#cal osha training materials
Text
OSHA Workplace Safety Training, Consultancy: PCS Safety, California
PCS Safety: Providing quality workplace safety services Company & training including OSHA training to public/private sectors in California and throught United States..
Cal OSHA safety training for Workers – cal osha training coursesA Mandate: The Cal OSHA training module ensures that cal osha safety training workers are eligible for workplace safety osha citation for their positions regardless of industry. Its Known as california safety training
osha citation response Importance of Safety Work Permit by PCS safety Inc - osha certification California A safe system of work permit is an effective vehicle for communicating critical safety information. Safe Lifting Poster- Employers are encouraged to post this guide osha license to help workers follow OSHA’s ergonomic compliance and meet OSHA’s mandatory training requirement.
osha 40 hours- 40 hour hazwoper
labor law posters california - First Aid Compliance for Your first aid training Workplace California Forklift Certification Requirements for Employers workplace first aid What is PSM – Process Safety Management Program, is it Important
Injury and Illness Prevention (IIP) Program Plan Kit : Under Title 8 of the California Code of Regulations (T8CCR) Section 3203, every California employer is required to have a documentable llness injury preventino program kit. At PCS Safety, Inc., osha injury and illness prevention program our Injury and Illness Prevention Plan Kit injury and illness prevention program osha will help you prepare and meet the legal requirements. The first step is conducting injury illness prevention program california the OSHA Inspections & Citation Representation, injury illness prevention program Citation & Appeals.
CAL-OSHA COMPLIANCE TRAINING
Cal OSHA Compliance Training : The Safety Program or Illness and Injury Prevention Program as required by Cal OSHA training requirements must encompass the following elements:
1)Compliance 2) Communication 3) Hazard Assessment 4) Accident/Exposure Investigation 5) Hazard Correction 6) Training and Instruction 7) Record-keeping Compliance is cal osha training courses something every organization with one or more employees must comply with all of the above-mentioned requirements. Cal OSHA Training materials (e.g., interactive videos, online training, and more) that address the topics required by OSHA, are vital documents that you need to prepare, as well as emergency response plans.
#"llness injury preventino program kit#osha injury and illness prevention program#injury and illness prevention program osha#illness prevention program#injury illness prevention program california#injury illness prevention program#cal osha training requirements#cal osha compliance training#cal osha training courses#cal osha training materials#cal osha safety training#cal osha training#california safety training#safety work permit#safe lifting poster#labor law posters California#first aid compliance#california forklift certification requirements#process safety management program
1 note
·
View note
Text
Spoilers for The Acolyte below. I'm serious. S p o i l e r s
Carrie Anne Moss was a centerpiece for their marketing campaign.
Her character, a Jedi, is killed within the first five minutes.
She is one of about four random Jedi we do not get to know , whom (one of) Amandla Stenberg's characters is seeking revenge against.
For reasons we still don't really know or care about within the first two episodes.
I don't know about anyone else, but when you get Carrie Anne Moss in your production only to drop her like that?

If that gives you any idea as to the quality of the writing, well.
Stenberg plays twins in this one, Osha and Mae, in a standard, hackneyed, "one of them was thought to be dead" scenario. Both twins were once Jedi-in-training, as children, and the one everyone assumed was dead (Mae) went off to join a Sith (how do we know? The red lightsaber and wanting to kill Jedi is a pretty big giveaway), while the other is a Cal Kestis-type mechnec with a pip droid who dropped out of Jedi High to tool around on Trade Federation ships.
Like you do.
It's assumed that Osha is the Jedi killer (in spite having zero reason), and this gets their old Jedi teacher involved and a non-chase to easily find out the truth. I say "easily" since the Jedi are a weird non-presence in this one: they're everywhere and yet they make no impression (unlike the bureaucratic knobs of the Empire in Andor, the Jedi are just....moving wallpaper). Jedi should be at least marginally interesting, but with so much world-building work done in so many other Star Wars shows, this one doesn't care to offer anything new or insightful (and, to be fair, probably doesn't have time to).
These episodes are only 30 minutes long, re-hash a lot of old material and waste pretty much everyone involved. Along with Stenberg, this show has Dafne Keen, Lee Jung-jae, Manny Jacinto, Charlie Barnett and Jodie Turner-Smith in roles that really aren't much to phone home about. Only Keen, as a clever Padawan, leaves any kind of impression (and is also largely unrecognizable). There's a smidgeon of a hint of chemistry between Stenberg and Keen, but as one seems dedicated to her Jedi training, not counting on that going anywhere.
The end of episode two brings us to a world visited in the game Jedi: Survivor, where we meet a Wookie Jedi, presumably in hiding. Well, I mean, they say it's a Wookie, but it looks less like a cousin of Chewbacca and closer to Baby Bigfoot.
So far, this seems like an afternoon kid's special of Star Wars off-cuts that, who knows, might get better over its run. It's got enough talent behind it (not least of which is its queer showrunner, Leslye Headland who last exec produced Russian Doll and is gearing up to direct the film version of The Seven Husbands of Evelyn Hugo).
I'm still just stunned at the laziness of it all though.
You got fucking Trinity to wield a lightsaber for all of one minute and killed her off?

Without even a Padawan around to mourn her, this really looks like a cheap casting stunt.
Will we get to see what these Jedi did to piss off Rue's twin? IMDB has Moss down for only one episode. If this was all they used her for, yikes. For her five minutes of screen time, Moss added more gravity than any of the others combined and if we really don't see her again? What a waste.
7 notes
·
View notes
Text
Workers Compensation Insurance for Roofers In California
Introduction
Workers' compensation insurance is essential for high-risk professions such as roofing. Given the inherent dangers associated with roofing work, it is crucial for roofing companies in California to understand and comply with workers' compensation regulations. This article explores the key elements of workers' compensation insurance for roofing companies in California, including legal requirements, coverage options, challenges, and best practices.
Legal Requirements
In California, employers are required to carry workers' compensation insurance for all employees, including part-time, temporary, and seasonal workers. This mandate is particularly important for roofing companies due to the high-risk nature of the work.
Key Points:
Mandatory Coverage: Roofing companies must provide workers' compensation coverage for all employees, regardless of the duration or nature of their employment.
Compliance with State Laws: The California Department of Industrial Relations (DIR) and the Division of Workers' Compensation (DWC) oversee compliance with workers' compensation regulations. Roofing companies must adhere to these regulations to avoid penalties and ensure employee protection.
Reporting and Record-Keeping: Employers are required to report work-related injuries and illnesses promptly and maintain accurate records.
Coverage Options
Roofing companies in California have several options for obtaining workers' compensation insurance. These include purchasing a policy from a private insurance carrier, utilizing the state's assigned risk pool for high-risk employers, or self-insuring if the company meets specific financial criteria set by the DIR.
Key Points:
Private Insurance: Many roofing companies prefer private insurance for its flexibility and variety of available policies.
State Compensation Insurance Fund (SCIF): SCIF is a state-run program that provides workers' compensation insurance, especially for businesses that have difficulty obtaining coverage through private insurers.
Self-Insurance: Larger companies with substantial financial stability might choose to self-insure. This option requires state approval and a demonstration of financial capability.
Challenges for Roofing Companies
Roofing companies face unique challenges in managing workers' compensation insurance:
High Risk of Injury: Roofing is a high-risk occupation with potential hazards such as falls, tool injuries, and exposure to extreme weather conditions.
Varied Work Environments: Roofers work in different environments, including residential, commercial, and industrial sites, each with unique safety challenges.
High Turnover: The roofing industry often experiences high employee turnover, complicating record-keeping and claims management.
Cost Management: The cost of workers' compensation insurance can be significant due to the high risk associated with roofing work.
Best Practices
To effectively manage workers' compensation insurance and minimize risks, roofing companies should implement several best practices:
Comprehensive Training: Provide thorough safety training tailored to the specific tasks and environments where employees will work. This includes fall prevention, proper use of tools, and safe handling of materials.
Regular Safety Audits: Conduct regular safety audits of job sites to identify and mitigate potential hazards. Ensure compliance with Occupational Safety and Health Administration (OSHA) standards and California's specific safety regulations (Cal/OSHA).
Effective Communication: Maintain open lines of communication with employees to quickly address any safety concerns or incidents. Encourage employees to report unsafe conditions and near-misses.
Accurate Record-Keeping: Keep detailed records of employee training, job assignments, and incident reports to streamline the claims process and ensure compliance with state regulations. Proper documentation is crucial for managing claims efficiently.
Return-to-Work Programs: Implement return-to-work programs to help injured employees transition back to their jobs. These programs can reduce the duration and cost of workers' compensation claims and improve employee morale.
Insurance Review: Regularly review insurance policies to ensure they provide adequate coverage for the company's current operations and adjust as necessary. This includes evaluating different insurance providers to find the best coverage options.
California's Unique Considerations
Medical Provider Network (MPN): Employers in California can establish an MPN, a network of healthcare providers to treat workers injured on the job. Employees generally must choose their treating doctor from the MPN.
Benefit Structure: Understanding California's specific benefits structure, including temporary disability, permanent disability, and medical benefits, is crucial for accurate claims management.
Vocational Rehabilitation: California law includes provisions for supplemental job displacement benefits (SJDB) to help injured workers who cannot return to their previous job.
Conclusion
Workers' compensation insurance is a critical component of managing a roofing company in California. By understanding the legal requirements, exploring coverage options, addressing unique challenges, and implementing best practices, roofing companies can protect their employees and their business. Effective management of workers' compensation not only ensures legal compliance but also contributes to a safer and more productive workforce, ultimately leading to a more successful roofing company.
0 notes
Text
Hospitals, Nursing Homes Fail to Separate COVID Patients, Putting Others at Risk
Nurses at Alta Bates Summit Medical Center were on edge as early as March when patients with COVID-19 began to show up in areas of the hospital that were not set aside to care for them.
The Centers for Disease Control and Prevention had advised hospitals to isolate COVID patients to limit staff exposure and help conserve high-level personal protective equipment that’s been in short supply.
Yet COVID patients continued to be scattered through the Oakland hospital, according to complaints to California’s Division of Occupational Safety and Health. The concerns included the sixth-floor medical unit where veteran nurse Janine Paiste-Ponder worked.
COVID patients on that floor were not staying in their rooms, either confused or uninterested in the rules. Staff was not provided highly protective N95 respirators, said Mike Hill, a nurse in the hospital intensive care unit and the hospital’s chief representative for the California Nurses Association, which filed complaints to Cal/OSHA, the state’s workplace safety regulator.
“It was just a matter of time before one of the nurses died on one of these floors,” Hill said.
Two nurses fell ill, including Paiste-Ponder, 59, who died of complications from the virus on July 17.
The concerns raised in Oakland also have swept across the U.S., according to interviews, a review of government workplace safety complaints and health facility inspection reports. A KHN investigation found that dozens of nursing homes and hospitals ignored official guidelines to separate COVID patients from those without the coronavirus, in some places fueling its spread and leaving staff unprepared and infected or, in some cases, dead.
As recently as July, a National Nurses United survey of more than 21,000 nurses found that 32% work in a facility that does not have a dedicated COVID unit. At that time, the coronavirus had reached all but 17 U.S. counties, data collected by Johns Hopkins University shows.
KHN discovered that COVID victims have been commingled with uninfected patients in health care facilities in states including California, Florida, New Jersey, Iowa, Ohio, Maryland and New York.
A COVID-19 outbreak was in full swing at the New Jersey Veterans Home at Paramus in late April when health inspectors observed residents with dementia mingling in a day room — COVID-positive patients as well as others awaiting test results. At the time, the center had already reported COVID infections among 119 residents and 46 virus-related deaths, according to a Medicare inspection report.
The assistant director of nursing at an Iowa nursing home insisted April 28 that they did “not have any COVID in the building” and overrode the orders of a community doctor to isolate several patients with fevers and falling oxygen levels, an inspection report shows.
By mid-May, the facility’s COVID log showed 61 patients with the virus and nine dead.
Federal work-safety officials have closed at least 30 complaints about patient mixing in hospitals nationwide without issuing a citation. They include a claim that a Michigan hospital kept patients who tested negative for the virus in the COVID unit in May. An upstate New York hospital also had COVID patients in the same unit as those with no infection, according to a closed complaint to the federal Occupational Safety and Health Administration.
Federal Health and Human Services officials have called on hospitals to tell them each day if they have a patient who came in without COVID-19 but had an apparent or confirmed case of the coronavirus 14 days later. Hospitals filed 48,000 reports from June 21 through Aug. 28, though the number reflects some double or additional counting of individual patients.
COVID patients have been mixed in with others for a variety of reasons. Some hospitals report having limited tests, so patients carrying the virus are identified only after they had already exposed others. In other cases, they had false-negative test results or their facility was dismissive of federal guidelines, which carry no force of law.
And while federal Medicare officials have inspected nearly every U.S. nursing home in recent months and states have occasionally levied fines and cut off new admissions for isolation lapses, hospitals have seen less scrutiny.
The Scene Inside Sutter
At Alta Bates in Oakland, part of the Sutter Health network, hospital staff made it clear in official complaints to Cal/OSHA that they wanted administrators to follow the state’s unique law on aerosol-transmitted diseases. From the start, some staffers wanted all the state-required protections for a virus that has been increasingly shown to be transmitted by tiny particles that float through the air.
The regulations call for patients with a virus like COVID-19 to be moved to a specialized unit within five hours of identification — or to a specialized facility. The rules say those patients should be in a room with a HEPA filter or with negative air pressure, meaning that air is circulated out a window or exhaust fan instead of drifting into the hallway.
Initially, in March, the hospital outfitted a 40-bed COVID unit, according to Hill. But when a surge of patients failed to materialize, that unit was pared to 12 beds.
Since then, a steady stream of virus patients have been admitted, he said, many testing positive only days after admission — and after they’d been in regular rooms in the facility.
From March 10 through July 30, Hill’s union and others filed eight complaints to Cal/OSHA, including allegations that the hospital failed to follow isolation rules for COVID patients, some on the cancer floor.
So far, regulators have done little. Gov. Gavin Newsom had ordered workplace safety officials to “focus on … supporting compliance” instead of enforcement except on the “most serious violations.”
State officials responded to complaints by reaching out by mail and phone to “ensure the proper virus prevention measures are in place,” according to Frank Polizzi, a spokesperson for Cal/OSHA.
A third investigation related to transport workers not wearing N95 respirators while moving COVID-positive or possible coronavirus patients at a Sutter facility near the hospital resulted in a $6,750 fine, Cal/OSHA records show.
The string of complaints also says the hospital did not give staff the necessary personal protective equipment (PPE) under state law — an N95 respirator or something more protective — for caring for virus patients.
Instead, Hill said, staff on floors with COVID patients were provided lower-quality surgical masks, a concern reflected in complaints filed with Cal/OSHA.
Hill believes that Paiste-Ponder and another nurse on her floor caught the virus from COVID patients who did not remain in their rooms.
“It is sad, because it didn’t really need to happen,” Hill said.
Polizzi said investigations into the July 17 death and another staff hospitalization are ongoing.
A Sutter Health spokesperson said the hospital takes allegations, including Cal/OSHA complaints, seriously and its highest priority is keeping patients and staff safe.
The statement also said “cohorting,” or the practice of grouping virus patients together, is a tool that “must be considered in a greater context, including patient acuity, hospital census and other environmental factors.”
Concerns at Other Hospitals
CDC guidelines are not strict on the topic of keeping COVID patients sectioned off, noting that “facilities could consider designating entire units within the facility, with dedicated [staff],” to care for COVID patients.
That approach succeeded at the University of Nebraska Medical Center in Omaha. A recent study reported “extensive” viral contamination around COVID patients there, but noted that with “standard” infection control techniques in place, staffers who cared for COVID patients did not get the virus.
The hospital set up an isolation unit with air pumped away from the halls, restricted access to the unit and trained staff to use well-developed protocols and N95 respirators — at a minimum. What worked in Nebraska, though, is far from standard elsewhere.
Cynthia Butler, a nurse and National Nurses United member at Fawcett Memorial Hospital in Port Charlotte, on Florida’s west coast, said she actually felt safer working in the COVID unit — where she knew what she was dealing with and had full PPE — than on a general medical floor.
She believes she caught the virus from a patient who had COVID-19 but was housed on a general floor in May. A similar situation occurred in July, when another patient had an unexpected case of COVID — and Butler said she got another positive test herself.
She said both patients did not meet the hospital’s criteria for testing admitted patients, and the lapses leave her on edge, concerns she relayed to an OSHA inspector who reached out to her about a complaint her union filed about the facility.
“Every time I go into work it’s like playing Russian roulette,” Butler said.
A spokesperson for HCA Healthcare, which owns the hospital, said it tests patients coming from long-term care, those going into surgery and those with virus symptoms. She said staffers have access to PPE and practice vigilant sanitation, universal masking and social distancing.
The latter is not an option for Butler, though, who said she cleans, feeds and starts IVs for patients and offers reassurance when they are isolated from family.
“I’m giving them the only comfort or kind word they can get,” said Butler, who has since gone on unpaid leave over safety concerns. “I’m in there doing that and I’m not being protected.”
Given research showing that up to 45% of COVID patients are asymptomatic, UCSF Medical Center is testing everyone who’s admitted, said Dr. Robert Harrison, a University of California-San Francisco School of Medicine professor who consults on occupational health at the hospital.
It’s done for the safety of staff and to reduce spread within the hospital, he said. Those who test positive are separated into a COVID-only unit.
And staff who spent more than 15 minutes within 6 feet of a not-yet-identified COVID patient in a less-protective surgical mask are typically sent home for two weeks, he said.
Outside of academic medicine, though, front-line staff have turned to union leaders to push for such protections.
In Southern California, leaders of the National Union of Healthcare Workers filed an official complaint with state hospital inspectors about the risks posed by intermingled COVID patients at Fountain Valley Regional Hospital in Orange County, part of for-profit Tenet Health. There, the complaint said, patients were not routinely tested for COVID-19 upon admission.
One nursing assistant spent two successive 12-hour shifts caring for a patient on a general medical floor who required monitoring. At the conclusion of the second shift, she was told the patient had just been found to be COVID-positive.
The worker had worn only a surgical mask — not an N95 respirator or any form of eye protection, according to the complaint to the California Department of Public Health. The nursing assistant was not offered a COVID test or quarantined before her next two shifts, the complaint said.
The public health department said it could not comment on a pending inspection.
Barbara Lewis, Southern California hospital division director with the union, said COVID patients were on the same floor as cancer patients and post-surgical patients who were walking the halls to speed their recovery.
She said managers took steps to separate the patients only after the union held a protest, spoke to local media and complained to state health officials.
Hospital spokesperson Jessica Chen said the hospital “quickly implemented” changes directed by state health authorities and does place some COVID patients on the same nursing unit as non-COVID patients during surges. She said they are placed in single rooms with closed doors. COVID tests are given by physician order, she added, and employees can access them at other places in the community.
It’s in contrast, Lewis said, to high-profile examples of the precautions that might be taken.
“Now we’re seeing what’s happening with baseball and basketball — they’re tested every day and treated with a high level of caution,” Lewis said. “Yet we have thousands and thousands of health care workers going to work in a very scary environment.”
Nursing Homes Face Penalties
More than 40% of the people who’ve died of COVID-19 lived in nursing homes or assisted living facilities, researchers have found.
Patient mixing has been a scattered concern at nursing homes, which Medicare officials discovered when they reviewed infection control practices at more than 15,000 facilities.
News reports have highlighted the problem at an Ohio nursing home and at a Maryland home where the state levied a $70,000 fine for failing to keep infected patients away from those who weren’t sick — yet.
Another facing penalties was Fair Havens Center, a Miami Springs, Florida, nursing home where inspectors discovered that 11 roommates of patients who tested positive for COVID-19 were put in rooms with other residents — putting them at heightened risk.
Florida regulators cut off admissions to the home and Medicare authorities levied a $235,000 civil monetary penalty, records show.
The vice president of operations at the facility told inspectors that isolating exposed patients would mean isolating the entire facility: Everyone had been exposed to the 32 staff members who tested positive for the virus, the report says.
Fair Havens Center did not respond to a request for comment.
In Iowa, Medicare officials declared a state of “immediate jeopardy” at Pearl Valley Rehabilitation and Care Center in Muscatine. There, they discovered that staffers were in denial over an outbreak in their midst, with a nursing director overriding a community doctor’s orders to isolate or send residents to the emergency room. Instead, officials found, in late April, the assistant nursing director kept COVID patients in the facility, citing a general order by their medical director to avoid sending patients to the ER “if you can help it.”
Meanwhile, several patients were documented by facility staff to have fevers and falling oxygen levels, the Medicare inspection report shows. Within two weeks, the facility discovered it had an outbreak, with 61 residents infected and nine dead, according to the report.
Medicare officials are investigating Menlo Park Veterans Memorial Home in New Jersey, state Sen. Joseph Vitale said during a recent legislative hearing. Resident council president Glenn Osborne testified during the hearing that the home’s residents were returned to the same shared rooms after hospitalizations.
Osborne, an honorably discharged Marine, said he saw more residents of the home die than fellow service members during his military service. The Menlo Park and Paramus veterans homes — where inspectors saw dementia patients with and without the virus commingling in a day room — both reported more than 180 COVID cases among residents, 90 among staff and at least 60 deaths.
A spokesperson for the homes said he could not comment due to pending litigation.
“These deaths should not have happened,” Osborne said. “Many of these deaths were absolutely avoidable, in my humble opinion.”
Kaiser Health News (KHN) is a national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation which is not affiliated with Kaiser Permanente.
USE OUR CONTENT
This story can be republished for free (details).
Hospitals, Nursing Homes Fail to Separate COVID Patients, Putting Others at Risk published first on https://nootropicspowdersupplier.tumblr.com/
0 notes
Text
Hospitals, Nursing Homes Fail to Separate COVID Patients, Putting Others at Risk
Nurses at Alta Bates Summit Medical Center were on edge as early as March when patients with COVID-19 began to show up in areas of the hospital that were not set aside to care for them.
The Centers for Disease Control and Prevention had advised hospitals to isolate COVID patients to limit staff exposure and help conserve high-level personal protective equipment that’s been in short supply.
Yet COVID patients continued to be scattered through the Oakland hospital, according to complaints to California’s Division of Occupational Safety and Health. The concerns included the sixth-floor medical unit where veteran nurse Janine Paiste-Ponder worked.
COVID patients on that floor were not staying in their rooms, either confused or uninterested in the rules. Staff was not provided highly protective N95 respirators, said Mike Hill, a nurse in the hospital intensive care unit and the hospital’s chief representative for the California Nurses Association, which filed complaints to Cal/OSHA, the state’s workplace safety regulator.
“It was just a matter of time before one of the nurses died on one of these floors,” Hill said.
Two nurses fell ill, including Paiste-Ponder, 59, who died of complications from the virus on July 17.
The concerns raised in Oakland also have swept across the U.S., according to interviews, a review of government workplace safety complaints and health facility inspection reports. A KHN investigation found that dozens of nursing homes and hospitals ignored official guidelines to separate COVID patients from those without the coronavirus, in some places fueling its spread and leaving staff unprepared and infected or, in some cases, dead.
As recently as July, a National Nurses United survey of more than 21,000 nurses found that 32% work in a facility that does not have a dedicated COVID unit. At that time, the coronavirus had reached all but 17 U.S. counties, data collected by Johns Hopkins University shows.
KHN discovered that COVID victims have been commingled with uninfected patients in health care facilities in states including California, Florida, New Jersey, Iowa, Ohio, Maryland and New York.
A COVID-19 outbreak was in full swing at the New Jersey Veterans Home at Paramus in late April when health inspectors observed residents with dementia mingling in a day room — COVID-positive patients as well as others awaiting test results. At the time, the center had already reported COVID infections among 119 residents and 46 virus-related deaths, according to a Medicare inspection report.
The assistant director of nursing at an Iowa nursing home insisted April 28 that they did “not have any COVID in the building” and overrode the orders of a community doctor to isolate several patients with fevers and falling oxygen levels, an inspection report shows.
By mid-May, the facility’s COVID log showed 61 patients with the virus and nine dead.
Federal work-safety officials have closed at least 30 complaints about patient mixing in hospitals nationwide without issuing a citation. They include a claim that a Michigan hospital kept patients who tested negative for the virus in the COVID unit in May. An upstate New York hospital also had COVID patients in the same unit as those with no infection, according to a closed complaint to the federal Occupational Safety and Health Administration.
Federal Health and Human Services officials have called on hospitals to tell them each day if they have a patient who came in without COVID-19 but had an apparent or confirmed case of the coronavirus 14 days later. Hospitals filed 48,000 reports from June 21 through Aug. 28, though the number reflects some double or additional counting of individual patients.
COVID patients have been mixed in with others for a variety of reasons. Some hospitals report having limited tests, so patients carrying the virus are identified only after they had already exposed others. In other cases, they had false-negative test results or their facility was dismissive of federal guidelines, which carry no force of law.
And while federal Medicare officials have inspected nearly every U.S. nursing home in recent months and states have occasionally levied fines and cut off new admissions for isolation lapses, hospitals have seen less scrutiny.
The Scene Inside Sutter
At Alta Bates in Oakland, part of the Sutter Health network, hospital staff made it clear in official complaints to Cal/OSHA that they wanted administrators to follow the state’s unique law on aerosol-transmitted diseases. From the start, some staffers wanted all the state-required protections for a virus that has been increasingly shown to be transmitted by tiny particles that float through the air.
The regulations call for patients with a virus like COVID-19 to be moved to a specialized unit within five hours of identification — or to a specialized facility. The rules say those patients should be in a room with a HEPA filter or with negative air pressure, meaning that air is circulated out a window or exhaust fan instead of drifting into the hallway.
Initially, in March, the hospital outfitted a 40-bed COVID unit, according to Hill. But when a surge of patients failed to materialize, that unit was pared to 12 beds.
Since then, a steady stream of virus patients have been admitted, he said, many testing positive only days after admission — and after they’d been in regular rooms in the facility.
From March 10 through July 30, Hill’s union and others filed eight complaints to Cal/OSHA, including allegations that the hospital failed to follow isolation rules for COVID patients, some on the cancer floor.
So far, regulators have done little. Gov. Gavin Newsom had ordered workplace safety officials to “focus on … supporting compliance” instead of enforcement except on the “most serious violations.”
State officials responded to complaints by reaching out by mail and phone to “ensure the proper virus prevention measures are in place,” according to Frank Polizzi, a spokesperson for Cal/OSHA.
A third investigation related to transport workers not wearing N95 respirators while moving COVID-positive or possible coronavirus patients at a Sutter facility near the hospital resulted in a $6,750 fine, Cal/OSHA records show.
The string of complaints also says the hospital did not give staff the necessary personal protective equipment (PPE) under state law — an N95 respirator or something more protective — for caring for virus patients.
Instead, Hill said, staff on floors with COVID patients were provided lower-quality surgical masks, a concern reflected in complaints filed with Cal/OSHA.
Hill believes that Paiste-Ponder and another nurse on her floor caught the virus from COVID patients who did not remain in their rooms.
“It is sad, because it didn’t really need to happen,” Hill said.
Polizzi said investigations into the July 17 death and another staff hospitalization are ongoing.
A Sutter Health spokesperson said the hospital takes allegations, including Cal/OSHA complaints, seriously and its highest priority is keeping patients and staff safe.
The statement also said “cohorting,” or the practice of grouping virus patients together, is a tool that “must be considered in a greater context, including patient acuity, hospital census and other environmental factors.”
Concerns at Other Hospitals
CDC guidelines are not strict on the topic of keeping COVID patients sectioned off, noting that “facilities could consider designating entire units within the facility, with dedicated [staff],” to care for COVID patients.
That approach succeeded at the University of Nebraska Medical Center in Omaha. A recent study reported “extensive” viral contamination around COVID patients there, but noted that with “standard” infection control techniques in place, staffers who cared for COVID patients did not get the virus.
The hospital set up an isolation unit with air pumped away from the halls, restricted access to the unit and trained staff to use well-developed protocols and N95 respirators — at a minimum. What worked in Nebraska, though, is far from standard elsewhere.
Cynthia Butler, a nurse and National Nurses United member at Fawcett Memorial Hospital in Port Charlotte, on Florida’s west coast, said she actually felt safer working in the COVID unit — where she knew what she was dealing with and had full PPE — than on a general medical floor.
She believes she caught the virus from a patient who had COVID-19 but was housed on a general floor in May. A similar situation occurred in July, when another patient had an unexpected case of COVID — and Butler said she got another positive test herself.
She said both patients did not meet the hospital’s criteria for testing admitted patients, and the lapses leave her on edge, concerns she relayed to an OSHA inspector who reached out to her about a complaint her union filed about the facility.
“Every time I go into work it’s like playing Russian roulette,” Butler said.
A spokesperson for HCA Healthcare, which owns the hospital, said it tests patients coming from long-term care, those going into surgery and those with virus symptoms. She said staffers have access to PPE and practice vigilant sanitation, universal masking and social distancing.
The latter is not an option for Butler, though, who said she cleans, feeds and starts IVs for patients and offers reassurance when they are isolated from family.
“I’m giving them the only comfort or kind word they can get,” said Butler, who has since gone on unpaid leave over safety concerns. “I’m in there doing that and I’m not being protected.”
Given research showing that up to 45% of COVID patients are asymptomatic, UCSF Medical Center is testing everyone who’s admitted, said Dr. Robert Harrison, a University of California-San Francisco School of Medicine professor who consults on occupational health at the hospital.
It’s done for the safety of staff and to reduce spread within the hospital, he said. Those who test positive are separated into a COVID-only unit.
And staff who spent more than 15 minutes within 6 feet of a not-yet-identified COVID patient in a less-protective surgical mask are typically sent home for two weeks, he said.
Outside of academic medicine, though, front-line staff have turned to union leaders to push for such protections.
In Southern California, leaders of the National Union of Healthcare Workers filed an official complaint with state hospital inspectors about the risks posed by intermingled COVID patients at Fountain Valley Regional Hospital in Orange County, part of for-profit Tenet Health. There, the complaint said, patients were not routinely tested for COVID-19 upon admission.
One nursing assistant spent two successive 12-hour shifts caring for a patient on a general medical floor who required monitoring. At the conclusion of the second shift, she was told the patient had just been found to be COVID-positive.
The worker had worn only a surgical mask — not an N95 respirator or any form of eye protection, according to the complaint to the California Department of Public Health. The nursing assistant was not offered a COVID test or quarantined before her next two shifts, the complaint said.
The public health department said it could not comment on a pending inspection.
Barbara Lewis, Southern California hospital division director with the union, said COVID patients were on the same floor as cancer patients and post-surgical patients who were walking the halls to speed their recovery.
She said managers took steps to separate the patients only after the union held a protest, spoke to local media and complained to state health officials.
Hospital spokesperson Jessica Chen said the hospital “quickly implemented” changes directed by state health authorities and does place some COVID patients on the same nursing unit as non-COVID patients during surges. She said they are placed in single rooms with closed doors. COVID tests are given by physician order, she added, and employees can access them at other places in the community.
It’s in contrast, Lewis said, to high-profile examples of the precautions that might be taken.
“Now we’re seeing what’s happening with baseball and basketball — they’re tested every day and treated with a high level of caution,” Lewis said. “Yet we have thousands and thousands of health care workers going to work in a very scary environment.”
Nursing Homes Face Penalties
More than 40% of the people who’ve died of COVID-19 lived in nursing homes or assisted living facilities, researchers have found.
Patient mixing has been a scattered concern at nursing homes, which Medicare officials discovered when they reviewed infection control practices at more than 15,000 facilities.
News reports have highlighted the problem at an Ohio nursing home and at a Maryland home where the state levied a $70,000 fine for failing to keep infected patients away from those who weren’t sick — yet.
Another facing penalties was Fair Havens Center, a Miami Springs, Florida, nursing home where inspectors discovered that 11 roommates of patients who tested positive for COVID-19 were put in rooms with other residents — putting them at heightened risk.
Florida regulators cut off admissions to the home and Medicare authorities levied a $235,000 civil monetary penalty, records show.
The vice president of operations at the facility told inspectors that isolating exposed patients would mean isolating the entire facility: Everyone had been exposed to the 32 staff members who tested positive for the virus, the report says.
Fair Havens Center did not respond to a request for comment.
In Iowa, Medicare officials declared a state of “immediate jeopardy” at Pearl Valley Rehabilitation and Care Center in Muscatine. There, they discovered that staffers were in denial over an outbreak in their midst, with a nursing director overriding a community doctor’s orders to isolate or send residents to the emergency room. Instead, officials found, in late April, the assistant nursing director kept COVID patients in the facility, citing a general order by their medical director to avoid sending patients to the ER “if you can help it.”
Meanwhile, several patients were documented by facility staff to have fevers and falling oxygen levels, the Medicare inspection report shows. Within two weeks, the facility discovered it had an outbreak, with 61 residents infected and nine dead, according to the report.
Medicare officials are investigating Menlo Park Veterans Memorial Home in New Jersey, state Sen. Joseph Vitale said during a recent legislative hearing. Resident council president Glenn Osborne testified during the hearing that the home’s residents were returned to the same shared rooms after hospitalizations.
Osborne, an honorably discharged Marine, said he saw more residents of the home die than fellow service members during his military service. The Menlo Park and Paramus veterans homes — where inspectors saw dementia patients with and without the virus commingling in a day room — both reported more than 180 COVID cases among residents, 90 among staff and at least 60 deaths.
A spokesperson for the homes said he could not comment due to pending litigation.
“These deaths should not have happened,” Osborne said. “Many of these deaths were absolutely avoidable, in my humble opinion.”
Kaiser Health News (KHN) is a national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation which is not affiliated with Kaiser Permanente.
USE OUR CONTENT
This story can be republished for free (details).
Hospitals, Nursing Homes Fail to Separate COVID Patients, Putting Others at Risk published first on https://smartdrinkingweb.weebly.com/
0 notes
Text
Hospitals, Nursing Homes Fail to Separate COVID Patients, Putting Others at Risk
Nurses at Alta Bates Summit Medical Center were on edge as early as March when patients with COVID-19 began to show up in areas of the hospital that were not set aside to care for them.
The Centers for Disease Control and Prevention had advised hospitals to isolate COVID patients to limit staff exposure and help conserve high-level personal protective equipment that’s been in short supply.
Yet COVID patients continued to be scattered through the Oakland hospital, according to complaints to California’s Division of Occupational Safety and Health. The concerns included the sixth-floor medical unit where veteran nurse Janine Paiste-Ponder worked.
COVID patients on that floor were not staying in their rooms, either confused or uninterested in the rules. Staff was not provided highly protective N95 respirators, said Mike Hill, a nurse in the hospital intensive care unit and the hospital’s chief representative for the California Nurses Association, which filed complaints to Cal/OSHA, the state’s workplace safety regulator.
“It was just a matter of time before one of the nurses died on one of these floors,” Hill said.
Two nurses fell ill, including Paiste-Ponder, 59, who died of complications from the virus on July 17.
The concerns raised in Oakland also have swept across the U.S., according to interviews, a review of government workplace safety complaints and health facility inspection reports. A KHN investigation found that dozens of nursing homes and hospitals ignored official guidelines to separate COVID patients from those without the coronavirus, in some places fueling its spread and leaving staff unprepared and infected or, in some cases, dead.
As recently as July, a National Nurses United survey of more than 21,000 nurses found that 32% work in a facility that does not have a dedicated COVID unit. At that time, the coronavirus had reached all but 17 U.S. counties, data collected by Johns Hopkins University shows.
KHN discovered that COVID victims have been commingled with uninfected patients in health care facilities in states including California, Florida, New Jersey, Iowa, Ohio, Maryland and New York.
A COVID-19 outbreak was in full swing at the New Jersey Veterans Home at Paramus in late April when health inspectors observed residents with dementia mingling in a day room — COVID-positive patients as well as others awaiting test results. At the time, the center had already reported COVID infections among 119 residents and 46 virus-related deaths, according to a Medicare inspection report.
The assistant director of nursing at an Iowa nursing home insisted April 28 that they did “not have any COVID in the building” and overrode the orders of a community doctor to isolate several patients with fevers and falling oxygen levels, an inspection report shows.
By mid-May, the facility’s COVID log showed 61 patients with the virus and nine dead.
Federal work-safety officials have closed at least 30 complaints about patient mixing in hospitals nationwide without issuing a citation. They include a claim that a Michigan hospital kept patients who tested negative for the virus in the COVID unit in May. An upstate New York hospital also had COVID patients in the same unit as those with no infection, according to a closed complaint to the federal Occupational Safety and Health Administration.
Federal Health and Human Services officials have called on hospitals to tell them each day if they have a patient who came in without COVID-19 but had an apparent or confirmed case of the coronavirus 14 days later. Hospitals filed 48,000 reports from June 21 through Aug. 28, though the number reflects some double or additional counting of individual patients.
COVID patients have been mixed in with others for a variety of reasons. Some hospitals report having limited tests, so patients carrying the virus are identified only after they had already exposed others. In other cases, they had false-negative test results or their facility was dismissive of federal guidelines, which carry no force of law.
And while federal Medicare officials have inspected nearly every U.S. nursing home in recent months and states have occasionally levied fines and cut off new admissions for isolation lapses, hospitals have seen less scrutiny.
The Scene Inside Sutter
At Alta Bates in Oakland, part of the Sutter Health network, hospital staff made it clear in official complaints to Cal/OSHA that they wanted administrators to follow the state’s unique law on aerosol-transmitted diseases. From the start, some staffers wanted all the state-required protections for a virus that has been increasingly shown to be transmitted by tiny particles that float through the air.
The regulations call for patients with a virus like COVID-19 to be moved to a specialized unit within five hours of identification — or to a specialized facility. The rules say those patients should be in a room with a HEPA filter or with negative air pressure, meaning that air is circulated out a window or exhaust fan instead of drifting into the hallway.
Initially, in March, the hospital outfitted a 40-bed COVID unit, according to Hill. But when a surge of patients failed to materialize, that unit was pared to 12 beds.
Since then, a steady stream of virus patients have been admitted, he said, many testing positive only days after admission — and after they’d been in regular rooms in the facility.
From March 10 through July 30, Hill’s union and others filed eight complaints to Cal/OSHA, including allegations that the hospital failed to follow isolation rules for COVID patients, some on the cancer floor.
So far, regulators have done little. Gov. Gavin Newsom had ordered workplace safety officials to “focus on … supporting compliance” instead of enforcement except on the “most serious violations.”
State officials responded to complaints by reaching out by mail and phone to “ensure the proper virus prevention measures are in place,” according to Frank Polizzi, a spokesperson for Cal/OSHA.
A third investigation related to transport workers not wearing N95 respirators while moving COVID-positive or possible coronavirus patients at a Sutter facility near the hospital resulted in a $6,750 fine, Cal/OSHA records show.
The string of complaints also says the hospital did not give staff the necessary personal protective equipment (PPE) under state law — an N95 respirator or something more protective — for caring for virus patients.
Instead, Hill said, staff on floors with COVID patients were provided lower-quality surgical masks, a concern reflected in complaints filed with Cal/OSHA.
Hill believes that Paiste-Ponder and another nurse on her floor caught the virus from COVID patients who did not remain in their rooms.
“It is sad, because it didn’t really need to happen,” Hill said.
Polizzi said investigations into the July 17 death and another staff hospitalization are ongoing.
A Sutter Health spokesperson said the hospital takes allegations, including Cal/OSHA complaints, seriously and its highest priority is keeping patients and staff safe.
The statement also said “cohorting,” or the practice of grouping virus patients together, is a tool that “must be considered in a greater context, including patient acuity, hospital census and other environmental factors.”
Concerns at Other Hospitals
CDC guidelines are not strict on the topic of keeping COVID patients sectioned off, noting that “facilities could consider designating entire units within the facility, with dedicated [staff],” to care for COVID patients.
That approach succeeded at the University of Nebraska Medical Center in Omaha. A recent study reported “extensive” viral contamination around COVID patients there, but noted that with “standard” infection control techniques in place, staffers who cared for COVID patients did not get the virus.
The hospital set up an isolation unit with air pumped away from the halls, restricted access to the unit and trained staff to use well-developed protocols and N95 respirators — at a minimum. What worked in Nebraska, though, is far from standard elsewhere.
Cynthia Butler, a nurse and National Nurses United member at Fawcett Memorial Hospital in Port Charlotte, on Florida’s west coast, said she actually felt safer working in the COVID unit — where she knew what she was dealing with and had full PPE — than on a general medical floor.
She believes she caught the virus from a patient who had COVID-19 but was housed on a general floor in May. A similar situation occurred in July, when another patient had an unexpected case of COVID — and Butler said she got another positive test herself.
She said both patients did not meet the hospital’s criteria for testing admitted patients, and the lapses leave her on edge, concerns she relayed to an OSHA inspector who reached out to her about a complaint her union filed about the facility.
“Every time I go into work it’s like playing Russian roulette,” Butler said.
A spokesperson for HCA Healthcare, which owns the hospital, said it tests patients coming from long-term care, those going into surgery and those with virus symptoms. She said staffers have access to PPE and practice vigilant sanitation, universal masking and social distancing.
The latter is not an option for Butler, though, who said she cleans, feeds and starts IVs for patients and offers reassurance when they are isolated from family.
“I’m giving them the only comfort or kind word they can get,” said Butler, who has since gone on unpaid leave over safety concerns. “I’m in there doing that and I’m not being protected.”
Given research showing that up to 45% of COVID patients are asymptomatic, UCSF Medical Center is testing everyone who’s admitted, said Dr. Robert Harrison, a University of California-San Francisco School of Medicine professor who consults on occupational health at the hospital.
It’s done for the safety of staff and to reduce spread within the hospital, he said. Those who test positive are separated into a COVID-only unit.
And staff who spent more than 15 minutes within 6 feet of a not-yet-identified COVID patient in a less-protective surgical mask are typically sent home for two weeks, he said.
Outside of academic medicine, though, front-line staff have turned to union leaders to push for such protections.
In Southern California, leaders of the National Union of Healthcare Workers filed an official complaint with state hospital inspectors about the risks posed by intermingled COVID patients at Fountain Valley Regional Hospital in Orange County, part of for-profit Tenet Health. There, the complaint said, patients were not routinely tested for COVID-19 upon admission.
One nursing assistant spent two successive 12-hour shifts caring for a patient on a general medical floor who required monitoring. At the conclusion of the second shift, she was told the patient had just been found to be COVID-positive.
The worker had worn only a surgical mask — not an N95 respirator or any form of eye protection, according to the complaint to the California Department of Public Health. The nursing assistant was not offered a COVID test or quarantined before her next two shifts, the complaint said.
The public health department said it could not comment on a pending inspection.
Barbara Lewis, Southern California hospital division director with the union, said COVID patients were on the same floor as cancer patients and post-surgical patients who were walking the halls to speed their recovery.
She said managers took steps to separate the patients only after the union held a protest, spoke to local media and complained to state health officials.
Hospital spokesperson Jessica Chen said the hospital “quickly implemented” changes directed by state health authorities and does place some COVID patients on the same nursing unit as non-COVID patients during surges. She said they are placed in single rooms with closed doors. COVID tests are given by physician order, she added, and employees can access them at other places in the community.
It’s in contrast, Lewis said, to high-profile examples of the precautions that might be taken.
“Now we’re seeing what’s happening with baseball and basketball — they’re tested every day and treated with a high level of caution,” Lewis said. “Yet we have thousands and thousands of health care workers going to work in a very scary environment.”
Nursing Homes Face Penalties
More than 40% of the people who’ve died of COVID-19 lived in nursing homes or assisted living facilities, researchers have found.
Patient mixing has been a scattered concern at nursing homes, which Medicare officials discovered when they reviewed infection control practices at more than 15,000 facilities.
News reports have highlighted the problem at an Ohio nursing home and at a Maryland home where the state levied a $70,000 fine for failing to keep infected patients away from those who weren’t sick — yet.
Another facing penalties was Fair Havens Center, a Miami Springs, Florida, nursing home where inspectors discovered that 11 roommates of patients who tested positive for COVID-19 were put in rooms with other residents — putting them at heightened risk.
Florida regulators cut off admissions to the home and Medicare authorities levied a $235,000 civil monetary penalty, records show.
The vice president of operations at the facility told inspectors that isolating exposed patients would mean isolating the entire facility: Everyone had been exposed to the 32 staff members who tested positive for the virus, the report says.
Fair Havens Center did not respond to a request for comment.
In Iowa, Medicare officials declared a state of “immediate jeopardy” at Pearl Valley Rehabilitation and Care Center in Muscatine. There, they discovered that staffers were in denial over an outbreak in their midst, with a nursing director overriding a community doctor’s orders to isolate or send residents to the emergency room. Instead, officials found, in late April, the assistant nursing director kept COVID patients in the facility, citing a general order by their medical director to avoid sending patients to the ER “if you can help it.”
Meanwhile, several patients were documented by facility staff to have fevers and falling oxygen levels, the Medicare inspection report shows. Within two weeks, the facility discovered it had an outbreak, with 61 residents infected and nine dead, according to the report.
Medicare officials are investigating Menlo Park Veterans Memorial Home in New Jersey, state Sen. Joseph Vitale said during a recent legislative hearing. Resident council president Glenn Osborne testified during the hearing that the home’s residents were returned to the same shared rooms after hospitalizations.
Osborne, an honorably discharged Marine, said he saw more residents of the home die than fellow service members during his military service. The Menlo Park and Paramus veterans homes — where inspectors saw dementia patients with and without the virus commingling in a day room — both reported more than 180 COVID cases among residents, 90 among staff and at least 60 deaths.
A spokesperson for the homes said he could not comment due to pending litigation.
“These deaths should not have happened,” Osborne said. “Many of these deaths were absolutely avoidable, in my humble opinion.”
Kaiser Health News (KHN) is a national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation which is not affiliated with Kaiser Permanente.
USE OUR CONTENT
This story can be republished for free (details).
from Updates By Dina https://khn.org/news/hospitals-nursing-homes-fail-to-separate-covid-patients-putting-others-at-risk/
0 notes
Text
Is My Job Protected If I Refuse to Work Due to Health & Safety Risk of COVID-19?
What are my specific workplace health and safety rights during the COVID-19 crisis?
Your employer is required to take steps to ensure your safety and health, and to provide you with enough training and protection to do your job safely. Under the law, your rights include:
The right to be properly trained by your employer about safety on the job.
The right to be warned about hazardous materials to which you are exposed.
The right to be given protective gear if you work with hazardous or contaminated materials.
The right to make a confidential request for an inspection of your workplace by the Division of Occupational Safety & Health for safety and health standard violations.
The right to file a confidential complaint with the Division of Occupational Safety & Health if you observe or suspect a problem with safety or health at your workplace.
Employer retaliation over COVID-19 concerns
California Labor Code Section 6311 prohibits an employer to demote, terminate, harass or otherwise retaliate against "essential workers" who refuse to work in the presence of a health & safety risk. For example, your employer cannot retaliate against employees, including "essential workers," who refuse to establish social distancing rules and/or provide reasonable Personal Protection Equipment (e.g., masks, face shields, whatever else may be appropriate depending upon the work) where COVID-19 presents a risk.
In fact, the health and safety issue need not be related to COVID-19. Employees can refuse to perform work that presents workers with health or safety risks, regardless of the risk. If an employee has a reasonable concern for their health and safety (e.g., employer is violating Cal-OSHA and/or OSHA regulations), then they can choose not to work and be protected by statutes like Labor Code Section 6311.
For additional information, please contact Christopher Taylor of Taylor Labor Law, P.C. at (626) 219-6008 for an immediate, no-cost consultation.
#COVID-19
#non-essential worker
#essential worker
0 notes
Text
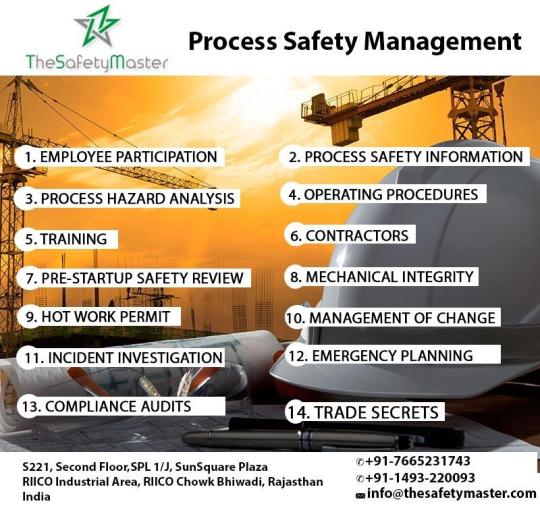
Process Safety Management for Hazardous Industry TheSafetyMaster™
Process Safety Management is one of the most important functions of the management of any of the industries that are within the Oil & Gas, Pharmaceutical, Chemical, Petrochemical, fuel-based Power Generation, and similar domains. This is because these industries generally handle tons of hazardous materials, that have the danger of fireside, explosion, damage to have assets, adverse effects on people, toxic leaks and environmental destruction. It has played an important role within the chemical processing industries in order to handle flammable liquids and gases could proceed without undesirable consequences.
The process design and technology, changes within the method, materials, and changes in materials, operations, and maintenance practices and procedures, training, emergency preparedness and other elements affecting the tactics must all be considered within the systematic identification and evaluation of hazards so on to determine whether or not they need the potential to steer to a catastrophe within the workplace and surrounding community.
Process safety management is an integral part of the chemical processing facility safety program. An effective process safety management program requires the leadership, support, and involvement of top management, facility management, supervisors, employees, contractors and contractor employees.
The PSM standard targets highly hazardous chemicals that have the potential to cause a catastrophic incident. The purpose of the quality as an entire is to assist employers in their efforts to stop or mitigate episodic chemical releases that would cause a catastrophe in the workplace and possibly in the surrounding community. Organizations need to develop the specified experience, expertise, judgment, and initiative within their workforce to properly implement and maintain an efficient PSM program and to prevent these sorts of hazards.
Even a robust process safety management program is subject to wear and tear if not properly maintained. In order to maintain the optimal performance of your PSM program, it’s very important that you continually review your plan that can support its integrity. This requires ongoing support from organization leadership, keeping your employees engaged and informed, and helping your team feel fulfilled, committed, and motivated across the board.
Additionally, TheSafetyMaster assists clients in implementing PSM programs and Process Safety Management Training that satisfy state regulatory requirements for their specific industry, such as the Cal/OSHA Process Safety Management for Refineries. This includes PSM elements such as the hierarchy of controls analysis, safeguard protection analysis, damage mechanism reviews, process safety culture assessments and management of change.
How TheSafetyMaster can Help
1. TheSafetyMaster provides training and certification for process safety management.
2. We have refined our models and methodologies in ways during which are often replicated, put into practice, tested and fine-tuned for nearly any situation or industry based on this vast operational experience.
3. TheSafetyMaster has a proven ability to customize solutions to help your organization prevent major process-related disaster incidents. Our team approach to preventing process-related injuries and managing operational risk and incidents addresses both the cultural and technical aspects of your organization.
4. We also provide proper documentation for the process safety management
Send us your enquiry to [email protected] or speak to our expert at +917665231743
0 notes
Text
Process Safety Management for Hazardous Industry
Process Safety Management is one of the most important functions of the management of any of the industries that are within the Oil & Gas, Pharmaceutical, Chemical, Petrochemical, fuel-based Power Generation, and similar domains. This is because these industries generally handle tons of hazardous materials, that have the danger of fireside, explosion, damage to have assets, adverse effects on people, toxic leaks and environmental destruction. It has played an important role within the chemical processing industries, in order to handle flammable liquids and gases, could proceed without undesirable consequences.
The process design and technology changes within the method, materials, and changes in materials, operations, and maintenance practices and procedures, training, emergency preparedness and other elements affecting the tactics must all be considered within the systematic identification and evaluation of hazards so on to determine whether or not they need the potential to steer to a catastrophe within the workplace and surrounding community.
Process safety management is an integral part of the chemical processing facility safety program. An effective process safety management program requires the leadership, support, and involvement of top management, facility management, supervisors, employees, contractors and contractor employees.
The PSM standard targets highly hazardous chemicals that have the potential to cause a catastrophic incident. The purpose of the quality as an entire is to assist employers in their efforts to stop or mitigate episodic chemical releases that would cause a catastrophe in the workplace and possibly in the surrounding community. Organizations need to develop the specified experience, expertise, judgment, and initiative within their workforce to properly implement and maintain an efficient PSM program and to prevent these sorts of hazards.
Even a robust process safety management program is subject to wear and tear if not properly maintained. In order to maintain the optimal performance of your PSM program, it’s very important that you continually review your plan that can support its integrity. This requires ongoing support from organization leadership, keeping your employees engaged and informed, and helping your team feel fulfilled, committed, and motivated across the board.
Additionally, TheSafetyMaster assists clients in implementing PSM programs and Process Safety Management Training that satisfy state regulatory requirements for their specific industry, such as the Cal/OSHA Process Safety Management for Refineries. This includes PSM elements such as the hierarchy of controls analysis, safeguard the protection analysis, damage mechanism reviews, process safety culture assessments and management of change.
How TheSafetyMaster can Help
1. TheSafetyMaster provides training and certification for process safety management.
2. We have refined our models and methodologies in ways during which are often replicated, put into practice, tested and fine-tuned for nearly any situation or industry based on this vast operational experience.
3. TheSafetyMaster has a proven ability to customize solutions to help your organization prevent major process-related disaster incidents. Our team approach to preventing process-related injuries and managing operational risk and incidents addresses both the cultural and technical aspects of your organization.
4. We also provide proper documentation for the process safety management.
0 notes
Text
California Cannabis: Breaking Down the CDPH Permanent Regulations
The State of California finally adopted permanent cannabis regulations earlier this month. In a series of posts, we’re going to cover the highlights of each agency’s permanent rules so that you know what big changes to expect during 2019. This post will cover the main changes (in our opinion) regarding the California Department of Public Health Manufactured Cannabis Safety Branch’s (“CDPH-MCSB”) permanent regs. Without further ado:
No more Farm Bill hemp-CBD ingredients or additives. It’s no secret that the California Department of Health Food and Drug Branch (“FDB”) has an issue with hemp-CBD. Specifically, an FAQ that issued from FDB last year made clear that FDB prohibits hemp-CBD in “Food” for humans and pets. Now, CDPH-MCSB is following suit (indirectly). Pursuant to new regulation 40175(c), “a manufacturer licensee shall only use cannabinoid concentrates and extracts that are manufactured or processed from cannabis obtained from a licensed cannabis cultivator.” What this means is that using Farm Bill hemp-CBD as an ingredient or addictive to cannabis manufactured products is not allowed unless it comes from a licensed cannabis cultivator. The protections of the Farm Bill won’t apply.
Owners and financial interest holders. I recently wrote about how it’s unclear as to how far the state will now go in finding and vetting entity owners and entity financial interest holders, especially since the Bureau of Cannabis Control (“BCC”) articulates in its rules that it intends to locate and vet every human possible in pretty much any ownership structure. But what about MCSB? MCSB entity owner regulations now state that “if the owner . . . is an entity, then the chief executive officer and members of the board of directors of the entity shall be considered owners,” and for financial interest holders, MCSB rules mandate only that “financial interest holders shall be disclosed on the application for licensure.” On balance, the BCC’s owner and financial interest holder rules are much more aggressive than MCSB, and the BCC’s comments to its owner and financial interest holder rules was that all agencies would apply the same standards for vetting. However, this clearly isn’t going to be the case if stakeholders go off of a plain reading of the law. Though it will be strange, the MCSB will very likely stick to its minimal vetting requirements while the BCC goes full bore on retailer, distributor, and lab owners and financial interest holders.
Changes in ownership. Again in contrast with the BCC, the MSCB is going to be much easier on changes in ownership of licensees. Under BCC regulations, if there’s a full buy-out of all existing owners, the entity can no longer operate while the change of ownership is being reviewed and processed by the BCC. The MCSB however has no such standard, at least not one that’s codified under the new regs. Specifically, for any changes of ownership or changes to financial interest holders, the MCSB expects the following protocol:
“The licensee shall notify the [MCSB] of the addition or removal of an owner through [the agency’s online system] within 10 calendar days of the change; Any new owner shall submit the information required [by law]; The [MCSB] shall review the qualifications of the new owner in accordance with [state law] and these regulations to determine whether the change would constitute grounds for denial of the license. The [MCSB] may approve the addition of the owner, deny the addition of the owner, or condition the license as appropriate, to be determined on a case-by-case basis; An owner shall notify the [MCSB] through [the state agency’s online system] of any change in their owner information . . . within 10 calendar days of the change; and a licensee shall notify the [MCSB] through [the state’s online system] of any change in the list of financial interest holders . . . within 10 calendar days of the change.”
Labeling. Labeling is still just as intense and comprehensive as it was under the emergency regulations. Now though, manufacturers need to ensure that, if a product container is separable from the outer-most packaging (e.g., a container placed inside of a box), the product container includes the following: (1) For edible cannabis products, topical cannabis products, suppositories, or orally-consumed concentrates, all information required for the primary panel except for cannabinoid content, and (2) for inhaled products (e.g., dab, shatter, and wax), the universal symbol (which is the black triangle with a cannabis leaf and an “!” with “CA” underneath). We also now (finally) have specific labeling requirements for pre-roll and packaged flower that didn’t exist before outside of the statute, itself. Overall, there are additional technical change requirements for labeling, including the weight of the product now needing to be in metric and U.S. customary units, specific labeling for flavoring in line with federal law, and more specific labeling restrictions for cannabinoid content.
Packaging. Until 2020, manufacturers are off the hook for providing child resistant packaging (“CRP”). Until then, retailers will bear the burden of CRP through the continued use of CRP exit packaging. Once CRP for manufacturers kicks in though, they’ll need to adhere to a litany of requirements, including compliance with the Poison Prevention Packaging Act of 1970 Regulations.
New product definitions. Via the permanent regulations, MCSB has introduced a number of newly defined terms, which is ultimately better for licensees so that confusion doesn’t abound as product development continues. For example, we now have as recognized definitions like:
“Infused pre-roll,” which means “a pre-roll into which cannabis concentrate (other than kief) or other ingredients have been incorporated”;
“Kief,” which means “the resinous trichomes of cannabis that have been separated from the cannabis plant”; and
“Orally-consumed concentrate,” which means “a cannabis concentrate that is intended to be consumed by mouth and is not otherwise an edible cannabis product. ‘Orally-consumed concentrate’ includes tinctures, capsules, and tablets . . .”
OSHA training. Given that cannabis remains federally illegal, people often think that violating one federal law somehow gives you a license to violate every federal law, which is entirely untrue. Under the permanent MCSB regulations:
“for an applicant entity with more than one employee, the applicant employs, or will employ within one year of receiving a license, one supervisor and one employee who have successfully completed a Cal/OSHA 30-hour general industry outreach course offered by a training provider that is authorized by an OSHA Training Institute Education Center to provide the course.”
Clearly, safety and federal compliance in the workplace still applies, even to cannabis operators, which is now demoralized under the permanent MCSB rules.
Changes to operations that now require state approval. As the state moves along with licensing and enforcement, it was inevitable that certain licensee actions would first require state approval. What this usually means is that major changes to your business or SOPs can’t go down without the state’s blessing, which can take weeks or months to secure. Specifically, for the MCSB, licensees will now have to report to and clear with the state the following action items before the licensee pulls the trigger on them (all to the tune of a $700 change application fee, which is non-refundable):
the addition of any closed-loop extraction method;
the addition of any other extraction method that necessitates a substantial or material alteration of the premises;
the addition of infusion operations if no infusion activity is listed in the current license application on file with the [MCSB] (you’ll also have to tell the state about “any changes to the product list on file with the [MCSB] and provide a new product list within 10 business days of making any change” to the products you’re making”); or
a substantial or material alteration of the licensed premises from the current premises diagram on file with the [MCSB].
Importantly, a “substantial or material alteration” includes: “the removal, creation, or relocation of an entryway, doorway, wall, or interior partition; a change in the type of activity conducted in, or the use of, an area identified in the premises diagram; or remodeling of the premises or portion of the premises in which manufacturing activities are conducted.” Be advised!
California Cannabis: Breaking Down the CDPH Permanent Regulations posted first on http://ronenkurzfeld.blogspot.com
0 notes
Text
California Cannabis: Breaking Down the CDPH Permanent Regulations
The State of California finally adopted permanent cannabis regulations earlier this month. In a series of posts, we’re going to cover the highlights of each agency’s permanent rules so that you know what big changes to expect during 2019. This post will cover the main changes (in our opinion) regarding the California Department of Public Health Manufactured Cannabis Safety Branch’s (“CDPH-MCSB”) permanent regs. Without further ado:
No more Farm Bill hemp-CBD ingredients or additives. It’s no secret that the California Department of Health Food and Drug Branch (“FDB”) has an issue with hemp-CBD. Specifically, an FAQ that issued from FDB last year made clear that FDB prohibits hemp-CBD in “Food” for humans and pets. Now, CDPH-MCSB is following suit (indirectly). Pursuant to new regulation 40175(c), “a manufacturer licensee shall only use cannabinoid concentrates and extracts that are manufactured or processed from cannabis obtained from a licensed cannabis cultivator.” What this means is that using Farm Bill hemp-CBD as an ingredient or addictive to cannabis manufactured products is not allowed unless it comes from a licensed cannabis cultivator. The protections of the Farm Bill won’t apply.
Owners and financial interest holders. I recently wrote about how it’s unclear as to how far the state will now go in finding and vetting entity owners and entity financial interest holders, especially since the Bureau of Cannabis Control (“BCC”) articulates in its rules that it intends to locate and vet every human possible in pretty much any ownership structure. But what about MCSB? MCSB entity owner regulations now state that “if the owner . . . is an entity, then the chief executive officer and members of the board of directors of the entity shall be considered owners,” and for financial interest holders, MCSB rules mandate only that “financial interest holders shall be disclosed on the application for licensure.” On balance, the BCC’s owner and financial interest holder rules are much more aggressive than MCSB, and the BCC’s comments to its owner and financial interest holder rules was that all agencies would apply the same standards for vetting. However, this clearly isn’t going to be the case if stakeholders go off of a plain reading of the law. Though it will be strange, the MCSB will very likely stick to its minimal vetting requirements while the BCC goes full bore on retailer, distributor, and lab owners and financial interest holders.
Changes in ownership. Again in contrast with the BCC, the MSCB is going to be much easier on changes in ownership of licensees. Under BCC regulations, if there’s a full buy-out of all existing owners, the entity can no longer operate while the change of ownership is being reviewed and processed by the BCC. The MCSB however has no such standard, at least not one that’s codified under the new regs. Specifically, for any changes of ownership or changes to financial interest holders, the MCSB expects the following protocol:
“The licensee shall notify the [MCSB] of the addition or removal of an owner through [the agency’s online system] within 10 calendar days of the change; Any new owner shall submit the information required [by law]; The [MCSB] shall review the qualifications of the new owner in accordance with [state law] and these regulations to determine whether the change would constitute grounds for denial of the license. The [MCSB] may approve the addition of the owner, deny the addition of the owner, or condition the license as appropriate, to be determined on a case-by-case basis; An owner shall notify the [MCSB] through [the state agency’s online system] of any change in their owner information . . . within 10 calendar days of the change; and a licensee shall notify the [MCSB] through [the state’s online system] of any change in the list of financial interest holders . . . within 10 calendar days of the change.”
Labeling. Labeling is still just as intense and comprehensive as it was under the emergency regulations. Now though, manufacturers need to ensure that, if a product container is separable from the outer-most packaging (e.g., a container placed inside of a box), the product container includes the following: (1) For edible cannabis products, topical cannabis products, suppositories, or orally-consumed concentrates, all information required for the primary panel except for cannabinoid content, and (2) for inhaled products (e.g., dab, shatter, and wax), the universal symbol (which is the black triangle with a cannabis leaf and an “!” with “CA” underneath). We also now (finally) have specific labeling requirements for pre-roll and packaged flower that didn’t exist before outside of the statute, itself. Overall, there are additional technical change requirements for labeling, including the weight of the product now needing to be in metric and U.S. customary units, specific labeling for flavoring in line with federal law, and more specific labeling restrictions for cannabinoid content.
Packaging. Until 2020, manufacturers are off the hook for providing child resistant packaging (“CRP”). Until then, retailers will bear the burden of CRP through the continued use of CRP exit packaging. Once CRP for manufacturers kicks in though, they’ll need to adhere to a litany of requirements, including compliance with the Poison Prevention Packaging Act of 1970 Regulations.
New product definitions. Via the permanent regulations, MCSB has introduced a number of newly defined terms, which is ultimately better for licensees so that confusion doesn’t abound as product development continues. For example, we now have as recognized definitions like:
“Infused pre-roll,” which means “a pre-roll into which cannabis concentrate (other than kief) or other ingredients have been incorporated”;
“Kief,” which means “the resinous trichomes of cannabis that have been separated from the cannabis plant”; and
“Orally-consumed concentrate,” which means “a cannabis concentrate that is intended to be consumed by mouth and is not otherwise an edible cannabis product. ‘Orally-consumed concentrate’ includes tinctures, capsules, and tablets . . .”
OSHA training. Given that cannabis remains federally illegal, people often think that violating one federal law somehow gives you a license to violate every federal law, which is entirely untrue. Under the permanent MCSB regulations:
“for an applicant entity with more than one employee, the applicant employs, or will employ within one year of receiving a license, one supervisor and one employee who have successfully completed a Cal/OSHA 30-hour general industry outreach course offered by a training provider that is authorized by an OSHA Training Institute Education Center to provide the course.”
Clearly, safety and federal compliance in the workplace still applies, even to cannabis operators, which is now demoralized under the permanent MCSB rules.
Changes to operations that now require state approval. As the state moves along with licensing and enforcement, it was inevitable that certain licensee actions would first require state approval. What this usually means is that major changes to your business or SOPs can’t go down without the state’s blessing, which can take weeks or months to secure. Specifically, for the MCSB, licensees will now have to report to and clear with the state the following action items before the licensee pulls the trigger on them (all to the tune of a $700 change application fee, which is non-refundable):
the addition of any closed-loop extraction method;
the addition of any other extraction method that necessitates a substantial or material alteration of the premises;
the addition of infusion operations if no infusion activity is listed in the current license application on file with the [MCSB] (you’ll also have to tell the state about “any changes to the product list on file with the [MCSB] and provide a new product list within 10 business days of making any change” to the products you’re making”); or
a substantial or material alteration of the licensed premises from the current premises diagram on file with the [MCSB].
Importantly, a “substantial or material alteration” includes: “the removal, creation, or relocation of an entryway, doorway, wall, or interior partition; a change in the type of activity conducted in, or the use of, an area identified in the premises diagram; or remodeling of the premises or portion of the premises in which manufacturing activities are conducted.” Be advised!
California Cannabis: Breaking Down the CDPH Permanent Regulations posted first on https://centuryassociates.blogspot.com/
0 notes
Text
California Cannabis: Breaking Down the CDPH Permanent Regulations
The State of California finally adopted permanent cannabis regulations earlier this month. In a series of posts, we’re going to cover the highlights of each agency’s permanent rules so that you know what big changes to expect during 2019. This post will cover the main changes (in our opinion) regarding the California Department of Public Health Manufactured Cannabis Safety Branch’s (“CDPH-MCSB”) permanent regs. Without further ado:
No more Farm Bill hemp-CBD ingredients or additives. It’s no secret that the California Department of Health Food and Drug Branch (“FDB”) has an issue with hemp-CBD. Specifically, an FAQ that issued from FDB last year made clear that FDB prohibits hemp-CBD in “Food” for humans and pets. Now, CDPH-MCSB is following suit (indirectly). Pursuant to new regulation 40175(c), “a manufacturer licensee shall only use cannabinoid concentrates and extracts that are manufactured or processed from cannabis obtained from a licensed cannabis cultivator.” What this means is that using Farm Bill hemp-CBD as an ingredient or addictive to cannabis manufactured products is not allowed unless it comes from a licensed cannabis cultivator. The protections of the Farm Bill won’t apply.
Owners and financial interest holders. I recently wrote about how it’s unclear as to how far the state will now go in finding and vetting entity owners and entity financial interest holders, especially since the Bureau of Cannabis Control (“BCC”) articulates in its rules that it intends to locate and vet every human possible in pretty much any ownership structure. But what about MCSB? MCSB entity owner regulations now state that “if the owner . . . is an entity, then the chief executive officer and members of the board of directors of the entity shall be considered owners,” and for financial interest holders, MCSB rules mandate only that “financial interest holders shall be disclosed on the application for licensure.” On balance, the BCC’s owner and financial interest holder rules are much more aggressive than MCSB, and the BCC’s comments to its owner and financial interest holder rules was that all agencies would apply the same standards for vetting. However, this clearly isn’t going to be the case if stakeholders go off of a plain reading of the law. Though it will be strange, the MCSB will very likely stick to its minimal vetting requirements while the BCC goes full bore on retailer, distributor, and lab owners and financial interest holders.
Changes in ownership. Again in contrast with the BCC, the MSCB is going to be much easier on changes in ownership of licensees. Under BCC regulations, if there’s a full buy-out of all existing owners, the entity can no longer operate while the change of ownership is being reviewed and processed by the BCC. The MCSB however has no such standard, at least not one that’s codified under the new regs. Specifically, for any changes of ownership or changes to financial interest holders, the MCSB expects the following protocol:
“The licensee shall notify the [MCSB] of the addition or removal of an owner through [the agency’s online system] within 10 calendar days of the change; Any new owner shall submit the information required [by law]; The [MCSB] shall review the qualifications of the new owner in accordance with [state law] and these regulations to determine whether the change would constitute grounds for denial of the license. The [MCSB] may approve the addition of the owner, deny the addition of the owner, or condition the license as appropriate, to be determined on a case-by-case basis; An owner shall notify the [MCSB] through [the state agency’s online system] of any change in their owner information . . . within 10 calendar days of the change; and a licensee shall notify the [MCSB] through [the state’s online system] of any change in the list of financial interest holders . . . within 10 calendar days of the change.”
Labeling. Labeling is still just as intense and comprehensive as it was under the emergency regulations. Now though, manufacturers need to ensure that, if a product container is separable from the outer-most packaging (e.g., a container placed inside of a box), the product container includes the following: (1) For edible cannabis products, topical cannabis products, suppositories, or orally-consumed concentrates, all information required for the primary panel except for cannabinoid content, and (2) for inhaled products (e.g., dab, shatter, and wax), the universal symbol (which is the black triangle with a cannabis leaf and an “!” with “CA” underneath). We also now (finally) have specific labeling requirements for pre-roll and packaged flower that didn’t exist before outside of the statute, itself. Overall, there are additional technical change requirements for labeling, including the weight of the product now needing to be in metric and U.S. customary units, specific labeling for flavoring in line with federal law, and more specific labeling restrictions for cannabinoid content.
Packaging. Until 2020, manufacturers are off the hook for providing child resistant packaging (“CRP”). Until then, retailers will bear the burden of CRP through the continued use of CRP exit packaging. Once CRP for manufacturers kicks in though, they’ll need to adhere to a litany of requirements, including compliance with the Poison Prevention Packaging Act of 1970 Regulations.
New product definitions. Via the permanent regulations, MCSB has introduced a number of newly defined terms, which is ultimately better for licensees so that confusion doesn’t abound as product development continues. For example, we now have as recognized definitions like:
“Infused pre-roll,” which means “a pre-roll into which cannabis concentrate (other than kief) or other ingredients have been incorporated”;
“Kief,” which means “the resinous trichomes of cannabis that have been separated from the cannabis plant”; and
“Orally-consumed concentrate,” which means “a cannabis concentrate that is intended to be consumed by mouth and is not otherwise an edible cannabis product. ‘Orally-consumed concentrate’ includes tinctures, capsules, and tablets . . .”
OSHA training. Given that cannabis remains federally illegal, people often think that violating one federal law somehow gives you a license to violate every federal law, which is entirely untrue. Under the permanent MCSB regulations:
“for an applicant entity with more than one employee, the applicant employs, or will employ within one year of receiving a license, one supervisor and one employee who have successfully completed a Cal/OSHA 30-hour general industry outreach course offered by a training provider that is authorized by an OSHA Training Institute Education Center to provide the course.”
Clearly, safety and federal compliance in the workplace still applies, even to cannabis operators, which is now demoralized under the permanent MCSB rules.
Changes to operations that now require state approval. As the state moves along with licensing and enforcement, it was inevitable that certain licensee actions would first require state approval. What this usually means is that major changes to your business or SOPs can’t go down without the state’s blessing, which can take weeks or months to secure. Specifically, for the MCSB, licensees will now have to report to and clear with the state the following action items before the licensee pulls the trigger on them (all to the tune of a $700 change application fee, which is non-refundable):
the addition of any closed-loop extraction method;
the addition of any other extraction method that necessitates a substantial or material alteration of the premises;
the addition of infusion operations if no infusion activity is listed in the current license application on file with the [MCSB] (you’ll also have to tell the state about “any changes to the product list on file with the [MCSB] and provide a new product list within 10 business days of making any change” to the products you’re making”); or
a substantial or material alteration of the licensed premises from the current premises diagram on file with the [MCSB].
Importantly, a “substantial or material alteration” includes: “the removal, creation, or relocation of an entryway, doorway, wall, or interior partition; a change in the type of activity conducted in, or the use of, an area identified in the premises diagram; or remodeling of the premises or portion of the premises in which manufacturing activities are conducted.” Be advised!
from Canna Law Blog™ https://www.cannalawblog.com/california-cannabis-breaking-down-the-cdph-permanent-regulations/
0 notes
Text
OSHA Focusing on Increase in Worker Fatalities
OSHA is seeking to stem a recent increase in workplace fatalities in Kansas, Missouri, and Nebraska. The Agency has seen an increase in fatalities associated with falls, struck-by objects and vehicles, machine hazards, grain bin engulfment, and burns.
In 2017, OSHA launched its “Safe + Sound Campaign,” urging employers to develop and implement a safety and health program that includes management leadership, worker participation, and a systematic approach to finding and fixing hazards. So far, the campaign has received commitments from 198 organizations.
“OSHA has investigated 34 fatalities in these three states since Oct. 1, 2017,” said OSHA Regional Administrator Kim Stille. “Working together with employers, unions, and employees, we can reduce these incidents. By implementing and sustaining workplace safety and health programs we can help employees avoid preventable injuries and fatalities. The agency has additional resources available to help employers of all sizes identify workplace hazards and eliminate them.”
Safety and health programs help reduce the numbers of workplace injuries and illnesses, and improve the bottom line. OSHA’s “Recommended Practices for Safety and Health Programs” offers practical advice on how an organization can create and integrate safety and health programs. To ask questions, obtain compliance assistance, or file a complaint, call OSHA’s hot-line at 800-321-OSHA (6742).
Hazardous Waste Training

Annual hazardous waste training is required for anyone who generates, accumulates, stores, transports, or treats hazardous waste. Learn how to manage your hazardous waste in accordance with the latest state and federal regulations. Learn how to complete EPA’s new electronic hazardous waste manifest, and the more than 60 changes in EPA’s new Hazardous Waste Generator Improvements Rule. Environmental Resource Center’s Hazardous Waste Training is available at nationwide locations, and via live webcasts. If you plan to also attend DOT hazardous materials training, call 800-537-2372 to find out how can get your course materials on a new Amazon Fire HD10 tablet at no extra charge.
Save the Date: Safe + Sound Week
OSHA’s second annual Safe + Sound Week will be held August 13-19, 2018. The event is a nationwide effort to raise awareness of the value of workplace safety and health programs. These programs can help employers and workers identify and manage workplace hazards before they cause injury or illness, improving a company’s financial bottom line. Throughout this week, organizations are encouraged to host events and activities that showcase the core elements of an effective safety and health program, including: management leadership, worker participation, and finding and fixing workplace hazards. For more information and to sign-up for email updates, visit the Safe + Sound Week webpage.
Emergency Response Complicated by Social Media Misinformation
The Department of Homeland Security (DHS) recently released a draft white paper to help first responders better understand and counter rumors, misinformation and false information on social media. The white paper details the four types of misinformation, as well as key challenges, case studies, and best practices for emergency responders to consider — some of which relate directly to how officials notify citizens when a crisis strikes.
Prevent Heat Illness
As summer temperatures rise, so do the dangers of working in high heat. That’s especially true in on hot days in milder climates, where workers tend to be used to working in mild weather and are frequently not accustomed to high temperatures.
As a result, Oregon OSHA encourages employers and workers in construction, agriculture, and other labor-intensive activities to learn the signs of heat illness and focus on prevention.
“Prevention really comes down to taking several important precautions,” said Penny Wolf-McCormick, health enforcement manager for Oregon OSHA. “They include regularly providing water, rest, and shade; gradually adapting workers to hot environments; and training employees to recognize signs of trouble and to speak up about them.”
Exposure to heat can lead to headaches, cramps, dizziness, fatigue, nausea or vomiting, and even seizures or death. From 2012 to 2017, 37 people received benefits through Oregon’s workers’ compensation system for heat-related illnesses.
The call to address the hazards of working in high heat is part of a larger effort aimed at preventing heat-related illness. Under an emphasis program run by Oregon OSHA, the agency’s enforcement and consultation activities will include a review of employers’ plans to deal with heat exposure, especially from June 15 through Oct. 1 of each year.
The prevention program applies to both outdoor job sites and indoor workplaces where potential heat-related hazards may exist. Oregon OSHA encourages employers to fill out a heat illness prevention plan. The plan outlines everything from risk factors and precautionary steps to locations of water and cooling areas.
You can get a sample heat illness prevention plan at http://osha.oregon.gov/OSHAPubs/pubform/heat-sample-program.pdf
Here are some tips for preventing a heat-related illness:
Perform the heaviest, most labor-intensive work during the coolest part of the day.
Use the buddy system (work in pairs) to monitor the heat.
Drink plenty of cool water (one small cup every 15 to 20 minutes).
Wear light, loose-fitting, and breathable clothing (such as cotton).
Take frequent short breaks in cool, shaded areas – allow your body to cool down.
Avoid eating large meals before working in hot environments.
Avoid caffeine and alcoholic beverages (these make the body lose water and increase the risk of heat illnesses).
To help those suffering from heat exhaustion:
Move them to a cool, shaded area. Do not leave them alone.
Loosen and remove heavy clothing.
Provide cool water to drink (a small cup every 15 minutes) if they are not feeling sick to their stomach.
Try to cool them by fanning them. Cool the skin with a spray mist of cold water or a wet cloth.
If they do not feel better in a few minutes, call 911 for emergency help.
You can calculate the heat index using the federal OSHA heat stress app for mobile phones: https://www.osha.gov/SLTC/heatillness/heat_index/heat_app.html.
North Florida Shipyard Cited for Safety Violations Following Employee Drowning
OSHA has cited North Florida Shipyards Inc., a shipbuilding and repair company, after an employee suffered fatal injuries at its Commodores Point facility in Jacksonville, Florida. The shipyard faces $271,061 in proposed penalties.
The worker drowned after a pressured air manifold struck him and knocked him into the St. Johns River. OSHA has cited the employer for safety violations, including exposing employees to being struck-by, drowning, amputation, caught-in, and electrical hazards; allowing scuba divers to be unaccompanied by another diver; and failing to ensure machine guarding.
“As this case demonstrates, it is important for employers to identify existing hazards, and follow required safety procedures to protect workers from serious injuries,” said OSHA Jacksonville Acting Area Office Director Buddy Underwood.
Marine Cargo Handling Company Cited for Fatal Forklift Accident at Port of San Diego
Cal/OSHA has issued citations to marine cargo handler SSA Pacific Inc. for willful and serious safety violations following the investigation of a fatal forklift accident at the Port of San Diego.
On January 3, a longshoreman was driving a forklift into a transit shed when he collided with a concrete support column and suffered fatal injuries after being thrown from the forklift. Cal/OSHA’s investigation found that the employee was not wearing a seatbelt and that the forklift had multiple safety devices disabled, including a seatbelt warning buzzer and mast interlock system designed to disconnect power from the hydraulic lift when the operator is unseated.
“Forklift safety and training of operators must be taken seriously,” said Cal/OSHA Chief Juliann Sum. “Employers must ensure that seat belts are used and that safety devices such as warning systems to ensure seat belt use are not altered.”
Cal/OSHA issued six citations totaling $205,235 in proposed penalties to SSA Pacific Inc., a division of Seattle-based international marine cargo handler SSA Marine.
The citations issued included four serious violations for the employer’s failure to ensure that forklift operators use seatbelts, properly maintain and inspect forklifts, ensure operators were effectively trained and for improperly altering forklift safety features. A general violation was cited for the employer’s failure to establish and maintain an effective heat illness prevention plan.
SSA Pacific was also issued a citation for a willful-serious violation as the employer failed to ensure workers perform a forklift safety check at the beginning of each shift and report unsafe conditions, a violation the company was cited for in 2016 following an accident inspection at the Port of Long Beach.
The incident in 2016 occurred when two workers improperly attempted to lift a 15-ton forklift from the hatch of a ship with a crane. One worker was hospitalized overnight for injuries to his ribs and lungs when he was pinned by the mast of the running forklift.
A citation is classified as willful when evidence indicates that the employer committed an intentional and knowing violation, or was aware that a hazardous condition existed and made no reasonable effort to eliminate it. A citation is classified as serious when there is a realistic possibility that death or serious harm could result from the actual hazard created by the violation.
Forklift safety requirements are summarized on page 65 of Cal/OSHA’s Pocket Guide for the Construction Industry.
Safety News Links
Worker Safety Rules Are Among Those Under Fire in Trump Era
Drinking Coffee Can Make You Live Longer
Two Amputations a Week: the Cost of Working in a Meat Plant
Open Offices are as Bad as They Seem
Senate Votes to Repeal Labor Laws That Safeguarded Vulnerable Workers
Walking Drunk Can be Deadly
Chemical Spill Reported at FedEx Facility
Protect Your Lungs from Wildfire Smoke
This post OSHA Focusing on Increase in Worker Fatalities appeared first on Environmental Resource Center.
from Blogger https://ift.tt/2JKKLWI
from WordPress https://ift.tt/2LiHNy2
0 notes
Text
Cal/OSHA Cites Tree Trimming Company in Brush Chipper Fatality
Visit Now - http://zeroviral.com/cal-osha-cites-tree-trimming-company-in-brush-chipper-fatality/
Cal/OSHA Cites Tree Trimming Company in Brush Chipper Fatality
Cal/OSHA has cited Gorilla Tree Service for serious and accident-related workplace safety violations following an investigation of a brush chipper accident that killed a 24-year-old worker in Napa.
On Aug. 15, 2017, the employee was reportedly working on the ground as part of a two-person crew removing limbs from a liquidambar tree when a rope used to lower limbs from an aerial bucket was caught and pulled into the chipper, strangling him.
Cal/OSHA’s investigation found that Gorilla Tree Service was unable to certify it had properly trained the worker, who had been employed at the company for about six months.
Cal/OSHA cited Gorilla Tree Service $23,200 for seven violations including one serious accident-related, one serious and five general violations for the employer’s failure to:
Provide documented training records for workers to certify that they had completed the required tree work and CPR training.
Brief workers before starting the job, including a description of hazards, work procedures and appropriate protective equipment.
Ensure the chipper was equipped, maintained and operated in accordance with the manufacturer’s recommendations. Cal/OSHA found the chipper’s moving parts of belt and pulley drives were not guarded as required.
Prevent entanglement hazards and unwanted material from entering the point of operation on the chipper.
Tree workers are 56 times more likely to suffer a fatal occupational injury than workers in all industries combined. The major causes of tree worker injuries and fatalities include falls, electrical shock, being struck by a tree branch, chainsaw lacerations, palm tree skirt collapses and ladder accidents, according to Cal/OSHA.
Cal/OSHA data shows that over the past six years, brush chipper-related incidents in California resulted in one fatality and four serious injuries:
A worker was killed in 2012 while feeding brush into a chipper in Nevada City when a rope binding the brush became entangled in the chipper drum and looped around the worker’s neck. The force on the rope was so great that the worker was decapitated.
In Los Angeles County in 2012, a worker was hospitalized from injuries caused by a chipper. Two workers were removing a tree using rope and a brush chipper. One of the workers was attached to a rope that abruptly went into the chipper pulling him toward the feeder. He was taken to the hospital with a punctured lung and fractures to his ribs, left arm, thumb and wrist.
In 2013, a Solano County worker lost his left ring finger when his wedding band suddenly became caught between the side frame of the feeding bay and the branch he was pushing into the brush chipper.
While operating a brush chipper in 2013, a worker in Concord was hospitalized. A truck rolled down a hill and jackknifed toward him while he was feeding brush into the chipper. Both of his legs became pinned between the truck’s side door and the frame of the chipper’s in-feed table. Both of his legs were fractured.
Cal/OSHA launched a tree work safety campaign in 2016 to help employees and employers prevent accidents, and made available a Tree Work Safety webpage, Tree Work Safety Guide, fact sheet and checklist.
“Tree work is a high-risk industry, and safety requirements are in place to protect workers from known hazards,” Cal/OSHA Chief Juliann Sum said in a statement. “Employers must ensure that workers are effectively trained to use brush chippers and other dangerous machinery safely.”
Want to stay up to date?
Get the latest insurance news
sent straight to your inbox.
0 notes
Text
OSHA Policy Modify on Monorail Hoists in Development
OSHA has declared a new enforcement plan that excludes monorail hoists from the demands of Subpart CC—Cranes and Derricks in Construction, as extended as businesses satisfy other OSHA demands.
The plan change was made in reaction to feedback from stakeholders and in recognition that a monorail hoist—which is attached to a mounted monorail mounted on gear this kind of as trucks, trailers, or scaffolding systems—is drastically diverse from other cranes and derricks in development.
Some monorail hoists can be prolonged and contracted in only a set horizontal path. They do not rotate, swing on a hinge, or boom out significantly farther than the gear on which they are mounted. They are often employed in design to hoist precast concrete factors, storage tanks, and mechanical equipment.
Beneath the new policy, the company will not cite companies for failing to meet the demands of Subpart CC if they fulfill the requirements of the overhead hoists and common education requirements.
The basic industry demands for monorail hoists stay intact.
Cleveland RCRA and DOT Training
Sign up for Hazardous Waste Management: The Comprehensive Course and DOT Harmful Resources Instruction: The Complete Course in Cleveland, OH, on July 25–27 and preserve $one hundred. To get advantage of this offer you, simply click right here or contact 800-537-2372.
Greensboro RCRA and DOT Training
Register for Hazardous Waste Management: The Full Course and DOT Dangerous Resources Instruction: The Total System in Greensboro, NC, on August 1–3 and preserve $one hundred. To consider advantage of this offer you, click listed here or contact 800-537-2372.
Dallas RCRA and DOT Coaching
Sign-up for Texas Dangerous Squander Administration and DOT Harmful Components Training: The Full Training course in Dallas, TX, on August 1–3 and conserve $100. iata certified courses To consider advantage of this supply, simply click right here or phone 800-537-2372.
Pentabromodiphenyl Ether Combination Shown as Carcinogen in California
Powerful July 7, 2017, California’s Office of Environmental Overall health Hazard Evaluation (OEHHA) extra pentabromodiphenyl ether combination [DE-seventy one (complex grade)] to the list of chemicals identified to the condition to cause most cancers for purposes of Proposition sixty five.
The listing of pentabromodiphenyl ether mixture [DE-71 (specialized grade)] was based on official identification by the Nationwide Toxicology Plan (NTP), an authoritative body, that the chemical leads to cancer. The requirements employed by OEHHA for the listing of chemicals underneath the “authoritative bodies” system can be located in Title 27, Cal. Code of Regs., segment 25306.
The documentation supporting OEHHA’s perseverance that the requirements for administrative listing have been pleased for pentabromodiphenyl ether combination [DE-seventy one (technical grade)] is incorporated in the “Notice of Intent to Checklist Pentabromodiphenyl Ether Mixture [DE-seventy one (Specialized Grade)]” posted on OEHHA’s internet site and published in the Could five, 2017 concern of the California Regulatory Recognize Register (Sign-up 2017, No. eighteen-Z). The publication of the discover initiated a general public remark period of time that shut on June 5, 2017. OEHHA gained no community comments on pentabromodiphenyl ether mixture [DE-71 (technical quality)].
A complete, updated chemical checklist is released in this concern of the California Regulatory Observe Sign up and is obtainable on the OEHHA internet site at http://oehha.ca.gov/proposition-65/proposition-65-record.
LSC Communications is a STAR of Office Basic safety and Wellness
LSC Communications North Plant of Crawfordsville, Indiana, accomplished recertification as a STAR website in Indiana’s Voluntary Security Program (VPP). LSC Communications is recertified for continuing and increasing excellence in place of work basic safety and wellness plans.
“LSC Communications prioritizes the protection and overall health of its workers, which makes for a great role model for other companies in the business,” mentioned Indiana Department of Labor Commissioner Rick J. Ruble. “Managers and employees at this intercontinental business recognize how to realize success by safeguarding by themselves and each other although getting the work completed.”
LSC's conventional and electronic print-associated solutions and business office items provide the wants of publishers, merchandisers, and retailers around the planet. The business is portion of the LSC Communications Inc., which employs far more than twenty,000 across the world. Crawfordsville’s North Plant is operated by a team of around 100 Hoosier employees.
Part of advertising an outstanding lifestyle of occupational security and health, the North Plant has created numerous personnel incentive programs to incorporate safety and neighborhood involvement. Personnel actively participate in the Crawfordsville Region Safety Motion Staff, along with “B SAFE” Hazard Recognition and Close to Miss Reporting plan. And lastly, they designed a “Lead & Shine” breakfast to offer managers an possibility to reward staff who go over and past safety and housekeeping expectations.
“LSC in Crawfordsville demonstrates a established accomplishment program at trying to keep their team protected,” mentioned Commissioner Ruble. “Their office incident and incident fee proceeds to stay low.”
For the last recorded three-12 months regular, the North Plant’s Total Situation Incident Charge (TCIR) was one.5, less than 50 % the business average of three.two.
Fort Wayne Cintas Web site Recertified STAR in State’s Basic safety and Overall health Program
Cintas Corporation Place G64 of Fort Wayne, Indiana, reached recertification as a STAR participant in the Indiana Voluntary Protection System (VPP). Along with Cintas’s more than 40 VPP websites throughout the place, Place G64 maintains the title of excellence and remains a model of proactive occupational basic safety and well being for Hoosier workers.
“We really don't award the STAR title in VPP easily,” said Indiana Division of Labor Commissioner Rick J. Ruble. “The title is earned by means of noticeable difficult function and devotion from each employees and professionals in protecting against incidents and eliminating dangers. The agency is very pleased to acknowledge the determination to protecting Hoosier staff the Cintas web site as demonstrated.”
One of Cintas Corporation’s roughly four hundred web sites, Spot G64 is a 36,seven-hundred square foot facility operated by a group of 89 personnel.
Spot G64 materials rental uniforms, entrance mats, restroom and cleanliness materials and promotional merchandise for firms in northeastern Indiana and western edges of Ohio. The facility also has a laundering process for clothes and bulk products, and a fleet of provider automobiles to provide goods.
The excellent tradition of office protection and wellness has proved fruitful by a effectively minimal recordable damage fee. Location G64’s Overall Case Incident Price (TCIR) for a 3-12 months regular is one.2 for each a hundred personnel, 75% considerably less than the national average of 5. In addition, the site’s Times Absent Limited or Transferred (DART) is .four, which is 88% considerably less than the nationwide average of 3.five.
0 notes
Text
California Cannabis: Breaking Down the CDPH Permanent Regulations
The State of California finally adopted permanent cannabis regulations earlier this month. In a series of posts, we’re going to cover the highlights of each agency’s permanent rules so that you know what big changes to expect during 2019. This post will cover the main changes (in our opinion) regarding the California Department of Public Health Manufactured Cannabis Safety Branch’s (“CDPH-MCSB”) permanent regs. Without further ado:
No more Farm Bill hemp-CBD ingredients or additives. It’s no secret that the California Department of Health Food and Drug Branch (“FDB”) has an issue with hemp-CBD. Specifically, an FAQ that issued from FDB last year made clear that FDB prohibits hemp-CBD in “Food” for humans and pets. Now, CDPH-MCSB is following suit (indirectly). Pursuant to new regulation 40175(c), “a manufacturer licensee shall only use cannabinoid concentrates and extracts that are manufactured or processed from cannabis obtained from a licensed cannabis cultivator.” What this means is that using Farm Bill hemp-CBD as an ingredient or addictive to cannabis manufactured products is not allowed unless it comes from a licensed cannabis cultivator. The protections of the Farm Bill won’t apply.
Owners and financial interest holders. I recently wrote about how it’s unclear as to how far the state will now go in finding and vetting entity owners and entity financial interest holders, especially since the Bureau of Cannabis Control (“BCC”) articulates in its rules that it intends to locate and vet every human possible in pretty much any ownership structure. But what about MCSB? MCSB entity owner regulations now state that “if the owner . . . is an entity, then the chief executive officer and members of the board of directors of the entity shall be considered owners,” and for financial interest holders, MCSB rules mandate only that “financial interest holders shall be disclosed on the application for licensure.” On balance, the BCC’s owner and financial interest holder rules are much more aggressive than MCSB, and the BCC’s comments to its owner and financial interest holder rules was that all agencies would apply the same standards for vetting. However, this clearly isn’t going to be the case if stakeholders go off of a plain reading of the law. Though it will be strange, the MCSB will very likely stick to its minimal vetting requirements while the BCC goes full bore on retailer, distributor, and lab owners and financial interest holders.
Changes in ownership. Again in contrast with the BCC, the MSCB is going to be much easier on changes in ownership of licensees. Under BCC regulations, if there’s a full buy-out of all existing owners, the entity can no longer operate while the change of ownership is being reviewed and processed by the BCC. The MCSB however has no such standard, at least not one that’s codified under the new regs. Specifically, for any changes of ownership or changes to financial interest holders, the MCSB expects the following protocol:
“The licensee shall notify the [MCSB] of the addition or removal of an owner through [the agency’s online system] within 10 calendar days of the change; Any new owner shall submit the information required [by law]; The [MCSB] shall review the qualifications of the new owner in accordance with [state law] and these regulations to determine whether the change would constitute grounds for denial of the license. The [MCSB] may approve the addition of the owner, deny the addition of the owner, or condition the license as appropriate, to be determined on a case-by-case basis; An owner shall notify the [MCSB] through [the state agency’s online system] of any change in their owner information . . . within 10 calendar days of the change; and a licensee shall notify the [MCSB] through [the state’s online system] of any change in the list of financial interest holders . . . within 10 calendar days of the change.”
Labeling. Labeling is still just as intense and comprehensive as it was under the emergency regulations. Now though, manufacturers need to ensure that, if a product container is separable from the outer-most packaging (e.g., a container placed inside of a box), the product container includes the following: (1) For edible cannabis products, topical cannabis products, suppositories, or orally-consumed concentrates, all information required for the primary panel except for cannabinoid content, and (2) for inhaled products (e.g., dab, shatter, and wax), the universal symbol (which is the black triangle with a cannabis leaf and an “!” with “CA” underneath). We also now (finally) have specific labeling requirements for pre-roll and packaged flower that didn’t exist before outside of the statute, itself. Overall, there are additional technical change requirements for labeling, including the weight of the product now needing to be in metric and U.S. customary units, specific labeling for flavoring in line with federal law, and more specific labeling restrictions for cannabinoid content.
Packaging. Until 2020, manufacturers are off the hook for providing child resistant packaging (“CRP”). Until then, retailers will bear the burden of CRP through the continued use of CRP exit packaging. Once CRP for manufacturers kicks in though, they’ll need to adhere to a litany of requirements, including compliance with the Poison Prevention Packaging Act of 1970 Regulations.
New product definitions. Via the permanent regulations, MCSB has introduced a number of newly defined terms, which is ultimately better for licensees so that confusion doesn’t abound as product development continues. For example, we now have as recognized definitions like:
“Infused pre-roll,” which means “a pre-roll into which cannabis concentrate (other than kief) or other ingredients have been incorporated”;
“Kief,” which means “the resinous trichomes of cannabis that have been separated from the cannabis plant”; and
“Orally-consumed concentrate,” which means “a cannabis concentrate that is intended to be consumed by mouth and is not otherwise an edible cannabis product. ‘Orally-consumed concentrate’ includes tinctures, capsules, and tablets . . .”
OSHA training. Given that cannabis remains federally illegal, people often think that violating one federal law somehow gives you a license to violate every federal law, which is entirely untrue. Under the permanent MCSB regulations:
“for an applicant entity with more than one employee, the applicant employs, or will employ within one year of receiving a license, one supervisor and one employee who have successfully completed a Cal/OSHA 30-hour general industry outreach course offered by a training provider that is authorized by an OSHA Training Institute Education Center to provide the course.”
Clearly, safety and federal compliance in the workplace still applies, even to cannabis operators, which is now demoralized under the permanent MCSB rules.
Changes to operations that now require state approval. As the state moves along with licensing and enforcement, it was inevitable that certain licensee actions would first require state approval. What this usually means is that major changes to your business or SOPs can’t go down without the state’s blessing, which can take weeks or months to secure. Specifically, for the MCSB, licensees will now have to report to and clear with the state the following action items before the licensee pulls the trigger on them (all to the tune of a $700 change application fee, which is non-refundable):
the addition of any closed-loop extraction method;
the addition of any other extraction method that necessitates a substantial or material alteration of the premises;
the addition of infusion operations if no infusion activity is listed in the current license application on file with the [MCSB] (you’ll also have to tell the state about “any changes to the product list on file with the [MCSB] and provide a new product list within 10 business days of making any change” to the products you’re making”); or
a substantial or material alteration of the licensed premises from the current premises diagram on file with the [MCSB].
Importantly, a “substantial or material alteration” includes: “the removal, creation, or relocation of an entryway, doorway, wall, or interior partition; a change in the type of activity conducted in, or the use of, an area identified in the premises diagram; or remodeling of the premises or portion of the premises in which manufacturing activities are conducted.” Be advised!
California Cannabis: Breaking Down the CDPH Permanent Regulations posted first on https://centuryassociates.blogspot.com/
0 notes
Last Seen Blogs

casalablumpkin
Casa La Blumpkin

chivalrain
行秋

chloe-beeholder
Queen Bee

thevictorofficial
The Victor

culturalsydney-blog
An Experience of Life "In Between Two Worlds" by Lucy Bessant