#on site oxygen generator
Text
On Site Oxygen Generators - Efficient and Reliable

Absstem Technologies also deals in modern on-site oxygen generating plants which can be integrated & operated in different sectors. Our generators deliver an unbroken stream and ISO quality oxygen that eliminates interruptions and lowers expenses. Making use of new technologies and improved construction, our products are suitable for use in medical, industrial, and business applications. Get the advantage of having a source of oxygen in-house at your desired concentration. You are welcome to Absstem Technologies to get more details and to schedule an appointment with us.
0 notes
Text
The Advantages of On-Site Medical Oxygen Generators in Healthcare Facilities
The global healthcare sector has recently witnessed a paradigm shift in how medical facilities manage their oxygen supply. Innovative solutions have replaced traditional methods of relying on external suppliers for medical oxygen; among them, on site medical oxygen generators stand out prominently. In this article, we delve into the myriad advantages of on site medical oxygen generators, particularly those utilizing Pressure Swing Adsorption (PSA) technology, and why healthcare facilities should consider them indispensable. As we explore this revolutionary approach, we'll also touch upon the key players in the industry, with a special focus on Trident Pneumatics, a leading manufacturer of PSA medical oxygen generators.
Advantages of OnSite Medical Oxygen Generators:
On-site medical oxygen plant manufacturers provide healthcare facilities with unparalleled reliability and independence. By producing oxygen on-site, facilities can ensure a continuous and reliable supply, reducing the risk of disruptions arising from external factors such as transportation delays or supply chain issues.
Traditional methods of sourcing medical oxygen often involve significant transportation, storage, and delivery costs. On-site generators eliminate these expenses, offering a cost-effective solution in the long run. Facilities can redirect the funds previously allocated for logistical challenges towards improving patient care and upgrading medical infrastructure.
On site medical oxygen generators contribute to sustainability efforts by minimizing the carbon footprint of transporting oxygen cylinders. This environmentally friendly approach aligns with global initiatives to reduce the healthcare sector's environmental impact and supports the overall goal of creating more sustainable healthcare practices.
Unlike traditional methods that require facilities to estimate their oxygen needs in advance, on-site generators can adapt to varying demands in real time. This adaptability ensures a continuous supply of medical oxygen, even during unexpected surges in demand, offering healthcare providers the flexibility to respond to emergencies effectively.
On site medical oxygen generators allow healthcare facilities to exercise greater control over the production and distribution of medical oxygen. This enhanced control improves safety standards and quality assurance, crucial factors in a healthcare setting where patient well-being is paramount.
On-site generators are designed to be compact and space-efficient, allowing healthcare facilities to optimize their available space. This is especially advantageous for smaller healthcare centers or those facing space constraints. The modular nature of PSA medical oxygen generators ensures scalability, accommodating the needs of varying-sized facilities.
Relying on external suppliers for medical oxygen carries inherent risks. On-site generators empower healthcare facilities to reduce dependency on external sources, mitigating potential disruptions and ensuring a consistent oxygen supply critical for patient care and life-saving procedures.
Trident Pneumatics - Leaders in On-Site Medical Oxygen Solutions:
As the demand for on site medical oxygen generators grows, Trident Pneumatics stands out as a pioneer and a trusted name in the industry. Renowned for their cutting-edge PSA medical oxygen generators, Trident Pneumatics has been at the forefront of revolutionizing healthcare infrastructure.
The company's commitment to innovation, quality, and customer satisfaction has made it a preferred choice for healthcare facilities worldwide. Trident's on site medical oxygen generators are built on advanced PSA technology, ensuring efficiency, reliability, and compliance with the highest industry standards.
In conclusion, the advantages of on site medical oxygen generators, particularly those utilizing PSA technology, are evident in their reliability, cost-efficiency, sustainability, and adaptability. These generators have transformed how healthcare facilities approach oxygen supply, providing a solution that is both technologically advanced and environmentally conscious.
As healthcare facilities prioritize patient care and operational efficiency, on site medical oxygen generators are indispensable. Trident Pneumatics, among the leaders in this transformative field, has consistently delivered innovative, high-quality solutions, earning the trust of the healthcare industry.
For healthcare facilities seeking a reliable partner in implementing on-site medical oxygen solutions, Trident Pneumatics stands as a beacon of excellence, providing cutting-edge PSA medical oxygen generator that redefine the standards of healthcare infrastructure. Invest in the future of healthcare with Trident Pneumatics and experience the benefits of on-site medical oxygen generation firsthand.
0 notes
Text
On-site medical oxygen generators
On-site medical oxygen generators have several advantages over traditional oxygen delivery systems, such as cylinder-based oxygen supply. They eliminate the need for oxygen deliveries, reduce the risk of supply chain disruptions, and are more cost-effective in the long run. Additionally, they provide a more reliable and safe source of oxygen, as there is less risk of contamination and leakage.
0 notes
Text
Medical oxygen plant manufacturers
Trident Medical oxygen plant manufacturers are designed in such way, it is Low operating cost and PSA Medical oxygen generator will work at site 24 x7 without any trouble. Air dryer manufacturer, which enable it to develop dryers with highest quality performance.
0 notes
Text
PSA medical oxygen generator
PSA medical oxygen generator Plant is designed in such way, it will work at site 24 x7 without any trouble. All the components used in product are highly reliable and tested as per the Industrial standards. Trident makes a range of Heatless adsorption dryers type compressed air dryers which are regenerated by heat.
0 notes
Note
I’m not sure if this is off topic for your blog, but out of fear for my search history and the police, I wanted to ask if there is a means of someone producing a homemade bomb or something throwable that generates high levels of heat?
For context, the character I am writing is a lab intern that is secretly studying how to get rid of a parasite (think of something like Venom/Carnage) that can only be injured/destroyed with high levels of heat.
Two thoughts come to mind immediately, thermite and white phosphorous. So, in both cases, we're going to be setting metals on fire.
Thermite is more of a process than a specific chemical composition, which means getting the materials to make thermite explosives isn't that challenging. It involves getting a highly reactive metal, and then getting it to oxidize aggressively. Turns out, if you force aluminum to rust on the spot, it gets a bit warm. In some cases (such as with copper) the reaction is energetic enough to cause molten metal to splatter.
Because we're talking about different chemical mixtures, it's a bit hard to predict the exact tempreture, but most thermite reactions (at least, all of the ones I've ever looked up) will burn in excess of 2000K (3000F.)
Rigging thermite into a more portable form isn't that complicated, and crude pipe bomb-like containers should get the job done. Though, this would likely cause further problems.
The second option is white phosphorous. This burns at a lower temperature (around 800C), but this stuff ignites on contact with oxygen. Something you might be able to find in the air you're breathing. White phosphorous is a bit more tightly controlled, and is used in a wide variety of munitions. (In theory, it's used for tracers, as the phosphorous will ignite and glow while the round is traveling to its destination.) Because it will continue to burn in the wound, white phosphorous wounds are particularly horrific (as you'll see, if you ever visit the Wikipedia page.) However, it is already available as a payload for most military small arms cartridges.
A third option is classic napalm. This stuff tends to burn north of 800C. The actual material is a bit more disturbing than you might realize. Nalpalm isn't just a burning liquid, it's more like a burning goop, that sticks to whatever it hits... and continues to burn. Imagine a Vaseline sprayer (except, the Vaseline is ignited just after it leaves the nozzle.) Producing napalm in a modern chemlab, with a reasonable stockpile of ingredients shouldn't be too difficult, though it's unlikely the stockroom would have enough of the relevant chemicals to make much of the stuff. (Nalpalm flamethrowers go through a lot of fuel, so making the stuff on site might not be a great option.)
Using any of these methods will get a lot of attention on your character. While we tend to overestimate just how much casual searches for this kind of information are likely to land you on a watch list (this used to be more true than it is today), actually using them in the field will get an anti-terrorism taskforce crawling down around your character's ears. (Especially if they're making thermite loaded pipe bombs.)
Now, here's the funny thing about all of this: It's unnecessary.
You've got a monster that is vulnerable to flames. The simplest, and cheapest solution, is probably to go buy one of those orange, plastic, flare guns. This'll set you back less than $40 dollars (plus the cost of the included flares.) Then load up on extra flares, (at this moment, they're around $10 per flare.) (If you already have a 12 gauge shotgun, you can skip the flare gun entirely, and just buy 12ga flare shells.)
Those flares burn at similar temperatures to white phosphorous rounds, and are much, much, less regulated. (Though, if you're wandering out and buying up hundreds of flare shell rounds, that's likely to raise a few eyebrows.) (This is also true of normal emergency flares, similar temperatures, and they burn for much longer.)
This is without even thinking about Dragon's Breath shells, which will burn in the range of some of the hotter thermite reaction ranges. (To be honest, it probably is a thermite reaction, but I'd need to look into them a bit more to verify that.)
So, ultimately, the problem for a monster vulnerable to heat is that there are a lot of ways to throw burning metal at it, and let that cook it for you.
-Starke
This blog is supported through Patreon. Patrons get access to new posts three days early, and direct access to us through Discord. If you’re already a Patron, thank you. If you’d like to support us, please consider becoming a Patron.
158 notes
·
View notes
Text
youtube
Interesting video on the missing Titanic sub. While I'm sickened by individuals spending $250,000 on a tourist visit to the site of a tragedy, my anger and blame is mostly at the company (or companies!) offering such "experiences".
Even if we put aside the fact that this is a mass grave being monetized, there is a complete disregard for health and safety and risk assessment. Some libertarians are against such things, but they should be in place to protect consumers. Individuals do not necessarily understand the risks involved with such activities, even if they sign a waiver to say they do.
The sub does not have a GPS, a radio, a way to remove exhaled carbon dioxide (that we're aware of). It has limited oxygen. It would be diving to depths greater than nuclear submarines do, and we don't know if rescue vehicles can reach those depths. I'm going to guess the answer is no. It is a tiny pod with up to 5 people inside - what happens if an untrained passenger freaks out, hurts others, hyperventillates and uses up too much oxygen, etc.? The possibilities for catastrophe are endless. It's dangerous enough with trained team members on board.
Tourism to the Titanic should not be allowed, not only out of respect but because it is not safe. I've seen people argue that WW1/2 battlefields have "tourism" but these are a) generally much safer, with munition disposal procedures in place, and b) not exploiting the victims' deaths by charging a quarter of a million dollars per ticket.
This should never have been allowed and stricter controls must be put in place to prevent further tragedy and exploitation.
Edit: Want to add that some of my comments are likely incorrect, such as the lack of GPS. Please see sourced articles for facts. However such articles do describe a laughable state of the craft, which does support my message, which is that unregulated activities kill and it is deeply immoral to profit off the Titanic. Want to do research? Apply for funding, or approach a billionaire. But don't slap together a submersible and charge people to ride it.
357 notes
·
View notes
Text
writing share tag!
Oh shit, @cowboybrunch left an open tag on that beautiful excerpt of babygirl Theo being an asshole. And I'm whittling away at this short story.
Yesterday I posted the first 3.1k words of "Among the Elements," which I am revising.
Today I'm offering up 1,930 words and content warnings for DIY surgery, first-person past-tense body horror, and general Mad Science in the name of self-impregnation. It's explicit. IDK how else to tag this. Be careful.
Week 12
Wednesday
Most obvious answer has been in front of me the entire time. , Or, rather, adjacent to the experiment itself--it is within my own corpus.
Incubator biosynthetic for sake of fetus's health and safety--never designed with goal of implanation--odds of rejection significant--lower than odds of discovery if left exposed.
Will need to procure robotic assistance. Unable to perform procedure alone. Will require magnetic nerve block, suction, traction, cauterization, waste management if the procedure is successful…
Uncertain as to best incision site. If transverse, reduced risk of hernia and shorter recovery time--limited exposure to surgical site, challenging closure, risk of nerve damage.
Longitudinal…
Had I known I would be installing through a longitudinal incision I may have made different methodological decisions. Earlier installation for one. Will have to manually extract incubator at conclusion of gestation.
Worry about that later.
//
Completed risk assessment.
Incubator 49.5cm in length. Able to accommodate utilizing space in abdominal cavity.
Circumference presents concern. Material somewhat inflexible. Will have to rearrange cavity interior. Possible organ removal necessary.
//
Must be longitudinal incision. Large scar, slower recovery; fewer surgical complications due to open site, will be able to visualize organ migration.
Nothing more to consider. Prepping now. Will update after.
Thursday
Glad I'm not two centimeters shorter.
//
Anti-rejectants performing admirably. No redness at site of incision. Pain persistent but tolerable--pharmaceutical intervention will cause unwanted mutations at this stage of gestation even if our systems are not enmeshed.
Acclimating to persistent feeling of fullness and the effect it is having on the gastrointestinal and urogenital systems. Unable to rest supinated--incubator weight occludes the inferior vena cava. Pressure on diaphragm also an unforeseen concern. Several pre-surgical consideration for future application of this prototype.
//
Awakened with realization that THIS IS A PROTOTYPE.
If this doesn't kill either myself or the fetus the implication of successful implantation is phenomenal.
Of course the probability of our both expiring is significant. Compared to this afternoon the fetus's vitals are stable and strong while father vitals are stable and show hypotension and hypoxemia. Lower limb elevation with compression and oxygen adjunct resolved.
I must proceed with caution.
Friday
Limited space in hollow organs.
Have learned to vomit without use of abdominal muscles.
Longitudinal incision a terrible idea. That robot was a terrible idea. This was all a terrible idea. I am the king of terrible ideas.
//
Terrible Idea That Wasn't Terrible After All #18: program robot to feed cat in morning. Stay in bed.
She did join me, which was unforeseen. Cleaned her face for roughly an hour and then--purring--laid on my side. Desires the heat of the incubator, doubtless. Considered kicking her out of bed but felt unwell. Feel less unwell, now.
Saturday
Fetal heartrate elevated today.
Corpus temperature 38.1C.
This may be how I die. I'd always hoped it would be an explosion that did it. Or an electrical mishap.
Adjusting anti-rejectant dosage.
Sunday
Fetal heartrate returned to 110bpm. Corpus temperature reduced to 37.8C. All other systems nominal.
Would say it is easier to breathe but that would be both a colloquialism and a lie. Am however much improved compared to yesterday. Damned cat purred and refused to leave my side until I was able to remove her myself. Robot shuttled broth from the nutrient synthesizer to the bed--I've not taken in nutrients since Wednesday evening.
Thus far the onboard biometrics have reported no issues with the fetus's metabolism or gestation. Incubator nutrient system is unaffected by change in environmental conditions.
Too soon to celebrate.
Monday
Cat insists on running in front of me as I'm walking.
Blood loss within acceptable limits--stitches holding--some internal shifting that resolved with external binding. Incubator switching from internal nutrition and filtration to transplacental--connecting its vascular system to mine--a strange sensation I'm unable to put into words, knowing how like and unalike a plumbing system, it can be.
Thinking of my body as a house. Must still be delirious. Back to bed.
Week 13
Wednesday
Condition improving--post-operative pain and swelling have subsided significantly--am able to walk from one side of the apartment to the other and have attempted stairs--the incubator appears settled in the abdominal cavity.
One benefit of this arrangement is the incubator will not grow. It is sized for a 12-week-old infant. If I am careful I believe I will be able to keep the incubator hidden for the duration--either in my person, which is less than ideal, or upon returning to a secure laboratory where I can work uninterrupted to perform an extraction. Until such time, I suppose the fetus--
Continuing to refer to the experiment as "the fetus" is unideal. Will have to decide upon a more appropriate name.
Week 18
Friday
Initial consideration of healing factor accelerant not entirely baseless--however, I've decided to allow the installation site to close on its own without interfering with placental growth factor. Elastic bandage ensured the incubator did not exert excess pressure on--quite a bit of in and ex in those two sentences for there being not a lot of either, until this stage of the experiment.
Five weeks to complete closure--I should say that's nominal healing, under the circumstances. My own biology may be resistant to the experiment but it continues to perform its essential functions. Equilibrium is returning.
Final and admittedly unthought-through stage of phase I complete.
The experiment is safe.
Week 19
Monday
The temptation--the need, I would say, if I were inclined to enter hyperbole into scientific record at some point in the future. I don't need. I want to run scans on this experiment, and the frequency of that want is… overwhelming. Until this point, it would have been too early to scan. Yet that want reared its head near every week for the past month.
Today I was able to measure the fetus's development, and observed continued healthy growth and functionality. Fetus is in the 25th percentile for height and weight with no abnormalities. All vital organs and systems functioning within normal parameters. The incubator is effectively supporting fetal growth and well-being.
While the incubator itself is completely self-contained and able to produce its own hormones, mine has now joined the lymphatic and vascular systems in reducing the incubator's energy consumption.
Am uncertain what to make of this, and look forward to postpartum dissection of the incubator to determine what caused spontaneous integration.
[See supplemental data log for biometric data for week 19 fetal growth.]
//
The biometric scanner is capable of producing imagery of the fetus based on soundwaves.
I saw them. I saw them tonight. They're alive.
//
For the sake of transparency--yes. I was overcome with emotion. It would appear as though the incubator's presence within my abdominal cavity is also exerting bottom-up control over the corpus's endocrine system. I am drawn to think of abstract concepts such as embodiment and caregiving. Of how my corpus had not changed in the milliseconds before the biometric scanner produced an image of the experiment's face, but the experiment became the baby upon subjection to the observer effect. Whether that meant I, by extension, was changed. Whether I had inherited personhood with the death of my ignorance.
I was overcome. I now know everything there is to know about the baby.
I saw my child tonight.
Week 21
Monday
The temptation to perform a scan more frequently than every four weeks is maddening. I have the incubator set to alert me if anything changes--not even to suboptimal levels; any change at all--I know when the heartbeat increases, when not enough nutrients are moving through the exchange--when the baby puts their thumb in their mouth.
The only metric I have not gathered concerns their sex. All I know is they are healthy, and I have to be patient.
That sad, I am finding it increasingly difficult to focus on other projects with earlier deadlines. This requires patience, and I keep daydreaming. Knowing months are left between myself and the conclusion of this experiment--for which I was unable to gather consent from the most important participant! Not quite six months, and the difference in how I think of this baby today compared to a series of CRISPR instructions… it may be the literal internalization of my role in the infant's development, or knowing that soon they could survive outside the incubator--so much time has passed, and yet it is not near soon enough to extract the unit.
Nothing to do between here and then but gather data--and, I suppose, as the child has ears, to read to them. Or sing.
Unable to recall if my parents sang to me, when I was only a possibility. Before they sent me away. I was an agreeable child, is my recollection. The Society came for me, and appealed to my parents. They could not give me the sort of education the Society was offering to pay for, and my parents wanted to give me everything. They did not want me to have to work the way they worked.
I wish I would have argued with them. It would have made no difference. But I wish I had told them I didn't want to go.
This child deserves a promise--not to be sent away, and not to be made to be agreeable, if we are not in agreement.
Now I understand why strangers ask if other strangers want to see pictures of their babies, the new ones, all the way up to teenagerhood. I want to show everyone I pass on the street that printout of the impression of this child, the unformed features of their face, and I want to tell them, I made this. This is the only important thing I'll ever do in my life.
Week 23
Neighborhood hot when I returned from the metro. Counted no fewer than four MIB per square kilometer. Uncertain whether they're looking for me--no reason why they ought to be. Simplest and most obvious answer is someone else in the area is drawing attention to themselves. See prev entry re: Omens. Foolish to think ignoring the presence of Technocrats reduces their interest in me, should their interest be above zero. Will proceed with caution.
Week 24
Weight increased substantially, though the incubator has not changed in size. Baby has been gaining 29 grams per week, and the placenta is keeping pace with their development. Anticipate accelerated growth as the trimester continues.
Plenty to discuss, and nothing at all of note. My impatience rears when I acknowledge it; and, in acknowledging it, I have to wonder if impatience doesn't serve as this child's mother, rather than Scientific inquiry.
Week 25
I'm certain other events occurred yesterday that are worth noting. Every other day I make a new discovery, or experience a breakthrough. Were I not frightened of it being entered into evidence, I would record much more of the child's development than I have been.
I am afraid--paranoid, even--and yet.
Every ounce of fear I've felt thus far was erased by a sensation I'd never felt before--never would have felt before--replaced by what can only be described as enlightenment.
I felt like a mortal man stealing fire from the divine. One who went up the mountain sightless and returned with fire. I was, for a moment, a god.
And in that moment I was aware of the presence of life growing within my own, housed within a structure that defies reason or sanity, and I was aware because I felt. I ought not to have been able to feel--I never programmed the biopolymers to transmit information--yet they have.
This is not referred mechanoreception.
I can feel my child move.
#short story: among the elements#c: khalid#when i tell you i tina belcher groaned my way through the first half of this
21 notes
·
View notes
Note
Sorry I keep asking about the down in the deep au but I noticed you said ‘melded state’.
Is he stuck in a mix of ghost and humanish? So does he have the use of his powers but also more solid/has internal organs like a human?
Can he still fly. Important question. Can he just hover in the air?
Are his powers like normal ghost powers? Are they altered?
Also is his mental state younger as Little Baby Man?
I’m intensely curious about this. Thanks for making this crossover au!
Vibrates.
So, keep in mind this might change as I write more of the story and things develop, but how I have it right now is that technically he's always slightly both ghost and human.
For example he's always giving off ecto in either form, a human doesn't do that. He has a heartbeat in both forms, a ghost doesn't.
However, it's usually mostly separated, assisted by how Danny himself sees it as two forms. And ghosts are influenced by how they see themselves.
Now, right now it's more melded than before. He has organs like the living, a heart and lungs and everything else, he still needs oxygen. But unlike a human, it's not fully fueled by blood. There's still blood carrying oxygen, but it's not carrying any energy.
That is where the ectoplasm comes in. It's acting like the nutrients and energy everything else functions off of. Food gets broken into ectoplasm that fuels the body.
But. The ectoplasm he naturally generates is the equivalent of a ghost his age. And he's no longer near his ecto-charged death site that would be charging him up. Meaning that he can't use much of his powers.
Now the abilities he does have access to are mostly the things his human body could already use. For example super strength is limited by what he could use before risking tearing muscles, so he can't use that.
He does however, have more durability than a human, helped by the scales that have formed. He has slightly better human, due to the fact his body fueled by ectoplasm, but it's also exhausting.
He can't fly or anything, but he's practically immune to cold and pressure, the ectoplasm preventing things like his bones and organs being crushed.
Again, very limited to what he has access to because this form is new to him, and he was already previously injured and exhausted.
Actually, he does keep things like electrokinesis, photokinesis, and similar, but again, very limited. More like the shock of an electric eel than a proper manipulation. More internal manipulation than anything else, if that makes sense.
Now! Mentally. It's a mixed bag. Sometimes he acts more his previous age, especially at the beginning, but as his body and core adjusts to the new form, there's more flashes of a younger state of mind.
Not quite as young as his ghost age, but something inbetween. Closer to a 7 to 9 year old than a 14 year old human or a 2 year old ghost.
Because his form right now is a mixture of the two. If that makes sense at all lol.
#ask answered#down in the deep au#pressure crossover#danny phantom crossover#roblox pressure#danny phantom#Don't worry I enjoy asks#Glad you're enjoying it <3#Sebastian is very concerned about this kid
46 notes
·
View notes
Text
The Sign of Four: The Baker Street Irregulars
I'm rather behind with these and will be for a while.
London had many, many wharfs; the number topped out at around 1,700.
London would have had a huge number of boats and ships of varying types plying the Thames at this point, moving cargo and people back and forth - it could be quicker than going by horse depending on the traffic. Today, the number is far smaller, mostly consisting of tourist vessels, the Thames Clipper passenger services that are part of the TfL network and tenders carrying rubbish.
Coke is a hard, grey fuel created by heating coal or oil in the absence of oxygen. It produces much less smoke than regular coal, allow most homes and other operations didn't use it at this point. Hence the yellow fog...
It takes quite a while to warm up a steam boiler; you're generally looking at two to three hours for a steam locomotive before it can be used.
A wherry is a small boat with a sail and oars used for transporting people on rivers like the Thames. The long bow makes it easier for passengers to get on and off on a shoreline without getting their shoes wet.
Millbank Penitentiary was a prison that had formerly held those due to be transported to Australia and then became a local prison, followed by a military one. It had ceased to hold prisoners in 1886, closed entirely in 1890 and was mostly demolished soon after that. Many of its red bricks were reused for housing as the Millbank Estate and the Tate Britain is also on the site.
"A tanner" is six pence, or half a shilling. "Three bob and a tanner" means 3 shillings and six pence, which is what Wiggins paid for the bus tickets.
Not sure about the whole sandal thing, but the Special Operations Executive, themselves known as the "Baker Street Irregulars" due to their HQ's location, developed special overshoes in the shape of bare feet to deceive the Japanese into thinking they were barefooted locals when leaving footprints.
Bushmen is an older and still sometimes used term for the San people of southern Africa, one of the oldest hunter-gatherer peoples on the planet. Much of the rest of the stuff about height seems a lot of racist rubbish.
#letters from watson#sherlock holmes#history#factoids#acd canon#the sign of four#sign#hungry like the wharf
23 notes
·
View notes
Text
Reliable On-Site Oxygen Generators by Absstem Technologies
The On-Site Oxygen Generators from Absstem Technologies will increase your operational efficiency. Our oxygen generating systems are meant for use in hospitals, factories, and laboratories to supply high purity oxygen round the clock at your convenience. Cut down the business’s dependency on outside suppliers and minimize the expenses by utilizing our advanced innovation. Oxygen generation is now easier and more affordable with Absstem Technologies; get in touch with us today to find out more.
0 notes
Text
Medical oxygen plant manufacturers
Medical oxygen plant manufacturers typically use a process called pressure swing adsorption (PSA) to separate oxygen from air. This involves compressing air and passing it through a molecular sieve that traps nitrogen and other gases, leaving behind concentrated oxygen. The oxygen is then purified to remove any remaining impurities before it is bottled or piped directly to the hospital or medical facility.
0 notes
Text
PSA medical oxygen generator
PSA Medical oxygen generators are essential for hospitals and clinics, especially in areas where there may be a shortage of oxygen cylinders or where it may not be feasible to transport large quantities of oxygen. These generators are also useful during emergencies or disasters, where a steady supply of oxygen is critical.
0 notes
Text
Waking up and recovery
Masterlist
So you're all stitched up, but you're still asleep? Guess we'd better wake you up then!
This either happens in the operating room or in recovery, but is mostly the same. The anaesthetist turns off the anaesthetic gas and gives a muscle relaxant reverser. Then you just wait.
Usually within 15 minutes the patient will start waking up. Everyone is slightly different. Some people will flap their hands a bit but are still asleep, others wake up all at once.
What you're looking for is that they can follow a basic command - opening their eyes, squeezing a hand, lifting their head up. This is proof that they can protect their airway and it's safe to remove the et tube.
The cuff on the tube gets deflated and the tube is just pulled out. It usually smells a bit gross by the way. An oxygen mask goes on immediately, and if they get laryngospasm (the vocal chords spasm) then we give positive pressure (force oxygen into their lungs with a bag).
If they were woken up in the OR, they'll go to recovery now. The anaesthetist will bugger off really fast once the tube's out, and the recovery practitioner takes over.
Most patients are very very sleepy after anaesthesia. This is generally fine and makes it easier to do all the paperwork. The recovery nurse will take observations every five minutes, and will look at the surgical site to check for bleeding.
If everything's peachy then the patient will go back to the ward after 30 minutes, otherwise we just wait until all their vital signs are stable and there's no signs of deterioration. If the patient's in a lot of pain they'll get some pain relief (usually morphine).
Congrats! The journey's finished! (well, in the surgical department anyway)
34 notes
·
View notes
Note
okay I'm trying to write something with anesthesia, are local/general anesthetics the same drug or different ones? and does local anesthetic have to be injected in a specific thing? like general has to be a vein iirc but idk if the exact location matters with local. thank you!
Great question!
There are actually a lot of different forms of anesthesia and they are all super interesting in how they work. Below is a selection:
General Anesthesia:
General anesthesia is the kind most folks are familiar with. In general anesthesia, a patient is given a mix of drugs that cause them to be unconscious, paralyzed, and free from pain. Some of these drugs, like fentanyl (pain med), propofol (sedative), or succinylcholine (paralytic), can be given intravenously. Others are gasses that must be breathed in order to work. Most of the time, a combination of IV and inhaled medications are used.
When unconscious and paralyzed, a person cannot breathe for themself (an exception being when ether is the only drug used). A ventilator along with oxygen and other drugs are used to keep the person alive, and their blood pressure, heart rate, temperature, and oxygen saturation are constantly monitored while they are under general anesthesia.
The person who administers anesthetic medication and monitors the patient during surgery is either a doctor (anesthesiologist) or a specially trained nurse practitioner (nurse anesthetist).
Procedural Sedation:
Procedural sedation is a little like general anesthesia "lite". It is usually used when there is a short procedure that is painful or very unpleasant (like setting a simple fracture, performing cardioversion, some wound debridement, or performing a colonoscopy), but that doesn't require paralysis or cutting the person open.
In procedural sedation, the person is given one or more drugs intravenously to decrease pain and anxiety (fentanyl, , which usually causes them to become very drowsy. The person is still somewhat conscious and is able to follow commands, but probably will not remember the procedure.
Generally, the person under procedural sedation is able to control their own airway and breathe for themself, and only requires monitoring and some supplemental oxygen. Procedural sedation can be given by a critical care nurse.
Local Anesthesia:
Local anesthesia numbs a particular small area of the body, usually so that a procedure can be performed. Procedures under local anesthesia tend to be fairly small, like biopsies, mole removals, suturing a cut, and cyst removals. In local anesthesia, the drug is injected directly into the site where the procedure will take place.
Local anesthetic agents are very different from the drugs used for general anesthesia or procedural sedation. These include lidocaine or bupivicaine (which prevent nerves from being able to send signals, thus being unable to send pain signals), usually mixed with epinephrine (which makes blood vessels in the area smaller, decreasing blood loss and making the drugs last longer).
Local anesthesia does not by itself impair consciousness. However for some procedures a combination of local anesthesia and procedural sedation might be used, especially if there are unpleasant components to the procedure that aren't just pain.
Local anesthesia is usually administered by the doctor or advanced practice provider that is performing the procedure.
Nerve Block/Regional Anesthesia:
Nerve blocks are cool. They use largely the same drugs as local anesthesia, but instead of being injected directly into the location where a procedure will take place (which can only be a limited size), they are injected into the area around the main nerve conduit that serves a particular part of the body. This makes everything served by that nerve (say, a whole leg for example) numb.
This is useful for limb surgeries when a person might not be a good candidate for general anesthesia, or for reducing pain after an injury or surgery. Like local anesthesia, nerve blocks don't make people drowsy, but they can be combined with procedural sedation if needed for larger, more unpleasant procedures.
A nerve block is usually placed by an anesthesiologist.
Epidural/Spinal Anesthesia:
Epidurals or spinal blocks are a special type of nerve block. Instead of being injected around a bundle of nerves, the same type of medication is injected either around the sac that houses the spinal cord (epidural), or directly into that sac (spinal). This involves sticking a long needle in between the bones of the spine to get the medicine where it needs to be.
These work very well for painful things like childbirth, cesarean section, or other lower abdominal/pelvic/lower body surgery. Epidurals are a little safer since they don't actually pierce the sac, but they do take longer to take effect. In contrast, spinals work immediately.
An epidural catheter or spinal is usually placed by an anesthesiologist or other advanced practice provider.
85 notes
·
View notes
Text
Space Shuttle Development, Phase B: North American Rockwell and General Dynamics B9U/NAR-161-B



North American and General Dynamics B9U / NAR-161-B proposed their final Phase B shuttle proposal on June 25, 1971.


"The fully reusable 'B9U / NAR-161-B' configuration would now weigh 2,290t at liftoff vs. the Phase-A limit of 1,587t and the total estimated cost of the development project had doubled, to almost $10 billion. The thrust of the space shuttle main engines had to be increased from 1,850KN to 2,450KN. Part of the problem was the shuttle now would have to be a much more versatile and capable vehicle than originally anticipated, since the space station and the manned lunar/planetary program evaporated in 1970. Critics in Congress contended that it was 'a project searching for a mission.' As a result, the new space transportation system was instead increasingly being promoted as a low-cost 'space truck' for unmanned NASA & USAF satellites."
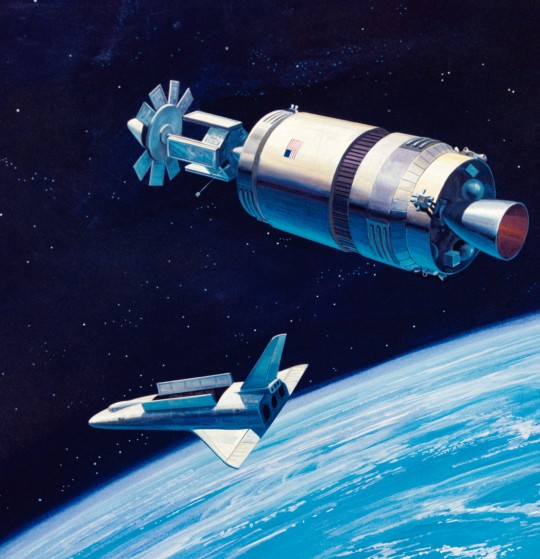

"The North American Rockwell 'NAR-161-B' orbiter was designed for carrying a crew of two plus up to ten passengers in the forward crew module. Note the four deployable landing jet engines on top of the vehicle; NASA was planning to use modified F-15 or B-1B aircraft jet engines on some missions and for ferry flights from test sites or alternative landing fields. But the jets would be omitted for heavy-lift missions since the additional weight greatly reduced the shuttle's payload capability. The thermal protection system was based on silica tiles. The blended wing/body design was chosen for uniform load distribution. It would have produced a 2300-kilometer crossrange capability to satisfy USAF reentry requirements; North American also decided to replace the wingtip fins with a single vertical tail. The 2,450KN main engine thrust upgrade was motivated in part by the need to have a single engine-out abort capability. Analysis showed that the orbiter still would be able to return to the launch site after a single orbit in case one of its two main engines failed during ascent, but only if the engines were powerful enough. Unlike McDonnell-Douglas (who proposed to use RL-10s), North American favored a brand new oxygen/hydrogen 45KN-thrust orbital maneuvering system (OMS) engines. Three OMS engines would have been carried for orbit insertion, orbital changes and the de-orbit burn."

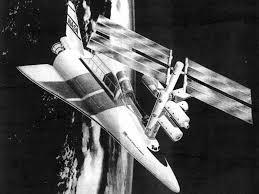
"General Dynamics' final 'B9U' booster design differed considerably from the earlier straight-wing 'B8D' concept. The landing jets were moved from the nose back to the delta wing in order to reduce the launch drag & heating effects and to minimize the jet engine exhaust effects on stability, control and drag. General Dynamics felt the delta wing would provide better stability & control over the entire flight regime than the B8's straight wing. It would also create more room for the main landing gear and jet engine installation. The gross liftoff mass was 1,886.2t including a jet fuel load of 62.2t for the 850km flight back to the launch site. The high staging velocity (3300m/s) and altitude (73.8km) created some problems since the booster would have to be very large, require a relatively advanced thermal protection system and carry lots of jet fuel for the return flight. The contractors also examined downrange landing sites or in-flight propellant transfer in order to reduce the amount of booster jet fuel. NASA also seriously considered a proposal to use gaseous hydrogen rather than jet fuel since it would have saved thousands of kilograms, but decided against the idea in the end since it would have increased the technical risk."
North American Rockwell Phase-B shuttle orbiter docks with modular space station.
"Payload capability (without landing jets): 29,484kg into a 185km 28.5 deg. Orbit; 18,144kg into a 185km 90 deg. polar orbit; 11,340kg into a 500km 55 deg. orbit with landing jets installed on orbiter and 20,411kg without landing engines.
Cost per mission: $100-200/lb. [1970 rates] or $950-$1900/kg in 1999. 75 missions/year max. Space station rescue mission capability within 48 hours of emergency call.
Liftoff Thrust: 2,606,810 kgf. Total Mass: 2,188,488 kg. Core Diameter: 10.4 m. Total Length: 98.0 m.
Stage Number: 1. 1 x Shuttle R134C-1 Gross Mass: 1,886,200 kg. Empty Mass: 290,000 kg. Thrust: 29,370-32,233.575 KN. Isp: 442 sec. Burn time: 209 sec. Isp(sl): 392 sec. Diameter: 10.4 m. Span: 43.9 m. Length: 82 m. Propellants: Lox/LH2 No Engines: 12. SSME Study
Stage Number: 2. 1 x Shuttle R134C-2 Gross Mass: 383,260 kg. Empty Mass: 121,560 kg. Thrust (vac): 5,624.8 KN. Isp: 459 sec. Burn time: 264 sec. Isp(sl): 359 sec. Diameter: 4.6 m. Span: 32.6 m. Length: 62.8 m. Propellants: Lox/LH2 No Engines: 2. SSME Study

- information from "INTRODUCTION TO FUTURE LAUNCH VEHICLE PLANS [1963-2001]" by Marcus Lindroos: link
SDASM Archives: 08_00941, 08_00943, 08_00944
Mike Acs's Collection: link, link
Numbers Station: link, link, link, link, link
source
Boeing image: 71SV13043
#Space Shuttle Development#Phase B#North American Rockwell General Dynamics B9U/NAR-161-B#North American RockwellNAR-161-B#NAR-160-B#General Dynamics B9U#concept art#Space Shuttle Phase B#Space Shuttle#Orbiter#NASA#Space Shuttle Program#June#1971#B9U#my post
59 notes
·
View notes
Last Seen Blogs

musicistheair-blog
Music Is The Air

mandydotexe
mandy.exe

sl-shopomania
Sl-shopomania

harrystyles-music
Harry Styles

ohmygoodtea-blog
Untitled