#unilocular
Text
In plants
In plants, a new plant can be formed from every organ like root, leaf, flower or fruit. Whereas in humans, a new human can be born from just one organ, the uterus. Are reproductive organs like the uterus present in every part of a plant?
As a plant's reproductive part, a flower contains a stamen (male flower part) or pistil (female flower part), or both, plus accessory parts such as sepals, petals, and nectar glands (Figure 19). The stamen is the male reproductive organ.
Ovary (botany)
Wikipedia
https://en.wikipedia.org › wiki › Ovary_(botany)
In the flowering plants, an ovary is a part of the female reproductive organ of the flower or gynoecium. Specifically, it is the part of the pistil which holds the ovule(s) and is located above or below or at the point of connection with the base of the petals and sepals. The pistil may be made up of one carpel or of several fused carpels (e.g. dicarpel or tricarpel), and therefore the ovary can contain part of one carpel or parts of several fused carpels. Above the ovary is the style and the stigma, which is where the pollen lands and germinates to grow down through the style to the ovary, and, for each individual pollen grain, to fertilize one individual ovule. Some wind pollinated flowers have much reduced and modified ovaries.
Parts of the ovary
Locules are chambers within the ovary of the flower and fruits. The locules contain the ovules (seeds), and may or may not be filled with fruit flesh. Depending on the number of locules in the ovary, fruits can be classified as uni-locular (unilocular), bi-locular, tri-locular or multi-locular. Some plants have septa between the carpels; the number of locules present in a gynoecium may be equal to or less than the number of carpels, depending on whether septa are present.
The ovules are attached to parts of the interior ovary walls called the placentae. Placental areas occur in various positions, corresponding to various parts of the carpels that make up the ovary. See Ovule#Location within the plant. An obturator is present in the ovary of some plants, near the micropyle of each ovule. It is an outgrowth of the placenta, important in nourishing and guiding pollen tubes to the micropyle.[17]
The ovary of some types of fruit is dehiscent; the ovary wall splits into sections called valves. There is no standard correspondence between the valves and the position of the septa; the valves may separate by splitting the septa (septicidal dehiscence), or by spitting between them (loculicidal dehiscence), or the ovary may open in other ways, as through pores or because a cap falls off.
Translate Hindi
पौधों में जड़ पत्ते फूल या फल हर एक अंग में से एक नए पौधें बन सकते है
जबकि हम मनुष्य में एक ही अंग यूटेरस में ही सिर्फ एक नए मनुष्य की जन्म हो सकते है
क्या यूटेरस जैसे जन्मदायी अंग पौधों की हर एक अंग अंश में होते है
पौधे के प्रजनन अंग के रूप में, एक फूल में पुंकेसर (नर फूल वाला भाग) या स्त्रीकेसर (मादा फूल वाला भाग), या दोनों होते हैं, साथ ही बाह्यदल, पंखुड़ियाँ और अमृत ग्रंथियाँ जैसे सहायक भाग भी होते हैं (चित्र 19)। पुंकेसर नर प्रजनन अंग है।
अंडाशय (वनस्पति विज्ञान)
विकिपीडिया
https://en.wikipedia.org › wiki › अंडाशय_(वनस्पति विज्ञान)
फूलों वाले पौधों में, अंडाशय फूल या जायांग के मादा प्रजनन अंग का एक हिस्सा होता है। विशेष रूप से, यह स्त्रीकेसर का वह हिस्सा होता है जो बीजांड (अंडाणुओं) को धारण करता है और पंखुड़ियों और बाह्यदलों के आधार के साथ जुड़ने के बिंदु के ऊपर या नीचे या उस पर स्थित होता है। स्त्रीकेसर एक कार्पेल या कई जुड़े हुए कार्पेल (जैसे कि द्विकार्पेल या त्रिकार्पेल) से बना हो सकता है, और इसलिए अंडाशय में एक कार्पेल का हिस्सा या कई जुड़े हुए कार्पेल के हिस्से हो सकते हैं। अंडाशय के ऊपर वर्तिका और वर्तिकाग्र होता है, जहां पराग उतरता है और वर्तिका से नीचे अंडाशय तक बढ़ने के लिए अंकुरित होता है, और प्रत्येक पराग कण के लिए, एक व्यक्तिगत बीजांड को निषेचित करता है। कुछ पवन परागित फूलों में बहुत कम और संशोधित अंडाशय होते हैं।
अंडाशय के भाग
स्थान फूल और फलों के अंडाशय के भीतर कक्ष होते हैं। स्थानों में बीजांड (बीज) होते हैं, और वे फलों के गूदे से भरे हो भी सकते हैं और नहीं भी। अंडाशय में स्थानों की संख्या के आधार पर, फलों को एक-स्थानिक (यूनीलोकुलर), द्वि-स्थानिक, त्रि-स्थानिक या बहु-स्थानिक के रूप में वर्गीकृत किया जा सकता है। कुछ पौधों में कार्पेल के बीच सेप्टा होते हैं; एक गाइनोकियम में मौजूद स्थानों की संख्या कार्पेल की संख्या के बराबर या उससे कम हो सकती है, यह इस बात पर निर्भर करता है कि सेप्टा मौजूद हैं या नहीं।
अंडाशय आंतरिक अंडाशय की दीवारों के कुछ हिस्सों से जुड़े होते हैं जिन्हें प्लेसेंटा कहा जाता है। प्लेसेंटल क्षेत्र विभिन्न स्थितियों में होते हैं, जो अंडाशय को बनाने वाले कार्पेल के विभिन्न हिस्सों के अनुरूप होते हैं। देखें बीजांड#पौधे के भीतर स्थान। कुछ पौधों के अंडाशय में प्रत्येक बीजांड के माइक्रोपाइल के पास एक ओबट्यूरेटर मौजूद होता है। यह प्लेसेंटा का एक प्रकोप है, जो पराग नलिकाओं को माइक्रोपाइल तक पोषण देने और मार्गदर्शन करने में महत्वपूर्ण है।[17]
कुछ प्रकार के फलों का अंडाशय विखंडित होता है; अंडाशय की दीवार वाल्व नामक खंडों में विभाजित हो जाती है। वाल्व और सेप्टा की स्थिति के बीच कोई मानक पत्राचार नहीं है; वाल्व सेप्टा को विभाजित करके (सेप्टीसाइडल डिहिसेंस) या उनके बीच थूकने से (लोकुलिसाइडल डिहिसेंस) अलग हो सकते हैं,
0 notes
Text
Ronda Cx general.
Eliana, 33 años.
Cx:
Absceso pélvico de origen a establecer.
Procedimiento:
25/08/2023: laparotomía + drenaje de absceso.
**Se palpa quiste izquierdo con contenido de pus, sin mal olor (Absceso frio). Se palpa mada dura al lado contralateral, que consideramos requiere estudio tomografico. Se palpa quiste derecho que consideramos que puede ser anexial, con salida de materia purulento, pero sin mal olor. No hay peritonitis perse. Contiguidad con apendice, se realiza apendicectomia.
Tratamiento:
Piptazo 4.5 g cada 6 horas (FI 25/08/2023, D2), Nadroparina 40 mg cada 24 horas, Solución salina 0.9% 100 cc / h.
Subjetivo: paciente refiere tener dolor abdominal difuso 6/10, sin via oral en el momento, sin nuevos picos febriles.
EF:
Paciente en aceptables condiciones generales, estable hemodinamicamente, afebril, colaboradora al momento de la evaluación.
Mucosas hidratadas.
Abdomen blando, depresible, dolor difuso a la palpación, sin signos de irritación peritoneal.
Extremidades sin edema.
Paraclinicos:
25/08/2023: cultivo liquido peritoneal con BGN en identificación.
Imágenes:
26/08/2023: TAC de abdomen con contraste: liquido abdominal loculado en hopogastrico con pared y engrosamiento peritoneal, posquirurigico vs asociado a catéter, catéter de derivación peritoneal, imagen cosistente con ovario derecho (remanente) en fosa iliaca derecha, sin otras alteraciones focales, quiste unilocular de 4.5 x 5 cm en el ovario izquierdo, muy probablemente funcional / folicular. Miomatosis uterina, DIU en posicion.
Análisis:
Paciente de 33 años de edad, presentó abdomen agudo + signos de irritacion peritoneal, por lo que requirió el 25/08/2023 una laparotomía y drenaje de absceso encontrado a nivel de la pelvis, en donde además encontraron masa dura al lado contralateral, por lo cual el día de ayer se realiza TAC de abdomen liquido abdominal loculado en hopogastrico con pared y engrosamiento peritoneal, posquirurigico vs asociado a catéter, además de quiste unilocular de 4.5 x 5 cm en el ovario izquierdo, muy probablemente funcional / folicular, sin otros hallazgos. El día de hoy paciente se encuentra estable hemodinamicamente, afebril, dolor no controlado, se ajusta analgesia, hoy segundo día de tratamiento AB, en cultivos de liquido peritoneal con crecimiento de BGN, continuamos vigilancia.
0 notes
Text
TECIDO ADIPOSO
- É um tecido conjuntivo especializado que armazena gordura em suas células adiposas, ou adipócitos.
- É considerado a maior reserva de energia do organismo na forma de triglicerídeos.
Classificado de duas formas:
* Unilocular (ou amarelo)
* Multilocular (ou pardo).
Constituição do tecido adiposo:
É constituído predominantemente por células adiposas, ou adipócitos, envoltas por uma lâmina basal e fibras reticulares.
Os adipócitos encontram-se distribuídos de forma isolada, podendo também ser encontrados formando pequenos aglomerados pelo tecido conjuntivo frouxo ou formando grandes agregados, constituindo, assim, o tecido adiposo.
Os adipócitos são capazes de acumular gordura em seu interior.
O seu núcleo localiza-se de forma mais periférica.
ORIGEM DA CÉLULA ADIPOSA
- O tecido adiposo origina-se de células mesenquimáticas. indiferenciadas.
- Essas células acumulam triglicerídeos em forma de gotas que podem fundir-se com o passar do tempo, formando uma única gota, ou permanecerem nesse estado, sem que haja a fusão. Após essas células diferenciarem-se, elas passam a não mais se dividirem.
- quebra das moléculas de triglicerídios, liberam ácidos graxos e glicerol.
- Os ácidos graxos serão encaminhados a outros tecidos para serem utilizados como fonte de energia, e o glicerol será absorvido pelo fígado para ser reutilizado.


0 notes
Text
Hydatid Cysts & Echinococcosis
Parasites are fun.
It's a tapeworm that forms cysts.
Cold open with a very short case report
30F in Mexico presents with RUQ pain and nausea
on examination of her abdo, authors felt a RUQ mass
She received an MRI of her abdo, revealing a cystic mass
on histopatho following a cystectomy, they found Echinococcosis cysts, she also had positive IgG serology to echinococcosis granulosus
Microbiology
a tapeworm that forms cysts that are usually found in the liver or lungs (if not filtered out by the liver), rarely found elsewhere but possible (numerous case reports out there reported in the brain, bones, spleen, kidneys, muscles etc.)
in humans, these cysts can remain in a person's body for years, causing no harm and no symptoms
they can grow by 1 cm per year in the liver
Cyst image from wiki

The tapeworm itself is incredibly eerie to look out, as per CDC website:

4 species of concern in people:
E. granulosus = cystic echinococcosis, or hydatid cysts
E mlutilocularis = alveolar
E. vogeli & oligarthrus = polycystic
Hosts:
generally dogs
intermediates: sheep, goats, pigs
humans are 'incidental or accidental hosts" via contact with a reservoir animal - that is to say, the parasite relies on the above 2 hosts for it's life cycle (not necessarily humans)
transmission: faecal oral, ingestion of eggs in from host faeces
larvae from the eggs penetrate the intestine and is transported in blood/lymphatics to liver (and if through liver to lungs), sometimes other organs
cysts = layers with a fibrous capsule, daughter cysts can bud off, can grow up to multiple litres and can septate and have daughter cysts over time, so may not remain unilocular. hosts may develop a granulomatous reaction
Clinical presentation
can be asymptoamtic for decades, as per 1 case report in a South Korean journal, cysts in one patient caused no issues for 30-40 years (after exposure during the Vietnam war)
become symptomatic when large enough to cause them (if in liver = nausea, vomiting, RUQ pain as per the case report, on exam: abdo distension, palpable mass and hepatomegaly, obstructive jaundice)
in cystic liver disease, it's considered a hydatid cyst and usually assiocaited with cystic echinococcosis
cysts can also eventually rupture and the fluid can cause extreme reactions such as anaphylaxis (IgE mediated Type 1 hypersensitivity reaction), leaking into the peritoneum = hydatidosis
65%: liver, 25% lungs, but 20-40% of patients can have multiorgan involvement
often acquired in childhood but present later in life (excpetion: eye and brain)
in lung: SOB, chest pain, chronic cough, haemoptysis
Rare (from stat pearls)
heart: tamponade
brain = raised ICP, seizures
spinal cord = compression
kidneys = haematuria, flank pain
bones = pathologic fractures
INcreased risk
a/w endemic areas - South America (as per case report above), former soviet union (kinda random), middle east, eastern med, Western China (I suppose these areas are all geographically connected), but also East Africa and Australia
however, alveolar echinococcosis is endemic only to Russia, China, North America and Europe
rural/grazing areas (not surprisingly given the hosts are dogs and sheep), communities needing dogs for herding

30-40 yos more likely to have hydatid cysts while > 50 are a/w alveolar
elderly and immunocompromised are more vulnerable
look for these RFs above (esp contact with dogs + cattle)
Investigations
imaging is definitive, look for the cysts, pretty big if symptomatic
nonspecific, but clues on bloods: mild eosinophilia, leukopaenia and thrombocytopaenia, deranged LFTs in hydatid cysts (abnormal in only 40% of patients, ALP usually high the rest can be normal)
imaging: USS, CT are sufficient, MRI great but no real advantage over CT, useful in the seronegative
serology is useful both in diagnosis and in follow-up after treatment, but many do not have an immune response depending on cyst wall intactness
avoids: aspiration, unless USS/CT guided given the risk of the fluid causing anaphylaxis
in the event the biliary tree is affected, await an ERCP
Stages determine management
WHO informal working group stages (IWGE) based on USS:
CE 1: simple cyst, double line sign
CE2: mlutiseptated, honeycomb/rosette
CE3A: watery lily sign - fluid collection with a detached membrane
CE3B: daughter cysts ina. solid matrix
CE4: heterogenous, hyperechoic, matrix, no duaghter cysts
CE5: solid cystic wall
1&2: active, 3 = transitional (cyst compromised), 4 and 5= inactive
ring like calcifications can be present in all stages
CT over USS = complications, like rupture, infection and biliary/vascular involvement
Treatment
albendazole - antiparasite medication is the foundation
generally depends on the size and number of cysts and there's whole WHO staging and guidelines for this
medical therapy can be anywhere from 1-3 months up to 6, but are futile if the sole treatment cysts > 5 cm or daughter cysts involved
Stage 4&5: watch and wait, USS regularly, these are uncomplicated
CE1 and CE3a: cysts < 5 cm in liver and lung, but inoperable and >2 organs involved = albendazole (CI: pregnancy and cysts vulnerable to rupture), also used following surgery and perc drainage (CT/USS guided) to prevent recurrence
surgery in: complicated cysts for removal of large stage 2 and 3b cysts or cysts that can rupture (superficial), infected, biliary tree communication and pressure on organ. Inovlves excision of cyst and possibly liver resection, contamination with daughter cysts is possible so adj albendazole and praziquantel often done (i.e. 1-4 weeks prior then 4 weeks post. has lower recurrence rates
PAIR = puncture, aspiration, inj with 20% hypertonic saline and re aspiration = USS guided in the inoperable or relapsing cases or failing to respond. usually in cysts > 5 cm with albendazole for 4 weeks, stage 1 only/single compartment cysts (PAIR ineffective in higher stages = multiple compartments)
post treatment: USS 3-6 monthly then yearly
lungs: 2 years of treatment and surgery, simple cysts may just require medical therapy
Differentials
straight from stat pearls - abscess, simple benign cysts, budd chiari, biliary colic, cirrhosis, TB, carcinoma, haemagiomas
Sources:
wikipaedia
statpearls
CDC guidelines
WHO
Australian guidelines (behind a paywall)
#hydatid cyst#echinococcosis#infectious diseases#infectious disease#medblr#microbiology#parasitology
1 note
·
View note
Text
lupine publishers|Management of a Dentigerous Cyst in a 6-Year-Old Child –
A Case Report
Management of a Dentigerous Cyst in a 6-Year-Old Child –A Case Report

Abstract
Dentigerous cysts are epithelial in origin and most common odontogenic cysts. They are usually asymptomatic and hence
diagnosed on radiological examination. The standard treatment for these cysts is enucleation and extraction of the affected teeth.
This is a case report of a 6-year-old female patient with dentigerous cyst associated with a primary molar. The cyst was enucleated
and unerupted premolars were removed from the lower left region. The patient was given a fixed functional band and loop post-
surgical treatment. No recurrence was observed after 6months follow up.
Introduction
Cyst has been known to arise in man ever since he has teeth
and are also seen in certain animals. They are consequential, not
only because they often attain a large size but also produce facial
asymmetry, disturbance of dentition, neurological symptoms and
predispose the jaws to fracture but particularly because they have a
very high frequency of occurrence. Kramer in 1974 defined a cyst as
a pathological cavity having fluid, semi fluid or gaseous content but
not always lined by epithelium [1]. The dentigerous cyst is a type of
epithelial odontogenic cyst and is also called as ‘follicular cyst’ or
‘pericoronal cyst.’ It is the most common type of odontogenic cyst
which encloses the crown of the unerupted tooth by expansion of
its follicle [1,2]. A higher incidence of these cysts is usually found
in the second and third decade of life and slightly more common in
males. They account for 14-20% of mandibular cysts and between
15.2% and 33.7% of all odontogenic cysts. The frequency of these
dentigerous cysts in children is less and about 4-9% of these cysts
occur in the first 10 years of life [3]. They are predominantly
associated with third molars, maxillary canines and mandibular
premolars. Dentigerous cysts are often asymptomatic and are an
incidental finding on routine radiographs. In the radiographic
examination, the lesion has a well-defined sclerotic border, and a
well- demarcated unilocular radiolucency which is surrounding the
crown of an unerupted tooth. In some instances, these cysts can
grow to very large size and can trigger the inflammation, expansion
and erosion of the cortical bone. In such a case, they can generate
a differential diagnosis to an ameloblastoma or an odontogenic
keratocystic tumour.
The following case report describes the management of a
dentigerous cyst in a young child.
Case Report
A 6-year-old female patient reported to the Department of
Pedodontics and Preventive Dentistry, DY Patil School of Dentistry
with a chief complaint of pain in the lower left back region of the
mouth. On general examination, the patient was healthy without
any significant past medical history. Intra oral examination revealed
that the patient presented with a mixed dentition. The area of chief
complaint had deep occlusal caries with loss of crown structure in
relation with 74 and 75 (Figure 1). The primary molars were non
vital and adjacent mucosa was apparently normal, with no signs of
inflammation. An initial intra oral periapical radiograph was taken
for radiological examination. which revealed a huge radiolucency
with no signs of underlying premolar. Hence, a panoramic radiograph
was advised (Figure 2) and it revealed the presence of a well-
defined unilocular radiolucent cystic lesion with sclerotic border
enveloping the crown of mandibular left second premolar. The first
premolar was displaced medially while the second premolar was
apically displaced close to the lower border of the mandible. After
the clinical and radiological examination, a provisional diagnosis
of the dentigerous cyst was made. Surgical enucleation of the cyst
was chosen as the treatment of choice. The surgical intervention
was carried out under general anaesthesia. Blood investigations
(PT, PTT, INR) and cone beam computed tomography (CBCT) was
done prior to the procedure. Both the primary mandibular molars
were extracted followed by opening of the mucoperiosteal flap
to disclose the cystic cavity. After the flap was opened, the cavity
was identified and 3ml of cystic fluid was aspirated. The cystic
lining enclosed both the premolars and hence were removed along
with the soft tissue. The flap was then sutured to close the wound
primarily. The specimen was fixed in 10% formalin and sent for a
histopathological examination. The histopathologic examination
confirmed the diagnostic hypothesis of a dentigerous cyst (Figure
3). The patient was followed up regularly for a month and was
advised to maintain good oral hygiene. When the lesion was
completely healed, prosthetic rehabilitation was done using fixed
functional band and loop space maintainer (Figure 4).
Discussion
Dentigerous cysts are reported to be of two types –
Developmental and inflammatory. The developmental type is most
common and appears to be due to accumulation of fluid between
the reduced enamel epithelium and enamel organ. In rare cases,
the dentigerous cyst develops as a result of the intrafollicular
spread of periapical inflammation from an overlying primary tooth.
(Murakami et al 1995) [4]. Accordingly, in the present case, the
presence of overlying nonvital necrotic primary mandibular first
and second molars increase the possibility of being an inflammatory
type of the dentigerous cyst. The nature of the causative tooth,
size of the lesion and location influences the type of treatment
required for the dentigerous cyst which includes enucleation with
primary closure or marsupialization. Marsupialization of the cyst
is the treatment of choice which gives a chance to the unerupted
tooth to erupt in large cysts [3]. However, in the present case, the
cystic sac was surrounded by the unerupted premolar and was
firmly attached to it; hence, enucleation of the cyst along with
the extraction of premolar was carried out [5]. The histologic
examination of the specimen showed cystic lining composed of
reduced enamel epithelium which was 2-3 cell layers thick and
proliferative at some places. The outer connective tissue stroma
showed inflammatory infiltrate. The aspirated cystic fluid was pink
in colour and thick consistency. Correlating clinically, the features
were suggestive of dentigerous cyst. Owing to the age of the patient
and growth phase, it was decided to rehabilitate the patient with
a suitable prosthesis. Various options were considered and finally
based on the comfort and acceptance of the patient a fixed functional
band and loop was fabricated and cemented. This would restore
the occlusal function of lost primary teeth and will also maintain
the space till the time patient develops permanent dentition and
there is bone development for further fixed prosthesis [6]. For the
fabrication of the appliance, a conventional band and loop was
constructed. The acrylic teeth were placed in the edentulous area
of the cast and stabilized with modelling wax. The occlusion was
checked with the cast of the opposing arch and adjusted. Cold cure
acrylic was used to attach the poetic to the loop. The completed
appliance was then finished and polished. Trial fit was done in
patient’s mouth and checked for soft tissue irritation or occlusal
interferences and adjusted accordingly. The final cementation of
the appliance was done using glass ionomer luting cement [7]. The
patient was evaluated one week post cementation of the appliance
and no complications were reported.
Follow up
The patient was followed up for 6 months with no reports of
fracture of the appliance or food lodgment. Clinical and radiographic
examination did not reveal any signs of recurrence of the cystic
lesion.
Conclusion
Dentigerous cysts are rare in primary dentition and
asymptomatic, usually diagnosed during routine radiographs. The
sequelae of an untreated or undiagnosed cyst could be harmful to
the patient’s future dental development. Thus, regular check-ups by
the patient and close observation on the part of treating doctor are
essential. This results in elimination of pathology and maintenance
of dentition with minimum surgical interventio
for more information about Interventions in Pediatric Dentistry Open Access Journal archive page click on below link
https://lupinepublishers.com/pediatric-dentistry-journal/archive.php
for more information about lupine publishers page click on below link
https://lupinepublishers.com/index.php
#lupine publishers group#Interventions in Pediatric Dentistry Open Access Journal#The nature of the causative tooth
4 notes
·
View notes
Text
Foraminifera: Introduction and anatomy
There’s a lot more to palaeontology than just dinosaurs. I’m sure you’re familiar with fossil mammals like mammoths and sabre-tooths. Everyone loves fossil fish like Dunkleosteus and Megalodon. Fossil invertebrates, like trilobites or ammonites, are some of the most famous fossils of all time. And fossil plants are all over the place, from petrified wood to leaf impressions in coal. But have you ever thought about fossil microorganisms?

(Image: Single-celled organisms like this foraminifera are among the most common organisms today, but the vast majority are microscopically small. [Source])
Microbes are everywhere on Earth today, and they have been everywhere on Earth for seemingly as long as life has existed. They live in practically every environment—but their small size and soft bodies have meant that fossils of them are very rare.
Well, almost all of them, that is. One particular group of single-celled organisms is among the best-studied groups in the entire fossil record, having a highly detailed fossil record stretching back for over 540 million years. These are the hard-shelled foraminifera.
I’ve become enamoured with this neat little group of protists lately. But I’ve been really disappointed with a lot that’s been written about them. For despite being some of the most interesting and geologically famous protists, there has been very little written about them that is accessible to anyone who doesn’t already know a lot about them. I’d like to change that.
What are foraminifera?

(Image: An assortment of foraminifera shells, with a huge variety of shapes and sizes. More on that later... [Source])
Foraminifera (literally meaning “opening bearers”), or “forams” as they are commonly called, are a group of single-celled eukaryotes. In other words, they have a nucleus (or often multiple of them), and they have mitochondria that act as (say it with me) the powerhouse of the cell. Most forams consume smaller microorganisms as food; however, some are capable of utilising dissolved organic carbon, and many groups have convergently evolved endosymbiotic relationships with photosynthetic algae, including rhodophytes, chlorophytes, and dinoflagellates. In fact, certain foraminifera can extract the chloroplasts from algae they consume and incorporate them into their own cells to do photosynthesis! These don’t last forever, though, and the forams eventually digest the chloroplasts. Some other foraminifera actually actively predate on and kill small animals—an amazing feat for a single-celled organism!
Some of the most famous foraminifera are the planktonic forms that float within the water column; however, the vast majority of forams are benthic organisms. These include forms from shallow water to forms found at the very deepest point of the ocean. Though some benthic species live only above the sediment-water interface and others live only interstitially, most benthic forams are not confined to one mode of life and may move between layers of the community in order to seek out food. Some of these forms can even survive without oxygen for extended periods! This allows them to live in conditions that would kill many other organisms.
A few species of forams have been identified from freshwater environments, and one study presented molecular evidence suggesting foraminifera may be widespread in soils, although no actual forams have been found from soils yet. It seems that there might be a lot of diversity even among living forams that we still have yet to uncover.
Anatomy
Of all single-celled organisms, why is it that foraminifera have such a good fossil record? The answer lies in the hard shell of many species, known as a test.
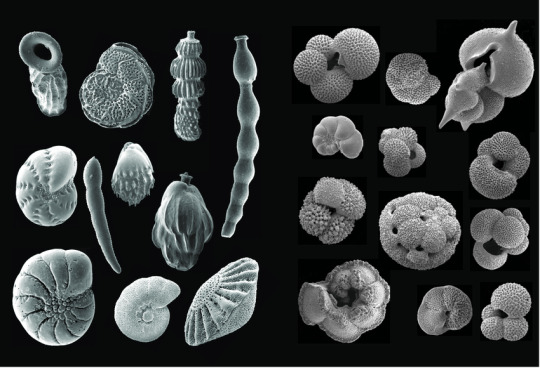
(Image: A variety of test shapes in different foraminifera groups, viewed with a scanning electron microscope. They include may shapes—coiled, glob-shaped, linear, egglike, and more. There are many other shapes of tests that aren’t shown here—like spiralled, branched, disc-like, and more. All of these tests are calcareous. [Source])
These tests are not simply external structures within which foraminifera live; rather, the test is actually within the cell membrane. Although the soft parts of the foraminiferal cell are almost never preserved in the fossil record, modern species of forams have helped us learn a lot about their anatomy. Extending from the opening(s) of the test are pseudopodia, fingerlike extensions of the cell membrane. As the most prominent extensions of the cell outside of the test, they serve a multitude of functions, including locomotion, feeding, agglutinating the test, reproduction, respiration, and excretion. In many forms these pseudopodia extend in all directions through numerous tiny holes in the shell of the test. In other ways the foraminifera anatomically resemble typical single-celled eukaryotes, with nuclei and mitochondria. Some species have multiple nuclei within a single cell). During reproduction, some species of forams can even leave their shell behind entirely to undergo cell division.
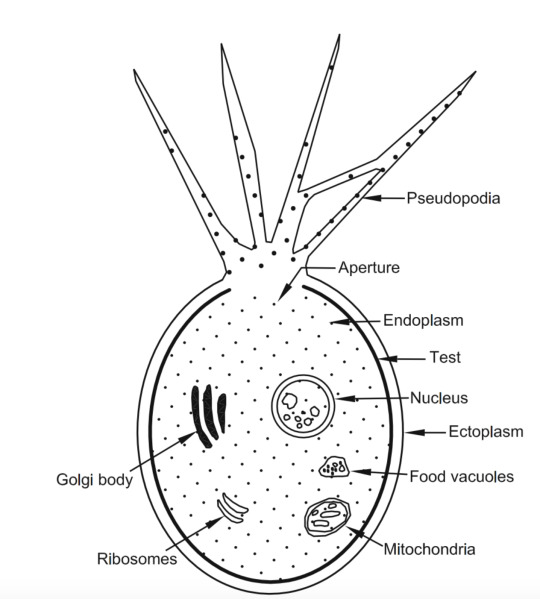
(Image: The anatomy of a foraminiferan. Note that the test is actually inside of the cell wall, but most of the cell materials are inside the test. The pseudopodia are the main thing that extend out of the aperture, or hole. This drawing is a unilocular, or single-chambered, foram.)
The most famous and diverse of these are foraminifera with calcareous tests. Calcareous means that they are made of calcium carbonate, and calcium carbonate takes two main forms: Calcite and aragonite. Calcite is a very common mineral in nature; it’s the stuff that makes up limestone, marble, antacids, coral skeletons, and more. And aragonite is a mineral with the same chemical composition as calcite, but with a different crystal structure. It’s found in the shells of many organisms, like snails. Both calcite and aragonite tests are found in foraminifera, and many species have their own particular composition and crystal structure.
Other forams have agglutinated tests: that is, tests that are made by collecting bits of sand and cementing them together, using either organic proteins or calcite to hold them together.
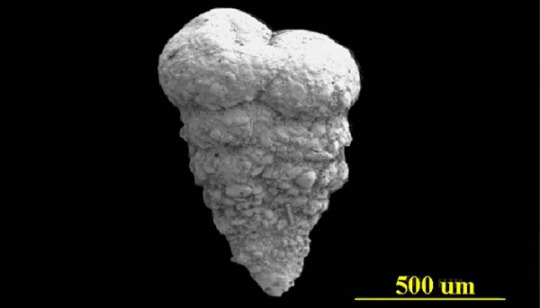
(Image: An agglutinated textulariid foram. Its test is made from sediment grains connected together. It looks a bit like an ice cream cone in shape, but rather than conical, it’s flat. And the top is sealed off. So really, it looks nothing like an ice cream cone. [Source])
Fewer still forams secrete tests of silica—the material that quartz and glass are made of. Others have softer tests made completely from proteins and other organic material. Even rarer are foraminifera which entirely lack tests and were until recently considered to be amoebae; these species likely secondarily lost the test.
Test composition appears to be pretty fluid in foram evolution. In the family tree of foraminifera, it seems that calcite tests evolved multiple times, and so did agglutinated tests. In some cases it looks like they might have even gone from calcite tests to agglutinated tests.
Test shape is also highly diverse within foraminifera. The simplest shape of test are the unilocular, or single-chambered, forms; however, unilocular forms may also have more complex chamber shapes, including spiraled tubes outwardly resembling snail shells. Unilocular forms are found in several groups of forams. The earliest foraminifera were probably all unilocular, and modern unilocular forams probably form a paraphyletic “grade” rather than a true branch of the tree of life. Single-chambered foraminifera probably make up the bulk of forams alive today, but many of these species remained undiscovered and unnamed.
Although unilocular forams are frequently considered the “simplest” forams, they also include some of the most bizarre protists, the xenophyophores. These are my favourite group of foraminifera, and the reason is, I think, pretty clear—they’re enormous. Like, I mean, the largest ones can get up to 20cm/8in across! These are the largest known single-celled organisms on the planet. All of the known species live on the floor of the deep ocean, where they filter-feed.

(Image: A xenophyophore, a giant, single-celled foraminifera. It looks a bit like a sponge, which is what it was once mistaken for. [Source])
Most named species of forams, however, are multilocular, having multiple chambers within their tests. The tests of the most well-known forms superficially resemble the shells of ammonites or nautili. In fact, the earliest scientific descriptions of foraminifera described them as being tiny cephalopods! The septa (internal dividing walls) of foraminiferal tests have holes that allow for the cytoplasm to flow between compartments, so that the cell can make use of all of the available space within the test. These openings—or foramina—also provided the name for the group: When initially thought to be cephalopods, they could be distinguished from all other coiled forms by the foramina between compartments.
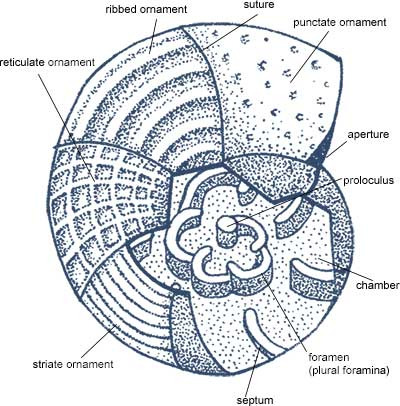
(Image: Cross-sectional diagram of a coiled, multichambered foraminifera. It does look a lot like a nautilus, and even has multiple chambers in its shell. However, unlike nautili, these chambers are connected by holes. [Source])
Not all multilocular foraminifera are coiled, however; many form more linear or globular shapes. Some are even star-shaped! Giants in their own right are found among the multilocular forms: the rotaliid genus Nummulites, though now smaller, has extinct representatives that could reach 15cm across, with up to 4300 distinct compartments. These lens-shaped forams make up the limestone that was used to build the Great Pyramids in Giza.

(Image: Fossil Nummulites shells being held by a human. They kind of look like pancakes, and are about 15cm/6in in diametre. Though you can’t see it here, they are actually coiled shells. [Source])
This post is the first in a multi-part series covering foraminifera—their anatomy, reproduction, evolutionary history, major groups, and geological applications. Later parts will be linked here, or check the “Foraminifera” tag on my blog!
#palaeontology#palaeoblr#foraminifera#biology#marine biology#microbiology#protists#long post#sunday long posts
272 notes
·
View notes
Text
How USG has helped in early diagnosis & treatment in infertility
How USG has helped in early diagnosis & treatment in infertility
Ultrasonongraphy (USG) is a useful and first line investigation used to assess the cause of infertility and to institute treatment accordingly. USG is an effective, safe, inexpensive, radiation free, non-invasive and readily available tool.
Role of ultrasound in female infertility
Ultrasound is used to evaluate the pelvic organs (uterus and ovaries), growing ovarian follicles, and cyclic uterine endometrial changes.
Evaluation of uterus :
A) Structural anatomy - Using both 2D and 3D ultrasound congenital mullerian anomalies can be diagnosed and classified according to ESHRE/ESGE classification of uterine anomalies.
B) Pathologies:
1) Fibroid : seen in 5-10% of infertile women. Distortion of the endometrial cavity, abnormal endometrial receptivity, altered hormonal milieu, and endometrial development are the causative factors for infertility in fibroids.
USG provides the number, exact location and size of fibroids, thus helps in thorough planning of surgical intervention if necessary.
2) Adenomyosis : Adenomyosis results in structural and functional defects of the uterine junctional zone and thus resulting in disturbed uterine peristalsis and sperm transport, increased inflammatory response in the endometrium causing impaired implantation. All these factors contribute to sub fertility and increased risk of miscarriage in Adenomyosis.
The ultrasonographic features of Adenomyosis are globular uterus, asymmetrical myohyperplasia, rain shower appearance and myometrial cyst.
Endometrium :
Is a dynamic structure undergoing cyclical changes. The endometrial pattern acts as an indirect measure of hormonal status during the cycle. Pathological features such as thin endometrium, poor endometrial blood flow, presence of polyp or intrauterine adhesions can result in sub fertility. And all these pathologies are accurately assessed using USG (both 2D + 3D).
Ovary :
USG is used for diagnosis and monitoring of treatment cycle in sub fertile women.
1) Follicular monitoring : Is an integral part of investigation in subfertile women. Serial scans during follicular phase evaluates the growth of the follicle, estimates the time of follicular rupture, the ideal time to trigger ovulation and occurrence of ovulation.
2) Antral follicular count: Estimated on day 2 of menstrual cycle, follicles of 2- 8 mm size measured and counted in each ovary. Diminished ovarian reserve diagnosed when AFC < 5. Early diagnosis of diminished ovarian reserve helps planning accurate treatment such as IVF, thus reducing time to pregnancy.
3) Endometriotic cysts :Endometriosis causes profound inflammatory response in the pelvis, affecting oocyte quality, sperm transport and function, luteinized unruptured follicle, defective corpus luteum, altered endometrial receptivity and also presence of adhesions results in sub fertility. Presence of unilocular cyst with ground glass appearance of the contents and peripheral blood flow are the USG features of endometriotic cyst.
4) Functional cysts : Thin walled, unilocular, anechoic cyst with minimal to absent blood flow. Functional cysts are unlikely to cause subfertility.
All these ultrasonographic features helps in early diagnosis and management of female infertility.
Role of ultrasound in male infertility
Ultrasound of scrotum evaluates abnormalities within the testis and the peritesticular structures, such as varicocoeles and epididymal abnormalities. Thus aiding in identifying causative factor for male factor infertility.
Transrectal ultrasound enables high-resolution imaging of the prostate, seminal vesicles and vas deferens and is the modality of choice in diagnosing congenital and acquired abnormalities implicated in the cause of obstructive azoospermia (OA).
Penile ultrasound is used to evaluate physical causes of erectile dysfunction, including structural penile abnormalities, problems with arterial inflow and malfunction of the venous occlusive mechanism.
1 note
·
View note
Text
Past Tense
read it on the AO3 at https://ift.tt/2ZeqEvd
by sexycazzy
Story Summary: by unilocular
When Tony left the team, he cut ties with Tim. It was entirely Tim's fault, even he admits that. Three years later, Tim has a chance to make it right when Tony returns to DC. Can he fix their friendship? Or is it too far gone?
Story links:
A03 ~ FF.Net
Words: 8, Chapters: 1/1, Language: English
Fandoms: NCIS
Rating: Teen And Up Audiences
Warnings: Creator Chose Not To Use Archive Warnings
Characters: Timothy McGee, Anthony DiNozzo
read it on the AO3 at https://ift.tt/2ZeqEvd
1 note
·
View note
Text
A woman’s risk for development of ovarian cancer during her lifetime is approximately 1 percent. Factors associated with development of ovarian cancer include low parity and delayed childbearing. Long-term suppression of ovulation appears to be protective against the development of ovarian cancer. Oral contraceptives that cause anovulation appear to provide protection against the development of ovarian cancer. Five years’ cumulative use decreases the lifetime risk by one-half. Risk-reducing salpingo-oophorectomy is not a practical choice for this patient with no family history, even once she completes childbearing. This option might be considered for a woman with a strong family history and the BRCA mutation.
BRCA1 and BRCA2 mutations are typically seen in cases of hereditary ovarian cancers. Overall, it has been estimated that inherited BRCA1 and BRCA2 mutations account for 5 percent to 10 percent of breast cancers and 10 percent to 15 percent of ovarian cancers among white women in the United States. Given this family history, it is highly likely that a mutation is present, and the affected individual (proband) should be tested if still alive. Because breast cancers are part of the BRCA mutation, the affected mother should be tested. Routine screening for ovarian cancer has not been established.
Functional ovarian cysts are a result of normal ovulation. They may present as an asymptomatic adnexal mass or become symptomatic. Ultrasound characteristics include a unilocular simple cyst without evidence of blood, soft tissue elements or excrescences. An endometrioma is an isolated collection of endometriosis involving an ovary. This would not classically appear as a simple cyst on ultrasound. Serous cystadenomas are generally larger than functional cysts and patients may present with increasing abdominal girth. Mucinous cystadenomas tend to be multilocular and quite large. Dermoid tumors usually have solid components or appear echogenic on ultrasound, as they may contain teeth, cartilage, bone, fat and hair.
The most useful radiologic tool for evaluating the entire peritoneal cavity and the retroperitoneum is computerized tomography. Specifically, in this patient, it would be important to look for significant involvement of the omentum. A chest X-ray provides adequate evaluation of the chest, unless it is abnormal. If there is a suspicion for chest involvement on the chest film, then a chest CT is necessary. With a normal colonoscopy and no symptoms suggestive of colonic obstruction, a barium enema would not be useful. PET scan, to date, has not been shown to play a role in the initial evaluation of women with a suspected ovarian malignancy. However, PET scan may play a role in evaluating women with a known diagnosis of ovarian cancer who have a suspected recurrence. An IVP would be useful if there was suspected ureteral obstruction, but otherwise is quite limited in assessing the entire abdominal/pelvic cavity.
The most likely diagnosis of the adnexal mass that would also explain the finding of endometrial hyperplasia would be a granulosa cell tumor (sex-cord stromal tumor). GCT are functional tumors that secrete high levels of estrogen, which can ultimately stimulate the endometrium to undergo hyperplastic changes and even lead to endometrial cancer. Approximately 25 percent to 50 percent of women with GCT will have endometrial hyperplasia on biopsy, and 5 percent to 10 percent will have endometrial cancer. Granulosa cell tumors represent 70 percent of sex-cord stromal tumors and typically affect women in their 50s (most common type is the adult GCT – 95 percent; the juvenile type affects females before puberty). The three main histologic sub-types of ovarian cancer include germ cell tumors (5 percent), sex-cord stromal tumors (1 percent to 2 percent) and epithelial tumors (90 percent). Germ cell tumors typically affect women of younger age groups (ages 10 to30), comprise 20 percent to 25 percent of ovarian neoplasms overall (benign and malignant) and account for 70 percent of tumors in this age group. Epithelial ovarian tumors are the most common and can affect women of all ages, but typically the malignant types occur in women in their sixth decade of life.
The five-year survival of patients with epithelial ovarian cancer is directly correlated with the tumor stage. The volume of residual disease following cytoreductive surgery is also directly correlated with survival. Patients who have been optimally debulked (generally <2 cm or <1 cm maximal residual tumor diameter) have a significant improvement in median survival. Histologic grade of tumor is important. Women with poorly differentiated tumors or clear-cell carcinomas typically have a worse survival than those with well to moderately differentiated tumors. This is especially important in early-stage disease. Tumor size, bilaterality and ascites without cytologically positive cells, are not considered to be of prognostic importance.
Although the only way to diagnose ovarian malignancy is by pathology, certain sonographic characteristics make cancer more likely. Complexity with solid components, size greater than 10 centimeters, mural nodules or excrescences, presence of ascites and bilaterality all increase the index of suspicion for cancer. Smaller unilateral cysts that are simple and unilocular or that have septations less than 3 millimeters are usually benign.
1 note
·
View note
Text
Hybrid Variant of Adenomatoid Odentogenic Tumour

Hybrid Variant of Adenomatoid Odentogenic Tumour by Shaju Jacob Pulikkotil in Biomedical Journal of Scientific & Technical Research (BJSTR) https://biomedres.us/fulltexts/BJSTR.MS.ID.000273.php
#biomedicalsciencejournal#Adenoatoid odontogenic tumour#Dentigerous cyst#Odontogenic tumour#Unerupted tooth#Unilocular
0 notes
Link
Visto primeiro no site: http://bit.ly/2LXRkrz
0 notes
Text
Research - Cells



The Human Body is composed of trillions of cells that provide structure, take nutrients from food, converts nutrients into energy and carry out specialised functions. Cells have there own parts each with a different function. Cytoplasm - it is made up of a jelly like fluid called the cytosol. Cytoskeleton - these are long fibres that make up the cells structural framework. It’s functions are to determine the cells shape and cell division, allowed the cells to move and also directs the movement of organelles within the cells. Mitochondria - these are organelles that convert energy from food into a form that the cell can use. Nucleus - this is the cells command centre which allowed the cell to to grow, mature, divide and also die. Plasma Membrane - this is the outer lining of the cell and it allowed the things to enter and leave the cell. Ribosomes - these process the cells genetics in order to create protein. There are many types of cells in The Human Body such as stem cells, bone cells, blood cells, muscle cells, sperm cells, female egg cells, fat cells and nerve cells.
Here is my Pinterest board that I have created. It includes photos of cells underneath microscopes and it also includes photographs of other artists work that have been inspired by cells. When I start to create samples I will look back at them and seek inspiration from them.
youtube
This video is an animation about the functions and molecular components of a human cell and it also shows how proteins and acids interact together. I believe that this video is extremely informative as it clearly visually shows what happens after conception.
Harvard Reference
St. Jude Children's Research Hospital. (2018). Beginnings of a Human Cell. Available: https://youtu.be/GdQBe2Efl9w. Last accessed 2nd March 2022.
Primary Research




In the library I found a book on cells and genetics. I found photographs and information on white adipose tissue, elastic fenestrated membranes, dense regular elastic connective tissue and unilocular fat cells.
Harvard Reference
John Adds, Erica Larkcom and Ruth Miller. (1999). Soft Connective Tissues . In: John Adds, Erica Larkcom and Ruth Miller Cell Biology and Genetics. England: Nelson Thornes. 122.
0 notes
Text
lupine publishers|Management of a Dentigerous Cyst in a 6-Year-Old Child –
A Case Report
Management of a Dentigerous Cyst in a 6-Year-Old Child – A Case Report

Abstract
Dentigerous cysts are epithelial in origin and most common odontogenic cysts. They are usually asymptomatic and hence
diagnosed on radiological examination. The standard treatment for these cysts is enucleation and extraction of the affected teeth.
This is a case report of a 6-year-old female patient with dentigerous cyst associated with a primary molar. The cyst was enucleated
and unerupted premolars were removed from the lower left region. The patient was given a fixed functional band and loop post-
surgical treatment. No recurrence was observed after 6months follow up.
Introduction
Cyst has been known to arise in man ever since he has teeth
and are also seen in certain animals. They are consequential, not
only because they often attain a large size but also produce facial
asymmetry, disturbance of dentition, neurological symptoms and
predispose the jaws to fracture but particularly because they have a
very high frequency of occurrence. Kramer in 1974 defined a cyst as
a pathological cavity having fluid, semi fluid or gaseous content but
not always lined by epithelium [1]. The dentigerous cyst is a type of
epithelial odontogenic cyst and is also called as ‘follicular cyst’ or
‘pericoronal cyst.’ It is the most common type of odontogenic cyst
which encloses the crown of the unerupted tooth by expansion of
its follicle [1,2]. A higher incidence of these cysts is usually found
in the second and third decade of life and slightly more common in
males. They account for 14-20% of mandibular cysts and between
15.2% and 33.7% of all odontogenic cysts. The frequency of these
dentigerous cysts in children is less and about 4-9% of these cysts
occur in the first 10 years of life [3]. They are predominantly
associated with third molars, maxillary canines and mandibular
premolars. Dentigerous cysts are often asymptomatic and are an
incidental finding on routine radiographs. In the radiographic
examination, the lesion has a well-defined sclerotic border, and a
well- demarcated unilocular radiolucency which is surrounding the
crown of an unerupted tooth. In some instances, these cysts can
grow to very large size and can trigger the inflammation, expansion
and erosion of the cortical bone. In such a case, they can generate
a differential diagnosis to an ameloblastoma or an odontogenic
keratocystic tumour.
The following case report describes the management of a
dentigerous cyst in a young child.
Case Report
A 6-year-old female patient reported to the Department of
Pedodontics and Preventive Dentistry, DY Patil School of Dentistry
with a chief complaint of pain in the lower left back region of the
mouth. On general examination, the patient was healthy without
any significant past medical history. Intra oral examination revealed
that the patient presented with a mixed dentition. The area of chief
complaint had deep occlusal caries with loss of crown structure in
relation with 74 and 75 (Figure 1). The primary molars were non
vital and adjacent mucosa was apparently normal, with no signs of
inflammation. An initial intra oral periapical radiograph was taken
for radiological examination. which revealed a huge radiolucency
with no signs of underlying premolar. Hence, a panoramic radiograph
was advised (Figure 2) and it revealed the presence of a well-
defined unilocular radiolucent cystic lesion with sclerotic border
enveloping the crown of mandibular left second premolar. The first
premolar was displaced medially while the second premolar was
apically displaced close to the lower border of the mandible. After
the clinical and radiological examination, a provisional diagnosis
of the dentigerous cyst was made. Surgical enucleation of the cyst
was chosen as the treatment of choice. The surgical intervention
was carried out under general anaesthesia. Blood investigations
(PT, PTT, INR) and cone beam computed tomography (CBCT) was
done prior to the procedure. Both the primary mandibular molars were extracted followed by opening of the mucoperiosteal flap
to disclose the cystic cavity. After the flap was opened, the cavity
was identified and 3ml of cystic fluid was aspirated. The cystic
lining enclosed both the premolars and hence were removed along
with the soft tissue. The flap was then sutured to close the wound
primarily. The specimen was fixed in 10% formalin and sent for a
histopathological examination. The histopathologic examination
confirmed the diagnostic hypothesis of a dentigerous cyst (Figure
3). The patient was followed up regularly for a month and was
advised to maintain good oral hygiene. When the lesion was
completely healed, prosthetic rehabilitation was done using fixed
functional band and loop
space maintainer (Figure 4)
Discussion
Dentigerous cysts are reported to be of two types –
Developmental and inflammatory. The developmental type is most
common and appears to be due to accumulation of fluid between
the reduced enamel epithelium and enamel organ. In rare cases,
the dentigerous cyst develops as a result of the intrafollicular
spread of periapical inflammation from an overlying primary tooth.
(Murakami et al 1995) [4]. Accordingly, in the present case, the
presence of overlying nonvital necrotic primary mandibular first
and second molars increase the possibility of being an inflammatory
type of the dentigerous cyst. The nature of the causative tooth,
size of the lesion and location influences the type of treatment
required for the dentigerous cyst which includes enucleation with
primary closure or marsupialization. Marsupialization of the cyst
is the treatment of choice which gives a chance to the unerupted
tooth to erupt in large cysts [3]. However, in the present case, the
cystic sac was surrounded by the unerupted premolar and was
firmly attached to it; hence, enucleation of the cyst along with
the extraction of premolar was carried out [5]. The histologic
examination of the specimen showed cystic lining composed of
reduced enamel epithelium which was 2-3 cell layers thick and
proliferative at some places. The outer connective tissue stroma
showed inflammatory infiltrate. The aspirated cystic fluid was pink
in colour and thick consistency. Correlating clinically, the features
were suggestive of dentigerous cyst. Owing to the age of the patient
and growth phase, it was decided to rehabilitate the patient with
a suitable prosthesis. Various options were considered and finally
based on the comfort and acceptance of the patient a fixed functional
band and loop was fabricated and cemented. This would restore
the occlusal function of lost primary teeth and will also maintain
the space till the time patient develops permanent dentition and
there is bone development for further fixed prosthesis [6]. For the
fabrication of the appliance, a conventional band and loop was
constructed. The acrylic teeth were placed in the edentulous area
of the cast and stabilized with modelling wax. The occlusion was
checked with the cast of the opposing arch and adjusted. Cold cure
acrylic was used to attach the poetic to the loop. The completed
appliance was then finished and polished. Trial fit was done in
patient’s mouth and checked for soft tissue irritation or occlusal
interferences and adjusted accordingly. The final cementation of
the appliance was done using glass ionomer luting cement [7]. The
patient was evaluated one week post cementation of the appliance
and no complications were reported.
Follow up
The patient was followed up for 6 months with no reports of
fracture of the appliance or food lodgment. Clinical and radiographic
examination did not reveal any signs of recurrence of the cystic
lesion.
Conclusion
Dentigerous cysts are rare in primary dentition and
asymptomatic, usually diagnosed during routine radiographs. The
sequelae of an untreated or undiagnosed cyst could be harmful to
the patient’s future dental development. Thus, regular check-ups by
the patient and close observation on the part of treating doctor are
essential. This results in elimination of pathology and maintenance
of dentition with minimum surgical intervention.
Financial Support
Nil.
Conflict of Interests
There is no conflict of interests.
for more information about Interventions in Pediatric Dentistry Open Access Journal archive page click on below link
https://lupinepublishers.com/pediatric-dentistry-journal/archive.php
for more information about lupine publishers page click on below link
https://lupinepublishers.com/index.php
#lupine publishers group#Interventions in Pediatric Dentistry Open Access Journal#occlusal#interferences
4 notes
·
View notes
Photo

The prickly pear is a unilocular fruit, with many seeds (polyspermic) whose weight can vary from 50 to 400 g. It derives from the inferior ovary adherent to the floral receptacle. Certain authors consider it as a false aril. Its color is variable according to varieties: yellow, red, white... The shape is also very variable, not only according to varieties but also according to the time of formation: the first ones are rounded, the later ones have a shape of more lengthened peduncle. The number of seeds is very high, about 300 for a 160 g fruit. use The taste is very sweet, very different according to the colors, and very appreciated by connoisseurs. It is best eaten very fresh. It can be used to make fruit juice or jam. The difficulty of its consumption comes from the picking and the cutting of the skin because this one is provided with glochides, tiny spines invisible to the naked eye but very aggressive and very difficult to remove. It is customary in many producing countries (Mexico, Peru, Tunisia, etc.) to have the skin peeled by the seller at the time of purchase (at no additional cost). In this case, it is peeled with a protective glove and a kitchen knife. This service is not usually included in supermarkets in northern countries, where it is sold with the skin (and spines) for conservation reasons, which reduces its appeal to the unseasoned consumer. #arganoil #skincare #beauty #argan #makeupartist #haircare #hairtreatment #organic #hair #arganoilserum #makeup #skincareroutine #faceoil #vitamine #essentialoils #purearganoil #natural #almondoil #naturalskincare #beautytips #arganoil #beautycare #skincareproducts #marrakech Link to the website 💻🛒✅: https://rosahuile.ma/ For more information contact the mailbox 📧✅: [email protected] https://www.instagram.com/p/CWL0bHzNvqI/?utm_medium=tumblr
#arganoil#skincare#beauty#argan#makeupartist#haircare#hairtreatment#organic#hair#arganoilserum#makeup#skincareroutine#faceoil#vitamine#essentialoils#purearganoil#natural#almondoil#naturalskincare#beautytips#beautycare#skincareproducts#marrakech
0 notes
Text
Biomed Grid | Cavernous Lymphangioma in the Mediastinum in an Adult Patient. Case Report
Introduction
Lymphangioma was first described by Redenbacker in 1828 [1]. It is rare benign congenital malformations involving focal proliferations well-differentiated of lymphatic tissue [2]. Probably represent embryological remains of lymphatic ducts, which arose from portions of lymphatic sacs that were hijacked during development or could not connect to the efferent channels [3]. Approximately 1% of all lymphangiomas are confined to the thorax, most commonly located in the mediastinum, where represent 0.7%-4.5% of all mediastinal tumors. [2] We present the case of an adult woman with cavernous mediastinal lymphagioma.
Clinical Case
Figure 1a: Tumor in contact with the innominate artery and the ascending aorta.
Figure 1b:Tumor in contact with the aortic arch.
Figure 1c: Tumor in contact with the right pulmonary artery
A 52-year-old woman with a history of diabetes mellitus, hypertension, heart failure functional class I, primary hypothyroidism, Cushing’s syndrome of pituitary origin, treated with bilateral adrenalectomy. During the follow-up of Cushing’s syndrome, presents intermittent painful, without dyspnea or weight loss. Computed tomography (CT), shows an oval image, lobulated contours, well delimited, homogeneous, with a density of 20 UH, which extends from the prevascular space to the upper and lower paratracheal of 4.1 x 3.2 x 5.7 cm. (Figure 1a, b, c ). After evaluation by the surgeon, surgery is decided. Performed posterolateral thoracotomy+ mediastinal tumor resection, we found in medium mediastinum a tumor of 7 cm, lobulated, cystic aspect related in the anterior side with superior vena cava, external side vein with azigos vein, and internal side with aorta. Report histopathology is cavernous lymphangioma (Figure 2a, b, c ).
Figure 2a: Multiple spaces corresponding to dilated lymphatic vessels are observed.
Figure 2b: Fibrous stroma, where groups of lymphocytes can also be seen.
Figure 2c: Vascular spaces are lined by flattened endothelial cells, which do not show atypia.
Discussion
Charruau L, et al. in a series of 9 patients, described according to the locations in the mediastinum, 2 patients with lymphangioma in the anterior mediastinum, 4 patients in right paratracheal location, 1 patient in subcarinal location, 1 patients in aortopulmonary location and 1 patient with lymphangioma located below the left hilum with extension to the posterior mediastinum [4].
Teramoto, et al. reported mean age in 36.4 years, range of 20-57 years, with a slight predominance of women, [2] according to Park J et al, the size of the tumor varies of 1.7 to 12.0 cm, with a median of 6.1 cm and incidence of 1 x every 70,000 cases / year [1].
Patients may present asymptomatically, cough and dyspnea may be observed due to extrinsic compression of the respiratory tract; it can also be observed stridor, hemoptysis, Horner’s syndrome, dysphagia, superior vena cava syndrome, constrictive pericarditis, phrenic nerve paralysis, or symptoms related to a secondary lymphangioma infection [2,5].
Histologically, lymphangiomas are thin-walled unilocular or multilocular cystic tumors lined by endothelial cells that contain a light-yellow fluid [6]. They are subdivided into three types according to the size of the lymphatic channels they contain, cystic, capillary and cavernous. Cystic lymphangiomas are the most common, and the cavernous type is relatively rare [2]. Cavernous lymphangiomas present indiscrete margins and insinuate themselves into the surrounding structures [5]. Immunohistochemistry staining for CD31 confirms the diagnosis of mediastinal cystic tumors, as well as positive D2-40 staining for the endothelium of the lymphatic vessels and positive staining of the epithelium with cytokeratin AE1/3. The cavernous lymphangiomas have discrete amounts of loose connective tissue compared with the cystic lesions, which may be covered with thick adventitia. The connective tissue stromas consist of varying amounts of smooth muscle cells in the form of a spindle, bundles of collagen, fibroblasts and lymphocytes. The presence of benign lymphoid aggregates is useful in the identification of lymphangiomas. The cellular components are generally well differentiated and lack cytological atypia [5].
On chest radiographs, lymphangiomas are observed as welldefined and round masses; unilateral or bilateral pleural effusions may be present. Computed Tomography (CT) shows a smooth, lobulated mass that can wrap and / or displace adjacent mediastinal structures. They usually have a homogeneous attenuation like water, but it´s can also have a greater attenuation or a combination of liquid, solid and fat. It´s can be loculated or multiloculated. In magnetic resonance imaging (MRI), a heterogeneous signal intensity can be observed in T1, while in T2, show a high signal intensity [4,7].
Surgery is often required to confirm the diagnosis and prevent complications arising from compression in vital structures [2]. Okubo T, et al. and Oshikiri T, et al. reported a complete resection avoids recurrences after surgery [8,9].
Park J et al, observed recurrences occur up to 33%, with a mean until the recurrence of 3.6 years, but recurrences have been observed up to 10 years after surgery. The reported recurrence was local and all cases when the complete resection was not performed due to its proximity to vital structures [1].
With respect to survival among patients with lymphagioma and the expected survival for age and gender, no statistically significant difference was found (P = .13) [1].
Several alternative treatments have been tried, including chemotherapy, radiation therapy, sclerosing agents and laser therapy. The efficacy of these treatments is very variable in the incidental reports [3,10].
Interest conflict
The authors declare no conflict of interest.

Read More About this Article: https://biomedgrid.com/fulltext/volume5/cavernous-lymphangioma-in-the-mediastinum-in-an-adult-patient.000973.php
For more about: Journals on Biomedical Science :Biomed Grid | Current Issue
#biomedgrid#american journal of biomedical science & research#journals on medical microbiology#physical medicine and rehabilation
0 notes
Last Seen Blogs

phalesnn-blog
phalesNN

ika-nas
AkiSiko

weirdlittlecorner
My Own Little Corner

pusinblood
I don't like eyes

kermitspussy
fish don't even think about me :/