insurer with its teeth in the Medicare privatization pilot, "improperly collected almost $200 million from Medicare by overstating the sickness of patients," PNHP observed, citing a recent federal audit.
"It appears that in its selection process [for ACO REACH], CMS did not prevent the inclusion of companies with histories of such behavior," Verhoef wrote. "Given these findings, we are concerned that CMS is inappropriately allowing these DCEs to continue unimpeded into ACO REACH in 2023."

While the Medicare pilot garnered little attention from lawmakers when the Trump administration first launched it during its final months in power, progressive members of Congress have recently ramped up scrutiny of the program.
Last month, Sen. Elizabeth Warren (D-Mass.) and Rep. Pramila Jayapal (D-Wash.) led a group of lawmakers in warning that ACO REACH "provides an opportunity for healthcare insurers with a history of defrauding and abusing Medicare and ripping off taxpayers to further encroach on the Medicare system."
"We have long been concerned about ensuring this model does not give corporate profiteers yet another opportunity to take a chunk out of traditional Medicare," the lawmakers wrote, echoing PNHP's concerns. "The continued participation of corporate actors with a history of fraud and abuse threatens the integrity of the program."
#us politics#news#2023#common dreams#medicare#trump administration#biden administration#Accountable Care Organization Realizing Equity Access and Community Health model#department of health and human services#Xavier Becerra#Chiquita Brooks-LaSure#Physicians for a National Health Program#Centers for Medicare and Medicaid Services#Dr. Philip Verhoef#Direct Contracting Entities#Medicare Advantage#sen. elizabeth warren#Rep. Pramila Jayapal#medicare for all#us healthcare#us health insurance
95 notes
·
View notes
Text
Keep seeing that super American-worded poll about 'when did you move to this country' and thinking about reblogging with tags like......technically I didn't move countries. Technically I also did. Technically my family has been here for many generations. But they were also over there when over there was here and when that wasn't a border, and then again over there when it was. Some of them came from the same country but before that fled another one that was one thing then and isn't now. What do you mean 'country' what do you mean 'move'? We've always been children of the border in this family.
#just coz i keep seeing it in the wake of reading a post katherine reblogged about modern progressive concepts of land and identity#and it's making my head and my heart sore#border kid#also whenever i see: what would we lose by leaving x and uniting with y??#i'm very clear on this: a free at the point of access health service. overnight my t1d husband's life would get a hell of a lot more complex#so can we think about some practicalities before?#and also to be explicit: i'm fine with being a border kid. i think maybe our definition of home could do with being more flexible
10 notes
·
View notes
Text
the fancy pants guy at my psych clinic had a fancy shirt on last time i went and it was a delight to see him as always
#It Speaks#i think hes a peer support specialist which is just someone who also gets treatment but is further along than you by their metric#basically a friend with psychiatric benefitsdskghskfgh#they have this thing called the wraparound approach which is like. intensive. but honestly i think its useful they just.#nobody read the room that i was too autistic to do my appointments in a fucking CUBICLE space#so ive been going to telehealth for appointments with people who dont have offices#its helped my ability to understand whats going on immensely#i reccomend checking into it for anyone who is struggling with sensory overload in mental health spaces bc this should be a full time optio#fingers cross ours miiiiiiiight have a program to sign up for a tablet with service so if the internet goes out i can still keep up#not hinging all my bets but its a possibility like the bus service thing im going to ask about and am writing in my book rn#i am going to access these services that are allowed to me for my problems even if it kills me
6 notes
·
View notes
Text

Lesbian World Volume 1 , Issue 1. Sep, 1992
#garlic speaks#queer history#this was published in euclid ohio#its reprinted from the lyon-martin womens health services access newsletter#from san francisco
54 notes
·
View notes
Text
A teen girl with mental health issues who expressed a desire to transition was removed from her family who wanted to try treating the mental health issues before transitioning was romeved from her home by the state’s child protective services and is now in Canada?
By Anna Slatz. January 29, 2024
A family in Glasgow, Montana is accusing the state’s child protective services of “kidnapping” their teenage daughter after the girl began to identify as a transgender “boy.” Krista and Todd Kolstad spoke to Reduxx about their ordeal, revealing that the child had been removed from their care and was now going to be sent to Canada.
Krista, the child’s step-mother, explains that their nightmare began in August of 2023 after they received a call that their 14-year-old daughter, Jennifer*, had expressed suicidal ideations while at school.
“She had always had problems at school,” Krista says, noting that she and Todd had even pulled her from one district and sent her to another due to issues with bullying in an effort to give her a fresh start. But despite experiencing some real-world hardships, Krista claims Jennifer also had some undiagnosed mental health concerns, including attention-seeking behavior.
Later on that same evening, a case worker with Montana Child and Family Services (CFS) showed up to the Kolstad home to speak with Jennifer and do an inspection. Krista had been preparing dinner at the time, and invited the case worker to tour the residence despite both her and her husband being distressed by the sudden appearance.

Todd, Krista, and Jennifer in a Christmas photo. SOURCE: Supplied.
During the interview with CFS, Jennifer claimed to have consumed toilet bowl cleaner and painkiller medications that day in an effort to commit suicide. Krista says that it had immediately struck her as being highly unlikely, as not only did Jennifer not have access to either substance unmonitored, but that Jennifer had expressed no symptoms of imminent illness that day.
Despite their doubts about the veracity of Jennifer’s claims, Krista and Todd agreed to take Jennifer to the local hospital on an emergency basis. While there, blood work returned that Jennifer had not consumed any toxic substances.
Krista and Todd provided Reduxx with copies of Jennifer’s medical paperwork to substantiate their claim that Jennifer had not consumed any dangerous substances the day she was admitted to hospital. The paperwork confirms that there were no abnormalities detected in Jennifer’s system, and that her overall physical health was good.
But notes taken at the hospital consistently mention that Jennifer identifies as a “male” and wishes to be called “Leo.”
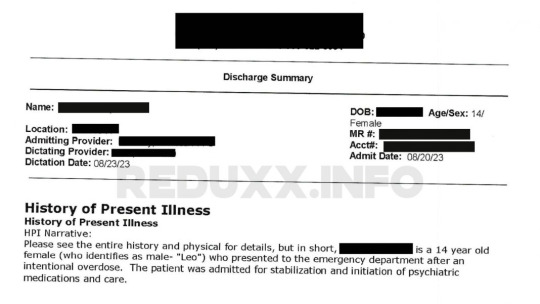
From the hospital documents. SOURCE: Provided.
Krista says she and Todd immediately made their objections known to Hospital staff, requesting Jennifer be called by her birth name.
“We were very clear to the emergency room staff as well as [CFS] that this goes against our values, morals, and our religious beliefs,” she said, but hospital staff refused to listen. “They told me to call their lawyer if I have an issue as they will do what the patient tells them.”
While the medical transitioning of minors was prohibited in the state of Montana at the time, Krista says the hospital told her that “social transitioning” was a “grey area” and continued to call Jennifer “Leo” and refer to her as a boy.
As a patient admitted for suicidal ideations, Jennifer was placed on 24/7 watch to keep her safe. But Krista says an aide was placed outside of her door who would regularly talk to Jennifer about “gender affirming” care.
“I came one day and she was talking about having top-surgery and being non-binary,” Krista says of the aide. She took her complaint to the on-duty Doctor, who dismissed her. “He told me, ‘why are not you more concerned that your daughter is trying to harm herself, then what [the aide] is talking about?'”
Another aide who had been set to watch over Jennifer similarly chastised Krista, telling her to “respect” Jennifer’s wishes to be called “Leo.”
Krista describes Jennifer’s time in the hospital as a period of constant efforts to undermine her and Todd’s parental authority. In addition to not respecting their wishes to refer to Jennifer by her birth name, hospital staff refused to abide by any other requests, such as limiting Jennifer’s TV and phone time, encouraging her to do her school work, and not allowing her to have copious amounts of junk food.
During this time, Krista and Todd had communication with Child and Family Services, and all agreed that Jennifer would benefit from specialized residential care for treatment and counseling. But during a conversation about where Jennifer could be placed, Krista says the possibility of her being moved to Wyoming was presented.

Jennifer and Todd. SOURCE: Provided
“They told us that there were 6 facilities in Montana, but that there was also a facility in Wyoming. And at that point, because we were already in such a state from the hospital disrespecting us and our wishes, we immediately looked up Wyoming’s laws on transitioning minors,” Krista says. “It looked to us like kids could go ahead and have procedures done and have hormones without parental consent.”
Concern began to set in, but Krista and Todd were assured that the most likely scenario was Jennifer being placed in a Montana-based facility, and on August 22, Krista and Todd were told that Jennifer was next in line for a bed in Billings, Montana.
But hours later that same day, Krista and Todd were called and informed Jennifer would be moved to Wyoming.
“They called and told us that a bed had opened up in Wyoming and that Jennifer needed to go. [The Doctor] said ‘she has to go. she’s not doing any good here,’ and we were really blown away,” Krista recounts. “No one talked to us about the the name of the facility — we had no one to answer our questions. We told them we wanted our questions answered before we accepted the bed.”
Ten minutes later, Child and Family Services arrived at the Kolstad residence with police.
“They showed up at our home to serve us with papers to take Jennifer out of our care,” Krista says. “They told me the reason was that we were ‘unable or refusing to provide medical care.’ That’s just not true.”
The next day, August 23, Jennifer was transported to Wyoming. Despite the fact that Krista and Todd were not allowed to see Jennifer during her move, CFS did allow Jennifer to stop and see friends and co-workers prior to leaving the city. Krista would later find out that Jennifer had told her friends that she was “crazy and trying to kill herself” and was being taken away from her parents.
“I feel this was a lapse in judgement by [CFS], a violation of HIPAA, and a miscarriage to Jennifer, as she is only 14. What if, when she is 17, this incident is behind her and she is in a good place mentally? This is a very small town and they have just let her brand herself as the ‘crazy kid’ who tried to kill themselves.”
While Jennifer was in Wyoming, neither Krista nor Todd were allowed to speak with her directly. Instead, they had to go through Jennifer’s counsellor, but Krista says they were very reluctant to give her information.
Krista later had to request Jennifer’s records from the center in order to get an understanding of what had happened to her while she was at the facility.
A letter sent by Krista to CFS expressing dismay at the situation and offering Jennifer clothes and comfort items. SOURCE: Provided.
On September 25, Jennifer was returned to Montana and placed in a Youth Dynamics group home where she has remained ever since.
“They called it ‘temporary legal custody,’ which means they have the say over where she is at, but we are supposed to be able to have the say over everything else. But that was not upheld. There were incidents of her getting vaccines we did not consent to, we were not told the name of the Doctors involved, and she was allowed to shave her head,” Krista says.
Since Jennifer returned to Montana, Krista and Todd have had monthly court meetings along with Child and Family Services to determine next steps. The couple was assigned a public defender, who simply encouraged them to keep their head down until the process was complete.
“I am not trying to throw them under the bus… but all of their advice has been ‘play nice, just let her finish the group home program and then get her back in your care and move on with your lives.'”
But while the group home placement should have been just 6-9 months, the family’s situation took a dramatic turn for the worse during their hearing on January 19, 2024, when the court decided to hand custody of Jennifer over to Child and Family Services.
“We were told that letting Jennifer transition and live as a boy was in her ‘therapeutic best interest’ and because we aren’t willing to follow that recommendation, the court gave CFS custody of Jennifer for six months,” Krista says. “CFS is now going to place Jennifer in the care of her birth mother in Canada, who has never really been apart of her life. The judge said to us ‘you need to expect that reunification with your family may not be what you are expecting.'”

Krista and Jennifer. SOURCE: Supplied.
Jennifer’s birth mother, Christine, currently lives in Kitchener, Ontario with her new husband. After Jennifer was born, Christine reportedly left the child with Todd, and has never been involved in her care since.
“She’s never called to see how [Jennifer] is. She’s never sent her anything. Nothing,” Krista says.
According to Krista, any communication from Christine at all has been sparse, and she has never made a meaningful effort to have a relationship with the children she left in Montana. Despite her apparent lack of interest, Krista has been sending Christine semi-regular updates on all of her children for the past seven years.
But disturbingly, Krista explains that she and Todd have grave concerns about Christine’s fitness as a parent.
“I have this letter from one of Jennifer’s previous counsellors that recommends that if Christine wants to come back into her children’s lives, she should do unification therapy, there should be trial visits… all of this stuff should happen because the children reported her as being abusive,” Krista says.
Krista and Todd provided Reduxx with a copy of a statement from a licensed professional counselor detailing sessions that Jennifer and her sister had attended. Both girls described Christine as being uncaring, abusive, and even “crazy.”
In one section of the statement, the counselor describes one of the girls as witnessing “incidents of violence directed at an older sibling,” which involved Christine “throwing that sibling against the refrigerator after becoming enraged at her” for wearing her mother’s jewelry without permission. The child goes on to detail “incidents when her biological mother would punch, hit, slap, and kick her and her siblings.”

An excerpt from the counseling report reviewed by Reduxx. SOURCE: Provided.
Jennifer similarly alleged disturbing cases of abuse by her biological mother, including one time Christine reportedly grabbed and held her around her waist while repeatedly slapping her in the face.
Of the five children Christine and Todd had together, only one had lived in Canada with Christine prior to aging out of her care. While living with Christine, the boy exhibited severe behavioral problems to a point where Christine approached Krista and Todd for help.
In one conversation, Christine admits to regularly checking homeless encampments and police records in anticipation she would one day find her son in jail.
Child and Family Services was provided both the counselor’s statement and the text messages, but Krista said that nothing could be done to intervene in Jennifer’s placement.
“Our family has been destroyed by this. We have little to no contact with Jennifer and our rights as her parents have been trampled on,” Krista says. But despite the turmoil that has been brought into their lives, the couple says they will never stop trying to help their daughter come home.
Krista and Todd chose to defy a judge’s order to remain silent on the case in order to tell their story. They were set to appear in court today to respond to charges of contempt, but have had to delay the hearing due to a family emergency.
“We will continue to fight. We will never give up on our daughter and for what we believe is morally right. We will continue to tell our story, even though we are currently in contempt of court, and try to keep other families from going through this. Our greatest fear is that our daughter is now going to become a victim of this system and eventually take her own life.”
While Krista has expressed fear that the family’s legal avenues are limited, she has said that they intend to find any means they can against Montana Child and Family Services as well as the hospital where Jennifer was treated.
“I will also be looking at if we have a case against Youth Dynamics Group Home for socially transitioning our daughter against our wishes,” Krista says. “This is NOT about money, this is about standing up and telling our story so this does not happen to another family. We will fight to save our daughter no matter what it costs us financially or emotionally. That’s what parents do for their children.”
*The child’s name has been changed at the request of her parents.
#usa#montana#Glasgow#Montana Child and Family Services (CFS)#The link between mental health issues and gender dysphoria#The kid lied to CPS about consuming dangerous substances#Hospital staff allowed a mentally fragile teen unlimited access to TV and her phone?#While not monitoring her diet?#And not encouraging her to catch up on homework?#The kid is going to be sent to live in Canada with a biological mother who she barely knows?#And the bio mother was abusive?#Youth Dynamics Group Home
5 notes
·
View notes
Text

Just finished my Pulmonologist Apt. Lung function is normal but she agrees we might not have caught an episode if it’s transient. Unfortunately, she can’t prescribe me anything until it shows up on their tests. She’s sending me a one-night sleep apnea test bc that’s all they have to test for things at home and said I can stop by whenever I’m feeling symptomatic and they can try to test it spontaneously.
She also brought up abdominal aortic issues that can be caused by EDS which was a surprising coincidence considering I just went to urgent care for new symptoms that would correlate with that. Urgent Care thought it was related to my gastroparesis so I scheduled a GI apt but the Pulmonologist thinks I should talk to my Cardiologist about it.
She believes me. Even if my oxymeter isn’t accurate there’s no reason it should be completely normal for my husband & crazy for me. I just gotta catch it on their tests before they can do anything about it.
Mandana was better in some ways and worse in others. I seem to be narrowing it down to a particular situation that gets her worked up. She’s completely fine in the waiting room even when I walk away (I did training there before and after the apt). In the exam room she wants to be all up in my lap which is unacceptable. She needs to just lay down & chill while they examine me. It seems like maybe she’s carrying over some of the stress from previous vet appointments. She’s completely fine at her usual vet but she acts like she does when we took her to the dentist or the university vet & had to leave her for emergencies. I’m not sure how to train for that besides just generalizing her mat/settle and going to a lot of boring appointments. It might work out for the best anyways. If the sleep apnea test doesn’t catch anything I could go to the hospital regularly for training and if I start flaring up they could test me.

Focused & alerting in the waiting room. She alerted in the exam room too but she was way too worked up. Advice welcome 😕
Besides all that, I asked if it could be Lupus related and she said no because we would see way more damage before it started affecting my blood oxygen levels. The only thing that showed up was my chest X-ray showed mild hyperinflation which was weird but she didn’t know what it could mean in relation to everything else and didn’t think it was related to my symptoms. I wanted to ask about the Lupus because my Rheumatology apt is next week and I’m trying to stay on top of all the questions I need to be asking each specialist.

#belgian malinois#3 years#service dog in training#service dog training#service dogblr#positive reinforcement#medical alert service dog#medical alert#doctors appointment#pulmonologist#health flare#public access#public access training
22 notes
·
View notes
Text
Finally working as a social worker in the field and yeah we're cops too. We're churning ppl thru the system too. Most fucked up thing is my job is considered a "mental health" agency and we're supposed to prioritize linking ppl to mental health resources... whole time like 95% of our clients are homeless and utilize us primarily for a hotel stay. These ppl are worrying about where they're gonna get their next meal, what's going to happen to them after their hotel stay runs out. I have clients who are single mothers on the verge of homelessness and I'm supposed to ask "how do you feel about outpatient counseling? Psychiatry? Mental health skill building?" It's fucked.
#it's a systemic issue for sure and i do my best to go against management when i can#and yeah there are clients who do need mental health resources. but if their homelessness is the root CAUSE of their mental health status-#-its just putting a band aid over a massive open wound#i'm realizing crisis stabilization as a concept is just fucked bc it assumes clients are in the best possible circumstance aside from their-#-mental health. assuming ppl have the income to utilize additional services. the transportation to access them#this company i work for is so evil anyway. they're trying to make our nurses 1099 now after hiring them on full time
2 notes
·
View notes
Last Seen Blogs

quickfixkitchen
Untitled

nebowskii
very cool blog, would recomend

korecowshop
korecow shop blog

korebu
KOREBU

shiftingaround
nira 💫