#virginia medicaid expansion
Text
Erin Reed at Erin In The Morning:
Days after a landmark ruling in the 4th U.S. Circuit Court of Appeals that found medical discrimination against transgender people unconstitutional, the South Carolina Senate passed a broad gender-affirming care ban. The bill, House Bill 4624, prohibits gender-affirming care for transgender youth and also targets mental health providers. It forces teachers to out transgender students to their parents. It also includes an expansive public funding ban, prohibiting the use of public funds "directly or indirectly" for gender-affirming care at any age, potentially affecting the availability of all transgender care in the state. By doing so, South Carolina appears to be ignoring a ruling from the very court circuit in which it is located, just days after the decision was issued.
The bill states that “A physician, mental health provider, or other health care professional shall not knowingly provide gender transition procedures to a person under eighteen years of age.” The mental health provider portion of the bill was a heavy point of contention, with the ACLU of South Carolina interpreting it to cover at least some counseling for gender dysphoria. Though a later amendment was added that says it would not “impose liability on any speech protected by federal or state law,” the vagueness of the bill means that mental health providers who give out of state treatment locations to the families of transgender youth may still be targeted.
The bill also includes an extremely broad prohibition on public funding for gender-affirming care. It specifies that "public funds may not be used directly or indirectly" for such care, regardless of the recipient's age. This would eliminate Medicaid coverage, prohibit gender-affirming care under the state employee health insurance plan, and could potentially target any doctor or hospital that receives public funding. Notably, "indirectly" funding gender-affirming care could mean that any doctor providing such care might see state grants jeopardized. Such actions have already been taken against the Medical University of South Carolina, whose funding was threatened unless it ceased all transgender care in 2023. The hospital discontinued care for all transgender youth shortly thereafter. This provision, along with much of the bill, appears to come from the Family Policy Alliance’s model legislation, although it goes further than that model legislation in applying the ban to any age.
The bill seems to both directly and indirectly disregard a recent decision by the 4th U.S. Circuit Court of Appeals, to which South Carolina belongs. In that decision, a Medicaid ban on transgender care in West Virginia and a public employee health care policy ban in North Carolina were deemed unconstitutional. The court determined that gender identity is a protected characteristic and that medical discrimination infringes upon the equal protection rights of transgender individuals. Similarly, it ruled that Medicaid bans contravene both the Affordable Care Act and the Medicaid Act.
South Carolina shamefully decided to circumvent the 4th Circuit Court’s Kadel v. Folwell ruling by passing a bill (H4624) to ban not only gender-affirming care but also tack on a forced outing provision.
#South Carolina#4th Circuit Court#Gender Affirming Healthcare#Transgender Health#Anti Trans Extremism#Family Policy Alliance#Medicaid#South Carolina H4624#Kadel v. Folwell#Forced Outing
7 notes
·
View notes
Text
North Carolina on Monday became the 40th state to expand Medicaid under the Affordable Care Act, the latest sign of how Republican opposition to the health measure has weakened more than a decade after President Barack Obama signed it into law.
Gov. Roy Cooper, a Democrat, signed legislation expanding the state’s Medicaid program during a sunny afternoon ceremony on the lawn of the Executive Mansion, days after the Republican-controlled legislature gave final approval to the measure. He was surrounded by patients, advocates and some of the same Republican leaders who had previously blocked expansion in the state.
The bill will expand Medicaid to adults who make less than 138% of the federal poverty level, or about $41,000 for a family of four. State officials say the expansion will cover an estimated 600,000 people. It will take effect when the state adopts a budget, likely by June, Mr. Cooper said in an interview before the signing ceremony.
“Today is a historic step toward a healthier North Carolina,” the governor declared before signing the measure. When a reporter pressed him on when the expansion would take effect, he said, “It’s only a question of when, not if.”
It has been nearly 11 years since the Supreme Court ruled that states did not have to expand Medicaid — the government health insurance program for low-income people — under the Affordable Care Act. Nearly half the states opted out. More recently, progressives have helped to expand Medicaid in seven states — all of them with either Republican-controlled or divided governments — by putting the question directly to voters; in November, South Dakota adopted Medicaid expansion via the ballot box.
But getting Republican elected officials to abandon their opposition to expanding the program has not been easy. The last state where a Republican-controlled legislature voted to expand Medicaid was Virginia, in 2018. The governor at the time was a Democrat, Ralph Northam.
The battle over Medicaid has been particularly intense in North Carolina. Supporters of expansion conducted hundreds of “Moral Mondays” protests at the State Capitol. In 2014, the Republican mayor of a town that lost its hospital walked all the way to Washington to build support for expansion.
Monday’s bill signing leaves just 10 states — all with divided or Republican leadership, and most of them in the South — that have yet to expand Medicaid. Advocates say they now have their sights set on Alabama, where Gov. Kay Ivey, a Republican, can expand her state’s program with her own authority.
In North Carolina, there are various reasons for Republicans’ recent change of heart. Much of the opposition in the state and elsewhere has been both ideological and partisan — a reflection of Republicans’ deep distaste for Mr. Obama. But it is now clear that the Affordable Care Act, known as Obamacare, is here to stay. Republicans in Washington have been unable to repeal the law and appear to have largely given up fighting it, helping to pave the way for expansion in North Carolina.
“The argument that this is somehow an endorsement of Obamacare is losing a lot of political currency, even among conservatives,” said Frederick Isasi, the executive director of Families USA, a health care advocacy group based in Washington.
Hospitals, especially struggling rural ones, are eager for the extra revenue that Medicaid reimbursement will bring. The federal government picks up 90% of the costs of reimbursement under the expansion, and in North Carolina, hospitals will pay the other 10%. The state has revamped its Medicaid program, moving it from a fee-for-service program to one that relies on managed care — a long-sought goal of Republicans.
“This has been a long day coming, but it’s been as a result of a lot of reforms,” Tim Moore, the Speaker of the state’s House of Representatives and a Republican, said during the signing ceremony. The changes, he said, “allowed us to be in the position that we’re in today to be able to expand this coverage.”
For Mr. Cooper, who is in his second term and has been mentioned as a possible future Democratic candidate for Senate or even president, the bill signing was a significant victory. He sought to expand Medicaid when he first took office in 2017, and Republicans sued in federal court to stop him from doing it.
The push for expansion picked up steam last year, when the state’s House and Senate approved separate measures. But the two chambers were unable to reconcile differences.
The signing ceremony on Monday was at turns poignant and celebratory. Cassandra Brooks, who operates Little Believer’s Academy, a day care center in the Raleigh area, choked back tears as she recalled two of her teachers who had died, she said, because they could not afford health care.
“They were excellent early childhood teachers who didn’t have health insurance and passed away due to preventable health conditions,” she said. She cast the expansion measure as a boon to small businesses that operate on thin margins and cannot afford to offer their employees coverage.
“Here’s to Medicaid expansion in North Carolina,” she said. “Here’s to supporting small business in North Carolina. Here’s to continued growth in North Carolina. I believe in North Carolina.”
#us politics#news#the new york times#2023#expand medicaid#medicaid#obamacare#affordable care act#Gov. Roy Cooper#north carolina#Tim Moore
18 notes
·
View notes
Text
Tomorrow is Election Day. In Mississippi, Medicaid expansion is on the ballot. In Virginia, Kentucky, and Ohio, abortion rights are on the ballot. If you care about Medicaid expansion and keeping abortion rights, vote for Democrats!

0 notes
Text
..."The United States’ poverty rate experienced its largest one-year jump on record last year, with the rate among children more than doubling from 2021’s historic low of 5.2 percent to 12.4 percent according to new numbers from the US Census Bureau out today. They’re the latest data to reflect the devastating effects following the expiration of nearly all pandemic-era relief programs. That includes the end of Medicaid rules that protected recipients from getting kicked off because of administrative errors, an end to rental assistance policies, and the restart of student loan payments.
These policies might seem like a distant memory at this point. But they’re worth recalling with the arrival of every new report. Each demonstrates what happens when politicians long hostile to caregivers, universal health care, and the welfare state, for a brief moment, acted to create powerful, federally-backed safety net programs aimed at helping everyday Americans. One of the most effective programs to emerge was the expansion of the child tax credit, which provided families monthly checks of up to $300 per child and broadened eligibility rules for qualifying families. In turn, child poverty rates plummeted; the extra income allowed caregivers to quit grueling second and third jobs; parents were able to buy their kids decent clothes and help stop taunting at school. The Census Bureau previously reported that food insecurity dropped dramatically after just the first extended payment, from 10.7 million households reporting they didn’t have enough food to 7.4 million.
But as the pandemic receded, Republicans with the help of West Virginia Sen. Joe Manchin, who in private remarks reportedly warned that families were using the extra income to buy drugs, appeared to remember the country’s longstanding pre-pandemic hostility. Their opposition ultimately tanked President Biden’s agenda, and along with it, the brief life of the expanded child tax credit. That’s something worth remembering today as the predictable crowd is likely to cry about Democratic-engineered inflation."
0 notes
Link
0 notes
Text
The likelihood of experiencing pain differs greatly from state to state.

The prevalence of moderate or severe joint pain due to arthritis varies strikingly across American states, ranging from 6.9% of the population in Minnesota to 23.1% in West Virginia, according to a new study led by a University at Buffalo researcher.
The paper published in the journal PAIN is providing new insights — through its novel combination of individual- and macro-level measures — into geographic differences in pain and their causes.
The prevalence of moderate or severe joint pain due to arthritis varies strikingly across American states, ranging from 6.9% of the population in Minnesota to 23.1% in West Virginia, according to a new study led by a University at Buffalo researcher.
The paper published in the journal PAIN is providing new insights — through its novel combination of individual- and macro-level measures — into geographic differences in pain and their causes.
“The risk of joint pain is over three times higher in some states compared to others, with states in the South, especially the lower Mississippi Valley and southern Appalachia, having particularly high prevalence of joint pain,” says Rui Huang, a sociology PhD student in the UB College of Arts and Sciences, and the paper’s first author. “We also observed educational disparities in joint pain in all states that vary substantially in magnitude, even after adjusting for demographic characteristics.”
The percentage point difference in pain prevalence between people who did not complete high school versus those who obtained at least a bachelor’s degree is much larger in West Virginia (31.1), Arkansas (29.7), and Alabama (28.3) than in California (8.8), Nevada (9.8) and Utah (10.1).
“Education can function as a ‘personal firewall’ that protects more highly educated people from undesirable state-level contexts, while increasing the vulnerability of less educated individuals,” says Huang.
Nearly 59 million people in the U.S. have arthritis, and at least 15 million of them experience severe joint pain because of that condition. Severe joint pain is associated with diminished range of motion, disability and mortality.
While existing research on the social determinants of pain has relied primarily on individual-level data, individuals are embedded in social contexts, such as a specific U.S. state.
Different states can have dramatically different policies that affect many aspects of life including opportunities, resources and social relationships, which can in turn influence individuals’ pain, a potential influence that has gone largely unexplored in previous research.
“Very little research has examined the geography of chronic pain, and virtually none has examined the role of state-level policies in shaping pain prevalence,” says Hanna Grol-Prokopczyk, PhD, UB associate professor of sociology, and a co-author of the study. “We were excited to identify state characteristics that reduce residents’ risk of pain.”
The current study does so by combining data on nearly 408,000 adults (ages 25-80) from the 2017 Behavioral Risk Factor Surveillance System with state-level data about SNAP programs (formerly known as food stamps), Earned Income Tax Credits, income inequality, social cohesion (relationship strength among community members), Medicaid Generosity Scores, and tobacco taxes.
Although SNAP programs exist in all 50 states, some states offer more expansive benefits to qualifying residents than others. States with more generous SNAP benefits had a lower prevalence of pain. The same was true for states with greater social cohesion, indicating that both material resources and social functioning play critical roles in shaping pain risk.
“The increase in the generosity of SNAP benefits could potentially alleviate pain by promoting healthier eating habits and alleviating the life stress associated with food insecurity,” says Huang. “Social factors such as conflict, isolation and devaluation are also among the ‘social threats’ that can lead to physical reactions such as inflammation and immune system changes.”
In addition to providing new information on pain disparities across states, the paper might also fuel a reorientation of pain research that puts equal emphasis on macro- and individual-level factors, according to Huang.
“Chronic pain can — and should — be addressed through macro-level policies, as well as through individual-level interventions,” says Huang. “This study also implies that pain research in general should move towards a greater understanding of the macro contextual factors that shape pain and pain inequalities.”
“The risk of joint pain is over three times higher in some states compared to others, with states in the South, especially the lower Mississippi Valley and southern Appalachia, having particularly high prevalence of joint pain,” says Rui Huang, a sociology PhD student in the UB College of Arts and Sciences, and the paper’s first author. “We also observed educational disparities in joint pain in all states that vary substantially in magnitude, even after adjusting for demographic characteristics.”
The percentage point difference in pain prevalence between people who did not complete high school versus those who obtained at least a bachelor’s degree is much larger in West Virginia (31.1), Arkansas (29.7), and Alabama (28.3) than in California (8.8), Nevada (9.8) and Utah (10.1).
“Education can function as a ‘personal firewall’ that protects more highly educated people from undesirable state-level contexts, while increasing the vulnerability of less educated individuals,” says Huang.
Nearly 59 million people in the U.S. have arthritis, and at least 15 million of them experience severe joint pain because of that condition. Severe joint pain is associated with diminished range of motion, disability and mortality.
While existing research on the social determinants of pain has relied primarily on individual-level data, individuals are embedded in social contexts, such as a specific U.S. state.
Different states can have dramatically different policies that affect many aspects of life including opportunities, resources and social relationships, which can in turn influence individuals’ pain, a potential influence that has gone largely unexplored in previous research.
“Very little research has examined the geography of chronic pain, and virtually none has examined the role of state-level policies in shaping pain prevalence,” says Hanna Grol-Prokopczyk, PhD, UB associate professor of sociology, and a co-author of the study. “We were excited to identify state characteristics that reduce residents’ risk of pain.”
The current study does so by combining data on nearly 408,000 adults (ages 25-80) from the 2017 Behavioral Risk Factor Surveillance System with state-level data about SNAP programs (formerly known as food stamps), Earned Income Tax Credits, income inequality, social cohesion (relationship strength among community members), Medicaid Generosity Scores, and tobacco taxes.
Although SNAP programs exist in all 50 states, some states offer more expansive benefits to qualifying residents than others. States with more generous SNAP benefits had a lower prevalence of pain. The same was true for states with greater social cohesion, indicating that both material resources and social functioning play critical roles in shaping pain risk.
“The increase in the generosity of SNAP benefits could potentially alleviate pain by promoting healthier eating habits and alleviating the life stress associated with food insecurity,” says Huang. “Social factors such as conflict, isolation and devaluation are also among the ‘social threats’ that can lead to physical reactions such as inflammation and immune system changes.”
In addition to providing new information on pain disparities across states, the paper might also fuel a reorientation of pain research that puts equal emphasis on macro- and individual-level factors, according to Huang.
“Chronic pain can — and should — be addressed through macro-level policies, as well as through individual-level interventions,” says Huang. “This study also implies that pain research in general should move towards a greater understanding of the macro contextual factors that shape pain and pain inequalities.”
Visit our main website to learn more about our clinic, our medical professionals and our treatments.
Source: Science Daily
0 notes
Text
Virginia governor race national ad wars

Following the unsuccessful campaign, McAuliffe attended Georgetown University Law Center, where he obtained his Juris Doctor degree in 1984. After graduating, McAuliffe worked for President Jimmy Carter's re-election campaign, becoming the national finance director at age 22. In 1979, he earned a bachelor's degree from the Catholic University of America, where he served as a resident adviser. He graduated from Bishop Ludden Junior/Senior High School in 1975. His father was a real estate agent and local Democratic politician. McAuliffe was born and raised in Syracuse, New York, the son of Mildred Katherine (née Lonergan) and Jack McAuliffe. 3.3 Chair of the Democratic National Committee.3.2 2000 Democratic National Convention.McAuliffe left office with high approval ratings, though not as high as his immediate predecessors. During his final year in office, he responded to the Unite the Right rally in Charlottesville, condemning the rally and calling for the removal of Confederate monuments from public spaces throughout Virginia Northam began the removal of these monuments a few years later. As governor, McAuliffe focused heavily on economic development and restored voting rights to a record number of released felons. Because of this partisan division, he was unable to achieve many of his legislative goals, principle among them, Medicaid expansion, which was later enacted by McAuliffe's successor, Ralph Northam. Throughout his term in office, McAuliffe presided over a Republican-controlled legislature and issued a record number of vetoes for a Virginia governor. He ran for a non-consecutive second term as governor in the 2021 gubernatorial election but narrowly lost to Republican nominee Glenn Youngkin. In the 2013 gubernatorial election, after he ran unopposed in the Democratic primary, he defeated Republican Ken Cuccinelli and Libertarian Robert Sarvis in the general election. McAuliffe was an unsuccessful candidate for the Democratic nomination in the 2009 Virginia gubernatorial election. A member of the Democratic Party, he was co-chairman of President Bill Clinton's 1996 reelection campaign, chairman of the Democratic National Committee from 2001 to 2005 and chairman of Hillary Clinton's 2008 presidential campaign. Terence Richard McAuliffe (born February 9, 1957) is an American businessman and politician who served as the 72nd governor of Virginia from 2014 to 2018.
1 note
·
View note
Link
“Coverage starts Jan. 1 and the state said in mid-December that more than 180,000 people have been enrolled.”
21 notes
·
View notes
Link
Congratulations to the Virginians who will now be eligible for health care!
#medicaid expansion#healthcare#virginia#medicaid#health care#disability#actuallydisabled#disability rights#affordable care act
7 notes
·
View notes
Text
Daily Tweet: 5/30/18

Medicaid expansion will give 400,000 low-income people access to health coverage. This is a great day for Virginia.
#tweet#medicaid#medicaid expansion#virginia#health care#health insurance#medicine#poverty#terry mcauliffe#politics#liberal#conservative#democrat#republican
14 notes
·
View notes

Text
People voted for this:
"Miyares opposes increased gun-control policies and says gun violence should be solved by targeting criminals. [People should know what it means when Republicons say this.]
"Miyares also opposes abortion except for cases of rape, incest, and medical emergencies. He's voted against Medicaid expansion and a minimum-wage increase.
Virginia rejected this:
"During his tenure as attorney general, Herring fought to uphold same-sex marriage, decriminalize marijuana, and protect the state's environment. He also successfully defended the Affordable Care Act against a [t]rump administration challenge at the US Supreme Court.
"Herring told local TV station WJLA that he's running 'to continue the progress we've been making in Virginia.' His platform addressed building the economy, fighting for equality, tackling the opioid epidemic, and reducing gun violence."
Except that more Americans believe in Democratic policies. But they lacked the "enthusiasm" for actual support. Republicons turned out in more numbers than Democrats.
So the end result will be more hardship, cruelty, danger, strife, illness, ignorance, misinformation, and misery, because those are cumulative and state-favored when Republicons win.
It's also crucial to note that this year Virginia’s elections took place under Blue state voting laws, more open, fair, and honest by far than the repressive laws enacted by many Red states. Democratic voting laws are now at risk in Virginia.
It remains to be seen if, when Blue voters next feel like voting, whether it will be more expensive, difficult, and time-consuming, or in truth, whether there will again be a realistic opportunity to make their voices count as they had for this election, when they chose not to be counted.
13 notes
·
View notes
Text
Breaking Down Barriers Will Help Virginia Build on Medicaid Expansion Milestone
Over 300,000 newly-eligible adults have enrolled in health coverage through Medicaid, according to just-released data from the state. The Department of Medical Assistance Services (DMAS) automatically enrolling or expediting the enrollment of certain people, such as parents of children already enrolled in Medicaid, are likely part of this success. And partner organizations have strengthened enrollment efforts through outreach. Not only has enrollment been strong, but research has shown that the use of health services by the expansion population is strong as well. So far, 229,100 expansion enrollees have visited a health care provider, filled a prescription, or accessed some other health care service. Strong enrollment and high utilization make it clear: Medicaid expansion is working and meeting the demand for high-quality, comprehensive health coverage for individuals and families across Virginia.
DMAS has set up an information tool (Medicaid expansion dashboard) that provides a picture of who is benefiting from expansion. But what the tool does not capture is the benefit of expansion for Virginia’s children. Of all new enrollees, nearly 103,000 are parents. Because eligibility requirements are generally more generous for children than adults, if a parent is eligible, their children likely are too. As a result, engaging more parents in health coverage can lead to coverage gains for previously uninsured children.
A new report finds that while children’s enrollment in Medicaid/CHIP has declined overall in the United States since March 2017, Virginia has seen a 8.6% growth in children's participation in Medicaid/CHIP. Since the start of Medicaid expansion enrollment, child participation in Medicaid/CHIP has increased by 13,000. It’s likely that higher eligibility rates for parents will continue to result in better coverage rates for their children, and potentially better health outcomes.
Virginia is also seeing significant coverage gains for women due to expansion -- 60% of all expansion enrollees have been identified as female as of July 26, 2019. In particular, young women (ages 19 to 34) have accounted for nearly half (46%) of all female-identified new enrollees. This increased access to health care coverage could lead to better maternal and infant health outcomes -- not just for young women, but all women who may choose to have a child. This coverage is especially important for Black mothers, who are 3.4 times more likely than white women to die during pregnancy or within one year of pregnancy. There has been an increased focus statewide on maternal mortality, specifically addressing the heightened risk of maternal mortality for Black women. Gov. Northam has ordered an expedited enrollment process for expecting mothers applying for Medicaid, which should result in more people receiving health care earlier in their pregnancy. In addition, with expanded access to Medicaid, women are better able to assess their reproductive health and contraceptive options with a primary care physician.

Expanded access to coverage has also increased the ability to diagnose and manage long-term illnesses. Many new enrollees have chronic illnesses for which they can now access treatment, including 33,000 hypertension diagnoses, 18,800 diabetes diagnoses, 16,100 diagnoses for a substance use disorder, and 3,300 for cancer. There is also new evidence that access to Medicaid, and Medicaid expansion in particular, can improve racial disparities in the care of patients with cancer. Prior to the enactment of the Affordable Care Act, Black patients diagnosed with advanced cancer were 4.8 percentage points less likely to start treatment within 30 days of being diagnosed. But in states that have expanded Medicaid, they are accessing early treatment at nearly the same rate as their white counterparts. The success of Medicaid expansion has clearly led to Virginians’ ability to receive the health care they need.
But there is more work to do in providing health care access for all who call Virginia home. Data on new enrollees is still not broken down by race. Advocates need this data in order to evaluate enrollment and use of services by race, and to assess how well the state and care providers are doing when it comes to providing quality health care to patients of every race and health status. Availability of this data also affords us an opportunity to see what communities are in need of targeted outreach and enrollment efforts. Without expansion data by race, we won’t be able to see how these policies affect communities of color.
Other barriers to coverage remain, particularly for immigrants in Virginia. Virginia is one of only six states where a lawfully present immigrant must establish a 40 quarter work history, alongside the federal five-year requirement, before reaching eligibility for Medicaid. This is a clear barrier to coverage and prevents agency staff and community partners from making the most out of expansion and covering more people who have chosen to call Virginia home. Two companion budget amendments were introduced last year in the state House and Senate in order to remove this barrier but were ultimately not included in the final budget.
And new barriers will be erected unless policymakers change course. Virginia is currently waiting on federal permission to take health coverage away from people who do not report a certain number of hours worked each month. This, along with increased premiums for some Medicaid enrollees, will lead to tens of thousands of newly covered Virginians losing access to health care. Taking away Medicaid coverage for those who are underemployed or even have trouble reporting hours in order to retain coverage would make it more difficult for families to receive the services they need to stay healthy.
Securing health care coverage for over 300,000 people is a milestone worth celebrating. Unfortunately, there are policies that continue to actively prevent coverage for certain people. Advocates and stakeholders can continue strengthening enrollment with their successful outreach efforts and oppose barriers to coverage in order to make sure that everyone in Virginia has access to health care.
-- Kathy Mendes, Research Assistant, and Freddy Mejia, Policy Analyst
Print-friendly Version (pdf)
Learn more about The Commonwealth Institute at www.thecommonwealthinstitute.org
0 notes
Text
Emergency Department Information System Market Opportunity 2021, Industy Analysis, upcoming trends, research industry by 2027
Emergency Department Information System Market Synopsis :
As per the report published by Market Research Future (MRFR), the global emergency department information system market is set to thrive exponentially at a CAGR of 15.10% during the forecast period 2017 to 2023.

These systems are designed to enhance the quality of emergency services by taking care of functions such as clinical documentation, patient entry, patient and resource tracking, etc. It is presumed to gain popularity globally in the foreseeable future owing to the rapid developments in the healthcare sector.
One of the key factors responsible for dictating the future trajectory of the global emergency department information system market is the increasing geriatric population. Elderly people are always at a higher risk of developing diseases, and the increase in their population has necessitated the adoption of technologically advanced systems in the healthcare sector. This, in turn, has paved the way for emergency department information systems into the hospitals and clinics.
Other factors that are likely to complement the proliferation of the emergency department information system market include rising healthcare expenditure, growing patient pool, increasing need for advanced treatments, etc. In addition, the growing number of hospitals and clinics in the developing regions resonate strong potential for growth in the upcoming years.
Emergency Department Information System Market Segmentation :
On the basis of component, the global emergency department information system market has been segmented into software, services, and hardware. Furthermore, the software is sub-segmented into Best-of-Breed solutions and enterprise solutions.
On the basis of delivery mode, the emergency department information system market has been segmented into Software-as-a-Service and on-premise.
On the basis of the application, the global emergency department information system market has been segmented into clinical functionalities and administrative functionalities.
On the basis of the end users, the emergency department information system market has been segmented into large hospitals, medium-sized hospitals, and small hospitals.
Get Sample Report @ https://www.marketresearchfuture.com/sample_request/5926
Emergency Department Information System Market Regional Analysis :
The global emergency department information system market, by region, has been segmented into Americas, Europe, Asia Pacific, and the Middle East and Africa. Americas had the largest share of the market in 2016 and is poised to grow significantly over the next couple of years. The factors that are favoring the expansion of the emergency department information system in the region include consolidation of key players, accelerated adoption of novel technologies, technological innovations, etc.
Asia Pacific is set to strike a high CAGR of 15.71% during the forecast period. It is estimated to emerge as the fastest growing regional market towards the end of the assessment period. Factors such as rapid healthcare developments, strong economic growth rate, increasing count of healthcare providers, etc. are expected to augment the emergency department information system market in the region.
Europe is a significant growth pocket positioned at the second position in the marketplace. Meanwhile, the Middle East & Africa is anticipated to account for the least share of the global market. The slow growth rate is attributable to the slow economic development and low income.
Emergency Department Information System Market Competitive Dashboard :
Some of the key players profiled in the report are Allscripts, Cerner Corporation, Mckesson Corporation, Healthland, Inc, Epic Systems, Evident, Logibec Canada, T-System Inc, Siemens Healthcare, EPOWERdoc, Inc, Medical Information Technology, Inc, Unitedhealth Group, Inc, veEDIS Clinical Systems LLC, Medhost Inc, and Wellsoft.
Emergency Department Information System Industry News :
In August 2018, Allscripts Healthcare Solutions, Inc., a healthcare service provider, has achieved full accreditation for Allscripts PayerpathTM with the Healthcare Network Accreditation Program (HNAP).
In July 2018, Virginia has launched an Emergency Department Care Coordination Program where all of its emergency departments are electronically linked for improved care and trimmed costs.
In January 2019, the Centers for Medicare and Medicaid Services (CMS), a federal agency within the United States Department of Health and Human Services has initiated posting prices of healthcare services online.
Access Report Details @ https://www.marketresearchfuture.com/reports/emergency-department-information-system-market-5926
2 notes
·
View notes
Text
0 notes
Text
What You Need to Know About the Wave of Unconstitutional Abortion Bans in the States
Attempts To Ban Access to Safe, Legal Abortion Have Soared to an All Time High
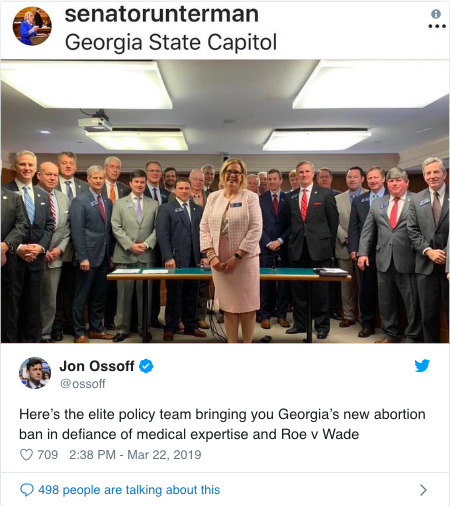
BREAKING: As this post was published, Georgia became the third state this year—after Kentucky and Mississippi—to pass a ban on abortion before many people know they are pregnant. The bill passed by one vote. Georgia is just one of 32 states to introduce abortion bans this year as part of a national strategy to outlaw safe, legal abortion.
2019 is barely one-fourth behind us, but one fact is clear: anti-abortion politicians have dropped all pretense of wanting anything less than a ban on access to safe, legal abortion.
In state after state, lawmakers have rushed this year to try to ban abortion access—at a point before most people even know they’re pregnant. These new laws run counter to long-standing Supreme Court precedents, and amount to an effort—in the wake of the confirmation of Brett Kavanaugh and other Trump judicial nominees to lifetime appointments—to invite the Supreme Court to overturn or eviscerate the finding, in Roe v. Wade, that access to safe and legal abortion is a constitutional right.
Abortion is health care. But with outrageous bill after outrageous bill—from six-week bans to attacks on crucial reproductive health services such as those funded by the Title X program—politicians have signaled an aggressive new phase in their attacks on reproductive rights.
Here’s what you need to know about this expanding attack on reproductive health care.
1. Opponents of safe, legal abortion are mounting a concerted campaign
News accounts have covered the laws advancing in state legislatures one by one—but when one steps back, a troubling pattern emerges. Through March of 2019, state lawmakers in Georgia, Kentucky, and Mississippi banned access to abortion at six weeks. Four other states—Missouri, Ohio, South Carolina, and Tennessee—stand poised to soon follow suit. Politicians have filed proposals for similar bans in eight other states: Florida, Illinois, Maine, Maryland, Minnesota, New York, Texas, and West Virginia.
2. A “six-week ban on abortion” = a ban on abortion
The rationales offered by politicians in support of six-week bans belie a simple fact: at the six-week point in pregnancy, most people don’t even know they’re pregnant. For those with regular menstrual cycles, such a ban would stop access to safe, legal abortion a mere two weeks after a missed period.
These unconstitutional laws would be awful enough if they stopped there—but they don’t. For instance, the six-week ban proposed in Georgia would subject a person to criminal liability for termination of a pregnancy—exposing a mother to the potential risk of criminal charges over a miscarriage. As a Georgia state senator who spoke out against this outrageous ban explained:
In other words, a pregnant woman who suffers a miscarriage could be subjected to criminal investigation, indictment, prosecution long before a jury is asked to determine whether she intentionally did anything to cause the loss. And if you think everything I just said was exaggeration or hyperbole, I read it directly from a Georgia court case where the implications of prosecuting women for seeking abortions was laid out in no uncertain terms.
youtube
3. Efforts to restrict or ban abortion are spreading quickly
Here’s a startling statistic: since January 1, 2019, lawmakers have proposed more than 250 separate restrictions on abortion in state legislatures across the country.
The six-week bans moving through states are part of this wave of anti-reproductive health legislation. The rate at which such unconstitutional bans have spread this year is without precedent:
Prior to this year, six-week bans were rarely enacted, as antiabortion activists and politicians publicly focused their efforts on other restrictions, like targeted regulation of abortion providers (TRAP) laws, that severely undermine access but are designed not to appear to be frontal assaults on abortion rights.
4. Low-income people and people of color are among those disproportionately affected
States where unconstitutional bans have advanced in 2019 are among those with the nation’s largest populations of people of color.
In Georgia, the nation’s eighth-largest state, nearly 10% of the population identifies as Hispanic or Latino—and a full 32% identifies as Black.
In Ohio, the nation’s seventh-largest state, 13% of the population identifies as Black.
In Mississippi, 38% of people identify as Black.
Median household incomes in those states — Georgia, Mississippi, and Ohio — fall below the national average. All three of them report higher poverty rates than the nation as a whole. Georgia and Mississippi have refused the federal Medicaid expansion funds offered under the Affordable Care Act—and both states have among the nation’s highest percentages of residents living without health insurance.
People in these states often already have to travel hundreds of miles, cross state lines, and wait for weeks to get an abortion—if they can access services at all. For many women, these barriers effectively ban abortion, and women of color—who already face significant barriers to health care and attacks on their bodily autonomy—bear the brunt of it.
This in part explains why these unconstitutional bans feel so infuriating and needless: in the states attempting to enact them, maternal health outcomes rank among the nation’s worst. Mississippi has the nation’s worst infant mortality rate, and Georgia has the nation’s worst maternal mortality rate. In both states—as in the country as a whole—African-Americans face a disproportionate share of the consequences of those public-health failures.
5. The goal: Permitting every state to ban abortion
The logic behind the rush to enact these unconstitutional abortion bans is simple: with senators confirming judges with views hostile to reproductive health and rights to the federal courts—including the Supreme Court—Roe v. Wade is at risk like never before.
Trump has installed more federal appeals court judges in his first two years than any other president—and has installed as many Supreme Court justices in two years as President Obama installed in eight.
Trump promised as a candidate to choose judges who would “automatically” overturn Roe, and has worked since to keep that promise. Trump nominee Brett Kavanaugh has already acted to restrict access to abortion during his brief tenure on the Supreme Court—writing to say that courts should let a state proceed with abortion restrictions that that were ruled unconstitutional just a few short years ago.
That explains why a state like Mississippi, which courts blocked from enforcing an unconstitutional 15-week ban in 2018, would advance an even more stringent ban on safe, legal abortion a year later. Anti-abortion politicians believe that Trump’s judicial nominees may overturn Roe v. Wade—and intend to test just how far judges will let them go to restrict people’s ability to access their constitutional right.
There have been more than 250 abortion restrictions introduced in this country since January.
Pair those with the effort to undermine Title X—the nation’s only program dedicated to affordable reproductive health care—by gagging doctors from referring patients to abortion services, and the pattern is undeniable. Even as seven in 10 Americans consistently say they favor abortion access, opponents of safe, legal abortion think they can achieve a ban on abortion nationwide within the next few years.
These attacks are only the beginning. We can count on politicians to introduce unconstitutional abortion bans in other states. It’s up to us to stand united against this unprecedented effort—and to fight back.
5K notes
·
View notes
Last Seen Blogs

romancevsreality-blog
romance vs. reality.

geopneumapyrohydrologist
On The Study & Practice Of Magick.

od-uw-spl
SPL Directed Fieldwork

puckingbeautiessss
Pucking Beauties!

john-boards-blog
Untitled