#posterosuperior
Text
Sexy Jerk off instruction from russian pornostar
Super cute skinny blonde gets oiled up and fucked hard by huge cock (Kiera Cole)
young wife bbc cuckold
He Wants Her Tight And Wet Pussy Right Now Right Here, At The Public Beach
Desi stepsister fucked by her stepbrother in park behn ki park me chudai
Hot ebony teen punish fucked on CCTV after shoplifting
Dude spying tranny in bubble bath
Submissive whore blow job
Crystal Westbrooks creamy wet pussy
TeenyBlack Skinny naturally busty ebony teen fucked
#reassortments#estherian#bodgie#serradella#snow-dropping#metaclase#Deino#co-afforest#Delphina#posterosuperior#nonculpable#renvoi#erudit#arche#pot-liquor#grassnut#Cazenovia#arenites#Pitney#confidants
0 notes
Photo

Dzimumlocekļa sakne (radix): tā ir pievienotā daļa, kas sastāv no // https://t.co/kXexVOPkTO /// dzimumlocekļa spuldze vidū un dzimumlocekļa kruss, viens abās spuldzes pusēs. Tas atrodas virspusējā starpsienas maisiņā.
Dzimumlocekļa ķermenis (korpuss): Tam ir divas virsmas: muguras (posterosuperior uzceltā dzimumloceklī) un vēdera vai urīnizvadkanāla (pavirša dzimumloceklī vērsta uz leju un atpakaļ). Ventrālā virsma ir iezīmēta ar rievu sānu virzienā.
Epitēlijs dzimumlocekļa sastāv no vārpstas āda, priekšādiņa un priekšgala gļotāda priekšādiņas iekšpusē un pārklājot dzimumlocekļa dzimumloceklis. Epitēlijs nav piestiprināts pie pamata vārpstas, tāpēc tas var brīvi slīdēt turp un atpakaļ.[5]
Struktūra
Cilvēka dzimumloceklis sastāv no trim kolonnām audi: divi corpora cavernosa gulēt blakus viens otram muguras puse un viens corpus spongiosum atrodas starp tām uz ventrālā puse.[6]
Spongiosum korpusa paplašinātais un sīpolu formas gals veido dzimumlocekļa dzimumloceklis ar diviem specifiskiem sinusoīdu veidiem, kas atbalsta priekšādiņa vai prepuce, vaļīga ādas kroka, kas pieaugušajiem var ievilkties, lai atklātu dzimumlocekli.[7] Vietu dzimumlocekļa apakšpusē, kur piestiprināta priekšādiņa, sauc par frenum vai frenulum. Noapaļoto dzimumlocekļa pamatni sauc par vainags. The starpsienu raphe ir pamanāma līnija dzimumlocekļa apakšpusē.
Cilvēka dzimumlocekļa anatomiskā shēma
The urīnizvadkanāla, kas ir urīnceļi, šķērso corpus spongiosum, un tā atvere, kas pazīstama kā gaļa /miːˈeɪtəs/, atrodas uz dzimumlocekļa dzimumlocekļa gala. Tas ir fragments abiem urīns un par ejakulācija gada sperma. Sperma tiek ražoti sēklinieki un glabājas pievienotajā epididymis. Ejakulācijas laikā spermu dzen uz augšu vas deferens, divi kanāli, kas iet pāri un aiz urīnpūšļa. Šķidrumus pievieno sēklas pūslīši un vas deferens pārvēršas par ejakulācijas kanāli, kas pievienojas urīnizvadkanālam iekšpusē prostatas dziedzeris. Prostatas, kā arī bulbourethral dziedzeri pievieno vēl sekrēcijas, un sperma tiek izvadīta caur dzimumlocekli.
The raphe ir redzamā grēda starp sānu dzimumlocekļa puses, kas atrodas dzimumlocekļa vēderā vai apakšpusē, ejot no gaļas (urīnizvadkanāla atveres) pāri sēklinieku maisiņš uz starpenē (laukums starp sēklinieku maisiņu un tūpļa ).
Cilvēka dzimumloceklis atšķiras no citiem zīdītājiem, tā kā tam nav baculum (vai erektilais kauls), un tā vietā pilnībā paļaujas uz asinīm, lai tās sasniegtu uzcelt stāvokli. Distālā saite balstās uz dzimumlocekļa dzimumlocekļa un spēlē neatņemamu lomu dzimumlocekļa fibroskeletonā, un struktūru sauc par "os analog" - terminu, ko izdomāja Geng Long Hsu reprodukcijas enciklopēdijā.[9] Tas ir paliekas baculum attīstījās, iespējams, mainoties pārošanās praksē.[10]
Cilvēka dzimumlocekli nevar izvilkt cirkšņā, un tas ir lielāks nekā vidēji dzīvnieku valstī proporcionāli ķermeņa masa. Cilvēka dzimumloceklis pārvietojas no mīkstas kokvilnas līdz kaulainai stingrībai, ko izraisa dzimumlocekļa artēriju plūsma, kas svārstās no 2-3 līdz 60-80 ml / min, nozīmē ideālāko vidi, lai Paskala likumu piemērotu visā cilvēka ķermenī; kopējā struktūra ir unikāla.[9]
Izmērs
Galvenais raksts: Cilvēka dzimumlocekļa izmērs
Dzimumlocekļa mērījumi atšķiras, un pētījumos, kas balstās uz pašmērījumu, vidējais lielums ir ievērojami lielāks nekā mērījumos, kurus veikuši veselības aprūpes speciālisti. Sākot ar 2015. gadu, a sistemātiska pārskatīšana no 15 521 vīrieša (un līdz šim labākais pētījums par šo tēmu, jo priekšmetus mērīja veselības aprūpes speciālisti) secināja, ka vidējais uzcelt cilvēka dzimumlocekļa garums ir 13,12 cm (5,17 collas), savukārt uzceltā cilvēka dzimumlocekļa vidējais apkārtmērs ir 11,66 cm (4,59 collas).[3][4]
Starp visiem primātiem cilvēka dzimumlocekļa apkārtmērs ir vislielākais, bet tas ir salīdzināms ar šimpanze dzimumlocekļa un dažu citu primātu dzimumlocekļu garumā.[11] Dzimumlocekļa izmēru ietekmē ģenētika, bet arī ar tādiem vides faktoriem kā auglības zāles[12] ķīmiskā / piesārņojuma iedarbība.[13][14][15] Visilgāk oficiāli dokumentēto cilvēka dzimumlocekli atrada ārsts Roberts Latou Dikinsons. Tas bija 34,3 cm (13,5 collas) garš un 15,9 cm (6,26 collas) apkārt.[16]
0 notes
Photo

‼️ESSKA-ESA MEMBERS MEETING FEBRUARY 2023 LJUBLJANA, SLOVENIA. Partial posterosuperior rotator cuff tears, diagnosis and treatment. Brainstorming an socializing with shoulder surgeons from all the Europe. ‼️Συνέδριο μελών της Ευρωπαϊκής Εταιρείας Ώμου ESA-ESSKA, 2023 Λουμπλιάνα, Σλοβενία. Μερικές ρήξεις του τενοντίου πετάλου του Ώμου, διάγνωση και αντιμετώπιση. Ανταλλαγή απόψεων, ιδεών, τεχνικών για κοινά προβλήματα με συναδέλφους χειρουργούς ώμου απο όλη την Ευρώπη. Αλλά και περιήγηση στην όμορφη Λουμπλιάνα. #esaesska #esa #esska #shoulder #ώμος #Αρθροσκόπηση #Ορθοπαιδικός #ορθοπεδικός #Χαλκίδα #Μαρούσι (στην τοποθεσία Ljubiana, Slovenia) https://www.instagram.com/p/CoRbE-FIpuo/?igshid=NGJjMDIxMWI=
0 notes
Text
Lupine Publishers | Haglund Syndrome – A Case of Bilateral Involvement
Lupine Publishers | Orthopedics and Sports Medicine
Abstract
Haglund syndrome is a cause of posterior heel pain and occurs commonly in adolescent girls who wear high heels with restrictive heel counters and may occur in people with rheumatoid arthritis. Is characterized clinically by thickening of the soft tissues at the Achilles tendon insertion or a painful “pump bump” and retrocalcaneal bursitis, Achilles tendinitis, and a prominent posterosuperior calcaneal border or bursal projection. We report a case of a 59 years-old woman with bilateral Haglund syndrome which did not needed surgical treatment, being the conservative treatment enough to improve the patient’s quality of life.
Keywords: Calcaneus; Magnetic resonance imaging; Foot diseases
Introduction
Haglund syndrome is a cause of posterior heel pain and was first described by Patrick Haglund, in 1928, to occur in patients who had a prominence of the posterosuperior surface of the calcaneus [1]. It occurs commonly in adolescent girls who wear high heels with restrictive heel counters and may occur in people with rheumatoid arthritis [1]. Haglund syndrome has also been termed “pump bump,” “winter heel,” “knobby heels,” “calcaneal altus,” “highbrow heels,” and “cucumber heels” [1]. Haglund syndrome is characterized clinically by thickening of the soft tissues at the Achilles tendon insertion or a painful “pump bump” and retrocalcaneal bursitis, Achilles tendinitis, and a prominent posterosuperior calcaneal border or bursal projection [1-4].
Case Presentation
59 years-old woman with pain and swelling in both feet for four months that get worse when use slippers and when she wake up and put her feet in the floor for the first time in the day. The patient denies other complaints and surgeries. At physical examination refers pain at the palpation of in the posterior and inferior regions of the ankle. The Magnetic Resonance Imaging (MRI) demonstrates posterior and plantar calcaneal spurs, liquid in retrocalcaneal and subcutaneous calcaneous bursa, and calcaneal tendon with heterogeneous signal and thickened (1.4cm at left and 1.2cm at right), markedly in their insertion with adjacent bone edema (Figures 1 & 2). The set of findings are compatible with Haglund syndrome. The patient started conservative treatment with non-steroidal anti-inflammatories, change of footwear and physiotherapy, presenting a good response, not requiring surgery.
Discussion
Haglund syndrome is caused by mechanically induced inflammation of the Achilles tendon and its bursa, from abnormally high pressure between the bursal projection of the calcaneus, the Achilles tendon, and the bursa [1,5]. Patients with bursitis have erythema and swelling over the bursa and tenderness to direct palpation [2] besides pain with dorsiflexion of the foot [6]. Clinically, by physical examination alone, it may be difficult to distinguish Haglund’s syndrome from other causes of hindfoot pain such as Reiter’s disease, rheumatoid arthritis, or isolated local conditions such as superficial tendon Achilles bursitis secondary to poor shoe fit [7]. Plain radiograph in a lateral standing position is useful to assess the presence of a prominent bursal projection of the calcaneum, the Haglund deformity [3]. Loss of a lucent retrocalcaneal recess is an important indication of underlying retrocalcaneal bursitis [3]. The Achilles tendon is swollen, and dystrophic calcifications may also be seen [3].
MRI may be required for ambiguous or clinically equivocal cases [3]. The cardinal soft tissue abnormalities, namely Achilles tendinopathy, and retrocalcaneal and retroachilles bursitis are more easily and directly depicted by MRI [3]. The detection of marrow oedema within the prominent bursal projection is likely to support the repetitive mechanical compression and inflammation as the pathological mechanism in this condition [3]. Treatment of Haglund deformity, with or without bursitis, targets decreasing the pressure and inflammation with openheeled shoes, anti-inflammatory or analgesic medications, and corticosteroid injections [2]. Physical therapy may also help reduce pain. In recalcitrant cases, surgery to remove the Haglund deformity may be necessary [2].
The nonsurgical treatment, combined with modifications in daily shoe wear, is an appropriate initial treatment for pain relief of Haglund’s syndrome [7]. Using ultrasound guidance to inject the retrocalcaneal bursa is a simple, reliable method of ensuring accurate delivery of medication into the bursa and avoiding intratendinous injection [7].
For more Lupine Publishers Open Access Journals Please visit our website: h http://lupinepublishers.us/
For more Orthopedics and Sports Medicine Open Access Journal (OSMOAJ)
Please Click Here: https://lupinepublishers.com/orthopedics-sportsmedicine-journal/index.php
To Know More About Open Access Publishers Please Click on Lupine Publishers
Follow on Linkedin https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
4 notes
·
View notes
Video
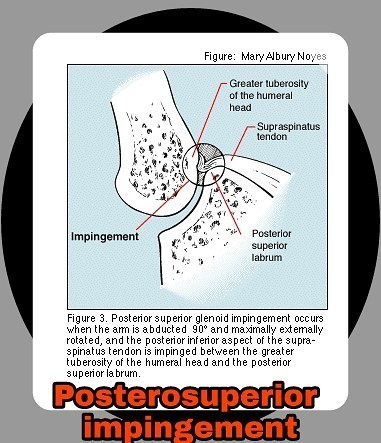
Задне-верхий импинджмент, также известный как внутренний #импинджмент, является относительно нечастой формой импинджмент синдрома, развивается преимущественно у спортсменов 👇🇺🇸#Posterosuperior #impingement, also known as #internal impingement, is a relatively uncommon form of #shoulder impingement. -----#sting----- #MRI ----- --#infraspinatus tendinosis and tears, usually superior fibers at the humeral surface --#supraspinatus tendinosis and #tear involving the posterior fibers --posterosuperior #labral tear or fraying --#humeral head #cysts underlying the infraspinatus tendon
#labral#impingement#humeral#cysts#posterosuperior#supraspinatus#shoulder#sting#mri#tear#infraspinatus#internal#импинджмент
0 notes
Text
Angles Of Parietal Bone
Anterosuperior - Bregma (♦️ shaped in newborn)
Anteroinferior - Pterion (🔫 point)
Posterosuperior - Lambda ( λ )
Posteroinferior - Asterion ( ⭐ shaped)

#mnemonic#student#medicine#exam#doctor#study#trick#symptoms#anatomy#bones#osteology#parietal#fontanelles#school#college
4 notes
·
View notes
Photo

A veces nos dejamos llevar por las palabras del vocablo popular, entonces algo que quizás comience por un juego termina siendo nuestra realidad, es lo que sucede con está palabra, que en vez de decir Gastronemius la cambiamos por batata 😄. 🏁BATATA Raíz comestible, en forma de tubérculo. Es rica en fécula y fibra, y de sabor dulce que permite su uso en una gran variedad de preparaciones, tanto de plato como de postre. 🙄. . 🏁 GASTRONEMIUS músculo formado por 2 cabezas, una externa y otra interna, de las cuáles la interna es la más alta y gruesa. El musculo interno en la cara posterosuperior del cóndilo femoral interno, es mucho más alto que el origen externo. También llamado popularmente gemelos, por estar separado en dos mitades, está situado en la región posterior de la pierna y es el músculo más superficial de la pantorrilla. Está ubicado sobre el músculo sóleo y se extiende desde los cóndilos femorales, porción superior, hasta el tendón calcáneo en su porción inferior. Es voluminoso, oval, aplanado, con dos cabezas: «medial» y «lateral». Se dice que es un músculo biauricular ya que en su trayecto atraviesa dos articulaciones, la de la rodilla y la del tobillo. . Debemos cambiar y romper con esos vocablos mal expresados, por eso es importante estar constantemente profesionalizandonos y hacer el esfuerzo por mejorar. . @crosstrainingrf #crosstrainingrf #crosstraining #actividadfisicorporal #ipreview via @preview.app (en GYM Health Fitness Center) https://www.instagram.com/p/CCXAYjSFWHs/?igshid=5eubqr6v3epk
0 notes
Photo

Una parte importante de las artroplastias de revisión de cadera, es decir, aquellas caderas que fueron operadas y por alguna razón requieren un nuevo recambio ameritan de la una reconstrucción adecuada del componente acetabular (parte de la cadera que esta unida a la pelvis). Existen diferentes métodos que han evolucionada desde la experiencia de cada cirujano hasta las técnicas más recientes, pero los objetivos siempre buscan: preservar el mayor tejido oseo posible, permitir estabilidad adecuada, conservar inclinación anatómica de la copa acetabular, reparar o reconstruir defectos posterosuperiores y garantizar el apoyo con una marcha adecuada.//- -// An important part of hip revision arthroplasties, i.e. those hips that have been operated on and for some reason require a new replacement require adequate reconstruction of the acetabular component (part of the hip that is attached to the pelvis). There are different methods that have evolved from the experience of each surgeon to the most recent techniques, but the objectives are always: to preserve as much bone tissue as possible, to allow adequate stability, to preserve the anatomical inclination of the acetabular cup, to repair or reconstruct superior posterior defects and to guarantee support with an adequate gait. #drmaizo #cirugiadecadera #acetabulo #hipsurgery #hip #orthopedicsurgery #caracas #cirugiaortopedica #truamtologia #traumatology https://www.instagram.com/p/B0HfJ5znQMK/?igshid=1xp4z6lqfnbo7
#drmaizo#cirugiadecadera#acetabulo#hipsurgery#hip#orthopedicsurgery#caracas#cirugiaortopedica#truamtologia#traumatology
0 notes
Text
Lupine Publishers - Journal of Otolaryngology

External auditory canal cholesteatoma: A case report by Indira Acharya
We present a case of cholesteatoma of external auditory canal with invasion to atic, aditus and antrum. Tympanic membrane remained intact. Malleus, incus and stapes supra structure were absent with dehiscent horizontal segment of facial nerve. Cochlea was totally dehiscent. Symptoms were only chronic otorrhoea and hearing impairment. Diagnosis was based on clinical analysis. CT Scan was used to measure pathology. Treatment was Modified radical mastoidectomy associated with meatoplasty. 17 years old female, presented to Otorhinolaryngological outpatient department of IOM, TUTH with complains of bilateral ear discharge and bilateral decreased hearing since childhood. She had a history of right atticotomy with PORP placement 2 years back. Since then there is no history of discharge from right ear. Otoscopy showed intact left tympanic membrane with cholesteatoma in left external auditory canal attached with posterosuperior part of pars tense and posterior atic. Pure tone audiometry showed 40dB mild conductive hearing loss in right ear and 59dB moderate conductive hearing loss in left ear. Cholesteatoma of external canal was suspected and high resolution CT scan of temporal bone was requested.To Read more please click on below link
https://lupinepublishers.com/otolaryngology-journal/fulltext/external-auditory-canal-cholesteatoma-a-case-report.ID.000103.php
For more Lupine Publishers Open Access Journals Please visit our website: h
http://www.lupinepublishers.us/
For more Journal of Otolaryngology-ENT Research articles Please Click Here:
https://lupinepublishers.com/otolaryngology-journal/
#Lupinepublishers#Otolaryngology Journal#ENT Research Journal#Peer Review Journal on Otolaryngology#Rhinology Journal
0 notes
Text
Saha to undergo shoulder <b>surgery</b> in Manchester: BCCI
"Wriddhiman Saha has sustained a posterosuperior labral tear. He will undergo surgery on his shoulder in Manchester at the end of July or the 1st ...
from Google Alert - surgery https://ift.tt/2mC1Dpo
0 notes
Text
Giải phẫu, chức năng & sơ đồ động mạch não giữa Blog-Health.com
Bài viết Giải phẫu, chức năng & sơ đồ động mạch não giữa Blog-Health.com được chia sẻ bởi website Blog-Health
#bloghealth #suckhoe #lamdep #sinhly
Động mạch não giữa (MCA) là một nhánh tận cùng của động mạch cảnh trong và là một phần của tuần hoàn não trước. Động mạch não giữa cung cấp nhiều cấu trúc não sâu, phần lớn bề mặt bên của bán cầu đại não và cực thái dương của não. Bài báo này sẽ thảo luận về giải phẫu, chức năng và sơ đồ của động mạch não giữa.
1. Giải phẫu động mạch não giữa
Các động mạch não giữa (MCA) là một chi nhánh thiết bị đầu cuối của động mạch cảnh trong và là một phần của tuần hoàn não trước. Động mạch não giữa cung cấp nhiều cấu trúc não sâu, phần lớn bề mặt bên của bán cầu đại não và cực thái dương của não. Động mạch não giữa đi từ đáy não qua sulcus bên (của Sylvius), trước khi kết thúc trên bề mặt bên của não. Phân loại phẫu thuật chia động mạch não giữa thành 4 đoạn (M1-M4), tạo ra tổng cộng 10 nhánh. Động mạch não giữa phát sinh trong lỗ liên mấu, từ động mạch cảnh trong từ góc bên của vòng tròn Willis. Nó nằm ngang giữa thùy trán và thùy thái dương, đi ngang qua khe nứt Sylvian. Sau đó nó đi qua bề mặt posterosuperior của insula , nơi nó rẽ đôi vào thân cao và thấp kém. Các thân này đi cùng nhau qua khe nứt Sylvian về phía bề mặt bên của não.
Chia động mạch não giữa thành bốn đoạn giúp xác định rõ hơn đường đi của nó bao gồm:
Đoạn M1 (hình cầu/ngang) di chuyển theo kiểu gần như nằm ngang từ động mạch cảnh trong đến điểm phân đôi động mạch não giữa giữa thùy thái dương và thùy trán. Nó nằm trong phần hình cầu của khe nứt Sylvian, qua đó nó tiến xa tới điểm giao nhau của đoạn hình cầu và hình cầu của khe nứt Sylvian. Tại vị trí kết thúc của đoạn M1, các thân của động mạch não giữa quay 90 ° theo hướng ra sau, được phân định là chi (vĩ độ “đầu gối”) của động mạch não giữa. Ở đây, động mạch não giữa chia thành trung kế cao cấp và trung kế thấp hơn.
Đoạn M2 (nội tiếp) bắt đầu tại điểm phân đôi động mạch não giữa và bao gồm một thân cao hơn và thấp hơn. Phân đoạn này bắt đầu với chi động mạch não giữa ở cấp độ của limen và sau đó di chuyển dọc theo bề mặt của lime. Nó kết thúc ở mức sulcus tròn của insula.
Đoạn M3 (thị giác) bắt đầu đi lên từ đường kính tròn của lỗ nhãn áp về phía bề mặt của não. Đoạn này hướng qua các bề mặt bên trong của phần đỉnh và phần thái dương của thể mi.
Đoạn M4 (đầu cuối, vỏ não) tiếp tục đi vào đoạn M3 khi nó xuất hiện qua đường nứt bên để đến bề mặt của não và di chuyển trên bề mặt của bán cầu đại não.

Động mạch não giữa được chia thành bốn đoạn giúp xác định rõ hơn đường đi của nó
Động mạch não giữa có 10 nhánh, được phân loại thành trung ương và vỏ não.
Nhiều nhánh trung tâm phát sinh từ động mạch não giữa khi nó đi vào khe nứt Sylvian. Chúng còn được gọi là động mạch vân hoặc động mạch bên , và chức năng chính của chúng là cung cấp cho các cấu trúc sâu của não.
Các nhánh vỏ não phân chia ra khỏi động mạch não giữa khi nó nổi lên trên bề mặt não. Chức năng chính của các nhánh vỏ não là cung cấp phần lớn bề mặt bên của não, tức là các phần quỹ đạo, trán, đỉnh và thái dương của vỏ não .
Chi nhánh trung tâm
Các nhánh trung tâm của động mạch não giữa phát sinh trong đường nứt Sylvian, từ các đoạn M1 và M2 của động mạch não giữa. Tất cả chúng đều được gọi chung là động mạch vân bên (lenticulostriate) .
Các động mạch vôi hóa bên xuyên qua sàn của khe nứt Sylvian và đi sâu tới bề mặt bên ngoài của đồi thị . Chúng cung cấp các hạch cơ bản, tức là thể vân, phần lớn ở đầu và thân của nhân đuôi, và các phần lớn của nhân dạng thấu kính và của bao bên ngoài và bên trong.
Nhánh vỏ não
Các nhánh vỏ não của động mạch não giữa phát sinh từ tất cả các đoạn của nó. Chúng tăng dần về kích thước, với những khẩu có nguồn gốc từ M1 là ngắn nhất, trong khi những khẩu có nguồn gốc từ M4 là dài nhất. Đáng chú ý là các nhánh vỏ não phát sinh trước sự phân đôi của MCA thường được gọi là các nhánh trung ương ban đầu vì mục đích phân biệt giải phẫu thần kinh.
Các nhánh vỏ não được đặt tên theo vùng não mà chúng cung cấp;
Các động mạch thái dương trước tạo mạch máu cho cực thái dương của não, là phần trước nhất của thùy thái dương. Chúng phát sinh từ đoạn M1 của động mạch não giữa.
Động mạch trán bên cung cấp phần bên của bề mặt quỹ đạo của thùy trán, cũng như hồi tràng phía trước dưới. Nó phát sinh từ đoạn M2 của động mạch não giữa.
Phần còn lại của các nhánh vỏ não phát sinh từ đoạn M4 của động mạch não giữa;
Động mạch của sulcus trước trán cung cấp các khía cạnh phía trước của con quay hồi chuyển trán dưới và giữa.
Động mạch của sulcus trước trung tâm di chuyển trong sulcus trước trung tâm để cung cấp cho khía cạnh sau của con quay trán dưới và giữa, vùng Broca và con quay trước trung tâm, nơi chứa vỏ não vận động chính cho đầu, chi trên và thân.
Động mạch của sulcus trung tâm di chuyển trong sulcus trung tâm và góp phần cung cấp máu cho con quay trước và sau trung tâm
Động mạch của sulcus sau di chuyển trong sulcus sau để cung cấp cho mặt trước của thùy đỉnh và hồi chuyển trung tâm chứa vỏ não somatosensory chính cho đầu, chi trên và thân.
Một loạt các nhánh đỉnh cung cấp mặt bên của thùy đỉnh, bao gồm cả các tiểu thùy bên trên và dưới.
Động mạch góc cung cấp gyri góc và trên của thùy đỉnh, phần sau của gyrus thái dương trên, và phần trên của bề mặt bên của thùy chẩm.
Các nhánh thái dương giữa cung cấp khía cạnh giữa của con quay thái dương trên và giữa, cũng như vỏ não thính giác chính và khu vực của Wernicke
Các biến thể của giải phẫu
Động mạch não giữa có thể thay đổi về nguồn gốc của nó. Một động mạch não giữa nhân đôi chỉ được nhìn thấy ở dưới 3% số người nhưng sẽ được nhìn thấy phát sinh từ động mạch cảnh trong, song song với động mạch não giữa chính và đi về phía thùy thái dương trước để cung cấp cho nó.
Có tới 4% số người có động mạch não giữa phụ thường cung cấp vùng quỹ đạo phía trước của não. Nó có thể được nhìn thấy phát sinh từ động mạch cảnh trong (Loại 1), đoạn A1 của não trước (Loại 2), hoặc đoạn A2 của não trước (Loại 3).

Trong một cơn đột quỵ não cấp, động mạch não giữa là động mạch thường bị tắc nghẽn
2. Chức năng động mạch não giữa
Trong 3 động mạch lớn mà kênh máu tưới đến não thì có các động mạch não giữa (MCA) là lớn nhất.động mạch não giữa bắt đầu phân nhánh ở động mạch cảnh trong. Nó vận chuyển máu đến các vùng bên của thùy trán, thái dương và thùy đỉnh. Các thùy trán, thái dương và thùy đỉnh tham gia vào kiểm soát các chức năng cảm giác của cánh tay, cổ họng, bàn tay và mặt.
Các phần của động mạch não giữa là:
Đoạn ngang : “chui vào” mô não bằng các nhánh và được gọi là động mạch bên. Nhiệm vụ của đoạn này là cung cấp máu cho các hạch nền. Các hạch nền là các cụm tế bào thần kinh rộng lớn hay còn được gọi là tế bào thần kinh, chịu trách nhiệm cho các chuyển động không chủ ý.
Phân đoạn Sylvian : Phân đoạn này cung cấp máu cho thùy thái dương và vỏ não. Thùy thái dương tham gia trực tiếp vào quá trình xử lý âm thanh. Vỏ não là bộ phận đảm nhiệm nhiệm vụ điều chỉnh một số chức năng vận động và giúp ghép nối cảm xúc với trải nghiệm. Các nhánh của phân đoạn Sylvian có thể phân đôi (tách làm hai) hoặc phân nhánh (chia làm ba) thành các nhánh riêng. Vùng não này cũng chứa vỏ não, một lớp bao phủ của não, kéo dài từ đường bao theo hướng của vỏ não, lớp ngoài của não. Phân đoạn Sylvian đôi khi được tách thành phân đoạn mắt và phân đoạn nội nhãn.
Các đoạn vỏ não: Cung cấp máu cho vỏ não cơ thể.
Trong một cơn đột quỵ não cấp, động mạch não giữa là động mạch thường bị tắc nghẽn. Các công cụ hình ảnh thần kinh, chẳng hạn như chụp CT Scanner, là những xét nghiệm chẩn đoán thường được sử dụng để xác định đột quỵ. Các bác sĩ tìm kiếm huyết khối tĩnh mạch não giữa cấp tính - một cục máu đông trong mạch - vì đây là một dấu hiệu rất tốt của tắc nghẽn động mạch não giữa do huyết khối, tắc nghẽn động mạch não giữa do cục máu đông hoặc hạt đến từ nơi khác gây ra.
3. Sơ đồ động mạch não giữa

Sơ đồ cấu trúc và vị trí của động mạch não giữa
Để được tư vấn trực tiếp, Quý Khách vui lòng bấm số HOTLINE hoặc đăng ký trực tuyến TẠI ĐÂY. Ngoài ra, Quý khách có thể Đăng ký tư vấn từ xa TẠI ĐÂY
Nguồn tham khảo: kenhub.com, healthline.com, physio-pedia.com
source https://blog-health.com/giai-phau-chuc-nang-so-do-dong-mach-nao-giua-blog-health-com/
0 notes
Text
Lóbulo paracentral: características, ubicación y funciones
La corteza del cerebro humano contiene varios giros y circunvoluciones que delimitan diferentes regiones y estructuras cerebrales, cada una de ellas con sus respectivas funciones e interconectadas unas con otras. Una de ellas es el denominado lóbulo paracentral, una circunvolución localizada en la parte medial de los hemisferios cerebrales que contiene varias áreas relacionadas con la planificación y la gestión de acciones motoras. **En este artículo te explicamos qué es el lóbulo paracentral**, dónde se ubica, qué funciones desempeñan las áreas que pertenecen a esta circunvolución y qué tipo de trastornos pueden originarse si se daña esta región del cerebro. * Artículo relacionado: "[Partes del cerebro humano (y funciones)](/neurociencias/partes-cerebro-humano)" ## Lóbulo paracentral: definición y localización neuroanatómica El lóbulo paracentral es **una circunvolución del cerebro situada en la superficie medial del hemisferio, contiguo a las circunvoluciones precentral y postcentral**. Incluye áreas del lóbulo frontal y del [lóbulo parietal](/neurociencias/lobulo-parietal). Constituye la parte más medial del giro frontal superior. Esta región cerebral delimita, posteriormente, con el surco marginal; la extensión terminal ascendente del surco cingulado, que separa el lóbulo paracentral de la precuña o precúneo. Su límite inferior es el surco cingulado, que separa este lóbulo del giro cingulado. Por su parte, el surco central se extiende hacia la zona posterosuperior del lóbulo paracentral, creando la división entre la zona anterior del lóbulo frontal y la porción posterior del lóbulo parietal. El cerebro contiene numerosas circunvoluciones o giros a lo largo de toda la corteza cerebral, lo que le confiere un aspecto arrugado. En la corteza es, precisamente, donde se procesan y se llevan a cabo las funciones cognitivas superiores que implican la planificación y gestión de movimientos o las decisiones ejecutivas. **El lóbulo paracentral puede dividirse en su porción anterior y posterior**: la zona anterior del lóbulo paracentral forma parte del lóbulo frontal y, a menudo, recibe el nombre de área motora suplementaria; y la porción posterior se considera como parte del lóbulo parietal, responsable de las funciones somatosensoriales de las extremidades distales. A continuación veremos cuáles son las principales funciones de las áreas que se incluyen en esta parte del cerebro. ## Funciones El lóbulo paracentral está formado por núcleos neuronales que se encargan de la inervación motora y sensorial de las extremidades inferiores contralaterales, así como de la regulación de funciones fisiológicas básicas, como la micción y la defecación. **Una de las áreas incluídas en este lóbulo es el área motora suplementaria**, una región cerebral que forma parte de la corteza motora y cuya principal función es regular la producción de movimientos voluntarios en el sistema musculoesquelético. Esta área, junto con el área premotora, forman ambas parte de la corteza motora secundaria, responsable de la planificación e iniciación de los movimientos que, posteriormente, se encargará de ejecutar la corteza motora primaria. **La corteza motora primaria**, localizada en la circunvolución precentral y el lóbulo paracentral, están organizada de forma somatotópica; esto significa que están sobrerrepresentadas en un mapa topográfico las distintas partes del cuerpo que realizan movimientos precisos, como las manos y la cara, en comparación con otras zonas, como el tronco y las piernas, que realizan movimientos más gruesos. Por ejemplo, cuando se utilizan electrodos para estimular la porción anterior del lóbulo paracentral se inician movimientos de la pierna contralateral. Y si después estos electrodos se desplazan desde la parte dorsomedial a una ventrolateral en la circunvolución precentral, los movimientos generados irán progresando desde el torso, el brazo y la mano, hasta llegar a la parte más lateral de la cara. * Quizás te interese: "[Corteza motora del cerebro: partes, ubicación y funciones](/neurociencias/corteza-motora-cerebro)" ## Trastornos relacionados con un daño en esta región cerebral Las principales manifestaciones clínicas causadas por un daño en las áreas del lóbulo paracentral incluyen normalmente déficits motores. Los pacientes pueden presentar signos clínicos como la paresia (sensación de debilidad en uno o varios músculos) o, directamente, una plejia o parálisis muscular completa. **Las lesiones en áreas premotoras provocan alteraciones en la planificación y la secuenciación de acciones motoras**. En ocasiones, se observa un deterioro o una incapacidad para ejecutar planes motores aprendidos, sin que exista una parálisis muscular: un trastorno denominado apraxia. Existen varios tipos de apraxias, pero el síndrome motor más habitual cuando existe un daño en áreas premotoras suele incluir la incapacidad para usar objetos cotidianos y para producir movimientos con cierta complejidad: por ejemplo, lavarse los dientes, abrir una puerta o vestirse. Cuando las dificultades motoras afectan a la capacidad de escribir de la persona, el trastorno recibe el nombre de agrafia. Otro de los trastornos originados por la lesión o la resección del área motora suplementaria, localizada, como hemos comentado, en el lóbulo paracentral, es un síndrome que lleva su nombre. **El síndrome del área motora suplementaria** afecta a la capacidad para iniciar movimientos, provocando inicialmente una acinesia global. También pueden aparecer alteraciones del lenguaje y, más adelante, problemas de coordinación, parálisis facial y hemiplejia contralateral al daño en esta región cerebral. En particular, **el daño provocado en el área motora suplementaria izquierda puede producir afasia motora transcortical**, un trastorno que provoca falta de fluidez verbal, a pesar de que se conserva la repetición. También se produce la ausencia de iniciativa y motivación a la hora de establecer la comunicación, pudiendo aparecer disnomia (incapacidad para nombrar objetos o personas) y un enlentecimiento del habla, con la aparición de lenguaje telegráfico y, en ocasiones, ecolalia (repetición involuntaria de palabras o frases recién escuchadas). **En los casos más extremos, se puede producir un mutismo absoluto** que impide al paciente hablar o comunicarse con los demás. Los problemas motores son también relevantes, con la aparición de acinesia y la pérdida de movimientos en los miembros proximales. Las dificultades a la hora de ejecutar movimientos automatizados también son habituales, aunque si los pacientes son capaces de moverse voluntariamente no suelen presentar estas alteraciones. #### Referencias bibliográficas: * Cervio, A.; Espeche, M.; Mormandi,R.; Alcorta, S.C. & Salvat, S. (2007). Síndrome del área motora suplementaria postoperatoria. Reporte de un caso. Revista argentina de neurocirugía, 21 (3). Ciudad Autónoma de Buenos Aires. * Roland, P. E., Larsen, B., Lassen, N. A., & Skinhoj, E. (1980). Supplementary motor area and other cortical areas in organization of voluntary movements in man. Journal of neurophysiology, 43(1), 118-136. * Snell, R. S. (2007). Neuroanatomía clínica. Ed. Médica Panamericana.
Ver Fuente
Ver Fuente
0 notes
Text
Laparoscopic partial liver resection improves the short-term outcomes compared to open surgery for liver tumors in the posterosuperior segments
Abstract
Purpose
The aim of this study was to compare the clinical outcomes between laparoscopic partial liver resection and open partial hepatectomy for tumors in the posterosuperior segments.
Methods
The clinical outcomes of patients who underwent either laparoscopic (n = 20) or open (n = 44) resection in segments 7/8 of the liver were initially evaluated. Because of disparities in the background characteristics, a case-matched study (1:1) was conducted. In addition, a comparative study of the patients who met the institutional criteria for laparoscopic partial hepatectomy was performed.
Results
In the case-matched study, the laparoscopic technique required a longer operation time (p = 0.001), but was associated with less intraoperative blood loss (p = 0.021), a lower incidence of major complications (p = 0.014), higher levels of serum albumin on postoperative days 3 and 7 (p = 0.031 and p = 0.035), and earlier discharge (p = 0.001) than open resection. The results of the latter study were similar to those of the case-matched analysis.
Conclusions
Laparoscopic partial hepatectomy was a feasible procedure for treating tumors in the posterosuperior segments without compromising oncological safety and yielded better short-term outcomes than open techniques. In addition, this study provides concrete selection criteria for laparoscopic partial hepatectomy for difficult lesions.
https://ift.tt/2O830LG
0 notes
Text
Lupine Publishers | Haglund Syndrome – A Case of Bilateral Involvement
Orthopedics and Sports Medicine Orthopedics and Sports Medicine
Lupine Publishers | Orthopedics and Sports Medicine
Abstract
Haglund syndrome is a cause of posterior heel pain and occurs commonly in adolescent girls who wear high heels with restrictive heel counters and may occur in people with rheumatoid arthritis. Is characterized clinically by thickening of the soft tissues at the Achilles tendon insertion or a painful “pump bump” and retrocalcaneal bursitis, Achilles tendinitis, and a prominent posterosuperior calcaneal border or bursal projection. We report a case of a 59 years-old woman with bilateral Haglund syndrome which did not needed surgical treatment, being the conservative treatment enough to improve the patient’s quality of life.
Keywords: Calcaneus; Magnetic resonance imaging; Foot diseases
Introduction
Haglund syndrome is a cause of posterior heel pain and was first described by Patrick Haglund, in 1928, to occur in patients who had a prominence of the posterosuperior surface of the calcaneus [1]. It occurs commonly in adolescent girls who wear high heels with restrictive heel counters and may occur in people with rheumatoid arthritis [1]. Haglund syndrome has also been termed “pump bump,” “winter heel,” “knobby heels,” “calcaneal altus,” “highbrow heels,” and “cucumber heels” [1]. Haglund syndrome is characterized clinically by thickening of the soft tissues at the Achilles tendon insertion or a painful “pump bump” and retrocalcaneal bursitis, Achilles tendinitis, and a prominent posterosuperior calcaneal border or bursal projection [1-4].
Figure 1: Sagittal section MRI in T1 sequence in A and T2 STIR sequence in B of the right ankle demonstrating posterior calcaneal spur (red arrow), liquid in retrocalcaneal bursa (blue arrow), liquid in subcutaneous calcaneous bursa (orange arrow), and calcaneal tendinopathy (green arrow).
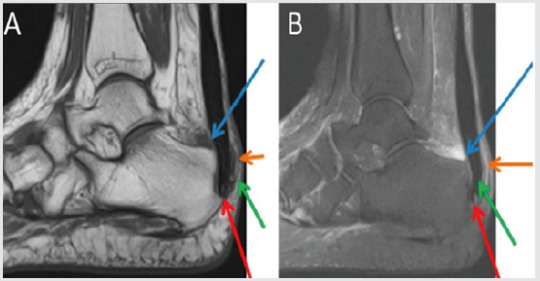
Figure 2: Sagittal section MRI in T1 sequence in A and T2 STIR sequence in B of the left ankle demonstrating posterior calcaneal spur (red arrow), liquid in retrocalcaneal bursa (blue arrow), liquid in subcutaneous calcaneous bursa (orange arrow), and calcaneal tendinopathy (green arrow).
Case Presentation
59 years-old woman with pain and swelling in both feet for four months that get worse when use slippers and when she wake up and put her feet in the floor for the first time in the day. The patient denies other complaints and surgeries. At physical examination refers pain at the palpation of in the posterior and inferior regions of the ankle. The Magnetic Resonance Imaging (MRI) demonstrates posterior and plantar calcaneal spurs, liquid in retrocalcaneal and subcutaneous calcaneous bursa, and calcaneal tendon with heterogeneous signal and thickened (1.4cm at left and 1.2cm at right), markedly in their insertion with adjacent bone edema (Figures 1 & 2). The set of findings are compatible with Haglund syndrome. The patient started conservative treatment with non-steroidal anti-inflammatories, change of footwear and physiotherapy, presenting a good response, not requiring surgery.
Discussion
Haglund syndrome is caused by mechanically induced inflammation of the Achilles tendon and its bursa, from abnormally high pressure between the bursal projection of the calcaneus, the Achilles tendon, and the bursa [1,5]. Patients with bursitis have erythema and swelling over the bursa and tenderness to direct palpation [2] besides pain with dorsiflexion of the foot [6]. Clinically, by physical examination alone, it may be difficult to distinguish Haglund’s syndrome from other causes of hindfoot pain such as Reiter’s disease, rheumatoid arthritis, or isolated local conditions such as superficial tendon Achilles bursitis secondary to poor shoe fit [7]. Plain radiograph in a lateral standing position is useful to assess the presence of a prominent bursal projection of the calcaneum, the Haglund deformity [3]. Loss of a lucent retrocalcaneal recess is an important indication of underlying retrocalcaneal bursitis [3]. The Achilles tendon is swollen, and dystrophic calcifications may also be seen [3].
MRI may be required for ambiguous or clinically equivocal cases [3]. The cardinal soft tissue abnormalities, namely Achilles tendinopathy, and retrocalcaneal and retroachilles bursitis are more easily and directly depicted by MRI [3]. The detection of marrow oedema within the prominent bursal projection is likely to support the repetitive mechanical compression and inflammation as the pathological mechanism in this condition [3]. Treatment of Haglund deformity, with or without bursitis, targets decreasing the pressure and inflammation with openheeled shoes, anti-inflammatory or analgesic medications, and corticosteroid injections [2]. Physical therapy may also help reduce pain. In recalcitrant cases, surgery to remove the Haglund deformity may be necessary [2].
The nonsurgical treatment, combined with modifications in daily shoe wear, is an appropriate initial treatment for pain relief of Haglund’s syndrome [7]. Using ultrasound guidance to inject the retrocalcaneal bursa is a simple, reliable method of ensuring accurate delivery of medication into the bursa and avoiding intratendinous injection [7].
For more Lupine Publishers Open Access Journals Please visit our website: h http://lupinepublishers.us/
For more Orthopedics and Sports Medicine Open Access Journal (OSMOAJ) Please Click Here: https://lupinepublishers.com/orthopedics-sportsmedicine-journal/index.php
To Know More About Open Access Publishers Please Click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
0 notes
Photo
#Posterosuperior #impingement #mri#sport#schoulder#radiopaedia#mri_radiology
0 notes
Text
Quantitative anatomical comparison of the ipsilateral and contralateral interhemispheric transcallosal approaches to the lateral ventricle
Journal of Neurosurgery, Ahead of Print.
OBJECTIVEThe best approach to deep-seated lateral and third ventricle lesions is a function of lesion characteristics, location, and relationship to the ventricles. The authors sought to examine and compare angles of attack and surgical freedom of anterior ipsilateral and contralateral interhemispheric transcallosal approaches to the frontal horn of the lateral ventricle using human cadaveric head dissections. Illustrative clinical experiences with a contralateral interhemispheric transcallosal approach and an anterior interhemispheric transcallosal transchoroidal approach are also related.METHODSFive formalin-fixed human cadaveric heads (10 sides) were examined microsurgically. CT and MRI scans obtained before dissection were uploaded and fused into the navigation system. The authors performed contralateral and ipsilateral transcallosal approaches to the lateral ventricle. Using the navigation system, they measured areas of exposure, surgical freedom, angles of attack, and angle of view to the surgical surface. Two clinical cases are described.RESULTSThe exposed areas of the ipsilateral (mean [± SD] 313.8 ± 85.0 mm2) and contralateral (344 ± 87.73 mm2) interhemispheric approaches were not significantly different (p = 0.12). Surgical freedom and vertical angles of attack were significantly larger for the contralateral approach to the most midsuperior reachable point (p = 0.02 and p = 0.01, respectively) and to the posterosuperior (p = 0.02 and p = 0.04) and central (p = 0.04 and p = 0.02) regions of the lateral wall of the lateral ventricle. Surgical freedom and vertical angles of attack to central and anterior points on the floor of the lateral ventricle did not differ significantly with approach. The angle to the surface of the caudate head region was less steep for the contralateral (135.6° ± 15.6°) than for the ipsilateral (152.0° ± 13.6°) approach (p = 0.02).CONCLUSIONSThe anterior contralateral interhemispheric transcallosal approach provided a more expansive exposure to the lower two-thirds of the lateral ventricle and striothalamocapsular region. In normal-sized ventricles, the foramen of Monro and the choroidal fissure were better visualized through the lateral ventricle ipsilateral to the craniotomy than through the contralateral approach.
from # All Medicine by Alexandros G. Sfakianakis via alkiviadis.1961 on Inoreader http://ift.tt/2wgn3fg
from OtoRhinoLaryngology - Alexandros G. Sfakianakis via Alexandros G.Sfakianakis on Inoreader http://ift.tt/2vBRBLB
0 notes
Last Seen Blogs

sevyn-stars
i don't negotiate with terrorists

vannajamma
stuff...thangs

marzngo
Maria Ngo

silkyskingoldenheart
all the pretty things I like

just-kate3
Kate