#fluvoxamine overdose
Text
A Comprehensive Analysis on Eric Harris, 3.
Disclaimer: This analysis/psychoanalysis is limited only to analysis as a means to reflect and understand the people involved. It is strictly informative. Just like all of my posts, I am detached from the media I write about and solely focus on the people to understand their psychology, for others to gain insight. There is no room for me to romanticize or glorify anything I write because I am only here to explain. I understand and research, but I do not condone. Thank you.
note: This is all solely based on independent research. If I may be wrong with the medical aspects of this post, please correct me. I would appreciate it a lot.
Fluvoxamine Maleate

Just a few days before the shooting, Eric was promptly rejected from his application to serve in the marines. Despite his desirable qualities, he was rejected for the sole reason of being tested positive for consuming a prescripted drug after rejecting that he was off any medication. With a trace of Luvox in his system, theories speculate that the drug's side effects played a role on the events that have transpired. Luvox is a medication prescription drug that is used to treat mental illnesses such as Obsessive Compulsive Disorder (OCD), anxiety, depression, and others. While there are positive effects, the downside are heightened sensations of dread, irritation, depression, and arising violent behaviors. It also has a chance to increase manic symptoms, especially if taken in particularly large doses.
Anti-depressant usage, effects of overdose, and detoxification
When taken over the prescribed dosage, Luvox can lead to increased agression and suicidal ideation and tendencies. Eric was in anger management therapy after being on probation alongside Dylan for attempting to steal a vehicle containing thousands worth of valuable electronics and tools. After getting caught, Eric openly expressed his difficulties in managing his anxiety and explosive anger issues that his counselor said, "he frequently blew up and often cried." Revealing that this influences his homicidal and suicidal thoughts, so he was prescribed Fluvoxamine, which is a selective serotonin reuptake inhibitor (SSRIs). These drugs increase the capacity of the brain to receive serotonin.
According to an interview with Eric's friends, they speculate that Eric was off his medication completely for sometime. Abruptly stopping medication can lead to the development of a more violent response. For some people, drugs are able to fix their chemical imbalances, but it can also lead to withdrawal symptoms of taken for over the duration of 6 weeks. Abruptly discontinuing anti-depressants can lead ro rebound depression or relapse. Symptoms may return stronger than before. Furthermore, SSRI's such as Luvox and Prozac take about 5 days to linger in one's system before subsequently washing off.
In a period of 11 months, Eric and Dylan have been under a juvenile detention program at Jefferson County district — this was in 1998, just a year before the shooting. They were allowed to leave the program by early February 1999. After finishing, Eric wrote a letter contained in his juvenile diversion program file. He states, "I learned that thousands of suggestions are worthless if you still believe in violence."
After public demands for stricter regulations on SSRIs after the tragic shooting, Luvox was temporarily banned in 2002. By 2008, drug manufacturers had reformulated Luvox to a controlled-release version specifically designed to treat OCD, excluding indications for depression or anxiety. Subsequently, the FDA approved Luvox CR for the treatment of OCD. The label does not explicitly prohibit prescribing it to the pediatric population, it notes that the smallest dose "may not be appropriate" for children, without providing further explanation.
Eric was about 17 at the time of taking the medication, which means he is part of the pediatric population. Though it's still unclear if he was taking normal doses for a long period of time or taken more than what was prescribed, it is clear that there was negligence with prescribing a child a SSRI that has the posibility of worsening their already apparent symptoms.
Columbine was really a case that opened the public's eyes into the dysfunctional aspects of society and institutions, transcending even to the medical field.
338 notes
·
View notes
Text
What is the fastest medicine for muscle pain?

Soma uses
Carisoprodol, also known as Soma, is a generic medication. It is a muscle relaxant and pain medication used to treat muscle spasms and musculoskeletal discomfort. It is a prescription drug that was approved by the Food and Drug Administration (FDA) in 2007. Soma should only be used for two to three weeks at a time because it can cause violence, addiction, and physical dependence. Because of its potential for violence, it is classified as a restricted substance. In the United States, the sale of Soma without a prescription is illegal, and no one can buy soma without a prescription.
It is only one part of the recovery process; proper rest, physical therapy, and other therapies are also important. The usual soma dosage is 250-350 mg three times a day, depending on the user's condition. The drug can only be used for two or three weeks at a time. It can be taken with or without meals, however the pill should not be broken or crushed. You may experience withdrawal symptoms like as stomach cramps, headaches, sleeplessness, and nausea if you stop taking the medicine suddenly. Stick to the correct dose to avoid becoming addicted to soma.
Side effects
Headaches, dizziness, back discomfort, anxiety, nausea, stuffy nose, and upset stomach are just a few of the Soma side effects. Hives, difficulty breathing, and swelling of the ears, mouth, lips, and tongue are just a few of the side effects of carisoprodol. Stop taking the medicine and seek medical care if you have any of the following symptoms:
Seizures
A rash on the skin and a slow heartbeat
Drowsiness that is severe
Shakiness or a loss of coordination
Problems with the stomach, nausea, or vomiting
Soma abuse and addiction
Carisoprodol abuse is common, and it is classified as a Schedule IV narcotic in the United States. However, soma is lawful to take with a prescription. Because soma has sedative and anxiolytic qualities, addicts abuse it by taking massive amounts to get the most out of it. Because of the way soma interacts with the brain, it can lead to addiction and dependency; once an individual has become dependant on the chemical, withdrawal symptoms can occur if they stop taking it. Changes in Cognitive Function, increased anxiety, depression or sadness, tremors, increased heart rate, agitation, and hostility are among withdrawal and dependence signs. In some circumstances, these symptoms might be fatal. As a result, for your own safety, we urge that you only buy soma online or offline with a doctor's prescription and utilise it with caution.
Warnings and precautions
When you combine carisoprodol with opioids, the opioid effects become stronger and more potent, increasing the risk of overdose and death.
When taking soma, avoid drinking alcohol because it can induce serious side effects like slurred speech, blackouts, and loss of coordination.
Because the liver and kidneys are involved in the removal of carisoprodol from the body, your healthcare practitioner may need to keep a closer eye on your response to it if you have a problem with their function.
Because Soma can make you drowsy and dizzy, you should avoid driving or doing anything else that demands focus or concentration until you know how it affects you.
Soma use is not advised during pregnancy.
Because a small quantity of the medicine can pass through breastmilk, speak with your healthcare professional before taking it.
If you're on any other medications, tell your doctor because soma can cause seizures.
Soma interactions
Carisoprodol has the potential to interfere with and change the actions of other medications. Some Soma interactions are as follows:
It may exacerbate soma symptoms, such as sleepiness, when taken with benzodiazepines.
It can increase the amount of Soma in your bloodstream when combined with other medications like omeprazole and Fluvoxamine, as well as exacerbate the negative effects of Soma when combined with opioids.
It does not perform as well when used with rifampin, prompting you to increase your soma dosage, which could lead to Soma addiction.
Order soma online
Do your research before purchasing soma online, as many websites perpetrate fraud or sell counterfeit medications. If you're looking for a site to buy cheap soma pills online, you've come to the perfect place. Several of our websites offer authentic carisoprodol tablets at a low cost.
We also provide the option of ordering carisoprodol cod. So, if you don't have a credit or debit card, we can help. You can easily select COD at the payment portal, and we will deliver your drugs on time after your order is received.
0 notes
Text
Fluvoxamine side effects are common in USA

Fluvoxamine can be used for a number of different things that are not mentioned in this medication guide. There is often a low intensity similar to high intensity. All you have to do is try to take the prescription prescribed for your illness. Dizziness, nausea, vomiting, dry mouth, indigestion, loss of appetite, hyperbolic sweating, nervousness, and tremors are some of the side effects of Fluvoxamine. Fluvoxamine should be taken at bedtime without food.
If you suddenly stop using fluvoxamine, you may experience unpleasant side effects (such as agitation, confusion, tingling, or electric shock sensations). Before you stop taking your medicine, ask your doctor for advice. Store tightly closed at room temperature away from moisture and heat. Take the pills as soon as possible, but skip this delayed dose if your next dose is near. Do not mix 2 doses at the same time. Fluvoxamine enhances this effect when combined with different tranquilizers.
Visit Us:-https://alloverchemist.uk/
#fluvoxamine#fluvoxamine 100 mg#fluvoxamine maleate#fluvoxamine side effects#fluvoxamine brand name#fluvoxamine overdose
0 notes
Text
Fluvoxamine 100mg Benefits in the United States

Fluvoxamine 100 mg, one of the most well-known selective 5-hydroxytryptamine uptake inhibitors, is used to patients suffering from severe depression in a few countries. Many studies have looked into the viability and efficacy of fluvoxamine 100 mg as a treatment for major depression. Obsessive Compulsive Disorder is treated with fluvoxamine audits. Fluvoxamine gets a seven on a scale of one to ten.
From a total of 177 evaluations, three out of ten were positive for the treatment of obsessive-compulsive disorder. Sixty-three experts reported a good effect, while eighteen reported a negative effect. Fluvoxamine 100 mg was the only energizer that was approved for clinical usage in the United Kingdom. In 1983, Kali-Duphar created it in European countries and marketed it as Floxyfral in Switzerland and industrialist in European countries.It was approved by the Food and Drug Administration on December 5, 1994, and is sold in the United States as fluvoxamine UK (Luvox).
Visit Us:-https://alloverchemist.uk/
#fluvoxamine#fluvoxamine 100 mg#fluvoxamine side effects#fluvoxamine covid#fluvoxamine maleate#fluvoxamine brand name#fluvoxamine overdose
0 notes
Text
Addiction is a chronic, relapsing brain disease that results in changes to motivation. Dopamine (DA) drives motivation. Drugs cause increased DA.
They don't say "detox" anymore. Now it's called "medically-supervised withdrawal." "Abuse" and "dependence" are no longer used; now it's called "substance use disorder." Substance use disorder (SUD):
Physiology (tolerance and withdrawal) + loss of control (use more than intended, spend a lot of time trying to obtain drug, can't cut down, give up activities, have cravings) + consequences (unfulfilled obligations at work, school, home, interpersonal problems, dangerous situations, medical problems).
OBOT = Office-Based Opioid Treatment.
In 2000, the Drug Addiction Treatment Act (DATA) allowed qualified physicians to offer OBOT; allowed physicians to prescribe schedule III, IV, and V narcotic medications approved by the FDA in treatment settings other than Opioid Treatment Programs (OTP).
In 2016, the Comprehensive Addiction and Recovery Act (CARA) allowed NPs and PAs to become eligible to prescribe buprenorphine.
The pt must have 2 or more of the 11 criteria within the past year in order for you to diagnose an OUD.
Drugs for tx of OUD:
-Buprenorphine (partial mu-opioid receptor agonist)
-Methadone (mu-opioid receptor agonist)
-Naltrexone/naloxone (mu-opioid receptor antagonist)
90% of heroin addicts relapse without Medication-Assisted Treatment (MAT). MAT decreases mortality, increases retention in treatment, and improves social functioning. The risk of death without treatment is 500% higher than the general population! Even with treatment, there is a 2x increased risk of death in pts with OUD compared to the general population.
Endogenous opioids: endorphins, dynorphins, enkephalins
Opiates: morphine, codeine
Semisynthetic opioids: buprenorphine, heroin, oxycodone
Fully synthetic opioids: fentanyl, methadone
Opioids in the thalamus cause analgesia. Opioids in the Ventral Tegmental Area (VTA) cause DA release to the Nucleus Accumbens (NAc), the pleasure/reward center of the brain-> addiction.
Buprenorphine is schedule III, unlike full agonists. It's unlikely to cause fatal respiratory depression since it's a partial mu-opioid receptor agonist. Buprenorphine has higher affinity for the mu-opioid receptor than other opioids (e.g., heroin, methadone), and can displace them, leading to precipitated withdrawal.
Naltrexone can be taken PO QD or IM monthly. It reduces cravings by reducing endorphins. It prevents heroin and other opioid agonists from binding the mu-opioid receptor. Treats alcoholism too.
Pts with OUD develop tolerance to the effects of sedation, euphoria, respiratory depression, and nausea caused by opioids, but do not develop tolerance to the constipation and miosis caused by opioids. Treatment causes loss of tolerance, which increases the risk of overdose, should the pt take the opioid again at the same dose he used to take it before gettting treatment. So you have to warn patients that if they get treatment and then go back to abusing opioids, they could overdose and die.
Clonidine is an alpha-2 agonist, decreases presynaptic release of norepinephrine; decreases anxiety/restlessness that occurs in withdrawal from opioids. You can give loperamide for the diarrhea; NSAID for muscle and bone aches; and ondansetron for the N/V that occur in withdrawal. Methadone and buprenorphine treat withdrawal sxs. Only a federally and state-licensed program can prescribe methadone.
The R-enantiomer of methadone is therapeutic; was used to treat pain in 1947 and OUD in 1970. The MAT waiver training is a waiver to the 1973 law that allowed methadone to be used for maintenance treatment of OUD.
Methadone is metabolized by CYP3A4 and is detectable in urine. It's a full mu-opioid receptor agonist with weak affinity for the receptor; can be displaced from the receptor by buprenorphine, naloxone, and naltrexone. Overdose of methadone can lead to respiratory arrest and QT prolongation.
Buprenorphine doesn't cause respiratory arrest if used as prescribed; can be lethal if mixed with other sedatives (e.g., EtOH or benzodiazepines). It has high affinity for the mu-opioid receptor. The pt needs to be withdrawing from opioids to start buprenorphine, otherwise the buprenorphine triggers withdrawal.
I remember one of the nurses at the psych hospital I worked at would say "the pt is having a sub for lunch" to let me know she had just given the sublingual suboxone (buprenorphine + naloxone) to a pt. Buprenorphine is mixed with naloxone to prevent people from abusing it. If the pt takes the combination sublingually, then the naloxone has poor bioavailaility. If the pt injected the combination, then the naloxone would have higher bioavailability, so injecting the combination of drugs can't cause the pt to get high. It prevents diversion of the drug to abuse. The ratio of buprenorphine to naloxone is 4:1. So suboxone is 2 mg buprenorphine to 0.5 mg naloxone.
Naltrexone can be given after the pt is off opioids for 7 to 10 days; works just as well as buprenorphine, but waiting the 7 to 10 days to start it can be difficult for pts who are experiencing withdrawal sxs.
Dosing:
-Methadone: 80-100 mg
-Buprenorphine: 4-32 mg
-Naltrexone: 380 mg depot
Since naltrexone is an opioid receptor antagonist, you can't give pts on naltrexone opioids for pain management--it won't work.
Buprenorphine dosage is changed based on the pt's cravings--increase the dose to decrease cravings; treatment lasts as long as the pt benefits from it. AEs of buprenorphine: HA, constipation, xerostomia. All opioids cause dry mouth (one of the reasons heroin addicts can have poor dental health--the drugs dry the mouth out and increase risk of cavities).
DDIs of methadone:
-SSRIs (esp. fluvoxamine) cause decreased metabolism of methadone-> increased blood levels of methadone -Carbamazepine induces methadone metabolism. So use valproate or something other than carbamazepine; but if carbamazepine is necessary, increase or split methadone dose.
-Do not use MAOIs with methadone; TCAs have decreased metabolism when combined with methadone-> increased TCAs (increased risk of TCA toxicity, which is convulsions, cardiac toxicity, and coma).
If pt is on buprenorphine, stop it before giving naltrexone.
16 notes
·
View notes
Text
Waklert 150mg Pills: Uses, Dosages Side-Effects and Precautions
What conditions are treated using this medication?
Waklert is medically approved and traditionally used for treating excessive daytime sleepiness caused by sleep apnea, shift work sleep disorder and narcolepsy. It is also regularly used off label to treat a wide range of conditions including jet lag, "atypical" depression, neurological fatigue, weight loss, Parkinson's disease and ADHD. University students routinely use it for it's cognitive enhancement effects and militaries from several countries around the world including the US military use it as an alternative to amphetamines. (Buy Waklert 150mg COD)

In 2009, the Canadian Medical Association Journal reported that Armodafinil is used by ISS (International Space Station) crew members due to it's vigilance enhancing effects allowing them to optimize their performance, regardless of how fatigued they feel. In the last four years alone, sales of Armodafinil have increased by 74% due to a number of factors including many senior executives such as Silicon Valley investor, Dave Asprey, going public about their daily use which they claim allows them to perform better with elevated mental clarity, focus, concentration and drive.
A quick search of his name in YouTube will reveal countless videos of this colloquially named "bullet proof executive" plus many other people in professional capacities discussing their personal use of the medication with the likes of CNN and ABC news.
Recommended dosage of Waklert:
The recommended dose of Waklert 150 mg taken once a day in the morning or early afternoon with a glass of water except in the case of shift work sleep disorder where it should be taken approximately one hour before work.
Doses of up to 300 mg a day in a single dose or split into two doses of 150 mg have been well tolerated and whereas some people benefit from the increased dosage, others have reported no additional benefit beyond that of a single dose.
If you want to learn about the Best Pills For Cognitive Enhancers Waklert is non addictive and the potential to suffer severe or even moderate adverse reactions is extremely low. Clinical trials involving high doses for extended periods indicate no long terms damage occurs and there are no recorded cases of overdose.
Are there any side effects associated with taking this drug?
Most people suffer no side effects from using Waklert but about 5% of users reported mild side effects including headache, nervousness, rhinitis, nausea, anxiety, insomnia, dizziness, back pain, stomach upset or diarrhea.
Rare side effects include mental or mood changes (confusion, agitation, depression, hallucinations and abnormal thoughts), chest pain, fast/irregular/pounding heartbeat, signs of an infection (fever, persistent sore throat) and users should seek medical attention in any of these cases. (Buy Waklert Online in USA)
A severe allergic reaction to the active ingredient is extremely rare but stop using it and seek immediate medical attention if after using Armodafinil, you notice a skin rash developing, blister/peeling skin, trouble breathing, severe dizziness, itching or swelling of the face, throat or tongue.
Contraindications and warnings:
If you plan on using Waklert, it is important to consult with a doctor beforehand if you have had any previous cardiovascular problems particularly when using other pharmaceutical stimulants. Individuals with a history of cardiac condition such as left ventricular hypertrophy and mitral valve prolapse should also consult a doctor before taking Armodafinil.
Before using generic Nuvigil, consult with your doctor or a pharmacist regarding any prescription or non-prescription/herbal products you are using, especially medications for high blood pressure and/or stimulants ("beta blockers" (e.g. metoprolol, atenolol, guanabenz, methyldopa, clonidine, prazosin) "blood thinners" (e.g. warfarin), stimulants (e.g. ritalin, adderall, dexedrine), "drugs that affect liver enzymes" (e.g. rifamycins such as rifabutin/rifampin, antifungals such as itraconazole/ketoconazole, anti-seizure medications such as carbamazepine/phenobarbital).
The active ingredient, Armodafinil, may speed up or slow down the removal of other prescription drugs from the body by affecting certain liver enzymes. The affected medications include cyclosporine, propranolol, phenytoin, diazepam, theophylline, triazolam and certain antidepressants (e.g. clomipramine, desipramine, fluoxetine, fluvoxamine). Avoid taking MAO inhibitors (furazolidone, moclobemide, linezolid, isocarboxazid, phenelzine, tranylcypromine, selegiline, procarbazine) in the 2 weeks before, during, and after treatment.
Please note this is only a brief summary of the warnings and contraindications associated with the use of Armodafinil and potential users should seek more details either from a qualified physician.
Visit us to Buy Waklert Online without Prescription
#Buy Waklert Online#Waklert Pills Online#Buy Waklert Cash On Delivery#Waklert COD#Buy Waklert 150mg COD#Waklert Tablets Online#Purchase Waklert Online#waklert online paypal#waklert 150 buy online#waklert buy online
3 notes
·
View notes
Text
Marijuana and Medications
Marijuana refers to the parts of the Cannabis plant that are smoked or consumed in edibles. This plant contains 483 substances, some of which are psychoactive (cause changes in the brain). Sixty-five of these substances are called “cannabinoids” because when they get into your body, they bind to these molecules called “cannabinoid receptors” which then triggers a cascade of other biochemical reactions in the body. The most potently psychoactive compound in marijuana is a cannabinoid called tetrahydrocannabinol, or THC. Another prominent cannabinoid is cannabidiol, or CBD.
Marijuana has been classified by the Drug Enforcement Agency (DEA) as a schedule 1 narcotic. This classification means that according to the federal government, marijuana is a highly addictive drug with no medical usage whatsoever. For comparison, methamphetamine is a schedule 2 narcotic. So is cocaine. The classification of marijuana as a schedule 1 substance is, well, ridiculous, but also problematic because since the government says it has no medical use, it’s really hard to do controlled studies to determine if it DOES have a medical use. So good, hard evidence about the efficacy of marijuana and its derivatives for various health complaints is lacking.
As a recreational drug, marijuana causes feelings of being “high” or stoned, changes in perception (how the world looks/sounds/smells etc), increased appetite, and an elevated mood. Adverse effects include paranoia, red eyes, short term memory loss, and loss of motor skills.
Is marijuana safe? Well, that depends on what you mean. Marijuana is almost impossible to overdose on. That said, it does cause loss of motor skills that can lead to accidents including motor vehicle accidents. Smoking marijuana carries many of the same risks as smoking cigarettes. High THC strains of marijuana have also been linked to new cases of psychosis. It’s true that no one has ever died of a marijuana overdose, but that doesn’t mean it’s completely safe. It is also possible to develop a psychological dependence on marijuana, though physical addiction is much less common.
As a medication, marijuana or its derivatives have been cited as effective for everything from chemotherapy induced nausea and vomiting to pain relief to depression and anxiety. Dronabinol, a synthetic form of THC, is FDA approved to treat HIV-associated anorexia and chemo-induced nausea and vomiting, so natural THC probably has similar effects..
One of the biggest questions facing the medical community is, how effective is marijuana for pain relief? Well, that’s not a simple answer. Hill et al. [1] published a review in 2017 of studies that looked at marijuana as a treatment for pain. In general, studies have shown that marijuana can alleviate pain, especially chronic pain, but the pain relief isn’t caused by a simple dose-response mechanism (higher doses don’t lead to greater pain relief). Anecdotally, I’ve had patients swear that marijuana has worked for them when nothing else touched their pain. I’ve had patients tell me that marijuana gave them their lives back. I’ve also had patients tell me that marijuana did nothing for them. I’m hoping with more states decriminalizing marijuana, we’ll start to see some robust research coming out so we can start figuring out how marijuana actually works.
Because research about marijuana is lacking, we don’t have a lot of good information about drugs that interact with marijuana. We do have a few theories though.
Remember those CYP enzymes I was talking about in an earlier post? Here’s a quick review. CYP enzymes are molecules in the body, predominantly the liver, that cause chemical reactions to occur. Most of these chemical reactions help your body eliminate drugs from your body, though some of the chemical reactions also activate drugs in your body. There are a ton of CYP enzymes, and they’re all named with a combination of letters and numbers to tell them apart.
THC is metabolized (broken down) by CYP2C9 and CYP3A4. Some medications can “turn off” a CYP enzyme, which prevents it from working to eliminate THC from the body. If CYP2C9 or CYP3A4 is turned off, then they can’t metabolize THC, which could lead to THC building up in the body and causing toxicity. Drugs that turn off CYP2C9 include amiodarone, cimetidine, cotrimoxazole, metronidazole, fluoxetine, fluvoxamine, fluconazole, and voriconazole. Drugs that turn off CYP3A4 include clarithromycin, erythromycin, cyclosporine, verapamil, itraconazole, voriconazole, and boceprevir.
It gets more complicated. It turns out that THC and CBD have the ability to affect CYP enzymes, too. Except they don’t turn CYP enzymes off, they RAMP IT UP. Specifically, CYP1A2. THC and CBD put CYP1A2 into overdrive, so any drugs metabolized by that enzyme get metabolized FASTER, leading to patients not getting enough exposure to the medication for it to work. Drugs that could get metabolized too quickly include theophylline and chlorpromazine [2].
One final thing concerning drug interactions. Patients should be cautious using marijuana if they’re using other drugs that have similar effects. You can expect interactions between marijuana and drugs with sympathomimetic activity (tachycardia, hypertension), central nervous system depressants (drowsiness), and drugs with anticholinergic effects (tachycardia, drowsiness). For example, diphenhydramine (Benadryl) causes drowsiness. Using marijuana and Benadryl together can cause more drowsiness than either would cause alone. Side effects can stack up.
I hope this was at least a little bit helpful. If you have any questions, feel free to shoot me a message or an ask. I’m more than happy to break things down or explain concepts further.
1. Hill KP, Palastro MD, Johnson B, Ditre JW. Cannabis and Pain: A Clinical Review. Cannabis Cannabinoid Res. 2017;2(1):96–104. Published 2017 May 1. doi:10.1089/can.2017.0017
2. https://www.pharmacytimes.com/publications/issue/2014/december2014/drug-interactions-with-marijuana
19 notes
·
View notes
Text
Fluvoxamine May Well Be a Conformity Pill in USA

Fluvoxamine 100 mg Tablets might even be a wide illustrious medication that will be conversant in treating a selection of depressive and compulsive disorders. many folks face in their real activities. As a mark, the prescription will quickly appease the recession. One pill of Fluvoxamine 100mg should be taken once on a daily basis, with or whereas not food. additionally, each day's dose consumption ought to be timed. Your dose won't be lost throughout this fashion. once analyzing your condition, the doctor determines the dose to be taken.
1st and foremost, don't skip a dose since this might delay your recovery. Also, if you forget to want your medicine, take it as presently as you remember. Overdosing won't assist you to recover quickly from your illness. Follow your doctor' directions for administering your drug. The oral pill Fluvoxamine 100 mg has been incontestable to be effective in the treatment of depression and neurotic disorder. it's really advantageous to any or all folks.
Visit Us:-https://pillsinpocket.com/
0 notes
Text
What we know about Ivermectin: correlation is not causation
Unlike the huge amount of high-quality data we have gathered on vaccines (5.6 billion doses and counting), the available data on Ivermectin is a dog’s breakfast – despite the fact that millions of people around the world have used it to treat COVID, especially in poor countries.
The hope that Ivermectin could vanquish COVID was seeded from Kylie Wagstaff’s lab at Melbourne’s Monash University. Knowing that the drug had anti-viral effects, they decided to test it against COVID using infected monkey cells growing in a dish. In April 2020 they published a paper describing how, 48 hours after dosing the monkey cells with Ivermectin at a concentration over 10 times that used to treat parasites, virtually no virus was detectable.
Credit: Cosmos Magazine
There was almost nothing around to treat COVID patients in April 2020. Given the horrific rising death toll in South America and India, and that Ivermectin was already widely used as a medication to treat diseases caused by parasitic worms like river blindness or scabies, the WHO kept an open mind, as they did for other cheap off-label drugs like dexamethasone and hydroxychloroquine.
But the WHO made it clear that Ivermectin should only be used in the context of a trial – drugs can make things better or worse. Indeed, thanks to trials, we now know that dexamethasone helps COVID patients; hydroxychloroquine makes them worse.
But in places reeling from the pandemic, particularly across South America, there was a massive uptake in the use of Ivermectin, sometimes officially sanctioned by local or national authorities as in Peru, Bolivia, Brazil, some states of India (Uttar Pradesh), Bangladesh and Zimbabwe.
June 2020 alone saw Brazilians purchase 12 million packets of Ivermectin – a year’s worth of the drug in a single month. It didn’t seem to affect the death rate. One Brazilian scientist observed, “the shape of COVID curves did not exhibit any modification when comparing groups of treated and untreated people from the same area”.
On the other hand, Zimbabwean doctor Jackie Stone trumpeted the success of Ivermectin, because after its use was authorised in Zimbabwe on 26 January 2021, death rates fell from 60–70 per day to zero by 2 February 2021.
That sort of correlation is intriguing. But it’s famously fallible – the “correlation is not causation” conundrum. You can show that drownings increase after ice cream consumption but it’s not because a belly full of ice cream cramps your muscles. It’s because both events are more common in summer. Statisticians refer to summer, the sneaky third wheel, as a confounding variable.
You can show that drownings increase after ice cream consumption but it’s not because a belly full of ice cream cramps your muscles. It’s because both events are more common in summer.
The fact is COVID death rates fluctuate and researchers have yet to figure out why. Zimbabwe was back up to over 100 deaths per day in late July, and then down to 19 per day in September. As Gideon Meyerowitz-Katz, an epidemiologist from the University of Wollongong, put it: “Merely correlating news reports of Ivermectin use with later declines in mortality as if those two things are realistically connected; it’s not science in any meaningful sense.”
Meyerowitz-Katz’s blog on Ivermectin is a great source of information. So is this August article from Liam Mannix in the Sydney Morning Herald.
With so many people taking Ivermectin in some countries, it became hard to do placebo-controlled clinical trials.
Those that were done were often small – just dozens of people – and “observational”, meaning the doctor prescribed the drug to the patients and watched to see how they fared. If a drug has a large beneficial or adverse effect, observational studies should pick it up. But observational studies do poorly with small effects and can’t accurately measure their size. Without a concurrent matched control group who are not taking the drug, you can’t zero out the turning of that hidden third wheel.
Most of the observational studies aimed to see if Ivermectin could be used to treat patients at home and prevent them from progressing to severe disease. Some showed benefit in terms of lowering viral loads and quicker recovery times. Others did not. One of the few statistically significant placebo-controlled studies from Colombia showed no effect of Ivermectin.
A few of the studies weren’t just compromised by being flawed: they were possibly fraudulent. Taking advantage of the desperation for answers, some researchers sought to make a name for themselves in the dodgy world of online pre-prints. These are papers that have yet to clear the hurdle of peer review and their findings should be treated with caution. In the case of Ivermectin, two pre-prints that showed a significant protective effect of Ivermectin were later retracted; one from the Chicago-based data company Surgisphere and another from researchers at Benha University, in Egypt.
To try to read an overall signal from the many small studies, researchers have collected them in what is known as a ‘meta-analysis’. But it all depends on which studies they picked. Some meta-analyses showed a net positive effect (particularly if they used the retracted Egyptian data). Others found no conclusive effects.
The most reliable of these meta-analyses was a 28 July Cochrane review. This international organisation specialises in adjudicating medical controversies by deploying independent statisticians and medical experts to sift out and analyse credible published studies. Their review concluded: “We are uncertain whether Ivermectin reduces or increases mortality compared to no treatment.”
It’s easy to understand the desperation of people turning to Ivermectin in 2020. In 2021, it’s harder to fathom why people in the US and Australia – who have easy access to vaccines – would opt to bet their health and their life on it. Merck, the company that manufactures Ivermectin, is certainly not pushing its use for COVID.
A recent alert from the US CDC noted a 24-fold increase in Ivermectin prescriptions from pre-pandemic levels, as well as cases of people using veterinary products. It noted: “Overdoses of Ivermectin are linked with low blood pressure, confusion, hallucinations, seizures, coma and even death.”
“Overdoses of Ivermectin are linked with low blood pressure, confusion, hallucinations, seizures, coma and even death.”
The FDA took to Twitter to convey the dangers: “You are not a horse. You are not a cow. Seriously, y’all. Stop it.” It warned that “taking large doses of this drug is dangerous and can cause serious harm”. Australia has followed suit, with prescriptions up 3-4 fold leading the TGA to take the extraordinary step of banning its off-label use for fear of depriving people who need to use Ivermectin to treat parasites.
One of my vaccine-hesitant friends who is keen on Ivermectin pointed me to the trials being done by Sydney doctor Thomas Borody. Borody has treated around 25 COVID-positive patients in home quarantine, some as young as 16. He says most recovered without being hospitalised, though one died. Yet we know 90% of people do recover without being hospitalised. These do not strike me as good statistics upon which to be making life-and-death decisions. Nor is Borody claiming that Ivermectin is an alternative to vaccines. It is, he says, “another string to the bow”.
To find out how well that string plays, we’ll need to wait for the results of large placebo-controlled clinical trials currently underway.
These include the Oxford trial known as PRINCIPLE, another at McMaster University in Canada called TOGETHER and one at the US National Institutes of Health known as Activ-6.
These trials focus on repurposed drugs like Ivermectin that are cheap and readily available. A key goal is to find the ones that will stop home-based patients from progressing to severe disease.
So far there are two: the inhaled steroid budesonide and (surprisingly) the anti-depressant fluvoxamine.
PRINCIPLE has shown budesonide shortens recovery time by three days in some patients. And preliminary results from the TOGETHER trial showed that fluvoxamine was mildly effective, reducing the relative risk of getting worse by 30%.
In August the TOGETHER trial showed Ivermectin had no statistically significant effect.
The other trials have yet to report – but don’t hold your breath.
“The evidence so far doesn’t point to a large effect, if any at all. To detect a small effect you need a much larger sample size – hence it will take a long time.”
Oxford is loathe to predict when they will have their results, but after badgering head investigator Christopher Butler, he guessed it might be in the first quarter of next year. The NIH apparently won’t have anything to say till 2023.
That seems absurd, given the epidemic of people taking the drug in the hope it will work.
Carlos Chaccour, an infectious disease specialist at the Barcelona Institute for Global Health who works on Ivermectin for malaria control and has tested it in a small trial for COVID, helped clarify the situation for me. “The evidence so far doesn’t point to a large effect, if any at all. To detect a small effect you need a much larger sample size – hence it will take a long time.”
YOUR COVID TOOLBOX: This article is one of a five-part series where Cosmos editor-at-large Elizabeth Finkel hunts down all the facts and figures you need to understand COVID-19 vaccines.
Elizabeth Finkel: A letter to my vaccine-hesitant friends
Are COVID-19 vaccines experimental?
The rollout: The danger of vaccines vs the danger of COVID
Adverse reactions: Guillain Barre, TTS and the fine mesh net
What we know about Ivermectin: correlation is not causation published first on https://triviaqaweb.weebly.com/
0 notes
Text
Fluvoxamine 100MG Be a Hardening Pill in USA

Fluvoxamine 100mg Tablets is also a well-known medicament that can be used to treat a selection of depressive and compulsive disorders. several people face in their real activities. As a result, the new meds can relieve low mood quickly. One pill of Fluvoxamine 100mg should be taken once on a daily basis, with or while not food. additionally, everyday' dose bodily processes should be timed. Your dose won't be lost during this way. when analyzing your condition, the doctor determines the dose to be taken.
1st and superior, don't skip a dose since this might delay your recovery. Also, if you forget to want your medicine, take it as shortly as you remember. Overdosing won't assist you to recover quickly from your illness. Follow your doctor' directions for administering your drug. The oral pill Fluvoxamine 100 mg has been incontestable to be effective in the treatment of depression and psychoneurotic disorder. it's terribly useful to any or all or any people.
Visit Us:-https://alloverchemist.uk/
#fluvoxamine#fluvoxamine maleate#fluvoxamine side effects#fluvoxamine brand name#fluvoxamine overdose
0 notes
Text
How Will Fluvoxamine Dosage Be In the Future in the United States?

Fluvoxamine maleate belongs to the class of drugs known as selective serotonin reuptake inhibitors. These drugs function in a similar manner. These drugs help to increase the volume of serotonin in our brain. This synthetic aids in the treatment of exaggerated impulsive behavior. Fluvoxamine measurements have been based on their medical condition, and a specialist's advice should be followed. The standard portion of this drug was mentioned here. The strength of the medication determines the volume of the medication. Regardless, the number of servings and dosages will be determined by your clinical problem.
Visit Us:- https://alloverchemist.uk/
#Fluvoxamine#fluvoxaminemaleate#fluvoxamine 100mg#fluvoxamine side effects#fluvoxamine covid#fluvoxamine overdose
1 note
·
View note
Photo



I fixed the spelling error and added more about how MAOIs work and their side effects.
Aside from imipramine and Doxepin, TCAs include amitriptyline, nortriptyline, and other “-triptylines.”
Bupropion (Wellbutrin) is a DA and NE reuptake inhibitor. Mirtazapine (Remeron) is an alpha 2-adrenergic receptor antagonist.
MAOIs are not used as first-line agents because of the increased safety and tolerability of newer agents, notably SSRIs/SNRIs. However, MAOIs are used for certain types of refractory depression and in refractory anxiety disorders: Phenelzine (Nardil), tranylcypromine (Parnate), isocarboxazid (Marplan).
HAM side effects (antiHistamine—sedation, weight gain; antiAdrenergic— hypotension; antiMuscarinic (anticholinergic)—dry mouth, blurred vision, urinary retention, constipation, exacerbation of neurocognitive disorders (i.e., dementias). Found in tricyclic antidepressants (TCAs) and low-potency anti - psychotics.
Serotonin syndrome: Confusion, flushing, diaphoresis, tremor, myoclonic jerks, hyperthermia, hypertonicity, rhabdomyolysis, renal failure, and death. Occurs when there is too much serotonin, classically when selective serotonin reuptake inhibitors (SSRIs) and monoamine oxidase inhibi-tors (MAOIs) are combined. As this combination is rarely seen in practice anymore, serotonin syndrome is more commonly seen when a patient is prescribed multiple medications with serotonergic activity (e.g., SSRIs/SNRIs, trazodone, Tramadol, triptans, dextromethorphan, St. John’s wort, ondansetron). Treatment: Stop medications, supportive care.
Hypertensive crisis: Caused by a buildup of stored catecholamines; triggered by the combination of MAOIs with tyramine-rich foods (e.g., red wine, cheese, chicken liver, cured meats) or with sympathomimetics.
Extrapyramidal side effects (EPS): Parkinsonism—masklike face, cog-wheel rigidity, bradykinesia, pill-rolling tremor; akathisia—restlessness, need to move, and agitation; dystonia—sustained, painful contraction of muscles of neck, tongue, eyes, diaphragm. Occur more frequently with high-potency, typical (first generation) antipsychotics, but can also be seen with atypical (second generation) antipsychotics. Reversible. Occur within hours to days of starting medications or increasing doses. In rare cases, can be life threatening (e.g., dystonia of the diaphragm causing asphyxiation).
Hyperprolactinemia: Occurs with high-potency, typical (first generation) antipsychotics and risperidone.
Tardive dyskinesia (TD): Choreoathetoid muscle movements, usually of the mouth and tongue (can affect extremities, as well). Occurs after years of antipsychotic use (more likely with high-potency, first-generation antipsychotics). Usually irreversible.
Neuroleptic malignant syndrome: Mental status changes, fever, tachycardia, hypertension, tremor, elevated creatine phosphokinase (CPK), “lead pipe” rigidity. Can be caused by any antipsychotic after a short or long time (increased with high-potency, typical antipsychotics). A medical emergency with up to a 20% mortality rate.
Drug interactions: Cytochrome P450 is a group of enzymes in the liver that metabolizes many common drugs, including psychiatric medications. Some medications induce the system, in other words the system metabolizes medications faster—drug levels decrease. Some medications inhibit the system, in other words the system metabolizes medications more slowly—drug levels increase. Common cytochrome P450 enzymes important in metabolizing psychiatric medications include CYP3A4, CYP2D6, CYP1A2, CYP2C9, CYP2C19.
Important CYP450 inducers include: Tobacco (1A2), Carbamazepine (1A2, 2C9, 3A4), Barbiturates (2C9), St. John’s wort (2C19, 3A4). Important CYP450 inhibitors include: Fluvoxamine (1A2, 2C19, 3A4), Fluoxetine (2C19, 2C9, 2D6), Paroxetine (2D6), Duloxetine (2D6), Sertraline (2D6).
New form, desvenlafaxine (Pristiq), is the active metabolite of venlafaxine; it is expensive and without known benefit over venlafaxine.
Bupropion (Wellbutrin) can decrease the seizure threshold and is contraindicated in pts with bulimia. Tricyclic antidepressants include amitriptyline, imipramine (treats enuresis), clomipramine (treats OCD), and doxepin (may be used as a sleep aid in low doses). Amitriptyline, imipramine, clompiramine, and doxepin are tertiary amines (highly anticholinergic/antihistaminergic [more sedating]/antiadrenergic [more orthostasis] with a greater lethality in overdose). Secondary amines (metabolites of tertiary amines (less anticholinergic/antihistaminic/antiadrenergic) are nortriptyline and desipramine. Tetracyclic antidepressant = amoxapine.
#antidepressants#mood stabilizers#TCAs#MAOIs#SNRI#SSRI#benzos#benzodiazepines#pharm#zoloft#tyramine#wellbutrin
6 notes
·
View notes
Text
well that was easy
I just--showed up at a random GP’s office, handed him my bottle of meds and said “hey I’m running low on these can I get a refill” and after quickly looking fluvoxamine up on the internet because I didn’t know its proprietary name in France and he didn’t recognize the generic, he was like “okay here’s a prescription for three months, that’ll be 25 euros” and even that I can probably get reimbursed if I fill out the correct forms
he didn’t make me give him paperwork from my psychiatrist or anything, he didn’t even check my ID to make sure I was the person named on the bottle
as he said, it’s not like you can really get high off it or die from an overdose so why would I lie about needing it
5 notes
·
View notes
Text
Fluvoxamine 100MG Is Curative Pill in USA

Fluvoxamine 100mg Tablets could be a well-known medicament that may be accustomed treat a range of depressive and obsessive-compulsive disorders. many folks collide in their actual activities. this enables the drug to quickly relieve depression. One 100 mg fluvoxamine tablet should be taken once daily with or without food. additionally, the intake of every daily dose should be timed. Your dose won't be wasted in this fashion. After analyzing your condition, the doctor will resolve the dose to be taken.
Past all, don't miss a dose because it will delay your recovery. If you forget to require your antidote, take it as soon as you recall. Overdosing won't facilitate your convalescence fast from your malady. Follow your doctor's instructions for administering your medication. Fluvoxamine 100mg oral tablet has been shown to be effective as an antidote to depression and obsessive-obsessional disorder. it's very beneficial for all somebody.
Visit Us:-https://pillsinpocket.com/
0 notes
Text
A Brief Explanation On Anti-Anxiety Medications
Americans' utilization of anti-anxiety meds has expanded significantly, and keeping in mind that drugs can play an important role in the treatment of anxiety disorders, they are not chance free and sometimes may intensify a problem. Nonetheless, because anti-anxiety drugs work rapidly and include less exertion than psychotherapy, they are a popular decision of treatment among the two doctors and patients. This might be particularly valid in the primary-care setting, where anxiety disorders are much of the time treated. You can now buy antianxiety medicine online from an online pharmacy and control your condition.
Types of Anti-Anxiety Medications
Selective Serotonin Reuptake Inhibitors (SSRIs). SSRIs are one of the most generally utilized types of the drug for anxiety and are regularly a psychiatrist's first decision for this purpose. SSRIs have been proven to be successful for anxiety, are non-addictive, don't cause memory impairment or meddle with psychotherapy, and have negligible side effects. At the point when SSRIs do cause side effects, they, for the most part, subside inside the principal week. An outstanding exception, however, is diminished sexual sensation, which happens in a significant minority of patients.

SSRIs work by expanding the measure of motioning between neurons that utilization a chemical called serotonin to speak with one another. They are additionally used to treat depression. As of now, accessible SSRIs incorporate Prozac (fluoxetine), Celexa (citalopram), Lexapro (escitalopram), Zoloft (sertraline), Paxil (paroxetine), and Luvox (fluvoxamine).
Serotonin Norepinephrine Reuptake Inhibitors (SNRIs). SNRIs do something very similar that SSRIs do; however, they additionally increment the measure of motioning between neurons that utilization a chemical considered norepinephrine to speak with each other. At the point when used to treat anxiety, the advantages and side effects of SNRIs are equivalent to those for SSRIs. Like the SSRI, the SNRIs take 4-to about a month and a half to arrive at the most extreme impact. The three right now accessible SNRIs are Effexor (venlafaxine), Cymbalta (duloxetine), and Pristiq (desvenlafaxine).
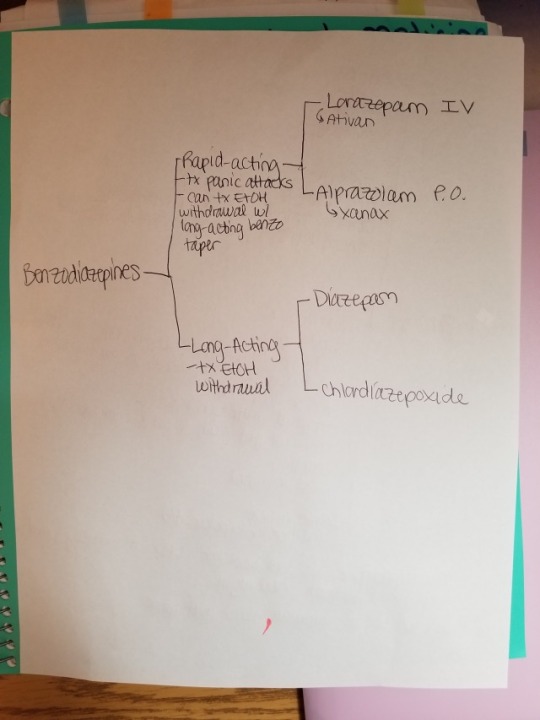
Benzodiazepines. This class of medicine incorporates the notable drugs Valium (diazepam), Xanax (alprazolam), Klonopin (clonazepam), and Ativan (lorazepam). Even though benzodiazepines are often prescribed for anxiety, particularly by non-psychiatrists, they are never again considered to be the first-line treatment for these conditions. They diminish anxiety rapidly; however, they can cause problems when taken long haul and ought to be utilized with alert.
Benzodiazepines cause resilience, which implies that over time a greater amount of the drug should be taken to accomplish a similar impact. There is likewise a withdrawal syndrome related to these prescriptions, which in the outrageous can cause seizures and even passing. Further, certain people may develop an addiction to these drugs. Benzodiazepines likewise repress the arrangement of new recollections, which can negatively affect psychotherapy. Also, these meds can be deadly when joined with alcohol or opioids and are engaged with a significant percentage of lethal overdoses.
Nonetheless, when utilized appropriately, benzodiazepines can play an important role in the treatment of an anxiety disorder. For example, they are once in a while utilized in combination with an SSRI for the initial hardly any long stretches of treatment before the SSRI arrives at greatest viability.
Click Here For More Information!
#buy antianxiety medicine online#antianxiety medicine#antianxiety medicine for sale#antianxiety medicine suppliers
1 note
·
View note
Text
Fluvoxamine Side Effects Are Standard in USA

Fluvoxamine side effects are available during a range of strengths, the foremost common of that being 50mg. there's often low intensity the same as high intensity. All you've to undertake and do is take the prescription that's prescribed for your illness. Fluvoxamine is often used for a range of various things that are not lined during this medication guide. Dizziness, nausea, vomiting, dry mouth, indigestion, loss of appetite, hyperbolic sweating, nervousness, and tremor are a variety of the Fluvoxamine side effects. Fluvoxamine must be taken before bedtime, while not eating.
If you suddenly stop exploiting fluvoxamine, you may expertise unpleasant aspects impacts (such as agitation, confusion, tingling, or reflex feelings). Before you stop taking your drug, seek advice from your doctor. Keep firmly closed and much aloof from wetness and heat at area temperature. Take the pills as shortly as possible, however, skip this delayed dose as your next dose is approaching. don't mix 2 dosages directly. Fluvoxamine will exacerbate this effect once combined with different sedatives.
Visit Us:-https://alloverchemist.uk/
#fluvoxamine#fluvoxamine maleate#fluvoxamine side effects#fluvoxamine brand name#fluvoxamine overdose
0 notes
Last Seen Blogs

realspear
Bang/Bang

starry-carrousel
Spica

rosariofigura
Siciliadom.ru

yanivkeymaster-blog
Untitled

daughter-of-the-clayr
does the walker choose the path?