#fetal growth restriction
Photo
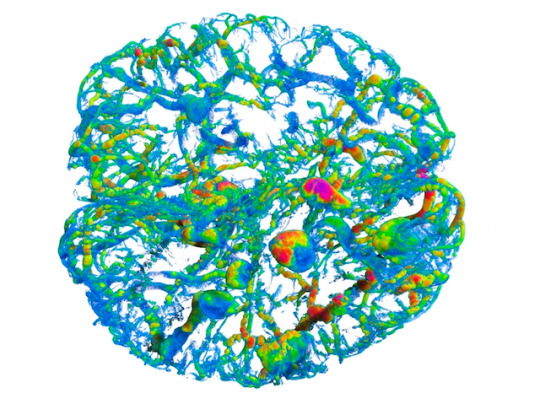
Feeding Foetuses
During pregnancy, a foetus needs a steady supply of nutrients via the placenta. If something goes wrong with the placenta, foetal growth restriction (FGR) can occur, which can be fatal. Currently, there's no treatment, other than early delivery. Research into treatments has proven challenging as animal models aren’t yet well-characterised enough to provide useful results for translation into human trials. Researchers now describe placenta function and structure in an FGR rabbit model. Rabbit foetuses and accompanying placentas were delivered 5 days after inducing FGR. Placentas were analysed using computed microtomography (normal placenta pictured, colours indicate vessel diameter) revealing fewer blood vessels in the region supplying nutrients to the foetus. What's more, the delivered foetuses showed behavioural and lung problems, with subsequent testing of their brains and lungs revealing structural changes too. This model highlights how placenta blood vessel changes coincide with brain and lung problems in foetuses during FGR.
Written by Lux Fatimathas
Image from work by Ignacio Valenzuela and colleagues
Department of Development and Regeneration, Cluster Woman and Child, Group Biomedical Sciences, KU Leuven, Leuven, Belgium
Image originally published with a Creative Commons Attribution 4.0 International (CC BY 4.0)
Published in Scientific Reports, November 2022
You can also follow BPoD on Instagram, Twitter and Facebook
#science#biomedicine#fetal growth restriction#foetal growth#intrauterine growth restriction#blood vessels#micro-ct
9 notes
·
View notes
Text
IUGR: Understanding Intrauterine Growth Restriction and Its Implications for Your Baby's Health
IntroductionCauses of IUGRSymptoms of IUGRDiagnosis of IUGRTreatment of IUGRRisks Associated with Intrauterine Growth Restriction (IUGR)Prevention of IUGRFacts and Tips Maternal stress and anxiety can contribute to IUGR:Adequate sleep is crucial for fetal growth: Omega-3 fatty acids may improve fetal growth:IUGR baby may be at higher risk for developmental delays:Certain medications can cause…

View On WordPress
#baby&039;s health#fetal development#fetal growth#fetal health#Intrauterine Growth Restriction#IUGR#maternal health#pregnancy#pregnancy complications#Pregnancy Health#prenatal care
1 note
·
View note
Text
Researchers from Western and Brown University have made groundbreaking progress towards identifying the root cause and potential therapy for preeclampsia.
The pregnancy complication affects up to eight per cent of pregnancies globally and is the leading cause of maternal and fetal mortality due to premature delivery, complications with the placenta and lack of oxygen.
The research, led by Drs. Kun Ping Lu and Xiao Zhen Zhou at Western, and Drs. Surendra Sharma and Sukanta Jash at Brown, has identified a toxic protein, cis P-tau, in the blood and placenta of preeclampsia patients.
According to the study published in Nature Communications, cis P-tau is a central circulating driver of preeclampsia – a “troublemaker” that plays a major role in causing the deadly complication...
“The root cause of preeclampsia has (so far) remained unknown, and without a known cause there has been no cure. Preterm delivery is the only life-saving measure,” said Lu, professor of biochemistry and oncology at Schulich School of Medicine & Dentistry...
“Our study identifies cis P-tau as a crucial culprit and biomarker for preeclampsia. It can be used for early diagnosis of the complication and is a crucial therapeutic target,” said Sharma...
Until now, cis P-tau was mainly associated with neurological disorders like Alzheimer’s disease, traumatic brain injuries (TBI) and stroke. This association was discovered by Lu and Zhou in 2015 as a result of their decades of research on the role of tau protein in cancer and Alzheimer’s.
An antibody developed by Zhou in 2012 to target only the toxic protein while leaving its healthy counterpart unscathed is currently undergoing clinical trials in human patients suffering from TBI and Alzheimer’s Disease. The antibody has shown promising results in animal models and human cell cultures in treating the brain conditions.
The researchers were curious whether the same antibody could work as a potential treatment for preeclampsia. Upon testing the antibody in mouse models they found astonishing results.
“In this study, we found the cis P-tau antibody efficiently depleted the toxic protein in the blood and placenta, and corrected all features associated with preeclampsia in mice. Clinical features of preeclampsia, like elevated blood pressure, excessive protein in urine and fetal growth restriction, among others, were eliminated and pregnancy was normal,” said Sharma.
Sharma and his team at Brown have been working on developing an assay for early detection of preeclampsia and therapies to treat the condition. He believes the findings of this study have brought them closer to their goal...
“The results have far-reaching implications. This could revolutionize how we understand and treat a range of conditions, from pregnancy-related issues to brain disorders,” said Lu.
-via India Education Diary, September 22, 2023
#preeclampsia#maternal mortality#infant mortality#medical news#medical research#alzheimers#biology#pregnancy complications#good news#hope
315 notes
·
View notes
Text
My Future in You | 2.3 | Bradley Bradshaw x Reader
Previous Chapter | Next Chapter | Masterlist
Synopsis: Bradley’s twenty-two years old and not where he’s supposed to be. He’s supposed to be out of the academy by now. Instead, he’s retaking his senior year of college and praying to god that he gets into flight school. Mav’s gone, his mom’s gone. He’s mad at the world. Then, a hook up at a Halloween party changes his future even more than he could have imagined.
Warnings: accidental pregnancy, references to abortion in a few chapters, angst, will be fluff eventually, enemies to lovers kinda thing, mentions of pregnancy / birth complications, mentions of not eating frequently, lack of hunger
…
The drive home in silence just gives Bradley’s anger time to multiply, growing until he’s so restless that his car door is open before the engine is even off. He slams it behind him, knuckles white around the strap of his bag as he walks around to the front door. That slams too.
It startles you, making you flinch and almost drop the mug in your hand. The now lukewarm coffee that you’ve been trying to sip at for an hour spills down onto the white of your sweater. It’s just a small mark, easy enough to ignore.
His brows knit together slightly as he catches sight of your face from the other end of your open living space. The whole way here, it had felt like he practically had steam coming out of his ears. His palms are still reddish and warm from how tightly he was grabbing the wheel. But, he sees it in the way you’re looking at him and knows that his thing — all of the anger, resentment, blinding rage that Mav brings up in him — it doesn’t matter.
Immediately, he lets his bag, and everything that seeing Mav had just stirred up within him, go.
“What’s wrong?” He’s already rushing forwards, heading for you.
You had promised yourself that you wouldn’t do this and that you wouldn’t freak him out by crying. It just happens. A soft, heartbroken squeak as he reaches you and you throw yourself against his chest.
“Did something happen at the appointment?” He breathes out, wrapping his arms around you and squeezing.
“It’s — it’s not that bad, but he…” You have to pull back and force yourself to breathe to even attempt at the words. “He’s smaller than he should be, and the doctor gave me this pamphlet, and I’ve just been freaking out all day.”
Bradley secures you against him with one arm and turns his attention to the little orange leaflet on the counter with a smiling baby girl with glasses on the front of it. He presses his lips softly to the top of your head. With his free hand, he cautiously opens up the front page.
Your hands curl into the fabric of his khakis, breathing him in, pulling him closer to you. It takes him a few moments, to read what it says and to process it. He never once lets you go.
Just giving a small shake of his head, he exhales and squeezes you closer. “Okay. What did the doctor say we need to do?”
“I need to go for a blood test on Friday and another ultrasound on Tuesday. She said that I should be eating healthy, and more frequently, um — eight hours of sleep, rest. If it’s fetal growth restriction then he could have issues during birth or even after.”
Bradley cups your face in his hands and nods slowly. You can feel his heartbeat in his chest and it just doesn’t make sense that he’s able to appear so calm when you know that he isn’t.
“Okay,” He nods, his voice low. “Alright. When was the last time you ate?”
“I had a sandwich for lunch but I just don’t feel hungry, I’ve been crying all day.” You mumble out as he presses closer to you, smoothing a large palm down your back. You nuzzle your cheek against his shirt, exhaling slowly.
Both of you stand in the kitchen, holding each other close, shit scared of what this means. This future that you have committed absolutely everything to, this little thing that you’re so ready to love, and the fear that there could be absolutely no way of protecting it.
Bradley closes his eyes and turns his face towards yours, hugging you closer. His memories of his dad are fuzzy. His memories of his mother back then are fuzzy too. He doesn’t remember her crying much. He remembers them laughing a lot. Standing here, he wishes he had at least one clear memory left — just so that he’d know what to do now.
Most people probably get to share these worries with their parents, to ask them these questions. You’ve just got each other.
He doesn’t know what to do. The silence is setting in and the orange on that pamphlet feels like it’s becoming more obnoxious by the second.
“Well, I’ll cook tonight, and I’ll be really offended if you don’t finish what I make you.” It’s half playful, he presses his lips to your cheek and pulls back to look at you, fingers trembling against your sides, “It’s just been a stressful couple of months, you just need to relax these last few weeks. ‘M gonna take care of you.”
Crowded against the kitchen counter, you take a few seconds to just be held by him, tucking yourself back in against his chest.
You imagine your mother, probably staring at those six missed calls and feeling smug with herself — knowing that you’d have come crawling back for help eventually. You’re an idiot for thinking that she would’ve been able to help. You tug Bradley closer and press your face into his shoulder. Maybe she’s not really doing that. Maybe she’s sitting there and wondering if she should call you back. Either way, it doesn’t matter.
Everything you’ve given up and gone through, this new family that you’ve scraped together, it’s all that you need.
“You wanna come to the store with me or you wanna take a nap?” Bradley asks you, smoothing his hands down along your middle.
Your answer is immediate, filling the air before silence has a chance to set in.
“I don’t want to be on my own.” You admit, exhaling softly into the warmth of his chest. Bradley nods and kisses your temple. He keeps it to himself that he’s pleased with your answer. After the mood he was in and the day that you’ve had, he just wants you where he can see you.
So, the two of you take your car. It’s easier to get into than trying to haul yourself up into the bronco these days. It’s more of a family car. It’s crazy, actually, how much you’re starting to look like a family. Him, in his uniform and an arm draped around you, your hand resting on your swollen stomach.
He drives with his hand on your thigh, your arm looped through his. Then, once you’re in the store, he pushes the cart with you at his side.
“I could ask you what you want, or I could surprise you. What are you two in the mood for?” Bradley asks, leaning down to kiss the top of your head as you hug his arm.
“I’m not hungry, I don’t know.” You shake your head softly.
“Surprise it is.” Bradley decides, taking his arm out from the loop you’re holding it in and draping it around your shoulders instead. He pulls you in against his side and presses his palm over both of your eyes, covering your vision with a sudden darkness.
“Bradley, I’m seriously going to fall break my face!” You gasp, grabbing at his hand. You don’t even notice it. He beams with pride as you smile, finally.
He nudges you in front of him, between him and the cart, laughing softly as he guides you forwards, blind. “Have a little faith in me, I’m not gonna let anything happen to you. Just can’t risk you seeing my ingredients and ruining my surprise.”
“You’re an idiot,” You giggle, grabbing tightly onto the cart to steady yourself. He grins, kissing your cheek. “I’m so scared right now.”
“Scared? — C’mon, Mama, you’ve gotta start trusting me. I’ve got you.” Bradley teases, pressing his mouth to you jaw, pressing his chest into your back and making your laugh harder. He slows you, then stops. “Stay there, I’m grabbing something. Don’t open your eyes.”
Your heart flutters as his hands briefly leave you. There’s a chill in the supermarket without his body crowding around you to keep you warm. He’s back quickly anyway, something clatters into the cart.
“What a beautiful family you are!” The voice is soft, pleasant sounding. An older lady. You peek one eye open and find her beaming at you from a few feet away.
“Thank you.” Bradley answers, surging with pride as he puts a polite amount of space between you and him, still close enough to keep you bracketed between him and the cart.
“You’ll do just fine, making each other laugh like that,” Her eyes as crinkling at the corners, a smile spreading across her aged face. She looks fondly between the two of you, then nods. “Congratulations on the little one. How lovely. Your first?”
“Yes, Ma’am.” Bradley answers. You almost sigh in relief that he’s not choosing now to try to make funny jokes.
“How lucky they will be, to have parents so in love.” She smiles. Bradley’s hand covers yours over the top of the cart, knitting his fingers through yours. Neither one of you says a word, at first. You’ve not said that yet. Technically, you’ve only been together for a few weeks. “You two have a lovely day.”
“You too, thank you.” Bradley remains polite, smiling at her softly. She looks the two of you over, fondly, almost reminiscent, and then she walks away.
Bradley catches you off guard, tearing you back away from your own thoughts as he covers your eyes once more. His lips press to your earlobe as he growls playfully, “You better not have checked out my ingredients, Seresin.”
“You’re paranoid.” You tell him, blinded under his palm, grinning dumbly as you let him guide you forwards again.
He hums playfully, pressing a gentle kiss to your neck, “Mm, I just know what Seresins are like.”
“Your baby’s going to be one,” You point out. He chuckled behind you. “You’re gonna be outnumbered.”
He uses his hold on your face to turn your head, leaning over your shoulder and kissing your lips. “Can’t wait.”
So, like the love-sick fool that you are, you let him lead you blindly around the grocery store, whispering jokes into your ear and planting playful kisses onto your neck. Your heart’s swollen and you’re so confused about how it could ever have been hurt by this same person.
Finally, after making you promise not to look several times, he uncovers your eyes and hands you the keys. Your feet are sore and there’s no point waiting in the checkout line with him. He watches you waddle out of the store with a dumb grin on his face.
It makes him want to grin as big as he can, watching the changes that come with your pregnancy. Not being able to tie your shoe laces anymore, knocking things off of the bathroom counter with your belly — waddling is a new one. It’s a special type of adorable, he’s certain that he’ll never grow tired of seeing it.
Loading your items onto the checkout, he pulls his phone from his pocket and waits, unaware of the eyes on him.
It was made abundantly clear earlier, that Bradley had no desire to speak to Maverick. He had turned, looked, and swiftly walked away. That familiar red flush covering his face and neck. He’s had that since he was in diapers, blushing a deep shade of pink whenever he was upset about something.
But now, for Maverick to be standing in a grocery store, staring at the kid that he hasn’t seen in almost two years, for the second time in the same day — it feels like fate.
He drops his items down onto a random shelf and silently walks towards the checkout as Bradley loads his groceries back into the cart.
“Bradley?”
Bradley looks up, finding Pete staring at him again. His face goes blank, and he straightens up like a cat raising its heckles. Pete doesn’t move. Bradley turns swiftly and walks out of the store without a word.
You get out of the car as you see him coming, your smile fading slightly as you notice the look on his face. That hardened, terracotta flushed look.
“Are you okay?”
“Yeah, let’s just go home.” Bradley practically tears open the trunk. Your brows draw together as you watch him load the groceries into it.
There’s a feeling, something in your peripheral that makes you turn your head. There’s a man standing by the edge of the parking lot, the colour drained from his face, staring right at you.
Pete’s head spins, heat flooding his nerves.
Looking at Bradley already feels like he’s got to be eye-to-eye with a ghost. Now, he’s standing there and suddenly it’s the summer of 1984, and his best friend’s about to have a kid. The picture’s fuzzy now, as it sits in Pete’s wallet, but it’s clear as day in his mind. Goose and Carole on the end of the Santa Monica boardwalk. She’s so pregnant that she could barely walk, but she was beaming — she had demanded to go to the beach that day.
He studies the crystal clear image before him now. Bradley in his khakis from work. The pregnant girl who’s smile has just faded, staring back at him.
Bradley takes one look at your face and then turns, following your gaze.
“Do you know that guy?” You ask gently, glancing up at Bradley.
“Wait in the car for me.” He answers you, slamming the trunk shut and turning. His pace is purposeful, storming across the parking lot until he’s almost nose-to-nose with Pete.
“What do you want?” Bradley spits.
“You… You’re having a kid?” Pete breathes out, confused, shaking his head. The reality of it hasn’t quite set in yet.
“I said: what do you want?” The same angry kid as he knew before stands in front of him again. Pete shakes his head again.
“You’re not ready to be a parent.”
“Just like I wasn’t ready to be a pilot?” Bradley answers back. You watch from beside the car as he steps closer to the older man, squaring his shoulders like he’s about to hit him.
“Think about your future! I mean — have you even thought this throu—“
“Don’t talk to me about my future after what you did.” He barks, loud enough for you to hear finally, eyes ablaze, shoulders squared. Maverick always forgets how much Bradley has grown. He looks up slightly as Bradley walks closer to him.
Maverick looks now to you, with one hand on your stomach and a confused look on your face.
“This isn’t what I wanted for you.” Maverick admits quietly. He’s not sure what makes him say it, it’s already too late, you look pretty far along. But, he says it anyway. When it comes to Bradley, there’s this intense need to do the right thing that usually propels him into doing the wrong thing.
“I didn’t mean — I shouldn’t have —“ Maverick stutters, shaking his head. It always ends like this. He always does the wrong thing. He sees the worry in your eyes. He always upsets Bradley without meaning to. “I’m sorry. Can we talk about this?”
“I don’t give a shit what you want, Mav,” Bradley shakes his head, disbelief. He stops walking finally and points a finger into Pete’s chest, deadly serious — less emotional than last time. “Stay the fuck away from me, stay the fuck away from my family.”
Blue eyes widened, serious, Maverick stares back at the boy before him. Bradley’s always had a temper, that’s nothing new. The sincerity in his tone is. He’s serious about you, it seems.
“Bradley?”
Both of them turn their heads to look at you at the same time. You swallow. His mouth sets into a hard line and it almost makes you wince. You’ve seen this before; it almost always winds up with you getting hurt.
It’s growing colder now that the sun has set. After the day you’ve had, you miss the days when you could take a hot bath. Going home and crawling under your covers would be enough at this point.
“I’m serious,” Bradley says slowly, giving his uncle a quick once over, and then taking a step back with a shake of his head. “You will never be family to me. Leave me alone.”
Without giving the man who had raised him time to argue, Bradley turns and walks back to the car, grinding his jaw.
“Who was that?” You frown.
“Come on,” Bradley sighs, shaking his head as he tugs open the passenger side door and motions for you to get in. “I’ll tell you later. I just want to go.”
You’ve seen Bradley angry — you’ve seen him being an asshole just for the sake of it. This isn’t that. You’ve never seen him rattled like this. So, you get in the car and you let him take you home, pretending not to see the way that the dark haired man watches you car pull out of the lot.
You let him cook for you and tell you about his week. You eat everything he makes you and he grins, proud of himself. After that, he insists that you spend the rest of the evening in bed. So, you do.
You spend it laying sideways with your head resting on his stomach and your legs dangling over the edge, his fingers toying with stands of your hair.
“So, who was that guy?” You ask finally.
And so, he tells you about Pete Mitchell for the first time. The man who raised him. Uncle Pete who let him stay up late and eat pizza, who came over on the days that Bradley’s mom just couldn’t stop crying. Uncle Pete who sometimes forgot that he promised to come to baseball games or pissed off an admiral and wound up in the middle of the ocean for a couple of months, so couldn’t come to that birthday party anymore.
The let downs and the wonderful memories weigh each other out. For every upside, there’s a downside with Maverick. And then it gets to Bradley’s senior year of high school, when Mav betrayed him. They hadn’t spoken since, other than at Carole’s funeral, briefly. That had gone worse than today had.
You squeeze his hand softly. “I’m sorry.”
“It’s alright,” Bradley says quietly. He smooths his hand down across my stomach. “I’m sorry that I did that in front of you. I’ve been trying to—“
You turn your head, pressing your lips gently to his knuckles. “I know.”
He exhales slowly. You know exactly how hard he had been trying for you.
“I love you.” You decide finally, leaning your head back so that you can look at him. Bradley raises his eyebrows. He’s had a couple of girls say it to him before, he’s never felt inclined to say it back. He would’ve never told them about Maverick, about his mother. He wouldn’t have ever been lying here with them, like this.
“I love you too.” He takes his hand away from your hair and strokes it along your jaw instead. You push yourself up, turning slowly towards him, kissing his lips chastely.
“We’re going to be alright. Right?” You ask quietly, resting your hand against his bare chest. His eyes soften just slightly as he gives you a calm nod.
…
@chaoticweirdogeek @alanadetigy @itsmytimetoodream @oldnatgwenaccount @khaylin27 @bioodforbiood @luckyladycreator2 @mizzzpink @cherrycola27 @unordinare @shanimallina87 @marvel-f1-and-more @heli991113 @pauv-0414 @ghxst-heart @momc95 @asteria33 @lilyevanswhore @diamond-3 @galaxy-moon @jostyriggslover96 @forgiveliv @shawnsblue @little-wiseone @lovemesomevesey @alm334 @averyhotchner @diorrfairy @thedroneranger @batdanceq @wkndwlff @littlemissobsessedwitholdermen @sunflowerziva @cassiemitchell @himbos-on-ice @bradshawseresinbabe @damrlovq @fudge13 @xoxabs88xox @mak-32 @slutfordw
#bradley bradshaw#bradley rooster bradshaw#miles teller#bradley bradshaw smut#rooster x you#rooster bradshaw imagine#top gun smut#bradley bradshaw x reader#bradley bradshaw au#my future in you#MFIY
634 notes
·
View notes
Text
Carter Sherman at The Guardian:
Awash in soft, peach-colored light, the infant yawns, sticks her thumb in her mouth and flutters her eyes at the camera. As the camera pulls away from her, an umbilical cord and the fleshy tunnel surrounding the infant comes into focus. This isn’t a newborn baby: it’s a fetus in a disembodied womb.
“This is Olivia,” a British female voice narrates. “Though she has yet to greet the outside world, she has already completed an amazing journey.”
Say hello to “Meet Baby Olivia”, an animated video made by an American anti-abortion group that purports to depict humans’ embryonic and fetal development in an alleged effort to convert young people to the anti-abortion cause. The video – or something very close to it – will be required viewing for public school students in two states, with several more potentially on the way.
Last year, North Dakota became the first state in the nation to pass a law mandating that schools screen “Meet Baby Olivia” or a similar video. This year, Tennessee enacted its own “Meet Baby Olivia” law, requiring that “Meet Baby Olivia” or something like it be shown as part of schools’ sex education curriculum.
So far in 2024, legislators in at least 10 other states have introduced bills that would require schools to show students “Meet Baby Olivia” or, in language that appears repeatedly throughout the bills, a similar “high-quality, computer-generated rendering or animation” that shows “every stage of human development inside the uterus, noting significant markers in cell growth and organ development for every significant marker of pregnancy until birth”. Including Tennessee’s legislation, bills in at least five of the states cite “Meet Baby Olivia” by name.
Classrooms are a burgeoning front in the post-Roe v Wade abortion wars, as conservative activists have increasingly intertwined their attacks on abortion with their distaste for sex ed that discusses alternatives to premarital abstinence. But medical professionals have accused the anti-abortion group behind “Meet Baby Olivia” of spreading propaganda and even misinformation in order to convert young people to their cause.
Seven of the 12 states where the bills have been introduced or passed ban almost all abortions. So far this year, state legislatures have considered at least 135 sex-ed bills – a record number, according to a CNN analysis. Sixty per cent of them would restrict sex ed in some way.
Live Action has denied accusations that any sentence of “Meet Baby Olivia” is inaccurate.
“‘Baby Olivia’ isn’t about abortion. It never says the word ‘abortion’,” said Noah Brandt, Live Action’s vice-president of communications. “‘Baby Olivia’ is an important place for states like Tennessee and North Dakota to turn to next, to continue to do work to educate on both biology and life, because they’ve already protected life so now it’s about teaching people when life begins and to respect that.”
A quiet success story
The emergence of the “Meet Baby Olivia” legislation comes at a precarious time for the anti-abortion movement. Since the overturning of Roe, support for abortion rights has mounted even in conservative states. Some Republicans have tried to downplay their opposition to the procedure or even supported efforts to protect it, in a sharp departure from decades of marching in lock step with the anti-abortion movement.
But as the anti-abortion movement flounders, the “Meet Baby Olivia” bills are a quiet success story. Abortion opponents overturned Roe by spending years pushing for state-level abortion restrictions; if a restriction was successful in one state, lawmakers in other states would copy-paste its language and introduce their own versions. This strategy gnawed away access to abortion.
In the “Meet Baby Olivia” bills, observers see a similar strategy at play – and evidence of mission creep.
“Anti-abortion, anti-sexual and [anti]-reproductive health movements have been focusing on other areas and expanding their scope in terms of what is relevant to them and what they’re working on,” said Kimya Forouzan, principal policy associate of state issues at the Guttmacher Institute, which supports abortion rights. Although Guttmacher tracks restrictions on sexual and reproductive health, Forouzan said that she had never before seen legislation quite like the “Meet Baby Olivia” bills.
[...]
In at least two states, West Virginia and Iowa, “Meet Baby Olivia” bills passed one legislative chamber, but both state legislatures have now shuttered for the year. Most of the legislatures that introduced “Meet Baby Olivia” bills have either ended their 2024 sessions or are set to do so in the next few weeks.
Compared to the rest of the country, the states that have introduced “Meet Baby Olivia” bills this year – which also include Georgia, Hawaii, Kentucky, Michigan, Missouri, Pennsylvania, and South Carolina – have less comprehensive sex-ed policies, according to Siecus: Sex Ed for Social Change, a decades-old organization that issues best practice guidelines for comprehensive sex ed. (None of the states garnered more than a C grade in the Siecus ranking system.) Most states do not require public school sex ed to be medically accurate, culturally appropriate or unbiased, according to Guttmacher. Only four states say that sex ed cannot promote religion.
The Guardian reports on the disturbing trend of red states pushing new bills that require the showing of the propagandistic "Baby Olivia" video by anti-abortion extremist group Live Action in classrooms as part of the right-wing war on sex ed in schools.
#School Curriculums#Abortion#Indoctrination#Anti Abortion Extremism#Schools#Meet Baby Olivia#Live Action#Noah Brandt#Sex Education#Abstinence#Abstinence Only#Iowa HF2617#West Virginia SB468#SIECUS#North Dakota HB1265
23 notes
·
View notes
Text

When New York politicians legalized late-term abortions in January, Hannah Sudlow thought of her 2-year-old daughter Evelyn and the discrimination she faced while still in the womb.
In an interview with Live Action News, Sudlow said doctors immediately assumed she wanted an abortion after Evelyn was diagnosed with a fatal fetal anomaly. They even scheduled an abortion without asking her.
But Sudlow and her husband refused. They knew that their daughter’s life was too precious to end.
“She is our greatest, greatest, greatest joy,” Sudlow said. “She has brought so much love and life to our family. The only tragedy would have been to never have met Evelyn. She has brought so much to our life.”
The trouble began at Sudlow’s 20 week ultrasound. After the initial scan detected problems, she said they were sent to a doctor for more testing. The doctor’s attitude was not what they expected.
“He said, ‘Basically everything is wrong with this child. She has cysts on her brain. She is four weeks behind on her growth. She has intrauterine growth restriction, a hypo-plastic left ventricle, a single ventricle heart. She is missing half her heart. She has a cleft palate, clenched fists, and oh, by the way, two clubbed feet. Oh and by the way, it’s a girl,’” Sudlow said.
137 notes
·
View notes
Text
women prenatal
Prenatal vitamins are a fundamental mix of important vitamins and minerals that are critical for the development of the unborn child as well as the well-being of the pregnant mother. women prenatal-Beli Best Women prenatal Vitamins (Review 2024)
They are needed for women's prenatal health. Folic acid, also known as folate, calcium, iron, vitamin D, and iodine are often included in this specific formulation. All of these nutrients are essential for maintaining the health of the mother and promoting the best possible growth of the fetus at every stage of pregnancy.
Women's prenatal vitamins benefits
The benefits of women's prenatal vitamins are manifold, catering to the diverse needs of expectant mothers and their developing babies. These specialized supplements provide essential nutrients like folic acid, iron, calcium, and iodine, crucial for supporting maternal health and optimal fetal development throughout pregnancy.
Best prenatal vitamins
Ranked among the best prenatal vitamins, Beli Women's prenatal vitamins are meticulously formulated to cater to the nutritional requirements of women during preconception, pregnancy, postpartum recovery, and breastfeeding. Loaded with 20 essential nutrients deemed critical for fetal development and maternal well-being, Beli earns a remarkable 9.7 rating for its excellence.

beli.pxf.io
Complete nutrition from conception to pregnancy and beyond
When you purchase through links on our site, we may earn an affiliate commission.
Shop & Save 10%
On Beli's Website
Pros:
Enjoy 10% Off Beli Women prenatal vitamins.
Boost preconception nutrition and postpartum healing.
400mg of choline aids in healthy neural tube development.
Quality iron and TRAACS minerals for enhanced absorption.
Optimal levels of methyl folate support healthy fetal development.
Cons:
Can be pricey compared to other prenatal supplements.
What's in the Beli Women Prenatal Vitamins
These vitamins are made up of a wide range of vitamins, minerals, and other healthful components. Important elements consist of:
Methylated folate: is essential for the early, healthy development of the fetal brain, spine, and neural tube.
Iron: Essential for the synthesis of red blood cells and the prevention of anemia.
Choline: Lowers the risk of neural tube defects and promotes brain growth.
Iodine: Necessary for healthy thyroid function and the development of a baby's brain.
Vitamin D: Aids in the immune system and bone health.
B vitamins: Support the production of red blood cells, nerve transmission, and energy.
beli.pxf.io
Complete nutrition from conception to pregnancy and beyond
When you purchase through links on our site, we may earn an affiliate commission.
Shop & Save 10%
On Beli's Website
What Benefits Prenatal Vitamins for Beli Women Can Offer: Beli Women's prenatal vitamins provide a nutritional boost for several aspects of fertility, pregnancy, fetal growth, and postpartum healing when combined with a nutritious diet. Advantages consist of:
consistent regular dietary assistance.
Promotion of fetal development.
Increased vigor and energy.
assistance for healthy muscles and bones.
reduction of morning sickness and indigestion
How Much Do Beli Women's Prenatal Vitamins Cost:
A one-month supply costs $50, but regular specials offer discounts. Sold via monthly subscription, subscribers enjoy free shipping and can cancel anytime.
Do You Need to Take Beli Women's Prenatal Vitamins?
You can benefit from Beli Women prenatal vitamins if:
You intend to get pregnant, nursing, or both.
You are looking for a complete prenatal vitamin.
You like your ingredients to be verified as high-quality.
Beli Women may not benefit from prenatal vitamins if:
You suffer from certain allergies or dietary limitations.
You now take prenatal supplements or vitamins.
Budgetary restrictions are a problem.
beli.pxf.io
Complete nutrition from conception to pregnancy and beyond
When you purchase through links on our site, we may earn an affiliate commission.
Shop & Save 10%
On Beli's Website
4 notes
·
View notes
Text

What factors can make your pregnancy high-risk
👉 Placental abnormalities
👉 Fetal growth restrictions
👉 Congenital fetal anomalies
👉 History of recurrent miscarriages
Connect with us to know more!
📞: : +91-81252 02545, 80192 12545
🌐: : https://eeshanhospitals.com/
Follow us for latest Eeshan Yamjal 🏥Hospital updates on….
https://www.facebook.com/eeshanyamjalhospital/
https://www.instagram.com/eeshanyamjalhospital/
https://twitter.com/eeshanyamjal
https://www.youtube.com/@EeshanYamjalHospital
#highriskpregnancy#pregnancy#pregnancycare#teenagepregnancy#elderlypregnancy#hospital#hyderabad#sagarhighway#emergencycare#24hrservice#emergencyhealthcare#eeshanyamjalhospital#turkayamjal#besthospitalinhyderabad#besthospitalinturkayamjal#drchandana#drprashanth#eeshanhospital
2 notes
·
View notes
Text
I'm on OB rotation again. I asked the attending what are things the PCP should know about prenatal and postpartum pts. Stuff we discussed:
SSRIs can be continued during pregnancy. I often see patients on Zoloft during pregnancy if they need an antidepressant. In fact, I just started a prenatal patient on Zoloft the other day in clinic. It is safe to continue SSRIs during pregnancy because you should treat the patient's depression. Babies can come out sort of jittery because of the SSRI, but that goes away.
Postpartum patients will have bleeding somewhat similar to a menstrual period right after giving birth. It starts to decrease and becomes like a brownish color and can last up to 6 weeks postpartum. Any bleeding beyond that point is abnormal.
There is some evidence that if you have estrogen-containing birth control, it can decrease milk supply. Actually, I had a patient in clinic recently who was seen by an attending and he started her on a progesterone only birth control so that it would not affect her milk supply. Estrogen decreases the patient's milk supply, so patients who plan to breast-feed should not be started on estrogen-containing birth control. Right after giving birth, your body has increased amounts of estrogen, so you would not start estrogen containing birth control until at least 6 weeks postpartum anyway. Increasing estrogen immediately postpartum increases risk of blood clots. For patients who plan to breastfeed and want to be on an oral contraceptive, use progesterone only oral contraceptives until she stops breastfeeding.
If the mother is breastfeeding at least every 4 hours, then this can be used for contraception. It's about 80% effective. Once baby starts sleeping through the night or once baby starts feeding more than every 4 hours, this method won't work! If you go more than 4 hours without breastfeeding, breastfeeding will not protect you from pregnancy! You can also ovulate before your menstrual period returns, so you can't say you can't get pregnant because your period has not returned yet!
I asked the attending I worked with today about how she goes about prescribing birth control. She said she will usually start with Sprintec. It's usually covered by insurance and if it's not covered, it's pretty affordable. She also said Junel is pretty well tolerated. Certain progestins in certain brands of birth control may work better for certain things like acne control, but she didn't have as much knowledge on that. I'll ask another attending again about that. I usually start people on Sprintec as well.
PCP should know that alkaline phosphatase is high in pregnant patients. It comes from the placenta. So don't be freaked out by that.
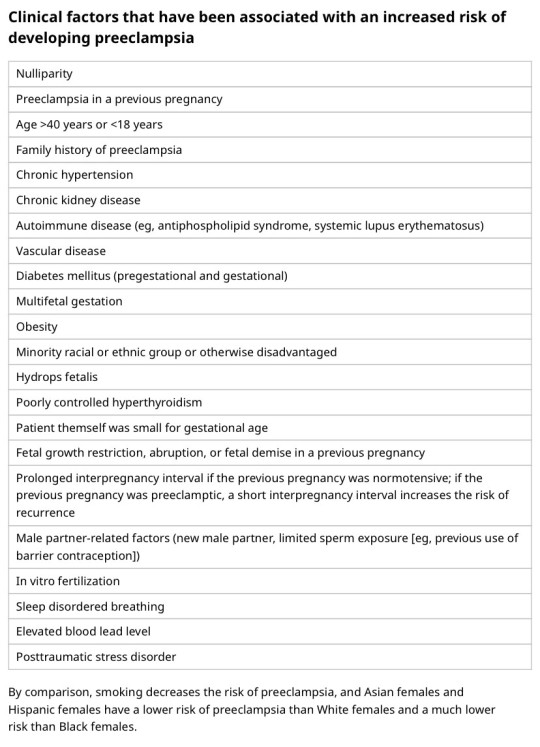
You should know HTN in pregnancy and preeclampsia workup. High BP is 140/90. Severely high BP is 160/110. Swelling occurs in many pregnant pts, but that should also alert you to start preeclampsia workup.
[Preeclampsia w/u from UpToDate:
Diagnostic evaluation
•Laboratory – Patients with suspected preeclampsia should have a complete blood count with platelets, creatinine level, liver chemistries, and determination of urinary protein excretion.
•Fetal status – Fetal status is assessed concurrently or postdiagnosis, depending on the degree of concern during maternal evaluation. At a minimum, a nonstress test or biophysical profile is performed if appropriate for gestational age. Ultrasound is used to evaluate amniotic fluid volume and estimate fetal weight, given the increased risk for oligohydramnios and growth restriction.
•Consultation with the neurology service is generally indicated in patients with neurologic deficits/abnormal neurologic examination, which may include ocular symptoms or a severe persistent headache that does not respond to initial routine management of preeclampsia.]
An important thing to review is physiology of pregnancy. Blood volume increases during pregnancy, so there are lots of new RBCs and that will throw off a HgbA1c reading, therefore HgbA1c is not measured during pregnancy and will not be accurate! My attending today told me there was a midwife who offered pts either HgbA1c or oral glucose tolerance tests to screen for gestational DM. The HgbA1c is not accurate in pregnancy, so this should not be done. That would be bad to miss a diagnosis of gestational diabetes. You have to wait until 3 months postpartum to measure HgbA1c to get an accurate reading. Had a pt who did not have a PCP prior to getting pregnant, was on insulin during the pregnancy, and after giving birth, still needs to establish with PCP for diabetes f/u. After you give birth, you insulin needs drastically change, so you don't need as much as you did when you were pregnant. So I stopped her insulin and advised that she f/u with her new PCP for diabetes care.
I still need to review fetal heart tracings. The attending today said the first thing to look at is the baseline (the baseline HR should be about 160 beats/min), then the variability, then look for accelerations and decelerations. If more than 32 weeks GA, accelerations are 15 beats/min above the baseline lasting at least 15 seconds. Early decelerations are representative of compression of the fetal head, which is normal during labor as baby moves down the pelvis/birth canal. Variable decelerations look sharper like a "V" and can represent compression of the umbilical cord. Late decelerations represent placental insufficiency.
ACOG has very helpful practice bulletins.
I can't take screen shots on my work laptop, so I'm just going to summarize gestational HTN w/u from UpToDate:
Gestational HTN: New onset of systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg on at least 2 occasions 4 hours apart after 20 weeks of gestation in a previously normotensive individual
And:
No proteinuria
No signs/symptoms of preeclampsia-related end-organ dysfunction (eg, thrombocytopenia, renal insufficiency, elevated liver transaminases, pulmonary edema, cerebral or visual symptoms)
Preeclampsia: New onset of systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg on at least 2 occasions at least 4 hours apart after 20 weeks of gestation in a previously normotensive individual. Patients with systolic blood pressure ≥160 mmHg and/or diastolic blood pressure ≥110 mmHg should have blood pressure confirmed within a short interval (minutes) to facilitate timely administration of antihypertensive therapy.
And:
Proteinuria (≥300 mg per 24-hour urine collection [or this amount extrapolated from a timed collection], or protein:creatinine ratio ≥0.3, or urine dipstick reading ≥2+ [if other quantitative methods are not available]).
In a patient with new-onset hypertension without proteinuria, the diagnosis of preeclampsia can still be made if any features of severe disease are present.
Preeclampsia with severe features: In a patient with preeclampsia, presence of any of the following findings are features of severe disease:
Systolic blood pressure ≥160 mmHg and/or diastolic blood pressure ≥110 mmHg on 2 occasions at least 4 hours apart (unless antihypertensive therapy is initiated before this time)
Thrombocytopenia (platelet count <100,000/microL)
Impaired liver function as indicated by liver transaminase levels at least twice the normal concentration or severe persistent right upper quadrant or epigastric pain unresponsive to medication and not accounted for by alternative diagnoses, or both
Progressive renal insufficiency (serum creatinine concentration >1.1 mg/dL [97 micromol/L] or doubling of the serum creatinine concentration in the absence of other renal disease)
Pulmonary edema
Persistent cerebral or visual disturbances
Eclampsia: A generalized seizure in a pt with preeclampsia that cannot be attributed to other causes.
HELLP syndrome: hemolysis, elevated liver enzymes, low platelets. Hypertension may be present (HELLP in such cases is often considered a variant of preeclampsia).
Chronic (pre-existing) hypertension: hypertension diagnosed or present before pregnancy or on at least 2 occasions before 20 weeks of gestation. Hypertension that is first diagnosed during pregnancy and persists for at least 12 weeks postpartum is also consider chronic hypertension.
Blood pressure criteria during pregnancy are:
Systolic ≥140 mmHg and/or diastolic ≥90 mmHg
Prepregnancy and 12 weeks postpartum blood pressure criteria are:
Stage 1 – Systolic 130 to 139 mmHg or diastolic 80 to 89 mmHg
Stage 2 – Systolic ≥140 mmHg or diastolic ≥90 mmHg
Chronic HTN with superimposed preeclampsia*:
Any of these findings in a patient with chronic hypertension:
A sudden increase in blood pressure that was previously well-controlled or an escalation of antihypertensive therapy to control blood pressure
New onset of proteinuria or a sudden increase in proteinuria in a patient with known proteinuria before or early in pregnancy
Significant new end-organ dysfunction consistent with preeclampsia after 20 weeks of gestation or postpartum
*Precise diagnosis is often challenging. High clinical suspicion is warranted given the increase in maternal and fetal-neonatal risks associated with superimposed preeclampsia.
Chronic hypertension with superimposed preeclampsia with severe features:
Any of these findings in a patient with chronic hypertension and superimposed preeclampsia:
Systolic blood pressure ≥160 mmHg and/or diastolic blood pressure ≥110 mmHg despite escalation of antihypertensive therapy
Thrombocytopenia (platelet count <100,000/microL)
Impaired liver function as indicated by liver transaminase levels at least twice the normal concentration or severe persistent right upper quadrant or epigastric pain unresponsive to medication and not accounted for by alternative diagnoses, or both
New-onset or worsening renal insufficiency
Pulmonary edema
Persistent cerebral or visual disturbances
A reduction in blood pressure early in pregnancy is a normal physiologic occurrence. For this reason, women with chronic hypertension may be normotensive at their first few prenatal visits. Later in pregnancy, when their blood pressure returns to its prepregnancy baseline, they may appear to be developing preeclampsia or gestational hypertension if there are no documented prepregnancy blood pressure measurements.
BP: blood pressure.
* Blood pressure should be elevated on at least two occasions at least four hours apart. However, if systolic pressure is ≥160 mmHg or diastolic pressure is ≥110 mmHg, confirmation after a short interval, even within a few minutes, is acceptable to facilitate timely initiation of antihypertensive therapy.
¶ The onset of preeclampsia and gestational hypertension is almost always after 20 weeks of gestation. Preeclampsia before 20 weeks of gestation may be associated with a complete or partial molar pregnancy or fetal hydrops. Postpartum preeclampsia usually presents within two days of delivery. The term "delayed postpartum preeclampsia" is used for signs and symptoms of the disease leading to readmission more than two days but less than six weeks after delivery.
Δ Significant proteinuria is defined as ≥0.3 g in a 24-hour urine specimen or protein/creatinine ratio ≥0.3 (mg/mg) (34 mg/mmol) in a random urine specimen or dipstick ≥1+ if a quantitative measurement is unavailable.
◊ Almost all women with the new onset of hypertension and proteinuria at this gestational age or postpartum have preeclampsia, but a rare patient may have occult renal disease exacerbated by the physiologic changes of pregnancy. An active urine sediment (red and white cells and/or cellular casts) is consistent with a proliferative glomerular disorder but not a feature of preeclampsia. Women with chronic hypertension who had proteinuria prior to or in early pregnancy may develop superimposed preeclampsia. This can be difficult to diagnose definitively, but should be suspected when blood pressure increases significantly (especially acutely) in the last half of pregnancy/postpartum or signs/symptoms associated with the severe end of the disease spectrum develop.
§ Photopsia (flashes of light), scotomata (dark areas or gaps in the visual field), blurred vision, or temporary blindness (rare); severe headache (ie, incapacitating, "the worst headache I've ever had") or headache that persists and progresses despite analgesic therapy; altered mental status. Seizure occurrence upgrades the diagnosis to eclampsia.¥ The differential diagnosis of preeclampsia with severe features includes but is not limited to:
Antiphospholipid syndrome
Acute fatty liver of pregnancy
Thrombotic thrombocytopenic purpura (TTP)
Hemolytic uremic syndrome (HUS)
The laboratory findings in these disorders overlap with those in preeclampsia with severe features. (Refer to table in the UpToDate topic on the clinical manifestations and diagnosis of preeclampsia.) The prepregnancy history, magnitude and spectrum of laboratory abnormalities, and additional presence of signs and symptoms not typically associated with preeclampsia help in making the correct diagnosis, which is not always possible during pregnancy.
In addition, a variety of medical disorders may be associated with hypertension and one or more of the signs and symptoms that occur in women with preeclampsia with severe features. These patients can usually be distinguished from patients with preeclampsia by taking a detailed history, performing a thorough physical examination, and obtaining relevant laboratory studies.‡ In contrast to preeclampsia, gestational hypertension is not associated with end-organ involvement, so neither proteinuria nor the symptoms or laboratory findings of preeclampsia are present.
#OB#OBGYN#birth control#gestational HTN#preeclampsia#eclampsia#breastfeeding#gestational diabetes#fetal heart tracing#FHT
2 notes
·
View notes
Text
Alexzandra The Warden VI


Date of Birth: Approximately 4/5
Place of Birth: Fetal Production Facility 01, Metro 04, (Nation) Onsoro, (Planet) Aeraia-02
Aliases: Warden VI, The Scarlet Angel, Alex, Alexa, Zandra
Species: Artificial Humanoid (Contains various genetic components of a number of different species, the “Warden” species only has six members at this time and only two are approximately similar on a genetic-basis; 58% of her DNA is from homo sapiens sapiens)
Height: 6’0” (in-heels) 5’8” (no-heels)
Weight: 137 lb.
Family: Wardens I-V (Counterparts/Functional Siblings), Various Genetic Templates (Technical Parents), Archon Scientist who provided their ovum (Creator/Parent)
Appearance
Alexzandra appears to be a young human woman of tall height and athletic build, with long red hair, and green eyes. Her ethnicity is somewhat equivalent to that of a mediterranean-european person on Earth, as Metro 04 is in a climatologically similar region. Due to her training and lifestyle as a soldier-in-training through her childhood and adolescence, Zandra’s musculature is well-toned and described as wiry, able to produce strength with fairly minimal effort, but still remaining compact enough to not slow her movements. Her features are often described as “delicate” and “fair” otherwise.
Typically on most days, Alex prefers to wear comfortable clothes that don’t restrict her mobility, while also maintaining some type of modern style resembling streetwear aesthetic. In service when she acts as a warden, however, she tends to dress in a mode evoking the classical ideas of a warrior on Earth and Aeraia-02, drawing explicitly from the latter’s history. Usually this includes light underclothes and clothing, usually with some red or scarlet coloration, with various plated armor placed along the torso, forearms, and legs, with boots. The plating of this armor is often varied, but never seems to cover as broadly as historic armor on earth, instead favoring a more “ceremonial” design, as the armor isn’t strictly functional but aesthetic. This armor, and all metal she wears, tends to be of a bronze or copper-like metal native to Aeraia-02 which is chemically distinct from the versions of those elements found on Earth. Accompanying this is a bronze circlet inlaid with a small emerald which allows her to receive psionic impressions from her handlers among the archons. Additionally she often wears a narrow bronze gorget around her neck, though she will usually change this out for various kinds of necklaces. Finally, this metal also is usually worn as an arm band around one or both of her biceps.
Always on her person, somewhere, is a medallion forged of the same metals she wears, which bears her personal insignia, which appears like that of a bow with a spear beneath it as if it were knocked as an arrow.
Despite her ability to heal from most injuries effectively, Alexzandra still has a number of scars along her body, particularly her upper back, legs, and parts of her arms, from various fights that she’s had, though they steadily fade with time as it passes. Accordingly, particularly if she has had recent and intense fights, these scars may vary in number, pattern, and freshness.
At various times, a brand that roughly translates to the number 6 in the Archon's language can become visible on and over her left eye. It's an energy-based imprinting in a fashion akin to a brand, which serves partly as her badge as the Warden VI, but also as a reminder of by whose authority she acts, on the part of the Archons. This sign will often glow when she is in the process of using her powers or channeling a large amount of energy in the moment, or in a moment of pitched emotion.
Personality
Her identity and personality were programmed/printed onto her during her creation, with a combination of genetic coding modification, as well as utero-environmental manipulation, and a very intentional and curated experience in key growth periods of early childhood through to young adulthood. The intention of this was to produce an Alexzandra who would feel a sense of altruism that would allow her to be caring for others and willing to protect them both without conventional condition, and with no promise of reward, while also balanced against a utilitarian mindset that would be able to execute a necessary endgame that will involve killing those who may or may no deserve it, but whose death may be necessary.
In terms of this spectrum, Alexzandra biases more on the “guardian angel” side, being caring, kind, and soft-spoken in most cases. Her first instinct in most situations is to protect, mediate, and de-escalate. She cherishes and values life in all of its forms, but has an understanding of the reality of life and its predisposition towards chaos and competition. With that, Zandra is often eager to learn and experience the various ways of life that she encounters.
Determined to follow through on her purpose, at the expense of even her own life, she will refuse to stand down or fold in the face of danger and tyranny. This same valuation of others, though, causes a great degree of conflict when it comes to the reality of the position of Warden, a hesitation that has been observed in several simulations.
Disregarding the primary disposition of the warden preferring to protect sentient forms of life, and place them as often imperative than somewhat less sapient ones, Alexzandra has a massive affection for animals, particularly avians.
Biography
Wardens aren’t born, but built. When the Archons determined that the earth would be an emphasis for conflict and growth as a result of a high variability in species of all kinds, with dinosaura initially being thought to be the primary emphasis, before determining that a homo sapiens variation would then later become the dominating force on said planet. In anticipation of this, the 5th Warden was made to be the model of what would someday become the homo sapiens sapiens, Lila was created Aeraia-01. For approximately 1 billion years on earth, Lila was the protector of life in the universe, resembling the fast-booming human-like species who quickly spread throughout the stars.
Throughout this billion years, the interest of Archons in the planet earth and its specific homo sapiens variations only grew, and so when the time came to begin production on Warden VI, it was deemed that Alexzandra was to be the first of the warden species to closely resemble a preceding warden on a genetic level.
The Wardens are a group (or rather a series) of protectors devised by the Archons in service of protecting and fostering life within this universe. If Archons were to view life as a garden, then Wardens are the tools with which they keep up and grow that garden. And this was what was in-mind when they designed Alexzandra, a perfect warrior who would be able to defeat any of Archon’s creations, and if she measured up short would be able to grow to defeat those threats.
As typical for Wardens before her, Alexzandra was created after the long-term establishment of a planet, set of species, and cultures, that had been cultivated and had an unusually protracted interaction with the native beings that were evolved there, all of who would have parts of their genetics included into the Warden that would be created as a result. This planet would be in a similar system to Lila’s, and was named Aeraia-02, to indicate the connection between the worlds. This planet had its own evolution, growth, development, peoples, and cultures that progressed over the course of millions of years.
Once the species and technology had been developed to her engineer’s satisfaction, the fetus that was to someday be known as Alexzandra was produced via the manipulation of a “Lock Point” (the means of reproduction that the extradimensional Archons usually rely on) forcibly condensed and conceptualized into an ovum in our physical dimension, presented by the lead on the “VI Project”. This ovum then was modified to contain specific genetic traits that were rendered and sampled from numerous domestic species of Aeraia-02 who were intentionally ensured to be on the planet, to create Alexzandra.
Born with a name that cannot be properly romanized, due to a lack of script for it on this website, Alexzandra was born in the fashion that had quickly become normal by the year 046YL (via the systems and explanation for the calendar) on Aeraia-02. Birth and reproduction by most of the inhabitants on the planet occurred via artificial fertilization of eggs with manipulated and favored traits to produce a complete infant person. Alexzandra’s facility being purposed specifically to create a Warden was the only unusual factor, as birthing facilities number in at least one per settlement. And as was still typical, for the time, Alexzandra was placed into the care of parents who volunteered to foster a child or children from the facility as a family unit. Alexzandra’s parents were not terribly creative in naming, however, and knowing that she was to be trained to become a Warden named her their language’s translation to the word, which would also read as something like “Great Protector” or “Guardian of Life”.
The understanding of Alexzandra’s person was communicated preemptively to her parents, as well as to her once she was old enough to understand the sort of self-sacrifice she would need to make, and to begin her training. This started at roughly age 8 (in terms of Earth years, Aeraia-02’s orbit is 800 day-night cycles long, so Alexzandra was 4 cycles by the numeration she is accustomed to). Training for a future lifestyle as a warrior included her being removed from the mainstream educational infrastructure of her culture, and placed into a series of private tutoring for her early growth years.
Studied on a number of languages that had been developed across her planet, as well as the process of learning and becoming fluent in languages, and importing commonly spoken languages throughout the universe, the majority of Alexzandra’s early studies emphasized becoming a polyglot, as well as developing an ethical and moral center that was consistent with the Archon’s expectations of her as Warden VI, and including numerous tactical and military-theoretical disciplines. Ultimately, her focus of study was in: MSE (Mathematics, Science, and Engineering), Humanities, and Languages. At one point she was expected to learn the arts, though Alexzandra was often expressed as “too hard-headed” or “too willful” and often got into arguments with her instructors for those disciplines.
Her studies would ramp-up as she got older and more intense physical instruction began to integrate as Alexzandra reached adolescence. This was the part of her education that she preferred in both the moment and hindsight, as not only did it come easily to her, but the physical education allowed her to reintegrate with her peers and begin socializing with them. This included many things, but primarily emphasized martial arts, shooting, weapons training, and team sports, as well as something called “applied battlefield training and tactics” in which she would participate in military drills and training with recruits and later ongoing trained members of the Onsorian military.
It was from these drills that she would also become educated more on her planet’s history and culture by others who knew it, particularly Onsorian history and how its armed forces have developed and grown with time. Zandra would become particularly fascinated with the warriors of antiquity, and various myths that might resemble earth’s own greco-roman traditions. When the time came she would factor these aesthetics and ideas heavily into her presentation.
Once she reached the age of 7 Cycles (roughly 15.3 earth years) her training was considered to be largely “complete” in terms of her development into a suitable soldier. Without her active awareness of the true nature and depth of her powers, though, the 6th Warden’s powers allowing her physicality to catch up and meet any challenge had already allowed her to develop into what would otherwise be considered and elite or top soldier not only in Onsoro, but on the entire planet of Aeraia-02. The next phase would be regarding the use of her powers, and finally accommodating the “perfect” part of the “Perfect Warrior”. Her next 3 cycles (by the end of this she would be nearly 22 earth years) would be spent learning to harness and sophisticate her broader range of powers, to actively and intentionally utilize her Adaptive Development, how to interact with her Combat Sense, and ultimately how to properly use her Weapon Creation.
This completion of her training would eventually be seen when she was bestowed “The Sigil of Sixth” an ink branding that was placed on her left eye that glows when she taps into the true depths of her power, or can be forced to glow to illustrate her identity. This sigil, as explained to her, is meant to serve as her badge, evidence of her birthright and accomplishments, but on some level, it feels more like a serial number to her, a brand showing Alexzandra as property to the Archons. The actual sigil shape resembles the number 6 in the Archon's script.
Set forth from the completion of her training at 10 cycles old, Alex set off to Earth, the primary planet of concern, and a future junction point for conflict in the universe. Upon arriving on earth, she began immediately acting as a hero, she took the name “Alexander” as suggested to her by the Archons for its etymological identical nature to her homeworld name… Though after getting enough weird looks, and having the concept of gendered language explained to her, she adjusted to Alexzandra, still etymologically equivalent, but also of a gendering appropriate to her self-ID.
Powers and Abilities
-Warden-Hybrid Physiology: As the Sixth Warden, Alexzandra was a designed being built with corporeal genetics from the inherently acorporial Lock Point of an Archon. Composed from a number of different species, her powers are produced as a direct result of her physiology, particularly her physicality, potential, and adaptability.
–Parahuman Physicality: Factors of Alexzandra’s physical development were already of an inhuman nature by way of DNA that was factored in which created a sort of “above human but not inherently” state of being. Many of Alex’s physical aptitudes started within the human range, but has since then, thanks to her adaptation and training, crossed beyond typical maximums.
–Superhuman Combat Potential: Drawn primarily from homo sapiens DNA, and enhanced through various synergy against other DNAs integrated into her design. Essentially it contributes to a “growth potential” that Alexzandra can experience in terms of more or less anything, though in order to make it “infinite” she had her potential relegated largely to combat-relevant disciplines.
–Superhuman Reflexes: Her natural reflexes and ability to react are enhanced by her sensory capabilities, but Alex’s physicality (particularly in terms of speed) also results in the ability to react to things outside of reasonable timing, even without any psychic or similar powers.
–Enhanced Senses: Through a variety of means throughout her biology, Alexzandra is able to perceive beyond the bounds of typical humans, including the ability to receive information before light or sound physically reach her eyes and ears, as well as perceiving at a number of spectrums that usually require technology. In part this is thanks to the fact that she has a Lock Point, permitting the same perceptive abilities as a “Pure Archon”.
–Enhanced Longevity: Any being with a Lock Point lives in terms of an Archon’s relative lifespan, once her body reaches its physical prime (for a human this would be somewhere between 30 and 35) Alexzandra will age only about 1 decade for every billion years that she experiences, accordant roughly to how a human might expect to age.
–Enhanced Learning Ability: Pertinent to the desire for a Warden to be able to become adaptable, and capable, not only physically but also mentally, Alexzandra’s brain is enhanced, allowing her to more easily retain and apply information than a human does, as well as store much more. This happens because she essentially has no capacity for short-term memory, but rather all information is stored into her long-term memory until she actively chooses to forget the data in question.
–Pure Energy Generation: An Archon ability, and accordingly also native to her Lock Point, is the ability to generate “pure energy”, energy which is independent of its particles and is able to create momentum freely. This energy is able to also become dense enough to turn into particles that aren’t simple carriers of momentum (and thus heat), becoming hyper-dense to the point that they might eventually slow down and become liquid, gas, or solid matter. This is how archons are able to create living creatures and objects. This output occurs naturally, but is stronger than a typical Archon in their corporeal form due to certain genetic selections, and through an ability to grow if necessary when adapting.
–Energy Manipulation: Everyone with a Lock Point is able to manipulate the same pure energy which they generate, but can also manipulate similar energies external to this definition. These energies, when becoming matter, must be turned into something which the individual in particular understands on a physical and chemical level. Zandra is able to manipulate hers to fairly capable effect, though she’s only been manipulating her energies for about half a decade.
-Psychic Potential: Applied to her brain while still a fetus, Alexzandra has a brain which is capable of controlling the waves produced by its thought, and interacting with the same waves produced by the brains of others. This also enables her to use these waves to give her additional sensory range and perceptions. At present this potential mostly feeds into other powers, rather than provides anything on their own.
-Combat Sense: A power developed specifically via a combination of her extrasensory abilities via psychic power, and her enhanced natural senses, as well as several other intentional installments throughout her body, Alexzandra has a curated ability that gives her a vaguely hyper-present sense during a fight. She is aware of any danger as it approaches, because her Combat Sense dictates it. She is aware of the correct decision to make in any fight, because her Combat Sense tells her. Alex’s combat sense specifically dictates the most immediate decision, and doesn’t account for her desires, wants, or strategies, simply giving an objective read on the next action she should take; further it may feed multiple courses of action, but only if they are absolutely equally viable to each other, meaning that it may feed many actions if they are all equally net positive, or the least net negative. These impulses aren’t hard data or written, and still have to be interpreted, with danger impulses reading similarly to tactical ones at times.
-Perfect Adaptive Development: Or by some called “Combat Loneliness”, this power was designed, and possibly is connected to her Lock Point, to allow Alexzandra to quickly and effectively capitalize on her potential. Through experiential stimuli and challenge in the heat of combat, Alexzandra’s body is able to push beyond its understood and present limits in the moment, rising to the challenge before her. Inevitably, Alexzandra is able to eventually grow to defeat an opponent, once she’s able to conceptualize the hurdle that she must overcome. The rate at which this growth occurs is more dramatic the greater a degree of growth is necessary, but it will slow or peter out if it’s only a small difference to be made up, and she cannot grow if she doesn’t know of a need to, or if she cannot conceptualize how strong her adversary is.
–Regeneration: An enhanced healing factor that has been bolstered artificially from the already-improved one she possesses via her anatomy, Alexzandra is able to rapidly recover from injuries and damage sustained in the course of action, particularly relating to her development. At typical times, her regeneration allows her to recover from serious injuries and lost limbs in a matter of days, and even broken ones in minutes, but when in active development her recovery becomes so rapid that it’s practically instantaneous.
-Weapon Creation: All Archons at some point express a specialty in terms of that which they can create and do with pure energy, and like them, Wardens do too. Alexzandra’s aptitude is the creation of weapons, being able to form weapons of any kind which she understands the construction and functions of. The more complex and individual parts of a weapon, the more energy it requires, though she may invest additional energy to enhance the parameters of a weapon which she creates. These weapons can appear in her hand, or from thin air, and may be reconverted back into its original energy form freely.
Weaknesses
-Evolution Boom: Lock Points, by their very nature, foster growth and change in other beings. This seems connected to the Archon disposition to propel and create life throughout this universe. Accordingly, Alexzandra’s very presence is a sort of cosmological “takes all comers” challenge, wherever she goes, the evolution and growth of others experiences a boom in various ways, and inherently attracts greater threats that she can thereby adapt and overcome, for the next subsequent threat in the future.
-Misleading Impulses: Her most problematic weakness, Alexandra’s combat sense has a very specific intention and function, and does not, or possibly cannot, account for longer-term events which have not happened. It is only able to calculate with fairly recent or immediate consequences to actions carried out in its impulse. This means that, if she were to need to take a long-term strategy, it may cause her to fight contrary to these impulses, which similarly makes them louder and louder as the sensory ability believes she is putting herself in more and more danger. Even then, an impulse may be extremely correct in one moment, but become extremely incorrect in the next.
-Nonspecific Impulses: Impulses that are regarding tactics, or impulses warning of danger, may sometimes be similar to each other in terms of how Zandra’s brain interprets it. Fleeing a fight because an enemy is strong, or being aware of the danger of an incoming attack that needs to be dodged, are two VERY different streams of information that will read as similar to Alexzandra, and thus it can be difficult to make a decision based on said impulse.
-Excessive Data: Combat Sense provides information that is ultimately the most net positive or least net negative to its user. However, situations where multiple results are equally viable in the immediate-term are extremely common in pitched combat, and Combat Sense functions in such a way that those multiple options are presented to Alexzandra in a fight. These multiple streams of data can become difficult to parse, and accordingly can occasionally cloud her perceptive abilities, causing her to mistake a guideline or impulse for reality.
-Sensory Overload: Combat Sense can be overwhelming on its own, but the sensory abilities that inform it cause a sensitivity to sensory stimuli. Extremely loud noises, particularly sharp frequencies, extremely bright and sudden bursts of light, and the like can cause Alexzandra both a great degree of suffering, and can occasionally even shut off her receivers temporarily if potent enough. In such cases, if she couldn’t regenerate, this would likely mean blindness, deafness, or the like, but these parts can repair like any other part of her body. Similarly, the damage and pain she sustains can be especially distracting and difficult to cope with.
-Decisive Defeat: Attacking and defeating Alexzandra before she can completely adapt to her opponent is a surefire way to defeat her. There are various ranges of advantage or speed from which one can do this, without increasing her growth rate to such a degree that she almost immediately might catch up. Generally this falls either into the range of “insurmountably stronger” or “stronger but not too much stronger”. She often relies on Combat Sense to delay these fights for longer to combat this, but it is a true issue.
-Granular Difference: Alexzandra’s worst case is when a foe is stronger than her, but only just enough that it would take quite a while for her Combat Loneliness to overcome them. Just as much that an enemy who is radically stronger than her causes her growth to speed up radically, an enemy who is only marginally stronger than her can maintain this lead for quite a long time. She often calls this the “Challenge Paradox”, in which fighting and overcoming threats that are weaker than her don’t really provide any benefit, but even those who aren’t overwhelmingly strong against her also prompt only slow growth.
-Imperceptibility: If an opponent’s power is at such a level that Alexzandra cannot contextualize/visualize, and therefore pursue it effectively, she cannot grow relative to it. This is the same if the nature or style of an enemy’s strength is beyond her understanding.
Equipment
-Weapon-Constructs: Weapons devised specifically through her energy manipulation tend to possess a greater durability and destructive power than those made through mundane means, this increases in terms of potency based on the more energy compressed into the weapon’s form. These weapons can be of any kind and design, so long as Alexzandra has a detailed understanding of how it works.
-Focusing Gem: Inlaid into her circlet is a small precious rock that is able to act as a conduit for the energy she produces, as well as her brain waves, enhancing their intensity by essentially refracting them to have a larger area. This function is considered to be superior than the baseline, despite being a less focused application of her power.
3 notes
·
View notes
Text
Erin Wolf of Falmouth loves being a mom. She and her husband already had two boys when she found out she was expecting a third in 2016.
"Which was a very much wanted and planned for pregnancy," she says.
They decided to name him Dylan. Wolf was 35 and considered advanced maternal age, which meant she had extra testing to check for fetal anomalies. For the first four months, everything was fine. But at 17 weeks, some routine lab work came back abnormal.
After more testing, Wolf received a grim prognosis. Dylan had an open neural tube defect. It was a severe form of spina bifida. He had irreversible brain damage and would need multiple shunts put in his brain after he was born. He wouldn't be able to walk. His life would be spent in and out of hospitals.
"After soul searching, and really thinking about the quality of life that we wanted for our son, and for our other living children, we made what was really a heartbreaking decision," Wolf says. "And we elected to end my pregnancy."
By this time, Wolf was 18 and a half weeks pregnant. It was a decision that she couldn't have made any earlier.
....
Dana Peirce of Yarmouth was 39 when she was pregnant with her second child. And, like Wolf, she had many tests. Genetic screenings. Ultrasounds. They all came back normal.
Then, at 32 weeks, she went in for a routine growth scan. She couldn't wait. She had already started a baby book for her son, named Cameron, and she wanted pictures. But as she glanced at the screen she noticed two numbers in the corner. They didn't match.
"His head was measuring about 36 weeks, and his limbs were measuring about 22 weeks," Peirce says.
Peirce knew something wasn't right. Shortly after the scan, the obstetrician delivered devastating news. Cameron had a rare bone disorder called lethal skeletal dysplasia.
"I remember crying and then apologizing for crying," Peirce says. "And she said something like, 'Oh, no, this is really bad. It never happens, but it is happening. And it is totally appropriate for you to be very upset.'"
If Cameron survived until birth, he would have difficulty breathing. He had a broken femur and several healed fractures.
"That was incredibly upsetting and horrible to know that he had essentially been normal at 20 weeks, and then for who knows how long breaking bones inside of me," Peirce says. "And I just was so horrified that he was broken and I hadn't known and he had been suffering this whole time."
Peirce didn't want Cameron to suffer any more. She wanted an abortion. But she was at 32 weeks, well beyond Maine's typical limit of 24 weeks, when a fetus is considered viable. Even so, Dr. Andrea Pelletier, the medical director of Planned Parenthood of Northern New England, says viability is a gray zone and it depends on the conditions of each pregnancy.
8 notes
·
View notes
Text
Global Doppler Ultrasound Industry Growth Analysis by Manufacturers, Regions, Type and Application, Forecast Analysis to 2032
The global Doppler ultrasound market is projected to experience steady growth over the next decade, with a compound annual growth rate (CAGR) of 3.77% from 2024 to 2032. Valued at USD 1.83 billion in 2023, the market is anticipated to reach USD 2.53 billion by 2032. This growth is driven by technological advancements in medical imaging, the rising prevalence of cardiovascular diseases, and the increasing demand for non-invasive diagnostic techniques.
Doppler ultrasound is a medical imaging technique that uses high-frequency sound waves to evaluate blood flow in blood vessels and organs. It is commonly used in cardiology, obstetrics, and vascular studies to detect blockages, abnormal blood flow, and other medical conditions, making it an essential tool in the healthcare industry.
Key Growth Drivers
Rising Incidence of Cardiovascular Diseases: Cardiovascular diseases, including hypertension, atherosclerosis, and heart disease, remain leading causes of mortality worldwide. Doppler ultrasound is a critical tool for diagnosing these conditions early by assessing blood flow and detecting abnormalities. The increasing prevalence of these diseases, particularly in aging populations, is expected to drive demand for Doppler ultrasound equipment.
Advancements in Doppler Technology: Technological advancements have enhanced the accuracy, efficiency, and portability of Doppler ultrasound devices. Innovations such as 3D and 4D Doppler ultrasound, as well as the integration of AI and machine learning into imaging systems, have improved diagnostic capabilities. These advancements allow for more precise assessments of blood flow, fetal monitoring, and the detection of vascular diseases, contributing to the market’s growth.
Rising Demand for Non-Invasive Diagnostic Techniques: As patients and healthcare providers increasingly prefer non-invasive and radiation-free diagnostic options, Doppler ultrasound stands out as a safe, efficient, and cost-effective tool. The non-invasive nature of Doppler ultrasound makes it ideal for monitoring a wide range of medical conditions without the need for surgical intervention or exposure to ionizing radiation.
Growing Use in Obstetrics and Gynecology: In obstetrics, Doppler ultrasound is extensively used to monitor fetal health by evaluating blood flow in the umbilical cord and fetal vessels. It helps detect issues such as fetal growth restrictions and placental insufficiency. As awareness of maternal and fetal health grows, the demand for Doppler ultrasound in prenatal care is expected to rise, further fueling market expansion.
Get Free Sample Report: https://www.snsinsider.com/sample-request/4499
Challenges and Opportunities
While the Doppler ultrasound market shows promising growth, several challenges remain. One significant obstacle is the high cost of advanced Doppler systems, which may limit their adoption, particularly in emerging markets and smaller healthcare facilities. Additionally, the need for skilled technicians to operate these systems and interpret results may hinder widespread implementation in underdeveloped healthcare settings.
However, increasing government investments in healthcare infrastructure, especially in developing regions, and rising awareness of early diagnosis are creating new growth opportunities. Additionally, portable and handheld Doppler ultrasound devices are gaining popularity due to their ease of use and affordability, expanding the market to remote and rural areas where access to advanced diagnostic tools may be limited.
Regional Insights
North America currently dominates the Doppler ultrasound market, driven by a well-established healthcare infrastructure, a high prevalence of cardiovascular diseases, and the early adoption of advanced diagnostic technologies. Europe follows closely, with a growing focus on improving healthcare services and investments in medical imaging.
The Asia-Pacific region is expected to witness significant growth during the forecast period, driven by increasing healthcare spending, growing awareness of non-invasive diagnostic techniques, and a rise in cardiovascular diseases. Countries such as China, India, and Japan are at the forefront of this growth due to their large patient populations and expanding healthcare infrastructure.
Future Outlook
As the healthcare industry continues to evolve, the Doppler ultrasound market is set to experience steady growth. The increasing prevalence of chronic diseases, combined with the demand for non-invasive diagnostics and technological advancements, will drive the market forward. With a projected CAGR of 3.77% from 2024 to 2032, the Doppler ultrasound market is expected to reach USD 2.53 billion by 2032, cementing its role as a vital tool in modern healthcare diagnostics.
In conclusion, the global Doppler ultrasound market is on a path of sustainable growth, driven by innovation, rising healthcare needs, and expanding applications in various medical fields. From its current value of USD 1.83 billion in 2023, the market is poised to grow steadily over the next decade, offering enhanced diagnostic solutions for cardiovascular, obstetric, and vascular conditions.
Other Trending Reports
Functional Endoscopic Sinus Surgery Market
Artificial Intelligence in Healthcare Market
Radiotherapy Market
Nicotine Replacement Therapy Market
0 notes
Text
According to recent research, about 30-40% of drug-exposed babies (Drug Addiction on Babies) suffer from various problems such as controlling behavior, developmental problems, congenital anomalies, poor mental health, difficulty in concentrating, and fine motor control disorders. Previous research has already concluded that babies born to addicted mother face long term effects drug exposure in addition to limitations in community and environmental health. Here we will discuss the long-term effects of certain drugs on babies.
Cocaine Addiction
Cocaine exposure affects the babies in the uterus by interacting with serotonin and dopamine pathways that cause neurological changes. Some of these neurological changes persist even during adulthood which causes behavioral problems, while others may resolve before adulthood at some stage. Prenatal exposure to cocaine leads to various diseases that have been proved via clinical trials. These diseases include seizures, schizophrenia, depression, and Parkinson’s disease.
Some researchers also suggest the prevalence of cardiac diseases in babies whose mothers' abused cocaine during the pregnancy. Cocaine reduces the blood supply to the fetus causing fetal distress and growth restriction inside the uterus.
Heroin Addiction
Heroin addiction during pregnancy is associated with cognitive and behavioral problems in addition to the instability of the home environment in babies. According to epidemiological surveys, a small number of children live with their heroin-addicted biological mothers at the age of five years. More than 65% of children whose mothers are addicted to heroin require special education services or additional time to pass a grade.
Heroin addiction is also associated with low birth weight, small head circumference, poor memory and thinking, and low IQ levels. However, according to studies, children adopted by non-addicted parents showed significant improvement in developmental and cognitive functions. Babies born to heroin-addicted mothers are often born with an addiction to heroin and suffer the consequences such as adverse and withdrawal effects of heroin throughout their lives.
Caffeine and Nicotine Addiction
Caffeine intake in adequate amounts is usually safe for both pregnant mothers and babies. However, consumption of more than 300 mg per day is hazardous and increases the risk of heart defects and low birth weight.
Smoking is associated with behavioral and mental issues in addition to growth restriction inside the uterus. According to research, there is a significant decrease in the risk of sudden infant death syndrome in babies whose mothers are chronic smokers and did not quit smoking even during pregnancy. Other problems include learning disabilities and anxiety.
Alcohol Addiction
According to research, a fetus born to an alcoholic mother has a high risk of suffering from Fetal Alcohol Spectrum Disorder. Fetal Alcohol Spectrum Disorder includes a combination of disorders associated with alcohol consumption, which include Fetal Alcohol Effects, Fetal Alcohol Syndrome, and Alcohol-Related Neurodevelopmental Disorder.
Other abnormalities associated with alcohol addiction during pregnancy include bone deformities, low birth weight, small head circumference, cognitive disabilities, and motor problems.
References:
The developmental outcome of children born to heroin-dependent mothers, raised at home or adopted. Child Abuse & Neglect
Alcohol, nicotine, caffeine, and mental disorders. Dialogues in clinical neuroscience
0 notes
Text
High-risk pregnancy: Know what to expect

If you have a high-risk pregnancy, you might have questions. Will you need special prenatal care? Will your baby be OK? Get the facts about promoting a healthy pregnancy. If you have a high-risk pregnancy, you or your baby might be at increased risk of health problems before, during or after delivery. Typically, special monitoring or care throughout pregnancy is needed. Understand the risk factors for a high-risk pregnancy and what you can do to take care of yourself and your baby.
What are the risk factors for a high-risk pregnancy?
Sometimes a high-risk pregnancy is the result of a medical condition present before pregnancy. In other cases, a medical condition that develops during pregnancy for either you or your baby causes a pregnancy to become high-risk.
Specific factors that might contribute to a high-risk pregnancy include the following:
Advanced maternal age. Pregnancy risks are higher for mothers older than 35.
Lifestyle choices. Smoking cigarettes, drinking alcohol and using illegal drugs can put a pregnancy at risk.
Maternal health problems. High blood pressure, obesity, diabetes, epilepsy, thyroid disease, heart or blood disorders, poorly controlled asthma, and infections can increase pregnancy risks.
Pregnancy complications. Various complications that develop during pregnancy can pose risks. Examples include an unusual placenta position, fetal growth less than the 10th percentile for gestational age (fetal growth restriction), and rhesus (Rh) sensitization, a potentially serious condition that can occur when your blood group is Rh negative and your baby’s blood group is Rh positive.
Multiple pregnancy. Pregnancy risks are higher for women carrying more than one fetus.
Pregnancy history. A history of pregnancy-related hypertension disorders, such as preeclampsia, increases the risk of having this diagnosis during the next pregnancy. If you gave birth prematurely in your last pregnancy or if you’ve had multiple premature births, you’re at increased risk of an early delivery in your next pregnancy. Talk to your health care provider about your complete obstetric history.
What steps can I take to promote a healthy pregnancy?
Whether you know ahead of time that you’ll have a high-risk pregnancy or you simply want to do whatever you can to prevent a high-risk pregnancy, stick to the basics. For example:
Schedule a pre-conception appointment. If you’re thinking about becoming pregnant, consult your health care provider. Your provider might counsel you to start taking a daily prenatal vitamin with folic acid and reach a healthy weight before you become pregnant. If you have a medical condition, your treatment might be adjusted in preparation for pregnancy. Your health care provider might also discuss your risk of having a baby with a genetic condition.
Seek regular prenatal care. Prenatal visits can help your health care provider monitor your health and your baby’s health. You might be referred to a specialist in maternal-fetal medicine, genetics, pediatrics or other areas.
Avoid risky substances. If you smoke, quit. Alcohol and illegal drugs are off-limits, too. Talk to your health care provider about any medications or supplements you’re taking.
Do I need special tests?
Depending on the circumstances, your health care provider might recommend:
Specialized or targeted ultrasound. This type of fetal ultrasound — aan imaging technique that uses high-frequency sound waves to produce images of a baby in the uterus — ttargets a suspected problem, such as development that’s not typical.
Prenatal cell-free DNA (cfDNA) screening. During this procedure, DNA from the mother and fetus is extracted from a maternal blood sample, and the fetal DNA is screened for the increased chance of specific chromosome problems.
Invasive genetic screening. Your health care provider might recommend amniocentesis or chorionic villus sampling (CVS). During amniocentesis, a sample of the fluid that surrounds and protects a baby during pregnancy (amniotic fluid) is withdrawn from the uterus. Typically done after week 15 of pregnancy, amniocentesis can identify certain genetic conditions as well as serious problems of the brain or spinal cord (neural tube defects).
During CVS, a sample of cells is removed from the placenta. Typically done between weeks 10 and 12 of pregnancy, CVS can identify certain genetic conditions.
Ultrasound for cervical length. Your health care provider might use an ultrasound to measure the length of your cervix at prenatal appointments to determine if you’re at risk of preterm labor.
Lab tests. Your health care provider will test your urine for urinary tract infections and screen you for infectious diseases such as HIV and syphilis.
Biophysical profile. This prenatal ultrasound is used to check on a baby’s well-being. It might involve only an ultrasound to evaluate fetal well-being or, depending on the results of the ultrasound, also fetal heart rate monitoring (nonstress test).
What else do I need to know about high-risk pregnancy?
Talk to your health care provider about how to manage any medical conditions you have during pregnancy and how your health might affect labor and delivery. Contact your health care provider if you have:
Vaginal bleeding or watery vaginal discharge
Severe headaches
Pain or cramping in the lower abdomen
Decreased fetal activity
Pain or burning with urination
Changes in vision, including blurred vision
Sudden or severe swelling in the face, hands or fingers
Fever or chills
Vomiting or persistent nausea
Dizziness
Thoughts of harming yourself or your baby
A high-risk pregnancy might have ups and downs. Do your best to stay positive as you take steps to promote a healthy pregnancy.
#caesarean section specialist in pcmc#gynecologist in pcmc#normal delivery in pcmc#pcos treatment in pcmc#painless devlivery in pcmc
0 notes
Text
Placental Network Differences Among Obstetric Syndromes Identified With An Integrated Multiomics Approach
The placenta is essential for a healthy pregnancy, and placental pathology can endanger both maternal and fetal health. Placental function is affected by dynamic, complex, and interconnected molecular, cellular, and environmental events; therefore, we need a systems biology approach to study disease in normal physiological placenta function. We use placental multiomics (short and bulk transcriptomics, untargeted metabolomics, and targeted proteomics) paired with clinical data and placental histopathology reports from 321 placentas across multiple obstetric conditions: fetal growth restriction (FGR), FGR with pregnancy-related hypertension (FGR+HDP), preeclampsia (PE), and spontaneous preterm delivery (PTD). We first performed cellular deconvolution to estimate cell type numbers from bulk transcriptomes: FGR+HDP placentas were the most different from control placentas driven by a higher estimated number of extravillous trophoblast (p http://dlvr.it/TCz2n2
0 notes
Text
Premature Birth: Signs, Causes, Complications, and Treatment

Premature birth, or preterm birth, is when a baby is born before 37 weeks of pregnancy, whereas a full-term pregnancy lasts around 40 weeks. This early delivery can lead to various health problems, making it crucial for expectant mothers to understand the signs, causes, and treatment options.
What is Premature Birth?
Premature birth happens when delivery occurs before 37 weeks of pregnancy. It is the leading cause of death in children under five and can result in lifelong disabilities. Premature births are categorized based on gestational age:
Extremely Preterm: Born before 28 weeks
Very Preterm: Born between 28 and less than 32 weeks
Moderate to Late Preterm: Born between 32 and 37 weeks
Signs and Symptoms of Premature Birth
Call your doctor immediately if you notice any of these signs before 37 weeks of pregnancy:
Regular Contractions: Tightenings or cramps that come at regular intervals, sharp backache, or persistent pelvic pressure.
Fluid Leakage: Gushing or trickling of fluid from the vagina, especially if the fluid is discoloured.
Vaginal Bleeding: Any bleeding during pregnancy.
Decreased Fetal Movement: A noticeable reduction in your baby’s movements.
Early detection and treatment can help prevent complications and improve outcomes for both mother and baby.
Causes of Premature Birth
Premature birth can occur spontaneously or be medically induced. Common causes include:
Previous premature birth increases the risk.
Placental problems, such as placental abruption or placenta previa.
Abnormal amounts of amniotic fluid.
Preterm premature rupture of membranes (PPROM).
Uterine abnormalities or a short cervix.
Multiple pregnancies (twins, triplets).
Chronic maternal health conditions like high blood pressure or diabetes.
Pregnancy-related conditions such as preeclampsia or gestational diabetes.
Infections and fetal growth restrictions.
Risk Factors
Being very young (under 18) or older (over 40).
Higher incidence in Black women compared to other ethnicities.
Being underweight or overweight before pregnancy.
Smoking, alcohol use, or illicit drug abuse.
High levels of stress or depression.
Diagnosis
Doctors diagnose premature birth through:
Pelvic Assessment: Checking cervix dilation and uterus firmness.
Ultrasound: Measuring cervical length and assessing fetal and placental issues.
Uterine Monitoring: Measuring contraction duration and spacing.
Urine Test: Checking for bacterial presence.
Treatment
For preterm labour or risk of premature birth, treatments may include:
Antenatal Steroids: To help mature the baby’s lungs faster.
Tocolytic Medications: To delay labour temporarily.
Antibiotics: To prevent infections if water breaks early.
After birth, premature babies often need specialized care in the NICU, including:
Incubator Care: To maintain body temperature.
Respiratory Support: Using ventilators or CPAP machines.
Feeding Assistance: Initially through IV or feeding tubes.
Phototherapy: To treat jaundice.
Complications
Premature birth can lead to:
Short-term complications: Breathing problems, heart issues, brain problems, digestive issues, blood problems, metabolism problems, and immune system problems.
Long-Term Complications: Cerebral palsy, learning disabilities, retinopathy of prematurity, hearing loss, enamel defects, and increased risk of conditions like autism spectrum disorder.
When to See a Doctor
Contact your doctor if you experience:
Regular contractions or tightenings.
Excess fluid leakage.
Vaginal bleeding.
Reduced fetal movements.
Persistent pelvic pressure.
Prevention
To reduce the risk of premature birth:
Maintain a Healthy Weight: Through a balanced diet and exercise.
Stay Active: To reduce risks of complications.
Manage Stress and Depression: Seek help if needed.
Quit Smoking and Avoid Alcohol: For a healthier pregnancy.
Check Medication Safety: Ensure medications are safe for pregnancy
Prevent Infections: Practice good hygiene.
Even with no identifiable risk factors, regular prenatal care is essential.
Conclusion
Premature birth is a complex issue with significant implications. Understanding the signs, causes, and potential complications can help expectant parents manage this challenging situation. With advances in medical care, many premature babies lead healthy lives. For comprehensive care, choose the best hospital in Varanasi.
For personalized care and support, visit Arvachin Hospital, a leading medical facility dedicated to providing top-notch healthcare.
0 notes
Last Seen Blogs


hxndsofstone
eyes like a car crash

hqmillioncorn
bwah

gummihosencleverinternetpos-blog
Unbetitelt

veliaoceanlight
Velia