
trans-axolotl2
backup blog!
main is @trans-axolotl this one is a backup :) since I’m shadowbanned I message and sometimes reply from here!
83 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs




Text
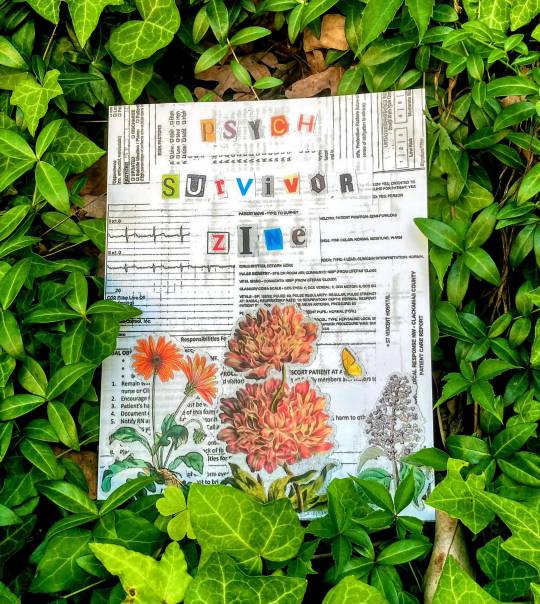
Image description: [ a photo of the Psych Survivor zine in a bush of ivy. The cover is a collage made out of medical records, vintage flower drawings, and magazine letters spelling “psych survivor zine".]
Hello everyone! I am so thrilled to announce the launch of the psych survivor zine, now available to download on www.psychsurvivorarchive.com.
A little bit about this project:
The Psych Survivor Archive is an abolitionist organization deeply invested in mad liberation and cross-movement organizing.
We host two projects: the Psych Survivor Zine and the Digital Story Archive. The Psych Survivor Zine celebrates Mad art in volumes released twice a year, with thematic prompts for each edition. The Digital Story Archive is a more informal forum for psych survivors to write about our lives and share as much as we want, when we want, how we want.
Through this archive, I hope to create a platform where psych survivors are believed and the psych system is held accountable for the ways it has harmed us. Our pain, resistance, knowledge, and grief are worth listening to, and I offer up this archive as a communal method of bearing witness.
This space is for the imperfect crazy person, the noncompliant patient, those of us who trash our rooms in the psych ward and yell to ourselves on the street. This space is for our comrades still incarcerated in all kinds of institutions and prisons. This space is for anyone who has been harmed by the psychiatric system and wants to rage about it–and this space is for anyone who doesn’t have the words to talk about it.
This space is for you.
You can download a pdf and an image described pdf for free on the website, or order a physical copy for printing! This zine is incredible-featuring artwork by 13 different Mad artists, the 55 page zine includes collages, poems, harm reduction toolkits, and more!!
Artists include @kihnindewa, @bioethicists, and @librarycards, among many more!
This project has been really vulnerable and cathartic with me, and I am so excited to share it with you. Feel free to explore the website, submit your story, and check out our resource guide.
870 notes
·
View notes
Text
one of the things we talked about in harm reduction training today was learning how to fuck up better. We've been spending a lot of time talking about the power dynamics of nonprofit direct service work, especially when it comes to providing noncoercive and nonjudgemental service. today our facilitator said that the point of the skills she was teaching us was not for us to never do the wrong thing; the goal was to learn how to fuck up better so that when we do inevitably make mistakes, they're mistakes that will cause less harm and leave less damage.
And I just really like that. The goal isn't perfection, it's to learn how to fuck up better.
131 notes
·
View notes
Text
#intersex#actuallyintersex#i will just do the math and get the accurate results by taking the dyadic people out of it#<3
29 notes
·
View notes
Note
hi, I really like your blog and your antipsych thoughts have been very helpful to me. i hope this is ok to ask for advice (sorry i have brain fog and this question is vague)? i think i'm looking for 'unconventional' advice or suggestions, the kind that someone in the psych system would not necessarily recommend to me.
i have had a bad history with therapy, but i very much need some kind of mental support that i am not getting otherwise in my life (issues like CPTSD, DID, among other things). im in a position where i /can/ go to therapy, and i've been with a therapist that specializes in the things that are causing me the most problems for a year and theyre fine (i.e. has not ever helped me figure out anything about how to improve my life but has been someone who can perscribe me stuff, and hasn't done anything actively harmful to me like other therapists and psychiatrists have), but going is so upsetting for some reason (maybe because the therapy environment has been so bad in the past?) and not at all helpful. it's useful for me to have a relationship to a psychiatrist/therapist for medication and other 'navigating the system' reasons, but it's absolutely unhelpful. i am very frustrated and disillusioned with the whole concept of 'therapy' in general (maybe due to my history)!! but i don't know how else to get help!
it's harder because of the brain fog. i also feel very isolated partially because i'm in a not great environment, and partially because i have multiple mental illnesses in addition to not being a very nice person. i have felt really let down by supposed friends i've come to for help who just said therapy speak stuff like 'you should get help....' and 'sorry i don't have the emotional bandwidth to help <3' and stuff like that. it really makes me feel like i'm too messed up to be able to ask for help from regular people and i have to go to the psych industry but of course i've already been failed by them too :(
hey anon!
I think what you've said makes so much sense. I feel like we're so often told "go get help" but when we do try to seek support, it isn't as simple as just going and easily finding a therapist who is able to provide all the support and care we need. It can be so hard to find and pay for therapy in the first place, harder still to find someone who specializes in a therapy style to meet our needs, and sometimes we might not just be in a place in our life where we are in an environment that allows us to do in depth therapy work. And I just want to say that it isn't your fault if therapy isn't meeting your needs right now--that doesn't mean that you're failing at therapy. You absolutely aren't alone in feeling dissatisfied with therapy and wanting other options.
For me, what's helped when I've been considering making changes about how I approach my mental health has first been sitting down and really taking a thorough look at what things are working and what things aren't working. It seems like you've done a lot of that already--you know that it's helpful to have a therapeutic relationship to get meds and for help in the system, you know that the therapy environment hasn't been particuarly helpful for other types of healing work, and it seems like another thing you're thinking about is how to get mental support from your friends and other people in your everyday life. I think those are really good starting places to consider where you want to go from here. It might be helpful to make a list of what feels like priorities to focus on right now--do you want to develop more skills for navigating crisis? Do you want to focus on changing your relationship with dissociation? harm reduction for self destructive behaviors? building resilience and cultivating relationships in your life? There's no right or wrong answers here--you're going to be the expert on what feels most important right now.
I also just want to say that I think it's really shitty when we're made to feel like we're too crazy or too needy or too messed up to be able to be cared for and supported in our community. I've definitely had people tell me that, and it really hurts and makes me feel hopeless, like I'm always going to be struggling and that there's no chance that I'll be able to get better. But fuck that. We deserve to have meaningful connections in our community, access to resources that help us, and to be able to build resilient relationships where getting emotional support isn't considered an unmanageable burden, even if we're mad/mentally ill/ neurodivergent. I'm sorry that you haven't been able to rely on your friends and community that way, although I know it's hard when everyone we know is struggling and people don't have the energy or skills or knowledge to be able to help each other.
This is getting long, so I'm just going to list off a ton of random tips and suggestions, and I hope some of them might resonate with you.
Join a peer support group aligned with antipsych values. Hearing Voices Network, Alternatives to Suicide with the Wildflower alliance, Multiplied by One, FEDUP trans/intersex eating disorder support groups are all great options.
harm reduction! this can be especially applicable for self-destructive behaviors, but just in general moving outside of an "abstinence-only model." working to understand your actions on a spectrum of totally chaotic, unmanaged behaviors to more managed, intentional relationships with those behaviors. embracing any positive change as an important step instead of self-blame and all-or-nothing thinking.
Trying to think of the best way to describe what I'm thinking here, so I might not have the best phrasing. But basically, spending time separating your ideas for what wellbeing and quality of life look like for you from the psychiatric system's ideas of what a "normal," "healthly," quality of life looks like. For me, this looked like realizing that I wasn't actually interested in getting rid of all my hallucinations, but instead I just wanted to lessen the distress I experienced and find a way to hallucinate without panicking. So I guess just in general--really exploring what is actually important to you for your wellbeing and not limiting yourself to mainstream definitions of "recovery."
Unconventional coping skills, or coping skills that traditional psychiatry deems "risky." I've talked with some people who things like getting tattoos and piercings are actually incredibly healing for them, and are an important part of their "therapeutic" journey. Not going to go into detail or promote other "risky" coping skills on Tumblr lmao, but more just say that it's okay if there's things that therapists view as risky that you might have another perspective on how it fits into your personal healing.
Building up your and your loved ones capacity for community care. This can be a really hard one, because I know it always frustrated me when I would see people talking online about how great things like care webs or the power of peer support when I just didn't have any of that in my physical everyday life. So I'm not just going to put this here like it's a magical solution or something that's easy to accomplish. It's something that can take a ton of work and we're allowed to be frustrated about that. I think one strategy that helped me with this was spending a lot of time building my own understanding of my own capacity to help, my own needs, and what ways I would like to be cared for. That helped me start small, just by having conversations with my loved ones when I wasn't in crisis and saying "Hey, this is how I would like things to go when I'm in crisis. This is something that helps me when I'm hallucinating. This is a way you could let me know that you can't support me tonight but still leaves room for us to have connection. This is how I can help you. Let's talk openly together and develop and practice how we want to care for each other." Starting with just one person and one conversation really went a long way for me in terms of eventually building up an actual support network and for me was super instrumental in healing work.
Setting out an hour a week that's my "self therapizing time." just using one hour a week to look up new resources, try out new skills, journal, do self-inquiry, participate in activism, do something that brings me joy, read something new about mental health, literally anything that feels intentional in that hour. trying out a lot of new things and quitting a lot of new things!
Incorporating your physical needs. I'm sure we've heard a million times things like "get sleep, nourish yourself, go outside," and all that is great but often feels fucking impossible when we're mentally doing not great. but I guess just saying it can be good to be aware of how our physical body impacts our mental health in other ways. things like trying to get our sensory needs met, embracing movement that feels good + making space for rest, embracing things that bring our physical body pleasure whether that's tasty food, sex or other kinds of physical intimacy with other people, if it's using substances in a way that feels helpful or joyful or fun--anything really!
Here's a bunch of random orgs and resources that I have found helpful: Fireweed Collective, Wildflower Alliance, Project LETS, Mapping our Madness, Mad Survival Tools, Organizing Guide for Psychiatric Survivors, MindFreedom Resources, Multiplied by one (I can't personally vouch because I haven't been to their groups, but I have a friend with DID who attends these groups and had positive things to say about them.)
I'd also add on this book: "Psychosis, Dissociation, and Trauma: Evolving perspectives on Severe Psychopathy" although I do want to give a warning that this book is a heavy academic text that has a lot of clinical and stigmatizing language. For me, it had some helpful information that helped me make connections between my experiences of trauma, dissociation, and psychosis, but I would not recommend reading it unless you feel like you're in the right headspace and can deal with wading through a lot of the psychiatric narrative.
These are all just some things that sometimes work for me, so please feel free to disregard anything that doesn't resonate with you. I'd also love it if followers could add on with any tips, resources, any "unconventional" advice!
thanks for reaching out, anon, and I hope you have a good night 💜
68 notes
·
View notes
Text
this is a survey and i'm very interested to see the results so please reblog after answering!
(also everything with two or more pronouns in one option is in any order of preference)
#once again reminding people that he/she is often used as a derogatory term towards intersex people and transfem people#and that listing out pronouns as she/he. he/her. any way of listing them#is an easy way to show a little consideration for#intersex people who r going to be navigating spaces and terms and our relationship with feeing safe in trans spaces
7K notes
·
View notes
Note
hi! What is peer respite?
hi anon! I love talking about peer respite :D
Peer respite is a community-based alternative to psych wards. They offer 24/7 short term crisis stabilization-usually for around a week to 2 weeks. Unlike psych wards, they are completely voluntary and all the staff are people with experience with mental health/extreme states/being in the mental health system. Staff are extensively trained in peer support and mental health first aid, and oftentimes staff members will have other degrees in mental health or healthcare related fields. Usually, peer respite is in a house and it is a homelike environment where you can leave at any time, can have visitors, can have your phone, and can bring comfort items and preferred activities. At peer respites, there are no restraints used, no strip searches, and no solitary confinement.
Each peer respite is a little different, but I can tell you about one that my friend works at who is a social worker with lived experience of psychosis! When people decide to come to the peer respite, they usually make a plan for how they want their stay there to look like. Peer support workers will lead optional life skills/coping skills groups throughout the week, as well as other group activities for anyone who wants to participate. There is self-advocacy education, crisis planning options, and art wellness activities. Everyone is assigned a personal support worker who they can go to any time they need a check in or one-on-one support. Staff and guests work together to cook meals, and the entire stay is free of cost.
Since peer respite is an alternative to the psychiatric systems, most peer respites do not provide traditional therapy or psychiatric medications. Most peer respites will work with you to set up outpatient therapy services if you're interested, and I know a lot of people who continue to see the outpatient providers that they already have throughout their stay at peer respite.
A lot of people who go to peer respite have really positive experiences, and there's been several studies done looking at the outcome of crisis stays at peer respite. A lot of people speak positively about the homelike environment, being able to get emotional and crisis support without the fear of institutionalization, and being able to have autonomy about what your days look like, what choices you make, and what healing looks like to you. Some people stay at peer respite and are still able to go to school or work for the week while knowing that they have a safer environment to go back to.
Peer respite is not a perfect solution for everyone's experience of crisis. If you need a longer term stay, are looking for immediate clinical therapy, are someone who is searching for immediate medication support, or who needs immediate physical medical care--peer respite might not be able to meet your needs. Each peer respite house is going to be different, have different staff and visitors, and different policies, and some people might just not feel comfortable in a particular peer respite house. It's shitty and I hope this changes, but some peer respite houses are inaccessible, will have policies around drug use that might prevent people from staying, or have policies that prevent people who are homeless from staying. So, peer respite definitely isn't a perfect solution or something that can meet everyone's crisis needs, but is a really cool option that I hope continues to become available in more states.
Here's a directory with links to peer respites in the US, and here's research done about peer respite!
#antipsych#peer respite#save#sorry for double reblogging my own posts#since being shadowbanned im so paranoid im going to be deleted that now i want to save things on here
2K notes
·
View notes
Text
In my last residential treatment stay, I did have one psychiatrist who I trusted and had a positive relationship with. Her name was Dr. R, and when I came in on the first day of treatment and told her that I would not take any psych meds and that I had a lot of past psych trauma, she validated me and told me that she would not bring up meds unless I did. Throughout my stay there, she was empathetic, listened to my concerns, helped advocate for me, and generally made me feel heard. At the same time, when management took away our doors-she did nothing. When I needed to get a feeding tube--she lied to me about how long it would be in, and what I needed to do to get it out. She enforced policies about restricting outside breaks, restrictions on items, and contributed to treatment plans that my friends felt were unfair and damaging.
She was a good person and I liked her, but she was choosing to work within a system where she could not control the dozens of things happening there that harmed us every single day. This is what I mean when I say there is no such thing as a good psychiatrist in inpatient units--she was a progressive, validating, nice person --but her very job description made it impossible for a “good provider” to exist. To be a provider who wasn’t a part of the harm that was occurring on that unit, she would have had to quit, because the very requirements of her job required committing ethical violations, restricting peoples autonomy, and perpetrating iatrogenic harm. If she had stopped enforcing harmful policies and challenged her coworkers publically, she probably would have gotten fired. And that really is the problem--causing iatrogenic harm has essentially become a job requirement on inpatient units, and being a “good provider” by the metrics of the system require you to participate in that harm.
I think Dr. R did a better job than most inpatient psychs in mitigating the harms she participated in, and finding ways to resist shitty systems when possible. I was glad she was there and I think she made my treatment better, but the two of us had a lot of conversations together where she acknowledged the fucked up things happening in the treatment center, acknowledged her role in them, and also stated that she did not have any power to change them. She could not fix the system by working within the system.
I get a lot of questions by people who are interested in careers in the mental health system, and asking me on whether I think it’s okay for them to work there. My first response is usually if you’re asking because you’re feeling guilty after seeing what psych survivors say, I’m not someone who’s going to give you permission to ignore that guilt. The second thing I usually say is this: you need to go into this job aware with the fact that you will cause people harm, you will get into ethical dilemmas, and there will be times where you will either have to betray your personal values or quit. There isn’t one right answer on how to engage with mental healthcare as a provider, with the reality that until we build up alternative systems of care, the current structures still exist and have people who need support inside of them. If that’s something that you think you can navigate in a way that lets you create the least harm possible, then that’s something you need to decide for yourself, and to think really deeply about if the reality of the psych system matches up with your goals.
#antipsychiatry#antipsych#mad studies#disability justice#psych ward tw#i think u also need to understand that if u go to school to work professionally in mental health#if u become a psychiatrist or a therapist or a social worker#even if you're one who does it outpatientt. even if you're an abolitionist social worker#that means there are probably going to be barriers to community spaces. that some people might not trust you any longer. if you are#coming into spaces as a professional#part of that decision might be grappling with the fact that even as you gain legitmacy from a societal side. that as u gain#new opportunities for jobs. to work within systems#you might also lose community trust. opportunities within activism spaces. opportunities#to share and be in those spaces as a survivor and patient#and im not saying this as a judgemnt or to put moral value on it#but i think that's just something you Also need to understand and weigh. sure you will gain something. by getting liscenced#but what will you lose? why might people not trust you in community spaces any longer?#what trade offs will you be making and are they worth it to you? what new communities can you build#what matters to you and what are your passions#<- all things i am really grappling with right now as i decide whether or not i want to go get my masters in social work
134 notes
·
View notes
Text
And here’s the thing. I have met professionals who have deeply thought about all of those questions, directly grappled with the harm they cause patients in this system, and really intentionally shaped their practice based on their understanding of the ethical dilemmas they face. I’ve met providers who take responsibility for their role, and still choose to stay in their positions because they believe having a position within the system helps them mitigate some of the harms of their colleagues, and that the help they provide outweighs the harms they are causing. I can’t say that I agree with these professionals, or that I would make the same choices, but I can say that the professionals who actively recognize the ethical violations inherent in the practice of psychiatry and work to build their value system around that knowledge—those are the only professionals that have ever listened to my input and insight. Those are the only professionals in inpatient wards who were able to mitigate some of the damage I was facing while locked up, and the only professionals I was able to conditionally trust.
I’m not sure I believe there is a “good psychiatrist,” but I can say with 100% certainty that entering into the field believing that you’re “one of the good ones” who doesn’t have those same ethical issues that crazy people online complain about—that’s a way to guarantee that you will be ignorant of and complicit in all the ethical violations happening in your workplace. If you really want to be able to support, connect with, and actually help mad/mentally ill/neurodivergent people, the first step might be to acknowledge you’re entering into a harmful field that does not line up with your stated goals.
So annoyed with psychiatry students that I’ve seen lately who reply to posts attacking the DSM in order to claim that “all of their professors criticize the DSM and none of us in the profession like it these days!” This is such a blatantly false statement it almost makes me laugh. Firstly, many, many professors still glorify the DSM and teach it uncritically—I’ve been in classes with many professors who love the DSM! Secondly, even if you have one class that criticizes the DSM, the DSM and ICD is still the operative paradigm through which psychiatry operates in the United States—look at diagnostic codes, billing codes, and just how the whole fucking system operates—even if you criticize the DSM, psychs are still engaging with and offering legitimacy to the medical model of psychiatry. Thirdly most of us have so many issues with psychiatry beyond just the DSM, and the DSM is just a a reflection of the larger dynamics of power and control. So even if you are a psych who is critical of the DSM, there’s still probably a million other things you do that participate in a system that harms mad/neurodivergent/mentally ill people.
if you constantly feel the need to justify that you’re “not like everyone else in your profession” maybe consider what that means about the system you work in, the ethical dilemmas you are 100% going to face when you try to work within that system, and whether the personal values you are going to have to betray are worth the benefits you might bring to people.
#and that’s all I have to say about ppl who ask me if they’re bad for going into the mental health field#like I don’t know. i can’t tell you. if you’re asking other ppl those questions#might be a sign you’re not ready to navigate that field in a way that reduces harm
420 notes
·
View notes
Text
So annoyed with psychiatry students that I’ve seen lately who reply to posts attacking the DSM in order to claim that “all of their professors criticize the DSM and none of us in the profession like it these days!” This is such a blatantly false statement it almost makes me laugh. Firstly, many, many professors still glorify the DSM and teach it uncritically—I’ve been in classes with many professors who love the DSM! Secondly, even if you have one class that criticizes the DSM, the DSM and ICD is still the operative paradigm through which psychiatry operates in the United States—look at diagnostic codes, billing codes, and just how the whole fucking system operates—even if you criticize the DSM, psychs are still engaging with and offering legitimacy to the medical model of psychiatry. Thirdly most of us have so many issues with psychiatry beyond just the DSM, and the DSM is just a a reflection of the larger dynamics of power and control. So even if you are a psych who is critical of the DSM, there’s still probably a million other things you do that participate in a system that harms mad/neurodivergent/mentally ill people.
if you constantly feel the need to justify that you’re “not like everyone else in your profession” maybe consider what that means about the system you work in, the ethical dilemmas you are 100% going to face when you try to work within that system, and whether the personal values you are going to have to betray are worth the benefits you might bring to people.
420 notes
·
View notes
Text
i should say in terms of antipsychiatry its very funny to me that people use psychosis or more specifically schizophrenia as a “gotcha”, like theres an expected reaction of “oh wait you’re right Real crazy people dont deserve autonomy & to not have to endure abuse” (which of course just reflects how people that defend psychiatry view us) + especially when theyre against social understandings of mi, the (incorrect) assumption that schizophrenia is, objectively, the most wholly biological mental illness despite the absolutely massive amount of evidence to the contrary (everything from the mildest biopsychosocial approach to diathesis-stress to the traumagenic neurodevelopmental model of psychosis: no one in this day and age believes it is “wholly biological” if they arent trying to sell you $900 antipsychotics)
… like at least in my experience, people diagnosed with/psychiatrized as schizophrenic know the material harm that comes from being stripped of your autonomy. like we know what its like to have all of our experiences disbelieved and seen as completely irrational and to have our problems with treatment brushed off as psychotic and delusional, i dont know a single person diagnosed with schizophrenia that hasnt been coerced into taking medication they didnt want to take, oftentimes in the context of hospitalization under the threat of not being released unless they did. and ill take that a step further and say we know what its like to have people, especially professionals, use our diagnoses to justify abusing us, because if you believe that schizophrenic people shouldnt have control over their own treatment, and usually by extension, lives, because theyre too paranoid, delusional, incoherent, etc. - this is what you advocate for: abuse
3K notes
·
View notes
Text
Just for anyone still thinking the civil rights movement was “SO long ago!”
Fred Hampton would be 51 this year if police hadn’t executed him at age 21.
Ruby Bridges is 65.
MLK would be 91 (he was assassinated at 39).
Malcom X would be 95 (he was assassinated at 39).
Claudette Colvin (the first Black woman known to refuse to give up her seat AT 15) is only 80.
Mary Louise Smith is 83.
Fred Gray is 89.
EMMETT TILL WOULD BE 79 (he was murdered at age 14 because of a white woman’s lie).
Ask yourself how old your grandparents are. Hell, how old your PARENTS are. How old are the people in most government seats right now?
Miss me with that bullshit of “It’S sO lOnG aGo. Things are better now.” These people and so many more who aren’t able to be here would be distraught at what is STILL fucking happening today. To say things like that is just willfully turning your head away from the injustices that we see today! That’s the that on that.
65K notes
·
View notes
Text
By the way. Before you rush to get a professional diagnosis for a Brain Thing you should really weigh your options. Like do you just want to "prove it" or will this actually give you access to treatment you can't have otherwise? Are the treatment options available worth having the government know you're neurodivergent? Because sometimes it's better to keep things off the record because unfortunately we still live in a very deeply ableist society and you might not want to have more real material oppression stacked against you than you have to
#^^^^ so much this. yes#diagnosis is not neutral! sometimes helpful often harmful but never ever neutral#<- im paraphrasing eli clare#but anyway. diagnosis is like. who the fuck cares what doctors have to say. if people hate self diagnosis then they can come#break me out of the psych ward. when having diagnoses on my record prompts the ER to do a 72 hour hold simply bc of the risk of delusions#anyway
33K notes
·
View notes
Text
Fuck the DSM. Seriously, fuck the DSM.
The DSM is and always has been used primarily as a method of rationalizing mistreatment of the people it labels as "deviant." When you look at the history of psychiatry, it becomes clear that things like drapetomania, protest psychosis, hysteria, and homosexuality as a disorder were not just thrown into there randomly. Rather, it showcases the power of the DSM: labeling and categorizing ways of being as mental illness opens up new paths of incarceration, social control, and curative violence. I need people to understand that the modern DSM still works like this: these classifications of madness/mental distress/neurodivergence into psychiatric labels encourage society to treat madness/mental distress/neurodivergence with the apparatuses used to eradicate "deviance." Diagnosis is not neutral.
As mad/mentally ill/neurodivergent people, we deserve access to more explanatory models of madness/mental illness/ neurodivergence than what the psychiatric language of normalcy and disorder offers us. Whether this looks like rejecting diagnosis, embracing varying cultural understandings of mental experience, or any million different ways of interpreting our bodymind, we deserve the option to move beyond clinical language that tries to convince us not to trust ourselves. We deserve to view ourselves wholly, leaving room for all our experiences of madness/mental illness/neurodivergence--the meaningful, the terrifying, the joyful, the exhausting. We deserve to have our own relationship with our madness, instead of being pushed to view ourselves as an inherent "danger to self or others" simply by existing as crazy.
Here's another truth: I hate the DSM, and I still call myself bipolar, a diagnosis that came to me through psych incarceration. While I wholeheartedly reject the DSM and the system intertwined with it, I simultaneously acknowledge and believe that many of the collections of symptoms that the DSM describes are very, very real ways of living in the world, and that the distress that they can cause are very very real. When I say fuck the DSM, I don't mean "Mental distress, disability, and neurodivergence aren't real." Rather, I mean that the DSM can never hold my experience of what it is like to be bipolar, the meaning I derive from experiencing life with cyclical moods. The DSM can't hold within its pages what it's like to see my mood cycle not as a tragedy or disaster, but instead as an opportunity, a gift, to grow and shift and go back to the same place over and over again, dying in winter and blooming again in spring. The DSM can't hold the fact that even though I experience very, very real distress due to those mood cycles--they're still mine and I claim that as something that matters to me. I call myself bipolar as a shorthand to tell people that I experience many things both extreme high and low, but I do not mean the same thing when I say "bipolar" as a psychiatrist does.
When we build community as mad/mentally ill/neurodivergent people, I want us to have room to share, relate, and care for each other in ways that isn't calling to the authority of a fucked up system with strictly defined categories. I don't want us to take those same ways of thinking and rebrand it into advocacy that claims to fight stigma, but really just ends up reinforcing these same ideas about deviance, cure, control, and danger. I dream of the day when psychiatry doesn't loom as a threat in all of our lives, and I think part of that work requires us as mad/mentally ill/neurodivergent people to really grapple with and untangle the ways we label and make meaning of our minds.
ok to reblog, if you want to learn more about antipsychiatry/mad studies check out this reading list.
#personal#antipsychiatry#antipsych#mad pride#mad studies#disability justice#disability#prompted by. idk. being tangential to certain spaces lately#seeing ppl who r forming communities focused on neurodivergency#in a way that really just. reinforces and legitimizes the dsm#and constantly refers to the authority of the dsm as a reason why they r right#not going to get into the specific discourse of the week except to say that something i feel strongly. is that we get to have different#explanatory models. but also that we r allowed to critique explanatory models as a community#like i hate the indigo child shit. i think its full of white supremascist dogwhistles#that's not an explanatory model i feel like the autistic community should ever support u know#anyway. getting offtrack
971 notes
·
View notes
Text
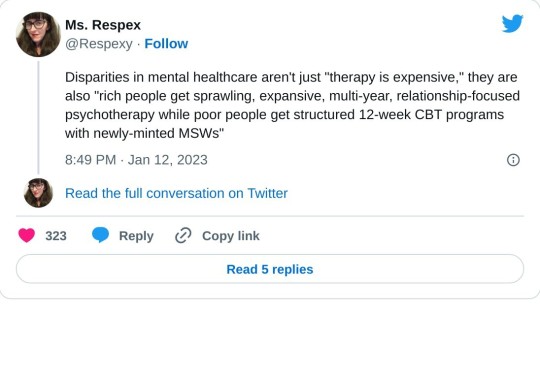
[Disparities in mental healthcare aren't just "therapy is expensive," they are also "rich people get sprawling, expansive, multi-year, relationship-focused psychotherapy while poor people get structured 12-week CBT programs with newly-minted MSWs"]
#LITERALLY#literally literally#also like. if u are rich. u are more likely to be able to navigate the system#in a way that lets you avoid or mitigate. some of the carceral aspects#whereas if you don't have insurance. the ability to shop for therapists. etc etc#you are much more likely to end up psych incarcerated. court ordered treatment. shitty CBT programs#of course being rich doesn't mean that you can't also be faced with those shitty parts of the mental health system. it does usually mean#that you have access to more options then just those shitty parts though#i mean abolish the whole system don't get me wrong. but i think this is an important conversation to have#about how class affects access + ability to navigate the system and mitigate the inherent damages
4K notes
·
View notes
Text
met with my advisor for my antipsych research project for the first time, went in and told her my plans and she was very supportive and excited!!!! part of the project involves making a zine and im going to be putting a call out for participants (it will be paid <3) so if you're a psych survivor who does any kind of writing, essays, poetry, drawing, photography, art of any form...keep an eye on my tumblr! in the next month or so i'll probably be putting the call for submissions out and explaining the prompt + what this project is. so :) just letting everyone who follows this blog know early LMAO
#personal#some of u over here on this side of antipsych tumblr r like my favorite people ever#so if u want to participate i woudl be honored and delighted#antipsych
21 notes
·
View notes
Note
have you read alexandre baril's "Suicidism: A new theoretical framework to conceptualize suicide from an anti-oppressive perspective"? it was a really powerful read for me as a suicidal person & the first (and tbh only) place I've seen someone discuss suicidal people as an oppressed group and not as people who need their autonomy taken away & any complaints they have abt treatment should be ignored
Haha indeed I have! Baril is a close colleague, coauthor, and former research advisor of mine. I helped him compile resources for that article while it was a WIP, so suffice it to say I’m very familiar. And yes, it’s a crucial intervention into a largely taboo part of disability / Mad discourse, and has been hugely influential on my thinking around disorderly eating too.
299 notes
·
View notes
Text
a lot of people, when faced with antipsych rhetoric, will accuse us of trying to take their meds away.
the stock response is that no, we’re not trying to take anyone’s meds away, we’re trying to remove the gatekeeping and prescriptive framework that meds are currently accessed in to begin with, making it so that no-one is forced to take meds they don’t want to take and that anyone can access any meds they want to take without needing to go through an institutional authority.
and like, that’s true, but i think it’s missing the inherent anxiety being expressed: that less people will be on meds, if the psychiatric institution is abolished and we are able to disseminate accurate information about the long-term effects of some of the most commonly prescribed psych meds (SSRIs and antipsychotics in particular). i don’t think these people would ever articulate it this way themselves, but i think a lot of pathologized peoples who have bought into the psychiatric institution’s narrative have an idea of medicated=good, and unmedicated=bad, and therefore have an automatic anxiety response to the idea of a large number of people going off their meds, even if that doesn’t include them, personally.
there’s an anxiety deeply embedded in MI and neurodivergent spaces that buy into the pathology framework about unmedicated MI people being dangerous, or just unpredictable in a way that is framed as harmful to themselves and others. there’s also a strong attitude of like… not trusting individual MI people to ascertain accurately if their meds work for them or not. there’s a reason MI spaces love to lean heavily on the “i was doing great, so i decided i didn’t need my meds, and when i went off them i was suddenly suicidal and miserable, because my meds were the only thing making me do great” anecdote–while it’s an accurate anecdote for many people, it’s also incredibly useful for pushing the narrative that MI people cannot accurately assess our relationships with medication, and that it’s necessary to leave that assessment to a doctor or other outside professional.
the idea of less people being on medication of their own free will is genuinely incredibly anxiety-provoking to a lot of pathologized peoples. the idea that MI people might not need the meds they’re currently, right now, taking, is incredibly destabilizing to their worldview. the idea that they themselves might have the option to go off their meds is anxiety-provoking! from an internal view, it feels like they’re being threatened. no matter how many times you explain that nobody’s trying to personally take their meds away, they still have the feeling of being under threat. i think that’s where the disconnect in a lot of these discussions happens.
#oh this is a great post!#very much agree and i think is why sometimes like. when we will be talking about#how a particular med has been harmful for me when i took it#im used to getting the response from people that its 'dangerous for me to talk about this publically#in case it stops other people from wanting to try it#and i think societally and culturally we are so attached to the idea that mad/mi/ND people are#dangerous. without meds without intervention#so much rhetoric is centered around ideas of safety and danger that ultimately#work to pathologize our experiences and shut down our voices#anyway sorry for rambling but good post!!!
318 notes
·
View notes